the lpn - afscme · lpn employment trends ... nursing staff that followed ... and their staff about...
TRANSCRIPT

The LPN: A Practical Wayto Alleviate the
Nursing ShortageBy
Gordon Lafer, Ph.D.
and Helen Moss, M.A.
Labor Education and
Research Center
University of Oregon
A Report Prepared for the United Nurses of America,AFSCME, AFL-CIO
May 2007

By
Gordon Lafer, Ph.D.
and Helen Moss, M.A.
Labor Education and
Research Center
University of Oregon
By
Gordon Lafer, Ph.D.
and Helen Moss, M.A.
Labor Education and
Research Center
University of Oregon
A Report Prepared for the United Nurses of America,AFSCME, AFL-CIO
May 2007
The LPN: A Practical Wayto Alleviate the
Nursing Shortage


Table of ContentsExecutive Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Introduction: Who are LPNs? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Typical Duties of an LPN . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11 Professional Training and Qualifications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12 LPN Scope of Practice . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12 Employer Restrictions on LPN Scope of Practice . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .13
LPN Employment Trends . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
LPN Earnings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14 LPNs by the Numbers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15 Graduates from Foreign Nursing Programs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .18 The Disappearing Hospital LPN . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .18 Trends in Work Organization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .19 Managed Care, Cost Containment and Workforce Cuts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .20 LPN Cutbacks Lead to Poor Job Conditions for RNs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .20 The Impact of Cuts on Patient Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .21 Fixing the Problem: Bring Back the LPNs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .21 Examples of Successful Models . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .22 Summary of Best Practices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
Recruitment and Retention of Hospital LPNs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .23
Recouping LPNs Who Have Left the Health Care Field . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .23 Recruiting New LPNs: Innovative Training Programs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .23 Magnet Hospitals: A Good Idea that has Gone Astray . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .26 Giving Nurses a Voice: Unionization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .27
Conclusions and Recommendations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .28
The Next Steps . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
Appendix . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
State Scope of Practice Restrictiveness Scale Scores (Table 9a) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .31 State Scope of Practice Specificity Scale Scores (Table 9b) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .31 LPN Scopes of Practice (Table 10) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .32 Sources . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36 Endnotes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38


Executive Summary 7
Across the country, hospitals face a shortage of nursing staff . Many hospital executives report difficulty recruiting sufficient numbers of nurses . Over the next 15 years – as the baby boom generation ages and increasing numbers of nurses themselves near retirement – the demand for nurses is projected to significantly outstrip supply .
In the face of such a potential crisis, hospitals have failed to make use of a readily available and highly qualified workforce: licensed practical nurses (LPNs) . For a variety of reasons, hospitals have cut back their LPN staff at exactly the time that bedside caregivers are in short supply . To address the nation’s nursing needs and, with the aim of guaranteeing the highest quality of cost-effective patient care, hospitals must look to re-integrating LPNs as a critical component of nursing staff .
Who are LPNs?
There are currently over 700,000 licensed practical nurses employed in the United States, 25 percent of whom work in hospitals . Like RNs, LPNs are licensed professionals, and in non-intensive settings RNs and LPNs often fill the same role . In acute care hospitals, LPNs care for the sick, injured, convales-cent and disabled under the direction of physicians and RNs . In the course of this work, they perform a remarkably wide range of duties . Typically, their responsibilities include basic bedside care (such as taking vital signs), preparing and administering injections, monitoring catheters, applying dressings, treating bedsores and giving special bed care such as alcohol rubs or massages . LPNs are charged with monitoring patients and reporting adverse reactions to medications or treatments . They collect samples for testing, perform routine laboratory tests, feed patients, and record food and fluid intake and out-
put . They assist with bathing, dressing and personal hygiene . They treat wounds and, where state law allows, give medications and perform venipuncture . In most states, LPNs give intravenous (IV) medica-tions, hang blood, and perform other duties of care in keeping with their training and certification .
The duties that an LPN can legally perform are gov-erned by state statute or regulation . Each state’s “scope of practice” defines the parameters within which LPNs are legally authorized to work .1 All states allow LPNs to perform the basic nursing duties associ-ated with bedside care, but beyond that point state rules vary considerably . Most state boards of nursing allow for IV infusions, IV medications or hemodi-alysis if LPNs have undergone additional education and certification, although there is variation among state rules for each of these duties . In most states, LPNs don’t independently develop or make changes in the plan of care or perform telephone triage .2
The Decline of LPN Employment in Hospitals
In the past 20 years, the number of LPNs working in hospitals has plummeted . Between 1984 and 2005 (the last year for which data is available), the number of LPNs employed in hospitals fell by 153,000, or 47 percent, even while the total number of LPNs in the country grew by 18 percent .3,4 This falloff pri-marily results from two factors: the general cuts in nursing staff that followed the adoption of managed care and capitated insurance plans in the 1990s; and a more specific shift from “team nursing” to “pri-mary care” as the dominant model of nurse staffing within the hospital industry . As is discussed in this report, each of these decisions is understandable in its historic context . But taken together, they have left hospitals without access to a critical workforce .
Executive Summary
NOTE: In Texas and California, licensed practical nurses are known as licensed vocational nurses. For the purpose of this report, when the term LPN is used, it will include LVNs unless otherwise specified.
Bring Back the LPNs
Hospitals need qualified, experienced bedside caregivers – RNs, LPNs and aides . The combina-tion of LPNs’ education, skills, commitment and diversity enable them to make a vital contribu-tion to hospital care . LPNs who are utilized to their full scope of practice are highly qualified, cost-effective members of the nursing team .
Hospitals are scrambling to staff units, and RNs are struggling to provide professional care and avoid burnout in the face of severely strained patient-to-nurse ratios . If hospitals redesign their work processes to make greater use of LPNs, there is a ready popula-tion to meet the immediate demand for skilled and qualified nurses: LPNs who are not currently working in the occupation for which they trained . Evidence suggests that many LPNs view hospitals as the most desirable employer due to the combination of higher pay and more exciting work than in other health care settings .5 If there were more positions available in hos-pitals, some of these LPNs might return to practice .
Bring Back Effective Teams
For both immediate and longer-term staffing needs, it is time for hospitals to reconsider LPNs and models of team nursing as a strategy to meet their nursing needs . Primary care may be the appropriate staffing model for certain situations, but its advantages become less meaningful if nurses don’t have enough time to spend with the patient due to staffing shortages .
Indeed, it is possible to combine elements of both models in a manner that allows hospitals to make use of LPNs while retaining many of the beneficial aspects of primary care nursing . Sonia Moseley, a registered nurse practitioner and AFSCME member in California, advocates the use of team nursing, because otherwise “[T]he RN is unable to fully practice to her entire scope of practice if time is spent doing things that others are qualified to do .” In cases where unions have bargained staffing ratios for RNs, they have found it necessary to guarantee that other nurs-ing staff are not cut as a result, leaving RNs hope-lessly overworked . Tom Connelly, an RN and
8 The LPN: A Practical Way to Alleviate the Nursing Shortage

Executive Summary 9
president of AFSCME Local 2026 (Ohio Council 8), negotiated a minimum staffing agreement for RNs, but had to make sure that the LPNs and ancillary staff were not being cut to fund the RNs .
Recommendations
To allow LPNs to make the fullest possible contribution to patient care, and to allow hospitals to effectively meet ongoing staffing needs, a few key principles are critical .
• Hospitals can and should increase their employ-ment of LPNs while instituting practices that enable LPNs, RNs and other members of the nursing staff to function as an effective team .
• Hospital administrators should educate themselves and their staff about the LPN scope of practice in their state . While LPNs cannot substitute for RNs, they can be utilized to their full scope of practice, thus adding a highly qualified, cost-effective member to the nursing team .
• Hospitals need to work with other stakeholders to increase the number of accessible LPN programs in order to increase the number of new LPNs .
• Nurses scope of practice, standards of practice and curriculum for training programs need to be standardized at a national level, in accordance with the recommendations of the National Association for Practical Nurse Education and Service Inc . (NAPNES) .
• Research is needed on LPNs in the acute setting, including the factors driving LPNs to leave hospital
nursing jobs, as well as new models of nursing that integrate RNs, LPNs and aides into effective teams .
• Nursing staff working at the bedside should have a voice in the decisions that affect them, including appropriate staffing levels and mix .
Such a process should include:
- Creating appropriate job descriptions for LPNs, including any specialty experience needed, and making sure that the job description is clearly communicated to all current staff to prevent role confusion .
- Developing a unit-specific curriculum for training LPNs to work to the full extent of their authority .
- Developing and implementing an orientation and mentoring plan for LPNs .
• While the plan is being developed and implemented, it is critical to establish effective communication structures between management, RNs and LPNs .
• RNs must be trained in leadership skills, and RN programs need to include these skills in the curriculum .
• To make the transition succeed, it is important that hospitals provide additional compensation for mentors, as well as for LPNs who upgrade skills and take on expanded duties .
These recommendations will put the hospital industry in a much stronger position to address nursing shortages and to guarantee the highest quality of patient care .


