the next decade of service relationship to canada’s health system relationship to ontario’s...
TRANSCRIPT

Mobile Crisis InterventionThe Next Decade of Service

St. Joseph’s Health Centre
Relationship to Canada’s health system Relationship to Ontario’s health system Relationship to health system of the GTA Relationship with Toronto Police Service Where we work How we work How we’re doing Where we’re going

St. Joseph’s Health Centre

Canada

Ontario

Greater Toronto Area

Greater Toronto Area
SJHC

In Comparison…New York, N.Y. 8,175,133 Los Angeles, Calif. 3,792,621 Chicago, Ill. 2,695,598Toronto, ON. 2,615,060 Houston, Tex. 2,099,451Philadelphia, Pa. 1,526,006Phoenix, Ariz. 1,445,632 San Antonio, Tex. 1,327,407 San Diego, Calif. 1,307,402Dallas, Tex. 1,197,816San Jose, Calif. 945,942

SJHC Statistics for 2010-2011
Beds: 376Admissions: 21,657Births: 3,080Ambulatory care visits: 272,689 Surgical Cases: 31,568Diagnostic Imaging Procedures: 165,125Emergency Department Visits: 93,741
Mental Health ED Visits: 7,248

Mental Health and Addictions
• 26 bed Withdrawal Management Service offering residential, day and community services
• Addiction Medicine service with 13 family physicians
• 6 bed Child and Adolescent MH beds• 6 bed Short Stay Unit• 6 bed Psychiatric Intensive Care Unit• 29 general adult psychiatric unit

Mental Health and Addictions• Mobile Crisis Intervention Team• Geriatric Mental Health Outreach Team• Assertive Community Treatment Team• Case Management Team• Day Hospital• Depot Clinic• Shared Care Service• Psychiatric Outpatient clinic (16 docs, RN,
dietician)• Recovery Support Program

Hospitals in Toronto
SJHC

SJHC MHA ED visits compared to PEERS
0
1000
2000
3000
4000
5000
6000
7000
US Psych DT(homeless)
DT(Manhattan)
Uptown East End
MHA ED visits

(works for us)
socialized health care
OHIP• The Ontario Health Insurance Plan is funded
by taxes paid by the residents and businesses of Ontario and by transfer payments from the federal government.
• Every Ontario resident with his or her primary and permanent home in Ontario is entitled to access emergency and preventive medical care under OHIP free of charge. Ontario residents may go to any doctor practicing in the province any time they wish. It does not cover such areas as prescription drugs or dental care.

LHINThe 14 Local Health Integration Networks of Ontario
plan, fund and coordinate services delivered in their region by:
• Hospitals • Long-Term Care Homes • Community Care Access Centre's (CCAC) • Community Support Service Agencies • Mental Health and Addiction Agencies • Community Health Centre's (CHCs)

LHIN Priorities• INTEGRATION INITIATIVES include a continuum of
relationships that can exist between and among individual service providers, programs, organizations and systems of services
• Creating HEALTH EQUITY

MCITs in TorontoHOSPITAL PARTNER TPS
DIVISIONSSTART-UP YEAR
St. Michael’s Hospital 51/52 2000/1
St. Joseph’s Health Centre
11/14 2005/6
The Scarborough Hospital
41/42/43 2006/7
Humber River Regional Hospital
12/31 2006/7

TPS Divisions
SJHC MCIT Catchment Area
SMH MCIT Catchment Area
Scarborough Hospital MCIT Catchment Area
Humber River Regional Hospital MCIT Catchment Area

ParkdaleThe team works in an area which is heavily
populated by individuals suffering from a major mental illness:
Proximity to a former provincial psychiatric hospital
City by-laws that allow boarding homesA neighborhood with a large proportion of
former mansion-like homes with the potential to be subdivided
Becoming gentrified (which brings in even more drug traffic)

