the g-formula for competing risks -...
TRANSCRIPT
The g-formula for competing risks
Brice Ozenne & Thomas Alexander Gerds
Biostatistics, University of Copenhagen
April 21, 2017
1 / 30
Outline
Appetizer
Example 1
Average treatment e�ects
Asymptotics
Software
2 / 30
Appetizer
3 / 30
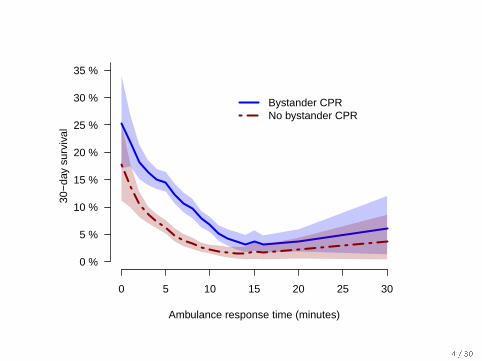
0 5 10 15 20 25 30
0 %
5 %
10 %
15 %
20 %
25 %
30 %
35 %30
−da
y su
rviv
al
Ambulance response time (minutes)
Bystander CPRNo bystander CPR
4 / 30
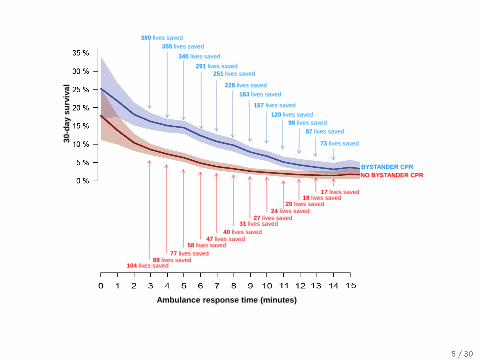
380 lives saved
355 lives saved
340 lives saved
291 lives saved
251 lives saved
228 lives saved
183 lives saved
157 lives saved
120 lives saved
98 lives saved
87 lives saved
NO BYSTANDER CPR
BYSTANDER CPR
89 lives saved 77 lives saved
58 lives saved
40 lives saved 47 lives saved
18 lives saved
31 lives saved 27 lives saved
24 lives saved 20 lives saved
104 lives saved
17 lives saved
73 lives saved
Ambulance response time (minutes)
30
-day s
urv
iva
l
5 / 30
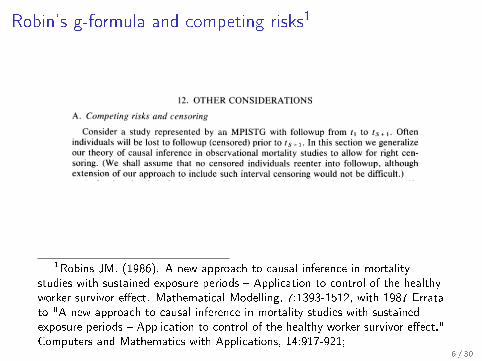
Robin's g-formula and competing risks1
1Robins JM. (1986). A new approach to causal inference in mortalitystudies with sustained exposure periods � Application to control of the healthyworker survivor e�ect. Mathematical Modelling, 7:1393-1512, with 1987 Erratato "A new approach to causal inference in mortality studies with sustainedexposure periods � Application to control of the healthy worker survivor e�ect."Computers and Mathematics with Applications, 14:917-921;
6 / 30
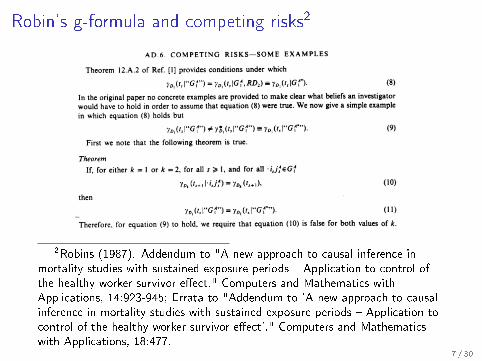
Robin's g-formula and competing risks2
2Robins (1987). Addendum to "A new approach to causal inference inmortality studies with sustained exposure periods � Application to control ofthe healthy worker survivor e�ect." Computers and Mathematics withApplications, 14:923-945; Errata to "Addendum to 'A new approach to causalinference in mortality studies with sustained exposure periods � Application tocontrol of the healthy worker survivor e�ect'." Computers and Mathematicswith Applications, 18:477.
