the greenfield filter: an advance in pulmonary embolism management
TRANSCRIPT
THE GREENFIELD FILTER: AN ADVANCE IN PULMONARY EMBOLISM MANAGEMENT
Paul Burke, Denis G. Mehigan, James R. Stewart, John M. P. Hyland, James Carr and David J. Bouchier-Hayes
Department of Surgery, Royal College of Surgeons in/re/and, and Department of Radiology, St. Laurence's Hospital, Dublin 7.
Summary
I N the nine months from September 1st, 1982-June 30th, 1983 nine patients
underwent an insertion of a Greenfield Inferior Vena Caval filter for prevention of pulmonary embolism from deep ven- ous thrombosis at St. Laurence's Hos- pital, Dublin. In these patients antico- agulant therapy had been found to be either inappropriate or ineffective. Four patients had developed recurrent pul- monary embolism while adequately anti- coagulated. In the other five, anticoagu- lation was contra-indicated: four because of the need for an operation and one because of intracranial haemmorhage.
Two of the filters were placed above the renal veins without adverse effect. No patients developed embolism sub- sequent to insertion of the filter. Two patients developed recurrent acute deep venous thrombosis. One patient devel- oped a neck haematoma.
The Greenfield filter appears to be a significant advance in the prevention of pulmonary embolism in a particular small group of patients. It has been safe and effective in clinical use in this small series of patients, the majority of whom were seriously ill.
Introduction Pulmonary embolism remains a major
clinical problem accounting for 15% of
Correspondence and Requests for Reprints to: Professor David Bouchier-Hayes, Department of Surgery, Royal College of Surgeons in Ireland, (AT) St. Laurence's Hospital, North Brunswick Street, Dublin 7.
deaths in acute care hospitals (Donald- son et al, 1980). Although anticoagula- tion remains the corner stone of both therapy and prophylaxis of pulmonary embolism it is sometimes either ineffect- ive or inappropriate. The therapy is ineffective in a small number of patients who develop recurrent pulmonary em- bolus despite adequate anticoagulation. It is inappropriate in patients who have a contra-indication to anticoagulation, for example those in whom a major sur- gical operation is necessary following a recent episode of venous thromboem- bolism. In the latter patients the usual methods of prophylaxis during surgery are likely to be inadequate in view of the very high risk. Whilst full anticoagu- lation would be sufficient prophylaxis in these cases most surgeons would prefer a safer method particularly in those procedures where haemorrhage compli- cations would be anticipated.
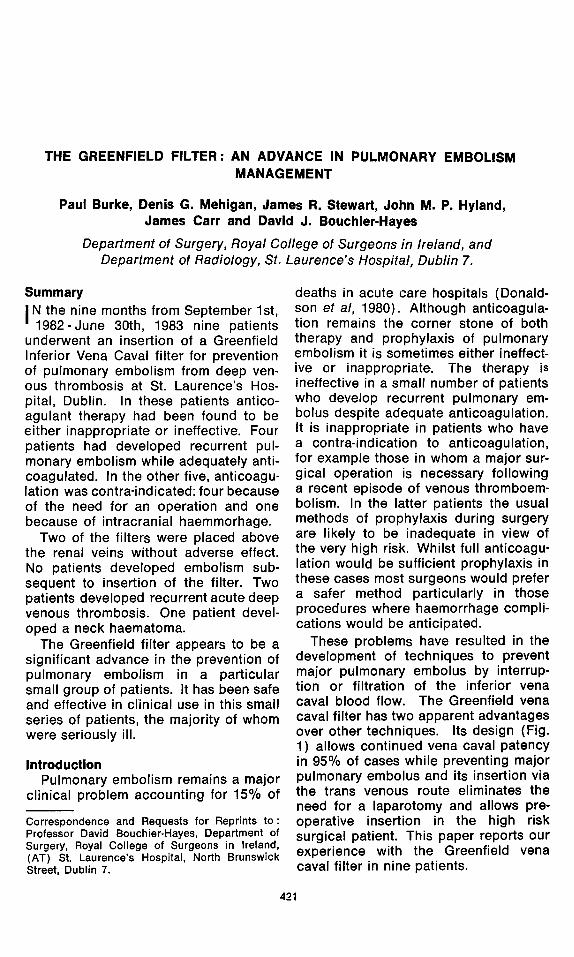
These problems have resulted in the development of techniques to prevent major pulmonary embolus by interrup- tion or filtration of the inferior vena caval blood flow. The Greenfield vena caval filter has two apparent advantages over other techniques. Its design (Fig. 1) allows continued vena caval patency in 95% of cases while preventing major pulmonary embolus and its insertion via the trans venous route eliminates the need for a laparotomy and allows pre- operative insertion in the high risk surgical patient. This paper reports our experience with the Greenfield vena caval filter in nine patients.
