the hiv/aids pandemic: a human rights and health barometer of our times timothy h. holtz, md, mph...
TRANSCRIPT


The HIV/AIDS Pandemic:a Human Rights and Health
Barometer of Our Times
Timothy H. Holtz, MD, MPH
MEDI 645: Human Rights, Social Medicine, and the Physician
Emory School of Medicine
March 14, 2005

We will cover…
HIV/AIDS pandemic
Human rights violations and HIV/AIDS
Human rights approaches to HIV/AIDS
Current global response
Community actions

00002-E-4 – 1 December 2002
“The full realization of human rights and fundamental freedoms for all is an essential element in a global response to the HIV/AIDS pandemic, including in the areas of prevention, care, support and treatment, and that it reduces vulnerability to HIV/AIDS and prevents stigma and related discrimination against people living with or at risk of HIV/AIDS."
00002-E-5 – 1 December 2002
The HIV epidemic has been accompanied by a parallel epidemic
of fear, stigma and discrimination.
Therefore…any modern dialogue about HIV prevention or care
requires also a discussion of human rights and how to protect
them.
AIDS pandemic

Adults and children estimated to be living Adults and children estimated to be living with HIV as of end 2003with HIV as of end 2003
Total: 37.8 (34.6 – 42.3) million 4.8 million new infections annually
Western Europe580 000580 000
[460 000 – 730 000][460 000 – 730 000]
North Africa & Middle East480 000480 000
[200 000 – 1.4 million][200 000 – 1.4 million]
Sub-Saharan Africa25.0 million25.0 million
[23.1 – 27.9 million][23.1 – 27.9 million]
Eastern Europe & Central Asia1.3 million 1.3 million [860 000 – [860 000 – 1.9 million]1.9 million]
South & South-East Asia
6.5 million6.5 million[4.1 – 9.6 million][4.1 – 9.6 million]
Oceania32 00032 000
[21 000 – 46 000][21 000 – 46 000]
North America1.0 million1.0 million
[520 000 – 1.6 million][520 000 – 1.6 million]
Caribbean430 000430 000
[270 000 – 760 000][270 000 – 760 000]
Latin America1.6 million1.6 million
[1.2 – 2.1 million][1.2 – 2.1 million]
East Asia900 000900 000
[450 000 – 1.5 million][450 000 – 1.5 million]

Estimated adult and child deaths Estimated adult and child deaths from AIDS during 2003from AIDS during 2003
Total: 2.9 (2.6 – 3.3) million
Western Europe6 0006 000[<8 000][<8 000]
North Africa & Middle East24 00024 000
[9 900 – 62 000][9 900 – 62 000]
Sub-Saharan Africa2.2 million2.2 million
[2.0 – 2.5 million][2.0 – 2.5 million]
Eastern Europe & Central Asia49 00049 000[32 000 – 71 000][32 000 – 71 000] East Asia
44 00044 000[22 000 – 75 000][22 000 – 75 000]South
& South-East Asia460 000460 000[290 000 – 700 000][290 000 – 700 000]
Oceania700700
[<1 300][<1 300]
North America 16 00016 000
[8 300 – 25 000][8 300 – 25 000]
Caribbean35 00035 000
[23 000 – 59 000][23 000 – 59 000]
Latin America84 00084 000
[65 000 – 110 000][65 000 – 110 000]

About 14,000 new HIV infections per day in 2003
More than 95% are in low and middle income
countries
Almost 2,000 are in children under 15 years of age
About 6,000 are in persons aged 15 to 24 years
Almost 50% of all new infections are in women

Women are heavily impacted…

Percent of Pregnant Women 15-24 Years Old who are HIV-Infected, 2000-3
0 5 10 15 20 25 30 35
AFRICABotswana
South AfricaZambia
NamibiaKenya
MozambiqueEthiopiaUgandaNigeria
TanzaniaCote d'Ivoire
RwandaCARIBBEAN
HaitiGuyana
Percent HIV-infected

