the role of human mast cell-derived cytokines in eosinophil biology
TRANSCRIPT

JOURNAL OF INTERFERON & CYTOKINE RESEARCH 24:271–281 (2004)© Mary Ann Liebert, Inc.
The Role of Human Mast Cell-Derived Cytokines in Eosinophil Biology
BITA SHAKOORY, S. MATTHEW FITZGERALD, STEVEN A. LEE, DAVID S. CHI, and GUHA KRISHNASWAMY
ABSTRACT
Eosinophil-mediated diseases, such as allergic asthma, eosinophilic fasciitis, and certain hypersensitivity pul-monary disorders, are characterized by eosinophil infiltration and tissue injury. Mast cells and T cells oftencolocalize to these areas. Recent data suggest that mast cells can contribute to eosinophil-mediated inflam-matory responses. Activation of mast cells can occur by antigen and immunoglobulin E (IgE) via the high-affinity receptor (Fc«RI) for IgE. The liberation of proteases, leukotrienes, lipid mediators, and histamine cancontribute to tissue inflammation and allow recruitment of eosinophils to tissue. In addition, the synthesis andexpression of a plethora of cytokines and chemokines (such as granulocyte-macrophage colony-stimulatingfactor [GM-CSF], interleukin-1 [IL-1], IL-3, IL-5, tumor necrosis factor-a [TNF-a], and the chemokines IL-8, regulated upon activation normal T cell expressed and secreted [RANTES], monocyte chemotactic pro-tein-1 [MCP-1], and eotaxin) by mast cells can influence eosinophil biology. Stem cell factor (SCF)-c-kit, cy-tokine-cytokine receptor, and chemokine-chemokine receptor (CCR3) interactions leading to nuclear factor-kB (NF-kB), mitogen-activated protein kinase (MAPK) expression, and other signaling pathways can modulateeosinophil function. Eosinophil hematopoiesis, activation, survival, and elaboration of mediators can all beregulated thus by mast cells in tissue. Moreover, because eosinophils can secrete SCF, eosinophils can regu-late mast cell function in a paracrine manner. This two-way interaction between eosinophils and mast cellscan pave the way for chronic inflammatory responses in a variety of human diseases. This review summa-rizes this pivotal interaction between human mast cells and eosinophils.
271
INTRODUCTION
HUMAN MAST CELLS ARE MULTIFUNCTIONAL, tissue-dwellingcells. They are typically found in a perivascular location
in tissue. These cells were first described by Paul Ehrlich in1879, who called them mast cells from the German wordmastzellen meaning well fed, as he observed the granular na-ture of these cells. This prolific investigator was also the firstto demonstrate the metachromatic nature of the mast cells us-ing special stains. Typically, mast cells stain metachromaticallybecause of the interaction of the aniline dyes with acid heparincontained in their cell granules.(1–5) Traditionally, mast cellsand basophils have been considered to be pivotal to the devel-opment of chronic allergic inflammation, as seen in allergicasthma.(3,6) This is because these cells also express the uniquehigh-affinity receptor, FceRI, for immunoglobulin E (IgE) ontheir surfaces. Cross-linking of cell surface IgE bound to FceRI
by antigen leads to the rapid release of inflammatory media-tors, including histamine, proteases, chemotactic molecules,and arachidonic acid metabolites, such as prostaglandins andleukotrienes.(1–5) Studies from several laboratories, includingour own, have demonstrated the capacity of these cells to express certain cytokines regulating the inflammatory re-sponse.(7–9) Through their various effects, mast cell-derived cy-tokines and inflammatory mediators may play an important rolein eosinophil-mediated disease. It is now clear that mast cell-derived and T cell-derived cytokines, such as interleukin-5 (IL-5) and granulocyte-macrophage colony-stimulating factor(GM-CSF), are pivotal in eosinophil maturation and chemo-taxis.(10–12) Mast cell-derived chemokines and inflammatorycytokines, such as tumor necrosis factor-a (TNF-a) and IL-2,also can regulate eosinophil chemotaxis, activation, and func-tion. This mast cell-eosinophil axis needs further study, as itcould lead to insights into the pathogenesis of chronic airway
Department of Internal Medicine, Division of Allergy and Immunology, East Tennessee State University, Johnson City, TN 37614.
REVIEW
inflammation and may lead to new therapeutic targets. This pa-per reviews current understanding of the mast cell-eosinophilaxis and its relevance to human eosinophil-mediated disease.
THE MAST CELL-EOSINOPHIL AXIS
Mast cells and eosinophils often colocalize in such diseasesas allergic asthma and parasitic diseases. Eosinophil participa-tion in allergic responses is in turn mediated by release of aplethora of mediators when activated.(13) Studies from severallaboratories suggest that ligand-receptor interactions, such asstem cell factor (SCF)-c-kit and cytokine-cytokine receptor interactions, as well as tryptase protein-activated receptor 2(PAR2) binding, may mediate mutual activation and signalingin mast cell-eosinophil interactions. These interactions are sum-marized in Figure 1. Among the mast cell products that affecteosinophils are cytokines, including IL-1, IL-3, IL-4, IL-5, IL-13, TNF-a, and GM-CSF, and chemokines, including IL-8,
eotaxin, regulated upon activation normal T cell expressed andsecreted (RANTES), and monocyte chemotactic protein-1(MCP-1) (Table 1). In human allergic diseases, mast cells mayserve as amplifiers of IgE-mediated inflammatory responsesand eosinophil influx, as summarized by Williams and Galli.(14)
In one study, investigators using mast cell-deficient mice dem-onstrated that these mice develop less eosinophilia than theirnormal counterparts.(15) In another study, by Das et al.,(16) mastcells were required for the induction of eosinophilia in responseto eotaxin injection in air pouches of sensitized mice. Yu andChen(17) have suggested that in their mouse model of asthmainduced by Dermatophagoides farinae, mast cells were essen-tial for cytokine and chemokine elaboration, macrophage andT cell activation, and Th2 cell development.(17) Th2 cytokineelaboration and mast cell-derived cytokines and chemokines allcan lead to eosinophil activation.
Thus, in all likelihood, based on their prolific cytokine/chemokine synthetic capacity, human mast cells play pivotalroles in airway inflammation and eosinophil-mediated diseases.
SHAKOORY ET AL.272
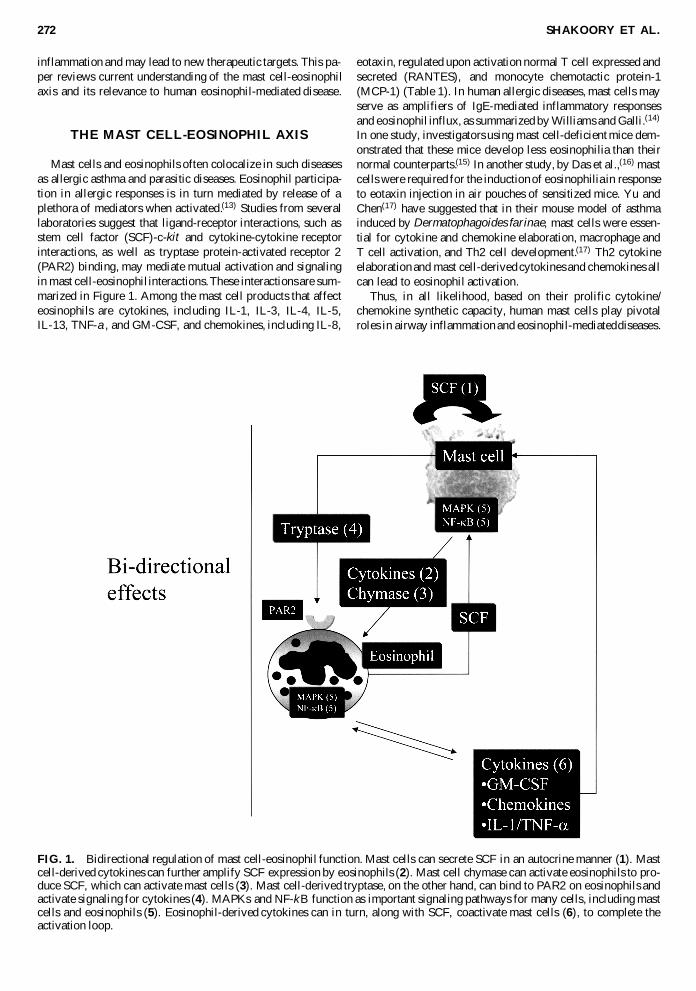
FIG. 1. Bidirectional regulation of mast cell-eosinophil function. Mast cells can secrete SCF in an autocrine manner (1). Mastcell-derived cytokines can further amplify SCF expression by eosinophils (2). Mast cell chymase can activate eosinophils to pro-duce SCF, which can activate mast cells (3). Mast cell-derived tryptase, on the other hand, can bind to PAR2 on eosinophils andactivate signaling for cytokines (4). MAPKs and NF-kB function as important signaling pathways for many cells, including mastcells and eosinophils (5). Eosinophil-derived cytokines can in turn, along with SCF, coactivate mast cells (6), to complete theactivation loop.
