the second thing you should think about at every ... · think about at every deliverythink about at...
TRANSCRIPT
The Second Thing You Should Think About at Every DeliveryThink About at Every Delivery
T dd R L MD FACOGTodd R Lovgren, MD FACOGMethodist Perinatal Center
Methodist Women’s HospitalMethodist Women s Hospital6/14/2013
DisclosuresDisclosures
N l t fi i lNo relevant financial relationships.relationships.
ObjectivesObjectives
U l i f thi t ti thUpon conclusion of this presentation, the participants should be able to:• Identify patients at risk for shoulder dystocia (ShD).• Discuss the use of ultrasound in macrosomia and ShD.• Discuss the impact of diabetes on ShD.• Describe the standard and alternative maneuvers to
l ShDresolve a ShD.• Discuss appropriate documentation and follow-up
when ShD is encounteredwhen ShD is encountered.
Shoulder DystociaShoulder Dystocia Background
• Difficult vaginal delivery of the fetal shoulder.A delivery requiring additional obstetric maneuvers– A delivery requiring additional obstetric maneuvers following the failure of gentle downward traction on the fetal head to effect delivery of the shoulders.
• Rates of occurrence:– All deliveries: 0.6% to 3.0%– BW>4500g: 9.2-24%– BW>4500g + DM: 20-50%
• Majority occur in infants of normal BW.
Shoulder DystociaNeonatal Complications
• Brachial Plexus Injuries (4 40% of all ShD)• Brachial Plexus Injuries (4-40% of all ShD)– Most resolve w/o permanent disability by 1 year
• <10% permanent injury10% permanent injury– 34-47% of all brachial plexus injuries are NOT
associated with ShD– 4% of brachial plexus injuries occur at C/S– Posterior ShD does occur
Cla icle fract re (0 5% of all deli eries)• Clavicle fracture (0.5% of all deliveries)– 10X risk with macrosomia
• Humeral fracture• Humeral fracture• Hypoxic-ischemic encephalopathy / Death
Can Shoulder DystociaCan Shoulder Dystocia Be Predicted Accurately?
• Risk FactorsAntepartum– Antepartum
– Intrapartum Ult d• Ultrasound– Estimated Fetal Weight (EFW)– Biometric ratios
Shoulder DystociaRisk Factors - Antepartum
• Macrosomia• Macrosomia– Maternal obesity
• BW increases with maternal BMI.• More likely to be diabetic• Excessive pregnancy weight gain
Previous macrosomic infant– Previous macrosomic infant– Postdates– MultiparityMultiparity– Diabetes
• Diabetes - pregestational & gestationalabe es p eges a o a & ges a o a• Prior shoulder dystocia
Excessive Fetal Growth
LGA M iLGA vs Macrosomia• LGA: BW ≥ 90th percentile for GA
• Pediatric diagnosis• Macrosomia: Ultrasound estimated weight
greater than cut-off• 4000g vs 4250g vs 4500g vs 5000g
What estimated fetal weight cut off do you use definecut-off do you use define
macrosomia?
A 4000gA. 4000gB. 4250ggC. 4500gD 5000D. 5000g
MacrosomiaD fi i iDefinition
• Growth beyond a specific weight regardless of y g ggestational age: >4000g or >4500g– Morbidity of infants and mothers
• 4000 4500g: greater than general ob population• 4000 – 4500g: greater than general ob population• >4500g: sharply increased
– Parallel increase in birth injuriesUsher 1988Usher, 1988
– 10-20% incidence of BW >4000g– 3% incidence of BW >4500g
P ll k 1992 Ed 1987Pollack, 1992; Eden, 1987
– ACOG suggested definition: >4500g
• Important: Be consistent in your own definition and p ythis is not/should not be the same threshold to recommend primary CD
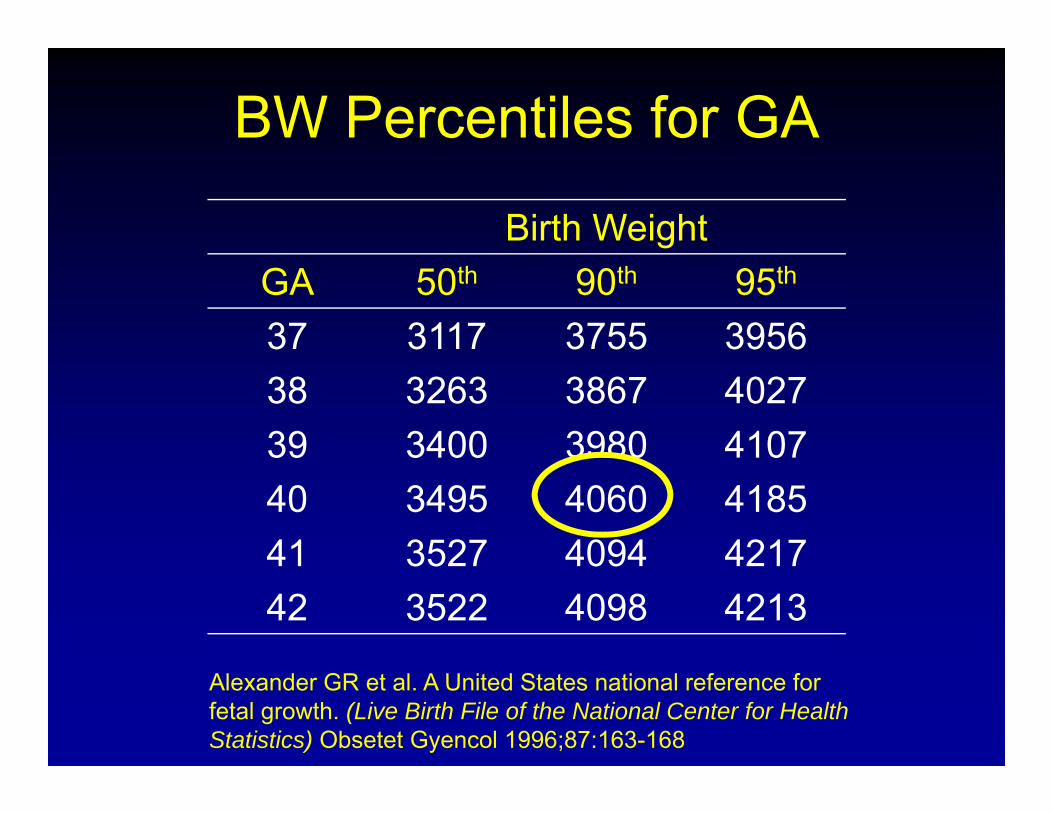
BW Percentiles for GA
Birth WeightGA 50th 90th 95th
37 3117 3755 395638 3263 3867 402739 3400 3980 410740 3495 4060 418541 3527 4094 421741 3527 4094 421742 3522 4098 4213
Alexander GR et al. A United States national reference for fetal growth. (Live Birth File of the National Center for Health Statistics) Obsetet Gyencol 1996;87:163-168
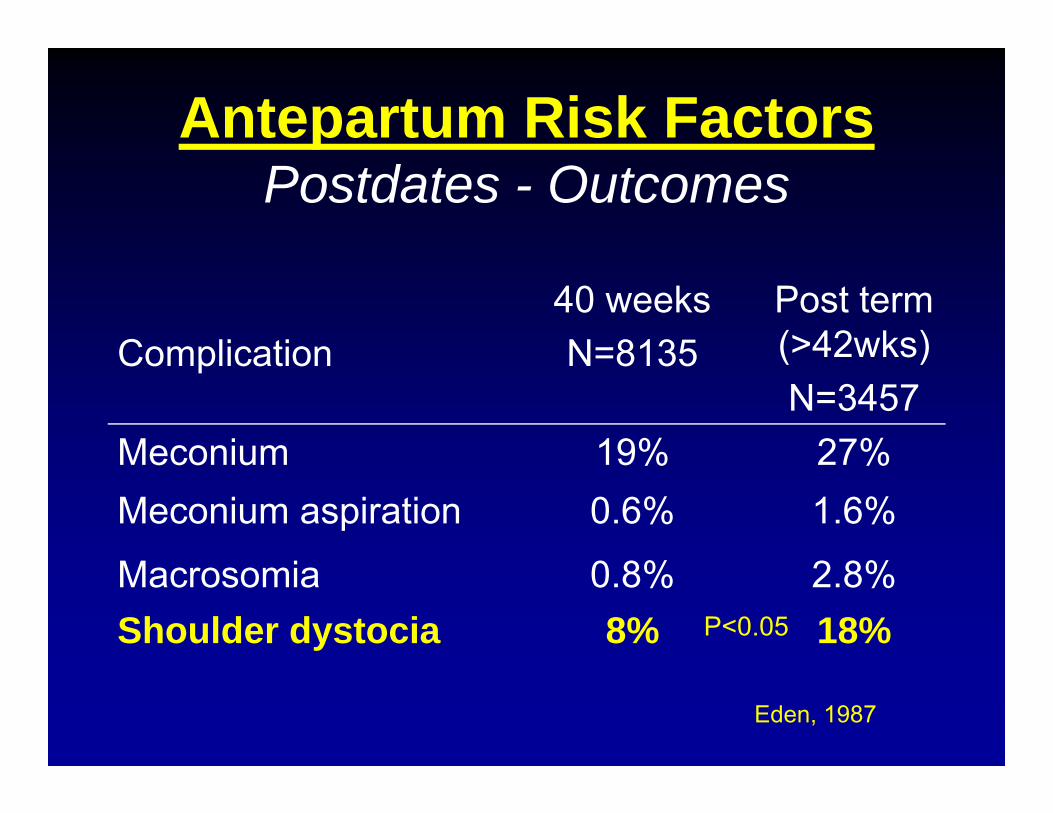
Antepartum Risk FactorsPostdates - Outcomes
Complication40 weeksN=8135
Post term (>42wks)Complication N=8135 ( 42wks)N=3457
Meconium 19% 27%Meconium 19% 27%Meconium aspiration 0.6% 1.6%
M i 0 8% 2 8%Macrosomia 0.8% 2.8%Shoulder dystocia 8% 18%P<0.05
Eden, 1987
Other IntrapartumOther Intrapartum Considerations
• Abnormal 1 hour normal 3 hour• Excessive weight gainExcessive weight gain• Obese patient
P i i i f t• Prior macrosomic infant
Shoulder DystociaShoulder DystociaRisk Factors - Intrapartum
Reported Risk FactorsReported Risk Factors
• Epidural anesthesia → No!p
• Labor dystocia
• Operative vaginal delivery
Do LaborDo Labor Abnormalities Predict S ?Shoulder Dystocia?
