the musculoskeletal system roman a. goy md medical officer odp/office of medical assistance...
TRANSCRIPT

The Musculoskeletal System The Musculoskeletal System
Roman A. Goy MD
Medical Officer
ODP/Office of Medical Assistance
September 1, 2015[This presentation has not been approved by ODP to convey policy.]
1

The Musculoskeletal System The Musculoskeletal System
Disability Evaluation Under Social Security
1.00 Musculoskeletal System - Adult
2

The Musculoskeletal System The Musculoskeletal System
Disability Evaluation Under Social Security
1.00 Musculoskeletal System – Adult
1.02 Major Dysfunction Peripheral Joints
1.03 Reconstructive Surgery
1.04 Disorders of the Spine
1.05 Amputation
1.06 Fracture of major lower extremity bones
1.07 Fracture of upper extremity bones
1.08 Soft tissue injury (burns)
3

1.02 - 1.02 - Major dysfunction of a jointMajor dysfunction of a joint
A) One major peripheral weight bearing joint -
Resulting in inability to ambulate effectively.
B) One major peripheral joint in each upper extremity –
Resulting in inability to perform fine & gross movements effectively.
4

Disorders of the MS System Disorders of the MS System 1.00
Inability to ambulate:
•The inability to ambulate effectively
•on a sustained basis for any reason,
•including pain associated with the underlying musculoskeletal impairment.
5

Disorders of the MS System Disorders of the MS System 1.00
Effective ambulation requires being:
•Capable of sustaining a
• Reasonable walking pace • Over a sufficient distance • To carry out activities of daily living.
6
Effective AmbulationEffective Ambulation
Important:
The ability to walk independently at home without use of assistive devices does not, in and of itself, constitute effective ambulation
7

Examples of Effective AmbulationExamples of Effective Ambulation
Able to travel to and from work or school without companion assistance
8

Ineffective AmbulationIneffective Ambulation
Is an extreme limitation of the ability to walk
i.e. to independently initiate, sustain, or complete activities.
Generally defined as…
9

Definition of Ineffective AmbulationDefinition of Ineffective Ambulation
• Insufficient lower extremity functioning
to permit independent ambulation
• without the use of a hand-held assistive device(s) that limits the functioning of both upper extremities
10

Examples of Ineffective AmbulationExamples of Ineffective Ambulation
Inability to walk without use of a
walker
Inability to walk without use of two
crutches or two canes
11

Examples of Ineffective AmbulationExamples of Ineffective Ambulation
Inability to use standard public transportation
12

Examples of Ineffective AmbulationExamples of Ineffective Ambulation
Inability to carry out routine ambulatory activities such as
•SHOPPING
•BANKING
13

Examples of Ineffective AmbulationExamples of Ineffective Ambulation
Inability of climb a few steps at a reasonable pace with use of a single hand rail
14

Examples of Ineffective AmbulationExamples of Ineffective Ambulation
Inability to walk a block
at a reasonable pace
on rough or uneven surfaces
15

1.02 - 1.02 - Major dysfunction of a jointMajor dysfunction of a joint
Characterized by:
Gross anatomical deformity (subluxation, contracture, ankylosis, instability)
Chronic pain & stiffnessSigns of limitation of motionJoint space narrowing, bony destruction, or ankylosis on appropriate imaging
16

Major dysfunction of a joint(s) due to Major dysfunction of a joint(s) due to any cause any cause Listing 1.02
Shoulder
Elbow
Wrist-hand
17
Inability to perform fine and gross Inability to perform fine and gross movements effectivelymovements effectively
Means an extreme loss of function of both upper extremities.
18

Loss of Function – Upper Loss of Function – Upper ExtremitiesExtremities
Extreme loss of function of both upper extremities,
i.e., inability to initiate, sustain, or complete activities, such as:
•Reach, push, pull, grasp, and finger to complete ADLs.•Prepare meals and feed oneself.•Take care of personal hygiene.•Sort and handle papers and files.•Place files in a cabinet at waist or higher level.
19

