the evolving paradigm of prehospital hemorrhage control ...johnmohler.com/documents/n. lyon co....
TRANSCRIPT

10/18/2017
1
3
John Mohler, RN, BSN, CFRN, CCRN
REACH Air – Elko, NV
Hemorrhage Control
Hemorrhage Control
The Evolving Paradigmof Hemorrhage Control
in the Prehospital Setting
A special thanks toJeffrey P. Salomone, MD, NREMT-P and
And Mike McElvoy, PhD, RN for theircontributions to this presentation
Blood Everywhere:How to Stop a Gusher

10/18/2017
2
An Overview
Tourniquets
Hemostatic agents or adjuncts
Other hemorrhage control devices
Permissive hypotenstion
Hypotensive resuscitation
Tranexamic Acid (TXA)
Freeze dried plasma
Resuscitation
Hemorrhage
Number ONE causeof preventabledeaths on thebattlefield
Old surgeon’s adage:
All bleeding stops. . .
10/18/2017
3
MARCH
Massive hemorrhage control
Airway
Respirations
Circulation
Hypothermia
Triage Life-Savers
1. Stop bleeding
2. Decompress tension pneumothorax
3. Insert nasopharyngeal airway
Every RBC Counts!
10/18/2017
4
Shock: 4 Kinds
Despite what you might read or hear, there areONLY four shock states:
1. Hypovolemic
2. Obstructive
3. Distributive
4. Cardiogenic
Normal Adult Blood Volume5 Liters
5 Liters Blood Volume
1 literby
volume
1 literby
volume
1 literby
volume
1 literby
volume
1 literby
volume

10/18/2017
5
ACS Classification of Acute Hemorrhage
Class % BloodLoss
Clinical Signs
I Up to 750ml (15%)
Slight increase in HR; no change inBP or respirations
II 750-1500ml (15-30%)
Increased HR and respirations;restlessness (anxiety, fright orhostility); [increased diastolic BP]
III 1500-2000ml (30-40%)
Increased HR and respirations; falling
systolic BP; significant AMS
IV >2000(>40%)
Severe tachycardia; severe BP;cold, pale skin; decreased LOC
2500 ml Blood Loss
2.5 Liters Blood Volume Left
2500 ml Blood Loss Mental State: Unconscious
Radial Pulse: Absent
Heart Rate: 140+
Systolic Blood pressure: Markedlydecreased
Respiratory Rate: Over 35
Is the patient going to die from this?
Probably

10/18/2017
6
So What’s the Problem?
Military
9% fatal bleeds are preventable
Civilian
10 million ED visits annually in US for externalhemorrhage
Definite advances have been made/are beingmade in hemorrhage control (both externaland internal)
CAUSES OF DEATH ON THE MODERNBATTLEFIELD: 2001-2005
COL John B. Holcomb, MAJ Lisa A. Pearse, CDR Jim Caruso, MimiLawnick RN, Charles E. Wade, Howard R. Champion
USAISR, AFMES, USUHS
Battlefield Deaths
Explosion57%
Aviation11%
GSW27%
MVC2%
Multi2%
Unk1%
n=413