Parkdale
Parkdale

Parkdale

MCIT STATS 2011-12
Visits/calls: 903
Number of individuals served: 594
Telephone Consultations: 324
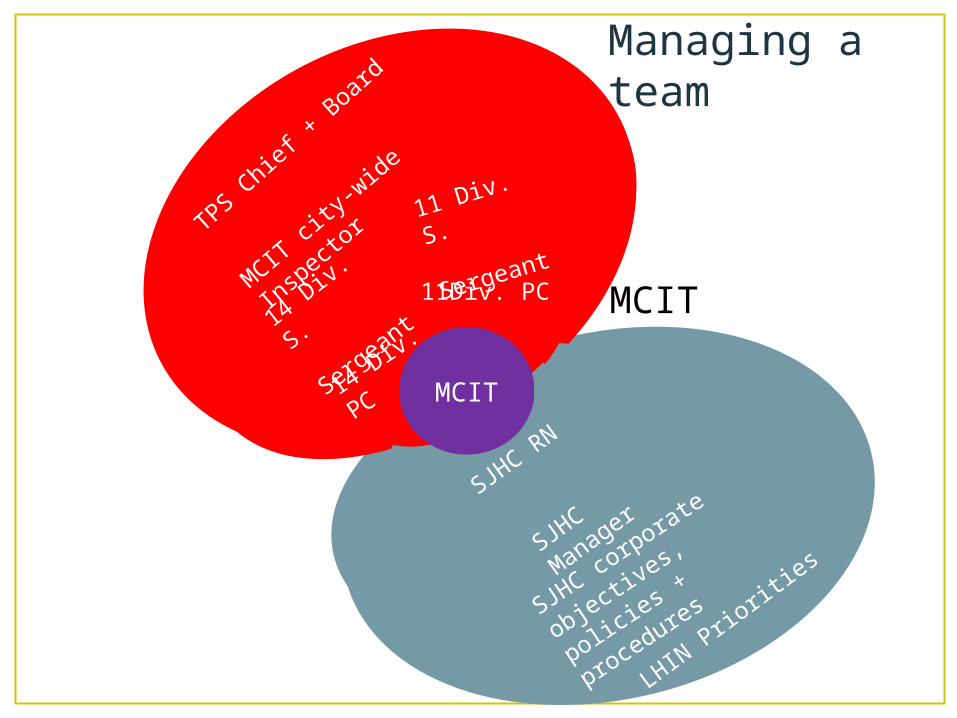
MCIT
TPS Chie
f + B
oard
MCIT ci
ty-wide In
specto
r
14 Div.
S.
Sergeant
11 Div. S.
Sergeant
11Div. PC
14 Div. PC
SJHC R
N
SJHC M
anager
SJHC corporate objectives,
policies + procedures
MCIT
LHIN P
rioriti
es
Managing a team


What’s Working
40%

What’s working• 2000 Pre-MCIT 2007
Post-MCIT
Source: St. Michael’s Hospital, 2007

How do we do it? Communication – RN and PC, manager and staff
sergeants cc on everything MOU Quarterly meetings Involved in each other’s hiring decisions Keep in the forefront the other organization's
mandate Education

Future goals
TrainingCity-wide coverage /standardization
EMS

Training for RN’s• Driving police vehicles• Firearms safety• Use of force

City-wide coverage

EMS• Communication between EMS & MCIT.
• Avoid unnecessary transports to hospital.
• Stop transport of people threatening suicide by EMS prior to MCIT arrival.
One our success stories:• 52 year old female• Borderline Personality • Dissociative Identity
Disorder• Numerous overdoses• Depression and anxiety• Frequent user of the
emergency services• Hospital visits varied
but could be as many as 3 per week

END OF ACT 1
Mobile Crisis InterventionThe Frontline Nurse Perspective

Mobile Crisis Intervention Team
• “Bringing the Emergency Room to the person in Crisis”