7 / 30
Example 1
8 / 30
9 / 30
Danish registry data
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
1970
1971
1972
1994
2001
2008
2015
● ● ●●
● ● ●● ● ●●
●● ● ● ● ● ● ●●
●● ● ●
●● ●
● ●●● ● ● ●● ● ● ● ● ●
● ● ● ● ●● ● ● ●●● ● ● ● ● ● ●
● ● ●● ● ●● ● ● ● ●
● ● ●● ●
●● ● ●
● ● ● ● ● ● ●● ●
● ● ● ●●
● ● ● ● ●●
●● ●
● ● ● ●● ● ● ● ● ●
● ● ● ●● ● ● ● ●
● ● ●● ● ● ● ● ● ● ● ●
● ● ● ● ● ● ●● ● ●
● ●● ● ●
●● ● ●
● ● ●● ● ● ● ●
● ● ● ● ● ● ●● ●● ●
● ● ● ●● ● ● ● ● ● ●
●● ● ● ● ●●
● ● ● ● ●
●
●
●
●
●
●
● ●
● ● ● ●
● ● ●●
10 / 30
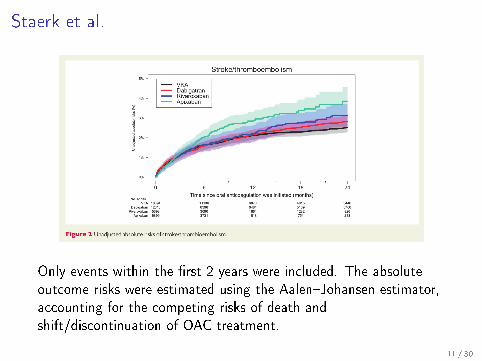
Staerk et al.
Only events within the �rst 2 years were included. The absoluteoutcome risks were estimated using the Aalen�Johansen estimator,accounting for the competing risks of death andshift/discontinuation of OAC treatment.
11 / 30
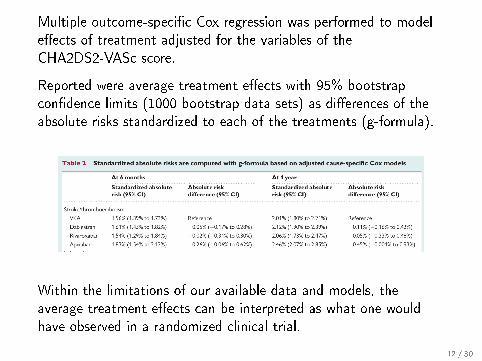
Multiple outcome-speci�c Cox regression was performed to modele�ects of treatment adjusted for the variables of theCHA2DS2-VASc score.
Reported were average treatment e�ects with 95% bootstrapcon�dence limits (1000 bootstrap data sets) as di�erences of theabsolute risks standardized to each of the treatments (g-formula).
Within the limitations of our available data and models, theaverage treatment e�ects can be interpreted as what one wouldhave observed in a randomized clinical trial.
12 / 30
Average treatment e�ects
13 / 30
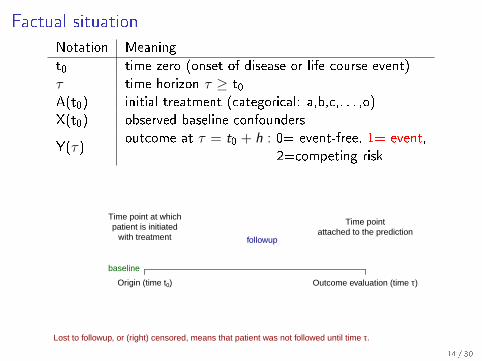
Factual situation
Notation Meaning
t0 time zero (onset of disease or life course event)τ time horizon τ ≥ t0A(t0) initial treatment (categorical: a,b,c,. . . ,o)X(t0) observed baseline confounders
Y(τ)outcome at τ = t0 + h : 0= event-free, 1= event,
2=competing risk
Time point at whichpatient is initiated
with treatment
Time pointattached to the prediction
baseline
followup
Origin (time t0) Outcome evaluation (time τ)
Lost to followup, or (right) censored, means that patient was not followed until time τ.
