the journal of pulmonary technique - respiratorytherapy.ca · 4 respiratory therapy vol. 5 no. 1 n...
TRANSCRIPT
Volume 5 Number 1 February-March 2010
The Journal of Pulmonary Technique
Capnographyaerosol DeliveryTraCheosTomyCorTiCosTeroiDsinTubaTion

Wright DJ10 1 9/21/09 3:58:04 PM


4 Respiratory Therapy Vol. 5 No. 1 n February-March 2010
Editorial
Table of ContentsDEPARTMENTS
4 Editorial
11 News
17 Products & Companies
20 Spotlight on Capnography/ Aerosol Delivery
20 Ventilation Roundtable
23 Executive Profiles
ARTICLES
26 Tracheostomy Complications
28 Closed Airway Access Systems
31 GER and Pneumonia
35 Esophageal Perforation
38 Fatigue and COPD
45 Inhaled Corticosteroids
52 Difficult Intubation
54 Asthma Development
58 Preparing for the Pandemic
Vol. 5 No. 1February-March 2010
Care For The CaregiversWhile the foreseeable shortage of ventilators in case of a major pandemic has been well documented in the media, another question is: who will insure that those treating the victims of a major outbreak will themselves be able to get treatment – so they can keep treating?
The answer is: nobody knows. We just don’t know what’ll happen, and an informal query of attendees at AARC by our journal revealed that not one RT was able to say what plans their institution had for them in case of a serious pandemic.
While it’s always easy to offer flip solutions: let’s make sure our RTs and other medical professionals are taken care of, the question of course is, how. But all solutions run up against a number of basic conundrums. It’s hard to know where to begin.
We might want to start with addressing the shortage of healthcare personnel, across the board. The Los Angeles Times recently reported that hospitals are “scrambling” for healthcare workers, with healthcare providers such as respiratory therapists already working 12-hour shifts [google LA Times keyword labor-shortages].
The next consideration, in case of a pandemic, becomes: will those workers come to work? Biothethics International reports: “Studies show that 40-50% of healthcare staff will not report to work in the event of a pandemic influenza.” (Reported by Jennifer Miller, google Bioethics International.)
If and when the workforce shows up, not only will they need ventilators, they’ll have to make decisions about who gets treatment, and they will be in the unenviable position of being both deciders and decidees, as it were.
A recent Q&A on the website of the New York State Department of Health is worth a look, insofar as the department has tried to address some basic questions about the ramifications of a pandemic for healthcare workers. According to the state website: “Although New York State continues to purchase and stockpile ventilators, we know that no matter how many ventilators are available overall, in a severe pandemic there will be shortages in individual facilities… The ill will include healthcare workers, so there also will not be enough staff to provide the extra level of care for all patients who need ventilators. Undoubtedly, difficult decisions on ventilator allocation will need to be made. A severe pandemic would also result in a shortage of staff trained to operate ventilators, forcing hospitals to decide which patients will and will not be provided ventilator support.” While New York has implemented basic policies for triage and ventilator allocation, it has noted: in the event of a severe pandemic, even these measures would still fall short of addressing the anticipated need for ventilators.” New York’s guidelines specifically address ventilator availability for healthcare workers: “Q: Will health care workers or other first responders get first access to ventilators?” Here’s the answer: “No. Other guidance documents recommend prioritized access for health care workers and others to vaccines and medicines that prevent influenza, to help protect these workers and keep them on the job. However, people who are sick enough to require ventilators are unlikely to return to work during the acute phase of the epidemic. Also, if ventilators are in very short supply, prioritizing all first responders might mean that no community members, including children, could gain access to ventilators. This guidance document recommends assessing all patients who require ventilators by health criteria only, regardless of job description.” The New York State report concludes that all decisions about ventilator allocation will be made based solely on clinical criteria: “In an overwhelming pandemic with a severe shortage of ventilators and staff to operate them, access to ventilators would depend only on clinical factors, primarily, which patients have the greatest medical need — and the best chance of survival — if they receive ventilator support.”Continued on page 37…

Fully automated critical
care testing. The revolution
is at your fingertips.
Unmatched quality assurance, total remote management and the most accurate results—in a single touch. The GEM Premier 4000 brings complete
automation to the most labor- and skill-intensive tasks in critical care testing. At the touch of
a button, the GEM Premier 4000 automates: quality management through Intelligent Quality
Management (iQM), instrument maintenance with its multi-use disposable cartridge PAK, and
information management with GEMweb Plus connectivity software and automated operator
certifi cation. The GEM Premier 4000—it’s advanced, simple, revolutionary—and leading the
automation revolution in critical care.
Measured Parameters:� Blood Gas: pH, pCO
2, pO
2
� Electrolytes: Na+, K+, Ca++, Cl-
� Metabolites: Glucose, Lactate� Hematocrit� Liver Function: Total Bilirubin*� CO-Oximetry: tHb, O
2Hb, COHb, MetHb, HHb, s0
2
� Renal Function: BUN/Creatinine**
* CE marked. Not currently saleable in US and Canada.** In development
Visit www.ilus.com/GOGEM or contact your local IL sales representative today.
CU
ST:K
HJ 3
96
64
_0
9
D
AT
E:1
2-3
-09
DE
SC
:Ne
on
ata
l In
ten
siv
e C
are
LS
:15
0
39664_09_GEM-176 8_125x10_875 NIC 1 12/3/09 6:57:25 AM
39664_09_GEM-176_8_125x10_875_NIC.pgs 12.03.2009 06:56 BLACK YELLOW MAGENTA CYAN

ISSN 2152-355XPublished six times each year byGoldstein and Associates, Inc.10940 Wilshire Blvd., Suite 600Los Angeles, CA 90024 USATel: 310-443-4109 · Fax: 310-443-4110E-mail: [email protected]: www.respiratorytherapy.ca Video website: www.rttv.caPublisher Steve GoldsteinEditor Les PleskoSenior Editor Carol BrassAssistant Editor Laszlo SandorDesign & Production http://accugraphics.net
Circulation, Coverage, Advertising Rates: Complete details regarding circulation, coverage, advertising rates, space sizes, and similar information are available to prospective advertisers. Closing date is 45 days preceding date of issue.
Change of Address notices should be sent promptly to Circulation Department. Provide old mailing label as well as new address. Allow two months for change.
Editorial Contributions will be handled with reasonable care. However, publishers assume no responsibility for the safety of artwork, photographs or manuscripts. All submissions may be emailed to [email protected]. Every precaution is taken to ensure accuracy, but the publish ers cannot accept responsi bility for the correctness or accuracy of information supplied herein or for any opinion expressed. Editorial closing date is the first day of the month preceding month of issue.
©2010 by Goldstein & Associates, Inc. All rights reserved. Reproduction in whole or in part without written permission is strictly prohibited.
Mohammed Al Ahmari, BSRT, MSc., RRT Prince Sultan Military College of Health Sciences Al-Khobar, Saudi Arabia
Muhammad Aslam, MD Clinical Fellow in Newborn Medicine Harvard Neonatal-Perinatal Fellowship Program Children’s Hospital Boston Instructor in Pediatrics, Harvard Medical School Boston, MA
Larry H. Conway, BS, RRT Chief, Respiratory Care Service VA Medical Center Washington, DC
Ed Coombs, MA, RRT Sr. Marketing Manager–Ventilation Draeger Medical Telford, PA
Antonio Esquinas, MD, PhD, FCCP Intensive Care Unit, Hospital Morales Meseguer Murcia, Spain
Dr. Javier Fernandez Director of Clinical Affairs & Education Respiratory Division Latin America Miami, FL
Gerardo N. Ferrero, PT Clinical Specialist, Latin America Buenos Aires, Argentina
Charles J. Gutierrez, PhD, RRT, FAARC Assistant Chief Neurorespiratory Care Program–Spinal Cord Injury Center James A. Haley Veterans Hospital Tampa, FL
Surinder K. Jindal, MD Postgraduate Institute of Medical Education & Research Chandigarh, India
Scott E. Leonard, MBA, BA, RRT Chief Administrative Director Department of Respiratory Care Services UMass Memorial Medical Center Worcester, MA
Rebecca A. Mabry General Sleep Manager Viasys Healthcare Yorba Linda, CA
Paul Mathews, PhD, RRT, FCCM, FCCP, FAARC, Associate Professor, Respiratory Care, University of Kansas Medical Center Kansas City, KS
Nawal M. Mofarreh MBBS, Arab Board-Internal Medicine I, Cardiac center- Al-Thawra General Modern Hospital, CPR instructor & co-ordinator Saudi Heart Association in affiliation with American Heart Association, CPR center, Al-Thawra Hospital Sana’a-Yemen
Hossein Razavi, MD, FCCP Pulmonary, Critical Care & Sleep Medicine St. Helena, CA
Dr. John H. Riggs, PhD, RCP, FAARC Director of Respiratory Services Mission Hospitals Asheville, NC
Daniel D. Rowley, B.S. RRT-NPS, RPFT, FAARC, Respiratory Therapy Supervisor, Pulmonary Diagnostics & Respiratory Therapy Services, University of Virginia Health System, Charlottesville, VA
J. Kyle Schwab, MD Medical Director Louisiana Sleep Foundation Baton Rouge, LA
Dave Swift, RRT Ottawa Hospital–Civic Site; Campus Coordinator (Professional Practice) & Special Care Nursery Charge Therapist; Respiratory Therapy Team Lead; National Office of the Health Care Emergency Response Team (NOHERT); Subject Matter Expert, Health Canada
Editorial Advisory Board
Only One Medical Gas Company Refuses to Take a BreatherNow, getting heliox to your patients in the emergency room or ICU has never been faster or easier. The Grab’n Go® Heliox unit from Praxair Healthcare Services pro-vides a highly portable means to respond. If you’re also using heliox with a nebulizer, the dual-port design en-ables you to connect to both a mask and a nebulizer.
This heliox unit was inspired by our award-winning Grab ‘n Go family of advanced Medipure® medical gas delivery systems. Praxiar ships more than one million Grab ‘n Go units a year to healthcare facilities throughout the U.S. and Canada. Now you can take advantage of this proven technology for even more therapies.
FREE 3-month trial*Limited time offer
call 1.800.299.7977 today
Praxair, the Flowing Airstream design, Grab ‘n Go and Medipure are trademarks or registered trademarks of Praxair Technology, Inc. in the United States and / or other countries.© Copyright 2010 Praxair Technology, Inc. All rights reserved.
* Subject to contractual availability

PalmSAT® 2500 LifeSense®
Actual size is 7.9 x 5.3 x 2 inches
WristOx® 3100
Avant® 4000
Onyx® II 9550Actual size is 1.4 x 2.3 inches
PureSAT Family Ad.indd 1 12/29/2009 4:47:48 PM

CRITICAL CARE
SERVO-i wNAVA Ad_RespTher_print.indd 1 7/2/08 3:19:00 PM
MAQUET, Inc.45 Barbour Pond DriveWayne, NJ 07470Phone: 888-627-8383Fax: [email protected]
MAQUET Edit DEC09.indd 1 12/30/09 11:24:07 AM

One glance at Salter’s NebuTech® HDN® design tells you that it is truly in a class by itself.
IT LOOKS DIFFERENT BECAUSE IT IS DIFFERENT
Delivers a high density 50cc bolus on inspiration
Faster Treatment Times
Improved Outcomes
Greater Versatility
Eliminate Concurrent Therapy
Eliminate Missed Treatments
For complete information, contact your Salter representative or call 1-800-235-4203
Optional Disposable Filter Set: Reduces second hand aerosol exposure
Exhalation filter minimizes occupational exposure
Filters 99.56% of exhaled particles
Attaches easily to existing one way valves on the NebuTech® HDN® nebulizer
Quality Care Begins With Quality Productswww.salterlabs.com
© copyright 2009, Salter Labs, Arvin, CA

Respiratory Therapy Vol. 5 No. 1 n February-March 2010 11
NewsM February-March 2010
FUNDEDThe National Institute for Health Research (NIHR) is funding Supporter Membership of BioMed Central. The NIHR has agreed on a membership arrangement with BioMed Central to support publication of research articles in the publisher’s open access journals. Under the terms of the NIHR’s Supporter Membership arrangement, all NHS researchers supported by the NIHR and its partners will benefit from a 15% discount on publication fees when publishing in any of BioMed Central’s 200 peer-reviewed open access journals. Researchers are expected to acknowledge NIHR support. With support through the NIHR, researchers already publish hundreds of open access articles each year in BioMed Central’s journals, and Supporter Membership will further encourage open access publication, increasing public access to the results of taxpayer funded research while saving money. A list of open access articles by NIHR-funded researchers recently published in BioMed Central journals can be found at biomedcentral.com. In other BMC news, BioMed Central is once again publishing the Journal of Medical Case Reports (JMCR) and Cases Journals. Since their inception both of these journals, which currently provide over 2,000 freely accessible case reports have received widespread recognition and high quality submissions from across the medical community. Through their innovative approach, both these journals make each individual patient’s case a valuable addition to medical literature. BMC also reported that Nobel laureates and scientists collaborated by lobbying Congress through an open letter. The legislation seeks to enhance access to federally funded published research articles, ensuring they are made available in an online repository no later than 6 months after publication… EvoDevo is a new journal on evolutionary developmental biology, now open for submissions… BMC Health Services Research has published the abstracts, Patient Classification Systems International: 2009 Case Mix Conference Fukuoka, Japan… BMC Bioinformatics has published a collection of articles from Biodiversity Informatics… BMC Pharmacology has published the abstracts from the 15th Scientific Symposium of the Austrian Pharmacological Society (APHAR)… Malaria Journal has published a collection of reviews… BMC Pulmonary Medicine (2009, 9:45) has published Oral administration of geranylgeranylacetone, an anti-ulcer drug.
LIVE OR DIEThe CDC debated who gets ventilators for swine flu, according to website Politico. The issue was debated by a CDC ethics advisory panel. There has been some recent concern about ventilator shortages, in light of the H1N1 outbreak, and possible future pandemics. Reported by Josh Gerstein, Politico.
CLINICAL TRIALSThe Huffington Post reports on investigations of clinical trials. Federal regulators, the Post reports, are looking into trials at
various universities and have recently cited some for mistakes in clinical trials which have injuried or killed patients. A review by the Hastings Center concluded that human subjects are not well protected, and pointed up weaknesses in safeguards, specifically in the procedures for obtaining informed consent. Collaboration between industry and academic institutions to test drugs and medical devices has increased at such a rate in the past decade that oversight panels are hard pressed to fully review all such trials. The gaps mean that a medical product may receive federal approval and be marketed without regulators or doctors being aware of limitations and biases in its testing history. Vulnerabilities in the oversight system have led the Obama administration to appoint a well-known bioethicist to take a look. The ethicist has argued that patients are often not fully informed or protected when they sign consent forms. He said the notion remains that to have the appropriate amount of research, researchers need to deceive many patients when they are being asked to participate in clinical trials. About 300,000 studies with 7 million human subjects are conducted each year in the US. No government agency or private entity tracks these numbers closely, though there are 4,000 institutional review boards in the country, reviewing dozens to hundreds of proposals each year. Patient protection runs on the honor system. Everything’s presumed to be okay unless there’s a complaint, and review boards, which operate behind closed doors, tend to trust researchers, according to the federal Office of Human Research Protection. Because universities are in collaboration with the healthcare industry, clinical trial divisions are often organized like their commercial counterparts, and as such, some say, members of review boards are loathe to interfere with their colleagues, who are often prominent faculty members, especially insofar as research brings money to universities. This article is based on a report by The Huffington Post, by Jeanne Lenzer, an independent medical investigative journalist and a frequent contributor to BMJ, and Shannon Brown, the author of Overtreated: Why Too Much Medicine is Making Us Sicker and Poorer.
FEEELINGSA recent survey of patients with COPD and their caregivers found, unsurprisingly, that patients feel better about themselves when their disease is managed properly. In a telephone survey, 400 patients and 400 caregivers were asked about their thoughts on nebulization therapy and how they manage their COPD. Well-informed patients with self-reported, moderate breathing conditions were most likely to have high levels of satisfaction with their current mode of therapy. Nine in 10 patients who use nebulizers reported satisfaction with their current treatments, and caregivers were significantly more likely than patients to wish that those they cared for had been placed on nebulization therapy sooner. Patients and caregivers reported that the benefits of nebulization — mainly the perception of easier and more comfortable breathing — outweigh any challenges or constraints. Eighty percent preferred using a nebulizer over only an inhaler; 68% reported easier breathing as the most positive aspect of nebulization therapy, and 86% reported a more comfortable feeling in their chest as a result of their nebulizer use; 25% of patients cited the immobility of the nebulizer as a disadvantage.
READ ALL ABOUT ITThe European Federation of Allergy and Airways Diseases Patients Associations launched a book comparing and analyzing COPD in Europe from the patient’s perspective. The “EFA Book

12 Respiratory Therapy Vol. 5 No. 1 n February-March 2010
on COPD in Europe. Sharing and Caring” highlights the need to reduce the suffering and mortality from COPD, which is predicted to be the third leading cause of death worldwide by 2030. The book stresses that the misclassification and different definitions of COPD throughout Europe lead to underestimations of the actual impact of the disease. The authors noted that patient associations reported access to early diagnosis of COPD as difficult or very difficult in their countries. Even when it’s diagnosed, access to programs, treatments, support services and rehabilitation in most countries is reported to be problematic. In Austria for example, only hospitalized patients undergo rehab and there is a long waiting list. The total financial burden of COPD in Europe is estimated to be over 50 billion euros and is expected to increase. COPD often leads to work absenteeism and loss in productivity, which, for example, accounts for 67% of overall costs in France and 50% in the Netherlands. The book calls on the EU Commission to establish a framework for sharing best practices on COPD management by the end of this year.
CELEBRATIONSaint Joseph Medical Center in Lexington, KY recently celebrated National Respiratory Care Week, in October. The department reported growth in 47 years from an Inhalation Department to a large Respiratory Care Department, with 35 full time employees, ten of whom have worked 20-plus years at the facility, with one employee who’s been there 41 years. Eighteen therapists are part of the Rapid Response Team, comprising trained intubators who partner with crit care nurses. Saint Joseph Medical Center in Stockton, CA, which ensures that RCPs are available at all times, had staff lunches for its caregivers. Castle Medical Center in Kailua, HI, celebrated by holding an Identify the Respiratory Therapist contest, and hosted a breakfast. Florida Hospital in Orlando, which started a century ago as a 20-bed cottage, hosted lectures on respiratory therapy topics. Hamilton Medical has partnered with hospitals for 25 years to offer respiratory therapy. Information above was provided by Hamilton Medical.
PARTNERSHIPResMed and Philips Respironics announced a joint undertaking to educate primary care physicians about untreated sleep apnea through CME programs funded by educational grants. Programs are being provided through Primary Care Network and Pri-Med Institute in 17 US cities. The goal is to educate 7,200 clinicians by June of this year. Primary care, family practice, and internal medicine doctors, along with nurse practitioners and physician assistants are being presented information about symptoms of sleep apnea, screening implementation, diagnostic pathways, therapy and the latest research on the association of mortality and morbidity with untreated sleep apnea, and can earn 1.25 CME credits per program. Close to 2,000 participants joined to learn more about sleep apnea in the first go-round. Upcoming sessions offered by Primary Care Network will be held in March in New York, in April in Philly, and in June in Orlando (primarycared.com); Pri-Med Institute is presenting sessions in Houston in March, Anaheim in May, and June in New York (pri-med.com). For more contact resmed.com.
RATSAn international team of scientists led by Dr Bernard Thébaud, neonatal specialist at Alberta Health Services, has demonstrated that stem cells protect and repair the lungs of newborn rats. Thébaud’s team simulated the conditions of prematurity, giving the newborn rats oxygen. The scientists then took stem cells,
derived from bone marrow, and injected them into the rats’ airways. Two weeks later, the rats treated with stem cells were able to run twice as far, and had better survival rates. When Thébaud’s team looked at the lungs, they found the stem cells had repaired them and had prevented further damage. The research team included physicians and scientists from Canada, France, and the US. The team is investigating the long-term safety of using stem cells as a lung therapy. The scientists are examining rats at 3 months and 6 months after treatment, studying the lungs, and checking organs to rule out any risk of cancer. Thébaud’s team is also exploring whether human cord blood is a better option than bone marrow stem cells in treating lung disease, and are also studying the healing liquid produced by the stem cells, to see if it can be used on its own to grow and repair the lungs, which would make stem cell injection unnecessary. The study is: Airway Delivery of Mesenchymal Stem Cells Prevents Arrested Alveolar Growth In Neonatal Lung Injury In Rats, available at ajrccm.atsjournals.org/current.shtml.
FEARFUL VERMINThe portion of our brains that is responsible for registering fear and panic has a built-in chemical sensor triggered by the primordial terror of suffocation. Studies of mice at the U of Iowa have shown that the rise in acid levels in the brain when breathing carbon dioxide triggers the acid-sensors that evoke fear behavior. The findings may explain what happens in people who suffer panic attacks, especially given that breathing carbon dioxide can trigger the attacks. The relevant circuit is in the amygdala, which triggers fight-and-flight. Researchers posited that a reduced pH might induce fear behavior. In the study, mice breathing 5% carbon dioxide avoided open spaces and displayed exaggerated freezing behaviors. Treatments that prevented the pH change reduced fear behavior, while acidic microinjections into the amygdala did just the opposite. The results also give a molecular explanation for how rising carbon dioxide concentrations elicit intense fear and provide a foundation for dissecting the bases of anxiety and panic disorders. A single breath of carbon dioxide can trigger panic attacks in patients with panic disorder, and disregulated brain pH has also been implicated in the condition. In addition, patients suffering from respiratory failure are also known to become extremely anxious.
LARGER ANIMALSA research team at the University of Rostock in Germany evaluated the feasibility and efficacy of autologous umbilical cord blood mononuclear cell (UCMNC) transplantation on right ventricular function in a large animal model of chronic RV overload. Their study examined the potential therapeutic role of UCMNCs in treating one of the most common cyanotic congenital heart defects in the Tetralogy of Fallot (TOF), a group of congenital heart defects. Transplant was found to enhance diastolic properties, likely through angiogenesis. The authors noted that UCMNCs have already been shown to be therapeutic agents in patients with hematological disorders. They concluded that UCMNC transplantation was feasible and safe and seemed to positively influence the diastolic properties of the RV under chronic volume overload. Three months post-transplantation into sheep, the researchers were able to observe an alteration in the RV function, which is one of the long-term determinants of morbidity and mortality after TOF correction.
RATS & TRANSPLANTSTransplanted human-derived umbilical cord blood stem cells transplanted in an animal model had positive therapeutic

Respiratory Therapy Vol. 5 No. 1 n February-March 2010 13
effects on specific lung and heart disorders the animal models, in a study at Samsung Medical Center in Seoul. Researchers investigated the therapeutic benefits of transplanting UCB mensenchymal stem cells (MSCs) into newborn laboratory rats with oxygen-deprived lung injury, and found that MSCs have a protective effect against hyperoxia-induced lung injury, likely due to anti-inflammatory effects. The researchers noted that their findings are expected to have important therapeutic potential for BPD in premature human infants. The optimal route for transplantation had not previously been determined. The intratracheal, rather than the intraperitoneal transplantation of human UCB-derived MSCs significantly attenuated the hyperoxia-induced lung injury, such as decreased alveolarization and fibrosis. Survival rate was not improved by the MSC transplants, however. Questions remain over whether the donor cells exert a therapeutic effect by inducing direct tissue repair and regeneration of damaged cells, said the researchers.
RESEARCH, EH?The Canadian Lung Association and the Canadian Thoracic Society have launched the development of a national research agenda that aims to prioritize areas of significant need as it relates to the treatment and management of lung disease. At least 6 million Canadians, one out of five, suffer from asthma, COPD, lung cancer, sleep apnea and other forms of lung disease. According to the WHO, Canada has one of the highest rates of asthma in the world, 15.6% among children aged 4 to 11 and 8.3% of Canadians 12 years of age or older. Three million Canadians may have COPD, which is projected to be the third leading cause of death worldwide by 2030. The estimated cost of respiratory diseases in Canada is over $12 billion annually.
ANOTHER CHOICEChest ultrasound can be a viable alternative to chest CT in the evaluation of pediatric patients with complicated pneumonia and parapneumonic effusion, according to a study at Albert Einstein College of Medicine and Montefiore Medical Center in the Bronx. Chest CT and chest ultrasound was performed on 19 children with complicated pneumonia accompanied by parapneumonic effusion. Results showed that chest CT did not provide additional clinically useful information that was not also seen on chest ultrasound. Although chest CT allows rapid image acquisition, the rising use of CT in the pediatric population has raised concerns about the ionizing radiation burden. Other benefits of chest ultrasound were said to be its portability and no need for sedation.
HORSING AROUNDPeople working with horses may be at risk for developing respiratory symptoms because of the air in horse barns, according to a study at Tuft University’s Cummings School of Veterinary Medicine. The study polled more than 80 New England horse barn workers and found that half complained of coughing, wheezing, or other ailments in the last year, compared to just 15% in the control group of 74 people. Exposure to barns also yielded higher rates of self-reported respiratory symptoms. Researchers said the results may be similar among pig, dairy and chicken farmers, who work in environments similarly high in organic dust. A 2001 study of European animal farmers found similar results.
COUGH IT UPScientists at the Imperial College of London and the University of Hull have identified the reaction in the lungs when they’re
exposed to environmental irritants such as air pollution and cigarette smoke and cause people to cough. The study showed that irritants can switch on TRPA1 receptor proteins on the surface of nerve endings in the lungs, thus switching on sensory nerves which trigger the cough reflex. As such, coughing could potentially be treated by blocking these receptors. Researchers first looked at sensory nerves from mice, guinea pigs and humans, and showed that the receptors on the nerves were activated by, among other things, a key compound in cigarette smoke, acrolein, and cinnamaldehyde. The researchers then blocked the receptors and showed that these substances no longer activated the nerves. The researchers were able to stop coughing in guinea pigs. For people research, ten healthy non-smokers inhaled cinnamaldehyde and their cough response was measured. All the subjects coughed.
SAD SOUGHINGDepressed moms can worsen asthma symptoms in their kids, according to researchers at Johns Hopkins. Data from interviews of 262 black children with asthma (who are disproportionately affected), found that kids with depressed moms had more frequent asthma symptoms. But while maternal depression aggravated a child’s asthma, kids with asthma didn’t make the moms depressed. Past studies have shown that kids with chronic health conditions fare worse if their primary caregiver is depressed, but it’s been thought to be a chicken and egg situation. Now, researchers, say, they know it’s all the moms’ fault. The next question is why. Researchers posit that because depressed people are tired and can’t concentrate, they don’t pay attention to their kids’ asthma or its treatment.
DON’T STOP!Particles released by car brake pads can harm lung cells in vitro, according to research at the University of Bern and the Institute for Work and Health in Switzerland. Researchers found that heavy braking caused the most damage, but normal braking and even close proximity to a disengaged brake resulted in potentially dangerous cellular stress. Researchers studied the effects of brake particles on cultured lung cells placed in a chamber close to the axle of a car. The metals in brake wear particles were found to damage junctions between cells by a mechanism involving oxidative stress. Brake wear particles contain iron, copper and organic carbon. Exposure to these pollutants caused increased signs of oxidative stress and inflammation in the cells. Some exposure occurred even when the brakes weren’t being applied, due to particles coming off the turning axle and braking system.
SWEET KILLERSSugar-coated polymer strands can selectively kill off cells involved in triggering aggressive allergy and asthma attacks, according to researchers at Johns Hopkins. The scientists have been studying the Siglec-8 protein, which is present on the surfaces of some immune cells, including eosinophils, basophils and mast cells, which have roles in normal immune function and allergic diseases. When functioning correctly, they keep the body healthy and infection-free, but during allergic reactions, they respond in a way that causes damage. Researchers found that when they bound antibodies that specifically target Siglec-8 to the protein on eosinophils, the cells died, an effect they thought could be useful in stemming an allergy or asthma attack, but producing antibodies was expensive, so another way was sought to activate the protein. The team developed soft, flexible polymer strands coated with the sugar-like microscopic spaghetti

14 Respiratory Therapy Vol. 5 No. 1 n February-March 2010
candy, then tested whether the polymer bound when applied to the Siglec-8 cells. The researchers added the polymer to vials of whole human blood and found that the polymer only attached to eosinophils. The polymer killed about 65% of the eosinophils over 72 hours, not quite as effective as the antibody, which killed up to 90% in 24 hours. The researchers will try more rigid polymers with denser sugars, or nanoparticles coated with the sugars.
UH OHA new study on pediatric H1N1 influenza admissions at The Hospital for Sick Children in Toronto found that asthma is a significant risk factor for severe disease in children with the pandemic compared with the seasonal flu. Researchers reviewed the charts of 58 children and compared them to 200 children admitted with seasonal influenza. Twenty-two per cent of kids admitted with H1N1 had asthma compared with 6% admitted with seasonal influenza. Almost half of all admissions to the ICU for H1N1 influenza were children with asthma. The children with H1N1 influenza were older than those admitted for seasonal flu, with significantly more over the age of 5 years. Eighty-four percent presented with fever and cough, with or without additional symptoms and 37% had gastrointestinal symptoms. The median duration of hospital stay for both H1N1 and seasonal influenza was 4 days. None of the children with pandemic influenza died.
GET IT IN QUICKResearchers at Johns Hopkins showed that a comprehensive program designed to help physicians quickly identify and treat anesthetized patients for whom tube placement is difficult reduced the need for high-risk emergency surgical procedures to open obstructed airways. The program enlists a rolling cart with all the supplies a physician needs to navigate a difficult airway, including flexible scopes, long catheters, medications and a surgical airway kit. The standardized cart cuts out the need for operating room staff to run around looking for gear during an intubation emergency. Before the program was instituted, 6.5 patients a year needed to have their airways opened surgically. Over the 11 years that the cart has been in operation, just 2.2 patients a year needed the emergency procedure. In the past year, no patients needed unplanned emergency airway surgery. Doctors have also been shown how to identify patients with potentially life-threatening obstructions, and this information is recorded in the patient’s health record. The decrease in surgical airway procedures came about despite more patients with problem airways.
TAKE IT EASYPharmacists can make sure they don’t over-dispense and patients don’t over-use asthma medications without endangering patients, according to a study by Medco Health Solutions. Its study revealed that when physicians were provided with educational materials and a series of follow-up communications outreach that included information about the consequences of excessive use of rescue inhalers, and required a physician response before a new prescription was dispensed, the number of new prescriptions written for excessive quantities of inhalers dropped by 60%. Two hundred thousand fewer inhalers were used over a one-year period by 250,000 asthma patients identified as being prescribed excessive quantities of rescue inhalers. The adjusted savings from this reduction amounted to $4.2 million.
ALARM APPSResearchers at Tampere University of Technology and the University of Helsinki are utilizing a way to analyze snoring sounds by using a PC with a microphone connection and a wireless microphone, to be used as a home monitor to record snoring. By using this technology, by MScTech Väinö Virtanen, researchers have investigated sleep disorders and refined related screening technologies. A new product based on the technology, a smart alarm clock, HappyWakeUp, was launched last year. It’s billed as the first health-promoting mobile phone application in the world. Users can record their sleep all through the night with a mobile phone or an MP3 player. The microphone is placed in the bed to record the sounds produced by the sleeper’s movements. The storage capacity of applicable devices can record data for over 10 nights, which is transferred to a home PC for analysis and output. The analysis software is available at sleeprecording.com, and a basic analysis is free. An analysis of seven nights costs 10 euros, which is a hundred times cheaper than any other method of sleep measurement. The developers of the software, HomeSleep, noted that at-home screening isn’t meant to substitute for diagnosis by a medical professional. The smart alarm clock HappyWakeUp can be installed on Nokia mobile phones and on iPhones. Contact happywakeup.com, and for the software, sleeprecording.com.
FLATHEADResearchers at Arizona State University have analyzed a database of 20,000 kids and found that the number of babies who have developed deformational plagiocephaly has dramatically increased since 1992. The increase coincides with the AAPs “Back to Sleep” campaign that recommended parents place their infants on their backs to reduce the risk of SIDS. The largest factor in flat-headedness was the sleep position of the baby, and comes from babies spending too much time in one position. Babies who slept on their right-side or left-side tended to have right-side and left-side flat spots, respectively. The study also found that boys were twice as likely as girls to have the condition and it was also more common in firstborn infants, babies with low birth weight, in breech and transverse positions in the womb, and in fraternal twins. The research was by Jessica Jorganic, for her undergrad honors thesis. She’s pursuing a doctorate in physical anthropology at St Louis’s Washington University.
WHAT A JOBResearchers at The University of Queensland and Brisbane have spent hours analyzing snoring sounds, and the result is a noninvasive way of diagnosing OSA, which features snoring as its earliest symptom. The researchers said they can screen for OSA with a 90% sensitivity and specificity, validating the viability of a snore-based, non-contact OSA screening device, thus negating the need for PSG, which requires a lab stay and costs more money. The home screening method will likely be available within the next two to five years. Researchers said their work will probably also result in a standard treatment for OSA that measures efficacy using breathing sound analysis, thus revolutionizing the diagnosis and treatment of sleep apnea.
A CASE OF NERVESWomen with asthma are more anxious, find it harder to sleep and are more tired during the day than men, according to a study at the University of Gothenburg and Sahlgrenska University Hospital in Sweden. However, women are still better at following their treatment protocol. Women with asthma feel worse than

