the oral-systemic connection: a different angle - your oral …€¦ · · 2017-05-24the...
TRANSCRIPT

1
Scott S. De Rossi, DMDChairman, Oral Health & Diagnostic Sciences
Professor of Oral MedicineProfessor of Otolaryngology/Head & Neck Surgery
Professor of DermatologyGeorgia Regents University, Augusta GA
THE ORAL-SYSTEMIC CONNECTION:A DIFFERENT ANGLE
Scott S. De Rossi, DMD
Scott S. De Rossi, DMD
• Oral & Maxillofacial PathologyBiopsy Service
– Dr. Rafik Abdelsayed, Director
– Dr. Zoya Kurago
• Oral & Maxillofacial Radiology3D Imaging Center
– Dr. Sajitha Kalathingal, Director
– Dr. Allison K. Hunter
Scott S. De Rossi, DMD
• Oral MedicineMucosal Disease, Facial Pain,
Salivary Gland Disease
– Dr. Scott S. De Rossi, Director
– Dr. Katharine N. Ciarrocca
– Dr. Wayne Herman
– Dr. Ilanit Stern
Scott S. De Rossi, DMD
What is Oral Medicine?
• The specialty of dentistry that includes the diagnosis and primarily non-surgical management of:– Oral mucosal disease– Orofacial pain and TMD– Salivary gland disorders/Xerostomia
Prescription drug use (CDC)
• Percent of persons using at least one prescription drug in the past 30 days: 48.5% (2007-2010)
• Percent of persons using three or more prescription drugs in the past 30 days: 21.7% (2007-2010)
• Percent of persons using five or more prescription drugs in the past 30 days: 10.6% (2007-2010)
Scott S. De Rossi, DMD

2
Physician office visits
• Number of drugs ordered or provided: 2.6 billion
• Percent of visits involving drug therapy: 75.1%
• Most frequently prescribed therapeutic classes:– Analgesics
– Antihyperlipidemic agents
– Antidepressants
Scott S. De Rossi, DMD
Clinical Pearl
• In the presence of oral lesions and dry mouth, consider medication use a potential cause
• Carefully explore the temporal relationship of signs and symptoms with medication use (new use, dose change, generic/brand)
Scott S. De Rossi, DMD
Scott S. De Rossi, DMD
A review of adverse oral reactions to systemic medicationScott S. De Rossi, DMD and Elliot V. Hersh, DMD, MS, PhD
Potential oral manifestations of cardiovascular drugs.
• The frequency of potential oral manifestations in patients receiving cardiovascular agents was 14.1%.
• The occurrence and character of the oral manifestations had no significant relation with individual cardiac drugs, although there was a trend for oral manifestations to be likely with increasing number of drugs.
• Oral symptoms and/or signs were recorded in 75 (14.1%) patients with xerostomia being the most common (7.5%), followed by lichenoid (lichen planus-like) lesions (3.6%) and dysgeusia (1.9%).
– Xerostomia was significantly more frequent in patients with a history of diabetes mellitus and in female patients (P < 0.05).
– There were no statistically significant differences (P > 0.05) between patients with or without oral manifestations when age, gender, cardiovascular risk factor, cardiac disease, type of cardiac drug used or the number of medications were assessed.
Scott S. De Rossi, DMD Habbab KM1, Moles DR, Porter SR.Oral Dis. 2010 Nov;16(8):769-73.
Scott S. De Rossi, DMD
Introduction
• Many commonly prescribed medications have adverse oral sequelae
• Little scientific data as to the prevalence
• Dental and oral manifestations are often nonspecific and vary in significance
• Manifestations may mimic many disease processes (e.g. EM) while others are very characteristics (drug-induced gingival enlargement)
Scott S. De Rossi, DMD

3
Scott S. De Rossi, DMD
Introduction
• Many commonly prescribed medications have adverse oral sequelae
• Little scientific data as to the prevalence
• Dental and oral manifestations are often nonspecific and vary in significance
• Manifestations may mimic many disease processes (e.g. EM) while others are very characteristics (drug-induced gingival enlargement)
Scott S. De Rossi, DMD
Scott S. De Rossi, DMD
Oral manifestations of drugs are dependent on:
1. The type of drug
2. The drug dose
3. The chronicity of dosing
4. The variability in patient response
• Reactions may be immediate or develop over several weeks
Scott S. De Rossi, DMD
Etiology and pathogenesis of drug-induced oral reactions
Reactions generally result from one of two mechanisms:• Immune-mediated
– IgE-mediated reactions when the drug reacts with IgEantibodies bound to mast cells
– Drug-related cytotoxic reactions when antibodies bind to a drug attached to a cell surface
– Circulation of antigens for extended periods allowing for sensitization and antibody production
• Non-immune-mediated
– Drugs that directly affect cells leading to chemical mediator release and inflammation and cell death
Drug Actions/Interactions
• Therapeutic (desired) effects and adverse (unwanted) effects
• 81% of Americans take at least 1 medication routinely and many take >1
• 42% use at least 1 OTC medication
• 49% use at least 1 dietary supplement
• 29% use at least 5 medications concurrently
Scott S. De Rossi, DMD
Kauffman DW, et al. JAMA 2002.
Scott S. De Rossi, DMD

4
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
Scott S. De Rossi, DMD
Angioedema
• Common clinical presentation of a group of allergic conditions
• Previously known as “angioneurotic edema” because of a presumed psychologic or CNS stimulation
• Defined as rapid, painless swelling of the lips and adjacent structures after contact with an allergen or medication
Scott S. De Rossi, DMD
Angioedema
• Very concerning when posterior structures are involved (airway compromise)
• Upon cessation of contact with the suspected allergen, swelling subsides within 24-48 hrs
• Two forms: – Hereditary
– Acquired
Scott S. De Rossi, DMD
Hereditary Angioedema
• Rare autosomal dominant disorder• Deficiency in C1 esterase inhibitor (C1INH) of
the complement cascade – This innate immune response is the first line of
defense against invading microorganisms. This system is not specific for a given pathogen, but can aid in the induction of cell-mediated immunity (antibody and specific killer cells)
• Unlike the acquired form, swellings usually result from mild trauma
Scott S. De Rossi, DMD
Acquired Angioedema
• More common form and frequently the result of recent ingestion of a new medication or exposure to a chemical– May affect 10-20% of US population
• Although it can occur after long-term therapy
• Most cases are mediated by an IgE immune reaction (antibiotics)
• Some cases are non-immune mediated (NSAIDs)

