the experience of fatigue as a distressing symptom of heart failure
TRANSCRIPT

The experience of fatigue as a distressing symptomof heart failure
Jacqueline Jones, RN, BN, PhD, FRCNAa,*,Carrie M. McDermott, RN, MSN, CCRN, APRN-BCa, Carolyn T. Nowels, MSPHb,c,
Daniel D. Matlock, MD, MPHb, David B. Bekelman, MD, MPHc
aCollege of Nursing, University of Colorado, Anchutz Medical Campus, Aurora, Coloradob School of Medicine, University of Colorado, Anchutz Medical Campus, Aurora, Colorado
cDenver Veterans Affairs Medical Center, Denver, Colorado
a r t i c l e i n f o
Article history:Received 26 October 2011Revised 8 April 2012Accepted 10 April 2012Online 30 May 2012
Keywords:FatigueHeart failurePatient experiencesQualitative researchPatient-centered care
* Corresponding author: Jacqueline Jones, RN13120 East 19th Avenue, Campus Box C-288-
E-mail address: jacqueline.jones@ucdenv
0147-9563/$ - see front matter � 2012 Elsevidoi:10.1016/j.hrtlng.2012.04.004
a b s t r a c t
Objective: We explored the perceptions, experience, and meaning of fatigue asa distressing symptom of chronic heart failure (HF).
Background: Fatigue, a common symptom of HF, may indicate worseningcondition. Patients interpret their symptoms to determine the need for assis-tance. The meaning of fatigue in everyday life for HF patients in the UnitedStates is not well understood.
Methods: We performed an interpretive study of in-depth interviews with HFpatients (n ¼ 26) who reported fatigue as a symptom, using a thematic analysisof transcripts within an iterative group framework.
Results: Fatigue is characterized by patient values related to their self-identity,their body, their experience of time, their environment, and their relationshipswith others, including the healthcare system.
Conclusions: Fatigue influences perceived proximity to death and how patientstry to preserve what they can do. A patient’s HF management plan should betailored and responsive to that patient’s experience of fatigue as communicatedby the patient.
Cite this article: Jones, J., McDermott, C. M., Nowels, C. T., Matlock, D. D., & Bekelman, D. B. (2012,
SEPTEMBER/OCTOBER). The experience of fatigue as a distressing symptom of heart failure. Heart & Lung,
41(5), 484-491. doi:10.1016/j.hrtlng.2012.04.004.
The patient’s perceived symptomburden in the contextof heart failure (HF) is vitally important. A newlyreleased scientific statement by the American HeartAssociation on decision-making in advanced HF1
emphasizes care that aligns with patient values, goals,
, BN, PhD, FRCNA, Colle19, Aurora, CO 80045.er.edu (J. Jones).
er Inc. All rights reserved
and preferences, including a focus on outcomes impor-tant to patients, such as fatigue. Although symptomsoftenoccur together,2 fatigue isoneof themostcommonand distressing symptoms of HF.3-5 Despite its signifi-cance and the belief that fatigue is amenable to
ge of Nursing, University of Colorado, Anchutz Medical Campus,
.

h e a r t & l ung 4 1 ( 2 0 1 2 ) 4 8 4e4 9 1 485
treatment, a recent Cochrane systematic review ofinterventions for the management of fatigue inadvanced illnesses such as HF identified that very littleclear guidance existsonhowto treat fatigueeffectively.6
The review called for more research to inform patient-oriented approaches to treatment, because the experi-ence of fatigue influences quality of life.7-11
Fatigue may be undervalued by HF providers. Inaddition to the many concurrent symptoms experi-enced by patients with HF,8-12 fatigue is difficult toisolate and therefore treat.6,13 For providers to focus onfatigue is challenging, because disease managementguidelines address the signs of HF, such as blood pres-sure, pulse, ejection fraction, and volume status.14 Thescience on the symptoms of fatigue during HFcurrently offers limited guidance. Studies of fatigue inHF have described the multidimensional nature of thesymptom5,7,15 and how fatigue can be connected tophysiological9,16-18 or psychological19-21 symptoms, orboth.2 Smith et al identified multiple trajectories forboth exertion and general fatigue in HF, and thesediverse trajectories may help target interventions orpredict mortality.22,23
Sometimes fatigue and depression are linked.Research in Sweden by Falk et al5 found that in 112patients with HF, emotional fatigue was linked toanxiety, and depression was linked to a reduction inphysical activity and low motivation. Beyond breath-lessness, poor agreementwasobservedbetween fatigueandotherprototypical symptoms, leading theseauthorsto advocate closer attention to apatient’s appraisal of allsymptoms and their perceived significance. A study ofTaiwanese patients with HF and symptomatic orpsychological (anxietyanddepression)distress reportedhigher levels of fatigue.20 Vital exhaustion is anotherconcept used to represent the psychological dimensionof fatigue that negatively affects quality of life.24
