the pathway to child health - racha · the pathway framework is an idealized “model” that...
TRANSCRIPT

1
The Pathwayto Child Health
(Siem Reap, Pursat,Stung Treng,and Kampot)
Study Conducted by:
The National Center for Maternal and Child HealthThe National Pediatric Hospital
The Reproductive and Child Health Alliance (RACHA)
Report Produced by:
The Reproductive and Child Health Alliance (RACHA)May 26, 2000
Table of Contents

2
Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . i
Executive Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Note on Methodology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Infant and Under-five Mortality . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Perinatal Mortality . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Conclusions and Recommendations . . . . . . . . . . . . . . . . . . . . . . . . . 37
Attachments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Attachment One – Comments on the Pathway to Health Model/Diagram . . 3
Attachment Two – Sample Size Determination . . . . . . . . . . . . . . . 5
Attachment Three – List of Villages Selected for Death Surveillance . . . . 7
Attachment Four – List of Staff . . . . . . . . . . . . . . . . . . . . . . . 9
Attachment Five – Diagnosis Determination of Causes of Infant and . . . 17Child Deaths
Attachment Six – Data Collection Instruments . . . . . . . . . . . . . . . 19
Death Investigation Questionnaire (For deaths among infantsand children one week to 59 month of age - 20 pages) . . . . . . 21
Death Investigation Questionnaire (Perinatal Deaths – 31 pages). . 41

3
Acknowledgements
The Reproductive and Child Health Alliance in Cambodia (RACHA) wascreated in 1997 by the United States Agency for International Development (USAID)to assist Cambodia in the implementation of its Maternal and Child Health (MCH)Strategy. USAID asked RACHA to work with Cambodian partners, e.g., the NationalMaternal and Child Health Center (NMCHC) and National Pediatric Hospital (NPH) ofthe Ministry of Health (MoH) to improve quality of health care within four focusprovinces —Pursat, Kampot, Siem Reap and Stung Treng (Stung Treng has since beendropped as a focus province for RACHA, but is included within the Pathway study).When this Pathway to Survival Study began, RACHA consisted of a partnership amongthree US-based, USAID-funded organizations that included the Basic Support forInstitutionalizing Child Survival (BASICS) project, AVSC, and the Service Expansionand Technical Support (SEATS) project. As of 2000, RACHA is solely administeredby AVSC, but continues to receive collaborative assistance from John SnowInternational and other organizations.
RACHA supported this Pathway to Survival Study in collaboration with theNMCHC, the NPH, and the Provincial MCH Offices of the MoH in Pursat, Kampot,Siem Reap and Stung Treng. RACHA supplied technical assistance in the design,survey implementation, the data processing, and data analysis. The MoH provided thestaffing to implement and supervise the surveillance system for recording perinatal andchild deaths in 40 villages. Sixty-seven village monitors were supervised by 10 MoHsupervisors. MoH Community Advisory Councils and the Provincial ManagementCommittees established in each of the four provinces provided coordination and otherresources. Representatives from NMCHC and NPH provided technical assistance inthe analysis of the causes of death, home care treatment, and care-seeking behavior ofthe caregivers.
Following are the names of RACHA and MOH staff whose effort and support wereessential to the success of this study throughout its duration:
Name Position Organization/Institution
Dr. Sally Stansfield Child Survival Advisor RACHAMr. James Eberle Research/Logistics Advisor RACHADr. Sin Somuny Research Manager RACHAMs. Cheang Kannitha Research Assistant RACHADr. Houy Sikheng Research Assistant RACHADr. Kong Kannitha Research Assistant RACHAMs. Im Phally Research Assistant RACHAMr. Neou Vongsa MIS Coordinator RACHAMr. Ket Suntharak MIS Intern RACHADr. Khdan Yuvutha Chief of Technical Bureau NPHDr. Sam Sophan Pediatrician NPHDr. Auy Eam Pediatrician NPHDr. Ou Keo Vanna ARI National Program Officer NMCHCDr. Chhorn Veasna CDD/ARI/Cholera National Program Manager NMCHCMr. Sun Pov Vice Director MCH, Kampot MOHDr. Cheng Libunty Vice Director MCH, Pursat MOH

4
Mr. So Sothy Technical Bureau, Siem Reap MOHMs. Bou Vatha Deputy HD, Stung Treng MOH
*See Attachment Four for a full list of NPH participants and others who supported the PathwayStudy.
RACHA would like to express its profound and wholehearted gratitude to Ms.Judith Moore for providing technical assistance in the original design/implementationof the study, to Mr. John Stoeckel for his assistance in redesigning and reorienting thestudy in early 1999, and to Dr. Renata Schumacher for her assistance in the redesign,implementation, data processing, and data analysis of the study. RACHA would alsolike to express its gratitude to the NPH and NMCHC staff who supported the designand implementation of the study, as well as all the village monitors and supervisorswho contributed in the implementation. Finally, RACHA would like to thank themothers and other caregivers who provided their time during the interviewing process.Without them this study could not have taken place.

5
Executive Summary
The Pathway Study makes an important contribution to the accumulation ofresearch data on infant, under five, and perinatal mortality in Cambodia and to thedevelopment of a better understanding of what caretakers do when children become ill.A surveillance system recorded, for one year, all births and deaths between the sixthmonth of pregnancy through the 59th month of age. This covered a total population of10,000 women of reproductive age (15 - 49 years) in 40 villages in four provinces –Kampot, Pursat, Siem Reap and Stung Treng.
The mothers or caretakers associated with each death event were interviewed toobtain information on the care-seeking behavior that was followed during the child'sillness and to determine possible causes of death. Cause of death was determined byThe Pathway Working Group (PWG) composed of Cambodian experts, based on verbalautopsies (recorded descriptions provided by mothers and caretakers).
The rates and causes of mortality found in the Pathway Study are similar tothose reported in the National Health Survey, 1998 (NHS); however, perinatal mortalitywas not measured in the NHS1.
Mortality Rates Pathway NHS
Neonatal Mortality 30 36Post Neonatal Mortality 61 54Infant Mortality 91 89Under Five Mortality 124 115Perinatal Mortality 47 --
The causes of death in this study, based on the judgment of the PWG, areconsistent with the findings of the NHS. Meningitis, pneumonia and diarrhea/dysentery account for almost 60 percent of all deaths among infants aged 1 – 12months. Acute hemorrhagic fever is responsible for almost a quarter of the deaths inthe age group of one to four years. Diarrhea/dysentery and pneumonia, together,account for another fifth of the deaths in this group.
Out of all the actions taken by caretakers, only 40 percent could be considered"home care" or actions taken in the home. Forty-five percent of the home treatmentsconsisted of the caretaker giving modern medicine to the child, 36 percent consisted ofthe caretaker performing a traditional external practice on the child, and 19 percent
1 It should be remembered that the NHS was based on a national representative sample. ThePathway is based on a rural-focused, four province sample. Consequently, the results of the two surveysfrom a statistical viewpoint are not comparable. Nevertheless, a few comparisons are shown in thefollowing pages. Given the scope and size of the Pathway study, and the value in having even roughcomparisons, they are included.

6
consisted of the caretaker giving traditional medicine.
Care seeking behavior outside of the home resulted in 235 contacts/visits(sometimes more than once to the same provider or more than one provider for anillness). Out of these contacts/visits 33 percent were to Kru Khmers, 27 percent were todrug sellers, 23 percent were to private clinics, 11 percent were to hospitals and 6percent to health centers.
The most important conclusions of the study reaffirm and add to otherevidence:
1) most of the deaths recorded are preventable;2) caretakers do not understand well enough the danger signs of serious
infant and childhood illnesses;3) caretakers do not yet use the public health care system (and/or the
public system is not yet easily accessible in more remote areas); and4) there are clear steps that can be made by the public and private health
systems of Cambodia to reduce perinatal, infant, and under-fivemortality.

7
Section One
Introduction
1.1 BACKGROUND
Death rates among infants and children-under five in Cambodia are among thehighest in Asia, at 90 and 115 per thousand live births, respectively. The limited dataavailable from community-based studies in Cambodia suggest that more than half ofpost-neonatal deaths are due to pneumonia and diarrhea. In many areas in Cambodia,malaria and dengue are also known to be significant causes of death among childrenunder five.
Improved recognition and management of childhood illnesses represent the besthope of reducing the high death rate among Cambodian children. Yet it is impossible todesign an appropriate strategy to reduce childhood mortality in the absence of morespecific information on cause of death, and especially on case management at home,and on care seeking for childhood illness among providers outside of the home.
The Centers for Diseases Control (CDC) and US Agency for InternationalDevelopment (USAID) have developed a conceptual framework to assist in addressingissues associated with case management and care seeking. The framework, “Pathwayto Survival” is useful for the development and monitoring of programs to improve thecase management of childhood illness. The "Pathway" is designed to promote a moreholistic, integrated approach towards defining case management practices both insideand outside the home. The framework emphasizes that a death of a child represents abreakdown in one or more of the steps of this "Pathway." It implies the need foraccepted standards of quality of care, both within the community and in healthfacilities.
The National Maternal and Child Health Center (NMCHC) and NationalPediatric Hospital (NPH) of the Ministry of Health (MoH) in Cambodia recognized theneed for information regarding child deaths in Cambodia. This information wasnecessary to prioritize health problems, allocate resources, develop strategies forinterventions, and mobilize community and health personnel. The NMCHC incollaboration with NPH and the USAID-funded Reproductive and Child HealthAlliance (RACHA) program, proposed the Pathway to Survival Study of infant andchild mortality to address the lack of information.
The Pathway framework is an idealized “model” that assumes that decisions aremade that lead, to the eventual outcome of “survival and improved child health.” TheCambodia Pathway Study being reported herein has death as the final outcome, i.e.,information was collected only about children who died. Consequently, although welearn about decisions made that had negative outcomes, we do not have a comparativegroup, where decisions were made leading to “survival and improved child health.”Nevertheless, there is a very strong impression from conducting this study and fromother work in the provinces included in the sample, that the decisions reported in thisstudy are representative of the decisions that are made for sick children in rural

8
Cambodia, whether they eventually get well or not. Because of the simplicity of thediagram depicting the model of the Pathway, the fact that it outlines the broad avenuesavailable for making interventions, and that it initially helped focus this study, thediagram has been included in Attachment One. A “comment” has been included withthe diagram that suggests a much greater degree of complexity for a caregiver in ruralCambodia and the need for the diagram to be altered if it is to be used as an explanatorymodel for Cambodia. However, it remains a useful idealized model of how casemanagement of childhood illness ought to occur.
1.2 OBJECTIVES
The objectives of the "Pathway" study were:
1) To identify the main causes of perinatal, infant and child mortality;
2) To describe the care and/or treatment given to children in the home for thesymptoms and problems of childhood illness;
3) To identify health care providers (outside of the home) contacted by caretakersand the treatment and/or recommendation given by these providers foraddressing the symptoms/problems of the children’s illness;
4) To identify the caretakers' reasons for choosing providers (outside of the home),and their reasons for not choosing public health providers; and
5) To identify points of intervention that could help to prevent future perinatal,infant, and child death.
9
Section Two
Note on Methodology
2.1 SAMPLE POPULATION
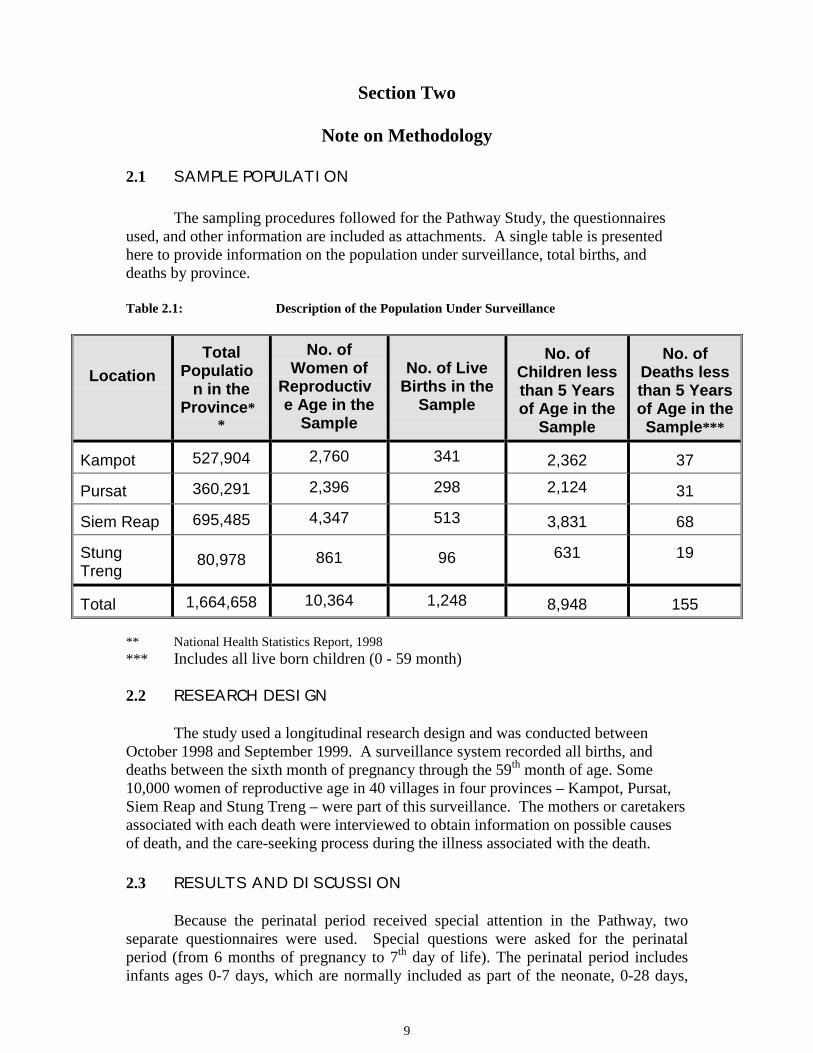
The sampling procedures followed for the Pathway Study, the questionnairesused, and other information are included as attachments. A single table is presentedhere to provide information on the population under surveillance, total births, anddeaths by province.
Table 2.1: Description of the Population Under Surveillance
LocationTotal
Population in the
Province**
No. ofWomen of
Reproductive Age in the
Sample
No. of LiveBirths in the
Sample
No. ofChildren lessthan 5 Yearsof Age in the
Sample
No. ofDeaths lessthan 5 Yearsof Age in theSample***
Kampot 527,904 2,760 341 2,362 37
Pursat 360,291 2,396 298 2,124 31
Siem Reap 695,485 4,347 513 3,831 68
StungTreng
80,978 861 96 631 19
Total 1,664,658 10,364 1,248 8,948 155
** National Health Statistics Report, 1998*** Includes all live born children (0 - 59 month)
2.2 RESEARCH DESIGN
The study used a longitudinal research design and was conducted betweenOctober 1998 and September 1999. A surveillance system recorded all births, anddeaths between the sixth month of pregnancy through the 59th month of age. Some10,000 women of reproductive age in 40 villages in four provinces – Kampot, Pursat,Siem Reap and Stung Treng – were part of this surveillance. The mothers or caretakersassociated with each death were interviewed to obtain information on possible causesof death, and the care-seeking process during the illness associated with the death.
2.3 RESULTS AND DISCUSSION
Because the perinatal period received special attention in the Pathway, twoseparate questionnaires were used. Special questions were asked for the perinatalperiod (from 6 months of pregnancy to 7th day of life). The perinatal period includesinfants ages 0-7 days, which are normally included as part of the neonate, 0-28 days,

10
category in presentation and analysis. In order to determine neonatal, infant, and 0 tofive-year mortality rates, the 0-7 day old infants were included in the appropriatenumerators. However, information from caretakers of infants of this age was notincluded with information for children 8 days to five years of age. This creates adifferent presentation issue from the norm. In section three, tables often refer tochildren one week to 5 years of age, because the 0-7 day olds are included in thesection focused on perinatal deaths. Examination of the results, from presenting theinformation in this format, does not indicate that patterns or conclusions reached woulddiffer if 0-7 day old children had been included. Also, separate data and descriptionsare available for infants 0-7 days in Section Four.
One additional comment on the number of deaths and the number of interviewsis important. Pathway interviewers were not able to complete interviews for 11 of thedeaths. The ages of these children at death are known and their deaths are included incalculating the rates, but there is no information from their caretakers. There was a totalof 155 deaths of infants and children ages 0 to five years of age. Twenty-six deathsoccurred to children 0-7 days of age, and for one of these deaths there was nointerview. One hundred twenty-nine deaths occurred to children 8 days to five years ofage, and for ten of these deaths there were no interviews.
To summarize, the following specifies the number of cases on which the PathwayStudy is based:
! Total number of child deaths recorded during the study period – 155! Number of child deaths 8 days to 5 years recorded during the study period – 129! Number of interviews completed for child deaths 8 days to 5 years – 119! Number of child deaths 0-7 days after birth – 26! Number of interviews completed for child deaths 0-7 days – 25

11
Section Three
Infant and Under-Five Mortality
3.1 MORTALITY RATES AND CAUSES OF DEATH
As shown in Table 3.1, the mortality rates obtained in this study are similar tothe rates found in the NHS. Each of these studies found relatively high rates of post-neonatal deaths, compared to neonatal mortality. The higher post-neonatal rates couldbe due to many things, including a relative high incidence and/or lack of appropriatetreatment of infectious diseases, especially acute respiratory infection and diarrhealdisease in this population (see comments in National Health Statistics Report, 1998). Inmaking comparisons, it should be remembered that the NHS rates were based on birthsand deaths over five years or two years preceding that survey (an “average” of 1993 to1997 or 1996 to 1997), and the Pathway Study rates were based on its samplepopulation during the last half of 1998 and the first half of 1999. Further, the sampledpopulation of Pathway is rural, while the NHS includes representative numbers ofurban.
Table 3.1: Comparison of the Mortality Rates of the Pathway Study and the NHS(1998)
Neonatal MortalityRate
(Day 0-28)
Post-neonatalMortality Rate (one
month to one year ofage)
Infant Mortality Rate(Day 0 to one year of
age)
Under Five MortalityRate (Day 0 to five
years of age)
PathwayStudy NHS Pathway
Study NHS PathwayStudy NHS Pathway
Study NHS
30 36 61 54 91 89 124 115
To determine the possible causes of death, the Pathway Working Group (PWG)reviewed all verbal autopsy questionnaires and open histories, and proposed up to threemain diagnoses. In some cases, up to two additional diagnoses or conditions weregrouped as contributing factors. The group based its judgment on the child’s history,the group’s clinical experience, and diagnostic algorithms of the most common childmortality conditions.
According to health statistics, the main causes of death among children less thanfive years of age in Cambodia are ARI (especially pneumonia), diarrhea, malaria,dengue hemorraghic fever, dysentery and meningitis (National Health Statistics Report,1998 (NHSR)). The causes of death in this study, based on the assessment of the PWG,are relatively consistent with the national health statistics.

12
Neonatal tetanus and prematurity are the causes for almost a third of the deathsamong infants under one month, followed by hypoxia and septicemia that account foranother quarter of the deaths. The high proportion of neonatal deaths attributed toneonatal tetanus is consistent with other studies conducted in Cambodia.
Table 3.2: Primary Causes of Death among Infants and Children by Age
Age Cause of Death(n=145)
Percentage of ThoseWho Died
Less than oneMonth (Neonates)
Neonatal TetanusPrematureHypoxia
Septicemia
(N=35)*
15.815.813.213.2
58.0
One Month through 11Months (Post
neonates)
MeningitisPneumoniaDiarrhea/DysenterySepticemia
(N=74)*
21.619.317.112.5
70.5
One Year throughFour Years
Acute HemorrhagicFeverDrowningDiarrhea/DysenteryPneumonia
(N=36)*
23.814.39.59.5
57.1
* The numbers used here are smaller than the number of actual deaths, andrepresent the deaths where it was possible to conduct interviews with caretakers (seepage 12).
Meningitis, pneumonia and diarrhea/dysentery account for almost 60 percent ofall deaths among infants aged 1 – 12 months. Acute hemorrhagic fever is responsiblefor almost a quarter of the deaths in the age group one to four years.

13
Diarrhea/dysentery and pneumonia, together, account for another fifth of the deaths inthis group.
Childhood deaths most often have contributing factors in addition to a primaryor major cause of death. Although not grouped with the same age categories shown inthe previous table, the PWG assigned contributing factors to thirty of the infant andchildhood deaths, where group members believed there were appropriate indications todo so. These are shown in Table 3.3. It can be seen that malnutrition and diarrhea – twoof Cambodia’s well-known killers – stand out as major contributors to the primarycauses identified for infant and child deaths.
Table 3.3: Contributing Factors to Infant and Child Deaths
ContributingFactors
Number Percent
Malnutrition 12 40
Diarrhea/Dysentery 7 23.3
Drug or IV FluidOverdose
2 6.7
Hearth Disease 2 6.7
Malaria 2 6.7
Blood Problem 1 3.3
Anemia 1 3.3Premature/Low BirthWeight 1 3.3
Liver Failure 1 3.3
Burn 1 3.3
Total 30 100%
To identify program solutions that respond to infant and childhood deaths inCambodia, it is essential to understand caretakers’ experiences, behaviors, and theirbeliefs associated with those experiences. The following excerpt describes the illness ofa child, 6 days of age at the time of death.

14
Forty-five percent (54 out of 119) of the mothers and other caretakersinterviewed (119) mentioned what they thought was the cause of death of their child(see Table 3.4). The caretaker’s perception about the cause of the illness will determinenot only the home treatment given, but also the care-seeking behavior. It is noteworthythat 39 percent of the caretakers (46 out of 119) thought that the illness was due tosupernatural forces, spirits, ancestors or ghosts. In some cases, the cause of deathmentioned by the mother was influenced by a provider's diagnosis (e.g. Typhoid fever).However, causes like septicemia and thrush seem to have been recognized by boththe caretakers and the health care providers.
Table 3.4: Causes of Death for Children One Week to Five YearsOf Age, according to Mothers
Causes of Deaths Number Percent
Something Wrong withAncestor
10 19
Septicemia 8 15Dengue 6 11Spirits/Ghost/Spell 6 11Thrush of the Previous Mother 5 9Hot Inside or Fever 5 9Diarrhea 3 6Convulsions 3 6Other 8 15
Total 54 100
Thrush is one of the most commonly mentioned symptoms that leads to care-seeking and a specific treatment. Sometimes thrush is perceived as a danger sign by thecaretaker. However, it is commonly accepted that thrush can be treated effectively bythe Kru Khmer, as described in the following interview about the illness of a child thatwas 25 days old at the time of death.
The Mother,
“My child was born normally, and then he cried, but nothing was wrongwith him. I cut his cord with the black scissors that was used for cuttinghair. He was first breast-fed when he was three days old. On the fourthday, my child contracted his arms and cried. I asked my husband why mychild cried and cried. When I put him on my breast, he refused to breast-feed. I wondered why my child contracted his arms and legs since henever had before. I didn't know what to do because my child was so small.Then my husband told me that only Kru Khmer know what to do. So Ifetched my uncle, a Kru Khmer, to give my child a blessing.