14 / 30
Parameter of interest
Potential outcomes3:
Yi (τ ; x) = outcome of patient i under initial treatment x
Average treatment e�ect
ATE(τ ; a, b) = P(Y (τ ; a) = 1)− P(Y (τ ; b) = 1)
The ATE is generally understood as a causal parameter (i.e., an
estimate or property of a population) that a researcher desires to
know, de�ned without reference to the study design.
3Rosenbaum and Rubin (1983)15 / 30
Parameter of interest
Potential outcomes3:
Yi (τ ; x) = outcome of patient i under initial treatment x
Average treatment e�ect
ATE(τ ; a, b) = P(Y (τ ; a) = 1)− P(Y (τ ; b) = 1)
The ATE is generally understood as a causal parameter (i.e., an
estimate or property of a population) that a researcher desires to
know, de�ned without reference to the study design.
3Rosenbaum and Rubin (1983)15 / 30
Substantive model
Observational studies with random treatment assignment mayenable one to estimate ATE in various ways4
An alternative to inverse probability weighting is standardization:
P(Y (τ ; a) = 1) = E[P(Y (τ) = 1|A(t0) = a,X (t0))
]Under exchangeability, consistency etc., g-estimation is often basedon a semiparametric structural nested mean model:
Y ∼ A + X + AX
4Hernan & Robins (book): Ideally, we would estimate the conditional meansnonparametrically . . . but we need to resort to modeling
16 / 30
Substantive model
Observational studies with random treatment assignment mayenable one to estimate ATE in various ways4
An alternative to inverse probability weighting is standardization:
P(Y (τ ; a) = 1) = E[P(Y (τ) = 1|A(t0) = a,X (t0))
]Under exchangeability, consistency etc., g-estimation is often basedon a semiparametric structural nested mean model:
Y ∼ A + X + AX
4Hernan & Robins (book): Ideally, we would estimate the conditional meansnonparametrically . . . but we need to resort to modeling
16 / 30
Formule I
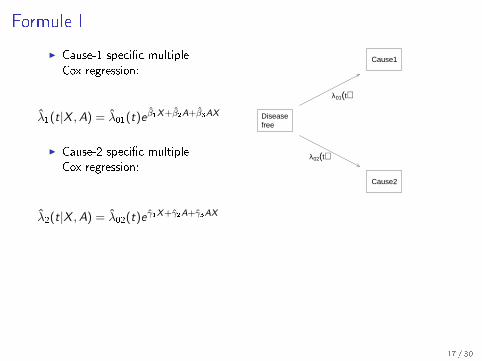
I Cause-1 speci�c multipleCox regression:
λ1(t|X ,A) = λ01(t)e β1X+β2A+β3AX
I Cause-2 speci�c multipleCox regression:
λ2(t|X ,A) = λ02(t)e γ1X+γ2A+γ3AX
Diseasefree
Cause1
Cause2
λ01(t)
λ02(t)
Expected outcome under treatment a
Yi (τ ; a) =
∫ τ
t0
exp
{−∫ s
0
[λ1(u|Xi , a) + λ2(u|Xi , a)
]du
}︸ ︷︷ ︸
event-free until s
λ1(s|Xi , a)ds︸ ︷︷ ︸event of type 1 at s
17 / 30
Formule I
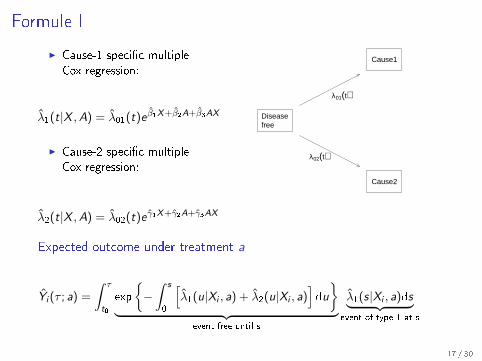
I Cause-1 speci�c multipleCox regression:
λ1(t|X ,A) = λ01(t)e β1X+β2A+β3AX
I Cause-2 speci�c multipleCox regression:
λ2(t|X ,A) = λ02(t)e γ1X+γ2A+γ3AX
Diseasefree
Cause1
Cause2
λ01(t)
λ02(t)
Expected outcome under treatment a
Yi (τ ; a) =
∫ τ
t0
exp
{−∫ s
0
[λ1(u|Xi , a) + λ2(u|Xi , a)
]du
}︸ ︷︷ ︸
event-free until s
λ1(s|Xi , a)ds︸ ︷︷ ︸event of type 1 at s
17 / 30
Regression method to estimate average e�ects
Backdoor adjustment (Pearl, 1995) aka g-estimation (Robins,1986):
ATE(a, b; τ) =1
n
n∑i=1
[Yi (τ ; a)− Yi (τ ; b)]
Glynn & Quinn5:Further, many versions of the regression estimator for ATE tend to
be quite sensitive to small amounts of misspeci�cation. Given these
de�ciencies, many researchers have opted for methods of estimation
that utilize models for treatment assignment instead of regression
models for the outcome.
