the quebec system of monitoring and enhancement of physicians performance
DESCRIPTION
Expect the Unexpected: Are We Clearly Prepared?. The Quebec system of Monitoring and Enhancement of Physicians Performance. André Jacques, MD, Director Practice Enhancement Division Collège des médecins du Québec. - PowerPoint PPT PresentationTRANSCRIPT

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
The Quebec system of Monitoring and Enhancement of Physicians PerformanceAndré Jacques, MD, Director
Practice Enhancement Division
Collège des médecins du Québec
Expect the Unexpected: Are We Clearly Prepared?

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Potential conflict of interests disclosure
Dr André Jacques declare:
“ I do not have any affiliation or financial interest of any nature in
a business corporation, or I do not receive remuneration,
royalties or research grants from a business corporation”

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Mission of the College
The mission of the
Collège des médecins du Québec
is to promote a quality
medicine in order to protect the
public and to contribute to
enhance the health of Quebecers

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Governance of the College
Bureau(28 Governors)
Executive Committee(5 Governors)
President
ProfessionalInspectionCommittee
Committeeon Revision
Committeeon Discipline
Committeeon Admission
to practice
Committeeon CPD
Committeeon Budget

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Management structure
Legal ServicesDivision
External AffairsDivision
Administrative Services Division
General Division
MedicalEducationDivision
PracticeEnhancement
DivisionInquiry Division

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Role of the College of physicians
• Admission to practice - registration
– Accreditation of training programs and sites
– Licensure examination for family physicians (written and oral examinations, OSCE and SOO)
– Specialist certification examination (written and oral and/or clinical examination)

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Role of the College of physicians
• Supervision of physicians’ practice– Assessment of practice of physicians in :
• Offices • Hospital• Nursing homes• Etc.
– Interventions to promote quality of practice • CME activities• Training programs• Coaching• Etc.

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Role of the College of physicians
• Investigation of complaints related to both physicians and illegal practitioners
– Disciplinary process (for physicians)
– Legal proceedings against illegal practitioners
– Alternate resolution of complaints

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Role of the College of physicians
• Political role
– Physicians and medical organizations
– Public and media's
– Government and official bodies
– Other health professions

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Human and financial resources
• Staff of the College:– 23 full time physicians– 78 support staff
• Budget :– 18.6 millions (Canadian dollars)

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Quebec medical manpowerDistribution by type of practice (N = 18 746)
49,30% 50,70%
GPs ( N= 9 242) Specialists (N = 9 504)
Based on data of December 2005

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Quebec medical manpower
Distribution by sex (N = 18 746)
64,60%
35,40%
Male (N = 12 120)Female (N = 6 626)
Based on data of December 2005
Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Code of ethics
Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
• A physician must practice his profession in accordance with the highest current standards; to that end he must improve and keep his knowledge up to date.
(Section 44)
Code of Ethics of physicians

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Professional Code

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
By-laws related to supervision of physicians practice
• A Professional Inspection Committee is established within each order.
(Professional Code, section 109)

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
• The committee shall supervise the practice of the profession by the members of the order.
(Professional Code, section 112)
By-laws related to supervision of physicians practice

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
• The committee may recommend that it require a member of the order to serve a period of refresher training or take a refresher course or both and that it restrict or suspend his right to engage in professional activities during the training period or course.
(Professional Code, section 113)
By-laws related to supervision of
physicians practice

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
• It is forbidden to hinder in any way a member of the committee, an inspector or an expert in the performance of the duties conferred upon him by this code.
(Professional Code, section 114)
By-laws related to supervision of
physicians practice

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Professional Inspection CommitteeFunctions
• Inquiries into the professional competence of a physician
• Inquiries into the the quality of the medical care provided in establishments

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Practice Enhancement
Division

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Practice Enhancement DivisionMandate
The mandate of the Practice Enhancement Division of the College of physicians of Quebec is the monitoring
of the practice of physicians and its enhancement in order to protect the public and contribute to enhance the
health of Quebecers