Respiratory Therapy Vol. 5 No. 1 n February-March 2010 15
men, and believe more strongly that they’re limited by their condition. The study is the thesis for a PhD in medicine by Rosita Sundberg, registered nurse, titled, “Quality of life, school performance, treatment adherence and gender differences in asthma.” See hdl.handle.net/2077/21259.
TURKEY TIMEMelatonin is a good replacement for somniferous to correct the sleep/wakefulness pace when human biological clock becomes altered, according to researchers at the University of Granada. Melatonin, the so-called “hormone of darkness,” is used by pharmaceutical companies to design synthetic medicines. The researchers found that melatonin is very effective but only if taken at certain hours of the day, and that if it didn’t work, it was because it was administered at the wrong time. The ability of melatonin to readapt the biological clock had previously been studied in blind people, since they can’t activate the endogenous pacemaker secreted by melatonin at night. The administration of melatonin every 24 hours (1-10 mg/day) re-established the pace in these subjects. Researchers also found that melatonin can slow cell ageing, and can slow cell death caused by sepsis.
UPDATES FROM CHEST 2009Some papers presented at CHEST 2009: Children With Asthma May Benefit From Reduction in Daily Steroids: Children with status asthmaticus may be able to safely reduce their daily corticosteroid dose. Researchers from Kosair Children’s Hospital in Kentucky conducted reviews of 292 patients young patients and concluded that decreasing the daily dose of systemic corticosteroids didn’t affect the length of hospital stay. High-Dose Inhaled Albuterol Associated With Metabolic Acidosis: Patients with severe acute asthma may be at a higher risk of developing metabolic acidosis. In a retrospective analysis, researchers from Yale reviewed demographic and physiologic data of 201 pediatric patients admitted with a diagnosis of severe acute asthma. Results showed that heart rate and respiratory rate were higher in patients receiving high-dose albuterol, and 14 patients developed metabolic acidosis. Thirteen patients receiving high-dose albuterol developed metabolic acidosis compared with one patient receiving low-dose inhaled albuterol. There was no difference between age, gender, duration of symptoms before hospital presentation, and pediatric risk of mortality score between patients on high-dose and low-dose albuterol. Tonsil Size May Predict Sleep Apnea in Kids: Children with large tonsils may be at an increased risk of developing obstructive sleep apnea-hypopnea syndrome. Researchers from the Philippines assessed the link between obesity and OSAHS in 285 children who snored. Of the patients, 118 patients were found to be obese. Among these, 34% had OSAHS, while 50% of patients who were not obese also had the condition. Results indicated that the BMI Z-score did not demonstrate a significant risk factor or predictor for the presence and severity of OSAHS. Yet, tonsillar size, apneas in the sleep history, and nasal congestion due to allergic rhinitis were found to be significant risk factors for the presence of OSAHS.
GRINDHOUSEBruxism is highly prevalent in patients with OSA, especially among white males, according to researchers at Baylor College of Medicine, Houston. One in 4 patients with OSA suffer from nighttime teeth grinding. Researchers noted that the relationship between obstructive sleep apnea and sleep bruxism is usually related to an arousal response. The ending of an apneic event may be accompanied by a number of mouth phenomena, such
as snoring, gasps, mumbles, and teeth grinding. Men typically have more severe sleep apnea, and thus may have more arousal responses, ergo, the teeth grinding. Also, researchers noted, men tend to report more symptoms like snoring and grunting. Others factors, the researchers posited, could be anxiety and drinking lots of coffee. Researchers assessed the prevalence of bruxism and GERD in 150 men and 150 women with OSA. Each group consisted of 50 whites, 50 blacks and 50 Hispanics. Results showed that 25.6% suffered from teeth grinding, while 35% with OSA complained of nocturnal heartburn and GERD symptoms. Bruxism was at 43% in men and 31% in women. Caucasians had the highest rate, 35% vs 19% in Hispanics. Blacks had the highest prevalence of GERD, 40% vs 31% in Hispanics and 34% in whites.
FORE-PLAYGolfers who undergo treatment for sleep apnea may improve their golf game, too, according to a study by Atlantic Sleep and Pulmonary Associates, Madison, NJ. Golfers with OSA who received NPAP improved their daytime sleepiness scores and lowered their golf handicap by as much as three strokes. Researchers suggest that the possibility of improving one’s golf game may be a significant motivator to improve NPAP compliance rates among golfers. According to the chief researchers, OSAS can affect the intellectual acumen of golfers, perhaps more than the smarts of participants in dumber sports. Researchers, apparently with time on their hands, evaluated the impact of NPAP on the golf handicap index (HI) of 12 golfers with moderate to severe OSA. HI was recorded upon study entry, as was the Epworth sleepiness scale, and the results of a sleep questionnaire developed by the researchers. After 20 rounds of golf while receiving NPAP treatment for 3 to 5 months, the treatment group demonstrated a significant drop in average HI, 12.4 to 11.0. Patients in the study group also improved their ESS score, 11.8 to 5.5. A control group of 12 subjects demonstrated no change in HI, ESS score, or SQ score during this study. Results of the study also showed that the best golfers, defined as HI <12, had the biggest improvements in their game. The researchers noted that the biggest handicap improvements occurred in the lower handicap, often among older golfers, a group that might be expended to trend in the opposite direction due to their age and its related deterioration in endurance and strength. Researchers noted that there were likely up to 3 million golfers playing 10 or more rounds per year who have OSA, that most of these players were undiagnosed or untreated, and noted that the chance to improve their game might prompt them to take some action.
GO AHEAD, QUITRetirement leads to a decrease in sleep disturbances, according to a study by the University of Turku in Finland. The odds of having disturbed sleep in the seven years after retirement were 26% lower than in the seven years before retiring. Sleep disturbance prevalence rates among 14,714 participants in the study fell from 24.2% in the last year before retirement to 17.8% in the first year after retiring. The greatest reduction in sleep disturbances was reported by participants with depression or mental fatigue before they punched their final time clock. The postretirement improvement in sleep was also more pronounced in men, management-level workers, employees who reported high psychological job demands, and people who worked night shifts. The authors noted that the study used data from a recent time when workers had job stability, a retirement age between 55 and 60, and a decent pension that hadn’t been trashed by their companies. The study involved employees from the French

16 Respiratory Therapy Vol. 5 No. 1 n February-March 2010
national gas and electricity company, who retired between 1990 and 2006 at a mean age of 55 years and included data from 11,581 male and 3,133 female workers who reported sleep disturbances at least once before and once after the year of retirement. Thirty-five percent of participants had worked night shifts, and 17% reported having depression. The only exception to the general improvement in sleep after retirement was related to the 4% of participants whose retirement was based on health reasons, who had a 46% increased risk of sleep disturbances after retiring. For the full study, see the journal Sleep, Effect of Retirement on Sleep Disturbances: the GAZEL Prospective Cohort Study. Reported in Medical News Today.
TIOTROPIUM STUDYPresented at the CHEST 2009 Annual Meeting was the following paper: Long-Acting Bronchodilator Treatment Type and COPD-Related Inpatient Admission in a Commercially Insured Population.” Background & Objectives: COPD-related inpatient admission accounts for a substantial proportion of the cost of care for COPD. Hospitalization is often a consequence of an acute exacerbation event. Long-acting bronchodilator (LABD) treatment is associated with fewer exacerbations and hospitalizations. The objective of this study was to evaluate the relationship between LABD treatment type and COPD-related inpatient admission. Study design: Review of a database, collected by the MarketScan Research, Databases of Thomson Reuters — sample selection: ages 35 and older; diagnosis of COPD on either 2 outpatient, or 1 inpatient or 1 emergency department visit; at least 1 prescription claim for an LABD between 2004 and 2006; 6 months of continuous health plan enrollment prior to index; 12 months of continuous health plan enrollment. The sample was classified into 5 cohorts based on index LABD regimen: 1. Tiotropium (Spiriva), 2. Salmeterol/fluticasone propionate, 3. Formoterol fumarate, 4. Salmeterol, 5. Combination therapy with 2 or more LABDs. All variables were examined descriptively by index LABD regimen. Multivariate logistic regression analysis was used to evaluate the relationship between index LABD regimen and COPD-related inpatient admission, adjusting for demographic and pre-period clinical characteristics. Tiotropium monotherapy was the reference group. Odds ratios and 95% confidence intervals of other treatment regimens were computed. The significance of the coefficients was tested using two-sided t- tests. The results showed that following adjustment for differences in patient demographic and clinical characteristics, the risk of COPD-related IP admission varies by LABD treatment type. COPD patients treated with salmeterol/fluticasone propionate, formoterol fumarate, salmeterol, and combination LABD therapy were more likely than those treated with tiotropium monotherapy to have an COPD-related inpatient admission during follow-up. The above information was provided by Ogilvy PR for its client, Spiriva.
COPD STUDYA new post-hoc, pooled analysis of the serial spirometry subset of the pivotal efficacy and safety trials, SHINE and SUN, demonstrated that a large percentage (51.8%) of patients with moderate to very severe COPD receiving two inhalations of Symbicort (budesonide/formoterol fumarate dihydrate) Inhalation Aerosol 160/4.5 mcg showed improvement of airflow obstruction on day of randomization, as evidenced by the American Thoracic Society (ATS) criteria. The analysis found that Symbicort 160/4.5 mcg demonstrated improvement in airflow obstruction (within 30 minutes postdose) in a large percentage
(51.8%) of patients with moderate to very severe COPD based on ATS criterion on the day of randomization. At screening, 39.2% of the patients who were subsequently randomized to Symbicort 160/4.5 mcg demonstrated reversibility by ATS criteria when tested within 15-30 minutes after receiving two inhalations of albuterol 90 mcg. The onset of bronchodilation, based on a ≥15 percent improvement from baseline in FEV1, was rapid (within 5 minutes) with Symbicort 160/4.5 mcg on the day of randomization, and this effect was maintained at the end of six months. Symbicort does not replace fast-acting inhalers and should not be used to treat acute symptoms of COPD. Data were pooled from the serial spirometry subset (n=1,109) and analyzed from common treatment arms within SHINE (6 months, 1,704 patients) and SUN (12 months, 1,964 patients) — which are randomized, double-blind, multicenter efficacy and safety trials that evaluated more than 3,600 patients ages 40 years and older with moderate to very severe COPD. After two weeks of treatment based on previous therapy (inhaled corticosteroids and short-acting bronchodilators were allowed), patients were randomized to receive two inhalations of one of the following twice daily: Symbicort pMDI 160/4.5 mcg (the FDA-approved dosage for COPD), Symbicort pMDI 80/4.5 mcg, formoterol DPI 4.5 mcg or placebo, which were the common treatment arms within the trials. On the day of screening, FEV1 was measured predose and 15-30 minutes after two inhalations of albuterol 90 mcg. Airflow obstruction for albuterol was assessed based on the proportion of patients who achieved ATS criterion 15-30 minutes postdose on the screening day. Airflow obstruction for the study medication was assessed based on the proportion of patients who achieved ATS criterion within 30 minutes postdose on the day of randomization. Patients refrained from using treatment before testing for ≥6 hours for albuterol, ≥8 hours for ipratropium and ≥48 hours for long-acting bronchodilators. Additionally, the study assessed the median time to onset of bronchodilation, or opening of the airways, which was defined as the point at which ≥50 percent of patients achieved a ≥15 percent FEV1 improvement, after dosing on the day of randomization and at the end of six months. For more contact AstraZeneca, (800) 236-9933.
APPROVALDiscovery Laboratories, Inc announced that it has submitted to the FDA its proposed protocol for a Surfaxin (lucinactant) limited clinical trial. The protocol incorporates a clinical trial design that is primarily intended to assess a pharmacodynamic response following Surfaxin administration in preterm infants with RDS. Discovery Labs proposed this trial design in response to a comment by the FDA that a limited clinical trial could potentially resolve the key remaining issue for approval of Surfaxin for the prevention of RDS in premature infants. Discovery Labs received a Complete Response Letter for Surfaxin in the spring of last year, and the FDA suggested that, to increase the likelihood of gaining Surfaxin approval, Discovery Labs could consider conducting a limited clinical trial. In the fall, Discovery Labs held a teleconference with the FDA to discuss, among other things, whether a PD approach would satisfy the FDA’s requirement for a limited clinical trial. Typically, PD-based clinical trials primarily assess short-term, physiologic responses to therapy and, therefore, are generally less expensive and of shorter duration than trials that have clinical outcomes as a primary endpoint. The FDA indicated that Discovery Labs’ proposed concept of a PD trial design is acceptable and also provided direction regarding certain trial design specifics. Employing the FDA’s guidance, Discovery Labs worked closely

Respiratory Therapy Vol. 5 No. 1 n February-March 2010 17
with leading academic neonatologists to design the PD protocol. The final protocol and clinical trial design is subject to FDA review and comment.
VICTORIOUSFollowing a three-week trial, a California federal jury recently awarded a victory to Nova Biomedical Corporation against Medtronic MiniMed, Inc, which had brought claims against Nova for misappropriation of trade secrets, breach of contract, tortuous interference and conversion. Medtronic MiniMed had sought actual damages of over $30 million, a permanent injunction, a finding of willful misappropriation and punitive damages. The lawsuit centered around Nova’s introduction of the Nova Max Link blood glucose meter, which is used by diabetics to measure their blood glucose levels, and can wirelessly communicate a patient’s blood glucose level to Medtronic’s Paradigm-series insulin pumps. The jury verdict is the culmination of almost two years of litigation in which Medtronic alleged that the Nova Max Link meter’s wireless communication features used Medtronic’s trade secrets. The jury said, no. The above information was provided by Nova Biomedical,. For more contact novabio.com.
PRODUCTS AND COMPANIES
SUPPORTDräger and ICON are providing clinical support services for H1N1 caregivers. Dräger and Intensive Care On-line Network (ICON) have agreed to provide clinical services to any hospital managing an H1N1 patient on APRV or APRV-like ventilation (ie, Bi-Vent, Bi-level, etc). Ed Coombs, associate director of marketing for respiratory care at Dräger stated, “As a world leader in mechanical ventilation, Dräger wants to do everything possible to help support the medical and respiratory care communities in the wake of the H1N1 flu pandemic.” Typically, ICON services are exclusive to Dräger ventilation customers; however, this pandemic is nationwide and shared expertise is required to improve overall outcomes. As a result of this critical situation, ICON has agreed to provide any hospital which uses other brands of mechanical ventilators access to ICON’s 24x7 call center to discuss patients clinically diagnosed with the H1N1 virus via real-time RT-PCR. The American Thoracic Society has posted “Guidelines for Alternative Modes of Ventilation Used in the Management of Patients with ARDS Secondary to H1N1 Infection.” These guidelines include the mode Airway Pressure Release Ventilation (APRV). ICON’s team of clinical specialists has extensive experience with APRV. The clinical team at ICON includes nurses, respiratory therapists, pharmacists, and physicians — all of whom can provide guidance and support during this pandemic including direct physician to physician consultation, said Penny Andrews, RN, Chief Operations Officer of ICON. ICON currently maintains a 24x7 clinical support call center to assist with troubleshooting and support of all Dräger mechanical ventilators. Caregivers who wish to take advantage of this support service can call (888) 404-ICON. Contact draeger.com.
ALL SETMasimo announced that Brookdale University Hospital and Medical Center in Brooklyn has completed its system-wide conversion to Masimo SET pulse oximetry technology. As part of its system-wide technology standardization, Brookdale has also installed first-ever continuous and noninvasive hemoglobin
monitoring (SpHb) technology in select care settings — allowing clinicians to detect and treat chronic or acute anemia earlier, identify internal bleeding sooner, and more effectively manage blood transfusions for their patients. By converting to Masimo SET, Brookdale clinicians gain all the Measure-Through Motion and Low Perfusion benefits of Masimo SET pulse oximetry, along with the breakthrough noninvasive blood constituent monitoring capabilities of Masimo Rainbow SET Pulse CO-Oximetry. Masimo Rainbow SET is the first and only technology platform capable of continuously and noninvasively measuring multiple blood constituents that previously required invasive procedures, including: total hemoglobin (SpHb), oxygen content (SpOC), carboxyhemoglobin (SpCO), methemoglobin (SpMet), and PVI, in addition to oxyhemoglobin (SpO2), pulse rate (PR), and perfusion index (PI). The ability to immediately detect and treat potentially life-threatening conditions, without having to draw blood and wait for the results, enables earlier and better clinical decisions that may help save lives and improve patient outcomes. The Brookdale University Hospital and Medical Center is one of Brooklyn’s largest voluntary nonprofit teaching hospitals with 530 inpatient beds. Contact masimo.com.
ADVENT-UREAdvent Product Development offers the Timer For Nebulizer Compressor, a modification to the design of nebulizer compressors comprised of a simple timer mechanism connected to an automatic shutoff valve. The Timer for Nebulizer Compressor will keep the machine from overheating and times out after a specified period set for the required treatment. The timer is activated and automatically shuts off the nebulizer, preventing it from overheating when the session is complete. The Timer was invented by Jesus Padilla of Rialto, CA, a respiratory therapist. To view a graphic of the Timer For Nebulizer Compressor, along with more information, go to adventproduct.net/24983/default.htm.
SERVICESiemens won a $135 million service contract from The University of Pennsylvania Health System. Over the next seven years, Siemens will be servicing and ensuring around-the-clock availability of diagnostic systems and biomedical devices from diverse manufacturers in the U of PA’s various hospitals. The diagnostic systems involved include MRI scanners, CT scanners and ultrasound systems, laboratory systems, surveillance monitors and anesthesia units. Constant monitoring makes it possible to prevent or repair faults without having to dispatch a service engineer to the installation site. Another important aspect of Integrated Service Management is that Siemens provides consulting services to the clinic on workflow optimization and offers advanced training for service engineers and operating personnel. The new contract represents a continuous extension of the preceding eight-year service agreement. Contact usa.siemens.com.
THE EAR WHISPERERBunnell Incorporated announced a sound reduction upgrade for the Life Pulse High-Frequency ventilator. The upgrade reduces sound output from an average 56 dB to 41 dB (using an A-weight averaging meter). The upgrade results in a 15 dB decrease that is perceived as a 60% reduction in sound level compared to the current Life Pulse model. The Life Pulse is now 4 dB below the American Academy of Pediatrics’ recommended sound level of 45 dB for NICUs. This upgrade is the second sound reduction for Bunnell’s ventilator in the last five years. Contact bunl.com.

18 Respiratory Therapy Vol. 5 No. 1 n February-March 2010
IMPLANTEDImThera Medical, Inc announced that two patients have been surgically implanted with ImThera’s aura6000 neurostimulation device for treating tongue-based OSA. Patients are being enrolled in ImThera’s pilot clinical investigation in Belgium, with the first results expected to be published in the first half of 2010. The patients were implanted with the aura6000, during which the hypoglossal nerve was briefly stimulated to verify system and nerve integrity. One week post-surgery, the patients underwent an in-laboratory PSG titration process during which stimulation parameters were determined in order to maintain proper tongue position and to provide an open airway during sleep. The surgical procedures went smoothly, taking approximately 90 minutes to complete. There were no surgical complications; minor surgical issues were quickly resolved. At one week, patients were not disturbed by the implanted stimulator, lead or electrode. Speech, swallowing and tongue sensibility were not disturbed by surgery. Stimulation resulted in effective and painless tongue movement during wakefulness. During sleep, stimulation at sufficient levels was not perceived by the patients and did not interrupt sleep. Although this was not at all an outcome planned for the analysis, at one week after surgery, sleep apnea severity was improved during electrical stimulation. The aura6000 is not for sale in the US. Contact imtheramedical.com.
NEWS FROM DRAEGERDräger presented several products at the recently-held MEDICA trade fair and conference in Dusseldorf, Germany. Among the products presented were: precision lighting with the new Dräger Polaris Medical light system with LED technology, which provides shadow control, color fidelity and optimal depth-of-OR-field illumination; Primus IE and accessories that communicate via radio RFID and help connect medical equipment accessories; combined use of face and nasal masks, such as the new ClassicStar, which provide increased patient comfort during NIV; new blood pressure cuffs for non-invasive measurement, which are properly fitting, easy to apply and also skin-friendly; and a new monitoring component for the Infinity Acute Care System, Dräger Infinity M540, that supports hospital workflow. The medical division of Dräger has been honored with the 2009 Zenith Award, given by AARC to outstanding equipment manufacturers in the respiratory care field at its annual congress. Dräger was one of five companies chosen for the award by the AARC’s more than 48,000 members. Selection was based on the quality of the company’s equipment, accessibility, and helpfulness of its sales personnel, overall responsiveness, service record, commitment to truth in advertising, and support of the respiratory care profession. Dräger’s ventilator portfolio covers a wide range of patient needs, from neonatal to pediatric and adult. Contact draeger.com.
TRACH KITSmiths Medical announced the market release of the Portex Griggs Percutaneous Dilation Blue Line Ultra Tracheostomy Kit designed to save money, time and reduce procedural risk for the patient. The kit enables clinicians to perform tracheostomies at the bedside using the Griggs Guidewire Dilating Forceps (GWDF) Technique developed by noted Australian trauma surgeon Dr William Griggs and used extensively for more than 15 years by clinicians in Europe and Asia. The central element of the kit is the guidewire dilating forceps for pre-tracheal dissection and tracheal dilation. By laterally spreading the jaws of the forceps, when positioned in the trachea, the aperture opens smoothly and with less compression compared to cone-
shaped, single-stage dilators which typically require repeated forward and backward movement. Fewer movements also make for less trauma to tracheal structures, a shorter procedure, and earlier insertion of the tracheostomy tube. Some features of the kit: • ratcheted forceps lock keeps jaws closed while penetrating the trachea, helping to minimize downward pressure on the anterior wall; • guiding channel in forceps jaws enables passage over guidewire, consistent with the Seldinger technique; • curved tip of the forceps aids positioning within the contours of the tracheal anatomy; • taped tube tip and low profile Soft-Seal cuff eases insertion; and • conforming thermosensitive tube material and anatomically shaped flange allows for a better fit and easier cleaning. The Portex Griggs Percutaneous Tracheostomy Kit is packaged in six configurations: three containing the Blue Line Ultra Suctionaid Tracheostomy Tube (sizes 7, 8 and 9 mm inner diameter) and three featuring the standard Blue Line Ultra Tracheostomy Tube, also in sizes 7, 8 and 9 mm inner diameter. For more information on Smiths Medical’s Tracheostomy, Respiratory and Airway Management products, and for more detail regarding the Griggs GWDF technique, please contact the Customer Service team at (800) 258-5361 or smiths-medical.com.
CLEARANCEImThera Medical, Inc has received ethics committee clearance to begin human clinical trials in Belgium. The trials will include ImThera’s Targeted Hypoglossal Neurostimulation (THN) Sleep Therapy to treat OSA. Along with the clinical trial approvals, ImThera has received ISO 13485 certification of its quality system as a pre-requisite for the future CE mark application for European commercialization of medical products. ImThera’s European clinical trial, a pilot study involving ImThera’s THN sleep therapy system, is expected to publish its first results in the first quarter of this year. ImThera’s THN Sleep Therapy was developed as a surgical option to CPAP, delivering neurostimulation to the hypoglossal nerve to control certain muscles of the tongue. Using a multi-contact electrode and a programmable implantable pulse generator, the system delivers muscle tone to key tongue muscles to prevent the tongue from collapsing into the upper airway. ImThera’s device is not for sale in the US. Contact imtheramedical.com.
EXPANDINGInvacare is expanding its broad and comprehensive line of oxygen products with new, high-quality and competitively priced oxygen conservers and regulators. The new line of oxygen conservers and regulators includes: Invacare Pneumatic Oxygen Conserver with 3.5 to 1 savings ratio — IOC100P; Lotus Electronic Oxygen Conserver with 5 to 1 savings ratio — IOC100E; four CGA870 compatible style regulators from 4 L/min to 15 L/min (including one pediatric model); and a CGA540 compatible style regulator up to 15 L/min. Invacare offers a full range of respiratory products for home respiratory providers and patients. The company has 6,100 associates and markets its products in 80 countries around the world. Contact invacare.com.
TRANSPORTABLEThe new Invacare SOLO2 Transportable Oxygen Concentrator carries on Invacare’s tradition of producing the most reliable and cost-effective oxygen products for providers and patients. Offering both continuous flow oxygen delivery up to 3 LPM and pulse dose oxygen delivery in settings 1-5, the SOLO2
Concentrator is designed to meet the needs of oxygen patients in nearly any setting. The SOLO2 Transportable Concentrator

Respiratory Therapy Vol. 5 No. 1 n February-March 2010 19
features a sound level of approximately 39 dB when operating on continuous flow settings up to 2 LPM and all pulse dose settings. It operates using AC, DC or battery power and includes an easy-to-read LCD control panel. Units are shipped with a custom wheeled cart featuring large diameter wheels and a 2.5” raised platform designed to keep the SOLO2 Concentrator off of the ground and away from the elements. Contact invacare.com.
BEAR-ABLEThe Invacare Pediatric Bear Nebulizer System is the latest addition to Invacare’s line of quality aerosol compressors, offering the performance, reliability and value that providers and patients expect from Invacare. The cute, kid-friendly bear design will relax and calm children, while the included mouthpiece and pediatric mask promote child acceptance for an effective aerosol treatment. The Pediatric Bear Nebulizer is packaged with a built-in carrying handle and includes a five-year limited warranty. Contact invacare.com.
HEADLINESPepper Medical Inc introduced its new AvalonAire line of CPAP headgear and chinstraps similar to Tiara, Viasys, Cardinal, and CareFusion, according to the company. Pepper offers a 100% price guarantee. If buyers aren’t satisfied, the company will accept return of any product. The products are 100% hypoallergenic and latex-free, with Velcro brand hook & loop. The range of AvalonAire products include 3 pt and 4 pt headgear, Super Deluxe chinstraps, Topaz-style adjustable chinstraps, Ruby-style chinstraps and more. AvalonAire is a division of Pepper Medical. The new Pepper Medical Inc Pedi-Vent-Tie #401-P is a patented ventilator anti-disconnect device coupled with a trach tube neckband. The Pedi-Vent-Tie features a quick release Velcro strap compatible with all trach tubes, elbow connectors, and closed suction devices. The integral anti-disconnect strap eliminates the use of rubber bands, shoelaces and tape to secure the ventilator circuitry to the trach tube. The disposable Pedi-Vent-Tie neckband is made of a soft, 100% cotton flannel that offers moisture wicking properties to keep skin dry and cool. The Tie is priced at $3.95 each, individually packaged in boxes of 20 each. Contact peppermedical.com, (800) 647-0172.
SLEEP SOLUTIONRoyal Philips Electronics introduced the next generation Philips Respironics Sleep Therapy System at Medtrade 2009, the conference and expo for the home medical equipment industry. The arrival of the new product line brings significant advancements in therapy for millions of sleep apnea sufferers, along with solutions to healthcare providers to help meet today’s healthcare challenges. Contact medical.philips.com.
BRIGHT NOT BLANDAt the 95th Scientific Assembly and Annual Meeting of RSNA, Siemens Healthcare presented “Healthcare Lighting,” a concept for lighting design in medical facilities, aimed at creating a friendly and colorful environment instead of the common bland hospital atmosphere. Typical areas of application for light installations are CT, AX and MRI examination rooms. Light tubes — operated via computer to emit different light colors — can be mounted on walls. Walls and ceilings can be attractively decorated with different motifs, such as a mountain landscape and a blue sky with white clouds. With a special software program, the operator can choose from the full color spectrum and combine different tints. A special system for the MRI room works with a large number of small LEDs mounted
on the ceiling that light up the entire room in color. The Center for Diagnostic Radiology at Butzbach near Frankfurt, Germany, has achieved very positive experiences with Healthcare Lighting, because it helps keep patients distracted when doing CT scans. Economic figures from Butzbach clearly showed that only about 1% of patients had to be sedated before undergoing an MRI scan. Because of the lighting, claustrophobic patients can make it through the procedure without sedation. The distraction with colors also works well with children. Contact usa.siemens.com.
APPROVEDThe FDA has approved SPIRIVA HandiHaler (tiotropium bromide inhalation powder) for the reduction of exacerbations in patients with chronic obstructive pulmonary disease (COPD). SPIRIVA HandiHaler is already FDA-approved as a once-daily maintenance treatment for breathing problems associated with COPD, which includes chronic bronchitis, emphysema, or both. Said Dr Donald P. Tashkin, emeritus professor of medicine, David Geffen School of Medicine at UCLA, Los Angeles, “People with COPD now have a once-daily treatment option that not only helps them manage the debilitating symptoms of COPD, but also can help them reduce the chance of an exacerbation.” The SPIRIVA HandiHaler product label now includes clinical trial data from the UPLIFT study. In this trial, COPD patients in both treatment groups were allowed to use all of their respiratory medications with the exception of inhaled anticholinergics in order to simulate a real-world environment. The clinical data demonstrated that SPIRIVA HandiHaler sustained improved lung function over four years when compared with placebo and reduced COPD exacerbations, even with the use of these medications. Additionally, the inclusion of the safety data reaffirmed the established safety profile of SPIRIVA HandiHaler. The safety profile of SPIRIVA HandiHaler has been well-established in clinical studies involving more than 17,000 COPD patients, 11,000 of whom were treated with SPIRIVA HandiHaler. Contact spiriva.com or us.boehringer-ingelheim.com.
TAKING CAREGE Healthcare announced availability of its FDA-cleared CARESCAPE Monitor B850, which provides caregivers with a unique level of integration between patient monitoring data and hospital information systems. Unlike traditional patient monitors, CARESCAPE Monitor B850 directly links hospital networks, electronic medical records (EMRs), diagnostic images, lab results and third-party devices with real-time patient monitoring data, to support efficient clinical decision-making. This enables the CARESCAPE Monitor B850 to integrate its continuous clinical measurements with other elements of the patient record, delivering it at the point of care. The CARESCAPE Monitor B850 brings together the strong clinical heritage of Datex-Ohmeda’s anesthesia and Marquette Electronics’ cardiac expertise. It provides customized clinical information displays by care area and clinician preference, while also enabling hospitals to standardize on a monitoring platform throughout the organization. Developed with thousands of hours of field and in-house testing, the CARESCAPE Monitor B850 is the latest product in the GE Healthcare CARESCAPE portfolio, designed to deliver streamlined access to critical patient information for enhanced decision making. The CARESCAPE Monitor B850 is part of an easy to use system that can be customized to meet a variety of clinical needs, for example: ECG, administering anesthetics, diagnostic images, lab information, and more. Built upon the latest Intel embedded processing technology, the CARESCAPE Monitor B850 performs quickly and reliably. The

20 Respiratory Therapy Vol. 5 No. 1 n February-March 2010
CARESCAPE Monitor B850 is compatible with existing Marquette and Datex-Ohmeda products. GE’s component innovation strategy provides for an unprecedented level of backwards compatibility, allowing hospitals to leverage prior technology investments while updating monitors in the areas of strongest clinical need. Contact gehealthcare.com.
Continued on page 30…
SPOTLIGHT ON CAPNOGRAPHY
INTEGRATEDOridion has introduced its newest capnography technology — Integrated Pulmonary Index (IPI), which recognizes changes in a patient’s ventilatory status, enabling timely decisions and interventions, improved patient outcomes and increased patient safety. IPI is the latest addition to the Smart Capnography family of innovative algorithms developed by Oridion that simplify the use of CO2 monitoring on Microstream enabled products. The algorithm utilizes the real time measures and interactions of four complex parameters: end-tidal CO2 (etCO2), respiration rate, pulse rate and SpO2 (oxygen saturation), incorporating them into a single index, to provide an uncomplicated, inclusive assessment of the adequacy of ventilation in pediatric and adult patients. IPI provides an early indication of changes in the patient’s ventilatory status that may not be reflected by the current values of any of the four individual parameters. With IPI, clinicians can quickly and easily assess a patient’s ventilatory status and monitor a patient’s changing condition. IPI can be found only in Microstream Capnography equipped patient monitors, specifically in the Capnostream20 monitors. Contact oridion.com.
CHECKCapnocheck Plus from Smiths Medical is a full-featured quantitative sidestream capnograph ideally suited for a variety of clinical environments. It features a Remote Alarm which interfaces with a hospital nurse call system and alerts clinicians to any alarm violation. This is particularly useful when the Capnocheck Plus is used to monitor patients utilizing Patient Controlled Analgesia (PCA) and allows rapid response to changes in respiratory status. The Capnocheck Plus is a stand alone device, allowing it to be used in numerous areas of the hospital. Available with optional pulse oximetry, the Capnocheck Plus is a cost effective solution to safe patient respiratory monitoring. Contact smiths-medical.com.
SPOTLIGHT ON AEROSOL DELIVERY
GOING SOLOThe Aeroneb Solo Single Patient Use Nebulizer is designed for use with ventilated patients from infants through adults. The Aeroneb Solo represents a new dimension in acute care nebulization and is the first single patient use, high efficiency nebulizer available to caregivers. It is a dual functional nebulizer with both continuous and intermittent modes. No other nebulizer offers such flexibility, and, when coupled with the high efficiency that our customers have become accustomed to from the Aeroneb Pro, the Aeroneb Solo nebulizer creates a new standard of care for nebulization of mechanically ventilated patients. Contact aerogen.com.
FILTEREDTo minimize the risks of second hand aerosol exposure, Salter Labs has made available a disposable Filter Set that attaches to the existing one way valves on their high efficiency NebuTech HDN high density jet nebulizers. This concept of combining the nebulizer with a highly efficient exhalation filter can reduce the threat of contamination and long term risks to attending personnel by filtering 99.56% of exhaled aerosolized particles. Contact Salter Labs at salterlabs.com, (800) 235-4203.
VENTILATION ROUNDTABLE
Dräger MedicalInformation provided by Ed Coombs, MA, RRT, Associate Director of
Marketing, Respiratory Care Systems
What ventilation products do you offer?Dräger offers specialized ventilation platforms for intensive care, neonatal care, chronic care, noninvasive therapy, and emergency/transport. These ventilators are designed specifically to meet the wide-ranging needs of community hospitals as well as tertiary care centers. Our current ventilator line includes our flagship product, the Evita XL, which is a universal ventilator that can be utilized in the neonatal, pediatric, and adult critical care areas. The Babylog 8000 plus is Dräger’s neonatal-specific ventilator that can perform both pressure and volume ventilation. Our most recent addition to the portfolio is the Carina ventilator, which provides noninvasive and chronic care ventilation and is well suited for areas outside of the ICU.
In light of the economic situation, what R&D are you pursuing?Dräger is constantly investing in R&D efforts with a goal of improving patient outcomes and facilitating efficiencies for healthcare professionals. Approximately 7% of revenues are dedicated to research and development. The development of the lung protection package option for the Evita XL, which provides two methods of lung recruitment, is an example. Now caregivers have the option of using a slow volume inflation curve or an incremental/decremental EIP/PEEP procedure to safely and effectively recruit the lung. Through customer feedback, Dräger has provided a customizable interface that can match the monitoring needs of the most critical patients as well as those requiring less diagnostic bedside care. Understanding how clinicians use our equipment to help improve patient outcomes gives us greater insight and inspiration to advance technology beyond today and into the future.
Describe the latest technological advances for your products.Dräger has developed an innovative type of high-performance NIV ventilator that offers clinicians a wide array of ventilation therapies in a single device. One that is comfortable for both the patient and the caregiver, compact and mobile enough to optimize workflow and work space usage and clever enough to recognize changes in flow parameters and patient status, providing just the right amount of support while giving the patient room to breathe. The new Carina ventilator offers both invasive and non-invasive capabilities in one device and features a range of ventilation modes for spontaneous and mandatory ventilation and an integrated blender which can supply oxygen