Often fatigue and limitations in physical activity areconnected, prompting the use of functional capacity oractivities of daily living as a proxy for fatigue.16,25 Ina sample of 54 older Americans (aged >65 years),intensity of fatigue and self-reported functional status,including exercise, were unrelated in patients with HF.Fatigue was identified as a persistent symptom thatmay be underreported because it is often attributed toaging.25 Hagglund et al qualitatively explored fatigueamong elderly Swedish women with HF (n ¼ 10, aged>73 years), and found fatigue to be more of a physicalexperience, or a loss of physical energy, where inac-tivity was viewed as dangerous, and with limited bodycapacity.3 Falk et al also studied hospitalized patientswith HF (n ¼ 93) in Sweden and found fatigue to bea physical sensation but not a unified experienceacross their sample.5 Their qualitative work26 (n ¼ 15)identified fatigue as a circular process between thedominant physical experience and the consequencesof being fatigued, which produced an exaggeration ofthe symptom experience. Although Falk et al identifiedfatigue as involving the whole person, they argued thatfatigue could be alleviated by restorative activities and
by monitoring for the sensation of “giving up andhopelessness” that fatigue brings.26
Previous research into fatigue provided under-standings of how fatigue is related to other symptomsand some clues about the experience of fatigue. Ametastudy of qualitative research exploring fatigueacross conditions (n ¼ 35 primary studies) recom-mended that fatigue be studied with attention to thepersonal and sociocultural context in which it occurs.27
International research has begun to highlight elementsof the fatigue life experience, but given that themeaning of fatigue is related to the context of theexperience, cultural and system nuances can influencethe perceived impact on life, quality of life, and adap-tation strategies. An understanding of fatigue in anAmerican context is needed to help inform partnershipdevelopment with patients, so that providers can workwithin a patient-centered framework. This under-standing could generate new insights into fatigue asa source of distress, characterize the place of fatigue ina patient’s life and HF trajectory, and inform thera-peutic interventions from the patient’s uniqueperspective. This study sought to define the patient’sperception of fatigue as a distressing symptom of HF.The outcome will provide an anchor for patient-centered interventions addressing fatigue, and movediscussions of treatment toward alignment withpatients’ values, goals, and preferences.
Methods
This work is part of a larger study exploring the expe-rience of living with HF, the unmet needs of patientswithHF, and the potential for a palliative care approachto HF.28 We performed in-depth, semistructured, indi-vidual interviews with patients with HF from 2007through 2008. The interviews were conducted by2 qualitative researchers and lasted 60 to 90 minutes.During these interviews, individual patients with HFwere asked:28
(1) What is most difficult for you about your heartcondition?(a) What is most distressing about it?(b) What is the hardest thing about living with it on
a daily basis?
Patients were asked about their symptoms of HF:
(1) Can you tell me about any of your symptoms thatmight need better treatment?(a) What 1 or 2 are the most distressing to you?(b) How do you deal with your symptoms?
Patients with HF and their family caregivers sup-ported the early integration of palliative care services,

Table 1 e Characteristics of patients included infatigue analysis
Patients(n ¼ 26)
AgeMedian (IQR), years 61 (50.5 to 71.2)
Women, n (%) 8 (30.8)NYHA classification, n (%)
II 11 (42.3)III 13 (50.0)IV 2 (7.6)
Comorbid conditions, n (%)Hypertension 17 (65.3)Diabetes 11 (42.3)Atrial fibrillation 14 (53.8)Stroke 3 (11.5)COPD 10 (38.5)
Ejection fraction, median (IQR) 30 (23 to 41.8)BNP, median (IQR) (pg/mL) 363 (139 to 630)
h e a r t & l ung 4 1 ( 2 0 1 2 ) 4 8 4e4 9 1486
and particularly psychosocial support and symptomcontrol, using a collaborative team approach.28
Patients described experiencing a variety of symp-toms, of which fatigue was most distressing. The focusof this interpretive study involves an in-depth explo-ration of three key questions:
(1) “What is it like to experience fatigue in the contextof HF?”
(2) “What does it mean to experience fatigue as a dis-tressing symptom of HF?”
(3) “How can an in-depth understanding of fatigueinform the content, structure, and timing forservices to enhance quality of life for patientswith HF?”
Ischemic etiology, n (%) 12 (46.1)Time since diagnosis, median
(IQR), years9.5 (2.73 to 13.7)
BNP, brain natriuretic peptide; COPD, chronic obstructivepulmonary disease; IQR, interquartile range; NYHA, NewYork Heart Association functional class.