1.03 – 1.03 – Reconstructive surgery of a Reconstructive surgery of a jointjoint
Major weight-bearing joint
Inability to ambulate effectively
Within 12 months of onset
20

Reconstructive surgery or surgical Reconstructive surgery or surgical arthrodesis of a major weight bearing joint arthrodesis of a major weight bearing joint
1.031.03
Talus fracture dislocation•s/p ORIF and ankle fusion
•with inability to ambulate effectively•for 12 months from onset
21Meets Listing 1.03

Reconstructive surgery or surgical Reconstructive surgery or surgical arthrodesis of a major weight bearing joint arthrodesis of a major weight bearing joint
1.031.03
Osteoarthritis of the knee•s/p total knee replacement•With complications infection, failure of revision•And inability to ambulate effectively, •For 12 months from onset
22Meets Listing 1.03

Reconstructive Surgery - ArthroplastiesReconstructive Surgery - Arthroplasties
• Joint replacements (arthroplasties) generally have a >95% success rate
• Most provide improvement of function within 1 month
• Do not assume work-related functional limitations merely because a claimant has a prosthetic joint
23

Normal Spine, Disc & NervesNormal Spine, Disc & Nerves
Lumbar spine
•Vertebral bodies•Intervertebral discs•Facet joints•Foramen
24
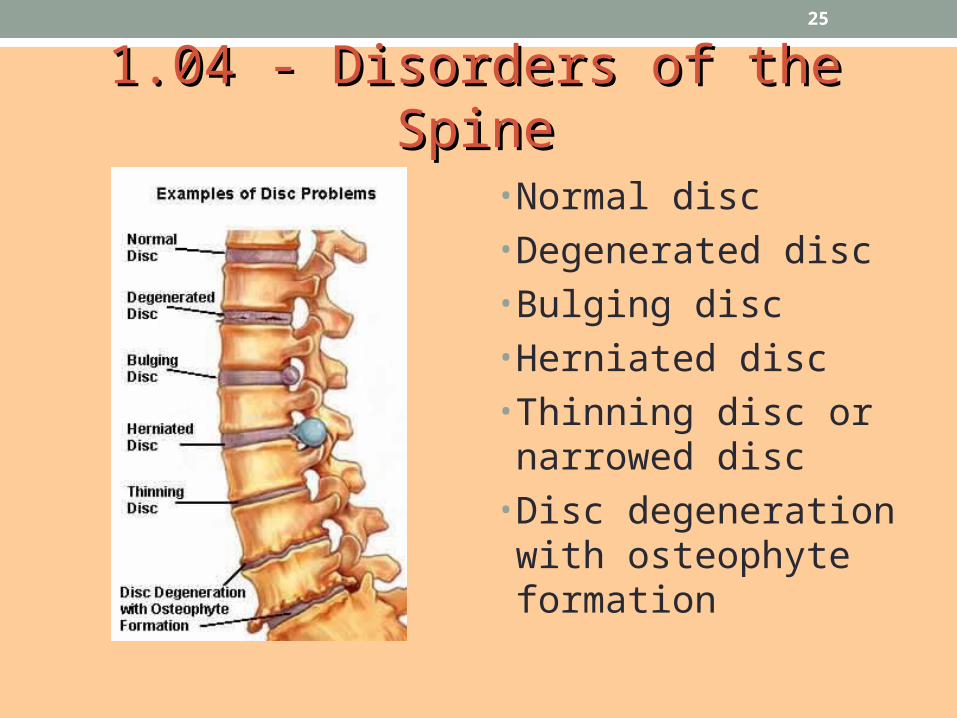
1.04 - Disorders of the Spine1.04 - Disorders of the Spine
• Normal disc• Degenerated disc• Bulging disc• Herniated disc• Thinning disc or narrowed disc
• Disc degeneration with osteophyte formation
25

1.04 - Disorders of the Spine1.04 - Disorders of the Spine
Herniated lumbar disc can cause a •Compressed spinal nerve, or •Compressed thecal sac compression
26