5
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
Airway compromise with angioedema
6
Scott S. De Rossi, DMD
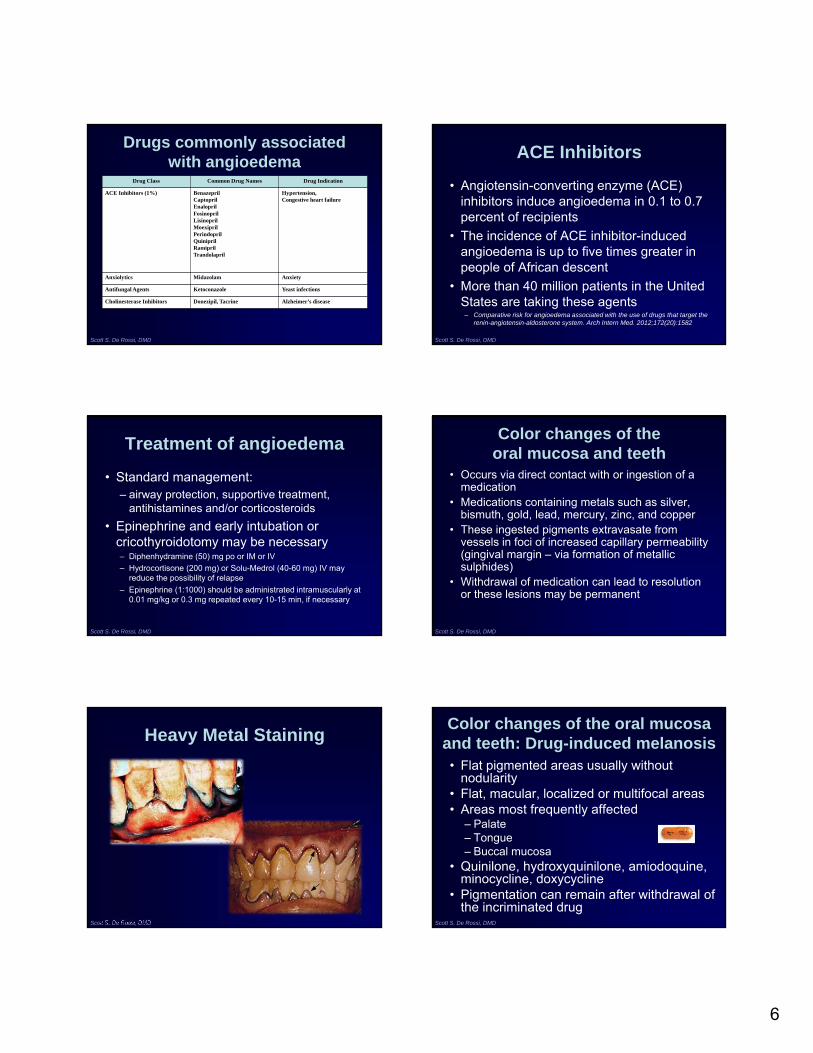
Drugs commonly associated with angioedema
Drug Class Common Drug Names Drug Indication
ACE Inhibitors (1%) BenazeprilCaptoprilEnaloprilFosinoprilLisinoprilMoexiprilPerindoprilQuiniprilRamiprilTrandolapril
Hypertension, Congestive heart failure
Anxiolytics Midazolam Anxiety
Antifungal Agents Ketoconazole Yeast infections
Cholinesterase Inhibitors Donezipil, Tacrine Alzheimer’s disease
ACE Inhibitors
• Angiotensin-converting enzyme (ACE) inhibitors induce angioedema in 0.1 to 0.7 percent of recipients
• The incidence of ACE inhibitor-induced angioedema is up to five times greater in people of African descent
• More than 40 million patients in the United States are taking these agents
– Comparative risk for angioedema associated with the use of drugs that target the renin-angiotensin-aldosterone system. Arch Intern Med. 2012;172(20):1582
Scott S. De Rossi, DMD
Scott S. De Rossi, DMD
Treatment of angioedema
• Standard management: – airway protection, supportive treatment,
antihistamines and/or corticosteroids
• Epinephrine and early intubation or cricothyroidotomy may be necessary– Diphenhydramine (50) mg po or IM or IV
– Hydrocortisone (200 mg) or Solu-Medrol (40-60 mg) IV may reduce the possibility of relapse
– Epinephrine (1:1000) should be administrated intramuscularly at 0.01 mg/kg or 0.3 mg repeated every 10-15 min, if necessary
Scott S. De Rossi, DMD
Color changes of the oral mucosa and teeth
• Occurs via direct contact with or ingestion of a medication
• Medications containing metals such as silver, bismuth, gold, lead, mercury, zinc, and copper
• These ingested pigments extravasate from vessels in foci of increased capillary permeability (gingival margin – via formation of metallic sulphides)
• Withdrawal of medication can lead to resolution or these lesions may be permanent
Heavy Metal Staining
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
Color changes of the oral mucosa and teeth: Drug-induced melanosis• Flat pigmented areas usually without
nodularity• Flat, macular, localized or multifocal areas• Areas most frequently affected
– Palate– Tongue– Buccal mucosa
• Quinilone, hydroxyquinilone, amiodoquine, minocycline, doxycycline
• Pigmentation can remain after withdrawal of the incriminated drug
7
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
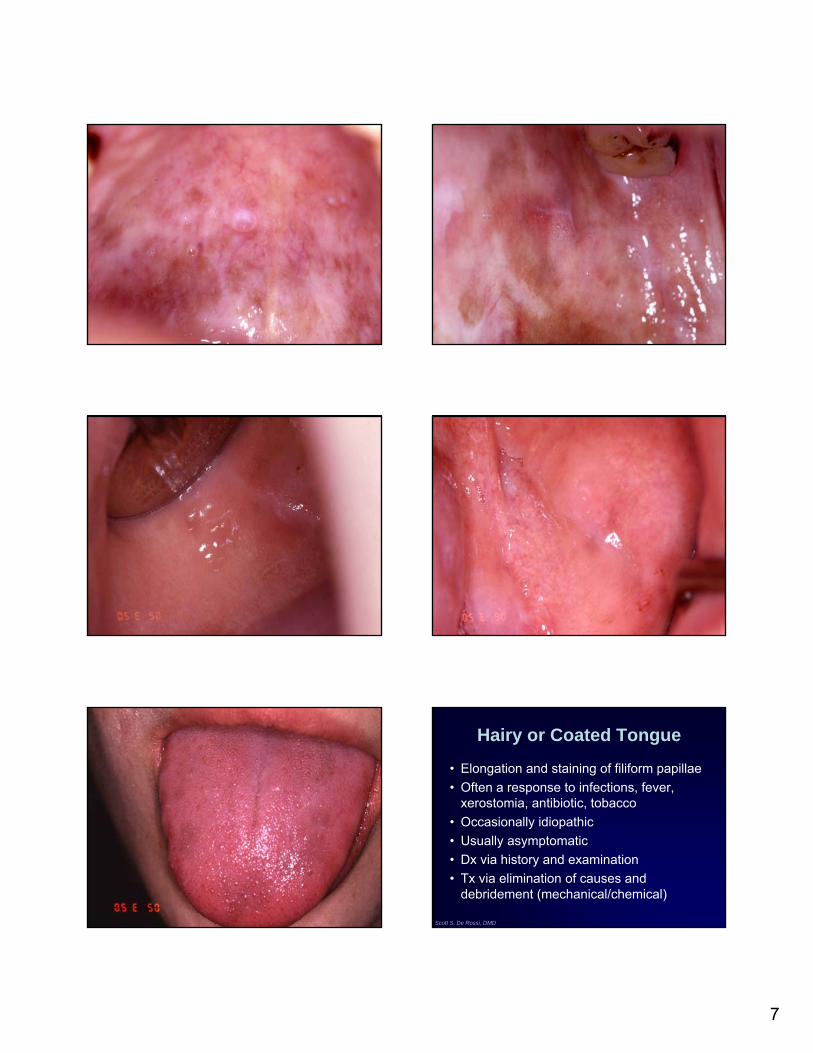
Hairy or Coated Tongue
• Elongation and staining of filiform papillae
• Often a response to infections, fever, xerostomia, antibiotic, tobacco
• Occasionally idiopathic
• Usually asymptomatic
• Dx via history and examination
• Tx via elimination of causes and debridement (mechanical/chemical)