5An introduction to the augmented inverse propensity weighted estimator.Political Analysis, 18(1):pp. 36�56, 2010.
18 / 30
Regression method to estimate average e�ects
Backdoor adjustment (Pearl, 1995) aka g-estimation (Robins,1986):
ATE(a, b; τ) =1
n
n∑i=1
[Yi (τ ; a)− Yi (τ ; b)]
Glynn & Quinn5:Further, many versions of the regression estimator for ATE tend to
be quite sensitive to small amounts of misspeci�cation. Given these
de�ciencies, many researchers have opted for methods of estimation
that utilize models for treatment assignment instead of regression
models for the outcome.
5An introduction to the augmented inverse propensity weighted estimator.Political Analysis, 18(1):pp. 36�56, 2010.
18 / 30
Asymptotics
19 / 30
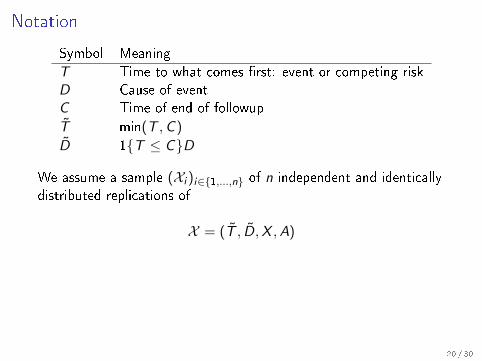
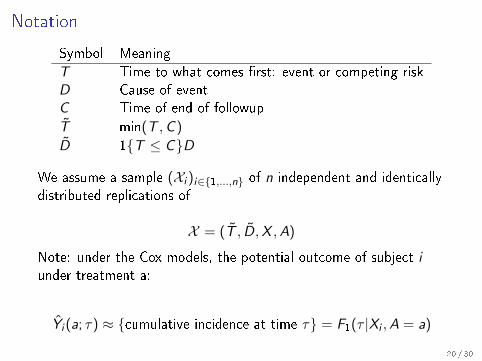
Notation
Symbol Meaning
T Time to what comes �rst: event or competing riskD Cause of eventC Time of end of followup
T min(T ,C )
D 1{T ≤ C}D
We assume a sample (Xi )i∈{1,...,n} of n independent and identicallydistributed replications of
X = (T , D,X ,A)
Note: under the Cox models, the potential outcome of subject iunder treatment a:
Yi (a; τ) ≈ {cumulative incidence at time τ} = F1(τ |Xi ,A = a)
20 / 30
Notation
Symbol Meaning
T Time to what comes �rst: event or competing riskD Cause of eventC Time of end of followup
T min(T ,C )
D 1{T ≤ C}D
We assume a sample (Xi )i∈{1,...,n} of n independent and identicallydistributed replications of
X = (T , D,X ,A)
Note: under the Cox models, the potential outcome of subject iunder treatment a:
Yi (a; τ) ≈ {cumulative incidence at time τ} = F1(τ |Xi ,A = a)
20 / 30
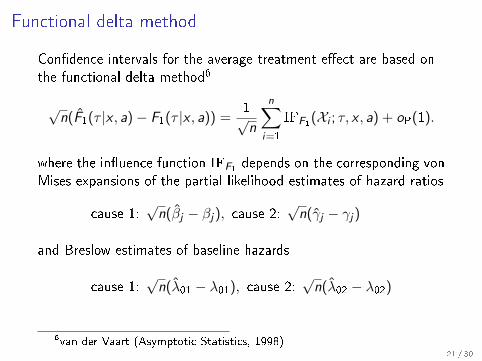
Functional delta method
Con�dence intervals for the average treatment e�ect are based onthe functional delta method6
√n(F1(τ |x , a)− F1(τ |x , a)) =
1√n
n∑i=1
IFF1(Xi ; τ, x , a) + oP(1).