1.04 - Disorders of the Spine1.04 - Disorders of the Spine
Facet joint arthritis can cause:
•Low back pain•Impingement of nerve roots leaving foramen•Radiculopathy (pain radiating down thighs and legs with sensory loss and motor loss)
27

1.04 - Disorders of the Spine1.04 - Disorders of the Spine
• Lumbar spinal stenosis—the lumbar canal is smaller on the right
• Compressing the neural canal (pressure on nerve roots, cauda equina
• Causing low back pain, motor and sensory loss
28

1.04 - Disorders of the Spine1.04 - Disorders of the Spine
• Cauda equina (horse’s tail) is the nerve roots which come off the end of the spinal cord
• Nerve roots to rectum, anus, bladder (damage causes loss urine and bowel control)
29

Similar, But Confusing TermsSimilar, But Confusing Terms
Spondylitis
• Autoimmune disorder (ankylosing s.)• Causes inflammation between the vertebrae
30

Similar, But Confusing TermsSimilar, But Confusing Terms
Spondylosis
• Degenerative osteoarthritis of the spine• Changes in the cartilage, disk, and bone
Spondylolysis
• Fracture of a pars interarticularis vertebra• Usually affects 5th lumbar vertebrae
31

Similar, But Confusing TermsSimilar, But Confusing Terms
Courtesy American Academy of Orthopedic Surgeons
32

Similar, But Confusing TermsSimilar, But Confusing Terms
Spondylolisthesis
• Slippage of one vertebrae on another (usually lumbar)
• Graded from I – IV (depending upon %)
33

Similar, But Confusing TermsSimilar, But Confusing Terms
Bulging disc
• Disc “bulges” from its “normal” anatomic position
• Does not necessarily cause symptoms• Often temporary
34

Similar, But Confusing TermsSimilar, But Confusing Terms
Protruding disk
• More than a “bulge”, but less than herniation• May cause intermittent symptoms depending upon location
• Usually resolves spontaneously or with conservative management
35

Similar, But Confusing TermsSimilar, But Confusing Terms
Herniated disc
• Gelatinous material in center of disc pushes out through fibrous outer layer
• Think hockeypuck sized jelly doughnut
• Most resolve (heal) spontaneously or with conservative management
• More common in cervical and lumbar spines
36

Intervertebral Disc HerniationIntervertebral Disc Herniation
37

Similar, But Confusing TermsSimilar, But Confusing Terms
Spinal canal stenosis
• Narrowing of the spinal canal through which the spinal cord or cauda equina passes
• Touching vs. impingement• Impingement of the cord is neurosurg emergency
• Trauma• Posterior disc herniation in C-spine
38

Similar, But Confusing TermsSimilar, But Confusing Terms
Spinal canal stenosis
• Spinal stenosis of the cauda equina (below L3) much more common• Often degenerative in nature• May be due to trauma
39

Similar, But Confusing TermsSimilar, But Confusing Terms
Foraminal Stenosis
•Foramina are the bony opening of the vertebrae through which the peripheral nerves pass
•May be due to
• Degenerative spine disease• Osteophytes/spurs (also degenerative)• Trauma
40

Sensory DermatomesSensory Dermatomes
Correlation between the nerve roots coming out of the spine and the areas of innervation
41

1.04 - Disorders of the Spine1.04 - Disorders of the Spine
• Neuroanatomic distribution of pain
• L5 nerve root compression causes pain and paresthesias (numbness tingling) along lateral thigh, anterolateral leg, top of foot between 1st & 2nd toes
42

Motor MyotomesMotor Myotomes
Correlation between the nerve roots and the areas of motor innervation
43

1.04 - Disorders of the Spine1.04 - Disorders of the Spine
Some Causes of Arachnoiditis
Infection e.g. Meningitis Myelographic Dyes
(Especially Oil Based Myodil (pantopaque)
Epidural Steroid InjectionDepo-MedrolChemonucleosis with
chymopapainSubarachnoid Hemorrhage
44