HIV prevalence among pregnant women in South Africa, 1990 to 1999
Source: Department of Health, South Africa
0.71.7 2.1
4
7.6
10.4
14.2
17
22.8 22.4
0
5
10
15
20
25
90 91 92 93 94 95 96 97 98 99
HIV
pre
vale
nc
e (%
)
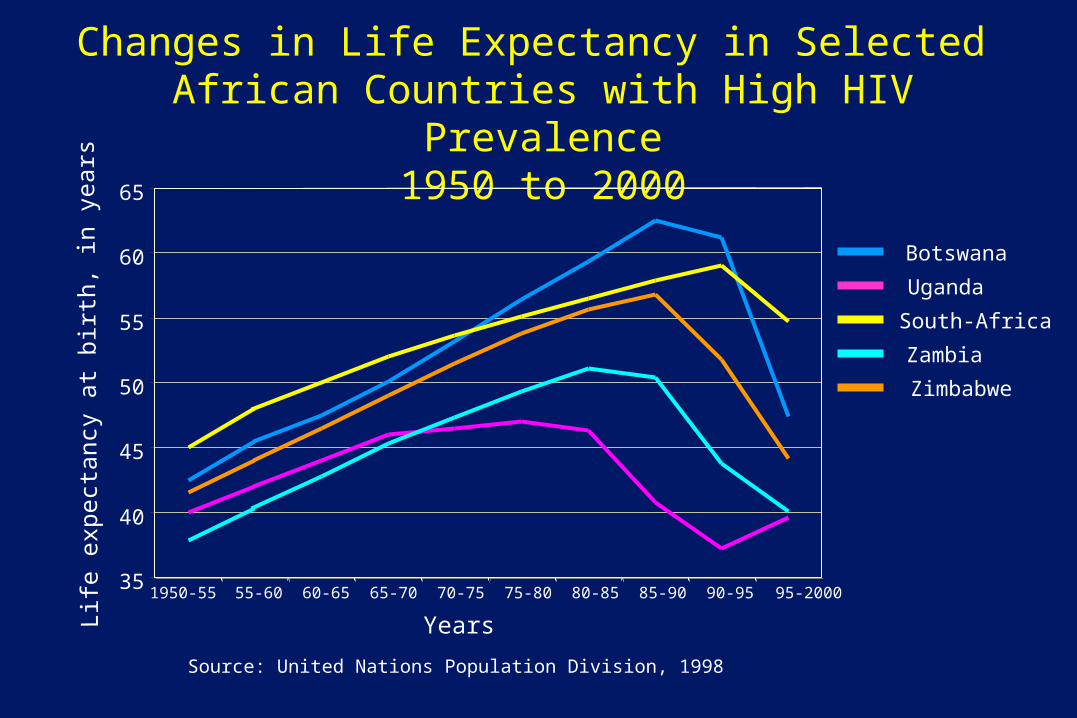
Changes in Life Expectancy in Selected African Countries with High HIV Prevalence
1950 to 2000
Source: United Nations Population Division, 1998
35
40
45
50
55
60
65
1950-55 55-60 60-65 65-70 70-75 75-80 80-85 85-90 90-95 95-2000
Life
expect
ancy
at
bir
th,
in y
ears
Botswana
Uganda
South-Africa
Zambia
Zimbabwe
Years

United States: Invisible Epidemic?

Estimated Incidence of AIDS, Deaths, Prevalence by Year of Diagnosis/Death
US, 1981 – 2002
*Adjusted for reporting delays
81 83 15 87 89 91 93 95 97 9982 84 86 88 90 92 94 96 98 00 01 02
IncidenceDeathsPrevalence
1993 definitionimplementation
Nu
mb
er
of C
ase
s/D
eath
s(T
hou
san
ds) P
revalence
(Th
ousan
ds)
Year
0
10
20
30
40
50
60
70
80
90
0
50
100
150
200
250
300
350
400

0
10
20
30
40
50
60
70
Pe
rce
nt o
f Cas
es
Year of Report
Proportion of AIDS Cases, by Race/Ethnicity and Year of Report, 1985 – 2002, US
White, not Hispanic
Black, not Hispanic
Hispanic
Asian/Pacific Islander American Indian/Alaska Native
85 86 87 88 89 90 91 92 93 94 95 96 97 98 99 00 01 02
HIV/AIDS in African Americans
African Americans are only 13% of US population but are half of the new AIDS cases and AIDS deaths in 2002
By the end of 2002, more than 185,000 African Americans had died with AIDS
Poorest survival rates of all racial and ethnic groups – late diagnosis – poor access HIV therapy

Leading Causes of Death Among Black Americans, 25- to 44-Years-Old,
United States, 2001*
0 500 1000 1500 2000 2500 3000 3500 4000 4500
Cancer
HIV infection
Diabetes mellitus
Unintentional injury
Homicide
Heart disease
Nephritis, nephrosis & nephrotic syndrome
SuicideCerebrovascular disease
Chronic liver disease10
123456789
* Preliminary death-certificate data for 2001
Deaths

Majority of people with HIV/AIDS have no access to treatment….