where the in�uence function IFF1 depends on
the corresponding vonMises expansions of the partial likelihood estimates of hazard ratios
cause 1:√n(βj − βj), cause 2:
√n(γj − γj)
and Breslow estimates of baseline hazards
cause 1:√n(λ01 − λ01), cause 2:
√n(λ02 − λ02)
6van der Vaart (Asymptotic Statistics, 1998)21 / 30
Functional delta method
Con�dence intervals for the average treatment e�ect are based onthe functional delta method6
√n(F1(τ |x , a)− F1(τ |x , a)) =
1√n
n∑i=1
IFF1(Xi ; τ, x , a) + oP(1).
where the in�uence function IFF1 depends on the corresponding vonMises expansions of the partial likelihood estimates of hazard ratios
cause 1:√n(βj − βj), cause 2:
√n(γj − γj)
and Breslow estimates of baseline hazards
cause 1:√n(λ01 − λ01), cause 2:
√n(λ02 − λ02)
6van der Vaart (Asymptotic Statistics, 1998)21 / 30
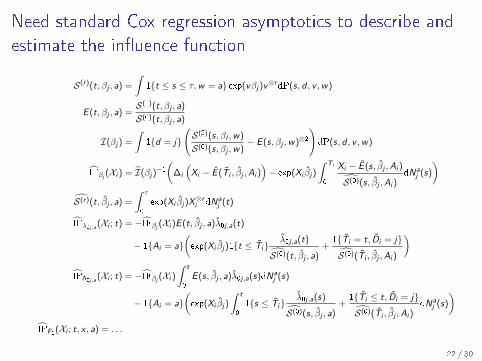
Need standard Cox regression asymptotics to describe and
estimate the in�uence function
S(r)(t, βj , a) =
∫1{t ≤ s ≤ τ,w = a} exp(vβj)v
⊗rdP(s, d , v ,w)
E (t, βj , a) =S(1)(t, βj , a)
S(0)(t, βj , a)
I(βj) =
∫1{d = j}
(S(2)(s, βl ,w)
S(0)(s, βj ,w)− E (s, βj ,w)⊗2
)dP(s, d , v ,w)
IFβj (Xi ) = I(βj)−1(
∆i
(Xi − E (Ti , βj ,Ai )
)− exp(Xi βj)
∫ Ti
0
Xi − E (s, βj ,Ai )
S(0)(s, βj ,Ai )dNa
j (s)
)S(r)(t, βj , a) =
∫ τ
0
exp(Xi βj)X⊗ri dNa
j (t)
IFλ0j,a(Xi ; t) = −IFβj (Xi )E (t, βj , a)λ0j ,a(t)
− 1{Ai = a}(exp(Xi βj)1{t ≤ Ti}
λ0j ,a(t)
S(0)(t, βj , a)+
1{Ti = t, Di = j}
S(0)(Ti , βj ,Ai )
)IFΛ0j,a
(Xi ; t) = −IFβj (Xi )
∫ t
0
E (s, βj , a)λ0j ,a(s)dNaj (s)
− 1{Ai = a}(exp(Xi βj)
∫ t
0
1{s ≤ Ti}λ0j ,a(s)
S(0)(s, βj , a)+
1{Ti ≤ t, Di = j}
S(0)(Ti , βj ,Ai )dNa
j (s)
)IFF1(Xi ; t, x , a) = . . .
22 / 30
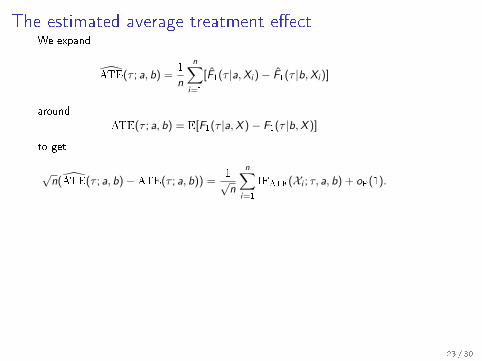
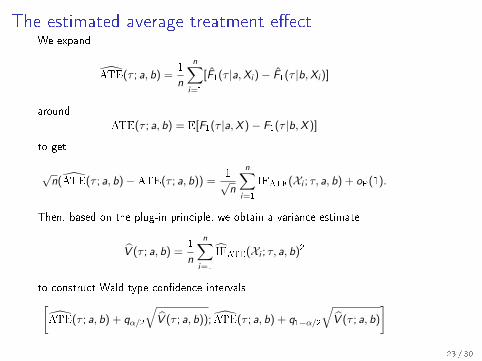
The estimated average treatment e�ectWe expand
ATE(τ ; a, b) =1
n
n∑i=1
[F1(τ |a,Xi )− F1(τ |b,Xi )]
aroundATE(τ ; a, b) = E[F1(τ |a,X )− F1(τ |b,X )]
to get
√n(ATE(τ ; a, b)−ATE(τ ; a, b)) =
1√n
n∑i=1
IFATE(Xi ; τ, a, b) + oP(1).