1.04 Disorders of the Spine1.04 Disorders of the Spine
45

1.04 – 1.04 – Disorders of the spineDisorders of the spine
E.g. herniated disk, arachnoiditis, stenosis,
osteoarthritis, DJD, facet arthritis, fracture
Compromise of a nerve root or cord
WITH
46

1.04 1.04 AA – – Disorders of the spineDisorders of the spine
Nerve root compression
Neuroanatomical distribution of pain
Limitation of motion of spine
Motor loss (atrophy or weakness)
Sensory of reflex loss
SLR if Lumbar (sitting & standing)
OR
47

1.04 1.04 BB – – Disorders of the spineDisorders of the spine
Spinal arachnoiditis
Confirmed by operative or path report or AMAI
Severe burning or dysthesias
Need to change position every 2 hours
OR
48

1.04 1.04 CC – – Disorders of the spineDisorders of the spine
Lumbar spinal stenosis
Resulting in pseudoclaudication
Established by AMAI
Chronic non-radicular pain & weakiness
Inability to ambulate effectively
49

1.05 – 1.05 – AmputationAmputation
A) Both hands or
B) 1 or both extremities at or above tarsalsInability to use prosthesis to ambulate effectively due to stump complications
At least 12 months or
D) 1 hand & 1 lower extremity w/ ITAE or
D) Hemipelvectomy or hip disarticulation
50

Prognosis after AmputationPrognosis after Amputation
Over 90% expected to be successful after 4- 6 months
51
Prognosis after AmputationPrognosis after Amputation
Normal Steps (barring complications):
• Healing of the stump• Fitting of the prosthesis• Learning to use the prosthesis
52

Orthotic, Prosthetic, Orthotic, Prosthetic, or Assistive Devicesor Assistive Devices
• Must be medically necessary
• Assess function rather than presume inability based on amputation or use of an assistive device
• New lightweight/energy storing materials decrease exertion associated with walking
53

Natural Foot
Energy Storing Foot
Origin of Photographs Unknown
54

1.05D Hemipelvectomy/hip 1.05D Hemipelvectomy/hip disarticulationdisarticulation
• Hemipelvectomy
• Hip disarticulation
55

Prosthesis for Above the Knee Amputation
Origin of Photograph Unknown
56

1.05D - Hemipelvectomy/Disarticulation1.05D - Hemipelvectomy/Disarticulation
• Prosthesis
• Requires walker or two crutches to walk
57

Types of FracturesTypes of Fractures
• Simple: clean break of bone with no open wound
• Comminuted: Bone is broken into small fragments (more serious)
• Compound (Open): external wound leading to the break of a bone
58
Treatment of FracturesTreatment of Fractures
Reduction: realignment and repositioning of a fx
• Closed reduction: manipulation without incision
• Open reduction: manipulation where incision is necessary
• Internal Fixation: repair may require the placement of rods, screws, plates, or other hardware
What is ORIF ?
59

Non-union of a FractureNon-union of a Fracture
• Bones will usually repair within 2 months
• Complications can delay healing and may result in bone deformities
• Duration then is very case specific
60

Ankle subluxationAnkle subluxation
• Bones are shifted out of place
• Ankle after open reduction and internal fixation (ORIF)
• Restored back to normal anatomical relationship
61

Open Dislocation of ankleOpen Dislocation of ankle
• Talus bone out of ankle joint.
• After ORIF of ankle—now talus is located in the joint anatomically (normal)
62

Medically acceptable image—X-ray Medically acceptable image—X-ray ankleankle• Normal ankle joint space—note joint space between tibia and talus
• Note narrowing of joint space between tibia and talus of ankle
63

Limitation of MotionLimitation of Motion
Normal ankle joint range of motion:
•20 degrees extension• •60 degrees flexion
64

Range of MotionRange of Motion
Measurement of Joint Motion(except for the spine)
Use AMA Guides to the Evaluation of Permanent Impairment
for technique & normal values6th edition
65

