the ntrc protocol - spectrum learning biomedical... · the ntrc protocol: a logical sequencing ......
TRANSCRIPT

The NTRC Protocol:A logical sequencing of biomedical interventions for the
treatment of autism and related disorders.
DR SUNDARDAS D. ANNAMALAYBSc (Phys) (S’pore), ND (Aust,USA), MD (MA), DSc (Sri Lanka),
PhD, MIFHI, FUNM (USA)
Naturopathic Physician, Functional Medicine Specialist,Acupuncturist, Homoeopath,Clinical Nutritionist
CEO, Sundardas Naturopathic Clinic Pte Ltd
Professor, Naturopathic Medicine (YINS Colleges Worldwide,Aust,.USA)
Visiting Professor, Open International University for ComplementaryMedicine (Sri Lanka)
NEUROFEEDBACK CONFERENCE JAN 2014
BIOLOGICALMODIFICATIONS
Positively impact children’slives by meeting their
biological, behavioral, andnutritional needs.

Toddler HIBToddler HIB
Infant HIB
PREVALENCE
Mandatroy 15 mo. MMR
Voluntary Childhood Measles
NewbornHep B

Dev. Delay PREVALENCE = 541,000 ages 5 & under = 2.4%Dev. Delay PREVALENCE = 541,000 ages 5 & under = 2.4%
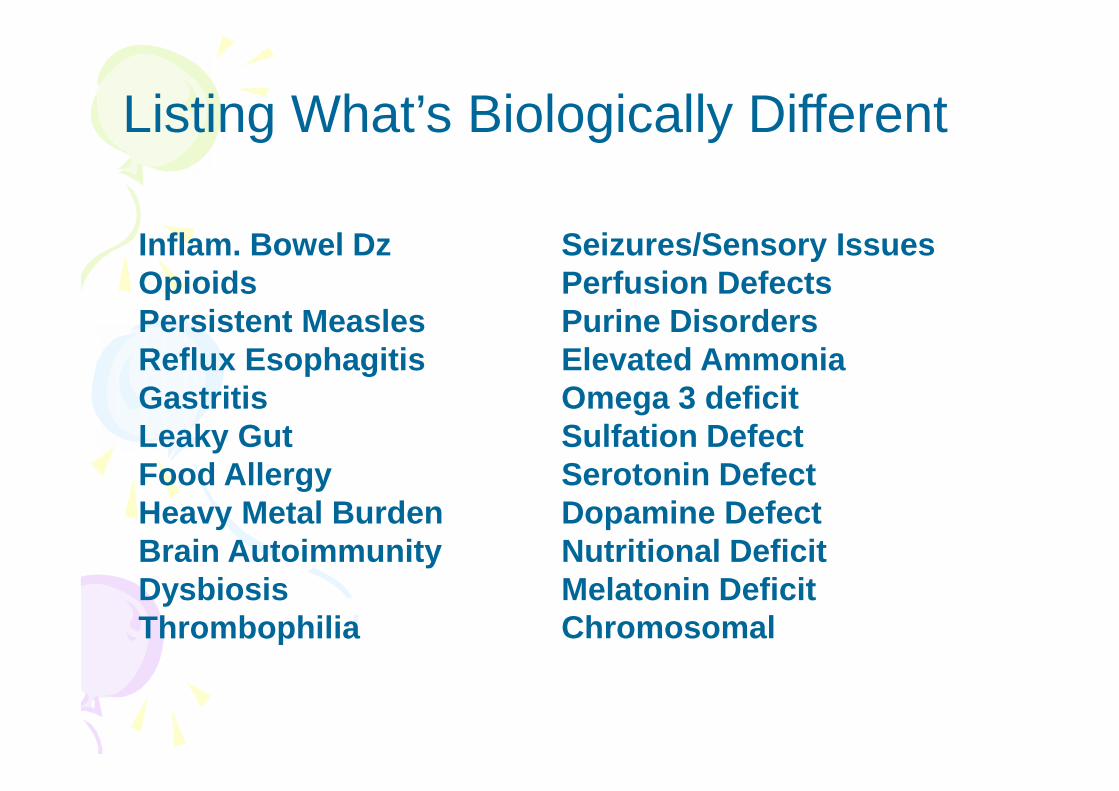
Listing What’s Biologically Different
Inflam. Bowel DzOpioidsPersistent MeaslesReflux EsophagitisGastritisLeaky GutFood AllergyHeavy Metal BurdenBrain AutoimmunityDysbiosisThrombophilia
Seizures/Sensory IssuesPerfusion DefectsPurine DisordersElevated AmmoniaOmega 3 deficitSulfation DefectSerotonin DefectDopamine DefectNutritional DeficitMelatonin DeficitChromosomal

Known factors in ASD
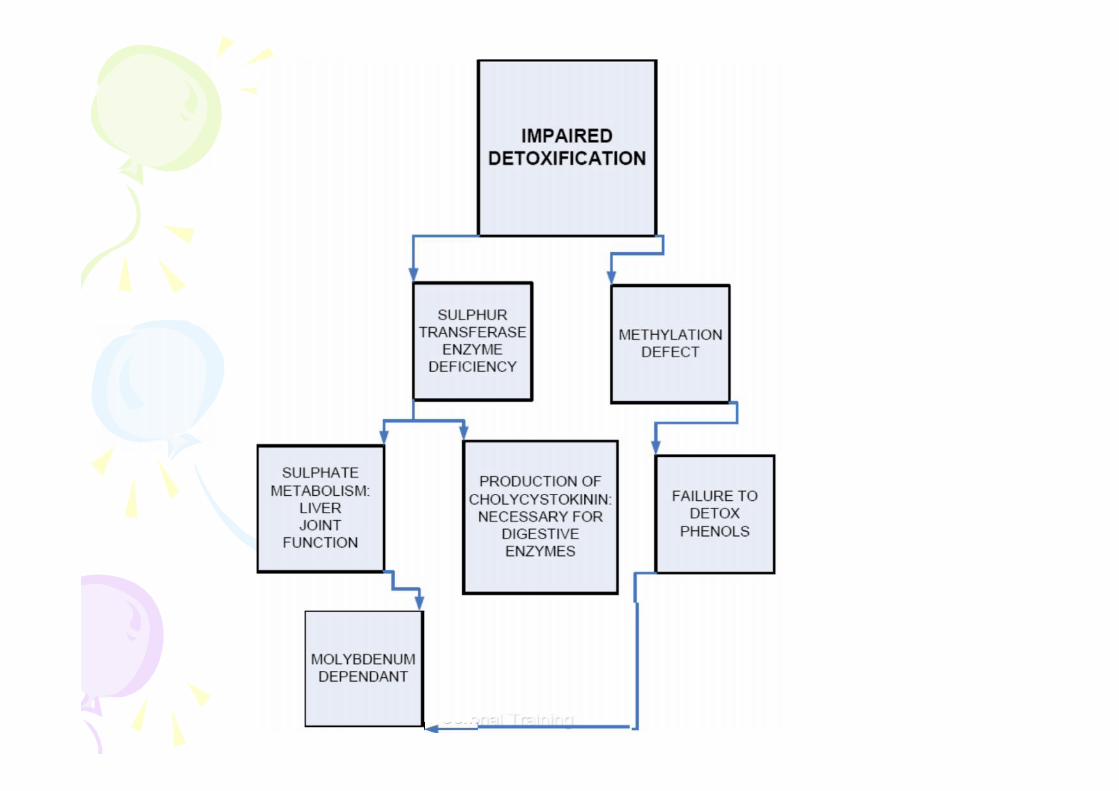
• Impaired detoxification pathways especially insulphation and methylation pathways
• Increased oxidative stress
• Disruption of gut function
• Abnormal gut permeability possibly followingincreased use of antibiotics
• Disruption of immune function
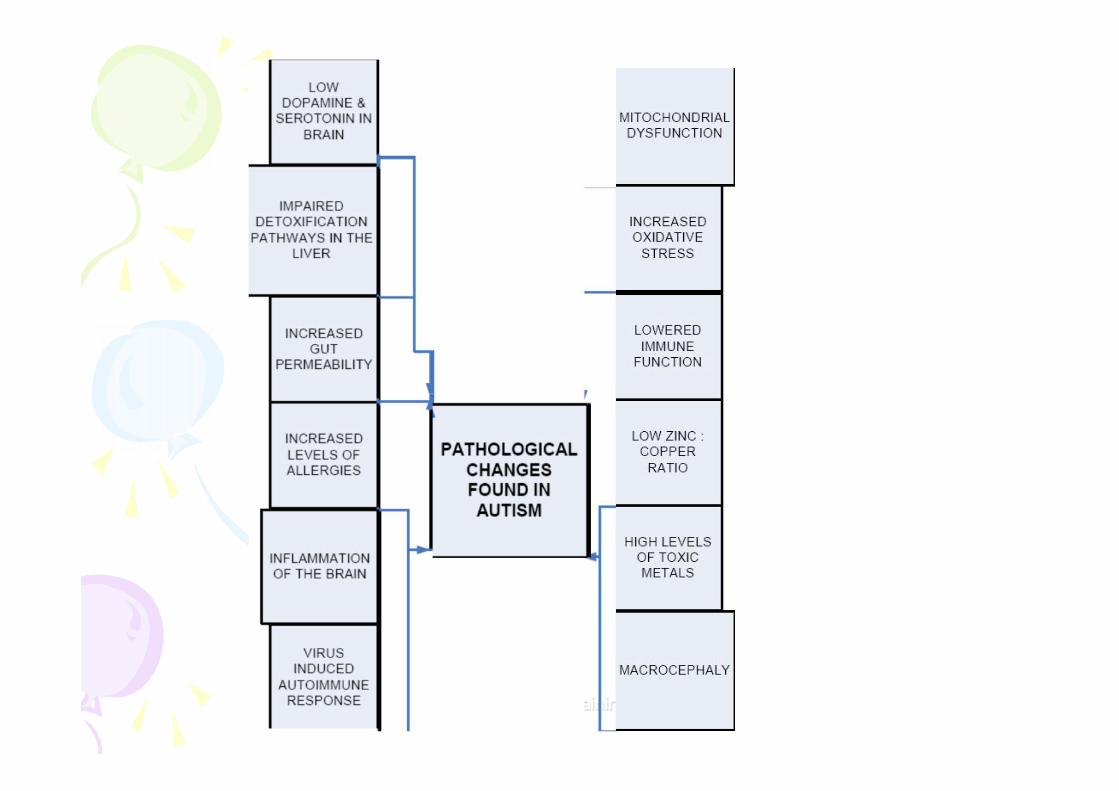
Known factors in ASD
• mitochondrial dysfunction with associated defects inneuronal oxidative phosphorylation within the centralnervous system.
– This hypothesis is supported by a frequent associationof lactic acidosis and carnitine deficiency in autisticpatients.
– Mitochondria are vulnerable to a wide array of bothendogenous and exogenous influences, all of which arelinked by excessive nitric oxide production.
• a virus-induced autoimmune response to developingbrain myelin may impair anatomical development ofneural pathways in autistic children.