Participant Recruitment
In the parent study,28 outpatientswith symptomatic HF(n ¼ 33) were recruited from cardiology and geriatricclinics at a large university medical center, usingpurposive sampling. Eligible patients were at least18 years of age, and had received a diagnosis of HF fromany cause (ischemic or nonischemic) with New YorkHeart Association Class II to IV symptoms. Patientswere excluded if they had received a diagnosis ofdementia. Sampling progressed until a sufficientnumber of patients varying across age, health status,and time since diagnosis was collected.28
Patients with HF in the parent study talked aboutvariable symptoms, alone or in combinationwith othersymptoms. Although fatigue was the most commonsymptom reported in this sample, 7 patients with HFdid not talk about fatigue as a symptom or as exertinginfluence in their lives. The interpretive descriptionreported here comprises the analysis of patients’experiences of fatigue as a symptom of HF (n ¼ 26) andwhat it meant to them in daily life. Fatigue was iden-tified bymany (n¼ 13) as their “most difficult” or “mostdistressing” symptom. It was also identified (n ¼ 6) asan important symptom of HF, but not the “most diffi-cult.” Patients who identified fatigue as a generalsymptom of their HF during the interview were alsoincluded in this analysis (n ¼ 7). These 26 transcribedinterviews form the basis for our analysis, providinga rich and comprehensive sample to inform potentialcare directions for HF patients experiencing fatigue.29
Table 1 illustrates the characteristics of those whoexperienced fatigue.
Analysis
Transcribed interviews were analyzed, using interpre-tive methods to illuminate the symptom experience,context, and meaning of fatigue.30,31 Using a generalinductive approach,32 each researcher read transcripts
to derive an understanding of the whole, and thenthe data were read again, with the researcher makingmargin notes and establishing initial codes. Once thesewere identified with the participant’s language, wegrouped data into themes, and then described thetextural, structural, and overall description andmeaning of the fatigue experience.30-32 Our unit ofanalysis comprised examples of fatigue across thepatient sample. We looked for the descriptors andcontext of each subjective experience of fatigue relatedto time, environment, body awareness (including othersymptoms), and relationships. Our team consideredand recontextualized the findings, similarities, anddifferences, and arrived at a consensus regardingdisagreements of language, meaning, or interpreta-tions31 of fatigue as a distressing symptom. Rigor wasenhanced by using established qualitative strategiesof audit trail development, the reflexive and iterativemanagement of individual and team analysis, induc-tive and deductive approaches to coding, memos,and journals to monitor analytic development, lead-ership by experienced doctoral-prepared qualitativeresearchers, and confirmability through the presenta-tion of emerging findings to professional groups.30-32
Results
Two broad themes emerged from patients’ experienceswith fatigue, ie, symptom experience and meaning. Thesymptom experience of fatigue included “knowing” thesymptom, the “physical experience” of the symptom,and the “timemanagement and planning” necessary to

h e a r t & l ung 4 1 ( 2 0 1 2 ) 4 8 4e4 9 1 487
adapt to the symptom. The meaning of fatigue asa symptom of HF involves both “existential meaning”and “contextual meaning.” Each is revealed in thedescriptions of fatigue, and is highlighted in the waytime, environment, body, and relationships withothers are expressed. Table 2 illustrates participants’text exemplars associated with each element (eg,time), and then provides our interpretation ofwhat thisnarrative of fatigue experiences means in the contextof HF.
Symptom Experience
Fatigue as a symptom was described by patientsthrough a variety of terms, including expressions of“being tired,” “body tired,” and “physically tired,” butmost often through descriptors related to not having“full energy” or “low energy levels.” Only 9 patientsused the term “fatigue,” often after it was introduced asa clarifying term for energy level by the researcher.When patients discussed their experience of fatigue,they tended to describe it as a symptom in isolation.Although they described other symptoms at differenttimes during interviews, such as shortness of breath,worry, depression, pain, and problems with sleep, ingeneral they did not spontaneously associate fatiguewith these other symptoms.
Knowing
Patients with HF described a sense of “knowing” andanticipating the symptom of fatigue. They knew thissymptom based on past experience. They recognizedthe warning signs and anticipated the symptom.Patients with HF read their body like a barometer uponwaking. This sensation of “knowing” indicates thatfatigue is not necessarily related to tasks or activity:“Usually you can tell right away whether you are oraren’t going to have a bad day. I mean you kind ofknow.” Knowing the symptom of fatigue is to under-stand the signs that can warn of the symptom, andunderstanding the consequences of not heeding thosesigns. Using caution or watchful waiting is a way ofresponding to “knowing” the symptom of fatigue:“Your body will tell you, a person has to be in tune withtheir body to learn.” The learning can take months toyears for some patients as they make some adjust-ments in terms of what they can do, what helps, andwhat does not. Ultimately they learn to “take it 1 day ata time.”
The Physical Experience
Patients with HF emphasize the physical burden offatigue: “ I get tired. I get tired real fast.” Theydescribed the loss of strength and physical changesbrought by fatigue. They listen to their body so thatthey do not “overdo it.” Patients spoke of their energybeing “sapped” and their mind wanting what their“body will not cooperate” to do. Many usual activities
became too heavy, too physically demanding, such asdoing laundry or shopping for groceries. Breathless-ness may occur at this time, but is perceived as self-limiting. Fatigue, however, endures. For many, thisincluded the need to sleep much earlier in the day.Often, sleep made no difference to their level of fatigueon waking: “I wake up in the morning, and I am notrested.”
