the risk of urinary retention after nerve...
TRANSCRIPT
THE RISK OF URINARY RETENTION AFTER NERVE-SPARING
SURGERY FOR DEEP INFILTRATING ENDOMETRIOSIS:
A SYSTEMATIC REVIEW AND META-ANALYSIS
JOSÉ ANACLETO RESENDE JR (Urology)
LUCIANA CAVALINI (Epidemiology)
CLAUDIO CRISPI (Gynecology)
MARLON FONSECA (Anesthesiology)
*Authors have no competing interests.
Background
• The radical surgical exeresis of the lesions can
improve symptoms and quality of life (the
mainstay of the treatment).
• Important urinary complications may occur
due to iatrogenic injury of autonomic pelvic
nerves.
SEUD 2015 - Marlon Fonseca - Brazil

Background
• Recently, nerve-sparing (NS) approaches have
been performed in order to prevent urinary
complications.
• What about the scientific evidences?
SEUD 2015 - Marlon Fonseca - Brazil
Objective
• To perform a systematic review and a meta-
analysis to assess the risk of urinary retention
(need of urinary catheterization) after a NS
surgery for DIE when compared to classical
(non-NS) techniques.
SEUD 2015 - Marlon Fonseca - Brazil

Methods
• The present review was conduced according
to the MOOSE guidelines for systematic
reviews of observational studies.
[Stroup DF, et al. Meta-analysis of observational studies in epidemiology: a proposal
for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group.
JAMA 2000; 283:2008–2012]
SEUD 2015 - Marlon Fonseca - Brazil
Methods
• Published research articles (up to Dec/2014)
comparing NS technique to non-NS technique
regarding urinary complications after surgery
for DIE.
• Endpoint: relative risk for urinary retention.
SEUD 2015 - Marlon Fonseca - Brazil
Methods
• Inclusion criteria: randomized clinical trials,
intervention and observational studies.
• Exclusion criteria: cancer surgery, bladder or
ureteral resections.
• The same two authors evaluated all publications.
• There were no restrictions for language.
• No attempt was made to identify grey literature.
SEUD 2015 - Marlon Fonseca - Brazil

Combinations of medical subject heading terms (search strategy)
• (Endometriosis) AND (Surgery OR Resection OR Laparotomy OR Laparotomic OR
Open OR Laparoscopy OR Laparoscopic OR Hand Assisted OR Video Assisted OR
Robotic OR Robot OR Nerve sparing OR Colorectal OR Rectum OR Rectosigmoid OR
Intestine OR Bowel OR Pelvic OR Pelvis OR Uterosacral OR Parametrial OR
Parametrium OR Bladder OR Ureter) AND (Nerve OR Nervous OR Plexus) AND
(Urinary OR Retention OR Urethral OR Catheterization OR Complication OR Voiding
OR Disorders OR Dysfunction OR Urologic OR Urological OR Urology OR Bladder OR
Neurogenic OR Incontinence OR Stress OR Overactive OR Urge OR Urgency OR
Urination OR Urodynamics).
SEUD 2015 - Marlon Fonseca - Brazil

Combinations of medical subject heading terms (search strategy)
• (Endometriosis) AND (Surgery OR Resection OR Laparotomy OR Laparotomic OR
Open OR Laparoscopy OR Laparoscopic OR Hand Assisted OR Video Assisted OR
Robotic OR Robot OR Nerve sparing OR Colorectal OR Rectum OR Rectosigmoid OR
Intestine OR Bowel OR Pelvic OR Pelvis OR Uterosacral OR Parametrial OR
Parametrium OR Bladder OR Ureter) AND (Nerve OR Nervous OR Plexus) AND
(Urinary OR Retention OR Urethral OR Catheterization OR Complication OR Voiding
OR Disorders OR Dysfunction OR Urologic OR Urological OR Urology OR Bladder OR
Neurogenic OR Incontinence OR Stress OR Overactive OR Urge OR Urgency OR
Urination OR Urodynamics).
SEUD 2015 - Marlon Fonseca - Brazil
Combinations of medical subject heading terms (search strategy)
• (Endometriosis) AND (Surgery OR Resection OR Laparotomy OR Laparotomic OR
Open OR Laparoscopy OR Laparoscopic OR Hand Assisted OR Video Assisted OR
Robotic OR Robot OR Nerve sparing OR Colorectal OR Rectum OR Rectosigmoid
OR Intestine OR Bowel OR Pelvic OR Pelvis OR Uterosacral OR Parametrial OR
Parametrium OR Bladder OR Ureter) AND (Nerve OR Nervous OR Plexus) AND
(Urinary OR Retention OR Urethral OR Catheterization OR Complication OR Voiding
OR Disorders OR Dysfunction OR Urologic OR Urological OR Urology OR Bladder OR
Neurogenic OR Incontinence OR Stress OR Overactive OR Urge OR Urgency OR
Urination OR Urodynamics).
SEUD 2015 - Marlon Fonseca - Brazil