MCIT:• Is the partnership between St Joseph’s Health Centre and
Toronto Police Divisions 11/14• Utilizes the resources of 1 base hospitals and 2 local hospitals• Care provided is flexible re: hospitals & jurisdictions• Consists of a police officer in a modified uniform and a mental
health nurse, combining the expertise of both professions to determine the best care/response to each situation
• Responds to 911 calls involving individuals who are in crisis, non-emergency calls
• Respond to location of individuals in crisis within our divisional boundaries
• Operates 7 days a week, 365 days a year, 10 hours per day based on statistical analysis (1300-2300 hrs)

Purpose of MCIT:• To de-escalate crisis and avoid
unnecessary arrest and/or emergency room visits
• Provides short term support and stabilization in order to manage the crisis
• Provide referrals to services and resources available in the community
• Ensure continuity of care between the initial intervention and the involvement of follow up agencies
• Or simply EDP (Emotional Disturbed Person)

Mental Illness
• There is NO cookie cutter fix for those suffering from Mental Illness
• Symptoms of mental illness vary from mild to severe depending on the type of illness , the family and the socio-economic environment
• Severe impairments of thoughts & judgment - constituting a medical emergency
• Characterized by alternations in thinking ,mood or behavior

MCIT : Who do we serve ?• We provide
immediate on site response to people of all ages in our catchment area with urgent or emergent mental health
• This often includes addictions and/or homelessness issues

How do we get dispatched:
• Dispatched (radio calls)
• Divisions / Supervisors
• MCIT Cell• Hospitals / Doctors• Community agencies• Families• In car Computer /
volunteer

MCIT: calls we attend • Responds to calls involving bizarre behavior,
substance abuse and caring for people in crisis • Mental crisis could include thoughts of suicide ,
distorted or psychotic thinking , anxiety , overwhelming depression , feeling unable to cope and out of control
• Cases of suicidal attempts/ideation and self harm• Executes Forms 1, 2, 47 & 49 in conjunction with
other teams in the Mental Health and Addiction programs

Calls we do not attend:• Persons intoxicated
on drugs or alcohol• Elopee• Violent individuals or
people with weapons• Overdoses• Barricaded EDP’s• Individuals wanted on
“Forms” who’s location is not known.

MCIT: What do we do ?• Perform a mental health
assessment on site• Conduct appropriate
referrals to community agencies
• Provide telephone support and follow up visits
• Find appropriate shelter for the homeless
• Take client to hospital if deemed necessary
• Offer confidential , non-judgmental crisis support

CIT01

CIT01

CIT01

CIT01

CIT01

Difference in models of care used between the 2 disciplinesPolice : Use of Force
WheelNurse : Non-violent Crisis
Intervention Model

On the scene arrival:• Assess the situation• Attempt to stabilize and
defuse the crisis• Provide supportive counseling
as needed• Provide information and
referrals, linkages to appropriate community services and support for ongoing treatment
• Transport individuals to the hospital emergency dept. if further psychiatric and/or medical treatment needed
• Follow up visit

MCIT : Goals• Immediate response to people in crisis• To quickly and safely de-escalate the situation• Provide on site response to a crisis ensuring the best
care• Diversion from the emergency dept.• Keep frontline workers free and available • Provide referrals to services and resource in the
community• Teaching and educate clients, families, colleagues and
community about crisis intervention and prevention • Proactive approach to avoid unnecessary contact with
the criminal justice system

Challenges – Nurses Perspective
PROS• Utilizing RN’s• Client centered care• Close working
relationship with Police Officers
• Ongoing education to PRU increases utilization of CIT
CONS• Accommodating 2
perspectives (i.e..: Medical vs. Police)
• Dealing with old school thinking
• Difficulty with EMS• Police car (office on
wheels)