What this tells us…
These tremendous (overwhelming) number of problem areasmean something is impacting many areas all at once – or
There are many subgroups of autism – orBoth - subgroups exist, and something has widespread impacton the body
The event usually seems to be GUT thenBRAIN wounding

Precipitating Event
To make sense of the regression history we need awounding event, which causes changes in the gut and thebrain at nearly the same time.
What can do this??????Toxins, viruses, heavy metals are all within the realm of
possibilities.Synergistic combinations likely

None Can Be Ignored, but we need to prioritize….
Progress requires attention to detailsAll issues must be addressed – eventuallyThe priority is unique to each childHowever, the Gut is generally the best place to start

Gut Issues – Core Focus (Wakefield)
Inflammatory bowel disease/MeaslesOpioidsDysmotility = Constipation/Diarrhea/RefluxLeaky Gut – Matrix MetaloproteinasesDysbiosis
Other Important Issues
Elevated AmmoniaSulfation DeficitsAutoimmunity to MyelinAntibodies to Blood VesselsThrombophiliaSeizuresNutritional Disorders/MetalsFood Allergy

Chromosomal Abnormalities
No defining genetic pattern has emerged despite$80M in NIH funded research.
In general we are left with what are thought of assusceptibility genes which are common in thegeneral population as well as the ASD group
It is desirable to look for Fragile X disorder
As any as 20 or more other minor chromosomalareas may be acting in autism.
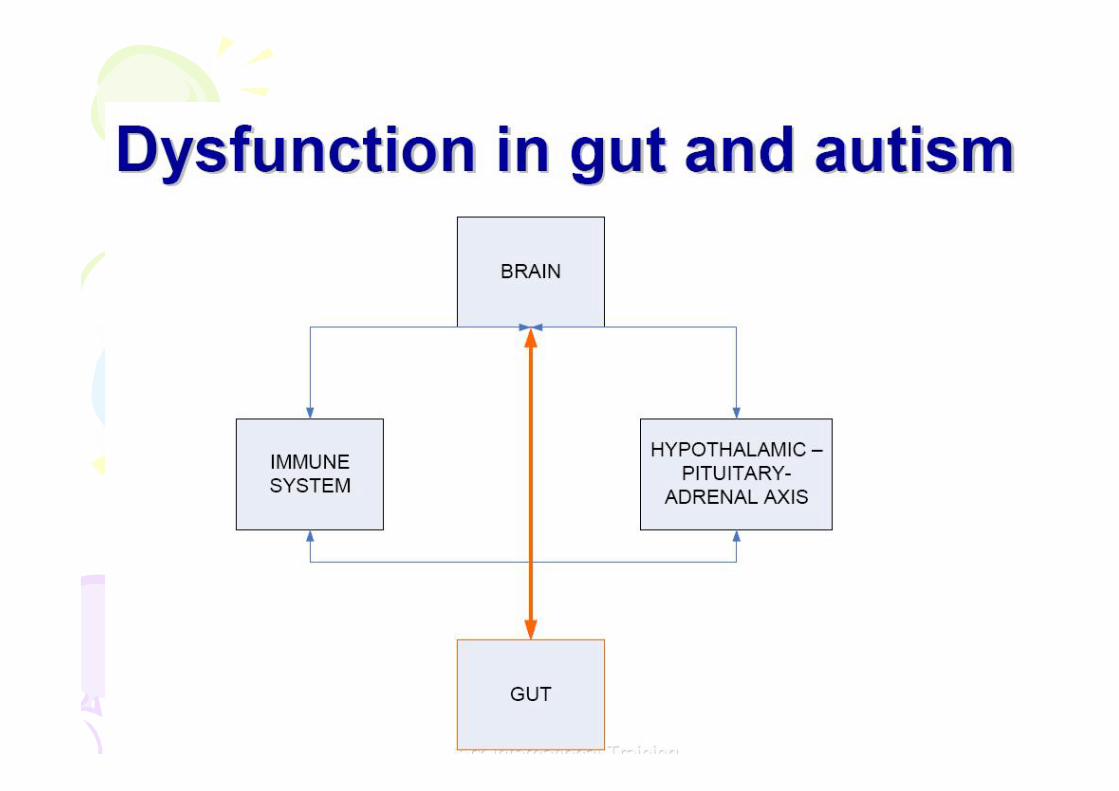
GUT – BRAIN LINK
IMMUNE SYSTEM, VAGUS NERVE , TOXINS & LIVER
VAGUS NERVE, EMOTIONS &ENDOCRINE CONTROL
Exogenous Opioids
Short pieces ofProteins
Lack of DPP-IV

Gastrointestinal Abnomalities: Upper andLower - Reflux Esophagitis, Gastritis,Defective Secretin Activation, &Inflammation
Gut Mothers (Beck & Kessick)
Gut Guys: Horvath, Wakefield and theteam at Royal Free

THE AUTOREGULATORY SYSTEM:ORGANS OF DETOXIFICATION
Toxins are processed by various organs inthe body. The liver, kidneys, skin andmucous membranes all take part in theexcretion of homotoxins. In someinstances, toxins must be prepared forexcretion through a complex series ofchemical processes, like we see in theliver. Detoxifying ability is dependent onvarious factors such as genetics, genderand the nutritional status of the patient.

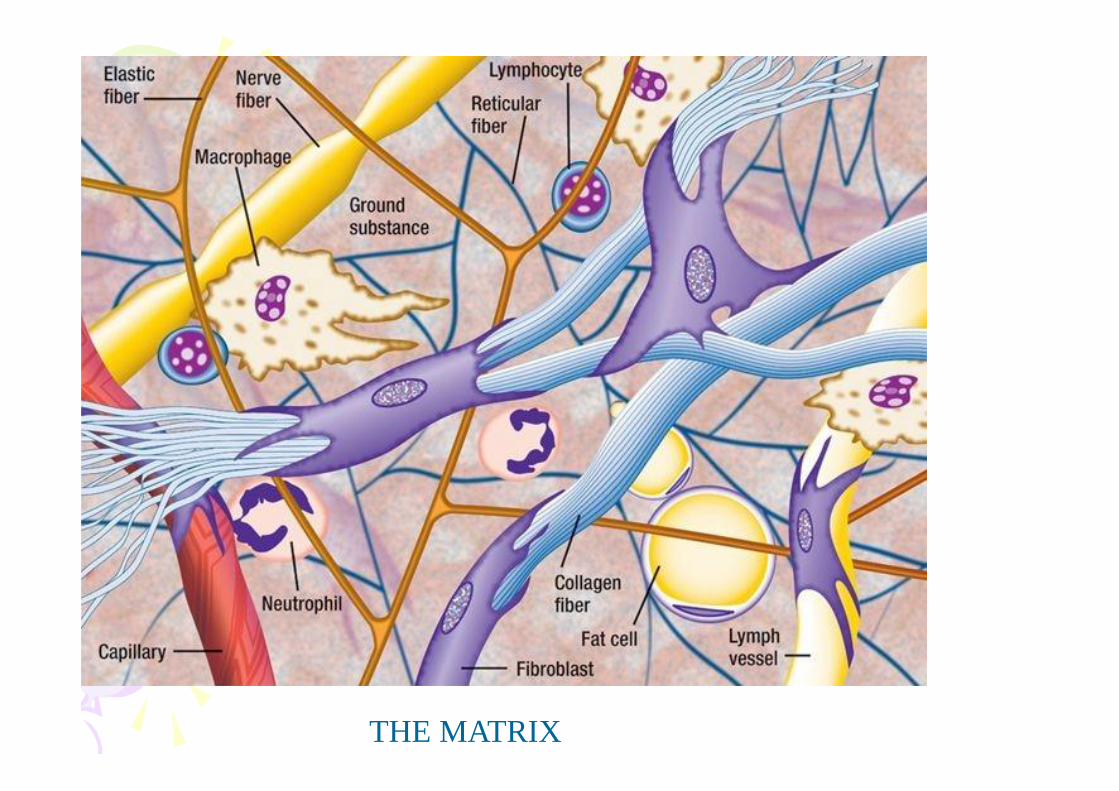
THE MATRIX



FUNGUS: CANDIDA ALBICANS
PARASITES
ALLERGIES
HEAVY METAL POISONING
INSUFFICIENT ENZYMES
INSUFFICIENT GOOD BACTERIA
IMPAIRED LIVER DETOX
LEAKY GUT
INTESTINAL DYSBIOSIS






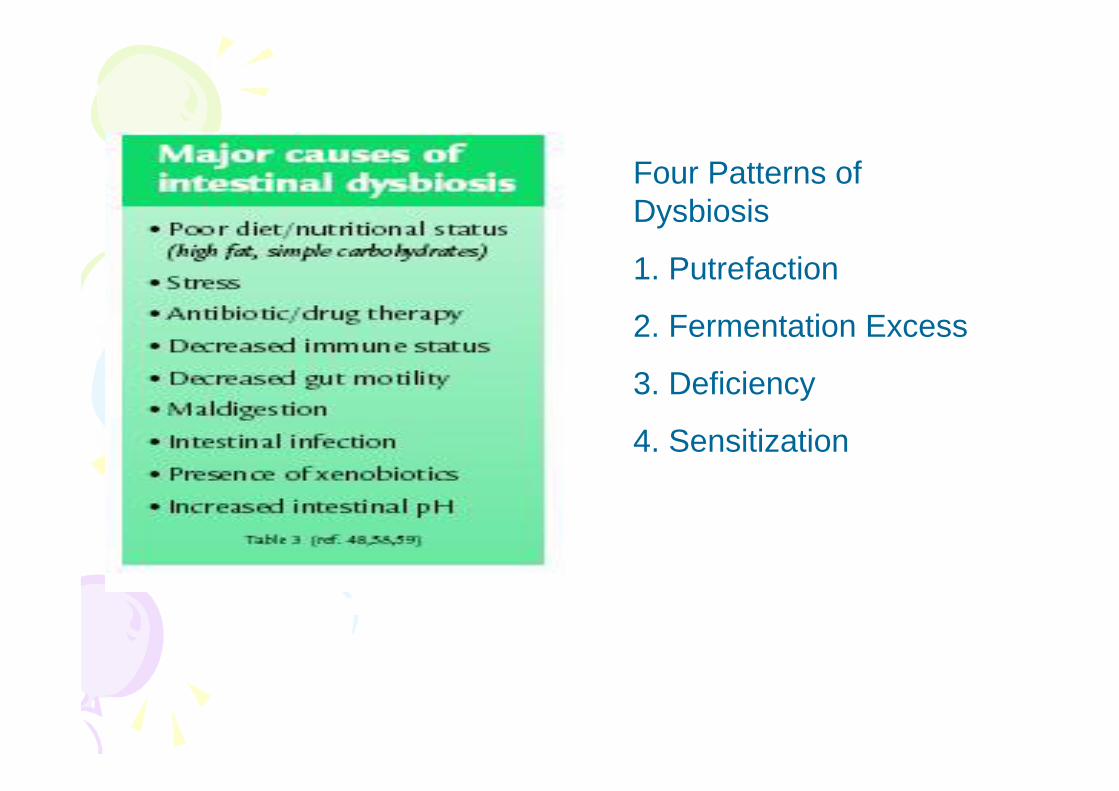
Four Patterns ofDysbiosis
1. Putrefaction
2. Fermentation Excess
3. Deficiency
4. Sensitization



PEPTIDES
ANSERINE/CARNOSINE – Measure of digestive function. Alsochelate copper. Increase tissue deposits of copper
INDOLYLACROLYLGLYCINE(IAG) – Tryptophan malabsorption
EXORPHINS – Dietary exorphins. Biologically active peptides thatcome from the incomplete absorption of gluten and casein and havepowerful opium or morphine like effects on the brain

Mineral and Other malnutrition
Calcium * GoldMagnesium * AntimonySodium BariumPotassium BismuthCopper * LithiumZinc * NickelPhosphorus PlatinumIron RutheniumManganese ScandiumIron Silver
Chromium StrontiumSelenium TinBoron TitaniumCobalt TungstenGermanium ZirconiumMolybdenumSulfurVanadium
TOXIC
ArsenicBerylliumMercuryCadmiumLeadAluminiumBoron


CLINICAL FINDINGS
Neurofeedback
Craniosacral
Not therapeutic/useful in the presence of heavy metals,high copper or magnesium deficiencies
Classic Homoeopathy – Limited Use
Complex Homoeopathy – Very useful if used correctly

BloodType
Antigen Antibody-O
Antibody-A
Antibody-B
Comments
O No No Yes Yes O recipient can onlyreceive O blood –universal donor
A A No No Yes A recipient can receiveO and A blood
B B No Yes No B recipient can receiveO and B blood
AB A&B No No No AB recipient can receiveall blood – universalrecipient
The Four Blood Types & Their Antigens

Blood Type - Food Lectins Interaction
Lectins are protein found in foods that have agglutinating propertieswhich affect your blood and organs.
OK. No clumping of cells
MILK antigenBlood B & AB – don’t have antibody B
Blood 0& A –have antibody B CLUMPINGPROCESS
B B
B BB

Lectins also found in germs and organs (e.g. bileduct) for cleaning up process and attachment foreasy disposal by immune cells. Lectins (mitogens)also stimulate production of WBC (mitogenesis)
I have been in practice for 25 years. Have seen 15, 000patients. About 1000 children, 700 for learning disabilities. 500plus for autism. About 80% of the autistic/learning disabledchildren improve between 60% to 80%.
CORE KEY CONCEPTS
Diet Modulation –treating allergies, sensitivities andreversing lectin damage
Detoxification – Liver Detox, Heavy Metal,Homoeopathics, Sanum Remedies, AntihomotoxicPreparations
Nutritional Supplementation – deficiencies as well asblood type supplementation
Structural Work – Craniosacral Therapy
Neurofeedback
Improvements are defined as
* Better focus academically
* Less or no spinning, head banging, etc
* Reduction or elimination in self stimming behaviour
* Improved social behaviour, greater eye contact
* Improvements in health and nutrtional status
* Allergy symptoms if any clear up (eczema, sinus, asthma)
* Improved sleep patterns
* Improvements in gait patterns
* Improvements in speech patterns
* Less Hyperactivity
DAN PROTOCOL OUTLINE
Testing
Vega Testing for Food/Chemical Sensitivities andIntolerances
Dark Field Blood testing for terrain assessment
Standard labs: CBC with differential, Chemistry, Lipids,Thyroid Panel with TSH, Iron Profile
Vega Testing/CDSA with parasitology: CompleteDiagnostic Stool Analysis to access the Gl tract
OAT : Organic Acid Test to access balances ofmetabolites, vitamins, minerals, aminos, etc.
Metals+ Minerals (Hair, Urine (12 hours), Fecal, RBC):Levels accessing various body compartments of toxic metalsas well as essential minerals.

