the riddle of uveitis*
TRANSCRIPT

POSTGRAD. MED. J. (1964), 40, 686
THE RIDDLE OF UVEITIS*
D. GERAINT JAMES, M.A., M.D.(Cantab), F.R.C.P.Consultant Physician, Royal Northern Hospital and
Medical Ophthalmology Unit, Lambeth Hospital, London.
INFLAMMATION of the uveal tract, which com-prises the iris, ciliary body and choroid, is thecause in 8.3% of cases of blindness in thefourth decade of life and in 2.5% of all casesof blindness in Britain (Sorsby 1956). In otherwords, about 2,500 of the 100,000 registeredblind people in this country were blinded byuveitis and its complications, and this wasparticularly so in young people in the 30-40decade. It is traditional to subdivide uveitisinto anterior uveitis (or iridocyclitis) andposterior uveitis (or choroiditis), but it is onlyconvenient to retain this concept if it can con-tribute a better understanding of the causes ormechanisms of the inflammatory process. Itshould nevertheless be remembered that it isan artificial distinction since the iris-ciliary-body-choroid is a continuous structure, derivedfrom the mesoderm surrounding the optic cup,and this uveal tract is extremely vascular. Itwould indeed be surprising if inflammation ofthe anterior part did not affect the posteriorpart and vice-versa.
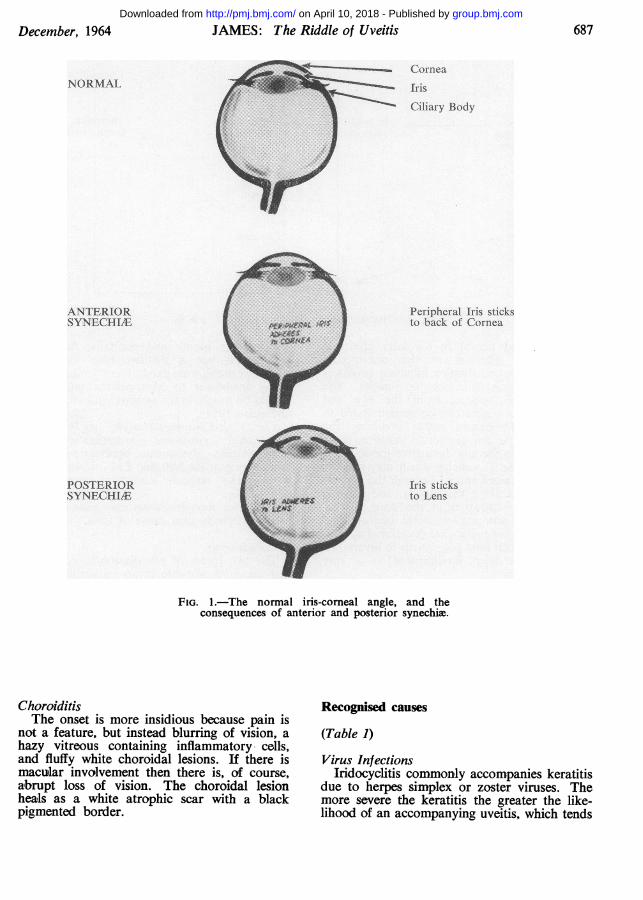
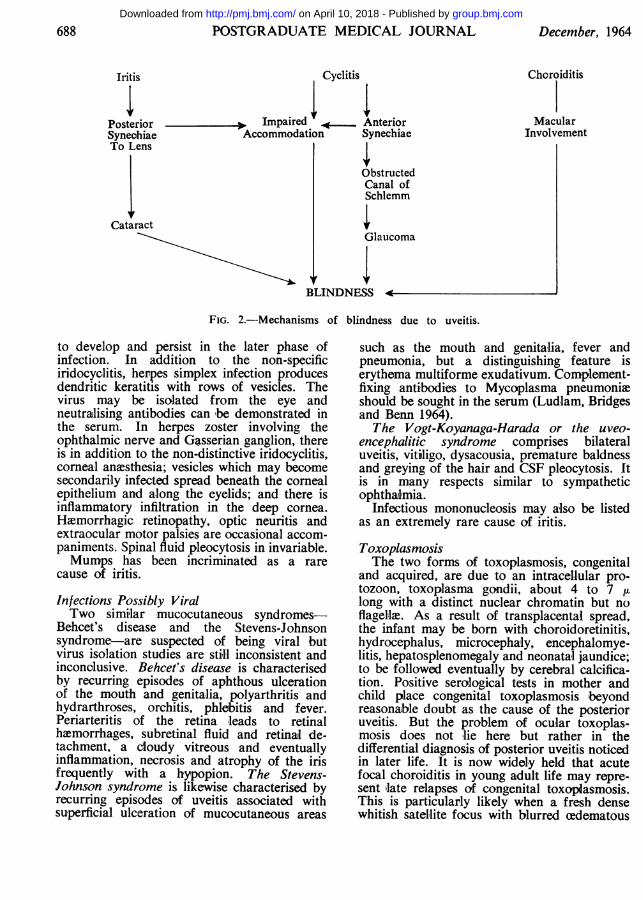
Mechanism of BlindnessInflammatory exudate in the uveal tract leads
to adhesions (synechiae) which ultimately stickthe peripheral iris to the back of the cornea(anterior synechiae) or the iris adheres to thefront of the lens (posterior synechiae) (Fig. 1).Over the years, the pupil aperture is obliteratedand, with ciliary damage, leads to loss ofaccommodation; defective drainage leads toglaucoma; lens involvement leads to cataractformation; and finally macular involvement dueto choroiditis directly leads to failure of vision.There is often an interplay of several of thesefactors (Fig. 2).Classification of Endogenous Uveitis
Uveitis may be secondary to penetrating*Based on the Presidential Address delivered to theHarveian Society of London, January, 15th, 1964.