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Practice Enhancement DivisionHuman and Financial Resources
• Staff of the Division :– 10 physicians
•1 director•2 assistant directors •6 inspectors-investigators•1 physician for sick MD
– 1 coordinator– 1 research agent– 11 secretaries
• Budget 2006-2007 : 4.3 M $

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Practice Enhancement DivisionFunctions
• Evaluation of the quality of physicians' practice in office as well as in hospital
• Evaluation of the quality of the practice of medicine in health establishments
• Support to the Professional Inspection Committee

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Practice Enhancement DivisionFunctions
•Intervene to enhance the physicians' performance in office as well as in hospital
•Support the Continuing Professional Development (CPD) Committee
•Maintain the secretariat of the Conseil québécois du développement professionnel continu des médecins

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Who will be the winner !

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Study of a representative sampling of 100 GPs
• Observational analysis of medical records randomly selected
• Assessment of some aspects of the quality of general practitioners’ professional practice
• Period : 1995-1996

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Study of a representative sampling of 100 GPs
• Professional inspection visits to 100 family physicians
• Random selection among Quebec’s family physicians :– practicing either entirely or partially in a
private office– in the greater metropolitan Montreal
region

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Study of a representative sampling of 100 GPs
• Two random sample groups :
– 52 family physicians licensed before 1980
– 48 family physicians licensed between 1980 and 1996
Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Study of a representative sampling of 100 GPs
• Professional inspection visits made by– 5 inspectors/investigators from the College– Average of 10 years of experience in
assessment of competence
• Study of at least 30 patients records randomly chosen
• Using of a standard grid listing the criteria, including a scores scale
Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Sampling of 100 GPs Criteria of evaluation
• Office practices
• Record-keeping
• Quality and quantity of CME
• Quality of practice– Investigation– Diagnosis accuracy– Treatment plan– Relevance of care

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Sampling of 100 GPs Demographic data
Distribution of physicians by sex
0% 25% 50% 75% 100%
Board of Collège desmédecins du Québec
Physicians of thestudy
Male Female

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Sampling of 100 GPs Demographic data
Distribution by licensing period
0% 25% 50% 75% 100%
Board of Collège desmédecins du Québec
Physicians of the study
License obtained after 1980 (Group 1)
License obtained before 1980 (Group 2)

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Sampling of 100 GPs Results
• Comparisons between physicians of groups 1 and 2 regarding :
– Sex – Age– Status in hospital – University of issuance of the medical degree – Average number of consults per week

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Sampling of 100 GPs Results
• No significant statistical difference detected between the two groups (except for record-keeping)
• No link between demographic variables and quality of care
• Strong link between :– record-keeping and quality of care– CME activities and quality of care

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Sampling of 100 GPs Results
0% 20% 40% 60% 80% 100%
Office practices
Record-keeping
Quality and quantityof CME
Combined results (Groups 1 and 2)
Satisfactory Unsatisfactory

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Sampling of 100 GPs Results
0% 20% 40% 60% 80% 100%
Treatment plan
Investigation plan
Diagnosis accuracy
Relevance of care
Combined results (Groups 1 and 2)
Satisfactory Unsatisfactory

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Sampling of 100 GPs Conclusion of the study
• Results enable the College to reassure the public with regard to the overall quality of the professional practices of family physicians in Quebec
• Study confirms the PIC decision to evaluate the practice of physicians who present a potential risk of deviant profile, based on quality indicators

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Monitoring and enhancement of physician’s performance
Screening of all physicians
Monitoring
Monitoring
Feedback to all physicians
Enhancement
Enhancement
CME programs for groups and/or
individuals
Assessment of physicians in need
or at risk
Remediation programs
Detailed needs assessment
Monitoring Enhancement
Step 3
Step 2
Step 1

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Step

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Development of indicators for
individual physicians
• Choice of indicator– By Professional Inspection Committee
and Practice enhancement division, after consultation with different organizations
• Responsibility of the development– One staff physician