At the very least, they can contribute to the pool of eosinophil-active cytokines that permeate inflamed tissue. On the otherhand, direct cell-cell contact of mast cells and eosinophils mayinduce eosinophil activation and nuclear factor-kB (NF-kB) nu-clear translocation and promote eosinophil survival.
Mast cell-derived cytokines and chemokines: effects on eosinophils
In this section, we review the plethora of eosinophil-regu-lating mast cell-derived cytokines and chemokines (Table 1 andFigs. 1–3). Many of the effects of mast cell-derived cytokineson eosinophil biology are mediated by signaling molecules,such as mitogen-activated protein kinases (MAPK) and NF-kB.Recent studies by Hartman’s group(18) have shown that mastcell tryptase is capable of activating MAPKs and cytokine se-cretion from eosinophils.(18) HMC-1 cells as well as tryptaseinduced IL-6 and IL-8 secretion from eosinophils, a process thatwas inhibited by MAPK inhibitors, cyclohexamide, actino-mycin D, and dexamethasone. This was likely mediated byPAR2, as antagonists to this receptor inhibited signaling (Fig.1). Mast cell-derived cytokines can also serve to activate NF-kB in eosinophils, leading to cytokine gene expression, adhe-sion molecule expression, and enhanced survival (Figs. 1–3).
Stem cell factor
Mast cells arise from CD341 hematopoietic stem cells in thebone marrow. Fibroblasts play a major role in mast cell differ-entiation by secreting SCF, but interestingly, eosinophils mayalso serve as a source of SCF, as can the mast cell itself (Fig.1). SCF binds to its receptor, c-kit, which is present on botheosinophils and mast cells. Hence, SCF is also called c-kit li-gand, and because it is encoded by the steel locus, it has alsobeen referred to as the steel factor. SCF induces growth of mastcells and also regulates their activation, degranulation, andchemotaxis. Many factors, including mast cell cytokines and
chymase, regulate expression of SCF by human eosinophils.This leads to the concept of bidirectional interactions betweenmast cells and eosinophils (Fig. 1). Thus, the addition of cyto-kines or chymase to eosinophils induces SCF secretion(19) (Fig.1). On the other hand, SCF can activate mast cell synthesis ofeosinophil-active cytokines. Studies by Hogabam et al.(20) havedemonstrated that mast cell-fibroblast cocultures induce thesynthesis of eotaxin, a major eosinophil chemoattractant, frommast cells.(20) This appears to be SCF and contact dependent.When anti-SCF antibody was added or when mast cells and fibroblasts were separated by a transwell plate, eotaxin pro-duction was inhibited.(20) Hence, paracrine and autocrine SCF-based loops can regulate bidirectional mast cell-fibro-blast-eosinophil interactions, leading to chronic inflammation (Fig. 1).
IL-1b AND TNF-a
IL-1b and TNF-a are important cytokines expressed by hu-man mast cells.(21–23) Mast cell-derived monokines can haveparacrine effects on eosinophils and other adventitial cells aswell as autocrine effects on mast cells themselves. For exam-ple, monokines induce expression of chemokines from adven-titial cells, such as fibroblasts, which in turn serve to chemo-attract eosinophils.(13) IL-1b increases eosinophil survivalthrough paracrine production of GM-CSF(24) while also en-hancing production of TNF-a, IL-5, and GM-CSF from mastcells in an autocrine manner.(23)
TNF-a, which is preformed and stored in mast cell granules,has many important effects on eosinophil function. IL-1b in-creases eosinophil survival and activates eosinophils. This wasshown by Levi-Schaffer et al.,(25) who demonstrated that ratperitoneal sonicates activated human eosinophils.(25) These in-vestigators showed a 2-fold enhancement of eosinophil viabilitywhen activated by mast cell sonicates. Most of the mast cell ac-
MAST CELL-DERIVED CYTOKINES 273
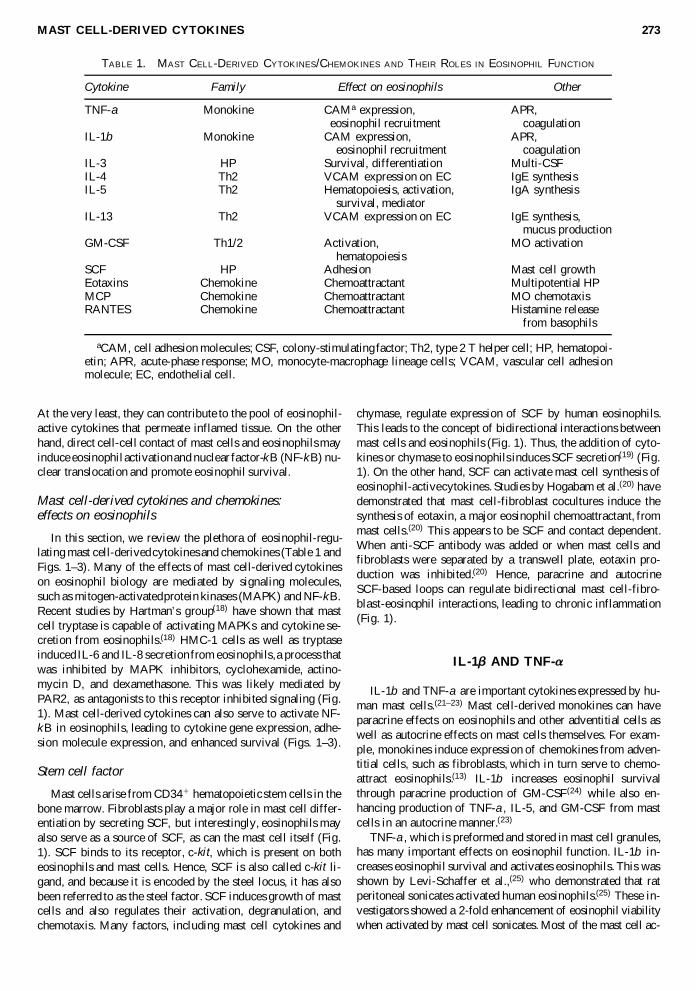
TABLE 1. MAST CELL-DERIVED CYTOKINES/CHEMOKINES AND THEIR ROLES IN EOSINOPHIL FUNCTION
Cytokine Family Effect on eosinophils Other
TNF-a Monokine CAMa expression, APR,eosinophil recruitment coagulation
IL-1b Monokine CAM expression, APR,eosinophil recruitment coagulation
IL-3 HP Survival, differentiation Multi-CSFIL-4 Th2 VCAM expression on EC IgE synthesisIL-5 Th2 Hematopoiesis, activation, IgA synthesis
survival, mediatorIL-13 Th2 VCAM expression on EC IgE synthesis,
mucus productionGM-CSF Th1/2 Activation, MO activation
hematopoiesisSCF HP Adhesion Mast cell growthEotaxins Chemokine Chemoattractant Multipotential HPMCP Chemokine Chemoattractant MO chemotaxisRANTES Chemokine Chemoattractant Histamine release
from basophils
aCAM, cell adhesion molecules; CSF, colony-stimulating factor; Th2, type 2 T helper cell; HP, hematopoi-etin; APR, acute-phase response; MO, monocyte-macrophage lineage cells; VCAM, vascular cell adhesionmolecule; EC, endothelial cell.

