the not-for-profit hospital corporation
TRANSCRIPT



Page 1 of 2
THE NOT-FOR-PROFIT HOSPITAL CORPORATION BOARD OF DIRECTORS
NOTICE OF PUBLIC MEETING The monthly Governing Board meeting of the Board of Directors of the Not-For-Profit Hospital Corporation, an independent instrumentality of the District of Columbia Government, will be held at 9:00am on Wednesday, March 23, 2016. The meeting will be held at 1310 Southern Avenue, SE, Washington, DC 20032, in Conference Room 2/3. Notice of a location, time change, or intent to have a closed meeting will be published in the D.C. Register, posted in the Hospital, and/or posted on the Not-For-Profit Hospital Corporation’s website (www.united-medicalcenter.com).
DRAFT AGENDA
I. CALL TO ORDER
II. DETERMINATION OF A QUORUM
III. APPROVAL OF AGENDA
IV. BOARD EDUCATION
Confidentiality and FOIA – Traci L. Hughes, Esquire Director, District of Columbia Office of Open Government and Board of Ethics and Government Accountability (BEGA)
V. CONSENT AGENDA
A. READING AND APPROVAL OF MINUTES
1. February 24, 2016 – General Board Meeting
B. EXECUTIVE REPORTS 1. Dr. Julian Craig, Chief Medical Officer 2. Thomas E. Hallisey, Chief Information Officer 3. Jackie Johnson, EVP of Human Resources 4. Pamela R. Lee, EVP Hospital Operations & CQO 5. David Thompson, Director of Public Relations and Communications 6. Maribel Torres, Chief Nursing Officer

Page 2 of 2
7. Charletta Washington, VP of Ambulatory & Ancillary Services
VI. NONCONSENT AGENDA
A. CHIEF EXECUTIVE REPORTS 1. Andrew L. Davis, Interim CEO 2. Finance Report – Steve Lyons, Finance Committee Chair
B. MEDICAL STAFF REPORT
1. Dr. Raymond Tu, Medical Chief of Staff
C. COMMITTEE REPORTS 1. Governance Committee Report 2. Patient Safety & Quality Committee
D. OTHER BUSINESS
1. Old Business 2. New Business
E. ANNOUNCEMENT
Next Meeting – Saturday, April 23, 2016 at 9:00am in Conference Rooms 2/3 on the ground level.
F. ADJOURNMENT
NOTICE OF INTENT TO CLOSE. The NFPHC Board hereby gives notice that it may close the meeting and move to executive session to discuss collective bargaining agreements, personnel, and discipline matters. D.C. Official Code §§2 -575(b)(2)(4A)(5),(9),(10),(11),(14).

1
Not-For-Profit Hospital Corporation
General Board Meeting Minutes February 24, 2016
Present: Chris Gardiner, Chairman, Girume Ashenafi, Dr. Julian Craig, Andrew Davis, Dr. Konrad Dawson, Maria Gomez, Steve Lyons,
Virgil McDonald, Robert Malson, Khadijah Tribble, Dr. Raymond Tu, Donna Freeman (Corporate Secretary), Kai Blissett (General Counsel)
Excused: Public: Pamela Gray, S B & Company, LLC Agenda Item Discussion Action Item Call to Order The meeting was called to order at 9:20am Determination of a Quorum
A quorum was determined by Donna Freeman, Corporate Secretary.
Approval of the Agenda
Chairman Chris Gardiner requested the Audit Committee report be moved to the beginning of the agenda. The Board moved and seconded the change and approved the agenda.
Board Education Session
Thomas Hallisey, CIO reviewed UMC email, and the board portal overhaul. Kai Blissett, General Counsel, discussed the Office of Open Government, Board of Ethics and Government Accountability (BEGA) and the training available to Board members.
Approval of Minutes
Correction: the date for the next General Board meeting will be February 24, 2016 not March 23, 2016. The minutes were approved with the necessary correction.
Consent Agenda
N/A

2
Non Consent Agenda
N/A
Executive Reports The following Executive Reports were moved. Seconded. Passed unanimously. • Dr. Julian Craig, Chief Medical Officer • Jackie Johnson, EVP, Human Resources
• Maribel Torres, CNO • Tom Hallisey, CIO • David Thompson, Director of Communications and Public Relations • Charletta Washington, VP of Ambulatory & Ancillary Services
FY 2015 Audit Pamela Gray of S B & Company, LLC, provided an overview of the FY 2015 audit for UMC. Ms. Gray shared observations and recommendations for UMC going forward. The final report should be completed within 7-10 working days. Ms. Gray and staff will be working closely with Ms. Chukwuma, CFO on an on-going basis. An extensive discussion continued regarding the relationship with the OCFO’s Office and the former and current auditors.
Chief Executive Reports
Andrew Davis, Interim CEO, presented CEO Report. (Report presented to Board Members) Board moved to accept and approve the CEO report. Seconded. Passed unanimously. The following highlights were discussed: • The UMC mission and vision statement voted on in 2014 will remain. • A values statement is currently the focus and a strategy is being formed to include input from UMC staff and board members. • Positive results were shared about UMC during the Oversight Hearing chaired by CM Yvette Alexander. • In 2015 the consistent rise in the patient satisfaction surveys • The formation of a Patient Family Advisory Board and a Community Benefits Committee. • Three (3) new family medicine physicians will be joining UMC in late 2016. • Introduced Lilian Chukwuma as our new CFO and Perry Sheeley as our new Controller. • Robert Malson was acknowledged for his retirement and his last meeting as a board Member.
Khadijah Tribble requested a report to determine how the different marketing techniques are penetrating our target market. Virgil McDonald requested a report updating the status of physician recruitment funds awarded by the District.

3
Finance Committee Report
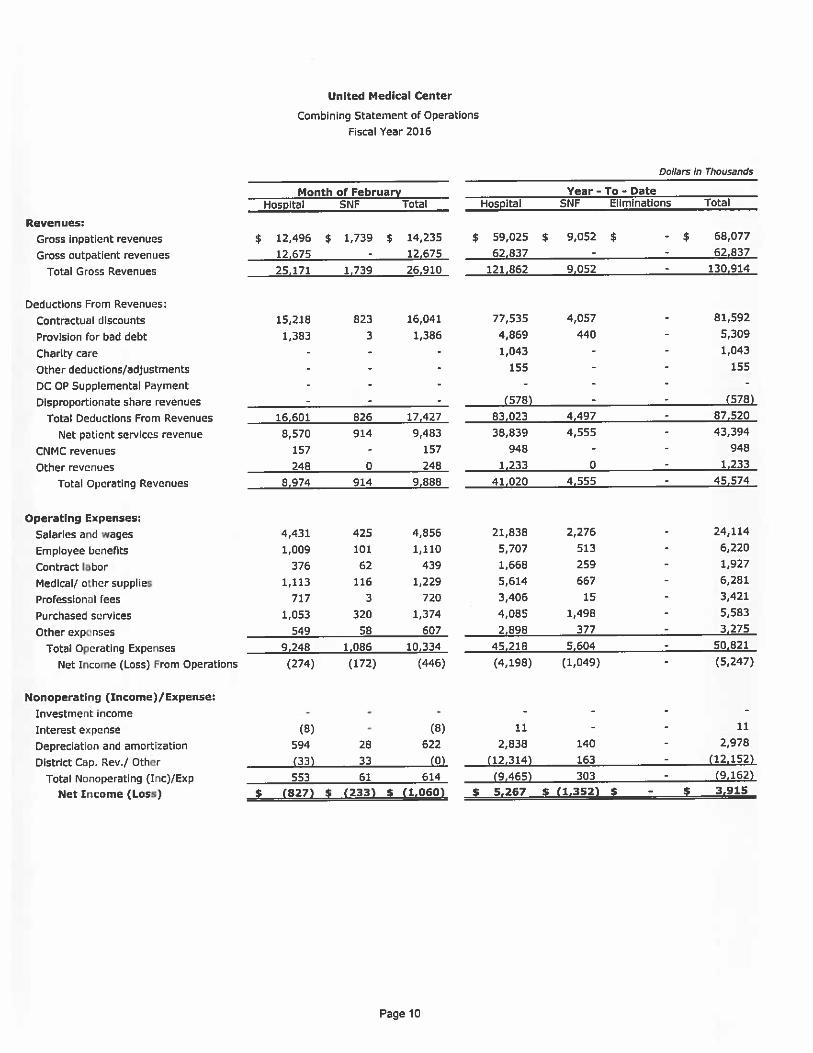
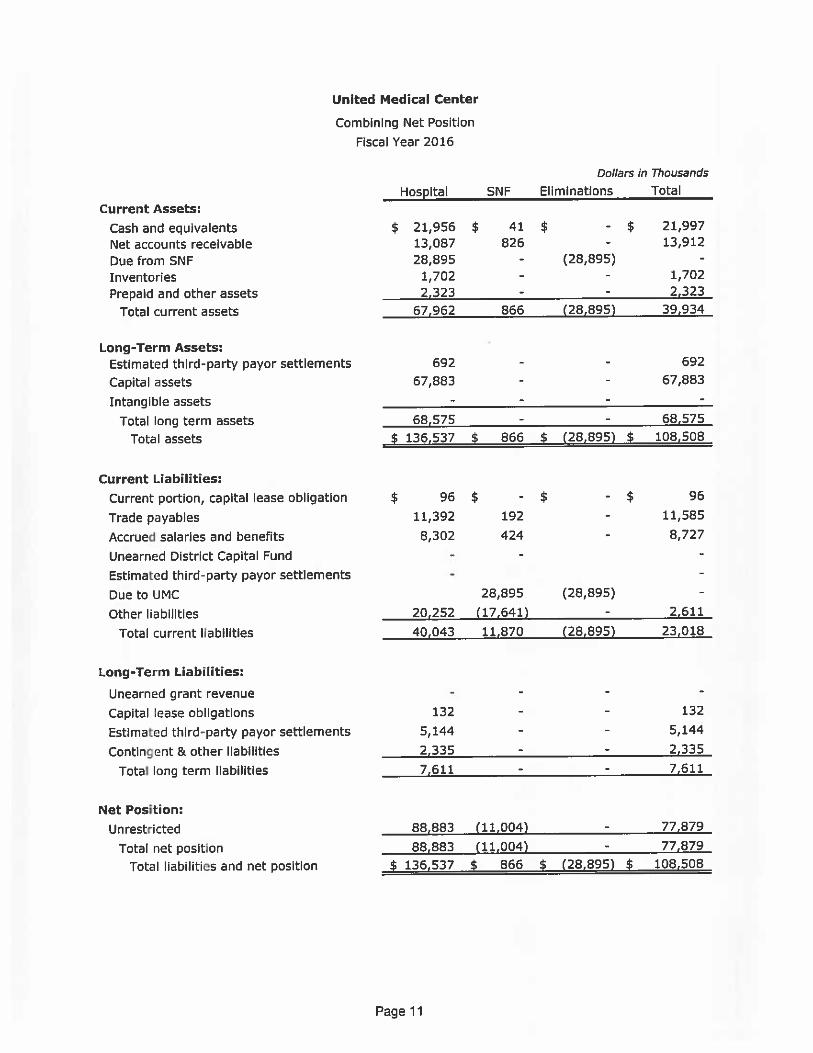
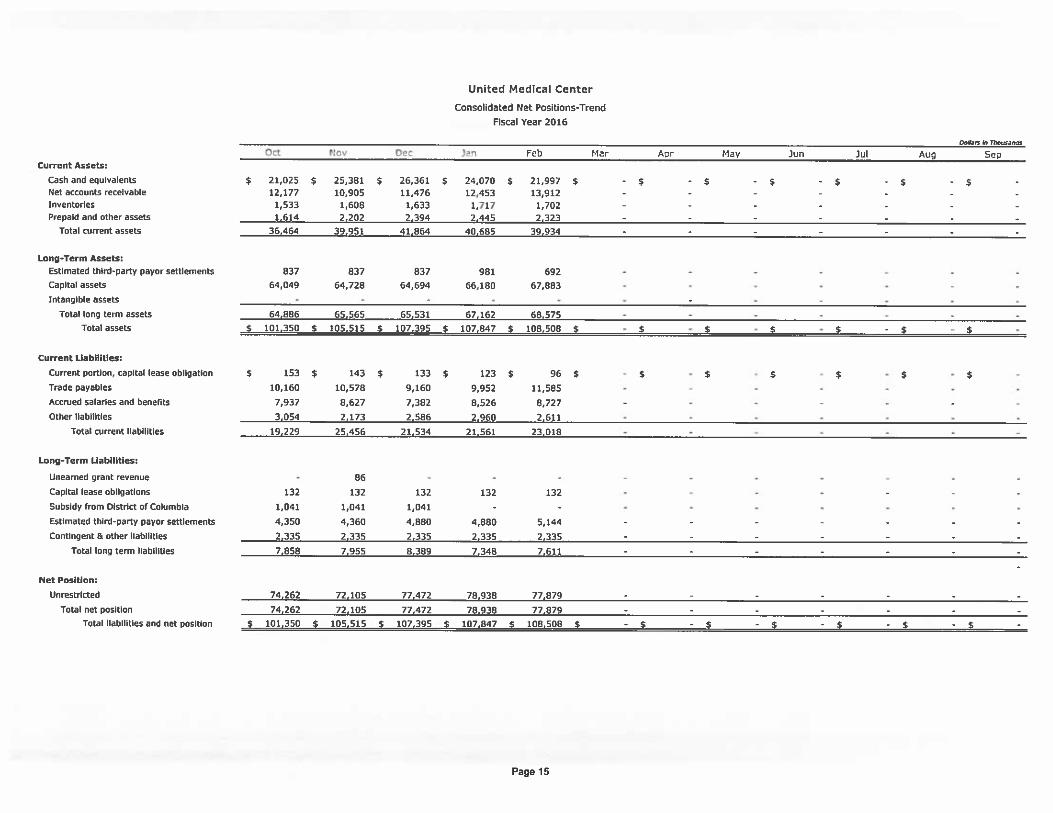
• UMC held their first community education session on the Healthy Heart in February. • An extensive discussion was held regarding physician productivity. Steve Lyons, Finance Committee Chairman presented the financials for UMC. (Reports presented to the Board Members and filed in the Office of the Secretary of the Corporation) Lilian Chukwuma, CFO reviewed the process of calculating expenses and projecting revenues. The Finance Committee Report was approved. Seconded. Passed unanimously.
Dr. Konrad Dawson requested a breakdown of the legal costs incurred by UMC in 2015. Khadijah Tribble requested Finance to consider reporting the cash flow in the Dashboard format.
Chief Medical Report
Dr. Raymond Tu, Medical Chief of Staff, presented the Credentialing report. The Board moved to accept and approve the credentialing report. Seconded. Passed unanimously. (Report presented to Board Members and filed in the Office of the Secretary of the Corporation)
Governance Committee Report
Virgil McDonald, Committee Chair, presented the Committee Report. Moved. Seconded. Passed unanimously. The following highlights were discussed: • Kai Blisset, General counsel, provided an update on the following: ◦ Dr.(s) Julianne Malveaux and Ricardo Brown, their service has ended and they will not be reappointed to the Board. ◦ Two Mayoral appointees are being reviewed to replace the vacancy. ◦ Two Council appointee seats are vacant also. ◦ The new DCHA president will fill R. Malson’s seat once selected. • Board Meeting Evaluation Summary was discussed. • Board Self-Assessment Survey Form
Virgil McDonald requested the Board members to submit their evaluation forms to Donna Freeman.
Chairman Chris Gardiner announced the General Board meeting will go into Executive Closed Session.
Chairman Chris Gardiner reconvened the public General Board meeting @ 12:30 p.m. Audit Committee Girume Ashenafi, Committee Chair answered questions regarding auditors report. Other Business
Old Business Chairman Gardiner explained the details of the Restructuring Plan. An extensive

4
discussion of the financial condition continued. The status of the Revenue Cycle and its efficiency was discussed.
New Business Three (3) board members whose terms have expired; letters of appreciation will be sent acknowledging their service to the Board. Chairman Gardiner suggested including Saturday General Board Meetings on the schedule. The dates proposed are April 23, 2016 and July 23, 2016. More details to follow. The Annual Meeting is usually on Saturday which may be included in the total of three.
Announcement The next General Board meeting is scheduled on Wednesday, March 23, 2016 at 9am in Conference Rooms 2/3 on the ground level.