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Development of indicators for
individual physicians• Elaboration with :
– Group of «experts» in the domain – Group of interested physicians in a hospital – Research group
• Pilot process evaluating feasibility• Validation of the indicator• Diffusion of the indicator with
appropriate guidelines• Implementation of the indicator

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
The use of PSA levels as a means of
detecting prostate cancer
The use of PSA level as a means of detecting prostate cancer …
When available data does not always allow to document practices and
changes inducted by an intervention

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
The use of PSA levels as a means of
detecting prostate cancer
• Medical controversy about extended use of PSA as a means of detecting prostate cancer
• Publication of an evidence-based guideline

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
The use of PSA levels as a means of
detecting prostate cancer • Publication of an information
booklet for patients (in French)• Local CME activity (in a single
region)• Analysis of physicians'
perceptions : – 90% say they are aware of it– 76% agree with it– 58% say it has influenced their practice

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
The use of PSA levels as a means of
detecting prostate cancer
Evolution of the number of PSA tests (all of Quebec excluding Montreal)
0
50000
100000
150000
200000
250000
93-94 94-95 95-96 96-97 97-98 98-99
Follow-up PSA
Screening PSA
Average number of PSA tests(excluding cases of prostate cancer)
0
5
10
15
Period 1 Period 2 Period 3
Physicians who attended a workshopAll physiciansPhysicians who did not attend a workshop
Evolution of prescription profiles in Québec and in the region where a continuing medical intervention was conducted
After dissemination
After intervention
Dissemination of
guideline

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
The use of PSA levels as a means of
detecting prostate cancer• Data analysis …
– Significant decreasing of the use of PSA levels as a means of detecting prostate cancer
– Incomplete and impossible to analyze data •Especially in Montreal area
– Data to be collected locally by archivists (in patient records)•Hard and long job

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Step
Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Professional Inspection CommitteeComposition
• 2 physicians from the Practice Enhancement Division :
•The Director•One Assistant director
• 6 physicians in practice, representative of both medical and surgical specialties
• 10 meetings per year

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Professional inspection visits Usual procedures
• Sending of a notice and a questionnaire to be completed before the visit by the physician or the establishment
• Inspection visit, with or without an expert
• Writing of a report and of a project of recommendations
• Submission of the report to the Professional Inspection Committee

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Professional inspection visits’ algorithm
Recommendations
Meeting with PIC secretary CME Syndic Administrati
ve Committee
PAM
No control Control
With expert
Without expert
Structured oral
interview
New recommendatio
ns
Voluntary
training
Imposed
training
No limitation of practice
Limitation of practice
No control Control

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Professional inspection visits’ algorithm
Sending of recommendations
Meeting with PIC secretary
Transfert to Syndic
Transfert to the PAMQ
No control visit Control visit With expert
Without expert
SOI
New recommendations
Volontary training program
Imposed training program
Without limitation of practice
With limitation of practice
No control visit Control visit
Good practice Unsatisfactory practice
Felicitations from the PIC
Good practice Unsatisfactory practice

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Individual inquiries
49
24 25
0 0 0 0 0 0 0 0 0
10
18
7
0
12
7
10
0
5
10
15
20
25
30
35
40
45
50
Number of visited physicans
Requests from Syndic OfficeReceived informationDiplomees >35 years>25% of psychoth. (GP's)>50% house calls (GP's)>40% outside of specialtyWalk-in clinics (GP's)Requests from Exec. Comm.NSAID's prescriptionWitness groupAesthetic Medicine (GPs)>30% diagn.-ther. ActsSubstitute doctorsWork in office onlyMethadoneFailure at licence examPursuit of evaluationRestrictive permitOther programs
152 individual inquiries

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
54,4%
46,7%
73,6%
61,2%
69,7%
84,2%
72,8%
0%
20%
40%
60%
80%
100%
Office practices
Record Keeping
CME
Medical Examination
Accuracy of Diagnosis
Pertinencen of care
Treatment
Results of inquiries
Adequacy of :