• Three studies have specifically addressed labor patterns in patients who develop shoulder dystocia.
McFarland et al. AJOG 1995;173:1211-4Gemer et al. Acta Obstet Gynecol Scan 1999;78:735-6Gemer et al. Acta Obstet Gynecol Scan 1999;78:735 6Lurie et al. Am J Perinatol 1995;12:61-2
Shoulder DystociaShoulder DystociaLabor Abnormalities
• Data are inadequate to answer this question:– McFarland et al.; 276 ShD cases matched with 600
controls; no association
– Gemer et al.; 36 ShD; significant association
– Lurie et al ; 52 ShD cases; no association– Lurie et al.; 52 ShD cases; no association
• Anecdotally → still serve as a red flag
Is there a different definition for macrosomia in the diabeticfor macrosomia in the diabetic
patient?
A YesA. YesB. No
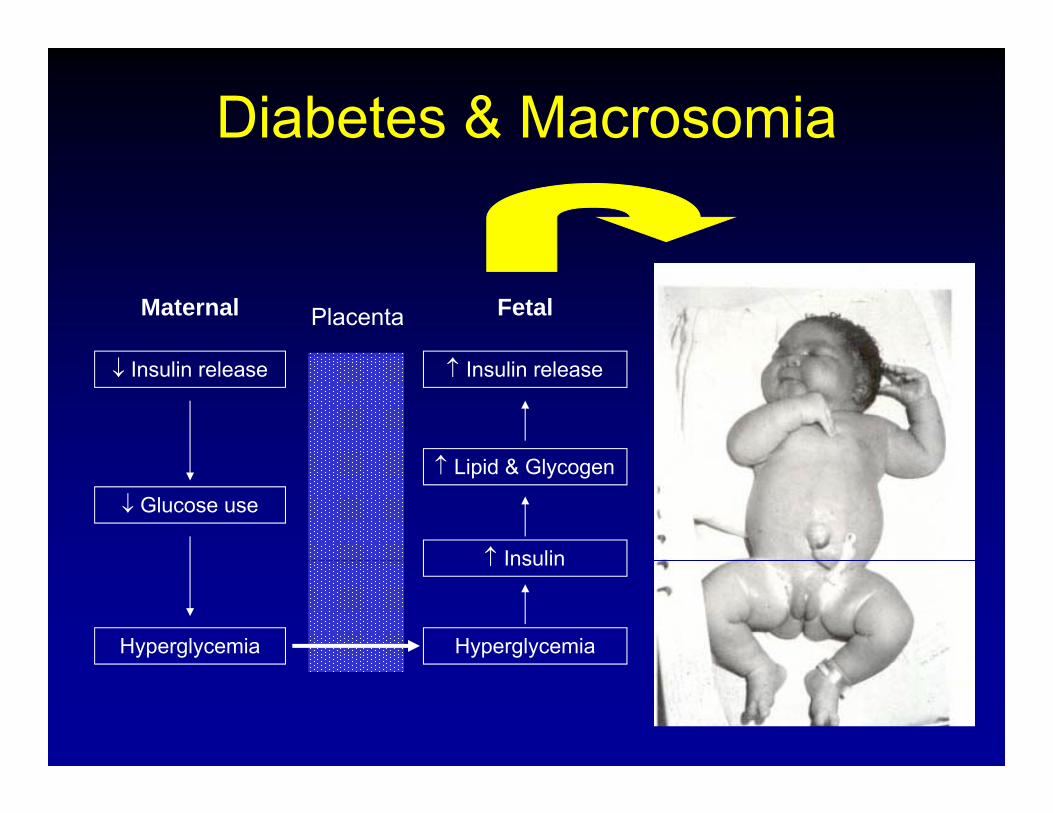
Diabetes & Macrosomia
Maternal FetalPlacenta
↓ Insulin release ↑ Insulin release
↑
↓ Glucose use
↑ Lipid & Glycogen
↑ Insulin
Hyperglycemia
↑ Insulin
Hyperglycemia
Diabetes & Shoulder DystociaDiabetes & Shoulder Dystocia
*
In the diabetic patient, what fetal weight cut off do you usefetal weight cut-off do you use
to offer cesarean delivery?y
A 4000gA. 4000gB. 4250ggC. 4500gD 5000
ACOG
D. 5000g
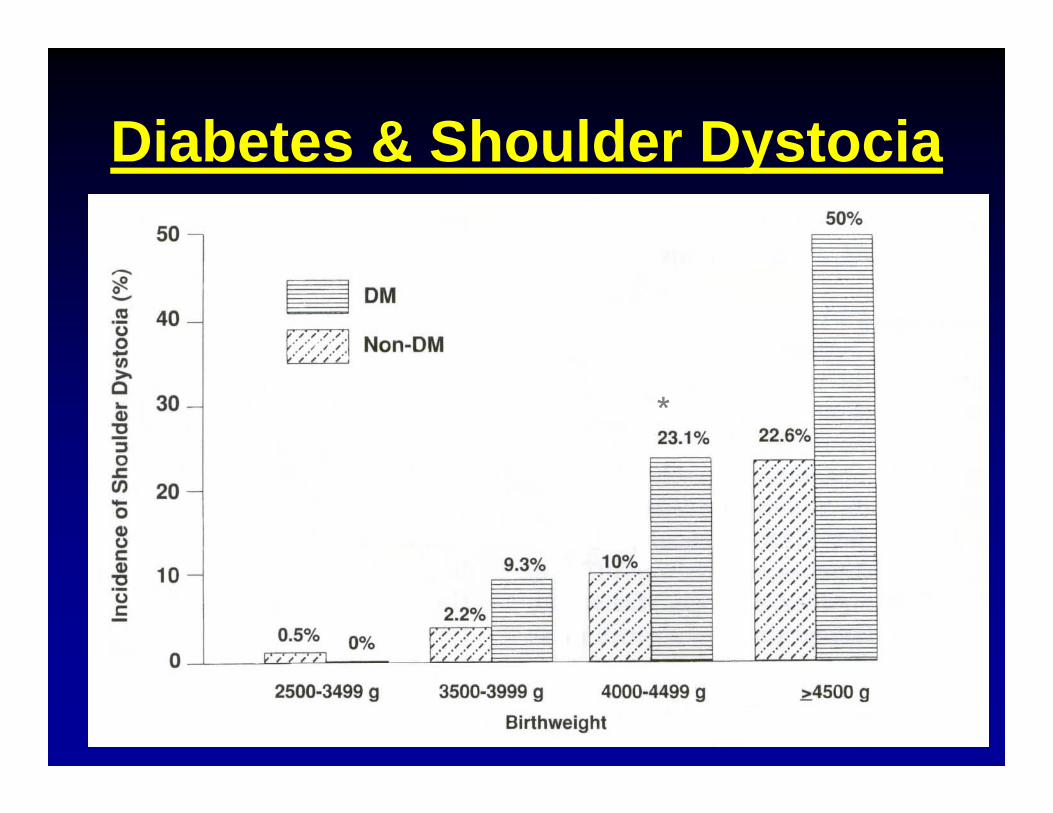
Shoulder DystociaShoulder DystociaDiabetes
• 3-9% in diabetics compared with 0.2-2.8% in non diabeticsnon-diabetics
• > 4000 gms 18-23%
• > 4500 gms ~50% (14-25% in non-diabetics)
• Brachial plexus injury (Erb’s palsy) clavicular• Brachial plexus injury (Erb s palsy), clavicular fracture, hypoxia, low Apgar scores
Uvena-Celebrezze and Catalano Clin Ob Gyn 2000; 43:127-139
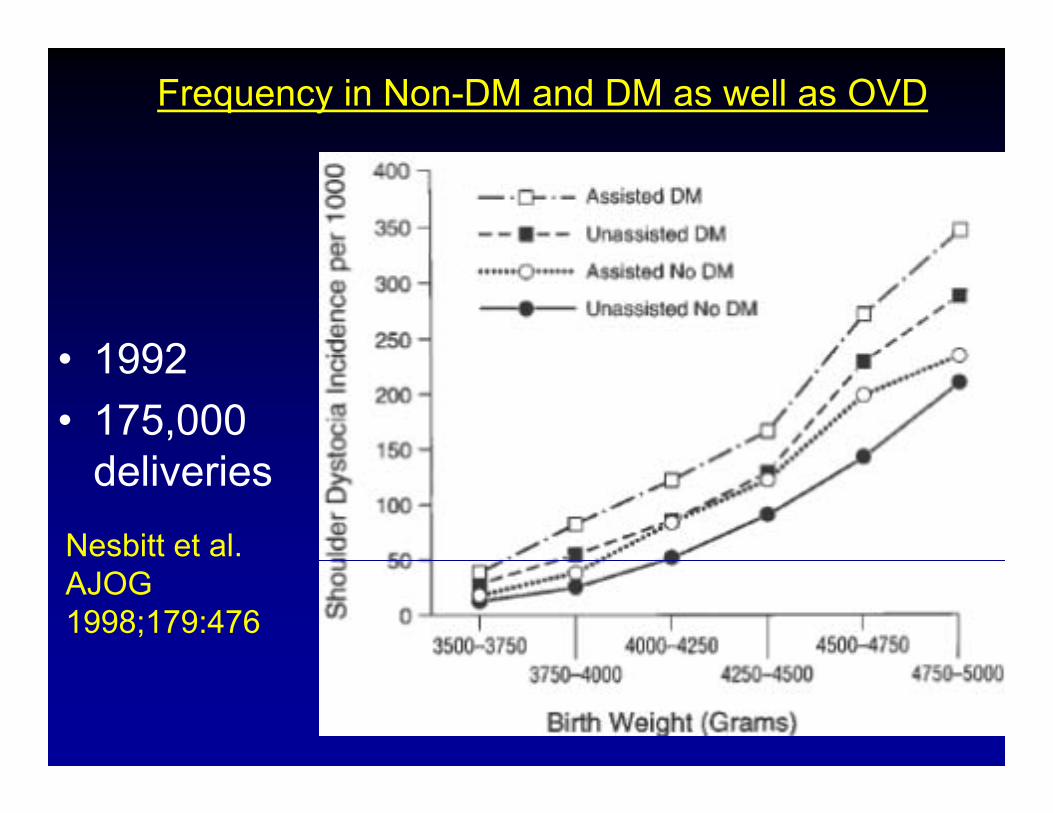
Frequency in Non-DM and DM as well as OVD
• 1992• 1992• 175,000
d li ideliveriesNesbitt et al. AJOG 1998;179:476
Can Ultrasound PredictCan Ultrasound Predict Shoulder Dystocia?
Macrosomia & UltrasoundMacrosomia & UltrasoundEFW• EFW– >50 formulas
– ideally 3 parameters
• Sheppard Formula (AC & BPD)pp ( )– 50% time-- 5% of true fetal weight
– 80% time-- 10% of true fetal weight80% time 10% of true fetal weight
– 20% time-- >10% discrepancy from weight
Ultrasound overestimates the FW/BW• Ultrasound overestimates the FW/BW
Macrosomia and Ultrasound
• 2002 Best et al– Retrospective– 1690 controls, 133 Diabetics
• EFW at 34-37 weeks is extrapolated pusing Alexander growth curve