10/18/2017
7
Potentially Preventable Deaths
n = 413
32% Compressible68% Non-compressible
Other2%
Causes of Preventable Deaths
Causes of Combat Wounds
(WWI, WWII, Korea, Vietnam, Middle East)
Fragments62%
Bullets23%
Burns6%
Blast3%
Other6%
10/18/2017
8
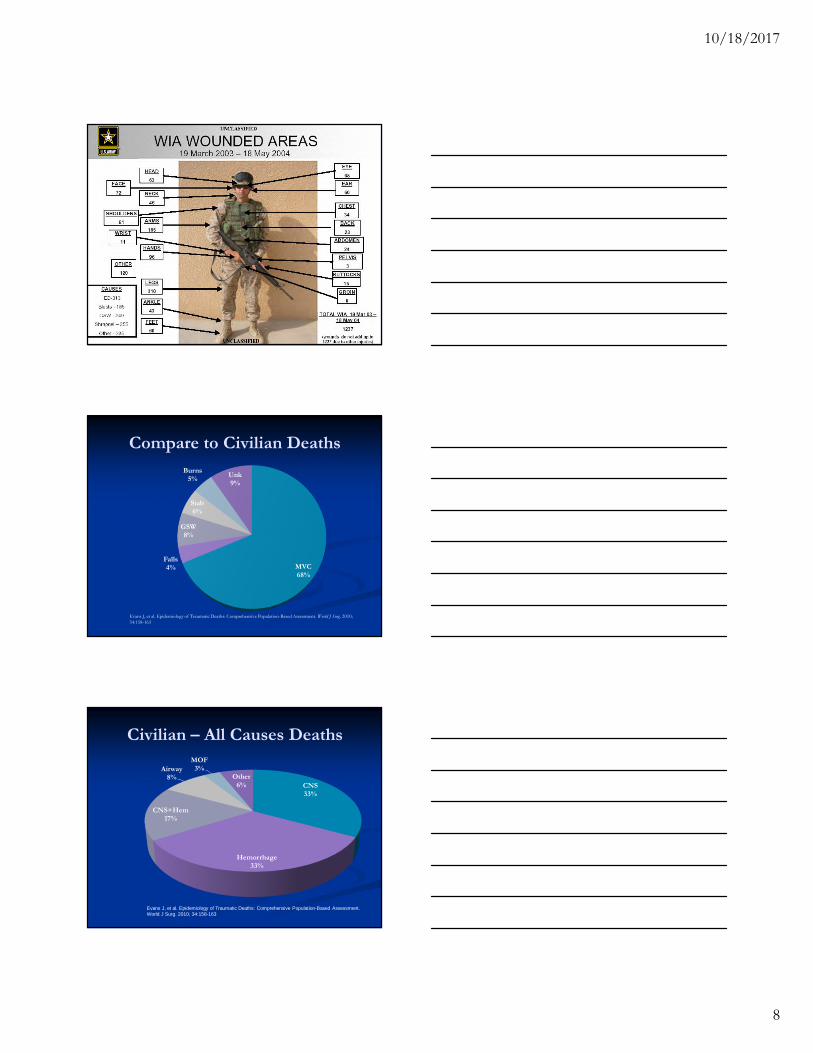
Compare to Civilian Deaths
MVC68%
Falls4%
GSW8%
Stab6%
Burns5%
Unk9%
Evans J, et al. Epidemiology of Traumatic Deaths: Comprehensive Population-Based Assessment. World J Surg. 2010;34:158-163
Civilian – All Causes Deaths