Introduction: Who are LPNs? 11
If you ask most patients who took care of them while they were in the hospital, they will likely say a “nurse .” It is natural to think of the people who bathe you, feed you, get you out of bed, take your vital signs and bring you medicine as part of a single category . In fact, however, hospital nursing staffs are composed of several distinct occupations, gen-erally including registered nurses (RNs), licensed practical nurses (LPNs), certified nurse assistants (CNAs) and orderlies . Figuring out the appropri-ate mix of these occupations within the nursing workforce is one of the most important policy deci-sions currently facing hospital administrators .
Most of the attention and research in hospitals has focused on RNs, thus overlooking the contri-bution of LPNs . While the training and licens-ing of LPNs does not allow them to perform all of the same duties as RNs, their work is critical in guaranteeing that patients receive proper medi-cal treatment and bedside care . With appropriate planning, training and oversight, the delegation of certain responsibilities to LPNs can free up RNs to work to their full scope of practice .
Within the hospital, LPNs may work in just about every setting, including operating rooms, nurser-ies, labor and delivery, medical/surgical units, cardiac and intensive care units, rehabilitation units and emergency rooms .6 Hospital administra-tors report that experienced, long-tenured LPNs are highly valued in their units . Their education and experience make them both highly skilled and highly trusted by RNs and nursing managers .7
Typical Duties of an LPN
LPNs care for the sick, injured, convalescent and disabled under the direction of physicians and RNs . In the course of this work, they perform a remarkably
wide range of duties . Typically, their responsibilities include basic bedside care (such as taking vital signs), preparing and administering injections, monitoring catheters, applying dressings, treating bedsores and giving special bed care such as alcohol rubs or massages . LPNs are charged with monitoring patients and reporting adverse reactions to medications or treatments . They collect samples for testing, perform routine laboratory tests, feed patients, and record food and fluid intake and output . They assist with bathing, dressing and personal hygiene . They treat wounds and, where state law allows, give medications and perform venipuncture . In most states, LPNs give intravenous medications, hang blood, and perform other higher levels of care in keeping with their training and certification .
Both LPNs and RNs are licensed nurses, and in non-intensive settings RNs and LPNs often fill the same role . In a survey done by the National Council of State Boards of Nursing (NCSBN) in 2003, nurses in their first six to 18 months of practice and the nurses’ employers were asked about the working relationships of RNs and LPNs in the work setting . Of those responding, 39 percent of employers, 52 percent of LPNs and 62 percent of the RNs wrote that RNs and LPNs in their workplace held the same role and performed the same work or that their roles were the same except for specific activities that the RN performed such as admitting assessments or IV medications .8,9 Indeed, an experienced LPN will often mentor new RN graduates . Glenn McGarvey, an RN who belongs to Connecticut Health Care Associates/AFSCME, comments that when he was an RN nursing student, he had, at the most, two patients at a time . When he began to work as a gradu-ate nurse, “[I]t was the three LPNs on the orthopedic unit where I worked who taught me the most about effectively taking care of up to 19 patients at the same time . I can’t say enough about how helpful the
Introduction: Who are LPNs?
LPNs were in teaching me about caring for patients and organizing my time .” Diana Mason, editor-in-chief of the American Journal of Nursing, likewise described how she was mentored by a superbly quali-fied LPN when she was a newly graduated RN .10
Professional Training and Qualifications
LPNs undergo a rigorous education and training process – usually lasting 12-18 months – before being licensed . Then the LPNs are required to com-plete a state-approved practical nursing program and pass a licensing examination: the National Council Licensure Examination-Practical Nurse (NCLEX-PN) . LPN programs combine classroom study with clinical practice, the latter typically located in a hospital . The standard LPN curriculum includes basic nursing concepts and anatomy, physiology, medi-cal-surgical nursing, pediatrics, obstetrics, psychiatric nursing, the administration of drugs, nutrition and first aid . Most states have additional educational requirements for LPN certification in advanced skills such as phlebotomy, IV infusion and IV medica-tion administration .11 In 2003, 65 percent of newly graduated LPNs reported earning additional certifi-cation or completing coursework since graduation .
Even after being licensed, many state boards of nurs-ing require LPNs to enroll in annual continuing education (CE) courses in order to maintain their licenses .12 Similarly, 24 state boards require LPNs to take a refresher course if they have an inactive license and wish to return to practice . A 2003 sur-vey by the National Council of the State Boards of Nursing (NCSBN) showed that the LPNs completed an average of 28 hours of CE per year, including LPNs from states where CE is not legally required .13
LPN training is available in about 1,100 state-approved programs in vocational or technical schools, community colleges and in a few cases, high schools . Some of these programs are “stand-alone” LPN pro-grams, where the LPN license is the goal . In other programs, a student may take the LPN exam and work as an LPN after completing the first year of an
RN program . These programs are sometimes called “ladder” programs . There are advantages and disad-vantages to both types of programs . A ladder program will usually have the same prerequisites as an RN program, and these prerequisites can take up to a year to complete . A stand-alone program will usually have fewer prerequisites . This makes it easier to recruit can-didates, but there may be problems transferring cred-its if the LPN wishes to become an RN at a later date .
Many “hands-on” aspects of nursing are taught in LPN programs . Dave Miller, a nurse practitioner from AFSCME Council 62 in Indiana, believes that he learned more about being a nurse in the LPN program than in any other part of his education: “In the LPN program it was one day of class and four days of clinical experience, and in the RN program that was reversed .”
LPN Scope of Practice
The duties that an LPN can legally perform are governed by state statute or regulation . Each state’s scope of practice defines the parameters within which LPNs are legally authorized to work .14
LPNs generally must work with an RN or a physi-cian . All states allow LPNs to perform the basic nursing duties associated with bedside care, but beyond that point state rules vary considerably . Most state boards allow for IV infusions, IV medications or hemodialysis if LPNs have undergone additional education and certification, although there is varia-tion among state boards’ rules governing each of these duties . In most states LPNs don’t indepen-dently develop the plan of care, make changes in the plan of care or perform telephone triage .15
Some state boards provide general guidelines for LPNs’ scope of practice, while others are very specific . A comprehensive review of state policies shows, for example, that Louisiana, Maine, Montana and Nevada all use detailed lists of allowable LPN duties, while Michigan and Texas have no specific legislation whatsoever defining LPN practice .16 In other cases, states mandate a methodology for assigning LPN
12 The LPN: A Practical Way to Alleviate the Nursing Shortage

Introduction: Who are LPNs? 13
duties, rather than enumerating specific tasks . Thus, Alaska, Georgia, Kentucky and Oklahoma have “decision trees” to determine what tasks may appropriately be delegated to LPNs . Colorado and Nebraska use the nursing care plan structure (goals, assessment, planning, intervention and evaluation) to decide what tasks can be delegated . In some jurisdictions, it is the RN scope of practice that dictates what LPNs may do, by limiting which RN tasks may be legally delegated to someone else .
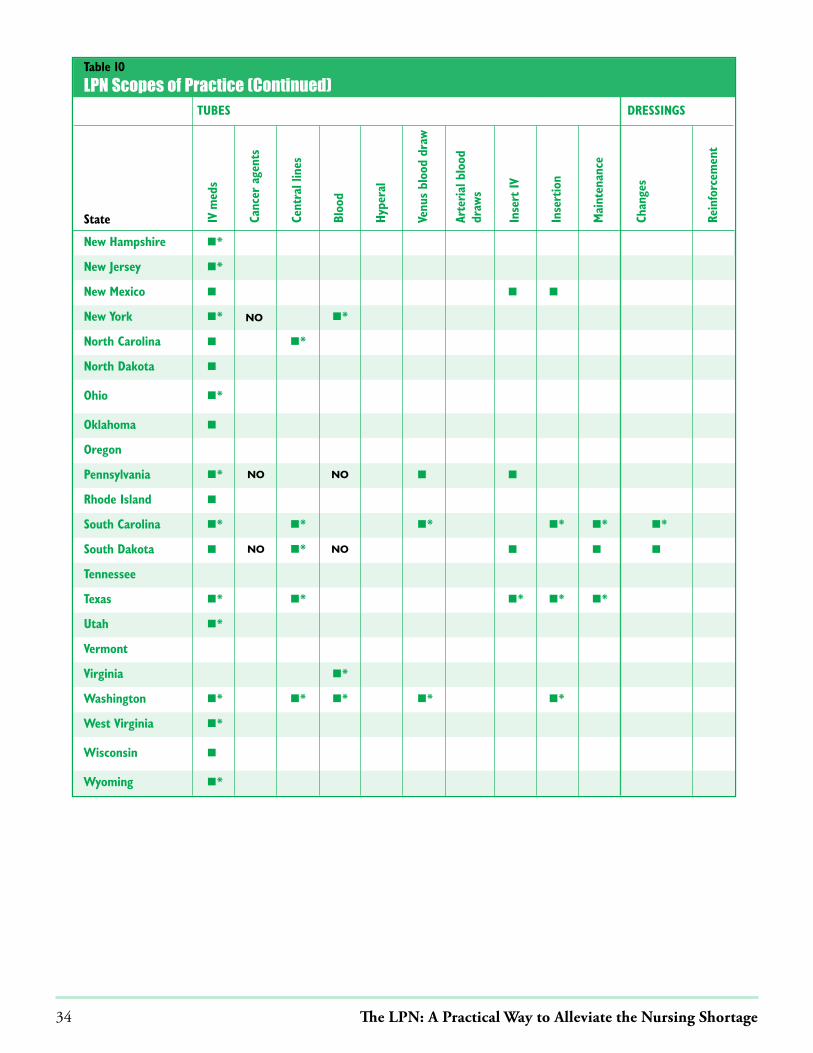
Thus, state statute, regulation, specific lists of duties, “decision tree” principles or the judgment of other health professionals variously define LPN respon-sibilities (Tables 9 and 10 in Appendix A, from the Bureau of Health Professions Report, summarize the major features of the scope of practice from each state, and rate each state on both the specificity and restrictiveness of the scope .) Unfortunately, the restrictions of some of these systems – together with the confusion created by multiple, diverse definitions of LPNs’ scope of practice – has unnecessarily lim-ited the contribution that LPNs can make to patient care and the extent to which hospitals may rely on LPNs as a critical part of the nursing workforce .17
In an interview in January 2007, Patrick Mahan, the executive director of the National Association for Practical Nurse Education and Service (NAPNES), pointed out the need for more evidence-based infor-mation before imposing limits on LPN practice . NAPNES is currently working with a team of nurs-ing experts to develop an updated recommended standard of practice for LPNs performing in acute care . According to Mahan, “there are 56 state boards of nursing and 56 standards of practice – if each state writes a laundry list of what a LPN can and cannot do the practice will stagnate, and that is not good for the medical community or the public .”
The NCSBN endorses standardizing practical nurse education and scope of practice . In its 2004 “Practical
Nurse Scope of Practice White Paper,” the NCSBN recommends:
• Developing initiatives to enhance the mobility of practical nurses by establishing statewide articulation programs .
• Establishing a national practical nurse curriculum .
• Decreasing the wide disparity in the Nurse Practice Acts regarding the practical nurse scope of practice .
• Developing a national clearinghouse for practical nurse data .
• Providing education to all health care workers about the LPN scope of practice .
• Conducting more research on the practical nurse scope of practice .18
All of these recommendations would help LPNs become a more integral part of the nurse workforce .
Employer Restrictions on LPN Scope of Practice
While state regulations establish the basic parameters of LPN practice, many employers have established policies that restrict LPN duties even further .19 For example, Pam Shelton, an LPN who belongs to AFSCME Ohio Council 8, reports that until 11 years ago LPNs at her hospital regularly distributed medications, a duty well within that state’s scope of practice . One day the hospital changed its policy, prohibiting LPNs from distributing medications . In this case the LPNs took action, standing together to fight this erosion of their practice, and the medica-tions duty was ultimately restored to LPNs . Their union also negotiated an agreement with the employer to continue expanding LPN duties within the state scope of practice . However, in many hospitals – par-ticularly where LPNs have no union through which to represent their concerns – LPNs are underutilized and unnecessarily restricted . In light of the national nursing shortage, such policies must be re-examined .