The widening treatment gap
Source: Adapted from WHO/UNAIDS Statistics, & HIV/AIDS Surveillance in Europe, End- year report 2001, No. 66, CESES
0.0
0.5
1.0
1.5
2.0
2.5
1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001Yearl
y d
eath
s as
a p
roport
ion o
f 1
99
5 v
alu
es
HAARTHAART
AIDS deaths in Africa
AIDS deaths in Western Europe

00002-E-21 – 1 December 2002
Commonly heard arguments against using ARVs in the resource poor settings…
Unsustainable
Inappropriate technology
Not cost effective
Not a priority in light of other demands
Too difficult to administer
Prevention is more important
Too expensive
Drug resistance
Corruption, thievery and sale
Stigma

00002-E-22 – 1 December 2002
What does human rights have to do with HIV/AIDS?
Human rights are inextricably linked with the spread and impact of HIV/AIDS on individuals and communities around the world.
A lack of respect for human rights fuels the spread and exacerbates the impact of the disease.
This link is apparent in the disproportionate incidence and spread of the disease among certain groups which include women and children, and particularly those living in poverty.
It is also apparent in the fact that the overwhelming burden of the epidemic today is borne by developing countries, where the disease threatens to reverse vital achievements in human development.
AIDS and poverty are now mutually reinforcing negative forces in many developing countries.

00002-E-23 – 1 December 2002
The major reasons why human rights violations increase the risk of HIV/AIDS
Increased vulnerability: Certain groups are more vulnerable to contracting the HIV virus because they are unable to achieve their civil and political, and economic, social and cultural rights. Women, and particularly young women, are more vulnerable to infection if they lack of access to information, education and services necessary to ensure sexual and reproductive health and prevention of infection. People living in poverty often are unable to access HIV care and treatment, including antiretrovirals and other medications for opportunistic infections.

00002-E-24 – 1 December 2002
The major reasons why human rights violations increase the risk of HIV/AIDS
Discrimination and stigma: The rights of people living with HIV/AIDS often are violated because of their presumed or known HIV status, causing them to suffer both the burden of the disease and the consequential loss of other rights.
Stigmatization and discrimination may obstruct their access to treatment and may affect their employment, housing and other rights. The result is that those most needing information, education and counselling will not benefit even where such services are available.
Impedes an effective response: Effective HIV prevention, treatment, support and care strategies are hampered in an environment where human rights are not respected.

00002-E-25 – 1 December 2002
A human rights approach to HIV/AIDS I
There is clear evidence that where individuals and communities
are able to realize their rights – to education, free association,
information and, most importantly, non-discrimination - the
personal and societal impact of HIV and AIDS are reduced.
The protection and promotion of human rights are therefore
essential to preventing the spread of HIV and to mitigating the
social and economic impact of the pandemic.

00002-E-26 – 1 December 2002
A human rights approach to HIV/AIDS II
The promotion and protection of human rights reduces vulnerability
to HIV infection by addressing its root causes; lessens the adverse
impact on those infected and affected by HIV ; and empowers
individuals and communities to respond to the pandemic.
An effective international response to the pandemic therefore must
be grounded in respect for all civil, cultural, economic, political, and
social rights as well as the right to development, in accordance with
international human rights principles, norms and standards.

00002-E-27 – 1 December 2002
States’ obligations to promote and protect HIV/AIDS-related human
rights are defined in existing international treaties.
The United Nations human rights instruments and mechanisms
provide the normative legal framework as well as the necessary
tools for ensuring the implementation of HIV-related rights.
A human rights approach to HIV/AIDS III

00002-E-28 – 1 December 2002
HIV/AIDS-related human rights include the right to life; the right to liberty and security of the person; the right to the highest attainable standard of mental and physical health; the right to non-discrimination, equal protection and equality before the law; the right to freedom of movement; the right to seek and enjoy asylum; the right to privacy; the right to freedom of expression and opinion and the right to freely receive and impart information; the right to freedom of association; the right to marry and found a family; the right to work; the right to equal access to education; the right to an adequate standard of living; the right to social security, assistance and welfare; the right to share in scientific advancement and its benefits; the right to participate in public and cultural life; the right to be free from torture and other cruel, inhuman or degrading treatment or punishment.
A human rights approach to HIV/AIDS IV