As one participant said, “My physical existence hasbeen stripped down to almost one quarter of what usedto be a full life.” The physical experience of fatigue isprimarily “an inside experience.” Others around themcannot “see” the patient’s fatigue. Family, friends, andeven health professionals are perceived to lackunderstanding about the experience of fatigue and theway that the HF patient’s energy level can vary from1 day to the next: “I wish that they did understandwhen I say I’m tired.” Sometimes patients felt thatothers saw their fatigue “as using it like an excuse,” or“being lazy.”
Patients with HF explained that they becameaccustomed to adaptations to being tired. Theyrecounted their ability to manage fatigue as beingrelated to their overall fatigue burden, and not justa sensation of being tired. “So when [I] say ‘fine’ itmeans something I can deal with. Not the same assomeone else’s ‘fine.’” Moreover, “there are a series ofadjustments. there is a fine line.”
Time Management and Planning
Patients with HF emphasized the importance of plan-ning and time management. They understood how tooptimize their reality to minimize the day-to-dayimpact of fatigue. Patients identified the need to beproactive and to protect their time as a way of pro-tecting their energy level. “They [ie, activities] alsohave to be planned out and everything. If I push thevacuum around today I can’t wash dishes because Ihave to stand.” The need to plan was a part of copingand “protecting” oneself from the symptom and theconsequences of “overdoing.” This extended beyondthe HF patient’s individual life circumstances toinclude his or her ability to interact with the healthsystems that support them: “I even changed primary-care physicians here because the one I was seeingonly had office hours from 1:00 on. I told him. I justhave to see somebody in the morning.”
Meaning of Fatigue
Contextual meaning involves the way the patientperceived the symptom to influence daily life. Patientsdescribed activities they “can’t do” as well as the wayfatigue affected relationships with others. Many saidthey were unable to meet the expectations of othersand were troubled by how they heard others to under-stand the symptom of fatigue. One patient relatedlosing a job over fatigue, whereas others had to give upwork because of it. Some gave examples of changing

Table 2 e Fatigue as interpreted experience as lived
Subjective framework Exemplar text Interpretation
Experience of time “No planning for the future”“Living on death’ doorstep”“Just waiting to die”
Living day to day with mortality ever present
Body awareness “Not like it used to be”“Knowing limits”“Push too hard; it takes day to recover”“Loss of physical strength”“I am still capable; just limited”
Body as a barometer for what patients can do today
Environment “My reality has shrunk”“Acceptance that my world has changed”“Need to learn”dStop working“Lost my job due to fatigue”
Reframe reality and existence by expandingand contracting boundaries to maximizewhat patients can do
Relationships “They don’t understand”“Don’t want to be dependent”“Edgy and sharp”“It’s hard for others to see it”“Need to focus on self”“People change toward you”
It’s an inside experience, making it difficultto communicate about fatigue with others
h e a r t & l ung 4 1 ( 2 0 1 2 ) 4 8 4e4 9 1488
roles and family rituals such as being a grandparent,cooking, doing housework, leading holiday festivities,or driving. Patients with HF even avoided communi-cationwith those around them “just so they don’t haveto deal with it,” ie, the topic of fatigue and being tired:“It’s like getting broke back to being a kid again.” “Youshouldn’t do that or you can’t do this.”
The contextual meaning of fatigue for the patientwith HF involves the understanding that their worldis made smaller by the experience of fatigue. Theirrelationships, physical activity, community engage-ment, employment, and social interaction can allbe limited by the experience of fatigue. Positivelanguage, however, came through, eg, “I’m stillcapable of doing things, it’s just very limited,” or “I cando it for a little bit.” This had a profound impact onpatients with HF and their families. The emotionalburden of fatiguemanifested itself in patientswithHFas irritability. They talked of “putting on a front” withothers and thinking of themselves because havingto communicate can also be exhausting. Patientswith HF would purposely “not talk” to family or comeacross as “being angry” as a way of conservingemotional energy and getting people to leave themalone: “You just got to dealwith it and themore you letthem indpeople who care about youdif you let themin on it, then they tend to get all upset.”
Existential meaning reflects the sense of vulnerabilityand mortality the patient felt as a result of experi-encing the symptom. Among those who describedfatigue as their most difficult symptom (n ¼ 13),6 referred directly to issues of mortality and the lack ofcure for HF as the most distressing thing about livingwith HF. Metaphors for life and existencewere found inthe language used to describe fatigue, eg, “The energylevel again. You kind of have to not think about it. Ifyou think about it, it is kind of like having a time bombin your chest.” At times, patients characterized thesymptom as if fatigue were a representation of life
itself: “There are days like you are like a match. In themorning it is just like you want to go and you just kindof fade out really quick. I get up feeling really good butthen you just burn out fast.” Patients understood thesymptom as an “inside experience,” a manifestation oftheir HF disease, and a real-world representation ofexistence and uncertain yet ultimate mortality.