LPN Earnings
In 2004, the median annual earnings for an LPN employed in a hospital was $32,570, compared with $53,450 for RNs .20 Median annual earnings in the industries employing the largest numbers of licensed nurses in May 2004 are compared in Table 1 and the hourly earnings of caregivers are compared in Table 2 .
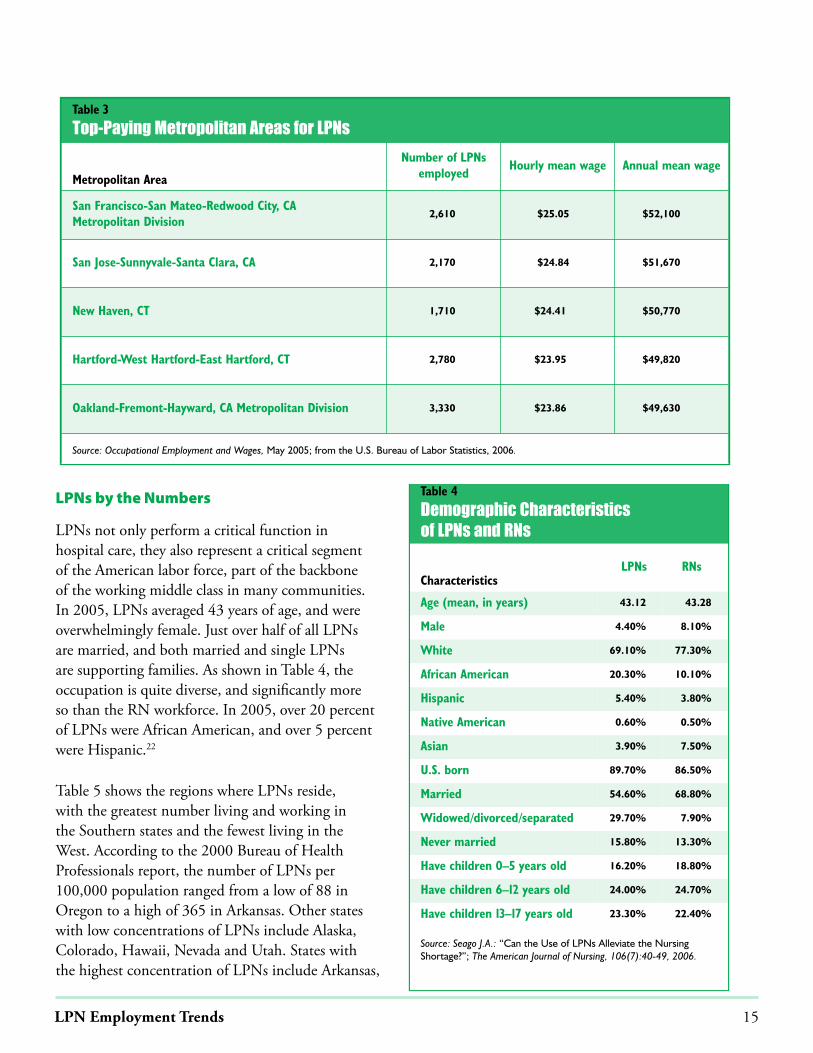
LPN earnings vary substantially by region . LPN wages average $13 .53 an hour in Mississippi but range to $23 .67 per hour in Connecticut . Table 3 compares LPN wages in various metropolitan areas . It appears likely that unionization is one of the major factors contributing to higher wages for LPNs . States that have high union density for hospital nurses – Alaska, California, Hawaii, Massachusetts, Minnesota, Montana, New York, Oregon, Rhode Island and Washington – also provide higher LPN wages . Nationally, nurses with a union earned 13 percent more than their non-union counterparts .21
Table 2
Median Hourly Earnings of the Largest Occupations in Health Services, May 2004
Occupation
Ambulatory healthcare services
HospitalsNursing and
residential carefacilities
All industries
Registered nurses $23.69 $25.66 $22.93 $25.16
Licensed practical and licensed vocational nurses
$15.59 $15.71 $16.95 $16.33
Nursing aides, orderlies and attendants $9.82 $10.43 $9.78 $10.09
Home health aides $8.58 $9.69 $8.84 $8.81
Personal and home care aides $7.05 $8.54 $8.85 $8.12
Source: Occupational Outlook Handbook; from the U.S. Department of Labor, 2006.
Table 1
LPN and RPN Median Wages, May 2004
LPN Median Wages
Employment services $41,550
Nursing care facilities $35,460
Home health care services $35,180
General medical and surgical hospitals $32,570
Offices of physicians $30,400
RN Median Wages
Employment services $63,170
Nursing care facilities $48,220
Home health care services $48,990
General medical and surgical hospitals $53,450
Offices of physicians $48,250
Source: Occupational Outlook Handbook; from the U.S. Department ofLabor, 2006.
LPN Employment Trends
14 The LPN: A Practical Way to Alleviate the Nursing Shortage
LPN Employment Trends 15
Table 3
Top-Paying Metropolitan Areas for LPNs
Metropolitan Area
Number of LPNsemployed
Hourly mean wage Annual mean wage
San Francisco-San Mateo-Redwood City, CA Metropolitan Division
2,610 $25.05 $52,100
San Jose-Sunnyvale-Santa Clara, CA 2,170 $24.84 $51,670
New Haven, CT 1,710 $24.41 $50,770
Hartford-West Hartford-East Hartford, CT 2,780 $23.95 $49,820
Oakland-Fremont-Hayward, CA Metropolitan Division 3,330 $23.86 $49,630
Source: Occupational Employment and Wages, May 2005; from the U.S. Bureau of Labor Statistics, 2006.
LPNs by the Numbers
LPNs not only perform a critical function in hospital care, they also represent a critical segment of the American labor force, part of the backbone of the working middle class in many communities . In 2005, LPNs averaged 43 years of age, and were overwhelmingly female . Just over half of all LPNs are married, and both married and single LPNs are supporting families . As shown in Table 4, the occupation is quite diverse, and significantly more so than the RN workforce . In 2005, over 20 percent of LPNs were African American, and over 5 percent were Hispanic .22
Table 5 shows the regions where LPNs reside, with the greatest number living and working in the Southern states and the fewest living in the West . According to the 2000 Bureau of Health Professionals report, the number of LPNs per 100,000 population ranged from a low of 88 in Oregon to a high of 365 in Arkansas . Other states with low concentrations of LPNs include Alaska, Colorado, Hawaii, Nevada and Utah . States with the highest concentration of LPNs include Arkansas,
Table 4
Demographic Characteristics of LPNs and RNs
CharacteristicsLPNs RNs
Age (mean, in years) 43.12 43.28
Male 4.40% 8.10%
White 69.10% 77.30%
African American 20.30% 10.10%
Hispanic 5.40% 3.80%
Native American 0.60% 0.50%
Asian 3.90% 7.50%
U.S. born 89.70% 86.50%
Married 54.60% 68.80%
Widowed/divorced/separated 29.70% 7.90%
Never married 15.80% 13.30%
Have children 0–5 years old 16.20% 18.80%
Have children 6–12 years old 24.00% 24.70%
Have children 13–17 years old 23.30% 22.40%
Source: Seago J.A.: “Can the Use of LPNs Alleviate the NursingShortage?”; The American Journal of Nursing, 106(7):40-49, 2006.

Table 5
Regional Distribution of LPNs
LPNs and RNs per 100,000 Population
State
Estimated number ofLPNs per 100,000
population
State rank –LPNs per 100,000
population
Estimated number ofRNs per 100,000
population
State rank –RNs per 100,000
population
Alabama 303.6 7 852.1 24
Alaska 90.0 50 793.5 33
Arizona 134.2 45 664.2 45
Arkansas 365.3 1 772.3 35
California 135.9 43 596.8 49
Colorado 118.8 48 716.8 41
Connecticut 187.0 31 977.1 8
Delaware 179.9 33 964.5 9
District of Columbia 161.9 40 303.6 51
Florida 234.8 20 801.4 32
Georgia 223.4 22 717.1 40
Hawaii 129.5 46 709.8 42
Idaho 194.7 28 641.0 47
Illinois 166.8 39 861.1 22
Indiana 245.0 15 867.2 21
Iowa 210.7 26 998.6 3
Kansas 237.9 19 947.0 13
Kentucky 243.4 17 858.3 23
Louisiana 324.6 3 760.1 37
Maine 176.9 35 952.0 12
Maryland 175.7 36 935.7 15
Massachusetts 190.9 30 1,099.0 1
Michigan 182.4 32 803.8 31
Minnesota 321.8 4 954.7 11
Mississippi 307.2 6 824.0 27
Missouri 274.2 11 878.3 20
Montana 213.6 23 805.9 30
Nebraska 290.7 10 943.0 14
Nevada 102.3 49 568.9 50
New Hampshire 172.9 38 1,059.3 2
New Jersey 179.2 34 880.4 19
New Mexico 145.2 42 672.0 44
New York 213.4 24 883.0 18
North Carolina 192.6 29 849.8 25
16 The LPN: A Practical Way to Alleviate the Nursing Shortage

LPN Employment Trends 17
Louisiana, Minnesota, Mississippi, Oklahoma and West Virginia .23
The national level data doesn’t always capture the demographic reality in specific regions . Depending on the location, the makeup of the LPN workforce can be significantly more diverse . For example, South Carolina reported that in 2003, 30 .5 percent of the state’s 9,307 LPNs were African American, 10 percentage points above the national average .24
Diversity also varies significantly based on LPNs’ employment setting . In public hospitals, 64 percent of the LPNs are racial or ethnic minorities, with African Americans accounting for almost half the LPNs working in public hospitals .25 The Veterans Health Administration (VHA) likewise has a more diverse
nurse workforce than the national average . The VHA is the largest employer of nurses in the world, with a total of over 60,000 RNs, advanced practice nurses, LPNs and nursing assistants . African Americans make up almost 15 percent of the VHA nursing ranks .26
Having a more diverse nursing population is impor-tant . Research shows that racial and ethnic minorities are more likely to serve under-represented commu-nities than their white cohorts, and patients prefer to see a health professional of their own racial or ethnic background .27 In addition, minority provid-ers can help bridge cultural and language gaps . There is a need for a more diverse workforce throughout health care, but LPN programs, especially those that consider the needs of working people, can be a way to attract members of underserved communi-
Table 5
Regional Distribution of LPNs (continued)
State
Estimated number of LPNs per 100,000
population
State rank –LPNs per 100,000
population
Estimated number ofRNs per 100,000
population
State rank –RNs per 100,000
population
North Dakota 315.9 5 992.9 6
Ohio 263.7 14 914.7 16
Oklahoma 333.2 2 706.9 43
Oregon 87.6 51 725.7 39
Pennsylvania 266.9 12 988.8 7
Rhode Island 174.7 37 997.5 5
South Carolina 244.6 16 811.8 29
South Dakota 211.7 25 997.8 4
Tennessee 298.5 9 821.5 28
Texas 232.8 21 653.5 46
Utah 120.1 47 614.8 48
Vermont 265.6 13 958.3 10
Virginia 241.9 18 780.8 34
Washington 159.2 41 769.8 36
West Virginia 302.7 8 846.8 26
Wisconsin 194.7 27 891.2 17
Wyoming 134.6 44 740.8 38
Total U.S. 211.3 n/a 803.7 n/a
Source: Seago J.A., Spetz J., Chapman S., Dyer W., Grumbach K.: Supply, Demand and Use of Licensed Practical Nurses; Bureau of Health Professionals, U.S. Department of Health and Human Services, 2004.
ties to the nursing profession . Over the next 15 years the expectation is that as the demographics of the general population changes, the nurse workforce, including the LPN workforce, will also change .
Graduates from Foreign Nursing Programs
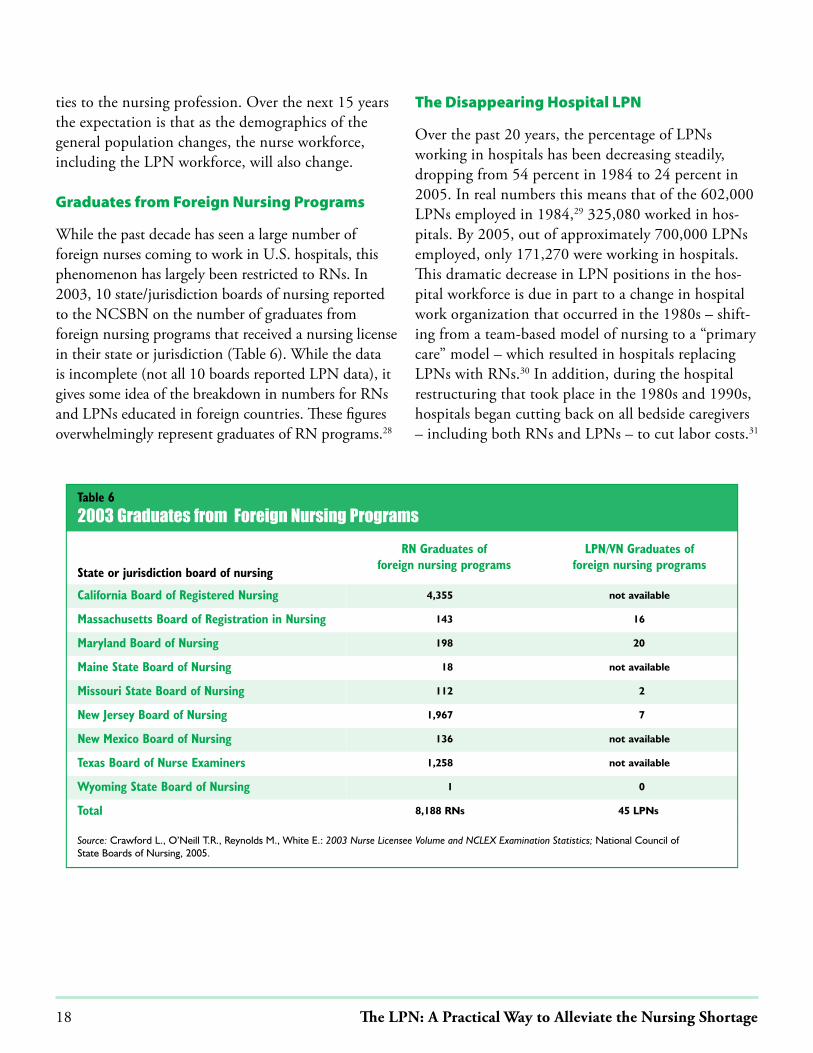
While the past decade has seen a large number of foreign nurses coming to work in U .S . hospitals, this phenomenon has largely been restricted to RNs . In 2003, 10 state/jurisdiction boards of nursing reported to the NCSBN on the number of graduates from foreign nursing programs that received a nursing license in their state or jurisdiction (Table 6) . While the data is incomplete (not all 10 boards reported LPN data), it gives some idea of the breakdown in numbers for RNs and LPNs educated in foreign countries . These figures overwhelmingly represent graduates of RN programs .28
The Disappearing Hospital LPN
Over the past 20 years, the percentage of LPNs working in hospitals has been decreasing steadily, dropping from 54 percent in 1984 to 24 percent in 2005 . In real numbers this means that of the 602,000 LPNs employed in 1984,29 325,080 worked in hos-pitals . By 2005, out of approximately 700,000 LPNs employed, only 171,270 were working in hospitals . This dramatic decrease in LPN positions in the hos-pital workforce is due in part to a change in hospital work organization that occurred in the 1980s – shift-ing from a team-based model of nursing to a “primary care” model – which resulted in hospitals replacing LPNs with RNs .30 In addition, during the hospital restructuring that took place in the 1980s and 1990s, hospitals began cutting back on all bedside caregivers – including both RNs and LPNs – to cut labor costs .31
18 The LPN: A Practical Way to Alleviate the Nursing Shortage
Table 6
2003 Graduates from Foreign Nursing Programs
State or jurisdiction board of nursing
RN Graduates of foreign nursing programs
LPN/VN Graduates of foreign nursing programs
California Board of Registered Nursing 4,355 not available
Massachusetts Board of Registration in Nursing 143 16
Maryland Board of Nursing 198 20
Maine State Board of Nursing 18 not available
Missouri State Board of Nursing 112 2
New Jersey Board of Nursing 1,967 7
New Mexico Board of Nursing 136 not available
Texas Board of Nurse Examiners 1,258 not available
Wyoming State Board of Nursing 1 0
Total 8,188 RNs 45 LPNs
Source: Crawford L., O’Neill T.R., Reynolds M., White E.: 2003 Nurse Licensee Volume and NCLEX Examination Statistics; National Council of State Boards of Nursing, 2005.