• Mean absolute error 7.4% +/- 6.3%
US EFW* [Mean BW at delivery/Mean BW at current EGA] = EFW at delivery
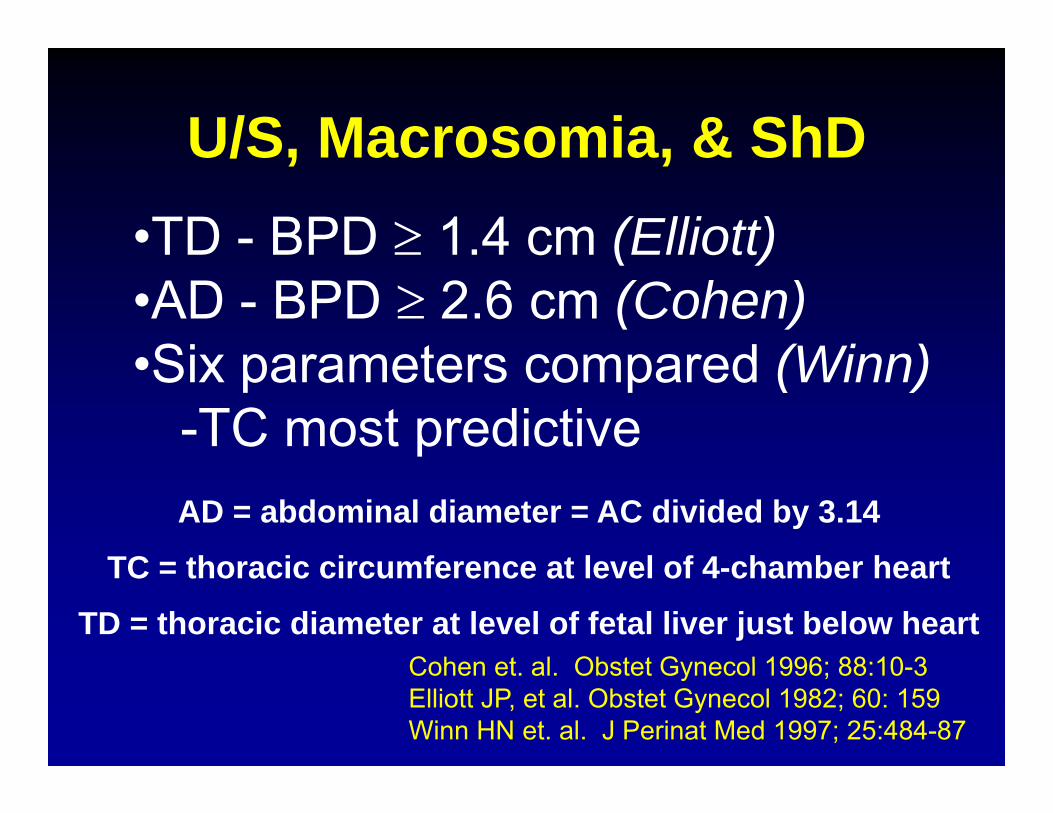
U/S, Macrosomia, & ShDU/S, Macrosomia, & ShD•TD - BPD ≥ 1.4 cm (Elliott)TD BPD ≥ 1.4 cm (Elliott)•AD - BPD ≥ 2.6 cm (Cohen)Six parameters compared (Winn)•Six parameters compared (Winn)-TC most predictive
TC th i i f t l l f 4 h b h t
AD = abdominal diameter = AC divided by 3.14
TC = thoracic circumference at level of 4-chamber heart
TD = thoracic diameter at level of fetal liver just below heartCohen et al Obstet Gynecol 1996; 88:10 3Cohen et. al. Obstet Gynecol 1996; 88:10-3Elliott JP, et al. Obstet Gynecol 1982; 60: 159Winn HN et. al. J Perinat Med 1997; 25:484-87
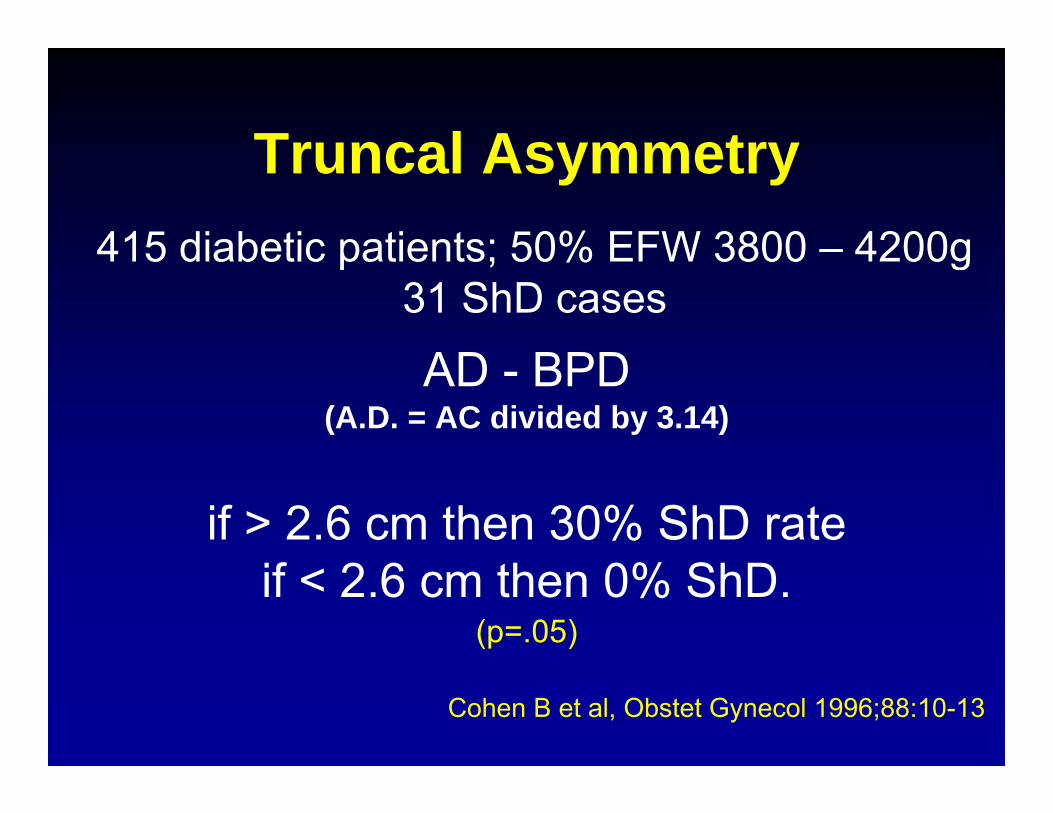
Truncal Asymmetry415 diabetic patients; 50% EFW 3800 – 4200g
Truncal Asymmetry415 diabetic patients; 50% EFW 3800 4200g
31 ShD cases
AD BPDAD - BPD (A.D. = AC divided by 3.14)
if > 2.6 cm then 30% ShD rateif < 2.6 cm then 0% ShD.
(p=.05)
Cohen B et al, Obstet Gynecol 1996;88:10-13
Cohen “Index”
• Follow up study in 1999 – Diabetics Only
• Normalized for GA– Determined “residual” AD-BPD
• Unpublished nomogram for “residual AD-BPD”
– Three categories10 20 and 34% risk of ShD– 10, 20 and 34% risk of ShD
– Third group was associated with necessity for advanced maneuvers
• Req post arm or Wood’s maneuver
Shoulder DystociaWhat to tell patients?
• X:100, (x%) risk of shoulder dystocia– 1:10 (10%) risk of BPI– 1:10 (10%) risk of permanent injury
3% risk of ShD=Roughly 1/3333 chance of permanent BPIRoughly 1/3333 chance of permanent BPI
*This is based on extrapolation from multiple studies
Where Do I get the ‘X’
I give patients 3 estimates and provide a range. i.e. 9-34% chanceg
• California population data– Nesbitt et al AJOG 1998;179:476– Nesbitt et al. AJOG 1998;179:476
• EFW based on Best calculationT l A t• Truncal Asymmetry
Does labor induction for suspected fetal macrosomiasuspected fetal macrosomia
affect the risk of ShD or brachial l i j ?plexus injury?
Does Labor Induction for suspected fetal macrosomia affect the risk of
ShD or brachial plexus injury?ShD or brachial plexus injury?
St di di id d i t 3 t iStudies are divided into 3 categories:1. Induction for macrosomia in non-DM2. Induction for macrosomia in DM3 I d ti f ti f3. Induction for prevention of