15
3.2 HOME CASE MANAGEMENT
Home care represents the first step in the chain of actions normally taken by acaretaker once the child is recognized to be ill. Home care will normally continue untilsuch time that the caretaker feels s/he is no longer capable of treating the child andneeds assistance. When analyzing “home care,” the actions or treatments should beseen as part of the overall sequence of health-seeking behavior. Home care actionsshould also be interpreted and understood within the cultural context of the caretaker.
Table 3.5: Most Common Symptoms Mentioned by Caretakers – forChildren 8 Days to Five Years of Age
Symptom*Number of
timesMentioned
Percent ofCases
(n=108)**Fever 97 90Stopped being able to follow movementwith her/his eyes 84 78Difficult Breathing 76 70Fast Breathing 68 63Convulsions 60 56Lethargic 57 53Stopped taking food, feeding 56 52Cough 54 50Very Pale 45 42Abdominal Distention 43 40Vomiting 34 31Other 435 --
The Mother,
“The time of the illness that led to the death was 5 days. At firstmy child often vomited. Every night I could not sleep because Ihad to change my child's sheet. After my child vomited for 3days, I was told that she had thrush and that I must take her to aKru Khmer to cut the thrush. The thrush contained white bumpslike the rice grains. Before cutting thrush, the Kru Khmersoaked a cloth in gin then used it to clean in my child's mouth.After that the Kru Khmer cut my child's thrush with the wing ofporcupine. After that, the Kru Khmer told me to take my child tocut thrush again because my child didn't recover from the firstcutting. When I arrived home, I found that my child was veryhot. Her arms and legs were purple. Sometimes she got up toplay around and sometimes she breast-fed, but she still vomited.I thought that my child was getting better and the next day Iwould take her to see the Kru Khmer again. The next day when

16
* It receives comment elsewhere, but caregivers do not see diarrhea as animportant symptom, i.e., it is seen as almost a “normal” or acceptableoccurrence.
** Number of cases that named symptoms.
Whether or not caretakers recognize the preceding symptoms as somethingrequiring treatment is another matter. For the purposes of this study, a home treatmentwas considered as anything given by the caretaker at home during the illness of thechild. The home treatments were grouped as traditional remedies applied externally(e.g. massage with oil or herbs, applied wet scarf on the body, coining, blessing...),traditional medicines given to the child (e.g. traditional herbs) and modern medicinegiven to the child (e.g. antibiotics, antipyretic, unspecified medicine...). During theinterview of the caretaker, great effort was made by the interviewer to identify allactions taken in relation to the illness within the home, including the names ofmedicines given or procedures applied.
Table 3.6 shows the number of times different types of home treatments weregiven/performed on children (age one week to five years of age) during an illness. Thehome treatment data are shown with the number of times outside care was sought andorganized according to the diagnosis determined by the PWG.
Out of all the actions taken by the caretaker (773 actions), only 40 percent (313actions) could be considered "home care" or actions taken in the home. Forty-fivepercent of these home treatments consisted of the caretaker giving modern medicine tothe child, 36 percent consisted of the caretaker performing an external traditionalpractice on the child, and 19 percent consisted of the caretaker giving internaltraditional medicine.
The PWG, using the information available in the questionnaires, tried to accessthe quality of the home treatment by evaluating those actions performed before anyoutside provider was visited or called (83 actions). Most of the treatments given to thechild were considered harmless or appropriate (35 percent harmless), for example,coining, praying or applying balm on the child’s body. Thirty-seven percent of thehome treatments were considered appropriate, like covering a child that has fever witha wet scarf, or giving a child with diarrhea guava bark in boiled water to drink. Whentraditional medicine was given to the child and the PWG did not have enoughinformation about its ingredients, it was not categorized. Only a small proportion ofhome remedies or actions were considered harmful (six percent). This included giving“anti diarrheal” medicines to a child with diarrhea.
The number of home treatments given to each child - ranging from one to fivetreatments - is quite similar for each diagnosis. One home remedy was given onaverage to children who were injured through an accident, while five remedies weregiven on average to children with chronic conditions. The large number given forchronic illness is explained by the long duration of the illness (almost 10 months ofduration on average).

17
Caretakers of all 119 children ages 8 days through 59 months in the study wentto visit or called a provider 460 times, with an average of 4 visits per illness. Aprovider was considered to be anyone outside the home that was visited or called by thecaretaker. It includes Kru Khmers, private providers, health center staff, and thehospital.1
1 It is important to understand who the various health care providers are that ruralvillagers use for health care services. In the Pathway Study, providers have beendistinguished as either public or private sector, or as medically trained or non-medicallytrained. Public providers include doctors, medical assistants, nurses and midwives whoare assigned to work at a government health facility. This includes provincial hospitals,referral hospitals, health centers and other government health-related offices. Privateproviders are those who operate a private practice in their home and/or by makinghome visits to their clients to provide services.
The distinction between public versus private is not so clear-cut. Many publicproviders maintain a private practice outside of their government jobs to earn enoughmoney to support their families. In effect, they wear two hats – their public one duringworking hours at the government facility, and their private one after hours.
Medically trained staff refers to any provider who has received at least some formal medical training andthose who have completed a formal program – i.e., doctors, nurses, etc. Non-medically trained providersinclude those who provide health services based on practical experience and/or with tutoring fromanother non-medical providers (e.g., a TBA who was taught her skills by her mother or other older,experienced TBA). This includes recognized Kru Khmer, TBAs, untrained drug sellers, and variousother peds (someone accepted by clients as having health care skills). Many non-medically trainedproviders have extensive practical experience, but are generally ill-equipped to deal with severe orcomplicated problems.

18
Table 3.6: Number of Times Home Treatments or Outside Care were “Given” foreach PWG Diagnosis (total number of actions taken for 119 children ageone week to Five Years of Age)
Home Treatment (Number of Actions)* Outside Care
PWG DiagnosisGave Traditional
Medicine(External)
Gave TraditionalMedicine(Internal)
Gave ModernMedicine
Went to orCalled aProvider
TotalNumber
ofActions
Meningitis (21) 27 11 24 102 164
Severe Infection (15) 17 4 20 53 94
Septicemia (14) 9 9 9 51 78
Severe Pneumonia (13) 9 6 18 56 89
Dengue Hemorrhagic Fever (10) 12 4 18 41 75
Accident (Drowning, Head Injury) (9) 3 0 4 6 13
Chronic Conditions (7) 12 13 9 46 80
Diarrhea (Acute & Persistent) (6) 4 5 11 22 42
Malaria (4) 6 1 5 22 34
Typhoid Fever (3) 2 2 4 11 19
Other (7) 7 4 10 34 55
No Diagnosis (10) 4 2 8 16 30
Total 112 61 140 460 773
* "Home Treatments" are categorized as those treatments given to the child bythe caretaker.
The traditional internal home remedies most frequently used by the caretakerare listed in Table 3.7, along with information regarding their possible medical use.There are many different traditional medicines used by Cambodians to treat a variety ofillnesses. Caretakers will often mix the herbs listed with other combinations of herbs,plants, fruits, animal parts and minerals from rocks to produce a concoction for treatinga specific disease. In most cases, there does not seem to be any particular medicalreason for adding these additional ingredients. However, in some cases herbs aremixed together so as to treat more than one ailment simultaneously.
The most popular herbal remedies are the ones used for diarrhea and fever.Guava bark is used throughout Cambodia to treat diarrhea and dysentery. The fruit andbark of the "sticky wood apple" tree is regularly used to treat persistent diarrhea and isoften mixed with guava and other ingredients.
The leaf of the marigold flower is often used for dysentery. It is said to act likeImodium® in the sense that it stops bleeding and defecating. The bark of the cottontree is used to treat food poisoning.

19
Table 3.7: Traditional Medicines Used by Caretakers and their Potential Usefulness
Traditional MedicineKhmer Name English
EquivalentPossible Medical
UseNotes
Sambo Trobeik Guava Bark Diarrhea, Dysentery Mixed with waterSambo Phnau Wood Apple Fruit Persistent Diarrhea Mixed with guava,
Sleuk Sabbai Rueng Marigold Flower Dysentery Acts like Imodium®
Sambo Kabbah Bark of Cotton Food Poisoning
Pengkal Kaek Bark of Parasite Fever Reduction Boiled in water
Sleuk Sdau Unknown Fever Reduction Boiled in water
Kroup Slang Seed of Vomiting and Fever Taken in small
Deik Kol Rusty Nail Anemia Boiled in waterDeum Pro Phlai Unknown Anemia, jaundiceSnau Chtol Phnum Clover ColitisPhlai Angkung Unknown Stomach PainBandal Pich Vine & Tamrind Malnutrition Mixed with salt
Fever reducers used by caregivers include the dried leaves of the "parasiteplant" boiled in water. It is said to quickly reduce fever. Another fever reducer oftenused by mothers is the sleuk sdau plant mixed with water. It is also said to reduce feverquickly.
The seed of the Nuxvomica tree is used in small quantities to treat Dengue. It issaid to reduce vomiting and fever. Care must be taken in using this medicine since it ispoisonous in large amounts.
Anemia is often treated by boiling rusty nails in water. A plant, known inKhmer as deum pro phlai, is also used to treat anemia. It is also said to be good forjaundice and other blood problems.
Colitis is treated with clover and with a big black fruit known as phlai angkung.Both are said to be good for treating stomach pain.
Finally, there is an herbal remedy used throughout Cambodia for treatingmalnutrition. It includes the vine of the bandal pich mixed together with Tamarind andsalt. Kru Khmers will often prescribe this medicine along with Guava bark to stopdiarrhea and gain weight.

20
3.3 CARE-SEEKING BEHAVIOR
The presence of danger signs, as indicative of severe illness, should lead thecaretakers to seek care from a health provider outside the home. The danger signs usedin this study are those proposed by the integrated management of childhood illness(IMCI) strategy: lethargic, unconscious, convulsions, difficult breathing, fast breathing,visible blood in stool, and stops taking food or feeding. Fever (most common signmentioned) and vomiting "everything" were not considered danger signs for this study.Vomiting "everything" was not included because confusion over the definition mayhave led certain caregivers to specify that the symptom was present when in fact it wasnot.
All the caretakers recognize possible danger signs, because they were includedin their response to questions regarding their infant/child symptoms prior to death (seeTable 3.7). However, as seen in Table 3.8, only 92 of the 108 caregivers associated oneor more of these symptoms as a serious danger sign. Only 40 of the 92 ( 44 percent)who recognized a danger sign sought care from a health provider, at the time ofrecognizing the danger sign. The remaining caretakers took no action apparently notrecognizing the severity of the symptom(s) and/or the need for seeking care. Whencare was sought for a dangerous symptom, a little over 40% reported they consulted aKru Khmer or drug seller. According to the open history and the open ended questions,when the caretaker recognizes the presence of convulsions, the child is more likely tobe taken to the Kru Khmer than to another provider, since it is widely believed thatconvulsions can only be cured by a Kru Khmer. This tendency is reflected in the table,where eight of the twelve children with convulsions were taken to the Kru Khmer.
Table 3.8: Care-seeking Behavior in Response to the First Time the CaretakerRecognized Any Danger Sign
Sought Care (sameday) in Response toDanger Sign (n=92)*
Type of Provider Consulted if Danger Sign wasRecognized (n= 40)Danger Sign
(Number)
Yes No
PrivateProvider
Health Center,Hospital
Kru Khmer,Drug seller
Lethargic (17) 7 10 3 1 3
Convulsions (25) 12 13 4 - 8
Fast breathing (27) 4 13 1 2 1
Difficult breathing (11) 3 8 2 1 -
Visible blood in stools (5) 3 2 - 3 -
Stop taking food or feeding (11) 7 4 2 1 4
Unconscious (6) 4 2 1 2 1
Total (92) 40 52 13 10 17
• The caretaker recognized the severity of the danger signs if, havingmentioned the presence of any of the listed symptoms/signs, any type

21
of care was sought the same day they noticed the sign for the first time.If they didn’t seek care that day it was presumed that they didn’trecognize the severity.
• The recognition and actions taken when fever and convulsions are present are
described in the following interview about the illness of a child one month and threedays old.
Fast breathing and difficult breathing, even though recognized by the caretaker,did not lead to consulting any provider immediately in 21 out of 38 cases. Therecognition of danger signs and the necessity of seeking care with a medicalprovider should be reinforced through the health system as well as at communitylevel. Any child with one or more of these signs is severely ill, and should be takento a medical provider.
Among the various factors to consider when evaluating the care-seekingbehavior of caretakers is the proximity of the caretaker to the various providers. Theaccessibility of various providers is often cited as a reason by the caretaker forvisiting/not visiting a given health provider. Table 3.9 shows the average time neededto access health facilities in the study villages.
Table 3.9: Approximate Travel Time to Health Provider in Minutes*Travel Time in Minutes in order to Reach:Province
Khru Khmer Drug Seller PrivateProvider
HealthCenter**
Hospital**
Kampot 14 20 26 61 58Pursat 23 27 48 13 54Siem Reap 17 20 23 29 75StungTreng***
21 28 24 1499 (25hrs.)
1756 (29hrs.)
Average**** 18 22 27 34 62
The Mother,
“My mother-in-law told my husband to fetch my father-in-law for blessing mychild. My son wasn't better but he no longer had a high temperature. At about8.00pm my son cried harder and harder. My father- in-law told me to fetch myuncle to blessing my son to stop his convulsions. During the convulsions, firstmy son had a stiff neck and stopped being able to feed. After the blessing, myuncle told me to fetch another Kru Khmer, in case my son had somethingwrong with an ancestor. After that my uncle gave him a blessing again but theresult was still bad. I fetched another Kru Khmer to see him. My son stoppedfeeding. His tongue was hard. He stopped taking everything and his neck wasstiff. At 1.00am his condition became most serious. I fetched my uncle to seehim again. At 3.00am I fetched the other Kru Khmer again. But the KruKhmer didn't come and said that my son could not be live because his previousmother got into his body. The Kru Khmer also told me to prepare rice and burnincenses. My son died while the incense was still burning.”

22
* Travel times based on dry season travel. Travel times can increase dramaticallyduring wet season when roads are often flooded and/or impassable.
** Distance to health centers and hospitals determined by MoH, while other timedistances estimated by mothers.*** The great length of time it takes to reach a health center or a hospital in Stung
Treng reflects the location of the study sample, but it is also a clear indication ofthe general travel problem for persons living in Stung Treng.
**** Stung Treng was not included in the calculations of average times.It was assumed that the time spent to travel to each of the health providers
mentioned by the mother is the “normal” amount of time in her usual way oftransportation. The Kru Khmer is, in all four provinces, the health provider closest tothe caretaker’s home.
Table 3.10: Number of Caretakers Who Sought Care for Their Children During theIllness that Lead to Death for Children from One Week to Five Years ofAge
Care-seeking by Caretakers (n=108)*
Provider
Number**who
Soughtcare fromProviderduringIllness
Percentwho
receivedany kind ofRecommen
da-tionfrom
Provider(n)
Percentwho
followedall
Recommnen-dations
(n)
Percent ofProviderswho gaveReferals
(n)
Percent ofMothers
whofollowedReferral
ofProvider
(n)
Kru Khmer 7877%(60)
87%(52)
33%(26)
58%(15)
Drug Seller 6491%(58)
97%(56)
25%(16)
31%(5)
Private Provider 5485%(46)
83%(38)
48%(26)
46%(12)
Health Center 1479%(11)
91%(10)
14%(2)
50%(1)
Hospital 2592%(23)
87%(20)
72%(18)
89%(16)
Total Care-seekingActions
23584%(198)
89%(176)
37%(88)
56%(49)
* Only eleven out of the 119 caretakers interviewed did not eventually seek any care outside the

23
home, and almost all of these caretakers were parents of children that drowned or had anothertype of accident. Others were caretakers of children whose illnesses that led to death were tooshort to take any action outside the home. Consequently, the above table represents the care-seeking behavior of 108 caretakers.
** Many caretakers visited multiple providers.
Table 3.10 presents the care-seeking behaviour of 108 caretakers by the type ofprovider visited and the actions taken/recommendations made by the provider. Theobjective of this table is not only to show how often caretakers visited certain providersbut also to show whether they received recommendations/referrals from thoseproviders, and, if so, whether the recommendations/referrals were followed.
It can be seen that the Kru Khmer were most often sought out by caretakers,with drug sellers second, and private providers third. Hospitals represent a distantfourth and surely received children who were often very seriously ill by the time mostarrived. Health centers received the fewest amount of contacts from caretakers seeingassistance.
The actions associated with this table will be further examined in later analyses,but the overall table is informative, regarding the care-seeking behavior of the mothersin the study. Using the Kru Khmer as the example, 78 mothers went to the Kru Khmersometime during their child’s illness. 77 percent of the time, the Kru Khmer gavespecific recommendations and 87 percent of the time, mothers followed therecommendations. Further, 26 (33 percent) of the Khru Khmer made referrals tomothers and 58 percent of the time, mothers followed those referrals. Some of the cellshave very low numbers, but percentages have been shown, with the number.
Table 3.11: Causes of Death Defined by the Pathway Working Group, theAverage Duration Of the Illness and When Care Was First Sought – for ChildrenOne Week to Five Years of Age (more than one cause can be assigned to adeath)
PossibleCause of death
Numberof Cases
AverageDuration of
Illness(days)
Average Numberof times Care was
Sought for thisIllness
Average Number of Daysbefore Care was Sought by
any Provider
Meningitis/Encephalitis 24 10 4.8 3.4
Severe Pneumonia 22 11 4.3 1.8
Diarrhea/Dysentery19 10 3.7 2.4
Septicemia 18 12 3.6 1.2
Severe Infection 15 16 3.5 1.3
Dengue HemorrhagicFever 12 6 4.1 0.2
Accident (Head Injury/Drowning) 9 0.8 0.3 0.5
Chronic Conditions(Malnutrition/TBC)
8130 6.5 8.4
Malaria 4 11 5.5 0.5
24
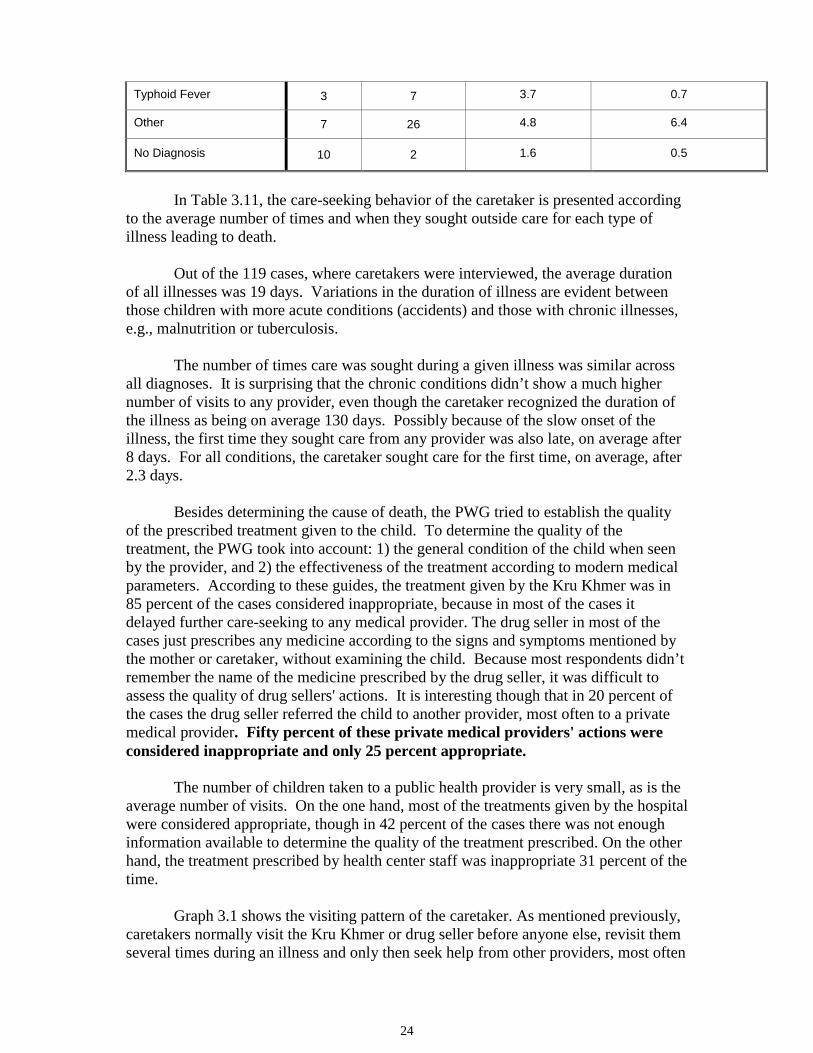
Typhoid Fever 3 7 3.7 0.7
Other 7 26 4.8 6.4
No Diagnosis 10 2 1.6 0.5
In Table 3.11, the care-seeking behavior of the caretaker is presented accordingto the average number of times and when they sought outside care for each type ofillness leading to death.
Out of the 119 cases, where caretakers were interviewed, the average durationof all illnesses was 19 days. Variations in the duration of illness are evident betweenthose children with more acute conditions (accidents) and those with chronic illnesses,e.g., malnutrition or tuberculosis.
The number of times care was sought during a given illness was similar acrossall diagnoses. It is surprising that the chronic conditions didn’t show a much highernumber of visits to any provider, even though the caretaker recognized the duration ofthe illness as being on average 130 days. Possibly because of the slow onset of theillness, the first time they sought care from any provider was also late, on average after8 days. For all conditions, the caretaker sought care for the first time, on average, after2.3 days.
Besides determining the cause of death, the PWG tried to establish the qualityof the prescribed treatment given to the child. To determine the quality of thetreatment, the PWG took into account: 1) the general condition of the child when seenby the provider, and 2) the effectiveness of the treatment according to modern medicalparameters. According to these guides, the treatment given by the Kru Khmer was in85 percent of the cases considered inappropriate, because in most of the cases itdelayed further care-seeking to any medical provider. The drug seller in most of thecases just prescribes any medicine according to the signs and symptoms mentioned bythe mother or caretaker, without examining the child. Because most respondents didn’tremember the name of the medicine prescribed by the drug seller, it was difficult toassess the quality of drug sellers' actions. It is interesting though that in 20 percent ofthe cases the drug seller referred the child to another provider, most often to a privatemedical provider. Fifty percent of these private medical providers' actions wereconsidered inappropriate and only 25 percent appropriate.
The number of children taken to a public health provider is very small, as is theaverage number of visits. On the one hand, most of the treatments given by the hospitalwere considered appropriate, though in 42 percent of the cases there was not enoughinformation available to determine the quality of the treatment prescribed. On the otherhand, the treatment prescribed by health center staff was inappropriate 31 percent of thetime.
Graph 3.1 shows the visiting pattern of the caretaker. As mentioned previously,caretakers normally visit the Kru Khmer or drug seller before anyone else, revisit themseveral times during an illness and only then seek help from other providers, most often

25
a private medical provider. Public health facilities are often only visited when the childhas gotten seriously ill and then caretakers normally visit a hospital.
Graph 3.1: First and Last Provider Visited During the Illness that Led to the Death ofthe
Child
It can be seen that while caretakers sought Kru Khmer and drug sellers 78percent of the time on the initial care-seeking visit, this percentage decreased to 44percent near the end of the child’s illness. It can be assumed that the child’s illness wasmore clearly identified as serious, and the earlier treatment from Kru Khmer and drugsellers as not effective. Seeking assistance from the health centers and hospitalsincreased, but the major increase was in seeking out private providers. Since manyprivate providers are also public health workers, there is most likely a large, if notcomplete, overlap between private providers and health center providers.
There were many reasons cited by caretakers for not visiting a public healthprovider. Table 3.12 lists the ten most often cited by caretakers. The most frequentlymentioned reason was the lack of money or the perceived cost of the consultation,which probably included in some cases the transportation cost. The distance and poortransportation was also a common reason for not using a public health facility.
Table 3.12: Reasons for Not Going to a Public Health Provider
Reasons Mentioned Spontaneously Number Percent
No money/too expensive 63 18.4
Child was not serious enough to seek care from public health provider 47 13.7
Health center too far away 38 11.1
Poor transportation 26 7.6
Public provider doesn't know how to treat certain diseases 18 5.3
Poor perceived quality of treatment 17 5.0
Nobody to look after the house or children 15 4.4
21%
48%
23%30%
37%
10% 7%4%12%
8%
0
10
20
30
40
50
60
First Provider Visited Last Provider Visited
Kru KhmerDrug SellerPrivate ProviderHealth CenterHospital