421
422 Burke et al. I.J.M.S. December. 1984
Fig. 1--Side and End on view of Kimray Green- field Filter Design.
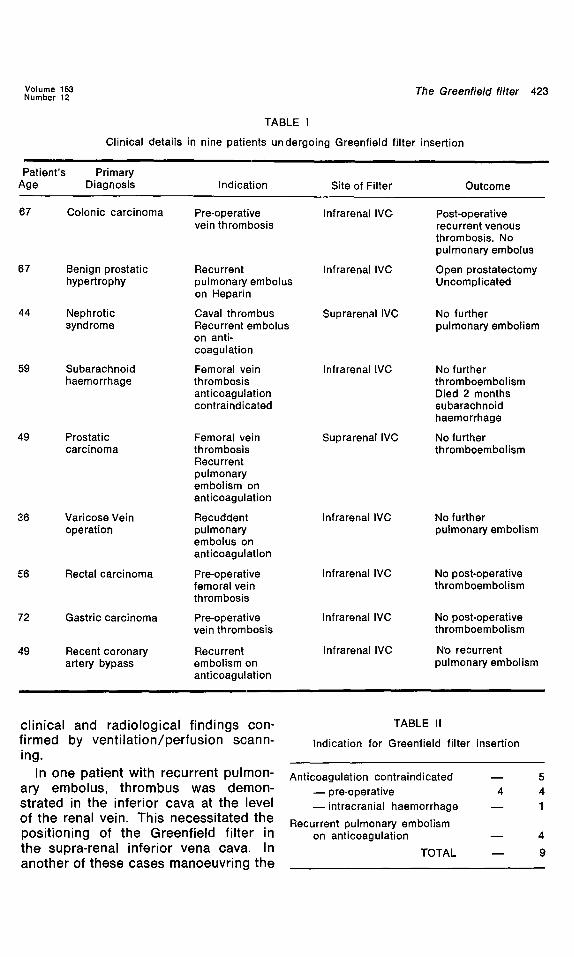
nal jugular vein cut down under local anaesthesia. The carrier was advanced under image intensifier control until it was positioned at~ the appropriate level in the inferior ven~ cava whereupon the filter was discharged from the carrier. The technique of insertion was as described by Greenfield (1979).
Prior to insertion all patients under- went ascending phlebography and where indicated inferior vena cavo- graphy to determine the presence and extent of thrombus in the deep veins.
Patients and Methods
Nine patients referred to the Vascular Surgical Unit at St. Laurence's Hospital with a diagnosis of dep venous throm- bosis or pulmonary embolism underwent Greenfield vena caval filter insertion as prophylaxis against pulmonary embol- ism between September 1st, 1982 and June 30th, 1983. The indication for in- sertion was pulmonary embolism pro- phylaxis where anticoagulation was con- traindicated or had been ineffective.
