the health technology assessment (hta) of cell … · the health technology assessment (hta) of...
TRANSCRIPT

The Health Technology Assessment (HTA) of Cell
Therapies
ISCT industry roundtable 1: transition of products from the payer
perspective, 02 October 2016, Memphis
Nick Crabb, Programme Director, Scientific Affairs

• Review of clinical and economic evidence leading to
recommendations on the appropriate use of new and existing
medicines for the NHS in England
• Includes cost utility analysis
– Outcomes (length and quality of life) and costs (full care pathway costs) are
compared to those for the current standard of care
– Outcomes measured in quality adjusted life years (QALY) – a metric that
combines the impact of the treatment on both length and quality of life
– Cost per QALY considered in decision making
• Perspective:
– National Health Services and Personal Social Services for costs
– Direct health effects on patients and carers for outcomes
• Mandatory funding of medicines recommended in TA
NICE Technology Appraisals (TA)

Exciting Times!
• Very strong pipelines of pharmaceuticals, biopharmaceuticals and
advanced therapy medicinal products with the potential for major
patient benefits
• Patients and healthcare systems need these products
• Challenges
– High costs
– Timely patient access while the evidence is still emerging

Initiatives impacting patient access to
medicines • Policy landscape evolving with several initiatives aiming to ensure
timely patient access to products addressing unmet medical need:
– Accelerated access review (England)
– Changes to the Cancer Drugs Fund (England)
– Early Access to Medicines Scheme (UK)
– EMA adaptive pathways (Europe)
– EMA PRIME (Europe)
• These initiatives mean that products are likely to come to NICE and
other HTA agencies sooner in their development cycle with less
evidence

Managing access to promising new
health technologies • A key challenge is to work with partner and stakeholder organisations to find
a way to provide patients with access to promising new medicines while the
evidence is still emerging, in a financially sustainable way
• Developments include:
– Wider use of managed access arrangements to achieve fair sharing of risks
across stakeholders
– Post marketing authorisation “real world” evidence collection to reduce
uncertainty with time
– Increased emphasis on “recommended with research” type recommendations in
HTA/Payer decision frameworks
– Innovative pricing and payment methods
• New Cancer Drugs Fund arrangements in England address these issues for
cancer medicines

Cancer Drugs Fund
• NICE and NHS England undertook a joint public consultation on
proposals for a new Cancer Drugs Fund operating model from
November 2015 – February 2016
• Cancer Drugs Fund has become a “managed access fund” to
enable patient access to cancer drugs which appear promising but
where NICE indicates that there is insufficient evidence to support a
recommendation for routine commissioning
• Details from https://www.england.nhs.uk/cancer/cdf/

NICE methods research related to early
evaluation and managed access • Collaborating on international research into optimised drug
development and adoption pathways
– HTA elements of EMA adaptive pathways pilots
– IMI ADAPT-SMART project
• Research to support NICE’s ability to assess products and
interventions where evidence is limited
– use of real world evidence (IMI GetReal project)
– expert elicitation
• Research to support the analysis and presentation of uncertainty
and how managed access arrangements impact uncertainty
Engagement Opportunities • NICE Scientific Advice
– Dedicated team of 16 staff
– Advice on HTA aspects of prospective clinical trials
– Pharma, biotech, ATMPs and medical technologies
– Advice in collaboration with UK and European regulators and other European
HTA agencies
– Educational seminars
• NICE Office for Market Access
– New initiative – opened in October 2015
– Allows engagement on all dimensions of patient and market access
– High interest in managed access arrangements, including innovative pricing
methods
– Multi-stakeholder “safe harbour” discussions

NICE regenerative medicine study
• Study undertaken by NICE in collaboration with the Centre for
Reviews and Dissemination / Centre for Health Economics,
University of York
• Exercise prompted by a recommendation from the Department of
Health Regenerative Medicine Expert Group
• Study allowed detailed consideration of any specific challenges
associated with the evaluation of ATMPs including the interplay
between evidence maturity, price and payment methods
• Reports available from https://www.nice.org.uk/about/what-we-
do/science-policy-research/nice-research

Study design
• Much of the study concerned a hypothetical example product with
characteristics based on early clinical data for related real products
supplemented with hypothetical evidence
• Multiple scenarios were developed which were considered by an
Expert Panel experienced in NICE TA who were asked what
decisions they would make if the scenarios were encountered in real
appraisals
• Also included a broad exploration of the applicability of NICE TA
methods to regenerative medicines
• Supported by a Project Advisory Group