Respiratory Therapy Vol. 5 No. 1 n February-March 2010 21
concentrations from 21-100%. Its latest technology, known as Synch Plus, will compensate for leakage and provide effective breath delivery. The Carina is well-suited for the emergency room, general ward, ICU, or sub-acute facilities as it features an internal battery and can operate independent of a high-pressure gas system. The transportability of the Carina makes patient transfer seamless and expedient, especially when a patient requires non-invasive support.
How are you training users as it pertains to your latest product advances?Dräger’s dedicated team of ventilation sales executives and clinical application staff are working closely with customers to realize the current trends in respiratory care. Dräger has a team of clinical applications specialists and ventilator-specific sales representatives who are well versed in respiratory care, most of whom are RRTs as well. This team provides on-site education as well as regional seminars that are open to all. Additionally, Dräger continues to work cooperatively with Intensive Care On-Line Network (ICON) where Dräger customers have access to online education, monthly webinars, and other clinical references 24 hours a day, 7 days a week, 365 days a year. Dräger recently extended its service coverage with ICON to provide state-of-the-art support services to all its ventilation customers. This enhanced clinical support gives clinicians the freedom to access information and continuing education at their convenience and provide the department manager with an online tool to view staff’s educational progress.
Smiths MedicalWhat ventilation products do you offer, and where are they used?Smiths Medical is a leading global provider of medical devices. The Pneupac range of ventilators provides ideal solutions for the demanding requirements of portable ventilation in the most challenging situations including harsh conditions resulting from natural and pandemic disasters. Pneupac ventilators have always been extremely robust and reliable. Users frequently describe Pneupac ventilators as the workhorse in their ventilator stock. Because they are intuitive and easy to use, less time is needed for in-servicing and training. Staff changes, costs of training, and the possibility of employing less experienced staff during mass casualty or pandemic conditions make it paramount that ventilation equipment is easy to use. The Pneupac VR1 and paraPAC transport and emergency ventilators can be used inside and outside ambulances or hospitals. The babyPAC is a specially developed pressure-controlled transport ventilator for neonatal patients. It is often used on transport incubators or as a stand-alone ventilator during an MRI scan. The ventiPAC completes our list of solely gas-powered ventilators. It gives flexibility to clinicians, allowing inspiratory and expiratory time adjustments, which makes it more suitable for transporting long-term ventilation patients. All these ventilators need only compressed oxygen to function. They have been drop tested, vibration tested, and tested for ingress of water. The Pneupac compPAC ventilator was specially developed for the military market. We’ve added a compressor and NBC filter to our proven ventilator technology so the ventilator can operate as independently as possible from its surrounding environment. Components of the compPAC can also be found in field anesthesia machines used by the US military.
In light of the economic situation, what R&D are you pursuing?Smiths Medical continues to invest in R&D for new product development to meet current and future customer needs in transport ventilation. Our latest product is the Pneupac VR1 Ventilator/Resuscitator. It incorporates key features such as the DEMAND function and relief valve technology previously only available in larger ventilators. Changes in AHA guidelines now mean that a first response ventilator should have a means for manually controlling the ventilation pattern. It is simple to do this with basic technology, but our goal was to achieve this in such a way that it functioned simply and safely. With the VR1 manual control we managed to incorporate safety features to avoid over-ventilation and dangerously high flows for smaller patients.
Describe the latest technological advances for your products.We continue to look at bringing new products to market that address current and future customer requirements for day-to-day management of ventilated patients. In addition to the development of next generation products, enhancements are made where appropriate to our existing product lines, such as the addition of an air mix option to the VR1.
How are you training users as pertains to your latest product advances?User training is an important part of our business. It starts with a well-educated sales force who are updated with regular training sessions supported by our Clinical Education Team and dedicated Product Specialists. Since a representative of the company can’t always be on site to answer a user’s question, we have also developed a range of training videos that can be accessed on the Smiths Medical website along with other training videos for Smiths Medical products. This, combined with our aim to keep the ventilators simple to operate and intuitive, ensures correct and safe use of our products.
Philips RespironicsWhat ventilation products do you offer?The new Respironics V60 Ventilator takes NIV further by giving you the confidence to treat a wide range of patients. The V60 uses Auto-Trak auto-adaptive technology to help ensure patient synchrony and therapy acceptance. The six-hour internal battery supports emergency back-up and intra-hospital transport for continuity of care. The V60 is cleared for invasive and noninvasive treatment of pediatric and adult patients. Hospital ventilatory care is further supported with exclusive modes and comfort features. The Respironics V60 fulfills the Philips commitment to simplify advanced healthcare. The new Respironics V200 Critical Care Ventilator provides state-of-the-art ventilation modes with synchrony options — Auto-Trak, Flow-Trak, and Baby-Trak — that reduce work of breathing and streamline patient care. The unique speaking mode allows appropriately selected tracheostomy patients to speak without an external valve. The V200 Ventilator has a range of treatment modalities for all patient populations — invasive modes for neonatal through adult patients and noninvasive for pediatric through adult patients. The V200 Ventilator also supports care in any environment by connecting to Philips patient monitors and hospital information systems for a seamless flow of ventilation information. The Respironics NM3 respiratory profile monitor

22 Respiratory Therapy Vol. 5 No. 1 n February-March 2010
non-invasively monitors volumetric (VCO2) and end-tidal (EtCO2) capnography. Clinicians can use this information to minimize the duration of mechanical ventilation and optimize the potential for successful extubation when managing critically ill patients. At every stage of care, the NM3 monitors the patient’s response to ventilation. Bright, sharp, and well organized display screens present physiologic information on the patient’s readiness for less support and spontaneous breathing trials (VCO2, MValv, Vd/Vt). The lightweight, portable design allows inter-departmental use on ventilated patients and non-ventilated patients under deep and conscious sedation. Philips also offers the Respironics NIV circuit with expiratory port filter. During pandemics, clinicians must provide the best individual patient care while protecting themselves and others. During non-invasive ventilation (NIV), exhaled gas exits the patient circuit through the exhalation port. Filtration of this port may reduce the risks of cross-contamination for surrounding family and caregivers. For this reason, Philips has released an NIV circuit with an expiratory port filter that provides greater than 99.99% bacterial and viral efficiency. Clinicians can add or remove the single-use filter at any time without affecting a patient’s work of breathing or Philips Respironics ventilator performance.
How are you training users as it pertains to your latest product advances?We have classroom workshops, computer-based training, and web-based training. And most of these training pieces come with CEUs.
CareFusionWhat ventilation products do you offer?CareFusion offers a full range of ventilation products for a variety of applications in the hospital, for transport and military applications and in the home. We are the market leader in mechanical ventilation with the EnVe, AVEA, Vela, 3100 series high frequency oscillatory ventilator (HFOV), LTV series, and Infant Flow Nasal CPAP products. In addition to mechanical ventilation products, CareFusion offers a full range of ventilation consumables.
In light of the economic situation, what R&D are you pursuing?With rising healthcare costs, declining reimbursement, personnel shortages and a global demand for quality, we have clear drivers for growth and innovation. Over the next couple of years we estimate that we will have about 40 new products available to further provide safety and value for our customers. We plan to meet our goals by increasing our R&D efforts and further development of our core technologies.
Describe the latest technological advances for your products.Our latest technology in ventilation called the EnVe ventilator represents a major paradigm shift in critical care ventilation. The EnVe is a comprehensive, full feature Intensive Care Ventilator with unique ActivCore technology. ActivCore is the basis for an extremely powerful and compact designed ventilator (9.5 lbs) that integrates a full color LCD display and 4 hour, hot-swappable internal battery for complete wall independence.
How are you training users as pertains to your latest product advances?CareFusion supports the education and training of users in a variety of ways for both existing products and our latest advances. We employ clinical support teams to provide training on the use of CareFusion products as well as support materials both in written and digital education form. CareFusion also offers biomedical training courses to CareFusion customers to empower users to support their devices in the long term.
Discuss the use of your products in various venues (ie, hospitals, homecare settings, etc).The EnVe, AVEA and Vela ventilators are conventional ventilators that are used widely in a variety of application in the hospital settings. Our specialty ventilation products support the neonatal patient range with the 3100A HFOV and the Infant Flow SiPAP, and the 3100B HFOV supports pediatric and adult patients. Compact and portable, the LTV series of ventilators offers the freedom of advanced care ventilation at home or in a post-acute setting. The LTV series makes for a smooth transition from hospital care, ensuring reliable ventilation while saving on clinical care costs. The LTV 1150 and LTV 1200 offer flow trigger for enhanced sensitivity, CPAP for use with ventilator dependent patients, configured for ground or air emergency transport.
Hamilton MedicalInformation provided by Robert Hamilton, Vice-President, Hamilton
Medical, Inc.
What ventilation products do you offer?The Hamilton G5, Hamilton C2, Hamilton GALILEO, Hamilton RAPHAEL XTC, and the ARABELLA Infant NCPAP System. In MD Buyline’s Ventilation Technology Report dated October 1, 2009, Hamilton Medical rated the top composite score in User Satisfaction.
In light of the economic situation, what R&D are you pursuing?With patient safety and staff efficiencies in mind, we continue to manufacture and develop products with automated functions to enhance patient care and provide advanced technology that is reliable, easy to understand and use, has low maintenance requirements, is easy to service and has a long useful life. We believe, as do our customers that our products are the best value in the industry. Hamilton Medical continues a long tradition of technology advances. Hamilton currently invests over 25% of its OPEX into research and development. By investing five times the industry average into research & development, Hamilton Medical continues to provide the technology that has become the standard expected from us.
Describe the latest technological advances for your products.Hamilton Medical is continuing a long tradition of bringing innovative new technology to the market. Our new C2 ventilator is a prime example, providing clinicians with a ventilation platform that works equally well in ICU, the ED, Step down, and transport applications. The C2 is an excellent choice for non-invasive ventilation and has standard and advanced ventilation modalities. This versatile product is equipped with advanced monitoring and graphics capability and like all Hamilton ventilators, is equipped with ASV (Adaptive Support Ventilation),

Respiratory Therapy Vol. 5 No. 1 n February-March 2010 23
the most automated and fully closed loop ventilation modality, which is unique to Hamilton Medical.
How are you training users as pertains to your latest product advances?In addition to a well trained group of professional sales representatives, many of whom have extensive clinical experience, Hamilton Medical employs a dedicated group of outstanding clinical applications specialists who orient staff to the new equipment during patient clinical trials. This work is done in the classroom and at the bedside. Our applications specialists also provide on-site formal training on all new products and they are available 24 hrs a day, 7 days a week as telephone clinical/technical support.
Discuss the use of your products in various venues; ie hospitals, homecare, etc.Hamilton Medical ventilation systems provide hospitals, from the NICU to all Adult ICUs, transport, and long term care facilities with the most clinically advanced yet easiest to use system in the industry. Our close work with facilities has helped us design systems that with the aid of ASV help relieve staff of constant vent setting changes, allowing them to spend their time focusing on the patient and not the machine.
EXECUTIVE PROFILES
AerogenInformation provided by John Power, CEO.
Describe your products and their unique features.Having spent many years working in the design of critical care ventilators, I was struck by the limited performance of typical drug delivery options available for ventilator applications. My objective became the design and development of a significantly improved nebulizer for ventilator application which addresses the shortfall of traditional devices. The result of this quest was the 2002 launch of our Aeroneb Pro nebulizer, a nebulizer specifically developed for critical care patients receiving mechanical ventilation that offers caregivers the opportunity for improving drug delivery efficiency while at the same time reducing drug and personnel costs associated with respiratory care in the hospital setting. Using OnQ micropump technology, and unlike traditional nebulizers, the Aeroneb Pro adds no pressure or volume to ventilator circuits and minimizes drug waste by nebulizing virtually all medication. The Aeroneb Pro produces a fine particle, low velocity aerosol optimized for deep lung drug deposition. This autoclavable nebulizer enables multipatient use in-line with mechanical ventilators. The latest addition to our critical care nebulizer range, the Aeroneb Solo nebulizer, is a product line extension of the Aeroneb Pro nebulizer and was developed and designed in direct response to market need. The Aeroneb Solo offers the same aerosol characteristics that caregivers have come to expect from the Aeroneb Pro. The Aeroneb Solo is a dual functional nebulizer. In addition to intermittent functionality; it also offers the caregiver the ability to conveniently continuously nebulize patients when powering the nebulizer with the Aeroneb Pro-X controller. It can be used for intermittent therapy for up to 28 days and for continuous therapy, for up to 7 days, after which time it is disposed of. Its light weight and small size makes it attractive for
use with pediatric and neonatal patients.
Discuss your R&D process, including clinical user input.As an organization, Aerogen is fully committed to research and development with 30% of turnover re-invested into the R&D process. We operate a structured 5 stage R&D system to ensure a timely advance from new idea concept through validation and ultimately to market launch. Our product development process ensures that continual updates and improvements are implemented in our portfolio of products. All our research and development efforts are supported by a dedicated and experienced team of engineers and marketers.
Discuss the educational services you offer for use of your product.As a leader in the field of aerosol science we promote continued education and research in the field and will continue our policy of supporting relevant researcher and RT programs and studies which further knowledge of ventilator nebulization. Continuing education credits, journal articles and case studies on the Aeroneb nebulizers are available on our website www.aerogen.com.
What new technology do you see as having the greatest impact on your area of expertise?The most significant advancement that will have the greatest impact on our field of expertise is the potential to deliver traditional systemic drugs via the pulmonary route. Inhaled insulin is a successful example of this trend, but we know of several other companies working on exciting programs ranging from pulmonary delivery of erythropoietin, human growth hormone, antibiotics, prostacyclin therapy to name but a few. These new applications will require highly efficient drug delivery with minimum waste. We believe Aerogen’s nebulizers, which deliver consistent repeatable doses, are well poised to meet such technology requirements.
ResMedDescribe your products and their unique features.ResMed is the global leader in the design and manufacture of products for the treatment of sleep apnea, including ventilators, positive airway pressure devices, patient interfaces, clinical data management software and technologies, equipment accessories and diagnostic devices. Our focus in this issue is our line of premium patient interfaces, which includes three categories: nasal pillows, nasal masks and full face masks. ResMed’s nasal pillows systems include the market-leading Swift LT and the Swift LT for Her, the first mask designed to meet the unique needs of female patients. In nasal masks, ResMed offers the Mirage Micro, the Mirage Activa LT, and the newly released Mirage SoftGel. The SoftGel is ResMed’s first entry into the popular gel mask category and features a fully encapsulated dual-layer gel mask with an incredibly soft upper layer for maximum comfort. In the full face category, ResMed again leads the market with the Mirage Quattro. The Quattro features an intuitive MicroFit dial for personalized fit and spring air technology to accommodate movement during sleep. Also in the full face category is the Mirage Liberty — an alternative full face and pillows combination mask for patients seeking a clearer field of view and the benefits of a less obtrusive full face mask. All of ResMed’s masks deliver exceptionally quiet therapy.

24 Respiratory Therapy Vol. 5 No. 1 n February-March 2010
How do your products directly affect patient care?Comfort and efficacy are essential components to successful patient care and patient compliance. Conversely, noncompliance often results from a patient’s frustration with an uncomfortable, bulky or poorly-fitted mask. By constantly striving to engineer comfortable, high-performance masks and products, ResMed helps make it easier for patients to accept therapy early on, remain compliant and receive all the benefits that come from successful sleep apnea treatment.
Tell us about the latest advances in the area your products serve.The most recent advance in the area of masks is the SoftGel, ResMed’s dual-layer silicone gel mask. In addition to being the first mask on the market to offer a dual-layer gel design for maximum comfort, it is also built on our new ConvertAble platform, which offers the choice of two different mask cushion styles — the SoftGel or the Activa LT — on one interchangeable frame. This new offering allows patients greater freedom of choice and also provides enhanced business efficiencies and cost savings for our customers.
What sets your products apart from others in the field?In nasal pillows, it is the patented dual-wall pillow design of the Swift LT and Swift LT for Her, which provides a soft, stable seal while allowing for patient movement. In nasal masks, it is the dual-layer gel design of the SoftGel, allowing for the ultimate in softness and stability, as well as the ability to interchange cushions with the Activa LT for additional freedom of choice. In full face masks, it is the Quattro’s spring air cushion and MicroFit dial, which allow an easy customized fit for comfortable and trouble-free performance.
Discuss your R&D process, including end-user input.Our business is founded upon empowering our customers to achieve exceptional clinical outcomes while profitably growing their business. Consequently, our product development team is in regular dialogue with global market research, sales and product management teams in order to funnel customer feedback into the product development cycle and translate the voice of the customer into sophisticated treatment technologies that will support our customers’ success.
Discuss the educational services you offer for use of your products.ResMed has a Clinical Education team responsible for the development of training and education initiatives for its customers and their patients. ResMed’s Clinical Education team is made up of a dedicated group of clinicians with extensive backgrounds in both cardiopulmonary medicine and sleep. We offer clinical and sales training to customers at regional and branch levels; clinical in-services, from product application to detailed disease processes; the opportunity for continuing education unit (CEU) credits; and access to our clinical literature library with over 1,600 articles on the topic of sleep-disordered breathing. In addition, we also provide product user guides and patient support materials, including easy-to-use mask fitting guides available online.
Talk about how you test and evaluate your products in actual day to day use.All ResMed mask products go through an extensive user evaluation phase during development. Once released, ongoing feedback is captured in post-market surveillance activities,
which are then reviewed at the beginning of following projects to ensure relevant feedback is incorporated in the next generation of products.
Discuss the international scope of your testing/marketing/development efforts.ResMed conducts research in all its major markets and has recently commissioned its largest market research project to date covering the Americas, Europe and Asia Pacific, with patients, equipment providers and clinicians. ResMed has R&D facilities in Sydney, Munich and Paris, and has recently established a manufacturing facility in Singapore to complement its global manufacturing base in Sydney.
Tell us how you utilize conferences, seminars and such to promote your products.We showcase our products at major medical equipment conferences and exhibitions around the world each year, typically having major display stands at Medtrade and Sleep in the US. We also attend and sponsor numerous regional tradeshows, conferences and events in a number of related markets. In addition to the conferences that directly promote our products, ResMed is highly involved in promoting awareness around sleep apnea via direct outreach initiatives to healthcare professionals involved in the treatment of comorbid disease categories, such as cardiovascular illness and diabetes. ResMed is dedicated to helping healthcare providers efficiently identify patients at risk for sleep apnea and support them through the diagnostic pathway to effective treatment.
B&B Medical TechnologiesDescribe your product and its unique features.B&B Medical Technologies’ Sil.Flex Stoma Pad is a revolutionary new product that maximizes comfort and care for patients with tracheostomies. Sil.Flex Stoma Pads are soft, flexible cushions intended for use between a tracheostomy neck plate and patient neck to provide a stable, comfortable interface. The patent-pending Sil.Flex Stoma Pad is an ergonomically designed cushion that absorbs pressure. The use of hypoallergenic, latex-free material allows the Sil.Flex Stoma Pad to provide a stable, comfortable platform between the tube neck plate and the patient’s skin. Sil.Flex Stoma Pads are available in multiple sizes, accommodating small infants to large adults.
How does your product directly affect patient care?Stoma sites require special attention throughout the day and even with the best of care may often become sensitive or compromised due to constant pressure or movement of the neck flange against the surrounding tissue. The Sil.Flex Stoma Pad is easy to use and absorbs the pressure points of the tracheostomy device, making the patient more comfortable with position changes. The Stoma Pad can be used in all critical care units, operating rooms, and special procedure units as well as alternate care facilities and home care. B&B’s TrachGuard or the TrachStay may be used in combination with the Sil.Flex Stoma Pad. Sil.Flex Stoma Pads enhance patient comfort with all brands and styles of tracheostomy tubes.
Tell us about the latest advances in the area your product serves.With changes in reimbursement strategies and procedures, reimbursement for institution-acquired pressure wounds

Respiratory Therapy Vol. 5 No. 1 n February-March 2010 25
and injuries is under scrutiny. Strategies to prevent these injuries have become foremost in quality patient care and cost containment. The unique design of Sil.Flex Stoma Pad relieves pressure to the skin and provides a safe, cost-effective answer to help prevent irritation at the stoma site.
What sets your product apart from others in the field?The Sil.Flex Stoma Pad is a unique product with the specific advantage of reducing and absorbing pressure. Each sterile pad is individually packaged and may be used for up to 14 days for single patient application. Once applied, Sil.Flex is easily removed for cleaning. Other attempts to provide tracheal stoma comfort are expensive disposable devices that require frequent attention from clinical staff. Sil.Flex Stoma Pads are a cost effective and convenient solution to assist in reducing irritation at the stoma site.
Discuss your R&D process, including end-user input, and your R&D goals.Patient comfort, safety, clinical efficacy and practitioner ease of use are the hallmarks of B&B Medical Technologies’ company charter. Our development team continually designs and seeks products to support the patient and clinician’s needs. B&B Medical Technologies’ products are clinically proven for critical care, anesthesia, emergency, transport, home care and alternate site care. B&B products are safe, versatile, convenient and cost-effective.
Discuss the educational services you offer for use of your product.Complete Instructions for Use are provided for each product. Downloadable instructions, policies and procedures, photographs and instructional videos are available at the B&B Medical Technologies website, BandB-Medical.com.
Discuss the role of critical care providers in developing and upgrading your product.B&B Medical Technologies is a clinician founded and owned company that works closely with respiratory therapists, physicians and nurses to provide cost effective solutions for patient care.
Tell us how you utilize conferences, seminars and such to promote your product.B&B Medical Technologies’ main purpose at international congresses and state and local education meetings is to provide an introduction to our safe and effective airway management products for use in hospitals and clinics.
Toll-free: +1.800.242.8778
www.BandB-Medical.com
We are B&B Medical Technologies.
Safe and effective products
Versatile applications
Convenient packaging
Cost effective solutions
www.BandB-Medical.com for
NEW SIL.FLEX™ STOMA PADRevolutionary comfort for tracheostomy patients

26 Respiratory Therapy Vol. 5 No. 1 n February-March 2010
Amidst all the talk about healthcare reform, policy makers and healthcare providers are focusing more on reducing costs and improving quality of care. One of the areas where this is most possible is with Potentially Preventable Conditions (PPCs). These are health conditions that might be avoided with better medical care. Preventing these complications could prevent hospital readmissions, lowering costs while improving patient outcomes at the same time. This is especially true for tracheostomy patients, particularly those without mechanical ventilation.
“There’s more pressure at all levels. There’s a trend toward doctors being paid not so much on the quantity of services but on the quality,” said Dr Eugene N. Myers, Distinguished Professor and Emeritus Chair of the Department of Otolaryngology of the University of Pittsburgh School of Medicine. “People want to ensure they’re getting the highest quality of healthcare with the least amount of complications.”
OverviewHospital care makes up the largest percentage of overall health care expenses, accounting for 30.8 percent of costs.i In 2006, nearly 4.4 million hospital admissions could have been potentially preventable with timely and effective ambulatory care or adequate patient self-management of PPVs. Those admissions totaled $30.8 billion in hospital costs and represented about one of every $10 of total hospital expenditures. Congestive heart failure and bacterial pneumonia were the two most common reasons for potentially preventable hospitalizations, accounting for half the total hospital costs ($8.4 billion and $7.2 billion, respectively).ii
In 2007, the Agency for Healthcare Research and Quality published a Statistical Brief analyzing the trends in potentially preventable hospitalizations from 1997-2004. Among the highlights:
• Total hospital costs for potentially preventable admissions increased by 31 percent (adjusted for inflation), while the number of admissions rose by only 3 percent, between 1997 and 2004.
• Costs increased for preventable admissions related to chronic
respiratory diseases (16 percent) and acute conditions (38 percent) even though admissions declined between 1997 and 2004.
• Total hospital costs for chronic obstructive pulmonary disease increased even though admissions declined; hospital costs for bacterial pneumonia increased despite stable hospitalization rates. The total costs suggest more complex cases or greater intensity of care.
• Total hospital costs associated with bacterial pneumonia increased by nearly 40 percent, from $5,089 million in 1997 to $7,050 million in 2004.iii
PPCs and Tracheostomy Patients Without Mechanical VentilationStatistics related to tracheostomy patients without mechanical ventilation are difficult to come by. However, it is known that tracheostomy patients do experience numerous potentially preventable conditions after they leave the hospital. These include mucus plugs, infection and bacterial and aspiration pneumonia.
“The patient who has a tracheostomy is sitting on a keg of dynamite,” said Dr Myers, who has performed more than 10,000 surgeries on patients with tumors of the head and neck. “Caregivers don’t like to take care of the trach. They don’t like to get their hands dirty. They don’t like people hocking this mucus at them. So they don’t take care of them. As a result, due to mucus plugs occluding the airway, it becomes potentially fatal.”
Table 1 shows the costs of treating numerous complications that have been associated with tracheostomies.
Humidification To Reduce Complications In Trach PatientsPolicy makers and healthcare providers are looking for ways to reduce PPCs. Dr Myers said he hoped the focus on improving the quality of care while simultaneously cutting costs would bring a sharper focus to the importance of humidification for tracheostomy patients. According to Myers, “Proper humidification plays a role in preventing or markedly reducing the obstructive phenomenon that we see. You can reduce the dryness effect and the formation of mucus plugs, which can kill people. Humidification is absolutely important and does make a difference.”
The nose, mouth and trach all need to be properly humidified. Vivian Wright knows this first-hand. Her husband, Dean, had a
Tracheostomy Care and Potentially Preventable ComplicationsJudi Villa
Judi Villa is the Director of Communications at Wright Solutions LLC.
She can be reached at [email protected]. Wright
Solutions is based in Marathon, FL and can be found on the Web at
wrighttrachsolutions.com.

Respiratory Therapy Vol. 5 No. 1 n February-March 2010 27
tracheostomy while battling head and neck cancer. But Dean refused to humidify his nose and mouth because he said it took too long. A mucus plug developed and occluded his airway, and he nearly expired during an airplane ride. When Dean was released from the hospital, Vivian invented a humidification system for him that she has named the Wright Face & Tracheostomy Nebulizing Mask. The Wright Mask allowed Dean to simultaneously humidify his nose, mouth and trach, cutting in half the time it took to humidify. Dean became a compliant patient and never again had to be hospitalized for a potentially preventable condition.
“Trach patients have insufficient respiration, absolutely,” Vivian said. “If they’re not cleaning the trach, if they’re not humidifying enough, it becomes worse. Most, if not all, of these issues can be reduced with humidification.”
The Wright Mask, which is patented, registered with the FDA and fully covered by Medicare and Medicaid, has undergone a clinical trial at the University of Miami. That clinical trial demonstrated that the Wright Mask was comparable to traditional aerosol face and aerosol trach masks in terms of saturation, comfort and ease of use, but it was superior in its ability to save time.iv This is critical to achieving compliance with trach patients and, thereby, reducing complications and costly hospital readmissions.
“The frustrating part is getting these patients to be compliant. Many trach patients are non-compliant,” Wright said. “That’s where the Wright Mask becomes important. Putting the Mask into their hands takes away their excuse.” It has to start with the clinicians prescribing the Mask for patients. Then the patient has to “step up and take a certain amount of responsibility” for their healthcare. When that happens, some of these potentially preventable conditions can be averted.
Consider these effects for a compliant patient:• Healthier upper airway and trach tissue• Fewer mucus plugs• Fewer infections• Fewer pneumonias
These translate into benefits for physicians and hospitals: • Physicians reduce complications while increasing
their PPC profile• Hospitals have fewer readmissions for complications• Hospitals reduce non-reimbursed expenses• Hospitals ensure the best pay profile• Costs are reduced to government and third-party payers
“When patients humidify properly, they feel better and they have fewer complications. Hospitals have fewer readmissions. Everybody benefits,” Vivian said. “This is just one way we can improve quality of life and reduce costs. And it’s so simple. There’s really no reason not to do it.”
Referencesi Trends in Health Care Costs and Spending, Online,
September 2007, Kaiser Family Foundation http://www.kff.org/insurance/upload/7692.pdf;
ii Nationwide Frequency and Costs of Potentially Preventable Hospitalizations, 2006, Online, April 2009, U.S. Agency for Healthcare Research and Quality http://www.hcup-us.ahrq.gov/reports/statbriefs/sb72.pdf;
iii Trends in Potentially Preventable Hospitalizations among Adults and Children, 1997-2004, Online, August 2007, U.S. Agency for Healthcare Research and Quality http://www.hcup-us.ahrq.gov/reports/statbriefs/sb36.pdf;
iv Evaluation of the Wright Mask in Chronic Tracheostomy Patients, Online, July 2009, University of Miami http://www.wrighttrachsolutions.com/Abstracts.html.
Table 1
Diagnoses Charges, $ (mean)
Costs, $ (mean)
Length of Stay, days (mean) National bill, $
Diseases of the respiratory system 27,565 9,293 5.4 92,349,555,358Respiratory infections 22,755 7,835 4.9 33,622,622,224Pneumonia (except that caused by TB or STD) 25,478 8,769 5.4 29,864,341,883Pneumococcal pneumonia 29,738 10,759 6.2 751,059,688Other bacterial pneumonia 47,558 16,231 9.3 5,250,354,965Pneumonia, organism unspecified 22,585 7,780 4.9 22,066,666,040Other pneumonia 30,206 10,315 5.9 1,796,261,190Other upper respiratory infections 12,103 4,225 2.5 939,360,804Acute upper respiratory infections of multiple or unspecified sites 10,888 3,887 2.4 250,352,738Chronic sinusitis 19,059 6,437 3.1 181,598,572Other and unspecified upper respiratory infections 14,160 4,915 2.9 395,215,512Chronic airway obstruction, not otherwise specified 21,002 7,441 5 377,775,108Aspiration pneumonitis, food/vomitus 39,237 12,970 8 7,199,256,640Other respiratory insufficiency 76,793 25,253 13.3 1,462,280,390Painful respiration 14,006 4,675 2.2 297,555,656

28 Respiratory Therapy Vol. 5 No. 1 n February-March 2010
Tom Bachman is a clinical research consultant in Lake Arrowhead, CA. He is
a regular contributor to Respiratory Therapy and Neonatal Intensive Care.
He can be reached at [email protected]. The information on
the products discussed in this article, Verso and Pucker, were provided by
CareFusion.
Closed Airway Access Systems: Improving Patient Care; Protecting the ClinicianThomas E. Bachman
Systems that permit suctioning of airway secretions have been available for nearly two decades, and have become the standard of practice.1,2 The adoption of closed suction systems was driven primarily by the fact that they permitted suctioning of airway secretions, without significant de-recruitment of the lung. This is believed to be especially important in severely ill patients, where re-recruitment could be a significant risk and effort. While there has been speculation that closed circuit suctioning should reduce the incidence of ventilator-associated pneumonia, the evidence does not support this conclusion.3 There appears to be a general consensus, however, that closed suctioning reduces the risk of infection of healthcare workers.1,4
Especially during times of heightened pandemic concern, it is imperative that every reasonable safety precaution and procedure for effective disease containment be utilized. This concern should be of particular importance when dealing with a highly infectious viral outbreak transmitted from patients via aerosolized vectors. The accelerated velocity and transmission of exhaled viral particles from patients requiring mechanical ventilatory support and even those just receiving oxygen with a standard mask is not always obvious to clinicians.2,5,6 This is not only a concern for healthcare workers but also nearby patients.
In order to properly manage a ventilated patient and minimize cross contamination, all efforts to maintain a closed system should be supported. Once a ventilator circuit is opened for any procedure, the natural recoil from the patient’s low lung compliance creates a high flow exhalation that sprays virus, pathogens and other particles. It is therefore no surprise that during the Toronto SARS outbreak of 2003 nearly half of the SARS patients were healthcare workers.7 To make matters worse, these are often the same patients who have excessive secretions and more than likely will require a direct bronchoscopic examination for specimen collection, airway lavage or mucus plug removal. All of these procedures are considered to be high risk during viral respiratory disease outbreaks.8,9
As can be seen in Figure 1, a simulation of breaking a ventilator circuit to perform a procedure, the aerosol droplets discharged
from the patient’s lungs can be considerable. Although the volume of aerosol in this simulation was significantly enhanced so that it would be visible to the naked eye, in real life ventilator management contaminated aerosolized particles that are not visible are discharged into the air and into the space occupied by healthcare workers and other patients, increasing their exposure and risk of infection.
Closed suction catheter systems are considered the standard of care for managing airway secretions in ventilated patients and are especially critical for patients with respiratory infections. There is room for improvement of these systems. Most available closed suction catheter systems have a catheter that is bonded to the airway adapter, requiring complete system replacement whenever the catheter is occluded or malfunctions. Furthermore, if bronchoscopy needs to be performed, the ventilator circuit needs to be broken twice, once to put the bronchoscopy adapter into the circuit and again when the procedure has been completed to remove it. This additional exposure of the
Figure 1