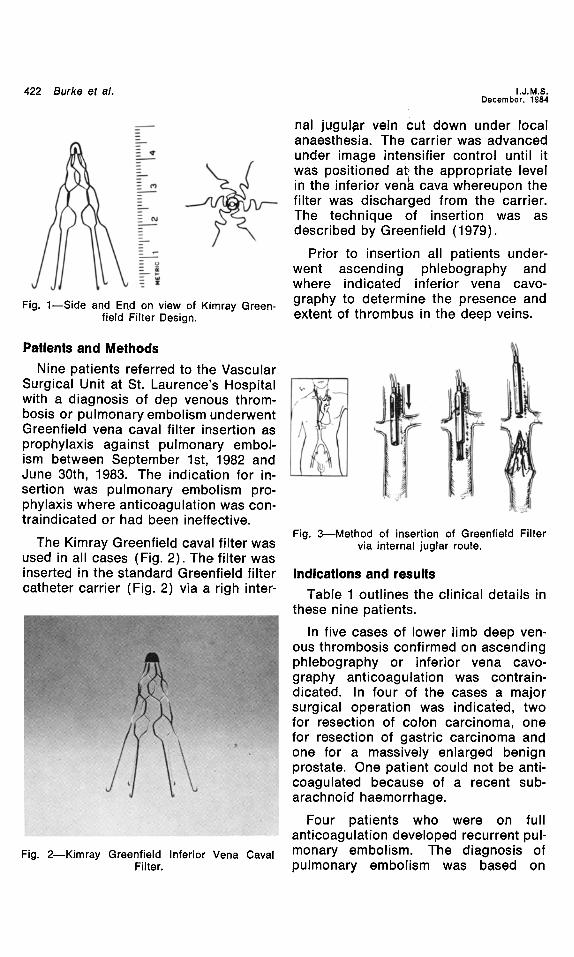
The Kimray Greenfield caval filter was used in all cases (Fig. 2). The filter was inserted in the standard Greenfield filter catheter carrier (Fig. 2) via a righ inter-
Fig. 2--Kimray Greenfield Inferior Vena Caval Filter.
Fig. 3--Method of insertion of Greenfield Filter via internal juglar route.
Indications and results
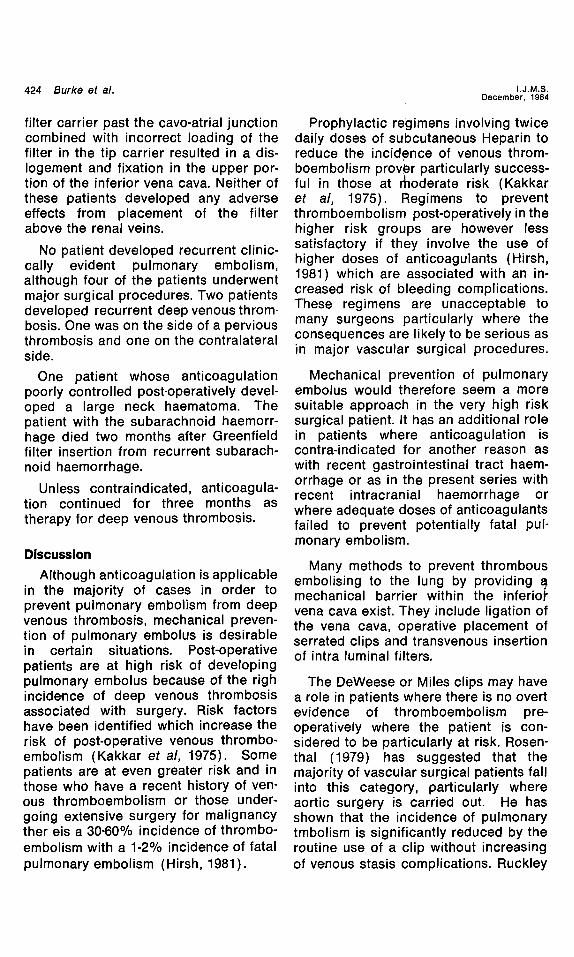
Table 1 outlines the clinical details in these nine patients.
In five cases of lower limb deep ven- ous thrombosis confirmed on ascending phlebography or inferior vena cavo- graphy anticoagulation was contrain- dicated. In four of the cases a major surgical operation was indicated, two for resection of colon carcinoma, one for resection of gastric carcinoma and one for a massively enlarged benign prostate. One patient could not be anti- coagulated because, of a recent sub- arachnoid haemorrhage.