Hypothetical example product • CAR (chimeric antigen receptor) T-cell therapy specific to antigen CD19, for
treating relapsed or refractory B-cell acute lymphoblastic leukaemia (B-ALL) in
children and young adults
• Based on the available clinical evidence, two target product profiles (TPPs)
were developed,
– CAR T-cell therapy used “as a bridge” to hematopoietic stem cell transplantation (HSCT)
– CAR T-cell therapy used with “curative intent”
• To explore the impact of different levels of evidence, three hypothetical evidence
sets were constructed for each TPP (minimum, intermediate, mature) providing
six evidence scenarios
• Within each of the six evidence sets, cost effectiveness analyses explored the
impact of price discounts, payment models and discounting rates used in the
economic analyses

Hypothetical acquisition costs
• No commercially available product or published price
• Hypothetical price set such that economic analyses would give a
result close to NICE’s cost effectiveness threshold
• NICE “end of life” criteria considered applicable where a QALY
weighting equivalent to an appraisal threshold of £50,000 per QALY
applies
Note – end of life criteria will not apply to all regenerative medicines –
normally a cost per QALY under £20,000 - £30,000 would be required for a
product to be considered cost effective

Benefits and costs of the two TPPs
Bridge to HSCT TPP
Curative Intent TPP
Assumed Individual
patient level Incremental
QALY gain
7.46 10.07
Assumed Price
(acquisition cost of the
therapy)
£356,100 £528,600

Analysis and presentation of uncertainty • The product characteristics in the TTPs represent the potential for profound
patient benefits but there is also very high uncertainty around the actual
benefits that these products would deliver
• In analysing and presenting uncertainty, the York team determined:
– Incremental cost effectiveness ratio and probability of being cost effective at the
applicable threshold (as normally considered by Committees)
– Incremental Net Health Effect (NHE): Considers impact of recommending the therapy
on population level health. NHE is negative where ICERs are above the threshold and the
therapy not considered cost effective. May be expressed in QALY or financially
– Consequences of Decision Uncertainty: Reflects the potential magnitude of NHE that
could be gained if uncertainty surrounding potential decisions could be resolved. May be
expressed in QALY or financially
• NHE and Decision Uncertainty values in the following slides are based on 38
patients per year over a 10 year period

Bridge to HSTC TPP (minimum evidence set)
Scenario ICER Incremental NHE
QALY (£)
Probability
Cost Effective
Consequences of
decision uncertainty
QALY (£)
Expert Panel
“Decision”
Base case (£356,100
one-off acquisition cost
per patient)
£55,090 -216
(-£10,794,902)
26.1% 56.3
(£2,813,197)
No
Discount of 20% on
base case acquisition
cost (£320,490 per
patient)
£44,336 241
(£12,067,402)
76.5% 47.3
(£2,365,835)
Borderline
Lifetime leasing
method (£2,756 per
month)
£54,227 -180
(-£8,997,139)
22.1% 22.5
(£1,123,900)
No

Bridge to HSTC TPP (minimum evidence set)
Scenario ICER Incremental NHE
QALY (£)
Probability
Cost Effective
Consequences of
decision uncertainty
QALY (£)
Expert Panel
“Decision”
Payment for patients
with remission only
(approx. 35% reduction
in average cost per
patient)
£36,430 577
(£28,861,808)
96.8% 3.9
(£195,152)
Yes
Additional scenario modelled by the York team after the Expert Panel meeting
Discount of 20% on
base case with Lifetime
Leasing (£2,205 per
month)
£44,015 252
(£12,624,164)
87.4% 19.0
(£948,311)
Assumed
Borderline/Yes

Bridge to HSCT TPP (intermediate and
mature evidence sets)
• Increasing maturity of evidence had relatively low impact on the
consequences of decision uncertainty
• In this example, the key outcome from therapy is clinical remission
to allow HSCT
• Can be estimated with reasonable accuracy from even the minimum
evidence set

Curative intent TPP (minimum evidence set) Scenario ICER Incremental NHE
QALY (£)
Probability
Cost Effective
Consequences of
decision uncertainty
QALY (£)
Expert Panel
“Decision”
Base case (£528,600
one-off acquisition cost
per patient)
£50,906 -56
(-£2,902,629)
50.7% 304.6
(£15,229,786)
No
Discount of 10% on
base case (£475,740
per patient)
£45,131 306
(£15,293,860)
64.2% 209.1
(£10,456,541)
Borderline/No
Lifetime leasing
method (£3,283 per
month)
£50,618 -38
(-£1,910,653)
49.2% 65.6
(£3,227,969)
No
Payment for patients
with remission only
(approx.10% reduction
in average cost per
patient)
£45,708 267
(£13,325,042)
63.9% 236.1
(£11,803,131)
Borderline/No