Respiratory Therapy Vol. 5 No. 1 n February-March 2010 29
caregiver to particulates and the patient to loss of ventilating pressures reduces the ability to maintain ventilation support and prevent cross contamination. Since viral particles can be infective in air and surfaces for more than a day, proactive containment is critical for healthcare worker safety.10 It is clearly important to eliminate as many circuit breaks as possible.
Recently, AirLife introduced their Verso airway access adapter along with a closed catheter system that appears to have addressed these problems. The Verso adapter provides direct airway access to the ventilated patient and connects to their full range of closed suction catheters and can be used during bronchoscopic examinations, mini-BAL procedures, open suction and even drug instillation, all while maintaining a closed system.
One of the enabling characteristics of the Verso airway access adapter is its Pucker Valve technology [figure 2], that seals the patient’s airway from the outside environment. This valve enables suction catheters, bronchoscopes or mini-BAL catheters to easily pass into the patient’s airway and yet prevent gas or
aerosolized particles from leaving the circuit. The Verso is reported to seal the ventilator circuit at more than three hundred centimeters of water when the catheter is withdrawn.
The Pucker Valve [figure 3] sits opposite the entrance to the airway so that suction catheters can be easily changed without exposing a healthcare worker or the environment to exhaled particles. If the patient requires bronchoscopy, an adapter seal (sizes available to use 2.8 to 6.3 mm scopes) placed on the access port prevents loss of pressure or particles during this procedure. As seen in figure 3 below, at no time during the patient’s care does the circuit need to be broken for bronchoscopic airway access. The same is true for instilled drug delivery or mini-BAL procedures. The Verso adapter also includes double swivel fittings so that the circuit can be moved as necessary for procedures without breaking the connection to get it in the right position.
Some believe that the greatest risk to our healthcare system during a respiratory viral outbreak is not that there won’t be enough ventilators to treat the patients but that there won’t be
Figure 2
Figure 3

30 Respiratory Therapy Vol. 5 No. 1 n February-March 2010
enough healthcare workers to manage the ventilators.11 [See the editorial in this issue.] The Verso Airway Access Adapters, with the AirLife Closed Suction Catheters, clearly may be an important technology for airway management of the ventilated patient during viral or pandemic outbreaks.
References1 Branson, RD. Secretion management in the mechanically
ventilated patient. Respiratory Care 2007 52(10),1328-47.2 Paul-Allen J, Ostrow CL. Survey of nursing practices with
closed-suction suctioning. American Journal of Critical Care. 2000. 9(1)
3 Vonberg RP, Eckmanns T, Welte T, Gastmeier P. Impact of the suctioning system (open vs closed) on the incidence of ventilator-associated pneumonia: a meta analysis of randomized controlled trials. Intensive Care Med. 2006 32(9)1329-35.
4 Pruitt B, Clearing the air with closed suctioning. Nursing 2005 35(7)44-5.
5 Somogyi, R., A. E. Vesely, T. Azami, D. Preiss, J. Fisher, J. Correia, and R. A. Fowler. 2004. Dispersal of Respiratory Droplets With Open vs Closed Oxygen Delivery Masks: Implications for the Transmission of Severe Acute Respiratory Syndrome. Chest 125:1155-1157.
6 Fowler, R. A., D. C. Scales, and R. Ilan. 2004. Evidence of airborne transmission of SARS. N.Engl.J.Med. 351:609-611.Oxygen Masks.
7 World Health Organization. Summary table of SARS cases by country, 1 November 2002–7 August 2003. Geneva (Switzerland): World Health Organization; 2003. Available at: http://www.who.int/csr/sars/country/en/country2003_08_15.pdf. Accessed October 15, 2005.
8 OfnerM, LemM, Sarwal S, et al, for the SARS Investigative Team, Centers for Disease Control. Cluster of severe acute respiratory syndrome cases among protected health careworkers, Toronto, Canada, April 2003. MMWR Morb Mortal Wkly Rep 2003;52(19):433–6.
9 Loeb M, McGeer A, Henry B, Ofner M, Rose D, Hlywka T, Levie J, McQueen J, Smith S, Moss L, Smith A, Green K, Walter SD SARS among critical care nurses, Toronto. Emerg Infect Dis. 2004 Feb;10(2):251-5.
10 Kramer A, Schwebke I, Kampf G. How long do nosocomial pathogens persist on inanimate surfaces? A systematic review. BMC Infect Dis. 2006 Aug 16;6:130.
11 Ruderman C, Tracy CS, Bensimon CM, Bernstein M, Hawryluck L, Shaul RZ, Upshur RE. On pandemics and the duty to care: whose duty? who cares? BMC Med Ethics. 2006 Apr 20;7:E5.
Products…continued from page 20
NEWS FROM ELECTROMEDBill Grimm, RRT, Regional Manager, Western US, has recently received the award for volunteer excellence in programs from the American Lung Association of the Southwest. Grimm is responsible for the planning, development and recruitment of the sales team within his region. He has an extensive sales and clinical background as a respiratory therapist since 1980. In addition to holding roles as President of the Arizona Society of Respiratory Care and Vice President of the Board of Directors for the National Emphysema and COPD Association, Grimm currently sits on the editorial board for the COPD Digest as well as the Asthma Camp Committee for the state of Arizona. He was awarded the Chairman’s Award in 2008 by Electromed, Inc… Brad Blascziek recently joined Electromed as a Manufacturing Engineer and, soon after, was promoted to Manufacturing Manager. In this position he brings over 13 years of broad experience in manufacturing operations for various sized companies… Sherie Wheeler, CRT, RCP, has been promoted to Regional Manager (Central US) She is now responsible for the planning, development and recruitment of the sales team in her region. Ms Wheeler has nearly 30 years of experience in the respiratory industry and was formerly a respiratory therapist in various hospital settings including pulmonary rehabilitation, smoking cessation and patient education. Prior to joining Electromed, she was the Director of Programs at the American Lung Association of Iowa and directed the Camp for Kids with Cystic Fibrosis and Asthma. Contact electromed.com.

Respiratory Therapy Vol. 5 No. 1 n February-March 2010 31
Gastroesophageal Reflux in Mechanically Ventilated Pediatric Patients and Its Relation to Ventilator-Associated PneumoniaTarek A. Abdel-Gawad, Mostafa A. El-Hodhod, Hanan M. Ibrahim, Yousef W. Michael
AbstractIntroduction: The objective was to determine the frequency of gastroesophageal reflux (GER) in mechanically ventilated pediatric patients and its role as a risk factor for ventilator-associated pneumonia (VAP), which may be enhanced among those patients.
Methods: The study is a prospective cohort study of mechanically ventilated pediatric patients in the pediatric intensive care unit (PICU) of Ain Shams University Children’s Hospital. It was conducted in 24 mechanically ventilated patients (16 of them developed VAP and 8 did not, with mean age of 16.6 ±20.5 and 18.6 ±22.4 months respectively). Esophageal 24-hour pH-metry beside clinical and laboratory evaluation of their underlying problem and severity of their condition were carried out.
Results: All VAP patients had GER (50% alkaline reflux, 12.5% acidic reflux and 37.5% combined reflux) compared to 75% of non-VAP ones (100% alkaline reflux). The mean total reflux time was significantly longer among VAP (50 minutes) versus non-VAP (3 minutes) patients. There was significant increase in acidic reflux parameters among non-survivors versus survivors (P <0.001). For VAP mortality, total acidic reflux at a cut-off value of 28.6 minutes is found to be a mortality predictor with a sensitivity of 100% and a specificity of 100%.
Conclusions: GER is a constant incident in mechanically ventilated pediatric patients, with alkaline reflux being more common than acidic reflux. Both acidic and alkaline refluxes were found to be associated with the development of VAP and total reflux time was found to be a reliable predictor of VAP. Moreover, acidic reflux was found to be more related to mortality than alkaline reflux.
IntroductionVentilator associated pneumonia (VAP) refers specifically to nosocomial pneumonia that has developed in patients who are
receiving mechanical ventilation. VAP that occurs within 48 to 72 hours after tracheal intubation is usually termed early-onset pneumonia; it often results from aspiration, which complicates the intubation process.1
One of the most common recognized risk factors for VAP is the bacterial colonization of the gastric content with subsequent gastro-esophageal reflux (GER) and aspiration into the airways.2
In mechanically ventilated patients in the pediatric intensive care unit (PICU), the physiological environment differs substantially from that in the awake subject.3 Low or absent lower esophageal sphincter (LES) pressure in critically ill patients may be due to many factors including drugs such as adrenergic agonists, bronchodilators and opiates used for sedation during mechanical ventilation. Also, hypotension and sepsis may contribute.4
The acid clearance of the esophagus is a two-step process: volume clearance by esophageal peristalsis followed by chemical neutralization by swallowed salivary bicarbonate. Both of these elements are likely to be severely impaired in ventilated patients, as well as the esophageal motility being markedly impaired and salivary secretion being diminished by sleep.5 Also supine body positioning is one of the most important predisposing factors of GER and aspiration in mechanically ventilated patients.6
We hypothesized that GER occurs in ventilated non-pneumonic infants and children and is possibly a predisposing factor for VAP development in such patients. So the aim of the work was to determine the frequency of GER in mechanically ventilated patients and its role as a risk factor for VAP.
Materials and MethodsThis prospective cohort study was conducted in the PICU of the Ain Shams University Children’s Hospital. In this PICU the admission rate is 30 patients per month, with the total mortality in 2007 being 30%. The overall rate of mechanical ventilation in the same year was 70% with half of these patients developing VAP. The mortality among the VAP patients was very high (70%). Twenty-four critically ill pediatric patients admitted from March 2007 to September 2007 were chosen for the present study. All patients were mechanically ventilated and had been followed to select cases of late-onset VAP (after the first 72 hours of mechanical ventilation) by broncho-alveolar lavage (BAL) cultures at end of third, fifth and seventh day of mechanical ventilation. Moreover, if the Clinical Pulmonary Infection Score (CPIS) was found to be above 6 at any time, additional
The authors are with the Pediatric Department, Ain Shams Faculty of
Medicine, Cairo, Egypt. The authors would like to thank the patients and
their parents for accepting to be subjects of this work. They also thank
the teams working in the pediatric gastroenterology unit and PICU for
their cooperation and facilitating efforts. Reprinted from BioMed Central,
Critical Care, ccforum, © 2009 Abdel-Gawad et al; licensee BioMed Central
Ltd. This is an open access article distributed under the terms of the
Creative Commons Attribution License.

32 Respiratory Therapy Vol. 5 No. 1 n February-March 2010
BAL culture was considered. All patients were mechanically ventilated on pressure mode Pressure-Synchronized Intermittent Mandatory Ventilation (P-SIMV) and Continuous Positive Airway Pressure with Pressure support (CPAP with PS) using non-cuffed Polyvinyl endotraceal tubes. Patients with evidence of pneumonia at the time of mechanical ventilation, patients on antacids, H2 blockers or proton pump inhibitors were excluded from the study. All patients were nutritionally supported through total parenteral nutrition during the study period and use of nasogastric tube feeding was an exclusion criterion.
The study protocol was approved by the ethical committee of the Pediatrics Department, Ain Shams Faculty of Medicine in December 2006. Informed written consent was given by the parents/caregivers of all patients. When parents/caregivers were illiterate, the consent was read to them by a hospital social worker who was not involved in the study, and the consent form was witnessed by an independent third party.
A full medical history was taken from all patients which included name, age, sex, date, and cause of PICU admission, duration of PICU stay, setting of mechanical ventilation, history of medications, type of nutrition and the fate of all patients. Full clinical examination and estimation of the angle of back rest elevation was performed for all subjects. Evaluation was performed through applying the pediatric risk of mortality score (PRISM II)7 at the time of admission.
All subjects were studied with esophageal 24 hours pH-metry using Quick Start Orion II pH monitor MMS (Medical Measurement Systems Company, Enschede, The Netherlands) using a single-use, one-way catheter. The study has been performed within the first 24 hours from starting mechanical ventilation and after hemodynamic stabilization of the patient. The catheter was calibrated before use with two solutions, one acidic (pH=4) and the other alkaline (pH=7). The catheter was inserted in the lower esophagus 5 cm above the gastroesophageal sphincter (as detected by a plain film), and then the pH was recorded in 24 hours. The pH monitor recorded the reflux either acidic or alkaline through recording the pH, total reflux time, number of reflux episodes, and longest reflux.8 The reflux was considered pathological when the total reflux time exceeds 4% of total recording time.9
Statistical methods: All data were tabulated. Software Package
for Social Statistics version 13 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Numerical data were expressed as mean ±standard deviation, while categorical data were expressed as number and percent. A chi squared test was used to compare two groups of categorical data e.g., sex. Unpaired t-student test was used to compare numerical parametric data eg, age. Mann-Whitney U test was used to compare two groups of non-parametric data e.g., results of pH metry. Pearson r-test was used to correlate different parameters. Sensitivity and specificity were calculated to determine the predictive accuracy of different diagnostic test. Receiver Operating Characteristic (ROC) curves were used to illustrate the relation between sensitivity (proportion of true positive results) and specificity (proportion of false positive results). The area under the ROC curve (AUC) was determined and considered to be of good accuracy if more than 0.70. P value was calculated after each statistical test, and considered to be significant if less than 0.05 and highly significant if less than 0.01.
ResultsAccording to BAL results, patients were subdivided into two groups. Group A: This group included patients with VAP. There were 16 patients with a mean age of 16.6 ±20.5 months. There were 12 males (75%) and 4 females (25%), and after follow up of these cases, they had been subdivided into 12 non-survivors and 4 survivors patients. Group B: This included patients who did not develop VAP and acted as a control group. There were 8 patients with a mean age of 41 ±50.7 months. There were 6 males and 2 females.
Age was not statistically different between the VAP patients and the control patients without VAP (mean age of 16.6 ±20.5 and 18.6 ±22.4 months, respectively). The original diagnosis among VAP patients was 2 with encephalitis, 1 with Guillain Barre Syndrome, 1 with Werding Hoffman disease, 4 with gastro-enteritis and shock, 2 with intracranial hemorrhage, 2 with onchological problems with central nervous system (CNS) infiltrates, 2 with acute severe asthma and 2 patients with acute bronchiolitis. The original diagnosis among non-VAP patients was 1 with encephalitis, 1 with Werding Hoffman disease, 2 with atonic cerebral palsy, 2 with acute leukemia with CNS infiltrates and 2 patients with congenital cyanotic heart disease. There was no statistically significant difference between VAP and non-VAP patients as regards PRISM II score (18.7 ±3.6 versus 17 ±3.2, respectively). Similarly, there was no significant difference
Available online http://ccforum.com/content/13/5/R164
Page 3 of 5(page number not for citation purposes)
non-VAP patients was 1 with encephalitis, 1 with WerdingHoffman disease, 2 with atonic cerebral palsy, 2 with acuteleukemia with CNS infiltrates and 2 patients with congenitalcyanotic heart disease. There was no statistically significantdifference between VAP and non-VAP patients as regardsPRISM II score (18.7 ± 3.6 versus 17 ± 3.2, respectively).Similarly, there was no significant difference between VAP andnon-VAP patients as regards the initial ventilatory settings(Respiratory rate was 48.58 ± 0.51 versus 41.50 ± 10.89; P> 0.05, Peak Inspiratory Pressure (PIP) was 17.00 ± 2.71 ver-sus 17.65 ± 0.81; P > 0.05, positive end-expiratory pressure(PEEP) was 4.00 ± 0.00 versus 4.00 ± 0.00, PS was 12.40± 0.27 versus 13.10 ± 0.94; P > 0.05 and fraction of inspiredoxygen (FiO2) was 79.8 ± 0.8% versus 75.00 ± 1.12; P >0.05). On day 5, the ventilatory settings were worsened in theVAP group and started to improve in the non-VAP one (respi-ratory rate was 55.13 ± 0.45 versus 38.12 ± 1.13, P < 0.05,PIP was 20.02 ± 0.4 versus 14.12 ± 0.65, P < 0.05, PEEPwas 6.000 ± 0.08 versus 4.000 ± 0.00, P < 0.05, PS was12.402 ± 0.27 versus 8.12 ± 0.36, P < 0.05, FiO2 was 80.24± 0.9% versus 50.14 ± 3.43, P < 0.05)
Regarding the drug use for patients, sedative use was not sig-nificantly different between VAP (10/16) and non-VAP (6/8)patients (P > 0.05). Inotropes have been used with the initia-tion of mechanical ventilation in 2 of 8 non-VAP patients and 5of 16 VAP patients with a non-significant difference. Addition-ally, 9 VAP patients needed inotropes that were started fromday 4 to day 7 after development of VAP because of a deteri-oration in their condition. All non-survivors were on inotropes.
BAL culture results revealed that Klebsiella was the most com-mon organism responsible for VAP among this group (7/16),
followed by Acinetobacter (5/16), Staphylococcus aureus (2/16) and Enterococci (2/16)
GER was demonstrated in all patients with VAP (100%) com-pared with non-VAP (75%) patients. Alkaline reflux was themost frequent finding seen in both groups with no significantdifference between them. Acid reflux whether isolated or com-bined with alkaline reflux was significantly seen in VAP (50%)compared with non-VAP (0%) patients.
Results of 24 hours pH-metry (Table 1) showed that total acidreflux time and its percentage, number of acid reflux episodes,number of long acid reflux episodes (>5 minutes), longest acidreflux time in minutes, acid reflux index and total reflux timewere significantly higher among VAP compared with non-VAPpatients.
The mortality of VAP patients was seen to be significantly highamong acid reflux (100%) and mixed reflux (100%) patientscompared with alkaline reflux (50%) patients. Overwhelmingly,sepsis and sepsis-induced multi-organ system failure was thedirect cause of death in all cases.
Regarding the acid reflux parameters (Table 2) in relation tomortality outcome it was shown that total acid reflux time andits percentage, number of acid reflux episodes, number of longacid reflux episodes (>5 minutes), longest acid reflux time andacid reflux index were significantly higher among non-survivorsthan survivors with VAP. Lowest pH reached was significantlylower in non-survivors compared with survivors. Alkaline refluxparameters were not different between survivors and non-sur-vivors.
Table 1
Comparison of pH metric results (median and range) in patients with ventilator associated pneumonia and controls
pH metric results Patients(n = 16)
Control(n = 8)
P-value by MWUT
Total acid reflux time (min) (pH 4) (acid pH) 50 (1.75-393) 3 (0.7-4.4) <0.05
Total acid reflux time (%) (pH 4%) (acid pH) 3.9 (0.12-31.3) 0.2 (0.05-2.3) <0.05
Number of acid reflux episodes 6.5 (0.75-16.5) 1 (0.25-2.5) <0.05
Number of long acid reflux episode >5 minutes 1.5 (0-3.7) 0 (0-0) <0.05
Longest acid reflux time 40.9 (0.97-140) 2.6 (0.4-4.42) <0.05
Lowest pH reached 0 (0-3.9) 1.15 (0-2.97) >0.05
Acid reflux index 0.35 (0.02-70) 0.05 (0-0.1) <0.05
Total alkaline time (min) 1068 (238-1185) 463 (221-847) >0.05
Total alkaline time (%) 69.3 (27.1-89.2) 36.2 (7.9-60) >0.05
Total reflux time (%) 83.2 (45.6-93.4) 36.3 (18-61) <0.05
MWUT = Mann-Whitney U-test; VAP = ventilator acquired pneumonia.

Respiratory Therapy Vol. 5 No. 1 n February-March 2010 33
between VAP and non-VAP patients as regards the initial ventilatory settings (Respiratory rate was 48.58 ±0.51 versus 41.50 ±10.89; P >0.05, Peak Inspiratory Pressure (PIP) was 17.00 ±2.71 versus 17.65 ±0.81; P >0.05, positive end-expiratory pressure (PEEP) was 4.00 ±0.00 versus 4.00 ±0.00, PS was 12.40 ±0.27 versus 13.10 ±0.94; P >0.05 and fraction of inspired oxygen (FiO2) was 79.8 ±0.8% versus 75.00 ±1.12; P >0.05). On day 5, the ventilatory settings were worsened in the VAP group and started to improve in the non-VAP one (respiratory rate was 55.13 ±0.45 versus 38.12 ±1.13, P <0.05, PIP was 20.02 ±0.4 versus 14.12 ±0.65, P <0.05, PEEP was 6.000 ±0.08 versus 4.000 ±0.00, P <0.05, PS was 12.402 ±0.27 versus 8.12 ±0.36, P <0.05, FiO2 was 80.24 ±0.9% versus 50.14 ±3.43, P <0.05)
Regarding the drug use for patients, sedative use was not significantly different between VAP (10/16) and non-VAP (6/8) patients (P >0.05). Inotropes have been used with the initiation of mechanical ventilation in 2 of 8 non-VAP patients and 5 of 16 VAP patients with a non-significant difference. Additionally, 9 VAP patients needed inotropes that were started from day 4 to day 7 after development of VAP because of a deterioration in their condition. All non-survivors were on inotropes.
BAL culture results revealed that Klebsiella was the most common organism responsible for VAP among this group (7/16), followed by Acinetobacter (5/16), Staphylococcus aureus (2/16) and Enterococci (2/16)
GER was demonstrated in all patients with VAP (100%) compared with non-VAP (75%) patients. Alkaline reflux was the most frequent finding seen in both groups with no significant difference between them. Acid reflux whether isolated or combined with alkaline reflux was significantly seen in VAP (50%) compared with non-VAP (0%) patients.
Results of 24 hours pH-metry (Table 1) showed that total acid reflux time and its percentage, number of acid reflux episodes, number of long acid reflux episodes ( >5 minutes), longest acid reflux time in minutes, acid reflux index and total reflux time were significantly higher among VAP compared with non-VAP patients.
The mortality of VAP patients was seen to be significantly high among acid reflux (100%) and mixed reflux (100%) patients compared with alkaline reflux (50%) patients. Overwhelmingly,
sepsis and sepsis-induced multi-organ system failure was the direct cause of death in all cases.
Regarding the acid reflux parameters (Table 2) in relation to mortality outcome it was shown that total acid reflux time and its percentage, number of acid reflux episodes, number of long acid reflux episodes (>5 minutes), longest acid reflux time and acid reflux index were significantly higher among non-survivors than survivors with VAP. Lowest pH reached was significantly lower in non-survivors compared with survivors. Alkaline reflux parameters were not different between survivors and non-survivors.
ROC curves of predictability of VAP and mortality showed that a total reflux time of 74.65 minutes per day has 75% sensitivity and 100% specificity for VAP development, while acidic reflux time of 28.6 minutes per day has 100% sensitivity and specificity for mortality prediction among VAP patients.
DiscussionIn the current study we found that GER occurred in up to 91.6% of all mechanically ventilated critically ill patients of either VAP or non-VAP patients. Many previous studies reported that the incidence of GER is increased in critically ill mechanically ventilated patients with the acidic reflux reaching up to 80% and bile reflux (duodenogastroesophageal reflux (DGER)) reaching up to 60%.3,10 Another study found that the GER reached up to 74% in patients with nasogastric tube (NGT) which increased to 81% in supine position.11 The patients are defined to have abnormal esophageal bile reflux (DGER) if the fraction of the time that the esophageal mucosa is exposed to alkaline refluxate exceeds 4% of the total study time and pathological acidic reflux if the fraction of the time that the esophageal mucosa is exposed to a refluxate with pH less than 4 exceeds 4% of the total recording time.12 Previous studies demonstrated that sedatives3 and adrenergic drugs13 do increase reflux. In the current study, a great proportion of the studied patients were on those suspected medications; however, the frequency of use was not different between VAP and non-VAP groups.
In the present study, there was a significant increase in GER parameters including total acidic time, number of reflux episodes, number of long reflux episodes longer than five minute, longest reflux time, reflux index and total reflux time in VAP than non-VAP patients. Alkaline reflux was more common
Critical Care Vol 13 No 5 Abdel-Gawad et al.
Page 4 of 5(page number not for citation purposes)
ROC curves of predictability of VAP and mortality showed thata total reflux time of 74.65 minutes per day has 75% sensitivityand 100% specificity for VAP development, while acidic refluxtime of 28.6 minutes per day has 100% sensitivity and specif-icity for mortality prediction among VAP patients.
DiscussionIn the current study we found that GER occurred in up to91.6% of all mechanically ventilated critically ill patients ofeither VAP or non-VAP patients. Many previous studiesreported that the incidence of GER is increased in critically illmechanically ventilated patients with the acidic reflux reachingup to 80% and bile reflux (duodenogastroesophageal reflux(DGER)) reaching up to 60% [3,10]. Another study found thatthe GER reached up to 74% in patients with nasogastric tube(NGT) which increased to 81% in supine position [11]. Thepatients are defined to have abnormal esophageal bile reflux(DGER) if the fraction of the time that the esophageal mucosais exposed to alkaline refluxate exceeds 4% of the total studytime and pathological acidic reflux if the fraction of the timethat the esophageal mucosa is exposed to a refluxate with pHless than 4 exceeds 4% of the total recording time [12]. Pre-vious studies demonstrated that sedatives [3] and adrenergicdrugs [13] do increase reflux. In the current study, a great pro-portion of the studied patients were on those suspected med-ications; however, the frequency of use was not differentbetween VAP and non-VAP groups.
In the present study, there was a significant increase in GERparameters including total acidic time, number of reflux epi-sodes, number of long reflux episodes longer than five minute,longest reflux time, reflux index and total reflux time in VAP thannon-VAP patients. Alkaline reflux was more common than
acidic one, and there was no statistically significant differencein alkaline pH parameters between VAP and non-VAPpatients. The use of acid suppressive medications werereported to increase frequency of non acid reflux [14]; how-ever, in the present study, patients using these medicationswere excluded. The demonstrated alkaline reflux can beexplained by duodenogastric reflux. Duodenogastric reflux isthe retrograde flow of duodenal contents into the stomach thatthen mix with acid and pepsin. These agents can reflux into theesophagus (ie, DGER) and cause gastro-esophageal refluxdisease [15].
The mortality rate in our study among VAP patients was 75%,but in non-VAP patients was 25%. The difference was statisti-cally significant. In general this high mortality rate can be attrib-uted to the highly pathogenic organisms that have beenisolated in cultures as well as the pulmonary devitalizing effectof severe acid reflux. This was in agreement with other work[16,17] that reported high mortality rate of VAP patients.
In the current study, all acidic parameters of pH metric resultswere significantly higher among non-survivors indicating astrong relation between acidic reflux and high mortality rate inVAP patients. Acid and pepsin are the major factors responsi-ble for symptoms and esophageal mucosal damage in gastro-esophageal reflux disease. Several investigators, however,have shown that the association between frequency of symp-toms and severity of mucosal lesions on one hand, and theamount of the esophageal acid exposure on the other one, isnot as straightforward as one might expect. The occurrence ofsymptoms is influenced by mucosal sensitivity, which is onlypartly dependent on increased esophageal acid exposure[18].
Table 2
Comparison of pH metric results and total reflux time (median and range) in survivors and non survivors among cases of ventila tor associated pneumonia
Variables Survivors(n = 4)
Non survivors(n = 12)
P-value by MWUT
Total acid reflux time (min) (pH 4) 0 (0-0) 183 (29-425.5) <0.01
Total acid reflux time (%) (pH 4%) 0 (0-0) 14.4 (2.1-34) <0.01
Number of acid reflux episodes 0 (0-0) 9.5 (6-18) <0.01
Number of long acid reflux episode >5 mins 0 (0-0) 2.5 (1-4) <0.05
Longest acid reflux time 0 (0-0) 91.8 (26.2-144.9) <0.01
Lowest pH reached 5 (4.7-5.3) 0 (0-0) <0.01
Acid reflux index 0 (0-0) 0.55 (0.3-0.7) <0.01
Total alkaline time (min) 636 (65.8-1206) 1068 (755-1122) >0.05
Total alkaline time (%) 53 (21.9-85.5) 69.3 (42.7-90) >0.05
Total reflux time (%) 53 (21.9-85.5) 83 (80.1-96) >0.05
MWUT = Mann-Whitney U-test.