CORE KEY CONCEPTS
Diet Modulation –treating allergies, sensitivities and reversinglectin damage
Detoxification – Liver Detox, Heavy Metal,Homoeopathics, Sanum Remedies, Antihomotoxic Preparations
Nutritional Supplementation – deficiencies as well as blood typesupplementation
Structural Work – CST, Visceral
Neurofeedback (Referral)
Currently no one else in Singapore does all of the above or hasthe experience. We also do cranio-sacral therapy and visceralmanipulation where necessary

The NTRC Protocol
REBOOT – Reset the digestive system
1) TESTING FOR SUBCLINICAL INFECTIONS – PARASITICORGANISMS
2) VACCINE DAMAGE
3) FOOD SENSITIVITIES :CASEIN, GLUTEN
4) GUT DYSBIOSIS
DETOXIFICATION
5) IMPAIRED LIVER DETOX PATHWAY , SULPHATION ISSUES
6) ENZYME SUPPLEMENTATION
7) TEST FOR HEAVY METAL TOXICITY

ACTIVE RECONSTRUCTION – Heal the intestinal lining
8) FATTY ACIDS
9) OTHER INTESTINAL NUTRIENTS -GLUTAMINE
10) SANUM THERAPY – Reconstruction of Intestinal Lining
WHAT’S NEXT ?
11) TEST FOR AMINO ACID METABOLIC FAULTS AND CORRECTION
12) TEST FOR ESSENTIAL FATTY ACIDS AND CORRECTION
13) OTHER TESTS

EXTRAS
14) 5-HYDROXY TRYPTOPHAN
15) PIGMENT-FREE DIET
16) MEGADOSE B6 & Mg
17) DIMETHYLGLYCINE (DMG)
18) OTHER SUPPLEMENTS
19) B12 INJECTIONS
20) NEUROFEEDBACK

Currently seeing ASD children from other countries as well like:
Bahrain
Indonesia
India
Malaysia
Pakistan
Philippines

CASE HISTORY
– JADEN aged 4+ (2001)
Came in on 3/2006
Presenting condition: Very quiet (almost non-verbal), Not compliant,could not socialize, not toilet trained , could not sit up on his own,could not play on his own. Also had significant self stimulatingbehaviour and could not hold a spoon and feed himself. Photophobicand sensitive to noise.
Additional comments: Parents noticed changes for the worse afterMMR injection after a year. He was also a delivered with the use ofvacuum and forceps. Mother had mercury fillings. They had donesome massage, some homoeopathy and some vitamins.

Ist Round of Treatment:
Initial testing: Involved blood testing, Electro-dermal screeningfor allergies, sensitivities fungus , yeast issuses and vaccinesdamage. Hair tissue mineral testing
1) TESTING FOR SUBCLINICAL INFECTION MARKERS –PARASITIC ORGANISMS
2) VACCINE DAMAGE
3) FOOD SENSITIVITIES :CASEIN, GLUTEN
4) GUT DYSBIOSIS

What the test results showed:
Blood Tests
Haemoglobin L
White Blood Cell Count H
ESR H
MCV L
MCH L
Creatinine L
Uric Acid L
SGOT H
T3 Concentration H
Summary: Insufficient nutrition for haemoglobin, allergiesand or worms, thyroid dysfunction, liver impaired function

Vega Testing:
Food sensitivities: wheat, dairy, yeast, soya, sugar, egg, peanut
Parasites
Lead
Acetylaldehyde
Variola (Vaccine damage)
Hair Tissue Mineral Analysis:
Lows: Magnesium, Zinc, Phosphorus
Highs: Sodium, Potassium
Toxic Metals: Boron, Arsenic, (Mercury), Cadmium , Lead ,Aluminium

Supplements 1:
Digestive Enzymes (2 types)
Essential Fatty Acids
Homoeopathic Detox
Homoeopathic Parasite Cleanse
Homoeopathics to neutralize vaccines damage
Magnesium
Anti-fungal diet
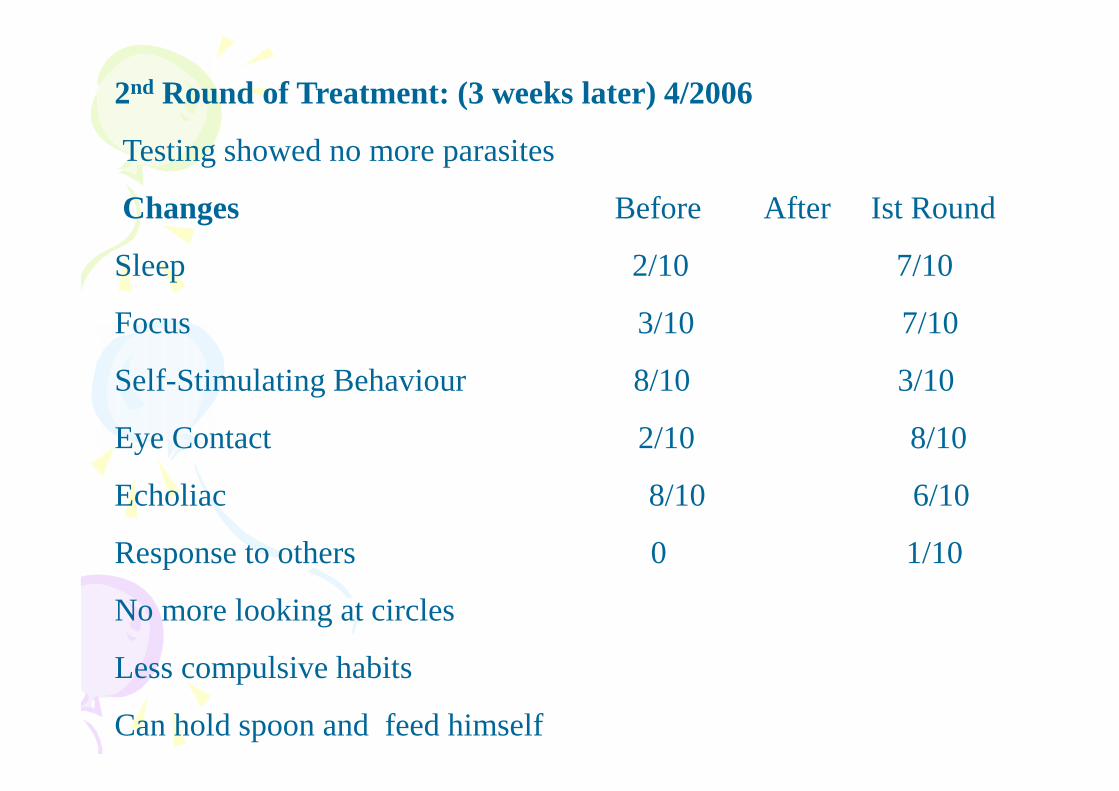
2nd Round of Treatment: (3 weeks later) 4/2006
Testing showed no more parasites
Changes Before After Ist Round
Sleep 2/10 7/10
Focus 3/10 7/10
Self-Stimulating Behaviour 8/10 3/10
Eye Contact 2/10 8/10
Echoliac 8/10 6/10
Response to others 0 1/10
No more looking at circles
Less compulsive habits
Can hold spoon and feed himself
Supplements (2)
Digestive Enzymes (2 types)
Essential Fatty Acids
Homoeopathic Detox
Magnesium
Zinc
Oral Heavy Metal Chelators
Amino Acid Supplements
Blood type diet

3rd Round of Treatment: (4months later) 8/2006
Darkfield testing: Sludge, echinocytes roleau
Interpretation: Poor absorption, free radical damage, impaired liverfunction, deficiency of B vitamins, minerals.
Vega Testing: Nerve degeneration: Diptheria , Tuberculinum, Typhus.
Changes:
More verbal
Capable of impulse control
Can ask for what he wants
Increased compliance with instructions
Good Toilet habits
Started ABA program

Supplements (3)
Digestive Enzymes (2 types)
Essential Fatty Acids
Homoeopathic Detox
Magnesium
Zinc
Oral Heavy Metal Chelators
Amino Acid Supplements
Germanium
Selenium
Homeopathics to stimulate the brain
Homeopathics to stimulate the immune system
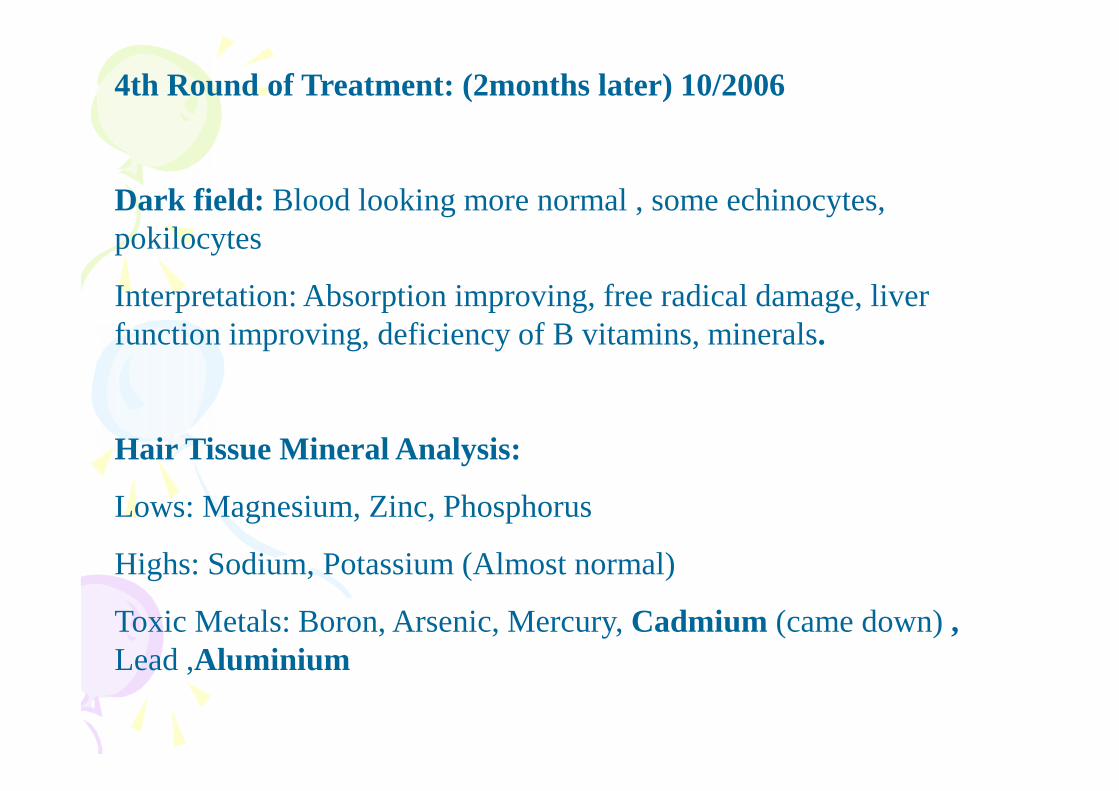
4th Round of Treatment: (2months later) 10/2006
Dark field: Blood looking more normal , some echinocytes,pokilocytes
Interpretation: Absorption improving, free radical damage, liverfunction improving, deficiency of B vitamins, minerals.
Hair Tissue Mineral Analysis:
Lows: Magnesium, Zinc, Phosphorus
Highs: Sodium, Potassium (Almost normal)
Toxic Metals: Boron, Arsenic, Mercury, Cadmium (came down) ,Lead ,Aluminium