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
144
35
7
0
6
7
7
7
18
6
30
15
0 20 40 60 80 100 120 140 160
Congratulations letter -Good practiceMeeting with PICsecretaryReferral to Syndic office
Recommendation of atraining programReferral to ExecutiveCommitteeRecommendations tophysicians' councilReferral for a SOI
Referral for CME
Request for a reportfrom hospitalRequest for a reportfrom physicianControl visit
Recommendations tophysician
Decisions of PIC

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Practice enhancement activities
• Sending of recommendations from the Professional Inspection Committee
• Follow-up of recommendations by inspectors
• Organization of CME group activities (workshops on patient-doctor relationship, workshops on periodical health examination, courses)

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Enhancement activities 1991-2003 (n=533)
11
4
12
31
51
39
78
64
46
52
66
79
0
20
40
60
80
'91-92 '92-93 '93-94 '94-95 '95-96 '96-97 '97-98 '98-99 '99-00 '00-01 '01-02 '02-03

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Workshops on Physician-patient relationship 1992-2000
(n=296)Number of workshops
75
70
67
84
0 20 40 60 80 100
Better communication
Right distance
Difficult relationship
Breaking bad news

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Workshops on Physician-patient relationship 1992-2000
(n=296)
Attendance to workshops
1036
913
823
1217
0 300 600 900 1200 1500
Better communication
Right distance
Difficult relationship
Breaking bad news

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Other courses and workshops 1992-2000 (n=125)
Number of sessions
84
37
4
0 20 40 60 80 100
Record-keeping
Pharmacotherapy
Periodical examination

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Step

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Detailed needs assessment
• Structured oral interview– Specific tool developed for GP’s– Individual evaluation of the performance– 25 clinical cases to resolve– 5 cases with simulated patients– Goal of the evaluation : personalized
remedial CME prescription
• Evaluation training period– Used for needs assessment of specialists

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Structured oral interview
• Since 1990 : clinical cases– Assessment of knowledge
• In 1997 : addition of OSCE cases– Assessment of skills and attitudes
• In 2000 : addition of Script concordance tests– Assessment of clinical reasoning

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Structured oral interview
Domains assessedDomains assessed
• «SOI» (20 cases)–Knowledge (data collection)–Problems solving–Interpretation of lab tests
• «OSCE» (5 cases)–Knowledge (data collection)–Physical examination (skills)–Interpretation of lab tests–Physician patient relationship
• Script concordance test –Knowledge (data collection)–Clinical reasoning–Interpretation of lab tests
Content of the reportContent of the report
• Analysis of resolved cases• Analysis of referred cases• Detail of strengths and
weaknesses• Analysis of performance :
–Emergency cases –Pharmaceutical treatments–Follow-up
• Interpretations–Responsibility level able to handle–Knowing of its limits–Inappropriate but not dangerous conducts
–Harmful of dangerous conducts–Informed of recent conducts
Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
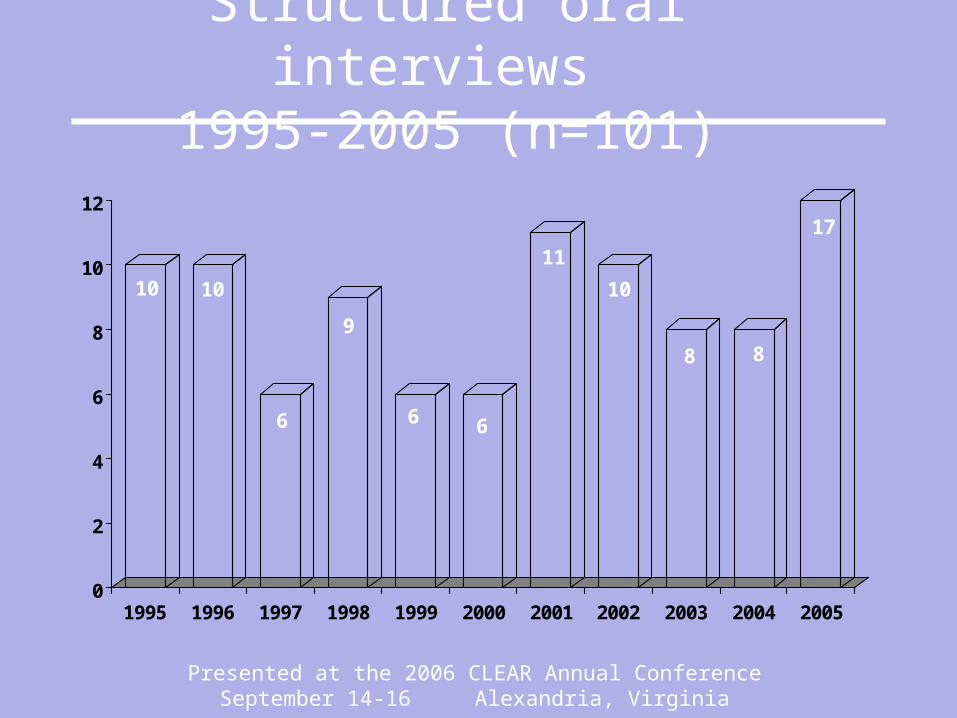
Structured oral interviews 1995-2005 (n=101)
10 10
6
9
6 6
11
10
8 8
17
0
2
4
6
8
10
12
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Structured Oral Interviews 1995-2001
Personnal request26%
Request from Syndic31%
Recommendation of PIC (16)
28%
Others7%
Re-entering the roll3%
Recommendation from Committee on
discipline5%