Chief Medical Officer Julian Craig, MD
Board Report March 2016

MEDICAL STAFF SUMMARY
MEDICAL STAFF COMMITTEE MEETINGS
Medical Executive Committee Meeting, Dr. Raymond Tu, Chief of Staff
The Medical Staff Executive Committee (MEC) provides oversight of care, treatment, and services provided by practitioners with privileges on the UMC medical staff. The committee provides for a uniform quality of patient care, treatment, and services, and reports to and is accountable to the Governing Board. The Medical Staff Executive Committee acts as liaison between the Governing Board and Medical Staff.
Peer-Review Committee, Dr. Gilbert Daniel, Committee Chairman
The purpose of peer review is to promote continuous improvement of the quality of care provided by the Medical Staff. The role of the Medical Staff is to provide evaluation of performance to ensure the effective and efficient assessments and education of the practitioner and to promote excellence in medical practices and procedures. The peer review function applies to all practitioners holding independent clinical privileges.
Pharmacy and Therapeutics Committee, Dr. Mina Yacoub, Committee Chairman
The Pharmacy and Therapeutics Committee discusses all policies, procedures, and forms regarding patient care, medication reconciliation, and formulary medications prior to submitting to the Medical Executive Committee for approval.
Credentials Committee, Dr. Barry Smith, Committee Chairman
The Credentials Committee is comprised of physicians who review all credential files to ensure all items such as applications, dues payment, etc. are appropriate. Once approved through Credentials Committee, files are submitted to the Medical Executive Committee and the Governing Board.
Medical Education Committee, Dr. David Reagin, Committee Chairman
The Medical Education Committee was formed to review all upcoming Grand Rounds presentations. The committee discusses improvements and new ideas for education of clinical staff.
Performance Improvement Committee, Committee Chairman
The Performance Improvement Committee is comprised of 1-2 representatives from each department who report monthly on the activity of each department based on

standards established by the Joint Commission, the Department of Health, and the Centers for Medicare and Medicaid Services (CMS).
Bylaws Committee, Dr. David Reagin, Committee Chairman
Members include physicians who meet to discuss implementation of new policies and procedures for bylaws, as it pertains to physician conduct. The Medical Staff Bylaws, Rules and Regulations have been revised in preparation for the upcoming Joint Commission inspection. The changes were reviewed, discussed and approved by the Bylaws Committee and will be forwarded to the Medical Executive Committee and then the Board of Directors for review and approval.
Physician IT Committee,
Members include physicians who meet to discuss the implementation of the new hospital-wide Meditech upgrade, as well as the physician documentation for ICD-10.
Physician Champions Meditech Program
Julian Craig, MD Gilbert Daniel, MD Russom Ghebrai, MD Cynthia Morgan, MD
Raymond Tu, MD Deborah Wilder, MD Mina Yacoub, MD

DEPARTMENT CHAIRPERSONS
Anesthesiology .................................................................. Dr. Amaechi Erondu (Medical Director)
Critical Care .......................................................................................................... Dr. Mina Yacoub
Emergency Medicine ........................................................ Dr. Mehdi Sattarian (Medical Director)
Medicine ............................................................................................................... Dr. Musa Momoh
Obstetrics and Gynecology ............................................................................ Dr. Sylvester Booker
Pathology .............................................................................................................. Dr. David Reagin
Pediatrics ....................................................................................... Dr. Marilyn McPherson-Corder
Psychiatry ............................................................................................................... Dr. Lisa Gordon
Radiology ................................................................................................................ Dr. Raymond Tu
Surgery ............................................................................................................ Dr. Gregory Morrow

DEPARTMENTAL REPORTS

ANESTHESIOLOGY Dr. Amaechi Erondu (Medical Director)
PERFORMANCE SUMMARY:
For the month of February, 2016, the Anesthesia Department had a total surgical and Obstetric anesthesia volume of 221 surgical cases. Our top 3 service providers remain: Gastroenterology, Vascular surgery and General surgery in that order. This is a volume growth from 176 the previous month.
QUALITY INITIATIVES AND OUTCOME:
Mortality and Morbidity Reviews:
No mortality was recorded in the OR this past month.
No anesthesia related morbidity was recorded.
ACUTE PAIN MANAGEMENT SERVICE (APMS)
The department is developing a protocol to commence an Acute Pain Management Service starting with our Surgical Patients. The service will evolve from the O.R. through the transition of patient care to the floor during the acute phase of surgical procedure and recovery.
EVIDENCE-BASED PRACTICE:
Anesthesia department is continuing to review all current policies and update them to align with the best practices and CPOE requirements. This will facilitate the evolution of the department into a Peri-operative service model and to include appropriate Care Coordination.
SERVICE (HCAHPS) SATISFACTION
Anesthesia Department has implemented the “Qualitick” program for real-time performance assessment of the anesthesia providers. Through this method, Patients and Surgeons will assess the anesthesia providers and give feedback. We would continue to rely on the Press Gurney for system wide performance assessment.

CRITICAL CARE Dr. Mina Yacoub ____________________________________________________________________________
PERFORMANCE SUMMARY
In February 2016, the Intensive Care Unit had 335 patient days, 72 admissions and 75 discharges. The ICU managed a total of 85 patients in February with a noted increased acuity. ICU Average Length of Stay (ALOS) was 4.6 days. QUALITY OUTCOMES Core Measures Performance ICU met and exceeded target goals for Venous ThromboEmbolism prophylaxis for the first two months of 2016. ICU is at 98% compliance. ICU is continuing to work with Quality Department and is monitoring performance.
1. Morbidity and Mortality Reviews February morbidity and mortality data was presented at March Critical Care Committee meeting. There were eleven ICU deaths in February for a mortality rate of 12.9%. Two cases are referred to Quality Dpt. for review.
2. Code Blue/Rapid Response Teams (“RRTs”) Outcomes ICU continues to lead, monitor and manage the early intervention Rapid Response and Code Blue Teams at UMC. Reports are reviewed in Critical Care Committee meetings.
3. Ventilator Associated Event (VAE) bundle ICU continues to implement evidence-based best practices for patients on mechanical ventilators and the ICU has had no Ventilator Associated Pneumonias (VAPs) for the month of February 2016.
4. Infection Control Data For the month of February 2016, ICU had no Ventilator Associated Pneumonias (VAPs), no Central Line Associated Blood Stream Infections (CLABSIs), and no Catheter Associated Urinary Tract Infections (CAUTIs). ICU infection control data is reported regularly to the National Healthcare Safety Network (NHSN). Our infection control data is currently being validated by the national Clinical Data Abstraction Center (CDAC). There were 168 ventilator days in February with no VAPs, 168 central line days with no CLABSIs. There was one CAUTI in January and no CAUTIs in February.
5. Care Coordination/Readmissions
For February 2016, 85 patients were managed in the ICU.

6. Evidence-Based Practice (Protocols/Guidelines) Evidence based practices continue to be implemented in ICU with multidisciplinary team rounding, infection control practices and frequent communication with patient families.
Growth/Volumes ICU is staffed 24/7 with in-house physicians and has a 16 bed capacity. ICU experienced increased admissions and patient acuity in February 2016 and is looking forward to maintain this trend.
Stewardship ICU continues to implement and monitor practices to keep ICU ALOS low and to keep hospital acquired infections and complications low. This leads to significant cost-savings for the hospital.
ICU continues to provide teaching opportunities for George Washington University Physician Assistant students through their clinical rotations in UMC ICU. Financials ICU continues to operate within its projected budget. Active Steps to Improve Performance Goal is to continue to provide safe and high quality patient care, caring for patients with increased illness acuity, providing best evidence based practice, all while keeping ALOS low and preventing Hospital Acquired infections and complications. Working closely with Quality Department and Infection preventionist to ensure we continue to meet benchmarks. EMERGENCY MEDICINE Dr. Mehdi Sattarian Performance Summary: Emergency department had a census of 4,842 patients.
February 2016 department metrics:
Patient Volumes: 4,725
% Change from 2015: 23% increase
Ambulance Volume: 1,317 Median Left without Treatment: 0.9 %

Admission Rate: 12.4% Transfers: 54 patients (1.1%) Turnaround time for D/C Patients: 206 minutes
Quality Initiatives, Outcomes, etc.
7. Improving the provider productivity
8. Improving throughput process including a. Door – Provider: 60 minutes b. Door – Disposition: 168 minutes
9. Adverse events (i.e. elopement, suicide attempts, assaults, etc.) a. Elopement Rate: 31 patients (0.65%) b. Suicide attempts: 0
10. Readmissions within 72h a. 11 Cases (0.23%)
11. AMA rate
a. 0.5%
12. LWBS rate a. 0.9%
13. Evidence-Based Practice (Protocols/Guidelines)
Implementation of low risk chest pain pathway implementation process
Implementation of acute stroke management based on last AHA guidelines.
Service (HCAHPS Performance/Doctor Communication)

Growth/Volumes
1. ED Volume: Emergency department had a significant increase in number of patients in the month of February. Also ED was able to operate in an efficient way and keep the LWBS at 0.9%.
2. Process Improvement: Emergency department had a significant improvement in triage process from 35 minutes in January to 20 minutes in February 2016.
Stewardship
1. One of the major goal for implementing low risk chest pain pathway is to decrease number of unnecessary admission with low re-imbursement and increase and facilitate the outpatient follow up.
2. The emergency department will continue collaboration with hospital patient’s concierge in increasing referral to Primary care clinic, and also specialists at the discharge time to help reducing the patient’s re-admission through ED.
Active Steps to Improve Performance:
1. Implementing the super-track area on busy days of week.
2. Continue our collaboration with nursing leadership in improving front end process including triage process and immediate bedding.
OBSTETRICS & GYNECOLOGY Dr. Sylvester Booker
INDICATOR JAN FEB MAR APR MAY JUN JUL AUG SEP OCT
NOV DEC
Total Deliveries 37 26 Normal Deliveries 28 21
Vacuum assisted deliveries 1 2 Primary C-Section 5 3 Repeat C-Section 4 2 VBAC Attempt 1 0
VBAC Successful 1 0 # of Induction of Labor 3 2
# of Aug. of Labor 3 3 HIV + Mom 1 0
HIV + Babies 0 0 Mother + for Substance 1 1
Abuse
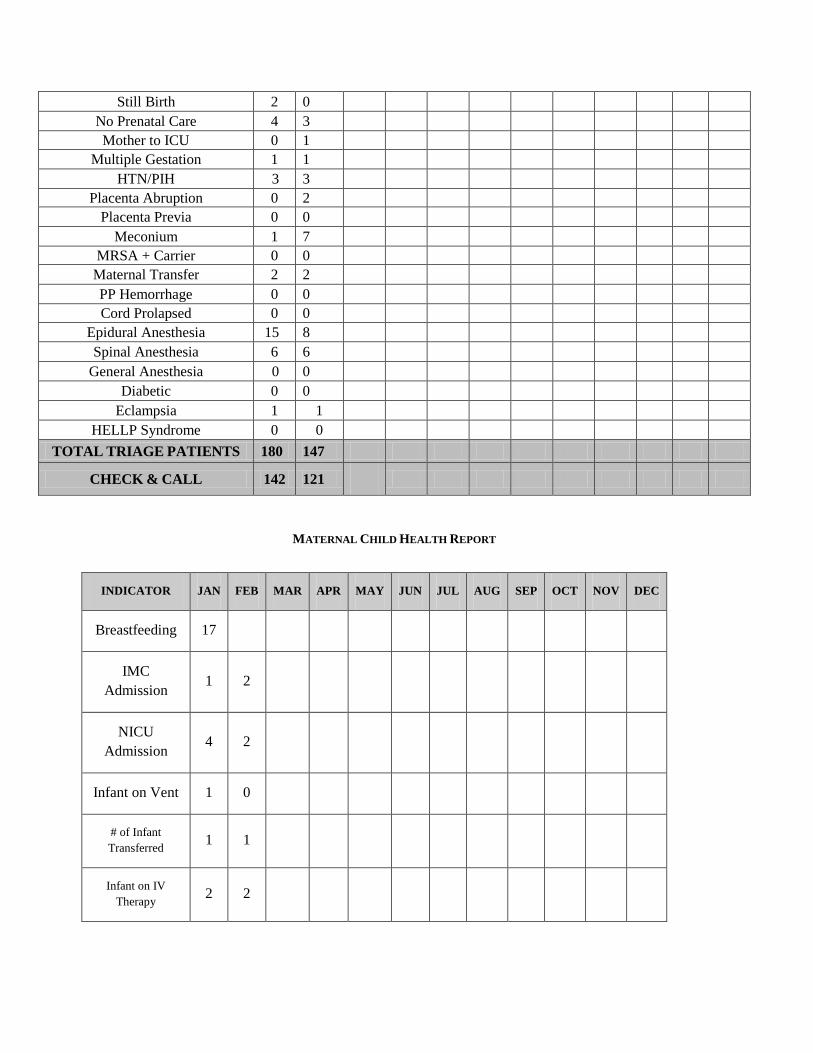
MATERNAL CHILD HEALTH REPORT
Still Birth 2 0 No Prenatal Care 4 3 Mother to ICU 0 1
Multiple Gestation 1 1 HTN/PIH 3 3
Placenta Abruption 0 2 Placenta Previa 0 0
Meconium 1 7 MRSA + Carrier 0 0
Maternal Transfer 2 2 PP Hemorrhage 0 0 Cord Prolapsed 0 0
Epidural Anesthesia 15 8 Spinal Anesthesia 6 6
General Anesthesia 0 0 Diabetic 0 0
Eclampsia 1 1 HELLP Syndrome 0 0
TOTAL TRIAGE PATIENTS 180 147
CHECK & CALL 142 121
INDICATOR JAN FEB MAR APR MAY JUN JUL AUG SEP OCT NOV DEC
Breastfeeding 17
IMC Admission 1 2
NICU Admission 4 2
Infant on Vent 1 0
# of Infant Transferred 1 1
Infant on IV Therapy 2 2

2015
Neonatal Death 0 1
PATHOLOGY Dr. David Reagin
The Transfusion Service (Blood Bank) was reaccredited by the AABB. This accreditation is for the period April 1, 2016 to March 31, 2018. The current accreditation is good through March 31, 2016.
Infant on Antibiotic Therapy 2 2
Phototherapy 0 1
Circumcision 14 6
Infant (+)Substance
Abuse 1 1
Boarding Baby 1 2
Failed Hearing Screen 0 1
# of Bili scan 34 24
# of CCHD Screening
34
24
GYN patient 5 12
Premature babies receiving steroids prior to birth *
1 0
Code Purple 30 15

PEDIATRICS Dr. Marilyn McPherson-Corder
Performance Summary: For the month of February 2016, 26 babies were admitted to the nursery. On the average length of stay was 2 days for NSVD and 3.5days for C-sections. The year-to-date total number of newborns admitted to the nursery is 61.
The Departmental meeting was held on February 8, 2016
Core Measures Performance
The Department of Pediatrics continues to meet the Core Measures Performance.
INDICATOR Target 2015
Annual Average
1Q2016 2Q2016 3Q2016 4Q2016
PC-04 - Health Care associated blood-stream infections in Newborns
0% 0% 0%
0%
0%
PC-05 - Exclusive breast milk feeding 50%
>65%
0% 0%
0%
0%
PC-05a - Exclusive breast milk feeding considering the mother's choice after discharge
64% >50%
0% 0%
0%
0%
1. Morbidity and Mortality Reviews
Two infants were born at less than 34 weeks of gestation.one infant was transfer to Children’s National Medical Center. One fetal death due to extreme prematurity, at 26 weeks of gestation.
All others were cared for in the UMC nursery and discharged home.
2. Evidence-Based Practice (Protocols/Guidelines)
Neonatal resuscitations guidelines continue to be followed resulting in one mortality and minimal morbidity. Increase education on the benefits of breastfeeding and skin-to-skin encouraged right after delivery of the infant with >60% breastfeeding rate within the first 24 hours. Hand washing encouraged repeatedly to prevent healthcare associated blood stream infections in the newborn. Zero incidence of healthcare associated bloodstream infections of the newborn.
Growth/Volumes The department continues to work to extend the breast feeding initiatives and to encourage pre and postnatal care with all mothers. Stewardship The Pediatric Contract has provided financial stability and has maintained operation below the budgeted expenses. Financials The Pediatric group provides 24 hours coverage, 7 days a week, without cost of overtime PSYCHIATRY Dr. Lisa Gordon
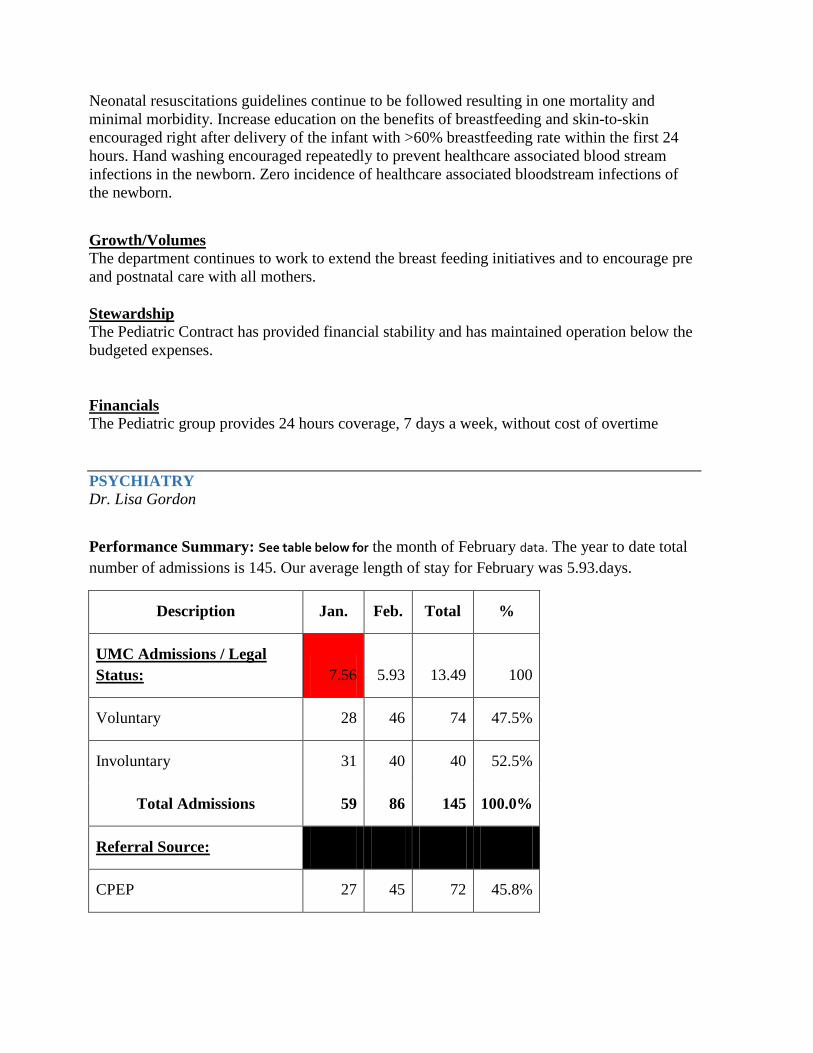
Performance Summary: See table below for the month of February data. The year to date total number of admissions is 145. Our average length of stay for February was 5.93.days.
Description Jan. Feb. Total %
UMC Admissions / Legal Status: 7.56 5.93 13.49 100
Voluntary 28 46 74 47.5%
Involuntary 31 40 40 52.5%
Total Admissions 59 86 145 100.0%
Referral Source:
CPEP 27 45 72 45.8%