8
Scott S. De Rossi, DMD
Elongation of filiform papillae
Scott S. De Rossi, DMD
Black/Brown Hairy Tongue
• Common condition of unknown etiology affecting the tongue dorsum
• Elongated papilla become pigmented by the colonization of chromogenic bacteria and extrinsic stains
• Can occur after ingestion of antibiotics or anti-diarrheals
• Treatment involves tongue brushing and scraping; eliminations of offending agent; and Dakin’s solution
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
Scott S. De Rossi, DMD Scott S. De Rossi, DMD

9
Scott S. De Rossi, DMD
Drugs commonly associated with color changes in the oral cavity
Drug Class Common Drug Names Drug Indication
Antidiarrheals Bismuth subsalicylate Acute diarrheaH. Pylori treatments
Centrally acting antihypertensives
Methyldopa Hypertension
Antibiotics Minocycline Bacterial infectionsPeriodontal diseasePemphigoidAcne
Oral Contraceptives Ethinyl estradiol/progestin combos
Birth controlDysmenorhhea
Antidysrythmics Quinidine Atrial fibrillation/flutterVentricular/supraventricular arrhythmia
Antivirals Zidovudine HIV infection
Scott S. De Rossi, DMD
Taste Disturbances
• Many medications induce abnormalities in taste by a yet to be understood process– Blunting or decreased taste (Hypoguesia)
– Total loss of taste (Aguesia)
– Distortion in the perception of a correct taste (Dysguesia)
• May manifest as an unusual, bitter, metallic, or change in taste perception or distaste
Scott S. De Rossi, DMD
Taste Disturbances
• Proposed mechanisms: – Interference with the chemical
composition or flow of saliva
– Direct effects on taste receptor function or signal transduction
• It does appear to be dose related
• Usually resolves with drug discontinuation
• May benefit from Zinc supplementation (220mg/day)
Scott S. De Rossi, DMD
Medications
• 0.12% chlorhexidine rinse has been reported to produce a reversible impairment of peripheral taste receptors
• Some medications cause alterations of specific tastes (sweet, bitter, salty, sour)
• Some increase taste or recognition thresholds
Medications
• Several drugs have been associated with total loss of taste:– local anesthetics (lidocaine), antineoplastics
(bleomycin), and antirheumatics(penicillamine)
• The mechanisms behind these effects are complex and not yet clearly defined, but medication-induced taste dysfunction can occur at any of the transport, sensory, or neuronal levels of the gustatory system
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
AntibioticsAmpicillinAzithromycin (Zithromax)Ciprofloxacin (Cipro)Clarithromycin (Biaxin)Griseofulvin (Grisactin)Metronidazole (Flagyl)Ofloxacin (Floxin)Tetracycline
AntidepressantsAmitriptyline (Elavil)Clomipramine (Anafranil)Desipramine (Norpramin)Doxepin (Sinequan)Imipramine (Tofranil)Nortriptyline (Pamelor)
Antihistamines and decongestantsChlorpheniramineLoratadine (Claritin)Pseudoephedrine
Antihypertensives and cardiac medicationsAcetazolamide (Diamox)Amiloride (Midamor)Betaxolol (Betoptic)Captopril (Capoten)Diltiazem (Cardizem)Enalapril (Vasotec)Hydrochlorothiazide (Esidix) and combinationsNifedipine (Procardia)NitroglycerinPropranolol (Inderal)Spironolactone (Aldactone)
AnticonvulsantsCarbamazepine (Tegretol)Phenytoin (Dilantin)
Anti-inflammatory agentsAuranofin (Ridaura)ColchicineDexamethasone (Decadron)Gold (Myochrysine)HydrocortisonePenicillamine (Cuprimine)
Antimanic drugLithium
AntineoplasticsCisplatin (Platinol)Doxorubicin (Adriamycin)Methotrexate (Rheumatrex)Vincristine (Oncovin)
Antiparkinsonian agentsLevodopa (Larodopa; with carbidopa: Sinemet)
AntipsychoticsClozapine (Clozaril)Trifluoperazine (Stelazine)
Antithyroid agentsMethimazole (Tapazole)Propylthiouracil
Lipid-lowering agentsFluvastatin (Lescol)Lovastatin (Mevacor)Pravastatin (Pravachol)
Muscle relaxantsBaclofen (Lioresal)Dantrolene (Dantrium)
Drugs that cause Taste Disorders

10
Scott S. De Rossi, DMD
Erythema Multiforme
• An acute inflammatory disease of the skin and mucous membranes
• Can cause a variety of lesions• Oral lesions – inflammation accompanied by
rapidly rupturing vesicles and bullae• Immune mediated process
– Initiated by deposition of immune complexes in the superficial microvasculature
– Direct cell-mediated toxicity
Scott S. De Rossi, DMD
Erythema Multiforme
• Skin lesions in 50% of cases
• Acute, multiple, ulcers involving any oral surface but usually sparing gingiva
• Lip crusting and “target lesions”
• Oral lesions– erythematous patches, necrosis,
erosions/ulcers
– hemmorhagic crusting of vermillion zone
Scott S. De Rossi, DMD
Erythema Multiforme
• Erythema multiforme major– Stevens-Johnson
– mortality = 2-10%
• Toxic epidermal necrolysis– older people with female predilection
– mortality = 34%
Scott S. De Rossi, DMD
Erythema Multiforme: diagnosis and treatment
• Non-specific histopathology
• Must be differentiated from HSV, lichen planus, pemphigoid, pemphigus
• Treatment– avoid known/suspected trigger
– supportive measures (analgesia, hydration, etc.)
– high dose steroids (prednisone 60-90mg/day)
– HSV prophylaxis for recurrent episodes
Scott S. De Rossi, DMD Scott S. De Rossi, DMD

11
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
Scott S. De Rossi, DMD Scott S. De Rossi, DMD

