the physician’s arc: visioning competency across the continuum englander ann11-312.… · the...
TRANSCRIPT

The Physician’s Arc: Visioning Competency Across the Continuum
Robert Englander, MD MPH Tuesday, November 8th, 2011

The Vision Physicians will spend their careers, from (pre)entrance to UME to exit from practice on a developmental trajectory, building mastery in: • Patient Care (PC) • Medical Knowledge (MK) • Interpersonal and Communication Skills (ICS) • Professionalism (P) • Systems-based Practice (SBP) • Practice-based Learning and Improvement (PBLI)

What are the competencies/attributes that would best serve the medical school matriculant to optimize and accelerate growth along the Arc?
Forward Visioning

Lessons from Hodgkins Elementary School

The MR5 Project
Knowledge Foundation

Natural Sciences: Biology (MK) Chemistry (MK) Physics (MK) Biochemistry (MK) Research methods and Statistics (MK, PBLI) Behavioral and Social Sciences Psychology (PC, ICS, P) Sociology (PC, ICS, P, SBP) Ethics (P) Culture (P, ICS, SBP)
Knowledge Foundation

Transforming Medical School Admissions Initiative
“Personal Competencies” Foundation

Integrity/Ethics (P) Reliability/Dependability (P) Service Orientation (PC, P, SBP) Adaptability, Resilience (PBLI, P, ICS, SBP)
Personal Competencies “Seeds”

Interpersonal and Social Skills (P, ICS) Teamwork Skills (ICS, SBP) Cultural Competence (P, ICS) Capacity for Improvement (PBLI, all?) Oral Communication Skills (ICS)
Personal Competency Seeds
Backwards Visioning

Lessons from Canada
Advantages of General Competencies
• Insures comprehensive conversation Identifies important physician KSA Improvement over “the mist of holistic waffle about
professional experience and the ineffability of…intuitive wisdom.”1
• How much improvement?2
• Focuses assessment on achievement of consensus competencies.
1. Cooke M et. al. Educating Physicians: A Call for Reform of Medical School and Residency. San Francisco: Jossey-Bass; 2010.
2. Kogan JR et.al. Opening the black box of clinical skills assessment via observation: a conceptual model. Medical Education 2011; 45; 1048-1060.

Disadvantages of General Competencies
Competency as a “god term”1
• Focus on the individual • Health outcomes depend on competent individuals within
a competent group within a competent system.
Competencies as “outcomes” • Outcomes should be discrete and measureable. • P, SBP, PBLI, ICS are not discrete and are difficult to
measure.
1. Lingard L. What we see and don’t see when we look at ‘competence’: Notes on a god term. Adv in Health Sci Educ. 2009; 14; 625-628.

Reductionist versus Holistic Approach
Assessment in the Context of Clinical Experience: EPAs1
1. ten Cate O, Scheele F. Viewpoint: Competency-based postgraduate training: Can we bridge the gap between theory and clinical practice? Academic Medicine. Jun 2007;82(6):542-547.
Entrustable Professional Activities (EPAs)
• Part of essential professional work • Require knowledge, skills and attitudes • Confined to qualified personnel • Lead to recognized output • Independently executable in a predictable
time frame • Observable and measurable • Reflect one or more competencies

Why Focus on Entrustment?
We constantly, often subconsciously, make entrustment decisions as we work with learners.
It is more meaningful to ask faculty: • “Do you trust this person to provide normal
newborn care without direct supervision?” Versus
• “Is this person competent in PBLI ?”

Criteria for Entrustment
• The ability to perform a function to a desired level of performance without direct supervision.

What Does “Entrustable” Mean?
You won’t find entrustable in the dictionary.
The important concept is trust.
Generally based on1: • Ability or level of KSA • Hard work-data gathering and following through
(conscientiousness) • Telling the truth-absence of deception (truthfulness) • Knowing one’s limits and asking for help (discernment)
1. Kennedy TJT, et.al. Point-of-care assessment of medical trainee competence for independent clinical work. Acad Med. 2008;83(10 Supp):S89-S92.

EPAs Map to Competencies, Sub-competencies & Milestones
• We can identify critical sub-competencies required for entrustment regardless of setting/context
• Some sub-competencies may be assessed
that are context-specific
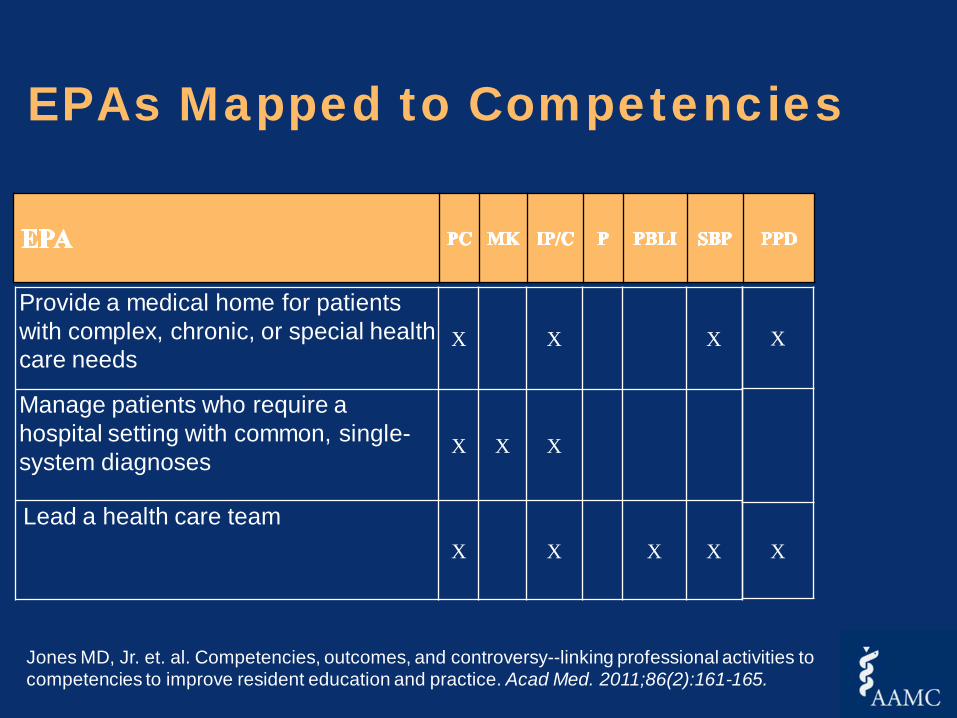
EPAs Mapped to Competencies
Provide a medical home for patients with complex, chronic, or special health care needs
X X X
Manage patients who require a hospital setting with common, single-system diagnoses
X X X
Lead a health care team X X X X
X
X
Jones MD, Jr. et. al. Competencies, outcomes, and controversy--linking professional activities to competencies to improve resident education and practice. Acad Med. 2011;86(2):161-165.

The Good Doctor
Entrustable Professional Activities
Sub-Competencies
M I L E S T O N E S
Slide courtesy of Ann Burke, MD
Summary: Why EPAs?
• They align what we assess with what we do. • They make sense to faculty, trainees and the
public. • They translate competencies, sub-
competencies and milestones into authentic clinical experiences
• They make explicit a crucial bond between mentor and student –TRUST
• They allow us to use backward visioning to identify gaps in training

The Education in Pediatrics Across the Continuum (EPAC) Project
Testing the EPA Concept
Thank you!