Discussion
Fatigue as a distressing symptom of HF has beenillustrated through the experiences of our participantsas an embodied understanding of their HF disease5,26,27
and of their mortality. Knowing fatigue, the embodi-ment of the symptom experience, and how thepatient’s world has changed all come together to createan understanding by the patient with HF of the spatial,temporal, and interpersonal limitations imposed onthose who experience fatigue as a symptom of HF,leading to a significant reduction of the world in whichthey had previously lived. The symptom meaning isunderstood as the limitations fatigue exerts on HFpatients’ ability to function and as the adaptations theymust make.
Fatigue Brings a Reframing of Existence andSense of Self
Patients expressed a changed reality where theyattempt over time to reframe their self-identity andlive a life doing what they can.3,15 They reframed byplanning and prioritizing daily activities andmanagingthe expectations of family and friends. They createdphysical and social boundaries to cope with the expe-rience of fatigue. Fatigue limited our patients’ world inamanner similar to that in a report describing patients’experience of living in a “shrunken” space and time.33

h e a r t & l ung 4 1 ( 2 0 1 2 ) 4 8 4e4 9 1 489
Fatigue became a barometer by which they measuredtheir life force, productivity, and self-worth.34 Ina study of elderly women with HF, the daily struggle ofcoping with fatigue was described as “living with theloss of physical energy” and “striving for independencewhile being aware of deteriorating health.”3 However,our patients reported actively changing their realityrather than “drifting along.”33
Patients with HF, through the experience of fatigue,came to a new sense of self. These changes seemedintegral to a reframing of HF patients’ self-identity andwhat they perceived they now “can do.” As in otherstudies, our patients with HF recounted that fatiguecan be dynamic, changing day to day and over time,and that they want to remain hopeful and don’t wantto give in.3,17,23 Patients described the impact of fatigueas a fear of overexertion. Patients balanced theirrestriction of activity to conserve energy with the needto participate, and they strove to maintain a self anda reality they were familiar with. Our study adds to thisgrowing picture of identity transformation.22,23
Interpersonal Aspects of Fatigue
This study supports the concept that patients with HFneed psychosocial support,5,11,21 first by understandingthat many limit their social interactions and emotionaltalk. Other studies found that fatigue can create anemotional burden, at different times involving anxietyor depression.5,11 However, our patients also sharedtheir perspective of fatigue in terms of “doing what youcan.” This extends previous work that described onlywhat patients can no longer do,35-38 and sometimes asa result described them as depressed.35,36 Our patients,like those in other studies, balanced a loss of partici-pation with their current capacity for socialinteraction.26,39
Patients’ perceptions of how others, such as familycaregivers, react to or see them reflected the strain thatfatigue exerted on interpersonal relationships, andsometimes left patients feeling isolated with theknowledge of their ownmortality. Our study highlightsthat patients with HF, in their fatigue-colored world,perceive others around them as outsiders because theydo not understand the patients’ experience of fatigue.These perceptions are often at odds with the waypatients adapt to the existentialmeaning of fatigue andtheir desire not to burden or become dependent onothers.3,36 Because of this intolerance and the fear offatigue being seen as an excuse, patients are oftenunwilling to burden their caregivers with some of theirconcerns. It takes too much energy, and their lifefunction revolves around conserving energy andspending it wisely in the context of a particular day.
Implications
If providers understand the importance of fatigue forthe patient and know where the patient is ona continuum of adjusting to fatigue, they could identify
“next steps” to help their patient adjust further to thatfatigue. This study challenges notions of how toreconcile the importance of attending to patients’experiences whilemanaging disease. Ideally, these twogoals should be aligned. How can health professionalsand systems of care be oriented to hear and under-stand expressions of a patient’s understanding of theirmortality and their disease? How do we best respect,empathize with, and use what the patient knows andunderstands about fatigue? Is this experience informationrelated to HF disease management, or solely tounderstanding and helping patients live with HF? Theway fatigue is comprehended and used to manage HFcould potentially be at odds with the patient’s reality.36
In our study, low energy or vital life-force metaphorswere more frequently used than the term “fatigue.”Healthcare providers should consider the existentialand contextual meaning of fatigue as an importantaspect in the daily struggle of living with HF. Duringtheir assessment, health professionals can considerasking their patients about the specific aspects of day-to-day life that are likely to be affected by fatigue, suchas socialization,34,35 relationships, and routine activi-ties. Table 3 lists suggested assessment questions thatcould frame the evaluation of fatigue, and help tailorinterventions aimed at treating fatigue and enhancingself-care.40 Identifying the severity, onset, duration,and pattern of fatigue over time, combined with iden-tifying its exacerbating and relieving factors, canisolate the impact of fatigue on all aspects of dailylife.41
The patient with HF is aware of the life-limitingnature of this disease, yet may live with HF for manyyears beyond original expectations. We build on otherstudies4,6,7 by describing the experience of fatigue asa representation and proximity of mortality. Usingfatigue as a reminder of uncertain mortality, providersshould be prepared to discuss death and dying ina patient-centered manner1,41-43 by (1) eliciting thepatients’ understanding of their illness, and if patientsare interested, providing information about the futureof their illness and prognosis; (2) addressing concernsand fears through empathic communication; and (3)involving family, other social support, or possibly otherproviders such as palliative care, mental health, orchaplaincy.