12
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
Medications associated with erythema multiforme
Drug Class Common Drug Names Drug Indication
Antiarthritic agents Allopurinol Gouty arthritisLeukemia associated gout
Antibiotics ClindamycinPenicillin V potassiumTetracycline
Bacterial infections
Anticonvulsant agents Carbamazepine Seizure disordersDepressionTrigeminal neuralgia
Antiviral agents Acyclovir Herpes infection/suppression
Barbituates PentobarbitalPhenobarbitalSecobarbital
Antianxiety/sedative hypnoticsAnticonvulsant
Non Steroidal Antiinflammatory Drugs
Phenylbutazone Pain and inflammation
Sulfonamides SulfacytineSulfamethizoleSulfamethoxazoleSulfisoxazole
Bacterial infections
Scott S. De Rossi, DMD
Medication-induced Gingival Enlargement/Overgrowth
• Formerly known as “gingival hyperplasia”
• Diffuse enlargement due to increase of the fibrous component of the gingiva
• Associated with normal color usually
• Local factors are ALWAYS an etiologic factor– Fibroblasts in non-inflamed tissue are less
likely to respond to circulating drugs
Histology
Scott S. De Rossi, DMD
Scott S. De Rossi, DMD
Medication-induced Gingival Enlargement
• Phenytoin– mast cell mediated androgen activity
• Calcium channel blockers– inhibit adherence and lipopolysaccharide-
stimulated/macrophage-induced fibroblast death
• Cyclosporine– increases fibroblast production of collagen
and matrix
Scott S. De Rossi, DMD
Treatment of drug-induced gingival enlargement
• Lesions do not resolve with drug withdrawal
• Aggressive oral hygiene
• Frequent recall maintenance
• Treatment with gingivectomy
• Explore alternative drug therapy

13
Scott S. De Rossi, DMD
Mild nifedipine induced GH
Scott S. De Rossi, DMD
Scott S. De Rossi, DMD
Moderate
Scott S. De Rossi, DMD
Scott S. De Rossi, DMD
Severe
Scott S. De Rossi, DMD

14
Scott S. De Rossi, DMD
Medications known to cause gingival overgrowth
Drug Class Common Drug Names Drug Indication
Anticonvulsants Phenytoin Epilepsy/seizures
Calcium channel blockers DiltiazemFelodipineNifedipineNisoldipineVerapamil
HypertensionRaynaud’s phenomenon
Immunosuppressive agents Cyclosporin AMycophenelate mofetil
Organ transplant rejectionMucocutaneous disease
Scott S. De Rossi, DMD
Lichen Planus/Lichenoid Rxn
• Common dermatologic disease of skin and mucous membranes
• Middle-aged adults; 60% women• Prevalence of oral LP = 0.1-2.2%• Chronic, multiple lesions• Various forms:
– Reticular/Wickham’s striae - asymptomatic– Plaque-like - asymptomatic– Bullous/erosive/ulcerative - symptomatic
Scott S. De Rossi, DMD
Lichenoid drug reactions
• Exhibit similar clinical and histological findings as ‘idiopathic’ LP
• Usually two distinguishing factors– The association with the administration of a
drug, contact with metal, foodstuff, or systemic disease
– Their resolution when the offending agent is eliminated
Scott S. De Rossi, DMD
Etiology of Lichen Planus
• Immune mediated - T cell mediated degeneration of the basal cell layer of epithelium
• Associated with stress, drug hypersensitivity (lichenoid drug reaction), or infection (HCV)– NSAIDs, allopurinol, sulfonamides, tetracyclines, ACE
inhibitors, HCTZ, lorazepam, sulfonylureas
– dental materials• amalgam and resins
– idiopathic
Scott S. De Rossi, DMD
EPITHELIUM
CONNECTIVETISSUE
PRIMARYRESPONSE
SECONDARYRESPONSE
LYMPH NODE
LC
CAPILLARIES
HYPERSENSITIVITYREACTIONS
CYTOKINERELEASE
T-CELLRECIRCULATION
T-CELLSENSITIZATION
Scott S. De Rossi, DMD

15
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
Scott S. De Rossi, DMD Scott S. De Rossi, DMD

16
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
Topical Corticosteroids Preparations: treatment of lichenoid reactions
• Flucinonide gel (Lidex) 0.05%
• Betamethasone (Diprolene) gel 0.05%
• Clobetasol(Temovate) gel 0.05%
• Dexamethasone rinse 0.5mg/5cc

17
Scott S. De Rossi, DMD
Intralesional GCS injection
Triamcinolone 5-40mg/cc - inject 0.1cc per cubic cm
Scott S. De Rossi, DMD
Scott S. De Rossi, DMD
Medications known to induce lichenoid reactions
Drug Class Common Drug Names Drug Indication
Antiarthritic agents Allopurinol Gouty arthritisLeukemia associated gout
Beta adrenergic antagonists Propranolol HypertensionCongestive heart failureMigraine prophylaxisDysrhthymia
ACE Inhibitors Captopril HypertensionCongestive heart failure
Oral hypoglycemic agents Chlorpropamide Type 2 diabetes
Centrally acting agents Methyldopa Hypertension
Duiretics FurosemideThiazides
HypertensionPeripheral edema
Non-Steroidal Anti-inflammatory Drugs
DiflusinalFlurbiprofenIbuprofen
PainInflammation
Medication-induced Xerostomia
• 80% of the most commonly prescribed medications have been reported to cause xerostomia
• Xerostomic drugs can be found in 42 drug categories and 56 sub-categories
• Most drugs do not cause damage to glands• DIX is a transient symptom• Inhibitory effects can be overcome with
gustatory stimulation
Medication-induced Xerostomia
• Drugs which directly damage salivary glands (e.g. anti-neoplastics)
• Drugs with anticholinergic activity (e.g. antihistamines)
• Drugs acting on sympathetic system (e.g. alpha 1 antagonists)
• Drugs that deplete fluid (e.g. diuretics)
Myth Vs. Reality
• TCAs are potent inhibitors of salivation that act on muscarinic-cholinergic receptors
• Alpha adrenergic antagonists consistently cause hyposalivation
• Beta blockers and ACE inhibitors cause neither hyposalivation nor xerostomia
• Diuretics cause xerostomia but not hyposalivation
Scott S. De Rossi, DMDNapenas J. Odonotol 2009.
18
Scott S. De Rossi, DMD
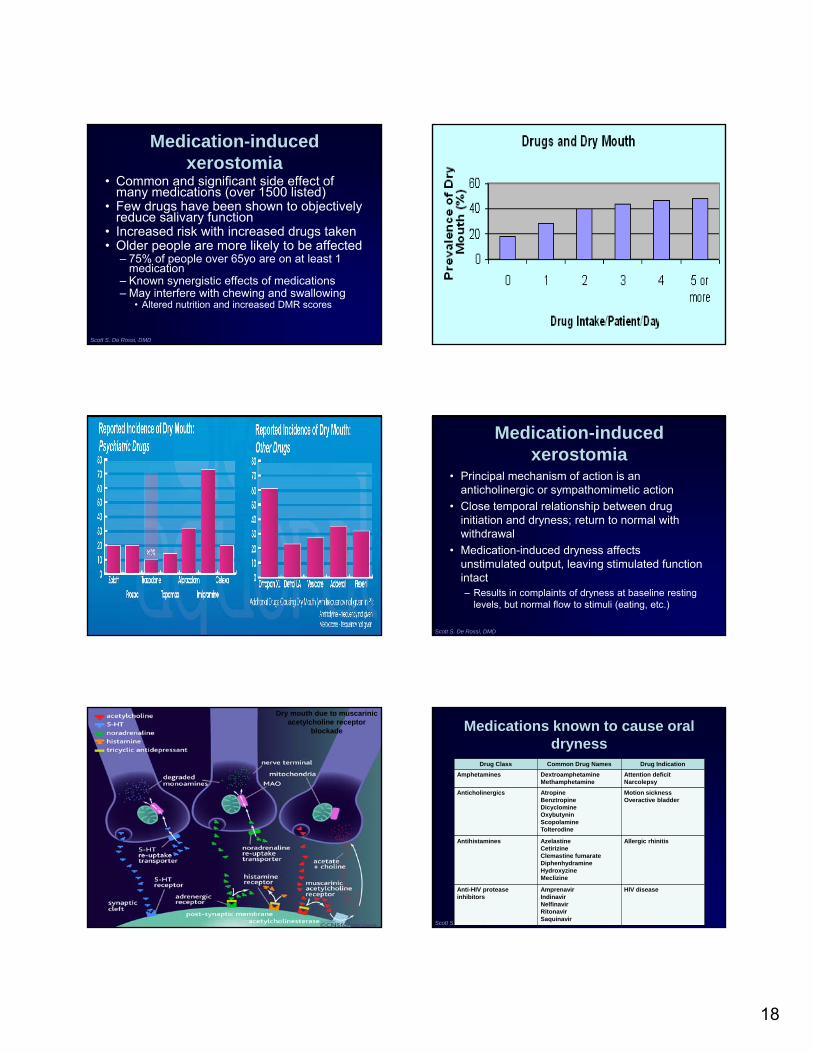
Medication-induced xerostomia
• Common and significant side effect of many medications (over 1500 listed)
• Few drugs have been shown to objectively reduce salivary function
• Increased risk with increased drugs taken• Older people are more likely to be affected
– 75% of people over 65yo are on at least 1 medication
– Known synergistic effects of medications– May interfere with chewing and swallowing
• Altered nutrition and increased DMR scores
Scott S. De Rossi, DMD
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
Medication-induced xerostomia
• Principal mechanism of action is an anticholinergic or sympathomimetic action
• Close temporal relationship between drug initiation and dryness; return to normal with withdrawal
• Medication-induced dryness affects unstimulated output, leaving stimulated function intact– Results in complaints of dryness at baseline resting
levels, but normal flow to stimuli (eating, etc.)
Scott S. De Rossi, DMD
Dry mouth due to muscarinicacetylcholine receptor
blockade
Scott S. De Rossi, DMD
Medications known to cause oral dryness
Drug Class Common Drug Names Drug Indication
Amphetamines DextroamphetamineMethamphetamine
Attention deficitNarcolepsy
Anticholinergics AtropineBenztropineDicyclomineOxybutyninScopolamineTolterodine
Motion sicknessOveractive bladder
Antihistamines AzelastineCetirizineClemastine fumarateDiphenhydramineHydroxyzineMeclizine
Allergic rhinitis
Anti-HIV protease inhibitors
AmprenavirIndinavirNelfinavirRitonavirSaquinavir
HIV disease