tivity in the sonicate could be attributed to TNF-a, which en-hanced eosinophil expression of GM-CSF. Temkin and Levi-Schaffer(26) also showed that eosinophil survival was enhancedby TNF-a and that this was inhibited by antibodies to TNF re-ceptors I and II as well as by an antibody to GM-CSF. The sur-vival effect was not inhibited by antibodies to either IL-3 or IL-5.(26) TNF-a also induced GM-CSF release from the eosinophiland NF-kB translocation to the nucleus (Fig. 2). TNF-a also in-duces release of eosinophil peroxidase (EPO) from eosinophils,(25)
and IL-1b and TNF-a, in conjunction with IL-5, increase migra-tion of eosinophils. To further complicate this pathway, these cytokines may also act in concert with the CCR3-bindingchemokines in enhancing eosinophil recruitment and chemo-taxis.(27) As shown in Fig. 2, IL-1b and TNF-a from mast cellscould activate eotaxin expression from epithelium/endothelium,thereby contributing to eosinophil chemotaxis.(28) It is also likelythat these cytokines activate NF-kB and MAPK in eosinophils,as stated earlier, leading to some of the observed biologic effectsin inflammatory states.
IL-2
IL-2 can serve as an important eosinophil chemoattractant.Although its dominant source is the T cells, mast cells and
eosinophils are capable of expressing this cytokine.(29–35) Si-mon et al.(36) have shown that most eosinophils from hypere-osinophilic patients express the IL-2 receptor alpha chain,CD25. They also show that IL-2 can enhance eosinophilcationic protein production in platelet activating factor-stimu-lated eosinophils. This effect was not seen in CD25-negativeeosinophils.(36) IL-2 is an important eosinophil activator and in-duces the release of eosinophil peroxidase and IL-6 fromeosinophils.(37) IL-2 regulates eosinophil chemotaxis, and eo-sinophilia is a recognized feature of the adverse effect of infu-sion of recombinant IL-2 in malignancy.(38) Functional IL-2 re-ceptors are expressed on eosinophils, suggesting that these cellscan bind and respond to this cytokine.(39) Thus, a mast cell-IL-2-IL-2R axis may exist in regulating eosinophil recruitment andfunction.
IL-3, IL-5, AND GM-CSF
Three cytokines of mast cell and T cell origin that are piv-otal to eosinophil biology are IL-3, IL-5, and GM-CSF.(40) Weand others have shown that mast cells are capable of express-ing IL-3, IL-5, and GM-CSF.(23,41–44) IL-3, IL-5, and GM-CSFtogether regulate growth, differentiation, and survival of eosi-
SHAKOORY ET AL.274
FIG. 2. Mast cell TNF-a induces GM-CSF release from the eosinophil and NF-kB translocation to the nucleus. GM-CSF hasautocrine effects on eosinophils, prolonging viability and inhibiting apoptosis. IL-1b, IL-4, and TNF-a from mast cells could ac-tivate eotaxin expression from epithelium/endothelium, thereby contributing to eosinophil chemotaxis, an effect mediated byCCR3.
nophils, and their absence has been shown to cause apoptosisand death of these cells.(25,45–50) This survival is especially nec-essary for eosinophils to sufficiently exert their effects.(25) IL-3, IL-5, and GM-CSF delay the apoptosis of eosinophils for aminimum of 12–14 days, whereas in their absence, the life-spanof these cells does not exceed 48 h.(10,51) They also causeeosinophils to express large numbers of receptors for cytokines,immunoglobulins, and complement.(10)
IL-5 induces eosinophil differentiation in the bone marrowand also stimulates eosinophil precursors to synthesize granuleproteins.(52) In addition to selective differentiation of eo-sinophils, IL-5 is responsible for their mobilization and releasefrom bone marrow into the bloodstream.(10,53,54) IL-5, like GM-CSF, is also essential for eosinophil activation and may play arole following tissue infiltration by the eosinophil.
IL-3 is a hematopoietic cytokine that activates eosinophilsand allows them to present superantigens and peptides to Tcells.(55) It also downregulates the chemokine receptor, CCR3,from the surface of the human eosinophil.(56) IL-3 works in tan-dem with IL-5 to induce differentiation of eosinophil progeni-tor cells.(57)
GM-CSF induces hypodense, activated eosinophils and pro-longs eosinophil survival secondary to its production and re-lease by activated mast cells through TNF-a.(25,26) GM-CSF
can also induce the release of EPO from eosinophils.(37) Thus,induction of autocrine and paracrine GM-CSF production is oneof the ways mast cells increase eosinophil survival.(25)
IL-4 AND IL-13
IL-4 and IL-13 are key cytokines responsible for the latephase reaction seen in allergic inflammation.(10) Both IL-4 andIL-13 are products of human mast cells.(58,59) IL-4 regulatesIgE synthesis(60) and also allows for eosinophil recruitment.(61)
IL-4 also regulates eosinophil apoptosis, thus contributing tothe resolution of inflammation.(62) IL-13 can prolong eosinophilsurvival by inducing autocrine production of IL-3, IL-5, andGM-CSF.(25) IL-4 and IL-13 can affect eosinophils by also en-hancing the activating effects of TNF-a on eosinophils. Thiseffect is also seen with IL-5, suggesting an in vitro synergismamong all four of these cytokines.(63–66)
IL-4 and IL-13, however, play a pivotal role in transmigra-tion of eosinophils across the endothelium of vasculature intopulmonary tissue, exclusively affecting the expansion of the tis-sue eosinophil population. They exert this by activation of ad-hesion pathways specific to eosinophils, as well as promotingIL-5 and eotaxin production by inflammatory cells.(67,68) Jaruga
MAST CELL-DERIVED CYTOKINES 275
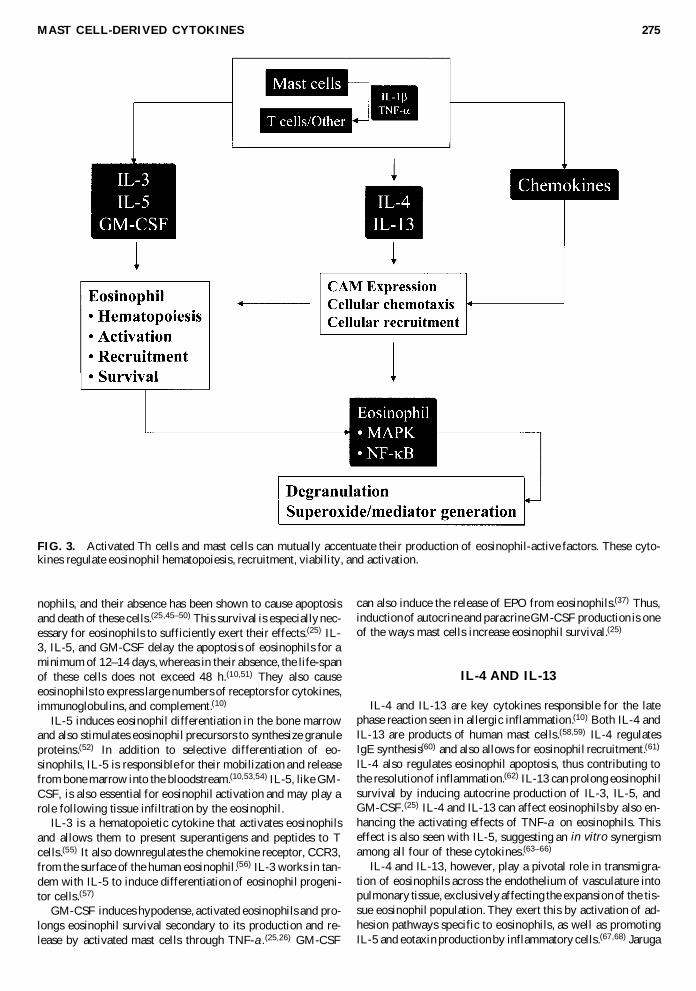
FIG. 3. Activated Th cells and mast cells can mutually accentuate their production of eosinophil-active factors. These cyto-kines regulate eosinophil hematopoiesis, recruitment, viability, and activation.

