the risk manager’s role in practitioner credentialing
TRANSCRIPT

The Risk Manager’s Role in Practitioner Credentialing

WHO ARE THESE PEOPLE?
When you go to the hospital seeking medical care, how do you know that the doctors are properly trained, licensed, and qualified to take care of you?

Why Credential?
Patient Safety
Risk Management - Negligent Credentialing
Accreditation and Regulatory Requirements

Definitions
Credentialing – The process of collecting, assessing and validating the qualifications and credentials against established criteria.
Privileging – The process health care organizations use to determine the specific procedures and treatments each health care practitioner may perform based on training and current competence.

Competence
Education
Training
Work History
Patient Care
Medical
Knowledge
Judgment
Technical
Skills
Practice
BasedLearni
ng
CommunicationSkills
System
BasedPracti
ce
Professionalism
Criminal
Background
NPDB
PatientComplain
ts
Claims History
HealthStaffComplaints

Negligent Credentialing Negligence is conduct that is
culpable because it falls short of what a reasonable person would do to protect another individual from a foreseeable risk of harm
Organizations can be found liable for negligent credentialing

Negligent Credentialing Cases
Darling v Charleston Memorial Community Hospital, 211 N.E. 2d
253 (Ill. 1965)
Hospital liable for negligent treatment resulting in amputation of teenager’s leg. Nurses failed to monitor; physician failed to consult; hospital claimed charitable immunity doctrine-court ruled against hospital for failure to provide proper supervision.

Errors in Credentialing Process
Information Errors
Process Errors
Decision Errors

Information Errors
Information existed that could have been known but wasn’t, and the information would have impacted a credentialing decision
Silos
MSS Quality Risk Medical Records

Information Errors
Elam v College Park Hospital, 132 Cal. App. 332, 183 Cal. Rptr. 156 (Ca. 1982):
Hospital liable for podiatrist’s negligence; failed to obtain malpractice claims data, even though medical records department was aware of claims-court ruled negligent credentialing.
Significant Court Decisions
Johnson v Misericordia Community Hospital, 294 N.W. 2d 501, 97 Wis. 2d 521 (Wis. 1981)
Hospital liable to patient injured by physician who had failed to disclose pending malpractice cases and lied about privileges at other hospitals; should have verified information-court ruled negligent credentialing; failure of initial credentialing process

Process Errors Failing to follow bylaws,
regulations and/or policies
Not consistently applying processes, requirements and criteria
Adopting an unreasonable policy and/or criteria

Lawrence R. Poliner, MD v. Texas Health Systems, James
Knochel, MD Upon review, the advisory committee
recommended a temporary restriction of Dr. Poliner's cardiac catheterization lab privileges for up to 15 days. Dr. Poliner agreed in writing after he was told he would receive a summary suspension of all his privileges if he didn't agree to the penalty.
Dr. Poliner brought federal and state antitrust claims, along with tort and breach of contract claims, against the defendants. A lengthy legal battle ensued, the result of which has significant meaning for those administering peer review and the physicians under evaluation.

Lawrence R. Poliner, MD v. Texas Health Systems, James Knochel,
MD The jury determined the defendants weren't
entitled to federal or state immunity. Jurors awarded Dr. Poliner more than $360 million in damages, $90 million of which were for alleged mental anguish and injury to career and reputation on Dr. Poliner's defamation claims and $110 million of which were for punitive damages.
The district court reduced the defamation damages to $22.5 million to comply with the law. Prejudgment interest added up to more than $11 million, making the total award more than $33 million.
Lawrence R. Poliner, MD v. Texas Health Systems, James Knochel,
MD On July 23, 2008, the 5th Circuit Court of
Appeals reversed the federal trial court's judgment and ruled for the hospital and Dr. Knochel based on federal immunity for their actions.
Dallas attorney Lewis Lefko, JD, said the Poliner case sends a message to entities conducting peer review that they should make every effort to follow their bylaws and treat physicians fairly.
"The Poliner case says that if you don't do it right, it may not look reasonable to a physician or to a jury," he said.

Decision Errors
The necessary information was known, but medical staff leaders failed to make a wise decision.
Failure to address concerns identified in the credentialing & recredentialing process.
One red flag may not be a problem or concern in itself but more than one
suggests closer scrutiny.