Benefits to having RN attend on scene crisis
• Provides a range of crisis services on multiple levels
• Knowledge of medications & ability to give prescribed medications
• Assess treatment needed• Establish a relationship & level of
trust• Cooperating with Dr’s, Psychiatrist
& community agencies to execute the care needed for individual
• Protect the rights of the client by advocating on their behalf
• Networks with law enforcement to facilitate medical services for individuals who are at imminent risk of danger

Medical issue presenting as mental illness: call MCIT 01 attended
Verbatim description as reported to CIT :“Complainant saying there is a male in the house and he doesn’t know him. Not talking to compliant . Male black, unknown age wearing black and white shirt. Compliant sounds EDP. Can’t give a description of male, has his pants over his head. Also reports seeing some kind of animal.”Police officer and Sergeant speaking to male. Admits to seeing the black male in police presence and unknown animals.Gun cabinet in room containing his hunting rifles. (properly/legally stored)

On Scene:• Many stressors.• Had not slept x 4 days.• Increased alcohol consumption since the death of his
father.• Denies any mental health history.• Concerned for his mothers well being since his father
death 1 year earlier.• Marriage breakup.• Chronic back pain x 2 yrs..• Fighting with city contractor re: faulty sidewalk repairs that
caused his mother to fall.• Fighting flu like symptoms.• Taking excessive over the counter medication.

Presenting issues:• Substance abuse• Financial burdens• Relationship problems• Legal problems• Specific symptoms of mental illness• Guarded in presence of police officer• Feeling run down and generally unwell
• Psychiatric illnesses:• None
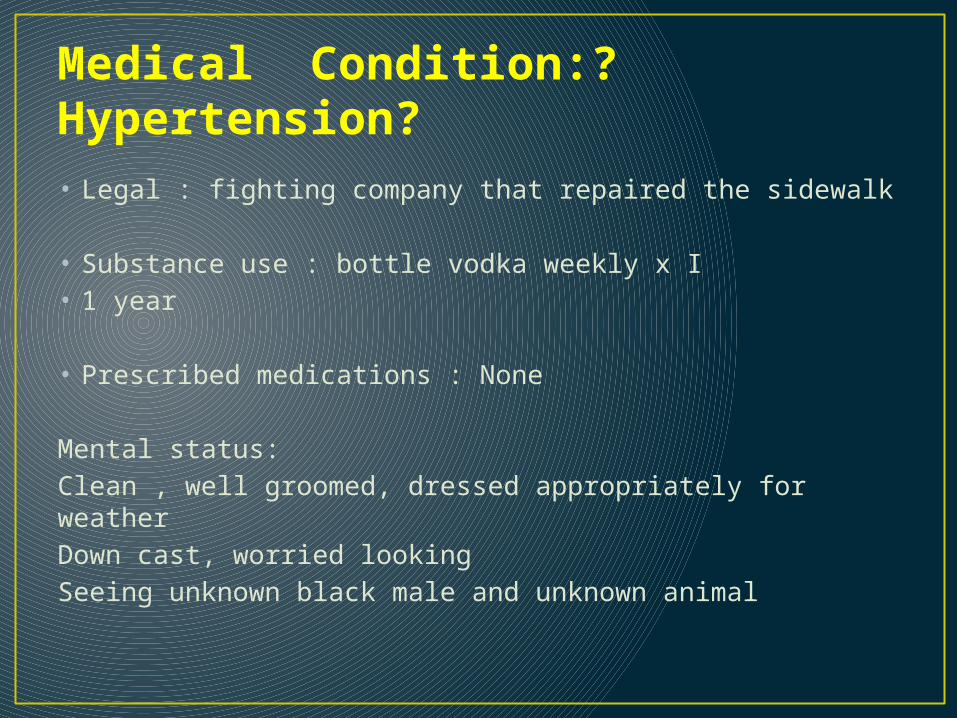
Medical Condition:? Hypertension?• Legal : fighting company that repaired the sidewalk
• Substance use : bottle vodka weekly x I• 1 year
• Prescribed medications : None
Mental status:Clean , well groomed, dressed appropriately for weatherDown cast, worried lookingSeeing unknown black male and unknown animal

Risk Assessment:• Denies/No evidence of suicidal ideation.• No past history of suicide attempts.• Denies/No evidence of harm to self or others.
• Recommendations:• No grounds for Mental Health Act apprehension.• Encouraged male to attend the hospital with MCIT
to be checked out medically.