Combinations of medical subject heading terms (search strategy)
• (Endometriosis) AND (Surgery OR Resection OR Laparotomy OR Laparotomic OR
Open OR Laparoscopy OR Laparoscopic OR Hand Assisted OR Video Assisted OR
Robotic OR Robot OR Nerve sparing OR Colorectal OR Rectum OR Rectosigmoid OR
Intestine OR Bowel OR Pelvic OR Pelvis OR Uterosacral OR Parametrial OR
Parametrium OR Bladder OR Ureter) AND (Nerve OR Nervous OR Plexus) AND
(Urinary OR Retention OR Urethral OR Catheterization OR Complication OR Voiding
OR Disorders OR Dysfunction OR Urologic OR Urological OR Urology OR Bladder OR
Neurogenic OR Incontinence OR Stress OR Overactive OR Urge OR Urgency OR
Urination OR Urodynamics).
SEUD 2015 - Marlon Fonseca - Brazil

Combinations of medical subject heading terms (search strategy)
• (Endometriosis) AND (Surgery OR Resection OR Laparotomy OR Laparotomic OR
Open OR Laparoscopy OR Laparoscopic OR Hand Assisted OR Video Assisted OR
Robotic OR Robot OR Nerve sparing OR Colorectal OR Rectum OR Rectosigmoid OR
Intestine OR Bowel OR Pelvic OR Pelvis OR Uterosacral OR Parametrial OR
Parametrium OR Bladder OR Ureter) AND (Nerve OR Nervous OR Plexus) AND
(Urinary OR Retention OR Urethral OR Catheterization OR Complication OR
Voiding OR Disorders OR Dysfunction OR Urologic OR Urological OR Urology OR
Bladder OR Neurogenic OR Incontinence OR Stress OR Overactive OR Urge OR
Urgency OR Urination OR Urodynamics).
SEUD 2015 - Marlon Fonseca - Brazil