19
Scott S. De Rossi, DMD
Medications known to cause oral dryness
Drug Class Common Drug Names Drug Indication
Selective serotonin reuptake inhibitors
CitalopramFluoxetineParoxetineSertraline
Depressions/anxietyPanic disorderObsessive compulsiveEating disorder
Tricyclic antidepressants AmitriptylineDesipramineDoxepinImipramineNortriptyline
Depressions/anxietyNocturnal enuresisChronic pain/TMDBurning mouth syndrome
Add lobulated tongue image
Scott S. De Rossi, DMD
Scott S. De Rossi, DMD
Diagnosing dry mouth
Scott S. De Rossi, DMD
Navazesh M. JADA 2003
Some Simple Questions
• Does the amount of saliva in your mouth seem to be too little? Too much? Don’t notice?
• Do you have any difficulty swallowing?
• Does your mouth feel dry when eating a meal?
• Do you sip liquids to aid in swallowing dry food?– Fox P. et al 1997
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
A simple clinical test to assess dryness – the ‘tongue blade test’• Place dry tongue
blade on against buccal mucosa
• Adherence of the tissue to the blade indicates tissue dryness and reduced salivary secretion

20
Scott S. De Rossi, DMD
Complications of xerostomia
• Caries
• Periodontal and gingival disease
• Mucosal abnormalities
• Halitosis
• Candidiasis
• Poor quality of life
Management of Dry Mouth
• After establishing a diagnosis, a step-wise management approach is implemented
• Five goals of management:1. Alleviating symptoms
2. Instituting preventive measures
3. Treating oral conditions
4. Improving salivary function (if possible)
5. Managing underlying systemic conditions
Scott S. De Rossi, DMD
Scott S. De Rossi, DMD
Systemic Strategies: Cholinergic drugs
• Parasympathomimetic stimulating agents to increase salivary production
• Require functioning glands
• GI, sweat, and cardiac side effects
• May alter cardiac conduction and should be avoided in patients with significant heart disease, asthma, and narrow angle glaucoma
Scott S. De Rossi, DMD
CevimelinePilocarpine
Scott S. De Rossi, DMD
Drug-induced Pemphigus

21
Scott S. De Rossi, DMD
Types of Pemphigus
• Vulgaris
• Vegetans
• Foliaceus
• Erythematosus
• Paraneoplastic pemphigus
• Drug-induced pemphigus
Scott S. De Rossi, DMD
Drug-induced pemphigus
• A drug origin should be considered with all new pemphigus patients
• Pemphigus foliaceous and vulgaris are the most common drug induced types
• Causative drugs can be classified intotwo groups:– Thiol drugs – Non-thiol drugs
Scott S. De Rossi, DMD
Drug-induced pemphigus
• Proposed mechanism:– Drugs induce antibody formation, resulting in
acantholysis via a mechanism identical to idiopathic pemphigus (non-thiol drugs)
– Other drugs induce acantholysis directly in the absence of antibody formation
• Although eosinophilic spongiosis is often present, it is not possible to distinguish them based on histologic features alone
Scott S. De Rossi, DMD
Binding of IgG autoantibodies to Desmoglein 3 on desmosomes.
Steric hindrance leads to loss of cell-to-cell adhesion resulting in blister formation.
Epithelial changes occur as a result of intercellular cement, widening of intercellular spaces, demosome destruction and cellular degeneration.
Scott S. De Rossi, DMD
Clinical Manifestations
• Classic lesion - thin-walled bulla arising on otherwise normal skin or mucosa
• Applying pressure to an intact area results in new lesion formation = Nikolsky sign
• 80-90% of patients develop oral lesions• 60% develop oral lesions as first sign • Shallow, irregular ulcers because of rapid
bullae rupture
Scott S. De Rossi, DMD

22
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
Scott S. De Rossi, DMD
Treatment
• Removal of the offending drug
• Most, but not all patients go into remission once the offending agent is stopped
• Systemic corticosteroids– Prednisone (0.5-2 mg/kg/day)
– Immunosuppressive therapy• Mycophenelate mofetil, azathioprine,
cyclophosphamide
Scott S. De Rossi, DMD
Antiresorptive Related Osteonecrosis (ARONJ):
• Since 2003 reports of BON associated with the use of zoledronic acid (Zometa) and pamidronate (Aredia) have appeared in the literature– intravenous bisphosphonates administered
every three to four weeks to treat certain cancers (primarily multiple myeloma and metastatic bone, breast or prostate cancer) and Paget’s disease of bone
• Some reports of BON related to po drugs