et al.(67) demonstrated that the IL-4/Stat6 system is instrumentalin upregulation of eotaxins and IL-5, thereby allowing leukocyterecruitment into tissue. These authors showed that recruitment ofneutrophils and eosinophils is deficient in IL-4 or Stat6 knockoutmice.(67) Mellor et al.(68) recently showed that cord blood-derivedmast cells when primed for 5 days with IL-4 secrete enhancedamounts of IL-5, TNF-a, and chemokines in response toleukotriene C4 (LTC4). This effect was blocked using a leukotrienereceptor antagonist. These results point to novel ways in whichIL-4/Stat6/leukotrienes can regulate Th2 cytokine productionfrom mast cells. IL-4 induces vascular cell adhesion molecule-1(VCAM-1) on endothelial cells,(69) allowing eosinophil recruit-ment into tissue involving VCAM-1-very late activation antigen-4 (VLA-4) interactions. Eosinophils tether, roll, and accumulatewhen exposed to endothelial cells activated by IL-4 and express-ing VCAM-1. Inhibition of VCAM-1 or VLA-4 integrin leads toinhibition of eosinophil tethering. When IL-4 is injected into thetissue, leukocyte recruitment occurs, and the majority of these in-filtrating cells are eosinophils.(70) IL-4, in conjunction with IL-1and TNF-a, also induces eotaxin from endothelial cells (Fig. 3),which, in turn, modulates eosinophil recruitment.
CHEMOKINES
Chemokines are cellular products that mediate the recruitmentof eosinophils, among other inflammatory cells.(10) Chemokinesconstitute a family (8–10 kDa) of chemotactic cytokines that reg-ulate leukocyte chemotaxis.(10) Although several groups havebeen characterized, the two major groups are the C-C and C-X-C chemokines that regulate mononuclear cell and leukocytechemotaxis, respectively. Most chemokines exert their effectthrough binding to specific receptors, such as the chemokine re-ceptor CCR3.(10,71,72) Among all the chemokines, MCP-3, MCP-4, macrophage inflammatory protein-1a (MIP-1a), RANTES, andeotaxin are responsible for migration of eosinophils. Thesechemokines exhibit a certain selectivity for eosinophil recruit-ment.(13) Chemokines and cytokines are both produced in the earlyand late phases of the asthmatic response and have been demon-strated to affect eosinophil recruitment. There is a particularly im-portant synergy between eotaxin and IL-5.(73)
Mast cells have been shown to express a variety of chemo-kines. Aoki et al.(74) demonstrated that tryptase-positive mastcells in lesional biopsies of basal cell carcinoma express IL-8and RANTES. (74) Baghestanian et al.(75) showed that humanlung mast cells activated with SCF and anti-IgE express thechemokine MCP-1. Mast cells and T cells in patients withKimura’s disease (angiolymphoid hyperplasia with eosinophiliaand elevated IgE) express RANTES and eotaxin along with theTh2 cytokines, IL-4 and IL-5.(41) Human mast cell lines acti-vated by dengue virus secreted RANTES, MIP-1a, and MIP-1b but not IL-8.(76) Cord blood-derived mast cells also ex-pressed RANTES when exposed to the dengue virus in the samestudy.(76) Studies have shown that mast cells, like eosinophils,also express the eotaxin receptor, CCR3.(77) Eotaxin andRANTES are chemotactic not only to eosinophils but also tohuman mast cells. Moreover, recent data suggest that ligationof CCR3 on mast cells by eotaxin 1 leads to greater generationof IL-13, which in turn can modulate eosinophil infiltration andmucosal inflammation.(78)
Eotaxin 1 and eotaxin 2 are two newly described chemokinesthat are relatively specific for eosinophils.(13) These chemokinesprobably play a role in clinical asthma and regulate eosinophil ac-tivation in this disease. Ying et al.(79) showed elevated expressionof eotaxin, eotaxin 2, RANTES, MCP-3, MCP-4, and CCR3 inthe bronchial mucosa of asthmatic patients. The activated mast cell,along with activated T cells, endothelial cells, macrophages, fi-broblasts, and epithelial cells, can be sources of these chemokinesin the airways. Eotaxin 1 not only is a major eosinophil chemoat-tractant but also promotes the growth of mast cell and myeloidprogenitors. Eotaxin 1 exerts its potent activating effect oneosinophils through interaction with CCR3, a receptor selectivelyexpressed on basophils, eosinophils, and Th2 cells, and in the caseof the eosinophil, this causes their chemotaxis and degranula-tion.(13,72) In a study to assess the ability of several C-C chemokinesin transendothelial migration, Shahabuddin et al.(27) showed thateotaxin 1, eotaxin 2, MCP-4, and RANTES induce eosinophil mi-gration by binding to CCR3. Eotaxin also influences the traffick-ing of eosinophils from bone marrow into the bloodstream, in-creasing the number of circulating eosinophils.(13) It has beensuggested that eotaxin primes eosinophil oxidative metabolism andinduces eosinophil activation,(13,80) and its activating effect oneosinophil oxidative metabolism is more potent than RANTES andIL-5.(80) Of the other chemokines, RANTES is essential fortransendothelial migration of eosinophils. This was shown by Ebi-sawa et al.(81) Eosinophil priming by IL-5 further enhances thetransendothelial migration in response to RANTES.(81) RANTESis a member of the C-C chemokine family and is chemotactic notonly for eosinophils but also for memory T cells and monocytes.RANTES has been shown to release histamine from basophils andalso activates eosinophils.
T CELL-MAST CELL-EOSINOPHIL AXIS
The three cell types that often contribute to allergic and parasitic diseases include the T cell, the mast cell, and theeosinophil. Mast cells can present antigen to T cells, and thereare some data suggesting that mast cell-derived cytokines mayenhance development of a Th2 T cell subset. On the flip side,recent data also suggest that Th cytokines can regulate mast celland eosinophil function. Th2 cytokine-stimulated mast cells express more inflammatory mediators that can activate eosi-nophils (Fig. 4). For example, IL-4-stimulated mast cells ex-press more histamine, leukotrienes, and IL-5 after FceRI cross-linking, whereas IL-5-stimulated mast cells secrete more IL-5,IL-13, GM-CSF, TNF-a, and MIP-1a.(82,83)
In summary, in the presence of activated Th cells, mast cellscan accentuate their production of eosinophil-active factors(Fig. 4). Thus, a T cell-mast cell-eosinophil axis may exist invivo, and activation of this axis by antigen can lead to elabo-ration of a cytokine pool that leads to further eosinophil acti-vation and induction of the chronic inflammatory response asseen in asthma and parasitic disorders.
ROLE FOR MAST CELLS IN EOSINOPHIL-MEDIATED INFLAMMATION
Allergic asthma is characterized by epithelial exfoliation,mast cell activation, eosinophil and inflammatory cell influx,
SHAKOORY ET AL.276

and airway obstruction. The mast cell plays a pivotal role inasthma pathogenesis.(84) Aspirin sensitivity, a form of asthma,is characterized by eosinophil infiltration of the affected tissues,sinusitis, and nasal polyposis. The asthma may be mediated bymast cells and respond to the leuktotriene modifier drugs, sug-gesting a role for mast cell-derived leukotrienes. These are piv-otal eosinophilic chemoattractants. Nasal polyposis in aspirinsensitivity is characterized by eosinophil infiltration and en-riched expression of the eosinophil-active cytokines IL-5, GM-CSF, RANTES, and eotaxin.(85) Tissues of patients withaspirin-sensitive asthma demonstrate increased numbers of ac-tivated mast cells, eosinophils, and T cells.(86) In patients withaspirin sensitivity, challenge of the nasal mucosa with aspirinleads to the elaboration of cysteinyl leukotrienes, tryptase, andeosinophilic cationic protein.(85,87,88) The challenge is often ac-companied by eosinophilic infiltration. This again suggests afunctional mast cell-eosinophil axis in this disease. These dataalso point toward a common etiopathogenic mechanism forrhinitis, asthma, and nasal polyposis.