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Individualized CME programs
• Clinical training programs• Focused readings• Tutorial chart recalls

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
68
2 9
0
10
20
30
40
50
60
70
Clinical training programs Focused reading Tutorial chart recalls
Individualized CME

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Personalized CME (1992-2000) Statistics for all physicians
(n=240)
Who are the candidates ?
199
41
177
63
0 20 40 60 80 100 120 140 160 180 200
Specialists
General practitioners
Female
Male

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Personalized CME (1992-2000) Statistics for all physicians
(n=240)
Who referred candidates ?
59
97
62
18
4
0 20 40 60 80 100
Executive Committee
Committee on Discipline
Syndic office
PIC
Personal request

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Personalized CME (1992-2000) Statistics for all physicians
(n=240)
Why do candidates need remedial CME ?
177
41
19
3
0 20 40 60 80 100 120 140 160 180 200
Striking off the Roll
Reorientation
Return to practice
Quality problems

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Personalized CME (1992-2000) Statistics for all physicians
(n=240)What problems are encountered ?
16,70%
35,80%
31,80%
4,60%
8,70%
2,40%
Record-keeping
Diagnosis accuracy
Treatment plan
Judgement
Skills
Communication

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Personalized CME (1992-2000)Training programs (n=225)
12
3
1
3
23
21
17
13
6
66
15
15
0 10 20 30 40 50 60 70
General Practice
Anaesthesia
Emergency
General Surgery
Geriatrics
Medical Specialties
Obs.-Gynaecology
Petiatrics
Psychiatry
Public Health
Radiology
Surgical Specialties

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
82,0%
15,0%3,0%
Successful activities
Abandon retraining
Non successful activities
Personalized CME (1992-2000)Results of remedial CME

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Monitoring and enhancement for improving performance in
hospitals
Screening of all health establishments
Monitoring
Monitoring
Comparative feedback to all health establishments
Enhancement
Enhancement
Feedback to the establishment
Screening of establishments in
need or at risk
Meeting with authorities
Control visit
Monitoring Enhancement
Step 3
Step 2
Step 1

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Step
Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Monitoring of Health establishmentsChoosing of the indicators
• In collaboration with the concerned professional Association :
– Selection of experts of the working group– Proposition of indicators by the working group– Evaluation of the feasibility by a pilot– Validation of indicators– Extension of the project to a group of hospital

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Monitoring with indicators
Content of the pathological report of
breast cancer

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Why choosing the pathology ?
• Request from the Professional Inspection Committee
• Interest of the Quebec's Pathologists Association for implementing a monitoring program with quality indicators