wounds or other trauma, or follow chemicalswhich inflame any of the anterior layers of theeye. Uveitis may also follow surgical inter-vention or be secondary to some local in-traocular cause. All these instances are usuallyobvious examples of exogenous or secondaryuveitis. The ophthalmologist is not perplexedby the cause; and the management, wheneverpossible, is to remove the irritative source ofthe inflammation.The riddle of uveitis lies in the causes and
course of endogenous uveitis. Our presentignorance of the cause of the great majorityof instances of endogenous uveitis precludes asatisfactory aetiological classification, and theanatomical classification into iridocyclitis andchoroiditis is artificial and probably inaccurate.Our only means at present is a descriptiveclassification combining anatomical and aetio-logical (when known) features and definingdirect complications when they add to thepicture. Thus a patient with sarcoid uveitismight be classified as iridocyclitis, associatedchoroiditis, due to sarcoidosis, with glaucomasecondary to cyclitis. Likewise, choroiditis,peripheral, due to toxoplasmosis, with fielddefect due to macular lesion. This is the basisof coded classifications and will remain onlyuntil the multiple causes have been deciphered.IridocyclitisThe onset of an acute attack is abrupt with
pain, photophobia, lacrimation and blurredvision. Vascular injection involves ciliary andconjunctival vessels, and the characteristicciliary or circumcorneal congestion is deep tothe conjunctiva. The pupil is small because ofspasm, the iris is oedematous; there is anoutpouring of inflammatory cells both into theaqueous and to become stuck to the back ofthe cornea (keratic precipitates). Fibrinousexudate leads to adhesions and the end resultof repeated attacks may be secondary glaucomaor cataract formation.
group.bmj.com on April 10, 2018 - Published by http://pmj.bmj.com/Downloaded from
December, 1964 JAMES: The Riddle of Uveitis 687
ComeaNORMAL
: Ciary Body
ANTERIOR Per. al Iris sticksSYNECL - to biack of Cornea
OSERIOR .ris sticks
FIG. 1.-The normal iris-comeal angle, and theconsequences of anterior and posterior synechime.
FI.1 h omliiVcrelage n hconequnce of antrio an'otrorsn i.'
ChoroiditisThe onset is more insidious because pain is
not a feature, but instead blurring of vision, ahazy vitreous containing inflammatory cells,and fluffy white choroidal lesions. If there ismacular involvement then there is, of course,abrupt loss of vision. The choroidal lesionheals as a white atrophic scar with a blackpigmented border.