Combinations of medical subject heading terms (search strategy)
• (Endometriosis) AND (Surgery OR Resection OR Laparotomy OR Laparotomic OR
Open OR Laparoscopy OR Laparoscopic OR Hand Assisted OR Video Assisted OR
Robotic OR Robot OR Nerve sparing OR Colorectal OR Rectum OR Rectosigmoid OR
Intestine OR Bowel OR Pelvic OR Pelvis OR Uterosacral OR Parametrial OR
Parametrium OR Bladder OR Ureter) AND (Nerve OR Nervous OR Plexus) AND
(Urinary OR Retention OR Urethral OR Catheterization OR Complication OR Voiding
OR Disorders OR Dysfunction OR Urologic OR Urological OR Urology OR Bladder OR
Neurogenic OR Incontinence OR Stress OR Overactive OR Urge OR Urgency OR
Urination OR Urodynamics).
SEUD 2015 - Marlon Fonseca - Brazil
1270 potentially relevant studies
1. Scin-finder 0
2. Scopus 393
3. Web of Science 577
4. Pubmed 204
5. Cochrane 0
6. Lilacs 96
7. Clinical Trials 0
SEUD 2015 - Marlon Fonseca - Brazil
1270 potentially relevant studies
1. Scin-finder 0
2. Scopus 393
3. Web of Science 577
4. Pubmed 204
5. Cochrane 0
6. Lilacs 96
7. Clinical Trials 0
5 publications were preliminarily
selected because its focus on
complications after NS surgery for
complete excision of DIE.
1 study was excluded due to lacks
regarding follow-up information.
Total = 4 publications
SEUD 2015 - Marlon Fonseca - Brazil
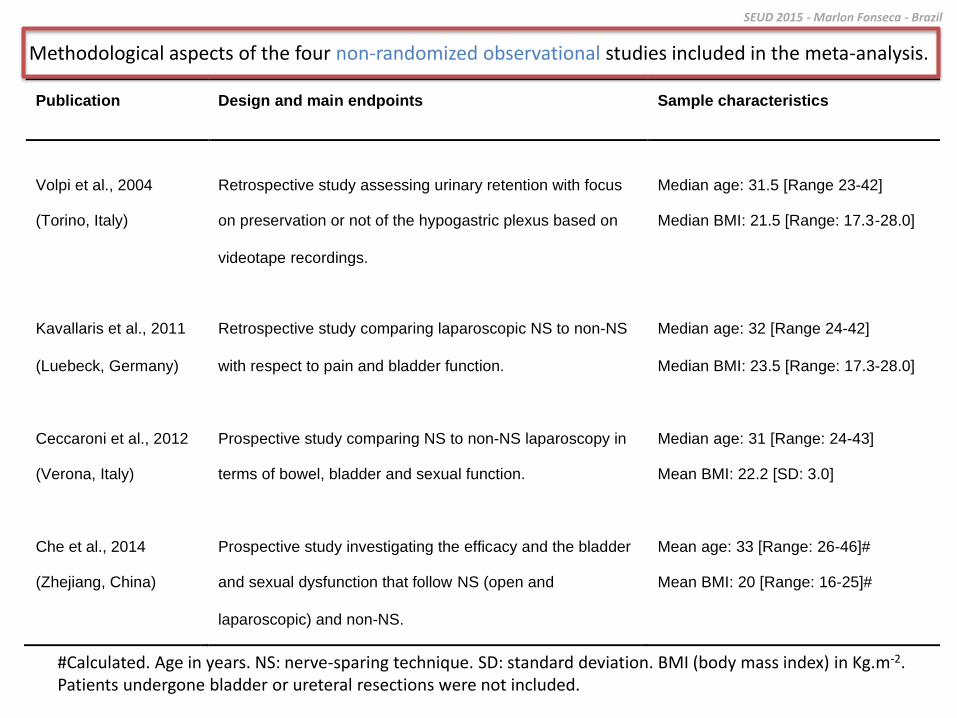
Methodological aspects of the four non-randomized observational studies included in the meta-analysis.
#Calculated. Age in years. NS: nerve-sparing technique. SD: standard deviation. BMI (body mass index) in Kg.m-2. Patients undergone bladder or ureteral resections were not included.
Publication Design and main endpoints Sample characteristics
Volpi et al., 2004
(Torino, Italy)
Retrospective study assessing urinary retention with focus
on preservation or not of the hypogastric plexus based on
videotape recordings.
Median age: 31.5 [Range 23-42]
Median BMI: 21.5 [Range: 17.3-28.0]
Kavallaris et al., 2011
(Luebeck, Germany)
Retrospective study comparing laparoscopic NS to non-NS
with respect to pain and bladder function.
Median age: 32 [Range 24-42]
Median BMI: 23.5 [Range: 17.3-28.0]
Ceccaroni et al., 2012
(Verona, Italy)
Prospective study comparing NS to non-NS laparoscopy in
terms of bowel, bladder and sexual function.
Median age: 31 [Range: 24-43]
Mean BMI: 22.2 [SD: 3.0]
Che et al., 2014
(Zhejiang, China)
Prospective study investigating the efficacy and the bladder
and sexual dysfunction that follow NS (open and
laparoscopic) and non-NS.
Mean age: 33 [Range: 26-46]#
Mean BMI: 20 [Range: 16-25]#
SEUD 2015 - Marlon Fonseca - Brazil