34 Respiratory Therapy Vol. 5 No. 1 n February-March 2010
than acidic one, and there was no statistically significant difference in alkaline pH parameters between VAP and non-VAP patients. The use of acid suppressive medications were reported to increase frequency of non acid reflux;14 however, in the present study, patients using these medications were excluded. The demonstrated alkaline reflux can be explained by duodenogastric reflux. Duodenogastric reflux is the retrograde flow of duodenal contents into the stomach that then mix with acid and pepsin. These agents can reflux into the esophagus (ie, DGER) and cause gastro-esophageal reflux disease.15
The mortality rate in our study among VAP patients was 75%, but in non-VAP patients was 25%. The difference was statistically significant. In general this high mortality rate can be attributed to the highly pathogenic organisms that have been isolated in cultures as well as the pulmonary devitalizing effect of severe acid reflux. This was in agreement with other work16,17 that reported high mortality rate of VAP patients.
In the current study, all acidic parameters of pH metric results were significantly higher among non-survivors indicating a strong relation between acidic reflux and high mortality rate in VAP patients. Acid and pepsin are the major factors responsible for symptoms and esophageal mucosal damage in gastroesophageal reflux disease. Several investigators, however, have shown that the association between frequency of symptoms and severity of mucosal lesions on one hand, and the amount of the esophageal acid exposure on the other one, is not as straightforward as one might expect. The occurrence of symptoms is influenced by mucosal sensitivity, which is only partly dependent on increased esophageal acid exposure.18
In view of similar base line PRISM results and other circumstantial risk factors between VAP and non-VAP groups, the significant association between acidic reflux and mortality in VAP group points to its detrimental effects in this group of patients.
ConclusionsIn conclusion, GER is a permanent incident in mechanically ventilated pediatric patients who were not on antacid therapy. Alkaline reflux is found to be more common than acidic reflux. Both acidic and alkaline refluxes were found to be associated with the development of VAP. Total reflux time was found to be a reliable predictor of developing VAP in these patients. Nevertheless, acidic reflux was found to be related more to high mortality among them. • GER is almost constant in ventilated children and is greatly linked to development of VAP. • Alkaline reflux is more common than acidic reflux. • Acidic reflux is more linked to mortality in such a group of patients.
References1 Chastre J, Fagon JY: Diagnosis of ventilator-associated
pneumonia. N Engl J Med 2007, 356:1469.2 du Moulin GC, Paterson DG, Hedley-Whyte J, Lisbon A:
Aspiration of gastric bacteria in antacid-treated patients: a frequent cause of postoperative colonization of the airway. Lancet 1982, 1:242-245.
3 Nind G, Chen WH, Protheroe R, Iwakiri K, Fraser R, Young R, Chapman M, Nguyen N, Sifrim D, Rigda R, Holloway RH: Mechanisms of gastro-esophageal reflux in critically ill mechanically ventilated patients. Gastroenterology 2005, 128:600-606.
4 Fan YP, Chakder S, Gao F, Rattan S: Inducible and
neuronal nitric oxide synthase involvement in lipopolysaccharideinduced sphincteric dysfunction. Am J Physiol Gastrointest Liver Physiol 2001, 280:G32-42.
5 Kölbel CB, Rippel K, Klar H, Singer MV, van Ackern K, Fiedler F: Esophageal motility disorders in critically ill patients: a 24-hour manometric study. Intensive Care Med 2000, 26:1421-1427.
6 Torres A, Serra-Batlles J, Ros E, Piera C, Puig de la Bellacasa J, Cobos A, Lomeña F, Rodríguez-Roisin R: Pulmonary aspiration of gastric contents in patients receiving mechanical ventilation the effect of body position. Ann Intern Med 1992, 116:540-543.
7 Pollack MM, Ruttimann UE, Getson PR: Pediatric risk of mortality (PRISM) score. Crit Care Med. 1988, 16:1110-1116.
8 Cavataio F, Guandalini S: Gastroesophageal reflux. In Essential Pediatric Gastroenterology and Nutrition Edited by: Guandalini S. New York, NY: McGraw-Hill; 2005:157-173.
9 Wilmer A, Tack J, Frans E, Dits H, Vanderschueren S, Gevers A, Bobbaers H: Duodenogastroesophageal reflux and esophageal mucosal injury in mechanically ventilated patients. Gastroenterology 1999, 116:1293-1299.
10 Xin Y, Dai N, Zhao L, Wang JG, Si JM: The effect of famotidine on gastro-esophageal and duodenogastro-esophageal refluxes in critically ill Patients. World J Gastroenterol 2003, 9:356-358.
11 Ibáñez J, Peñafiel A, Marsé P, Jordá R, Raurich JM, Mata F: Incidence of gastroesophageal reflux and aspiration in mechanically ventilated patients using small-bore nasogastric tubes. JPEN J Parenter Enteral Nutr. 2000, 24:103-106.
12 Richter JE, Bradley LA, DeMeester TR, Wu WC: Normal 24-hr ambulatory esophageal pH values. Influence of study center, pH electrode, age and gender. Dig Dis Sci 1992, 37:849-856.
13 Crowell MD, Zayat EN, Lacy BE, Schettler-Duncan A, Liu MC: The effects of an inhaled beta (2)-adrenergic agonist on lower esophageal function: a dose-response study. Chest 2001, 120:1184-1189.
14 Orr WC, Craddock A, Goodrich S: Acidic and non-acidic reflux during sleep under conditions of powerful acid suppression. Chest 2007, 131:460-465.
15 Hak NG, Mostafa M, Salah T, El-Hemaly M, Haleem M, Abd El-Raouf A, Hamdy E: Acid and bile reflux in erosive reflux disease, non-erosive reflux disease and Barrett’s esophagus. Hepatogastroenterology 2008, 55:442-447.
16 Alp E, Güven M, Yildiz O, Aygen B, Voss A, Doganay M: Incidence, risk factors and mortality of nosocomial pneumonia in intensive care units: a prospective study. Ann Clin Microbiol Antimicrob. 2004, 3:1-17.
17 Srinivasan R, Asselin J, Gildengorin G, Wiener-Kronish, Flori HR: A prospective study of ventilator-associated pneumonia in children. Pediatrics. 2009, 123:1108-1115.
18 Trimble KC, Pryde A, Heading RC: Lowered esophageal sensory thresholds in patients with symptomatic but not excess gastro- esophageal reflux: evidence for a spectrum of visceral sensitivity in GERD. Gut 1995, 37:7-12.
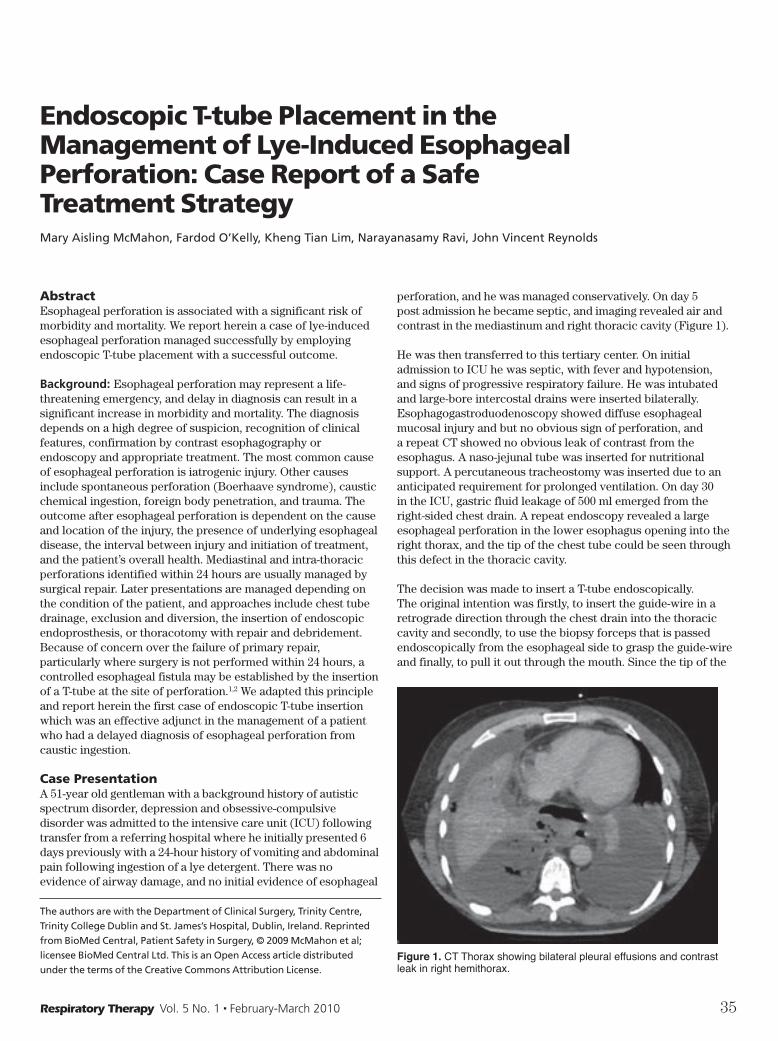
Respiratory Therapy Vol. 5 No. 1 n February-March 2010 35
Endoscopic T-tube Placement in the Management of Lye-Induced Esophageal Perforation: Case Report of a Safe Treatment StrategyMary Aisling McMahon, Fardod O’Kelly, Kheng Tian Lim, Narayanasamy Ravi, John Vincent Reynolds
AbstractEsophageal perforation is associated with a significant risk of morbidity and mortality. We report herein a case of lye-induced esophageal perforation managed successfully by employing endoscopic T-tube placement with a successful outcome.
Background: Esophageal perforation may represent a life-threatening emergency, and delay in diagnosis can result in a significant increase in morbidity and mortality. The diagnosis depends on a high degree of suspicion, recognition of clinical features, confirmation by contrast esophagography or endoscopy and appropriate treatment. The most common cause of esophageal perforation is iatrogenic injury. Other causes include spontaneous perforation (Boerhaave syndrome), caustic chemical ingestion, foreign body penetration, and trauma. The outcome after esophageal perforation is dependent on the cause and location of the injury, the presence of underlying esophageal disease, the interval between injury and initiation of treatment, and the patient’s overall health. Mediastinal and intra-thoracic perforations identified within 24 hours are usually managed by surgical repair. Later presentations are managed depending on the condition of the patient, and approaches include chest tube drainage, exclusion and diversion, the insertion of endoscopic endoprosthesis, or thoracotomy with repair and debridement. Because of concern over the failure of primary repair, particularly where surgery is not performed within 24 hours, a controlled esophageal fistula may be established by the insertion of a T-tube at the site of perforation.1,2 We adapted this principle and report herein the first case of endoscopic T-tube insertion which was an effective adjunct in the management of a patient who had a delayed diagnosis of esophageal perforation from caustic ingestion.
Case PresentationA 51-year old gentleman with a background history of autistic spectrum disorder, depression and obsessive-compulsive disorder was admitted to the intensive care unit (ICU) following transfer from a referring hospital where he initially presented 6 days previously with a 24-hour history of vomiting and abdominal pain following ingestion of a lye detergent. There was no evidence of airway damage, and no initial evidence of esophageal
The authors are with the Department of Clinical Surgery, Trinity Centre,
Trinity College Dublin and St. James’s Hospital, Dublin, Ireland. Reprinted
from BioMed Central, Patient Safety in Surgery, © 2009 McMahon et al;
licensee BioMed Central Ltd. This is an Open Access article distributed
under the terms of the Creative Commons Attribution License.
perforation, and he was managed conservatively. On day 5 post admission he became septic, and imaging revealed air and contrast in the mediastinum and right thoracic cavity (Figure 1).
He was then transferred to this tertiary center. On initial admission to ICU he was septic, with fever and hypotension, and signs of progressive respiratory failure. He was intubated and large-bore intercostal drains were inserted bilaterally. Esophagogastroduodenoscopy showed diffuse esophageal mucosal injury and but no obvious sign of perforation, and a repeat CT showed no obvious leak of contrast from the esophagus. A naso-jejunal tube was inserted for nutritional support. A percutaneous tracheostomy was inserted due to an anticipated requirement for prolonged ventilation. On day 30 in the ICU, gastric fluid leakage of 500 ml emerged from the right-sided chest drain. A repeat endoscopy revealed a large esophageal perforation in the lower esophagus opening into the right thorax, and the tip of the chest tube could be seen through this defect in the thoracic cavity.
The decision was made to insert a T-tube endoscopically. The original intention was firstly, to insert the guide-wire in a retrograde direction through the chest drain into the thoracic cavity and secondly, to use the biopsy forceps that is passed endoscopically from the esophageal side to grasp the guide-wire and finally, to pull it out through the mouth. Since the tip of the
Figure 1. CT Thorax showing bilateral pleural effusions and contrast leak in right hemithorax.

36 Respiratory Therapy Vol. 5 No. 1 n February-March 2010
chest drain was in continuity with the perforation, the guide-wire was firstly, inserted in an antegrade direction into the esophagus and out onto the chest wall through the right-sided chest drain (Figure 2). Secondly, the T-tube was attached to the guide-wire outside the mouth and then pulled through orally into the esophagus with the main stem of the T-tube pulled out onto the skin after the chest drain had been removed (Figure 3). Finally, the proximal and distal limbs of the T-tube were positioned in the esophagus and stomach respectively with the help of biopsy forceps (Figures 4 & 5).
A follow up tubogram showed good flow of contrast into the stomach and esophagus via the T limbs with no leak of contrast from the site of perforation (Figure 6). The T-tube was left on free drainage and allowed tract to mature. The patient’s condition gradually recovered and he was transferred to the ward on day 45. Oral nutrition was tolerated well without sequelae. The T-tube was removed on day 60 and the patient discharged well. He remains well at 6 months of follow-up.
Stomach
Perforatedesophagus
Thocaciccavity
Chestdrain
Guide-wire
Chestdrain
Thocaciccavity
Perforatedesophagus
Stomach
T-tube attached to the guide-wire
Stomach
Thocaciccavity
Perforatedesophagus
T-tube
Figure 2. Endoscopic antegrade insertion of guide-wire into the chest drain.
Figure 5. Esophageal T-tube can be seen on the right and nasojejunal feeding tube on the left.
Figure 3. Attachment of T-tube to the guide-wire which is then pulled through orally into the esophagus.
Figure 4. Position of T-tube in the esophagus, stomach and through the esophageal perforation and thoracic cavity.
DiscussionEsophageal perforation is associated with significant morbidity and mortality.3 It is unassailable that the best outcomes will be achieved in specialist units with appropriate expertise in esophageal surgery, interventional radiology, and intensive care. The choice of management depends on a number of factors, including etiology, location of perforation, condition of esophageal tissue, and the overall health of the patient. The length of time from injury to diagnosis profoundly influences the management approach, with an early ( <24 hrs) diagnosis often managed surgically in contrast to a more conservative approach for the majority of cases presenting later than 24 hrs.
Esophageal tissue is less amenable to repair after the first 24 hours. In a review, Brinster et al reported that primary repair of early esophageal perforations is associated with a low incidence of leak and a mortality rate of 10%, but that the mortality of surgery beyond 24 hours approaches 40%, and this may be associated with a high incidence of fistula.3 A number of reports accordingly have encouraged the use of T-tube insertion for late presentations, with reports of its safety and efficacy, and some use it for all cases.2,4-7
Figure 6. T-tubogram demonstrated good passage of contrast in both limbs without any leak.

Respiratory Therapy Vol. 5 No. 1 n February-March 2010 37
In this case, the delay in diagnosis and the initial assessment of a healed perforation suggested that a non-operative course was appropriate as long as the mediastinal and thoracic sepsis could be adequately drained. When gastric contents presented themselves via the chest drain a full month following the initial insult, we adapted this principle and were able simply to place the T-tube using the combination of access via endoscopy and the intercostal chest tube, thus establishing a controlled fistula. The exclusion criterion for this novel endoscopic treatment is acute esophageal perforation within first 24 hours. It is an option for delayed diagnosis of esophageal perforation. We acknowledge that the subsequent improvement in his clinical condition may have occurred in any case, and the perforation may eventually have healed, but we wish to highlight the ease of this technique and the benefits in terms of advancing his oral intake and a successful outcome.
ConclusionThis case report highlights the safety, simplicity and efficacy of T-tube drainage in the management of delayed esophageal perforation.
References1 Abbott OA, Mansour KA, Logan WD Jr, Hatcher CR Jr,
Symbas PN: Atraumatic so-called “spontaneous” rupture of the esophagus. A review of 47 personal cases with comments on a new method of surgical therapy. J Thorac Cardiovasc Surg 1970, 59:67-83.
2 Griffin SM, Lamb PJ, Shenfine J, Richardson DL, Karat D, Hayes N: Spontaneous rupture of the oesophagus. Br J Surg 2008, 95:1115-20.
3 Naylor AR, Walker WS, Dark J, Cameron EW: T tube intubation in the management of seriously ill patients with oesophagopleural fistulae. Br J Surg 1990, 77:40-2.
4 Brinster CJ, Singhal S, Lee L, Marshall MB, Kaiser LR, Kucharczuk JC: Evolving options in the management of esophageal perforation. Ann Thorac Surg 2004, 77:1475-1483.
5 Bufkin BL, Miller JI Jr, Mansour KA: Esophageal Perforation: Emphasis on Management. Ann Thorac Surg 1996, 61:1447-1451.
6 Sakamoto Y, Tanaka N, Furuya T, Ueno T, Okamoto H, Nagai M, Murakawa T, Takayama T, Mafune K, Makuuchi M, Nobori M: Surgical management of late esophageal perforation. Thorac Cardiovasc Surg 1997, 45:269-72.
7 Linden PA, Bueno R, Mentzer SJ, Zellos L, Lebenthal A, Colson YL, Sugarbaker DJ, Jaklitsch MT: Modified T-Tube Repair of Delayed Esophageal Perforation Results in a Low Mortality Rate Similar to That Seen With Acute Perforations. Ann Thorac Surg 2007, 83:1129-1133.
RATIONINGIt’s clear, then, based on the foregoing, that some sort of rationing will take place, and that, based on current availability of ventilators, it is inevitable. Some people will live, some will die. Scienceblogs.com recently reported on the actual numbers of people likely to affected by a major pandemic outbreak. (For a comprehensive calculation, go to PLoS Currents/Influenza, Zilberberg, et al.) Using a basic statistical approach, researchers have calculated that a pandemic attack rate would represent between 37 and 55 million people: “US pop: 300 million. Cases: 46 million (averaged). Hospitalizations: 2.8 million. On ventilators: 132,000. Deaths: 192,000.” Of course these figures are speculative. A recent report by Eurosurveillance, in a smaller population, using a 30% infection rate, predicted between 3,600 to 54,000 deaths. That’s a big point spread, especially since a 30% infection rate would jump the US death rate to about 400,000.
Thus we have estimates for the US that go from 3,600 to 400,000 deaths. The report underscores that no matter how you slice the numbers, the inevitable conclusion, already anticipated by New York State, is the dreaded word, rationing. The website Politico has reported on the contentious debates about the subject. According to an article by Josh Gerstein, “Members of a federal panel advising the Centers for Disease Control on guidelines for how ventilators should be allocated in the event swine flu worsens responded forcefully and… angrily to suggestions that the effort would cavalierly snuff out the lives of those deemed unworthy.” A conferee noted, “If we otherwise keep presuming we’re not going to build for the peak of a severe pandemic, in case this current one even if it comes back in waves isn’t, then we end up going down this road… It’s kind of Hitlerian. You’re going to have to decide who isn’t worthy to live and I think that’s the basic ethical consideration that should be raised and not just accept the kind of triage decisions you’re making. There’s triage in the case of absolute catastrophe, but not self made catastrophe.”
But of course dragging Hitler into any argument means one has reached the nadir of that argument, foreclosing further discussion, and we are now into mere name-calling. Not that this kind of “debate” hasn’t also become a pandemic of sorts in our national dialogue.
So let’s take a breath, while we can. I realize I have ranged far and wide in this discussion, but the subject reaches far and wide. Still, you have to start somewhere. A good place to begin would be for RTs to think about, at the least, finding out what plans their healthcare institutions have in case of a pandemic, and take it from there.
Les Plesko, Editor
Editorial…continued from page 4

38 Respiratory Therapy Vol. 5 No. 1 n February-March 2010
AbstractBackground: Fatigue in COPD impairs functional status; however there are few studies examining mechanistic pathways of this symptom. The aims of this study are to compare fatigue between COPD patients and healthy age-matched subjects, and to identify predictors of fatigue in COPD.
Methods: Seventy four COPD patients, mean age 69.9 (49-87) yrs, mean (SD) % predicted FEV1 46.5 (20.0) % and FEV1/FVC ratio 0.45 (0.13) and 35 healthy subjects, mean age 67.1 (50-84) yrs completed the Multidimensional Fatigue Inventory (MFI 20). Patients’ assessment included Depression (HADS), lung function, BMI, muscle strength, incremental shuttle walk test (ISWT), exercise oxygen saturation (SpO2), Borg breathlessness (CR-10) and exertion (RPE). Serum level of Interleukin 6 (IL-6) was recorded. Differences in MFI 20 between groups were examined and predictors of fatigue identified using logistic regression.
Results: Significant differences (p <0.01) were found between the COPD and healthy subjects for all MFI 20 dimensions. There were significant differences when classified according to GOLD and dyspnea stages for selected dimensions only. Predictors of General Fatigue were depression, muscle strength and end SpO2
(R2=.62); of Physical Fatigue: depression, % predicted FEV1, ISWT and age (R2=.57); Reduced Activity: % predicted FEV1, BMI and depression (R2=.36); Reduced Motivation: RPE, depression and end SpO2 (R2=.37) and Mental Fatigue: depression and end SpO2 (R2=.38).
Conclusion: All dimensions of fatigue were higher in COPD than healthy aged subjects. Predictive factors differ according to the dimension of fatigue under investigation. COPD-RF is a multi component symptom requiring further consideration.
Evaluation of Psychological and Physiological Predictors of Fatigue in Patients with COPDAgnieszka Lewko, Penelope L. Bidgood, Rachel Garrod
Agnieszka Lewko is with the Faculty of Health and Social Care Sciences,
St George’s University of London; Lewko is also with Kingston Universitiy,
Cranmer Terrace, London; Bidgood is with the Faculty of Computing,
Information Systems and Mathematics, Kingston University, Kingston
upon Thames, Surrey; Garrod is with Kings College NHS Foundation Trust,
Dulwich Hospital, London. The authors wish to gratefully acknowledge
the contribution of GlaxoSmithKline UK and the Therapies Services of
St. George’s NHS Trust, London, UK to this research. Reprinted from BMC
Pulmonary Medicine, © 2009 Lewko et al; licensee BioMed Central Ltd.
This is an Open Access article distributed under the terms of the Creative
Commons Attribution License.
BackgroundFatigue, as a symptom in chronic obstructive pulmonary disease (COPD) may have diverse manifestations, such as physical or mental tiredness, loss of attention, concentration or motivation.1,2 It is an important3-5 and highly prevalent symptom6-7 with data from one study suggesting that 90% of COPD patients may report fatigue.6 Although fatigue in COPD is acknowledged by clinicians, it is often neglected. In fact, compared with cancer the predictors and patho-mechanisms of fatigue are poorly evaluated in COPD and there is a lack of understanding regarding the management of fatigue. There are evident associations between fatigue, impaired quality of life and increased depression.8-10 Furthermore, fatigue and dyspnea in COPD, whilst related, appear to be separate entities.11,4 Using the FACIT-fatigue unidimensional scale, no association between disease severity and fatigue is noted.8 However, the Multidimensional Fatigue Inventory (MFI 20),12 which is well validated in COPD and shows moderate relationships with airflow obstruction.10,13 The MFI 20 provides a multi-dimensional evaluation of fatigue, enabling investigation of the different components. Since several factors are likely to be involved in the development of COPD related fatigue (COPD-RF), the use of a multi-dimensional tool enables further elucidation of mechanistic pathways. For instance, whilst hypoxia and hypoxaemia, impaired fat free mass and loss of fatigue resistant muscle fibres are associated with fatigue,14 it is not known if the variables relate to physical or mental fatigue specifically. In healthy subjects, acute exercise fatigue is associated with raised levels of Interleukin 6 (IL6);15,16 possibly, this pathway is important in the development of COPD-RF.17 There are few studies that comprehensively investigate predictors of the different domains of fatigue in COPD. This study attempts to draw together the psychological and physiological aspects of fatigue to develop working models of COPD-RF, by using comparative data from healthy age-matched subjects. This research hypothesises that increases in each component of fatigue in COPD may be predicted by differing factors. The aims of this study were firstly, to provide comparative data of fatigue, using the MFI 20, between COPD patients and healthy elderly subjects and secondly, to explore possible predictors of fatigue components of the MFI 20.
MethodsFull ethical consent was obtained for this cross sectional study from the Royal Marsden Local Research Ethics Committee (London, UK). Patients and control subjects gave written informed consent prior to entering the study.

Respiratory Therapy Vol. 5 No. 1 n February-March 2010 39
Subject recruitment: A total of 80 COPD patients (defined as FEV1/FVC ratio <0.7 with a general practitioner or chest physician diagnosis) and 37 healthy elderly subjects were recruited to the study. Patients with stable COPD (no exacerbation or change of medication in last 6 weeks) were recruited from the chest clinic of St. George’s Hospital. Figure 1 shows the patient recruitment flow chart. Healthy subjects were recruited from the staff and volunteers of St. George’s University, St. George’s Hospital and from an Open University group. Absence of airway obstruction was confirmed by spirometry. Additionally, patients and subjects were excluded if they had a history of significant inflammatory co-morbidities such as carcinoma, rheumatoid arthritis or stroke, unstable angina, a diagnosis of psychiatric disorders, or mobility limiting conditions.
Assessments: Fifty nine patients included in the study attended the hospital for a baseline morning assessment of approximately 2.5 - 3.5 hours (transport available). Assessment was carried out over two days if necessary, for instance, when the patient was too tired to continue. A further 15 housebound severe COPD patients were unable to attend the hospital for assessment; for these patients an adapted home assessment was provided.
Variables measured: Subjective fatigue: Fatigue was assessed in the morning prior to other assessments in patients and healthy subjects using MFI 20, a 20-item self-report validated instrument.12,18 This tool has been previously used in COPD population and it is recommended as an outcome measure in clinical settings.19 The questionnaire asks subjects to describe how they have been feeling lately. For issues of clarity this was specified as “within the last two weeks”. The tool consists of five dimensions covering General Fatigue (GF), Physical Fatigue
(PF), Reduced Activity (RA), Reduced Motivation (RM) and Mental Fatigue (MF). Each dimension has 4 items, each item scored from 1-5 with higher scores representing greater levels of fatigue.
Depression and breathlessness scores: All participants completed the Hospital Anxiety and Depression Scale (HADS). The HADS is a questionnaire designed to measure depressive moods and anxiety separately.20 A score of 11 or higher indicates probable presence of the mood disorder, but it is not a synonymous of the diagnosis.
Baseline breathlessness level was assessed using the Medical Research Council Dyspnea Grade (MRC).21
Health Related QoL was measured using Saint George’s Respiratory Questionnaire (SGRQ).22
Physiological measures: For all participants height (cm) and weight (kg) were measured. Body Mass (BMI) and Fat Free Mass (FFMI) indices were determined from body composition measurements using a non-invasive bioelectrical impedance technique (Body composition analyser, Tanita Ltd BC-418MA, UK). Baseline FEV1 and FVC were assessed using a spirometer Micro Plus MS03 (Micro Medical Ltd, Rochester UK) and according to BTS recommendations.23 GOLD classification was used to determine patients’ airway obstruction severity.24
Muscle strength: For all participants quadriceps maximal torque was measured using a “Cybex Norm Testing and Rehabilitation System.” The protocol consisted of 1 minute of consecutive concentric knee extensions and flexions, performed maximally at an angular velocity of 60°/sec, following a 10-repetition trial. The break between the trial and actual test was 20 seconds. Maximum torque was recorded as the best attempt during 1 minute isokinetic work of the dominant side (FtLbs) and as FtLbs/subject bodyweight (lb) *100.
Exercise tolerance: For patients only, maximal exercise tolerance was assessed using the Incremental Shuttle Walking Test (ISWT), an incremental, externally paced exercise capacity test conducted according to standardised procedure.25 Endurance exercise tolerance was then assessed using the Endurance Shuttle Walking Test (ESWT).26 Prior to and after each test percutaneous arterial oxygen saturation (SpO2) and heart rate were measured using a pulse oxymeter (Pulsox-3i-Konika Minolta, Singapore) applied to the finger. Borg CR 10 (Dyspnea assessment) and Borg Rating of Perceived Exertion (RPE) scales were scored after each test.27,28
Blood sampling: For patients only, a fasting, resting venous blood sample was obtained from the median cubital vein and Interleukin-6 (IL-6) was measured from serum. Blood samples were centrifuged within 2 hours of collection and serum was stored at -20°C until assay. The analysis was performed on an Immulite 1000 automated analyser (Siemens Medical Solutions Diagnostics, formally Euro/DPC Ltd Gwynedd Wales, UK). The limit of detection for serum IL-6 was 0.2 pg/mL-1. Patients’ hemoglobin (Hb) levels were determined from their ear lobe capillary blood sample, using blood gas/electrolyte analyser (model 5700; Instrumentation Laboratory, Lexington MA). Anaemia was defined according to WHO criteria.29
Home assessment: The 15 home assessments were as described
Flow chart of recruitment and assessmentFigure 1Flow chart of recruitment and assessment.
Agreed:
98 patients
(81 hospital assessment and
17 home assessment) &
37 healthy subjects
18 did not attend the first assessment
6 patients and 2 healthy subjects excluded after
an initial interview
Assessed: 74 patients
(59 hospital assessment
and 15 home assessment) &
35 healthy subjects
99 patients refused
18 patients not contacted (17 change in address
or telephone number, 1 RIP)
15 patients excluded
Invited: 230 patients &
37 healthy subjects
Figure 1. Flow chart of recruitment and assessment.

40 Respiratory Therapy Vol. 5 No. 1 n February-March 2010
above with the exception of measures of exercise tolerance, muscle strength and blood sampling.
Statistical analysis: Summary statistics of the healthy subjects’ and COPD patients’ characteristics were reported. Independent sample t-tests or Mann-Whitney tests as appropriate were used to test for differences between the patients and the healthy subjects. The Kruskal-Wallis test was used to determine differences between fatigue dimensions according to the MRC score and GOLD classification with the significance level set at α=0.05. When significant differences were found, post hoc analysis was carried out using Mann-Whitney tests with Bonferroni correction. The data used to measure fatigue are not metric and therefore multiple linear regression techniques are inappropriate. Due to the small number of subjects, logistic rather than ordinal regression was chosen to identify predictors of the 5 dimensions of fatigue; a backward elimination method was used. Therefore for each dimension of fatigue, a binominal category was defined using a cut-off point of the highest value of fatigue in the healthy subjects. Values above this point were considered as fatigued and values below as not fatigued. Explanatory variables that were independent of one another, according to appropriate correlation tests were included in the initial regression models. Other, clinically relevant variables, as identified from literature9,10,13,14,17,30,31 were also included. The final models, presented here, are those where all the remaining
independent variables are statistically significant predictors of the fatigue dimension under consideration and which have the highest R2 value. The data from 15 home assessments were excluded due to the modified assessment. All analyses were performed using SPSS 15.
ResultsComparative data: Fatigue in COPD subjects versus healthy older subjects: Seventy four mild-to-severe COPD patients and 35 healthy subjects completed all assessments. There were no significant differences in fatigue according to gender in either the COPD (52 male vs. 22 female) or the healthy group (12 male vs 23 female). Median scores for COPD patients were significantly higher than those of the healthy subjects in all dimensions of MFI 20. Table 1 shows the scores for fatigue and other variables and differences between COPD patients and the healthy subjects.
Fatigue and disease severity: Statistically significant differences in fatigue when categorised according to the GOLD and MRC dyspnea classifications were evident for selected dimensions of MFI 20 only (see figure 2 and figure 3).
Meaningful variables for fatigue dimensions: Regression analysis was performed on full data available from 59 patients (40 male) aged 68.7 (8.1), mean (SD) % predicted FEV1 48.2 (20.9) and FEV1/FVC ratio 0.45 (0.13). Clinically relevant variables were
Variables excluded from the analysisThe mean (SD) haemoglobin level was 15.6 (2.9) g/dL inmale and 14.6 (1.6) g/dL in female patients. Only 2patients had values below normal. Anaemia was thereforenot a feature of the patient population and thus was notincluded in the regression analysis. There were high corre-lations between anxiety and depression, BMI and FFMI,ISWT and ESWT. Hence anxiety, FFMI and ESWT were notentered into the regression as independent variables as theothers were considered more important clinically.
MRC score as a measure of dyspnoea was initially consid-ered as a predictor of fatigue. Although expected from lit-erature and from the results presented in figure 3, it wasnot a significant predictor for any of fatigue dimensionand it was eventually excluded in the final regression proc-ess. Measures of quality of life (SGRQ) were collected toenable baseline characterisation of the patients. Althoughquality of life has been shown to be associated withfatigue in previous studies [8,9], direction of causality isunknown. It was felt that fatigue was more likely to be a
Table 1: Characteristics and comparison of COPD and healthy subject groups
COPD (n = 74) Healthy (n = 35) p value
MFI 20 General Fatigue 13 (5) 8 (4) p < 0.001
MFI 20 Physical Fatigue 16 (5.25) 7 (5) p < 0.001
MFI 20 Reduced Activity 13.5 (6) 6 (5) p < 0.001
MFI 20 Reduced Motivation 10 (6) 6 (4) p < 0.001
MFI 20 Mental Fatigue 8 (7) 6 (4) p = 0.008
% FEV1 46.5(20.0) 96.5(13.2) p < 0.001
FEV1/FVC ratio 0.44 (0.13) 0.78(0.1) p < 0.001
Age (yrs) 69.9 (8.4) 67.11 (8.8) NS
BMI (kg/m2) 26.2 (5.4) 25.2 (3.4) NS
FFMI (kg/m2) 18.2 (2.6) 17.9 (2.2) NS
Depression (HADS) 6 (5) 1 (3) p < 0.001
Anxiety (HADS) 7 (6) 3 (4) p < 0.001
Peak Tq (% BW) 38.6 (12.0)* 51.6 (14.5) p < 0.001
ISWT (m) 343.3 (183.9) * - -
Post walk SpO2 (%) 90.0(5.9)* - -
Borg exertion (RPE) 13(2.0)* - -
IL 6 (pg/mL) (n = 57) 5.4(5.9) * - -
MRC dyspnoea score 3 (2) - -
SGRQ 56.0 (27.4) - -
Data presented as median (IQR) for MFI 20-Multidimensional Fatigue Inventory, HADS - Hospital Anxiety and Depression scale, SGRQ - Saint George's Respiratory Questionnaire, total score, Borg exertion, MRC score or mean (SD) for % FEV1 - % predicted forced expiratory volume in one second, FEV1/FVC - Forced Expiratory Volume in one second/Forced Vital Capacity, BMI - Body Mass Index; FFMI - Fat Free Mass Index; Peak Tq (% BW) - quadriceps peak torque (% Body Weight), ISWT - Incremental Shuttle walk test, SpO2 - Percutaneous arterial oxygen saturation. *not measured in home-assessed patients (n = 59).