Eosinophilic fasciitis is another disease where mast cell degranulation and eosinophil infiltration have been ob-served.(89,90) A causal relationship between these two eventshas not been demonstrated, but nevertheless these data suggesta possible mast cell-eosinophil axis that may be active in thisdisorder. Eosinophilic fasciitis typically responds to glucocor-ticoid therapy. These drugs inhibit the production of eosinophil-active cytokines from mast cells, as shown by us,(23) and alsohave direct effects on eosinophil survival. Patients with variousforms of gastrointestinal diseases, food hypersensitivity, and ir-ritable bowel-like syndromes demonstrate increased numbersof mast cells in their intestinal tissues.(91–93) Investigators havedescribed a subset of patients with eosinophilic gastroenteritiswho also have an underlying connective tissue disease and dem-onstrate excessive mast cells in their intestinal mucosa.(93) Be-cause of the ability of mast cells to recruit eosinophils and theproximity of mast cells to nerves, many eosinophil-mediatedgastrointestinal diseases may be caused by mast cell activation,leading to inflammatory mediator elaboration and culminat-ing in diarrhea, intestinal inflammation, and protein-losing en-teropathy.
Another set of disorders that may involve mast cell-eosinophil interactions are the parasitic diseases. Th2 cytokines,of either T cell or mast cell origin, are capable of inducing mastcell proliferation/hyperplasia, mucus production, and eosino-philia and eosinophil activation. This has been summarized byFinkelman and Urban.(94) Mast cell or T cell activation by par-asite antigens can lead to Th2 cytokine elaboration and resul-tant eosinophil-dependent inflammatory responses. Wildenburget al.(95) demonstrated a correlation between mast cell andeosinophil numbers in Onchocerca nodules with microfilaria-producing females. Bell(96) summarized the association amongIgE, mast cells, eosinophils, and parasitic disease but empha-sized that the protective effect of this interaction remains to beproven. In populations where parasitic diseases are rare, aller-gic diseases appear to be increasing. The potential interactionamong atopy, parasitic diseases, and immune responses in-volving mast cells and eosinophils has been studied by severalinvestigators.(96) A hypothesis is that parasitic infestation, byinduction of such immunoregulatory cytokines as IL-10, mayretard the development of allergy.(97) This remains to be proven.There have also been several cases in the literature of masto-cytosis characterized by peripheral and tissue eosinophilia,again confirming the presence of a functional mast cell-eosinophil axis.(98,99)
CONCLUSIONS
Mast cells play an important role in the biology of inflam-mation. They are highly potent, highly granulated cells that re-side in the peripheral tissues and are often the first responderswhen a host becomes antigenically challenged. An importantaspect of mast cell biology is their ability to initiate and or-chestrate an effective immune response. One way mast cells dothis is by regulating eosinophil activation and recruitment. Mastcells release a host of cytokines, for example, IL-3, IL-5, andGM-CSF, that potentiate eosinophil survival and function.Eosinophils are important in a number of allergic diseases, in-cluding asthma and parasitic invasion. Eosinophils themselves
MAST CELL-DERIVED CYTOKINES 277
FIG. 4. Th2 cytokine-stimulated mast cells express more in-flammatory mediators. IL-4-stimulated mast cells express morehistamine, leukotrienes, and IL-5 after FceRI cross-linking,whereas IL-5-stimulated mast cells secrete more IL-5, IL-13,GM-CSF, TNF-a, and MIP-1a. The T cell-mast cell axis canthus powerfully regulate eosinophil function.
can release numerous cytokines and chemokines that further ag-gravate the immune response. In this manner, a conspiratory re-lationship between eosinophils and mast cells can regulate thedevelopment and maturation of tissue inflammatory responses.The T cell-mast cell-eosinophil axis represents a crucial targetfor pharmacologic intervention using biotherapeutic inhibitorsof cytokines, chemokines, chemokine receptors, or transcrip-tion factor/signaling proteins. One can postulate a role for such inhibitors for diseases varying from allergic asthma toeosinophilic leukemia.
ACKNOWLEDGMENTS
This study was supported by NIH grants AI-43310 and HL-63070, The Rondal Cole Foundation, and the Chair of Excel-lence in Medicine (State of Tennessee Grant 20233), The Car-diovascular Research Institute, and the Research DevelopmentCommittee, East Tennessee State University.
REFERENCES
1. MARONE, G., CASOLARO, V., PATELLA, V., FLORIO, G., andTRIGGIANI, M. (1997). Molecular and cellular biology of mastcells and basophils. Int. Arch. Allergy Immunol. 114, 207–217.
2. METCALFE, D.D., BARAM, D., and MEKORI, Y.A. (1997).Mast cells. Physiol. Rev. 77, 1033–1079.
3. COSTA, J.J., WELLER, P.F., and GALLI, S.J. (1997). The cellsof the allergic response: mast cells, basophils, and eosinophils.JAMA 278, 1815–1822.
4. KRISHNASWAMY, G., KELLEY, J., JOHNSON, D., YOUNG-BERG, G., STONE, W., HUANG, S.K., BIEBER, J., and CHI,D.S. (2001). The human mast cell: functions in physiology and dis-ease. Front. Biosci. 6, D1109–D1127.
5. KELLEY, J.L., CHI, D.S., ABOU-AUDA, W., SMITH, J.K., andKRISHNASWAMY, G. (2000). The molecular role of mast cellsin atherosclerotic cardiovascular disease. Mol. Med. Today 6,304–308.
6. ROSSI, G.L., and OLIVIERI, D. (1997). Does the mast cell stillhave a key role in asthma? Chest 112, 523–529.
7. CHURCH, M.K., and LEVI-SCHAFFER, F. (1997). The humanmast cell. J. Allergy Clin. Immunol. 99, 155–160.
8. BRADDING, P. (1996). Human mast cell cytokines. Clin. Exp. Al-lergy 26, 13–19.
9. KRISHNASWAMY, G., LAKSHMAN, T., MILLER, A.R.,SRIKANTH, S., HALL, K., HUANG, S.K., SUTTLES, J., SMITH,J.K., and STOUT, R. (1997). Multifunctional cytokine expressionby human mast cells: regulation by T cell 17 membrane contactand glucocorticoids. J. Interferon Cytokine Res. 17, 167–176.
10. ROTHENBERG, M.E. (1998). Eosinophilia. N. Engl. J. Med. 338,1592–1600.
11. LAMPINEN, M., RAK, S., and VENGE, P. (1999). The role ofinterleukin-5, interleukin-8 and RANTES in the chemotactic at-traction of eosinophils to the allergic lung. Clin. Exp. Allergy 29,314–322.
12. OLIVEIRA, S.H., FACCIOLI, L.H., FERREIRA, S.H., andCUNHA, F.Q. (1997). Participation of interleukin-5, interleukin-8and leukotriene B4 in eosinophil accumulation in two different experimental models. Mem. Inst. Oswaldo Cruz 92 (Suppl. 2),205–210.
13. BLEASE, K., LUKACS, N.W., HOGABOAM, C.M., andKUNKEL, S.L. (2000). Chemokines and their role in airway hy-per-reactivity. Respir. Res. 1, 54–61.
14. WILLIAMS, C.M., and GALLI, S.J. (2000). The diverse potentialeffector and immunoregulatory roles of mast cells in allergic dis-ease. J. Allergy Clin. Immunol. 105, 847–859.
15. KUNG, T.T., STELTS, D., ZURCHER, J.A., JONES, H., UM-LAND, S.P., KREUTNER, W., EGAN, R.W., and CHAPMAN,R.W. (1995). Mast cells modulate allergic pulmonary eosinophiliain mice. Am. J. Respir. Cell Mol. Biol. 12, 404–409.
16. DAS, A.M., FLOWER, R.J., and PERRETTI, M. (1998). Residentmast cells are important for eotaxin-induced eosinophil accumula-tion in vivo. J. Leukocyte Biol. 64, 156–162.
17. YU, C.K., and CHEN, C.L. (2003). Activation of mast cells is es-sential for development of house dust mite Dermatophagoides fari-nae-induced allergic airway inflammation in mice. J. Immunol.171, 3808–3815.