Limitations
The use of a nonprobability sample limits broadgeneralizations. This study included more men thanwomen, and a mix of New York Heart Associationclasses, but “expression of fatigue” as the focus meansthat participants self-selected according to on theirexperiences of fatigue. The study was performed in thecontext of identifying unmet needs, which could biasresponses, but participants were included in thisanalysis if fatigue was discussed as a symptom.
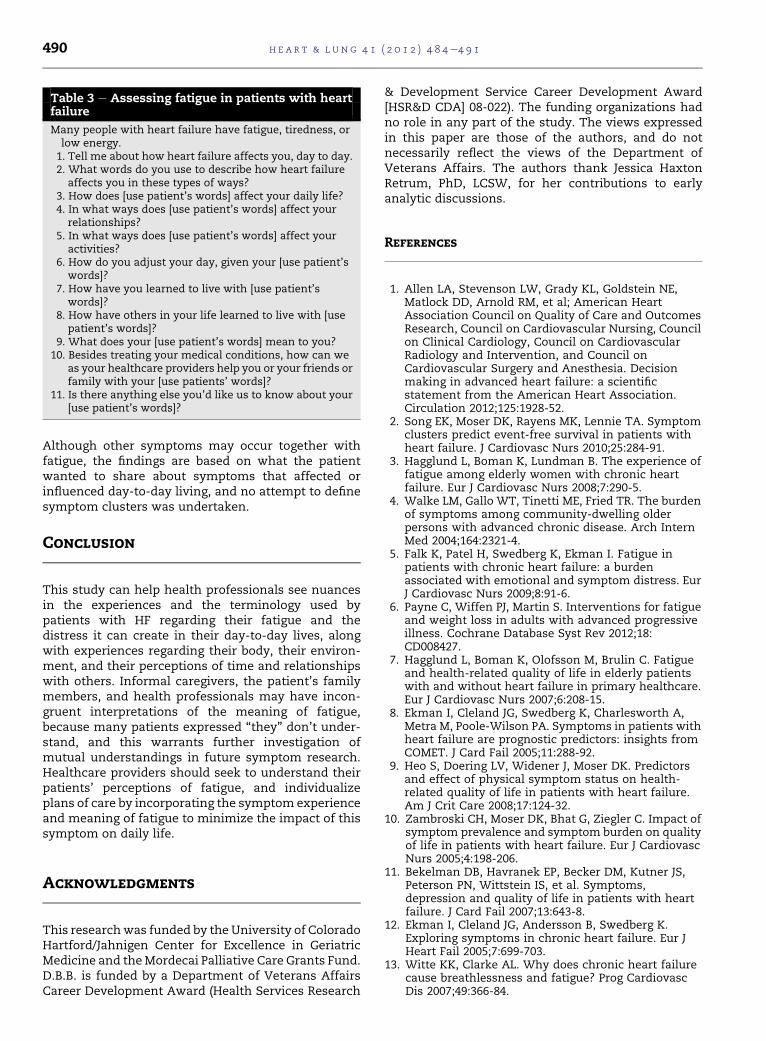
Table 3 e Assessing fatigue in patients with heartfailure
Many people with heart failure have fatigue, tiredness, orlow energy.1. Tell me about how heart failure affects you, day to day.2. What words do you use to describe how heart failure
affects you in these types of ways?3. How does [use patient’s words] affect your daily life?4. In what ways does [use patient’s words] affect your
relationships?5. In what ways does [use patient’s words] affect your
activities?6. How do you adjust your day, given your [use patient’s
words]?7. How have you learned to live with [use patient’s
words]?8. How have others in your life learned to live with [use
patient’s words]?9. What does your [use patient’s words] mean to you?
10. Besides treating your medical conditions, how can weas your healthcare providers help you or your friends orfamily with your [use patients’ words]?
11. Is there anything else you’d like us to know about your[use patient’s words]?
h e a r t & l ung 4 1 ( 2 0 1 2 ) 4 8 4e4 9 1490
Although other symptoms may occur together withfatigue, the findings are based on what the patientwanted to share about symptoms that affected orinfluenced day-to-day living, and no attempt to definesymptom clusters was undertaken.