1.06 – 1.06 – Non union lower extremityNon union lower extremity
Fracture femur, tibia, pelvis, or tarsal bones
WITH
A) No clinically solid union & on AMAI
AND
B) ITAE for at least 12 months
66

1.06 Fracture of femur 1.06 Fracture of femur
67

The FootThe Foot
Tarsals
Metatarsals
Phalanges
Calcaneus or Heel bone
Arch includes tarsals & metatarsals
68

1.07 – 1.07 – Nonunion of an upper Nonunion of an upper extremityextremity
Fracture of the shaft of the humerus, radius or ulna
Nonunion
Under continuous surgical management towards
restoration of functional use
Such function not restored within 12 months of onset
69

1.07 – 1.07 – Nonunion of an upper Nonunion of an upper extremityextremity
Under continuous surgical management:
Surgical procedures and associated treatments directed toward the salvage or restoration of functional use of the affected part, including post-surgical procedures, surgical complications, infections, or other medical complications, related illnesses, or related treatments
70

1.08 – 1.08 – Soft tissue injury (Burns)Soft tissue injury (Burns)
Extremities or face and head
Under continuous surgical management towards
restoration of major function
Such function not restored within 12 months of onset
71

1.00 - Major function face and head1.00 - Major function face and head
For purposes of listing 1.08, relates to impact on any or all activities of:
•Vision•Hearing•Speech•Mastication•Initiation of digestive process
72

Diagnosis & EvaluationDiagnosis & Evaluation
Should be supported by:
Applicable detailed description
(ROM, musculature, sensory & reflexes, etc.)
Laboratory findings (x-rays, CT, MRI, bone scans, etc.)
73

Medical ExaminationMedical Examination
• Chief Complaint• Past Medical History• Social History• Family History• Review of Systems• Examination• Lab results• Medications• Diagnosis• Treatment Plan
74
• Must Relate
• Be Based on Objective Observation
• Supported by Alternative Testing Methods
• Over Time if Intermittent
• Consistent with daily activities

Medical ExaminationMedical Examination
Subjective
Objective
Assessment
Plan
Note: Not “his leg is numb”
75
• Must Relate
• Be Based on Objective Observation
• Supported by Alternative Testing Methods
• Over Time if Intermittent
• Consistent with daily activities

Medical ExaminationMedical Examination
Note:
Observations are important: on/off table
Atrophy requires measurements in legs and arms, not hands
Strength grading 0 to 5***
76

AnatomyAnatomy
77
Peripheral Joints & Spine

The Upper ExtremityThe Upper Extremity
• Upper arm – humerus
• Forearm – radius (thumb side) & ulna
• Wrist bones – carpals
• Palm and back of hand – metacarpals
• Fingers – phalanges
78

The Lower ExtremityThe Lower Extremity
Thigh - femur
Hip Joint (femoral
head)Knee cap -
patella
Shin - tibiaFibula
Ankle - tarsals
79

The SpineThe Spine
Cervical
Thoracic spine(T1 – T12)
Lumbar spine(L1 – L5)
Sacrum (S1–S5)
Coccyx
Anterior Left Lateral
80

The PelvisThe Pelvis
Ilium (part of the pelvis) – lay term for hips
Iliac crest
Acetabulum(hip fits here)
Sacrum
81

JointsJoints
• Movable joints are held together with ligaments
• Contain synovial fluid for lubrication
• Pelvis joints flex slightly, but no true movement
• Some joints have no movement at all
82

LigamentsLigaments
• Bind bones together
• Flexible, but do not stretch
• Can deteriorate w/ age, etc.
• They can tear or fray
83

TendonsTendons
• Similar to ligaments, but…
• Attach muscles to bones
• Can deteriorate w/ age, etc.
• Can also tear
:
84

