the role of the midwife in providing maternal critical...
TRANSCRIPT

The role of the midwife in providing
maternal critical care
Clare Fitzpatrick
Intrapartum Matron/Trust lead for critical care
Liverpool Women's NHS Foundation Trust

Definition for midwifery critical care
“The provision of concentrated care, both physical, psychological, and social on a one to one basis in
an acute situation, where a woman's condition has or is at risk of deteriorating and where
advanced management such as drug therapy, more invasive forms of monitoring and
interpretation of results are required on a frequent basis”
Billington 2007

Midwifery: delivering our future
• Working in many different ways to deliver the
complete midwifery package
• Responding to the call of providing women
centred care (Changing Childbirth, DOH 1993).
• Becoming a member of the high risk team
• Expertise and additional critical care knowledge
Standing nursing and midwifery advisory committee (1998)

The need for HDU in maternity services
• Midwives are increasingly in contact with women who have the potential to become critically ill because of:
– Medical advances resulting in women with significant pre-existing health problems considering pregnancy
– Increasing obesity
– Immigration
– Vulnerable groups

Advantages of a Maternal HDU
• Early recognition and treatment of complications
• Better use of staff
• Improved staff skills
• Continuity of care
• Training opportunities
Mabie & Sibai Am J Obstet Gynecol 1990 Ryan et al Anaesthesia 2000

The ethos of midwifery 80’ & 90s
Gregson 2003
Midwives should be able to work
interchangeably in any part of the
maternity service
In practise this meant that women
where being cared for by midwives
without the necessary skills and
training to ensure that optimum care
was being delivered

Midwifery Issues
• Impact of direct entry midwives
• In house core competency training
• General critical care courses
• Obstetric critical care courses
• Skill maintenance
• Shortage of midwives
Are all midwives capable?
• At the point of registration as a midwife no critical care skills are required
• CEMD have recommended that a multidisciplinary approach
• Very little work being undertaken, as to what contribution midwives could make in HDU
• MW recognised as the ‘experts’ of normal birth.

Towards Safer Childbirth
“As far as midwifery cover for such units is
concerned, it will be necessary to develop a cadre
of midwives who have particular experience and
expertise in the management of the critically ill
woman”
RCM & RCOG 1999

• Post registration based at local university at level 2/3.
• Midwives allocated study time (course based over 15 sessions)
• Course adapted at our request to include changes in physiology of pregnancy and to include a practical maternity example.
• 1 external week at local level 3 ITU
• Competency based framework assessment in workplace by critical care sign off mentor.
Post registration – midwifery training

CEMACH 03- 05
Detection of life threatening illness alone
is of little value.
It is the subsequent management
that will alter the outcome.

How do you select your MW team?
• Adequate post registration experience
• Willingness, enthusiasm and aptitude for additional study
• Team players
• The confidence to play an equal role with other professionals
• Direct entry MW may need additional support in general nursing skills – biggest issue at LWH

The Midwife Lead
• Ideally dual qualification in midwifery and critical
care
• Leadership, organisational and teaching skills
• The confidence to play leading role with other
professionals

Now you have your team, what next?
• Are they available 24/7?
• Are your staffing levels of suitably trained staff enough to provide the recommended ratio of care
– 1:1 antenatal
– 2:1 postnatal
• Ability to flex between DS complement and critical care to deal with peaks and troughs of activity

Team

The extended team – what is our role?
• Midwives with appropriate training and competencies to manage your workload enabling ill women to receive the best of both high tech care combined with woman, baby and family centred philosophy
• Multidisciplinary medical team including obstetricians and obstetric anaesthetists.
• Access is required to haematology and other disciplines.
• Input from other professionals such as dieticians and physiotherapists

Day to Day – what’s our job?
• Care for women in HDU
• Outreach
• Pre and post op visits
• Debriefing
• Teaching
• Mentorship
• Clinical Audit
• Performance monitoring
• Research

Day to day running
• Joint ward rounds each shift
• Top – toe assessments daily
• Holistic care
• Monitoring using ITU charts
• Daily management chart
summarising
– Problems
– Management plan
– Investigations needed
• Structured handover with
supporting documentation and
plan of care for step down ( cf.
NPSA/NICE)