00002-E-29 – 1 December 2002
Jonathan M. Mann, MD, MPH1947-1998
“Most people who decide to become doctors respond to a deep intuition about life and their own lives. To become a doctor implicitly places us on the side of those who believe that the world can change--that the chains of pain and suffering in the world can be broken....Thus, at a profound, even instinctual level... people become physicians to find a way to say “no” to disease and pain, and to hopelessness and despair--in short, to place themselves squarely on the side of those who intervene in the present to change the future.The physician agrees to...stand by the patient regardless of what happens--through their suffering, and even to the edge of life itself. The physician steadfastly remains with the patient even when the only thing the physician can offer is the fact of his or her presence. This is as relevant to public health as for individual patient care. Public health must engage in difficult issues even when no cure or effective instruments are yet available and public health physicians also must remain with, and not abandon, vulnerable populations”.
July 1996

00002-E-30 – 1 December 2002
Global response has had devastating consequences:
Some advances but many
delays over last 20 years….
Insert favorite golfer here…

What have we been waiting for?
Why have we failed to stop the HIV/AIDS epidemic?An outbreak of “-isms” and a lack of human rights…
Racism, prejudice and discrimination
Sexism--lack of womens rights
Beliefs regarding drug use
World Poverty– Debt– Greed– Corruption– Economic colonialism– Structural adjustment/health
sector reform– Insufficient development aid
Military industrial complex/war
Complex biology
Individual vs. Community rights
Religion
Pharmaceutical industry
Ignorance--lack of education
Values regarding sex and commercial sex work
Fear of Death
Public health obstacles
Tribalism
Nationalism

Lack of women’s rights
HIV/AIDS epidemic has highlighted the lack of basic
rights for women
discriminationeconomic oppressionlegal oppressiondenial of equal opportunity to education
domestic violencerape

Religion
Religious views have sometimes been an obstacle to
confronting the epidemic
Same sex relations
Sex before marriage
Condom use vs. abstinence
Sexism/gender oppression
Science vs. religious dogma

World poverty…

HIV/AIDS and Poverty
Low economic status is a predictor of increased mortality from HIV
disease even after controlling for confounders such as age, disease
stage, and access to care
Economics influence risk of infection and the spread of HIV
– Urban centers
– Trade routes
– Commercial sex workers
– Migrant workers

Low income is associated with greater risk of HIV infection
A greater exposure to higher risk sexual experiences
Diminished access to health information
Higher frequency of sexually transmitted infections
Absent or delayed diagnosis
Less concern about one’s health and the future given harshness
of present
World Poverty/structural violence
6 billion people– 2 billion have no power– 2 billion live on less than 1$ a day– 1.5 billion lack access to safe water– 125 million children have no school– 28 million disease-related deaths per year
Increasing inequality
Vast majority of people with HIV are living in
“resource-poor” countries

The share of the world’s wealth among the poor is diminishing…
0
0.5
1
1.5
2
2.5
1960 1991 1997
Percentage of global income of world’s poorest 20%
%

Obscene economic disparity:1990’s “Decade of Despair”
United Nations Development Programme’s 2003 Human
Development Report – 54 countries becoming even poorer than before.
– Life expectancy has fallen in 34 nations
The income of the richest 10% of the US population is now equal to
that of the poorest 43% of the world
In Brazil less than 3% of the population own two-thirds of the
country’s arable land

Debt Servicing=AIDS Program Costs
Source: UNAIDS, 2001, World Bank "Financial Impact of the HIPC Initiative: first 22 country cases." 1st March 2001. Figures do not include related costs of infrastructure, capacity building, and impact mitigation.
Economic Solution?
New global economic system that is grounded in human
rights and environmental justice
Debt cancellation would be part of the new level playing
field

HIV/AIDS assistance: are we doing enough?
Very slow out of the blocks…
Fewer than one in five persons at risk for HIV infection has access to even the most basic services; standard services could prevent 29 million infections by 2010
2001 established Global Fund
2002 1.2 billion dollars spent on HIV/AIDS
2003 WHO 3x5 initiative
2004 President’s AIDS Initiative