Methodological aspects of the four non-randomized observational studies included in the meta-analysis.
#Calculated. Age in years. NS: nerve-sparing technique. SD: standard deviation. BMI (body mass index) in Kg.m-2. Patients undergone bladder or ureteral resections were not included.
Publication Design and main endpoints Sample characteristics
Volpi et al., 2004
(Torino, Italy)
Retrospective study assessing urinary retention with focus
on preservation or not of the hypogastric plexus based on
videotape recordings.
Median age: 31.5 [Range 23-42]
Median BMI: 21.5 [Range: 17.3-28.0]
Kavallaris et al., 2011
(Luebeck, Germany)
Retrospective study comparing laparoscopic NS to non-NS
with respect to pain and bladder function.
Median age: 32 [Range 24-42]
Median BMI: 23.5 [Range: 17.3-28.0]
Ceccaroni et al., 2012
(Verona, Italy)
Prospective study comparing NS to non-NS laparoscopy in
terms of bowel, bladder and sexual function.
Median age: 31 [Range: 24-43]
Mean BMI: 22.2 [SD: 3.0]
Che et al., 2014
(Zhejiang, China)
Prospective study investigating the efficacy and the bladder
and sexual dysfunction that follow NS (open and
laparoscopic) and non-NS.
Mean age: 33 [Range: 26-46]#
Mean BMI: 20 [Range: 16-25]#
Temporal evolution
SEUD 2015 - Marlon Fonseca - Brazil

What is nerve-sparing surgery..?
NS: nerve-sparing technique. Patients undergone bladder or ureteral resections were not included. DIE: deep infiltrating endometriosis.
SEUD 2015 - Marlon Fonseca - Brazil
Publication Description of nerve-sparing technique Urinary catheters after surgery
Volpi et al., 2004 Objective; based on radical hysterectomy technique described
by Trimbos et al. (2001).
Removed on 2nd
day.
Urinary retention was tested immediately after first voiding
(method not described).
Kavallaris et al., 2011 Comprehensive; representing a strategy to preserve nerves in
DIE surgery.
Removed on 1st day.
NS group: ISC if urinary residual urine volume >50 mL in two
ultrasound measurements.
Non-NS group: ISC if self-reported bladder dysfunction with
incomplete emptying of the bladder (details not described).
Ceccaroni et al., 2012 The most meticulous description; focused on DIE with segmental
rectal and parametrial resection.
Removed on 1st day.
ISC at discharge when voiding difficulty or urinary retention >100
mL on 3 consecutive catheterizations.
Che et al., 2014 Reported as the same used by Volpi et al (2004). Some patients needed ISC (criteria/methods not described).
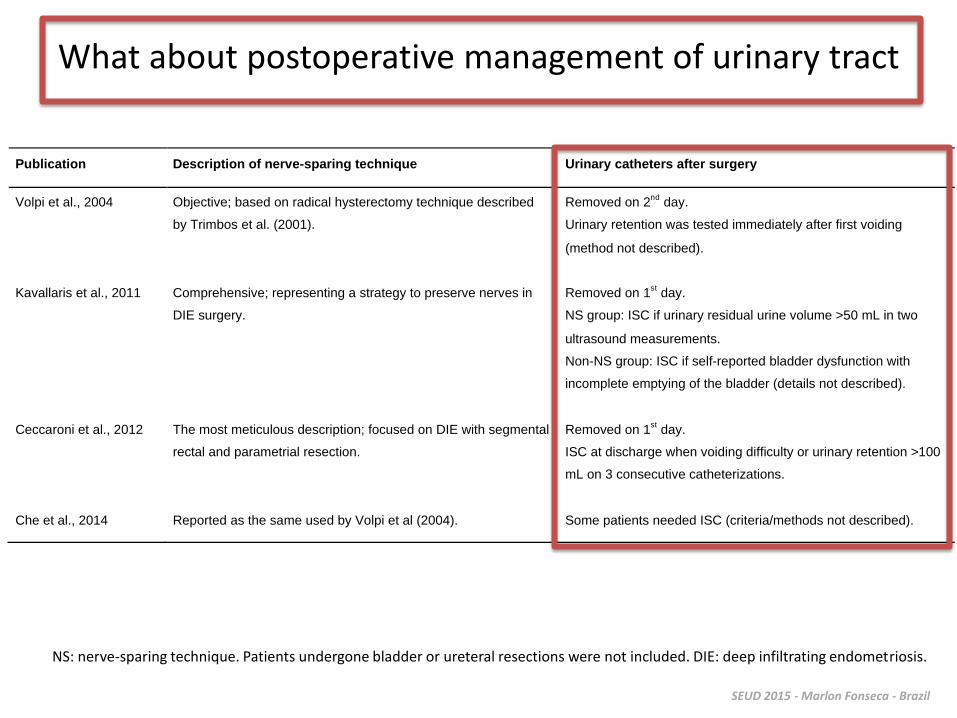
What about postoperative management of urinary tract
NS: nerve-sparing technique. Patients undergone bladder or ureteral resections were not included. DIE: deep infiltrating endometriosis.
SEUD 2015 - Marlon Fonseca - Brazil
Publication Description of nerve-sparing technique Urinary catheters after surgery
Volpi et al., 2004 Objective; based on radical hysterectomy technique described
by Trimbos et al. (2001).
Removed on 2nd
day.
Urinary retention was tested immediately after first voiding
(method not described).
Kavallaris et al., 2011 Comprehensive; representing a strategy to preserve nerves in
DIE surgery.
Removed on 1st day.
NS group: ISC if urinary residual urine volume >50 mL in two
ultrasound measurements.
Non-NS group: ISC if self-reported bladder dysfunction with
incomplete emptying of the bladder (details not described).
Ceccaroni et al., 2012 The most meticulous description; focused on DIE with segmental
rectal and parametrial resection.
Removed on 1st day.
ISC at discharge when voiding difficulty or urinary retention >100
mL on 3 consecutive catheterizations.
Che et al., 2014 Reported as the same used by Volpi et al (2004). Some patients needed ISC (criteria/methods not described).