LPN Employment Trends 19
Trends in Work Organization
The decline in LPN employment in hospitals over the last two decades has been largely driven by two factors: a shift from “team nursing” to “primary care” as the dominant model for hospital nursing practice, and the broader cuts in hospital staff that were occasioned by the rise of managed care and similar forms of capitated health insurance . As described later, each of these trends was understandable in its time . However, they have resulted in the under-utilization of LPNs at the exact moment when nursing staffs are more thinly stretched than ever and the contribution of LPNs is most urgently needed .
During the 1950s and 1960s, nursing services were predominantly organized on a team model: a team that included RNs, LPNs and aides – each performing the function for which they were best suited – cared for an individual patient . Under this model, RNs generally conducted patient assessments and provided medications and other medical treatments, while LPNs and aides attended to personal hygiene, turning and moving patients, and other care .32 Employees in each occupation carried out the full range of duties that they were trained (and legally authorized) to perform . RNs led the team of LPNs and aides, and
retained overall responsibilities for guaranteeing the quality of patient care . Thus, hospitals could avoid having RNs carry out all the tasks of patient care – a practice that is costly for hospitals and often frustrat-ing for RNs . At the time, most hospital administrators viewed the team model as the most cost-efficient way to utilize the different skill levels of each occupation .
The 1970s and 1980s saw a shift away from the team nursing model . Many hospitals came to prefer the model of “primary care nursing,” in which RNs are given full responsibility for a specific group of patients . In part, nursing leaders viewed this model as more “holistic,” providing RNs with increased control over all aspects of their patients’ care .33 In some cases, RNs themselves preferred this model because it gave them more control over nursing care, allowed more contact with the patient and eliminated the need to delegate tasks to others – a role that many RNs found uncomfortable .34,35 For all these reasons, variations of “primary care” became the norm by the mid-1980s .
It is important to note that primary care nurs-ing does not necessarily preclude the use of LPNs . In a number of hospitals, LPNs are assigned their own set of patients and are responsible for the care of this population under the oversight of an
Table 7
Industries with the Highest Employment of LPNs, 2005
Industry Employment
Nursing care facilities 186,560
General medical and surgical hospitals 171,270
Offices of physicians 89,170
Employment services 52,770
Home health care services 52,700
Source: Occupational Employment and Wages, May 2005; from the U.S. Bureau of Labor Statistics, 2006.

RN . When needed, the RN performs procedures that LPNs are not authorized to carry out, but the LPN remains the primary nurse . Despite using LPNs within a primary care model, many hospital administrators moved to cut their LPN workforce and increase hiring of RNs, based on a combina-tion of the perceived limits to the LPN scope of practice and the hospital’s business strategy .36
Unfortunately, the primary care model not only entailed cutbacks in the LPN workforce, but also led to changes in the nation’s nurse training system that make it hard to reverse course . As the model spread across the country, RN training programs dropped their focus on training in delegation and other lead-ership skills – making it that much more difficult for graduates of these programs to work within a team framework . Hospitals that seek to return to team nursing must include RN training in leader-ship skills if they are to make this transition succeed .
Managed Care, Cost Containment and Workforce Cuts
The second major force that reduced the LPN work-force in the nation’s hospitals is the onset of managed care and capitated insurance plans . This trend started not with private insurers but in a shift in insurance reimbursement practices in the Medicare system . In 1983, the federal government implemented the prospective payment system (PPS) for Medicare enrollees . Under PPS, Medicare shifted from a fee-for-service system to capitated payments . Hospitals were now paid a fixed fee for specific ailments, no matter what procedures were involved in treating a particular patient . In this system, hospitals earn a profit if their costs for treatment are below the pre-determined payment level .37 This gave hospitals a strong incentive to reduce the costs of patient care, and led to broad cuts in hospital staff . Between 1981 and 1993 the number of bedside caregivers declined by 7 .3 percent, even while the number of patients increased .38 At the same time, mergers and privatiza-tion of health care facilities were all accelerating .39 Laws permitting selective contracting between insur-
ers and health care providers resulted in growing enrollments in HMOs, PPOs and similar forms of managed care, all of which mirrored the Medicare system in capping the fees hospitals received for each patient . HMO penetration is also associated with dramatic reductions in the use of LPNs and aides .40
Across the nation, hospitals began to cut the LPN staff and replace them with aides – or not at all .
LPN Cutbacks Lead to Poor Job Conditions for RNs
The staff cutbacks precipitated by managed care left RNs in an untenable position . Along with the elimination of LPNs, hospitals often got rid of nurse specialists (who assist in complex situations and mentor new nurses) and ancillary staff such as ward clerks, dietary, housekeeping and transport staff .41 In many hospitals, RNs were now answering the phone, passing food trays and emptying trashcans in addition to providing all of the patient care .
For both RNs and the remaining LPNs, managed care led to increasing ratios of patients per staff, and by the late 1990s nurses across the country were complain-ing that they faced impossible and unsafe workloads . Under the new insurance model, patients who were admitted to the hospital were significantly sicker than in previous years, as hospitals sought to limit costs by delaying patients’ arrival until just prior to their procedure; prior to these changes, nurses could get to know their pre-operative patients because they were commonly admitted to the hospital a day or two in advance . As Linda Aiken notes: “Nurses used that pre-operative time to develop a trusting relationship, prepare patients and their families for what to expect following surgery, and assess the patient’s usual physical and mental state, to be able to evaluate abnormalities and detect complications postoperatively . … Now the first time the nurses see the patient is in the recovery room still groggy from anesthesia .”42 At the same time, nurses were encouraged to get patients out of the hospital as soon as possible, increasing the number of admissions and discharges that happened on a shift . The constant “in and out” of patients added to the
20 The LPN: A Practical Way to Alleviate the Nursing Shortage

LPN Employment Trends 21
RN workload, as the RNs had to bring themselves up to speed on each patient and complete the required paperwork for admission and discharge .43 The com-bination of higher acuity levels and fewer nurses at the bedside had a profound effect on the workload of nursing staff . In repeated surveys, insufficient staff-ing ratios are identified as the single most important factor leading nurses to quit hospital jobs, and scar-ing new nurses away from work in this industry .44
The Impact of Cuts on Patient Care
At all levels of the workforce, nurses are working harder than ever, but are still often unable to avoid burnout or to carry out their duties in a manner they deem fully professional . Multiple studies have documented the correlation between insufficient nurse staffing levels and poor health outcomes for hospital patients . The incidence of medication errors and nosocomial infections are directly impacted by the shortage of nurses . In addition, many nurses complain that they don’t have time to attend to basic patient needs such as giving medications on time, getting them to the bathroom, helping them walk, or making sure that they are not lying in feces or urine, putting them at risk for bedsores .45 In all these ways, the crisis in nurse staffing has frightening implications for hospital patients . To the extent that increased and better utilization of LPNs may help solve this crisis, it is an urgent priority not only for LPNs themselves, but also for the public as a whole .
Fixing the Problem: Bring Back the LPNs
The crisis in recruitment and retention of RNs cannot be solved by simply substituting LPNs for RNs, since the former’s scope of practice is too limited to replace RNs . However, many aspects of nursing care that are now assigned to impossibly overworked RNs can be shifted to LPNs, freeing RNs to focus on other duties .
The evidence from hospital administrators themselves suggests that LPNs can play a key role in alleviat-ing the current nursing shortage . In recent focus group discussions, administrators in hospitals that continue to use LPNs trumpeted the unique value of this workforce .46 Among the most important fac-tors identified by administrators are that LPNs have received more training than aides and thus can carry out a greater range of duties; that they can take over some of the hands-on tasks now performed by RNs; and that such a substitution results in cost sav-ings, since LPN wages are below those of RNs .47
The same administrators identified the prime bar-riers to expanded use of LPNs as the limitations (real or perceived) of the scope of practice; the fact that some RNs found sharing an assignment more burdensome than helpful; and lack of clini-cal experience in specialty units .48 This report will present data that will address each of these bar-riers and suggest strategies to overcome them .