CartilageCartilage
• Fibrous connective tissue found throughout the body• Joints• Nose
• Ears
• Usually found at ends of long bones to provide smooth surface for articulation
85
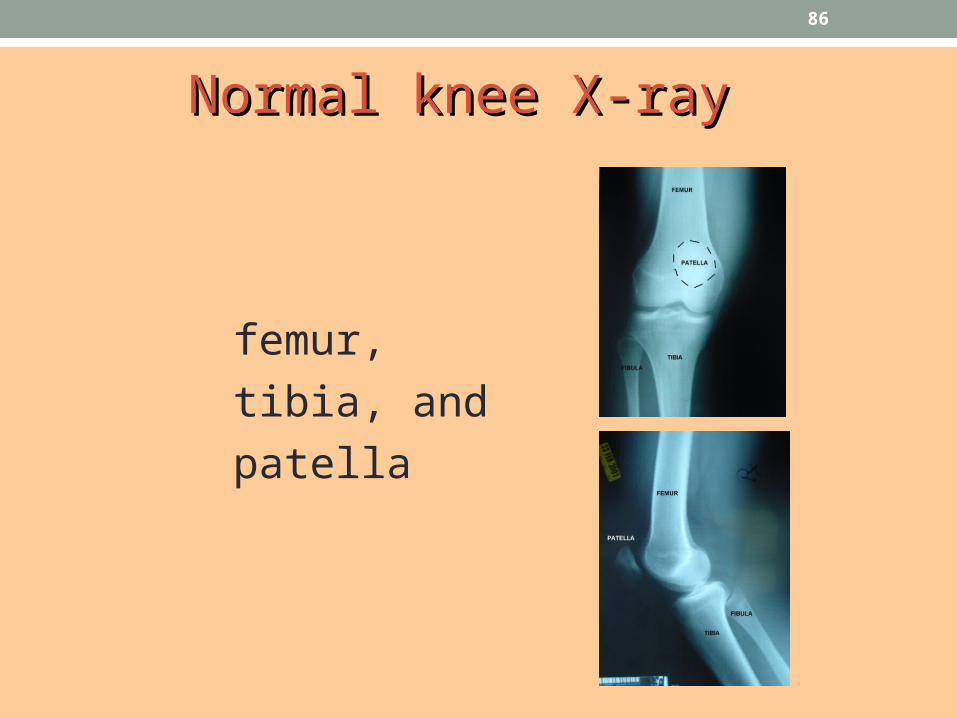
Normal knee X-ray Normal knee X-ray
femur,
tibia, and
patella
86

Dislocation of knee joint Dislocation of knee joint
• X-ray knee located
• X-ray knee dislocated
87

Major dysfunction of joint KneeMajor dysfunction of joint Knee
• X-ray right knee with normal joint space
• X-ray right knee with decreased joint space, especially medially
88

Major dysfunction of joint KneeMajor dysfunction of joint Knee
• Knee joint osteoarthritis with joint space narrowing
• After total knee replacement
89

Major Dysfunction of the Hip JointMajor Dysfunction of the Hip Joint
Normal hip joint
90

http://www.njsrlaserspine.com/Portals/16887/images/fibromyalgia_s7.jpg
* Pain* Pain91

* Pain* Pain
•May be an important contributor to functional loss
•Must be associated with medical signs or laboratory findings that could reasonably be expected to produce the pain or other symptom
•Intensity of pain may vary from mild to severe
•We must evaluate the intensity and persistence of the symptom(s)
92

Chronic Pain - What is it?Chronic Pain - What is it?
• Pain that continues beyond the point of expected tissue healing
• Sometimes, there is no clearly identifiable pain generator that explains the pain.
93

Chronic Pain – ExamplesChronic Pain – Examples
• Chronic low back pain
• Fibromyalgia (SSR 14-1p)
• Chronic Fatigue Syndrome (SSR 14-1p)
• Complex Regional Pain Syndrome (CRPS, aka Reflex Sympathetic Dystrophy – RSD; SSR 03-2p)
94

Common Causes of Chronic Back Common Causes of Chronic Back PainPain
• Osteoarthritis • Osteophytes or spurs• Degenerative Disk Disease• Nerve root or cord involvement- e.g. sciatica• Ankylosing spondylitis (14.00)
95