18. TEMKIN, V., KANTOR, B., WEG, V., HARTMAN, M.L., andLEVI-SCHAFFER, F. (2002). Tryptase activates the mitogen-ac-tivated protein kinase/activator protein-1 pathway in human pe-ripheral blood eosinophils, causing cytokine production and re-lease. J. Immunol. 169, 2662–2669.
19. HARTMAN, M., PILIPONSKY, A.M., TEMKIN, V., and LEVI-SCHAFFER, F. (2001). Human peripheral blood eosinophils ex-press stem cell factor. Blood 97, 1086–1091.
20. HOGABOAM, C., KUNKEL, S.L., STRIETER, R.M., TAUB,D.D., LINCOLN, P., STANDIFORD, T.J., and LUKACS, N.W.(1998). Novel role of transmembrane SCF for mast cell activationand eotaxin production in mast cell-fibroblast interactions. J. Im-munol. 160, 6166–6171.
21. GRABBE, J., WELKER, P., MOLLER, A., DIPPEL, E., ASH-MAN, L.K., and CZARNETZKI, B.M. (1994). Comparative cyto-kine release from human monocytes, monocyte-derived immaturemast cells, and a human mast cell line (HMC-1). J. Invest. Der-matol. 103, 504–508.
22. SILLABER, C., BEVEC, D., BUTTERFIELD, J.H., HEPPNER,C., VALENTA, R., SCHEINER, O., KRAFT, D., LECHNER, K.,BETTELHEIM, P., and VALENT, P. (1993). Tumor necrosis fac-tor alpha and interleukin-1 beta mRNA expression in HMC-1 cells:differential regulation of gene product expression by recombinantinterleukin-4. Exp. Hematol. 21, 1271–1275.
23. KRISHNASWAMY, G., HALL, K., YOUNGBERG, G.,HOSSLER, F., JOHNSON, D., BLOCK, W.A., HUANG, S.K.,KELLEY, J., and CHI, D.S. (2002). Regulation of eosinophil-ac-tive cytokine production from human cord blood-derived mastcells. J. Interferon Cytokine Res. 22, 379–388.
24. HALLSWORTH, M.P., SOH, C.P., TWORT, C.H., LEE, T.H., andHIRST, S.J. (1998). Cultured human airway smooth muscle cellsstimulated by interleukin-1beta enhance eosinophil survival. Am.J. Respir. Cell Mol. Biol. 19, 910–919.
25. LEVI-SCHAFFER, F., TEMKIN, V., MALAMUD, V., FELD, S.,and ZILBERMAN, Y. (1998). Mast cells enhance eosinophil sur-vival in vitro: role of TNF-alpha and granulocyte-macrophagecolony-stimulating factor. J. Immunol. 160, 5554–5562.
26. TEMKIN, V., and LEVI-SCHAFFER, F. (2001). Mechanism oftumour necrosis factor alpha mediated eosinophil survival. Cyto-kine 15, 20–26.
27. SHAHABUDDIN, S., PONATH, P., and SCHLEIMER, R.P.(2000). Migration of eosinophils across endothelial cell monolay-ers: interactions among IL-5, endothelial-activating cytokines, andC-C chemokines. J. Immunol. 164, 3847–3854.
28. LILLY, C.M., NAKAMURA, H., KESSELMAN, H., NAGLER-AN-DERSON, C., ASANO, K., GARCIA-ZEPEDA, E.A., ROTHEN-BERG, M.E., DRAZEN, J.M., and LUSTER, A.D. (1997). Expres-sion of eotaxin by human lung epithelial cells: induction by cytokinesand inhibition by glucocorticoids. J. Clin. Invest. 99, 1767–1773.
29. OH, C.K., FILLER, S.G., and CHO, S.H. (2001). Eukaryotic trans-lation initiation factor-6 enhances histamine and IL-2 productionin mast cells. J. Immunol. 166, 3606–3611.
SHAKOORY ET AL.278

30. KITAURA, J., ASAI, K., MAEDA-YAMAMOTO, M., KAWA-KAMI, Y., KIKKAWA, U., and KAWAKAMI, T. (2000). Akt-de-pendent cytokine production in mast 20 cells. J. Exp. Med. 192,729–740.
31. SONG, J.S., HALEEM-SMITH, H., ARUDCHANDRAN, R.,GOMEZ, J., SCOTT, P.M., MILL, J.F., TAN, T.H., and RIVERA,J. (1999). Tyrosine phosphorylation of Vav stimulates IL-6 pro-duction in mast cells by a Rac/c-Jun N-terminal kinase-dependentpathway. J. Immunol. 163, 802–810.
32. HATA, D., KITAURA, J., HARTMAN, S.E., KAWAKAMI, Y.,YOKOTA, T., and KAWAKAMI, T. (1998). Bruton’s tyrosine ki-nase-mediated interleukin-2 gene activation in mast cells. Depen-dence on the c-Jun N-terminal kinase activation pathway. J. Biol.Chem. 273, 10979–10987.
33. HATFIELD, S.M., and ROEHM, N.W. (1992). Cyclosporine andFK506 inhibition of murine mast cell cytokine production. J. Phar-macol. Exp. Ther. 260, 680–688.
34. LEVI-SCHAFFER, F., SEGAL, V., and SHALIT, M. (1991). Ef-fects of interleukins on connective tissue type mast cells co-cul-tured with fibroblasts. Immunology 72, 174–180.
35. LORENTZ, A., KLOPP, I., GEBHARDT, T., MANNS, P., andBISCHOFF, S.C. (2003). Role of activator protein 1, nuclear fac-tor-kappaB, and nuclear factor of activated T cells in IgE receptor-mediated cytokine expression in mature human mast cells. J. Al-lergy Clin. Immunol. 111, 1062–1068.
36. SIMON, H.U., PLOTZ, S., SIMON, D., SEITZER, U., BRAA-THEN, L.R., MENZ, G., STRAUMANN, A., DUMMER, R., andLEVI-SCHAFFER, F. (2003). Interleukin-2 primes eosinophil de-granulation in hypereosinophilia and Wells’ syndrome. Eur. J. Im-munol. 33, 834–839.
37. HOENSTEIN, R., ADMON, D., SOLOMON, A., NORRIS, A.,MOQBEL, R., and 21 LEVI-SCHAFFER, F. (2001). Interleukin-2 activates human peripheral blood eosinophils. Cell. Immunol.210, 116–124.
38. LISSONI, P., BRIVIO, F., VIVIANI, S., and FUMAGALLI, L.(1999). Which immunological parameters are clinically essentialto monitor IL-2 cancer immunotherapy? J. Biol. Regul. Homeost.Agents 13, 110–114.
39. RAND, T.H., SILBERSTEIN, D.S., KORNFELD, H., and WELL-ER, P.F. (1991). Human eosinophils express functional interleukin2 receptors. J. Clin. Invest. 88, 825–832.
40. RAMSHAW, H.S., WOODCOCK, J.M., BAGLEY, C.J., Mc-CLURE, B.J., HERCUS, T.R., and LOPEZ, A.F. (2001). New approaches in the treatment of asthma. Immunol. Cell Biol. 79,154–159.
41. KIMURA, Y., PAWANKAR, R., AOKI, M., NIIMI, Y., andKAWANA, S. (2002). Mast cells and T cells in Kimura’s diseaseexpress increased levels of interleukin-4, interleukin-5, eotaxin andRANTES. Clin. Exp. Allergy 32, 1787–1793.
42. BRESSLER, R.B., LESKO, J., JONES, M.L., WASSERMAN, M.,DICKASON, R.R., HUSTON, M.M., COOK, S.W., and HUSTON,D.P. (1997). Production of IL-5 and granulocyte-macrophagecolony-stimulating factor by naive human mast cells activated byhigh-affinity IgE receptor ligation. J. Allergy Clin. Immunol. 99,508–514.
43. WALLAERT, B., DESREUMAUX, P., COPIN, M.C., TILLIE,I., BENARD, A., COLOMBEL, J.F., GOSSELIN, B., TONNEL,A.B., and JANIN, A. (1995). Immunoreactivity for interleukin 3and 5 and granulocyte/macrophage colony-stimulating factor of intestinal mucosa in bronchial asthma. J. Exp. Med. 182,1897–1904.