Other (ER) 30 37 37 50.8%
GWU 1 2 3 1.7%
Providence 0 0 0 0.0%
Georgetown 1 0 1 1.7%
Sibley 0 1 1 0.0%
UMC Medical Surgical unit 0 0 0 0.0%
Children's Hospital 0 1 1 0.0%
Howard 0 0 0 0.0%
Holy Cross 0 0 0 0.0%
Washington Hospital Center 0 0 0 0.0%
DYRS 0 0 0
PIW 0 0 0 0.0%
Total # of Patients 59 86 145 100.0%
Description Jan. Feb. Total
St. Elizabeth Transfers 2 1 3
Transfers with LOS over 15 days 2 1 3
Number of Court Hearings 0 0 0
Quality Initiatives, Outcomes, etc.
1. Core Measures Performance
BHU is working with the PI team to improve the validity of the abstraction process for core measures.
2. Morbidity and Mortality Reviews – NA
3. Adverse events (i.e. elopement, suicide attempts, sexual harassment, assaults, etc.) There have been several incidences of seclusions/restraints due to highly agitated patients. Our staff continue to work to safely treat and manage patients.
4. Care Coordination/Readmissions - NA
5. Evidence-Based Practice (Protocols/Guidelines)
On hold.
Service (HCAHPS Performance/Doctor Communication)
NA
Growth/Volumes BHU has two full time physicians who are covering for 24 patients. Stewardship BHU has cross trained all nurses in conducting intakes to provide coverage for intake without overtime.
Financials
BHU continues to monitor overtime. Our Psychiatric Techs and Counselors are assigned as sitters when census is low.

Active Steps to Improve Performance:
The renovations continue to be on hold. However new furniture has been delivered an ____________________________________________________________________________ RADIOLOGY Dr. Raymond Tu
Performance Summary:
ER OUT TOTAL
Exam Type Exam Units Exams Units Exams Units Exams Units
Cardiac Cath 13 0 2 15
CT Scan 83 604 191 878
Fluoro 20 2 15 37
Mammography 249 249
Magnetic Resonance Angio 11 0 0 11
Magnetic Resonance Imaging 52 5 63 120
Nuclear Medicine 23 3 4 30
Special Procedures 33 0 11 44
Ultrasound 139 231 266 636
X-Ray 208 994 819 2021
CNMC CT Scan 22 22
CNMC X-Ray 480 480
Grand Total 582 2341 1618 4543
Quality Initiatives, Outcomes, etc.
Core Measures Performance
100% extra cranial carotid reporting using NASCET criteria
100% fluoroscopic time reporting
100% presence or absence hemorrhage, infarct, mass
100% reporting <10% BI RADS 3
Radiology staff continues to work to improve the turnaround of patients for CT and MRI of the brain through the department.

Morbidity and Mortality Reviews: There were no departmental deaths.
Code Blue/Rapid Response Teams (“RRTs”) Outcomes: There was 1 rapid response in radiology which was tended to by the cardiologist.
Care Coordination/Readmissions: N/A
Evidence-Based Practice (Protocols/Guidelines) We continue to improve patient transportation into and out of the emergency department.
Service (HCAHPS Performance/Doctor Communication)
The radiology department’s new equipment has been very well received for by our clinical staff elevating the status of our hospital. Additional training for technologist staff is planned to the full potential of the equipment may be utilized. We have completed coronary artery imaging with CT which is the first for us.
Stewardship: Dr. Tu continues to strongly recommend clinical decision support at the point of order entry to reduce unnecessary examinations and to aid in practioners to order the right test, the right time for the right patient. The old CT scanner was removed and the site will be prepared for the replacement.
Old Philips Brilliance CT scanner de-installation, being removed from CT suite (left) in route out of the building (middle) and site ready for preparation (right).
Financials: Active Steps to Improve Performance: The active review of staff performance and history to be provided for radiologic interpretation continues.

SURGERY Dr. Gregory Morrow
November 2015 the Surgery Department performed 150 total procedures.
December 2015 the Surgery Department performed 210 total procedures.
January 2016 the Surgery Department performed 147 total procedures.
February 2016 the Surgery Department performed 207 total procedures.
The chart and graft below show the trend over the last 3 years

SCIPInf. 9
Urinary catheter 68% 90% 94% 100% 100%
removal on post OP day 1 or
post op day 2
MONTH 2013 2014 2015 2016
JAN 173 159 183 147
FEB
134
143
157
207
MAR
170
162
187
APRIL
157
194
180
MAY
174
151
160
JUNE
159
169
175
JULY
164
172
193
AUG
170
170
174
SEP
177
168
166
OCT
194
191
181
NOV
137
157
150
DEC
143
183
210
Annual
Totals
1952 2019 2116
Our surgical volumes have increased and continue to do so as we work diligently to increase our efficiencies and productivity while, at the same time, delivering the highest quality of care.
We continue to meet and / or exceed the quality measures outlined for the Surgery Department
INDICATOR Target 98% 2014 Annual
Average 1Q2015 2Q2015 3Q2015 4Q2015
The department is currently working on:
1. Adding more physicians to orthopedic surgery staff to increase our elective and outpatient procedures, as well as, obtaining coverage for Emergency, In-patient and Out-patient (Clinic) coverage.
2. On-going evaluation of the service lines that will most benefit from implementation of best practices policies and procedures.
3. Moving the surgical assistant staff from under nursing to the medical staff to better utilize their skill sets and work-flow to best serve the OR and in-patient needs under direct physician supervision. The proposal has been submitted to the bylaws committee for review.
4. Finalizing the needs for the new ORs as it relates to the general design and work flow to include total information integration system.
5. We have secured a new Plastic Surgeon and Bariatric Surgeon on staff that will assist in retaining patients at our facility that might have to go elsewhere for their needed procedures.
6. Expanding availability of available OR time during regular business hours. We are working with the Anesthesia Department and Nursing to achieve these goals.

March 2016 CIO Report Thomas Hallisey
Information Technology and Systems Board Report – March 2016
Clinical Initiatives:
• UpToDate – The UpToDate system is a tool that links into our MEDITECH system and allows immediate contextual access to the latest medical information and research to assist caregivers in their decision making. This system has been rolled out linking directly into the MEDITECH system, with additional access available through their web site from any device.
• CRISP Connection – CRISP is the Health information Exchange used by all Maryland and DC hospitals. It can be used by clinicians to access patient records from other facilities in the area. UMC staff is working with CRISP now to schedule training and insure the proper security and network aspects are in place. The contract is expected to be signed in March and we will immediately notify physicians.
• Drug Dose Range Checking – Interactions checking is an integral part of the Computerized
Physician Order Entry implemented in 2014. A plan has been developed to expand that use to include Dose Range checking, lab result checking and diagnosis checking. We are setting up the team now and plan to start these checks by March of 2016, before our next Leapfrog survey.
• OR Module Implementation – The OR system implementation continues and is on track for the live date planned in June of 2016. The MM, billing, OR and IT staff are all involved in the process to improve the overall efficiency, documentation and billing that all part of this implementation.
• Meditech Upgrade to release 5.67 - The upgrade to the latest release of our MEDITECH Magic system is underway with a live date planned of April 6, 2016. This upgrade contains many changes to our multiple MEDITECH applications, but is focused mostly on meaningful use requirements and physician documentation improvements.
Operational Initiatives:
• Kronos Update – The Kronos system which handles our time and attendance application for all employees to be paid properly is being updated to the latest software. The existing system is no longer supported and lacks desired functionality. This upgrade will include all new timeclocks with added features available to better track employee time. The update has started in February 2016 and will be completed within 6-8 weeks.
• Meaningful Use (MU) We have successfully attested to Stage 1 year 2 of the Meaningful Use requirements for Medicare. The estimated payment for meeting these measures is $500,000, though that includes the Medicaid portion as well, which we cannot attest to until august of 2016.

March 2016 CIO Report Thomas Hallisey
• Move MEDITECH Systems In-house – The decision has been made to move the MEDITECH
servers and storage back into the UMC data center. This move is being done to provide better service (we experienced 3 unplanned downtimes in the last 6 months) and to save money, over $250,000 per year. This project is expected to be completed in April of 2016.
The Application Support, Help Desk, and Infrastructure teams continue to provide ongoing operational support of UMC’s systems. The team had 523 help desk requests and closed 567 in February 2016. The team was able to complete more tickets than requested this month and reduce the backlog.

Not-for-Profit Hospital Corporation
HUMAN RESOURCES
REPORT TO
Board of Directors
Submitted By:
Jackie W. Johnson Executive Vice President Human Resources
March 2016
Human Resources Board Report |March 2016 2
Workforce Development
Nursing Tuition Reimbursement Program Through the Health Resources and Service Administration, United Medical Center has been afforded the opportunity to provide our Nurses with tuition reimbursement for the pursuit of an advanced degree. The NURSE Corps Scholarship Program enables students who are accepted or enrolled in a diploma, associate, baccalaureate, or graduate nursing programs, including RN to BSN, RN to MSN-NP, Direct Entry MSN-NP program, to receive funding for tuition, fees and other educational costs in exchange for their commitment to work at an eligible NURSE Corps site upon graduation. Upon graduation, NURSE Corps Scholarship recipients work at these facilities for at least two years, earning the same competitive salary and benefits as any new hire in most Markets. Through the Health Resources and Service Administration (HRSA) Programs health professions loan repayment, scholarship and loan program, areas that are classified as “Underserved” by the Medical Community are now infused with highly competent and skilled clinicians, thus alleviating the critical shortage of nurses currently experienced by health care facilities located in Health Professional Shortage Areas (HPSAs).
Electronic Employability Verification In line with our continued effort to digitize our Processes, Procedures and Documents, we are in the process of reviewing the implementation of Home Land Security’s on-line electronic employability verification system known as E-Verify.
E-Verify is an Internet-based system that allows businesses to determine the eligibility of their employees to work in the United States in a matter of seconds vs. having a document that may never be reviewed again after its initial verification. By comparing information from an employee's Form I-9, Employment Eligibility Verification, to data from U.S. Department of Homeland Security and Social Security Administration records, E-Verify is able to continually confirm an applicant’s employment eligibility against millions of government records.

Human Resources Board Report |March 2016 3
USI’s Executive Review In preparation for the 2016 Benefits and Renewal cycle, USI’s, Michelle Martone, SVP, Consultant, conducted our 2015 Executive Review with CEO, Andy Davis. The purpose of the Review was to ensure that USI was staying in step with UMC’s need’s and objectives, learn and plan for changes in our business priorities and to discuss our questions and concerns about the changing landscape of benefits and healthcare The review focused on four (4) key Drivers for 2016:
- Healthcare Reform and its impact on a current basis and its impact in the future. - A multi-year analysis of UMC’s costs and various trend scenarios based upon adoption
of health and wellness strategies. - Discussion of the Population Health Management program designs and the ability to
drive lower cost trends and mitigate large catastrophic claims. - The Key Deliverables and impact for UMC in 2016.
This annual review reinforces USI’s commitment to ensuring UMC’s Benefit plans remain competitive and in line with our cost and coverage objectives, that USI remains attuned to our short and long term business objectives as well as reinforcing USI’s continued review of our program’s competitiveness through Benchmarking, objective setting and long range planning for Health Management, loss control, administrative efficiencies and consumer engagement.

Please refer to Patient Safety and Quality Committee Report
Pamela R. Lee
EVP, Hospital Operations and CQO

PUBLIC RELATIONS AND COMMUNICATIONS MARCH BOARD REPORT
Community Outreach:
March, April and May Community Outreach Event Calendar
MARCH:
• 15th -- Westminister Church/ Medstar Health Seminar 400 I St. S.W. UMC Mobile Health Clinic 10:00 a.m. until 2:00 p.m.
• 7th – Hillcrest Heights Civic Association Meeting Presentation Hillcrest Heights Community Center 2300 Oxon Run Drive Temple Hills, Maryland 7:00 pm
• 24th -- UMC Behavioral Health Education Seminar United Medical Center 1310 Southern Avenue 6:30 p.m. to 8:30 p.m.
• 26th --- Prince George’s County Council Member Karen Toles’ Hop Into Health Spring Extravaganza 2300 Oxon Run Drive Temple Hills, Maryland UMC Mobile Health Clinic on site 12:00 p.m. to 3:00 p.m.
APRIL:
• 3rd – New Samaritan Baptist Church 1100 Florida Ave. NE. UMC Mobile Health Clinic 10:00 a.m. to 1:00 p.m.

• 9th – Ward 8 Faith Leaders Monthly Meeting Presentation Location (TBD)
• 9th – Spring 2016 Barry Farm Saturday Academy 1292 Eaton Road S.E. UMC Mobile Health Clinic 12:00 p.m. to 3:00 p.m.
• New Image Baptist Church 1839 Alabama Ave. S.E. 10:00 a.m. to 3:00 p.m. Mobile Health Clinic
• 16th – Ebenezer AME Church Community Health Fair 7806 Allentown Road Ft. Washington, MD 10:00 a.m. to 3:00 p.m.
• 20th -- Westminister Church with Medstar Health Seminar 400 I Street S.W. 10:00 a.m. until 2:00 p.m. UMC Mobile Health Clinic
• 21st – United Medical Center Health Education Diabetes/Obesity Seminar Matthews Memorial Baptist Church 2626 Martin Luther King Jr. Ave. S.E. 6:30 p.m. until 8:00 p.m.
• 23rd -- United Medical Center April Board of Directors Meeting Conference Rooms 1 and 2 United Medical Center
• 26th -- North Tantallon Civic Association Presentation Harmony Hall Regional Center 10701 Livingston Road Ft. Washington, Maryland 7:45 p.m.