Other Examples of Diagnoses & Other Examples of Diagnoses & Conditions Related to Pain Conditions Related to Pain
• Bursitis – Trochanteric, etc.• Spina Bifida (myelomeningocele)• Scoliosis• Sacroillitis• Compression fractures• Plantar fasciitis
96
Chronic Pain – MedicationChronic Pain – Medication
Patients have variable tolerance to medication side effects.
Use or non-use of medication, per se, does not validate or invalidate pain symptoms
97

Chronic Pain - Putting it all Chronic Pain - Putting it all TogetherTogether
• Establish a MDI based on signs, symptoms and lab findings
• Evaluate for consistency of the MER, both internally, and with ADLs and third party reports
98

OsteoarthritisOsteoarthritis
• Most common cause of joint dysfunction
• Begins as a disintegration of cartilage
• Usually has an inflammatory component
• When cartilage wears away, the bone is exposed, leading to pain with movement
• Excess weight, smoking, injury, and physical strain predispose, but not required
99

Documentation of ArthritisDocumentation of Arthritis
• “Objective” findings (ROM, gait & station, strength testing)
• Imaging studies are necessary
There may be a poor correlation between findings and symptoms
100

Examination of the SpineExamination of the Spine
• Gait
• Range of motion (ROM)?
• Motor and sensory abnormalities
• Muscle spasm
• Deep tendon reflexes (DTRs)
• Straight leg raising (SLR)
• Give way test
101

SLR Sitting and SupineSLR Sitting and Supine
SLR in sitting position is a confirmatory test
•A Positive test
• Aggravates or produces radicular pain symptoms• Low back pain is not considered a positive test
102

SLR Sitting and SupineSLR Sitting and Supine
• Combining both sitting and supine tests is considered a clinical validation sign
• Results must be concordant (both + or -)• Angle of positivity should be approximately =
• Test must be + on same side as pathology, but may be + on opposite side as well
103

Supine Straight Leg RaisingSupine Straight Leg Raising
Courtesy Wikipedia.org
104

Lasegue TestLasegue Test
Courtesy Medscape.com
105

Observations During Observations During the Spinal Examination the Spinal Examination
• On and off the examination table
• Arising from a squatting position
• Atrophy with limb measurements
• Strength (0 to 5, or dynamometer)
106

Non-organic Findings of the SpineNon-organic Findings of the Spine (Waddell’s Signs or Clinical Validation Signs)
• .
•
107

Waddell’s Signs
• Unrelated tenderness • superficial or non-anatomic
• Simulation tests• axial compression or pseudo rotation
• Distraction test e.g. SLR
• Regional disturbances• dysfunction, weakness, or sensory
• Overreaction
108

Axial Compression &Pseudorotation
Photo courtesy of: http://revue.medhyg.ch/art/Images/22913_2.gif
109

Clinical Validation Signs Clinical Validation Signs (aka Waddell’s Signs)(aka Waddell’s Signs)• Interpretation
• Three or more positive signs indicate symptom exaggeration/magnification
• Does not equate to malingering
110

Examination of knee for instabilityExamination of knee for instability
Two tests:
Pulling the tibia forward with respect to the knee shows instability of knee
111

Other Medical SignsOther Medical Signs
112

Clinical Instruments:Clinical Instruments:DynamometerDynamometer
• Measures grip or pinch strength
• Measurements of other muscle groups usually done by physical therapist or physiatrist
Photo courtesy of Pro-Med Products, Inc.
113