Recognised causes
(Table 1)Virus Infections
Iridocyclitis commonly accompanies keratitisdue to herpes simplex or zoster viruses. Themore severe the keratitis the greater the like-lihood of an accompanying uveitis, which tends
group.bmj.com on April 10, 2018 - Published by http://pmj.bmj.com/Downloaded from
688 POSTGRADUATE MEDICAL JOURNAL December, 1964
Iritis Cyclitis Choroiditis
Posterior Impaired _ Anterior MacularSyneohiae Accommodation Synechiae InvolvementTo Lens
ObstructedCanal ofSchlemm
CataractGlaucoma
BLINDNESS
FIG. 2.--Mechanisms of blindness due to uveitis.
to develop and persist in the later phase ofinfection. In addition to the non-specificiridocyclitis, herpes simplex infection producesdendritic keratitis with rows of vesicles. Thevirus may be isolated from the eye andneutralising antibodies can -be demonstrated inthe serum. In herpes zoster involving theophthalmic nerve and Gasserian ganglion, thereis in addition to the non-distinctive iridocyclitis,corneal anaesthesia; vesicles which may becomesecondarily infected spread beneath the cornealepithelium and along the eyelids; and there isinflammatory infiltration in the deep cornea.Haemorrhagic retinopathy, optic neuritis andextraocular motor palsies are occasional accom-paniments. Spinal fluid pleocytosis in invariable.Mumps has been incriminated as a rare
cause of iritis.
Infections Possibly ViralTwo similar mucocutaneous syndromes-
Behcet's disease and the Stevens-Johnsonsyndrome-are suspected of being viral butvirus isolation studies are still inconsistent andinconclusive. Behcet's disease is characterisedby recurring episodes of aphthous ulcerationof the mouth and genitalia, polyarthritis andhydrarthroses, orchitis, phlebitis and fever.Periarteritis of the retina leads to retinalhaemorrhages, subretinal fluid and retinal de-tachment, a Cloudy vitreous and eventuallyinflammation, necrosis and atrophy of the irisfrequently with a hypopion. The Stevens-Johnson syndrome is likewise characterised byrecurring episodes of uveitis associated withsuperficial ulceration of mucocutaneous areas
such as the mouth and genitalia, fever andpneumonia, but a distinguishing feature iserythema multiforme exudativum. Complement-fixing antibodies to Mycoplasma pneumoniaeshould be sought in the serum (Ludlam, Bridgesand Benn 1964).The Vogt-Koyanaga-Harada or the uveo-
encephalitic syndrome comprises bilateraluveitis, vitiiligo, dysacousia, premature baldnessand greying of the hair and CSF pleocytosis. Itis in many respects similar to sympatheticophthalmia.
Infectious mononucleosis may also be listedas an extremely rare cause of iritis.
ToxoplasmosisThe two forms of toxoplasmosis, congenital
and acquired, are due to an intracellular pro-tozoon, toxoplasma gondii, about 4 to 7 tulong with a distinct nuclear chromatin but noflagella. As a result of transplacental spread,the infant may be born with choroidoretinitis,hydrocephalus, microcephaly, encephalomye-litis, hepatosplenomegaly and neonatal jaundice;to be followed eventually by cerebral calcifica-tion. Positive serological tests in mother andchild place congenital toxoplasmosis beyondreasonable doubt as the cause of the posterioruveitis. But the problem of ocular toxoplas-mosis does not lie here but rather in thedifferential diagnosis of posterior uveitis noticedin later life. It is now widely held that acutefocal choroiditis in young adult life may repre-sent late relapses of congenital toxoplasmosis.This is particularly likely when a fresh densewhitish satellite focus with blurred oedematous
group.bmj.com on April 10, 2018 - Published by http://pmj.bmj.com/Downloaded from
December, 1964 JAMES: The Riddle of Uveitis 689
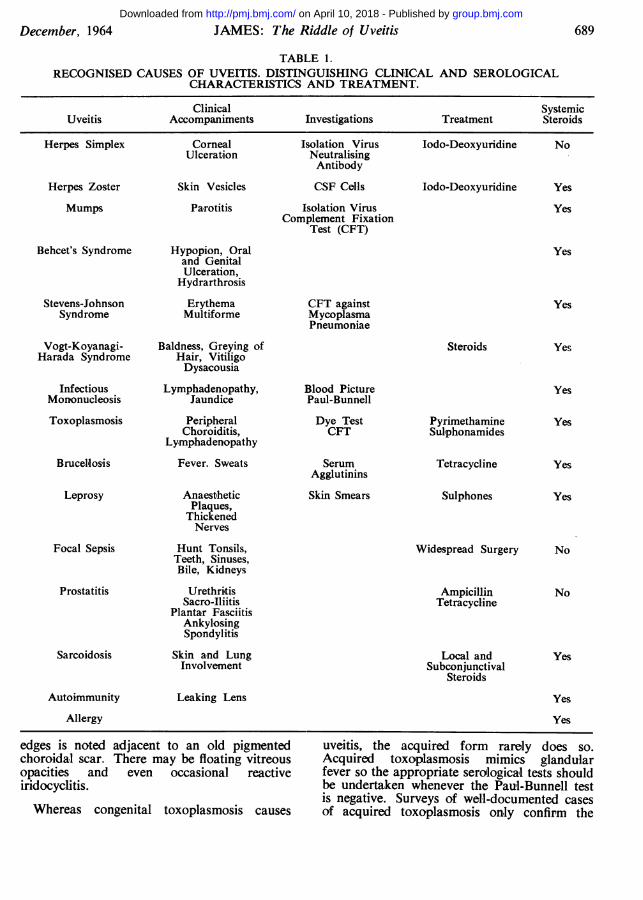
TABLE 1.RECOGNISED CAUSES OF UVEITIS. DISTINGUISHING CLINICAL AND SEROLOGICAL
CHARACTERISTICS AND TREATMENT.