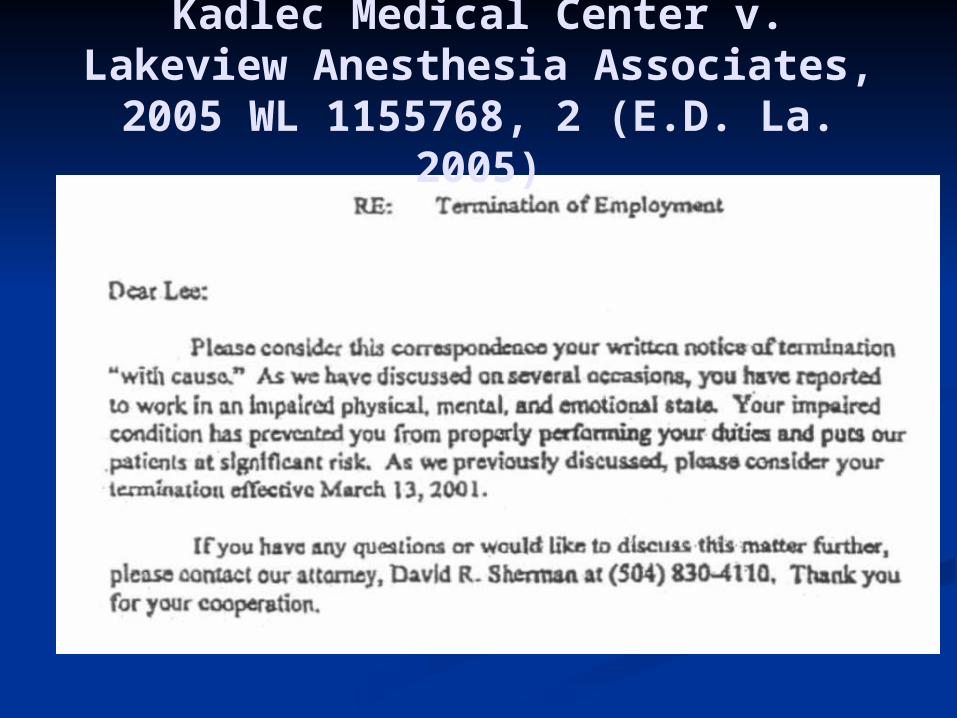
Kadlec Medical Center v. Lakeview Anesthesia Associates, 2005 WL
1155768, 2 (E.D. La. 2005)
Dr. Berry was known to have diverted controlled drugs for personal use at an Alabama hospital and appeared to have been under their influence when on duty. He was fired and lost privileges. Hired in Washington State. Harmed a patient (a young women in a non-responsive vegetative state) as a result of drug abuse problem.

Kadlec Medical Center v. Lakeview Anesthesia Associates, 2005 WL
1155768, 2 (E.D. La. 2005)

Kadlec Medical Center v. Lakeview Anesthesia Associates, 2005 WL
1155768, 2 (E.D. La. 2005)

Best Practices
Provide correct information when responding to verification requests
Don’t omit key information when providing verifications
Address letter to Credentialing and/or MEC
Sign as Agent of MEC
Best Practices
In addition to viewing a government issued photo identification, send the applicant’s picture with reference and training requests.
Why?
“Dr.” Gerald Barnes legally changed his name in the 1970’s to Gerald Barnes, the name of a licensed physician who was practicing in Stockton, California. He obtained copies of Dr. Barnes’ records and medical credentials and used the documents to obtain employment at numerous medical clinics and offices in Southern California.


Best Practices
Verify all clinical work history (when possible).
Request information from past groups as well as hospitals

Why?
Michael Swango, M.D.
In 1985, he was convicted of aggravated battery for the non-fatal poisoning of co-workers at an ambulance service. He spent 30 months in prison and lost his medical license. Despite his record, he was able to get jobs at hospitals in South Dakota, Virginia, New York and Zimbabwe. He is believed to have killed as many as 35 patients and is suspected in more than 60 deaths.
“Blind Eye: The Story of A Doctor who Got Away with Murder” by James Stewart.
Best Practices
Include practitioner’s picture in notices to departments.
Clinical areas should have access to privileges granted to each practitioner
Pictures included with privileging information


Best Practices

Why?
“Dr.” Ofari Mays
October 2005, Orlando Florida – Mr. Mays was arrested and accused of impersonating a doctor. He spent days at Orlando Regional Medical Center dressed in scrubs and lab coat. He had access to the hospital, reviewed patient records and discussed treatments with nurses and other doctors.

Best Practices
Sharing of information between hospitals
MS.06.01.05 EP 9Before recommending privileges, the organized medical staff also evaluates the following:
Relevant practitioner-specific data as compared to aggregate data, when available
Morbidity and mortality data, when available
NAMSS PASS
NAMSS PASS™ is a secure, online database that provides quick, easy, and inexpensive access to the affiliation history of practitioners and is the first and only universal resource for tracking practitioner affiliation history.

NAMSS PASS

NAMSS PASS


NAMSS PASS

Best Practices Google applicants Sharing of information medical staff,
quality and risk management within organization
Self query NPDB Don’t deny privileges –table requests
pending documentation. NPDB Continuous Query Program Additional reference Document current competence at
reappointment.

Risk Managers Advocate for education and training
for medical staff professionals and medical staff leaders
Encourage networking with other medical staff professionals
Champion certifications for medical staff professionals
Open communication with medical staff professionals

Risk Managers
Review credentialing policies and processes
Review reference, affiliation, and training verification forms
Review and collaborate on wording of sensitive topics and discussions in meeting minutes
Review and collaborate on sensitive affiliation verification responses