Changes
Single distinct words appear
Can play on his own
Can fight with his brother
Creativity
Concentration Span dipped
Can utter normal sentences
Supplements (4)
Digestive Enzymes (2 types)
Essential Fatty Acids
Homoeopathic Detox
Magnesium
Zinc
Oral Heavy Metal Chelators
Amino Acid Supplements
Germanium
Selenium
Homeopathics to stimulate the brain
Homeopathics to stimulate the immune system
Folinic Acid
5th Round of Treatment: (2months later) 2/2007
Darkfield: Greatly improved
Changes
Emotional Response to situations
Can hold pencil with correct grip and strength
Supplements (5)
Digestive Enzymes (2 types)
Essential Fatty Acids
Homoeopathic Detox
Magnesium
Zinc
Oral Heavy Metal Chelators
Amino Acid Supplements
Germanium
Selenium
Homeopathics to stimulate the brain
Homeopathics to stimulate the immune system
Folinic Acid
6th Round of Treatment: (3months later) 5/2007
Hair Tissue Mineral Analysis:
Lows: Magnesium, Zinc, Phosphorus - NORMAL
Highs: Sodium, Potassium, Iron,Maganese, Boron, Cobalt
Toxic Metals: Boron, Arsenic, Mercury, Cadmium, (Lead) ,Aluminium
Changes:
Can read
Assertive
Independent
Self-willed
Went to special kindergarten and was sent back to normal stream
Supplements (6)
Digestive Enzymes (2 types)
Essential Fatty Acids
Homoeopathic Detox
Magnesium
Zinc
Oral Heavy Metal Chelators
Amino Acid Supplements
Germanium
Selenium
Homeopathics to stimulate the brain
Homeopathics to stimulate the immune system
Follinic Acid
7th Round of Treatment: (3months later) 8/2007
Vega Testing: Parasites
Organic Acid Tests Results:
Mitochondrial Activity : Impaired energy production at cellular level
Fatty acid Oxidation: Uptake impaired, cellular membrane transportmechanism and immune system impaired
Markers of Cofactor Needs: Specific nutrients malabsorbed
Markers of Neurotransmitter Metabolism: Nerve function andactivity impaired
Markers of Detoxification: Liver function suboptimal
Markers of Bacterial Metabolism: Abnormal flora and fauna in thegut

Supplements (7)
Digestive Enzymes (2 types)Essential Fatty AcidsHomoeopathic DetoxMagnesiumZincOral Heavy Metal ChelatorsAmino Acid SupplementsGermaniumSeleniumHomeopathics to stimulate the brainHomeopathics to stimulate the immune systemFollinic AcidMethy B12Branch Chain Amino AcidsProtein Supplements

8th Round of Treatment: (2months later) 10/2007
Suggested Start Cranials, Than started Neurofeedback
Supplements (8)
Digestive Enzymes (2 types)Essential Fatty AcidsHomoeopathic DetoxMagnesium, ZincOral Heavy Metal ChelatorsAmino Acid SupplementsGermaniumSeleniumHomeopathics to stimulate the brainHomeopathics to stimulate the immune systemFollinic AcidMethy B12Branch Chain Amino AcidsProtein Supplements

9th Round of Treatment: (2months later) 8/2008
More Hyper
More Aggressive
Funny
More Compliant
More Verbal
Supplements (9)
Digestive Enzymes (2 types)Essential Fatty AcidsHomoeopathic DetoxMagnesium, ZincOral Heavy Metal ChelatorsAmino Acid SupplementsGermaniumSeleniumHomeopathics to stimulate the brainHomeopathics to stimulate the immune systemFollinic AcidMethy B12Branch Chain Amino AcidsProtein Supplements

Going to a normal kindergarten.
Next change B12 injections
Summary:
In 9 visits (from 3/2006 – 8/2008 or about 1 year 5 months),
Very quiet (almost non-verbal), not compliant, could not socialize,not toilet trained , could not sit up on his own, could not play on hisown. Also had significant self stimulating behaviour and could nothold a spoon and feed himself. Photophobic and sensitive to noise –ASD spectrum child
Became verbal, capable of controlling himself, toilet trained,increased socialability ,
Improved brain functioning and capable of attending a normalkindergarten.

FFEDBACK FROM MOTHER
B4- Non-verbal- no eye contact- non-awareness of surrounding- exhibit autistic related behaviour like spinning objects, running incircles, echolalia- use gestures to communicate- won't play or interact in group- no interest in any form of play- obsession in arranging things in a straight line- afraid of loud noises or noisy surrounding like going to shoppingcomplexes

After/Now- Slightly verbal- Better eye contact- Much more aware of his surrounding- No more spinning objects, running in circles- Use less gestures, attempt to tell what he wants- able to play with other children- love to play rough and tumble with his brother- no more arranging things in straight line. Able to create newgames to play- no longer afraid of loud surrounding. Love to go shoppingcomplexes- assertive- able to display his likes and dislikes- love to play computer games. Self learned by observingother children play- could sing “Happy Birthday” and clap his hands for hisbirthday


THANK YOU FOR LISTENING

1
The NTRC Protocol: A logical sequencing of biomedical interventions for thetreatment of autism and related disorders.
by SUNDARDAS D ANNAMALAYBSc (S’pore), BNSc(Hons) (Aust), ND (Aust,USA), PhD (USA),MD(MA), DSc (Sri Lanka)Defeat Autism Now PractitionerNaturopathic Physician(Lic Aust) , Acupuncturist (Lic S’pore)Functional Medicine Specialist,CEO, Natural Therapies Research Centre Pte Ltd
Sundardas Naturopathic Clinic
Professor, YINS Colleges Worldwide (Aust,.USA)
Visiting Professor, Open International University for Complementary Medicine (SriLanka
More and more published evidence supports the clinical insight that Autism SpectrumDisorder (ASD) is not a fixed, static, genetic insult to the brain, but rather a multi-systemdynamic condition where brain, body and behavior can change – through regression,transient improvements such as with fever, improvement through treatment or evenremission of symptoms/recovery. Moreover, the problems in the different involvedsystems – brain, gastrointestinal, immune, endocrine and more – are deeplyinterconnected through common underlying mechanisms, prominently includingdisturbed energy and signaling mechanisms.
Harm from environmental insults may ripple through the system by damage at theselevels. These insults can include allergies, infections and toxic substances like heavymetals. This is an overview of protocols fine-tuned over twenty years with at least 500cases of learning disabilities in the ASD spectrum.
We advocate introducing interventions one stage at a time and assessing the therapeuticadvantage to each individual child. Consideration should then be given to its continuationor discontinuation. Our protocol is divided into five parts. Using a martial metaphor - weare fighting a battle and we should be seeking to establish peace. There are five stages inthe establishment of a viable and permanent peace.
A. Reboot – Reset the digestive systemB. DetoxificationC. Active reconstruction - Heal the intestinal liningD .What’s next ?E. Extras

2
TESTING
STANDARD TESTING
FULL CHEM PANEL
T3,T4,TSH, rT3
FERRITIN,
HAIR MINERAL TESTING
OATS
DIFFICULT CASES
HUMAN GENOME TESTING
CONFIRMATORY
AMINO ACIDS
EFAS
The NTRC ProtocolA.REBOOT – Reset the digestive system
1) TESTING FOR SUBCLINICAL INFECTIONS – PARASITIC ORGANISMS
2) VACCINE DAMAGE
3) FOOD SENSITIVITIES :CASEIN, GLUTEN
4) GUT DYSBIOSIS
B.DETOXIFICATION
5) IMPAIRED LIVER DETOX PATHWAY , SULPHATION ISSUES

3
6) ENZYME SUPPLEMENTATION
7) TEST FOR HEAVY METAL TOXICITY
C.ACTIVE RECONSTRUCTION – Heal the intestinal lining
8) FATTY ACIDS
9) OTHER INTESTINAL NUTRIENTS -GLUTAMINE
10) SANUM THERAPY – Reconstruction of Intestinal Lining
D.WHAT’S NEXT ?
11) TEST FOR AMINO ACID METABOLIC FAULTS AND CORRECTION
12) TEST FOR ESSENTIAL FATTY ACIDS AND CORRECTION
13) OTHER TESTS
E.EXTRAS
14) 5-HYDROXY TRYPTOPHAN
15) PIGMENT-FREE DIET
16) MEGADOSE B6 & Mg
17) DIMETHYLGLYCINE (DMG)
18) OTHER SUPPLEMENTS
19) CRANIOSACRAL THERAPY
4
We advocate introducing interventions one stage at a time and assessing the therapeuticadvantage to each individual child. Consideration should then be given to its continuation ordiscontinuation. Our protocol is divided into five parts. Using a martial metaphor - we are fighting abattle and we should be seeking to establish peace. There are five stages in the establishment of aviable and permanent peace.
A. Reboot – Reset the digestive system
B. Detoxification
C. Active reconstruction - Heal the intestinal lining
D .What’s next ?
E. Extras
Stage A: REBOOT – Reset the digestive system
1 TestingIt is at this time that we initiate testing. The purpose of this initial screening is to differentiate thetype of initial diet, intervention or nutritional program required. At NTRC, we basically useFunctional Assessment techniques, particularly the German and the European approach. Muchlater on we shift to the American assessment methods which are more biochemical based.
1a) YeastsFor many years a close association between autism spectrum disorders and parasitic yeasts hasbeen noticed and reported and yet the nature of this relationship remains uncertain. We prefer tointervene against yeasts at this stage rather than, as some therapists prefer, as the later stage ofintervention. For some years, we took the view that yeasts, such as Candida, became establishedas a result of a depressed immune system which was, itself, consequent upon the actions of thefood derived opioid peptides. This colonisation by yeasts would be enhanced by the inappropriateuse of antibiotics early in the development of the child. For example, it is well known that manychildren with autism spectrum disorders suffer from ear infections (usually referred to as otitismedia). It is likely that these are at l east initially consequent upon problems caused by milk yetthey are treated by antibiotics. These powerful antibiotics are used routinely and sometimes withgreat regularity in particular children. Sure enough they kill bacteria even though their role in thecausation of the ear problems may be minimal. Unfortunately, they will also kill the bacteria in theintestines and this will permit the development of yeasts and other organisms much more akin tofungi. Thus, the use of antibiotics will encourage fun gal growth of this type. If yeasts are presentthey could increase the permeability of the intestinal wall especially where sulphate levels are low.Shaw has made a particular study of yeast related phenomena and has postulated a number ofmechanisms by which products of yeast growth could have more direct influence and we mustrefer the interested reader to his work (Shaw 1998) for further information. Recently (Shaw 2000),he has suggested that yeasts may be responsible for the production of compounds which may form