Then, based on the plug-in principle, we obtain a variance estimate
V (τ ; a, b) =1
n
n∑i=1
IFATE(Xi ; τ, a, b)2
to construct Wald type con�dence intervals[ATE(τ ; a, b) + qα/2
√V (τ ; a, b)); ATE(τ ; a, b) + q1−α/2
√V (τ ; a, b)
]
23 / 30
The estimated average treatment e�ectWe expand
ATE(τ ; a, b) =1
n
n∑i=1
[F1(τ |a,Xi )− F1(τ |b,Xi )]
aroundATE(τ ; a, b) = E[F1(τ |a,X )− F1(τ |b,X )]
to get
√n(ATE(τ ; a, b)−ATE(τ ; a, b)) =
1√n
n∑i=1
IFATE(Xi ; τ, a, b) + oP(1).
Then, based on the plug-in principle, we obtain a variance estimate
V (τ ; a, b) =1
n
n∑i=1
IFATE(Xi ; τ, a, b)2
to construct Wald type con�dence intervals[ATE(τ ; a, b) + qα/2
√V (τ ; a, b)); ATE(τ ; a, b) + q1−α/2
√V (τ ; a, b)
]23 / 30
Software
24 / 30
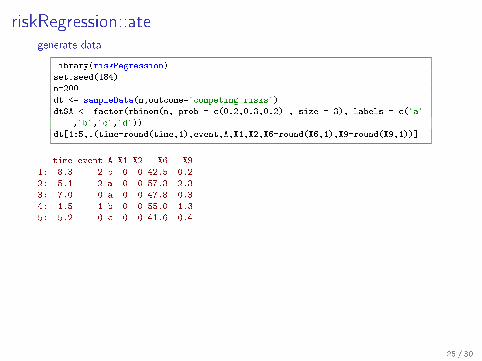
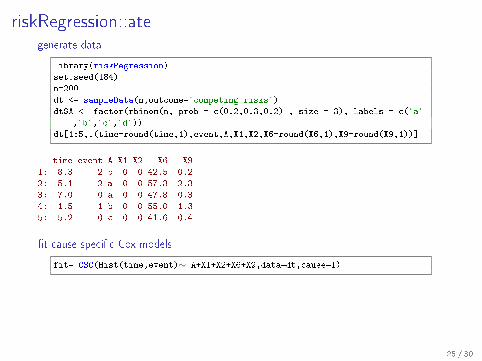
riskRegression::ategenerate data
library(riskRegression)
set.seed(184)
n=200
dt <- sampleData(n,outcome="competing.risks")
dt$A <- factor(rbinom(n, prob = c(0.2,0.3,0.2) , size = 3), labels = c("a"
,"b","c","d"))
dt[1:5,.(time=round(time,1),event,A,X1,X2,X6=round(X6,1),X9=round(X9,1))]
time event A X1 X2 X6 X9
1: 8.3 2 b 0 0 42.5 0.2
2: 5.1 2 a 0 0 57.3 2.3
3: 7.0 0 a 0 0 47.8 0.3
4: 1.5 1 b 0 0 55.0 -1.3
5: 5.2 0 c 0 0 41.6 0.4
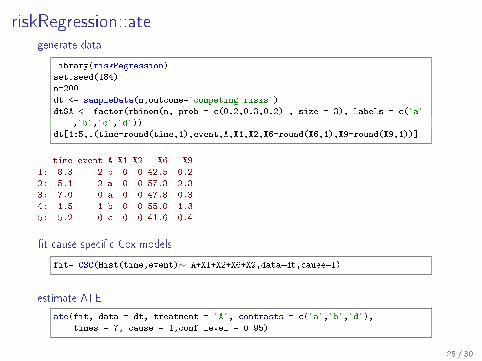
�t cause-speci�c Cox models
fit= CSC(Hist(time,event)∼ A+X1+X2+X6+X9,data=dt,cause=1)
estimate ATE
ate(fit, data = dt, treatment = "A", contrasts = c("a","b","d"),
times = 7, cause = 1,conf.level = 0.95)
25 / 30
riskRegression::ategenerate data
library(riskRegression)
set.seed(184)
n=200
dt <- sampleData(n,outcome="competing.risks")
dt$A <- factor(rbinom(n, prob = c(0.2,0.3,0.2) , size = 3), labels = c("a"
,"b","c","d"))
dt[1:5,.(time=round(time,1),event,A,X1,X2,X6=round(X6,1),X9=round(X9,1))]
time event A X1 X2 X6 X9
1: 8.3 2 b 0 0 42.5 0.2
2: 5.1 2 a 0 0 57.3 2.3
3: 7.0 0 a 0 0 47.8 0.3
4: 1.5 1 b 0 0 55.0 -1.3
5: 5.2 0 c 0 0 41.6 0.4
�t cause-speci�c Cox models