CNS33%
Hemorrhage33%
CNS+Hem17%
Airway8%
MOF3%
Other6%
Evans J, et al. Epidemiology of Traumatic Deaths: Comprehensive Population-Based Assessment.World J Surg. 2010; 34:158-163
10/18/2017
9
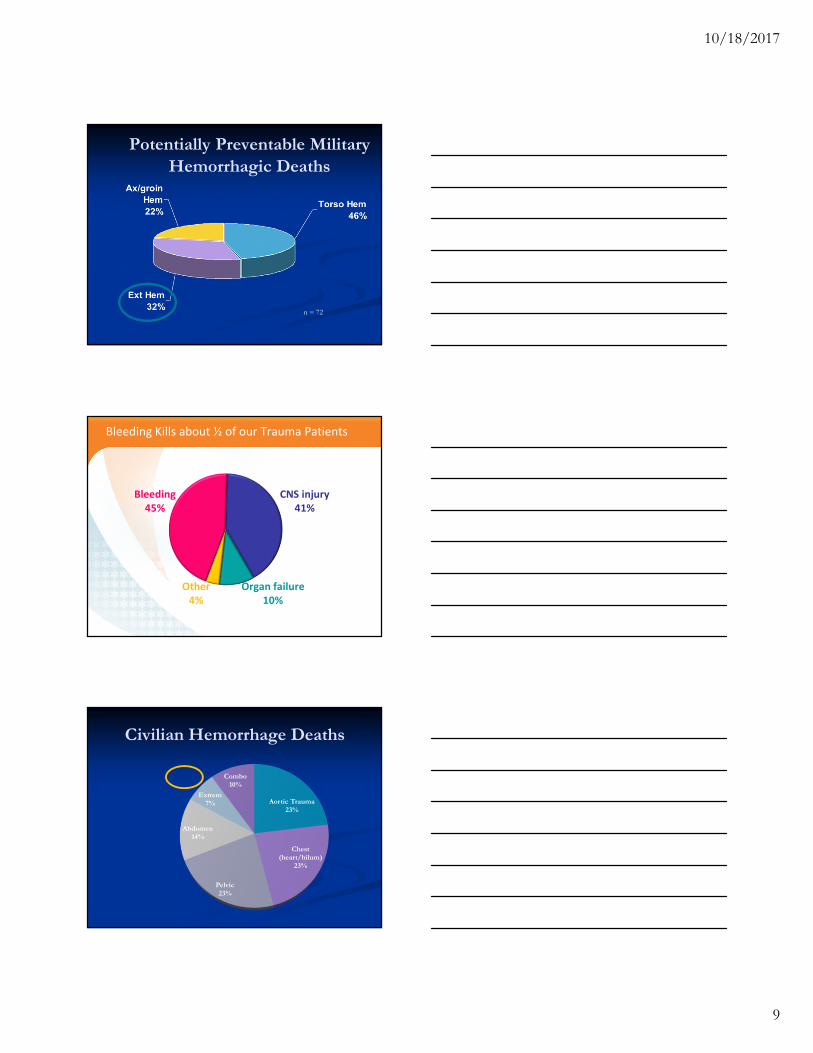
Potentially Preventable MilitaryHemorrhagic Deaths
n = 72
Bleeding45%
CNS injury41%
Organ failure10%
Other4%
Bleeding Kills about ½ of our Trauma Patients
Civilian Hemorrhage Deaths
Aortic Trauma23%
Chest(heart/hilum)
23%
Pelvic23%
Abdomen14%
Extrem7%
Combo10%