5
complexes with the enzymes (such as Di-Peptyl Peptidase IV) which would, under normalcircumstances, break down the food derived opioid peptides. There is certainly a logicality andreasonableness about this idea but strong supportive evidence is currently awaited.
These mechanisms may or may not pertain but it is clear that many parents believe that they seebenefits from treating these yeast infections. Unfortunately there are no published data to supporttheir observations but the numbers reporting behavioural improvements from the use of theantifungal product Nystatin suggest that these reports should be taken seriously. It has beensuggested that the Nystatin may be acting by some other mechanism, for example by making theintestinal wall less permeable. This is, indeed possible, but again there are no supportive data andthis would not explain the benefits alleged to result from the use of other antifungal agents such asDiflucan.
Yeasts thrive on sugar (sucrose and others) so many parents have attempted to control yeastinfections by limiting or removing dietary sugars completely. Additionally, some parents have gonefurther than this and removed and foodstuff containing yeasts at all. Other parents have attemptedto control yeast infections by supplementing the diet with tablets or medications containing highlevels of the beneficial bacteria which are normally found in the gut. Acidophilus or bifidophiluscontaining products are used for this purpose along with natural "yeasticides" such as grape-seedoil or garlic (although the latter could have its own consequences!).
There are a number of tests for yeast infections. These may involve examination of the stools (fordirect evidence of infections); the blood (for antibodies or antibody-antigen complexes) or urine (foryeast metabolites absorbed from the intestines). Each test has its strengths and none is without itsweaknesses. Many parents feel that it is simpler to assume infection and just go ahead withtreatment in terms of supplements
1b) Other intestinal parasitesLife for intestinal parasites is not always simple and survival depends not only on obtainingnourishment but also on being able to survive the body's defense mechanisms. The production ofsubstances which will depress the host's immune system would greatly enhance the survivalchances of any organism. Only a very "foolish" parasite would produce chemicals that would injureits host for its own chances of survival would depend upon the survival of the host organism.Opioid peptides are perfect for this task as they would depress the host's immune system butwould not, under normal circumstances, be absorbed. However, we know that people with autismspectrum disorders do have excessively permeable intestines and problems could accumulate.
Some worms and protozoal organisms are known to produce these compounds and we suspect,although it is not proven, that bacteria would utilize the same mechanisms. No one seriouslybelieves that "worms cause autism" but they could exacerbate the situation especially in oursubjects who may be especially prone to these types of infestation as a result of their alreadydepressed immune system. One theory for the existence of the unusual dermorphin typecompounds, referred to previously, suggests that they a re derived from bacteria (perhapsanaerobic bacteria such as the Clostridia) who seek to increase their chances of survival by thismeans. Although there is as yet no evidence to support the possibility, it could be that viruses or

6
even Candida could be utilizing similar mechanisms. In any case, it would seem important tonormalise intestinal flora as much as possible by using appropriate medication regimes.
2) Vaccine Damage
A certain percentage of children develop immune damage as s result of vaccinations. The greatestconcern surrounds accidental induction of full-blown illness when administering a vaccine. Asubtler, more important consideration is whether vaccines cause long-term impairment of theimmune system, or other subclinical syndromes. Many observant physicians have encounteredpediatric patients whose general condition or temperament or apparent general susceptibility haspermanently changed after vaccination. Almost 60% of the pediatric cases I see, have varyingstages of vaccination damage. In about 30% of the cases, the damage is severe enough to resultin clinical brain damage and neuro-degenerative conditions.
3a) Casein Removal
The effects of removing dairy produce are usually seen rapidly. Depending upon the age of thesubject it could be 2-3 days (in young children) or 10-14 days in adults although usually it is muchquicker than that. We normally suggest that a three week trial is appropriate in the first instant.Lucarelli (1995) felt that 66% of the subjects in her trial showed benefits from this intervention and,although we have no firm data to support this view, our experience would suggest that this isbroadly correct. Of course, there could be a period where side effects are seen but by the end ofthe third week the situation should be clear.
Any withdrawal effects are of comparatively short duration but can be quite severe especially inyoung or small children. This is another reason why we prefer to separate the removal of the twoelements, gluten and casein, during this protocol. We have found that the beta-casomorphin (1-7)peak does disappear from the urinary profiles rapidly after the removal of dairy produce from thediet (a couple of days). We speculate that this is the reason for any dramatic withdrawal effects.
We have also observed that many higher functioning children have voluntarily removed dairyproduce from their diet in any case. Since the peaks disappear from the profiles so quickly, it ishighly likely that subjects will be in a position to detect the difference that abstinence from dairyproduce makes. Many people with Asperger Syndrome, for example, complain of being confusedor having difficulty in concentrating when drinking milk. Many such people shun milk but willrationalise this avoidance in ter ms of "hating milk" or finding it "slimy". On the other hand, somechildren are clearly addicted to milk and will drink what are generally considered to be very largequantities. A three year old child, for example, who drinks 5 pints of milk a day, is by no meansuntypical of this group. Cultures based upon Western European principles are inculcated with theidea that milk is a wonderful and indispensable element of diet. Health visitors, nurses, dietitiansand orthodox medical practitioners are not easily convinced that bovine milk is not designed forhuman beings and that its consumption is, in many cases, inappropriate and undesirable. It hasbeen recorded that there is an increased incidence of autism amongst the immigrant population inSweden (Gillberg 1996) when compared to the indigenous population. There are a number ofpossible theoretical explanations but one must involve the utilisation of diets for which subjects arenot genetically equipped in terms of enzyme complement or metabolic processing ability. The

7
absence of lactase enzymes in subjects of African origins and the disappearance of enzymes,which break down casein from subjects of Chinese origin by the age of 12, are well-documentedexamples of such phenomena.
We have been very impressed by the number of parents, principally mothers, who have taken theinitiative, often against professional advice, to remove dairy produce from the diet. Clearly, theseparents have intuitively realised that something is wrong with their child's reaction to milk. Projectilevomiting of (cow) milk; eczema, particularly behind the knees and in the crook of the elbow;strange white bumps under the skin; an early history of ear discharges and infections possiblyrequiring the fitting of grommets (tubes); very early onset of constipation and/or diarrhoea andrespiratory disorders resembling asthma may all be taken as signs of a problem with casein.
A "review" of the situation is appropriate after three weeks of casein removal is appropriate.Clearly, in those situations where improvements are apparent this intervention should becontinued. Where improvements are not seen it is difficult to justify t he continued removal but mostparents feel that the difficulties inherent in this form of intervention are not so severe that theycannot continue with it. This must be a matter of personal choice. Since the removal of dairyproduce is comparatively simpl e, it does also provide parents with the opportunity to preparethemselves for the rigours of gluten removal. Of course, there are many people who prefer toremove both gluten and casein simultaneously and that is fine but we would still strongly advocateseparating the elements where children under 4 years of age are involved because of the potentialseverity of the withdrawal effects. However, we would still suggest a test of the role of milk beperformed soon after the implementation of such a diet.
3b) Gluten Removal
The nature of the intestinal microflora will be very much dependent upon the nature of the foodconsumed. A restricted diet, such as that selected by many people with autism would favourparticular bacteria at the expense of others. For example, a diet with a high wheat diet would tendto favour Clostridial organisms whereas they would be almost absent if rice were to be the soledietary carbohydrate source. Clearly these are areas that require detailed investigation but interestis only just beginning to develop.
Experience and theoretical considerations based upon the opioid excess theory of autism suggestthat the first stage in the treatment of autism must be the removal of the sources of these peptides.We are not suggesting that this is anything like the whole story but it would seem to be anappropriate first step. Since the sources of the bullets will almost always include casein and glutenthese should be removed from the diet. It may be that parents, carers, professionals or subjectsthemselves have had some form of analysis performed to detect these substances. The bestknown tests are the urinary peptide profiles but there are other methods.
Although these tests can provide much very useful information, when used in conjunction withclinical data, it may be worth considering excluding these products from the diet in any case. Wehave come across subjects with autism who do not show abnormal l levels of urinary peptides (orIndolyl Acryloyl Glycine (IAG)) - in fact their urinary peptide profiles appear to be, to all intents,normal - yet the subject exhibits florid symptoms of autism. We have come across subjects like this

8
who still respond to t he removal of casein and gluten from the diet. It could be that the subjects arebreaking down the peptides into abnormal components that are not detected in our systems. Itcould be that although the urinary levels are normal, the quantities crossing the blood brain barrierand reaching the CNS are high. Perhaps this is a consequence of abnormal permeability of thebarrier caused by infection natural or induced. We have also come across cases, fortunately veryfew, where the problems appear to have been triggered by hypoxia or anoxia at or around birth. Inthese cases, there may have been damage to the very sensitive developing cerebellum. Thoseareas still functioning may, as a consequence, be affected by even the normal levels of peptides,which may be derived from food via the blood.
Whatever the mechanisms involved or the results of biomedical tests, we would suggest thatconsideration should be given, first of all, to the removal of dietary milk of all sorts.As previously stated, gluten removal requires the removal of the proteins (prolamins) from anumber of cereals and especially wheat; barley; rye and oats. Given the modern Western diet andits dependence upon cereals this is not easy but most do seem to accomplish it without unduedifficulty. The peaks in the urinary profiles which the researchers (correctly or incorrectly) ascribe togluten persist for much longer that the casomorphins. In the trial (Whiteley 1999) there had onlybeen a 26% reduction in urinary levels after a 5 month period. This is explicable in terms of thepeptides being stored in body tissues and, perhaps, only partial compliance with the regime insome cases. If the body is incapable of breaking these peptides down which it has absorbed itmust do something with those it produces during digestion. It cannot break them down and themechanisms for dumping them in the urine are (it is speculates) swamped by the sheer quantity ofthe materials. As in other instances, the body has little option but to store them probably in fattissues. When dietary sources are removed these stores are depleted as rapidly as possible but asthe child/person becomes older, the quantities stored will, in absolute terms, be larger and the timerequired for their removal will be correspondingly longer.
For this reason, it is very rare for gluten to have been spotted as causing offence in the way thatmilk frequently has either by the parent or by the person primarily affected. There is almost alwaysa degree of craving for gluten products and we are aware of nobody with autism spectrumdisorders who has refused gluten containing products in the way that milk and dairy produce isavoided. It is strange that we are so hooked onto what is essentially the seed from an obscure typeof grass. It could be that this production of opioid substances is an element in its acceptance as astaple diet throughout so much of the world.
Although it can and does happen, gluten removal does not normally result in immediate, dramaticeffects. Except in very young children, where results are seen more rapidly, we normally expect tosee changes in 3-4 weeks so we suggest that people consider removal for a period of threemonths. After this time it is appropriate to review progress. We are aware of a number of caseswhere dramatic improvements have occurred 7-9 months after initiating the diet and in one case(Reichelt – Personal communication ) these improvements became apparent after two years ofrigid dietary intervention. As previously stated, the disappearance of the peptides from glutenappear to be more gradual than with the casomorphins. Therefore, the withdrawal effects tend tobe somewhat milder in severity but rather more prolonged particularly in adults.