26
No knowledge about public provider 11 3.2
Public provider was not the first choice 10 2.9
Other 97 28.4
Total 342 100
Since cost was the main reasons for not going to a public health provider, it isuseful to analyze the average cost paid to each provider during an illness as well as theaverage cost per visit. This information is provided in Table 3.13.
Table 3.13: Average Cost Paid to Each Provider During Entire Care-seeking Processby Province and Type of Provider*
Province Kru Khmer(n)**
Drug Seller(n)
PrivateProvider
(n)
Health Center(n)
Hospital(n)
Kampot $3.51***(23)
$0.49(8)
$2.61(9) (0)
$5.04(6)
Pursat $1.08(19)
$1.25(13)
$4.13(12)
$0.26(6)
$6.78(6)
Siem Reap $2.51(30)
$4.52(40)
$7.68(21)
$0.75(9)
$19.50(10)
Stung Treng $2.71(6)
$6.31(7)
$16.66(4) (0)
$0.00(1)
Average Cost perIllness
$2.41(78)
$3.51(64)
$6.08(46)
$0.56(15)
$11.56(23)
Average Cost perVisit $1.11 $2.79 $2.43 $0.36 $9.91
* Figures do not include those who did not pay for services, those who donot remember how much they paid and those who paid in kind forservices.
** Some figures vary slightly from those reported in Table 3.10 due toincomplete questionnaires.
*** The rate of exchange used was US$1 = 4,000 riel. US$ figures wererounded to the nearest cent.
The average cost per illness and average cost per visit is lowest by far at thepublic health center. This finding would seem to contradict the perception of caretakersthat the public health facility is expensive. However, one must take into considerationthat when a caretaker visits a health center they are often not provided service directlyat the health center. Instead, they are directed to visit the private practice of the healthprovider. In the data collected, there is no way of determine the magnitude of thispractice in the sample.
After the health center, the Kru Khmer cost the least ($2.41 per illness and$1.11 per visit). It should be noted that the Kru Khmer is sometimes paid in-kind bycaretakers. Kru Khmers will sometimes accept rice, chickens and other household

27
goods in lieu of money. Unlike the public providers, they will also provide credit tocaretakers, which may be an important consideration as to why they are chosen.
3.4 DIARRHEA MANAGEMENT
For all children who had diarrhea during the illness that led to death, a separateset of questions was asked of the caretaker. This included the type of home treatmentgiven to the child for diarrhea as well as the treatment prescribed by the providervisited during the illness.
A description of the events of the illness is recorded in the following interviewof a child 5 months and 6 days old at the time of his death.
Almost 30 percent of the children experienced diarrhea during their illness. It iswell known that children with diarrhea should receive considerably more fluids andfood than usual to replenish lost nutrients and electrolytes. However, nearly a quarterof caretakers gave less fluids and foods during the illness. Anecdotal informationsuggests that many caretakers do not view diarrhea as serious, and that some evenbelieve that one should reduce feeding to cure the disease.
The Mother,
“During the illness that led to the death was five days old. At first he had a cold with acough and a fever. After that he vomited. I went to buy medicine for him. After taking themedicine he did not get better but also had diarrhea with watery stools. I fetched thepractitioner in the village to see him but the practitioner was busy and he couldn't come.Then I took my child to the practitioner's house. He examined and gave my child twoshots. My child was still vomiting and had even heavier diarrhea. I took my child bymotorbike to see another private practitioner. When we arrived there this privatepractitioner examined and gave my child three shots and as much ORS possible becausemy child was very thirsty. My child still had heavy diarrhea even after drinking. Theprivate practitioner shaved my child's hair to give him IV fluid. He changed the place ofthe needle about ten times but he still couldn't get it in. Then he gave up. After that hetold me to bring my child home for praying because something was wrong with theancestors and that is why my child couldn't be given IV fluid. My child cried stronger,got agitated, and still had heavy diarrhea with abdominal distension. The practitioneralso told me to take my child to public hospital if my child was not better after prayingand he gave me some ORS and some medicine for my child's abdominal distension. Ibrought my child back home. When I arrived home at about 3.00pm, I found that mychild had sunken eyes. Many times he asked me for something drink. He cried and criedand could not sleep. I didn't pray, but only gave my child ORS and the medicine. Then hedied at 11.00pm.”

28
Graph 3.2: Amount of Fluid and Food Received from the Caretaker at Homeduring diarrhea
Most of the children who were seen by a provider outside the home receivedsome type of medicine, prescribed mainly by the drug seller or private provider. Themajority of the providers told the caretakers to boil water for the diarrhea. ORS wasrecommended by less than half of the providers visited (N=22).
3.5 SUMMARY
Given that the focus of the Pathway Study is on infant and child deaths, thereare not success stories to report. However, contained in Section Three are goodestimates of what the infant and child death rates are in the rural areas of the provincesstudied (and quite possibly in much of rural Cambodia) and what the attributed causesof death are.
While it is not surprising and quite logical, rural Cambodians – who live withpoor roads and have poor means of, and access to, transportation – find care for theirinfants and children largely within their communities. Clearly, when caregiversrecognize the seriousness of their child’s illness, they make decisions and findresources (often too late) to get the child to where more efficacious care might befound, i.e., private providers (at least some with medical knowledge), health centers,and hospitals.
The data presented here make clear that there is a tremendous challenge (and,we believe, partially achievable even in the short term) to awaken caregivers andproviders to simple, affordable preventive measures, e.g., immediate and exclusivebreastfeeding and clean deliveries.
The challenge also goes to all providers to increase their knowledge and to offerbetter services and outreach from fixed health sites. In order to make a contribution inthe struggle to reduce infant and child mortality in Cambodia, success on all of thesefronts is necessary and none will make much difference by itself.
6
10
Fluids Food
1013
7
1
8
15
8
0024
8
121416
MorThe sameLesNot at

29
Section 4
Perinatal Mortality
Perinatal death, as defined by WHO, includes all still births occurring after sixmonths of pregnancy and all deaths of infants through the seventh day of life. Theworldwide perinatal mortality rate is 57 per 1,000 live births, with Southeast Asiahaving the highest perinatal mortality rate, and accounting for almost one third of allperinatal death.
According to the World Health Organization (WHO), each year approximately7.3 million deaths occur worldwide during the perinatal period. Of these, 98 percentoccur in developing countries. A large proportion of perinatal deaths occur during thefirst 7 days of life. In Cambodia there is little data available about perinatal death.However, WHO, in a perinatal report summary, estimates the perinatal death rate forCambodia to be 65 per 1,000 live births.
Partially because of the particularly difficult task of collecting good informationon the last three months of pregnancy and the first few days of life in rural Cambodia,less data exist and less attention has been paid to perinatal mortality compared toneonatal, post-neonatal, and infant mortality. To give some perspective to theimportance of days 0-7 for an infant, those days account only for 2 percent of aninfant’s first year of life, but in this study represent 24 percent of all deaths duringthe first year. 1
This study, using the verbal and social autopsy methodology, aimed to obtaininformation at the community level about perinatal mortality. Through the verbalautopsy, the PWG determined the possible cause of death and other conditions thatmight have led to the death of the infant. The social autopsy focused on the problemsthat occurred during pregnancy, delivery and during the illness of the newborn infant.This section includes a description of antenatal care, causes of death, home-caremanagement and care-seeking behavior, associated with perinatal deaths.
4.1 CHARACTERISTICS OF THE STUDY POPULATION
The perinatal mortality study was conducted simultaneously with the infant andunder-five mortality study. Through the surveillance system, 70 village monitorstracked all women of reproductive age living in the 40 villages included in the study.Every month for one full year, the village monitors visited the residents of the villagesin the study, identifying all pregnant women and established whether there had beenany abortions/miscarriages, stillbirths or deaths of infants less than 7 days of age.Whenever such deaths were encountered, an interviewer was assigned to conduct an 1 Due to the initial leadership given the Pathway Study at RACHA, and the close relationship withBASICS, USAID’s premier program working with child health, an emphasis on the perinatal period wasdetermined and maintained. The BASICS program has been at the forefront in drawing attention to theimportance of the perinatal period. This study represents the first, large-scale attempt in Cambodia tobegin to develop a rigorous database about the perinatal period and the mortality associated with it.

30
interview with the primary caretaker of the deceased child. In most cases the caretakerwas the mother. Table 4.1 shows the total number of pregnant women followed duringthe one-year period of the study, as well as the number of abortions/miscarriages andperinatal deaths identified.

31
Table 4.1: Description of the Population Under Surveillance
Perinatal DeathLocation Number of
PregnantWomen
Tracked*
Number ofAbortions/
Miscarriages Numberof
Stillbirths
Number.of Babies(0- 7 days)
Total
PerinatalMortality
Rate
Kampot 518 21 12 8 20
Pursat 529 60 6 7 13
Siem Reap 857 55 12 10 22
StungTreng 117 3 4 1 5
Total 2,021 139 34 26** 60 47
* Some of these women did not give birth through the duration of thestudy.
** Twenty-six deaths were determined for infants age 0-7 days. For one ofthe cases it was not possible to collect information, so the number 25 isreported in most of the following tables.
Over the one-year period, 2,021 pregnant women were identified in the fourprovinces included in the study. One hundred thirty-nine abortions/miscarriages werealso identified. It is most probable that abortions/miscarriages were under-reported.Abortions/miscarriages that occurred during the first two to three months, as well asinduced abortions, may have been missed.
To assure that all perinatal deaths were identified correctly and included in thestudy, the interviewer had to interview all the mothers of an identifiedabortion/miscarriage, and establish if it was or was not a perinatal death. In a greatnumber of cases, the mother could not remember her last menstruation, or didn’t evenhave one after the birth of her last child. This made it very difficult to establish theexact duration of pregnancy. In these cases, the interviewers were instructed to identifya reference date using local calendar dates, and if this was not possible, to just take themother’s word about the duration of pregnancy. Under these circumstances, it ispossible there might be cases included in this study that didn’t complete the 6th monthof pregnancy, as well as some excluded with 6 months of pregnancy or more.
In the four provinces, 60 perinatal deaths were identified during the one-yearperiod. Since the total number of births was also known (1,248) the perinatal mortalityrate could be determined. The calculated rate of 47 deaths per 1,000 births is asignificantly lower rate than the WHO (1996) estimate of 65 per 1,000 births. While the

32
results found in this study have the benefit of on-the-ground, empirical data, they alsosuffer from the problems of identifying all cases, finding relevant and knowledgeablecaretakers and establishing firm dates. It is believed, however, that the informationcollected here provides a good beginning for building knowledge about perinatal deathsin rural Cambodia.
4.2 OBSTETRIC HISTORY OF THE MOTHER
Some factors related to the mother’s obstetric history and considered as risk factors forperinatal death are listed in Table 4.2.
Table 4.2: Risk Factors for Perinatal Mortality (n=59)
Risk Factors Number Percentage
The “case” was her first pregnancy 15 25
The “case” was her second or more death 0 -
The “case” is her second or more stillbirth 6 10
Number of mothers that didn't received any kind of antenatal care 18 31
Mothers with 4 or more previous pregnancies 29 49
For 25 percent of the mothers, the perinatal death included in this study was herfirst pregnancy. A previous abortion or miscarriage was not considered to be aprevious pregnancy. Almost 50 percent had more than four previous pregnancies.Lack of antenatal care (ANC) during the pregnancy was also the case for 31 percent ofthe mothers.
4.2.1 Antenatal Care
Table 4.3 provides information on those who actually sought antenatal care (38mothers). It shows which type of provider was visited, the average number of timesvisited, and the average month of pregnancy when first visited. It should be noted thatsome of the mothers might have visited the Kru Khmer and drug seller for more thanjust to receive antenatal care.
Table 4.3: Antenatal Care -- 38 Pregnant Women Received Antenatal Care from Oneor
More Providers

33
Provider Number that wentfor ANC at least
once to...
AverageNumber of
Visits
First ANCVisit was to . . .
Average month ofPregnancy at first
ANC visit
Kru Khmer 5 3 4 5
TBA 20 2 12 4
HealthCenter
22 2 10 5
PrivateProvider
8 5 5 5
Hospital 6 1 1 5
Drug Seller 12 3 6 3
Of 59 mothers in the perinatal study, 31 percent received no ANC whatsoever.As Table 4.3 shows, the majority of mothers sought ANC at either the public healthcenter or through a traditional birth attendant (TBA). The health center or the TBAwere the first providers sought by 58 percent of mothers. It is important to note thatmothers do identify health centers a proper provider for ANC, but that they are not yetregarded as important sources for treatment of childhood illness.
The average month of pregnancy when mothers first went to see any providerfor ANC was the fourth month, compared with the sixth month observed in the NHS.The frequency with which providers were visited varied between providers. Privatemedical providers were visited five times on average, while the hospital was visitedonly once. The TBA and health center were only consulted, on average, two times forANC. This level of antenatal care is normally considered inadequate and maycontribute not only to the high perinatal mortality, but also to maternal mortality.Furthermore, the Kru Khmer and drug seller cannot really be considered as capable ofproviding quality ANC according to WHO standards, and neither can the TBA.
In evaluating the quality of the ANC received by mothers during pregnancy,standard practices such as whether tetanus vaccine was given and whether routine testswere administered was assessed. Table 4.4 presents the findings.
Table 4.4: Quality of the Antenatal Care Received from Any Provider

34
Characteristics Number Percent
Women who received antenatal care 38 -
Women who received tetanus vaccine during this pregnancy Received 1 dose Received 2 or more doses
22139
583424
Height of uterus was measured 22 58
Blood pressure was measured 22 58
Urine test taken 2 5
Blood test taken 2 5
Medicine prescribed Iron Antibiotic Antimalarial Other
1521
20
3853
51
Out of the 38 women who received ANC, 22 (58 percent) received a tetanusvaccine during the pregnancy, but only 24 percent received the recommended two ormore doses. If we consider the percentage of all the women included in the studythat received the recommended two doses of tetanus toxoid, the percentage dropsto 15 percent; the same percentage observed in the NHS.
All of the 22 women who went to the health center for ANC received tetanustoxoid vaccine, had the height of their uterus measured, and had their blood pressuretaken. However, additional laboratory tests were only taken on two occasions at thehospital level. The quality of the ANC provided by the Kru Khmer, TBA and drugseller was difficult to evaluate since no information about what was done during theANC by these providers was recorded in the questionnaire.
4.2.2 Characteristics of the Delivery
Seventy-eight percent of all perinatal “births” in the four provinces occurred athome or at a relative/friend’s house. Also, 20 percent were delivered by medicallytrained staff. There is a definite need to improve delivery conditions at medicalfacilities, as well as to change the practice of delivering at home, especially when thepregnancies and/or deliveries are of high risk. No relationship between ANC anddelivery at a medical facility could be observed in this study, even though a positiverelationship has been described in the NHS.
Table 4.5: Place of Delivery for Perinatal Deaths

35
Place of Delivery Number PercentHome 41 70Relatives/Friends 5 8Health Center 2 3Hospital 10 17Other 1 2
Total 59 100
Out of the 59 deliveries, a TBA attended 55 percent of the deliveries, while 20percent of mothers delivered without the assistance of any provider (all still births afterthe sixth month of pregnancy are included as part of this percentage). In the PathwayStudy of perinatal births, a midwife delivered the baby in 17 percent of the cases, whilea doctor delivered in only 8 percent of the cases.
The most frequently mentioned reasons for preferring home delivery overdelivery assisted by trained medical personnel were that the mother was accustomed todelivering her baby at home, and it was less expensive to deliver at home. Most of themothers were the principal decision-maker in selecting the birthplace of the baby.Seventy-three percent of them delivered the baby at the place they initially planned todeliver. The remaining 27 percent were forced to change the place of birth (due tocomplications during delivery or because they were referred by another provider).
In most of the deliveries, the umbilical cord was cut with scissors (52 percent).Other tools were also used. In 44 percent of the cases a razor blade, whether new ornot, was used. Only one cord was cut with bamboo. In only four cases was somethingput on the cord (gentian violet and wasp nest). Most of the infants were bathed withinthe first hour after birth, and stayed with the mother.

36
4.3 CAUSES OF DEATH
Table 4.6: Number of Times Obstetric Factors Were Assigned to Stillbirths andInfants Born Alive by the Pathway Working Group
Perinatal DeathsObstetric Factors associated
with DeathNumber ofStillbirths
(n= 34)
NumberBorn Alive
(n=25)
Total(n=59)
Intrauterine Fetal Death DuringPregnancy
21 - 21
Intrauterine Fetal Death DuringLabor/Delivery
5 - 5
Bleeding During Pregnancy 9 1 10Placenta Praevia 1 - 1Pre/eclampsia 8 2 10Multiple Pregnancy 3 4 7Breech Presentation 7 4 11Preterm Labor 8 5 13Premature Rupture Of Membranes 4 - 4Infection of the Fetal Membrane (Chorio-amnionitis)
2 - 2
Difficult Labor 6 2 8Prolonged Labor 9 6 15Ruptured Uterus 1 - 1
Malaria 2 - 2Anemia 5 2 7
ComplicatingFactors
Trauma 5 2 7Total 96 28 124
Table 4.6 presents the causes of death assigned by the PWG for the stillbirthsand for the newborn infants. As was the case for the deaths among children betweenone week and five years, the PWG reviewed all cases of perinatal death to establish thepossible cause of death of the stillborn or infant born alive. To determine the cause orcontributing factors, the open history and the verbal autopsy were reviewed by thePWG. The causes were divided between those related to the mother’s obstetriccomplications, and those related to the newborn. The causes of the neonatal deathswere highlighted in Table 3.2.
The PWG found 124 obstetric compromising factors in 59 fatal cases. Seventy-eight percent of these factors were related to the stillborn children, while only 22percent were related to infants born alive. It is surprising that in 62 percent of thestillbirths, an intrauterine fetal death during pregnancy could be determined. Thismeans that the majority of these deaths were not caused by conditions related to laborand delivery.

37
In 30 out of 59 (52%) perinatal deaths, no possible cause of death could beidentified with the information available in the questionnaire. In only 15 percent of thestillbirths could it be determined that the baby died during labor/delivery. In 24 percentof the stillbirths it was not possible to determine if the death of the child was directlyrelated to the labor/delivery. This finding is in contrast to other Pathway studies, wheremost of the perinatal deaths occurred during labor and delivery.
4.4 HOME CASE MANAGEMENT
Table 4.7: Number of Times the Different Home Treatments Were Given/Done to theMother/Young Infant During Pregnancy, Labor/Delivery and/or Infant.
Home Treatment OutsidehomePerinatal Periods
TraditionalMedicine(external)
TraditionalMedicine(internal)
Medicine(modern
)
Wentto/called in a
Provider
Total
Pregnancy 5 2 - 25 32Delivery 19 1 - 82 102New Born 10 1 4 24 39
Total 34 4 4 131 173
Home case management of the newborn infant (0-7 days) was analyzed todetermine the patterns of treatment of newborns. As seen in Table 4.7, the number ofactions taken during pregnancy was low (only 32). This is because mothers were onlyinterviewed about their care-seeking behavior during pregnancy if severe problemswere present (e.g. vaginal bleeding, hand and facial swelling, labor contractions beforetime, convulsions, high blood pressure, oliguria and premature rupture of membranes).Conversely, mothers were interviewed about their care-seeking behavior duringdelivery when any symptom was present, (whether severe or not), which partiallyexplains why more actions are reported for delivery than for pregnancy.
Out of the perinatal death for which the pathway form was completed, a total of173 actions was taken. Traditional external medicine was the most common hometreatment for problems encountered during pregnancy, delivery and with the newborn.Almost no traditional internal medicine was given/taken by the mother duringpregnancy and delivery and modern medicine was only given/taken by mothersexperiencing live births. Unlike in the infant and child mortality study, home treatmentdoes not seem to be as important during the perinatal period.

38

39
4.5. CARE-SEEKING BEHAVIOR
Table 4.8 lists the most frequently mentioned symptoms reported by therespondent as present during pregnancy. The symptoms are divided into two groups,those most common in the case of stillbirth and those most common in the case ofinfant death.
Table 4.8: Ten Most Frequently Mentioned Symptoms Identified by the MotherDuringPregnancy of Stillbirths and by Mothers with Children Born Alive
Stillbirth withSymptom
(n= 34)
Born Alive withSymptom
(n=25)Symptoms
Number Percent Number Percent
Fever 28 82 9 36
Baby stopped moving duringpregnancy
18 53 1 4
Vaginal bleeding 11 32 2 8
Pale/breathless, weak or severeanemia
7 21 4 16
Chills 6 18 2 8
Hand and facial swelling 5 15
Abdominal pain 4 12 3 12
Water broke more than 1 day beforelabor began
4 12 - -
High blood pressure 4 12 - -
Labor contraction before time 4 12 - -
Waist pain - - 3 12
Poor appetite/sleep - - 3 12
Could not walk - - 2 8
Multiple pregnancy - - 2 8
Other 20 59 9 36
Total Number of Symptoms 94 - 40 -
During pregnancy, and also for mothers with born alive infants, the mostfrequently mentioned symptom was fever. In the cases where the pregnancy resulted instillbirth, 53 percent perceived that the baby stopped moving before labor, and vaginalbleeding was present in 32 percent of the cases. Only these mothers mentioned signscompatible with pre- or eclampsia. Other common complaints for the mothers of thestillborn and born alive were pale/breathless in 19 percent of cases and chills in 13percent.

40
Table 4.9 shows the number of times each type of provider was visited by themother during pregnancy, delivery, and during the life of the newborn. The care-seeking during pregnancy and delivery is divided into stillbirth and born alive.
Table 4.9: Number of Times Each Type of Provider Was Visited by MothersDuring Pregnancy, During Delivery and During the Life of the Born Alive Baby*
Delivery
Provider
PregnancyStillbirth(n=11)
Stillbirth(n=28)
BornAlive
(n=17)
Total(n=4
5)
Newborn0-7 Days
(n=15)
Total
Referral hospital 7 12 1 13 1 21
Health center 7 3 2 5 1 13
TBA 3 23 16 39 4 46
Midwife 1 10 3 13 2 16
Kru Khmer 2 2 4 6 13 21
Drug Seller 1 --- 1 --- 1
Private Provider 4 2 2 4 2 10
Total Visits 24 53 28 81 23 118
* Only 45 out of the 60 caretakers visited any kind of provider.
During pregnancy, all mothers identified at least one symptom. Out of these, 20had one or more severe symptoms (e.g. vaginal bleeding, hand and facial swelling,labor contractions before time, convulsions, high blood pressure, oliguria and/orpremature rupture of membranes), and only those were interviewed about their care-seeking behavior. Eleven of the mothers with a severe symptom sought care outside thehome during pregnancy. The most frequently visited provider was the referral hospitaland the health center during pregnancy. Conversely, mothers who experiencedproblems during delivery had visited a TBA most often, i.e., TBAs were usually theprovider at delivery.
All mothers with problems during delivery sought outside care. The TBA is themost commonly used provider. For stillbirth cases, the referral hospital was visited 12times, and a midwife 10 times. The difference in care-seeking between the stillbirth andthe born alive could be due to more problematic deliveries for stillbirths (5 died duringdelivery, according to the PWG). This could have led to a more frequent referral to thehospital. Only one mother of a born alive infant went to a referral hospital.