10/18/2017
10
Beyond Statistics
7 Caveats When ApplyingMilitary Literature
Different weapons Less pre-existing dehydration Shorter pre-hospital time Different surgical intervention More resources Better monitoring Less threatening environment
Hemorrhage control steps
Direct pressure
Elevation of extremity
Pressure points
Tourniquet as last resort

10/18/2017
11
Tourniquets should onlybe used as a last resortwhen all other methodsof hemorrhage control
fail.
DirectPressure
Hemorrhage related to transmural pressure
Difference between intraluminal and extraluminal(atmospheric) pressures
Direct pressure controls bleeding by:
Increases extraluminal pressure = decreasestransmural pressure
Decreases cross sectional area of opening
Direct Pressure
Controls MOSTbleeding
Size of vessels

10/18/2017
12
Pressure Dressing
Pressure dressingif limited manpower
Gauze sponges,roller bandage
Elastic bandage
10/18/2017
13
Israeli Trauma Dressing
ITS
ITD

10/18/2017
14
When direct pressure fails. . .
Elevation
Elevation may aggravatea fractured extremity
No published evidencedemonstrates thatelevation slowshemorrhage or that itdoesn’t
Pressure points?
10/18/2017
15
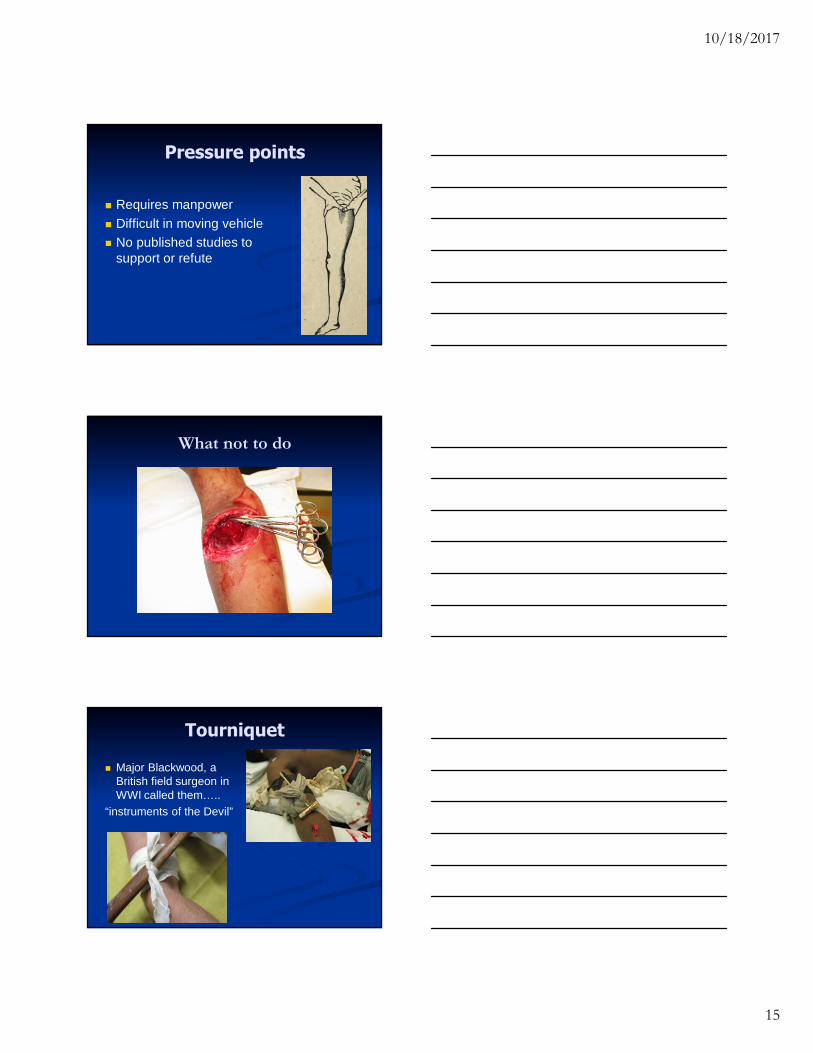
Pressure points
Requires manpower
Difficult in moving vehicle
No published studies tosupport or refute
What not to do
Tourniquet
Major Blackwood, aBritish field surgeon inWWI called them…..
“instruments of the Devil”

10/18/2017
16
Tourniquet
Tourniquets fell out offavor in the 60’s becauseof potential complications:
Inappropriate civilian use
Damage to nerves andblood vessels
Loss of the limb
Yet, used in ORs. . .
Safely used in surgery for hours (< 8)
Tourniquets
In military, evidencesuggests they mayprevent 7 out of 100combat deaths
Life over limb!