9
The Norwegian studies have been going on for the longest period of time (Knivsberg 1995) andthey have always proposed removal of gluten as well as casein. Interestingly, they observed aphenomenon we have also noted in subjects who have used this approach where the casein andgluten are removed simultaneously. There is an initial rapid withdrawal period and improvement.This tends to be followed by a period where not much happens at all and parents often begin towonder if their initial improvement observations were a result of self-delusion. After a further periodof time, other improvements appear, sometimes after a second set of withdrawal symptoms. Webelieve that this biphasic pattern is due to the sequential effects of casein and then gluten removalfrom the diet.
4 Gut Dysbiosis
The human intestine maintains within its inner cavity a complex, crowded environment offood remnants and microbial organisms (called "the intestinal flora") from which the body derivesnourishment and against which the body must be protected. The relationship between the humanhost and her army of microbes is described by the Greek word, symbiosis, which means "livingtogether". When symbiosis benefits both parties, it is called mutualism. When symbiosis becomesharmful, it is called dysbiosis.
The first line of protection against dysbiosis and intestinal toxicity is strict control of intestinalpermeability, the ability of the gut to allow some substances to pass through its walls while denyingaccess to others. The healthy gut selectively absorbs nutrients and seals out those components ofthe normal internal milieu which are most likely to cause harm, except for a small sampling which ituses to educate and strengthen its mechanisms of immunity and detoxification.
Bacteria form the largest segment of the intestinal flora. The number of bacteria in the largebowel (about a hundred trillion) exceeds the number of cells in the human body. Intestinal bacteriaperform some useful functions, so that our relationship with them is normally one of mutual benefit.They synthesize half a dozen vitamins, supplementing those which are obtained from food. Theyconvert dietary fibre--that part of food which humans cannot digest--into small fatty acids whichnourish the cells of the large intestine. They degrade dietary toxins like methyl mercury makingthem less harmful to the body. They crowd out pathogenic bacteria like Salmonella, decreasing therisk of food poisoning. They stimulate the development of a vigorous immune response. Four-fifthsof the body's immune system is located in the lining of the small intestine.
Bacteria are dangerous tenants, however, so that dysbiosis is a common problem. As powerfulchemical factories, bacteria not only make vitamins and destroy toxins, but also destroy vitaminsand make toxins. Bacterial enzymes can inactivate human digestive enzymes and convert humanbile or components of food into chemicals which promote the development of cancer. Some by-products of bacterial enzyme activity, like ammonia, hinder normal brain function. When absorbedinto the body, they must be removed by the liver. People whose livers fail this task, because ofconditions like cirrhosis, develop progressive neurologic dysfunction resulting in coma and death.For them, the administration of antibiotics which slow the production of nerve toxins by intestinalbacteria can be life saving.
10
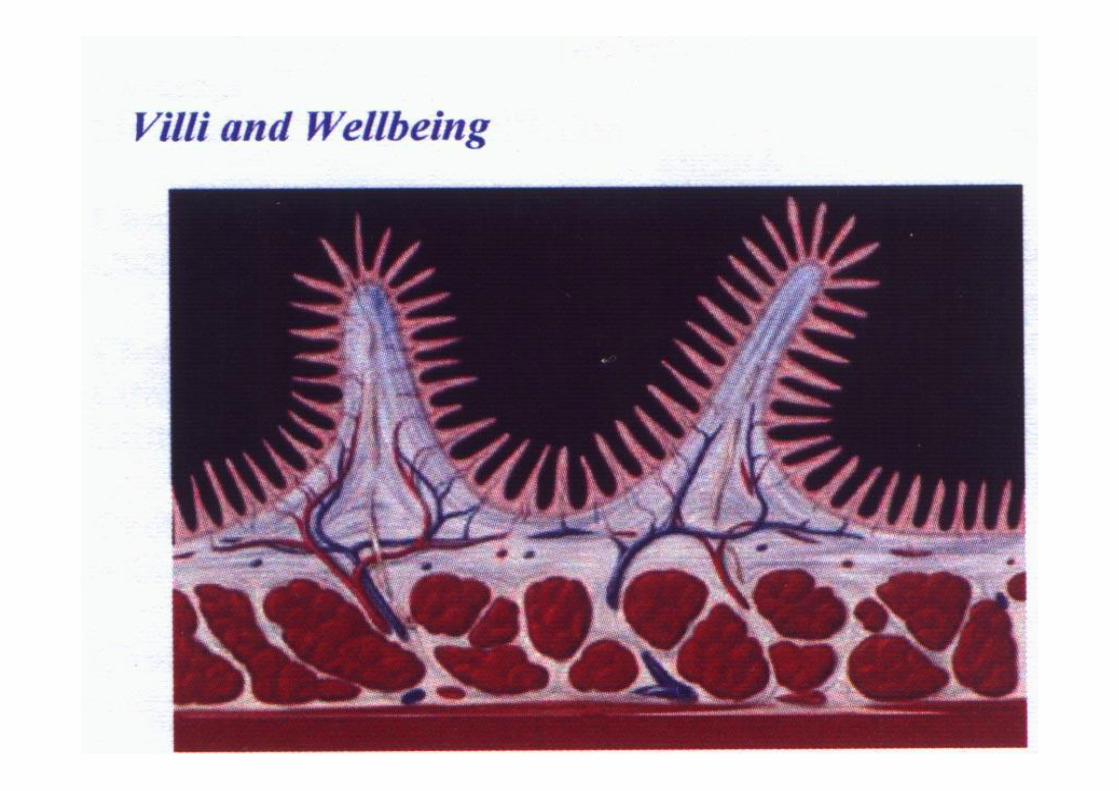
When there is significant damage to the lining of the intestinal villi, the integrity of the above systemis breached. This breach is often the forerunner of the multiple systems failure seen in the autisticspectrum condtion.
Perhaps of even greater importance is the effect on intestinal permeability. The intestines are linedwith a slimy layer of mucoproteins. This layer, as well as containing important immunoglobulins(specifically of the IgA class), provides lubrication and protection for the intestinal wall as foodpasses down the alimentary canal. These mucoproteins must be sulphated if they are to becontinuous, protective and effective. If they are not sulphated, the proteins clump together andleave exposed intestinal material and so the transport of peptides into the tissues will beencouraged.
We believe that these peptides are the agents (bullets) which are directly responsible for thecausation of the symptoms but there may be other agents, which can have a serious impact uponthe total picture. In some cases, gluten and casein appear to be t he sole elements but in othercases it is clear that other factors are involved. The relative involvement of these peptides (fromgluten and casein) is very large and it will obscure other factors. It is only after the main sources ofthe bullets, gluten and casein, are removed from the diet that the smoke will clear sufficiently toallow us to detect other causative elements which are largely of dietary origin.
Keeping a Food Diary. It is a good idea to keep a food diary in any case before, during (and after?)any intervention but this is doubly important after the gluten and casein have been removed as onlynow are we able to determine the role of other dietary factors. It is worthy of note that newmembers of the Spanish autistic society, APNA (Associacion de Padres de Ninos Autistas) has, forsome years, provided its members with just such a diary in which they can record daily food intakeas well as behavioural and performance estimates. Many parents have used these diaries andnoted that the consumption of a particular food is often associated with deterioration in behaviour,sleep patterns or performance. Without accurate record keeping it is unlikely that these culpritswould have been identified. Responses to these other foods tend to be idiosyncratic or personalbut some foods are commonly found to cause particular problems to groups of people. Eggs;tomatoes; avocados; aubergines; red peppers; soya; corn (maize) are common agents whereasbeef; pork; rice and potato are only very occasionally implicated. If a particular food is suspected itshould be removed from the diet for a trial period of, perhaps, two weeks and the effects noted. Weconcede that this is still a very hit and miss process but is all that is available to us at this time.There are, however, often clues to be picked up by observing the subject.
It is well known that children with autism are "faddy" eaters and will often have only a restrictedrange of foods that they will accept. This range usually involves large amounts of foods that arepotentially harmful although, as described above, some such foods are sometimes avoidedcompletely. If a child has a problem with a food he or she will either avoid it assiduously or becomemore or less addicted to it. The situation mirrors that seen in adults with a history of abusingalcohol. They either continue to abuse it or they avoid it like the plague. When the main culprits areremoved from the diet (presumably gluten and casein) the parent or carer must be alert to thepossibility of a switch to other foods with potentially harmful effects. On a number of occasions, wehave known children who detest milk yet have suddenly developed a craving for it once the glutenhas been removed from the diet.
11
Seroussi (2000) has described how corn was unmasked as a problem food for her child only afterthe very strict removal of the gluten and casein from the diet. Usually, when the offending foods areremoved, the child's diet will expand to take in things they had previously ignored. If the dietremains restricted, this can be a clue (but not a certainty) that an offending food is still forming apart of the diet. The same result is seen when a child is inadvertently reintroduced to one of theseoffending fo ods. Perhaps, for example, the content of a particular brand of baked beans ischanged without notice, by the introduction of gluten. The child's behaviour may change but alsohis tendency towards a restricted diet may well reappear. We would stress, yet again, that removalof staple elements of the diet are likely to result in reduced intakes of vitamins and minerals andother essential nutrients. A good, balanced, supplement system should be instituted. This is bestdone with the ac tive input of a knowledgeable professional who is sympathetic to andunderstanding of these approaches. Without appropriate levels of these essential nutrient elementsthe normal metabolic processes of digestion and absorption will be severely impaired in any case.
Stage B: Detoxification
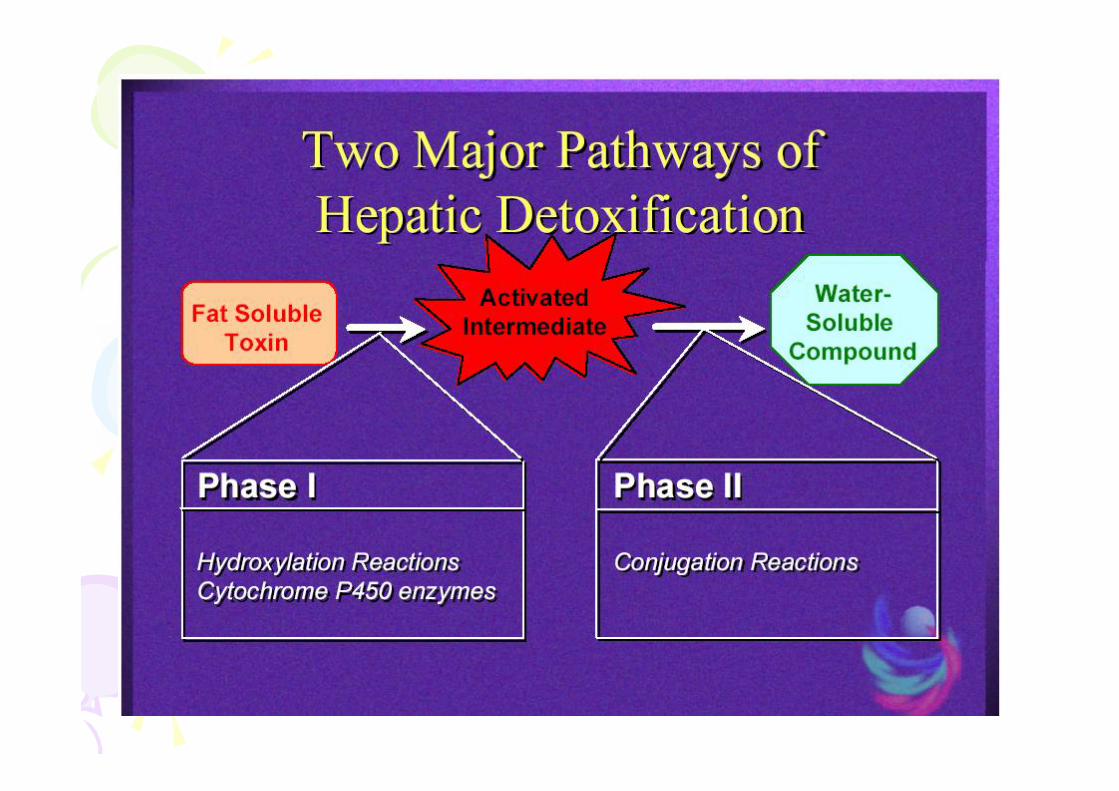
5. Impaired Liver Detox Pathway - Sulphotransferase and Phenolic Foods
Interest in these aspects came about as a result of parental observation and study. Parentsobserved that particular foods appeared to result in the appearance of bad behaviours in theirchildren. These foods such as apple juice, citrus fruits, chocolate and paracetamol were preciselythose that were known to precipitate migraine attacks in susceptible individuals. The parents alsonoted the high incidence of migraines within the families of people with autism. These observationsset the parents, who were without formal training in these areas, to biochemistry textbooks. Theynoted that certain enzymes tended to be functioning sub-optimally in migraine and wondered if thesame situation pertained in autism. They coerced Rosemary Waring, a well-known resea rcher intothese aspects, into testing a group of children with autism. The results were published some yearsback (1997) and have only recently been replicated and extended in dramatic fashion by Alberti(1999) and recently by Waring herself (2000a).
It would seem that the sulphotransferase systems are functioning at sub-optimality in people withautism. There are a number of consequences including effects upon the metabolism of classicalneurotransmitters; impaired breakdown and metabolism of the bile pigments bilirubin and biliverdin;impaired action of the hormone CCK which would result in decreased secretion of bile from the gallbladder and biliary tract into the intestines. This could, once again, result in low uptake of certainvitamins and oth er nutrients from the intestines; reduced activity of gastrin is the stomach (andsubsequent reduced secretion of stomach acid, mucus and pepsin in the stomach (and perhapsreduced production of secretin and absorption of other vitamins further downstream
Perhaps of even greater importance is the effect on intestinal permeability. The intestines are linedwith a slimy layer of mucoproteins. This layer, as well as containing important immunoglobulins(specifically of the IgA class), provides lubrication and protection for the intestinal wall as foodpasses down the alimentary canal. These mucoproteins must be sulphated if they are to becontinuous, protective and effective. If they are not sulphated, the proteins clump together andleave exposed intestinal material and so the transport of peptides into the tissues will beencouraged.