41
Only eleven mothers with born alive infants sought outside care. This could bedue to the short duration of illness, since 12 of the infants died during the first day oflife. As with children more than 8 days of age at the time of death, the Kru Khmer wasthe most commonly visited provider, followed by the TBA. Only two mothers visited apublic health provider.
Table 4.10: Average Number of Times Each Provider Was Visited by the Mother DuringPregnancy, Delivery and for the Born alive Baby
Provider Pregnancy Delivery New born Total
Referral hospital 1.4 1.4 1 1.4
Health center 1.8 1 1 1.3
TBA 1 1.1 1 1.1
Midwife 1 1.9 1 1.6
Kru khmer 1 1 1.3 1.2
Drug seller --- 1 --- 1
Private provider 2 1 1 1.3
Total Average 2.2 2.3 1.5 1.8
As seen in Table 4.10 care-seeking was most frequent during pregnancy anddelivery. Of all the perinatal deaths with a pathway form completed, the averagenumber of times a provider was visited was 1.8 times. This is similar to the averagefound for infant and child deaths. As mentioned, the provider changes according to theperinatal period. The public health provider is visited during pregnancy, the TBA andmidwife during delivery and the Kru Khmer for the born alive infant. The drug sellerwas only visited during delivery, and doesn’t seem to be an important provider duringthe perinatal period, where the client is most often the mother.
Table 4.11 presents the care-seeking behavior of the mothers during pregnancy,delivery and for the born alive, according to the type of provider visited and the actionstaken/recommendations made by the provider. The objective of this table is not only toshow how often mothers visited a certain provider, but to see whether they receivedrecommendations/referrals from providers.
Approximately half of the mothers with one or more severe problems duringpregnancy didn’t seek care outside of the home. Most of the mothers that sought carewent to a public health provider, and only 2 of them went to a private provider. Over

42
90 percent of the mothers received recommendations, but only 45 percent followed allof them. About three quarters of the mothers seen by a provider were referred, but only54 percent followed the referral.
Care-seeking is quite different during delivery. During this period, all womensought outside care, since for most women it is normal to call a provider or seek careoutside home for the delivery of the baby, even if they didn’t identify a problem. Mostof them contacted a TBA, followed by the public health provider. Thirty-four thewomen seen by a provider received a recommendation, thirty-one followed allrecommendations, 15 were referred and only 11 followed referral.
Table 4.11: Care-seeking During Pregnancy, Labor/Delivery and for the BornAlive
Care-seeking Pregnancy(n= 20)
Labor/Delivery(n= 45)
Born alive(n= 25)
Did not seek care 9 0 10
Sought care 11 45 15
Went to any TBA, Kru Khmer, drug seller 4 35 13
Went to any health center, midwife,hospital, 8 16 3
Went to a private practitioner 2 4 2
Received any recommendation 10 34 6
Followed all recommendations 5 31 6
Were referred by any provider 8 15 1
Followed referral by any provider 6 11 0
For the 25 women with born-alive infants, 10 did not seek care outside of thehome. The common provider, for the child, was the Kru Khmer. This care-seekingpattern could explain that only 6 of the caretakers received any recommendation, onlyone was referred but did not follow the referral.
In Table 4.12, the care-seeking behavior of the mother during the differentperinatal periods is presented according to the average duration of the illness, and the

43
average number of days of illness when they first sought care from any provider, andthen specifically from a medical provider.
Table 4.12: Average Duration of Illness, When Mothers First Sought Care from anyProvider and from a Medical Provider -- by Pregnancy, Delivery andBorn Alive
Perinatalperiod
TotalNumberof Cases
AverageDuration
ofIllness(days)
Numberwho
SoughtCare
DuringIllness
AverageNumber ofDays whenfirst Sought
care (any provider)
Average Number ofDays when first
Sought Care from aMedical Provider
Pregnancy 20 8 days 11 6.6 13
Delivery 45 0.5 days 45 0.29 0.5
Born Alive 25 2 days 15 1.2 3.3
The average duration of the severe symptoms for pregnancy was 8 days. Eventhough the mother should have sought care immediately, the average number of days ittook her was 6.6 days, and to a medical provider 13 days. It appears that mother’srecognize symptoms but not the severity, and that leads to late care-seeking andpossibly endangers the mother’s and baby’s life.
For the delivery, all women called or visited a provider, almost immediatelyafter they identified labor pain. A TBA or midwife referred most of the women thatwent to medical providers.
The duration of the illness of the newborn averaged 2 days. As alreadymentioned for pregnancy and delivery, the medical provider was visited, on average,later then any other provider. The medical provider seems to be the last choice in thecare-seeking process, visited only when the other providers have failed to cure themother or child.
The two main reasons for not going to a public health provider are: the lack ofmoney (or the perception that the public service is too expensive), and distance or badtransportation. For the delivery, 11 percent of the women reported that they wereaccustomed to home delivery as the reason for not going to the public health provider.These findings are similar to the ones encountered in other studies, where homedelivery was preferred by 60 percent of the women. For newborns, some mothersthought that the baby was too small to be taken to the public provider. Recognizing theseverity of the baby’s illness was also important for the care-seeking decision. Theperceived bad quality of service and the fact that the delivery or illness could have beennoticed at nighttime when no service at the health center was available, were alsoreasons mentioned for not going to a public health provider.

44
In Table 4.13 the average cost in riel and US$ for the different perinatal periods,show considerable variations. For the analysis of these numbers, the different care-seeking patterns during the perinatal period should be kept in mind. Even though thequestion about the expenses during pregnancy, delivery and newborn were asked to allrespondents, the data in the table excludes all those who didn’t know how much theyspent and those that didn’t spend any money.
As mentioned earlier, during pregnancy most of the women went to a publichealth provider for treatment who was farther from their house than the other providers.During delivery all women sought care: 16 went to a public provider and 11 acceptedreferrals. The transportation to the referral hospital could explain the high average costduring delivery. The data obtained for the newborn infant only represents a few cases,since only 3 went to a public provider and none accepted referrals. There is not muchcare-seeking in this group, due to the close relationship to labor-delivery, the severityof the illness, and that most of the newborns die shortly after delivery.
Table 4.13: Average Cost During the Care-seeking Process*
Pregnancy Delivery New BornExpenses
Avg. Riel(range)
Avg.Dollar
(number)
Avg. Riel(range)
Avg.Dollar
(number)
Avg. Riel(range)
Avg.Dollar
(number)
Transportation8,745
(1,000-30,000)
$2.2(n=20)
22,450(1,500-
100,000)$5.6
(n=10) 2,000 $0.5(n=1)
Consultationcost (includesdrugs)
14,428(500-
156,000)
$3.6 (n=36)
240,976(1,000-
8,000,000)
$60(n=54)
3,083(500-5,000)
$0.8(n=6)
Other expenses55,200(600-
150,000)
$13.8(n=3)
57,708(500-
200,000)
$14(n=24) 10,000 $2.5
(n=1)
Total 78,373 $19.60 321,134 $79.60 15,083 $3.80
* The rate of exchange used was US$1 = 4,000 riel. US$ figures wererounded to the nearest cent.
The consultation cost for delivery is the highest, due to hospitalization, use ofmedicines and in some cases surgery. Other expenses account for close to $14 duringpregnancy and labor (food, to pay the provider...). The overall cost seems high,especially during delivery. It is important to note that the expenses in this table wereobtained from women with complications during pregnancy and delivery. This makesthe treatment more expensive in comparison to a "normal” pregnancy or delivery.
4.6 SUMMARY

45
The Pathway perinatal information presents a formidable programmaticchallenge for the areas sampled in this study, and it is likely indicative of the challengefaced by rural Cambodians on the whole. Only 15 percent of women received anyantenatal care, 78 percent of the births of infants in the perinatal period took place athome or at the home of a relative or friend, and these cases included proportionatelymore difficult deliveries than the norm.
Even when symptoms were identified (Table 4.8), the dangerous nature ofthese symptoms were not adequately recognized, which often led to days of waitingbefore seeking medical care. As shown in Table 3.9, the travel time (for the sampledpopulation) to a hospital, where emergency obstetric treatment might be been found isabout an hour in Kampot, Pursat, and Siem Reap, and days in Stung Treng. These timedistances were calculated when the roads are dry, not during the rainy season. Fromdata not included in this report, it is known that only 7 percent of the households owneda moto, 8 percent a boat, 36 percent an ox cart and 36 percent a bicycle – not a viablemeans of transportation for a pregnant woman, or a feeble, sick infant.
Considerable attention is rightfully being given to finding ways to facilitateaccess to emergency obstetrical care. It can be assumed that this achievement will notonly result in lowering maternal deaths, but perinatal deaths as well. However, in ruralCambodia, the Pathway data suggest that achieving the target of access to EOC at afixed health site is some time off for much of ruralCambodia. Making what is here now work better is a necessity if perinatal deaths are
to be reduced.Some specific recommendations for doing this are included in the final section
“Conclusions and Recommendations.”

46
Postneonatal Deaths
The high postneonatal rate was aresult of the high proportion ofdeaths caused by meningitis,pneumonia and diarrhea/dysentery. These are the samediseases that the NHS maintainsmay be responsible for the relativehigh post neonatal rate it found.
Local Drug Sellers
After the Kru Khmer, the localdrug sellers are the mostfrequently used providers. Usingthe private drug system inpositive ways to effectively andsafely contribute towards infantand child health should be apriority of those looking forsolutions to improved health andreduced mortality.
Section Five
Conclusions and Recommendations
This prospective study has identified: 1) mortality rates and causes of deathamong infant and children that are consistent with (and have expanded upon) thefindings from the National Health Survey; and 2) a host of issues that need to beaddressed if infant and child health is to be improved, and mortality reduced. None ofthese issues is new; however, the study highlights the magnitude and the range of theproblems faced by Cambodia and, in general, health systems, like Cambodia’s, thatare in early stages of development.
The following discussion is divided into two parts. The first focuses upon themortality rates and causes of death among infants and children; and the second, onissues identified that need to be resolved through program interventions.
5.1 MORTALITY AND CAUSES OF DEATH
The postneonatal, infant, and child under 5 mortality rates found in the studyare very similar to the rates reported by the NationalHealth Survey, and lend additional credibility to thereliability of the data collected. The only exception wasthe neonatal rate which was lower than the NHS rate.
Of particular interest is the higher proportion ofinfant deaths found in the postneonatal compared to theneonatal period. This pattern is the opposite of what isgenerally found in other developing countries whereneonatal deaths make up a larger proportion of infantdeaths.
Theprimary causes of neonatal mortality wereneonatal tetanus and prematurity. However,hypoxia and prematurity were the main causesof perinatal mortality (stillbirths and newbornsthat died during the first 7 days of life). Itshould be noted that the perinatal mortality ratewas 47 per thousand births, the first perinatalrate for Cambodia that is based upon data (notestimated) from a surveillance system.
Acute hemorragic fever accounted foralmost a quarter of the deaths among childrenaged 1 – 4 years. Diarrhea/dysentery and
pneumonia were responsible for another fifth of the deaths in this age group.
The identification of the causes of death among infant and children highlightonce again that the majority of the causes could be reduced through effective treatment

47
Breastfeeding, aSustainable Intervention
Teaching women tobreastfeed immediatelyand exclusively is probablythe most easily sustainableintervention available forimproving infant and childhealth and reducingmortality
Teach Caregivers to RecognizeDanger Signs
If major improvements in infantand child health are to be madesoon, more attention needs to begiven to teaching caregivers inthe home to recognize andrespond correctly to dangersigns.
and prevention programs. These would obviously include programs on ARI, thecontrol of diarrheal diseases (CDD), tetanus toxoid vaccination (EPI) and efforts tointroduce bednets for the prevention of hemorragic fever.
5.2 ISSUES TO BE ADDRESSED WITH INTERVENTIONS
1. Breastfeeding is not exclusive and less than half of mothers gavecolostrum to their baby.
As encountered in other studies, breastfeeding seems to be a universalpractice. Almost all of the children included in the study were breastfed (97%),but only one percent received exclusive breastfeeding, according to the WHOdefinition. This percentage is smaller then the onespublished in other studies, but it could be due to the way“exclusive breastfeeding” was defined in those studies. Thepromotion of breastfeeding has been identified as a cost-effective intervention, since it reduces the risk of diarrhea,ARI, dysentery and malnutrition. Since breastfeeding isaccepted by most Cambodian women, programs shouldpromote the importance of giving colostrum to the baby(only 43% of the children in the study received colostrum),the immediate onset of breastfeeding after birth (most ofthe women give other fluids the first one-three days afterbirth), and exclusive breastfeeding up to the age of 6months.
2. There is insufficient recognition among caretakers of the danger signs of theillness that led to the death of their infant orchild.
Among the cases that resulted in death,most children were seriously ill from thebeginning of the illness or soon after the motherrecognized the danger signs. Once the dangersign was noticed by the caretaker, almost threefifths didn’t seek care immediately, and only alittle over ten percent sought care from amedical provider. The caretaker should notattempt to give home care at this time, butshould take the child to a medical healthprovider.
3. There is inappropriate careseeking behavior that contributes to a delay inseeking carefrom a qualified health provider.
The first and most important health provider is the Kru Khmer, followed by thedrug seller. The Kru Khmer generally prescribes a treatment that includes follow upvisits for prayer and blessing. The time spent for this treatment frequently delayed

48
The Kru Khmer
Can a complementary, safe rolebe found for the Kru Khmer inimproving infant and childhealth? It is the Khu Khmerwho first and most often sees asick child – and it is safe to saythis will continue to betrue forthe next ten years.
Aggressive Improvement of the PublicHealth Care System Must be Pursued
Those working within the public healthsystem, and those assisting, must makeincreased efforts to develop even morerapidly Cambodia’s new public healthsystem. Open, publicized hours need tobe maintained, courteous and qualitytreatment needs to be provided,commodities need to be on hand, andcosts need to be clearly advertised.Underpaid staff will remain a problem,but until that situation changessignificantly, greater collective effort hasto be made to make the new system workbetter, or hoped for improvements willnot occur.
seeking care from another more qualified, health provider (health center and referralhospital). Kru Khmer are commonly believed to be most effective in treating specificproblems, such as thrush and convulsions.Because the Kru Khmer are readily accessible tovillagers, and share the cultural beliefs of ruralpeople, they play a central role in currentpatterns of care-seeking. Therefore, the KruKhmer should be taken into consideration whendefining any health intervention. Most of thechildren die in their community and have nocontact with the public health sector until thelast stage of the illness.Self-medication and visiting the drug seller are
very common, especially at the beginning of the illness,as observed in other studies. The prescription of themedication is done according to the caretaker’sdescription of the illness, most commonly for symptoms like fever, diarrhea and respiratoryproblems. In most cases, it was not possible to assess the quality of the prescription, but insome cases, a harmful and prolonged treatment was prescribed, which also delayed seekingcare from other providers.
4. Public health providers are underutilized and their care is only sought afterthe infant or child’s illness reaches a severe stage.
The average duration of acuteillnesses was 10 days. Care was sought aftertwo days, following a slightly differentpattern than has been encountered in otherstudies, where the overall duration of illnessthat led to death was shorter. As mentionedabove, the Kru Khmer was the first and mostcommonly visited provider, followed by thedrug seller, the private provider and lessfrequently to the public health provider. Themost common reasons mentioned by thecaretaker for not going to the public healthprovider were the lack of money, and theperception that the service is expensive.Distance and difficulty of transportation, anda poor perception of the quality of servicewere also mentioned. It seems that thepublic health provider is visited only whenthe child’s illness is severe, and after thechild has been seen by other providers.
5. Caretakers are giving, and providers areprescribing, inappropriate treatmentfor diarrhea that leads to the death ofinfants and children.
Home treatment has been well defined and established for diarrhea, and is one of thekey actions that can lead to survival. Of all children with diarrhea, only one-third received morefluids during the episode at home. Less than half received the same amount as usual and a

49
ORS, An Inexpensive Solution
Children of all ages die fromdiarrhea. There are some solutionsthat are relatively easy; exclusivebreastfeeding is one and ORS isanother. Oral rehydration therapyshould be a well understood treatmentat all public and private providersites, in every home, and beingpromoted by all those working toimprove child health.
ANC/TT/Anemia Prevention
Until adequate transport and availableservices, health program efforts willstill have to rely upon promoting earlyand regular ANC visits, andincreasing tetanus toxoid coverageamong all pregnant women
quarter received less than usual. Drug sellers and private providers often prescribed some typesof medicine that are considered to be harmful or not useful for the child. ORS was onlyprescribed in a minimum number of cases
6. Available ANC services are insufficientto meet current needs.
About two-thirds of thewomen in this study received sometype of ANC during pregnancy, aslightly lower proportion thenreported in the NHS. The mostcommonly visited providers were thepublic health center and the TBA, andthe average month of pregnancy forthe first ANC visit was four months.The average frequency of two visitsduring pregnancy is considered asinappropriate according to nationalguidelines. If we consider national and WHO guidelines for ANC, the TBA,Kru Khmer and drug seller would not be considered as capable of providingquality ANC. This would lower the percentage of women with proper ANC inthis study to close to 40 percent. One of the indicators of quality was thecoverage of tetanus vaccine during pregnancy, which was only 15 percent, apercentage that is similar to the one found by the NHS.
ANC has been identified as an intervention that can reduce perinatalmortality, especially when a properreferral system and referral hospitalis available. In addition to routinetetanus vaccination and ironsupplementation, the identificationof risk factors for perinatal death, aswell as maternal death, has been thetraditional approach used in safemotherhood programs. Thisapproach however, has come undercriticism because of its allegedfailure to reduce maternal mortality rates. According to Maine and Rosenfield“the best strategy is to assume that all pregnant women are at risk for seriouscomplications and to focus efforts on improving the quality of, access to, andutilization of emergency obstetric care services.”∗ The provision of EOCservices assumes that a fully operational health facility with sufficient medicalstaff and equipment is available, as well as transport that can be used to bringthe pregnant women to the facility. This, of course, is not the case in Cambodia.Until these conditions can be met, i.e. adequate transport and available service,
∗ D. Maine and A. Rosenfield “The Safe Motherhood Inintiative: Why Has It Stalled?”, ‘AmericanJournal of Public Health, April 1999, Vol. 89, No. 4

50
Trained Assistance andClean Births
Trained providers, includingTBAs, that ensure clean andsafer births are a must forboth child and maternalhealth. Home birth kitsprovide one simple,inexpensive, intervention.
Credit for HealthIf rural Cambodians are going toaccess public health services in aserious way over the next decade,supportive credit systems at thehealth center and hospital levelneed to be developed.
health program efforts will still have to rely upon promoting early and regularANC visits, increasing tetanus toxoid coverage, and reducing anemia among allpregnant women.
7. Despite the presence of danger signs, pregnant women do not recognize theseverity of the signs and prefer to deliver their babies at home.
Most of the women in the study planned and preferred delivering theirbaby at home, despite the presence of danger signs or problems duringpregnancy and/or delivery. Mothers during pregnancy and labor/delivery didn’trecognize the severity of the symptoms. Thisis especially evident during pregnancy, wheremothers on average sought outside care afterhaving identified the presence of a dangersign for six days, and only went to a medicalprovider after thirteen days. Most babieswere delivered by the TBA, and 20 percent ofthe women experiencing perinatal deathsdelivered the baby without any assistance.
There is a definitive need to improvedelivery conditions at medical facilities aswell as to change the practice of delivering athome, especially when the pregnancies, labor and deliveries are of high risk.Since it is not feasible at present that all babies can be delivered at a medicalfacility, only those at risk should be identified and referred, leaving the“normal” deliveries to be assisted by a trained provider at home. Specialemphasis should be given to the hygienic conditions around birth, the propermanagement of the umbilicus cord, and proper care of the newborn infant.Home birth kits can play a major role in this activity. Breastfeeding practicesshould be encouraged, especially the immediate onset of breastfeeding, givingcolostrum to the baby, and exclusive breastfeeding for the first six months.
8. Credit is an established way of life for rural Cambodians, but credit is onlyavailable for health care in the private sector.
When caretakers were asked why they tooktheir children to the Kru Khmer, a frequentanswer was that that the Kru Khmer was willingto provide services on credit. It is well knownthat rural Cambodians routinely rely on credit. Itis a long recognized practice for agriculture and afew micro lending programs have been initiatedto assist the rural population to obtain farm creditat fair and affordable rates. In health it is wellknown that a family illness can cost a family a cow or ox and quite possibly itsmain work animal, often pushing the family further into debt. Currently, there arenot major efforts being implemented to offer credit for health care in ruralCambodia.

51
The recommendations based upon this study are straightforward.To have serious impact upon infant and child mortality, it will be necessaryto address all of the issues discussed above.
Attachments

52

53

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -1-
Attachment Two
Sample Size Determination
Sample size determination was originally based on the first study objective "to determine the main causesof deaths among infants and children". Assuming the "worst case" for the proportion of deaths due toacute ARI of 50 percent, the sample size calculation to determine a single proportion was as follows:
n = z2 (p)(q) d2
To establish the proportion (p) with 95 percent confidence and a level of precision of 0.05 implies thatd=0.05 and z=1.96. Since q = 1-p,
n = 1.962 (0.5)(0.5) 0.052
Therefore a sample size of 385 deaths would be required to determine the proportion of deaths due to ARIfor a simple random sample. In view of the need to sample villages, or "clusters", a design effect of 0.15was assumed, resulting in an increase of the necessary sample size to 443. Assuming a child mortality rateof 181 per 1000 live births, and that 19 percent of the population was under five years of age, there wouldhave been an estimated 43,120 deaths in one year among the 238,236 children under five. To obtain therequired sample of 443 deaths, all of the deaths among children under five had to be detected from asurveillance population of 12,882 persons or one percent of the total of the four provinces.
Some changes in methods
Information gathered during the study indicated that the sampling frame may have been incomplete.Using the original sampling frame, the study would have expected to find far more deaths than it actuallydid (443 expected versus 144). Here, a new sample size was calculated using more updated data.
According to the National Health Survey of 1998 conducted by the National Institute of Public Health, thetwo-week prevalence of ARI is 20 percent. Therefore, the "worst case " for the proportion of deaths due tois 20%. The sample size calculation to determine a single proportion is as follows:
n = z2 (p)(q) d2
To establish the proportion (p) with 95% confidence and a level of precision of 0.05 implies that d = 0.05and z = 1.96. Since q = 1-p,
n = 1.962 (0.2)(0.8) 0.052
Therefore, a sample size of 246 deaths would be required to determine the proportion of deaths due to ARIfor a simple random sample. In view of the need to sample villages or "cluster", a design effect of 0.15was assumed, resulting in an increase of the necessary sample size to 283.

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -2-
The recalculated sample size is much closer to the actual number of deaths recorded. The fact that thenumber of deaths recorded is still under the number required for the study might be explained by incorrectpopulation data used at the outset. It is very possible that many individuals have left the target villagessince the UNTAC estimates were made. This would account for the fewer number of deaths reported bythe village monitors.