44. ISHIZUKA, T., OKAYAMA, Y., KOBAYASHI, H., and MORI,M. (1999). Interleukin-3 production by mast cells from human lung.Inflammation 23, 25–35.
45. DOMAE, M., SAGARA, H., SAKAUE, M., FUKUDA, T., andKAMIKAWA, Y. (2003). The antiallergic drug oxatomide pro-
motes human eosinophil apoptosis and suppresses IL-5-inducedeosinophil survival. J. Allergy Clin. Immunol. 111, 567–572.
46. MORDVINOV, V.A., and SANDERSON, C.J. (2001). Regulationof IL-5 expression. Arch. Immunol. Ther. Exp. (Warsz.) 49,345–351.
47. STIRLING, R.G., VAN RENSEN, E.L., BARNES, P.J., andCHUNG, K.F. (2001). Interleukin-5 induces CD34(1) eosinophilprogenitor mobilization and eosinophil CCR3 expression inasthma. Am. J. Respir. Crit. Care Med. 164, 1403–1409.
48. O’BYRNE, P.M., INMAN, M.D., and PARAMESWARAN, K.(2001). The trials and tribulations of IL-5, eosinophils, and aller-gic asthma. J. Allergy Clin. Immunol. 108, 503–508.
49. CALDENHOVEN, E., VAN DIJK, T.B., RAAIJMAKERS, J.A.,LAMMERS, J.W., KOENDERMAN, L., and DE GROOT, R.P.(1999). Activation of a functionally distinct 80-kDa Stat5 isoformby IL-5 and GM-CSF in human eosinophils and neutrophils. Mol.Cell Biol. Res. Commun. 1, 95–101.
50. ROBOZ, G.J., and RAFII, S. (1999). Interleukin-5 and the regula-tion of eosinophil production. Curr. Opin. Hematol. 6, 164–168.
51. KANKAANRANTA, H., LINDSAY, M.A., GIEMBYCZ, M.A.,ZHANG, X., MOILANEN, E., and BARNES, P.J. (2000). Delayedeosinophil apoptosis in 23 asthma. J. Allergy Clin. Immunol. 106,77–83.
52. GLEICH, G.J. (2000). Mechanisms of eosinophil-associated in-flammation. J. Allergy Clin. Immunol. 105, 651–663.
53. MURATA, K., SUGIE, K., TAKAMURE, M., FUJIMOTO, T.,and UENO, S. (2003). Eosinophilic major basic protein and inter-leukin-5 in eosinophilic myositis. Eur. J. Neurol. 10, 35–38.
54. YAWALKAR, N., SHRIKHANDE, M., HARI, Y., NIEV-ERGELT, H., BRAATHEN, L.R., and PICHLER, W.J. (2000). Ev-idence for a role for IL-5 and eotaxin in activating and recruitingeosinophils in drug-induced cutaneous eruptions. J. Allergy Clin.Immunol. 106, 1171–1176.
55. CELESTIN, J., ROTSCHKE, O., FALK, K., RAMESH, N.,JABARA, H., STROMINGER, J., and GEHA, R.S. (2001). IL-3induces B7.2 (CD86) expression and costimulatory activity in hu-man eosinophils. J. Immunol. 167, 6097–6104.
56. DULKYS, Y., KLUTHE, C., BUSCHERMOHLE, T., BARG, I.,KNOSS, S., KAPP, A., PROUDFOOT, A.E., and ELSNER, J.(2001). IL-3 induces down-regulation of CCR3 protein and mRNAin human eosinophils. J. Immunol. 167, 3443–3453.
57. OCHIAI, K., OMURA, M., MOCHIZUKI, A., ITO, M., andTOMIOKA, H. (1999). Human umbilical vein endothelial cellssupport interleukin-3- and interleukin-5– induced eosinophil dif-ferentiation from cord blood CD341 cells. Int. Arch. Allergy Im-munol. 120 Suppl 1, 2–6.
58. ANDO, M., MIYAZAKI, E., FUKAMI, T., KUMAMOTO, T., andTSUDA, T. (1999). Interleukin-4–producing cells in idiopathic pul-monary fibrosis: an 24 immunohistochemical study. Respirology4, 383–391.
59. KOBAYASHI, H., OKAYAMA, Y., ISHIZUKA, T., PA-WANKAR, R., RA, C., and MORI, M. (1998). Production of IL-13 by human lung mast cells in response to Fcepsilon receptorcross-linkage. Clin. Exp. Allergy 28, 1219–1227.
60. TACHIBANA, H., KUBO, T., MIYASE, T., TANINO, S.,YOSHIMOTO, M., SANO, M., YAMAMOTO-MAEDA, M., andYAMADA, K. (2001). Identification of an inhibitor for interleukin4–induced epsilon germline transcription and antigenspecific IgEproduction in vivo. Biochem. Biophys. Res. Commun. 280, 53–60.
61. ALEXIS, N., GRIFFITH, K., ALMOND, M., and PEDEN, D.B.(2002). IL-4 induces IL- 6 and signs of allergic-type inflammationin the nasal airways of nonallergic individuals336. Clin.Immunol.104, 217–220.
62. WEDI, B., RAAP, U., LEWRICK, H., and KAPP, A. (1998). IL-4–induced apoptosis in peripheral blood eosinophils. J. AllergyClin. Immunol. 102, 1013–1020.
MAST CELL-DERIVED CYTOKINES 279

63. LUTTMANN, W., MATTHIESEN, T., MATTHYS, H., and VIR-CHOW, J.C., Jr. (1999). Synergistic effects of interleukin-4 or in-terleukin-13 and tumor necrosis factoralpha on eosinophil activa-tion in vitro. Am. J. Respir. Cell Mol. Biol. 20, 474–480.
64. TERADA, N., HAMANO, N., HOHKI, G., IKEDA, T., SAI, M.,YAMASHITA, T., and KONNO, A. (1998). The potential role ofinterleukin-13 in eosinophilic inflammation in nasal mucosa. Al-lergy 53, 690–697.
65. DE VRIES, J.E. (1998). The role of IL-13 and its receptor in al-lergy and inflammatory responses. J. Allergy Clin. Immunol. 102,165–169.
66. MATTES, J., YANG, M., MAHALINGAM, S., KUEHR, J.,WEBB, D.C., SIMSON, L., HOGAN, S.P., KOSKINEN, A.,McKENZIE, A.N., DENT, L.A., ROTHENBERG, M.E.,MATTHAEI, K.I., YOUNG, I.G., and FOSTER, P.S. (2002). In-trinsic defect in T cell production of interleukin (IL)-13 in the ab-sence of both IL-5 and eotaxin precludes the development of eo-sinophilia and airways hyperreactivity in experimental asthma. J.Exp. Med. 195, 1433–1444.
67. JARUGA, B., HONG, F., SUN, R., RADAEVA, S., and GAO, B.(2003). Crucial role of IL-4/Stat6 in T cell-mediated hepatitis: up-regulating eotaxins and IL-5 and recruiting leukocytes. J. Immunol.171, 3233–3244.
68. MELLOR, E.A., AUSTEN, K.F., and BOYCE, J.A. (2002). Cys-teinyl leukotrienes and uridine diphosphate induce cytokine gen-eration by human mast cells through an interleukin 4-regulatedpathway that is inhibited by leukotriene receptor antagonists. J.Exp. Med. 195, 583–592.
69. LEE, Y.W., KUHN, H., HENNIG, B., NEISH, A.S., and TOBOREK, M. (2001). IL-4-induced oxidative stress upregulatesVCAM-1 gene expression in human endothelial cells. J. Mol. Cell.Cardiol. 33, 83–94.
70. HICKEY, M.J., GRANGER, D.N., and KUBES, P. (1999). Mo-lecular mechanisms underlying IL-4-induced leukocyte recruitmentin vivo: a critical role for the alpha 4 integrin. J. Immunol. 163,3441–3448.
71. ZIMMERMANN, N., DAUGHERTY, B.L., STARK, J.M., andROTHENBERG, M.E. (2000). Molecular analysis of CCR-3 eventsin eosinophilic cells. J. Immunol. 164, 1055–1064.
