the nephrotic syndrome def: it is a clinico -biochemical state of many causes features 1-heavy...
TRANSCRIPT
The nephrotic syndrome
Def: It is a clinico -biochemical state of many causes
Features1-Heavy proteinuria.2-Hypoproteinemia.( decrease protein in the blood)3-Generalized oedema.4-Hyperlipidemia and lipiduria

Causes
Renal1-Membranous GN2-membranoproliferative GN3-Minimal change GN4-Focal segmental GS5-Focal GN.(Mesangial,IgANephropathy)
Systemic Diseases1-SLE2-DM3-Amyloidosis4-Infections e.g.; malaria, HBV,BSyphilis6-lymphoma7-Drugs:gold salt and NSAI

Common features of nephrotic syndrome
Gross
-Enlarged pale kidney. -yellow ting due to fat resorption by tubular epithelium.

Microscopic
1-Glomeruli;• LM&IF: Features specific to the disease.• EM: Fusion of foot processes of podocytes.
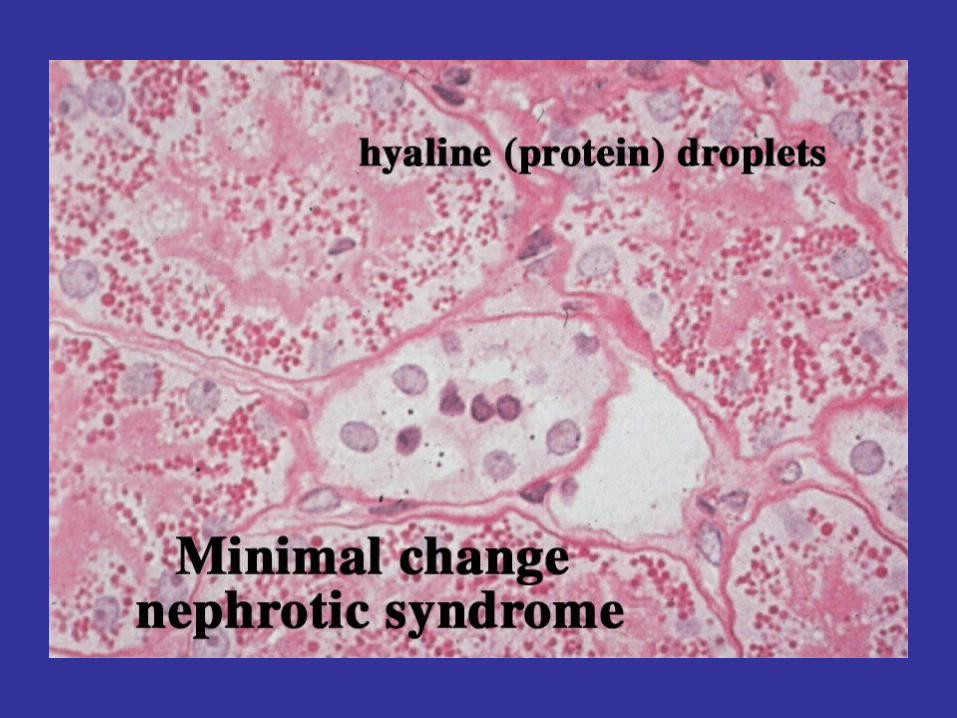
2-Tubules• 1-Hyaline droplets. • 2-Vacuolar degeneration due to resorption of
fat • 3-Hyaline casts
3-Interstitial tissue
variable oedema