Four patients who were on full anticoagulation developed recurrent pul- monary embolism. The diagnosis of pulmonary embolism was based on
Volume 153 The Greenfield filter 423 Number 12
TABLE I
Clinical details in nine patients undergoing Greenfield filter insertion
Patient's Primary Age Diagnosis Indication Site of Filter Outcome
67 Colonic carcinoma Pre-operative Infrarenal I V C , Post-operative vein thrombosis recurrent venous
thrombosis. No pulmonary embolus
67 Benign prostatic Recurrent Infrarenal IVC Open prostatectomy hypertrophy pulmonary embolus Uncomplicated
on Heparin
44 Nephrotic Caval thrombus Suprarenal IVC No further syndrome Recurrent embolus pulmonary embolism
on anti- coagulation
59 Subarachnoid Femoral vein Infrarenal IVC No further haemorrhage thrombosis thromboembolism
anticoagulation Died 2 months contraindicated subarachnoid
haemorrhage
No further thromboembolism
49 Prostatic Femoral vein Suprarenal IVC carcinoma thrombosis
Recurrent pulmonary embolism on anticoagulation
36 Varicose Vein Recuddent Infrarenal IVC operation pulmonary
embolus on anticoagulation
56 Rectal carcinoma Pre-operative Infrarenal IVC femoral vein thrombosis
72 Gastric carcinoma Pre-operative Infrarenal IVC vein thrombosis
49 Recent coronary Recurrent Infrarenal IVC artery bypass embolism on
an ticoagulation
No further pulmonary embolism
No post-operative thromboembolism
No post-operative thromboembolism
N'o recurrent pulmonary embolism
clinical and radiological findings con- firmed by' ventilation/perfusion scann- ing.
In one patient with recurrent pulmon- ary embolus, thrombus was demon- strated in the inferior cava at the level of the renal vein. This necessitated the positioning of the Greenfield filter in the supra-renal inferior vena cava. In another of these cases manoeuvring the
TABLE II
Indication for Greenfield filter insertion
Anticoagulation contraindicated - - 5 - - pre-operative 4 4 - - intracranial haemorrhage - - 1
Recurrent pulmonary embolism on anticoagulation m 4
TOTAL - - 9
424 Burke et al.
filter carrier past the cavo-atrial junction combined with incorrect loading of the filter in the tip carrier resulted in a dis- Iogement and fixation in the upper por- tion of the inferior vena cava. Neither of these patients developed any adverse effects from placement of the filter above the renal veins.
No patient developed recurrent clinic- cally evident pulmonary embolism, although four of the patients underwent major surgical procedures. Two patients developed recurrent deep venous throm- bosis. One was on the side of a pervious thrombosis and one on the contralateral side.
One patient whose anticoagulation poorly controlled post-operatively devel- oped a large neck haematoma. The patient with the subarachnoid haemorr- hage died two months after Greenfield filter insertion from recurrent subarach- noid haemorrhage.
Unless contraindicated, anticoagula- tion continued for three months as therapy for deep venous thrombosis.
Discussion
Although anticoagulation is applicable in the majority of cases in order to prevent pulmonary embolism from deep venous thrombosis, mechanical preven- tion of pulmonary embolus is desirable in certain situations. Post-operative patients are at high risk of developing pulmonary embolus because of the righ incidence of deep venous thrombosis associated with surgery. Risk factors have been identified which increase the risk of post-operative venous thrombo- embolism (Kakkar et al, 1975). Some patients are at even greater risk and in those who have a recent history of ven- ous thromboembolism or those under- going extensive surgery for malignancy ther eis a 30-60% incidence of thrombo- embolism with a 1-2% incidence of fatal pulmonary embolism (Hirsh, 1981).