Examples of Successful Models
In the cases here, we focus on hospitals’ efforts to guarantee that LPNs are empowered to work to their full scope of practice, and to ensure that LPNs receive the advanced training required for work in specialty units . Together, these cases provide a real-life roadmap for improving the utilization of LPNs in acute care hospitals .
Boulder Community Hospital and Reading Hospital: Employing LPNs to Their Full Scope of Practice
At Boulder Community Hospital in Colorado, LPNs working in the cardio-telemetry unit are given as much responsibility as their licensing allows . They pass medications, do phlebotomy, hang IVs, and assist with chest tube removals and closings . The unit supervisor reports that she encourages a “do it all” approach in part because it helps LPNs transition to RNs and “hit the ground running .” The telemetry unit director has similarly created an internal career ladder, pursuing a policy of recruiting people as aides and then using the unit’s education funds to pay for their training as LPNs and RNs . Here, letting the LPNs work to the bounds of their scope of practice not only meets critical staffing needs in the unit, but also helps those LPNs who aspire to move on to an RN position .49
LPNs are similarly encouraged to work to the limits of their scope at Reading Hospital in Pennsylvania . “Reading Hospital utilizes LPNs to the fullest of their practice act and provides maximum opportunities,” reports Susan Fisher, the hospital’s nurse recruiter . LPNs serve a critical role as part of Reading’s nursing team . While RNs are responsible for managing a unit and creating staff schedules, it is LPNs who are more likely to be at the bedside . These nurses are encouraged to assess a patient and “critically think” before calling an RN to determine treatment, with RNs relying on LPNs’ observations to formulate patient care programs .50
Summary of Best Practices
These case studies point to some of the key best practices for re-integrating LPNs into differ-ent hospital units, and for allowing current LPN employees to work at the highest level possible .
• Hospital administrators, RNs and LPNs must all be educated regarding their state’s scope of practice for LPNs .
• When expanding the role of LPNs, all bedside nursing staff should be involved in the process . Such a process should include:
- Creating appropriate job descriptions for LPNs, including any specialty experience needed, and making sure that the job description is clearly communicated to all current staff to prevent role confusion .
- Developing a unit-specific curriculum for training LPNs to work to the full extent of their authority .
- Developing and implementing an orientation and mentoring plan for LPNs .
• While the plan is being developed and implemented, it is critical to establish effective communication structures between management, RNs and LPNs .
• RNs must be trained in leadership skills .
• To make the transition succeed, it is important that hospitals provide additional compensation for mentors, as well as for LPNs who upgrade skills and take on expanded duties .
22 The LPN: A Practical Way to Alleviate the Nursing Shortage
Recruitment and Retention of Hospital LPNs 23
Recouping LPNs Who Have Left the Health Care Field
If hospitals redesign their work processes to make greater use of LPNs, there is a ready population to meet the demand for increased LPNs: licensed nurses who are not currently working in the occupa-tion for which they trained . Evidence suggests that many LPNs view hospitals as the most desirable employer, due to the combination of higher pay and more exciting work than in other health care set-tings . However, the historical trends described ear-lier have left many LPNs frozen out of the hospital workforce . If there were more positions available in hospitals, some of these LPNs might return to prac-tice . Table 8 on Page 24 shows the number of licenses and working LPNs in each state in the country . In every state, the number of licenses significantly exceeds the number currently employed as LPNs . Part of the discrepancy in the data may be explained by the fact that LPNs may hold a license in more
than one state . There is no hard data regarding why LPNs stop working in hospitals . However, it is rea-sonable to assume that if hospital demand for LPNs increased, and if the job became more attractive by expanding its range of duties, a significant share of these LPNs could be lured back into hospital work .
Recruiting New LPNs: Innovative Training Programs
Encouraging current LPNs to re-enter the hos-pital workforce will help meet immediate staff-ing needs . Over the long term, however, hospitals must adopt strategies for increasing the number of graduates from LPN training programs .
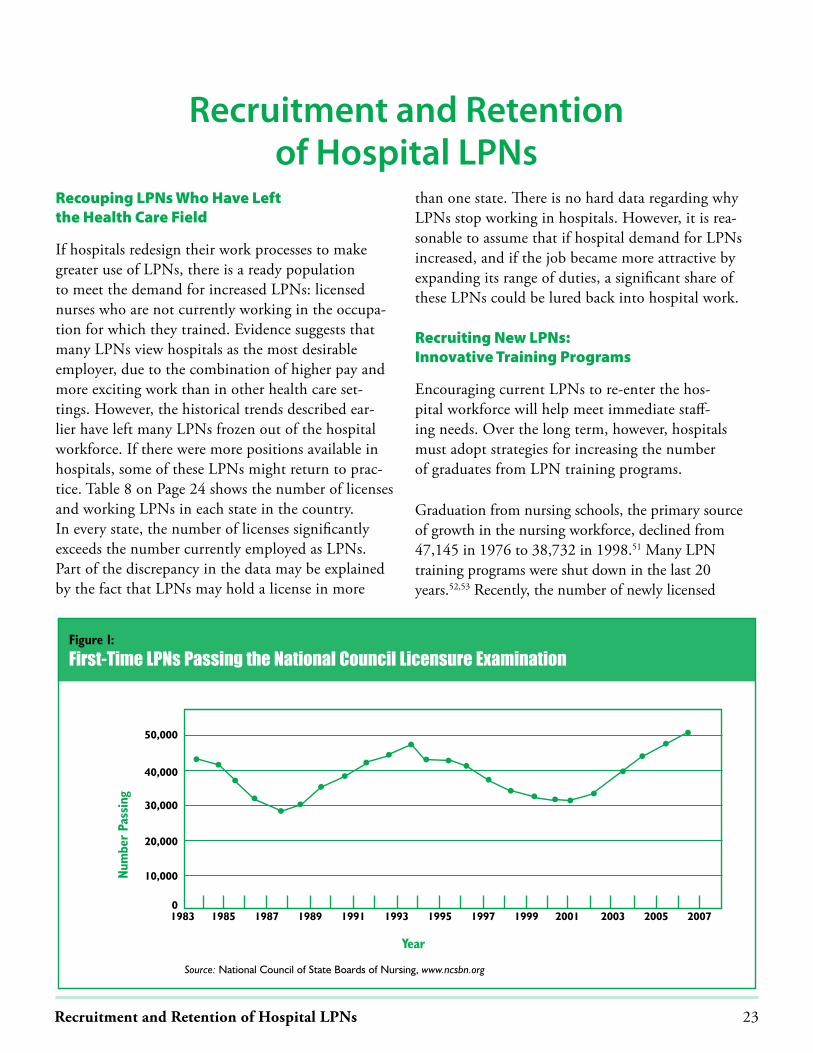
Graduation from nursing schools, the primary source of growth in the nursing workforce, declined from 47,145 in 1976 to 38,732 in 1998 .51 Many LPN training programs were shut down in the last 20 years .52,53 Recently, the number of newly licensed
Recruitment and Retention of Hospital LPNs
Year
Figure 1:
First-Time LPNs Passing the National Council Licensure Examination
Num
ber
Pass
ing
1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003 2005 2007
50,000
40,000
30,000
20,000
10,000
0
Source: National Council of State Boards of Nursing, www.ncsbn.org

Table 8
Total Active LPN Licenses and Estimated LPN Population
State
Total activelicenses in 2000
Number of people employedas LPNs in 2000 State
Total activelicenses in 2000
Number of people employedas LPNs in 2000
Alabama 16,676 13,515 Montana 3,223 1,930
Alaska 827 565 Nebraska 6,413 4,980
Arizona 9,271 6,930 Nevada 2,945 2,065
Arkansas 16,917 9,785 New Hampshire 2,989 2,145
California 65,383 46,190 New Jersey 22,855 15,110
Colorado 10,206 5,140 New Mexico 3,240 2,645
Connecticut 11,135 6,380 New York 69,820 40,545
Delaware 2,079 1,415 North Carolina 21,578 15,560
District of Columbia 2,675 925 North Dakota 3,031 2,025
Florida 51,899 37,675 Ohio 42,720 29,970
Georgia 30,042 18,385 Oklahoma 16,732 11,510
Hawaii 2,699 1,570 Oregon 4,225 3,005
Idaho 4,007 2,530 Pennsylvania 50,714 32,785
Illinois 28,742 20,745 Rhode Island 3,057 1,835
Indiana 25,997 14,925 South Carolina 11,559 9,840
Iowa 9,429 6,170 South Dakota 2,176 1,600
Kansas 8,718 6,405 Tennessee 26,421 17,025
Kentucky 13,231 9,855 Texas 77,044 48,760
Louisiana 22,369 14,505 Utah 3,470 2,695
Maine 3,463 2,260 Vermont 1,884 1,620
Maryland 8,426 9,335 Virginia 26,694 17,185
Massachusetts 22,445 12,145 Washington 13,869 9,410
Michigan 28,047 18,160 West Virginia 6,091 5,470
Minnesota 22,342 15,875 Wisconsin 14,521 10,465
Mississippi 11,315 8,750 Wyoming 1,120 665
Missouri 22,296 15,370 Total U.S. 889,027 596,355*
*Estimates may not add up to total due to rounding
Source: Seago J.A., Spetz J., Chapman S., Dyer W., Grumbach K.: Supply, Demand and Use of Licensed Practical Nurses; Bureau of Health Professionals;U.S. Department of Health and Human Services, 2004.
24 The LPN: A Practical Way to Alleviate the Nursing Shortage

Recruitment and Retention of Hospital LPNs 25
LPNs in the United States has been increasing, but in many states it is not increasing fast enough to meet the projected demand .54
Recent data on the number of new graduates of LPN programs, from the NCLEX-PN statistics gathered by the NCSBN, is illustrated in Figure 1 on Page 23 . The number of first-time candidates who pass the NCLEX exam is a good indicator of the num-ber of new graduates available to the workforce each year . The number of candidates dropped through most of the 1990s, picking up in 2002; by 2006 there were 50,931 LPNs who passed the exam .55
To increase the number of new LPNs, hospital employers will need to work with other stake-holders to expand the number of accessible LPN programs, attract qualified applicants, help them excel in the program and successfully integrate them into the hospital workforce . While this may appear a daunting task, a number of innovative programs serve as models for doing just that .
One model taking hold in many parts of the country focuses on creating partnerships between employers and educational programs to train current entry-level health care workers to become LPNs . Cheryl Feldman, director of the AFSCME 1199C Training and Upgrading Fund, located in Philadelphia, explains the logic behind such an approach by not-ing that “the employees have proven their worth as employees already, so training to upgrade their skills is worth the investment . The employers are in a much better position to have a long-term worker .” Such internal career ladders offer the added benefit of serv-ing as an effective retention strategy and building a workforce that is committed to quality care . “When the workers see the hospitals investing in them so they can move up, they are so grateful,” notes Feldman . “They feel valued, and they do a good job .” This sense of employer appreciation in turn makes these entry-level positions more attractive, making it easier to backfill the vacancies created when employees move up to become LPNs . What follows below are descrip-
tions of several innovative LPN training programs that suggest effective strategies through which hospital employers may boost this segment of their workforce .
AFSCME District 1199C’s Training and Upgrading Fund runs an LPN program that lasts 18 months and offers classes in the evenings and on weekends to accommodate working adults . The union works with more than 50 health care employers to jointly administer the program, which has seen enroll-ment grow from 31 students in 1999 (its first year of operation) to 120 students in 2006 . All classes are open to community members with no require-ment of prior union membership . The Pennsylvania State Board of Nursing accredits the program . Applicants must pass the math, English and scien-tific reasoning sections of the Nursing Entrance Test to enroll in the program . For those who need extra help, the program also offers an intensive, 16-week pre-nursing program and ESL classes . As of May 2006, 185 participants had successfully completed the Practical Nursing program, with 81 percent of graduates passing the LPN exam on the first try .56
In Oregon, Mt . Hood Community College is in the process of launching a stand-alone, web-based program to train LPNs . This one-year agenda was created in response to projections showing signifi-cantly increased demand for LPNs .57 The college received a $350,000 grant from the U .S . Department of Labor to start the program .58 Its director explains that the initiative is aimed at attracting incumbent health care workers, particularly CNAs . The course offerings will be primarily on-line for the didac-tic and theory portions, with participants meeting in classes for more hands-on training on weekends and evenings to make it easier for working adults to participate . The first term will include courses on study skills and medical terminology, which is criti-cal for participants who speak English as a second language . The cost for the full year is about $8,000, and the program has already forged partnerships with several health care employers in the area .59
Table 8
Total Active LPN Licenses and Estimated LPN Population
State
Total activelicenses in 2000
Number of people employedas LPNs in 2000 State
Total activelicenses in 2000
Number of people employedas LPNs in 2000
Alabama 16,676 13,515 Montana 3,223 1,930
Alaska 827 565 Nebraska 6,413 4,980
Arizona 9,271 6,930 Nevada 2,945 2,065
Arkansas 16,917 9,785 New Hampshire 2,989 2,145
California 65,383 46,190 New Jersey 22,855 15,110
Colorado 10,206 5,140 New Mexico 3,240 2,645
Connecticut 11,135 6,380 New York 69,820 40,545
Delaware 2,079 1,415 North Carolina 21,578 15,560
District of Columbia 2,675 925 North Dakota 3,031 2,025
Florida 51,899 37,675 Ohio 42,720 29,970
Georgia 30,042 18,385 Oklahoma 16,732 11,510
Hawaii 2,699 1,570 Oregon 4,225 3,005
Idaho 4,007 2,530 Pennsylvania 50,714 32,785
Illinois 28,742 20,745 Rhode Island 3,057 1,835
Indiana 25,997 14,925 South Carolina 11,559 9,840
Iowa 9,429 6,170 South Dakota 2,176 1,600
Kansas 8,718 6,405 Tennessee 26,421 17,025
Kentucky 13,231 9,855 Texas 77,044 48,760
Louisiana 22,369 14,505 Utah 3,470 2,695
Maine 3,463 2,260 Vermont 1,884 1,620
Maryland 8,426 9,335 Virginia 26,694 17,185
Massachusetts 22,445 12,145 Washington 13,869 9,410
Michigan 28,047 18,160 West Virginia 6,091 5,470
Minnesota 22,342 15,875 Wisconsin 14,521 10,465
Mississippi 11,315 8,750 Wyoming 1,120 665
Missouri 22,296 15,370 Total U.S. 889,027 596,355*
*Estimates may not add up to total due to rounding
Source: Seago J.A., Spetz J., Chapman S., Dyer W., Grumbach K.: Supply, Demand and Use of Licensed Practical Nurses; Bureau of Health Professionals;U.S. Department of Health and Human Services, 2004.