10/18/2017
17
Tourniquets- Devices
Spanish windlass created with cravat
Avoid narrow, bandlike material
Wider tourniquets more effective atcontrolling bleeding Inverse relationship between width and
pressure necessary to stop bleeding
Spanish Windlass
BP Cuff
10/18/2017
18
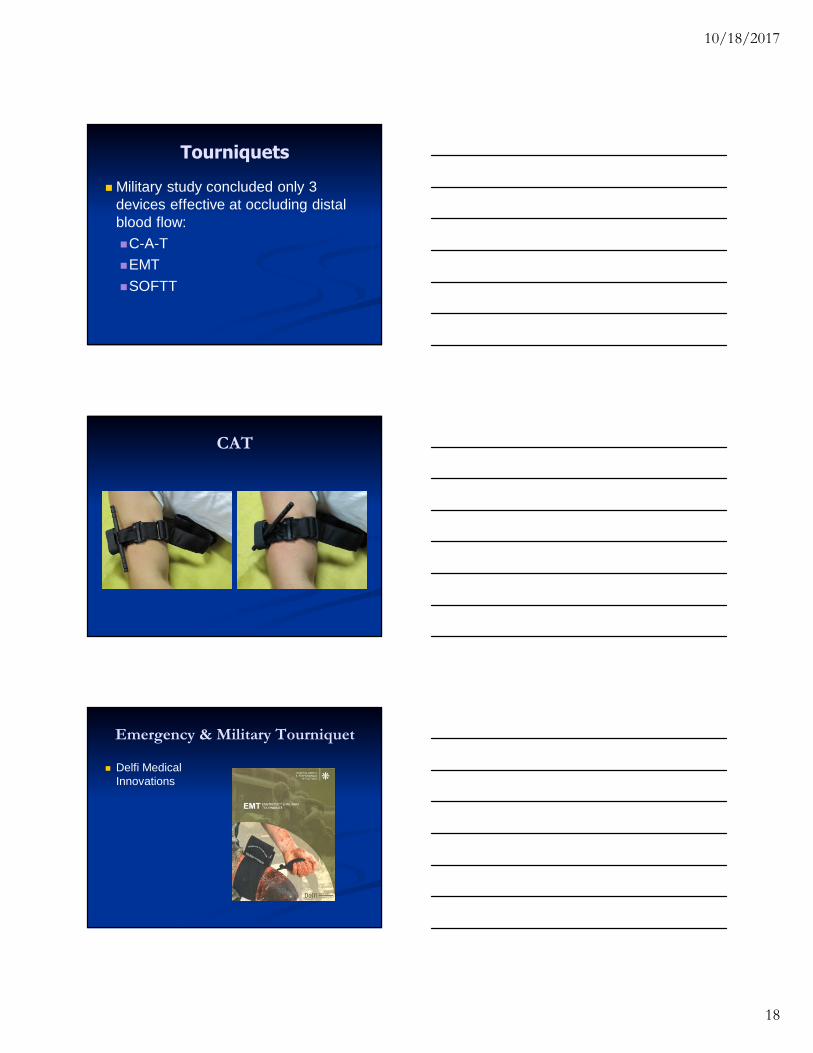
Tourniquets
Military study concluded only 3devices effective at occluding distalblood flow:
C-A-T
EMT
SOFTT
CAT
Emergency & Military Tourniquet
Delfi MedicalInnovations

10/18/2017
19
SOFT-T
10/18/2017
20
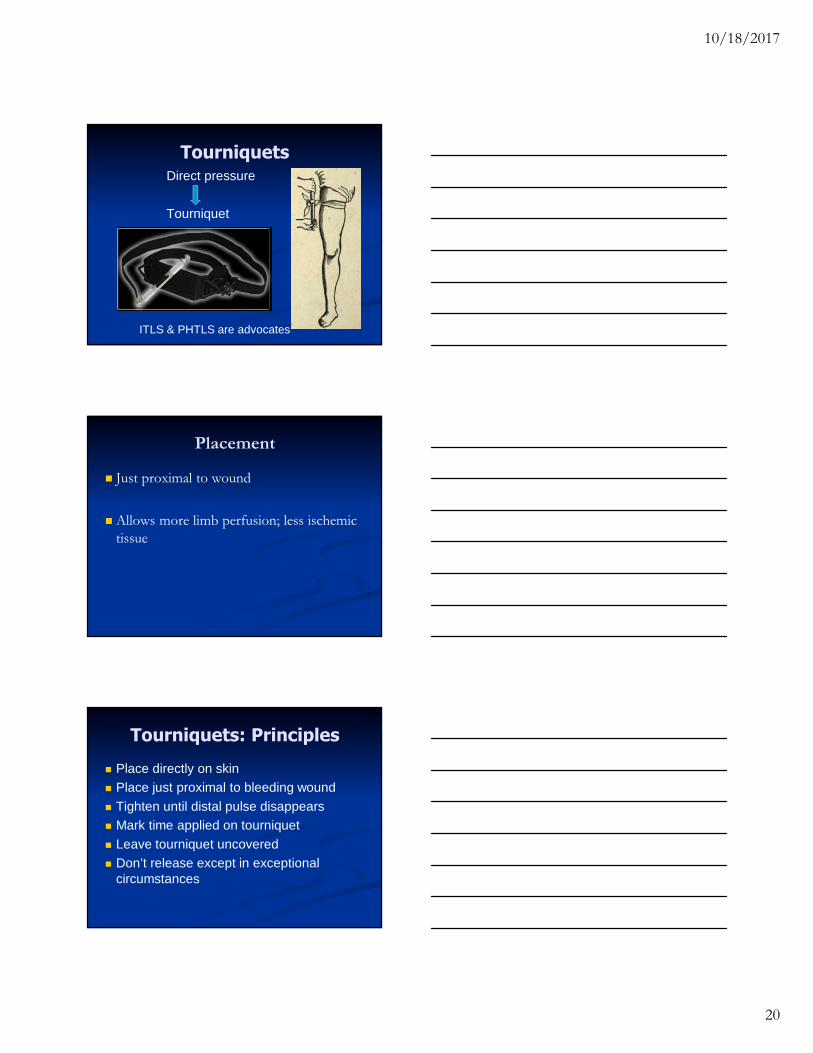
TourniquetsDirect pressure
Tourniquet
ITLS & PHTLS are advocates
Placement
Just proximal to wound
Allows more limb perfusion; less ischemictissue
Tourniquets: Principles
Place directly on skin
Place just proximal to bleeding wound
Tighten until distal pulse disappears
Mark time applied on tourniquet
Leave tourniquet uncovered
Don’t release except in exceptionalcircumstances