Respiratory Therapy Vol. 5 No. 1 n February-March 2010 41
identified based on literature and results of correlations with fatigue dimensions. Following the initial regression analyses nine possible predictors were identified: % predicted FEV1, depression, muscle torque, ISWT, end exercise SpO2, IL6, Borg RPE, BMI, age. The final decision on which variables to include was determined by clinical relevance and by the best possible model of predictive variables.
Variables excluded from the analysis: The mean (SD) hemoglobin level was 15.6 (2.9) g/dL in male and 14.6 (1.6) g/dL in female patients. Only 2 patients had values below normal. Anaemia was therefore not a feature of the patient population and thus was not included in the regression analysis. There were high correlations between anxiety and depression, BMI and FFMI, ISWT and ESWT. Hence anxiety, FFMI and ESWT were not entered into the regression as independent variables as the others were considered more important clinically.
MRC score as a measure of dyspnea was initially considered as a predictor of fatigue. Although expected from literature and from the results presented in figure 3, it was not a significant predictor for any of fatigue dimension and it was eventually excluded in the final regression process. Measures of quality of life (SGRQ) were collected to enable baseline characterisation of the patients. Although quality of life has been shown to be associated with fatigue in previous studies,8,9 direction of causality is unknown. It was felt that fatigue was more likely to be a mediator of impaired quality of life than the other direction, thus SGRQ data were not included in the regression as independent predictors.
Predictors of fatigue in COPD: For GF the following 5 variables were entered: depression, muscle torque, % predicted FEV1, end SpO2, IL 6; for PF: depression, ISWT, % predicted FEV1 and age; for RA: depression, ISWT, % predicted FEV1 and BMI; for RM: depression, end Borg RPE and end SpO2 and for MF: depression, IL6 and end SpO2. Tables 2, 3, 4, 5, and 6 give the results of the logistic regression analyses. Table 2 shows, for instance, that the significant predictors of GF (as measured by Wald statistic) are depression, muscle torque and end exercise SpO2. For every increase of 1 in the depression score a patient is approximately 1.5 times more likely to be fatigued and for lower end exercise SpO2 there is a slightly higher chance of being fatigued; similarly lower muscle strength is associated with higher risk of fatigue.
SummaryFatigue score was significantly higher in COPD compare to control group for all dimensions of MFI 20. After stratification for MRC and GOLD classifications there were significant differences only for selected dimensions of fatigue. Fatigue, when considered as a multi-component construct was explained by a different combination of variables.
DiscussionThe results from this study show that subjective fatigue measured with MFI 20 was significantly higher in the COPD group than in healthy elderly people. Previous work supports these findings,8,32
which suggests that the increased fatigue reflects disease entity and may therefore be considered as COPD-RF and it should be properly addressed in clinical practice. In contrast to other authors8 differences were found in fatigue according to GOLD staging, however these differences were specific for selected dimensions of fatigue only. The difference in findings likely reflects the different fatigue tools used, with this study using a multi-dimensional tool compared with the FACIT-fatigue, a uni-dimensional tool.
In line with this, it is demonstrated here that differing fatigue dimensions can be explained by different physiological and psychological variables associated with COPD and only depression was a common predictor. Although according to MRC dyspnea classification there were significant differences for Reduced Activities, General and Physical Fatigue, the regression analysis excluded dyspnea score as a possible predictive variable of fatigue. Importantly, the cohort used in regression
mediator of impaired quality of life than the other direc-tion, thus SGRQ data were not included in the regressionas independent predictors.
Predictors of fatigue in COPDFor GF the following 5 variables were entered: depression,muscle torque, % predicted FEV1, end SpO2, IL 6; for PF:depression, ISWT, % predicted FEV1 and age; for RA:depression, ISWT, % predicted FEV1 and BMI; for RM:depression, end Borg RPE and end SpO2 and for MF:depression, IL6 and end SpO2. Table 2, 3, 4, 5 and 6 givethe results of the logistic regression analyses. Table 2shows, for instance, that the significant predictors of GF(as measured by Wald statistic) are depression, muscletorque and end exercise SpO2. For every increase of 1 inthe depression score a patient is approximately 1.5 timesmore likely to be fatigued and for lower end exercise SpO2there is a slightly higher chance of being fatigued; simi-
larly lower muscle strength is associated with higher riskof fatigue.
SummaryFatigue score was significantly higher in COPD compareto control group for all dimensions of MFI 20. After strat-ification for MRC and GOLD classifications there were sig-nificant differences only for selected dimensions offatigue. Fatigue, when considered as a multi-componentconstruct was explained by a different combination of var-iables.
DiscussionThe results from this study show that subjective fatiguemeasured with MFI 20 was significantly higher in theCOPD group than in healthy elderly people. Previouswork supports these findings [8,32], which suggests thatthe increased fatigue reflects disease entity and may there-
Box plots showing MFI 20 dimensions (median and IQR) in COPD patients for GOLD stagesFigure 2Box plots showing MFI 20 dimensions (median and IQR) in COPD patients for GOLD stages. GOLD stage I & II (n = 27), III (n = 32) and IV (n = 15). Kruskal Wallis tests: p = 0.008 for Physical Fatigue and p = 0.045 for Reduced Activity; p > 0.05 for General Fatigue, Reduced Motivation and Mental Fatigue; †Mann-Whitney test (Bonferroni correction p = 0.02).
GOLD
Mental FatigueReduced MotivationReduced ActivityPhysical FatigueGeneral Fatigue
I VI III&III VI III&III VIIII&IIIVIIII&IIIVIIII&II
20.0
17.5
15.0
12.5
10.0
7.5
5.0
p=0.013
=0.007
p=0.02
p
fore be considered as COPD-RF and it should be properlyaddressed in clinical practice. In contrast to other authors[8] differences were found in fatigue according to GOLDstaging, however these differences were specific for
selected dimensions of fatigue only. The difference infindings likely reflects the different fatigue tools used,with this study using a multi-dimensional tool comparedwith the FACIT-fatigue, a uni-dimensional tool.
Box plots showing MFI 20 dimensions (median and IQR) in COPD patients for MRC scoresFigure 3Box plots showing MFI 20 dimensions (median and IQR) in COPD patients for MRC scores. MRC score 1&2 (n = 31), 3 (n = 12), 4 (n = 17), 5 (n = 14). Kruskal Wallis tests: p = 0.001 for General Fatigue, p = 0.004 for Physical Fatigue, p = 0.001 for Reduced Activity, p > .05 for Reduced Motivation and Mental Fatigue; †Mann-Whitney test (Bonferroni correction p = 0.008).
MRC
Mental FatigueReduced Motivat ionReduced ActivityPhysical FatigueGeneral Fatigue
5431&25431&25431&25431&25431&2
20.0
17.5
15.0
12.5
10.0
7.5
5.0
p=0.001 p p=0.001
p=0.004
=0.005
p=0.008
Table 2: Logistic regression results for General Fatigue
MFI 20 Variables included Wald 2 B (SE) Odd ratioExp b
95% CI lower-upper
General Fatigue(n = 48)
HADS depression 8.1 0.43 (0.15) 1.54 1.14-2.07
Tq %BW 5.0 -0.13 (0.06) 0.88 0.79-0.98
End SpO2 2.9 -0.014 (0.08) 0.87 0.74-1.02
Constant 3.4 13.9 (7.6) 1109057
R2 = .62 (Nagelkerke); HADS depression-depression score of hospital anxiety and depression scale, Tq%BM - quadriceps muscle torque % of body mass, End SpO2 - percutaneous arterial saturation post walking test

42 Respiratory Therapy Vol. 5 No. 1 n February-March 2010
study differ from one used in MRC classification analysis and data from home-assessed most severe patients may have been more insightful. Previous studies also showed associations between dyspnea and fatigue.8,30,31 Nonetheless, fatigue and dyspnea are both subjective symptoms of COPD and some of the patho-mechanisms of fatigue may be common for those of dyspnea. Therefore, this may explain the close association between these symptoms. Since fatigue is not routinely assessed in current clinical practice, the models from this study may help to identify patients who are at risk of being fatigued and develop effective fatigue management strategies. Furthermore, the regression analyses revealed that each component could be explained by different variations. Hence, the multi-rather than uni-dimensional assessment should be considered. Over half of the variation in general fatigue was explained by a combination of depression, exercise de-saturation and muscle strength. These data then provide further support for the role of muscle training, depression management and use of supplementary oxygen in COPD. In this present study exercise de-saturation was also a significant predictor for the MFI 20 Reduced Motivation component. For Reduced Motivation; depression, post exercise saturation and exertion explained a little less than 40% of the variation. This component includes items such as ‘I dread having to do things’ and ‘I don’t feel like doing anything’. Low oxygen levels may be associated with changes in cognitive function33,34 and stimulate affective areas of the brain, mainly in the frontal lobe, which is associated with motivational process.35,36 Feasibly, the administration of oxygen during exertion may be associated with lower fatigue levels and enhanced motivation. To date this application of oxygen has not been explored.
For physical fatigue the best model, a combination of depression, lung function and exercise tolerance, explained 57% of the variation. This provides some explanation as to how therapies
that improve exercise tolerance and depression can have an impact on fatigue in COPD.37 Muscle strength and exercise tolerance were significant predictors for general and physical fatigue, respectively. These two variables were highly correlated and therefore only one was used in the regression analysis. Muscle weakness and reduced exercise tolerance are well recognised in the COPD population38,39 and may be important factors influencing COPD RF.
Around 40% of the variation in Reduced Activity was explained by the combination of lung function, BMI and depression. In this instance a higher BMI was associated with greater fatigue. This probably reflects the U-shaped curve nature of the association between BMI and outcomes, both low and high BMI is generally associated with poorer outcome.40 Nutritional status remains an important therapeutic outcome in the management of COPD. Furthermore, in physically related dimensions of fatigue the severity of airway obstruction explained a significant amount of the variance, suggesting that treatments which affect airflow obstruction may also benefit the perception of physical fatigue. For mental fatigue few COPD patients were identified as fatigued and the results for this component should be treated with caution.
Anaemia may be one of the causes of fatigue and can be present in COPD patients;41 however, hemoglobin levels were generally within the normal range in the cohort, thus this factor could not be included in this analysis. Nevertheless, it is clear from this study, that COPD RF remains a significant problem even in patients with moderate disease and no anaemia. Although some variables were not included in the final regression model, they may still play a role in the development of COPD RF. For example, there was a strong correlation between anxiety and depression, but it was decided only to include depression.
In line with this, it is demonstrated here that differingfatigue dimensions can be explained by different physio-logical and psychological variables associated with COPDand only depression was a common predictor. Althoughaccording to MRC dyspnoea classification there were sig-nificant differences for Reduced Activities, General andPhysical Fatigue, the regression analysis excluded dysp-noea score as a possible predictive variable of fatigue.Importantly, the cohort used in regression study differfrom one used in MRC classification analysis and datafrom home-assessed most severe patients may have beenmore insightful. Previous studies also showed associa-tions between dyspnoea and fatigue [8,30,31]. Nonethe-less, fatigue and dyspnoea are both subjective symptomsof COPD and some of the patho-mechanisms of fatiguemay be common for those of dyspnoea. Therefore, thismay explain the close association between these symp-toms. Since fatigue is not routinely assessed in currentclinical practice, the models from this study may help toidentify patients who are at risk of being fatigued anddevelop effective fatigue management strategies. Further-more, the regression analyses revealed that each compo-nent could be explained by different variations. Hence,
the multi-rather than uni-dimensional assessment shouldbe considered. Over half of the variation in general fatiguewas explained by a combination of depression, exercisede-saturation and muscle strength. These data then pro-vide further support for the role of muscle training,depression management and use of supplementary oxy-gen in COPD. In this present study exercise de-saturationwas also a significant predictor for the MFI 20 ReducedMotivation component. For Reduced Motivation; depres-sion, post exercise saturation and exertion explained a lit-tle less than 40% of the variation. This componentincludes items such as 'I dread having to do things' and 'Idon't feel like doing anything'. Low oxygen levels may beassociated with changes in cognitive function [33,34] andstimulate affective areas of the brain, mainly in the frontallobe, which is associated with motivational process[35,36]. Feasibly, the administration of oxygen duringexertion may be associated with lower fatigue levels andenhanced motivation. To date this application of oxygenhas not been explored.
For physical fatigue the best model, a combination ofdepression, lung function and exercise tolerance,
Table 3: Logistic regression results for Physical Fatigue
MFI 20 Variables included Wald 2 B (SE) Odd ratioExp b
95% CI lower-upper
Physical Fatigue(n = 57)
HADS depression 11.3 0.47 (0.14) 1.61 1.22-2.12
%pred. FEV1 9.9 -0.11 (0.04) 0.90 0.83-0.96
ISWT 5.2 0.01 (0.003) 1.01 1.0-1.01
Age 2.8 0.9 (0.06) 1.1 0.98-1.22
Constant 2.6 -7.16 (4.48) 0.001
R2 = .57 (Nagelkerke). HADS depression-depression score of hospital anxiety and depression scale, %pred. FEV1 - % predicted forced expiratory volume in one second, ISWT-Incremental Shuttle Walk Test
Table 4: Logistic regression results for Reduced Activity
MFI 20 Variables included Wald 2 B (SE) Odd ratioExp b
95% CI lower-upper
Reduced Activity(n = 57)
%pred. FEV1 7.5 -0.06 (0.02) 0.95 0.91-0.98
BMI 4.5 0.19(0.08) 1.21 1.03-1.41
HADS depression 3.9 0.19 (0.94) 1.20 1.0-1.45
Constant 2.0 -3.12 (1.95) 0.04
R2 = .36 (Nagelkerke). %pred. FEV1 - % predicted forced expiratory volume in one second, BMI - Body Mass Index, HADS depression-depression score of hospital anxiety and depression scale
In line with this, it is demonstrated here that differingfatigue dimensions can be explained by different physio-logical and psychological variables associated with COPDand only depression was a common predictor. Althoughaccording to MRC dyspnoea classification there were sig-nificant differences for Reduced Activities, General andPhysical Fatigue, the regression analysis excluded dysp-noea score as a possible predictive variable of fatigue.Importantly, the cohort used in regression study differfrom one used in MRC classification analysis and datafrom home-assessed most severe patients may have beenmore insightful. Previous studies also showed associa-tions between dyspnoea and fatigue [8,30,31]. Nonethe-less, fatigue and dyspnoea are both subjective symptomsof COPD and some of the patho-mechanisms of fatiguemay be common for those of dyspnoea. Therefore, thismay explain the close association between these symp-toms. Since fatigue is not routinely assessed in currentclinical practice, the models from this study may help toidentify patients who are at risk of being fatigued anddevelop effective fatigue management strategies. Further-more, the regression analyses revealed that each compo-nent could be explained by different variations. Hence,
the multi-rather than uni-dimensional assessment shouldbe considered. Over half of the variation in general fatiguewas explained by a combination of depression, exercisede-saturation and muscle strength. These data then pro-vide further support for the role of muscle training,depression management and use of supplementary oxy-gen in COPD. In this present study exercise de-saturationwas also a significant predictor for the MFI 20 ReducedMotivation component. For Reduced Motivation; depres-sion, post exercise saturation and exertion explained a lit-tle less than 40% of the variation. This componentincludes items such as 'I dread having to do things' and 'Idon't feel like doing anything'. Low oxygen levels may beassociated with changes in cognitive function [33,34] andstimulate affective areas of the brain, mainly in the frontallobe, which is associated with motivational process[35,36]. Feasibly, the administration of oxygen duringexertion may be associated with lower fatigue levels andenhanced motivation. To date this application of oxygenhas not been explored.
For physical fatigue the best model, a combination ofdepression, lung function and exercise tolerance,
Table 3: Logistic regression results for Physical Fatigue
MFI 20 Variables included Wald 2 B (SE) Odd ratioExp b
95% CI lower-upper
Physical Fatigue(n = 57)
HADS depression 11.3 0.47 (0.14) 1.61 1.22-2.12
%pred. FEV1 9.9 -0.11 (0.04) 0.90 0.83-0.96
ISWT 5.2 0.01 (0.003) 1.01 1.0-1.01
Age 2.8 0.9 (0.06) 1.1 0.98-1.22
Constant 2.6 -7.16 (4.48) 0.001
R2 = .57 (Nagelkerke). HADS depression-depression score of hospital anxiety and depression scale, %pred. FEV1 - % predicted forced expiratory volume in one second, ISWT-Incremental Shuttle Walk Test
Table 4: Logistic regression results for Reduced Activity
MFI 20 Variables included Wald 2 B (SE) Odd ratioExp b
95% CI lower-upper
Reduced Activity(n = 57)
%pred. FEV1 7.5 -0.06 (0.02) 0.95 0.91-0.98
BMI 4.5 0.19(0.08) 1.21 1.03-1.41
HADS depression 3.9 0.19 (0.94) 1.20 1.0-1.45
Constant 2.0 -3.12 (1.95) 0.04
R2 = .36 (Nagelkerke). %pred. FEV1 - % predicted forced expiratory volume in one second, BMI - Body Mass Index, HADS depression-depression score of hospital anxiety and depression scale

Respiratory Therapy Vol. 5 No. 1 n February-March 2010 43
Similarly, ESWT was strongly related to ISWT but only the maximal test was included. Although IL6 was considered a possible predictor, none of the final regression models included it, which may be due to its correlation with both muscle strength and walking distance42 or reflects the need for other measures such as receptors.
Previous studies using a multiple regression identified depression as a predictive variable of uni-dimansional fatigue in COPD.8,30 However, findings here reveal that depression is a predictor for all dimensions of fatigue.
ConclusionThis study shows that all dimensions of fatigue are greater in COPD than in healthy people of a similar age range. Increased fatigue in this population is therefore a feature of COPD and not of age per se. COPD-RF is a multi component construct and as such different aspects of fatigue are influenced by different clinical manifestations. Comprehensive treatment of COPD-RF includes management of depression, muscle weakness, optimisation of BMI and exercise de-saturation levels. In contrast to other authors it was found that fatigue differs according to GOLD staging, however this is relevant only for Physical Fatigue and Reduced Activity. This study goes some way towards explaining the mechanistic pathway of COPD-RF and provides information to target hitherto neglected treatments.
References1 Armes J, Krishnasamy M, Higginson IJ: Fatigue in cancer.
New York, Oxford University Press; 2004.2 Del Fabbro E, Dalal S, Bruera E: Symptom control in
palliative care - Part II: Cachexia/anorexia and fatigue. Journal of Palliative Medicine 2006, 9:409-421.
3 Brissot R, Gonzalez-Bermejo J, Lassalle A, Desrues B, Doutrellot PL: Fatigue and respiratory disorders. Annales de Readaptation et de Medecine Physique 2006, 49 (6):403-412.
4 Small S, Lamb M: Fatigue in chronic illness: the experience of individuals with chronic obstructive pulmonary disease and
with asthma. Journal of Advanced Nursing 1999, 30:469-478.5 Yeh ML, Chen HH, Liao YC, Liao WY: Testing the functional
status model in patients with chronic obstructive pulmonary disease. Journal of Advanced Nursing 2004, 48:342-350.
6 Kinsman RA, Yaroush RA, Fernandez E, Dirks JF, Schocket M, Fukuhara J: Symptoms and experiences in chronic bronchitis and emphysema. Chest 1983, 83:755-761.
7 Walke LM, Byers AL, Tinetti ME, Dubin JA, McCorkle R, Fried TR: Range and severity of symptoms over time among older adults with chronic obstructive pulmonary disease and heart failure. Archives of Internal Medicine 2007, 167:2503-2508.
8 Baghai-Ravary R, Quint JK, Goldring JJP, Hurst JR, Donaldson GC, Wedzicha JA: Determinants and impact of fatigue in patients with chronic obstructive pulmonary disease. Respiratory Medicine 2008, 103:216-223.
9 Breslin E, Schans C Van der, Breukink SO, Meek P, Mercer K, Volz W, Louie S: Perception of fatigue and quality of life in patients with COPD. Chest 1998, 114:958-964.
10 Breukink SO, Strijbos JH, Koorn M, Koeter GH, Breslin EH, Schans CP Van der: Relationship between subjective fatigue and physiological variables in patients with chronic obstructive pulmonary disease. Respiratory Medicine 1998, 92:676-682.
11 Gift AG, Shepard CE: Fatigue and other symptoms in patients with chronic obstructive pulmonary disease: do women and men differ? Journal of Obstetric, Gynecologic, & Neonatal Nursing 1999, 28:201-208.
12 Smets EM, Garssen B, Bonke B, De Haes JC: The Multidimensional Fatigue Inventory (MFI) psychometric qualities of an instrument to assess fatigue. Journal of Psychosomatic Research 1995, 39:315-325.
13 Oh EG, Kim CJ, Lee WH, Kim SS: Correlates of fatigue in Koreans with chronic lung disease. Heart & Lung 2004, 33:13-20.
14 Evans WJ, Lambert CP: Physiological basis of fatigue. American Journal of Physical Medicine & Rehabilitation 2007, 86:S29-S46.
15 Robson-Ansley PJ, De Milander L, Collins M, Noakes
explained 57% of the variation. This provides some expla-nation as to how therapies that improve exercise toleranceand depression can have an impact on fatigue in COPD[37]. Muscle strength and exercise tolerance were signifi-cant predictors for general and physical fatigue, respec-tively. These two variables were highly correlated andtherefore only one was used in the regression analysis.Muscle weakness and reduced exercise tolerance are wellrecognised in the COPD population [38,39] and may beimportant factors influencing COPD RF.
Around 40% of the variation in Reduced Activity wasexplained by the combination of lung function, BMI anddepression. In this instance a higher BMI was associatedwith greater fatigue. This probably reflects the U-shapedcurve nature of the association between BMI and out-comes, both low and high BMI is generally associatedwith poorer outcome [40]. Nutritional status remains animportant therapeutic outcome in the management ofCOPD. Furthermore, in physically related dimensions offatigue the severity of airway obstruction explained a sig-nificant amount of the variance, suggesting that treat-ments which affect airflow obstruction may also benefitthe perception of physical fatigue. For mental fatigue fewCOPD patients were identified as fatigued and the resultsfor this component should be treated with caution.
Anaemia may be one of the causes of fatigue and can bepresent in COPD patients [41]; however, haemoglobinlevels were generally within the normal range in thecohort, thus this factor could not be included in this anal-ysis. Nevertheless, it is clear from this study, that COPDRF remains a significant problem even in patients withmoderate disease and no anaemia. Although some varia-bles were not included in the final regression model, theymay still play a role in the development of COPD RF. Forexample, there was a strong correlation between anxietyand depression, but it was decided only to include depres-sion. Similarly, ESWT was strongly related to ISWT butonly the maximal test was included. Although IL6 wasconsidered a possible predictor, none of the final regres-sion models included it, which may be due to its correla-tion with both muscle strength and walking distance [42]or reflects the need for other measures such as receptors.
Previous studies using a multiple regression identifieddepression as a predictive variable of uni-dimansionalfatigue in COPD [8,30]. However, findings here revealthat depression is a predictor for all dimensions of fatigue.
ConclusionThis study shows that all dimensions of fatigue are greaterin COPD than in healthy people of a similar age range.Increased fatigue in this population is therefore a feature
Table 5: Logistic regression results for Reduced Motivation
MFI 20 Variables included Wald 2 B (SE) Odd ratioExp b
95% CI lower-upper
Reduced Motivation(n = 56)
Borg exertion 5.8 0.54 (0.22) 1.71 1.11-2.66
HADS depression 5.7 0.24 (0.10) 1.28 1.04-1.56
End SpO2 4.9 -0.13(0.06) 0.88 0.78-0.99
Constant 0.3 2.69 (5.28) 14.67
R2 = .37 (Nagelkerke). Borg exertion (score) post walk test, HADS depression-depression score of hospital anxiety and depression scale, End SpO2 - percutaneous arterial saturation post walking test.
Table 6: Logistic regression results for Mental Fatigue
MFI 20 Variables included Wald 2 B (SE) Odd ratioExp b
95% CI lower-upper
Mental Fatigue(n = 52)
HADS depression 7.3 0.4 (0.15) 1.49 1.12-2.0
End SpO2 3.1 0.2 (0.12) 1.23 0.98-1.54
Constant 4.3 -23.06(11.16) 0.0
R2 = .38 (Nagelkerke). HADS depression-depression score of hospital anxiety and depression scale, End SpO2 - percutaneous arterial saturation post walking test.
explained 57% of the variation. This provides some expla-nation as to how therapies that improve exercise toleranceand depression can have an impact on fatigue in COPD[37]. Muscle strength and exercise tolerance were signifi-cant predictors for general and physical fatigue, respec-tively. These two variables were highly correlated andtherefore only one was used in the regression analysis.Muscle weakness and reduced exercise tolerance are wellrecognised in the COPD population [38,39] and may beimportant factors influencing COPD RF.
Around 40% of the variation in Reduced Activity wasexplained by the combination of lung function, BMI anddepression. In this instance a higher BMI was associatedwith greater fatigue. This probably reflects the U-shapedcurve nature of the association between BMI and out-comes, both low and high BMI is generally associatedwith poorer outcome [40]. Nutritional status remains animportant therapeutic outcome in the management ofCOPD. Furthermore, in physically related dimensions offatigue the severity of airway obstruction explained a sig-nificant amount of the variance, suggesting that treat-ments which affect airflow obstruction may also benefitthe perception of physical fatigue. For mental fatigue fewCOPD patients were identified as fatigued and the resultsfor this component should be treated with caution.
Anaemia may be one of the causes of fatigue and can bepresent in COPD patients [41]; however, haemoglobinlevels were generally within the normal range in thecohort, thus this factor could not be included in this anal-ysis. Nevertheless, it is clear from this study, that COPDRF remains a significant problem even in patients withmoderate disease and no anaemia. Although some varia-bles were not included in the final regression model, theymay still play a role in the development of COPD RF. Forexample, there was a strong correlation between anxietyand depression, but it was decided only to include depres-sion. Similarly, ESWT was strongly related to ISWT butonly the maximal test was included. Although IL6 wasconsidered a possible predictor, none of the final regres-sion models included it, which may be due to its correla-tion with both muscle strength and walking distance [42]or reflects the need for other measures such as receptors.
Previous studies using a multiple regression identifieddepression as a predictive variable of uni-dimansionalfatigue in COPD [8,30]. However, findings here revealthat depression is a predictor for all dimensions of fatigue.
ConclusionThis study shows that all dimensions of fatigue are greaterin COPD than in healthy people of a similar age range.Increased fatigue in this population is therefore a feature
Table 5: Logistic regression results for Reduced Motivation
MFI 20 Variables included Wald 2 B (SE) Odd ratioExp b
95% CI lower-upper
Reduced Motivation(n = 56)
Borg exertion 5.8 0.54 (0.22) 1.71 1.11-2.66
HADS depression 5.7 0.24 (0.10) 1.28 1.04-1.56
End SpO2 4.9 -0.13(0.06) 0.88 0.78-0.99
Constant 0.3 2.69 (5.28) 14.67
R2 = .37 (Nagelkerke). Borg exertion (score) post walk test, HADS depression-depression score of hospital anxiety and depression scale, End SpO2 - percutaneous arterial saturation post walking test.
Table 6: Logistic regression results for Mental Fatigue
MFI 20 Variables included Wald 2 B (SE) Odd ratioExp b
95% CI lower-upper
Mental Fatigue(n = 52)
HADS depression 7.3 0.4 (0.15) 1.49 1.12-2.0
End SpO2 3.1 0.2 (0.12) 1.23 0.98-1.54
Constant 4.3 -23.06(11.16) 0.0
R2 = .38 (Nagelkerke). HADS depression-depression score of hospital anxiety and depression scale, End SpO2 - percutaneous arterial saturation post walking test.

44 Respiratory Therapy Vol. 5 No. 1 n February-March 2010
TD: Acute interleukin-6 administration impairs athletic performance in healthy, trained male runners. Canadian J Appl Physiol 2004, 29:411-418.
16 Spath-Schwalbe E, Hansen K, Schmidt F, Schrezenmeier H, Marshall L, Burger K, Fehm HL, Born J: Acute effects of recombinant human interleukin-6 on endocrine and central nervous sleep functions in healthy men. Journal of Clinical Endocrinology & Metabolism 1998, 83:1573-1579.
17 Gan WQ, Man SF, Senthilselvan A, Sin DD, Gan WQ, Man SFP, Senthilselvan A, Sin DD: Association between chronic obstructive pulmonary disease and systemic inflammation: a systematic review and a meta-analysis. Thorax 2004, 59:574-580.
18 Smets EM, Garssen B, Cull A, De Haes JC: Application of the multidimensional fatigue inventory (MFI-20) in cancer patients receiving radiotherapy. British Journal of Cancer 1996, 73:241-245.
19. Meek PM, Lareau SC: Critical outcomes in pulmonary rehabilitation: assessment and evaluation of dyspnea and fatigue. Journal of Rehabilitation Research & Development 2003, 40:13-24.
20 Zigmond AS, Snaith RP: The hospital anxiety and depression scale. Acta Psychiatrica Scandinavica 1983, 67:361-370.
21 Fletcher CM: Standardised questionnaire on respiratory symptoms: a statement prepared and approved by the MRC committee on the aetiology of chronic bronchitis; MRC breathlessness score. BMJ 1960, 2:1665.
22 Jones PW, Quirk FH, Baveystock CM, Littlejohns P: A self-complete measure of health status for chronic airflow limitation. The St. George’s Respiratory Questionnaire. American Review of Respiratory Disease 1992, 145:1321-1327.
23 British Thoracic Society, BTS: Guidelines for the measurement of respiratory function. Respiratory Medicine 1994, 88:165-194.
24 Global Initiative for Chronic Obstructive Lung Disease (GOLD): Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. 2006 [http://www.who.int/respiratory/copd/GOLD_WR_06.pdf]. MCR VISION, Inc
25 Singh SJ, Morgan MD, Scott S, Walters D, Hardman AE: Development of a shuttle walking test of disability in patients with chronic airways obstruction. Thorax 1992, 47:1019-1024.
26 Revill SM, Morgan MD, Singh SJ, Williams J, Hardman AE: The endurance shuttle walk: a new field test for the assessment of endurance capacity in chronic obstructive pulmonary disease. Thorax 1999, 54:213-222.
27 Borg GA: Psychophysical bases of perceived exertion. Medicine & Science in Sports & Exercise 1982, 14:377-381.
28 Borg GA: Borg’s Perceived exertion and pain scales. In The Borg RPE Scale Champaign, IL, Human Kinetics; 1998:29-38.
29 World Health Organisation, WHO: Iron Deficiency Anemia. Assessment, Prevention, and Control. Geneva, Switzerland 2001. WHO/NHD/01.3
30 Kapella MC, Larson JL, Patel MK, Covey MK, Berry JK: Subjective fatigue, influencing variables, and consequences in chronic obstructive pulmonary disease. Nursing Research 2006, 55:10-17.
31 Woo K: A pilot study to examine the relationships of dyspnea, physical activity and fatigue in patients with chronic obstructive pulmonary disease. Journal of Clinical Nursing 2000, 9:526-533.
32 Theander K, Unosson M: Fatigue in patients with chronic obstructive pulmonary disease. Journal of Advanced Nursing 2004, 45:172-177.
33 Grant I, Prigatano GP, Heaton RK, McSweeny AJ, Wright EC, Adams KM: Progressive neuropsychologic impairment and hypoxemia. Relationship in chronic obstructive pulmonary disease. Archives of General Psychiatry 1987, 44:999-1006.
34 Kozora E, Filley CM, Julian LJ, Cullum CM: Cognitive functioning in patients with chronic obstructive pulmonary disease and mild hypoxemia compared with patients with mild Alzheimer disease and normal controls. Neuropsychiatry, Neuropsychology, & Behavioral Neurology 1999, 12:178-183.
35 Incalzi RA, Marra C, Giordano A, Calcagni ML, Cappa A, Basso S, Pagliari G, Fuso L: Cognitive impairment in chronic obstructive pulmonary disease: A neuropsychological and spect study. Journal of Neurology 2003, 250:325-332.
36 Sari A, Oshiata S, Toriumi T, Yamashita S, Kojima S, Kakumoto S, Yonei A: Cerebral blood flow and cerebral oxygen consumption in patients with COPD on mechanical ventilation. Intensive Care Medicine 1992, 18:455-458.
37 Lacasse Y, Martin S, Lasserson TJ, Goldstein RS: Meta-analysis of respiratory rehabilitation in chronic obstructive pulmonary disease. A Cochrane systematic review. Europa Medicophysica 2007, 43:475-485.
38 Celli BR, MacNee W, The ERS Task Force: Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. European Respiratory Journal 2004, 23:932-946.
39 Gosselink R, Troosters T, Decramer M: Distribution of muscle weakness in patients with stable chronic obstructive pulmonary disease. Journal of Cardiopulmonary Rehabilitation 2000, 20:353-360.
40 Landbo C, Prescott E, Lange P, Vestbo J, Almdal TP: Prognostic value of nutritional status in chronic obstructive pulmonary disease. Journal of Respiratory and Critical Care Medicine 1999, 160:1856-1861.
41 Shorr AF, Doyle J, Stern L, Dolgitser M, Zilberberg MD: Anemia in chronic obstructive pulmonary disease: epidemiology and economic implications. Current Medical Research & Opinion 2008, 24:1123-1130.
42 Garrod R, Marshall J, Barley E, Fredericks S, Hagan G: The relationship between inflammatory markers and disability in chronic obstructive pulmonary disease (COPD). Primary Care Respiratory Journal 2007, 16:236-240.

Respiratory Therapy Vol. 5 No. 1 n February-March 2010 45
Authors Dalby and Harrison are with the Respiratory Medicine Unit, City
Hospital Campus, Nottingham University, Nottingham, UK; Polanowski,
Borgstrom and Edsbacker are with AstraZeneca R&D, Lund, Sweden;
Larsson is a former employee of AstraZeneca. The authors would like
to acknowledge Hans Jagfeldt, Development DMPK (Drug Metabolism
& Pharmacokinetics) & Bioanalysis, Lund, Sweden for his contribution
towards the development of the sputum methods and Dr Jessica Sample
from MediTech Media Ltd who provided medical writing assistance on
behalf of AstraZeneca. This study was funded by AstraZeneca. AstraZeneca
was involved in the study design, interpretation of the data and the
decision to submit the paper for publication in conjunction with the study
investigators. Reprinted from BioMed Central, Respiratory Research, ©
2009 Dalby et al, licensee BioMed Central Ltd. This is an open access article
distributed under the terms of the Creative Commons Attribution License.
This article has been edited for our readers. For the full article, please go to
BioMed Central and type the full title.
The Bioavailability and Airway Clearance of the Steroid Component of BUD/FORM and SAL/FLUChris Dalby, Tomasz Polanowski, Thomas Larsson, Lars Borgström, Staffan Edsbäcker, Tim W. Harrison
Abstract Background: Airway absorption and bioavailability of inhaled corticosteroids (ICSs) may be influenced by differences in pharmacokinetic properties such as lipophilicity and patient characteristics such as lung function. This study aimed to further investigate and clarify the distribution of budesonide and fluticasone in patients with severe chronic obstructive pulmonary disease (COPD) by measuring the systemic availability and sputum concentration of budesonide and fluticasone, administered via combination inhalers with the respective long-acting ß2-agonists, formoterol and salmeterol.
Methods: This was a randomized, double-blind, double-dummy, two-way crossover, multicenter study. Following a run-in period, 28 patients with severe COPD (mean age 65 years, mean forced expiratory volume in 1 second [FEV1] 37.5% predicted normal) and 27 healthy subjects (mean age 31 years, FEV1 103.3% predicted normal) received two single-dose treatments of budesonide/formoterol (400/12 μg) and salmeterol/fluticasone (50/500 μg), separated by a 4-14-day washout period. ICS concentrations were measured over 10 hours post-inhalation in plasma in all subjects, and over 6 hours in spontaneously expectorated sputum in COPD patients. The primary end point was the area under the curve (AUC) of budesonide and fluticasone plasma concentrations in COPD patients relative to healthy subjects.
Results: Mean plasma AUC values were lower in COPD patients versus healthy subjects for budesonide (3.07 μM·hr versus 6.21 μM·hr) and fluticasone (0.84 μM·hr versus 1.50 μM·hr), and the
dose-adjusted AUC (geometric mean) ratios in healthy subjects and patients with severe COPD for plasma budesonide and fluticasone were similar (2.02 versus 1.80; primary end point). In COPD patients, the Tmax and the mean residence time in the systemic circulation were shorter for budesonide versus fluticasone (15.5 min versus 50.8 min and 4.41 hrs versus 12.78 hrs, respectively) and Cmax was higher (1.08 μM versus 0.09 μM). The amount of expectorated fluticasone (percentage of estimated lung-deposited dose) in sputum over 6 hours was significantly higher versus budesonide (ratio 5.21; p=0.006). Both treatments were well tolerated.
Conclusions: The relative systemic availabilities of budesonide and fluticasone between patients with severe COPD and healthy subjects were similar. In patients with COPD, a larger fraction of fluticasone was expectorated in the sputum as compared with budesonide.
Background Chronic obstructive pulmonary disease (COPD) is a preventable and treatable disease associated with considerable and increasing morbidity and mortality worldwide.1,2 It is characterized by progressive airflow limitation that is not fully reversible.1 Inhaled corticosteroids (ICSs) in combination with a long-acting ß2-agonist (LABA) are recommended for the treatment of patients with severe COPD and a history of repeated exacerbations.1,3 Two such combinations, budesonide/formoterol and salmeterol/fluticasone, are licensed for use in COPD and a number of randomized, double-blind clinical studies have demonstrated improvements in lung function and reduced numbers of exacerbations with their use.4-7
Although these combinations both contain an ICS and a LABA, differences exist with regard to the pharmacokinetic and pharmacodynamic properties of both components, such as the oral bioavailability and clearance, volume of distribution and speed of airway uptake, which may impact on the clinical efficacy and safety of the treatments. The degree of lipophilicity, for example, varies widely. Budesonide is several times less lipophilic than fluticasone and, as a result, dissolves more readily in airway mucus and is more rapidly absorbed into the airway tissue and systemic circulation.8-10 Fluticasone, being more lipophilic and thus less water soluble, is more likely to be retained in the lumen of the airways and therefore, has a greater chance of being removed from the airways by mucociliary clearance and cough.11 These differences in lipophilicity may be particularly relevant in patients with

46 Respiratory Therapy Vol. 5 No. 1 n February-March 2010
severe COPD because marked airflow obstruction will lead to greater proximal deposition of inhaled drugs12 and therefore mucociliary clearance. Indeed, previous studies in patients with asthma and airflow obstruction have shown that the systemic exposure of fluticasone is more affected by lung function than budesonide.13,14 This is the first study to investigate and clarify
the absorption of the two ICSs, budesonide and fluticasone delivered via ICS/LABA combination products, in patients with severe COPD and healthy subjects. The novel aspect of the study is the assessment of the proportion of ICS that is expectorated in sputum in patients with severe COPD.
Methods Subjects were either healthy, as determined by medical history, physical examination, vital signs, electrocardiogram and clinical laboratory tests, or diagnosed with severe COPD. The inclusion criteria for patients with severe COPD were: aged ≥40 years, COPD symptoms for ≥1 year, a smoking history of ≥10 pack-years, pre-bronchodilatory forced expiratory volume in 1 second (FEV1) ≤55% of predicted normal, FEV1/vital capacity (VC) ≤70%, a productive cough with expectoration at least twice before noon on most days, and stable symptoms with no signs of an infection or COPD exacerbation within 1 month prior to study start. Exclusion criteria included asthma and/or rhinitis before the age of 40 years and use of ß-blocking agents.
Healthy subjects aged ≥18 years with a pre-bronchodilatory FEV1 ≥80% of predicted normal and an FEV1/VC >70% were eligible for enrollment. Healthy subjects had to have never been regular smokers and were excluded if they were judged to have any significant illness or were using any prescribed medication, or over-the-counter remedies (except for oral contraceptives), herbal preparations, vitamins and mineral supplements ≤2 weeks prior to enrollment.
All subjects gave written informed consent to the study which was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines, and approved by independent ethics committees.
This was a double-blind, double-dummy, randomized, two-way crossover, single-dose, multicenter study. Severe COPD patients were enrolled in Germany (one center), the United Kingdom (one center) and Sweden (one center); healthy subjects were enrolled at one center in Sweden. The first subject was enrolled
Figure 1
Figure 1. Crossover study design BUD/FORM = budesonide/formoterol; SAL/FLU = salmeterol/fluticasone; R = randomization
Figure 2. Patient flow Figure 2
Table 1. Demographics and baseline characteristicsTreatment group
Severe COPD patients
Healthy subjects*
n = 28 n = 27Male, n (%) 21 (75) 11 (41)Age, years 65 (48-80) 31 (20-65)BMI, kg/m2 26.5 (21-32) 23.1 (18-29)FEV1, l 1.10 (0.5-1.9) 3.8 (2.3-5.9)FEV1, % PN 37.5 (24-51) 103.3 (84-131)VC, l 2.8 (1.2-5.2) 4.6 (3.5-6.6)FVC, l 2.7 (1.1-4.9) -FEV1, % FVC 42.4 (27-60) -FEV1, % VC 41.6 (26-63) 83.1 (66-103)Median time since diagnosis, years (range) 8.8 (1-37) -Median pack-years (range) 40 (10-64) -Smoking status -
Previous, n 16 -Habitual, n 22 -
Inhaled ICS at entryn 18 -µg/day 777 (160-1600) -
Data are mean (range) unless otherwise indicated. BMI = body mass index; FEV1 = forced expiratory volume in 1 second; FVC = forced vital capacity; ICS = inhaled corticosteroid; PN = predicted normal; VC = vital capacity. * Data not collected in healthy subjects on FVC, FEV1, time since diagnosis (not applicable [NA]), smoking (NA) and ICS (NA) at study entry.