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
And why the breast cancer pathology ?
• Integral part of most of pathologists
• Media coverage of unhappy events in an hospital
• Launching of Provincial program of breast cancer screening

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Main steps of the program
• Fall 1998 : – Nomination of the experts' group
• Winter 1998-1999 : – Completion of a pilot project
– Final choice of quality indicators
• Summer 1999 : – Data collection (First study)

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Main steps of the program
• Winter 1999-2000 : – Analyze and evaluation of data by the experts'
group
• Spring 2000 : – Feedback to hospitals
• Summer and Fall 2000 : – Enhancement activities by the Quebec’s
Pathologists Association

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Main steps of the program
• Spring 2003 : – Data collection (Second study)
• Fall and winter 2003-04 : – New feedback to hospitals

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Experts' group
• Mandate : Identify quality indicators
– Easy to monitor – Non expensive – Valid – Allowing to get a global view of the practice
of pathologists

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Experts' group
• Composition : – The 5 members of the Quality-insurance
Committee of Quebec's Pathologists Association
– One member of College of Physicians' Practice Enhancement Division

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
• Evaluation of the last 20 medical records of breast cancer surgery in each of participating hospital
• Essential information for physicians in order to plan the treatment and establish the prognosis
Quality indicators (Spring 1999)

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
• Number of cases with research of hormonal receptors
• Indication - in the report - of dimension of the tumor
• Mention in the report of the distance between lesion and at least one resection margin
Quality indicators (Spring 1999)

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
• Mention of histological type in final diagnosis
• Mention of histological / nuclear grade
• Mention of the presence or absence of lymphatic or vascular invasion
• Mention of histological evaluation of resection margins
Quality indicators (Spring 1999)