MAY:
• May 7 – Hillcrest Heights Community Day Hillcrest Heights Community Center 2300 Oxon Run Drive Temple Hills, Maryland 10:00 a.m. to 2:00 p.m. Mobile Health Clinic on site
• 14th – Riverdale Global Health and Education Riverdale Elementary School 5006 Riverdale Road Riverdale, Maryland UMC Mobile Health Clinic
• 16th – Washington Navy Yard Spring Into Fitness Health Fair 1022 O Street Southeast
9:30 a.m. until 2:30 p.m.
UMC Mobile Health Clinic
• 18th – Westminister Church with Medstar Health Seminar 400 I Street S.W. 10:00 a.m. until 2:00 p.m. UMC Mobile Health Clinic
• 21st -- Parkside Paradise Health Fair Mississippi Avenue Southeast 10:00 a.m. until 3:00 p.m. UMC Mobile Health Clinic
• 26th -- United Medical Center HIV Health Education Seminar Location in Ward 7 TBD

EXTERNAL COMMUNICATIONS:
Press Releases – Wrote and distributed the restructuring press release to the news media, city council members and other stakeholders. Facilitated interviews with reporters. Articles appeared in the Washington Business Journal and other outlets. Below are links to the news stories that have appeared.
Becker’s Hospital Review – United Medical Center to Cut 112 Positions – 4 Things to know – Becker’s Hospital Review
http://www.beckershospitalreview.com/hospital-management-administration/united-medical-center-to-cut-112-positions-4-things-to-know.html
United Medical Center is Tapping Another Turnaround Specialist. Is the Howard Deal Dead? – Washington Business Journal
http://www.bizjournals.com/washington/news/2016/03/11/united-medical-center-is-tapping-another.html
United Medical Center to Cut 10 Percent of Workforce – Washington Business Journal
http://www.bizjournals.com/washington/news/2016/03/11/united-medical-center-cuts-10-percent-of-workforce.html
After Layoffs, United Medical Center Takeover Deal in Question – Healthcare Dive News
http://www.healthcaredive.com/news/after-layoffs-united-medical-centers-takeover-deal-in-question/415615/
Feature Story --
A feature story on Sleep Disorders, with an emphasis on Sleep Apnea, will appear in the Washington Informer newspaper. Editor Kevin McNeir interviewed Dr. Beyene on how apnea can raise blood pressure and complicate other illnesses. United Medical Center has a Sleep Center that provides sleep studies to residents in the community. Those diagnosed with sleep apnea or other disorders are counseled and treated appropriately. The feature story will appear in the March 18 issue of the newspaper.
Internal Communications –
Black History Month Program --United Medical Center hosted a Black History Month program to recognize and honor Veterans who work at the hospital and those who live here. Speakers included Cherissa Jackson, a retired Air Force nurse who worked at combat hospitals in Afghanistan; Willie

Blanding, a retired Army Colonel who served in Vietnam and worked for Presidents Clinton and Bush; and Lieutenant Colonel Myles Caggins, who is assigned to the White House and works for the National Security Council. Jackson and Blanding spoke about their experiences in the service and why the military was such an important part of their life. Colonel Caggins spoke about the history of African Americans in the military and how we have always contributed to the success of our nation.


The Nursing Report will be available at the March 23, 2016 Board Meeting.
Maribel A. Torres, Chief Nursing Officer
Division Ambulatory and Ancillary Services
March 2016
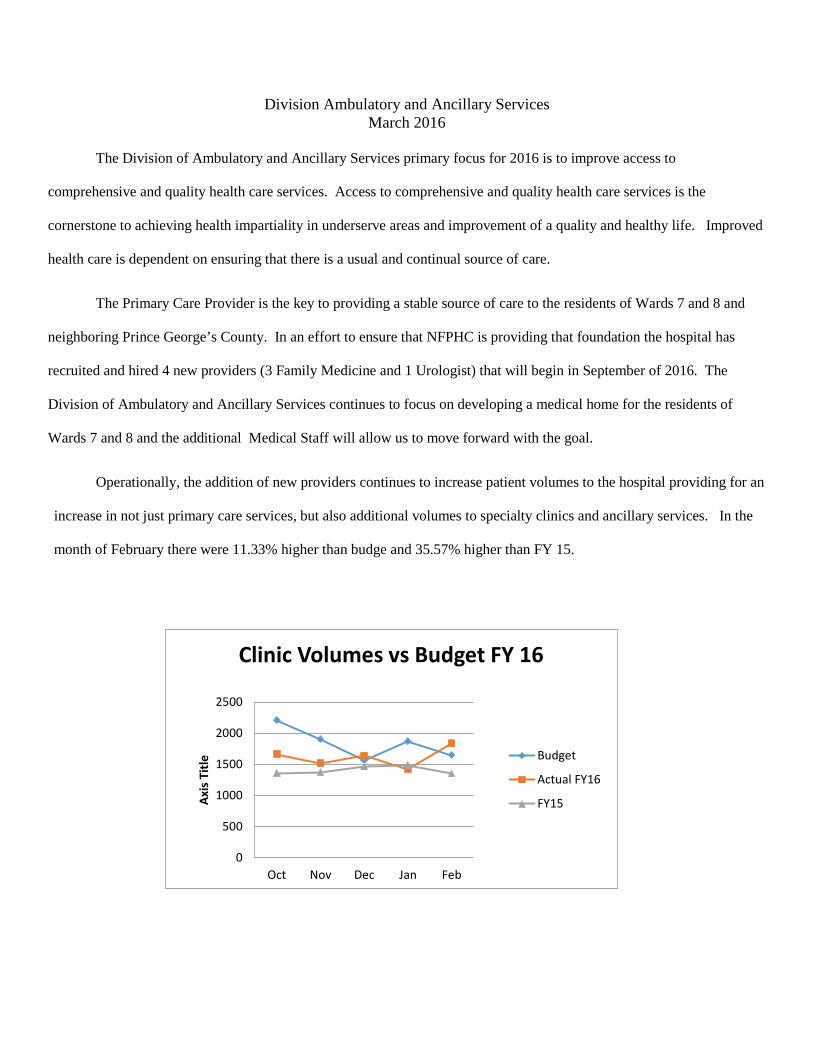
The Division of Ambulatory and Ancillary Services primary focus for 2016 is to improve access to
comprehensive and quality health care services. Access to comprehensive and quality health care services is the
cornerstone to achieving health impartiality in underserve areas and improvement of a quality and healthy life. Improved
health care is dependent on ensuring that there is a usual and continual source of care.
The Primary Care Provider is the key to providing a stable source of care to the residents of Wards 7 and 8 and
neighboring Prince George’s County. In an effort to ensure that NFPHC is providing that foundation the hospital has
recruited and hired 4 new providers (3 Family Medicine and 1 Urologist) that will begin in September of 2016. The
Division of Ambulatory and Ancillary Services continues to focus on developing a medical home for the residents of
Wards 7 and 8 and the additional Medical Staff will allow us to move forward with the goal.
Operationally, the addition of new providers continues to increase patient volumes to the hospital providing for an
increase in not just primary care services, but also additional volumes to specialty clinics and ancillary services. In the
month of February there were 11.33% higher than budge and 35.57% higher than FY 15.
0
500
1000
1500
2000
2500
Oct Nov Dec Jan Feb
Axis
Titl
e
Clinic Volumes vs Budget FY 16
Budget
Actual FY16
FY15
Ambulatory/Ancillary Data March 2016
1 In search of Orthopedic Surgeon
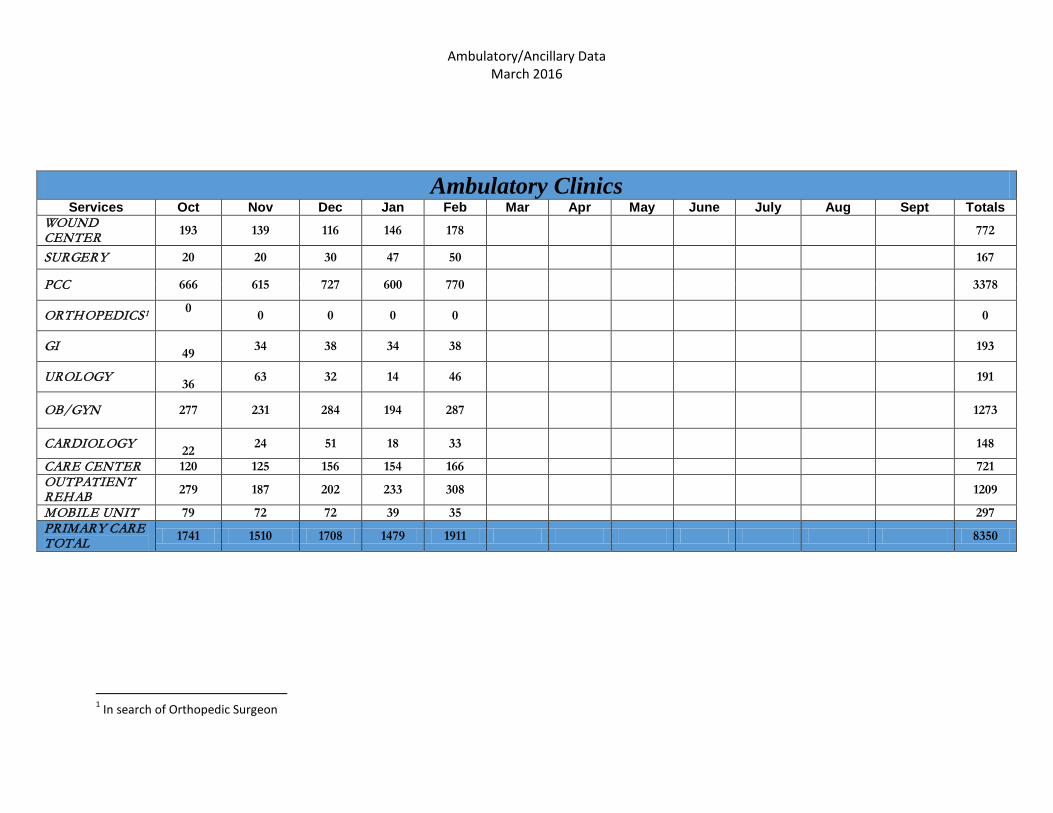
Ambulatory Clinics Services Oct Nov Dec Jan Feb Mar Apr May June July Aug Sept Totals
WOUND CENTER 193 139 116 146 178 772
SURGERY 20 20 30 47 50 167
PCC 666 615 727 600 770 3378
ORTHOPEDICS1 0 0 0 0 0 0
GI 49 34 38 34 38 193
UROLOGY 36 63 32 14 46 191
OB/GYN 277 231 284 194 287 1273
CARDIOLOGY 22 24 51 18 33 148
CARE CENTER 120 125 156 154 166 721 OUTPATIENT REHAB 279 187 202 233 308 1209
MOBILE UNIT 79 72 72 39 35 297 PRIMARY CARE TOTAL 1741 1510 1708 1479 1911 8350

Radiology/Cardiology Department February 2015 Inpatient Emergency
Department Outpatient TOTAL
EXAM TYPE EXAMS EXAMS EXAMS EXAMS
CT SCAN 83 604 191 878 FLUORO 20 2 15 37
MAMMOGRAPHY 0 0 249 249 MAGNETIC RESONANCE ANGIO 11 0 0 11
MAGNETIC RESONANCE IMAGING 52 5 63 120
NUCLEAR MEDICINE 23 3 4 30 SPECIAL PROCEDURES 33 0 11 44
ULTRASOUND 139 231 266 636 X-RAY 208 994 819 2021
CNMC CT SCAN 0 22 0 22 CNMC XRAY
480
480
GRAND TOTAL 582 2341 1618 4543

Ambulatory/Ancillary Data March 2016
3/15/2016
Client: St. Francis Regional
HighlightsMedical Director – Christian Paletta – 1/11/2016
clinic - 2/1/2016
HSP – Healogics Specialty Physician. Insurance - pending
Community EducationJanuary – 25 visitsFebruary – 35 visits
ADVANCE WOUND CARE--DASHBOARDToday’s Date 03/07/16 Original Contract Date: 12/2014 PD-Melody Britt
Human Resource MetricsCenter KPIs
Contract Scope: Wound Care Only WC & HBO X
Financial
People
Reimbursement* PD—monitor daily charges-accuracy * PD – monitor daily Dash Board* Reconciliation daily* Charge master reviewed for accuracy *
* Manual policy review* AVP/RDCO review/Consult
* Education/knowledge sharing
* Monthly conference calls
Community Education* Tracking Referral Sources* Letters to referring physicians* Physician visits* Inpatient referral- in progress*
Admin: Staffing, Safety, etc.* Implementation of i-heal 2.0 April* Leadership meeting every Monday* Action Plan—increase HBOT
utilization
Implementation of employee of the month - 2016.
Vital Few
Clinical
Service
Volumes: Patients, Encounters, HBOTGrowth
Last Month
Yr-to-Date
Staffing Matrix
Actual 2.64 2.64
Budget 2.0 2.0
Productivity/Effectiveness
RN/Pts 2/130 2/308
Turnover 0 FTE 0 FTE
YTD Last month Benchmark
Cancelation rate 22% 18% 10%
Wound types Venous pressureDFU
40% 20% 11%
32%15%9%
To create Patient Satisfaction survey for department
Quality
Last quarter totals
Budget quarterly
January February March Quarter YTD
New Patients
59 60 19 20
Encounters 381 672 146 178
HBO Segments 362 960 28 36
Last Year totals
January February March 1st quarter total YTD
Revenue $64,125 24,889
Expenses $107,274 7,089
Income/Loss $43,149 17,800
DenialsPurchase services
Outcomes Last Month YTD Benchmark
Healing
Days to Heal 28 30 32
Heal Rate 883% 83.87% 92%
Outliers 4.32% 7.28% <19%
Discharge Pts. 16 34 n/a
************************************************************************
Active pts. 53
New HBO pts. 1

Managed Care Log (Active Negotiations)
Managed Care Company BHU Acute OP Clinic OP ED SNF RAD LAB
Magellan X
Value Options X
Trusted Healthplan X X X
Carefirst BCBS
X X X X X
Health Services For Children with Special Needs X X X X
Amerihealth X X X X
MedStar Family Choice X X X X
Beacon X
Riverside Health state
facilitated X X X