12
The role of sulphation may well be one of the pivotal factors in the causation of autism yet it ispoorly understood and has received scant attention. The role of sulphate in the immune system, inthe effectiveness of hormones and in maintaining the integ rity of intestinal function, kidney functionand detoxification systems is deserving of much greater attention than it currently receives. Owens(1998) has drawn the attention to the importance of sulphation issues in chemical bodies calledGAGs (Glucosyl Acetyl Glucosamines) which have huge implications for many functions includingbrain development. Processes involving inflammation, such as that which would result frominfections that may be acquired naturally or from introduction through vaccine programmes, willresult in stripping of the sulphate containing GAGs from the intestinal wall. Owens has suggestedthat these GAGs will form the main reservoir of sulphates held in the body. Therefore, any lingeringinflammatory process will result in sulphate depletion. Waring (2000b) has also presented dataindicating that the conversion of sulphite to sulphate is severely inhibited after immunisation ofadult students against hepatitis B.
Ever since the days of the Feingold Diets people have been aware that foods high in salicylatesmay be problematic for people with autism. Salicylates (such as aspirin) are used medicinally fortheir anti-inflammatory, antipyretic (temperature lowering) a nd anti-pain properties. These effectsare achieved by blocking the actions of enzymes called COX1 and COX2. These enzymes, as wellas causing the production of inflammatory and other responses, are necessary for the productionof certain prostaglandins essential for the maintenance of intestinal integrity. Drugs such as aspirin,which inhibit COX1 reactions, will have serious effects on the intestines and lead to greatlyenhanced permeability especially in susceptible individuals. Some parents find it advisable to avoidsuch foods as almonds and others containing salicylates. For others, no such problems exist.
Sulphate ions are only poorly absorbed from foodstuffs but may well be absorbed through the skin.That is the rationale for the use of a cupful of Epsom Salts (Magnesium Sulphate) in the bathwaterof children with autism. Some parents are experimenting with home made "patches" containingcrystals of Magnesium Sulphate. The intention is that small amounts of the salt are absorbedthrough the skin on a continuous basis. Alternatively, Methyl Sulphonyl Methane (MSM) may begiven orally in an attempt to eleva te blood sulphate levels. Efficacy has not, however, beendemonstrated in terms of appropriate clinical trials but the body of anecdotal evidence isimpressive.
6. Supplementary Enzymes
If the peptides in the gut are not being broken down adequately, this could be a result of insufficientlevels of peptidase enzymes. For many years, parents of children with hyperactivity have beenutilising enzymes (orally) to ameliorate the problems. Many such products are on the market. Someof the plant-derived enzymes are particularly effective and we are aware of many parents who feelthat the enzyme from pineapples, bromelain produces beneficial results. Bromelain has a particularadvantage over so me of the other naturally occurring enzymes as it is known to break down theTyrosine-Glycine links which are crucial to the opioid activity of so many of these biologically activepeptides. Many of these products contain another enzyme "papain" which is also plant derived.However, we have come across a few instances where it appears that an allergy to this compoundexists

13
7. Heavy Metal and Mineral Testing
There are certain patterns, which are common. Some children are very low on calcium andmagnesium and the remedy is obvious. Others are high in toxic substances such as aluminium.The addition of supplementary zinc is said to remediate this situation. Zinc supplementation is, inany case, probably desirable since so many normal metabolic reactions require it. There are norigorous scientific studies which demonstrate effectiveness in ameliorating the symptoms of autismbut there are numerous anecdotal rep orts which support its effectiveness. Waring (2000) hasreported that the addition of trace amounts of Molybdenum has dramatic effects in correctingabnormalities in sulphate and sulphite levels. It is at this point that we do mineral and heavy metalassessments.
Stage C: ACTIVE RECONSTRUCTION – Heal the intestinal lining
The ultimate aim of these interventions must be to make it possible to eat a diet as near aspossible to normal. If, for example, we can reduce the levels of potentially harmful peptides in theintestines or decrease the permeability of the intestinal wall and/or the blood brain barrier (BBB) wecan minimise the risk of harm. This is the aim of the elements of the "Reconstruction Phase".
8. Fatty Acids (Fats and Oils)
There is a popular misconception that fats act as nothing more than storage systems for energy oras packing material. Only recently has it become acknowledged that fats have a very significantrole in the metabolism and development of the body. There exists a clear need for a greaterunderstanding of the role of fatty acid metabolism in the maintenance of membrane permeabilitythroughout the body. There are intriguing data being produced (Kane 1999 and Cosford 2000) but,as yet, there is no total consensus on which elements are of relevance and which are not. At thispoint we hesitate to make definitive statements about which interventions are appropriate and wemust suggest that those interested in the topic obtain advice elsewhere until the position clarifies..
Many have extolled the benefits of flaxseed oil; of cod liver oil; of olive leaf oil and many others butfor a variety of reasons. Evidence is accumulating that any intervention should involve a balancedapproach of (what are termed) Omega 3 and Omega 6 acids rather than gross overloading of oneform. One element in which there does seem to be universal agreement is the use of EveningPrimrose Oil. The benefits may be a consequence of its containing acids that are incorporated intothe structures of those prostaglandins required to maintain intestinal integrity. (Even here, it issuggested that it should be avoided where there is a risk of epilepsy.) Kane's work is controversialand her explanations are not accepted by all but we are in overall agreement with the sequence forutilisation of fats and oils she proposes.
Evening Primrose Oil; This consists largely of Gamma Linolenic Acid, an Omega 6 acid. There areother, richer sources of Gamma Linolenic Acid, such as Borage (Star Flower) Oil but it is claimedthat this is less well tolerated than the oil from Evening Pr imrose. We are unable to comment uponthat. It is probably wise to saturate with these before attempting to balance with Omega 3containing oils such as those derived from fish. Fish Oil such as Cod Liver Oil. This has the added
14
advantage of including supplementary Vitamin A, which is likely to be, is short supply in people withautism (Megson 1999).
Flax Seed Oil – A rich source of Omega 3 acids. The objective, as far as we are concerned, ofthese interventions with fatty acids is to ensure that the membranes lining the cells of the intestinesand blood brain barrier are permeable to an appropriate degree. Cholesterol is an importantelement in th is. Although there is a current anti-cholesterol feeling, it must be recognised that it isan important element of these membranes and some advocate ensuring adequate levels of thefatty acids which will be converted in the body to cholesterol
9. Other Intestinal Nutrients - Betaine (Tri-Methyl Glycine) Hydrochloride
As with the enzymes, referred to above, Tri-Methyl Glycine (TMG) has been used for many yearsin the treatment of hyperactivity even though the mode of action has remained unclear. Thiscompound will, by slowly releasing Hydrochloric Acid, increase the acidity of the stomach contents.There is soft evidence that some people with autism have insufficient acid in the stomach(achlorhydria) and that, as a consequence, the stomach enzymes act inefficiently to break downthe proteins. It may also be of relevance to consider that secretin is produced in the intestines as aconsequence of acid in the stomach. Thus, if there is insufficient acid there could be reduced levelsof secretin produced.
As with Di-Methyly Glycine, it is possible that any activity is dependent upon totally differentmechanisms. The role of DMG and TMG in cysteine metabolism is very well known. Alternatively,these compounds could, conceivably, have direct neurotransmission effects or act as a source ofglycine which is always in demand within the body. It is our opinion that this compound has little, ifdown here and will not be available for absorption lower down in the intestines.
10. Sanum Therapy
Sanum therapy consists of the use of specific microbiological products. These products have beenused for more than thirty years in Europe. Among one of the conditions for which there isconsiderable clinical evidence is regeneration of the damaged intestinal villi and the nearrestoration of the Gut Lymphoid Tissue (GALT).
Stage D: WHAT’S NEXT?
11. AMINO ACID TESTING
There are number of disorders which can result directly from amino-acid irregularities.Histidinaemia; PKU; Homocysteinuria and others could be involved in the causation of symptoms.Tests to rule out these gross problems should be performed routinely. There is considerablyanecdotal evidence that certain amino acids are beneficial to people with autism. Supportiveevidence tends to be lacking but supplementation could be considered and, in any case, their useis unlikely to cause any harm. L-Glutamine ha s found favour amongst many parents even thoughthe precise mode of action is unknown. It is used routinely in medicine to encourage growth of villi

15
and thereby improve absorption from the intestines. It has been suggested that glutamine levels, inthe blood, are low in people with autism in any case so supplementation may be no bad thing.
5-Hydroxy Tryptophan (5HTP) is a metabolite of the amino-acid tryptophan and is used in theformation of the transmitter substance serotonin. It may be that serotonin levels, in the areas whereit is required, are low and that supplementation with 5HTP is helpful. Many people feel that this isthe case although, once again, evidence of efficacy in autism is lacking. The theoretical conceptsare outlined by Shattock (1999).
It is at this time that further testing may be appropriate. There is no doubt that many of our childrenhave abnormal levels of minerals, vitamins and other materials in their systems. However, the trueposition is often obscured by the presence of the smokescreen resulting from gluten and caseinconsumption. It is now, after the removal of these offending dietary protein sources, thatmeaningful testing can be performed. On a number of occasions, parents have sent us the resultsof vitamin and mineral status determinations (on hair or blood) taken before and after gluten andcasein removal.The before results have been very abnormal indeed and the results followingexclusion of the offending proteins have shown normal patterns. We have interpreted this as anindication that the intestinal function has been partially restored by the removal of these elements;that dietary vitamins and minerals are now being absorbed as they should but there may, ofcourse, be other mechanisms involved.
We always suggest that anybody initiating a restrictive diet should take care to ensure an adequateintake of minerals and vitamins and for this reason we advocate the involvement of a qualifieddietitian or equivalent. We suggest a balanced multivitamin and multimineral supplement just toensure adequate levels. If these measurements are performed pre-diet, severe abnormalities maybe evident and remedial action in the form of a grossly unbalanced programme may be initiatedinappropriately. It is probably better to wait until this stage.
12. TESTING FOR ESSENTIAL FATTY ACIDS
Although definitive evidence has yet to be presented, it would appear that there are abnormalitiesin the fatty acid content in the circulating bloodstream as well as in the bound forms and there is noagreement as to whether circulating levels accurately reflect the situation in membranes. Given theinstability of these membranes and the fact that analyses are rarely performed immediately aftercollection there must still be some doubt about the reliability of any but the most carefully collecteddata. We use a standard EFA formula that has been documented to be useful in cases of childrenwith PDD. Subsequently we test the EFA status to check if the situation is table or not.
13. OTHER TESTS
We have also observed that classical allergies will frequently "disappear" when gluten and caseinare removed from the diet. At the same time, certain underlying and genuine allergies are revealed.For this reason, we believe that the most appropriate time for testing for allergies is after theremoval of the main offending foods. If allergies are suspected such interventions are worthy ofconsideration. We have come across numerous individuals who were tested, using VEGA (skinconductance) type tests, be fore initiating any interventions. These tests usually result in 30 or 40