35
21
26
46
12
7
4
117
57
103
69
7
19
17
14.8
7.8
1.5
15.0
14.0
2.0
21.5
14.9
15.2
2.1
26.3
147.3
5.2
12.2
150.0 100.0 50.0 0.0 50.0 100.0 150.0
AustraliaAustralia
BelgiumBelgium
CanadaCanada
DenmarkDenmark
FinlandFinland
GermanyGermany
JapanJapan
LuxembourgLuxembourg
NetherlandsNetherlands
NorwayNorway
SwedenSweden
SwitzerlandSwitzerland
UKUK
USAUSA
1998 HIV/AIDS ODA in US$ million HIV/AIDS ODA in US$ per US$ million 1998 GNP
HIV/AIDS ODA in 1998: HIV/AIDS ODA in 1998: Total amount obligated, in US$ million Total amount obligated, in US$ million
and per US$ million of donor country’s GNPand per US$ million of donor country’s GNP

HaitiHaiti
GuyanaGuyana
Côte d’IvoireCôte d’Ivoire
NigeriaNigeria
EthiopiaEthiopia
KenyaKenya
UgandaUganda
RwandaRwanda
TanzaniaTanzania
MozambiqueMozambique
ZambiaZambia
South AfricaSouth Africa
BotswanaBotswana
NamibiaNamibia
President’s Emergency Plan for AIDS Relief15 Focus Countries
VietnamVietnam

FY 2004 Budget for Global AIDS: $2.2 Billion
“Sense of Congress” for Distribution of Funds
Treatment** 55%
Palliative Care 15%
Prevention* 20%
Orphans and Vulnerable
Children 10%
*33% of prevention funds should be for abstinence-until-marriage programs**75% of treatment funds should be for purchase and distribution of ARVs
Source: Public Law 108-25Source: Public Law 108-25

1.61.7
3.41.8
1.10.45.20.5
0.94.72.05.41.61.00.30.19.20.50.32.3
12.9
United StatesItaly GreeceNew ZealandAustriaJapanPortugalAustraliaSpainGermanyCanadaBritainSwitzerlandFinlandFranceIrelandBelgiumSwedenNetherlandsNorwayDenmark0.0
0.2
0.4
0.6
0.8
1.0
As % of GDP
Billion US$
Net Official Aid (Billion US$) by rich country donors to poor countries
Goal is 0.7% of GNP

Military Industrial Complex
"Every gun that is made, every warship
launched, every rocket fired, signifies in
the final sense a theft from those who
hunger and are not fed, those who are
cold and are not clothed."
President Dwight D. Eisenhower
April 16, 1953

Military spending

Big Pharma and HIV/AIDS
Issues surrounding access to treatment have called into question
profit motive and corporate responsibility– Used enormous resources and clout to fight access to
treatment/use of generics– Profit motive vs. humanitarian or human rights concerns– 500 million drug development costs
• What about Government contribution to ARV development costs?
NGO/activists and developing country producers have won the first
round– WTO/TRIPS?

Competition is good for prices…


During the last 60 minutes…
571 people infected with HIV
342 deaths from AIDS
HIV/AIDS web counter/clock
Since the beginning of the epidemic….
25,000,000+ AIDS deaths

Not all bad news…

HIV prevalence rate among HIV prevalence rate among 13 to 19-year-olds, Masaka, Uganda, 1989 to 199713 to 19-year-olds, Masaka, Uganda, 1989 to 1997
0
1
2
3
4
5
1989/90 1990/91 1991/92 1992/93 1993/94 1994/95 1995/96 1996/97
girls
boys
Source: Kamali et al. AIDS 2000, 14: 427-434
HIV
pre
vale
nc
e (%
)

00002-E-57 – 1 December 2002
Côte d'Ivoire Minister of Health Gets Tested for HIV

00002-E-58 – 1 December 2002
Couple Counseling at Uganda Antenatal Clinic

00002-E-59 – 1 December 2002
HIV Testing Outreach, Botswana
00002-E-60 – 1 December 2002
Youth Center, Kenya