fit= CSC(Hist(time,event)∼ A+X1+X2+X6+X9,data=dt,cause=1)
estimate ATE
ate(fit, data = dt, treatment = "A", contrasts = c("a","b","d"),
times = 7, cause = 1,conf.level = 0.95)
25 / 30
riskRegression::ategenerate data
library(riskRegression)
set.seed(184)
n=200
dt <- sampleData(n,outcome="competing.risks")
dt$A <- factor(rbinom(n, prob = c(0.2,0.3,0.2) , size = 3), labels = c("a"
,"b","c","d"))
dt[1:5,.(time=round(time,1),event,A,X1,X2,X6=round(X6,1),X9=round(X9,1))]
time event A X1 X2 X6 X9
1: 8.3 2 b 0 0 42.5 0.2
2: 5.1 2 a 0 0 57.3 2.3
3: 7.0 0 a 0 0 47.8 0.3
4: 1.5 1 b 0 0 55.0 -1.3
5: 5.2 0 c 0 0 41.6 0.4
�t cause-speci�c Cox models
fit= CSC(Hist(time,event)∼ A+X1+X2+X6+X9,data=dt,cause=1)
estimate ATE
ate(fit, data = dt, treatment = "A", contrasts = c("a","b","d"),
times = 7, cause = 1,conf.level = 0.95)
25 / 30
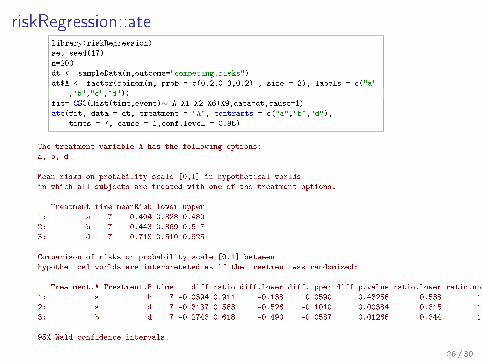
riskRegression::atelibrary(riskRegression)
set.seed(17)
n=200
dt <- sampleData(n,outcome="competing.risks")
dt$A <- factor(rbinom(n, prob = c(0.2,0.3,0.2) , size = 3), labels = c("a"
,"b","c","d"))
fit= CSC(Hist(time,event)∼ A+X1+X2+X6+X9,data=dt,cause=1)
ate(fit, data = dt, treatment = "A", contrasts = c("a","b","d"),
times = 7, cause = 1,conf.level = 0.95)
The treatment variable A has the following options:
a, b, d
Mean risks on probability scale [0,1] in hypothetical worlds
in which all subjects are treated with one of the treatment options:
Treatment time meanRisk lower upper
1: a 7 0.404 0.328 0.480
2: b 7 0.443 0.369 0.517
3: d 7 0.718 0.510 0.925
Comparison of risks on probability scale [0,1] between
hypothetical worlds are interpretated as if the treatment was randomized:
Treatment.A Treatment.B time diff ratio diff.lower diff.upper diff.p.value ratio.lower ratio.upper ratio.p.value
1: a b 7 -0.0394 0.911 -0.138 0.0590 0.43256 0.538 1.54 0.7294
2: a d 7 -0.3137 0.563 -0.526 -0.1010 0.00384 0.315 1.01 0.0521
3: b d 7 -0.2743 0.618 -0.490 -0.0587 0.01266 0.344 1.11 0.1059
95% Wald confidence intervals.