The Community College of Denver has adopted a strategy of providing intensive support for its LPN students, including assigning each student a col-lege case manager and a mentor . The case manager is charged with assisting students with tutoring services, financial aid and completing necessary paperwork . Health care employers affiliated with the program pair students with mentors who encourage them, and address cultural and language issues . These mentors receive a pay bonus when their students pass the state test, an additional bonus when a graduate stays on the job for six months and again if the student remains on the job a full year .60 This integration of college education with on-the-job mentoring has enabled employers to create a continuous training pipeline that stretches from the classroom to the hospital .
The Chicago Public Schools’ Practical Nursing Program provides an innovative model of early entry into nursing for high school students . This rigorous program, the only one of its kind in Illinois, recruits carefully selected high school juniors and seniors . The course regimen is free to residents of Chicago, and after graduation, these students are eligible to take the NCLEX-PN exam for licensure . Many local colleges and universities allow qualified graduates to transfer into associate degree nursing programs with 15-19 hours of college credit . About 80 percent of these graduates go on to earn their RN licenses, while 20 percent either stay employed as LPNs or turn to military or other allied health careers .61 Sandra Webb-Booker, the citywide coordinator for this innovative agenda, and a member of the Illinois State Board of Nursing, would like to see more of them developed, particularly in underserved areas . “You would not have a nursing shortage if there were a vocational LPN program in every high school,” she points out . “It’s a win-win scenario . The nursing workforce gets a shot of young blood and enthusiasm, and students get the opportunity to have exposure to a professional track .”62
As the demand for nurses continues to exceed the supply, it will become ever more urgent to increase the number of newly minted LPNs . This is not a simple task . But as the preceding examples make clear, there are myriad models for employers and educators to join together to effectively solve this problem .
Magnet Hospitals: A Good Idea that has Gone Astray
One popular strategy for recruiting and retaining nurses is the Magnet Recognition Program . This is a voluntary program, certified by the American Nurses Credentialing Center, a subsidiary of the American Nurses Association . Health care facilities often cite their “Magnet” status as proof that they have met a list of nursing standards linked to quality care, using the sales pitch “We’re Magnet” to attract nurses in tight labor markets . Magnet status is similarly presented to consumers as proof of “quality nurs-ing care .” Currently 224 health care organizations in 42 states have been awarded Magnet status .63
Many hospitals awarded Magnet designation have improved working conditions for nurses and improved patient care . However, there is a significant downside to the Magnet program . The application process is so costly and time consuming that some hospitals hire special consultants just to help them through it . Resources spent on becoming a Magnet hospital are diverted away from direct patient care . Worse yet, the marketing of Magnet status may be used to conceal serious flaws in a hospital’s nurs-ing practice . Ironically, some hospitals that use the Magnet application as a recruitment strategy never-theless avoid instituting the very practices that are known to most effectively attract and retain nurses, such as eliminating mandatory overtime, institut-ing flexible scheduling and setting staffing ratios .64
26 The LPN: A Practical Way to Alleviate the Nursing Shortage

Recruitment and Retention of Hospital LPNs 27
For LPNs, the Magnet program carries the added fear that hospitals may use the process as a pretext to eliminate their positions . For example, in 2004 Mercy Hospital in Coon Rapids, Minn ., was advised by a consulting firm to eliminate LPN positions as a way to cut costs . According to an interview with Deb Tauer, president of the Minnesota Licensed Practical Nurses Association, AFSCME Local 105 (Council 65), the consulting firm told the hospital that RNs had to “repeat all work done” by LPNs . LPNs were eliminated over an 18-month period to make room for more RN positions, according to the hospital spokesperson .65 The hospital wanted to beef up its RN-to-patient ratios to facilitate their Magnet appli-cation .66 According to Maxine Davis, LPN, a member of AFSCME Local 105 in Minnesota, the LPN is a “cost-effective, licensed bedside nurse who is an effi-cient, accountable member of the health care team .” By eliminating its LPN workforce, the hospital seems to have put marketing hype ahead of sensible practice .
Ultimately, hospitals that are serious about improv-ing their nursing practice can do so with or with-out “going Magnet .” That status cannot substitute for real transformations . Nowhere is this truer than with regard to the issue of employee “voice .” While many Magnet programs boast of encourag-ing nurse input, nurses can also represent them-selves very effectively through their own union .
Giving Nurses a Voice: Unionization
In 2003, 19 .5 percent of RNs and 12 .4 percent of LPNs had union representation in their workplace .67 Compensation is an important issue for nurses, and unions are instrumental in meeting this demand . Nationally, nurses with a union earned 13 percent more than their non-union counterparts .68 Yet the importance of unions extends far beyond the issue of compensation .
Research suggests that nurses turn to unions to safe-guard the professional standards of their work and to help them guarantee the quality of care received by their patients .69,70 Unions address these concerns in myriad ways, including negotiating agreements regarding nurse-to-patient ratios . Indeed, cities with the highest rate of unionized nurses report nurse-to-patient ratios that are 18 percent above those of the least-unionized areas .71 Similarly, nurse unions have negotiated agreements on occupational health and safety standards that protect patients as well as nurses, such as the regulating of patient lifting and the use of hypodermic needles . Finally, unions protect the ability of nurses to speak out in support of patient needs – or to report problems on the job – without fear of being fired for speaking their minds . As one LPN remarked, “If LPNs don’t have a union, all management has to do is tap you on the shoulder and say, ‘You’re gone .’”
Beyond issues of compensation or job duties, nurse unions have been expert advocates for policies to address the broader dimensions of the nursing crisis . In numerous states, unions have called on legislators to support regulations guaranteeing safe staffing and quality care . Unions have been instrumental in creat-ing training programs to expand the pool of licensed nurses . And within individual hospitals, unions have established joint labor/management processes for evaluating the appropriate duties and staffing levels for each segment of the nursing workforce .
As we look to a future in which LPNs will play an increasingly critical role in meeting the nation’s nurs-ing needs, the ability of nurses to represent themselves through a union will be more important than ever .

Hospitals need qualified, experienced bedside caregivers – RNs, LPNs and aides . Finding ways to recruit and retain competent nurses and staff should be the goal of hospitals . With proper planning, training, and oversight the delegation of certain responsibilities to LPNs can free up the RNs to perform to the full extent of their scope of practice .
It seems like an obvious solution to the nursing short-age in hospitals, but not everyone wants LPNs to play a role in hospital care . Several recent studies allege that a higher percentage of RNs in the workforce results in better patient care . Some have even recom-mended that the cost-effective way to improve patient care is to replace all remaining hospital LPNs with RNs .74 Further research on the most advantageous skill mix is needed, but clearly the goal of hospitals should be to provide excellent patient care in a cost-effective manner . And to state the obvious, upgrading the skill mix doesn’t help if there aren’t enough people at the bedside providing care . It doesn’t matter how educated a nurse is if she or he has too many patients to spend any time with them . The level of educa-tion and licensure of the nurse may play a role in the overall quality of a patient’s care, but other factors are more important . These include the patient’s acuity level, the nurses’ overall workload, skills and experi-ence, the level of support from ancillary staff and supervisors, and the physical working environment .
A large part of the solution to improving patient care lies in improving working conditions for both RNs and LPNs in order to attract qualified, com-petent people into the profession and keep them there . Study after study shows nurses leaving due to unbearable working conditions . The most sen-sible policy appears to be for hospitals to pursue an intelligent and strategic mix of RNs, LPNs and
assistants among the nursing staff, with each cat-egory of nursing care professional carrying out the tasks for which it is best trained and suited .
It is ironic that, while the country is facing a critical nursing shortage, the potential of the LPN workforce is so underutilized . As described above, the history of the past 20 years has seen hospital administrators unwittingly handicap themselves by denying their units access to a valuable and affordable part of the nursing corps . After these years of neglect, the LPN training system is significantly diminished, and in many places hospital administrators as well as RNs have lost the skills, knowledge and comfort needed to integrate LPNs into a broader nursing team . It will not be simple to reverse this process . But it is clearly possible, and there are many effective models that point the way to enabling LPNs to play a vital role in meeting the nursing needs of the 21st Century .
Conclusions and Recommendations
28 The LPN: A Practical Way to Alleviate the Nursing Shortage

Conclusions and Recommendations 29
The Next Steps
• Hospitals can and should increase their employment of LPNs while instituting practices that enable LPNs, RNs and other members of the nursing staff to function as an effective team .
• Hospital administrators should educate themselves and their staff about the LPN scope of practice in their state . While LPNs cannot substitute for RNs, they can be utilized to their full scope of practice, thus adding highly qualified, cost-effective members to the nursing team .
• Hospitals need to work with other stakeholders to increase the number of accessible LPN programs in order to increase the number of new LPNs .
• The LPN scope of practice, standards of practice and curriculum need to be standardized at a national level .
• There needs to be research on new models of nursing that integrate RNs, LPNs and aides into an effective team .
• There is a lack of research on LPNs . Additional research is needed on LPNs in the acute setting, their scope of practice and why LPNs leave nursing for other jobs .
• Nursing staff working at the bedside should have a voice in the decisions that affect them . RNs, LPNs and aides should participate in the discussions about appropriate staffing levels and mix .
• When expanding the role of LPNs, all bedside nursing staff should be involved in the process . Such a course of action should include:
- Creating appropriate job descriptions for LPNs, including any specialty experience needed, and making sure that the job description is clearly communicated to all current staff to prevent role confusion .
- Developing a unit-specific curriculum for training LPNs to work to the full extent of their authority .
- Developing and implementing an orientation and mentoring plan for LPNs .
• During the transition period while the plan is being developed and implemented, it is critical to establish effective communication structures between management, RNs and LPNs .
• RNs must be trained in leadership skills .
• To make the transition succeed, it is important that hospitals provide additional compensation for mentors, as well as for LPNs who upgrade skills and take on expanded duties .