Outcome:• The male was admitted to hospital.• Officers on scene took the male’s guns due to safety
issues regarding his hallucinations.• Was not to be put in the police system as an
“Emotionally Disturbed Person”.
• Follow up:• PC Zawerbny had found out that the male had been
put in the system as “EDP”. This meant the male would not get his guns back.
• A follow up visit was needed to find out his diagnosis.

Final Diagnoses/Outcome :• Myocardial infarction • Alcohol withdrawal
• The record of events was changed to show that no mental health issues existed and thus the male was able to get his firearms returned.
One our success stories:• 52 year old female• Borderline Personality • Dissociative Identity
Disorder• Numerous overdoses• Depression and anxiety• Frequent user of the
emergency services• Hospital visits varied
but could be as many as 3 per week

END OF ACT 2

The Psychiatrist’s Perspective


“What is Working Well”

“What is Working Well”
Nothing!Good RelationshipWith Police


Information Flow: Hospital

Information Flow: MCIT


“Perspectives of Psychiatry”
Disease
Dimensional
Behavior
Life Story

“Perspectives of Psychiatry”
Disease
Dimensional
Behavior
Life Story
Treat
Coach
Interrupt
“Rescript” (psychotherapy)

“Perspectives of Psychiatry”
Disease
Dimensional
Behavior
Life Story
Treat
Coach
Interrupt
“Rescript” (psychotherapy)
Requires patient engagement

“Mr. X”Disease
Dimensional
Behavior
Life Story
Schizophrenia
Mild MR, Narcissistic
Threatening, Assault
“unsocialized”
Requires patient engagement

Towards the Future
Consulting psychiatrist for every MCIT.
Liaison with Mental Health Courts

END OF ACT 3

Mobile Crisis Intervention
The Police Officers Perspective

The Toronto Police Service Uniformed Officers – 5,629 Population Served – 2,855,085 Gross Operating Budget – 1,000,778,700 Largest urban police
service in Canada.
• •

Calls for Service - 2011• Total calls received
– 2,067, 938• Total calls
dispatched – 921,722
• Calls dispatched in 11 & 14 Divisions
• 97,171

EDP Calls City Wide
2009 – 16,976
2010 - 17,513
2011 – 19,454
11 & 14 Division
2009 – 2785
2010 – 2970
2011 - 3336

Calls We Attended
2009 – 482 2010 – 545 2011 – 665

Hospital vs. Police “Police officers are concerned with
immediate crisis response whereas the mental health system is slow, cumbersome and looks for longer term solutions. Whereas the motto of the medical profession might be “Above all, do no harm”, the public expectation of the police is more likely, ”Above all, do something!
Dr. Dorothy Cotton, Feb 2005

The Perfect Team

The Uniform
“Depending on the background of the citizen, the police uniform can elicit emotions ranging from pride and respect, to fear and anger”Richard Johnson, The Psychological Influence of the Police Uniform

“We know that contact with police is often traumatic for people with mental illness.”
Canadian Mental Health AssociationStudy in Blue and Grey, 2003