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
The first study (Summer 1999)
• Questionnaire sent to 53 hospitals
• Rate of answers : 100 %
• Number of records evaluated : 1040 (from the 53 hospitals)
• Number of pathologists aimed at the program : 247
Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
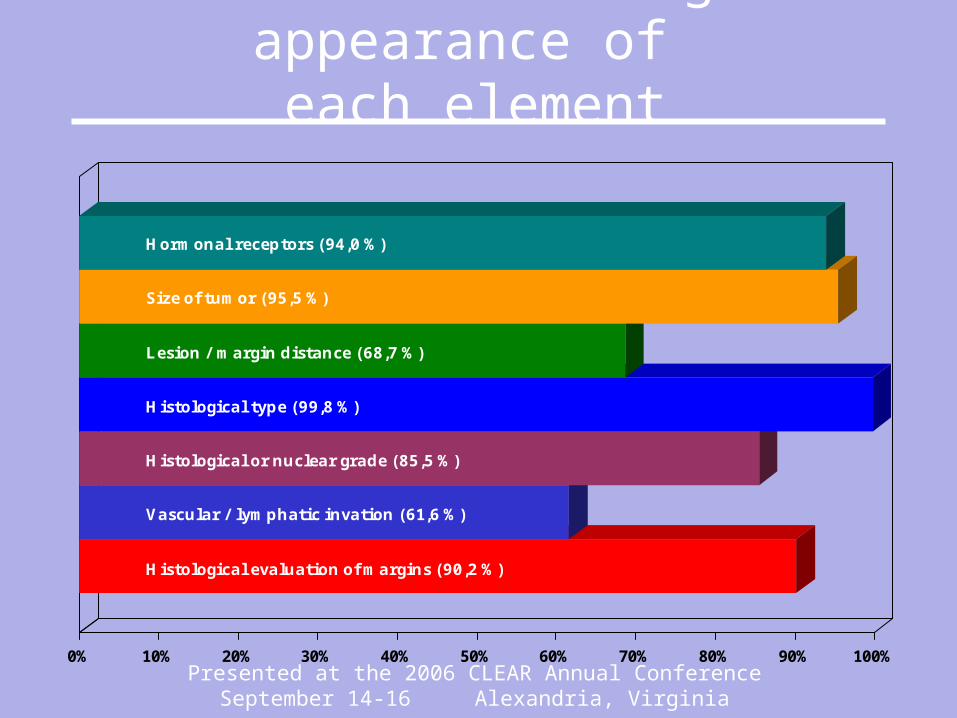
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Hormonal receptors (94,0 %)
Size of tumor (95,5 %)
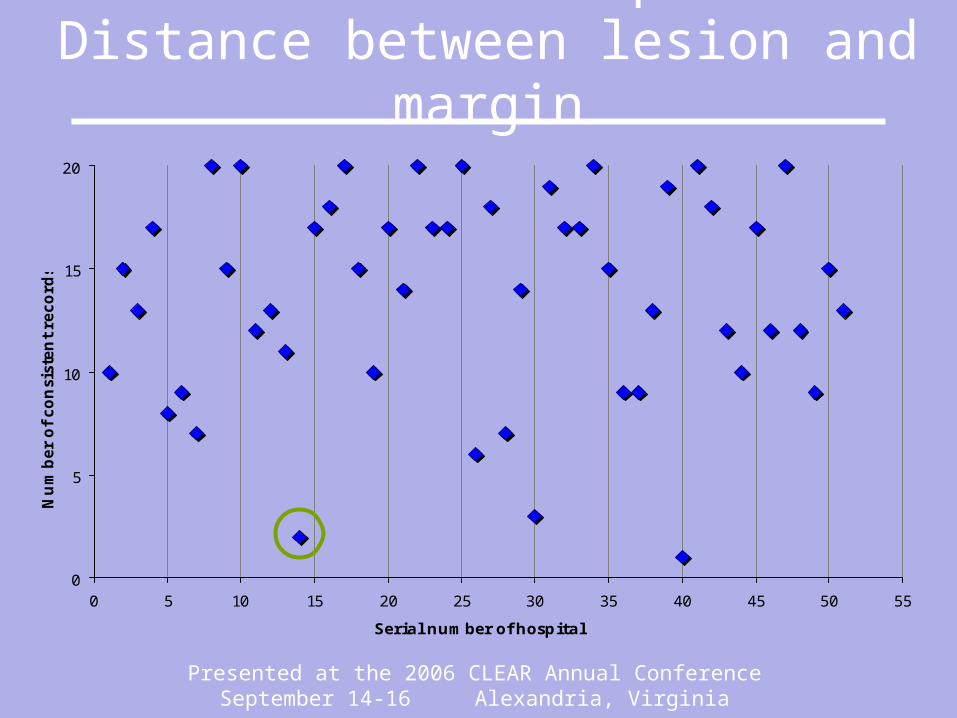
Lesion / margin distance (68,7 %)
Histological type (99,8 %)
Histological or nuclear grade (85,5 %)
Vascular / lymphatic invation (61,6 %)
Histological evaluation of margins (90,2 %)
Results - Percentage of appearance of each element

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
• Feedback made by the Professional Committee in March 2000 at each of the 51 hospitals aimed at the program
• Feedback made to each hospital :– with tables and graphics– about results of the study for all hospitals aimed
at the program– about their individual performance
Feedback to hospitals

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Feedback to hospitalsHistological evaluation of
margins
0
5
10
15
20
0 5 10 15 20 25 30 35 40 45 50 55
Serial number of hospital
Num
ber
of consi
stent re
cord
s

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Feedback to hospitalsVascular / lymphatic invasion
0
5
10
15
20
0 5 10 15 20 25 30 35 40 45 50 55
Serial number of hospital
Num
ber
of consi
stent re
cord
s
Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Feedback to hospitalsDistance between lesion and
margin
0
5
10
15
20
0 5 10 15 20 25 30 35 40 45 50 55
Serial number of hospital
Num
ber
of consi
stent re
cord
s

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Enhancement activities
•By Quebec's Pathologists Association
– Production of a CD-ROM (prototype only) about breast cancer pathology
– Presentation of the CD-ROM prototype at Quebec's Pathologists Association's annual meeting

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Enhancement activities
•By Quebec's Pathologists Association
– Production and implementation of guidelines about elements to include in the pathological report of breast cancer in order to help physicians and surgeons to plan treatment and evaluate the prognosis.