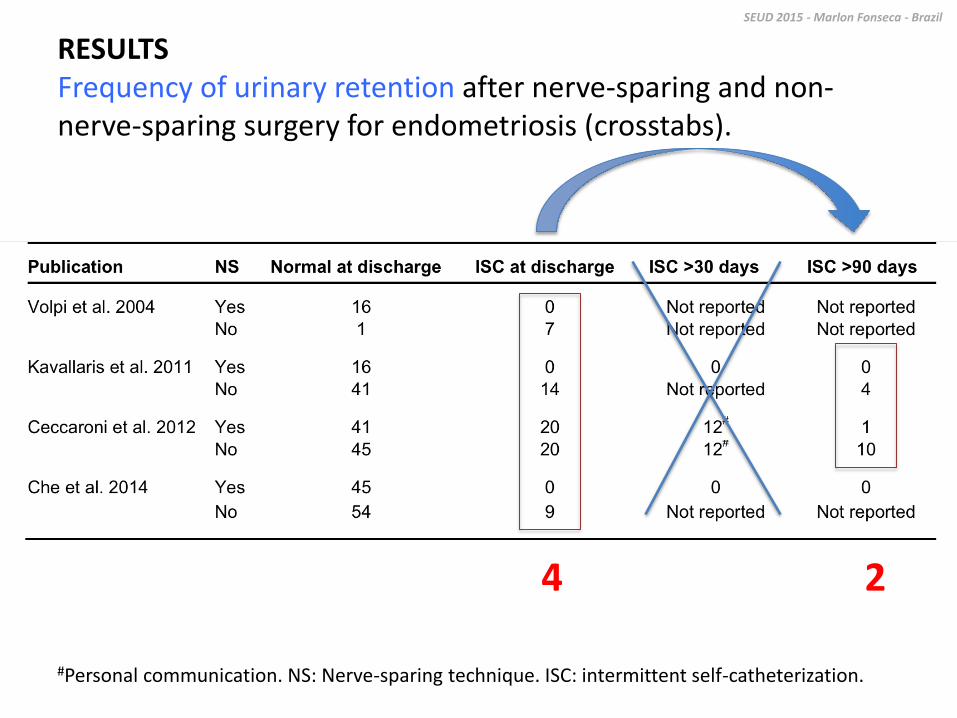
#Personal communication. NS: Nerve-sparing technique. ISC: intermittent self-catheterization.
RESULTS Frequency of urinary retention after nerve-sparing and non-nerve-sparing surgery for endometriosis (crosstabs).
SEUD 2015 - Marlon Fonseca - Brazil
#Personal communication. NS: Nerve-sparing technique. ISC: intermittent self-catheterization.
RESULTS Frequency of urinary retention after nerve-sparing and non-nerve-sparing surgery for endometriosis (crosstabs).
SEUD 2015 - Marlon Fonseca - Brazil
4 2
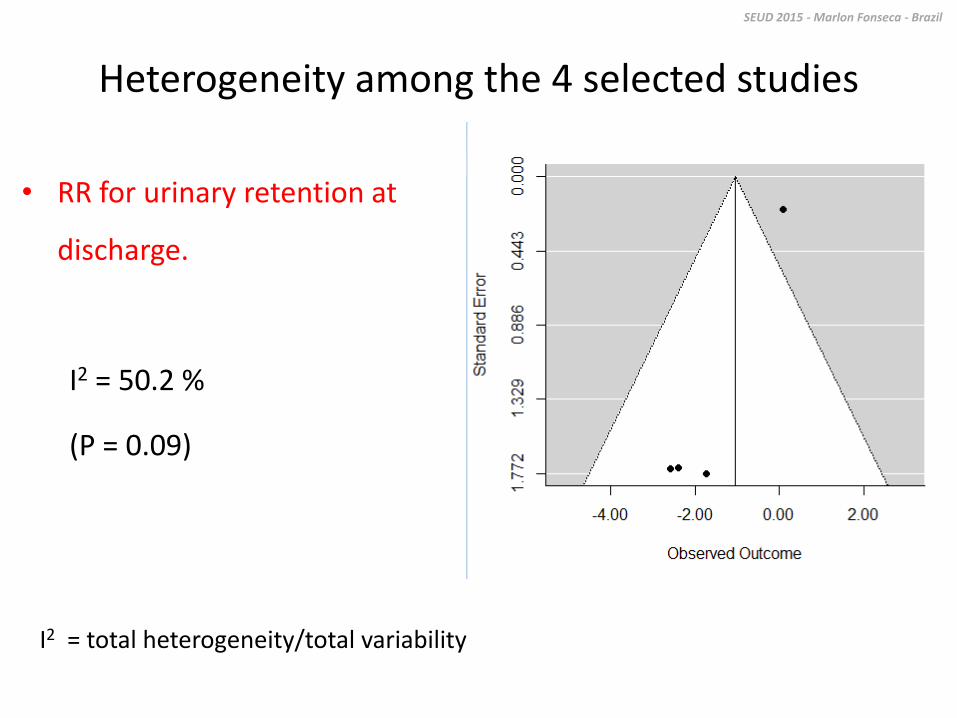
Heterogeneity among the 4 selected studies
• RR for urinary retention at
discharge.
I2 = 50.2 %
(P = 0.09)
SEUD 2015 - Marlon Fonseca - Brazil
I2 = total heterogeneity/total variability