Hyaline casts

Membranous GN
Age: adults (30-50 ys)
Cause:--Primary :Unknown (85%)-Secondary in course of infection like malaria syphilis, HBV, B, malignant tumors and gold salt therapy
Patho: ICD
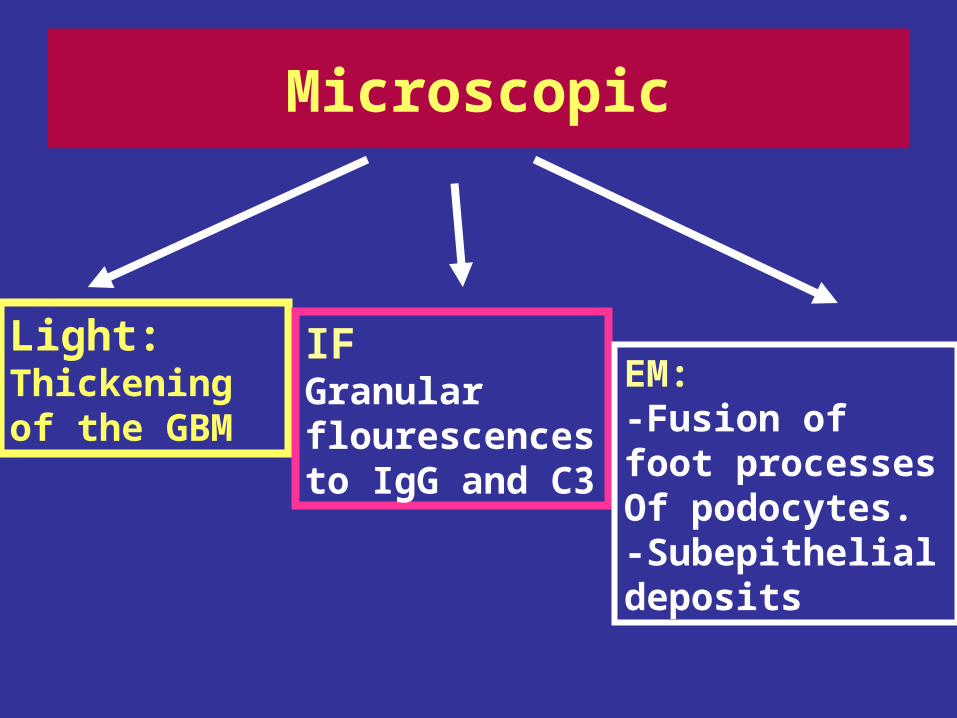
Light:Thickening of the GBM
IFGranular flourescences to IgG and C3
EM: -Fusion of foot processes Of podocytes.-Subepithelial deposits
Microscopic
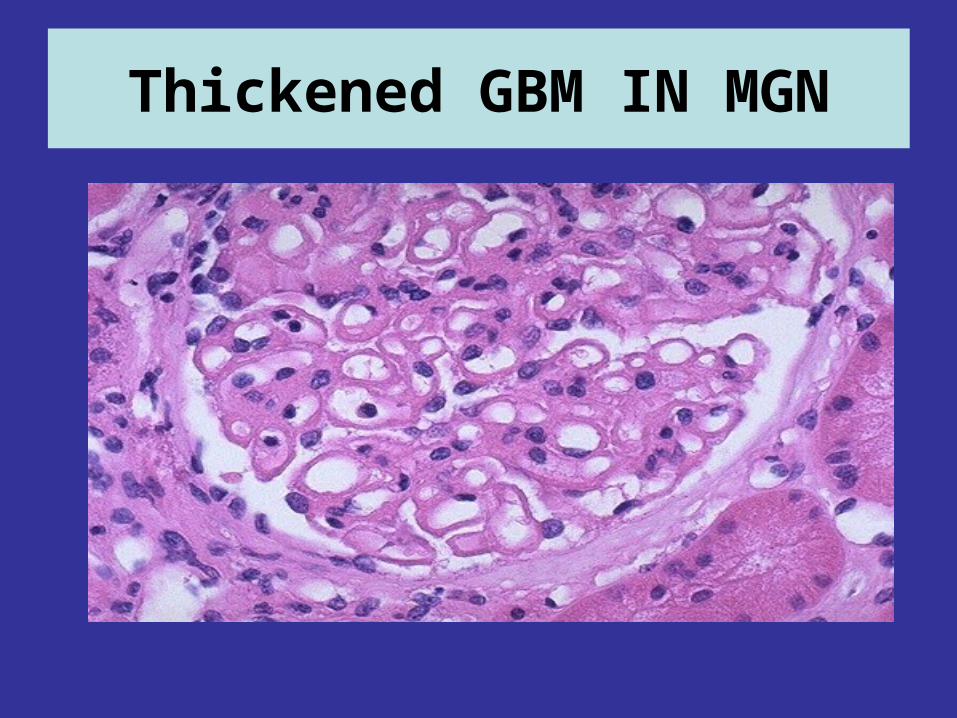
Thickened GBM IN MGN

Sikes formation in MGN.Silver stain

Spikes formation along GBMSilver stain

Diffuse granular fluorescence of GBM

EM in MGN, the darker electron dense immune deposits are seen scattered within the thickened
basement membrane.