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -3-
Attachment Three
List of Villages Selected for Death Surveillance
District Khum VillageSiem Reap Province
Kralanh
Angkor ChumPuok
Kroch KorTa AnKoulPrey Chruk
ReulTa AnPrey AarPhlang
PuokAngkor ThumSiem Reap
KhnatKhnar SandaySvay DangKumChreav
Boeng KhnaarBanteay SreySala KansaengTa Chek
Siem Reap
Soutr Nikum
AmpilMean CheyDam DekTa Yek
Thnai BakBanteay RuesseiTrabaekBoeung Ngot
Soutr NikumChi Kreng
Kien SangkeChi KrengKouk Thlok LeuRoessei Lok
Chrey Khang CheungBengKouk ThlokToteung Thngai
Pursat ProvinceBakan Boeung Khnar
Me ToekSnam PreahTrapeang Chorng
Prey PdaoTrangThnuoh Ta ChabKaoh Kaev
Sampov MeasPhnum Kravanh
Phteah PreyLeachSamraong
Chamkar Chek TbongTa NukSamraong Pir
KandiengKrakor
Sre SdokAnsa ChambakO Sandan
Banteay TraokKhsach L'etO Ach Kok
Kampot ProvinceAngkor Chey
Banteay Meas
Kampong Trach
Angk Phnum TochPhnum KongSamraong LeuWat Angk khang CheungKT Kang Lech
Paeng ThumTrapaeng KhlaTram SasarSou PengO Chranieng
ChhukChum kiriDang TongKampot(DC)
LbaeukSre knongAngk Ro MeasChum KrielStung Keo
Trapang kokirPrey YavAntong BaekTrapeang ThumKampong Chen
Stung TrengSeesan Kbal Romeas Krabei Chrum

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -4-
Siem PangStung TrengThala Borivat
Prek MeasStung TrengKaoh Sneng
Kham PhoukPhum Spien ThmorKaoh Snaeng

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -5-

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -6-
Attachment Four
List of Staff
The Pathway Working Group
Name Position InstitutionDr. Khdan YuvuthaDr. Auy EamDr. Sam SophanDr. Chea SokvengDr. Srey SokhonDr. Duch MonibothDr. Min TaingsoeunDr. Reth ChanDr. Chhorn Veasna
Dr. Ou KevannaDr. Bun ChanthornDr. Keo SonyDr. Ly VanthyDr. Renata SchumacherMr. Jim EberleDr. Sin SomunyDr. Houy SikhengDr. Kong KannithaMs. Cheang Kannitha (M.A )Ms. Im Phallay
Chief of Technical BureauPediatricianPediatricianPediatricianPediatricianPediatricianPediatricianPediatricianCDD, ARI, Cholera NationalProgram ManagerARI National Program OfficerCDD National Program OfficerPhysicianCBCSP ManagerConsultant to RACHAResearch AdvisorResearch ManagerResearch AssistantResearch AssistantResearch AssistantResearch Assistant
NPHNPHNPHNPHNPHNPHNPHNPHNMCHC
NMCHCNMCHCNMCHCWI-CN/ARACHARACHARACHARACHARACHARACHA
Village Monitor Supervisors
Kampot Pursat Siem Reap Stung Treng
Mr. Hun VunthayMr. Morm Simorn
Mr. Chim keahingMr. Eng Taing OrMr. Sou Penh
Mr. Seun MaoMr. Bouy SothearaMr. Sours BorinMr. Heng Sam Reth
Mr. Eam Lorm

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -7-
Village Monitors
Kampot Siem Reap Pursat Stung Treng
Ms. Muy khunaMs. Chan VunthyMs. Kim LyMs. Som LeanMs. Keut SaromMs. Hun ChantyMs. Mom SaryMs. Pak Kim AunMs. Sey SinaMs. Yim SunlyMs. Norng KangMs. Phou SimengMs. Prak SothyMs. San SilaMs. Long RathaMs. Sveth SokhalMs. Luy KimsearMs. Ou Sam AnMs. Pich ChanAunMs. Hang Sareun
Ms. Sun KimheangMs. Sath ReukMs. Khaun PheanMs. Chhurn RournMs. Loth SavuthMs. Smean EamMs. Loeun RunMs. Pheav SophalMs. Uy LabMs. Touch PhallyMs. Mao KimlyMs. Chhor SenglyMs. Chhourn SaromMs. Vun NaryMs. Pul PoaMs. Tun SothenMs. Nok OusMs. San SinathMs. Morm SavoeunMs. Horm SiengmayMs. Van KhunMs. Tab LemMs. Bun HeanMs. Ou KimchheanMs. Chea PhallyMs. Pen VannaMs. Em SamdeyMs. Sear HeangMs. Seng SovyMs. Kheus Soryun
Ms. Sin KongMs. Khun YornMs. Hin NyMs. Bun ThaMs. Chum SemMs. Chab ChanthournMs. Sak SithaMs. Pen KoeunMs. Nourn TyMs. Seang SokuntheaMs. Lach PaoMs. Bo DinaMs. Pho SopheanMs. Lamm ChrebMs. Lanh SothearyMs. Khut PaoMs. Sin SophalMs. Thea Kitleang
Ms. BourSamphosMs. Tay SophalMs. Pau VicheraMs. Na OssaMr. Phay OlaMs. Sou DanyMs. Heng Mom

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -8-
Provincial Mangement Committee
Name Position Province
Dr. Dy BunchemMr. Pao Hun (MA)Dr. Ney PorlenDr. Chim SopharoMr. Ith Sakhoeun(MA)Mr. Yorng Lorn (MA)Mr. Sor Sothy (MA)
Director of Provincial Health DepartmentDirector of Provincial Maternal and Child HealthDirector of Soutr Nikum Operational DistrictRACHA Provincial CoordinatorDirector of Siem Reap Operational DistrictDirector of Kralanh Operational District Staff of Technical Office
SIEM REAP
Mr. Khlim Sokun MA)Dr. Seang NormMs. Pal La In (MA)Dr. Cheng LibuntyDr. Nou SovannDr. Mao SovannaMr. Chey Ang
Director of Provincial Health DepartmentChief of Technical OfficeDirector of Maternal and Child Health OfficeDeputy Director of Maternal and Child Health OfficeRACHA Provincial CoordinatorDeputy Director of Sampov Meas Operational DistrictDeputy Director of Bakan Operational District
PURSAT
Dr. Lim Kaing EangDr. Sol SovathMr. Sun Po (MA)Dr. Soun BopheaDr. Phat VisalMr. Sao Ngat (MA)Mr. Phy Maly (MA)Mr. Heng Pheng MA)
Director of Provincial Health DepartmentDirector of Provincial Maternal and Child HealthDeputy Director of Provincial Maternal and ChildHealthRACHA Provincial CoordinatorDeputy Director of Chhuk Operational DistrictDeputy Director of Kampot Operational DistrictDeputy Director of Angkor Chey Operational DistrictDeputy Director of Kampong Trach Operational District
KAMPOT
Dr. Heng NgeuMs. Bour Vatha(MA)Dr. Tann Theng HorMs. Soeur Kea EngMs. Sann Channy
Director of Provincial Health DepartmentDeputy Director of Provincial Health DepartmentDirector of Stung Treng Referral HospitalDirector of Provincial Maternal and Child HealthDeputy Director of Provincial Maternal and ChildHealth
STUNGTRENG

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -9-
Community Advisory Council
Name Position Province
*Siem Reap ODMr. Mork KrapumMr. Eng Kim SannMr. Hourt HayMr. Kdeb SunMr. Meas TannMr. Teav TavMr. Chea PhatMr. Bouy SothearaMr. Kong SomMr. Nop TanMr. Bou UchMr. Tep BunChhayMr. Phum SoMr. Soeum SemMr. Thap SarornMr. Thip VeungMr. Leuk SarunMr. Lim BunloyMr. Paht PunMr. Uch Vann TholMs. Eang SomalayMr. San Ren
*Soutr Nikum ODMr. Un SengMr. Yin SorngMr. Heng LathMr. Soun HounMr. Sear SannMr. Sim SomMr. Koun KourMr. Mom Sam OrnMr. Lach LornMr. Sous MaoMr. Kao SophornMr. LipThanMs. Loeu ChindaMr. Mao SathMr. Mao SearMr. Maung ThoMr. Un Chhut
Puok Deputy District GovernorDeputy Director of Siem Reap Operational DistrictBoeung Khnar Commune SecretaryBoeung Khnar Village ChiefChreav Commune ChiefTa Chek Village ChiefDirector of Banteay Srey Health CenterInvestigator SupervisorMean Chey Commune ChiefAmpil Commune ChiefThnal Baek Village ChiefSiem Reap Deputy District GovernorSvay Dangkum Commune ChiefSala Kansaeng Village ChiefBanteay Srei Deputy District GovernorKhnar Sanday Commune ChiefBanteay Srei Village ChiefBanteay Srei Village SecretaryDeputy director of Siem Reap Operational DistrictPrasat Bakong District GovernorMean Chey Health Center StaffBanteay Ruessei Village Chief
Soutr Nikum Deputy District GovernorDeputy Director of Soutr Nikum Operational DistrictDam Dek Commune ChiefTrabaek Village ChiefTa Yek Commune ChiefBoeung Ngot Village ChiefKien Sangke Commune SecretaryChrey Khang Cheung Village ChiefKouk Thlok Leu Commune ChiefKouk Thlok Village ChiefChi Kreng Deputy District GovernorPeng Village ChiefChi Kreng Commune ChiefRuessei Lok Commune ChiefToteung thngai Village ChiefGroup Chief of Toteung Thngai VillageGroup Chief of Toteung Thngai Village
SIEMREAP

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -10-
Mr. Heng SamrethMr. Sous Borin
*Kralanh ODMs. Kim SophannMr. Uk KimsoeurMr. Naung HulMr. Leav SearMs. Poeung HearthMr. Neth SamnangMr. Kroeung SearthMr. Ream PhavMr. Roath ChumMr. Seun MaoMr. Tuy SothyMr. Lock PaoMs. Chhoun SopheapMr. Rom ChhoeurMr. Chhoun HathMr. Lath Phorn
Investigator SupervisorInvestigator Supervisor
Kralanh Deputy District GovernorDeputy Director of Kralanh Operational DistrictKoul Commune ChiefPrey Ar Deputy Village ChiefRepresentative of Kva VillageTa An Commune ChiefTa An Village ChiefTa An Deputy Village ChiefAngkor Chum Deputy District GovernorInvestigator SupervisorPrey Chruk Commune ClerkPhlang Village ChiefRepresentative of Women in Phlang VillageKroch Kor Commune SecretaryReul Village ChiefRepresentative of Reul Village
*Bakan ODMr. Long VeyMr. Sim SaminMr. Boeung BenMr. Ouch KhoeunMr. Chhim Kea HingMr. Um SithaMr. Mao TyMr. Chhim SophinMr. Prack KhimMr. Sock Moeun
*Sampov Meas ODMr. Seng ChhornMr. Kim Bun SambathMr. Sin SeuMr. Duch SaromMr. Hock ThornMr. Chhim HeanMr. Lach RornMr. Chum PhornMr. Eng Tain OrMr. Nhek LunMr. Chhim SarethMr. Ung NorinMr. Lanh SitholMr. Hem Choy
Me Tek Commune ChiefTrapang Chorng Commune ChiefBoeung Khnar Commune ChiefSnam Preah Commune First SecretaryInvestigator SupervisorBakan Deputy District GovernorTrang Village ChiefKaoh Keo Village ChiefPrey Pdao Village ChiefThnuoh Ta Chab Village Chief
Srae Sdok Commune ChiefO Sandan Commune ChiefO Ach Kok Village ChiefKhsach L'et Village ChiefSampov Meas Deputy District GovernorChamkar Chek Tbong Village ChiefTa Nuk Village ChiefSamraong Pir Village ChiefInvestigator SupervisorKandieng Deputy District GovernorBanteay Trok Village ChiefRepresentative of Krakor District GovernorAnsar Chambak Commune First SecretaryRepresentative of Kravanh District Governor
PURSAT

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -11-
Mr. Pil MubMr. Sou RethMr. Hul NoeurnMr. Sou Penh
Phteah Prey Commune First SecretaryLeach Village ChiefSamraong Commune ChiefInvestigator Supervisor
*Kampong Trach ODMr. Yim SavuthMr. Morm SimornMr. Yin NothMr. Phu Ouch
*Chhuk ODMr. Khem PannMr. Tith RenMr. Um NornMr. Nup KongMr. Maung ChhuthMr. Tith DoeunMr. Hun MonMr. Svay DenMr. Vann SinMr. Hun Vunthay
*Angkor Chey ODMr. Un ThoeurnMr. Pheng KimnyMr. Hun MannMr. Chhim VornMr. Khoun KimsengMr. Prum RunMr. Mok TorkMr. Long SarethMr. Pain PhengMr. Morm Simorn
*Kampot ODMr. Hay SengMr. Khang SeanMr. Hun VunthayMs. Meng SokeaMr. Em PhangMr. Prak Pel
Kampong Trach Khang Lech Commune ChiefInvestigator SupervisorRepresentative of Kampong Trach DistrictO Chranieng Village Chief
Dang Tong District GovernorAng Romeas Commune ChiefLbaeuk Commune ChiefSre Khnong Commune ChiefChhuk District GovernorChum Kiri District GovernorAntong Baek Village ChiefTrapang Kokir Village ChiefPrey Yav Village ChiefInvestigator Supervisor
Phnom Kong Commune ChiefAngk Phnom Toch Commune ChiefSamraong Leu Commune ChiefWat Angk Khang Cheung Commune ChiefAngkor Chey District GovernorTrapang Kva Village ChiefPeng Thum Village ChiefTram Sasor Village ChiefSou Peng Village ChiefInvestigator Supervisor
Chum Kriel Commune ChiefStung Keo Commune Second SecretaryInvestigator SupervisorDirector of Kampot District DepartmentChum Kriel Village ChiefKampong Chen Village Chief
KAMPOT
*Stung Treng ODMr. Houn VeyMr. Chea VannMr Tuy Hearn
Stung Treng Deputy District GovernorStung Treng Commune ChiefSpien Thmor Village Chief
STUNGTRENG

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -12-
Mr. Mao PannMr. Doung LeanMr. Nho PhorngMr. Bou KeosovannMr. Ky NouMr. Phen PhinMr. South SovannMr. Keo MornMr. Eam Lom
Thala Borivath Deputy District GovernorKaoh Snaeng Commune ChiefKaoh Snaeng Village ChiefSesan Deputy District GovernorKbal Romeas Commune ChiefKrabei Chrum Village ChiefSiem Pang Deputy District GovernorKham Pouk Village ChiefInvestigator Supervisor

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -13-

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -14-
Attachment Five
Diagnosis Determination ofCauses of Infant and Child Deaths
Diagnosis Determination of Causes of Infant and Child Deaths
The diagnosis of causes of infant and child deaths were determined by the Pathway Working Group (PWG) inconsultation with RACHA. Where possible, the diagnosis was determined based on standard algorithms developedby PWG and RACHA. In the cases where the observed symptoms did not easily lead to a diagnosis, the PWG andRACHA relied on information available in the open history and the pathway forms to determine the diagnosis. Thefollowing is the table of the algorithms on which the PWG based their judgments when possible.
Algorithms
Probable Diagnosis Diagnostic Criteria
Severe Pneumonia
Cough + fast breathing ORCough + chest indrawing ORDifficult breathing + fast breathing ORDifficult breathing + chest indrawing
Acute DiarrheaFrequent liquid, watery, loose stools atleast 3 times a day AND less than 14 daysof duration AND no blood in the stools.
Acute Dysentory Frequent liquid, watery, loose stools ANDwith blood in the stools.
Persistant DiarrheaFrequent liquid, watery, loose stools AND14 days or more AND no blood in thestools.
MeaslesAt least four months old AND fever ANDgeneralized rash for 3 days or more (rashlooks like tiger skin)
Severe MalnutritionVery skinny OR oedema of the extremities.Possibly apethetic AND/OR sparce reddishhair

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -15-
Meningitis
Neonatal : Fever with bulging fontanelleAND (convulsions ORunresponsive/unconscious)Post-neonatal : Fever AND (stiff neck ORbulging fontanelle) AND (unresponsive/unconscious OR stoppedbeing able to grasp OR stopped being ableto follow movement with the eyes ORstopped being able to respond to voice (allfor more than 12 hours))
Bacteremia/Septicemia
Neonatal :(Water broke for more than 12hours before labour OR had redness ordrainage of the umbilicus cord stump ORhad a skin rash with bumps containing pus)AND fever AND no other cause of death(pneumonia or meningitis)Post-neonatal : Fever AND (one or moreof the following signs: unconscious ORstopped being able to grasp OR stoppedbeing able to respond to voice OR stoppedbeing able to follow the movements withher/his eyes) AND no other causes ofdeath.
Dengue Hemorrhage Fever
(Fever AND somnolence AND hemorrhagein any natural orifice) OR(Fever AND somnolence AND hemorrhageinto the skin)
MalariaFever with no other causes found ANDunconscious AND (living in malaria riskarea OR had been to a malaria risk area)
Birth Asphyxia
Neonatal who was not able to breathe afterbirth AND had no fever AND (hadconvulsions/spasms OR not able to sucklein a normal way after birth OR not able tocry after birth).
Neonatal Tetanus
Neonatal who was able to suckle and crynormally at birth and stopped suckling orcrying at more than two days of age AND(had either spasms OR constrictionprovoked by touching, noise or light.(thisdiagnosis should not be made in presenceof birth trauma)).
Eclampsia
(High blood pressure during pregnancy ORhigh blood pressure during delivery) AND(convulsions OR hand and facial swellingOR oliguria)

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -16-
Attachment Six
Data Collection Instruments

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -17-
DEATH INVESTIGATION QUESTIONNAIRE(For death among infants and children one week to 59 month of age)
Section 1: Identifying Data
Interviewer _______________________________ Support Teammember____________________________
1. Date of interview_________________________ Date checked by supervisor________________________
2. Language of the interview__________________ Date entered to the computer_______________________
3. Province________________________________ 4. District______________________________________
Khum____________________________________ 5.Village_______________________________________
5.1 Estimated distance to health center_______________/motobike __________km
5.2 Estimated time to hospital_____________________/ motobike __________km
Name of the child___________________________ 6. Sex of the child Male......1 Female......2
Name of the mother_________________________ 7. Date of registration(from register)_________________
8. Age at registration(from register)____________ 9. Year of birth (from register)______________________
10. Month of birth(from register)_______________ 11. Day of birth(from register)______________________
12. Date of death (from register)______________ 13. Age of the child at the time of death_______________
Informed consent
By signing here, the Village Monitor indicates that she has seen the informant express agreement toparticipate. The Investigator/ Supervisor explained the five essential facts about participation: 1) What youwill do; 2) How long it will take 3) The purpose; 4) Freedom to choose; and 5) Use of the information.
Village Monitor’s Signature:______________________________________________________________
Attachment Page21

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -18-
Section 2: Informant Information
What is your name?_____________________________________________________________________
14. What was your relationship to (Child’s name)? Mother ...............................................................1Father ................................................................ 2Grandmother ......................................................3Grandfather ........................................................4Other family members .......................................5Other (specify)_____________ .............................8Don’t know .........................................................9
15. Who was _____’s usual caretaker? Mother ...............................................................1Father ................................................................ 2
Grandmother ......................................................3Grandfather ........................................................4Other family members .......................................5Other (specify)_____________ .............................8
16. Do you know the child’s age at the time of death? Yes ...............................1No ................................2
(if “No”, go to 17)If “Yes”, ask How old was the child?
16.1 Age in completed days (if less than 28 days) ...............................................___________days
16.2 Age in completed month (if 28 days or more )............................___________day/month
Verify that the age recorded from the Village Monitor’s registration form is the same that the one mentioned bythe respondent. If they are different try to clarify the age of the child when he/she died. Use the local eventcalender.

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -19-
DECISION BOX
Age of the child at the time of death:
8 DAYS UP TO 59 MONTHS: Continue with the interview.
7 OR LESS DAYS: stop the interview now and begin a new interview with the DeathInvestigation Questionnaire for Death among Infants less than one week of age.
MORE THAN 59 MONTHS: If the child is more than 59 months old, finish with theinterview now, thank the respondent for her/his time and give this questionnaire to the studycoordinator.
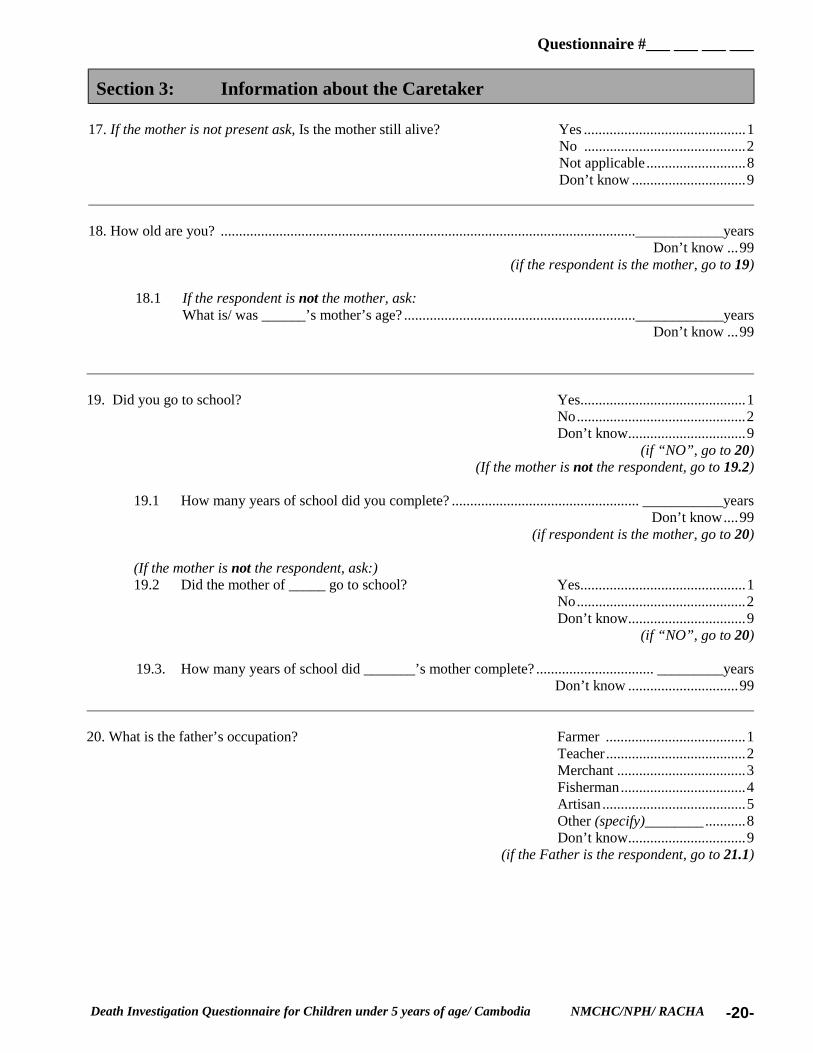
Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -20-
Section 3: Information about the Caretaker
17. If the mother is not present ask, Is the mother still alive? Yes ............................................1No ............................................2Not applicable ...........................8Don’t know ...............................9
18. How old are you? .................................................................................................................____________yearsDon’t know ...99
(if the respondent is the mother, go to 19)
18.1 If the respondent is not the mother, ask:What is/ was ______’s mother’s age? ...............................................................____________years
Don’t know ...99
19. Did you go to school? Yes.............................................1No..............................................2Don’t know................................9
(if “NO”, go to 20)(If the mother is not the respondent, go to 19.2)
19.1 How many years of school did you complete? ................................................... ___________yearsDon’t know....99
(if respondent is the mother, go to 20)
(If the mother is not the respondent, ask:)19.2 Did the mother of _____ go to school? Yes.............................................1
No..............................................2Don’t know................................9
(if “NO”, go to 20)
19.3. How many years of school did _______’s mother complete? ................................ _________yearsDon’t know ..............................99
20. What is the father’s occupation? Farmer ......................................1Teacher......................................2Merchant ...................................3Fisherman..................................4Artisan .......................................5Other (specify)________ ...........8Don’t know................................9
(if the Father is the respondent, go to 21.1)

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -21-
21. What is your occupation? Farmer .......................................1Housewife .................................2Merchant ...................................3Fisherman..................................4Artisan .......................................5Other (specify)____________ ...8Don’t know................................9
(if the respondent is the mother, go to 22)
(If the mother is not the respondent, ask:)21.1 What is/was the mother’s occupation? Farmer .......................................1
Housewife .................................2Merchant ...................................3Fisherman..................................4Artisan .......................................5Other (specify)____________ ...8Don’t know................................9
22. Do you own, at home... Yes (1) No (2) Don’t know(9)
22.1 a Boat? 1 2 9
22.2 an Ox Card? 1 2 9
22.3 cattle? 1 2 9
22.4 a bicycle? 1 2 9
22.5 a motorcycle? 1 2 9
22.6 any other transportation?(Specify)____________________
1 2 9
(If the respondent is the mother, go to 23)
If the respondent is NOT the mother, ask:
At the mother’s home, do they have... Yes (1) No (2) Don’t know(9)
22.7 a Boat? 1 2 9
22.8 an Ox Card? 1 2 9
22.9 cattle? 1 2 9
22.10 a bicycle? 1 2 9
22.11 a motorcycle? 1 2 9
22.12 any other transportation?(Specify)___________________
1 2 9