00002-E-61 – 1 December 2002
Radio Serial Drama for Behavior Change, Botswana

Thai AIDS Clinic

Trend in HIV prevalence in 21 year old military Trend in HIV prevalence in 21 year old military conscripts in Thailandconscripts in Thailand
Source: Armed Forces Research Institute of Medical Sciences, Thailand
1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999
HIV
pre
vale
nc
e (%
)H
IV p
reva
len
ce
(%)
00
55

Activists and generic drugs force lower prices for treatment…
Annual cost per person for triple therapy in Africa (US$)
$12,000
$10,000
$8,000
$6,000
$4,000
$2,000
$01991 1993 1995 1997 1999 2001 2003
Drug Access Initiative
Domestic production
Accelerated access initiative
February-April 2001 offers

Positive lessons from AIDS Epidemic People are heroic and often exhibit unimaginable dignity Epidemic is not inexorable
– Prevention works • Uganda, Senegal, Thailand
Effective prevention and care efforts involve– Governments, communities, individuals
Prevention and care efforts must involve and reach out to the marginalized
Prevention and care work together Top down and bottom up are both needed

Top down
Global commitment to confront the epidemic
Government commitment—ensure prevention and care services
Establish basic treatment approach for everyone
Guarantee regular supply of medicines for everyone
Involve stakeholders in key decisions

Baby getting nevirapine to prevent mother-child HIV transmission, Uganda

Field officers, who carry drugs, forms, and supplies for specimen collection, visit each
patient weekly and can visit up to 10 patients per day.
Drug Distribution Network and Field-Based Monitoring, Uganda

Antiretroviral Treatment Program, Kibera Slums, Kenya

Clinical Training, Ethiopia

Bottom-up
Community must organize to demand rights from their
governments
Meaningfully involve people with HIV/AIDS
Broad coalitions/common grounds
Enlist allies in dominant countries
Work to re-define the paradigm so that it is people-centered and
has a focus on achieving equity as soon as possible

HIV, Health and Your Community: A Guide for Action

Community mobilization is essential….

Extra Slides


Information Gap
Rwanda 1992—no materials
Fewer than five percent of people infected with HIV live in
industrialized countries– Most information regarding HIV/AIDS is written for people in
these countries– More than 100,000 scientific articles on HIV and AIDS
• Most have little relevance for most people living with HIV • Little usefulness for most health care providers
Comprehensive guide to prevention is needed

Commercial sex work
Economic exchange of sex
interdiction approach
moral judgement
denial
hypocrisy (e.g., international sex tourism)

HIV/AIDS forces us to confront death
Tough deathDenial—HIV/AIDS is uniformly fatal
Irrational fear of contagion
Prolonged suffering without the basic medical care

Human rights vs. Public Health
Does human rights emphasis hamper public health efforts?
Human rights minimally conflict with public health restrictions as long as the objectives and processes used to make the decision to restrict the rights are clear
SIRACUSA (1985)– Proposed restriction has to provided for and in accordance with the law– Restriction must be directed toward a legitimate objective of general interest
(e.g., prevention of HIV transmission)– Restriction must be strictly necessary to achieve objective– No less intrusive means should be available to reach objective– Cannot be unreasonable or discriminatory—burden of proof falls on those who
want to restrict the rights and concrete public health evidence is needed to respond to questions regarding the last three criteria
Human rights should be used a criteria for public health success

Human rights and health issues
Article 25 of the Universal Declaration of Human Rights (1949):
“everyone has the right to a standard of living adequate for
the health of himself and his family including food, clothing,
housing, and medical care and necessary social services”
Article 12 of the International Covenant on Economic, Social and
Cultural Rights (US has not ratified)
“Right of everyone to the enjoyment of the highest attainable standard of physical and mental health”
Equity is a major issue
Liberation Theology and Health
Observe– Analysis
Judge– Structural violence
Act– Not just report one’s findings but struggle for the less
fortunate’s liberation (read survival)

Evolution of an epidemic
1986 1991 2001


Americans’ Perceptions of Urgent Health Problems of the World
49%
25% 24%
11% 9%4% 3% 2% 1%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
HIV/AIDS Cancer Hunger Health CareCosts/
Insurance
InfectiousDiseases/Disease inGeneral
Violence/ War
BiologicalTerrorism/Smallpox
West NileVirus
Malaria
Q2. What would you say is the most urgent health problem facing the world at the present time?
THE GALLUP ORGANIZATIONCopyright © 2002 The Gallup Organization, Princeton, NJ. All rights reserved.
Based on interviews with 800 adults Based on interviews with 800 adults ≥≥18 18 years old done in October and November years old done in October and November 20022002
Based on interviews with 800 adults Based on interviews with 800 adults ≥≥18 18 years old done in October and November years old done in October and November 20022002