Clinical SystemicUveitis Accompaniments Investigations Treatment Steroids
Herpes Simplex Corneal Isolation Virus Iodo-Deoxyuridine NoUlceration Neutralising
AntibodyHerpes Zoster Skin Vesicles CSF Cells Iodo-Deoxyuridine Yes
Mumps Parotitis Isolation Virus YesComplement Fixation
Test (CFT)Behcet's Syndrome Hypopion, Oral Yes
and GenitalUlceration,
HydrarthrosisStevens-Johnson Erythema CFT against Yes
Syndrome Multiforme MycoplasmaPneumoniae
Vogt-Koyanagi- Baldness, Greying of Steroids YesHarada Syndrome Hair, Vitiligo
DysacousiaInfectious Lymphadenopathy, Blood Picture Yes
Mononucleosis Jaundice Paul-Bunnell
Toxoplasmosis Peripheral Dye Test Pyrimethamine YesChoroiditis, CFT Sulphonamides
LymphadenopathyBrucellosis Fever. Sweats Serum Tetracycline Yes
AgglutininsLeprosy Anaesthetic Skin Smears Sulphones Yes
Plaques,ThickenedNerves
Focal Sepsis Hunt Tonsils, Widespread Surgery NoTeeth, Sinuses,Bile, Kidneys
Prostatitis Urethritis Ampicillin NoSacro-Iliitis Tetracycline
Plantar FasciitisAnkylosingSpondylitis
Sarcoidosis Skin and Lung Local and YesInvolvement Subconjunctival
Steroids
Autoimmunity Leaking Lens Yes
Allergy Yes
edges is noted adjacent to an old pigmentedchoroidal scar. There may be floating vitreousopacities and even occasional reactiveiridocyclitis.Whereas congenital toxoplasmosis causes
uveitis, the acquired form rarely does so.Acquired toxoplasmosis mimics glandularfever so the appropriate serological tests shouldbe undertaken whenever the Paul-Bunnell testis negative. Surveys of well-documented casesof acquired toxoplasmosis only confirm the
group.bmj.com on April 10, 2018 - Published by http://pmj.bmj.com/Downloaded from
690 POSTGRADUATE MEDICAL JOURNAL December, 1964
rarity of uveitis as a manifestation of theacquired infection.The difficulties of recognising clinical ocular
toxoplasmosis are hampered still further bysome uncertainty in interpretation of theserological tests, which comprise the cytoplasm-modifying antibody or dye test and the com-plement-fixation test. About one-third ofnormal adults' sera give a positive dye testtitre up to 1: 128, and about 1% of normalsera may be expected to register a titreof 1:256. Although these titres indicate pastinfection, they must be interpreted with cautionwhen associated with a recent acute uveitis.Complement fixation test titres of 1: 4 or moreoccur in about 5% of the adult population.The dye test is the one routinely used inBritain for screening purposes. A negative testhelps to exclude toxoplasmosis and a fourfoldrise or fall in titres suggests recent infection.