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -22-
23. What is the roof of the house that the mother lives(d) made of? Thatches .................................................1Metal ......................................................2Tiles........................................................3Wood......................................................4Other (specify)_________________......8Don’t know ............................................9
24. What is the wall of the house that the mother lives(d) made of? Thatches .................................................1Metal ......................................................2Tiles........................................................3Wood......................................................4Other (specify)_________________......8Don’t know ............................................9
25. What language was spoken most often in the household where_____ lived? Khmer...........................1Lao................................2Thai...............................3Chinese .........................4Cham ............................5Vietnamese ...................6Other___________.......8Don’t know...................9

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -23-
Section 4: Information about the Child
Now I would like to ask you some questions about ________.
26. Where was _______ born? Home......................................................1Health Center .........................................2Private clinic ..........................................3Hospital ..................................................4Other (specify)________........................8Don’t know ............................................9
27. Who delivered the baby? Mother....................................................1TBA........................................................2Midwife..................................................3Doctor ....................................................4Nurse ......................................................5Medical Assistant ...................................6Family member ......................................7Other(specify)______________ .............8Don’t know ............................................9
28. Was the child ever breast-fed? Yes.............................................1No .............................................2Don’t know................................9
(If “No”, go to 29)
28.1 For how many month was the child breastfed? ............................... ________________month/dayDon’t know...................9
28.2 Up to what month of age did you only give breast milk to the child and nothing else?(Ask the mother if she gave the child: water, tea, cowmilk,porriage, __________month/day or any other fluid during these month and since when did she give it) Don’t know...............9
28.3 Did you give the initial breast milk (colostrum) to the baby?(Make sure that the mother did not squeeze it out before breastfeeding) Yes................................1
No ................................2Don’t know...................9
29. During the 30 days before _______’s illness leading to death, was he/ she hospitalized?Yes................................1No ................................2Don’t know...................9
(If “NO”, go to 30)If “YES”, ask:29.1. For what reason was the child hospitalized?__________________________________________
Don’t know .............................99
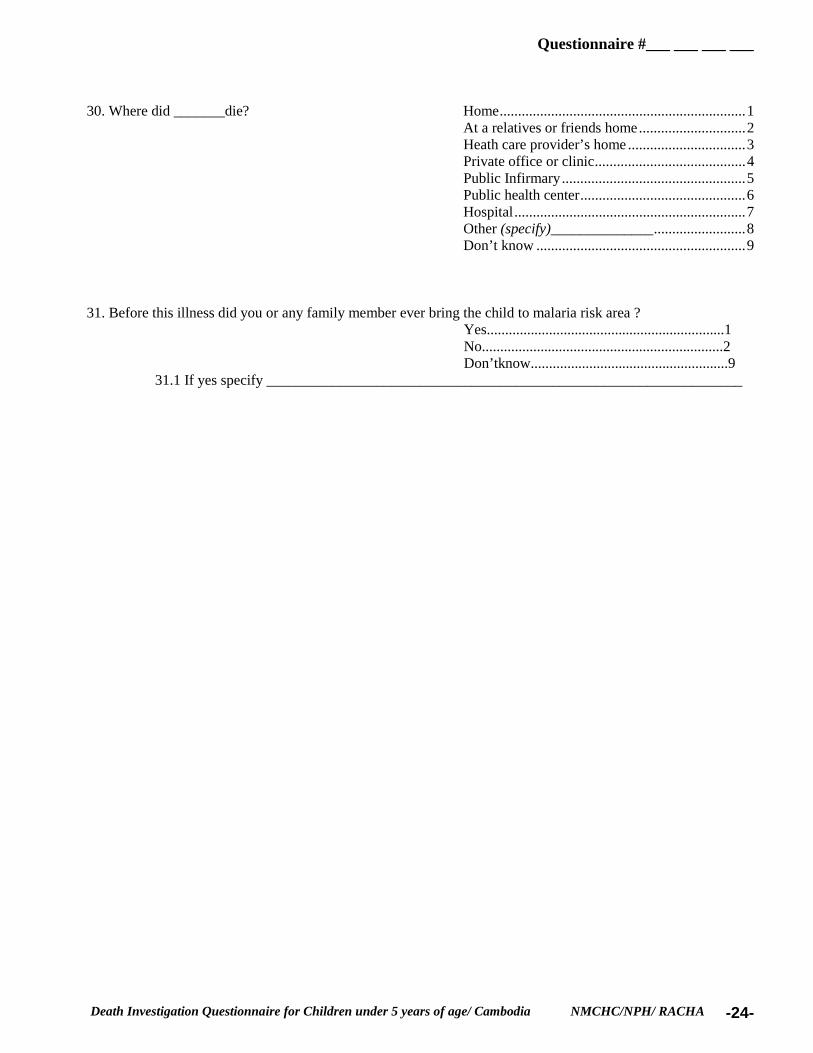
Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -24-
30. Where did _______die? Home...................................................................1At a relatives or friends home.............................2Heath care provider’s home ................................3Private office or clinic.........................................4Public Infirmary..................................................5Public health center.............................................6Hospital...............................................................7Other (specify)______________.........................8Don’t know .........................................................9
31. Before this illness did you or any family member ever bring the child to malaria risk area ?Yes.................................................................1No..................................................................2Don’tknow......................................................9
31.1 If yes specify _________________________________________________________________

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -25-
Section 5: Open history
“Now I would like to use a tape recorder so that I can understand clearly and remember everything you tell meabout the child’s illness and death. Is this OK with you?”
If the respondent agrees, prepare to tape the open history report. As you listen to the narrativemake note of any symptom of illness the mother mentions during her report and any otherimportant observation you might have. Don’t interrupt her until she finishes. Don’t stop therecording of the tape recorder until you finished the whole open history, which includes thequestion about the cause of death. After you finished with the whole interview and you areback at your working place, rewind the tape and transcribe everything the mother told you inher own and exact words, as well as the question asked by you and her answers.
1. Now I would like you to tell me the whole story of the child’s illness and death. Tell me everything thathappened to the child as the illness developed from the first moment you noticed any symptom, andinclude all the symptoms or problems of her (his) illness and what was done for the child.
Once the mother finished the description of the illness, ask:
2. Is there anything else?
If the respondent has nothing more to add to the description, ask:
3. Tell me, what do you think was the cause of the child’s death?

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -26-
Section 6: Injury
32. Did _______ die from any injury, bite, burn, poisoning or drowning? Yes.....................................1No .....................................2Don’t know........................9
(if “No”, go to section 7)
If “Yes”, ask:32.1 What kind of injury? Motor vehicle accident .............................................1
Fall ............................................................................2Poisoning ..................................................................3Bite or sting by venomous animals?.........................4Burn ..........................................................................5Violence....................................................................6Birth injury ...............................................................7Other(specify)________________ ...........................8Don’t know...............................................................9
32.2 Did (s)he die immediately .................................................1within the first 24 hours ..............................2after the first 24 hours..................................3Don’t know..................................................9
If the answer is number 1, stop the interview right away.
Go to page 7 (Open History) and look up the symptoms mentioned spontaneously by therespondent. Choose the section 7 according to the age of the child at the time of death.Then identify the mentioned symptom listed on page 10 /11 or 12/13 and circle (1) underthe column of question 32.

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -27-
Section 7: If less than 28 days of age at the time of deathCircle all of the problems on the list on this page which were spontaneously reported during the open history.Then, to obtain the prompted report, ask about the presence of each of the other symptoms listed to see if any ofthem occurred during the illness that led to death.
34.Promptedreport
Problem or symptom 33.SpontaneousreportYes(1) Yes
(1)No(2)
Don’tknow
(9)
101. Did the child’s pregnancy endearly?
1 1 2 9
102. At the time of birth, was ____smaller than usual?
1 1 2 9
35. How many days long was theillness that led to the child’s death?
_______hours _______Days Don’t know 99
“You told me that your childpresented..... (list symptoms mentionedin 32 and 33). Is there any othersymptom I did not mention?
103. Did (s)he have anymalformations?
1 1 2 9 36. What was the first symptom thatyou noticed in your child when he/shegot ill? What did you noticed next?How many days after _____(previoussymptom) did you notice it?37 For how long did he/she presentthis symptom?.
Be sure when asking for the following symptoms that they were presentduring the illness that led to death. If you think the respondent does notunderstand a certain symptom, explain it to her/him. Ask:
“During the illness that led to the death of ________, did (s)he... 36. Day ofonset
37. Duration
104.Stop feeding normally? 1 1 2 9 99 99
105. Stop feeding? 1 1 2 9 99 99
106. Stop being able to cry? 1 1 2 9 99 99
107. Convulsions or spasms? 1 1 2 9 99 99
108. Unresponsive/ unconscious? 1 1 2 9 99 99
109. Stop being able to followmovement of the eyes
1 1 2 9 99 99
110. Stop being able to grasp 1 1 2 9 99 99
111. Bulging fontanel 1 1 2 9 99 99
112. Redness or drainage fromumbilicus cord stump ?
1 1 2 9 99 99
113. Skin rash with bumpscontaining pus?
1 1 2 9 99 99
114. Fever? 1 1 2 9 99 99
115. Vomit everything? 1 1 2 9 99 99
116. Yellow skin and eyes? 1 1 2 9 99 99

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -28-
34.Promptedreport
Problem or symptom 33.SpontaneousreportYes(1) Yes
(1)No(2)
Don’tknow
(9)
36. Day ofonset
37. Duration
117. Blood in the stools? 1 1 2 9 99 99
118 . Cough? 1 1 2 9 99 99
119. Difficult breathing 1 1 2 9 99 99
120. Felt very cold? 1 1 2 9 99 99
121.Diarrhea ( watery stool at least 3times/day)(if “Yes”go to Section 8)
1 1 2 9 99 99
122. Watery stool less than 3times/day
1 1 2 9 99 99
123. Other(specify)______________ 1 99 99
124. Other(specify)______________ 1 99 99
125. Other(specify)______________ 1 99 99
126. Other(specify)______________ 1 99 99
If the young infant had “Diarrhea” and/ or “Frequent liquid and watery stools”, go to Section8; if not, continue with Section 9.

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -29-
Section 7: If the child has more than 28 days of age at the time of death.
Circle all of the problems on the list on this page which were spontaneously reported during the open history. Then, toobtain the prompted report, ask about the presence of each of the other symptoms listed to see if any of them occurred duringthe illness that led to death.
35. How many days long was the illness that led tothe child’s death? ................____________________
Don’t know...............99
34.Prompted reportProblem or symptom 33.SpontaneousreportYes(1)
Yes(1)
No(2)
Don’tknow (9)
“You told me that your child presented..... (listsymptoms mentioned in 32 and 33). Is thereany other symptom I did not mention?
36. What was the first symptom that younoticed in your child when he/she got ill?What did you noticed next? How amny daysafter the ______ (previous symptom) did younotice it?
37. For how long did he/she present thissymptom?.
Be sure when asking for the following symptoms that they werepresent during the illness that led to death. If you think therespondent does not understand a certain symptom, explain it toher/him. Ask:“During the illness that led to the death of ________, did (s)he...
36.Day of onset 37. Duration
227.Very skinny? 1 1 2 9 99 99
228.Apethetic 1 1 2 9 99 99
229.Sparce reddish hair 1 1 2 9 99 99
230. Fever 1 1 2 9 99 99
231. Stiff neck 1 1 2 9 99 99
232. Chills 1 1 2 9 99 99
233. Very pale (almostwhite) (pale palms or nails)
1 1 2 9 99 99
234. Cough? 1 1 2 9 99 99
235. Fast breathing? 1 1 2 9 99 99
236. Difficult breathing? 1 1 2 9 99 99
237. Chest indrawing? 1 1 2 9 99 99
238. Swollen legs or feet(both legs)
1 1 2 9 99 99

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -30-
34.Prompted reportProblem or symptom 33.SpontaneousreportYes(1)
Yes(1)
No(2)
Don’tknow (9)
36. Day of onset 37.Duration
239. Bleed from his/her skinor any body opening?
1 1 2 9 99 99
240. Vomit everything? 1 1 2 9 99 99
241. Convulsions? 1 1 2 9 99 99
242. Not responsive,unconscious
1 1 2 9 99 99
243. Larthegic 1 1 2 9 99 99
244. Stop being able tofollow the movement of theeyes
1 1 2 9 99 99
245. Difficulty opening themouth?
1 1 2 9 99 99
246. Stop taking food/feeding?
1 1 2 9 99 99
247.Generalized skin rash ormeasles?
1 1 2 9 99 99
248.flaking skin 1 1 2 9 99 99
249.Localized black scar 1 1 2 9 99 99
250.Bulging fontanelle?(Only if less than 1 year age)
1 1 2 9
NA 8
99 99
251.Visible blood in thestools?
1 1 2 9 99 99
252. Frequent and waterystools?
1 1 2 9 99 99
253.Diarrhoea? 1 1 2 9 99 99
254.Other(specify)________ 1 99 99
255.Other(specify)________ 1 99 99
256.Other(specify)________ 1 99 99
257.Other(specify)________ 1 99 99
If the child had “Diarrhea” and/ or “Frequent liquid and watery stools”, go to Section 8; ifnot, continue with Section 9.

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -31-
Section 8: Diarrhea management
Ask the questions about the diarrhea management at home and by the health provider only if thesymptom “frequent and watery stools” and/or “diarrhea” is “Yes”. If the answer is “No”, go to theSection 9.
“You told me before that your child had diarrhea..
38. Did you do anything at home to treat the diarrhoea? Yes .............................................1 No ............................................2
Don’t know...............................9 (if “No” go to 39)
If “Yes”, ask: 38.1 Can you tell me everything you did at home to treat it? _____________________________________
______________________________________________________________________________________
39. For the diarrhea, did you give the child more fluids than usual?..................................................................1 the same amount of fluids as usual...................................................2 less fluids than usual? ................................................................................3 no fluids at all? .................................................................................4
Don’t know ....................................................................................9
40. For the diarrhea, did you give the child more food than usual? ......................................................................1 the same amount of food as usual? .........................................2 less food than usual?...............................................................3 no food at all? .........................................................................4 Don’t know .............................................................................9
41. Did you seek care for your child because of the diarrhoea? Yes........................................1 No ...................................................2
Don’t know......................................9 (if “No” go to Section 9)
If “Yes”, ask: For all the persons you saw because of the diarrhea of you child , did any of them 41.1 give or prescribe you ORS? Yes.......................................1
No .......................................2Don’t know..........................9
(if “No”, go to 41.3)

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -32-
If “Yes”, ask:41.2 Which ones gave or prescribed you ORS? Kru Khamer...................................................1
Drug seller/pharmacy ................................2Health Center ................................................3Hospital .........................................................4Other (specify)________________ ...............8Don’t know ...................................................9
41.3 Did any of them prescribe you any other fluids? Yes...................................1(Probe: fluids like gava, tea, coconut, rice water, water...) No .......................................2
Don’t know..........................9(if “No”, go to 41.6)
If “Yes”, ask:41.4 Which ones prescribed you other fluids? Kru Khamer...................................................1
Drug seller/pharmacy ................................2Health Center ................................................3Hospital .........................................................4Other (specify)________________ ...............8Don’t know ...................................................9
41.5 Could you tell what fluids were prescribed to you?_________________________________
41.6 Did any of them tell you to boil the water? Yes .........................................1 No .......................................2
Don’t know..........................9(if “No”, go to 41.8)
If “YES”, ask:41.7 Which ones told you to boil the water? Kru Khamer...................................................1
Drug seller/pharmacy ................................2Health Center ................................................3Hospital .........................................................4Other (specify)________________ ...............8Don’t know ...................................................9
41.8 Did any of them give the child any IV fluids? Yes ..........................................1 No .......................................2
Don’t know..........................9(if “No”, go to 41.10)
If “YES”, ask:

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -33-
41.9 Which ones gave the IV fluids? Kru Khamer...................................................1Drug seller/pharmacy ................................2Health Center ................................................3Hospital .........................................................4Other (specify)________________ ...............8Don’t know ...................................................9
41.10 Did any of them prescribe you any tablets, medicine, syrup? Yes ........................................1 No .......................................2
Don’t know..........................9(if “No”, go to Section 9)
If “YES”, ask:41.11 Which ones prescribed the medicine? Kru Khamer...................................................1
Drug seller/pharmacy ................................2Health Center ................................................3Hospital .........................................................4Other (specify)________________ ...............8Don’t know ...................................................9

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -34-
Section 9: Care- Seeking
Could you please tell me for any illness, the time it takesyou to go to your usual
42.1 Time (Don’t know ...99)
42.2. Transportation(Don’t know ...9)
1. Kru Khamer? 99 9
2. Drug seller/pharmacy? 99 9
3. Private clinic or practitioner? 99 9
During the illness that led to the death of your child, could you now please tell me how much money you spent on...
EXPENSES 43. Kru Khamer
Don’t know...9I didn’t go....1
44. Drug Seller
Don’t know...9I didn’t go....1
45. HealthCenter
Don’t know...9I didn’t go....1
46. Hospital
Don’t know...9I didn’t go....1
47. Privateclinic/pract.
Don’t know...9I didn’t go....1
1.Total Consultation cost(includes drugs)
19
19
19
19
19
Only if the TOTAL CONSULTATION COST is not known, circle (9) and ask for consultation cost and drug costseparately. If the Total Consultation cost is known by the respondent, continue with question 2 and 3.
1.1 Consultation costonly
9 9 9 9 9
1.2 Drug cost only 9 9 9 9 9
TOTAL COST
2. Total transportation costfor child’s illness
Did not have any....1Don’t know....9
3.Other expenses Did not have any....1Don’t know...9
Total expense_____________________ (Specify)
Once you finished this section, go to the Pathway form.

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -35-
PATHWAY FORM QUESTIONNAIRE #: ___ ___ ___ DATE: ___/___/___ SURVEYOR ID #: ___ ___NSTRUCTIONS TO SURVEYOR: 1) COMPLETE I.D. .2-4 ASK ABOUT THE ACTIONS TAKEN FOR THE ILLNESS. COMPLETE ONE ROW FOR EACH ACTION. 7) CHECK FOR ERRORS.
“Now I would like to review the things you did at home and outside your home when the child got sick.1. ACTION
“ What was the first thing youdid when you noticed the
child was ill?”(What was the next thing you
did...?)
2 “How manydays had thechild been ill
when you (first)took this action?”
3. Who was the personthat decided to do...(action 1, 2, 3...)Mother (1)Father(2)Grandmother(3)Other(8) Don’t know(9)
4. “ For which symptoms the child had atthat moment did you do/ give ....(action 1,action 2...)?
(Write down the symptoms the motherspontaneously mentions)
FOR ACTIONS TAKENINSIDE or OUTSIDE THE HOME
IF THE CHILD WAS NOT SEEN BY A PUBLIC HEALTHAGENT, ASK:
5. “Why didn’t you go to the public health provider at this time?”
11 2 3 9
8 (specify)__________
21 2 3 98(specify)__________
.31 2 3 98(specify)__________
41 2 3 98(specify)__________
51 2 3 98(specify)__________
61 2 3 98(specify)__________
71 2 3 98(specify)__________
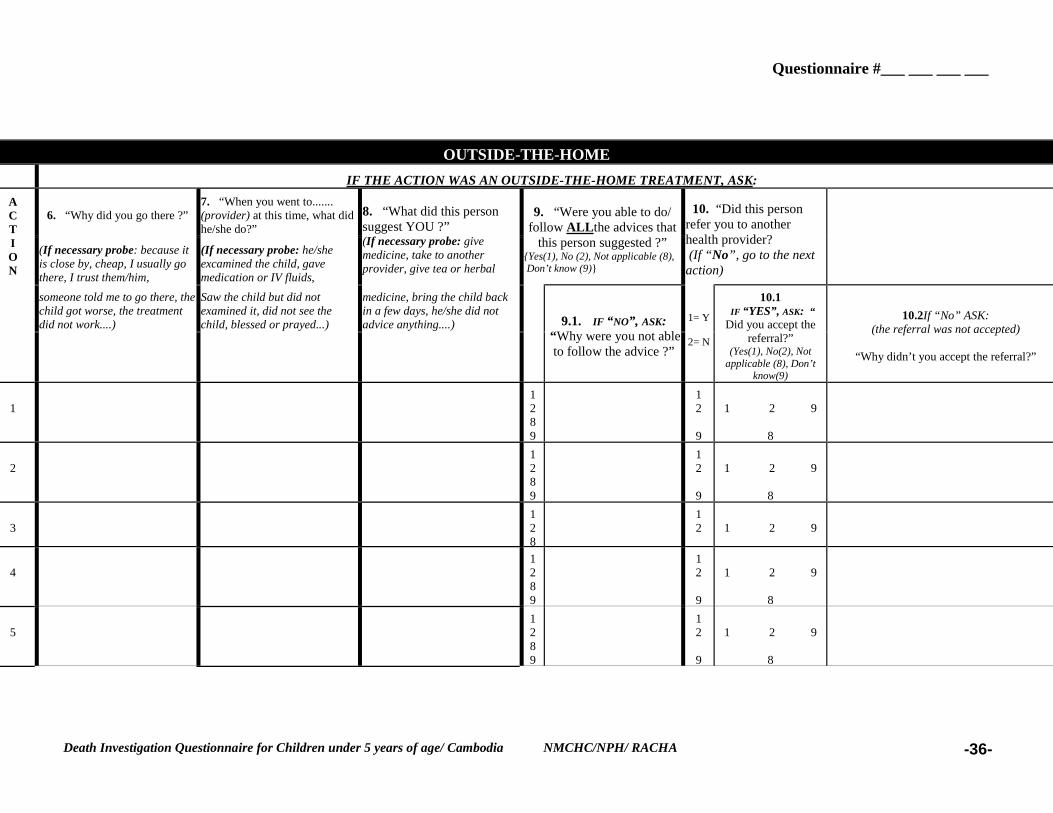
Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -36-
OUTSIDE-THE-HOME IF THE ACTION WAS AN OUTSIDE-THE-HOME TREATMENT, ASK:
6. “Why did you go there ?”7. “When you went to.......(provider) at this time, what didhe/she do?”
(If necessary probe: because itis close by, cheap, I usually gothere, I trust them/him,
(If necessary probe: he/sheexcamined the child, gavemedication or IV fluids,
8. “What did this personsuggest YOU ?”(If necessary probe: givemedicine, take to anotherprovider, give tea or herbal
9. “Were you able to do/follow ALLthe advices that
this person suggested ?”{Yes(1), No (2), Not applicable (8), Don’t know (9)}
10. “Did this personrefer you to anotherhealth provider? (If “No”, go to the nextaction)
someone told me to go there, thechild got worse, the treatmentdid not work....)
Saw the child but did notexamined it, did not see thechild, blessed or prayed...)
medicine, bring the child backin a few days, he/she did notadvice anything....)
ACTION
9.1. IF “NO”, ASK: “Why were you not ableto follow the advice ?”
1= Y
2= N
10.1 IF “YES”, ASK: “Did you accept the
referral?”(Yes(1), No(2), Not
applicable (8), Don’tknow(9)
10.2If “No” ASK:(the referral was not accepted)
“Why didn’t you accept the referral?”
11289
12
9
1 2 9
8
21289
12
9
1 2 9
8
3128
12 1 2 9
41289
12
9
1 2 9
8
51289
12
9
1 2 9
8

Questionnaire #___ ___ ___ ___
Death Investigation Questionnaire for Children under 5 years of age/ Cambodia NMCHC/NPH/ RACHA -37-
61289
12
9
1 2 9
8
71289
12
9
1 2 9
8
81289
12
9
1 2 9
8

Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA -38-
DEATH INVESTIGATION QUESTIONNAIRE(Perinatal death)
Section 1: Identifying Data
Interviewer________________________________ Support Teammember______________________________
1. Date of interview_________________________ Date checked by supervisor__________________________
2. Language of the interview__________________ Date entered to the computer_________________________
3. Province________________________________ 4. District________________________________________
Khum____________________________________ 5.Village______________________________________
___
5.1 Estimated distance to the closest health center_______________/motobike Km
5.2 Estimated distance to the closest hospital / motobike Km
6. Miscarriage Yes........1 No............2 7. Stillbirth Yes.........1 No.........2
8. Child 7 or less days old Yes....1 No....2 Name of the child__________________________________
9. Sex of the child:Male..1 Female..2 Don’t know..9 10. Age of the child at the time of death_________________
Name of the mother_________________________ 11. Date of registration(from register)__________________
12. Age at registration(from register)___________ 13. Year of birth (from register)_______________________
14. Month of birth(from register)______________ 15. Day of birth(from register)_______________________
16. Date of death (from register)______________
16 1. Date of abortion/ stillbirth ( from register)_________________
Informed consent
By signing here, the Village Monitor indicates that she has seen the informant express agreement toparticipate. The Interviewer explained the five essential facts about participation: 1) What you will do; 2)How long it will take 3) The purpose; 4) Freedom to choose and 5) The use of the information.
Village Monitor’s Signature:______________________________________________________________
Attachment Page41

Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA -39-
Section 2: Informant Information
What is your name?_____________________________________________________________________
17. What was your relationship to (The baby)? ........................................................................ Mother 1Father ...................................................................... 2Grandmother ............................................................ 3Grandfather .............................................................. 4Other family members ............................................. 5Other (specify)_____________ ................................... 8Don’t know............................................................... 9
(if the mother is the respondent, go to 18)If the mother is NOT the respondent, ask:17.1 Were you present during delivery? Yes ............................... 1
No ...................................... 2If the mother is NOT present, ask:17.2 Is the mother still alive? Yes ..................................... 1
No ...................................... 2Don’t know ........................ 9
Now I would like to ask you some questions about this pregnancy.
18. How many months long was the duration of the pregnancy? ..................................................____________monthDon’t know ......... 99
Ask ONLY if the mother is the respondent; if NOT, go to 2019. Could you tell the date of your last menstruation before this pregnancy? ................................. ________________
Don’t know ......... 99
20. What was the year of birth (abortion)....................................................................................... _______________
21. What was the month of birth (abortion) ...................................................................................... _______________
21.1 During what phase of the moon was the baby born (the abortion)? Waxing............................... 1Waning............................... 2Don’t know ........................ 9
21.2 On what day of this phase of the moon was the baby born (the abortion)? ................. ______________Don’t know ........... 9
21.3 On what day was the baby born/ abortion/ miscarriage/ stillbirth? .... .............______________Don’t know
............9
22. Was the baby born alive and then died? ................ 1born dead?....................................... 2Don’t know ..................................... 9

Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA -40-
(if “born dead” go to Decision Box)
If “born alive and then died”, ask:22.1 Do you know the child’s age at the time of death? Yes .................................................. 1
No .................................................. 2Don’t know ..................................... 9
(if “No”, go to Decision Box)If “Yes”, ask 22.2 How old was the child? ............................................................................________________days
DECISION BOX
With the above information, decide if the case was a still birth or born alive that died. Mark witha ( X ).
STILL BIRTH: Pregnancy of 6 or more months AND the baby was born dead
BORN ALIVE AND DIED DURING THE FIRST 7 DAYS OF LIFE: Any live birth regardless of the duration of pregnancy, where the baby died duringthe first 7 days of life.
MISCARRIAGE/ABORTION: Pregnancy that ended before the 6th month.If it is a miscarriage/ abortion, stop the interview at this point and give this questionnaire to the studycoordinator.
BORN ALIVE AND DIED AFTER THE FIRST 7 DAYS OF LIFE.
If the age of the child is more than 7 days, stop now the interview and begin a new interview with the DeathInvestigation Questionnaire for Death of Children under 5 years.

Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA ----41414141----
Section 3: Information about the Mother
23. How old are you? .......................................................................................................................____________yearsDon’t know ......... 99
(if the respondent is the mother, go to 24)
23.1 If the respondent is not the mother, ask:What is/ was ______’s mother’s age? .....................................................................____________years
Don’t know ......... 99
24. Did you go to school? Yes................................................... 1No.................................................... 2Don’t know...................................... 9
(if “NO”, and the mother is the respondent, go to 25)
24.1 How many years of school did you complete? ..........................................................___________yearsDon’t know.......... 99
(if respondent is the mother, go to 26)
(If the mother is not the respondent, ask:)24.2 Did the mother of _____ go to school? Yes................................................... 1
No.................................................... 2Don’t know...................................... 9
(if “NO”, go to 25)
24.3. How many years of school did _______’s mother complete? ......................................._________yearsDon’t know.......... 99
25. What is the father’s occupation? Farmer ............................................ 1Teacher............................................ 2Merchant ......................................... 3Fisherman........................................ 4Artisan ............................................. 5Other (specify)________ ................. 8Don’t know...................................... 9
(If the father is the respondent, go to 26.1)
26. What is your occupation? Farmer ............................................. 1

Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA ----42424242----
Housewife ....................................... 2Merchant ......................................... 3Fisherman........................................ 4Artisan ............................................. 5Other (specify)____________ ......... 8Don’t know...................................... 9
(if the respondent is the mother, go to 27)
(If the mother is not the respondent, ask:)26.1 What is/was the mother’s occupation? Farmer ............................................. 1
Housewife ....................................... 2Merchant ......................................... 3Fisherman........................................ 4Artisan ............................................. 5Other (specify)____________ ......... 8Don’t know...................................... 9
27. Do you own, at home... Yes (1) No (2) Don’t know(9)
27.1 a Boat? 1 2 9
27.2 an Ox Cart? 1 2 9
27.3 cattle? 1 2 9
27.4 a bicycle? 1 2 9
27.5 a motorcycle? 1 2 9
27.6 any other transportation?(specify)__________________________
1 2 9
(If the respondent is the mother, go to 28)If the respondent is NOT the mother, ask:
At the mother’s house, do they have... Yes (1) No (2) Don’t know(9)
27.1 a Boat? 1 2 9
27.2 an Ox Cart? 1 2 9
27.3 cattle? 1 2 9
27.4 a bicycle? 1 2 9
27.5 a motorcycle? 1 2 9
27.6 any other transportation?(Specify)___________________
1 2 9
28. What is the roof of the house that the mother lives(d) made of? Thatches ....................................................... 1

Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA ----43434343----
Metal ............................................................ 2Tiles.............................................................. 3Wood............................................................ 4Other (specify)_________________............ 8Don’t know .................................................. 9
29. What is the wall of the house that the mother lives(d) made of? Thatches ....................................................... 1Metal ............................................................ 2Tiles.............................................................. 3Wood............................................................ 4Other (specify)_________________............ 8Don’t know .................................................. 9
30. What language was spoken most often in the household? ( of the mother) Khmer................................. 1Lao...................................... 2Thai..................................... 3Chinese ............................... 4Cham .................................. 5Vietnamese ......................... 6Other___________............. 8Don’t know......................... 9

Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA ----44444444----
Section 4: Information about previous pregnancies and deliveries
Only if the mother is the respondent complete this section. If the mother is NOT the respondent, goto section 5. In this section the “STILLBIRTH” and the “BORN ALIVE” IS NOT INCLUDED.
Now I would like to ask you some questions about your previous pregnancies and deliveries.
31. Are you currently pregnant? Yes 1No ....................................... 2Don’t know......................... 9
32. How many times have you been pregnant previously? ..................................................................... _____________(The number of pregnancies INCLUDES all PREVIOUS abortion, stillbirth and Don’t know.......... 99born alive. It does NOT INCLUDE this ”Stillbirth” (If “0", go to Section 5)nor this “born alive”)
33.Out of ______(number of pregnancies), how many were miscarriages/ abortions? .......................... _____________Don’t know.............9
(If the mother did not have any previous delivery, go to Section 5)
34. Of all the deliveries you had, how many baby’s were born dead? ..................................................... _____________Don’t know........................99
34.1 Out of the deliveries, how many were born alive? ................................................................ ____________Don’t know...........99
(If “0", go to Section 5)
34.2 Out of the________born alive, are all still living? Yes..........................1No ...........................2Don’t know.............9
(if “YES”, go to Section 5)
If “NO”, ask:34.3 How many died? ......................................................................................................... ___________
Don’t know...........99
34.4 How many of them died before the age of 5 years?.................................. ____________________Don’t know.............9

Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA----45454545----
Section 5: Open history
Now I would like to use a tape recorder so that I can understand clearly and remember everything you tell meabout your pregnancy, labor and delivery (continue only if the child was born alive) and if the child was bornalive, about the child’s illness and death. Is this OK with you?
If the respondent agrees, prepare to tape the open history report. As you listen to the narrative,make note of any symptoms of illness the mother mentions during her report and any otherimportant observation you might have. Don’t interrupt her until she finishes. Don’t stop therecording of the tape recorder until you finished the whole open history, which includes thequestion about the cause of death. After you finished the whole interview and you are yourworking place, rewind the tape and transcribe everything the mother told you in her own andexact words, as well as the question asked by you and her answers.
1. “Now I would like you to tell everything that happened to you during pregnancy, labor and delivery. Ifyou noticed any problem during pregnancy, labor or delivery, what did you do for it at home, where didyou go to seek care for the problem, as well as everything the person you consulted did to solve yourproblem?”
Once the mother finished the description of the illness, ask:2. Did anything else happen during pregnancy?
3. Did anything else happen during labor and delivery?

Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA----46464646----
If the “Case” is a child that was born alive and died, ask:
. Now I would like you to tell me the whole story of the baby’s illness and death. Tell me everything thathappened right after delivery with the baby and how its illness developed, including all the symptoms orproblems and what was done for the child.
Once the mother finished the description of the illness, ask:
5. Is there anything else?
If STILLBIRTH or BORN ALIVE THAT DIED, ask:6. “Tell me, what do you think was the cause of your baby’s death?”
Look up the symptoms mentioned spontaneously by the respondent related to pregnancy, laboror delivery and to the child. Then identify the mentioned symptom listed in Section 6 (page 7 to10) and circle (1) under the column of question 35, 39 and 43. Only after you finishedtranscribing all symptoms mentioned, go on with question 36.
Section 6: Problems during pregnancy, labor or delivery and new born

Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA----47474747----
Circle all of the problems on the list on this page which were spontaneously reported during the open history.Then, to obtain the prompted report, ask about the presence of each of the other symptoms listed to see if any ofthem occurred during the illness that led to death.
Problems during pregnancy (before labor or delivery): All respondents36.Prompted report 37. “During which
month of pregnancyyou noticed ......
(symptom)?”
38. “How manydays or months didthe_____(symptom
) last?”
Problem or symptom 35.SpontaneousreportYes(1)
Yes(1)
No(2)
Don’tknow (9)
(Record the days or months. If “Don’tknow”, circle 99.
101.Vaginal bleeding 1 1 2 9 99 99
102.Hand and facial swelling 1 1 2 9 99 99
103.Labor Contractions beforetime (sometime before the actualdelivery)
1 1 2 9 99 99
104. Convulsions 1 1 2 9 99 99
105. High blood pressure(measured with cuf)
1 1 2 9 99 99
106. Oliguria 1 1 2 9 99 99
107. Water broke more than 1 daybefore labor began
1 1 2 9 99 99
108. Fever 1 1 2 9 99 99
109.Chills 1 1 2 9 99 99
110.Genital ulcer (told by physician) 1 1 2 9 99 99
111. Pale/breathless, weak or severeanemia
1 1 2 9 99
112. Multiple pregnancy (detectedduring pregnancy)
1 1 2 9 99
113. Baby stopped moving duringpregnancy
1 1 2 9 99
114. Positive syphilis test 1 1 2 9 99
115. Diabetes diagnosed by doctor 1 1 2 9 99
116. Other(specify)______________ 1 99 99

Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA----48484848----
117. Other (specify)_____________ 99 99
For the pathway, only take into account the first 6 symptoms listed (Bold)
Problems during labor and delivery Stillbirth and New born infant40.Prompted reportProblem or symptom 39.Sponta
neousreportYes(1)
Yes(1)
No(2)
Don’tknow (9)
41. What was the duration of the labor/delivery?__________________hours Don’t know 9
42. “ For how many hours did you have___________(symptom)?”(Record the hours, if “Don’t know” circle99.
201. Convulsions 1 1 2 9 Hours 99
202.Heavy vaginal bleeding duringlabor/delivery
1 1 2 9 Hours 99
203. Heavy vaginal bleeding afterdelivery
1 1 2 9 Hours 99
204. Made an effort for more than 2hours
1 1 2 9 Hours 99
205. Labor was longer than usual(more than 12 hours)
1
206. Hand and facial swelling 1 1 2 9
207. High blood pressure (measuredwith cuff)
1 1 2 9
208. Oliguria 1 1 2 9
209.Baby come out with buttock,feet, hands first
1 1 2 9
210. Instrument delivery (forceps,vacuum, C-section)
1 1 2 9
211. Waters was smelly 1 1 2 9
212. Water was brown, yellow orhad meconium
1 1 2 9
213. Did the person that deliveredthe baby say that something waswrong with the water?
1 1 2 9
214. Multiple pregnancy 1 1 2 9
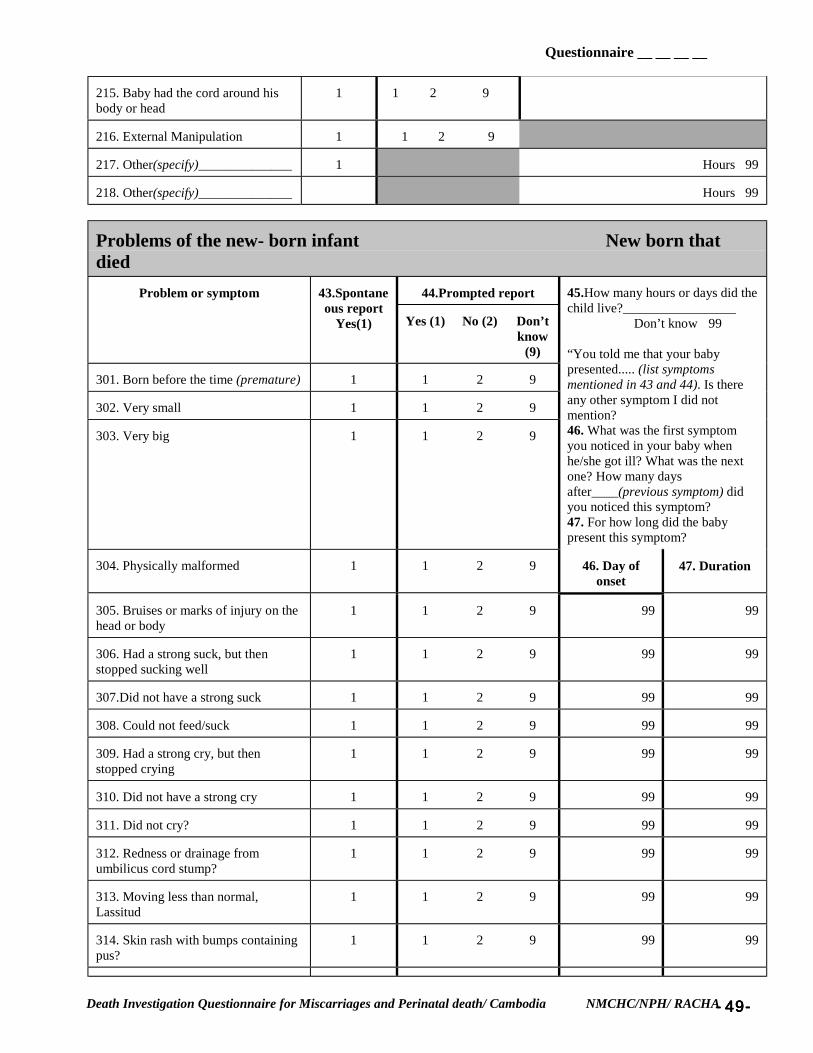
Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA----49494949----
215. Baby had the cord around hisbody or head
1 1 2 9
216. External Manipulation 1 1 2 9
217. Other(specify)______________ 1 Hours 99
218. Other(specify)______________ Hours 99
Problems of the new- born infant New born thatdied
44.Prompted reportProblem or symptom 43.Spontaneous report
Yes(1) Yes (1) No (2) Don’tknow
(9)
301. Born before the time (premature) 1 1 2 9
302. Very small 1 1 2 9
303. Very big 1 1 2 9
45.How many hours or days did thechild live?_________________ Don’t know 99
“You told me that your babypresented..... (list symptomsmentioned in 43 and 44). Is thereany other symptom I did notmention?46. What was the first symptomyou noticed in your baby whenhe/she got ill? What was the nextone? How many daysafter____(previous symptom) didyou noticed this symptom?47. For how long did the babypresent this symptom?
304. Physically malformed 1 1 2 9 46. Day ofonset
47. Duration
305. Bruises or marks of injury on thehead or body
1 1 2 9 99 99
306. Had a strong suck, but thenstopped sucking well
1 1 2 9 99 99
307.Did not have a strong suck 1 1 2 9 99 99
308. Could not feed/suck 1 1 2 9 99 99
309. Had a strong cry, but thenstopped crying
1 1 2 9 99 99
310. Did not have a strong cry 1 1 2 9 99 99
311. Did not cry? 1 1 2 9 99 99
312. Redness or drainage fromumbilicus cord stump?
1 1 2 9 99 99
313. Moving less than normal,Lassitud
1 1 2 9 99 99
314. Skin rash with bumps containingpus?
1 1 2 9 99 99

Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA----50505050----
315. Fever? 1 1 2 9 99 99
316. Yellow skin and eyes? 1 1 2 9 99 99
317. Cough? 2 1 2 9 99 99
318. Difficult breathing? 2 1 2 9 99 99
44.Prompted reportProblem or symptom 43.Spontaneous report
Yes(1)Yes (1) No (2) Don’t
know(9)
46. Day ofonset
47. Duration
319. Indrawing of the chest? 1 1 2 9 99 99
320. Frequent liquid and waterystools?
1 1 2 9 99 99
321. Blood in stool? 1 1 2 9 99 99
322. Bulging fontanelle? 1 1 2 9 99 99
323. Unresponsive/ unconscious? 1 1 2 9 99 99
324.Stop being able to grasp 1 1 2 9 99 99
325. Stop being able to follow themovement of the eyes
1 1 2 9 99 99
326. Larthegic 1 1 2 9 99 99
327. Convulsions? 1 1 2 9 99 99
328. Very pale? 1 1 2 9 99 99
329. Felt very cold? 1 1 2 9 99 99
330. Was born purple or got purple?(cyanosis)
1 1 2 9 99 99
331. Other(specify)_______________ 1 99 99
332. Other(specify)_______________ 1 99 99
333. Other(specify)_______________ 1 99 99
334. Other(specify)_______________ 1 99 99
335. Other(specify)_______________ 1 99 99

Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA ----51515151----
Section 7: Pregnancy care (only if the Mother is the respondent. If not, go to Section 8)
Now I would like to ask you some questions about the prenatal care you received during pregnancy.
48. Did you go anywhere outside the home for pregnancy care? Yes .................................1 (If “NO”, list the different providers to make sure she did not go to any of them) No ........................................2
Don’t know...........................9(If “NO”, go to Section 8)
48.1 Did you go for routinepregnancy care to...
Health provider
Yes(1) No(2) Don’tknow(9)
48.2 How many times didyou go to ....
(only ask for the “YES”mentioned in Q. 48.1)
48.3 What provider didyou see at....
(only ask for the “YES”mentioned in Q. 48.1)
1. Kru Khmer? 1 2 9 Don’t know .99 Kru Khamer ...................1
2. TBA? 1 2 9 Don’t know...99 TBA................................6
3. Health Center? 1 2 9 Don’t know .99 Doctor..2 Nurse...3Midwife..4 Other___..8Medical assistant....5Don’t know...9
4. Drug shop orpharmacy?
1 2 9 Don’t know .99 Drug seller...4Other___________...8Don’t know....9
5. Private office orclinic?
1 2 9 Don’t know .99 Doctor..2 Nurse...3Midwife..4 Other___..8Medical assistant....5Don’t know...9
6. Hospital? 1 2 9 Don’t know .99 Doctor..2 Nurse...3Midwife..4 Other___..8Medical assistant....5Don’t know...9
7. Other?(specify)_____________
1 2 9 Don’t know .99 Kru Khmer....1Doctor..2 Nurse...3Midwife..4 Other___..8Medical assistant....5Don’t know...9

Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA ----52525252----
49. To which of them did you go the first time? Kru Khmer ........................................1TBA...................................................2Health center .....................................3Drug shop or pharmacy .....................4Private office or clinic .......................5Hospital .............................................6Other(specify)_________ ..................8Don’t know........................................9
50. How many months pregnant were you when you first received this care .....................................___________monthDon’t know............99
51. Have you ever received any injections of a vaccine to prevent tetanus in you or your baby? Yes...........................1No ...........................2Don’t know..............9
(If “NO”, go to 52)
If “YES”, ask:51.1 How many doses of tetanus vaccine did you receive during your pregnancy? ........................ ___________
Don’t know..............9
51.2 How many doses of tetanus vaccine had you received prior to your pregnancy? .................... ___________Don’t know............99
52. During your pregnancy
52.1 did anyone measure the height of your uterus? Yes...........................1No ...........................2Don’t know..............9
52.2 did anyone measure your blood pressure? (With cuff) Yes...........................1No ...........................2Don’t know..............9
52.3 did anyone take a specimen of your urine for tests? Yes ....................1No ...........................2Don’t know..............9
52.4 did anyone take a specimen of your blood for test? Yes ....................1No ...........................2Don’t know..............9
52.5 did anyone give you any tablets or pills? Yes...........................1No ...........................2Don’t know..............9
(If “NO”, go to 53)If “YES”, ask:

Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA ----53535353----
52.6 Did you receive....Types of tablets or pills
Yes (1) No (2) Don’t know (9)
52.7 For how long did you take...(ask only for the “YES” of Q. 52.6)
1. Iron for prevention ortreatment of anemia?
1 2 9 Don’t know ..... 99
2. Antibiotic for treatmentof infection?
1 2 9 Don’t know ..... 99
3. Antimalarial 1 2 9 Don’t know ..... 99
4. Other (specify)_________ 1 2 9 Don’t know ..... 99
53. Did any of the persons you saw during pregnancy tell you that there was something wrong with it?Yes........................................1No ........................................2Don’t know...........................9
(if “NO”, go to 54)
If “YES”, ask:53.1 What did he/she tell you_______________________________________________________________
_______________________________________________________________________________________
54. Do you have any mother’s health card recording the care you received during your pregnancy and delivery?Yes........................................1No ........................................2Don’t know...........................9
(if “NO”, go to Section 8)
54.1 May I see it now? Yes ..............................................................................1I don’t have it with me now or lost the card ...............2
(If “don’t have it or lost it”, go to Section 8)
If you can see the card, record:54.2 Record the number of tetanus immunizations given.......................................... ________________
Not recorded ..........99
54.3. Record any results for any urine or blood test ............... _________________________________Not recorded ..........99

Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA ----54545454----
Section 8: Labor and delivery
Now I’d like to ask some questions about the last days of pregnancy and the baby’s birth.
55. Where was the baby born? Home..............................................................1Health Center .................................................2Private clinic ..................................................3Hospital ..........................................................4Other (specify)________................................8Don’t know ....................................................9
56. Why did you choose this place ? ........... ____________________________________________________________Don’t know ....................................................9
57. Did you plan for the baby to be born there? Yes ..................................................................1No ..................................................................2Don’t know ....................................................9
(If “YES”, go to 58)If “NO”, ask:57.1 Where had you planned for the baby to be born? ................ _____________________________________
57.2 What was the most important reason to change? ................. _____________________________________
58. Who was the principal decision-maker in selecting the planned location for the birth?Mother............................................................1Husband .........................................................2Mother and Husband......................................3Grandmother ..................................................4TBA ...............................................................5Other health care provider..............................6Other(specify)______________.....................8Don’t know ....................................................9
59. Who actually delivered the baby? Mother............................................................1TBA................................................................2Midwife..........................................................3Doctor ............................................................4Nurse ..............................................................5Family member_______________ ................6Neighbor.........................................................7Other(specify)______________.....................8Don’t know ....................................................9
60. Did you stop feeling the baby move before it was born? Yes .................................................................1No ..................................................................2

Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA ----55555555----
I never felt the baby move..............................3Don’t know ....................................................9
If “YES”, ask:60.1 When did you stop feeling the baby move? 2 or more days before birth? ..........................1
1 or 2 days before birth? ................................2Less than one day before birth .......................3During delivery ..............................................4Don’t know ....................................................9
" If the case is a STILL BIRTH, go to section 9
" If the case is a NEW BORN INFANT THAT DIED, go to section 10

Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA ----56565656----
Section 9: Still birth
61. How did you know that the baby was born dead? Did not cry .....................................................1 (Check all the answers spontaneously reported, do not Did not move..................................................2 Prompt) Did not breathe...............................................3
Other (specify)____________________........8Don’t know ....................................................9
(If mentioned spontaneously “did not cry, did not move”and “did not breath”, go to 62)
If didn’t mention “did not cry, did not move” and “did no breath”, ask:61.1 Did the baby cry? Yes .................................................................1
No ..................................................................2Don’t know ....................................................9
61.2 Did the baby move? Yes .................................................................1No ..................................................................2Don’t know ....................................................9
61.3 Did the baby breath? Yes .................................................................1No ..................................................................2Don’t know ....................................................9
62. Who determined that the baby was dead? Mother............................................................1Other family member______________ .........2TBA ...............................................................3Midwife..........................................................4Nurse ..............................................................5Doctor ............................................................6Other (specify)_______________ ..................8Don’t know ....................................................9
63. Did you determine immediately after birth, within a few minutes or one hour or more after birth that the child wasdead? Immediately ...................................................1
Within a few minutes .....................................2One hour or more ...........................................3Don’t know ....................................................9
64. Did you see the baby after birth? Yes .................................................................1No...................................................................2Don’t know ....................................................9
(If “NO”, go to 65)

Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA ----57575757----
If “YES”,ask:64.1 What did the baby look like? Normal ...........................................................1 (Don’t prompt, check all answers reported Physically malformed.....................................2 Spontaneously ) Macerated.......................................................3
Other (Specify)_______________ .................8Don’t know ....................................................9
64.2 Was the baby very small, about average or unusually large? Very small .........................................1About average ...................................2Unusually large .................................3Don’t know........................................9
65. Was the baby Male...................................................1Female ...............................................2Don’t know........................................9
Once you finished this section, go to Section 11

Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA ----58585858----
Section 10: Baby born alive that died
61. How did you know that the baby was born alive? Cried...............................................................1 (Check all the answers spontaneously reported, do not Moved ............................................................2 Prompt) Was breathing ................................................3
Other (specify)____________________........8Don’t know ....................................................9
(If mentioned spontaneously “cried, moved” or “was breathing”, go to 62)
If didn’t mention “cried, moved” or “was breathing”, ask:61.1 Did the baby cry? Yes .................................................................1
No ..................................................................2Don’t know ....................................................9
61.2 Did the baby move? Yes .................................................................1No ..................................................................2Don’t know ....................................................9
61.3 Did the baby breath? Yes .................................................................1No ..................................................................2Don’t know ....................................................9
62. Who determined that the baby was alive? Mother............................................................1Other family member______________ .........2TBA ...............................................................3Midwife..........................................................4Nurse ..............................................................5Doctor ............................................................6Other (specify)_______________ ..................8Don’t know ....................................................9
63. Was the baby Male ..................................................1Female ...............................................2Don’t know .......................................9
64. Did you see the baby after birth? Yes .................................................................1No...................................................................2Don’t know ....................................................9
(If “NO”, go to 65)
If “YES”,ask:

Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA ----59595959----
64.1 What did the baby look like? Normal ...........................................................1 (Don’t prompt, check all answers reported Physically malformed.....................................2 Spontaneously ) Other (Specify)_______________ .................8
Don’t know ....................................................9
64.2 How soon after birth did you (the mother) see the baby? Immediately ...................................................1Within a few minutes .....................................2One hour or more ...........................................3Don’t know ....................................................9
65. Was the baby very small, about average or unusually large? Very small...................................................................1About average ...................................2Unusually large .................................3Don’t know........................................9
Care of the baby after delivery
66. With what tool was the cord cut? Metal knife .....................................................1Razor blade ....................................................2Bamboo knife .................................................3Scissors ..........................................................4Other(specify)________________.................8Don’t know ....................................................9
67. Was anything put on the cord after it was cut? Yes........................................1No .........................................2Don’t know...........................9
(If “NO”, go to 68)
If “YES”, ask:67.1 What? ______________________________________________________________________________
Don’t know...........................9
68. Was the baby bathed Within the first hour after birth? ..................................11 to 4 hours after birth?................................................24 to 12 hours after birth?..............................................312 to 24 hours after birth?............................................4During the 2nd day after birth .......................................53 or more days after birth.............................................6Was never
bathed.............................................................7Don’t know ..................................................................9

Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA ----60606060----
69. Where did the baby sleep after birth? ............................................................................. Alone 1With the mother ...........................................................2With other relative(specify)_____________................3Other(specify)___________________.........................8Not applicable ..............................................................4Don’t know ..................................................................9
70. Was the baby ever breast-fed? Yes......................................................1No ......................................................2Don’t know.........................................9
(If “No”, go to 71)
70.1 When was the baby breast-fed for the first time? Within the first hour after birth? .....................11 to 4 hours after birth? ...................................24 to 12 hours after birth? .................................312 to 24 hours after birth.................................42 days after birth .............................................53 or more days after birth ................................6Don’t know .....................................................9
70.2 How many times per day (24 hours) was the baby breast-fed? ........................................... ______________ (Make sure that it includes the feeding during day and night) Don’t know.............99
70.3 Was the initial breast milk (colostrum) fed to the baby? Yes.........................................1 (Make sure it was not squeezed out before breastfeeding) No .........................................2
Don’t know............................9

Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA ----61616161----
71. Did you give the baby........... (Prompt for each response)
Yes (1) No (2) Don’t know (9)
711 Cowmilk? 1 2 9
71.2 Formula milk?( Like Dumex, Alaska, Francebebe...)
1 2 9
71.3 Water with sugar? 1 2 9
71.4 Water? 1 2 9
71.5 Tea or infusions? 1 2 9
71.6 Any other fluid? (Specify)________ 1 2 9
72 How much time after delivery did the baby get ill? .............................................................______hours / ______days The baby was born ill ............0
Don’t know..........................99
73. Where did the baby die? Home............................................................................1At a relatives or friends home......................................2Heath care provider’s home .........................................3Private office or clinic..................................................4Public health center......................................................5Hospital ........................................................................6Other (specify)______________ .................................8Don’t know ..................................................................9
Once you finished this section, go to Section 11

Questionnaire __ __ __ __
D th I ti ti Q ti i f Mi i d P i t l d th/ C b di NMCHC/NPH/ RACHA----25252525----
Section 11: Care- Seeking
Could you please tell me the time it takes you to go to your usual
Could you please tell me for any illness, the time it takes you to goto your usual
74.1 Time (Don’t know ...99)
74.2 Transportation(Don’t know ...9)
1. Kru Khamer? 99 9
2. Drug seller/pharmacy? 99 9
3. TBA? 99 9
4. Private clinic or practitioner? 99 9
Could you now please tell me how much money you spend, during this pregnancy and delivery, on...
EXPENSES 75. PREGNANCY(Don’t know...9;
Did not consult ...1)
76. DELIVERY(Don’t know...9;
Did not consult ...1)
77. NEW BORN(Don’t know...9;
Did not consult ...1)
1. Total transportation cost 9 9 9
2. Total Consultation cost (includesdrugs)
19
19
19
If the respondent doesn’t know the TOTAL consultation cost for either Pregnancy care, Delivery or the New Bornthat died, ask for Drug cost and Consultation cost only. Then continue with “other expenses”.
2.1. Drug cost only 9 9 9
2.2 Consultation cost only 9 9 9
3. Other expenses 9 9 9
Once you finished this section, go to the Pathway form.
" Copy only the symptoms the mother mentioned during pregnancy and delivery on the “PregnancyPathway Form” (page 10 and 11). If there aren’t any symptoms during pregnancy orlabor/delivery recorded, continue with the “Child Pathway Form” if it was a born alive child thatdied.

Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA----26262626----
PREGNANCY PATHWAY FORM QUESTIONNAIRE #: ___ ___ ___ ___ DATE: ___/___/___INSTRUCTIONS TO SURVEYOR: 1) COMPLETE I.D. .2-3 ASK ABOUT THE ACTIONS TAKEN FOR THE ILLNESS. COMPLETE ONE ROW FOR EACH ACTION. 7) CHECK FOR ERRORS.
Copy the symptoms and their codes that were present during pregnancy (page 11) and the month of pregnancy she noticed it , each symptom in one of theboxes (it will help you to find out the first and last one to appear during pregnancy)
Symptoms: #________________________ #_________________________ #__________________________ #_______________________ #______________________
“Now I would like to review the things you did at home and outside your home when you noticed________ (read symptoms) during your pregnancy.
LIST OF SYMPTOMSPREGNANCY
Symptoms (codes)
1. ACTION“ What did you do whenyou noticed ________
(symptom1,2,3...)?”
2 “How many days hadyou noticed ___ (1st, 2nd ,3rd ... symptom...) when
you first took thisaction?”
3. Who was the personthat decided to do....(action1,2,3...)Mother...1 Father ...2 Grandmother...3 Other....8 (specify) Don’t know...9
FOR ACTIONS TAKENINSIDE or OUTSIDE THE HOME
IF THE MOTHER DID NOT SEEK CARE AT A PUBLIC HEALTH AGENT, ASK:
4. “Why didn’t you go to the public health provider at this time?”
1 2 3 9
Other___________8
1 2 3 9
Other___________8
1 2 3 9
Other___________8
1 2 3 9
Other___________8
1 2 3 9
Other___________8
1 2 3 9
Other___________8

Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA----27272727----
PREGNANCY OUTSIDE-THE-HOME
IF THE ACTION WAS AN OUTSIDE-THE-HOME TREATMENT, ASK:
5. “Why did you go there?”
6. “When you wentto....... (provider) at thistime, what did he/she do?”
(If necessary probe:because it is close by,cheap, I usually go there, Itrust them/him,
(If necessary probe:he/she excamined me, gaveme medication or IV fluids,
7. “What did thisperson suggest toYOU ?”(If necessary probe: givemedicine, go to anotherprovider, take tea orherbal
8. “Were you able to do/follow ALLthe advices
that this person suggested?”
{Yes(1), No (2), Not applicable (8), Don’t know (9)}
9. “Did this personrefer you to anotherhealth provider? (If “No”, go to thenext action)
someone told me to gothere, I got worse, thetreatment did not work....)
blessed or prayed, tooksome blood or urine tests,saw if the baby waswell...)
medicine,come back in afew days, he/she did notadvice anything....)
SYMPTOM
CODE
8.1. IF “NO”, ASK: “Why were you not
able to follow theadvice ?”
1=Y
2=N
9.1 IF “YES”, ASK: “ Did
you accept the referral?”(Yes(1), No(2), Not
applicable (8), Don’tknow(9)
9.2If “No” ASK:(the referral was not accepted)
“Why didn’t you accept the referral?”
128
129
1 2 9 8
128
129
1 2 9 8
1289
129
1 2 9 8
1289
129
1 2 9 8
1289
129
1 2 9 8
1289
129
1 2 9 8
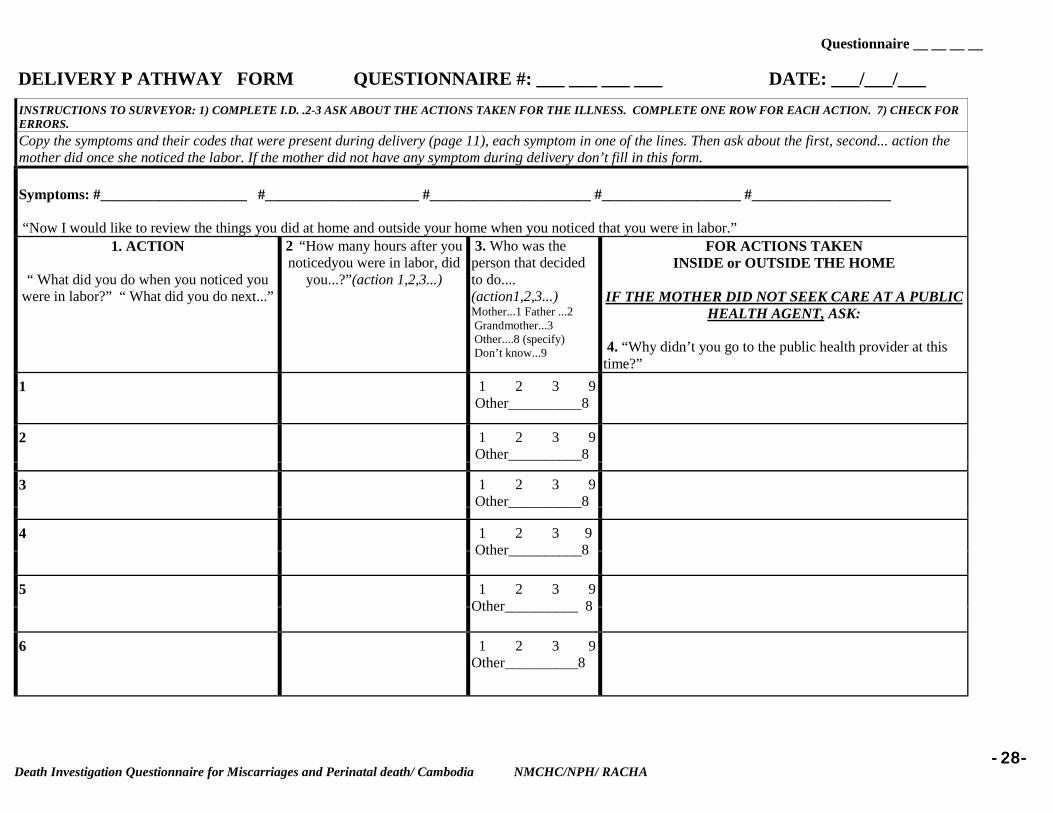
Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA----28282828----
DELIVERY P ATHWAY FORM QUESTIONNAIRE #: ___ ___ ___ ___ DATE: ___/___/___INSTRUCTIONS TO SURVEYOR: 1) COMPLETE I.D. .2-3 ASK ABOUT THE ACTIONS TAKEN FOR THE ILLNESS. COMPLETE ONE ROW FOR EACH ACTION. 7) CHECK FORERRORS.Copy the symptoms and their codes that were present during delivery (page 11), each symptom in one of the lines. Then ask about the first, second... action themother did once she noticed the labor. If the mother did not have any symptom during delivery don’t fill in this form.
Symptoms: #____________________ #_____________________ #______________________ #___________________ #___________________
“Now I would like to review the things you did at home and outside your home when you noticed that you were in labor.”1. ACTION
“ What did you do when you noticed youwere in labor?” “ What did you do next...”
2 “How many hours after younoticedyou were in labor, did
you...?”(action 1,2,3...)
3. Who was theperson that decidedto do....(action1,2,3...)Mother...1 Father ...2 Grandmother...3 Other....8 (specify) Don’t know...9
FOR ACTIONS TAKENINSIDE or OUTSIDE THE HOME
IF THE MOTHER DID NOT SEEK CARE AT A PUBLICHEALTH AGENT, ASK:
4. “Why didn’t you go to the public health provider at thistime?”
1 1 2 3 9 Other__________8
2 1 2 3 9 Other__________8
3 1 2 3 9 Other__________8
4 1 2 3 9 Other__________8
5 1 2 3 9Other__________ 8
6 1 2 3 9Other__________8

Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA----29292929----
Delivery IF THE ACTION WAS AN OUTSIDE-THE-HOME TREATMENT, ASK:
5. “Why did you go there ?”6. “When you went to.......(provider) at this time, whatdid he/she do?”
(If necessary probe: because itis close by, cheap, I usually gothere, I trust them/him,
(If necessary probe: he/sheexcamined me, gave memedication or IV fluids,
7. “What did thisperson suggest toYOU ?”(If necessary probe: givemedicine, go to anotherprovider, take tea or herbal
8. “Were you able to do/follow ALL the advices that
this person suggested ?”{Yes(1), No (2), Not applicable (8), Don’t know (9)}
9. “Did thisperson refer youto another healthprovider? (If “No”, go tothe next action)
someone told me to go there, Igot worse, the delivery wasdifficult....)
blessed or prayed, took someblood or urine tests,delivered the baby...)
medicine,come back in afew days, he/she did notadvice anything....)
SYMPTOM
CODE
8.1. IF “NO”, ASK: “Why were you not ableto follow the advice ?”
1=Y
2=N
9.1 IF “YES”, ASK: “Did you accept the
referral?”(Yes(1), No(2), Not
applicable (8), Don’tknow(9)
9.2If “No” ASK:(the referral was not
accepted)
“Why didn’t you accept thereferral?”
1289
12
9
1 2 9 8
1289
12
9
1 2 9 8
1289
12
9
1 2 9 8
1289
12
9
1 2 9 8
1289
12
9
1 2 9 8
1289
12
9
1 2 9 8

Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA----30303030----
PATHWAY FORM QUESTIONNAIRE #: ___ ___ ___ DATE: ___/___/___ SURVEYOR ID #: ___ ___INSTRUCTIONS TO SURVEYOR: 1) COMPLETE I.D. .2-4 ASK ABOUT THE ACTIONS TAKEN FOR THE ILLNESS. COMPLETE ONE ROW FOR EACH ACTION. 7) CHECK FOR ERRORS.
“Now I would like to review the things you did at home and outside your home when the child got sick.1. ACTION
“ What was the first thingyou did when you noticed
the child was ill?”(What was the next thing
you did...?)
2 “How manydays had thechild been ill
when you (first)took thisaction?”
3. Who was the personthat decided to do...(action 1, 2, 3...)Mother (1) Father(2)Grandmother(3)Other(8) Don’t know (9)
4. “ For which symptoms thechild had at that moment didyou do/ give ....(action 1,action 2...)?
(Write down the symptoms themother spontaneouslymentions)
FOR ACTIONS TAKENINSIDE or OUTSIDE THE HOME
IF THE CHILD WAS NOT SEEN BY A PUBLICHEALTH AGENT, ASK:
5. “Why didn’t you go to the public health provider atthis time?”
11 2 3 98 (specify)_________
21 2 3 98 (specify)________
31 2 3 9
8 (specify)__________
41 2 3 98(specify)__________
51 2 3 98(specify)__________
61 2 3 98(specify)__________
71 2 3 98(specify)__________
81 2 3 98(specify)__________
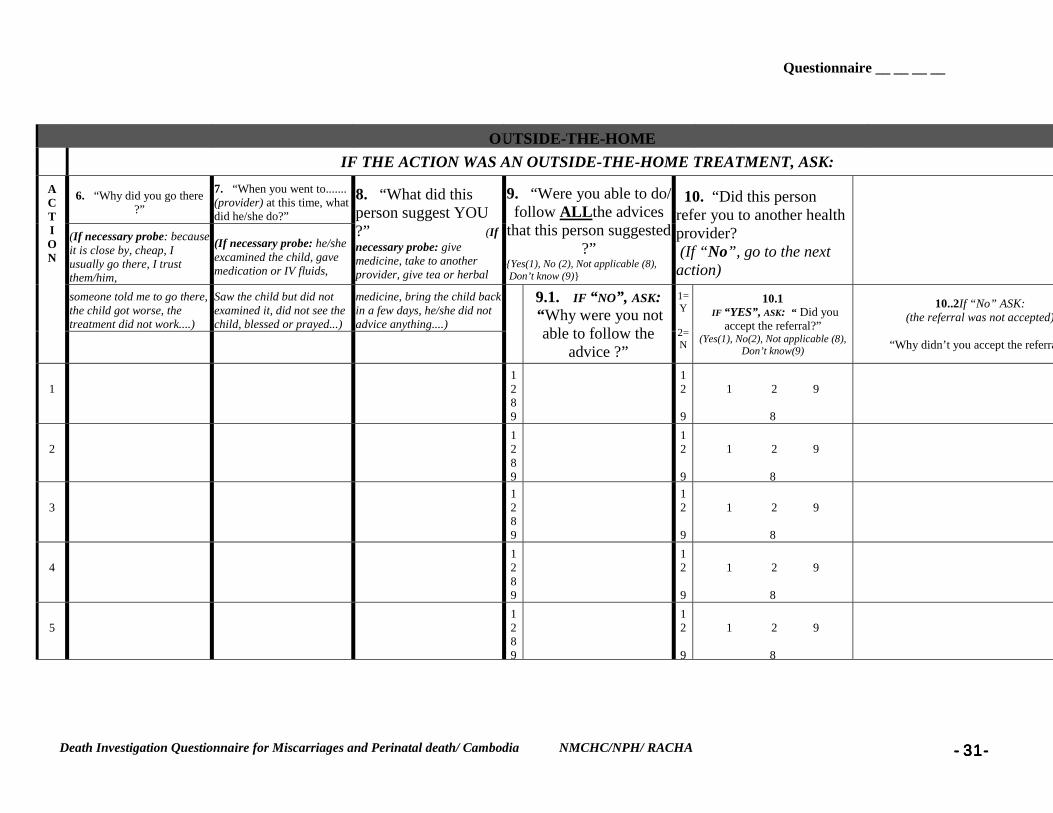
Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA ----31313131----
OUTSIDE-THE-HOMEIF THE ACTION WAS AN OUTSIDE-THE-HOME TREATMENT, ASK:
6. “Why did you go there?”
7. “When you went to.......(provider) at this time, whatdid he/she do?”
(If necessary probe: becauseit is close by, cheap, Iusually go there, I trustthem/him,
(If necessary probe: he/sheexcamined the child, gavemedication or IV fluids,
8. “What did thisperson suggest YOU?” (Ifnecessary probe: givemedicine, take to anotherprovider, give tea or herbal
9. “Were you able to do/follow ALLthe advices
that this person suggested?”
{Yes(1), No (2), Not applicable (8), Don’t know (9)}
10. “Did this personrefer you to another healthprovider? (If “No”, go to the nextaction)
someone told me to go there,the child got worse, thetreatment did not work....)
Saw the child but did notexamined it, did not see thechild, blessed or prayed...)
medicine, bring the child backin a few days, he/she did notadvice anything....)
ACTION
9.1. IF “NO”, ASK: “Why were you not
able to follow theadvice ?”
1=Y
2=N
10.1 IF “YES”, ASK: “ Did you
accept the referral?”(Yes(1), No(2), Not applicable (8),
Don’t know(9)
10..2If “No” ASK:(the referral was not accepted)
“Why didn’t you accept the referra
11289
12
9
1 2 9
8
21289
12
9
1 2 9
8
31289
12
9
1 2 9
8
41289
12
9
1 2 9
8
51289
12
9
1 2 9
8

Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA ----32323232----
61289
12
9
1 2 9
8

Questionnaire __ __ __ __
Death Investigation Questionnaire for Miscarriages and Perinatal death/ Cambodia NMCHC/NPH/ RACHA ----33333333----