Membranous GN.EM
Subepithelial Deposits
Clinical and laboratory findings Nephrotic syndrome
Prognosis: Remission and exacerbation, finally chronic renal failure.
Minimal change GNAge: Commonest cause of nephrotic syndrome in children (1-4 ys )
Pathog: unknown or it is a disorder of T cells cytokines that cause loss of epithelial foot processes
Gross: as Nephrotic syndrome.
Msc:1-Light
Glomeruli ; no changes.

Tubules and interstitial tissues show changes of nephrotic syndrome
2-IF: Negative.3-EM: Fusion of foot processes of podocytes
Clinical and laboratory findings : as NS with selective proteinuria.
Prognosis: good response to steroid therapy

Membranoproliferative GN
Age; any age, mainly late childhood
Pathogenesis;
Type I; Common. It is ICD
Type II (Dense deposit disease) :rare mediated by activation of the alternative complement pathway.
Hypercellularity
Accentuated lobulation
Patchy irregular thickening of GBM
Double contour of
GBM
MSC;1-Light

MPGN, the glomerulus has increased overall
cellularity, mainly mesangial
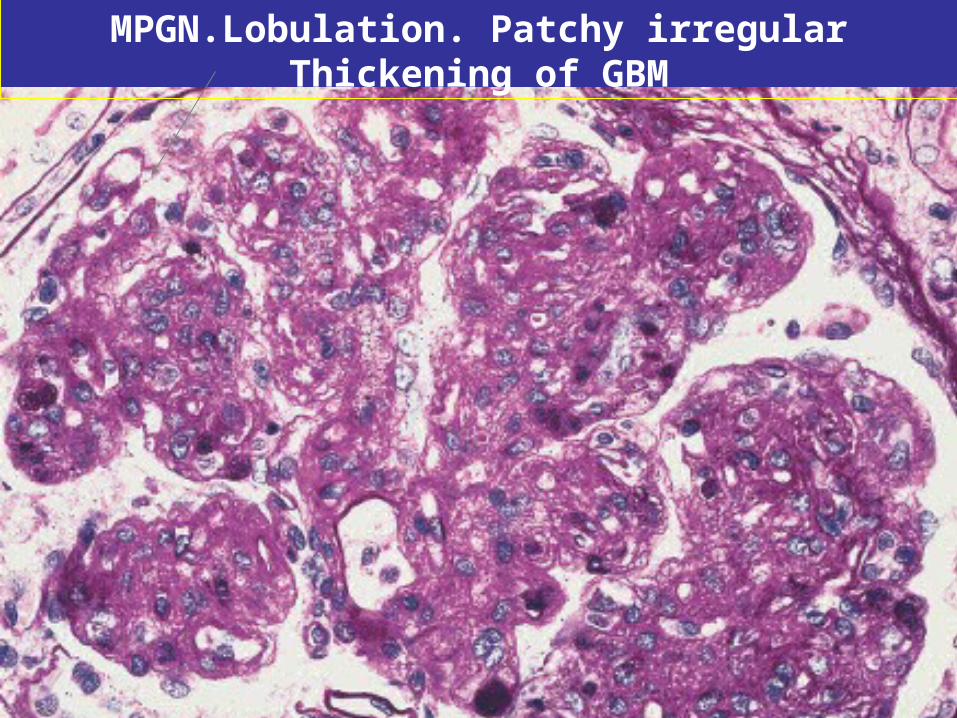
MPGN.Lobulation. Patchy irregular Thickening of GBM