I.J.M.S. December, 1984
Prophylactic regimens involving twice daily doses of subcutaneous Heparin to reduce the incid,ence of venous throm- boembolism prover particularly success- ful in those at ~oderate risk (Kakkar et al, 1975). Regimens to prevent thromboembolism post-operatively in the higher risk groups are however less satisfactory if they involve the use of higher doses of anticoagulants (Hirsh, 1981) which are associated with an in- creased risk of bleeding complications. These regimens are unacceptable to many surgeons particularly where the consequences are likely to be serious as in major vascular surgical procedures.
Mechanical prevention of pulmonary embolus would therefore seem a more suitable approach in the very high risk surgical patient. It has an additional role in patients where anticoagulation is contra-indicated for another reason as with recent gastrointestinal tract haem- orrhage or as in the present series with recent intracranial haemorrhage or where adequate doses of anticoagulants failed to prevent potentially fatal pul- monary embolism.
Many methods to prevent thrombous embolising to the lung by providing a mechanical barrier within the inferiol" vena cava exist. They include ligation of the vena cava, operative placement of serrated clips and transvenous insertion of intra luminal filters.
The DeWeese or Miles clips may have a role in patients where there is no overt evidence of thromboembolism pre- operatively where the patient is con- sidered to be particularly at risk. Rosen- thai (1979) has suggested that the majority of vascular surgical patients fall into this category, particularly where aortic surgery is carried out. He has shown that the incidence of pulmonary tmbolism is significantly reduced by the routine use of a clip without increasing of venous stasis complications. Ruckley
Vo=ume 153 Number 12 The Greenfield filter 425
(1982) suggested that any surgeon carrying out major abdominal surgery in patients with previously documented thromboembolism should apply a caval clip. Although the risk of venous stasis complications might be higher than the Greenfield filter convenience of clip on occasion may provide an advantage.
Two intra-luminal devices have been described namely the Greenfield filter and the Mobin-Uddin umbrella. Serious complications have been much more frequent with the umbrella even result- ing in a fatal outcome. In addition the long-term patency of the Greenfield filter is considerably higher than that of the Mobin-Uddin device. Most people now agree that the Greenfield filter is the method of choice (Wingerd et al, 1978).
Further significant advantage of the Greenfield filter is the safety of place- ment above the renal vein without deterioration in renal function with results from its high patency rate (Stewart, 1982). Two cases described in our series bring the total number of supraranel Greenfield filters to 20 (Stewart, personal communication). Six months after placement the renal func- tion in these patients has not deterior- ated and the vena cava remains patent.
The experience outlined in this paper in this small series confirms the experi- ence of the other large series reported. The procedure appears to be extremely effective, while being associated with minimal morbidity.
References
Donaldson, M. C., Wirthlin, M. D. and Donaldson, G. A. 1980. Thirty-year experience with surgi- cal interruption of the inferior vena cava for prevention of pulmonary embolims. Ann. Surg. 191, 367.
Greenfield, L. J. 1979. Technical considerations for insertion of vena caval filters. Surg. Gynec. Obstet. 148 : 422.
Hirsh, J. 1981. Prevention of deep venous throm- bosis. Brit. J. Hosp. Med. 26, 142.
Kakkar, V. V., Corrigan, T. P. and Fossard, D. P. 1975.. Prevention of fatal postoperative pul- monary embolism by low doses of heparin. An International Multicentre Trial. Lancet ii, 45.
Miles, R. M., Chappell, F. and Renner, O. 1964. A partially occluding vena caval clip for pro- tection of pulmonary embolism. Ann. Surg. 30, 40.
Rosenthal, D., Cossman, D., Matsumoto, G. and Callow, A. D. Prophylactic interruption of the inferior vena cava. Am. J. Surg. 137, 389.
Ruckley, C. V. 1982. Management of pulmonary embolism. Brit. Mad. J. 285, 831.
Stewart, J. R. and Greenfield, L. J. 1982. Trans. venous vena caval filtration and pulmonary
embolectomy. Surg. Clin. N. Amer. 62, 411. Wingerd, M., Bernhard, V. M., Maddison, F. and
Towne, J. B. 1978. Comparison of caval filters in the management of venous thromboembol- ism. Arch. Surg. 113, 1264.