Bacterial Infections. Brucellosis and leprosyare insignificant causes of uveitis in Britain.In endemic zones, tuberculoid leprosy is com-monly associated with troublesome iridocyclitis.It is interesting that leprosy should be almostentirely confined to the anterior uveal tract.Uveitis can no longer be ascribed to humantuberculosis, but anonymous or unclassifiedmycobacteria cannot be excluded as occasionalcausal agents, either of direct infection or,more likely, of hypersensitivity reactionsinvolving the uveal tract. Leptospirosismay also be complicated by anterior or pos-terior uveitis, either due to direct haematogenousinvolvement or as a hypersensitivity pheno-menon.
Focal sepsis is no longer fashionable unlessthe focus is in the prostate. Catterall (1961)investigated 211 men with uveitis and foundprostatovesiculitis in 69% (in controls of thesame age-group in the general medical andsurgical wards of two hospitals the prevalencewas 19%). Of male patients with acute anterioruveitis, no 'less than four-fifths had chronicprostatitis. Commonly associated with chronicprostatitis and uveitis were ankylosing spondy-litis, arthritis, sacro-iliitis, conjunctivitis,urethritis and plantar fasciitis. Nevertheless,extensive investigations failed to reveal a causalorganism. The fact that no such organism hasbeen identified in the century and a half sinceBrodie (1818) first drew attention to the syn-drome suggests that the cause may after allnot ibe infective.
SarcoidosisWhereas eye involvement, predominantly
uveitis, occurs in one-quarter of patients withsarcoidosis, nonetheless sarcoidosis is respon-sible for only about 4% of cases of uveitis(James, Anderson, Langley and Ainslie 1964).Sarcoid uveitis is most commonly acute irido-cyclitis. Evidence of involvement of othertissue systems is widespread, for iridocyclitis isaccompanied by intrathoracic involvement innearly three-quarters of instances, by skinlesions in one-half, and lymph node enlargementin one-third of cases. Sarcoid uveitis is part ofa multisystem disease with diagnostic clinicalfeatures elsewhere. Moreover the negativeMantoux test and positive Kveim test alsoserve to distinguish this cause of uveitis.
Lens-induced UveitisIt seems likely that certain individuals
develop hypersensitivity to lens protein eitherdue to local leaking or postoperatively if anylens material is left in the anterior chamberafter cataract extraction.
Rheumatic IridocyclitisIridocyclitis has been estimated to occur in
16% of patients with ankylosing spondylitisand 4.7% with rheumatoid arthritis (Woods1961). We find rheumatic disease of either ofthese two types to be present in about 10%of patients with iridocyclitis, and some abnor-mality or another of the sacro-iliac joints in upto one-third of our series with iridocyclitis.These associations form part of a wide spectrumof disease pattern in men comprising prostatitis,plantar fasciitis, polyarthralgia and hydrar-throsis.
TreatmentThe basis of treatment comprises local rest
to the inflamed area Iby means of mydriatics;the anti-inflammatory benefit of local and alsopossibly systemic corticosteroids; and, ofcourse, specific local and general treatmentwhen such means exist.
MydriaticsFrequently applied 1% atropine drops dilate
the pupil, prevent the development of posterioradhesions to the lens, relax the ciliary muscle,and increase the communication between an-terior and posterior chambers. If atropine eyedrops are not sufficiently effective, subcon-junctival mydricaine is indicated.
CorticosteroidsThere are several effective commerical
preparations for local treatment of iridocyclitis.