Respiratory Therapy Vol. 5 No. 1 n February-March 2010 47
on 4 September 2006 and the last subject completed the study on 22 July 2007.
COPD patients and healthy subjects attended the clinic at the beginning and end of run-in (visits 1-2). Informed consent was obtained at visit 1 and spirometry (FEV1) was performed at visit 2, from 2 to 8 days before visit 3 (start of the study drug administration). Forty-eight hours prior to visit 2, and throughout the study from then on, COPD patients using ICS or ICS/LABA combination therapies (budesonide/formoterol or salmeterol/fluticasone) were switched to equivalent doses of beclomethasone dipropionate (BDP). Use of other corticosteroids (including nasal and oral) was not permitted throughout the study. Patients were also not allowed to use long-acting anticholinergics, e.g. tiotropium 48 hours prior to visit 2 and throughout the study. Healthy subjects were instructed that no concomitant medication was permitted, except at the discretion of the study investigator.
Following run-in, eligible participants were randomized to the treatment sequence. At each treatment visit (visits 3 and 4), study participants received, in random order, one inhalation of either budesonide/formoterol (Symbicort Turbuhaler, AstraZeneca, Lund, Sweden) 400/12 μg (metered dose) plus placebo by Diskus (GlaxoSmithKline, Middlesex, UK) or salmeterol/fluticasone (Seretide Diskus, GlaxoSmithKline, Middlesex, UK) 50/500 μg plus placebo by Turbuhaler (Figure 1). COPD patients were not permitted to use BDP at either treatment visit. All participants were instructed and trained by the study investigator or nurse on the correct inhalation technique, and study drugs were administered at the same time point on both treatment visits ±30 minutes. Each treatment visit was separated by a washout period of 4-14 days.
Randomization codes were assigned in balanced blocks from a computer-generated list at AstraZeneca Research and Development, Södertälje. At each center, participants were randomized strictly sequentially as they became eligible.
Assessments The primary objective was to evaluate airway tissue availabilities of budesonide and fluticasone in patients with severe COPD, using the area under the curve (AUC) of the plasma concentrations for budesonide and fluticasone in COPD patients relative to healthy subjects as a surrogate marker for airway tissue availability.
In patients with severe COPD, secondary objectives included investigating the amounts of budesonide and fluticasone spontaneously expectorated in sputum (percentage of estimated lungdeposited dose [ELDD]) and the correlation between weight of sputum expectorated, lung function and the AUCs for budesonide and fluticasone.
Blood samples for measuring the pharmacokinetic variables (AUC, maximum plasma concentration (Cmax), time for maximum plasma concentration (Tmax) and mean residence time [MRT]) of inhaled budesonide and fluticasone in plasma were obtained from all study participants via an indwelling plastic catheter in the forearm at pre-decided time points; before (at any time point between arrival at the clinic in the morning and inhalation of study drug) and at 10, 20, 40 and 60 minutes, and 2, 4, 6, 8 and 10 hours post-inhalation of the study drug at visits 3 and 4. The validated budesonide and fluticasone assays were based on a combined method of liquid chromatography-mass spectrometry (LC-MS/MS).
Since the pharmacokinetics of budesonide and fluticasone differ markedly (ie, the uptake of fluticasone over the lung to the circulation is slower than for budesonide and the volume of distribution higher versus budesonide ),14,15 healthy subjects were used as a control.
2 3 4 5
Time since administration (hours)
Pla
sm
a s
tero
id c
on
cen
trati
on
(n
mo
l/l)
BUD/FORM
SAL/FLU
6 7 8 9 1010
0
0.4
0.8
1.2
2.0
1.6
2.4
Severe COPDPatients
BUD/FORM
SAL/FLU
Healthy Subjects
Figure 3
Figure 3. Mean plasma concentration of budesonide and fluticasone over 10-hour sampling period in severe COPD patients and healthy subjects.Mean (geometric) plasma concentration of budesonide and fluticasone after a single inhalation of budesonide/formoterol (BUD/FORM) (squares) and salmeterol/fluticasone (SAL/FLU) (circles), respectively, in severe COPD patients (solid lines) and healthy subjects (dashed lines).
Figure 4. Cumulative mean amounts of expectorated sputum (A) and budesonide and fluticasone (B) over 6-hour collection.Mean value plots of the amount of (A) expectorated sputum (arithmetic means) and (B) budesonide and fluticasone in the expectorated sputum (percentage of estimated lung deposited dose [ELDD], geometric mean), cumulative over the 6-hour collection period. BUD/FORM = budesonide/formoterol, SAL/FLU = salmeterol/fluticasone
Figure 4
2 3 4 5
Time since administration (hours)
Pla
sm
a s
tero
id c
on
cen
trati
on
(n
mo
l/l)
BUD/FORM
SAL/FLU
6 7 8 9 1010
0
0.4
0.8
1.2
2.0
1.6
2.4
Severe COPDPatients
BUD/FORM
SAL/FLU
Healthy Subjects
Figure 3

48 Respiratory Therapy Vol. 5 No. 1 n February-March 2010
Spontaneously expectorated sputum was collected from severe COPD patients over seven time intervals for up to 6 hours (0-10, 10-20, 20-40, 40-60, 60-120, 120-240, and 240-360 min) after study drug inhalation. Samples from each time interval were pooled, frozen immediately and stored at -20°C until further processing. After thawing, the entire expectorate was homogenized using an energetic ultrasonification treatment in combination with 0.1% dithiothreitol, as previously described.16 Analysis of the liquidized sputum was performed using an LC-MS/MS method to measure concentrations of budesonide and fluticasone propionate. The method was validated according to the principles of the FDA Guidance for Industry Bioanalytical Method Validation.17 The assay had a coefficient of variance at lower limit of quantification of ≤±20%, in accordance with the FDA Guidelines17 and lower and upper limits of detection of 5 nM and 10,000 nM respectively for budesonide, and 5 nM and 100 nM respectively for fluticasone.
All hypothesis testing was done using two-sided alternative hypotheses with P-values <5% considered statistically significant. Based on data from previous studies, the inter-individual (between-subject) standard deviation for the ratio of AUC between budesonide and fluticasone in healthy subjects has been
Figure 5. The relationship between drug exposure and expectorated steroid for budesonide (A) and fluticasone (B).Area under the curve (AUC) versus the amount of expectorated ICS. A) Budesonide: p = 0.33; B) fluticasone: p = 0.013 (Spearman’s rank correlation test).
Figure 6. Dependency of lung obstruction on AUC.The relationship between area under the curve (AUC) ratio for plasma concentration of fluticasone (FLU) versus budesonide (BUD) and lung function (forced expiratory volume in 1 second [FEV1], % predicted normal); p = 0.026 (Spearman’s rank correlation test).
Figure 5
Figure 6
estimated to be 0.29 (pooled) on the logarithmic scale.8
Assuming a similar variation among severe COPD patients, a total of 24 patients per group was required to give 90% power to detect a 24% reduction (fluticasone expected to give a lower ratio than budesonide) in the ratio of AUC (analyzed in a multiplicative model) between COPD patients and healthy subjects.
The primary end point (AUC for budesonide and fluticasone) was assessed by a multiplicative linear mixed-effect model, with subject as a random factor and treatment, period, group (severe COPD patient or healthy subject) and treatment-group interaction as fixed factors, which was fitted to the individual dose-adjusted AUCs of fluticasone and budesonide plasma concentrations.
The relative systemic bioavailability of each ICS was estimated from this model for patients with severe COPD and healthy subjects, and expressed as the mean AUC ratio (dose-adjusted) between fluticasone and budesonide. To address the primary objective, the systemic exposure of fluticasone and budesonide was estimated from the model as the mean ratio for the dose-adjusted AUC between fluticasone and budesonide in severe COPD patients, and the mean ratio for doseadjusted AUC between fluticasone and budesonide in healthy subjects. The associated 95% confidence intervals (CIs) were calculated.
The concentrations of budesonide and fluticasone in the expectorated sputum samples during 6 hours post-inhalation (percentage of the ELDD) were compared in severe COPD patients using a similar model, with treatment, period and patient as fixed factors. The correlation between drugadjusted AUC and the amount of expectorated sputum for each ICS was investigated using linear regression on log AUCs and log sputum weights. The lung-delivered doses of both steroids were calculated by assuming an ELDD that was 40% of nominal dose for Turbuhaler and 15% of nominal dose for Diskus.8
Safety outcomes were described using descriptive statistics. Safety analyses were performed on all patients who inhaled one dose or more of the study drug (full analysis set).
Results Forty-six COPD patients and 44 healthy subjects were enrolled for the study. Twenty-eight COPD patients (mean baseline FEV1 37.5% predicted normal) and 27 healthy subjects (mean

Respiratory Therapy Vol. 5 No. 1 n February-March 2010 49
baseline FEV1 103.3% predicted normal) were randomized (Figure 2). During the study, three subjects (5%) withdrew after randomization (two COPD patients and one healthy subject).
A greater proportion of severe COPD patients were male (75%) compared with healthy subjects (41%) (Table 1). Patients with severe COPD were also older and had a higher body mass index.
The mean plasma AUC values were lower in COPD patients versus healthy subjects for budesonide (3.07 μM·hr versus 6.21 μM·hr) and fluticasone (0.84 μM·hr versus 1.50 μM·hr) (Table 2A). The dose-adjusted AUC (geometric mean) ratios in healthy subjects and patients with severe COPD for plasma budesonide and fluticasone were similar (2.02 versus 1.80; primary end point) (Table 2B). The healthy subjects/severe COPD patient ratio of the fluticasone/budesonide ratios was estimated to be 89%, which was not significant between the drugs.
The pharmacokinetics of budesonide and fluticasone differed from one another and between the two study populations investigated. In the patients with severe COPD, budesonide showed a fast uptake from the airways (Figure 3) with a Tmax of 15.5 min compared with 50.8 min for fluticasone, and a Cmax of 1.08 μM compared with 0.09 μM for fluticasone (Table 3). In addition, budesonide had a lower MRT in the systemic circulation compared with fluticasone (4.41 hrs versus 12.78 hrs, respectively) in severe COPD patients. In the COPD patients, the plasma concentration curve showed a more distinct peak for budesonide than for fluticasone and a similar substance difference was seen in healthy subjects (Figure 3). However, there was a tendency for both ICSs to appear in lower concentrations in severe COPD patients than in healthy subjects (Figure 3, Table 2).
Budesonide and fluticasone in expectorated sputum over the 6-hour collection period in COPD patients The average weight of expectorated sputum over the 6-hour collection time period was similar for both treatment periods (Figure 4A). The majority of the expectorated fraction of budesonide was retrieved within the first 2 hours, after which very little was added (Figure 4B). In contrast, fluticasone was continuously expectorated over a longer time period (Figure 4B). The mean expectorated amount of fluticasone (a
percentage of ELDD; geometric mean 5.78; 95% CI: 2.59-12.9) was approximately five times higher than budesonide (geometric mean 1.11; 95% CI: 0.52-2.37) over the 6-hour post-dose time period (fluticasone/budesonide: geometric mean 5.21; 95% CI: 1.72-15.8; p=0.006).
There was a tendency for a negative relationship to exist between the amount of expectorated fluticasone and the fluticasone AUC. This was not observed for budesonide (Figure 5). There was also a tendency for the AUC ratio of fluticasone to budesonide to decline at lower FEV1 % predicted normal, i.e. AUC for fluticasone decreases relative to budesonide in patients with lower lung function (Figure 6).
Discussion This study demonstrated that after inhalation with a LABA, plasma levels of budesonide and fluticasone are lower in patients with severe COPD than in healthy volunteers; however, there is no difference in the AUC ratios between the two steroids. Fluticasone is present in the sputum for longer than budesonide resulting in a higher proportion of the inhaled dose being expectorated in the sputum.
The study did not demonstrate a difference in the ratio of the relative systemic availabilities of inhaled budesonide and fluticasone between healthy subjects and patients with severe COPD. This finding is counter to previous clinical studies that have reported a lower systemic bioavailability of fluticasone, but not budesonide, among patients with marked airway obstruction due to asthma compared with healthy subjects.13,14,18 These previous observations have been partly attributed to the more central deposition of ICS in obstructed airways and the higher lipophilicity of fluticasone relative to budesonide.10,11 Both drugs are likely to be deposited more proximally in the obstructive airway but being more lipophilic, fluticasone is less soluble in the airway mucus than budesonide and will therefore be present in the proximal airways for longer and thus, is more likely to be cleared from the airways than budesonide.
Possible reasons for the conflicting results between our study and these previous studies could include the fact that we selected patients with severe COPD (mean 37.5% FEV1 predicted normal) and daily sputum production, whereas the
Table 2. Systemic availability of budesonide and fluticasone A)ICS Subject group n AUC (µM·hr)
geometric meanCV
Budesonide Healthy subjects 24 6.21 32.7Severe COPD patients 24 3.07 106.4
Fluticasone Healthy subjects 26 1.50 42.5Severe COPD patients 23 0.84 46.0
B)Parameter Dose-adjusted AUC
geometric mean ratio95% CI
HS/COPD for BUD 2.02 1.48, 2.76HS/COPD for FLU 1.80 1.32, 2.45FLU/BUD for HS/COPD 0.89 0.58, 1.37
Summary of A) geometric means of area under the curve (AUC) for budesonide and fluticasone and B) geometric mean ratios for dose-adjusted AUC BUD = budesonide; CI = confidence interval; CV = coefficient of variation; FLU = fluticasone; HS = healthy subjects.

50 Respiratory Therapy Vol. 5 No. 1 n February-March 2010
aforementioned studies were in subjects with asthma.13,14,18 This may be of importance given the fact that mucociliary clearance is impaired in COPD due to long-term tobacco smoking19 and the presence of a compensatory cough mechanism. It can be speculated that uptransport of the lung deposited dose via cough is more rapid than via the slow mucociliary mechanism and that the more rapid cough uptransport in COPD would alleviate the differences between budesonide and fluticasone in the degree of mucociliary clearance compared to asthma. The extent to which long-term smoking affects absorption of inhaled steroids over airway epithelium is not known. A further difference between our study and previous studies is that we combined budesonide and fluticasone with a LABA (formoterol and salmeterol, respectively), whereas previous studies have used ICSs alone.13,14,18,20 Studies have shown that LABAs can affect mucociliary beat frequency,21-23 potentiate the inhibitory effect of ICSs on mucin secretion24 and increase mucus hydration,25 although we think these effects are not likely to be seen after a single dose of LABA.
Our data confirmed previously reported differences in the pharmacokinetics of both steroids in the severe COPD population.14,26 Budesonide was more rapidly absorbed in the airway tissue compared with the highly lipophilic fluticasone as evidenced by a budesonide Tmax of 15.5 minutes compared with 50.8 minutes for fluticasone, which is consistent with its contribution to a more rapid onset of action, as demonstrated when combined to formoterol, by Cazzola and colleagues.27
The differences in lung disposition could also have been influenced by differences in inhaler device and particle size.28-31 As reviewed by Newman and Chan,28 particle size and mode of inhalation are two important determinants of the proportion of ICS that is deposited in the respiratory tract. A particle with an aerodynamic diameter of <5 μm is more likely to be deposited in the bronchi and bronchioles compared with a particle >5 μm, which is deposited to a higher degree in the mouth and throat.32 In vitro studies have reported the amount of fine particles (aerodynamic diameter <5 μm) to be more than double with Turbuhaler compared with Diskus.33 This may correspond to a higher and more peripheral lung deposition of budesonide (via Turbuhaler) compared with fluticasone (via Diskus).8,29
A novel observation was the significant difference in the amount of the two ICSs in expectorated sputum. The amount of fluticasone expectorated (percentage of ELDD) was five times higher than for budesonide, supporting our hypothesis that its greater lipophilicity leads to greater airway clearance through mucociliary clearance and/or cough. On average, approximately
6% of ELDD (geometric mean) of inhaled fluticasone was expectorated over the 6 hours after drug administration, whereas most of the 1% of budesonide expectorated was within the first two hours. Whether this finding could result in decreased host defenses and therefore provide an explanation for the increased risk of developing pneumonia, as reported in a number of recent studies with fluticasone alone or in combination with salmeterol, is an intriguing hypothesis and one worthy of further evaluation.6,34-36
There was a weak inverse relationship between systemic availability, measured as AUC, for fluticasone and the amount expectorated in the sputum; a higher sputum clearance of fluticasone resulted in a lower airway tissue availability. Such a relationship was not observed for budesonide. Spirometry was not conducted directly before each treatment period so as not to affect spontaneous sputum sampling. However, the data suggest that there was a tendency for lower fluticasone AUC relative to budesonide in patients with lower FEV1 (% predicted normal), indicating that higher airway obstruction results in lower systemic and lung availability of fluticasone relative to budesonide.
Certain limitations of this analysis should be acknowledged. These include the relatively small sample size and lack of ICS monocomponent treatment to investigate how ICS is handled with and without LABAs, which can increase mucociliary clearance.21-23,37,38 However, now that combined therapy is recommended for patients with severe COPD, we believe the current study is more clinically relevant. It is also important to note that sputum was collected upon spontaneous expectoration and therefore probably only represents a fraction of the total amount of sputum produced during this period. Thus, the absolute amount of ICS measured in the sputum was likely to be an underestimate, with the remaining sputum being swallowed before expectoration. Nevertheless, differences in expectorated amounts were controlled for through the cross-over study design, and data were reproducible.
Conclusions The present study confirmed that plasma levels of both fluticasone and budesonide are lower in subjects with severe COPD but did not demonstrate a difference in the systemic exposure between budesonide and fluticasone in severe COPD patients relative to healthy subjects. In patients with COPD, a larger fraction of fluticasone was recovered in the expectorated sputum than for budesonide, indicating that fluticasone is more extensively cleared from the airways, while budesonide is more rapidly absorbed into the airway tissue.
References 1 Global strategy for the diagnosis, management, and
prevention of chronic obstructive pulmonary disease. Updated 2007 [http://www.goldcopd.org/Guidelineitem.asp?l1=2&l2=1&intId=989]
2 World Health Statistics [http://www.who.int/whosis/whostat/2008/en/index.html]
3 National Institute for Clinical Excellence: Chronic obstructive pulmonary disease (Clinical Guideline 12). London: National Institute for Clinical Excellence; 2004.
4 Calverley PM, Boonsawat W, Cseke Z, Zhong N, Peterson S, Olsson H: Maintenance therapy with budesonide and formoterol in chronic obstructive pulmonary disease. Eur Respir J 2003, 22:912-919.
Table 3. Summary of pharmacokinetic parameters in plasma for severe COPD patients.
Treatment n Mean SD/CVTmax (min) Budesonide 24 15.5* 7.2*
Fluticasone 23 50.8* 25.4* MRT (h) Budesonide 24 4.41* 1.59*
Fluticasone 23 12.78* 4.58* Cmax (μM) Budesonide 24 1.08† 95.9†
Fluticasone 23 0.09† 37.9†
Cmax = maximum concentration; CV = coefficient of variation; MRT = mean residence time; SD = standard deviation; Tmax = time to maximum concentration. *Arithmetic mean/SD; † Geometric mean/CV

Respiratory Therapy Vol. 5 No. 1 n February-March 2010 51
5 Szafranski W, Cukier A, Ramirez A, Menga G, Sansores R, Nahabedian S, Peterson S, Olsson H: Efficacy and safety of budesonide/formoterol in the management of chronic obstructive pulmonary disease. Eur Respir J 2003, 21:74-81.
6 Calverley PMA, Anderson JA, Celli B, Ferguson GT, Jenkins C, Jones PW, Yates JC, Vestbo J, for the TORCH investigators: Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med 2007, 356:775-789.
7 Calverley PM, Pauwels R, Vestbo J, Jones P, Pride N, Gulsvik A, Anderson J, Maden C: Combined salmeterol and fluticasone in the treatment of chronic obstructive pulmonary disease: a randomised controlled trial. Lancet 2003, 361:449-456.
8 Thorsson L, Edsbacker S, Kallen A, Lofdahl CG: Pharmacokinetics and systemic activity of fluticasone via Diskus and pMDI, and of budesonide via Turbuhaler. Br J Clin Pharmacol 2001, 52:529-538.
9 Volovitz B: Inhaled budesonide in the management of acute worsenings and exacerbations of asthma: a review of the evidence. Respir Med 2007, 101:685-695.
10 Brattsand R, Miller-Larsson A: The role of intracellular esterification in budesonide once-daily dosing and airway selectivity. Clin Ther 2003, 25 Suppl C:C28-C41.
11 Edsbacker S, Wollmer P, Selroos O, Borgstrom L, Olsson B, Ingelf J: Do airway clearance mechanisms influence the local and systemic effects of inhaled corticosteroids? Pulm Pharmacol Ther 2008, 21:247-258.
12 Yanai M, Hatazawa J, Ojima F, Sasaki H, Itoh M, Ido T: Deposition and clearance of inhaled 18FDG powder in patients with chronic obstructive pulmonary disease. Eur Respir J 1998, 11:1342-1348.
13 Harrison TW, Wisniewski A, Honour J, Tattersfield AE: Comparison of the systemic effects of fluticasone propionate and budesonide given by dry powder inhaler in healthy and asthmatic subjects. Thorax 2001, 56:186-191.
14 Harrison TW, Tattersfield AE: Plasma concentrations of fluticasone propionate and budesonide following inhalation from dry powder inhalers by healthy and asthmatic subjects. Thorax 2003, 58:258-260.
15 Winkler J, Hochhaus G, Derendorf H: How the lung handles drugs: pharmacokinetics and pharmacodynamics of inhaled corticosteroids. Proc Am Thorac Soc 2004, 1:356-363.
16 Grebski E, Peterson C, Medici TC: Effect of physical and chemical methods of homogenization on inflammatory mediators in sputum of asthma patients. Chest 2001, 119:1521-1525.
17 Guidance for Industry. Bioanalytical method validation [http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM070107.pdf]
18 Brutsche MH, Brutsche IC, Munawar M, Langley SJ, Masterson CM, Daley-Yates PT, Brown R, Custovic A, Woodcock A: Comparison of pharmacokinetics and systemic effects of inhaled fluticasone propionate in patients with asthma and healthy volunteers: a randomised crossover study. Lancet 2000, 356:556-561.
19 Rogers DF: Mucociliary dysfunction in COPD: effect of current pharmacotherapeutic options. Pulm Pharmacol Ther 2005, 18:1-8.
20 Singh SD, Whale C, Houghton N, Daley-Yates P, Kirby SM, Woodcock AA: Pharmacokinetics and systemic effects of inhaled fluticasone propionate in chronic obstructive pulmonary disease. Br J Clin Pharmacol 2003, 55:375-381.
21 Melloni B, Germouty J: [The influence of a new beta agonist: formoterol on mucociliary function]. Rev Mal Respir 1992, 9:503-507.
22 Piatti G, Ambrosetti U, Santus P, Allegra L: Effects of salmeterol on cilia and mucus in COPD and pneumonia patients. Pharmacol Res 2005, 51:165-168.
23 Lindberg S, Khan R, Runer T: The effects of formoterol, a long-acting beta 2-adrenoceptor agonist, on mucociliary activity. Eur J Pharmacol 1995, 285:275-280.
24 Salathe M: Effects of beta-agonists on airway epithelial cells. J Allergy Clin Immunol 2002, 110:S275-S281.
25 Wanner A, Salathe M, O’Riordan TG: Mucociliary clearance in the airways. Am J Respir Crit Care Med 1996, 154:1868-1902.
26 Mortimer KJ, Tattersfield AE, Tang Y, Wu K, Lewis S, Hochhaus G, Harrison TW: Plasma concentrations of fluticasone propionate and budesonide following inhalation: effect of induced bronchoconstriction. Br J Clin Pharmacol 2007, 64:439-444.
27 Cazzola M, Santus P, Di Marco F, Carlucci P, Mondoni M, Matera MG, Centanni S: Onset of action of formoterol/budesonide in single inhaler vs. formoterol in patients with COPD. Pulm Pharmacol Ther 2004, 17:121-125.
28 Newman SP, Chan HK: In vitro/in vivo comparisons in pulmonary drug delivery. J Aerosol Med Pulm Drug Deliv 2008, 21:77-84.
29 Agertoft L, Pedersen S: Lung deposition and systemic availability of fluticasone Diskus and budesonide Turbuhaler in children. Am J Respir Crit Care Med 2003, 168:779-782.
30 Hochhaus G: New developments in corticosteroids. Proc Am Thorac Soc 2004, 1:269-274.
31 Derendorf H, Nave R, Drollmann A, Cerasoli F, Wurst W: Relevance of pharmacokinetics and pharmacodynamics of inhaled corticosteroids to asthma. Eur Respir J 2006, 28:1042-1050.
32 Pritchard JN: The influence of lung deposition on clinical response. J Aerosol Med 2001, 14 Suppl 1:S19-S26.
33 Bisgaard H, Klug B, Sumby BS, Burnell PK: Fine particle mass from the Diskus inhaler and Turbuhaler inhaler in children with asthma. Eur Respir J 1998, 11:1111-1115.
34 Ferguson GT, Anzueto A, Fei R, Emmett A, Knobil K, Kalberg C: Effect of fluticasone propionate/salmeterol (250/50 microg) or salmeterol (50 microg) on COPD exacerbations. Respir Med 2008, 102:1099-1108.
35 Kardos P, Wencker M, Glaab T, Vogelmeier C: Impact of salmeterol/fluticasone propionate versus salmeterol on exacerbations in severe chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2007, 175:144-149.
36 Wedzicha JA, Calverley PM, Seemungal TA, Hagan G, Ansari Z, Stockley RA: The prevention of COPD exacerbations by salmeterol/fluticasone propionate or tiotropium bromide. Am J Respir Crit Care Med 2008, 177:19-26.
37 Bennett WD, Almond MA, Zeman KL, Johnson JG, Donohue JF: Effect of salmeterol on mucociliary and cough clearance in chronic bronchitis. Pulmonary Pharmacology & Therapeutics 2006, 19:96-100.
38 Hasani A, Toms N, Agnew JE, Lloyd J, Dilworth JP: Mucociliary clearance in COPD can be increased by both a D2/beta2 and a standard beta2 agonists. Respir Med 2005, 99:145-151.
52 Respiratory Therapy Vol. 5 No. 1 n February-March 2010
AbstractIntroduction: Tracheal agenesis is a very rare congenital airway anomaly. It may pose a great challenge to the first attending physician both in diagnosis and in establishing the airway during the first day of life.
Case presentation: We report a newborn Malay baby boy with trachea agenesis (type III by Floyd’s classification) who presented with severe respiratory distress immediately after birth. Clinical diagnosis in this case was not straightforward, as it started with difficulty in intubation followed by an unsuccessful emergency tracheostomy in the neonatal intensive care unit. Urgent surgical neck exploration with endoscopic examination in the general operating theatre revealed the final diagnosis. The authors present a short description of the embryopathology and diagnostic criteria of the abnormality.
Conclusion: We hope this case presentation will be valuable in increasing the awareness of physicians about this rare cause of tracheal obstruction or difficult intubation.
IntroductionTracheal agenesis is a rare congenital airway anomaly. There were 116 cases of tracheal agenesis reported in the literature between 1900 and (September) 2004.1 Airway management in this abnormality poses a great challenge to otolaryngologists, anaesthetists and pediatricians. This condition is incompatible with life. At present there is no specific surgical management technique that is associated with survival of tracheal agenesis
Tracheal Agenesis as a Rare Cause of Difficult Intubation in a Newborn with Respiratory Distress: a case reportRaja Ahmad, Kahairi Abdullah, Lukman Mokhtar, Ahmad Fadzil
The newborn with tracheal agenesis usually presents with immediate and severe respiratory distress, and the only way to provide ventilation is through the esophagus. Performing endotracheal intubation or tracheostomy does not normally help. Bag-mask ventilation and intubation of the esophagus may allow ventilation of the lungs. Neck exploration during the tracheostomy and endoscopic evaluation will establish the diagnosis. The ex-utero intrapartum treatment (EXIT) procedure is an excellent method developed for use in anticipation of possible airway compromises in newborn babies at birth.
Case PresentationA 2.4 kg Malay baby boy was delivered after 37 weeks of gestation by spontaneous vaginal delivery. The pregnancy was complicated by polyhydramnios. The baby developed immediate respiratory distress at birth with an Apgar score of 1 at 1 min, 5 at 5 min, and 6 at 10 minutes of life. He was initially resuscitated with bag-mask ventilation, and subsequently transferred to the neonatal intensive care unit (NICU). Multiple oral endotracheal intubations were attempted in the NICU with no success. Bag-mask ventilation was continued and an otolaryngologist was consulted for emergency tracheostomy. Oxygen saturation was successfully maintained at above 85% with bag-mask ventilation. It was possible to pass a Ryle’s tube through both nostrils.
During the surgical procedure, the trachea could not be identified. The baby was transferred to the operating theatre for neck exploration, and a complete endoscopic examination was performed to evaluate airway patency. During the neck exploration, it was noted that the larynx ended blindly at the cricoid level (Figure 1), while the trachea was absent. A laryngoscopic evaluation without muscle relaxant disclosed a cleft larynx with bilateral immobile vocal cords (Figure 2). A bronchoscope could not be passed below the vocal cords. An esophagoscopy was performed which revealed two openings at the distal portion of the esophagus, which communicated with the left and right bronchus, respectively (Figure 3).
At the end of the surgical procedure, an endotracheal tube was inserted into the esophagus and effective ventilation confirmed by visualization of normal chest expansion and good oxygen saturation. The baby also had persistent ductus arteriosus, dysplasia of the right radius and the right thumb, and an imperforated anus. A diagnosis of tracheal agenesis was made and the family members were counseled about the grim prognosis. Life support was discontinued with the agreement of the parents, and the baby was allowed to die.
Authors Ahmad and Abdullah are with the Department of
Otolaryngology — Head & Neck Surgery, Faculty of Medicine; Mokhtar
is with the Department of Anaesthesiology and Intensive Care, Faculty
of Medicine, International Islamic University Malaysia; Fadzil is with the
Department of Pediatric, Tengku Ampuan Afzan Hospital, Malaysia.
Reprinted from BioMed Central, Journal of Medical Case Reports, © 2009
Ahmad et al, licensee BioMed Central Ltd. This is an open access article
distributed under the terms of the Creative Commons Attribution License.
The authors note: Written informed consent could not be obtained in this
case since the patient was lost to follow-up. The authors believe that this
case report contains a worthwhile clinical lesson which could not be made
as effectively in any other way, and expect that the patient and her family
would not have objected to the publication since every effort was made so
that the infant remained anonymous.