AIDS is caused by HIV
Sexual transmission
Blood borne—transfusion, injection drug use
Perinatal--during and after birth

Massive HIV/AIDS case load
Impact on health care workers:
Increasing demand for care and support in health facilities and communities
Overburdened in-patient and out-patient services
Increased need for knowledge and skills on HIV/AIDS
Increased need for voluntary confidential counselling and HIV testing
Fear and discrimination Burn out

TB: Global Public Health Importance

Tuberculosis is a major global killer….
16–20 million people with active TB globally
11 million people are currently infected with TB and HIV
8 million new TB cases annually
2 million TB deaths annually (including TB-HIV)
TB is the biggest killer of people with HIV/AIDS
TB is the largest cause of death among womenof reproductive age

10 - 99
100 - 999
1000 - 4999
< 5
5 - 9.9
5000 or more
No estimate
Rate per 100 000
Estimated HIV-MTB co-infection prevalence, 2000
Source: Corbett EL, Watt CJ, Walker N, Maher D, Raviglione MC, Williams B, Dye C. (submitted for publication).

Africa: HIV is driving the TB Epidemic Africa: HIV is driving the TB Epidemic TB Notification Rates, 1980-1999TB Notification Rates, 1980-1999
World Health OrganizationWorld Health Organization
0
50
100
150
200
1980 1985 1990 1995 2000
250
300
350
400
450
500
Zimbabwe
Malawi
Tanzania
Côte d'Ivoire
Kenya
Years
Rat
e (x
100,
000)

0
10
20
30
40
50
60
70
Pe
rce
nt
of
Cas
es
MSM & IDU
Men who have sex with men (MSM)
Injection drug use (IDU)
Heterosexual contact
Year of Diagnosis
Estimated Adult/Adolescent AIDS Cases by Exposure Category and Year of Diagnosis,
1985 – 2002
85 86 87 88 89 90 91 92 93 94 95 96 97 98 99 00 01 02

Racism, prejudice and discrimination
There continues to be an outbreak of prejudice and discrimination…
In the United States….“Haitian disease”“GRID”Rock Hudson was a major breakthrough in US“Self-inflicted disease”“God’s wrath”Health care workers refused to work with people with HIV or who they thought had HIVKids not allowed to attend school—Ryan WhiteCurrent HIV epidemic among minorities
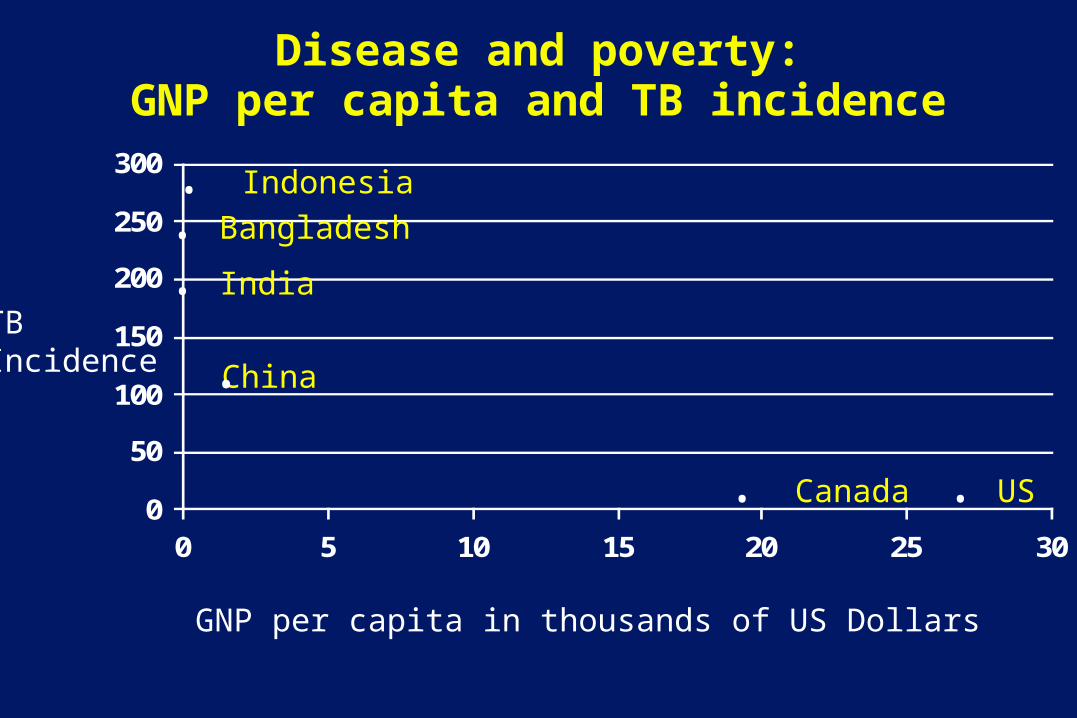
Disease and poverty:GNP per capita and TB incidence
0
50
100
150
200
250
300
0 5 10 15 20 25 30
TBIncidence
GNP per capita in thousands of US Dollars
. India
. Bangladesh
China.
. Indonesia
. Canada . US