group.bmj.com on April 10, 2018 - Published by http://pmj.bmj.com/Downloaded from
December, 1964 JAMES: The Riddle of Uveitis 691
Eye drops should be administered at least fourtimes daily and the more slowly absorbedointment applied 'last thing at night. The res-ponse is usually immediate and dramatic, butif there is continuing undesirable inflammationafter 10 to 14 days, then the more intensiveanti-inflammatory effect of subconjunctivalcortisone or a short intensive course of oralprednisolone should be considered. Onescheme is to prescribe 5 tablets (prednisolone5 mg; betamethasone or dexamethasone 0.5 mg)daily for 5 days, followed by 4 tablets daily for4 days, 3 tablets daily for 3 days, 2 tablets dailyfor 2 days and 1 tablet on a final day. Thiscourse of 55 tablets in 15 days is complementaryto rather than instead of local corticosteroideye drops and ointments. This short intensivecourse of topical and oral steroids is usuallysufficient to suppress acute iridocyclitis, but notfor acute posterior uveitis which is inaccessibleto topical applications. For acute choroido-retinitis, as for instance due to relapsing toxo-plasmosis, prednisolone is continued in dosesof 20 mg. daily as long as improvement occursand for at least 3 months.As in other fields of medicine, steroids can
be expected to suppress acute inflammation butthe response of chronic inflammatory processesis disappointing. Oral steroids will suppressacute exacerbations and may even preventthem, but the natural history of chronic uveitisremains virtually unchanged. It smouldersonwards with occasional exacerbations, andirreversible fibrosis gives rise to mechanicalcomplications such as secondary glaucoma andcataract formation (Fig. 2).Specific measures (Table 1).5-lodo-2'-deoxyuridineThymidine is needed for the intracellular
synthesis of desoxyribonucleic acid. This path-way in viral synthesis may ,be interrupted bythe halogenated pyrimidines, that most fre-quently used in clinical practice being 5-iodo-2' deoxyuridine (IDU) (Kaufman, Nesburn and
Maloney 1962; Hall-Smith, Corrigan and Gilkes1962). Inhibitory effects have been notedagainst herpes simplex, vaccinia and adenovirus,but viruses whose genetic information is in theform of RNA are unaffected by this group ofcompounds. The precise value of IDU eyedrops remains in doubt for enthusiastic earlyclaims have been critically countered; furthercontrolled blind trials are in progress to defineits use. Nevertheless attention has been focussedon a new field of antiviral chemotherapy, inwhich drugs may be designed to interrupt essen-tial viral metabolic pathways.Broad-spectrum Antibiotics
Ampicillin and tetracycline are effectivebroad-spectrum antibiotics for the control ofcontributory bacterial inflammation. Both maybe used in turn a week apiece to eradicatetroublesome prostatitis.PyrimethamineThe toxoplasma organism utilises the para-
aminobenzoic acid-folic acid chain for itsnutrition. Both the sulphonamides and pyrime-thamine antagonise the chain, sulphonamidesby competing with PABA and pyrimethamineby interfering with the conversion of folic tofolinic acid. This is the rationale of the treat-ment of toxoplasmosis with pyrimethamine 50mg. daily and sulphadiazine 1 gram daily forup to 3 months. Supplements of folinic acidor brewer's yeast may reduce the toxicity ofpyrimethamine to the host without affectingits action on the parasite. The true worth ofpyrimethamine in human toxoplasma uveitisremains in doubt. Moreover, if such treatmentis to be given, serial blood counts are essentialfor the detection of macrocytic anaemia andleucopenia.Sulphones
Leprosy uveitis is best treated by a com-bination of the anti-leprosy drugs, such as thesulphones, together with local and possiblysystemic corticosteroids.
REFERENCESBRODIE, B. C. (1818): Pathological and Surgical Observations on Diseases of the Joints*, p. 54.CATTERALL, R. D. (1961): Significance of Non-specific Genital Infection in Uveitis and Arthritis, Lancet, ii,739.HALL-SMITH, S. P., CORRIGAN, M. J., and GILKES, M. J. (1962): Treatment of Herpes Simplex with 5-Iodo-2'-
deoxyuridine, Brit. med. J., ii, 1515.JAMES, D. G., ANDERSON, R., LANGLEY, D., and AINSLIE, D. (1964): Ocular Sarcoidosis, Brit. J. Ophthal., 48,461.KAUFMAN, H. E., NESBURN, A. B., and MALONEY, E. D. (1962): IDU Therapy of Herpes Simplex, Arch.
Ophthal., 67, 583.LUDLAM, G. B., BRIDGES, J. B., and BENN, E. C. (1964): Association of Stevens-Johnson Syndrome with
Antibody for Mycoplasma Pneumonia:, Lancet, i, 958.WOODS, A. C. (1961): "Endogenous Inflammations of the Uveal Tract", p. 278, Baltimore: Williams and
Wilkins.
group.bmj.com on April 10, 2018 - Published by http://pmj.bmj.com/Downloaded from
The Riddle of Uveitis
D. Geraint James
doi: 10.1136/pgmj.40.470.6861964 40: 686-691 Postgrad Med J
nhttp://pmj.bmj.com/content/40/470/686.citatioat: Updated information and services can be found
These include:
serviceEmail alerting
corner of the online article. this article. Sign up in the box at the top right Receive free email alerts when new articles cite
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on April 10, 2018 - Published by http://pmj.bmj.com/Downloaded from