23
Scott S. De Rossi, DMD
Bisphosphonate-associated osteonecrosis
• Complication of cancer treatment
• Oral lesions similar in appearance to ORN
• Appear as ragged oral ulcerations that expose underlying bone
• Occasionally extremely painful
• Persistent and do not respond to traditional treatments
Scott S. De Rossi, DMD
Bisphosphonate-Induced Jaw Osteonecrosis
Ruggiero SL et al, J Oral Maxillofac Surg. 2004;62:527-34
Bisphosphonates - For the treatment of:• Hematological malignancies• Cancer metastasis to bone• Osteoporosis
Long term I.V Bisphosphonates ( Aredia™ and Zometa™)
Jaw osteonecrosis•Chronic bone devitalization•Tissue dehiscence•Radiolucency •Hypocellularity
Scott S. De Rossi, DMD
Bisphosphonates
• Used to treat osteoporosis, Paget’s disease of bone, and hypercalcemia of malignancy
• Goal: to arrest bone loss and increase bone density and reduce risk of pathologic fracture
• PO bisphosphonates are mostly used with osteoporosis
• Injectable bisphosphonates are used in cancer patients with primary or metastatic bone lesions
• More than 150 million prescriptions were dispensed to outpatients between 2005 and 2009– Whitaker M. NEJM 2102.
Scott S. De Rossi, DMD
Scott S. De Rossi, DMD
Bisphosphonates
• Potent inhibitors of osteoclast activity
• Accumulate in mineralized bone matrix
• Physiologic bone deposition and remodelling are severely compromised
Denosumab (Prolia, Xgeva)
• Monoclonal antibody with high affinity to RANK ligand which prevents the interaction of RANK ligand with its receptor, RANK, which is present on the surface of osteoclasts and their precursors.
• Denosumab thus inhibits osteoclast activity, thereby decreasing bone resorption in trabecular and cortical bone.
• Cases of ONJ develop quickly – within a few weeks
Scott S. De Rossi, DMD

24
Antiangiogenics
• Indirectly affect bone remodeling
• Sunitinib– Advanced renal cell Ca, pancreatic neuroendocrine
tumors
• Sorafenib – no cases reported yet– Hepatocellular Ca, advanced renal cell Ca
• Bevaacizumab– VEGF pathway inhibitor
– Metastatic colorectal;, advanced nonsquamous small-cell lung, metastatic kidney, glioblastoma
Scott S. De Rossi, DMD
Saad F et al. Ann Oncol 2011;annonc.mdr435
© The Author 2011. Published by Oxford University Press on behalf of the European Society for Medical Oncology. All rights reserved. For permissions, please email: [email protected]
Incidence, risk factors, and outcomes of osteonecrosis of the jaw: integrated analysis from three blinded active-controlled phase III trials in cancer patients with bone metastases
Cumulative incidence of ONJ. The crude incidence of ONJ reported for month 0–12, 0–24, and 0–36.
Saad F et al. Ann Oncol 2011;annonc.mdr435
© The Author 2011. Published by Oxford University Press on behalf of the European Society for Medical Oncology. All rights reserved. For permissions, please email: [email protected]
Efficacy of Antiresorptives
• Very effective
• Life saving medications
• Cut vertebral fracture rate by 70% and the hip fracture rate by 50%
Scott S. De Rossi, DMD
Rev. Bras. Reumatol. vol.51 no.4 São
Paulo July/Aug. 2011
Long-Term Efficacy against Fracture for Three Bisphosphonates in Core Registration and Extension Studies.
Whitaker M et al. N Engl J Med 2012;366:2048-2051.
Scott S. De Rossi, DMD
25
Scott S. De Rossi, DMD
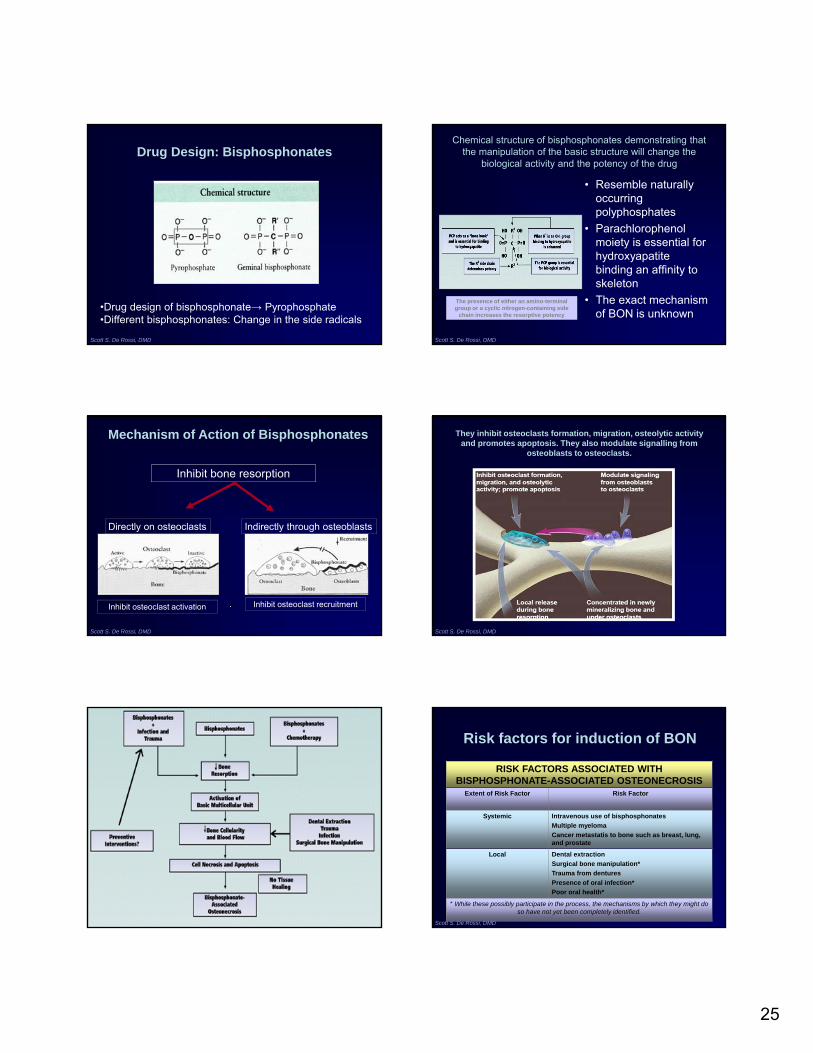
Drug Design: Bisphosphonates
•Drug design of bisphosphonate→ Pyrophosphate•Different bisphosphonates: Change in the side radicals
Scott S. De Rossi, DMD
Chemical structure of bisphosphonates demonstrating that the manipulation of the basic structure will change the
biological activity and the potency of the drug
• Resemble naturally occurring polyphosphates
• Parachlorophenol moiety is essential for hydroxyapatite binding an affinity to skeleton
• The exact mechanism of BON is unknown
The presence of either an amino-terminal group or a cyclic nitrogen-containing side
chain increases the resorptive potency
Scott S. De Rossi, DMD
This image cannot currently be displayed.
Mechanism of Action of Bisphosphonates
Inhibit bone resorption
Directly on osteoclasts Indirectly through osteoblasts
Inhibit osteoclast activation Inhibit osteoclast recruitment
They inhibit osteoclasts formation, migration, osteolytic activity and promotes apoptosis. They also modulate signalling from
osteoblasts to osteoclasts.
Scott S. De Rossi, DMD
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
Risk factors for induction of BON
RISK FACTORS ASSOCIATED WITH BISPHOSPHONATE-ASSOCIATED OSTEONECROSIS
Extent of Risk Factor Risk Factor
Systemic Intravenous use of bisphosphonates
Multiple myeloma
Cancer metastatis to bone such as breast, lung, and prostate
Local Dental extraction
Surgical bone manipulation*
Trauma from dentures
Presence of oral infection*
Poor oral health*
* While these possibly participate in the process, the mechanisms by which they might do so have not yet been completely identified.