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
The second study
• Period of the study : Fall / winter 2002-03
• Questionnaire sent to the 51 hospitals aimed at the first study
• Rate of answers : 100 %

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
The second study
• Number of record evaluated : 999– 1 hospital excluded (not enough records)– 1 hospital sent 19 records
• Number of pathologists aimed at the study : 246

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Hormonal receptors (97,1 %)
Size of tumor (96,2 %)
Lesion / margin distance (86,8 %)
Histological type (99,7 %)
Histological or nuclear grade (92,1 %)
Vascular / lymphatic invation (81,6 %)
Histological evaluation of margins (92,7 %)
Results - Percentage of appearance of each element

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Compared resultsRate of consistency per
criteria
0%
20%
40%
60%
80%
100%
First study 90,2% 61,6% 85,5% 99,8% 68,7% 95,5% 94,0%
Second study 92,7% 81,6% 92,1% 99,7% 86,8% 96,2% 97,1%
. p=0,09 p<0,01 p<0,01 p=1,00 p<0,01 p=0,57 p<0,01
Margin evaluation
Vscular / lymphatic Invasion
Histological / nuclear Grade
Histological Type Lesion / margin
Distance Size of tumor
Hormonal receptors

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Compared resultsEvaluation of lesion/margin
distance
0
5
10
15
20
0 5 10 15 20 25 30 35 40 45 50 55
Serial number of hospital
Num
ber
of consi
stent re
cord
s

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Performance enhancementEvaluation of lesion/margin
distance
-100%
-80%
-60%
-40%
-20%
0%
20%
40%
60%
80%
100%
0 5 10 15 20 25 30 35 40 45 50 55
Serial number of hospital
Per
form
ance
enhance
men
t ra
te

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Step

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
20
21 1
0
5
10
15
20
25
30
Hospitals Nursing homes CLSC Others
Visits in Health Establishments2002-2003 (n=24)

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Activities of practice enhancement in
health establishments• Sending of recommendations by the
Professional Inspection Committee and coaching by one of the College staff physician
• Organization of courses for answering specific needs
• Workshops on evaluation of quality given in health establishments

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Step
Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Control visits with an expert
• In 1998-1999 :
– 10 control visits of hospitals
– 1 control visit of a nursing home
– 1 control visit in another establishment
Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Meetings with authorities in 1998-1999
On 3 occasions, meeting with administrative authorities of an establishment (1 hospital and 2 nursing homes)
On 8 occasions, meeting with the “Régie régionale” (in regard with 2 hospitals and 4 nursing homes)
On 4 occasions, meeting with Health Minister (in regard with 1 hospital and 3 nursing homes)

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
The Future !

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Competency
AttitudeHability to
practice
Use of
ressources
Components of physician’s performance
Professionnalism
Patient
Patient
Patient Patient
TEAM TEAM

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
What are the conditions of success of that system?
4 key words who support that system:
CommitmentInvestmentTeam workPartnership

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
First key word: Commitment
Commitment from my organization to the mandate of the Practice Enhancement Division:
Assessment and Remediation at all levels More formative then punitive Research agenda

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Second key word: Investment
Support from my organization to the mandate of the Practice Enhancement Division:
Budget from 860,000 $ to 4.3 M $ 10 full time physicians dedicated to the
mandate 1 research agent (4 days/week) 22 full time persons

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Third key word: Team work
Merging, in 1997, the CPD Division with the Peer Assessment Division to the new Practice Enhancement Division with a new mandate of assess physicians with a goal of remediate those in need.
Developing the new levels (level 1) to enhance a wider scope of physicians.

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Fourth key word: Partnership
This system cannot work without collaboration and partnership with:
The four Universities in Quebec The two Unions (FMOQ-FMSQ) The two others Colleges (RCPSC-CFPC) The major medical associations

Presented at the 2006 CLEAR Annual ConferenceSeptember 14-16 Alexandria, Virginia
Questions and Exchanges