26 / 30
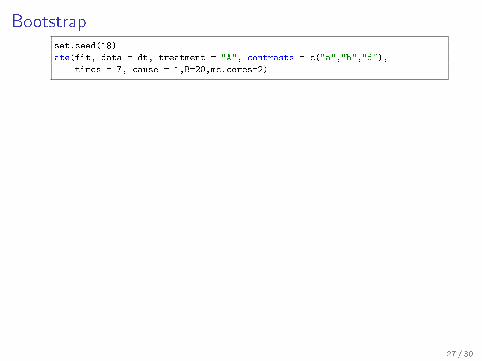
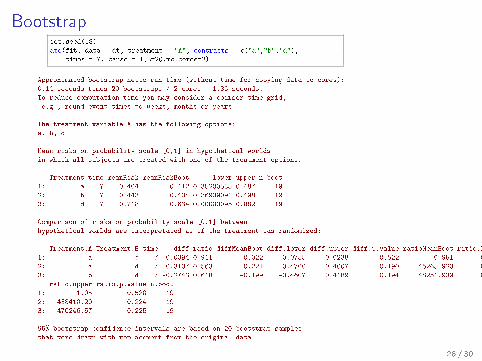
Bootstrapset.seed(18)
ate(fit, data = dt, treatment = "A", contrasts = c("a","b","d"),
times = 7, cause = 1,B=20,mc.cores=2)
27 / 30
Bootstrapset.seed(18)
ate(fit, data = dt, treatment = "A", contrasts = c("a","b","d"),
times = 7, cause = 1,B=20,mc.cores=2)
Approximated bootstrap netto run time (without time for copying data to cores):
0.14 seconds times 20 bootstraps / 2 cores = 1.36 seconds.
To reduce computation time you may consider a coarser time grid,
e.g., round event times to weeks, months or years.
The treatment variable A has the following options:
a, b, d
Mean risks on probability scale [0,1] in hypothetical worlds
in which all subjects are treated with one of the treatment options:
Treatment time meanRisk meanRiskBoot lower upper n.boot
1: a 7 0.404 0.412 0.35200585 0.487 19
2: b 7 0.443 0.434 0.36939091 0.498 19
3: d 7 0.718 0.634 0.00000095 0.882 19
Comparison of risks on probability scale [0,1] between
hypothetical worlds are interpretated as if the treatment was randomized:
Treatment.A Treatment.B time diff ratio diffMeanBoot diff.lower diff.upper diff.p.value ratioMeanBoot ratio.lower
1: a b 7 -0.0394 0.911 -0.022 -0.0755 0.0238 0.522 0.951 0.834
2: a d 7 -0.3137 0.563 -0.221 -0.4700 0.4007 0.190 45265.923 0.462
3: b d 7 -0.2743 0.618 -0.199 -0.4607 0.4189 0.194 48251.939 0.478
ratio.upper ratio.p.value n.boot
1: 1.05 0.520 19
2: 438410.20 0.224 19
3: 470246.57 0.225 19
95% bootstrap confidence intervals are based on 20 bootstrap samples
that were drawn with replacement from the original data.
28 / 30
Discussion
I Causal inference is still 'sexy' in many research groups
I It is important that one can imagine a randomized trial
I The hype has reached pharmacoepidemiologists who oftenhave large data sets, issues with time, and interesting problems
I Absolute risks can be estimated using cause-speci�c Coxregression 7
Modelling issues
I choice of τ
I compliance/intention to treat
I strati�ed baseline hazards
I interactions
7Benichou & Gail (1990)29 / 30
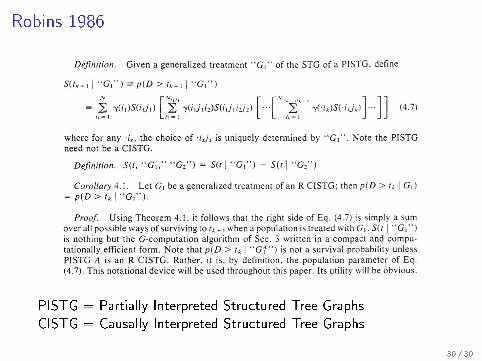
Robins 1986
PISTG = Partially Interpreted Structured Tree GraphsCISTG = Causally Interpreted Structured Tree Graphs
30 / 30