Clinical Instruments:Clinical Instruments:GoniometerGoniometer
• Protractor with arms for measuring joint movement
Photo courtesy of Pro-Med Products, Inc.
114
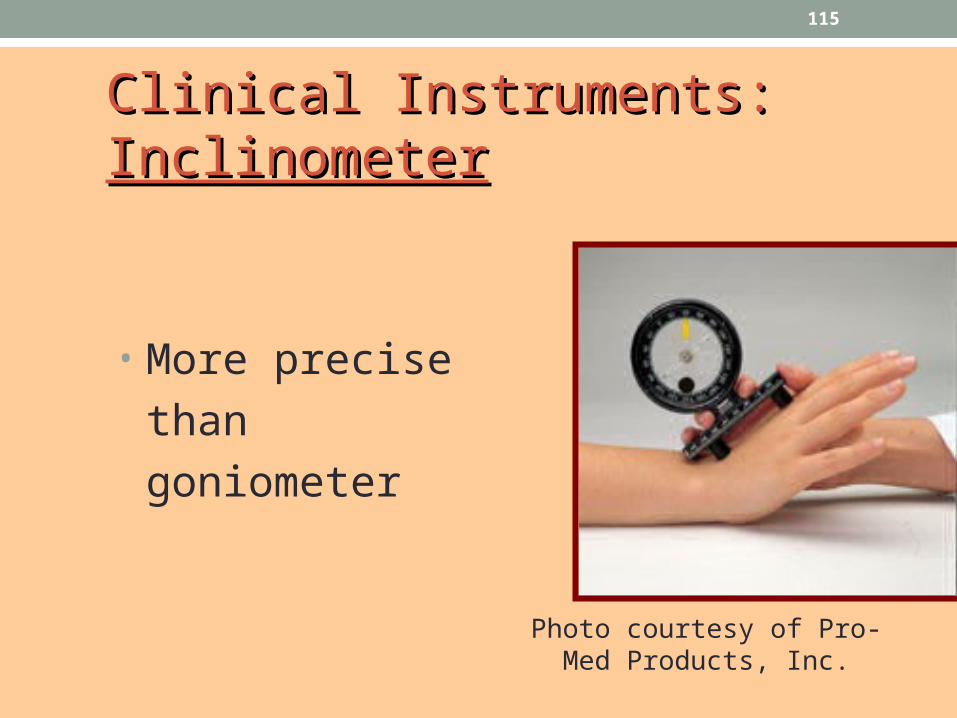
Clinical Instruments:Clinical Instruments:InclinometerInclinometer
• More precise
than goniometer
Photo courtesy of Pro-Med Products, Inc.
115

Laboratory Studies –Laboratory Studies –ImagingImaging
116

Laboratory Studies – Laboratory Studies – ElectrodiagnosticElectrodiagnostic
• Nerve conduction• Measures electrical impulse velocity along a nerve
• Electromyography (EMGs)• Records activity of skeletal muscles
117

ReminderReminder: Rheumatoid and : Rheumatoid and Inflammatory Arthritis Are Evaluated Inflammatory Arthritis Are Evaluated Under the Immune System ListingUnder the Immune System Listing
• Includes not just rheumatoid arthritis, but all forms of inflammatory arthritis.
• Functional consequences of joint inflammation are more important than specific diagnosis.
118

More information?More information?
Office of Learning on the Intranet
• Click on “Entry Level Training”
• Click on “Disability Examiner”
• Click on “Disability Examiner Basic Training Course”
• Double-click “Unit 4” folder• Musculoskeletal is the first body system
119

Other Other IntraIntranet Resourcesnet Resources
• Digital Library (intranet homepage)
• Click on “Medical”• Select an online reference
120
Internet Resourcesnet Resources
• National Library of Medicine (www.nlm.nih.gov)
• National Institutes of Health (www.nih.gov)
• CDC (www.cdc.gov)
• Mayo Clinic, Johns Hopkins, Cleveland Clinic
• Major Professional Society web sites
• WebMD, Medscape, eMedicine (careful!)
121

Article ResourcesArticle Resources
• PubMed (www.ncbi.nlm.nih.gov)
• Google (http://scholar.google.com)
122

Traditional (paper) ResourcesTraditional (paper) Resources
• AMA, Guides to the Evaluation of Permanent Impairment, 6th edition
• Presley Reed, MD, The Medical Disability Advisor, 5th edition• www.mdguidelines.com
• Both available in electronic format
123

Questions?
124