Conclusion
This study can help health professionals see nuancesin the experiences and the terminology used bypatients with HF regarding their fatigue and thedistress it can create in their day-to-day lives, alongwith experiences regarding their body, their environ-ment, and their perceptions of time and relationshipswith others. Informal caregivers, the patient’s familymembers, and health professionals may have incon-gruent interpretations of the meaning of fatigue,because many patients expressed “they” don’t under-stand, and this warrants further investigation ofmutual understandings in future symptom research.Healthcare providers should seek to understand theirpatients’ perceptions of fatigue, and individualizeplans of care by incorporating the symptom experienceand meaning of fatigue to minimize the impact of thissymptom on daily life.
Acknowledgments
This researchwas funded by the University of ColoradoHartford/Jahnigen Center for Excellence in GeriatricMedicine and theMordecai Palliative Care Grants Fund.D.B.B. is funded by a Department of Veterans AffairsCareer Development Award (Health Services Research
& Development Service Career Development Award[HSR&D CDA] 08-022). The funding organizations hadno role in any part of the study. The views expressedin this paper are those of the authors, and do notnecessarily reflect the views of the Department ofVeterans Affairs. The authors thank Jessica HaxtonRetrum, PhD, LCSW, for her contributions to earlyanalytic discussions.
References
1. Allen LA, Stevenson LW, Grady KL, Goldstein NE,Matlock DD, Arnold RM, et al; American HeartAssociation Council on Quality of Care and OutcomesResearch, Council on Cardiovascular Nursing, Councilon Clinical Cardiology, Council on CardiovascularRadiology and Intervention, and Council onCardiovascular Surgery and Anesthesia. Decisionmaking in advanced heart failure: a scientificstatement from the American Heart Association.Circulation 2012;125:1928-52.
2. Song EK, Moser DK, Rayens MK, Lennie TA. Symptomclusters predict event-free survival in patients withheart failure. J Cardiovasc Nurs 2010;25:284-91.
3. Hagglund L, Boman K, Lundman B. The experience offatigue among elderly women with chronic heartfailure. Eur J Cardiovasc Nurs 2008;7:290-5.
4. Walke LM, Gallo WT, Tinetti ME, Fried TR. The burdenof symptoms among community-dwelling olderpersons with advanced chronic disease. Arch InternMed 2004;164:2321-4.
5. Falk K, Patel H, Swedberg K, Ekman I. Fatigue inpatients with chronic heart failure: a burdenassociated with emotional and symptom distress. EurJ Cardiovasc Nurs 2009;8:91-6.
6. Payne C, Wiffen PJ, Martin S. Interventions for fatigueand weight loss in adults with advanced progressiveillness. Cochrane Database Syst Rev 2012;18:CD008427.
7. Hagglund L, Boman K, Olofsson M, Brulin C. Fatigueand health-related quality of life in elderly patientswith and without heart failure in primary healthcare.Eur J Cardiovasc Nurs 2007;6:208-15.
8. Ekman I, Cleland JG, Swedberg K, Charlesworth A,Metra M, Poole-Wilson PA. Symptoms in patients withheart failure are prognostic predictors: insights fromCOMET. J Card Fail 2005;11:288-92.
9. Heo S, Doering LV, Widener J, Moser DK. Predictorsand effect of physical symptom status on health-related quality of life in patients with heart failure.Am J Crit Care 2008;17:124-32.
10. Zambroski CH, Moser DK, Bhat G, Ziegler C. Impact ofsymptom prevalence and symptom burden on qualityof life in patients with heart failure. Eur J CardiovascNurs 2005;4:198-206.
11. Bekelman DB, Havranek EP, Becker DM, Kutner JS,Peterson PN, Wittstein IS, et al. Symptoms,depression and quality of life in patients with heartfailure. J Card Fail 2007;13:643-8.
12. Ekman I, Cleland JG, Andersson B, Swedberg K.Exploring symptoms in chronic heart failure. Eur JHeart Fail 2005;7:699-703.
13. Witte KK, Clarke AL. Why does chronic heart failurecause breathlessness and fatigue? Prog CardiovascDis 2007;49:366-84.

h e a r t & l ung 4 1 ( 2 0 1 2 ) 4 8 4e4 9 1 491
14. Jessup M, Abraham WT, Casey DE, Feldman AM,Francis GS, Ganiats TG, et al. Focused update: ACCF/AHA guidelines for the diagnosis and management ofheart failure in adults: a report of the AmericanCollege of Cardiology Foundation/American HeartAssociation Task Force on Practice Guidelines.Circulation 2009;119:1977-2016.
15. Falk K, Swedberg K, Gaston-Johansson F, Ekman I.Fatigue is a prevalent and severe symptom associatedwithuncertaintyandsenseof coherence inpatientswithchronicheart failure.Eur JCardiovascNurs2007;6:99-104.
16. Norberg EB, Boman K, Lofgren B. Impact of fatigue oneveryday life among older people with chronic heartfailure. Aust Occup Ther J 2010;57:34-41.