New matrix material is laid down resulting in replication of basement membrane material
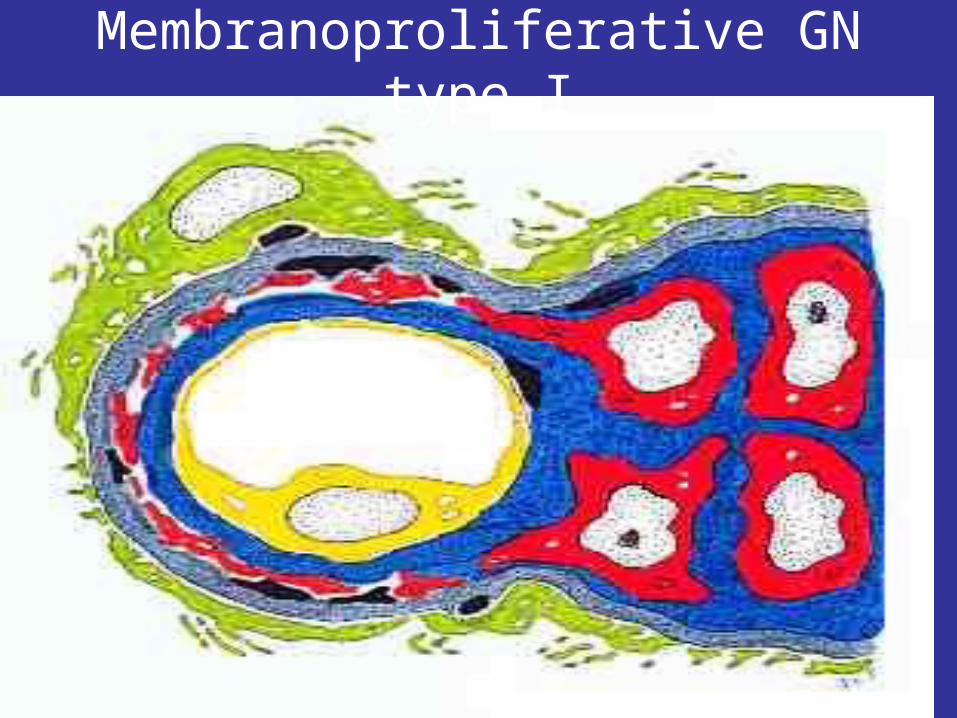
Membranoproliferative GN type I

This silver stain demonstrates a double contour to many basement membranes, or the "tram-tracking" that is
characteristic of MPGN
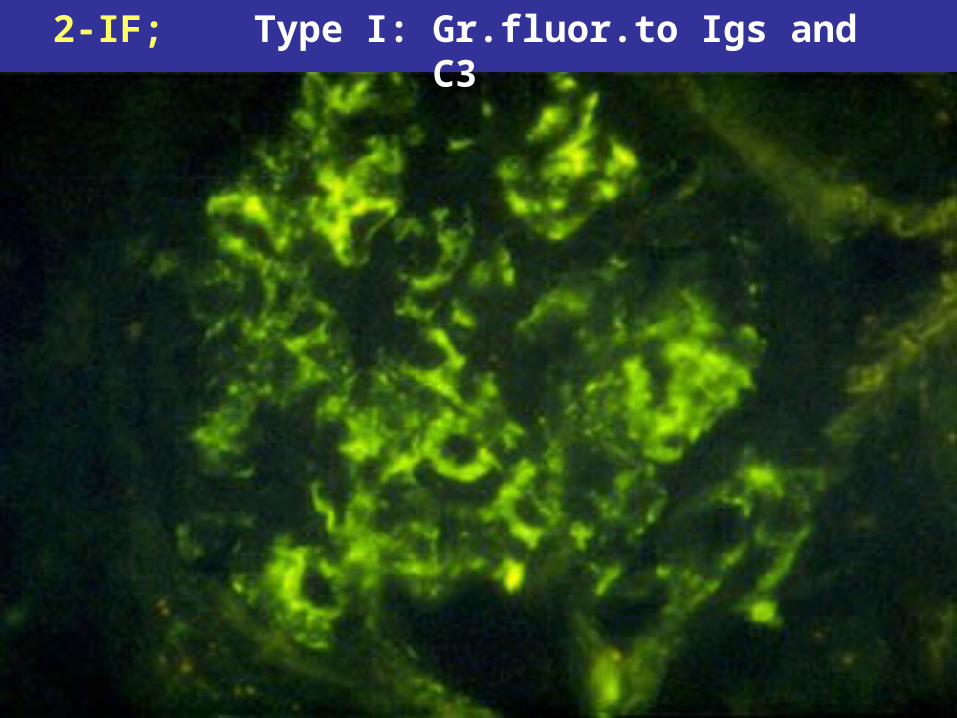
2-IF; Type I: Gr.fluor.to Igs and C3

Bright deposits in type II MPGN To C3

TYPE II, intramembranous deposit

Clinical and laboratory findingsPresentation
Nephrotic syndome+ hypertension
Nephritic syndrome
Asymptomatic proteinuria
Prognosis : remission exacerbation and finally chronic renal failure

Focal segmental glomerulosclerosis
Microscopic: -Sclerotic segments in some gl. and Hyalinosis -tubular atrophy -interstitial fibrosis
IF: Granular fluorescence of the GBM for IgM andC3.EM:Fusion of foot processes and detachement of epithelial cells