Respiratory Therapy Vol. 5 No. 1 n February-March 2010 53
DiscussionAt present, there is no specific surgical management that allows survival in cases of tracheal agenesis. Normally, a newborn with tracheal agenesis presents with immediate respiratory distress and an absent or very weak cry. This rare congenital anomaly might confound the attending doctor in the delivery room or operating theatre.
The embryopathology resulting in this abnormality occurs during the first eight weeks of gestation. The tracheo-pulmonary complex develops from the respiratory diverticulum at the ventral aspect of the primitive foregut. A compromised vascular supply to the developing trachea during this stage may cause tracheal agenesis or tracheal stenosis with complete tracheal ring.2 According to Merei et al,3 the point of bifurcation between the developing trachea at ventral and developing esophagus at dorsal foregut remains fixed in relation to the cervical vertebra. Caudally, the respiratory diverticulum will develop into the carina and broncho-pulmonary tree. The cephalic aspect of the respiratory diverticulum will be elongated to form the trachea and the infra-glottic structure. Tracheal agenesis results when this normal elongation process fails to take place.1 This anomaly is associated with relatively normal supra-glottic structures and pulmonary development, as seen in this case. The congenital abnormality is only limited to the region of the developing trachea. The severity of tracheal agenesis was described in detail by Floyd and colleagues and classified into three types.4 In Type I, a short segment of the trachea fails to elongate to fuse with the larynx. In Type II, the respiratory diverticulum fuses in midline to form the carina but tracheal elongation does not take place. And in type III, the respiratory diverticula does not
fuse in the midline, resulting in two fistula opening at the lower part of esophagus. The present case is compatible with a type III abnormality. Type II remains the most common abnormality (61%), followed by type III (23%) and type I (11%).1
Tracheal agenesis is commonly associated with other congenital anomalies such as vertebral defects, anal atresia, tracheoesophageal fistula, esophageal atresia, cardiovascular defects, limb defects, duodenal atresia and renal defects. Tracheal agenesis can be a manifestation of several syndromes such as VATER (vertebrae, anus, trachea, esophagus, and renal), also known as VACTERL, and TARCD (total alkaloids from rhizoma corydalis decumbeutis).
A high index of suspicion is required to diagnose tracheal atresia. Antepartum features that would corroborate such suspicion are the presence of polyhydramnios with multiple fetal anomalies. During birth, the baby may not cry or may have a weak cry. An acute severe respiratory distress develops and multiple attempts at intubations fail. Laryngoscopy will reveal immobile vocal cords lying in the midline position. Other findings are a cleft between the arytenoids, as well as associated congenital anomalies. Good oxygenation may be maintained with bag-mask ventilation or esophageal intubation. The diagnosis is made through neck exploration during emergency tracheostomy and an endoscopic evaluation of the larynx and esophagus. A pre-delivery procedure with three-dimensional ultrasound or fetal magnetic resonance imaging allows a complete evaluation of this upper airway abnormality. The ex-utero intrapartum treatment (EXIT) procedure can be planned based on the imaging results. EXIT procedure can reduce the risk of respiratory distress immediately after birth.5
ConclusionTracheal agenesis should be suspected in a newborn baby who presents with immediate respiratory distress, as well as extremely weak cry and failed intubation despite adequate ventilation with facemask. The establishment of airway after an insertion of endotracheal tube in the oesophagus will further enhance the index of suspicion before the definitive endoscopic evaluation.
References1 Lander TA, Schauer G, Bendel-Stenzel E, Sidman JD: Tracheal
agenesis in newborns. Laryngoscope 2004, 114:1633-1636.2 Holinger LD, Lusk RP, Green CG: Pediatric Larngology
Bronchoesophagology. Philadelphia: Lippincott-Raven Publishers; 1997: 6.
3 Merei JM, Hutson JM: Embryogenesis of tracheoesophageal anomalies: a review. Pediatr Surg Int 2002, 18:319-326.
4 Floyd J, Campbell DC, Dominy DE: Agenesis of the trachea. Am Rev Respir Dis 1962, 86: 557-560.
5 Peng SS, Hsu WC, Chou HC, Peng SS, Chen LK, Chang YL, Hsieh FJ: Prenatal three-dimensional ultrasound and magnetic resonance imaging evaluation of a fetal oral tumor in preparation for the ex utero intrapartum treatment (EXIT) procedure. Ultrasound Review of Obstetrics and Gynecology 2005. (25) 1: 76.
Figure 1. Neck exploration revealed a normal larynx that ended in a blind pouch at the level of cricoid (black arrow). The dome-shaped cricoid occludes the lumen.
Figure 2. Laryngoscopy examination revealed a cleft larynx with immobile vocal cords bilaterally in midline position.
Figure 3. Esophagoscopy view showing one of the openings into the left bronchus at the distal end of the esophagus.

54 Respiratory Therapy Vol. 5 No. 1 n February-March 2010
Determinants in Early Life for Asthma DevelopmentHugo P.S. Van Bever
AbstractA reliable screening test in newborns for the subsequent development of bronchial asthma (BA) has not been found yet. This is mainly due to the complexity of BA, being made up by different types and underlying mechanisms. In different studies, a number of risk factors for BA have been identified. These include a positive family history of BA, passive smoking (also during pregnancy), and prematurity (including pulmonary infections, RDS and BPD), early viral respiratory infections (such as RSV-bronchiolitis), male gender, early lung function abnormalities and atopic constitution. Therefore, early symptoms and markers of allergy (ie The Allergic March) and a positive family history for allergy should be considered as important risk factors for the development of BA.
BackgroundWhat is asthma? Bronchial asthma (BA) is more than just one disease of the lower airways, and is now considered to be a syndrome, the asthma syndrome, made by a spectrum of different conditions that are manifested by recurrent symptoms of bronchial obstruction, ie recurrent symptoms of wheezing and/or cough, and having as a major feature the existence of bronchial hyperreactivity, as a consequence of chronic bronchial inflammation. A number of classifications of BA have been proposed, based on severity, etiology or age of the patient. In one classification two major subtypes of BA are distinguished: primary and secondary BA. Furthermore, it is recognized that BA can also be a consequence of an underlying specific airway disease.1
Primary asthma can be considered as a type of asthma of which the etiology can be situated in the bronchi itself, ie bronchial hyperresponsiveness to a number of triggers, such as allergens, viruses and pollution. Secondary asthma is a type of asthma of which the etiology is situated outside the bronchi, such as in asthma maintained by chronic rhino-sinusitis or gastro-oesophageal reflux. In this latter type, bronchial hyperresponsiveness is a secondary phenomenon, indicating that treatment should be focused on pathologies outside the lower airways. Asthma with specific airway diseases is the existence of asthmatic symptoms (ie recurrent wheeze and/or cough)
in specific airway diseases such as cystic fibrosis, structural bronchial malformations, immune deficiencies, ciliar dyskinesia and others.
This classification of BA not only refers to the different causes of asthma, but also to a different prognosis, suggesting that specific treatment regimens should be used. This is clearly illustrated by looking at asthma in children younger than 3 years of age. The evidence suggests that recurrent obstructive symptoms (ie recurrent wheezing) remit in a large number of these children who develop these symptoms during the first 3 years of life. In these children, recurrent wheezing is usually evoked by viral infections and low lung function parameters seem to be the main risk factor for these transient episodes. On the other hand, children who will go on to develop persistent wheezing beyond infancy and early childhood usually have a family history of asthma and allergies and present with allergic symptoms very early in life.2,3
Determinants in early life for asthma development : Since asthma (ie recurrent wheezing) constitutes different types, it is very difficult to predict its occurrence, especially in newborns. Furthermore, a severe lower airway infection with RSV or with another respiratory virus is able to induce BA in a previously complete healthy baby with a complete negative family history for BA or allergy.4 Therefore, there are few truly justified recommendations for the prevention of asthma.5 The GINA guidelines (2006, chapter 4) mention “…few measures can be recommended for prevention of asthma because the development of the disease is complex and incompletely understood.”
However, in different studies, a number of risk factors for BA have been described.1 These include: 1. A positive family history of BA, 2. A passive smoking (prenatally and postnatally), 3. Prematurity (including pulmonary infections, RDS and BPD), 4. Early viral respiratory infections (such as RSVbronchiolitis), 5. Male gender, 6. Early lung function abnormalities and 7. An atopic constitution.
1. Family history of BA: In a large number of studies it was demonstrated that a positive family history for BA and for atopy (see below) are important risk factors for BA. In a recent study from the South Bronx it was shown that the most important risk factors for BA are Hispanic ethnicity, family history of asthma, and exposure to tobacco smoke.6 In other studies the effect of early-life environmental exposures on genetic factors has been
The author is with the Department of Pediatrics, National University
Singapore. Reprinted from BioMed Central, Allergy, Asthma & Clinical
Immunology© 2009 Van Bever, licensee BioMed Central Ltd. This is an
open access article distributed under the terms of the Creative Commons
Attribution License.

Respiratory Therapy Vol. 5 No. 1 n February-March 2010 55
shown. In a study by Kuiper et al, a modification of the effect of family history of BA on respiratory morbidity by environmental exposures in early life was demonstrated. Postnatal parental smoking and high indoor dust mite allergen levels accentuated the increased risk of wheeze associated with a positive family history, whereas breast-feeding attenuated the increased risk of upper airway pathologies.7
2. Passive smoking: Although passive exposure to cigarette smoke in young children is a risk factor for respiratory symptoms, childhood asthma, airway hyperresponsiveness and diminished pulmonary function status, no definitive study has implicated passive smoking as a risk factor for the persistence of recurrent wheezing.1 On the other hand, it seems very acceptable that passive smoking worsens prognosis of BA in young children, based on the observation that lung growth is diminished in children from smoking pregnant women.8
3. Prematurity: Prematurity with respiratory morbidity, such as RDS, can result in longterm lung damage (bronchopulmonary dysplasia) and bronchial hyperreactivity, which is predisposing situation for severe viral-induced wheezing during years.9
4. Viral respiratory infections: RSV lower respiratory tract illnesses in early life are an independent risk factor for the subsequent development of wheezing up to age 11 years. Severe RSV infections, requiring hospitalization, can induce persistent IgE-mediated hypersensitivity reactions up to the age of 7 years.10,11 The exact mechanisms are fairly unknown, but a RSV-induced switch from Th1 to Th2 features has been shown.12 However, the relation between RSV infection and subsequent BA is still very much debated. It seems that pre-existing atopy may be a marker for more severe bronchiolitis and atopy itself predisposes to BA.13
5. Male gender: Male gender has been demonstrated to be a risk factor for BA in children before the age of 14 years, while female gender to be a risk factor for asthma in adults. In one study it was shown that boys had a higher incidence rate of BA, while girls had a greater deficit in pulmonary function, suggesting a worse long term prognosis in female patients.14 An explanation for this could be that boys have a higher prevalence of allergic sensitization than girls, while in adults the gender difference is reversed.15
6. Early lung function abnormalities: Early lung function abnormalities have been associated with an increased risk of recurrent wheezing. In a recent study it was found that poor airway function shortly after birth should be recognized as a risk factor for airflow obstruction in young adults and that prevention of chronic obstructive pulmonary disease might need to start in fetal life.16
7. Allergy as a major risk factor to develop persistent asthma: The causes of allergy are multi-factorial and the
development of an allergic disease is the result of complex interactions between genetic constitution and environmental factors. Genetic constitution is important, as it is in genetically predisposed individuals that the environment is able to trigger symptoms of allergy. At birth allergic symptoms usually are not present, although it was demonstrated that allergic immune responses already can start during fetal life and that the fetus is able to respond to allergens from week 20 of pregnancy.17 In young children, eczema and food allergy (diarrhea, vomiting, failure to thrive) are usually the first manifestations of allergy, while in older subjects allergy manifests itself more often as a chronic or recurrent asthma and/or allergic rhinitis. This phenomenon of switching from one expression of allergy to another is called the “Allergic March.”
Among risk factors to develop BA, from a substantial number of studies it was concluded that atopy is one of the most important risk factors.18 Early allergen exposure seems to be a major trigger, but attempts at prevention by allergen avoidance have produced conflicting results.19 Moreover, from recent studies it seems that there is no linear relationship between early allergen contacts and the development of BA, as both exposure to high doses and low doses of allergens might have a protective effect, suggesting the existence of a bellshaped relationship.20
It is generally accepted that atopy is associated with a poorer prognosis of asthma during childhood.1 Atopy was associated with a poorer prognosis of asthma during childhood.1 Atopy was associated with persistent wheezing in a cohort of babies at high risk for allergic diseases and was associated with an increased risk for both early and later childhood onset of wheezing.21 In a follow-up of a 1958 birth cohort, subjects who had asthma or wheezy bronchitis by age 16 years were twice as likely to have a report of wheezing during the preceding year if they had hay fever, allergic rhinitis, or eczema.22 Furthermore, children experiencing persistent asthma beyond early life have increased serum IgE levels during the first year of life and are more likely than other children to be sensitized to foods..23,24 In one study a clinical index, based on family history and atopic features, was proposed (Table 1).25 In that study it was found that 95% of young wheezy children with a negative index never developed asthma between the ages 6-13 years. In another study from Finland, food allergy during the first three years of life was also a risk factor to develop persistence of wheezing until school age.26
Taken together, it is clear that allergy is a risk factor to develop persistent asthma in infants and young children. Once asthma has itself established in the child, allergy appears not to be an indepdent determinant of prognosis into adulthood, suggesting that inflammatory processes in the airways run their own courses irrespective of the subject’s atopic status.1
Determinants in early life of atopy: Early prevention of allergic diseases, including BA, has been regarded as an important corner stone in the management of atopic diseases. Therefore, the identification of reliable screening markers detecting individuals (newborns) at risk has been an area of intense research during the past thirty years. Many efforts have been made to find reliable predictors of atopy which might identify children at risk and allow the initiation of primary preventive strategies at an early stage. As a consequence, various studies have been performed in which markers of atopy in cord blood were assessed.18 These include genetic markers of allergy, IgE levels, levels of soluble mediators of atopy (cytokines,
Table 1. A clinical index to define asthma risk (from Castro-Rodriguez et al, 2000)Major Criteria Minor Criteria 1. Parental asthma* 1. allergic rhinitis*2. eczema* 2. Wheezing apart from colds 3. Eosinophilia ( >4 %)
*Physician diagnosis of asthma, eczema or allergic rhinitis.

56 Respiratory Therapy Vol. 5 No. 1 n February-March 2010
receptors), determination of receptors connected to bacterial immune defense (linked to the so-called “Hygiene Hypothesis”), determination of polyunsaturated fatty acids, cytokine profiles of mononuclear cells and markers of antigen presenting cells.
From a number of studies it seems that interferon-gamma (IFN-y) might be one of the appropriate candidate-markers for the prediction of BA and allergy Production of IFN-y has been used as a potential marker for the postnatal immune maturation processes that are associated with the subsequent risk for development of BA or allergic diseases. Studies on cord blood mononuclear cells have shown that subjects who will develop allergic symptoms have a characteristic pattern of response that includes decreased production of IFN-y, suggesting a Th2-type predominance.27,28 Stern et al found that low IFN-y production by mitogen-stimulated mononuclear cells at the age of 9 months was associated with an increased risk of wheezing between 2 and 13 years.29 Guerra et al reported that low IFN-y production at 3 months of age was associated with recurrent wheeze in the first year of life.30
Björksten et al showed that interleukin-4 (IL-4) production by peripheral bloodmononuclear cells in early life may be predictive of the subsequent development of allergic symptoms.31 In another cross-sectional study, no major differences in dendritic cell features were found between children from allergic and nonallergic studies. However, no follow-up for wheezing was performed.32 In a more recent study from Germany, a strong interaction of cord blood adiponectin and history of atopic disease in the mother with respect to the risk of physician reported asthma or obstructive bronchitis was found (p=0.006). The authors concluded that in children of mothers with a history of atopy concentrations of adiponectin in cord blood could play an important role in determining risk of wheezing disorders in early childhood.33
Although the findings of these studies have improved current knowledge on the initial mechanisms and evolution of atopy (eg the prenatal events of atopy), most of these parameters that were studied did not show any reliable association or predictive value, and studies showed conflicting results. The main reasons for screening difficulties in atopic diseases include: 1/ allergic manifestations are usually not present at birth, but usually start during the first years of life, as a consequence of interactions between genetic constitution and environment. 2/ features of allergy can be present in healthy persons (eg positive skin prick tests were found in >10% of healthy children). 3/ so-called symptoms of allergy (asthma, rhinitis, eczema) can be present without the presence of allergy (=patients have negative skin prick tests). 4/ allergy is multi-factorial (a large number of genes involved in allergy have been described), dynamic, unpredictable, and certainly not a constant disease.
Nowadays we still have no reliable predictive marker(s) of allergy, although, in theory, because of its large burden of allergic diseases to society, it would be of value to identify newborns at risk. Furthermore, the effectiveness of specific primary preventive measures is very limited for the newborn at risk (apart from breast feeding and avoidance of passive smoking). Nowadays, the best screening for allergy still is an extensive family history (including questions on childhood of the parents), in combination with an objective assessment of allergy in the parents or siblings using skin prick testing or determination of specific serum IgE.
Conclusion A reliable screening test in newborns for the subsequent development of BA has not been found yet. This is mainly due to the complexity of BA, which is made up by different types and underlying mechanisms (ie The Asthma Syndrome). However, in different studies, a number of risk factors for BA have been identified, such as: a positive family history of BA, passive smoking (also during pregnancy), prematurity (including pulmonary infections, RDS and BPD), early viral respiratory infections (such as RSV-bronchiolities), male gender, early lung function abnormalities and atopic constitution. The major risk factor for persistent BA is an underlying allergic constitution. Early symptoms and markers of allergy (ie The Allergic March) and a positive family history for allergy should be considered as important risk factors for the development of asthma. As such, the profile of the newborn at risk to develop BA can be summarized as follows: it is a male, prematurely born infant whose parents suffer from asthma and/or allergy and who smoke. The baby has a dry skin with eczematous patches and develops a severe bronchiolitis early in life for which he had to be admitted to PICU for 1 week.
References 1 Van Bever HP, Desager KN, Hagendorens M. Critical
evaluation of prognostic factors in childhood asthma. Pediatr Allergy Immunol 2002, 12, 1-9.
2 Martinez FD, Helms PJ. Types of asthma and wheezing. Eur Respir J 1998, 12, Suppl 27, 3s - 8s.
3 Frank PI, Morris JA, Hazell ML, Linehan MF, Frank TL. Long term prognosis in preschool children with wheeze: longitudinal postal questionnaire stuy 1993-2004. B Med J 24 June 2008 336(7658):1423-6. Epub 2008 Jun 16.
4 Singleton RJ, Redding GJ, Lewis TC, Martinez P, Bulkow L, Morray B, Peters H, Gove J, Jones C, Stamey D, Talkington DF, DeMain J, Bernert JT, Butler JC. Sequelae of severe respiratory syncytial virus infection in infancy and early childhood among Alaska Native children. Pediatrics 2003, 112, 285-290.
5 Eder W, Ege MJ, von Mutius E. The asthma epidemic. N Engl J Med 2006, 355, 2226-35.
6 Whu R, Cirilo G, Wong J, Finkel ML, Mendez HA, Leggiadro RJ. Risk factors for pediatric asthma in the South bronx. J Asthma. 2007, 44, 855-9.
7 Kuiper S, Muris JW, Dompeling E, Kester ADM, Wesseling G,Knottnerus JA, et al. Interactive effect of family history and environmental factors on respiratory tract-related morbidity in infancy. J Allergy Clin Immunol 2007, 120, 388-95.
8 Maritz GS, Woolward KM, Du Toit G. Maternal nicotine exposure during pregnancy and development of emphysema-like damage in the offspring. S Afr Med J 1993, 83, 195-198.
9 Smith J. An update on bronchopulmonary dysplasia: is there a relationship to the development of childhood asthma? Med Hypotheses 2003, 61, 495-502.
10 Sigurs N, Bjarnason R, Sigurbergsson F, Kjellman B. Respiratory syncytial virus bronchiolitis in infancy is an important risk factor for asthma and allergy at age 7. Am J Respir Crit Care Med 2000, 161, 1501-7.
11 Stein RT, Sherrill D, Morgan WJ, Holberg CJ, Halonen M, Taussig LM, Wright AL, Martinez FD. Respiratory syncytial virus in early life and risk of wheeze and allergy by age 13 years. Lancet 1999, 354, 541-545.
12 Roman M, Calhoun WJ, Hinton KL, Avendano LF, Simon V, Escobar AM, Gaggero A, Diaz PV. Respiratory syncytial virus infection in infants is associated with predominant Th-2 like

Respiratory Therapy Vol. 5 No. 1 n February-March 2010 57
response. Am J Respir Crit Care Med 1997, 156, 190-5. 13 Bush A, Thomson AH. Acute bronchiolitis. Br Med J 2007,
335, 1037-41. 14 Weiss ST, Tosteston TD, Segal MR, Tager IB, Redline S,
Speizer FE. Effects of asthma on pulmonary function in children. A longitudinal populationbased study. Am Rev Respir Dis 1992, 145, 58-64.
15 Govaere E, Van Gysel D, Massa G, Verhamme KMC, Doli E, De Baets F. The influence of age and gender on sensitization to aero-allergens. Pediatr Allergy Immunol 2007, 18, 671-8.
16 Stern DA, Morgan WJ, Wright AL, Guerra S, Martinez FD. Poor airway function in early infancy and lung function by age 22 years: a non-selective longitudinal cohort study. Lancet 2007, 370, 758-64.
17 Jones CA, Holloway JA, Warner JO. Fetal immune responsiveness and routes of allergic sensitization. Pediatr Allergy Immunol 2002, 13 Suppl 15, 19-22
18 Allam JP, Zivanovic O, Berg C, Gembruch U, Bieber T, Novak N. In search for predictive factors for atopy in human cord blood. Allergy, 2005, 60, 743-50.
19 Wahn U, Bergmann R, Kulig M, Forster J, Bauer CP. The natural course of sensitisation and atopic disease in infancy and childhood. Pediatr Allergy Immunol 1997, 8, Suppl 10, 16-20.
20 Tovey ER, Almqvist C, Li Q, Crisafulli D, Marks GB. Nonlinear relationship of mite allergen exposure to mite sensitization and asthma in a birth cohort. J Allergy Clin Immunol 2008, 122, 114-118.
21 Sporik R, Holgate ST, Platts-Miles TAE, Cogswell JJ. Exposure to housedust mite allergen (Der p I) and the development of asthma in childhood. N Engl J Med 1990, 323, 502-507.
22 Strachan DP, Butland BK, Anderson HR. Incidence and prognosis of asthma and wheezing illness from early childhood to age 33 in a national British cohort. Br Med J 1996, 312, 1195-1199.
23 Martinez FD, Wright AL, Taussig LM, Holberg CJ, Halonen M, Morgan WJ, and the Group Health Medical Associates. Asthma and wheezing in the first six years of life. N Engl J Med 1995, 332, 133-138.
24 Sigurs N, Bjarnason R, Sigurbergsson F, Kjellman B, Björksten B. Asthma and immunoglobulin E antibodies after respiratory syncytial virus bronchiolitis: a prospective cohort study with matched controls. Pediatrics 1995, 95, 500-505.
25 Castro-Rodriguez JA, Holberg CJ, Wright AL, Martinez FD. A clinical index to define risk of asthma in young children with recurrent wheezing. Am J Respir Crit Care Med 2000: 162: 1403-1406.
26 Csonka P, Kaila M, Laippala P, Kuusela A-L, Ashorn P. Wheezing in early life and asthma at school age: Predictors of symptom persistence. Pediatr Allergy Immunol 2000: 11: 225-229.
27 Holt PG, McMinamin C, Nelson D. Primary sensitisation to inhalant allergens during infancy. Pediatr Allergy Immunol 1990, 1, 3-13.
28 Macaubas C, de Klerk NH, Holt BJ, Wee C, Kendall G, Firth M, et al. Association between antenatal cytokine production and the development of atopy and asthma at age 6 years. Lancet 2003, 362, 1192-1197.
29 Stern DA, Guerra S, Halonen M, Wright AL, Martinez FD. Low IFN-g production in the first year of life as a predictor of wheeze during childhood. J Allergy Clin Immunol 2007, 120, 835-841.
30 Guerra S, Lohman IC, Halonen M, Martinez FD, Wright AL
> Reduced interferon gamma production and soluble CD14 levels in early life predict recurrent wheezing by 1 year of age. Am J Respir Crit Care Med 2004, 169, 70-76.
31 Björksten B, Borres MP, Einarsson R. Interleukin-4, soluble CD23 and interferon-gamma levels in serum during the first 18 months of life. Int Arch Allergy Immunol 1995, 107, 34-36.
32 Hagendorens MM, Ebo DG, Schuerwegh AJ, Huybrechs A, Van Bever HP, Bridts CH, De Clerck LS, Stevens WJ. Differences in circulating dendritic cell subtypes in cord blood and peripheral blood of healthy and allergic children. Clin Exp Allergy 2003, 33, 633-9.
33 Rothenbacher D, Weyermann M, Fantuzzi G, Brenner H. Adipokines in cord blood and risk of wheezing disorders within the first two years of life. Clin Exp Allergy 2007, 37, 1143-9.
VISIT WWW.RESPIRATORYTHERAPY.CARespiratory Therapy, The Journal of Pulmonary Technique, can now beaccessed on line. The site features everything you’ll find in our journal,and more.
Visitors to Respiratory Therapy’s official website can see informativevideos of new products, read the current issue of the journal on line,select and review all our previous issues in the Respiratory Therapyarchives, and catch up on the latest in respiratory therapy by viewingthe day’s updated news. The site also features information about articlesubmission guidelines, subscriptions, advertising, and opportunities foreditorial participation.
The website, like the journal, offers clinical studies, product reviews,news, facility reports, commentaries, and special sections about thecurrent trends in respiratory care.
Respiratory Therapy’s website, www.respiratorytherapy.ca, is publishedon line by Respiratory Therapy, The Journal of Pulmonary Technique,Goldstein & Associates, Inc., 10940 Wilshire Boulevard, Suite 600, LosAngeles, California 90024. For inquiries please contact us [email protected] or see the website.

58 Respiratory Therapy Vol. 5 No. 1 n February-March 2010
In April 2009, the Mexican Ministry of Health reported an increase in severe pneumonia cases in young adults.1 The 2009 swine-origin influenza A (H1N1) virus was identified as its cause and rapidly led to a worldwide pandemic.2 This pandemic began in the northern hemisphere during late spring and early summer and appeared to decrease in intensity within a few weeks.3 Shortly after, at the start of the southern hemisphere winter, it spread to Australia and New Zealand, causing an approximately 8-fold greater number of confirmed cases per head of population than in the United States.4-5
The spread of the virus to Australia and New Zealand was also associated with a large number of patients admitted to intensive care units (ICUs) across both countries.6 A proportion of these patients presented with, or developed, severe acute respiratory distress syndrome (ARDS). In some severe cases, extracorporeal membrane oxygenation (ECMO) was commenced for the treatment of refractory hypoxemia, hypercapnia, or both, which occurred despite mechanical ventilation and rescue ARDS therapies.7
A recent multicenter study published in the Journal of the American Medical Association (JAMA) by Dr Davies et al reported on the incidence, clinical features, severity of respiratory failure, technical characteristics, duration of extracorporeal support, complications, and most importantly survival in patients with severe influenza-related ARDS who were treated with ECMO. In addition, the authors discussed the relevance of their findings to the potential ECMO case load in northern hemisphere countries during the 2009-2010 winter.7
Dr Davies et al contacted all 187 ICUs in Australia and New Zealand and identified the 15 specialty centers which had ICUs that provided ECMO support during that period. All patients who received ECMO for severe ARDS during the 2009 influenza A (H1N1) winter pandemic in Australia and New Zealand were then identified. Davies et al studied adult and pediatric patients who were treated with ECMO between June 1 and August 31, 2009. Neonates and patients treated with ECMO for primary cardiac failure, following heart and/or lung transplantation or cardiac surgery were excluded from the study.7
Sixty-eight patients with severe influenza-associated ARDS were treated with ECMO, of whom 61 had either confirmed 2009 influenza A (H1N1) or influenza A not subtyped, representing an incidence rate of 2.6 ECMO cases per million population. An additional 133 patients with influenza A received mechanical ventilation but no ECMO in the same ICUs. The 68 patients who received ECMO had a median age of 34.4 (26.6-43.1) years and 34 patients (50%) were men. Before ECMO, patients had severe respiratory failure despite advanced mechanical ventilatory support with a median PaO2/fraction of inspired oxygen ratio of 56 (48-63), positive end-expiratory pressure of 18 (15-20) cm H2O, and an acute lung injury score of 3.8 (3.5-4.0). The median duration of ECMO support was 10 (7-15) days. At the time of reporting, 48 of the 68 patients (71%), had survived to ICU discharge, of whom 32 had survived to hospital discharge and 16 remained as hospital inpatients. Fourteen patients (21%) had died and 6 remained in the ICU, 2 of whom were still receiving ECMO.7
This is likely the first multicenter study on the use of ECMO for 2009 influenza A (H1N1)-associated ARDS. Affected patients were often young adults, pregnant or postpartum, obese, had severe respiratory failure before ECMO, and received prolonged mechanical ventilation and ECMO support. Children and elderly persons were infrequently treated with ECMO. Despite the disease severity and the intensity of treatment, the mortality rate was low at the end of the study period (21%).7
Publications from an international ECMO registry8 and from centers experienced in the use of ECMO for ARDS of heterogeneous etiology have reported mortality rates between 30% and 48%. The patients in this study had a mortality rate of only 21%, however, several patients still remained in the ICU at the time of reporting.7
According to the authors, several factors may have contributed to the observed mortality rate in this study. First, the patients were young and had ARDS secondary to viral pneumonia, which when managed with ECMO has been associated with higher survival rates than other causes of ARDS. Second, improvements in ECMO technology and staff training have occurred since previous publications, leading to safer and more effective ECMO application.7
The authors suggest that their findings may have implications for policy makers and clinicians. With a similar incidence of ECMO use for 2009 influenza A (H1N1)-associated ARDS, rough estimates are that the United States and the European Union might expect to provide ECMO to approximately 800 and 1,300 patients during this winter, and the information provided by this study may help facilitate future healthcare planning, resource utilization, and the clinical management of patients with influenza A (H1N1).
Reference1 World Health Organization. Influenza-like illness in the United
States and Mexico. http://www.who.int/csr/don/2009_04_24/en/index.html.
2 Dawood FS, Jain S, Finelli L; et al, Novel Swine-Origin Influenza A (H1N1) Virus Investigation Team. Emergence of a novel swine-origin influenza A (H1N1) virus in humans. N Engl J Med. 2009;360(25):2605-2615.
3 Perez-Padilla R, de la Rosa-Zamboni D, Ponce de Leon S; et al, INER Working Group on Influenza. Pneumonia and respiratory failure from swine-origin influenza A (H1N1) in Mexico. N Engl J Med. 2009;361(7):680-689.
4 Worldwide H1N1 (Swine Flu) Infection Data. http://www.flucount.org/.
5 Webb SAR, Seppelt IM, ANZIC Influenza Investigators. Pandemic H1N1 2009 influenza (“swine flu”) in Australian and New Zealand intensive care. Crit Care Resusc. 2009;11(3):170-172.
6 Australian Department of Health and Ageing. Pandemic (H1N1) 2009 update bulletins. http://www.healthemergency.gov.au/internet/healthemergency/publishing.nsf/Content/bulletins-13-19-july09. Accessed September 10, 2009.
7 Davies AR, et al. Extracorporeal Membrane Oxygenation for 2009 Influenza A (H1N1) Acute Respiratory Distress Syndrome. JAMA. 2009;302(17).
8 Conrad SA, Rycus PT, Dalton H. Extracorporeal Life Support Registry Report 2004. ASAIO J. 2005;51(1):4-10.
Preparing for the Pandemic: ECMO for Management of H1N1 Acute RDS Jeff Borrink, BS, RRT
Jeff Borrink is Clinical Application Specialist, Hamilton Medical. This article
is from the company’s newsletter.

www.smiths-medical.com800-558-2345Smiths Medical, part of the global technology business Smiths GroupBCI, SPECTRO2 and the Smiths Medical design mark are trademarks of the Smiths Medical family of companies. All other names and marks mentioned are the trade names, trademarks or service marks of their respective owners. © 2009 Smiths Medical family of companies. All Rights Reserved.
Choose the pulse oximetry solution that’s right for you.SPECTRO™
2 provides your choice of pulse oximeters and offers an array of features and optional accessories that enable you to customize the device to meet your specifi c needs.
Featuring proven BCI® technology, the SPECTRO™2 Series delivers
accurate and reliable readings on a wide range of patients – even in low perfusion or motion conditions.
Get more on the new SPECTRO™2 Series at:
www.smiths-medical.com/bci
Designed with you in mind

Tel: 866.246.6990 Intl: 919.544.8000 www.teleflexmedical.com
Osmo is a trademark of Teleflex Incorporated or its affiliates. Patent pending. ©2009 Teleflex Incorporated 2009-0120 Rev.00
OSMO: Maintenance Free Water Removal
Breathing circuit management takes time away from what really matters, the patient.
Introducing OSMO™, a universal solution that allows for maintenance-free water removal
from the expiratory limb during mechanical ventilation. An innovative approach to reducing
circuit condensation, OSMO allows you to provide optimal humidification without
significant clinician intervention.
To put it simply, OSMO manages condensate… so you don’t have to.
Visit teleflexmedical.com
to learn more