10/18/2017
21
Placement- Multiple wounds
Just proximal tomost proximalwound
Pitfalls- Inadequate control
Place second tourniquet more proximal
Pitfalls- Inadequate control
Ratchet tourniquet

10/18/2017
22
Pitfalls- Placement
Place directly on skin
Pitfalls- Placement
Pitfalls- Placement

10/18/2017
23
Break?
EMS Bleeding ControlOld
1. Direct Pressure
2. Elevation
3. Additional dressings
4. Pressure Point
5. Pressure dressing
6. Tourniquet
New
1. Direct Pressure
2. Tourniquet
OK, What About Non-tourniquetable Wounds?
10/18/2017
24
Non- tourniquet-ableHemorrhage
Groin / axilla
Torso
Neck
Face

10/18/2017
25

10/18/2017
26
Hemostatic Agents/Dressings The latest & greatest surgical advance
Continually evolving
Included in ITLS, PHTLS, ATLS, EMR, EMT
Available OTC
Hemostatic Dressing
Elevation helpful
Pressure points technically near impossible toproperly apply
Pressure dressings beneficial
Hemostatic dressings VERY helpful
Topical Hemostatic Agents
Military has extensively studied a number ofagents
Hemostatic dressing pad (Alltracel) Oxidized cellulose; physical effect (expansion)
ARC dressing (Am Red Cross) Human fibrinogen, thrombin, Factor XIII and
Ca
Hemostatin bandage (Anal. Contr. Systs) Propyl gallate (procoagulant)

10/18/2017
27
Topical Hemostatic Agents
Hemarrest dressing (Clarion Pharma.) Epsilon aminocaproic acid (antifibrinolytic) and
thrombin
Sorbstance microcaps (Hemostace LLC) Aluminum sulfate (astringent)
RDH (Marine Polymer Tech) Poly-N-acetyl glucosamine dressing (amino sugar
normally found in the body)
Military Experience
QuikClot®
Early versions very exothermic – up to 147°F(discontinued in 2008)
Difficult to debride
New Advanced Clotting Sponge (ACS)
Gauze sack – easily removed from wound
Prehydrated (reduces exothermic reaction)
Controls bleeding in 3 – 5 minutes
Can remain in place for up to 24 hours
Hemostatic Agents/Dsgs Compared
Military studies: Army (USAISR) & Navy (NMRC)

10/18/2017
28
Quik Clot
Combat Gauze
Gauze impregnated withKaolin clay Edible mineral used as
anti-caking agent inproducts
Rapidly effective
No heat generation
Moldable to wound
Now 1st Line per TCCC(because of preferencefor gauze like agent)
3-inch x 4-yard roll ofsterile gauze impregnatedwith kaolin. Activatesclotting factors andplatelets, absorbs water(increasing concentrationof platelets and clottingfactors at bleeding site)
REQUIRES TRAINING
Combat Gauze™