Appendix 31
AppendixTable 9b
State Scope of Practice SpecificityScale ScoresSorted by Specificity (With 1 being the least and 5 being the most)
Specificity Specificity
California 4 Tennessee 2
Idaho 4 Utah 2
Iowa 4 Vermont 2
Kansas 4 Washington 2
Maine 4 Wisconsin 2
Montana 4 Wyoming 2
Nebraska 4 Virgin Islands 2
New Jersey 4 Arizona 1
Ohio 4 Connecticut 1
Pennsylvania 4 Florida 1
South Carolina 4 Georgia 1
South Dakota 4 Hawaii 1
Alaska 3 Indiana 1
Illinois 3 Maryland 1
Mississippi 3 Massachusetts 1
Nevada 3 Michigan 1
New Hampshire 3 Minnesota 1
Oregon 3 Oklahoma 1
Alabama 2 Texas 1
Arkansas 2 Virginia 1
Colorado 2 West Virginia 1
Delaware 2
Dist. of Columbia 2
Kentucky 2
Louisiana 2
Missouri 2
New Mexico 2
New York 2
North Carolina 2
North Dakota 2
Rhode Island 2
Table 9a
State Scope of Practice Restrictiveness Scale ScoresSorted by Most Restrictive (With 1 being the least and 5 being the most)
Restrictive-ness
Restrictive-ness
Iowa 4 South Dakota 2
Virgin Islands 4 Tennessee 2
Alaska 3 Virginia 2
Arizona 3 West Virginia 2
Arkansas 3 Wisconsin 2
California 3 Wyoming 2
Colorado 3 Florida 1
Dist. of Columbia 3 Hawaii 1
Illinois 3 Indiana 1
Kansas 3 Louisiana 1
Maine 3 Massachusetts 1
Nebraska 3 Michigan 1
Utah 3 Minnesota 1
Alabama 2 New Jersey 1
Connecticut 2 New Mexico 1
Delaware 2 North Carolina 1
Georgia 2 Oklahoma 1
Idaho 2 Rhode Island 1
Kentucky 2 Texas 1
Maryland 2 Vermont 1
Mississippi 2 Washington 1
Missouri 2
Montana 2
Nevada 2
New Hampshire 2
New York 2
North Dakota 2
Ohio 2
Oregon 2
Pennsylvania 2
South Carolina 2
Source: Seago J.A., Spetz J., Chapman S., Dyer W., Grumbach K.: Supply, Demand and Use of Licensed Practical Nurses; Bureau of Health Professionals,U.S. Department of Health and Human Services, 2004.
Appendix A

32 The LPN: A Practical Way to Alleviate the Nursing Shortage
Table 10
LPN Scopes of PracticeTUBES DRESSINGS
State IVm
eds
Canc
erag
ents
Cent
rall
ines
Bloo
d
Hype
ral
Venu
sbl
ood
draw
Arte
rial
bloo
ddr
aws
Inse
rtIV
Inse
rtio
n
Mai
nten
ance
Chan
ges
Rein
forc
emen
t
Alabama
Alaska � � � �
Arizona �
Arkansas �* NO
California �* � �* � � � �
Colorado �* NO �* NO �
Connecticut �* �*
Delaware � �* �
District of Columbia � �* �
Florida �
Georgia �
Hawaii
Idaho � NO �* � � �* � � � �
Illinois � NO � NO � �
Indiana
Iowa �* NO � �* � �* �
Kansas �* NO NO NO �* �* �* �
Kentucky �*
Louisiana � � � � � � � �
Maine �* NO � �* �* �
Maryland � �*
Massachusetts �
Michigan �* NO
Minnesota �
Mississippi �* NO �* NO
Missouri �*
Montana � NO NO NO NO � � �
Nebraska � NO NO NO NO �* NO �
Nevada � NO NO NO � � � � �

Appendix 33
NURSE CAREPLANNING SUPERVISORS
Docu
men
tatio
n
Asse
ssm
ent
Data
colle
ctio
n
Obse
rvat
ion
Verb
alan
dph
one
orde
rs
Docu
men
tatio
nco
-sig
ned
Teac
hing
Stan
dard
ized
proc
edur
es/
expa
nded
prac
tice
Rest
rict
ive
Spec
ific
Othe
rpr
oced
ures
RN, MD �
NO RN, MD, Dentist �
� � �
RN, MD, Dentist, APN
RN, MD 4 4
� NO � � RN, MD, APN, Dentist, Podiatrist � 3 3
� � 1
� � 2
RN, MD, DO, Podiatrist, Dentist 1
� � 1
� � 1
� � � RN, MD, Dentist � 2 4
� � � RN, MD, Dentist � 3 3
RN, MD, Dentist, Chiropractor,Optometrist, Podiatrist
1 1
� � � 4 4
RN 3 4
� �RN, MD, Optometrist, Dentist,Psychologist � 1 2
� NO � � 3 3
� � � � 2
1
1
� � � RN, MD, Dentist 3 3
RN, MD 2
� � RN, MD, Dentist, OD, Podiatrist � 2 2
� � � RN � 4 3
� � � 3 3
� written * with additional educationnon-specific-specific=1- 5 unrestrictive-restrictive=1- 5 (with 1being the least and 5 being the most)
34 The LPN: A Practical Way to Alleviate the Nursing Shortage
Table 10
LPN Scopes of Practice (Continued)TUBES DRESSINGS
State IVm
eds
Canc
erag
ents
Cent
rall
ines
Bloo
d
Hype
ral
Venu
sbl
ood
draw
Arte
rial
bloo
ddr
aws
Inse
rtIV
Inse
rtio
n
Mai
nten
ance
Chan
ges
Rein
forc
emen
t
New Hampshire �*
New Jersey �*
New Mexico � � �
New York �* NO �*
North Carolina � �*
North Dakota �
Ohio �*
Oklahoma �
Oregon
Pennsylvania �* NO NO � �
Rhode Island �
South Carolina �* �* �* �* �* �*
South Dakota � NO �* NO � � �
Tennessee
Texas �* �* �* �* �*
Utah �*
Vermont
Virginia �*
Washington �* �* �* �* �*
West Virginia �*
Wisconsin �
Wyoming �*

Appendix 35
NURSE CAREPLANNING SUPERVISORS
Docu
men
tatio
n
Asse
ssm
ent
Data
colle
ctio
n
Obse
rvat
ion
Verb
alan
dph
one
orde
rs
Docu
men
tatio
nco
-sig
ned
Teac
hing
Stan
dard
ized
proc
edur
es/
expa
nded
prac
tice
Rest
rict
ive
Spec
ific
Othe
rpr
oced
ures
� � RN, MD, ARNP, Dentist 2
� � 2
2
� � � 2
� � � 1
� � � 1
� �RN, MD, Dentist, Optometrist,Podiatrist �
1
� � �
� 3 3
� � 4 5
RN, MD NO � 3 3
� � 1
� � 2 2
� � RN, MD 2
� � RN, MD, APRN, Dentist 1
1
� � � 3 3
� � � � 1
�RN, MD, Podiatrist, Dentist,Optometrist � 1
� � RN, MD, Dentist 1
Source: Seago J.A., Spetz J., Chapman S., Dyer W., Grumbach K.: Supply, Demand and Use of Licensed Practical Nurses; Bureau of HealthProfessionals, U.S. Department of Health and Human Services, 2004.

Sources“A Profile of the South Carolina Nursing Workforce”; Office of Research and Statistics, South Carolina Budget and Control Board, 2003.
Adams V., Price-Lea P.J.: “A Critical Need for a More Diverse Nursing Workforce”; North Carolina Medical Journal, 2004; 65(2).
Aiken L.H.: Improving Quality through Nursing. Princeton, N.J.: Robert Wood Johnson Foundation, 2005.
Aiken L.H., Sochalski J., Anderson G.F.: “Downsizing the Hospital Workforce”; Health Affairs, 1996; 15(4):88-92.
Beverage P.A.: “How LPNs Can Be Part of the Solution”; North Carolina Medical Journal, 2004; 65:2.
Brannon R.L.: Intensifying Care: The Hospital Industry, Professionalization and the Reorganization of the Nursing Labor Process. Amityville, N.Y.: Baywood Publishing Company Inc., 1994.
Burke K.: LPN Supply and Demand: The Future of Licensed Practical Nurses in Oregon. Oregon Health Care Career Center, 2004.
Cavarallo M.A.: “RNs and LPNs – A Powerful Team”; Nursing Spectrum, 2003.
Clark P.: “Union Strategies for Improving Patient Care: The Key to Nurse Unionism”; Labor Studies Journal, 2006; 31(1):51-70.
Correspondence with L. Kelsey, November 2006.
Crawford L., O’Neill T.R., Reynolds M., White E.: 2003 Nurse Licensee Volume and NCLEX Examination Statistics; National Council of State Boards of Nursing, 2005.
Eriksen A.B.: “Veterans Affairs Nursing in the 21st Century”; Minority Nurse, 2005.
Interview with Linda Fleshman, Mt. Hood Community College, 2006
Fogler J.: “Team Players”; Nurse Week, 2002.
Gordon S.: Nursing Against the Odds: How Health Care Cost Cutting, Media Stereotypes, and Medical Hubris Undermine Nurses and Patient Care; Ithaca: Cornell University Press, 2005.
Howatt G.: “Two Hospitals to Drop Licensed Practical Nurses”; Minneapolis Star Tribune, Nov. 21, 2005.
Kelsey L.: “Use ’em or Lose ’em: The Licensed Practical Nurse”; Gastroenterology Nursing, 2006; 29(1):37-41.
Labor Relations in the Health Care Industry for Nurses: Online Credit Program; at Michigan State University, 2006.
Lafer G., Moss H., Kirtner R., Rees V.: Solving the Nursing Shortage: Best and Worst Practices for Recruiting, Retaining and Recouping of Hospital Nurses; University of Oregon, May 2003.
Lovell V.: Solving the Nursing Shortage Through Higher Wages; Washington, D.C.: Institute for Women’s Policy Research, 2006.
36 The LPN: A Practical Way to Alleviate the Nursing Shortage

Sources 37
“Magnet Doesn’t Attract Everyone”; UNA Action, 2005.
Magnet Hospitals; American Nurses Credentialing Center, 2006.
Mason D.J.: “Mentored by an LPN: How We Can Support All Nurses’ Continued Education”; American Journal of Nursing, 2006; 106(7).
Melton K.: “Mt. Hood College Aims to Ease Nurse Shortage: The School Plans to Use a Federal Grant to Start a Practical Nurse Program”; The Oregonian, Oct. 23, 2006.
NCLEX data at www.ncsbn.org/462.htm; NCLEX also has a program database on LPN graduates, organized by state.
Needleman J., Buerhaus P., Stewart M., Zelevinsky K., Mattke S.: “Nurse Staffing in Hospitals: Is There a Business Case For Quality?”; Health Affairs, 2006; 25(1):204-211. Occupational Employment and Wages, May 2005; U.S. Bureau of Labor Statistics, 2006.
Occupational Outlook Handbook; from the U.S. Department of Labor, 2006.
Prince H.: “Creating Careers, Improving Care: A Win-Win Economic Advancement Strategy for Certified Nursing Assistants in Long-Term Care”; Jobs for the Future, 2006.
Seago J.A.: “Can the Use of LPNs Alleviate the Nursing Shortage?”; The American Journal of Nursing, 2006; 106(7):40-49.
Seago J.A., Spetz J., Chapman S., Dyer W., Grumbach K.: Supply, Demand and Use of Licensed Practical Nurses; Bureau of Health Professionals, U.S. Department of Health and Human Services, 2004.
Silvestri G.T., Lukasiewiez J.M.: Occupational Employment Projections: The 1984-1995 Outlook; Washington, D.C.: U.S. Bureau of Labor Statistics, November 1985.
Smith J., Crawford L.: Winter 2002 -- Practice & Professional Issues Survey: Preparation for RN Competencies and Characteristics of a Typical Day at Work; Chicago: National Council of State Boards of Nursing, 2003.
Smith J.: Executive Summary: Exploring the Value of Continuing Education Mandates; Chicago: National Council of State Boards of Nursing, September 2003.
Spader C.: “Wanted: More LPNs”; Nursing Spectrum, 2006.
Spector N.: Practical Nurse Scope of Practice White Paper; Chicago: National Council of State Boards of Nursing, 2005.
Spetz J.: “The Effects of Managed Care and Prospective Payment on the Demand for Hospital Nurses: Evidence from California”; Health Services Research, 1999; 34(5):993-1010.
Workforce Issues in America’s Public Hospitals: Issue Brief. Washington, D.C.: National Association of Public Hospitals and Health Systems, 2006.
Working with Others: A Position Paper; Chicago: National Council of State Boards of Nursing, 2005.