26
Scott S. De Rossi, DMD
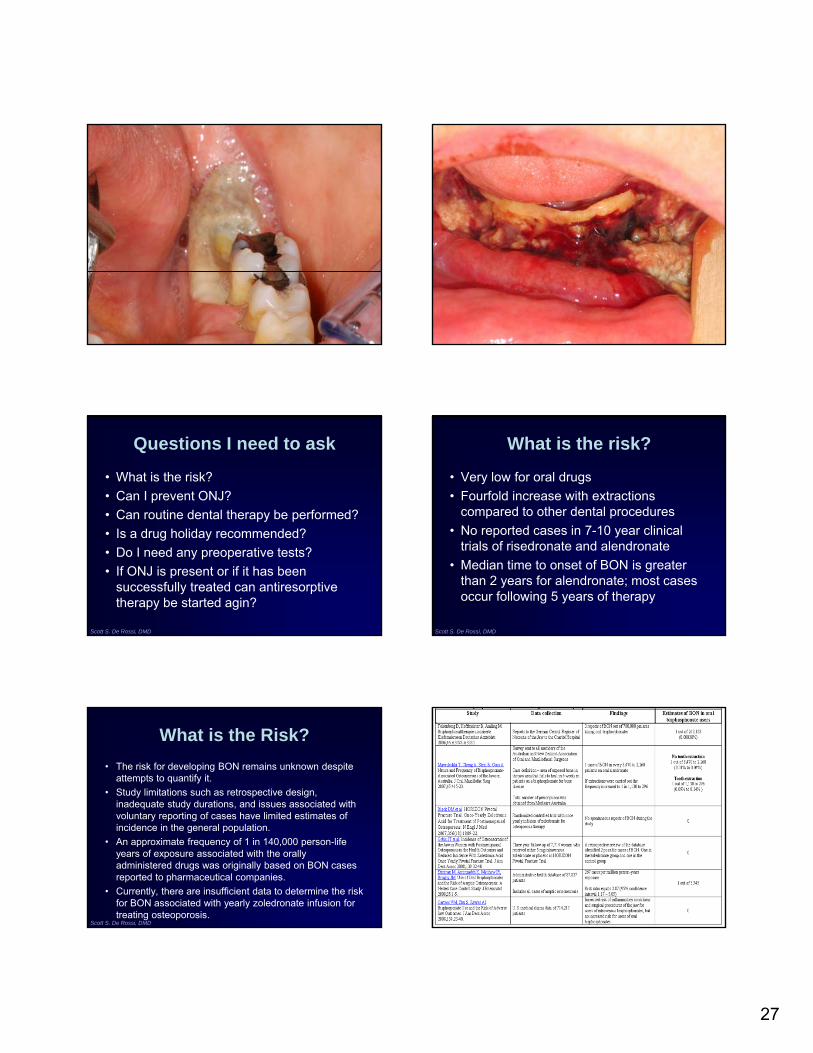
Clinical signs and symptoms of BON
• Absent or delayed hard- and soft-tissue healing following extraction or trauma induced by prosthodontic appliances
• No radiographic changes early!• Severe pain as necrotic bone becomes secondarily
infected• Progressive – leading to extensive areas of bony
exposure and dehiscence• Can occur spontaneously!
Scott S. De Rossi, DMD
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
27
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
Questions I need to ask
• What is the risk?
• Can I prevent ONJ?
• Can routine dental therapy be performed?
• Is a drug holiday recommended?
• Do I need any preoperative tests?
• If ONJ is present or if it has been successfully treated can antiresorptivetherapy be started agin?
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
What is the risk?
• Very low for oral drugs
• Fourfold increase with extractions compared to other dental procedures
• No reported cases in 7-10 year clinical trials of risedronate and alendronate
• Median time to onset of BON is greater than 2 years for alendronate; most cases occur following 5 years of therapy
What is the Risk?
• The risk for developing BON remains unknown despite attempts to quantify it.
• Study limitations such as retrospective design, inadequate study durations, and issues associated with voluntary reporting of cases have limited estimates of incidence in the general population.
• An approximate frequency of 1 in 140,000 person-life years of exposure associated with the orally administered drugs was originally based on BON cases reported to pharmaceutical companies.
• Currently, there are insufficient data to determine the risk for BON associated with yearly zoledronate infusion for treating osteoporosis.
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
28
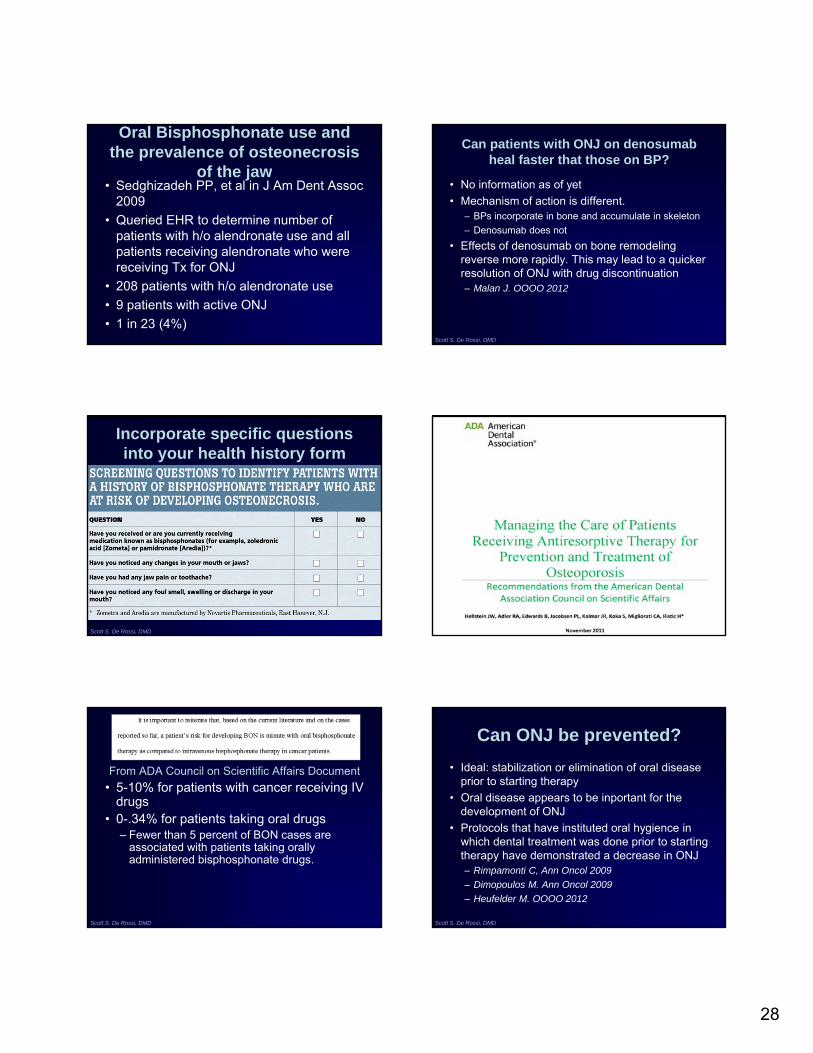
Oral Bisphosphonate use and the prevalence of osteonecrosis
of the jaw• Sedghizadeh PP, et al in J Am Dent Assoc
2009
• Queried EHR to determine number of patients with h/o alendronate use and all patients receiving alendronate who were receiving Tx for ONJ
• 208 patients with h/o alendronate use
• 9 patients with active ONJ
• 1 in 23 (4%)
Can patients with ONJ on denosumabheal faster that those on BP?
• No information as of yet
• Mechanism of action is different.– BPs incorporate in bone and accumulate in skeleton
– Denosumab does not
• Effects of denosumab on bone remodeling reverse more rapidly. This may lead to a quicker resolution of ONJ with drug discontinuation– Malan J. OOOO 2012
Scott S. De Rossi, DMD
Incorporate specific questions into your health history form
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
Scott S. De Rossi, DMD
From ADA Council on Scientific Affairs Document
• 5-10% for patients with cancer receiving IV drugs
• 0-.34% for patients taking oral drugs– Fewer than 5 percent of BON cases are
associated with patients taking orally administered bisphosphonate drugs.
Can ONJ be prevented?
• Ideal: stabilization or elimination of oral disease prior to starting therapy
• Oral disease appears to be inportant for the development of ONJ
• Protocols that have instituted oral hygience in which dental treatment was done prior to starting therapy have demonstrated a decrease in ONJ– Rimpamonti C, Ann Oncol 2009
– Dimopoulos M. Ann Oncol 2009
– Heufelder M. OOOO 2012
Scott S. De Rossi, DMD