10/18/2017
29
Combat Gauze Directions (2)Pack Wound Completely
Military Choices
Committee on Tactical Combat Casualty Care(CoTCCC) QuikClot Combat gauze
HemCon
Marine Corps / Navy QuikClot
Combat Ready Clamp (CRoC)
SAM junctional Tourniquet
iTClamp
10/18/2017
30
Hemostatics- Summary
Experimental models don’t correlate well withinjuries encountered in civilian prehospitaltrauma care
Little civilian prehospital experience with anyagent
Cost effective +/-
Still require direct pressure to work-NOT A MAGIC BULLET!
Hemostatics- Summary
No evidence these agents aresuperior to direct pressure, apressure dressing or a tourniquet!!
Consider for non-tourniquetablehemorrhage
Hemorrhage Control Summary
Apply direct pressure with/without elevation
Elevation is potentially helpful to wounds of lowerleg and forearm
Consider hemostatic agents
Early for the subset of patients that bleeding can’t becompletely controlled with direct pressure andelevation

10/18/2017
31
Rapidly apply a tourniquet
Massive bleeding that isn’t controlled by DP &elevation
MCIs or tactical situations
To stop bleeding until triage is complete or it’s safe toevaluate the actual need for the tourniquet
Break?
Resuscitation
Permissive Hypotension
TXA
Damage Control Surgery
Other stuff

10/18/2017
32
Resuscitate
IV fluids in hypovolemic shock:
No survival, some mortality
Theories on IVF in trauma:
1. BP dislodges clots
2. BP = bleeding
3. IVF hemodilutes clotting factors
EMS/ED: Permissive HypotensionDuchesne JC et al. Damage Control Resuscitation: From Emergency Department to theOperating Room. The Amer Surgeon. 2011; 77: 201-206.
ResuscitatePermissive hypotension – allow SBP 90 (MAP
50 – 60 mmHg):
1. Bleeding controlled, no shock = no IVF
2. Bleeding controlled, shock 500 ml IVF(may repeat X 1)
3. Bleeding uncontrolled = no IVF
Ideal permissive hypotension < 90 min.
Severe damage when > 120 min.
Li T, et al. Ideal Permissive Hypotension to Resuscitate Uncontrolled Hemorrhagic Shock and theTolerance Time in Rats. Anesthesiology. 2011; 114 (1): 111-119.

10/18/2017
33
In bleeding trauma patients:
Coagulation occurs rapidly at the site of injury.
Fibrinolysis begins immediately to break downblood clots.
In patients with serious bleeding fibrinolysiscan be detrimental and occasionally pathologicin “hyperfibrinolysis”
Coagulation and Fibrinolysis
TXA is a lysine analogue (similarto aminocaproic acid, but about8 times more potent)
TXA binds to plasminogen’sLysine receptor site - blockingthe conversion of plasminogento Plasmin
The amount of Plasmin is thenreduced, so less Fibrin (clot)breakdown occurs
TXA Inhibits Fibrinolysis: Stabilizing Developing Clots
Bleeding45%
CNS injury41%
Organ failure10%
Other4%
Bleeding Kills about ½ of our Trauma Patients

10/18/2017
34
Patient enrolment
20,211 patients
in 40 countries
from 274 hospitals
CRASH2 Randomised Many Trauma Patients
Cause of death TXA Placebo Risk of death P value10,060 10,067
Bleeding 489 574 0.85 (0.76–0.96) 0.0077
Thrombosis 33 48 0.69 (0.44–1.07) 0.096
Organ failure 209 233 0.90 (0.75–1.08) 0.25
Head injury 603 621 0.97 (0.87–1.08) 0.60
Other 129 137 0.94 (0.74–1.20) 0.63
Any death 1463 1613 0.91 (0.85–0·97) 0·0035
Results
TXA worseTXA better
0.8 0.9 1.0 1.1
RR (95% CI)TXA (n= 10,060)
489 (4.9%)
Placebo (n= 10,067)
574 (5.7%)
Risk = 0.85 (0.76–0.96)2P=0.0077
Most of the Benefit is for Bleeding Deaths