macrosomia in DM
Shoulder DystociaShoulder DystociaLabor Induction for Macrosomia (non-DM)
• Management of suspected macrosomia is t i lcontroversial
• Elective C/S and labor inductions have been proposed interventions to prevent maternal and fetal M&M.
• 3600 C/S required to prevent 1 permanent neonatal injury.
Rouse et al. JAMA 1996;276:1480-6
Shoulder DystociaLabor Induction for Macrosomia (non-DM)
• Expectant Management Versus Labor Induction for Suspected Fetal Macrosomia in non-diabetics
• 11/29 studies met inclusion criteria– 9 observational studies
– 2 randomized clinical studies
• 3751 patients (2700 Exp Mgmt; 1051 Indxn)p ( p g )
• Metanalysis; OR & 95% CI
• Primary outcomes: delivery mode & perinatal outcomePrimary outcomes: delivery mode & perinatal outcomeRamos et al. Obstet Gynecol 2002;100:997-1002
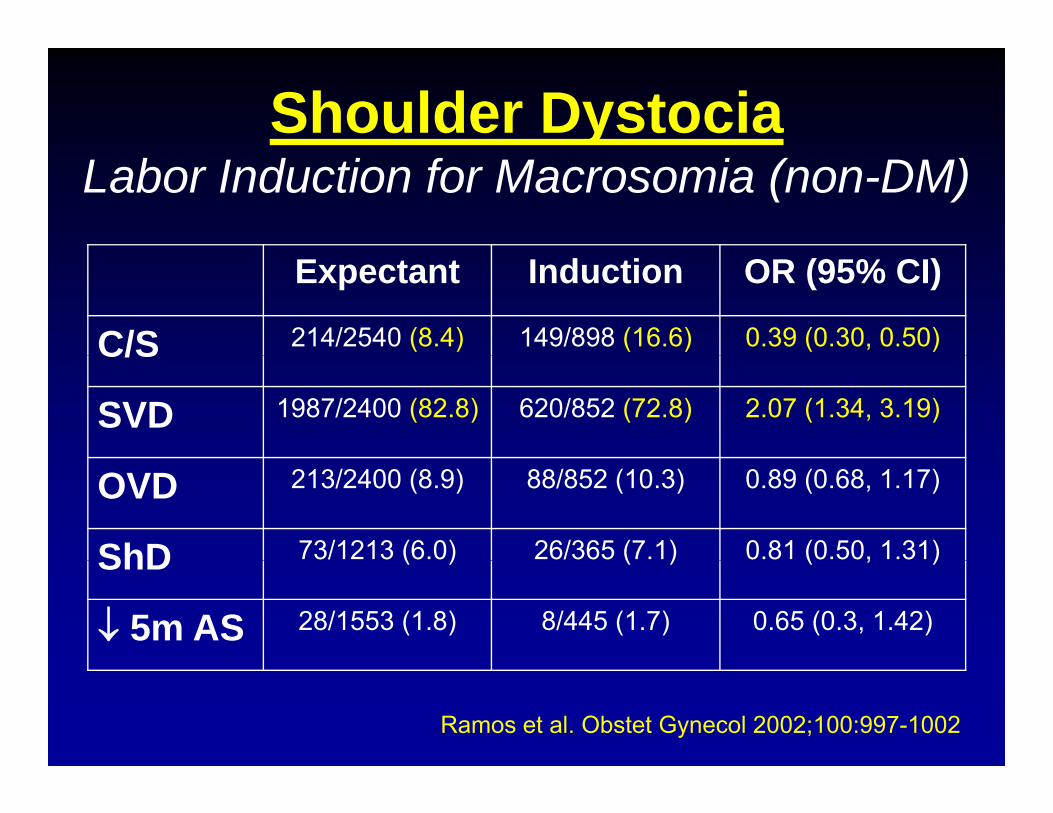
Shoulder DystociaLabor Induction for Macrosomia (non-DM)
Expectant Induction OR (95% CI)
C/S 214/2540 (8.4) 149/898 (16.6) 0.39 (0.30, 0.50)C/S
SVD 1987/2400 (82.8) 620/852 (72.8) 2.07 (1.34, 3.19)
OVD 213/2400 (8.9) 88/852 (10.3) 0.89 (0.68, 1.17)
ShD 73/1213 (6.0) 26/365 (7.1) 0.81 (0.50, 1.31)ShD ( ) ( ) ( , )
↓ 5m AS 28/1553 (1.8) 8/445 (1.7) 0.65 (0.3, 1.42)
Ramos et al. Obstet Gynecol 2002;100:997-1002
Labor Induction for Macrosomia Diabetic Patient
L b i d ti t 38 39 k f• Labor induction at 38-39 weeks for:– Macrosomia or LGA to prevent injury– Prevention of macrosomia
• Reduction in:– BW without a significant ↑ in C/S– LGA & macrosomia without a significant ↑ in C/Sg– ShD without at significant ↑ in C/S
Conway and Langer AJOG 1998; 178:922 5
Kjos SL et al, AJOG 1993; 169: 611-15Lurie et al. Am J Perinatology 1996; 13:293-6Conway and Langer. AJOG 1998; 178:922-5
Strategies for prevention of shoulder dystocia in diabetics
• Induction of labor when LGA fetus is suspectedInduction of labor when LGA fetus is suspected, especially if cervix favorable
I l i t l t d i• Improve glycemic control to reduce macrosomia
• Improve prediction of shoulder dystocia– reevaluate use of Cohen and Elliott criteria
• Avoid operative vaginal deliveryp g y
• Elective C/S: DM: >4250 or >4500
(Non DM: >5000g)(Non-DM: >5000g)
H h ld ithHow should a woman with a previous shoulder dystocia beprevious shoulder dystocia be
counseled regarding ?subsequent deliveries?