Plainclothes OptionLess intimidatingMore approachable
Shows understanding
Less noticeable to neighbors or bystanders.
Decreases Stigma
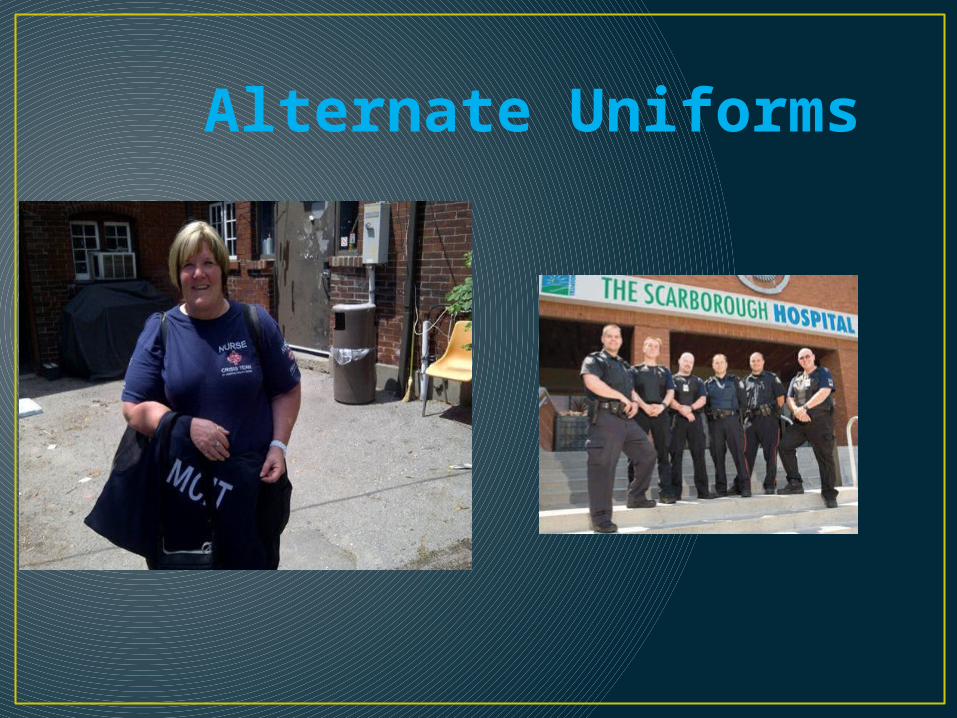
Alternate Uniforms

Specialized Units = Special Identification

UPDATED DESIGNS

Our Cars

VEHICLE OPTIONS

LITTLE THINGS

We’ll take you to the hospital
Sorry, It’s our Policy

Why?• “Because my daddy did it and his daddy did it and his
daddy before that did it.”
• Top 10 myths about mental illness – EDP’s are violent.
“Combating stigma is a continual process. This seems to be especially true when the very culture of a system, like the criminal justice system, has incorporated many of the most extreme manifestations of stigma and discrimination.”
Tom Lane, Director of Consumer Affairs, National Alliance on Mental Illness, USA

ARE THEY NECESSARY?No Handcuffs
reduces**
- Stress - Anxiety- Shame- Embarrassment- Stigma
(** All risk factors have been assessed)
Benefits
• Continuity of Care• Trust• Future contact


Training = Understanding
“When police respond to a person in a mental health crisis as they are trained to respond to a typical criminal emergency situation – with a show of force and authority – they may in fact escalate the crisis to a point of risking injury or death for police or the public, but most often for the person in mental health crisis.•
• Canadian Mental Health Association• British Columbia, 2005

Top to Bottom• Everyone in your organization needs EDP training.• Organize training days.• Organize or get involved with committees to study
the success, failures and necessity of your CIT program.
• Most common phrases heard by CIT member at committee meeting:
• “ I did not know that”• “ We’re glad you’re here to explain this”• “Your obviously very passionate about your work”.• Change old school thinking.

Goals worth reaching for.• Uniform changes/alterations - (Decision pending)• Vehicle changes/alterations – (Achieved in
principal)• Policy changes/recognition – Handcuffing Option
(Achieved?)• Simultaneous response – (Achieved)• Patient transport – (Achieved)• In car camera – No use option. – (Achieved)
• Getting all this in writing? (Ask me at the next conference)

Questions