Curative intent TPP (minimum evidence set)
Scenario ICER Incremental NHE
QALY (£)
Probability
Cost Effective
Consequences of
decision uncertainty
QALY (£)
Expert Panel
“Decision”
Additional scenarios modelled by the York team after the Expert Panel meeting
Discount of 10% on
base case price with
lifetime leasing (£2,955
per month)
£45,502 275
(£13,750,033)
87.2% 27.2
(£1,358,584)
Assumed
Borderline/Yes
Same pricing as
bridging to HSCT TPP
(£356,100 per patient)
£34,337 951
(£47,555,583)
85.6% 73.1
(£3,655,876)
Assumed Yes
Same total cost as
bridging TPP with
lifetime leasing (£2,221
per month)
£33,277 1050
(£52,500,851)
99.4% 2.3
(£112,597)
Assumed Yes
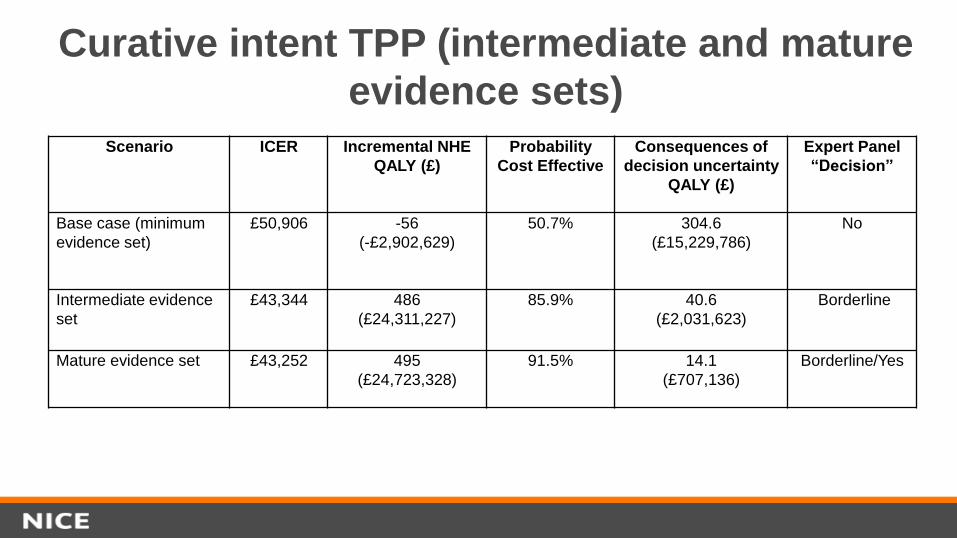
Curative intent TPP (intermediate and mature
evidence sets)
Scenario ICER Incremental NHE
QALY (£)
Probability
Cost Effective
Consequences of
decision uncertainty
QALY (£)
Expert Panel
“Decision”
Base case (minimum
evidence set)
£50,906 -56
(-£2,902,629)
50.7% 304.6
(£15,229,786)
No
Intermediate evidence
set
£43,344 486
(£24,311,227)
85.9% 40.6
(£2,031,623)
Borderline
Mature evidence set
£43,252 495
(£24,723,328)
91.5% 14.1
(£707,136)
Borderline/Yes

Curative intent TPP (intermediate and
mature evidence sets)
• Increasing maturity of evidence had a major impact on the
consequences of decision uncertainty
• The additional evidence increases the certainty around the curative
benefits and cost effectiveness of the treatment

Conclusions
• The NICE appraisal methods and decision frameworks are applicable to
regenerative medicines and cell therapies
• Quantifying and presenting clinical outcome and decision uncertainty
was key to the Expert Panel consideration of the hypothetical example
products
• Where there is a combination of great uncertainty but potentially
very substantial patient benefits, innovative payment methods
need to be developed to manage and share risk to facilitate timely
patient access while the evidence is immature
• The discounting rate applied to costs and benefits was found to have a
very significant impact on analyses of these types of technologies

Acknowledgements
• Cell and Gene Therapy Catapult
• Centre for Reviews and Dissemination / Centre for Health
Economics, University of York
• Department of Health Regenerative Medicine Expert Group
Secretariat
• Expert Panel
• Project Advisory Group