Endnotes
1 Working with Others: A Position Paper; Chicago: National Council of State Boards of Nursing, 2005.
2 Spector N.: Practical Nurse Scope of Practice White Paper; Chicago: National Council of State Boards of Nursing, 2005.
3 Silvestri G.T., Lukasiewiez J.M.: Occupational Employment Projections: The 1984-1995 Outlook; Washington, D.C.: U.S. Bureau of Labor Statistics, November 1985.
4 Occupational Employment and Wages, May 2005; U.S. Bureau of Labor Statistics, 2006.
5 Seago J.A., Spetz J., Chapman S., Dyer W., Grumbach K.: Supply, Demand and Use of Licensed Practical Nurses; Bureau of Health Professionals, U.S. Department of Health and Human Services, 2004.
6 Beverage, P.A.: “How LPNs Can Be Part of the Solution”; North Carolina Medical Journal, 2004; 65:2.
7 Seago J.A., Spetz J., Chapman S., Dyer W., Grumbach K.: Supply, Demand and Use of Licensed Practical Nurses; Bureau of Health Professionals, U.S. Department of Health and Human Services, 2004.
8 Spector N.: Practical Nurse Scope of Practice White Paper; Chicago: National Council of State Boards of Nursing, 2005.
9 Smith J., Crawford L.: Winter 2002 -- Practice & Professional Issues Survey: Preparation for RN Competencies and Characteristics of a Typical Day at Work; Chicago: National Council of State Boards of Nursing, 2003.
10 Mason D.J.: “Mentored by an LPN: How We Can Support All Nurses’ Continued Education”; American Journal of Nursing, 2006; 106(7).
11 Seago J.A., Spetz J., Chapman S., Dyer W., Grumbach K.: Supply, Demand and Use of Licensed Practical Nurses; Bureau of Health Professionals, U.S. Department of Health and Human Services, 2004.
12 Smith J.: Executive Summary: Exploring the Value of Continuing Education Mandates; Chicago: National Council of State Boards of Nursing, September 2003.
13 Smith J.: Executive Summary: Exploring the Value of Continuing Education Mandates; Chicago: National Council of State Boards of Nursing, September 2003.
14 Working with Others: A Position Paper; Chicago: National Council of State Boards of Nursing, 2005.
15 Spector N.: Practical Nurse Scope of Practice White Paper; Chicago: National Council of State Boards of Nursing, 2005.
16 Seago J.A.: “Can the Use of LPNs Alleviate the Nursing Shortage?”; The American Journal of Nursing, 2006; 106(7):40-49.
17 Seago J.A., Spetz J., Chapman S., Dyer W., Grumbach K.: Supply, Demand and Use of Licensed Practical Nurses; Bureau of Health Professionals, U.S. Department of Health and Human Services, 2004.
18 Spector N.: Practical Nurse Scope of Practice White Paper; Chicago: National Council of State Boards of Nursing, 2005.
38 The LPN: A Practical Way to Alleviate the Nursing Shortage
Endnotes 39
19 Seago J.A., Spetz J., Chapman S., Dyer W., Grumbach K.: Supply, Demand and Use of Licensed Practical Nurses; Bureau of Health Professionals, U.S. Department of Health and Human Services, 2004.
20 Occupational Employment and Wages, May 2005; U.S. Bureau of Labor Statistics, 2006.
21 Lovell V.: Solving the Nursing Shortage Through Higher Wages; Washington, D.C.: Institute for Women’s Policy Research, 2006.
22 Seago J.A., Spetz J., Chapman S., Dyer W., Grumbach K.: Supply, Demand and Use of Licensed Practical Nurses; Bureau of Health Professionals, U.S. Department of Health and Human Services, 2004.
23 Seago J.A., Spetz J., Chapman S., Dyer W., Grumbach K.: Supply, Demand and Use of Licensed Practical Nurses; Bureau of Health Professionals, U.S. Department of Health and Human Services, 2004.
24 “A Profile of the South Carolina Nursing Workforce”; Office of Research and Statistics, South Carolina Budget and Control Board, 2003.
25 Workforce Issues in America’s Public Hospitals: Issue Brief; Washington, D.C.: National Association of Public Hospitals and Health Systems, 2006.
26 Eriksen A.B.: “Veterans Affairs Nursing in the 21st Century”; Minority Nurse, 2005.
27 Adams V., Price-Lea P.J.: “A Critical Need for a More Diverse Nursing Workforce”; North Carolina Medical Journal, 2004; 65(2).
28 Crawford L., O’Neill T.R., Reynolds M., White E.: 2003 Nurse Licensee Volume and NCLEX Examination Statistics; National Council of State Boards of Nursing, 2005.
29 Silvestri G.T., Lukasiewiez J.M.: Occupational Employment Projections: The 1984-1995 Outlook; Washington, D.C.: U.S. Bureau of Labor Statistics, November 1985.
30 Aiken L.H.: Improving Quality through Nursing; Princeton, N.J.: Robert Wood Johnson Foundation, 2005.
31 Gordon S.: Nursing Against the Odds: How Health Care Cost Cutting, Media Stereotypes, and Medical Hubris Undermine Nurses and Patient Care; Ithaca: Cornell University Press, 2005.
32 Brannon R.L.: Intensifying Care: The Hospital Industry, Professionalization and the Reorganization of the Nursing Labor Process; Amityville, N.Y.: Baywood Publishing Company Inc., 1994.
33 Brannon R.L.: Intensifying Care: The Hospital Industry, Professionalization and the Reorganization of the Nursing Labor Process; Amityville, N.Y.: Baywood Publishing Company Inc., 1994.
34 Gordon S.: Nursing Against the Odds: How Health Care Cost Cutting, Media Stereotypes, and Medical Hubris Undermine Nurses and Patient Care; Ithaca: Cornell University Press, 2005.
35 Brannon R.L.: Intensifying Care: The Hospital Industry, Professionalization and the Reorganization of the Nursing Labor Process; Amityville, N.Y.: Baywood Publishing Company Inc., 1994.
36 Seago J.A.: “Can the Use of LPNs Alleviate the Nursing Shortage?”; The American Journal of Nursing, 2006; 106(7):40-49.

37 Spetz J.: “The Effects of Managed Care and Prospective Payment on the Demand for Hospital Nurses: Evidence from California”; Health Services Research, 1999; 34(5):993-1010.
38 Aiken L.H., Sochalski J., Anderson G.F.: “Downsizing the Hospital Workforce”; Health Affairs, 1996; 15(4):88-92.
39 Brannon R.L.: Intensifying Care: The Hospital Industry, Professionalization and the Reorganization of the Nursing Labor Process; Amityville, N.Y.: Baywood Publishing Company Inc., 1994.
40 Spetz J.: “The Effects of Managed Care and Prospective Payment on the Demand for Hospital Nurses: Evidence from California”; Health Services Research, 1999; 34(5):993-1010.
41 Gordon S.: Nursing Against the Odds: How Health Care Cost Cutting, Media Stereotypes, and Medical Hubris Undermine Nurses and Patient Care; Ithaca: Cornell University Press, 2005.
42 Aiken L.H.: Improving Quality through Nursing; Princeton, N.J.: Robert Wood Johnson Foundation, 2005.
43 Gordon S.: Nursing Against the Odds: How Health Care Cost Cutting, Media Stereotypes, and Medical Hubris Undermine Nurses and Patient Care; Ithaca: Cornell University Press, 2005.
44 Lafer G., Moss H., Kirtner R., Rees V.: Solving the Nursing Shortage: Best and Worst Practices for Recruiting, Retaining and Recouping of Hospital Nurses; University of Oregon, May 2003.
45 Gordon S.: Nursing Against the Odds: How Health Care Cost Cutting, Media Stereotypes, and Medical Hubris Undermine Nurses and Patient Care; Ithaca: Cornell University Press, 2005.
46 Seago J.A., Spetz J., Chapman S., Dyer W., Grumbach K.: Supply, Demand and Use of Licensed Practical Nurses; Bureau of Health Professionals, U.S. Department of Health and Human Services, 2004.
47 Seago J.A., Spetz J., Chapman S., Dyer W., Grumbach K.: Supply, Demand and Use of Licensed Practical Nurses; Bureau of Health Professionals, U.S. Department of Health and Human Services, 2004.
48 Seago J.A., Spetz J., Chapman S., Dyer W., Grumbach K.: Supply, Demand and Use of Licensed Practical Nurses; Bureau of Health Professionals, U.S. Department of Health and Human Services, 2004.
49 Fogler J.: “Team Players”; Nurse Week, 2002.
50 Cavarallo M.A.: “RNs and LPNs – A Powerful Team”; Nursing Spectrum, 2003.
51 Seago J.A., Spetz J., Chapman S., Dyer W., Grumbach K.: Supply, Demand and Use of Licensed Practical Nurses; Bureau of Health Professionals, U.S. Department of Health and Human Services, 2004.
52 Prince H.: “Creating Careers, Improving Care: A Win-Win Economic Advancement Strategy for Certified Nursing Assistants in Long-Term Care”; Jobs for the Future, 2006.
53 Melton K.: “Mt. Hood College Aims to Ease Nurse Shortage: The School Plans to Use a Federal Grant to Start a Practical Nurse Program”; The Oregonian, Oct. 23, 2006.
54 Burke K.: LPN Supply and Demand: The Future of Licensed Practical Nurses in Oregon. Oregon Health Care Career Center, 2004.
55 NCLEX data at www.ncsbn.org/462.htm; NCLEX also has a program database on LPN graduates, organized by state.
40 The LPN: A Practical Way to Alleviate the Nursing Shortage

Endnotes 41
56 Prince H.: “Creating Careers, Improving Care: A Win-Win Economic Advancement Strategy for Certified Nursing Assistants in Long-Term Care”; Jobs for the Future, 2006.
57 Burke K.: LPN Supply and Demand: The Future of Licensed Practical Nurses in Oregon. Oregon Health Care Career Center, 2004.
58 Burke K.: LPN Supply and Demand: The Future of Licensed Practical Nurses in Oregon. Oregon Health Care Career Center, 2004.
59 Interview with Linda Fleshman, Mt. Hood Community College, 2006.
60 Prince H.: “Creating Careers, Improving Care: A Win-Win Economic Advancement Strategy for Certified Nursing Assistants in Long-Term Care”; Jobs for the Future, 2006.
61 Spader C.: “Wanted: More LPNs”; Nursing Spectrum, 2006.
62 Spader C.: “Wanted: More LPNs”; Nursing Spectrum, 2006.
63 Magnet Hospitals; American Nurses Credentialing Center; 2006.
64 “Magnet Doesn’t Attract Everyone”; UNA Action, 2005.
65 Howatt G.: “Two Hospitals to Drop Licensed Practical Nurses”; Minneapolis Star Tribune, Nov. 21, 2005.
66 “Magnet Doesn’t Attract Everyone”; UNA Action, 2005.
67 Labor Relations in the Health Care Industry for Nurses: Online Credit Program; at Michigan State University, 2006.
68 Lovell V.: Solving the Nursing Shortage Through Higher Wages; Washington, D.C.: Institute for Women’s Policy Research, 2006.
69 Lovell V.: Solving the Nursing Shortage Through Higher Wages; Washington, D.C.: Institute for Women’s Policy Research, 2006.
70 Clark P.: “Union Strategies for Improving Patient Care: The Key to Nurse Unionism”; Labor Studies Journal, 2006; 31(1):51-70.
71 Lovell V.: Solving the Nursing Shortage Through Higher Wages; Washington, D.C.: Institute for Women’s Policy Research, 2006.
72 Needleman J., Buerhaus P., Stewart M., Zelevinsky K., Mattke S.: “Nurse Staffing in Hospitals: Is There a Business Case For Quality?”; Health Affairs, 2006; 25(1):204-211.
Notes:
Notes:
Notes:

American Federation of State, County and Municipal Employees, AFL-CIO
1625 L Street, N.W.Washington, D.C. 20036-5687
www.afscme.org
Gerald W. McEntee,International President
William Lucy,International Secretary-Treasurer 031-07 BUG