Focal segmental GS




Clinically: Nephrotic syndrome, may be hypertension and microscopic hematuria.
Prognosis: unfavorable (ending in chronic renal failure

Cause: -idiopathic -In association of SBE,SLE, Henoch-schonlein PAN, and Goodpasture’s syndromePathogenesis: -ICD -Activation of the alternative complement pathway by aggregation of IgA.(Berger’s disease)
Focal glomerulonephritis

IgA Nephropathy (Berger’s Disease)
-Common in children and young adults- Recurrent hematuria-It follows infection of the respiratory,GI
and urinary tracts.-The IgA is deposited mainly in
mesangium, which then increases mesangial cellularity

MSC: Focal and segmental proliferation of mesangial cells+ necrosis and crescent formation
Clinically: Hematuria, proteinuria and may be nephrotic syndrome
Course: Subsides without residual renal impairment

Focal glomerulonephritis
IF:Granular

Focal GN
Necrosis

Amyloidosis

Amyloidosis of the kidney

Disease LM EM IFMembranous GN
MPGN
Minimal change
Focal and
Seg.GS
Focal GN
Lupus Nephritis
Chronic GNDef: it is end stage renal glomerular disease.
Grossly:-Small contracted kidney.-Granular outer surface.-Firmly adherent capsule.-Loss of differentiation bet. cortex and medulla.-Thick BVs at corticomedullary junction.

Chronic GN: Note contacted kidney& granular outer surface

Msc:
Glomeruli: -Hyalinised and sclerotic.-Some are hypertrophied.
Tubules are atrophied and
dilated
Interstitial fibrosis and
chronic inflammatory cell
infiltration
Thick walle-blood vessels end arteritis obliterans

Chronic glomerulonephritis

Hyaline cast
Chronic GN

Clinical and laboratory Findings:
Marked hypertension
IncreaseBl. urea
Urine changes-Polyuria.- low Specific gra.-Mild albuminuria.-Hyaline and -granular casts
Prognosis: without Treatment is poor

Small- Sized Kidney (contracted kidney)
1-Hypoplastic kidney.
2-Chronic GN
3-Chronic PN
4-Senile(atherosclerotic) kidney.
5-Kidney of benign hypertension (Benign nephrosclerosis).

DMEffects of DM on the kidney:-Diabetic GS-Renal arteriolar sclerosis.-pyelonephritis.-papillary necrosis.
Diabetic GSIt leads to:a-Proteinuria.B-Nephrotic syndrome.C-CRF.

MSC: 1-Diffuse GS.-Diffuse increase in mesangial matrix-Thickening of GBM2-Nodular GS. (kimmelsteil Wilson disease)Hyaline nodule is present in the mesangium,Containing fibrin and lipid.
3-Insudative lesion:-fibrin cap; eosinophilic focal Thickening of peripheral capillary loop.-Capsular drop: eosinophilic thickening of Bowman’s capsule