Shoulder DystociayThe next pregnancy
• Rate of recurrence:– 1-16%, BUT, difficult to determine
• Most subsequent deliveries free of ShDBenefit of universal elective C/S?– Benefit of universal elective C/S?
• Other factors to dictate mode of delivery– EFW; gestational age; DM; severity of prior injury
• Discuss and review of prior deliveryp y• Either method of delivery is appropriate
What Do I Do When A Sh ld D t i IShoulder Dystocia Is
Encountered?Encountered?
Shoulder DystociaManeuversManeuvers
• Be prepared and be able to recognize!• Be prepared and be able to recognize!• Take a deep breath & note the time• Marshall your resources GET HELP• Marshall your resources – GET HELP• Episiotomy if necessary to access pelvis!!• McRobert’s maneuver & suprapubic pressure• McRobert s maneuver & suprapubic pressure• Wood’s screw & Rubin maneuvers• Delivery of posterior arm• Delivery of posterior arm• Zavanelli
(Fracture Clavicle)• (Fracture Clavicle)• (Symphysiotomy)
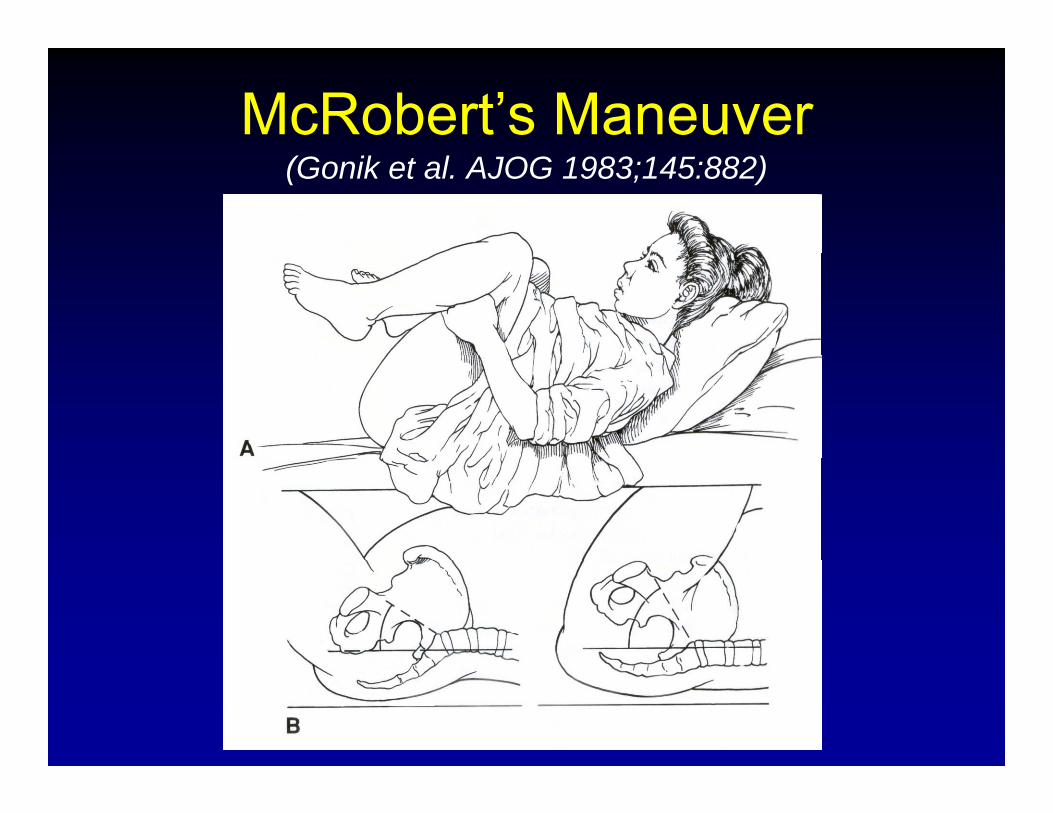
McRobert’s Maneuver(Gonik et al. AJOG 1983;145:882)
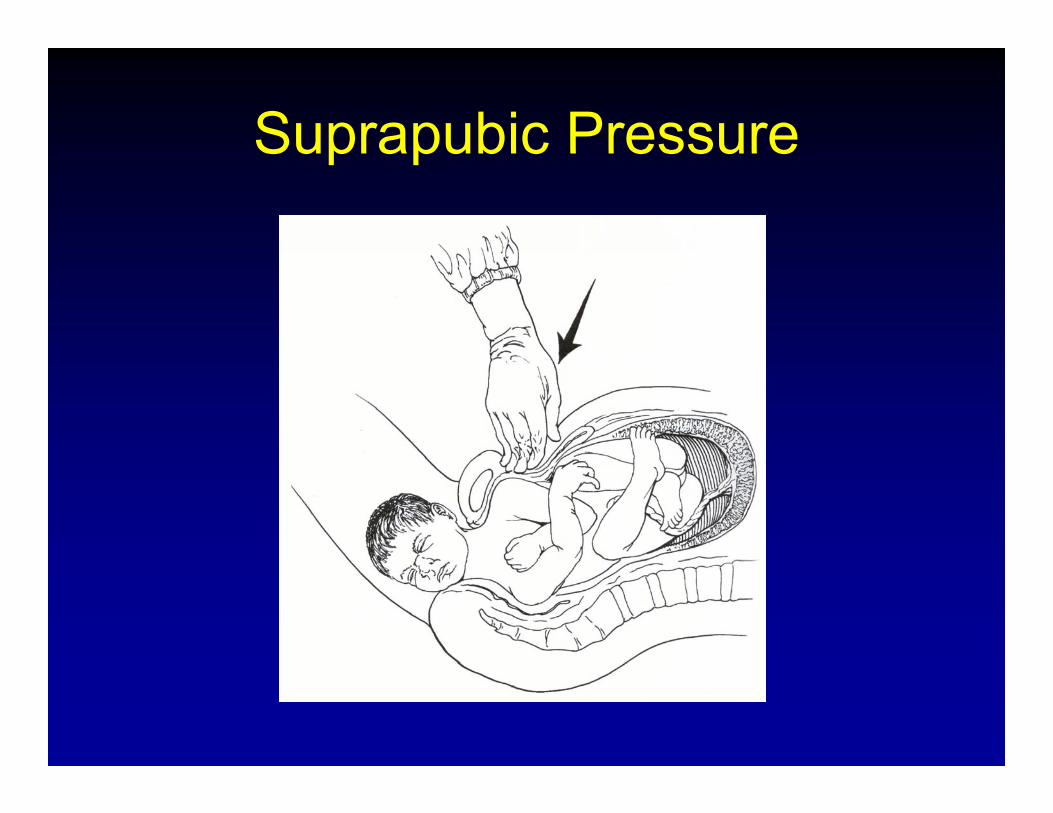
Suprapubic PressureSuprapubic Pressure
Know Your References
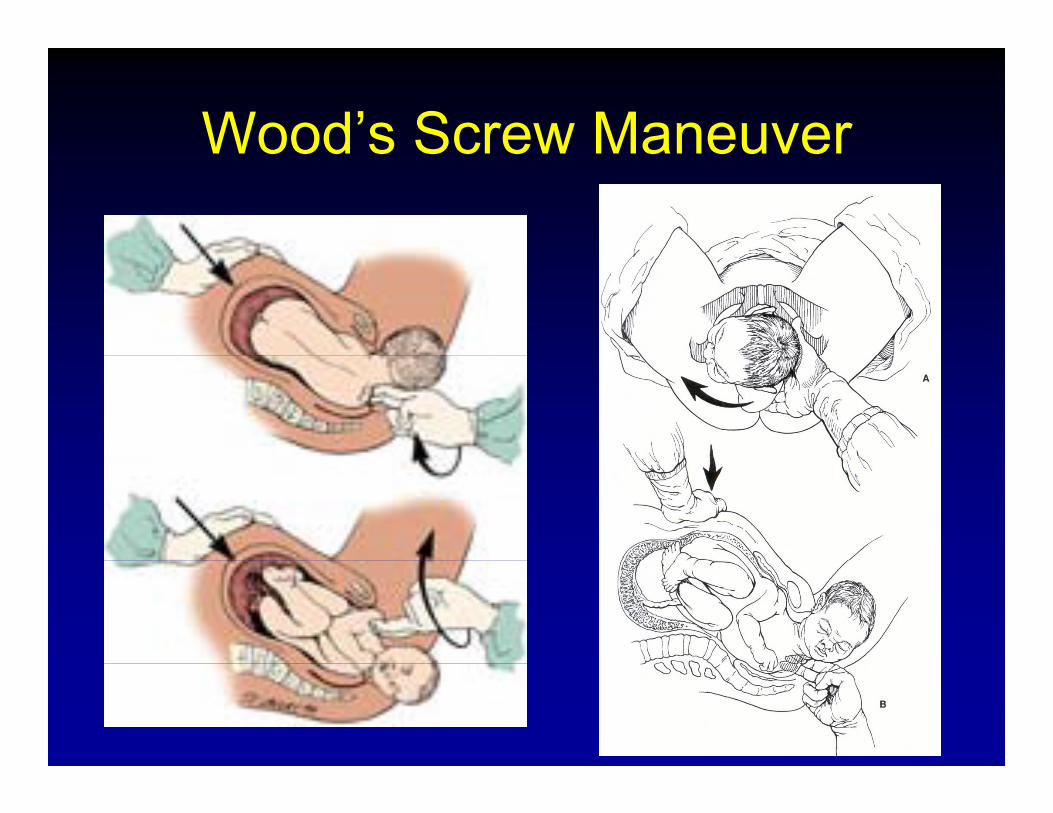
Wood’s Screw ManeuverWood s Screw Maneuver
dWilliam’s Obstetrics 23rd Ed.
“Woods maneuver. The hand is placed behind the posterior shoulder of the fetus. The shoulder is then rotated progressively 180 degrees in a corkscrew manner so that the impacted anterior shoulder is released ”impacted anterior shoulder is released.