Common RR for ISC at discharge in the NS group in relation
to the classical technique was 0.19 [95%CI: 0.03–1.17]
SEUD 2015 - Marlon Fonseca - Brazil

The common RR for need of ISC after 90 days was
0.16 [95%CI: 0.03-0.84]
SEUD 2015 - Marlon Fonseca - Brazil
Discussion
• A significant advantage of NS with respect to the
risk of persistent urinary retention (need of ISC for
3 months or more)
• No significant benefits of NS concerning the need of
ISC immediately after surgery (?)
• The criteria for indicating ISC after surgery has been
empirical (and not the same)
SEUD 2015 - Marlon Fonseca - Brazil
What about urinary function before surgery..?
SEUD 2015 - Marlon Fonseca - Brazil

CONCLUSION
• Considering the surgical treatment of DIE, a NS
technique showed a significant lower risk of
persistent urinary retention due to iatrogenic
injury of autonomic pelvic nerves when
compared to a classical (non-NS) technique.
SEUD 2015 - Marlon Fonseca - Brazil

Recommendations
• Clinical studies are required for evaluating concrete
consequences of different persistent residual urinary
volumes and the best individual postoperative
urinary tract management.
• Unnecessary invasive emptying of the bladder must
always be avoided, which is (at least) a risky,
inconvenient and uncomfortable duty.
SEUD 2015 - Marlon Fonseca - Brazil