United Medical Center
CEO Report
Operations Summary – March 2016
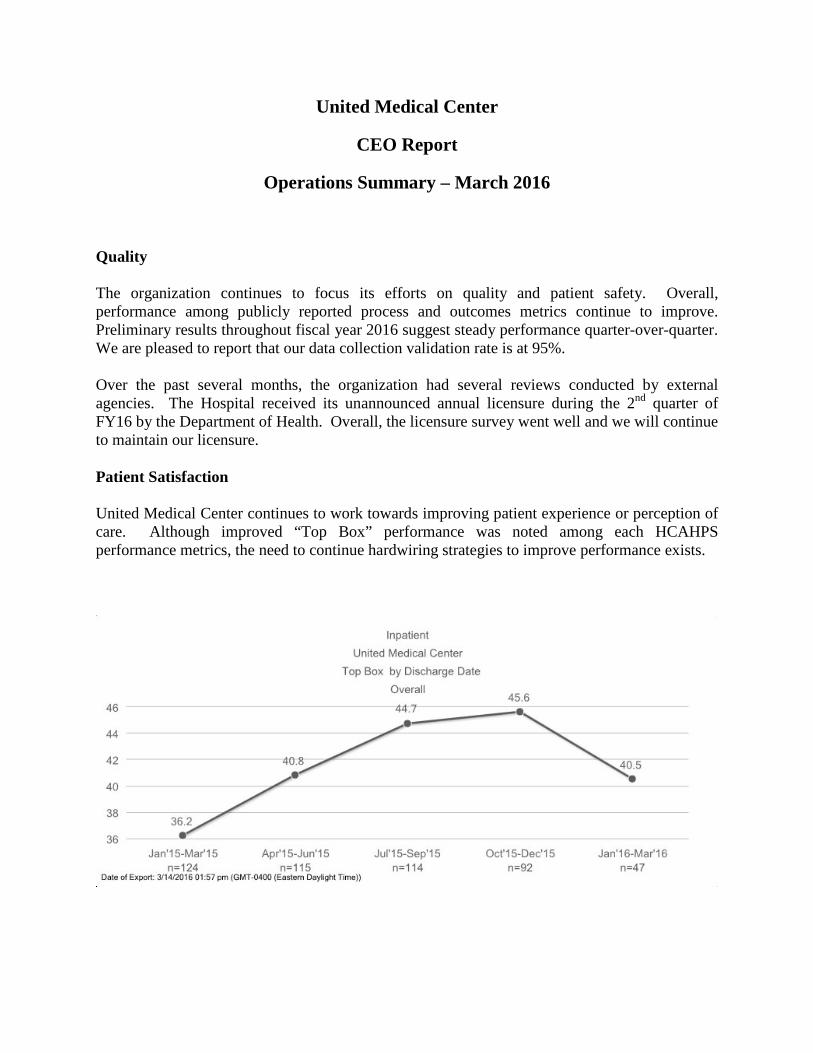
Quality The organization continues to focus its efforts on quality and patient safety. Overall, performance among publicly reported process and outcomes metrics continue to improve. Preliminary results throughout fiscal year 2016 suggest steady performance quarter-over-quarter. We are pleased to report that our data collection validation rate is at 95%. Over the past several months, the organization had several reviews conducted by external agencies. The Hospital received its unannounced annual licensure during the 2nd quarter of FY16 by the Department of Health. Overall, the licensure survey went well and we will continue to maintain our licensure. Patient Satisfaction United Medical Center continues to work towards improving patient experience or perception of care. Although improved “Top Box” performance was noted among each HCAHPS performance metrics, the need to continue hardwiring strategies to improve performance exists.
2
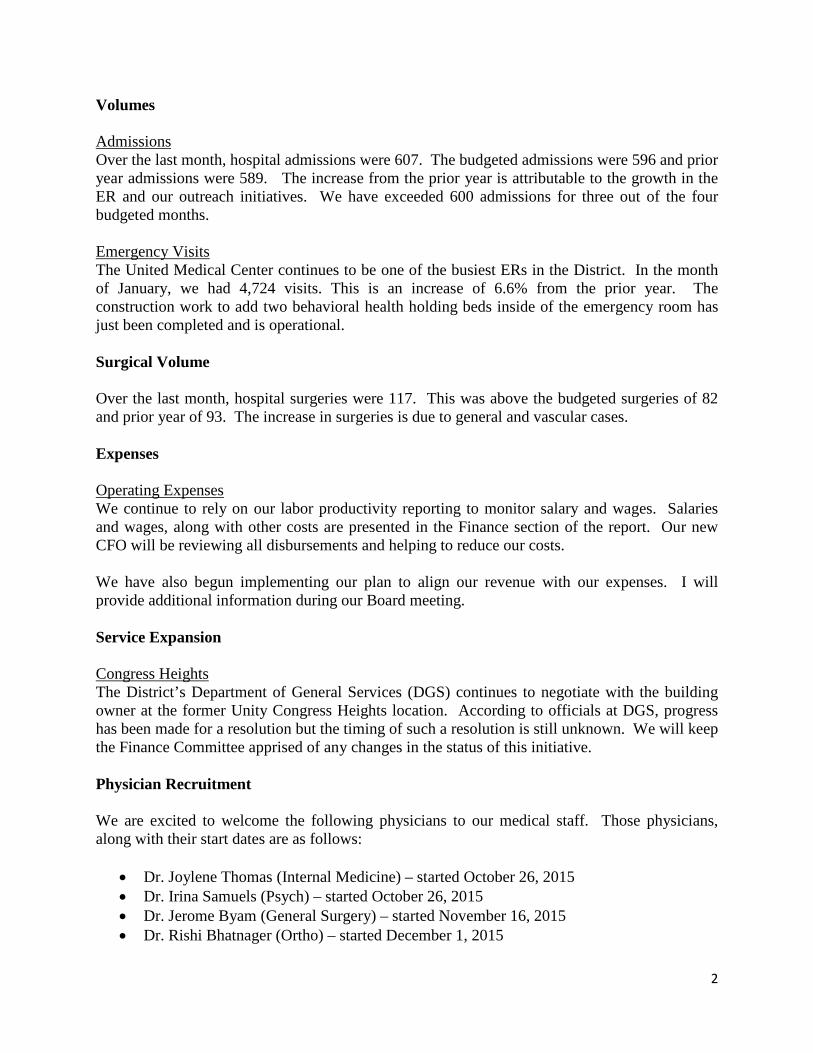
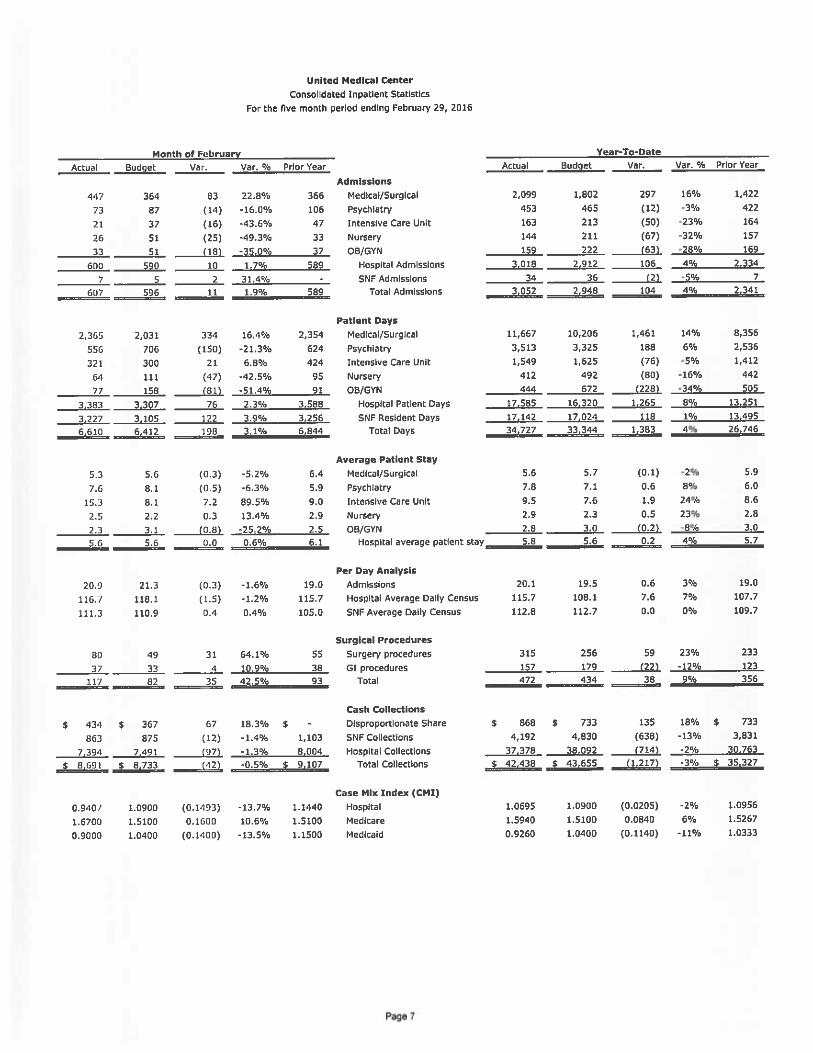
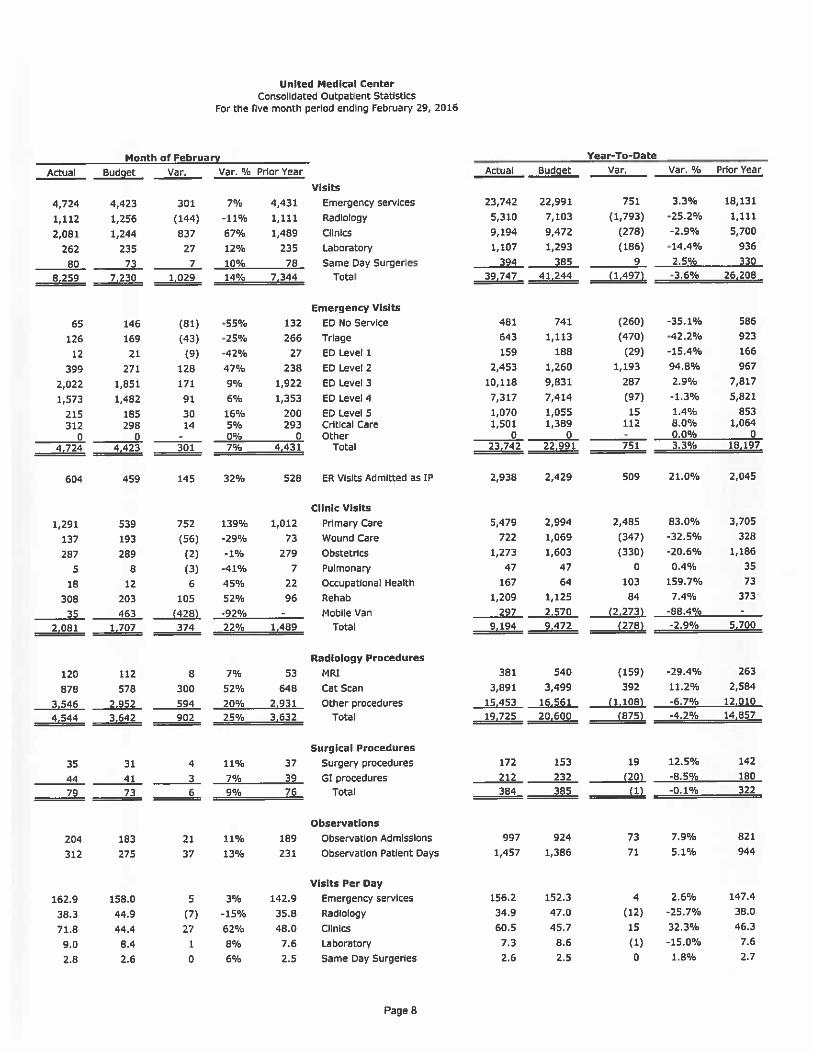
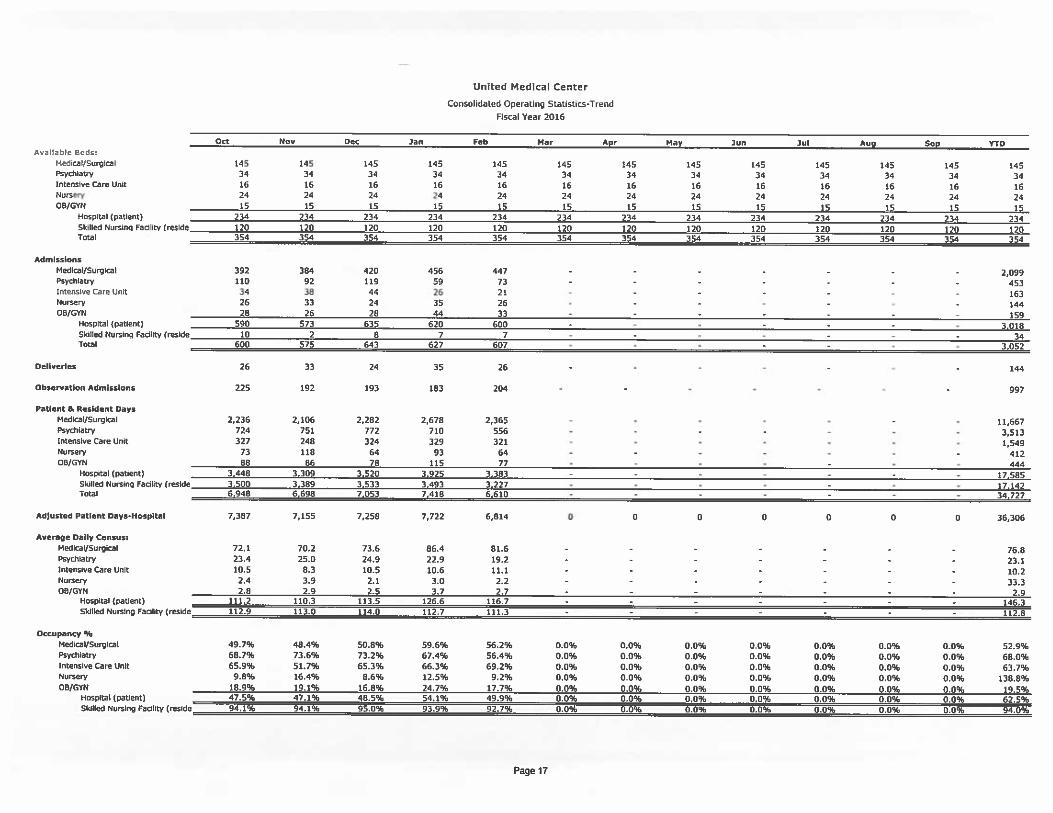
Volumes Admissions Over the last month, hospital admissions were 607. The budgeted admissions were 596 and prior year admissions were 589. The increase from the prior year is attributable to the growth in the ER and our outreach initiatives. We have exceeded 600 admissions for three out of the four budgeted months. Emergency Visits The United Medical Center continues to be one of the busiest ERs in the District. In the month of January, we had 4,724 visits. This is an increase of 6.6% from the prior year. The construction work to add two behavioral health holding beds inside of the emergency room has just been completed and is operational. Surgical Volume Over the last month, hospital surgeries were 117. This was above the budgeted surgeries of 82 and prior year of 93. The increase in surgeries is due to general and vascular cases. Expenses Operating Expenses We continue to rely on our labor productivity reporting to monitor salary and wages. Salaries and wages, along with other costs are presented in the Finance section of the report. Our new CFO will be reviewing all disbursements and helping to reduce our costs. We have also begun implementing our plan to align our revenue with our expenses. I will provide additional information during our Board meeting. Service Expansion Congress Heights The District’s Department of General Services (DGS) continues to negotiate with the building owner at the former Unity Congress Heights location. According to officials at DGS, progress has been made for a resolution but the timing of such a resolution is still unknown. We will keep the Finance Committee apprised of any changes in the status of this initiative. Physician Recruitment We are excited to welcome the following physicians to our medical staff. Those physicians, along with their start dates are as follows:
• Dr. Joylene Thomas (Internal Medicine) – started October 26, 2015 • Dr. Irina Samuels (Psych) – started October 26, 2015 • Dr. Jerome Byam (General Surgery) – started November 16, 2015 • Dr. Rishi Bhatnager (Ortho) – started December 1, 2015
3
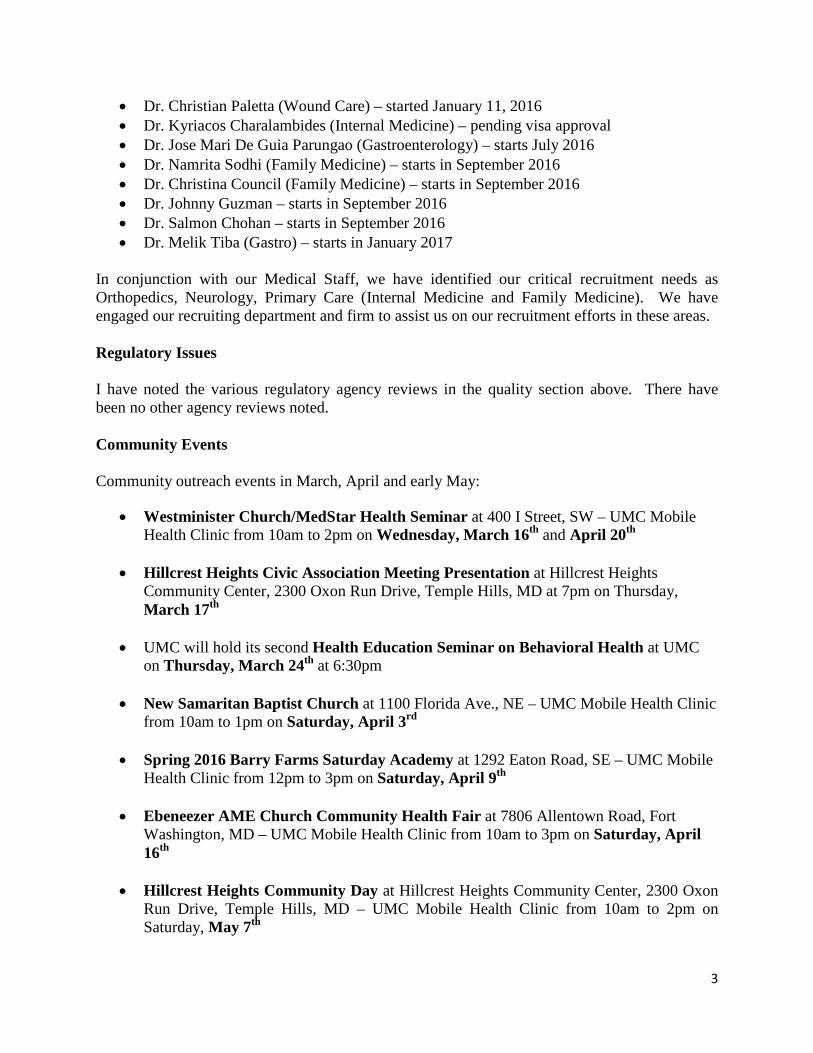
• Dr. Christian Paletta (Wound Care) – started January 11, 2016 • Dr. Kyriacos Charalambides (Internal Medicine) – pending visa approval • Dr. Jose Mari De Guia Parungao (Gastroenterology) – starts July 2016 • Dr. Namrita Sodhi (Family Medicine) – starts in September 2016 • Dr. Christina Council (Family Medicine) – starts in September 2016 • Dr. Johnny Guzman – starts in September 2016 • Dr. Salmon Chohan – starts in September 2016 • Dr. Melik Tiba (Gastro) – starts in January 2017
In conjunction with our Medical Staff, we have identified our critical recruitment needs as Orthopedics, Neurology, Primary Care (Internal Medicine and Family Medicine). We have engaged our recruiting department and firm to assist us on our recruitment efforts in these areas. Regulatory Issues I have noted the various regulatory agency reviews in the quality section above. There have been no other agency reviews noted. Community Events Community outreach events in March, April and early May:
• Westminister Church/MedStar Health Seminar at 400 I Street, SW – UMC Mobile Health Clinic from 10am to 2pm on Wednesday, March 16th and April 20th
• Hillcrest Heights Civic Association Meeting Presentation at Hillcrest Heights Community Center, 2300 Oxon Run Drive, Temple Hills, MD at 7pm on Thursday, March 17th
• UMC will hold its second Health Education Seminar on Behavioral Health at UMC on Thursday, March 24th at 6:30pm
• New Samaritan Baptist Church at 1100 Florida Ave., NE – UMC Mobile Health Clinic from 10am to 1pm on Saturday, April 3rd
• Spring 2016 Barry Farms Saturday Academy at 1292 Eaton Road, SE – UMC Mobile Health Clinic from 12pm to 3pm on Saturday, April 9th
• Ebeneezer AME Church Community Health Fair at 7806 Allentown Road, Fort Washington, MD – UMC Mobile Health Clinic from 10am to 3pm on Saturday, April 16th
• Hillcrest Heights Community Day at Hillcrest Heights Community Center, 2300 Oxon
Run Drive, Temple Hills, MD – UMC Mobile Health Clinic from 10am to 2pm on Saturday, May 7th

4
Other Notable I testified at the Committee on Health and Human Services FY15-16 Performance Oversight Hearing on February 23rd 2016 for Not-For-Profit Hospital Corporation.




