A i fi d t t ADd tiAccompanying figure demonstrates ADduction of the posterior shoulder.
Woods’ Manuever
• Woods was the physician’s name. – He described using the physics of a screw to affect delivery.
Woods, CE, Am J Obstet Gynecol 45:796, 1943 A principle of physics is applicable to shoulder delivery.
• Description per Dr. Woods (1943)– Demonstration with mannequins/models. ABduction of the q
shoulders which become the threads. Coccyx and pubic symphisis serve as counter threads.
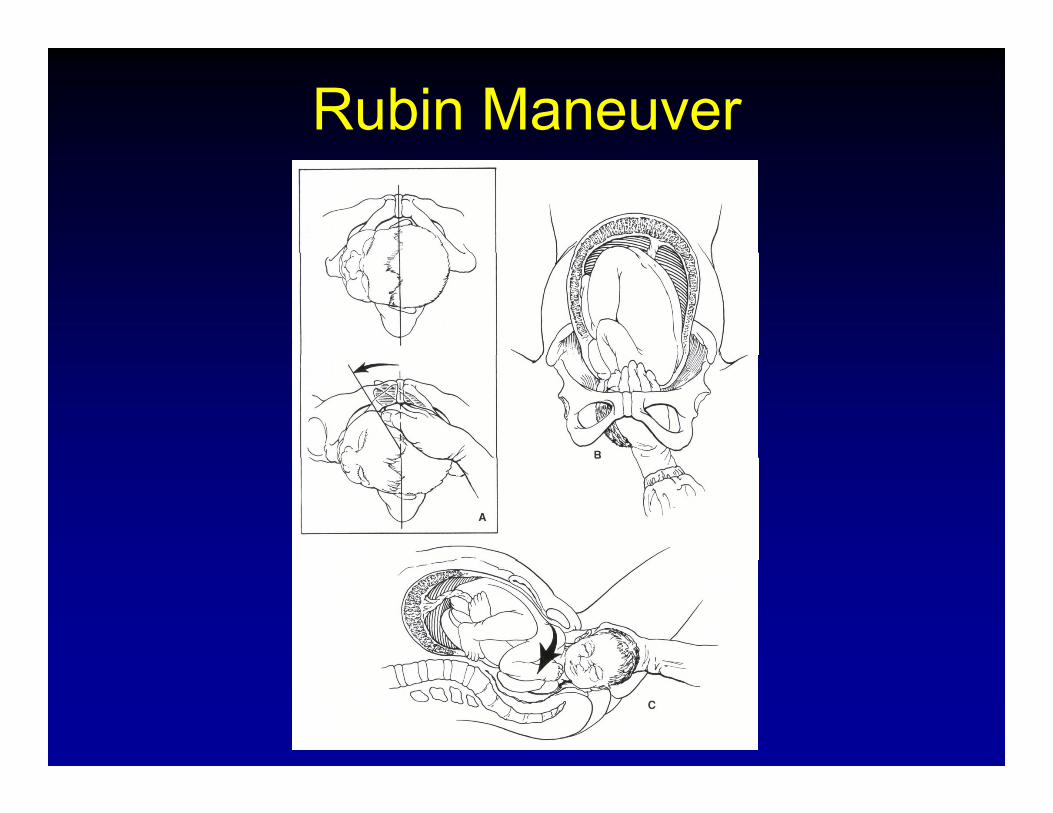
Rubin Maneuver
Rubin Maneuver“Two-Maneuver Program”– First
• Rock shoulders side to side by pushing on maternal• Rock shoulders side to side by pushing on maternal abdomen
• Repeat Fundal Pressure and gentle traction• Rock shoulders again and repeat with considerable• Rock shoulders again and repeat with considerable
fundal pressure– Second
• Place fingers behind whichever shoulder is readily• Place fingers behind whichever shoulder is readily accessible and push toward the fetal chest
• Finger can be placed in opposite axilla to assist descent• More fundal pressure after the shoulder is disimpacted• More fundal pressure after the shoulder is disimpacted
Don’t Use EponymsDon’t Use Eponyms-Describe what you did and be sure to identify which shoulder was anterior and posterior. This can be difficult to recall even 15-20 pminutes after a difficult delivery let alone 10years later at trial.