29
Predicting Risk
• A major goal in the prevention of BON is to limit the possibility of extensive or multifocal involvement.
• OK to proceed conservatively in some cases– Determine how a patient will heal in a relatively small region
before putting multiple quadrants at risk.
• After establishing the patient’s apparent adequate healing response a more accelerated surgical treatment plan involving multiple sextants at a single appointment could be considered.
Scott S. De Rossi, DMD
CTX testing and drug holidays
• Recently, the use of serum levels of the collagen breakdown product, C-terminal cross-linking telopeptide of type I collagen (CTX), has been advocated as a risk predictor for developing BON.
• Serum CTX and urinary N telopeptide of type I collagen (NTX) are considered markers for bone resorption.
• Higher levels of these markers are associated with active bone turnover.
• Reports suggest that dental treatment decisions should be based on the results of serum CTX/NTX levels.
Scott S. De Rossi, DMD
CTX testing and drug holidays
• These recommendations are derived from clinical observations at one institution that have not been validated. – It remains to be seen if these recommendations will be
corroborated by well-controlled, randomized clinical trials.
• Recognized value of predicting and mitigating the risk for developing BON in individual patients.
• Until objective research studies document and correlate specificity, predictive value and reliability of such tests, no recommendations can be made.
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
Laboratory Assessment
• CTx: serum test to evaluate bone turnover• C-terminal cross-linked telopeptide• Limited scientific data regarding its use as
a predictor of adverse events– R. Marx (1 study – 25 patients)
• CTx < 100pg/ml = high risk of BIONJ• CTx 100-150pg/ml = moderate risk• CTx > 150pg/ml = minimal to no risk
• Not a validated test to predict risk!
CTX biochemical marker of bone metabolism. Is it a reliable predictor of bisphosphonate-associated
osteonecrosis of the jaws after surgery? Implant Dent. 2009 Dec;18(6):492-500.
• Lee, et al. examine the scientific basis (validity) of the morning fasting serum CTX test in 163 consecutive patients who underwent various oral surgery procedures in the office.
• The authors also review the laboratory test results and the recommended protocol based on the test values.
• One hundred sixty-three patients (mean age, 75.9 years) were divided into 2 groups.
• Group I was the control group that consisted of 109 patients taking oral BPs who did not take the CTX test preoperatively. Group 2 consisted of 54 patients taking BPs and who elected to have the CTX test performed to assess their level of risk of developing ONJ, preoperatively.
• Both groups of patients were observed for a period of 8 weeks for signs and symptoms of BP-associated ONJ after surgery. The clinical data at 8 weeks and beyond revealed that there was no evidence of BP-associated ONJ in all participants.
• We conclude that the serum CTX is not a valid preoperative test to accurately assess the level of risk of developing ONJ and is not indicated in the oral surgery patient.
Serologic bone markers for predicting development of osteonecrosis of the jaw in patients receiving
bisphosphonatesJ Oral Maxillofac Surg. 2010 Sep;68(9):2241-7.
• Lazarovici TS, etal.• Data on the demographics, comorbidities, and BP
treatment were collected from 78 patients scheduled for dentoalveolar surgery. Of the 78 patients, 51 had been treated with oral BPs and 27 had been treated with frequent intravenous infusions of BPs. Blood samples for CTX, bone-specific alkaline phosphatase, and parathyroid hormone measurements were taken preoperatively. Surgery was performed conservatively, and antibiotic medications were prescribed for 7 days.
• Conclusion: The measurement of serum levels of CTX is not a definitive predictor of the development of BRONJ

30
Is a drug holiday a valid alternative?
• What is the rationale?
• Does the type of antiresorptive matter?Mostpatients now come to us for ONJ treatment when drug has been discontinued
• Risk of skeletal complications versus benefit of oral treatment
• Discontinuation of BP did not affect outcomes– Vrade M. JOMS 2011
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
General Recommendations
• Routine dental care should not be modified solely based on use of bisphosphonates
• Comprehensive examination prior to initiation of bisphosphonate therapy
• Inform patients BON can occur in response to dental disease or dental therapy
Scott S. De Rossi, DMD
Patients should be informed that:
Scott S. De Rossi, DMD
AAOMS Staging Criteria
Scott S. De Rossi, DMD
People taking bisphosphonates are often unfamiliar with the drug and its side effects
Bisphosphonate information provided by patients
YES NO or UNSURE
Reason for taking bisphosphonate? 84% 16%
How long are you going to be on therapy? 20% 80%
Informed about the risks or side effects? 18% 82%
Informed about bone densityimprovement?
30% 70%
Scott S. De Rossi, DMD
Miglorati CA, et al. JADA 2010
Dentists must be prepared to educate patients about the risks of developing oral complications from bisphosphonate use and the need for appropriate dental care!

31
Scott S. De Rossi, DMD Scott S. De Rossi, DMD
Consent for Treatment