Not-For-Profit Hospital Corporation Board of Directors
Governance Committee Agenda March 8, 2016
I. CALL TO ORDER
II. ROLL CALL
III. CONSENT AGENDA
• REVIEW MINUTES OF THE FEBRUARY 9, 2016 MEETING
IV. BOARD OF DIRECTORS ORIENTATION MANUAL
V. BOARD OF DIRECTORS EDUCATION SESSIONS FOR 2016 • BOARD SELF ASSESSMENT SURVEYS – STATUS
VI. CEO GOALS AND OBJECTIVES • PFAC AND CBA COMMITTEES VII. BOARD APPOINTMENTS-MOTA NOMINATIONS
• KAI BLISSETT, GENERAL COUNSEL VIII. UPDATE - UMC MISSION, VISION AND VALUES STATEMENTS
ADJOURNMENT

1
Not-For-Profit Hospital Corporation Governance Committee Meeting Minutes
February 9, 2016
Present: Virgil McDonald, Maria Gomez, Steve Lyons, Andrew Davis, Kai Blissett, General Counsel, Donna Freeman (Corporate Secretary) Excused: Guests: Agenda Item Discussion Action Item Call to Order The meeting was called to order at 8:05a.m. Determination of a Quorum
Virgil McDonald, Committee Chair determined a quorum.
Approval of the Agenda
The Governance Committee approved the agenda. Virgil McDonald added one item – Board Self-Assessment Survey update.
Approval of Minutes
Minutes from January 12, 2016 were approved.
Discussions
Highlights include: The Board of Directors Orientation Manual Virgil McDonald led the discussion regarding the orientation manual. Members of the committee presented their comments for updates: • Consider using a 3 ring binder • Manual to be available on the Board Portal for ease of access • The history section should include the strategic plan • Consider specific intervals for manual updates i.e.: every 6 months • Encourage the board members to use the board portal • Include the financial summary, annual budget and supportive documents • Include budgets for the last 5 years
Virgil McDonald requested Steve Lyons to include in the manual, the analysis he prepared for the Finance committee meeting addressing the subsidy funds provided by the District to UMC.

2
• Instructions for the entrance to the hospital • Parking location and fees (if any) • Include organizational Bylaws, Open Meetings Act, etc. • Include board member tracking from the District • Include Budget Oversight Hearing responses • Pamela Lee will request from staff members any materials that will be included in the orientation manual. • a Welcome page from the Mayor should be included Monthly Board Education Sessions Virgil McDonald addressed the need for the sessions and suggested the board portal and UMC email be the topic at the February General Board meeting. Steve Lyons suggested the use of personal email addresses and confidentiality be discussed also. The discussion continued regarding training and compliance issues in communication. The topic of the Board Education sessions and time allocation will be vetted through Andrew L. Davis, Interim CEO. The time allotment will be fifteen (15) minutes. 2016 Board Self- Assessment Survey Virgil McDonald led the discussion regarding the importance of completing the forms. Donna Freeman reminded the committee to submit their forms by February 12, 2016. CEO Goals and Objectives Virgil McDonald expressed the urgency for him to convene a meeting with Andrew L. Davis, Interim CEO and Chris Gardiner, BOD Chairman to discuss the goals and objectives of the Interim CEO. Once they have been formulated, they will be brought to the full Board. Update of MOTA Nominations to the UMC Board Kai Blissett, General Counsel provided an update to the committee on Dr. Ricardo Brown and Dr. Julianne Malveaux. Their terms have expired, should they be attending meetings? Kia Blissett explained all notification comes from MOTA. Virgil will speak with the Chairman regarding the status of Brown and Malveaux. Kai addressed Robert Malson’s retirement
Virgil McDonald, Donna Freeman and Pamela R. Lee plan to meet on Thursday, February 11, 2016 to discuss finalizing the organization of the orientation manual. Virgil McDonald will have UMC IT Dept. address UMC email/ board portal and Kai Blissett will address confidentiality and FOIA guidelines. Donna Freeman will schedule the meeting with Chris Gardiner, Virgil McDonald and Andy Davis to review the CEO goals and objectives. Virgil McDonald requested Kai Blissett update Chairman Chris Gardiner on regulations regarding non-voting

3
which will affect his tenure on the board. Kai updated the committee regarding non-voting members participating in committees. Mission, Vision, and Values Update Andrew (Andy) Davis, Interim CEO led the discussion. He shared the results of the Strategic Planning Committee meeting. The highlights were: • Mission statement was confirmed and will be used in all communication • Values were needed for the hospital • Hospital, staff and board will be included in the creation of the value statement • A focused approach to creating the values Board Committee Preferences Please send in preferences immediately. We are planning a meeting with MOTA to discuss the skill-set needs of the UMC board. A Parliamentarian: Maria Gomez expressed interest in accepting the position left vacant by Virgil McDonald being appointed Vice-Chair of the Board. Patient Family Advisory Council and Community Benefits Advisory Council Kai Blissett led the discussion on the legalities of the committees.
members participating on committees. . Donna Freeman will send Maria Gomez a description of the Parliamentarian’s duties.
Other Business The next conference call will be held on Tuesday, March 8, 2016 @ 8:00am. The meeting was adjourned at 9:25a.m.

Board of Directors Evaluation Form March 23, 2016
The purpose of this form is to evaluate the overall effectiveness of the monthly General Board Meeting process. Please rank the following items on a scale of 1-5. The results of this evaluation will demonstrate where changes can be made to increase the overall productivity of our meetings.
Proper notice was given to Board Members & community. 5 4 3 2 1 The Board packet was received in a timely manner. 5 4 3 2 1 The meeting agenda is appropriate. 5 4 3 2 1 The Board packet provided the appropriate information to support solid discussions and decisions.
5 4 3 2 1
Executive reports were concise, yet informative. 5 4 3 2 1 Directors’ discussions were on target and focused. 5 4 3 2 1 Directors were prepared and involved. 5 4 3 2 1 All recommendations and decisions made by the Board are documented and monitored to ensure implementation.
5 4 3 2 1
Appropriate Board and staff assignments were made. 5 4 3 2 1 Board Members’ conduct was business-like, cordial, results-oriented and respectful of diversity.
5 4 3 2 1
Meeting ran on time. 5 4 3 2 1 I am satisfied with this meeting. 5 4 3 2 1
What aspects of this meeting were particularly good?
What aspects of this meeting were particularly bad? Do you have any suggestions or comments about this meeting?
Exceeds Expectation
Meets Expectation
Below Expectation

Page 1 of 2
Thank you everyone for providing such valuable feedback. We can assure you that we will take your feedback in consideration in
planning our next board meeting to increase overall productivity.
Board of Directors Evaluation Summary February 24, 2016
Areas of Evaluation Average Response Rank
Proper notice was given to Board Members & community 5.0 The Board packet was received in a timely manner 5.0 The meeting agenda is appropriate. 4.6 The Board packet provided the appropriate information to support solid discussions and decisions.
3.7
Executive reports were concise, yet informative. 4.0 Directors’ discussions were on target and focused 4.0 Directors were prepared and involved. 4.3 All recommendations and decisions made by the Board are documented and monitored to ensure implementation.
4.1
Appropriate Board and staff assignments were made. 4.6 Board Members’ conduct was business-like, cordial, results-oriented and respectful of diversity.
4.6
Meeting ran on time. 4.1 I am satisfied with this meeting. 4.1 Board Member attendance: Present ___11__ Absent __0__ In the evaluation form, the board members were invited to provide feedback on three specific questions. Some of the comments received are summarized below. What aspects of this meeting were particularly good?
• Lively discussion on finances • Content • None
What aspects of this meeting were particularly bad? • Not nearly enough prep materials on closed session • As an ex-officio non-voting member being asked to leave before having discussion in closed
session. • Board is not given adequate information to make decisions.
Page 2 of 2
Thank you everyone for providing such valuable feedback. We can assure you that we will take your feedback in consideration in
planning our next board meeting to increase overall productivity.
Do you have any suggestions or comments about this meeting? • Closed session should be announced. • Need to make sure Dashboard of Key Indicators is a priority. • Non-voting members (ex-officio) should be allowed to stay for discussion in all closed sessions.

United Medical Center 2016 Board Member Self-Assessment
Full Name: Date Completed: Tenure on the Board: I. MISSION AND GOALS 1. I know the mission of United Medical Center. Yes Somewhat No 2. I can communicate our mission to others. Yes Somewhat No 3. I know the vision of the United Medical Center and can communicate it to others. Yes Somewhat No 4. I know the values of the organization and am able to communicate them to others. Yes Somewhat No 5. I know the strategic direction/I understand UMC’s strategic direction Yes Somewhat No
II. RESPONSIBILITIES 1. I have an understanding of the Board's legal responsibilities. Yes Somewhat No 2. I have an understanding of the Board's public responsibilities. Yes Somewhat No 3. I understand my basic responsibilities as a board member. Yes Somewhat No 4. I understand my fiduciary responsibilities as a board member. Yes Somewhat No 5. I understand the operations of our United Medical Center. Yes Somewhat No 6. I am an active member of one or more committees. Yes No
7. I attend most events sponsored by the United Medical Center system. Yes No 8. I believe I am an effective advocate for better community healthcare. Yes No 9. I would be willing to do more for United Medical Center if asked. Yes No 10. I understand the Board’s Conflict of Interest Policy. Yes Somewhat No 11. I routinely review meeting materials in advance. Yes No 12. I make significant contributions to the Board’s deliberations. Yes No 13. I respect the confidentiality of decisions made in the Boardroom. Yes No III. LEADERSHIP 1. The Board’s expectations and concerns are clearly and effectively communicated to the CEO. Yes No 2. The Board evaluates the CEO based on mutually agreed upon performance objectives. Yes No 3. The Board evaluates the CEO in a timely manner. Yes No 4. The Board periodically reviews, discusses and, if necessary, modifies the CEO’s performance objectives to ensure that they are current and reflect the changing market conditions and Board expectations. Yes No IV. BOARD EFFECTIVENESS – GENERAL 1. The working relationships among Board members are good. Yes No 2. The Board reviewed its structure, committee practices, tenure and bylaws within the last year. Yes No Don’t know 3. Board Committees and ad-hoc committees have clearly defined roles and responsibilities. Yes No Don’t know 4. The Board has a process for determining when a Board Member is not performing to the Board’s standards or requirements. Yes No Don’t know
5. The Board has a process for improving individual Board Member effectiveness when non-performance becomes an issue. Yes No Don’t know 6. The potential liabilities of governance are clearly spelled out to Board members. Yes No Don’t know V. BOARD EFFECTIVENESS – RECRUITMENT AND PREPARATION 1. Board members are required to disclose possible conflicts of interest before their appointment and periodically throughout their terms as Board Members. Yes No 2. Board education/development is a high priority for our Board. Yes No 3. The Board has an effective orientation process that broadens a Board member’s perspective and ensures high-quality decision-making. Yes No 4. Board member development is conducted and complemented by Board retreats and ongoing education. Yes No 5. The Board has an effective board succession plan for officers. Yes No VI. STRATEGIC INFORMATION FOR FUTURE PLANNING 1. I am comfortable with my knowledge of (check all that apply)
a. Quality Improvement b. Medical Staff Credentialing c. Strategic Planning d. Finances e. Long-term Care Issues
2. I enjoy participation on the Board because (check all that apply) a. It gives me a feeling of accomplishment b. United Medical Center supports my personal interest in healthcare. c. The Board meetings are well managed and efficient. d. It helps me professionally. e. United Medical Center is working to make a healthier community. f. I do not enjoy my participation on this Board.
3. I could benefit from training in the following areas (please list)
1.
2.
3.
4. List your top three (3) priorities for United Medical Center in the next 12 months 1.
2.
3.
5. From your perspective, what areas need improvement?
1.
2.
3.

!
Governing Board Patient Safety & Quality Committee
March 15, 2016
12:45pm-2:00 pm Location: Hospital Board Room (2nd Floor)
Purpose: To provide oversight and guidance for the delivery of high quality, safe, cost-effective health care at Not-For-Profit Hospital Corporation.

Governing Board Patient Safety & Quality Committee Meeting March 15, 2016
Location: Hospital Board Room (2nd Floor) Purpose: To provide oversight and guidance for the delivery of high quality, safe, cost-effective health
care at Not-For-Profit Hospital Corporation.
Agenda
I. Welcome All
II. Call to Order M. Gomez
III. Approval of Minutes All
IV. Old Business
A. Mortality and Morbidity Review S. Pierre
V. New Business
A. Patient Experience Report P. Lee
B. Annual Reports/Evaluation P. Lee/S. Pierre
• Patient Safety and Risk Management • Environment of Care • Infection Control • PI Program/Quality Performance Indicators
C. 2016 Performance Improvement Plan & Priorities P. Lee
D. Potential Impact of Hospital Restructuring on Patient Safety & Quality A. Davis/P. Lee
VI. Other Business All
Adjournment Next Meeting: April 12, 2016

Not-For-Profit Hospital Corporation GB Patient Safety & Quality Committee Meeting Minutes
January 19, 2016
Present: Maria Gomez, Andrew L. Davis, Pamela R. Lee, Maribel Torres, Dr. Raymond Tu, Stanley Pierre, Donna Freeman (Corporate Secretary)
Excused: Dr. Julianne Malveaux, Chris Gardiner, Dr. Julian Craig Others: N/A
Agenda Item Discussion Action Item Call to Order The meeting was called to order at 12:11 p.m. Determination of a Quorum
No quorum determined due to board member absences.
Approval of the Agenda
N/A
Approval of Minutes
Delayed until the next meeting.
Consent Agenda N/A Discussion Old Business
Highlights include: (Discussion materials have been filed in the Office of the Secretary of the Corporation) Leapfrog Gap Analysis: Pamela R. Lee led the discussion regarding ways for UMC to improve their Leapfrog scores from a current “C” (2.53) rating to an “A” (3.15) rating. Pamela also provided documents for the Gap Analysis and an action plan. The specific steps have been identified and accompanied by due dates to chart UMC’s progress. Recommendations for a Patient Family Advisory Committee and a Medication Safety Committee were discussed.

PFAC: Patient Family Advisory Committee: The guidelines are being reviewed by the Governance Committee. The committee will be comprised of approximately 12-15 individuals, meeting quarterly and an annual report will be submitted to the BOD along with the Leapfrog scores. Having a PFAC committee weighs heavily in improving the Leapfrog scores.
CBA: Community Benefits Advisory Committee: The committee will meet 3 times per year and include over 15 individuals from Ward 7 and 8. The committee will assist in determining services for the community and will help in UMC’s community assessment goals. The group will include 15 or more hospital ambassadors that will speak to the community and educate them on the services of UMC.
Maria Gomez suggested including questions with PFAC on the things that are working and continue to work from a positive point of view.
New Business
The following New Business topics were discussed: (Discussion materials have been filed in the Office of the Secretary of the Corporation) Regulatory (DOH) and Accreditation (CAP) Surveys Two successful unannounced surveys were completed this week. 1. The DOH completed UMC’s annual licensure survey and UMC maintains its license. 2. Lab and Pathology were successfully surveyed by CAP and both will maintain their accredited status. Andy Davis, Interim CEO mentioned the recent 3 surveys (which include SNF) continue to show our improvement.
Radiology Department
Dr. Raymond Tu, Chief of Staff, reported the Radiology Department received its accreditation from the College of Radiology (CACR) after being surveyed December 2, 2015. All other Radiology modalities have been surveyed are fully accredited.

2015 Performance Metrics Dashboard: Stanley Pierre led the discussion regarding the Metrics and the Dashboard. Overall significant improvement continues to be made. He provided an in-depth explanation of the data and discussed the effect of real-time concurrent monitoring and clinical intervention efforts and information. The results are positive and improving. Many factors have played a role in the improvement. SNF Licensure Survey: Maribel Torres, CNO lead the discussion regarding the SNF survey. There were no safety issues found and the opportunities weren’t over level 2. This is one of the best surveys in recent years. The improvements in staff, safety, and resident care were all recognized. The results were received on Dec. 31, 2015. Quality Data Abstraction Validation Reports: Pam Lee led the discussion regarding quality data. Pam reviewed the process used to validate data and the information sent to CMS for payment. A third party was used to evaluate the accuracy of UMC’s patient reporting. This information is used to compile the Dashboard which evaluates UMC’s performance. UMC’s reporting was validated at a rate of 90-95% accuracy. The average validation rate is 75% and UMC achieved 90-95%. Dr. Raymond Tu reviewed the death certificate reporting. We went from the worst in
Stanley Pierre will quantify the data in February regarding the stroke medications of the Dashboard due to a small patient population. Maria Gomez would like to see the 4th quarter 2015 results at the next meeting. Pamela Lee will provide a root cause analysis summary and coordinate with Donna Freeman to disseminate to the BOD by March 2016.

the city to the best in the District after having moved to electronic reporting. Dr. Raymond Tu reviewed the status of UMC’s FY 2016 physicians reporting.
Other Business N/A Announcements Next meeting will be held on February 9, 2016 Adjourned: 1:35 p.m.