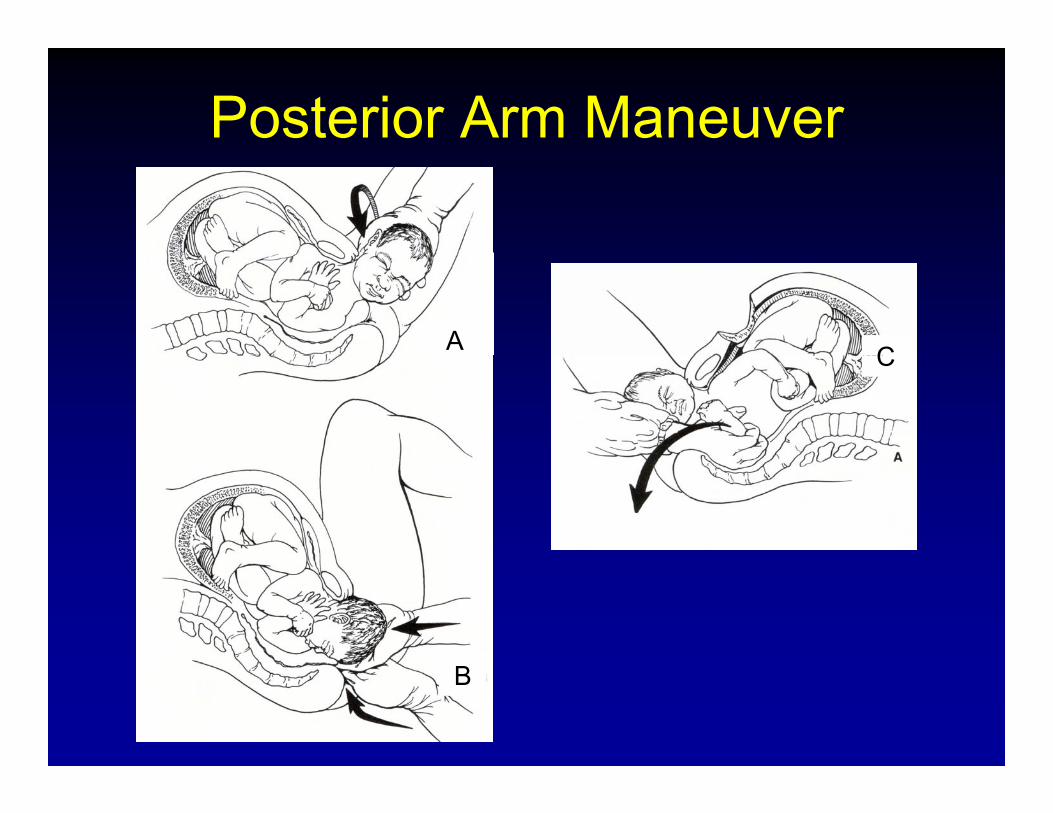
Posterior Arm Maneuver
A CC
B
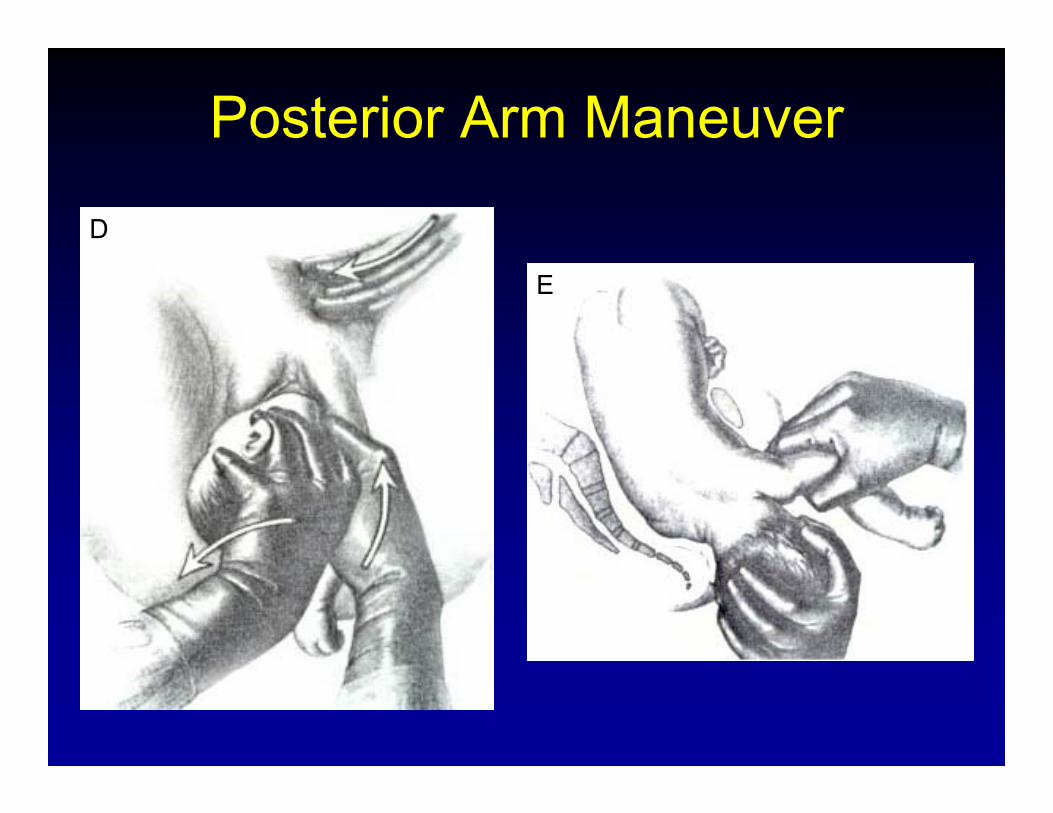
Posterior Arm Maneuver
D
E
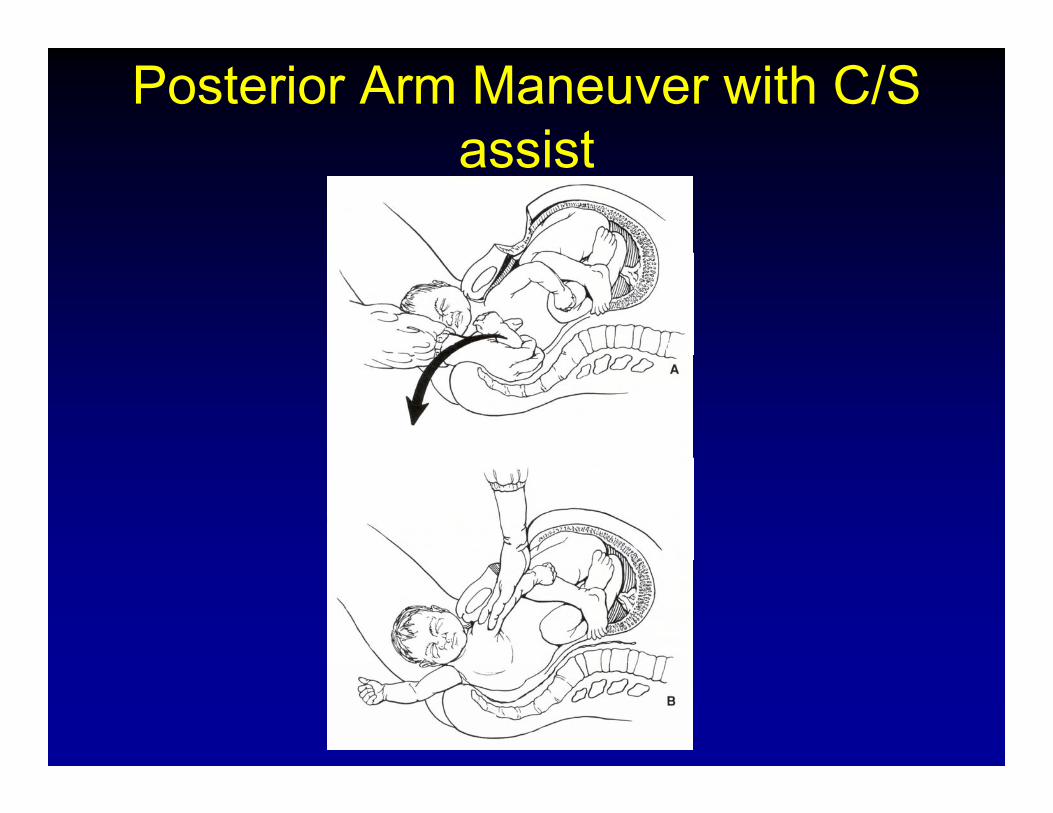
Posterior Arm Maneuver with C/S assistassist
Menticoglou• The head is gently held upward by an
assistant. The operator has the 4th and 5th fingers of each hand flexed and pressedfingers of each hand flexed and pressed against the woman’s perineal area. The middle fingers are both placed into the fetus’s posterior axilla one from the fetus’s front andposterior axilla, one from the fetus s front and the other from the fetus’s back. The fingers overlap each other. By using both fingers, traction is used to pull the posterior shouldertraction is used to pull the posterior shoulder downward and outward along the curve of the sacrum.
Menticoglou, S “A Modified Technique to Deliver the Posterior Arm in Severe Shoulder Dystocia” Ob Gyn 108, No 3. Part 2, p. 755-7.