72. FUJISAWA, T., KATO, Y., NAGASE, H., ATSUTA, J., TER-ADA, A., IGUCHI, K., KAMIYA, H., MORITA, Y., KITAURA,M., KAWASAKI, H., YOSHIE, O., and HIRAI, K. (2000).Chemokines induce eosinophil degranulation through CCR-3504.J. Allergy Clin. Immunol. 106, 507–513.
73. SIMSON, L., and FOSTER, P.S. (2000). Chemokine and cytokinecooperativity: eosinophil migration in the asthmatic response. Im-munol. Cell Biol. 78, 415–422.
74. AOKI, M., PAWANKAR, R., NIIMI, Y., and KAWANA, S.(2003). Mast cells in basal cell carcinoma express VEGF, IL-8 andRANTES. Int. Arch. Allergy Immunol. 130, 216–223.
75. BAGHESTANIAN, M., HOFBAUER, R., KIENER, H.P.,BANKL, H.C., WIMAZAL, F., WILLHEIM, M., SCHEINER, O.,FUREDER, W., MULLER, M.R., BEVEC, D., LECHNER, K.,and VALENT, P. (1997). The c-kit ligand stem cell factor and anti-IgE promote expression of monocyte chemoattractant protein-1 inhuman lung mast cells. Blood 90, 4438–4449.
76. KING, C.A., ANDERSON, R., and MARSHALL, J.S. (2002).Dengue virus selectively induces human mast cell chemokine pro-duction. J. Virol. 76, 8408–8419.
77. ROMAGNANI, P., DE PAULIS, A., BELTRAME, C., AN-NUNZIATO, F., DENTE, V., MAGGI, E., ROMAGNANI, S.,and MARONE, G. (1999). Tryptase-chymase double-positive hu-man mast cells express the eotaxin receptor CCR3 and are at-tracted by CCR3-binding chemokines. Am. J. Pathol. 155,1195–1204.
78. PRICE, K.S., FRIEND, D.S., MELLOR, E.A., DE JESUS, N.,WATTS, G.F., and BOYCE, J.A. (2003). CC chemokine receptor3 mobilizes to the surface of human mast cells and potentiates immunoglobulin E-dependent generation of interleukin 13. Am. J.Respir. Cell Mol. Biol. 28, 420–427.
79. YING, S., MENG, Q., ZEIBECOGLOU, K., ROBINSON, D.S.,MACFARLANE, A., 27 HUMBERT, M., and KAY, A.B. (1999).Eosinophil chemotactic chemokines (eotaxin, eotaxin-2, RANTES,monocyte chemoattractant protein-3 (MCP-3), and MCP-4), and C-C chemokine receptor 3 expression in bronchial biopsies from atopicand nonatopic (intrinsic) asthmatics. J. Immunol. 163, 6321–6329.
80. HONDA, K., and CHIHARA, J. (1999). Eosinophil activation byeotaxin—eotaxin primes the production of reactive oxygen speciesfrom eosinophils. Allergy 54, 1262–1269.
81. EBISAWA, M., YAMADA, T., BICKEL, C., KLUNK, D., andSCHLEIMER, R.P. (1994). Eosinophil transendothelial migrationinduced by cytokines. III. Effect of the chemokine RANTES. J.Immunol. 153, 2153–2160.
82. HSIEH, F.H., LAM, B.K., PENROSE, J.F., AUSTEN, K.F., andBOYCE, J.A. (2001). T helper cell type 2 cytokines coordinatelyregulate immunoglobulin E-dependent cysteinyl leukotriene pro-duction by human cord blood-derived mast cells: profound induc-tion of leukotriene C(4) synthase expression by interleukin 4. J.Exp. Med. 193, 123–133.
83. OCHI, H., DE JESUS, N.H., HSIEH, F.H., AUSTEN, K.F., andBOYCE, J.A. (2000). IL-4 and -5 prime human mast cells for dif-ferent profiles of IgE-dependent cytokine production. Proc. Natl.Acad. Sci. USA 97, 10509–10513.
84. KRISHNASWAMY, G. (2001). Treatment strategies for bronchialasthma: an update. Hosp. Pract. 36, 25–35.
85. PAWANKAR, R. (2003). Nasal polyposis: an update: editorial review. Curr. Opin. Allergy Clin. Immunol. 3, 1–6.
86. KOWALSKI, M.L., GRZEGORCZYK, J., PAWLICZAK, R., KORNATOWSKI, T., 28 WAGROWSKA-DANILEWICZ, M.,and DANILEWICZ, M. (2002). Decreased apoptosis and distinctprofile of infiltrating cells in the nasal polyps of patients with as-pirin hypersensitivity. Allergy 57, 493–500.
87. MITA, H., ENDOH, S., KUDOH, M., KAWAGISHI, Y., KOBA-YASHI, M., TANIGUCHI, M., and AKIYAMA, K. (2001). Pos-sible involvement of mast-cell activation in aspirin provocation ofaspirin-induced asthma. Allergy 56, 1061–1067.
88. PICADO, C. (2002). Aspirin intolerance and nasal polyposis. Curr.Allergy Asthma Rep. 2, 488–493.
89. GABRIELLI, A., DE NICTOLIS, M., CAMPANATI, G., andCINTI, S. (1983). Eosinophilic fasciitis: a mast cell disorder? Clin.Exp. Rheumatol. 1, 75–80.
90. JANIN-MERCIER, A., BOURGES, M., FONCK-CUSSAC, Y.,BUSSIERES, J.L., LEBLANC, B., and DELAGE, J. (1981).Eosinophilic fasciitis. Ultrastructural study of an early biopsiedcase. Virchows Arch. A Pathol. Anat. Histol. 394, 177–184.
91. GUI, X.Y. (1998). Mast cells: a possible link between psycholog-ical stress, enteric infection, food allergy and gut hypersensitivityin the irritable bowel syndrome. J. Gastroenterol. Hepatol. 13,980–989.
92. OYAIZU, N., UEMURA, Y., IZUMI, H., MORII, S., NISHI, M.,and HIOKI, K. (1985). Eosinophilic gastroenteritis. Immunohisto-chemical evidence for IgE mast cell-mediated allergy. Acta Pathol.Jpn. 35, 759–766.
93. DESCHRYVER-KECSKEMETI, K., and CLOUSE, R.E. (1984).A previously unrecognized subgroup of “eosinophilic gastroen-teritis.” Association with connective tissue diseases. Am. J. Surg.Pathol. 8, 171–180.
94. FINKELMAN, F.D., and URBAN, J.F., Jr. (2001). The other sideof the coin: the protective role of the Th2 cytokines. J. AllergyClin. Immunol. 107, 772–780.
SHAKOORY ET AL.280

95. WILDENBURG, G., KORTEN, S., and BUTTNER, D.W. (1998).Mast cell distribution in nodules of Onchocerca volvulus from un-treated patients with generalized onchocerciasis. Parasitology 116,257–268.
96. BELL, R.G. (1996). IgE, allergies and helminth parasites: a new perspective on an old conundrum. Immunol. Cell Biol. 74,337–345.
97. FERREIRA, M.B., DA SILVA, S.L., and CARLOS, A.G.(2002). Atopy and helminths. Allerg. Immunol. (Paris) 34, 10–12.
98. YAM, L. T., YAM, C.F., and LI, C.Y. (1980). Eosinophilia in sys-temic mastocytosis. Am. J. Clin. Pathol. 73, 48–54.
99. BLAHA, M., KACEROVSKY, J., HRNCIR, Z., NOZICKA, Z.,SPACEK, J., and SIROKY, O. (1977). Systemic mastocytosis. Re-port of a case. Haematologia (Budap.) 11, 349–357.
Address reprint requests or correspondence to:Dr. Guha Krishnaswamy
Department of Internal MedicineP.O Box 70622
East Tennessee State UniversityJohnson City, TN 37614-0622
Tel: (423) 439–6288Fax: (423) 439-6387
E-mail: [email protected]
Received 9 September 2003/Accepted 26 December 2003
MAST CELL-DERIVED CYTOKINES 281