Diffuse glomeruosclerosis


Nodular GS

Nodular GS

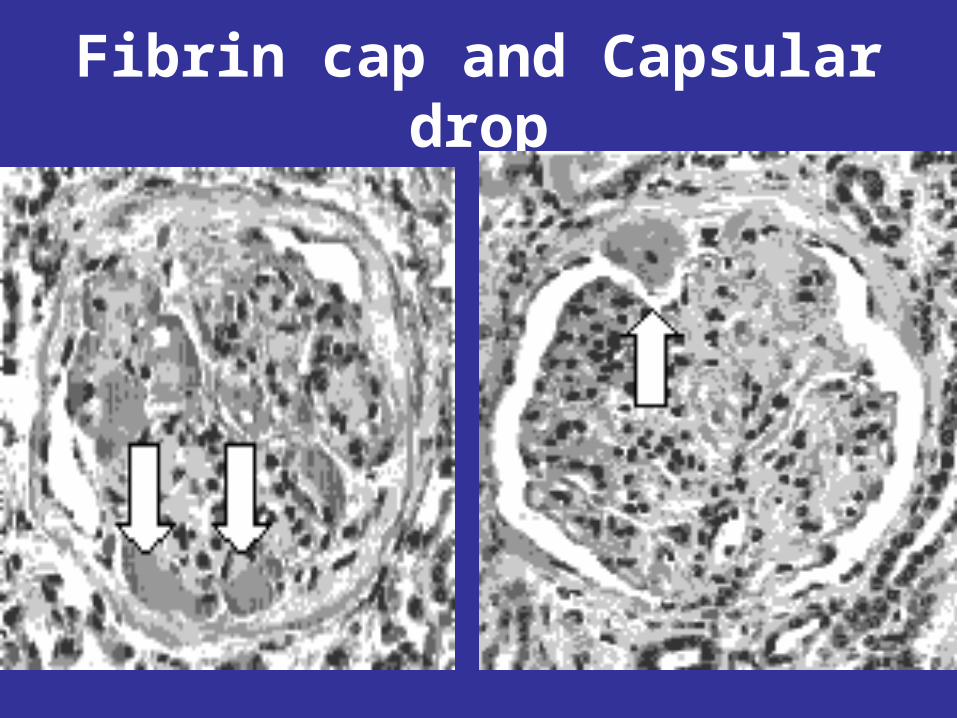
Fibrin cap and Capsular drop

Lupus nephritis
Presentation: Recurrent hematuria,nephritic s,nephrotic s,hypertension,CRF.
Classification;-class I:Normal kidney.-Class II:Mesangial glomerular lesion.-Class III:Focal proliferaive GN.-Class IV:Diffuse Proliferative GN.-Class V:Membranous GN.-Class VI:Advancing sclerosing GN.
MSC of Class IV: Diffuse Proliferative GN
-Diffuse hypercellularity due to Proliferation of endothelial cells and mesangial cells -Irregular thickening of GBM - Wire loop appearance-Few epith.crescents-Hematoxylin bodies.

Proliferative lupus nephritisFlea-Bitten appearance

Class II: Mesangial GN

Class III: Focal GN
Focal and segmental necrosis of glomerulus
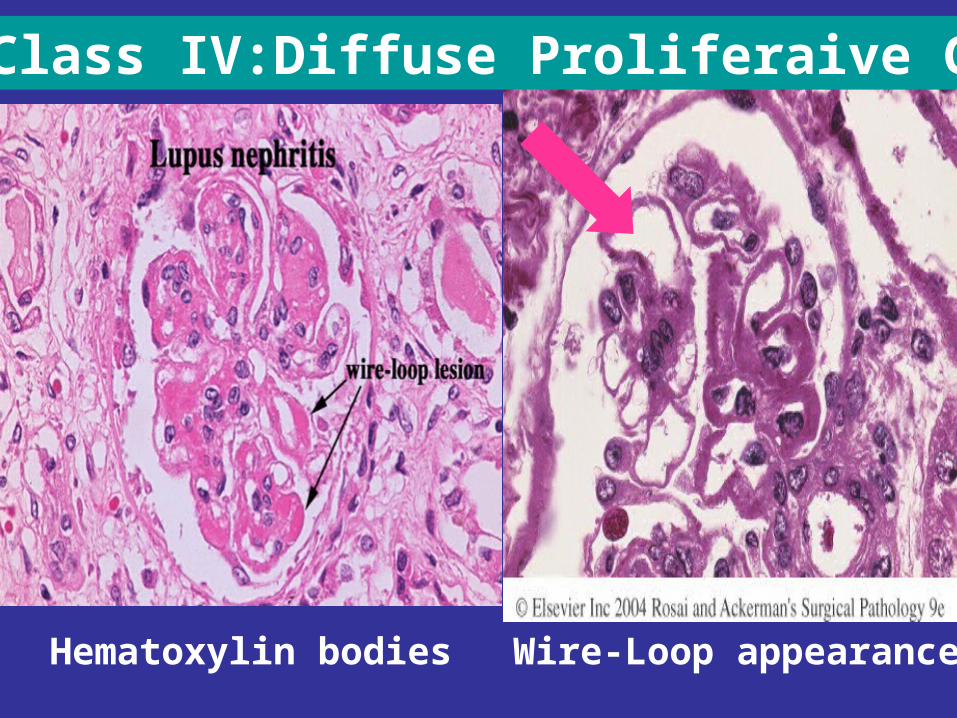
Class IV:Diffuse Proliferaive GN
Hematoxylin bodies Wire-Loop appearance

IF of Lupus Nephritis

EM of Lupus Nephritis

• IF: Granular fluorescence of capillary walls for Igs and comploments
• EM: Subendothelial and mesangial electron dense deposits