16
different products showing up as positive but subsequent to gluten and casein removal thesenumbers have been dramatically reduced. In some cases, children have been deprived of foodswhere the "allergies" which were detected before the other interventions are of no clinicalrelevance.
Hospital based laboratories tend to test blood for antibody levels (IgE in particular) to indicate"allergy" towards particular foodstuffs. In the UK at least, the results of these tests are notnecessarily communicated in full to parents. Traditionally they are rated at somewhere between 0and 4 (4 being the highest). Levels of 0 and 1 are pretty common and are usually ignored whereashigher numbers should be taken more seriously. It must be understood that these levels are nomore than a snapshot at a particular time and it may be appropriate to consider removal ofoffending food on a trial basis at some time in the future.
We believe that the relevance of these, genuine, allergies has been grossly underestimated in thepast and that research should be directed towards these areas. Avoidance of the allergen is theobvious therapy but there may be other alternatives. Enzyme Potentiated Desensitisation (EPD)techniques are employed by a limited number of practitioners who feel that it is effective. It has notbeen subjected to rigorous evaluation and practitioners in the US have attracted censure forutilising it.
We would like to stress that although we do not believe that classical allergy to casein or to glutenare heavily implicated in the causation of most cases of autism, it is important that this possibilitybe checked before their removal from the diet. It is, of course, of no value to perform such testsafter the potentially offending foods have been removed from the diet for any period of time. It isalways unfortunate when parents are required, quite correctly perhaps, by physicians toreintroduce gluten and casein to the diet so that allergy testing can be performed. Although thesereintroductions will almost invariably result in deterioration in the performance and abilities of thesubject, equally invariably, the tests have given entirely negative results. For this reason, weadvocate the testing for gluten and casein allergies (but not other allergies) before the introductionof restrictive diets involving their exclusion. We may also consider genetic testing if there aresufficient reasons to do so.
Stage E: ADDITIONAL IINTERVENTIONS
The following interventions have been placed in this comparatively late position in the protocol for avariety of reasons. The use of diets devoid of colour or salicylates, although supportable ontheoretical grounds and by experimentation in vitro (Waring 1999) is not easy to maintain andparents initiating these comparatively restrictive regimes do not find it easy to justify their actions toorthodox health professionals. Similarly the use of secretin must still, at this stage, be seen asexperimental rather than routine. As the newer and purer versions of the product become availableand evidence of safety and efficacy appears this situation may well change. Even the use of highdoses of Vitamin B6 is frowned upon as there are theoretical risks associated with its use. The useof DMG would not attract such criticism but since we do not know the reasons for any effectivenesswe were unable to allocate a ration al place in our protocol.

17
14. 5-HTP (5-HydroxyTryptophan)
The Mechanism we have proposed involves a pivotal role for Indole Acrylic Acid (I.Acr.A) which isan unusual metabolite of the amino-acid tryptophan and the immediate precursor of Indole AcryloylGlycine (IAG) which have been reported as being present in abnormally high quantities in the urineof people with autism. It has been suggested that this distortion of the normal pathways in favour ofthis route may be a consequence of partial inhibition of the enzyme tryptophan hydroxylase. This isthe enzyme respons ible for the conversion of tryptophan to 5-hydroxytryptophan (5-HTP) which isthen converted to 5 hydroxytryptamine (serotonin or 5-HT). Thus, an inhibition of the enzymetryptophan hydroxylase would result in an increase of the potentially harmful I.Acr .A and areduction in available serotonin throughout the body. he obvious remedy would be to providesupplementary tryptophan but there are two problems with this. Firstly, if the enzyme activity isdiminished as proposed, the tryptophan will be converted to I.Acr.A which is undesirable. Secondly,tryptophan is now only available as a prescription medicine in most of the world.
This banning of over the counter sales of tryptophan is unusual and controversial given the historyof the product but, in any case, the use of 5-HTP would be more appropriate. Once again, the onlyreports of usefulness are anecdotal but its use is both logical and unlikely to result in side effects.
15. Phenol (Pigment) Free Diet
It would seem that this sub-optimality of sulphotransferase activity is a function of low plasmasulphate levels rather than of deficits in the actual enzyme. Thus, any foodstuff requiring or usingup sulphate ions during its metabolism, will make the situation worse. These foodstuffs will includeapple juice, citrus fruit juices, chocolate and paracetamol. In fact, any chemicals with a highproportion of phenolic groupings will have this effect and enhance the problems referred to above.Many colouring materials, whether of natural or synthetic origin, possess phenolic groupings. Forthis reason, some practitioners recommend the removal of all pigmented foods from the diet. Ofcourse, the earliest dietary interventions to gain publicity (Feingold Diets) were heavily dependentupon the removal of synthetic colorants especially those given E numbers. Some of the negativepublicity for these products may result from a feeling o f distaste for these unnecessary additions toour food but for some people they are of significance. Except in a very few isolated instances wehave not seen great changes in people with autism when pigmented materials are removed unlessother elements ar e removed as described above.
There are those (perhaps the majority) in whom these foodstuffs, including paracetamol(acetaminophen), seem to make no difference at all but there are individuals who would be welladvised to avoid such products. Once again, it is a question of assessing the effects on eachindividual.
16. Megadose Vitamin B6 and Magnesium
Very high levels (500 - 1000mg/day) of Vitamin B6 (balanced by magnesium another vitamins ofthe B group) are advocated and many claim benefits from such usage. There are theoretical risksinvolved and attempts have been made, in the US as well as the UK, to limit availability. However, Iam unaware of anyone who has ever seen the deleterious effects described in the literature.

18
17. Di-Methyl Glycine (DMG)
Di-Methyl Glycine would appear to be a safe, and in some cases, useful supplement but, onceagain, the encouraging observations of parents and some professionals have yet to bedemonstrated by clinical investigation.
18. Other Supplements
There exists a plethora of substances which whilst, strictly speaking, are not medicines in the legalsense of the word, do have actions which push the borders between what could be considered as"Nutritional Supplements" and are sold accordingly. For example, Gingko (biloba) has been usedextensively for its action in increasing blood flow and, therefore, the supply of oxygen to the brain.Ginger, Liquorice and other herbal products are also being used on account of their effects uponthe gastro-intestinal tract and may have a place once more information becomes available.Although not food supplements in any sense of the word, the use of chelating agents will have tobe considered at some point. For a considerable period of time there have been insistent voicesconcerned about the potentially seriously harmful effects of mercury in children with autism.Indeed, there are closes parallels between the known effects of mercury and the symptoms ofautism. Evidence is beginning to emerge which suggests a greatly increased mercury burden inpeople with autism. This only becomes apparent when chelating agents are employed to removeheavy metals from the body. Research is currently being conducted to test these hypotheses andat this stage we feel it inappropriate to discuss the utilisation of these chelating agents. Thepotential for side-effects is unacceptably high for self-medication and such treatments should onlybe attempted under experienced medical supervision. Clearly this is an area that warrants veryclose attention.
19. CRANIOSACRAL THERAPY
Craniosacral therapy has been found to be useful when there are clinical signs of structuralabnormalities due to birth trauma, forceps delivery or the use of the vacuum.
Conclusions
Interventions involving manipulations in diet, in terms of avoiding certain components or takingdietary supplements are being increasingly used for autism spectrum disorders as well as manyother conditions. Western cultures are geared very much towards the use of drugs, often syntheticand very potent, to give symptomatic relief for particular problems which interfere with the quality oflife of the affected individual. This approach is acceptable only up to a point. Parents and carersare becoming increasingly interested in the processes which may underlie the symptoms and,where possible, intervening and thereby minimising the presentation of the symptoms. For sure,the predisposition, the fragility, the seeds of the autism will remain but by minimising the triggeringfactors amelioration of the problems is possible.____________________________________________________________________________
19
References
Alberti A., Pirrone P., Elia M., Waring RH and Romano C. (1999) "A sulphation deficit in autisticchildren: a pilot study" Biological Psychiatry, 8, 420-424.
Cade R., Wagemaker H., Privette M., Fregly MJ., Rogers J., Orlando J. (1990) "The effects ofdialysis and diet on schizophrenia" Psychiatry: A World Perspective, 3, 494-500.
Cosford R. (2000) "Vaccination, Early Infections; Antibiotic Use and the connection withGastrointestinal Dysbiosis and Autism in Children" Lecture at Autism-Europe Congress, Glasgow,May 2000.
Dohan FC. (1966) "Cereals and Schizophrenia - data and hypothesis" Acta Psychiatrica Scand.,42, 125-
D'Eufemia P., Celli M., Finocchiaro R. (1996) "Abnormal intestinal permeability in children withautism" Acta Paediatrica, 85,1076-1079.
Gillberg IC., Gillberg C. (1996) "Autism in immigrants: a population based study from Swedishrural and urban areas" J. Intell. Disability Research. 40 24-31.
Horvath K., Stefanotis G., Sokolski KN. (1998) "Improved social and language skills aftersecretin administration in patients with autistic spectrum disorders." J. Assoc Academic MinorityPhysicians, 9, 9-15
Kane P. (1999) Lecture at American Academy of Environmental Medicine Conference. Coeurd'Alene, October 2000.
Knivsberg AM., Reichelt KH., Nodland M. (1995) "Autistic syndromes and diet: a follow-up study"Scand. J. Educat. Res., 39, 223-236.
Lucarelli S., Frediani T., Zingani A., Ferruzzi S. et al. (1995) "Food Allergy and infantile autism"Panminerva Medica 37 (3) 137-141.
Megson M. (1999) Lecture presented at the Defeat Autism Now conference, Cherry Hills, NewJersey, September 1999.
Murch SH., Macdonald TT., Walker-Smith JH., Levin M., Lionnetti P., Klein NJ (1993)"Disruption of sulphated glycosaminoglycans in intestinal inflammation." Lancet (1993), 711-714.
20
Owens SC. (1998) "Exploration of the New Frontier between Gut and Brain: A look at GAGs, CCKand Motilin" in "Psychobiology of Autism: Current Research and Practice" Conference held atUniversity of Durham published by Autism Research Unit, University of Sunderland, 45 - 70.
Panksepp J. (1979) "A neurochemical theory of autism." Trends in NeuroScience, 2, 174-177.
Reichelt KL., Hole K., Hamberger A., Saelid G., Edminson PD., Braestrup CB., Lingjaerde O.,Ledaal P., Orbeck H. (1981) "Biologically active peptide-containing fractions in schizophrenia andchildhood autism." In: Martin JB., Reichlin S., Bick KL (Eds ). Neurosecretion and Brain Peptides,Raven, New York 627-643.
Serroussi K. (2000) "Unraveling the Mystery of Autism" Simon and Schuster, New York, USA
Shattock P., Kennedy A., Rowell F., Berney TP. (1990) "Role of neuropeptides in autism andtheir relationships with classical neurotransmitters" Brain Dysfunction, 3, 328-345
Shattock P., Lowdon G., (1991) "Proteins, peptides and autism Part 2: implications for theeducation and care of people with autism" Brain Dysfunction, 4, 323-334.
Shattock P. (1999) "Environmental factors in the causation of autism" Proceedings from theconference "From Research into Practice" held at the University of Durham April 2000, publishedby the Autism Research Unit, University of Sunderland. 163-174
Shaw W. (1998) "Biological Treatments for Autism and PDD" Published by the Author, Kansas,USA
Shaw W. (2000) Lecture at Autism Europe Congress, Glasgow, May 2000.
Waring RH., Ngong JM., Klovrza L., Green S., Sharp H. (1997) Biochemical parameters inautistic children. Developmental Brain Dysfunction, 10, 40-43
Waring R.H. (2000a) Biochemical Parameters in Autism. J.Nutritional and Environmental Medicine10 25-32.
Waring RH. (2000b) "Sulphation in Autism" Lecture at Autism Europe Congress, May 2000.
Whiteley P., Rodgers J., Savery D., Shattock P. (1999) A gluten free diet as intervention forautism and associated disorders: preliminary findings Autism: International Journal of Researchand Practice, 3, 45-65.
Paul Shattock & Paul Whiteley The Sunderland Protocol: A logical sequencing of biomedicalinterventions for the treatment of autism and related disorders.