All DB N = 1897
Large PG DB
N = 1037
150-299 Bed Grp N = 391
AHA Region 3 N = 176
Your Top Box Score
Domains and Questions nPrevious %
Aug-OctCurrent %Nov-Jan
Percentile Rank
Percentile Rank
Percentile Rank
Percentile Rank
Rate hospital 0-10 91 42.7% 45.1% � 1 1 1 1
Recommend the hospital 88 41.6% 42.0% � 1 1 1 1
Comm w/ Nurses 93 68.4% 71.7% � 5 5 5 2
Nurses treat with courtesy/respect 91 73.3% 78.0% � 5 5 5 2
Nurses listen carefully to you 93 64.4% 73.1% � 22 23 23 19
Nurses expl in way you understand 89 67.3% 64.0% � 2 1 2 2
Response of Hosp Staff 81 44.0% 57.3% � 9 10 10 10
Call button help soon as wanted it 76 44.2% 55.3% � 11 13 12 10
Help toileting soon as you wanted 32 43.8% 59.4% � 11 10 12 10
Comm w/ Doctors 93 76.0% 81.1% � 47 54 54 39
Doctors treat with courtesy/respect 93 81.6% 82.8% � 15 13 17 7
Doctors listen carefully to you 91 74.0% 81.3% � 59 68 65 52
Doctors expl in way you understand 91 72.3% 79.1% � 65 73 73 65
Hospital Environment 92 57.4% 56.9% � 8 10 11 5
Cleanliness of hospital environment 91 61.4% 64.8% � 10 13 10 11
Quietness of hospital environment 90 53.4% 48.9% � 14 16 18 11
Pain Management 57 57.5% 66.1% � 17 15 18 17
Pain well controlled 55 46.4% 67.3% � 75 81 78 82
Staff do everything help with pain 57 68.6% 64.9% � 2 1 1 2
Comm About Medicines 44 51.2% 54.3% � 5 4 6 4
Tell you what new medicine was for 44 60.5% 70.5% � 10 8 11 8
Staff describe medicine side effect 42 41.9% 38.1% � 3 2 3 3
Discharge Information 83 71.7% 78.7% � 3 2 4 2
Staff talk about help when you left 82 66.7% 70.7% � 1 1 1 1
Info re symptoms/prob to look for 82 76.7% 86.6% � 18 15 22 9
www.PressGaney.com | 800.232.8032
n = number of respondentsQuestions that are among this period's top ten priorities appear in bold italics.
1Click here to access the Summary Report Guide
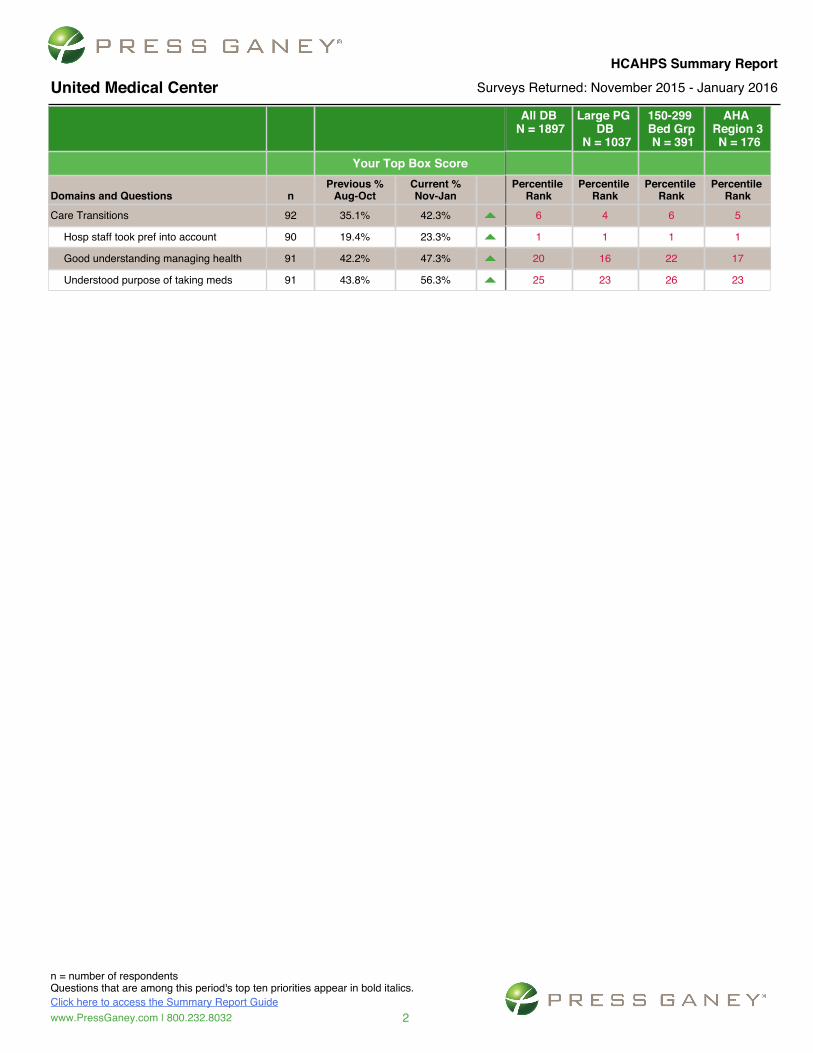
United Medical Center
HCAHPS Summary ReportSurveys Returned: November 2015 - January 2016
All DB N = 1897
Large PG DB
N = 1037
150-299 Bed Grp N = 391
AHA Region 3 N = 176
Your Top Box Score
Domains and Questions nPrevious %
Aug-OctCurrent %Nov-Jan
Percentile Rank
Percentile Rank
Percentile Rank
Percentile Rank
Care Transitions 92 35.1% 42.3% � 6 4 6 5
Hosp staff took pref into account 90 19.4% 23.3% � 1 1 1 1
Good understanding managing health 91 42.2% 47.3% � 20 16 22 17
Understood purpose of taking meds 91 43.8% 56.3% � 25 23 26 23
www.PressGaney.com | 800.232.8032
n = number of respondentsQuestions that are among this period's top ten priorities appear in bold italics.
2Click here to access the Summary Report Guide
United Medical Center
HCAHPS Summary ReportSurveys Returned: November 2015 - January 2016

2015 Program Evaluations Environment Of Care Plans
System Indicators Evaluation (Met/Not Met) Met = 90 – 100%
Plan of Correction Effectiveness of Program (Y/N)
Utility Management
1. Preventive maintenance completion rate - 90%
2. Cumulative number of unscheduled utility failures <2 per month
3. Track elevators failures
cause and ensure proper intervention – 90%
4. Testing Completion Rate
– 100%
:Met ☐Not Met
�
:Met ☐Not Met
:Met ☐Not Met
�
:Met ☐Not Met
Continue with current plan and metrics.
Y
Fire Safety Management
1. Track Staff Knowledge of location and use of fire extinguishers – 100%
2. Track Knowledge of pull station locations – 100%
3. Track knowledge of person authorized to shut off oxygen – 100%
:Met ☐Not Met
�
:Met ☐Not Met
:Met ☐Not Met
Continue with current plan and metrics.
Y

2015 Program Evaluations Environment Of Care Plans
System Indicators Evaluation (Met/Not Met) Plan of Correction Effectiveness of Program (Y/N)
Life Safety
Management
1. Educate contractors on ICRA and ISLM – 100%
2. Monthly Fire Extinguisher Inspection – 100%
3. Suppression (Quarterly) Annunciation (ANN) Test and Inspection – 100%
:Met ☐Not Met
�
:Met ☐Not Met
:Met ☐Not Met
Continue with current plan and metrics.
Y
Hazardous Material
(Hazmat) Management
1. Enhance Staff knowledge concerning hazardous material and waste – 90%
2. Ensure storage containers are properly labeled – 100%
3. Ensure hazardous materials and
waste are controlled – 100%
4. Ensure manifest for hazardous materials and waste is maintained – 100%
5. Ensure proper emergency
protocols are implemented in the event of spill or exposure – 100%
☐Met :Not Met
���
:Met ☐Not Met
:Met ☐Not Met
:Met ☐Not Met
:Met ☐Not Met
Basic Hazmat training did not occur in 2015. It will be integrated into the annual mandatory training for all staff. Continue with current plan and metrics.
Y

2015 Program Evaluations Environment Of Care Plans
System Indicators Evaluation (Met/Not Met) Plan of Correction Effectiveness of Program (Y/N)
Hazardous Material
(Hazmat) Management
6. Provide on-going training on proper handling of hazardous materials – 100%
7. Ensure that vendors making
deliveries follow protocol – 100%
☐Met :Not Met
����
:Met ☐Not Met
Training on Hazmat was postponed last November and is scheduled to take place in April 2016. Continue with current plan and metrics.
Medical Equipment
Management
1. Preventive maintenance (scheduled) completion rate – 95%
2. Corrective maintenance (response time-30minues) – 95%
3. Corrective maintenance down
time – 95%
4. Biomedical Test Equipment Calibration – 100%
:Met ☐Not Met
��
:Met ☐Not Met
:Met ☐Not Met
:Met ☐Not Met
Continue with current plan and incorporate new performance metrics.
Y

2015 Program Evaluations Environment Of Care Plans
System Indicators Evaluation (Met/Not Met) Plan of Correction Effectiveness of Program (Y/N)
Safety/Security Management
1. New employee knowledge of security practices – 100%
2. Wearing of ID badges by employees and other personnel within facility – 95%
3. Door checklist completed during high security shifts (nights/weekends) – 90%
4. Conduct Quarterly infant
abduction drills – 100%
:Met ☐Not Met
�
:Met ☐Not Met
:Met ☐Not Met
:Met ☐Not Met
Continue with current plan and metrics.
Y
Emergency
Management
1. Conduct a minimum of 2 emergency disaster drills or live events and evaluations per year – 100%
x L' enfant Plaza Incident x DC Coalition Drill
:Met ☐Not Met
��
Continue with current plan and metrics.
Y

CY 2015 Balanced Scorecard of Quality Performance Indicators
Prophylatic Antibiotic Received w/in 1h 99% 94% 95%Timely Removal of Urinary Catheters 98% 68% 94%Patients who received VTE Prophylaxis 73% 90% 93%Antithrombotics prescribed at d/c 99% 90% 93%Anticoagulants prescribed at d/c 95% 100% 50%IV thrombolytics was initiated 98% 0% NP New MeasureAntithrombotics administered by day 2 95% 96% 92%Statins prescribed at d/c 95% 76% 73%Education materials provided 90% 6% 34%Patients assessed for Rehab 98% 91% 93%Prophylaxis given 88% 78% 87%Prophylaxis received in ICU 94% 95% 98%Overlap Therapy received 94% 84% 68%
Unfractionated Heparin therapy received 98% 100% 100%
Warfarin d/c instructions ptovided 82% 35% 77%
Confirmed VTE during hospitalization 8% 0% 0%Elective deliveries 4% 2% 0%C-Section delivery by nulliparous mothers - 28%Antenatal steroids administered 90% - 63%Healthcare-associated blood infections 0% - 0%
Exclusive breast feeding 50% - 5%
IMM
Inpatient Immunization 95% 62% 96%
Time from Arrival to departure admitted pts <= 272' 453 484'Dwell time in ER <= 97' 366 196'Median time to transfer to another facility <= 59' - 84' New MeasureAspirin on arrival - AMI 97% 80% 84%Aspirin on arrival - Chest Pain 97% 92% 81%Median time to ECG - AMI <= 7' 22' 21'Median time to ECG - Chest Pain <= 7' 57' 16'Time from Arrival to departure d/c pts <= 133' 219' 221'Door to evbaluation by Medical personnel <= 24' 105' 82'Time to pain mgt. for long bone fracture <= 55' 102' 150'Head CT/MRI scan results received w/in 45' 61% - 0% New Measure
Key12 143 4
12 14
2014-2015 Change2014 Average
<75% of target75% - 89% of target90% - 100% of target
VTE
Perin
atal
Car
e
Target
SCIP
STRO
KEO
utpa
tient
Performance Indicators 2015 Average
New
M
easu
res
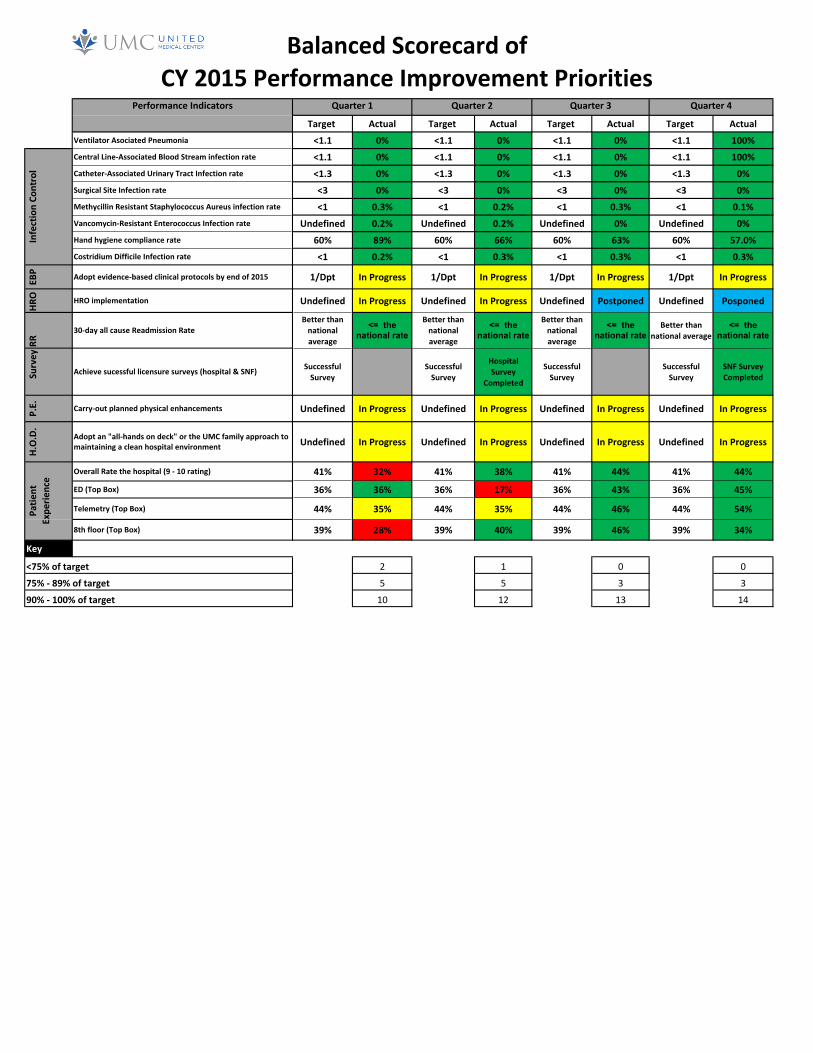
Balanced(Scorecard(of(CY(2015(Performance(Improvement(Priorities
Target( Actual Target( Actual Target( Actual Target( ActualVentilator(Asociated(Pneumonia <1.1 0% <1.1 0% <1.1 0% <1.1 100%Central(LineDAssociated(Blood(Stream(infection(rate <1.1 0% <1.1 0% <1.1 0% <1.1 100%CatheterDAssociated(Urinary(Tract(Infection(rate <1.3 0% <1.3 0% <1.3 0% <1.3 0%Surgical(Site(Infection(rate <3 0% <3 0% <3 0% <3 0%Methycillin(Resistant(Staphylococcus(Aureus(infection(rate <1 0.3% <1 0.2% <1 0.3% <1 0.1%VancomycinDResistant(Enterococcus(Infection(rate Undefined 0.2% Undefined 0.2% Undefined 0% Undefined 0%Hand(hygiene(compliance(rate 60% 89% 60% 66% 60% 63% 60% 57.0%Costridium(Difficile(Infection(rate <1 0.2% <1 0.3% <1 0.3% <1 0.3%
EBP Adopt(evidenceDbased(clinical(protocols(by(end(of(2015 1/Dpt In(Progress 1/Dpt In(Progress 1/Dpt In(Progress 1/Dpt In(Progress
HRO HRO(implementation Undefined In(Progress Undefined In(Progress Undefined Postponed Undefined Posponed
RR
30Dday(all(cause(Readmission(RateBetter(than(national(average
<= the national rate
Better(than(national(average
<= the national rate
Better(than(national(average
<= the national rate
Better(than(national(average
<= the national rate
Survey
Achieve(sucessful(licensure(surveys((hospital(&(SNF) Successful(Survey
Successful(Survey
Hospital(Survey(
Completed
Successful(Survey
Successful(Survey
SNF(Survey(Completed
P.E. CarryDout(planned(physical(enhancements Undefined In(Progress Undefined In(Progress Undefined In(Progress Undefined In(Progress
H.O.D.
Adopt(an("allDhands(on(deck"(or(the(UMC(family(approach(to(maintaining(a(clean(hospital(environment Undefined In(Progress Undefined In(Progress Undefined In(Progress Undefined In(Progress
Overall(Rate(the(hospital((9(D(10(rating) 41% 32% 41% 38% 41% 44% 41% 44%
ED((Top(Box) 36% 36% 36% 17% 36% 43% 36% 45%
Telemetry((Top(Box) 44% 35% 44% 35% 44% 46% 44% 54%
8th(floor((Top(Box) 39% 28% 39% 40% 39% 46% 39% 34%
Key
2 1 0 0
5 5 3 3
10 12 13 14
Quarter(1 Quarter(2 Quarter(3 Quarter(4
<75%(of(target
75%(D(89%(of(target
90%(D(100%(of(target
Patie
nt(
Expe
rience
Infection(Co
ntrol
Performance(Indicators