17. Pozehl B, Duncan K, Hertzog M. The effects of exercisetraining on fatigue and dyspnea in heart failure. Eur JCardiovasc Nurs 2008;7:127-32.
18. Pozehl B, Duncan K, HertzogM, Norman JF. Heart failureexercise and training camp: effects of amulticomponentexercise training intervention in patients with heartfailure. Heart Lung 2010;39(Suppl 6):S1-13.
19. Freidman MM, King KB. Correlates of fatigue in olderwomen with heart failure. Heart Lung 1995;24:512-8.
20. Chen LH, Li CY, Shieh SM, Yin WH, Chiou AF.Predictors of fatigue in patients with heart failure.J Clin Nurs 2010;19:1588-96.
21. Smith ORF, Michielsen HJ, Pelle AJ, Schiffer AA,Winter JB, Denollet J. Symptoms of fatigue in chronicheart failure patients: clinical and psychologicalpredictors. Eur J Heart Fail 2007;9:922-7.
22. Smith OR, Kupper N, de Jonge P, Denollet J. Distincttrajectories of fatigue in chronic heart failure and theirassociationwithprognosis. Eur JHeart Fail 2010;12:841-8.
23. Smith OR, Denollet J, Schiffer AA, Kupper N, Gidron Y.Patient-related changes in fatigue over a 12-monthperiod predict poor outcome in chronic heart failure.Eur J Heart Fail 2009;11:400-5.
24. Volz A, Schmid JP, Zwahlen M, Kohls S, Saner H,Bart J. Predictors of readmission and health relatedquality of life in patients with chronic heart failure:a comparison of different psychosocial aspects.J Behav Med 2011;34:13-22.
25. Stephen SA. Fatigue in older adults with stable heartfailure. Heart Lung 2008;37:122-31.
26. Falk K, Granger BB, Swedberg K, Ekman I. Breaking thevicious circle of fatigue in patients with chronic heartfailure. Qual Health Res 2007;17:1020-7.
27. Paterson B, Canam C, Joachim G, Thorne S. Embeddedassumptions in qualitative studies of fatigue. West JNurs Res 2003;25:119-33.
28. Bekelman DB, Nowels CT, Retrum JH, Allen LA,Shakar S, Hutt E, et al. Giving voice to patients’ and
family caregivers’ needs in chronic heart failure:implications for palliative care programs. J Palliat Med2011;14:1317-24.
29. Steinhauser KE, Barroso J. Using qualitative methodsto explore key questions in palliative care. J PalliatMed 2009;12:725-30.
30. Mayan MJ. Essentials of qualitative inquiry. WalnutCreek, CA: Left Coast Press; 2009.
31. Thorne S. Interpretive description. Walnut Creek, CA:Left Coast Press; 2008.
32. Thomas DR. A general inductive approach foranalyzing qualitative evaluation data. Am J Eval 2006;27:237-46.
33. Dougherty CM, Pyper GP, Au DH, Levy WC,Sulivan MD. Drifting in a shrinking future: living withadvanced heart failure. J Cardiovasc Nurs 2007;22:480-7.
34. Freydberg N, Strain L, Tsuyuki RT, McAlister FA,Clark AM. “If he gives in, he will be gone.”: theinfluence of work and place on experiences, reactionsand self-care of heart failure in rural Canada. Soc SciMed 2010;70:1077-83.
35. Nordgren L, Asp M, Fagerberg I. Living with moderate-severe chronic heart failure as a middle-aged person.Qual Health Res 2007;17:4-13.
36. Welstand J, Carson A, Rutherford P. Living with heartfailure: an integrative review. Int J Nurs Stud 2009;46:1374-85.
37. Jeon YH, Kraus SG, Jowsey T, Glasgow NJ. Theexperience of living with chronic heart failure:a narrative review of qualitative studies. BMC HealthServ Res 2010;10:77.
38. Annema C, Luttik ML, Jaarsma T. Reasons forreadmission in heart failure: perspectives of patients,caregivers, cardiologists, and heart failure nurses.Heart Lung 2009;38:427-34.
39. Pattenden JF, Roberts H, Lewin RJ. Living with heartfailure: patient and carer perspectives. Eur JCardiovasc Nurs 2007;6:273-9.
40. Riegel B, Moser DK, Anker SD, Appel LJ, Dunbar SB,Grady KL, et al. State of the science: promotingself-care in persons with heart failure: a scientificstatement from the American Heart Association.Circulation 2009;120:1141-63.
41. Zambroski C, Bekelman DB. Palliative symptommanagement in patients with heart failure. ProgPalliat Care 2008;16:241-9.
42. Goodlin SJ. Palliative care in congestive heart failure.J Am Coll Cardiol 2009;54:386-96.
43. Tulsky JA. Beyond advanced directives: importance ofcommunication skills at the end of life. JAMA 2005;294:359-65.