10/18/2017
35
1.7 .8 .9 1.1 1.2 1.3 1.4 1.5
RR (99% CI) p=0.000008
≤1 hour 0.68 (0.54–0.86)
>1 to ≤ 3 hours 0.79 (0.60–1.04)
>3 hours 1.44 (1.04–1.99)
0.85 (0.76–0.96) P=.0077
For Bleeding Deaths – Early Treatment is Better
All Bleeding Patients
After the CRASH-2 trial, tranexamic acid was added to theWHO List of Essential Medicines (March 2011)
TXA is Now Being Used
The military are using tranexamic acid to treat combatcasualties:--they consider TXA a class 1a drug – to be given before fluids!
Tranexamic acid is being used in hospitals around the world
Tranexamic acid is being given in most UK ambulances as ofsummer (2011)
Tranexamic acid is being given in Oklahoma City, New YorkCity, the catchment area of Mayo Clinic, and in California AirAmbulance Patients (CALSTAR) as well as Care Flight
Tranexamic acid is safe and reduces mortality and bleeding insurgical patients
Millions of trauma patients die from bleeding every year
Millions of trauma patients require surgery
TXA for Trauma Patients?? CRASH - 2

10/18/2017
36
Aeromedical Use of TXA
PREHOSPITAL use of tranexamic acid for hemorrhagic shock in primary and secondaryaeromedical evacuationAuthors: E.N. Vu, R.S. Schlamp, R.T. Wand, G. Kleine-Deters, S.J. Wheeler, J.M. Tallon;Introduction:Major hemorrhage remains a leading cause of death in both military and civilian trauma. Wereport the use of a tranexamic acid (TXA) as part of a trauma exsanguination/massive transfusionprotocol in the management of hemorrhagic shock in a civilian primary and secondaryaeromedical evacuation (AME) helicopter EMS program.Methods:TXA was introduced into our critical care flight paramedic program in June of 2011. Indications for use includeage > 16 years, major trauma (defined a priori, based on mechanism of injury or findings on primary survey),and HR > 110 bpm or SBP < 90 mm Hg. Our protocol includes 24-hour online medical oversight, rapid initiationof transport, permissive hypotension in select patients, early use of blood products (secondary AME only), andinfusion of TXA while en route to a major trauma centre.
Results:Over a 4-month period, our CCP flight crews used TXA a total of 13 times. Patients had an average HR of 111bpm (95% CI 90. 71–131. 90), SBP of 91 mm Hg (95% CI 64. 48–118. 60), and GCS of 7 (95% CI 4. 65–9. 96). Forprimary AME, average response time was 33 minutes (95% CI 19. 03–47. 72), scene time was 22 minutes(95% CI 20. 23–24. 27), and time to TXA administration was 32 minutes (95% CI 25. 76–38. 99) from firstpatient contact. There were no reported complications with the administration of TXA in any patient.
Conclusions:We report the first successful integration of TXA into a primary and secondary aeromedical evacuation programin the setting of major trauma with confirmed or suspected hemorrhagic shock. Further studies are needed toassess the effect of such a protocol in this patient population on outcomes.
Resuscitate Is time important?
“Golden Hour”conceived by MarylandShock Trauma Center
No evidence basis inrepeated studies
Newgard CD, et al. Emergency Medical Services Intervalsand Survival in Trauma: Assessment of the “GoldenHour” in a North American Prospective Cohort. AnnEmer Med. 2010; 55(3): 235-260
Resuscitate Are there time critical trauma patients?
First rule of hemorrhage control =
Find the leak (you cannot control what youcannot see)
Shock without evidentbleeding requires
“Cold hard steel”
10/18/2017
37
Damage Control Surgery Central tenet: Avoid the “Deadly Triad”:
Hypothermia
Coagulopathy
Metabolic acidosis
Each condition worsens the others
Stop the bleeding
Remove major contaminants
Left open (avoid compartment syndrome)
“Pack ‘em and wrap ‘em”
Transfer to ICU
ICU Resuscitation1. Normalize blood pressure
2. Normalize body temperature
3. Normalize coagulation factors
4. Return to OR 12-18 hours for definitivesurgery

10/18/2017
38
Hippocrates
Above all, do nofurther harm
The Future?
Freeze dried Plasma
Whole blood transfusions
PCC’s (Prothrombin Complex Concentrate) likeKcentra
REBOA
Balloon tamponade of the aorta
Arsenal’s foam abdominal packing
EPR (Emergency Preservation andResuscitation) with 10* C hypothermia
Questions orThoughts?