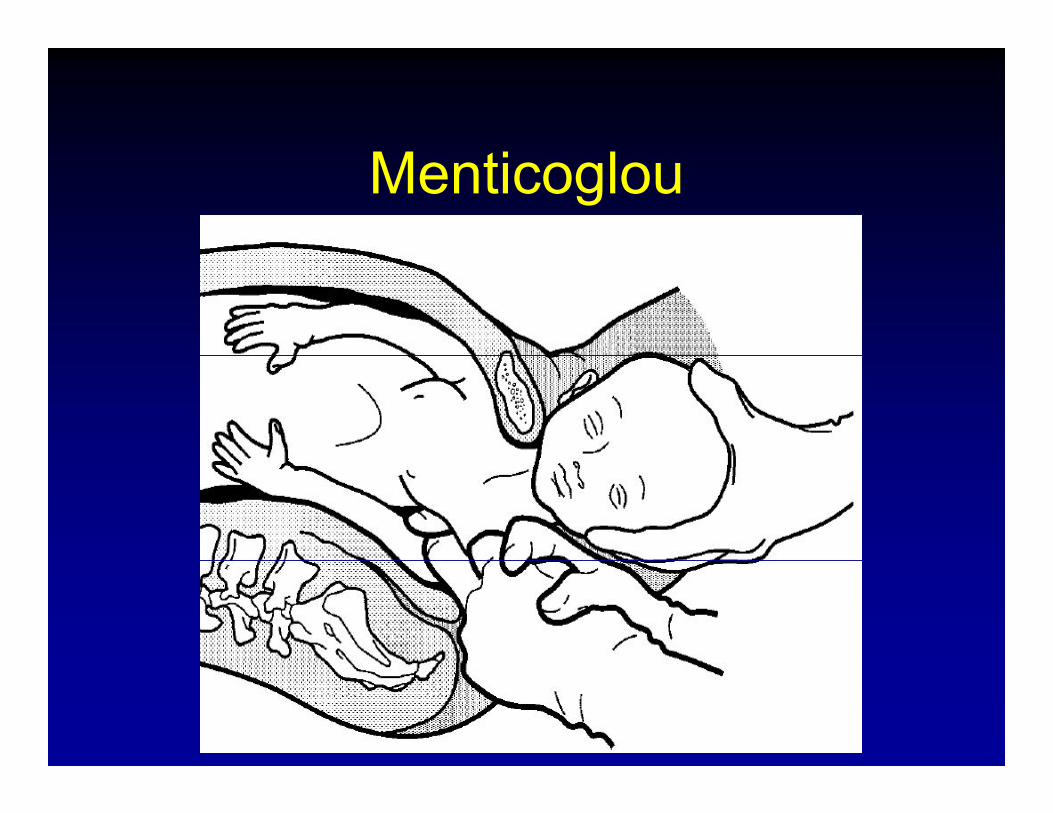
Menticoglou
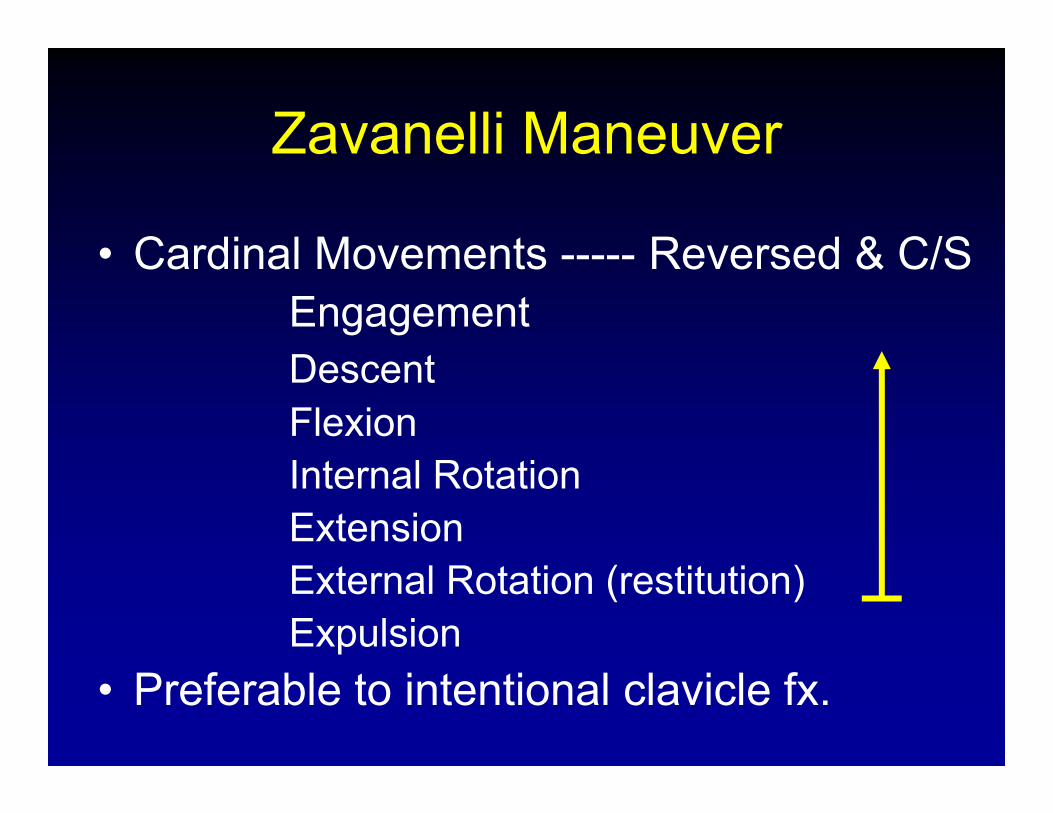
Zavanelli ManeuverZavanelli Maneuver
• Cardinal Movements Reversed & C/S• Cardinal Movements ----- Reversed & C/SEngagementD tDescentFlexionInternal RotationExtensionExternal Rotation (restitution)Expulsion
• Preferable to intentional clavicle fx.
How many providers have done a Zavanelli maneuver?done a Zavanelli maneuver?
Shoulder DystociaShoulder DystociaOther Maneuvers
• Lubrication – tough to do when you can’t put your hand past the fetal headBl dd D i “Bl dd D t i ” id thi• Bladder Drainage – “Bladder Dystocia”– avoid this by draining the bladder in the second stage prior to delivery—especially with an epidural. Can’t put adelivery especially with an epidural. Can t put a foley in after ShD present.
• Gaskin Maneuver • SP pressure + Fundal pressure- Frowned upon in
the US but common elsewhere.S hi• Symphisotomy
How many providers know the Gaskin maneuver?Gaskin maneuver?
Shoulder DystociayGaskin Maneuver
• Retrospective study; 17 years; Farm Midwifery Center, Summertown, TN
• 4452 deliveries; 82 ShD (1.8%)• All managed with the Gaskin maneuver (all 4’s
position)• No stillbirths, neonatal deaths, no Erb’s palsy
(transient or permanent), seizures, HIE, CP or fractured clavicle.
• Mechanism? Possible effect of gravity.Brunner et al. J Reprod Med 1998;43:439-43
Shoulder DystociaManeuversManeuvers
• Be prepared – GET HELPBe prepared GET HELP• Take a deep breath & note the time• Marshall your resources – GET HELP
E i i t f if h l f l!!• Episiotomy for access if helpful!!• McRobert’s maneuver & suprapubic pressure• Delivery of posterior arm/axillaDelivery of posterior arm/axilla• Wood’s screw & Rubin maneuvers• Delivery of posterior arm/axilla
Gaskin Maneuver
• Zavanelli • (Fracture Clavicle)• (Symphysiotomy)(Symphysiotomy)
Shoulder DystociaShoulder DystociaMinimizing Legal Risk
Problems:
Lack of Documentation
Lack of Follow-upp
Shoulder DystociaShoulder DystociaDocumentation
• Mother’s Chart:
– EFW upon admissionEFW upon admission
– Presence/absence of ShD documented
– Appropriate documentation:
• Obstetrical
• Pediatric
– Follow-up with the new parent after discharge;Follow up with the new parent after discharge;
don’t ignore the patient and family
Shoulder DystociaShoulder DystociaDocumentation
• Infant’s Chart:– Adm & D/C physical examination
documenting degree of injury and g g j ypresence of improvement or change.
If profoundly injured or if no evidence of– If profoundly injured or if no evidence of improvement, there must be documentation of pediatric follow updocumentation of pediatric follow-up.
Shoulder DystociayKey Points
1 A ti i t ! L k f R d Fl !1. Anticipate! Look for Red Flags!Macrosomia – head:body disproportion
Prior macrosomia
Prior shoulder dystociay
Maternal obesity
DiabetesDiabetes
Abnormal 1 hour glucola or 3 hour with 1 abnormal value
P td tPostdates
Multiparity
Shoulder DystociayKey Points
1. Be prepared & marshal forces.2 Diabetes is a major risk factor for ShD2. Diabetes is a major risk factor for ShD.3. Most often unpredictable &
unpreventable!unpreventable!4. Think about how you’re going to
manage before it happens!!5. Consider elective C/S in the diabetic5. Consider elective C/S in the diabetic
with EFW>4500g.
Shoulder DystociaKe PointsKey Points
• Induction for non-DM macrosomia increases C/S rate w/o a ↓ fetal M&Mincreases C/S rate w/o a ↓ fetal M&M.
• Debrief after mom and baby are stable.• Document carefully and honestly, review
nursing & pediatric notes.• Follow-up closely with the patient.

THANK YOU!THANK YOU!