Current WB/IMF debt relief programs are inadequate In 2002 Malawi received initial debt service cut of $28 million, or 30% per cent.
Money used for a 45% rise in total 2001 social expenditure
The breakdown of the $28 million for spending in the 2001 budget is: – $7.3 million more on critical drugs for hospitals and health centers – $2.7 million for extra staff and support in primary health centers – $1.1 million for training more nurses – $3.8 million for training new teachers – $6.1 million for repairs to schools and new teaching materials – $4.2 million for borehole construction and maintenance – $2.7 million for agriculture expansion
Source: Malawi's decision point document, 2000

Debt
In Zambia, where primary school rates are falling and one in five adults is HIV positive, has to find $176 million a year for debt repayments, compared to the $76 million currently spent on health and $70 million on education…….

Net official aid (billion US$) by rich country donors to poor countries
0.1 0.3 0.3 0.4 0.5 0.50.9 1 1.1
1.6 1.6 1.7 1.8 22.3
3.4
4.75.2 5.4
9.2
12.9
0
1
2
3
4
5
6
7
8
9
10
11
12
13
New Zealand
GreecePortugal
Ireland Austria Finland
Switzerland
AustraliaBelgium Spain
DenmarkNorwaySwedenCanada
Italy
Netherlands
BritainFranceGermany
Japan
United States
Aid in terms of billion US$

Comparison of Apparel Manufacturing Wages in 1998
By Kurt Salmon Associates
“Race to the Bottom” supported by World Bank / IMF policies
World Bank plans to loan $23 million for a new free trade zone in Haiti– The zone will build clothes factories for Tommy Hilfiger and
Levis– Haitian workers make 30 cents / hour– Mexican and Jamaican workers make 75-85 cents / hour– In July 2003, the management in Mexican factories that
produce Tommy Hilfiger and Levis products fired and assaulted union workers

Need for Holistic Public Health Perspective
Current focus on behavioral theory/interventions and biomedical
model– Improve individual “self-efficacy”– Provide treatment for individuals
Too little emphasis on changing global and societal structural
violence– Customs– Laws– Policies– Unfair economic system

World Economic System:
World Trade Organization– GATT, GATTS, TRIPS…etc.
Multi-lateral trade agreements– NAFTA, CAFTA, FTAA…..etc.
World Bank and IMF– US has veto power over WB and IMF– Structural adjustment programs control developing
country economies
Structural Adjustment Programs
Conditions for Structural Adjustment Loans
– Reduce govt. spending (cut health/education programs)– Devalue local currency (make exports cheaper for North)– Cut wages (become more “competitive”)– Change to export economy (e.g. grow coffee not corn)– Remove restrictions on foreign corps. (allow multinationals
to operate freely)– Privatize state companies (sell state resources to private
corps. - assisted thru devalued currency)Bello
International Forum on Globalization

Effects of Structural Adjustment Programs Diminished economic growth
– Latin America GNP: • Increased 73% 1960-80 • Increased only 7% 1980-02
Accruing interest has led to a cycle of dependency – Tremendous rising debt in the Global South
• 1980 was $609 billion / 2001 was $2.4 trillion– For example:
• Nigeria took $5B loan, has paid $16B, and owes $32B
International Forum on Globalization
Center for Economic Justice