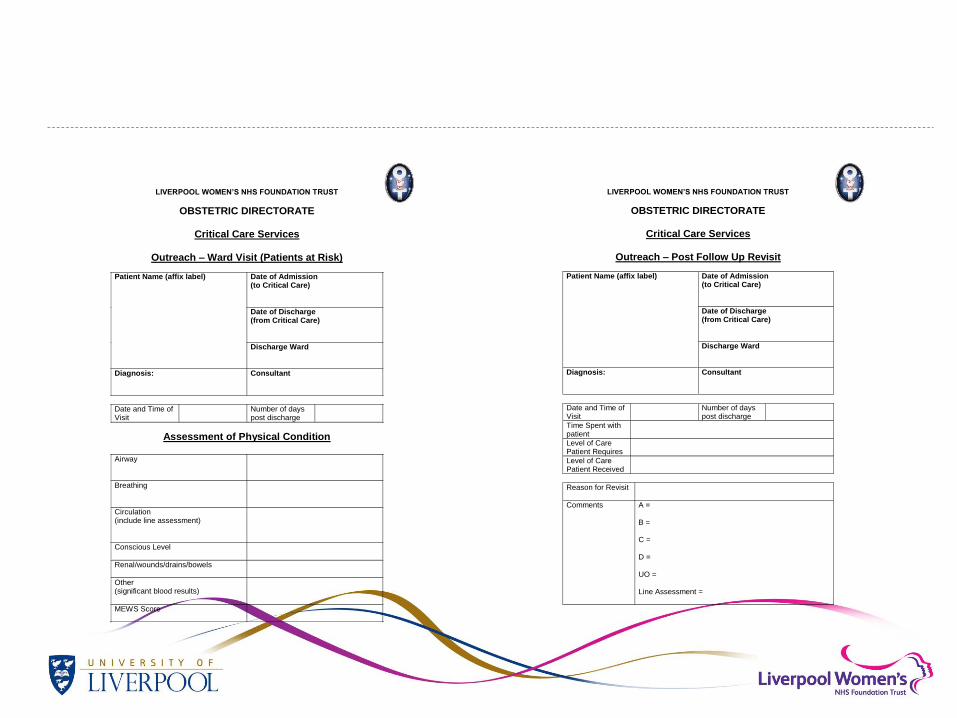
LIVERPOOL WOMEN’S NHS FOUNDATION TRUST
OBSTETRIC DIRECTORATE
Critical Care Services
Outreach – Ward Visit (Patients at Risk)
Date of Admission (to Critical Care)
Date of Discharge (from Critical Care)
Patient Name (affix label)
Discharge Ward
Diagnosis:
Consultant
Date and Time of Visit
Number of days post discharge
Assessment of Physical Condition
Airway
Breathing
Circulation (include line assessment)
Conscious Level
Renal/wounds/drains/bowels
Other (significant blood results)
MEWS Score
LIVERPOOL WOMEN’S NHS FOUNDATION TRUST
OBSTETRIC DIRECTORATE
Critical Care Services
Outreach – Post Follow Up Revisit
Date of Admission (to Critical Care)
Date of Discharge (from Critical Care)
Patient Name (affix label)
Discharge Ward
Diagnosis:
Consultant
Date and Time of Visit
Number of days post discharge
Time Spent with patient
Level of Care Patient Requires
Level of Care Patient Received
Reason for Revisit
Comments
A = B = C = D = UO = Line Assessment =

Skill maintenance
• Work placement
• Mandatory training
– Airway management, resuscitation etc
• Competency assessment
– KSF
– Additional skills assessment

Midwife role ???
• Recognition
– Track and Trigger
system
– Escalation of
management
– Referral including
direct by MWs to
critical care team
• Admission
• Management
• Discharge
• Transfer

Difficulties we have encountered
• Perception of elitism
• Medical staff no confidence in MW ability
• Inflexibility with MW staff
• Difficulty in ring fencing
• HDU beds being unavailable due to peaks of
normal DS activity
• Releasing staff for training and updating

Benefits we have noticed
• Enthusiasm
• Staff feel better supported
• Better compliance and
recording of routine observation
• Early identification of the ill
patient
• Prompt treatment
– Particularly sepsis with
implementing sepsis care
bundle
• Increase in confidence of staff
• Decrease in readmissions to
HDU
• Better team work
• Mentorship
• Improved mandatory training

Have we made a difference at LWH ?
2005 - 13 external transfers from Obstetric HDU
to ITU
2011- 5 in total
5 to ITU for ventilation
3 level 2 transfers for plasmaphoresis,
Infectious disease management
Improved patient experience
Conclusions
• If you are looking after high risk women you will need High
Dependency Team and HDU facilities
• Don’t forget women deteriorate in other areas
• Staffing
• Training and skill maintenance
• Team approach
• Facilities
• Equipment

Useful Reading
• Critical Care in Obstetrics Best Pract Res Clin
Obstet Gynaecol. 2008Oct;22(5)
• Billington M Critical Care in Childbirth for
Midwives Balckwell Publishing, Oxford 2007
• DoH Facilities for Critical Care. The Stationary
Office 2003