1 of 3
UNITED MEDICAL CENTER PERFORMANCE IMPROVEMENT PROGRAM
ANNUAL EVALUATION for Year 2015
Completed by: Hospital Quality Committee (Department Leaders) Date: March 6, 2015 1. Have improvements been made over the past year as a result of
department’s performance improvement activities? If so, please list on Page 2.
√ Yes No
a) Did the improvements involve a process?
√ Yes No
b) Did the improvements result in better patient outcomes?
√ Yes No
c) Were improvements directly related to departmental performance improvement measures?
√ Yes No
2. Have any of your performance improvement activities involved other departments or teams?
√ Yes No
3. Were any statistical tools and techniques (e.g. charts, graphs) used to analyze data?
√ Yes No
4. Has the scope of any department or team changed over the last year?
√ Yes No
5. Were performance measures developed for a new service or a department with changes to its scope of service?
√ Yes No
6. Over the past year, has it been necessary to prioritize any performance improvement activities due to multiple areas for improvement being identified?
√ Yes No
7. Were the performance measures and strategies reviewed at the department level with staff or team members before data collection was initiated?
√ Yes No
8. Were performance improvement results reviewed with staff or team members at he department level? √ Yes No
9. When problems or opportunities for improvement were identified, was input received from those closest to the process? √ Yes No
10. Were adequate processes in place to incorporate team(s) into the hospital-wide Performance Improvement Program?
√ Yes No
11. Was there sufficient physician leadership in PI activities during year 2015?
√ Yes No
12. Was there sufficient hospital leadership in PI activities during year 2015?
√ Yes No
13. Was there sufficient hospital front line staff involvement in PI activities during year 2015?
√ Yes No

2 of 3
Improvements made:
• Core Measures • ED flow • ED throughput process • ED “short registration” process • Emergency Medical Treatment and Labor Act (EMTALA) regulations • Continuous survey readiness • Infection Control • Employee evaluation compliance
Statistical and other tools used:
• Microsoft Excel • Survey Monkey • Leapfrog Survey • PI Audit Worksheets • Environment of Care rounds tools • Ventilator Associated Events data collection tools • Mortality review screening tool • Meditech • Summary Reports • Dashboards • Other
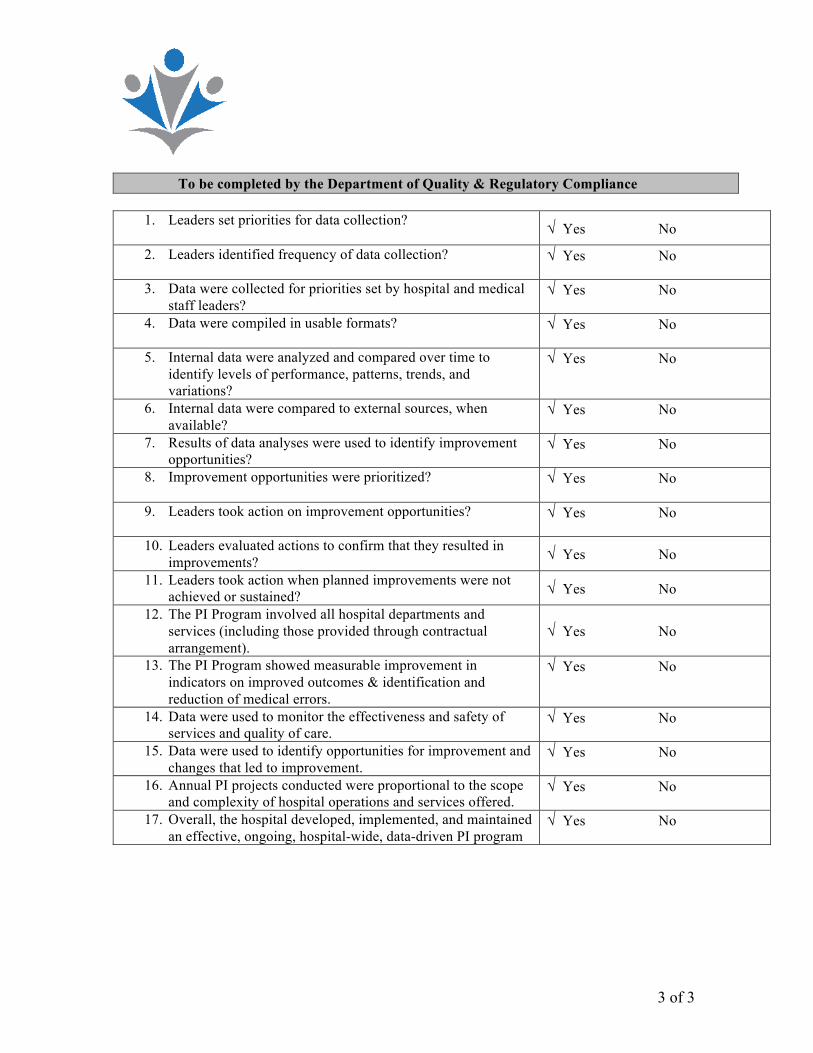
3 of 3
To be completed by the Department of Quality & Regulatory Compliance
1. Leaders set priorities for data collection?
√ Yes No
2. Leaders identified frequency of data collection?
√ Yes No
3. Data were collected for priorities set by hospital and medical staff leaders?
√ Yes No
4. Data were compiled in usable formats?
√ Yes No
5. Internal data were analyzed and compared over time to identify levels of performance, patterns, trends, and variations?
√ Yes No
6. Internal data were compared to external sources, when available?
√ Yes No
7. Results of data analyses were used to identify improvement opportunities?
√ Yes No
8. Improvement opportunities were prioritized?
√ Yes No
9. Leaders took action on improvement opportunities?
√ Yes No
10. Leaders evaluated actions to confirm that they resulted in improvements? √ Yes No
11. Leaders took action when planned improvements were not achieved or sustained? √ Yes No
12. The PI Program involved all hospital departments and services (including those provided through contractual arrangement).
√ Yes No
13. The PI Program showed measurable improvement in indicators on improved outcomes & identification and reduction of medical errors.
√ Yes No
14. Data were used to monitor the effectiveness and safety of services and quality of care.
√ Yes No
15. Data were used to identify opportunities for improvement and changes that led to improvement.
√ Yes No
16. Annual PI projects conducted were proportional to the scope and complexity of hospital operations and services offered.
√ Yes No
17. Overall, the hospital developed, implemented, and maintained an effective, ongoing, hospital-wide, data-driven PI program
√ Yes No
1
UNITED MEDICAL CENTER
Performance Improvement Plan
Year 2016
2
SECTION I United Medical Center (“UMC”) implements a systematic, well-coordinated, organization-wide approach to performance improvement to ensure a safe patient care environment exists. It’s Performance Improvement Plan (“PI Plan”) is fully implemented to ensure an effective strategy is undertaken to promote improvements in clinical and non-clinical processes. Integrated into the PI Plan are the hospital’s mission, vision, and values. Mission United Medical Center is dedicated to the health and well-being of individuals and communities entrusted to our care. Vision UMC is an efficient, patient-focused, provider of high-quality of healthcare the community needs. UMC will employ innovative approaches that yield excellent experiences. UMC will improve the lives of District residents by high value, integrated and patient-centered services. UMC will empower healthcare professionals live up to their potential to benefit our patients. UMC will collaborate with others to provide high value, integrated and patient-centered services.

3
SECTION II
Scope, Responsibility and Authority
UMC’s hospital and medical staff leaders are responsible for creating a culture and environment that fosters excellence in quality and service. The hospital is expected to fully implement the Performance Improvement Plan to identify and respond to improvement opportunities in order to fulfill or exceed its patients’ needs and expectations.
The Performance Improvement Plan promotes collaborative efforts among hospital, medical staff, governing board, and other individuals and applies to all departments, services and practitioners throughout the hospital. The plan is the central performance improvement plan in the organization and encompasses the inter-related functions and processes of clinical, governance, management, and support services. The hospital’s leadership must demonstrate commitment through consistent involvement in the process and constant reinforcement of the principles of continuous improvement. Leaders foster performance improvement through planning, educating, setting priorities, providing appropriate time and resources, and by empowering all staff.
Governing Body
The governing body is ultimately accountable for the safety and quality of care, treatment, and services. Therefore, ultimate responsibility for performance improvement rests with the hospital’s governing board. The authority and responsibility for implementation of the PI Plan is delegated to the Performance Improvement Committee.
Governing Board Patient Safety Quality Committee
The Government Board Patient Safety Quality Committee provides oversight and guidance for the delivery of high quality, safe, cost-effective healthcare at Not-For-Profit Hospital Corporation.
Performance Improvement Committee (“PIC”)
The Performance Improvement Committee (“PIC”) is the oversight body for all performance improvement activities within the hospital. It meets at least nine times per calendar year. A physician chairperson appointed by the Chief of Staff chairs the PIC. The Performance Improvement Committee membership includes representatives from departments across the organization at various levels (staff, department, hospital, and medical staff leaders).
The PIC oversees and coordinates performance improvement processes by:
5
� Use of information about adverse privileging decisions for any practitioner privileged through the medical staff process
� Use of medications � Use of blood and blood components � Operative and other procedures � Appropriateness of clinical practice patterns � Significant departures from established patterns of clinical practice � Use of developed criteria for autopsies � Sentinel event data � Patient safety data � Use of sedation/anesthesia � Outcomes related to Resuscitative Services � Core measures compliance
The medical staff participates in measurement, assessment, and improvement activities related to other patient care processes to include, but not limited to, the following:
� Education of patients and families � Coordination of care with other practitioners and hospital personnel, as
relevant to the care of an individual patient � Accurate, timely, and legible completion of patients' medical records � Review of findings of the assessment process that is relevant to an
individual’s performance. The medical staff is responsible for determining the use of this information in the ongoing evaluations of a practitioner's competence, in accordance with the standards on renewing or revising clinical privileges. This includes planned organizational and individual focused reviews
� Communication of findings, conclusions, recommendations, and actions taken to improve performance and patient safety to appropriate medical staff members and the governing body
4
� Establishing a planned, systematic, organization-wide approach to process design, performance measurement, analysis and improvement.
� Determining educational needs of hospital and medical staffs to facilitate performance improvement processes for hospital and medical staffs, the governing body, clinical and non-clinical staff, and hospital and medical staff leaders.
� Setting expectations for leadership and staff participation in multidisciplinary and interdepartmental performance improvement and patient safety activities.
� Adopting an approach to, and guiding implementation of hospital-wide performance improvement processes to include:
1. Planning the process of improvement; 2. Determining the scope and focus of measurement; 3. Setting priories for improvement, ensuring that important
processes and functions are included; 4. Systematically measuring, assessing and improving performance
and patient outcomes; 5. Implementing improvement activities based on assessment
conclusions; 6. Maintaining achieved improvements.
� Recommending resources for the hospital’s performance improvement
and patient safety activities. � Commissioning/convening performance improvement teams and
approving project selections for specific improvement efforts. � Monitoring the progress of all PI teams, projects, and initiatives. � Ensuring that processes for identifying and managing sentinel events are
defined and implemented. � Evaluating the effectiveness of the PI Plan and the effectiveness of the
leadership team’s contributions to performance improvement and patient safety, at least annually.
Medical Staff
The organized medical staff has a leadership role in hospital performance improvement activities to improve quality of care, treatment, and services, as well as patient safety. The medical staff also has a leadership role in organizational performance improvement when processes are dependent primarily on the activities of individuals with clinical privileges. UMC’s expectations of members of the medical staff, allied health professionals and their role in performance improvement are contained in the Medical Staff Bylaws. The medical staff is actively involved in the measurement, assessment, and improvement of the following:
� Medical assessment and treatment of patients

6
SECTION III Prioritization A strong commitment to continuous improvement typically produces many opportunities for performance improvement. As a result, it is necessary to have a defined, criteria-based process in place for prioritization of projects and the ability to adjust priorities in response to unusual or urgent events. The Performance Improvement Plan gives priority consideration to high volume, high risk, and problem-prone areas. The organization’s priority setting is sensitive to emerging needs such as those identified through data collection and assessment, unanticipated adverse occurrences affecting patients, changing regulatory requirements, significant patient and staff needs, changes in the environment of care, or changes in the community. Patient Safety is the highest priority and warrants immediate action. Data Collection, Analysis, and Tools Routine data collection activities will occur to support the hospital’s Performance Improvement Plan. Data will be collected throughout each month and analyzed at least quarterly to monitor organizational performance. Data collection will involve priorities set by the hospital’s leaders and will include high-risk, high-volume, problem-prone processes. Data will also be collected and analyzed on performance measures established as a result of accrediting body and regulatory agency surveys. See Attachment H (Performance Indicators). Additionally, data collection tools will be developed and used to capture required data and information. Action will be taken when undesirable patterns, trends, or variations are noted. In order to meet and exceed customer expectations, an understanding of on-going performance monitoring and improvement in critical systems and processes is a necessity. This plan addresses key performance improvement indicators and/or quality control monitors, by category, taking into consideration high volume, high risk, high cost issues, dimensions of performance and their relationship to the Six Pillars of Process Improvement This will not only allow focus on key indicators, but will also allow benchmarking for the purposes of collaboration on best practice models. Indicators are classified into three types: Benchmarking, Required (by regulation or accreditation) and Hospital/Department Specific indicators: Benchmark Indicators are those indicators considered key to United Medical Center. Benchmarking indicators must be collected in a consistent manner throughout the hospital in order to produce valid data and comparisons. Some Benchmark indicators will be used to meet the requirements of the ORYX Initiative. Data collection methodologies and specific definitions for each of the indicators are provided to assure this consistency.
7
Required Regulatory or Accreditation Indicators are those measures required as a condition of regulations or accreditation. All Quality Control monitors are considered to be Required Indicators. These indicators may be monitored using a standardized definition (e.g. case mix) or some formula defined by hospital to meet certain monitoring requirements. The following is a list of those required monitors. Hospital or Department Specific Indicators are those indicators that the hospital, in collaboration with the Performance Improvement Committee, has determined to be significant to the hospital. These indicators are not typically used for benchmarking purposes, but are useful to the hospital in evaluating hospital processes and outcomes. Reporting All performance improvement initiatives, activities, data and information will be reported horizontally across clinical and nonclinical department (as needed) as well as vertically to the hospital-wide Performance Improvement Committee, applicable medical staff committees, Medical Executive Committee, and Governing Board. Performance Improvement Evaluation An evaluation of the effectiveness of the Performance Improvement Plan will be conducted annually. Results from the plan evaluation will be used to set performance improvement priorities and goals for the upcoming year. Performance Improvement Priorities, Initiatives, and Projects Determination of performance improvement priorities and projects will be based on the results of the previous year’s PI efforts, program evaluation, and leadership input. See 2016 PI priorities. Action teams will be formulated to systematically address each of the priorities, while adjustments will be made if indicated during the current year.

2016%Quality%&%Performance%Improvement%Priorities%!
!!!
1. Become!a!Joint!Commission!certified!Stroke!Center!of!Excellence!and!explore!the!possibilities!of!becoming!Pain!and!Diabetes!Centers!of!Excellence.!!!
2. !Improve!Leapfrog!Hospital!Safety!Score!from!a!C!to!a!B!!!
3. Complete!basic!TeamSTEPPS!training!for!40%!of!the!workforce!!!
4. Meet!and!/!or!exceed!all!national!benchmarks!for!core!measures!and!publicly!reported!data!!!
5. Improve!overall!patient!experience!scores!to!national!average!!!
6. Hardwire!established!patient!experience!tactics!(AIDET,!white!board!usage,!bedside!shift!report,!hourly!rounding)!
!!
7. Adopt!at!least!2!evidenceTbased!clinical!protocols!by!department!!
!8. Maintain!healthcare!acquired!infections!below!national!benchmarks!
!!
9. Carry!out!planned!physical!enhancements,!renovations!and!maintenance!projects!to!further!improve!patient!experience!and!environmental!safety!!
!!
10. Adopt!an!“all!hands!on!deck”!or!the!“UMC!familyThome”!approach!to!maintaining!a!clean,!clutterTfree!and!wellTmaintained!hospital!environment!by!achieving!70%!of!Hospital!Consumer!Assessment!of!Healthcare!Providers!and!Systems!(HCAHPS)!cleanliness!rate.!