the epidemiology of e. coli o157 in scotland – tip of the iceberg? kevin pollock
TRANSCRIPT

The epidemiology of E. coli O157 in Scotland – tip of the iceberg?
Kevin Pollock

Health Protection Scotland
"to improve the health of the Scottish population by providing the best possible information and expert support to practitioners, policy-makers and others on infectious and environmental hazards."
www.hps.scot.nhs.uk

Why am I here?
• Central Scotland E. coli O157 outbreak (1996)– 512 cases (279 lab-confirmed)– 34 cases of HUS– 17 deaths
• E coli O157 Task Force report• Creation of a surveillance system for E. coli
O157 and HUS to include both children and adults

What is surveillance?
‘the ongoing systematic collection, analysis and interpretation of appropriate data, and the timely dissemination of the resultant information to those who need to know’
adapted from: Langmuir AD. The surveillance of communicable diseases of national importance. New England Journal of Medicine, 1963, vol 268, pp 182-192

Factors which affect surveillance
• Laboratory testing policies• Notification vs reporting
– Anthrax vs Campylobacter
• Clinician bias to pathogens• Enhanced surveillance

Epidemiology
“The study of the distribution and determinants of health-related states or events in specified populations and the application of this study to control health problems”
1. Human disease does not occur at random2. Human disease has causal and preventive
factors that can be identified through systematic investigation of different populations or subgroups of individuals within a population in different places or at different times

Appears in national surveillance
Organisms identified
Specimens sent
Cases presenting
Cases of illness
Cases of infection
Laboratory Surveillance

Lab reports and under-ascertainment
The study of IID in England (1996) showed factor is:
3.8 for salmonella 10.3 for campylobacter 22.5 for rotavirus 315 for norovirus
i.e. if there were 1400 reported cases of norovirus in
2005 then Scotland experienced 315 x 1400 = 441,000 cases

E. coli O157
• Gram (-) rods, usually sorbitol-fermenting, part of the VTEC family
• Reservoir – cattle/livestock/humans• Can exist in a VBNC state – problems with
detection• Abdominal cramps, bloody diarrhoea, afebrile• May develop into the haemolytic uraemic
syndrome in 10-15% of cases resulting in kidney failure and possible death
• Patients should not be treated with antibiotics

Orkney 15.4
Shetland 0.0
Western Isles 0.0 Highland 0.9
Greater Glasgow 0.8
Grampian 9.0
Lanarkshire 1.4
Tayside 3.6
Ayrshire & Arran 3.8
Argyll & Clyde 4.6Fife 2.0Forth Valley 2.1
Lothian 2.8
Borders 8.2
Dumfries & Galloway 9.5
Scotland 3.4
0 - 2.5
2.6 - 5.0
> 5.0
E.coli O157: NHS Board of Reporting Laboratory 2007

0
2
4
6
8
1 0
1 2
1 9 8 4 1 9 8 6 1 9 8 8 1 9 9 0 1 9 9 2 1 9 9 4 1 9 9 6 1 9 9 8 2 0 0 0 2 0 0 2 2 0 0 4 2 0 0 6
Ca
se
s p
er
10
0,0
00
po
pu
lati
on
S c o tla n d
E n g la n d & W a le s
N Ire la n d
Ire la n d
D a ta fro m o u tw ith S c o tla n d c o u rte s y o f H e a lth P ro te c tio n A g e n c y B e lfa s t & L o n d o na n d H e a lth P ro te c tio n S u rv e illa n c e C e n tre D u b lin (2 0 0 7 fig u re s a re p ro v is io n a l)
E.coli O157: rates per 100,000 population 1984-2007

E. coli O157/HUS in children

E. coli O157/HUS in adults

Progression of E. coli O157 (VTEC)
Tarr et al. 2005, Lancet; 365: 1073-1086.


How important?
Of 200-300 reported cases per year in Scotland:• ~ 2-3 die• 80-85% are sporadic infections• 70% have bloody diarrhoea• 50% are admitted hospital• 20% are in hospital for over a week• 10-15% have HUS (20-35 cases)• 90% of HUS cases are under 16• Potential for devastating outbreaks…….

Recent selected outbreaks
• 1996, Scotland, butcher– 512 cases, 17 deaths
• 1996, Japan, school meals– 10,000 cases, 11 deaths
• 2000, Canada, mains water– 1300 cases, 6 deaths
• 2005, Wales, school meals– 158 cases, 1 death

The Microbiological Safety of Food
Part II 1991
“We see poultry and their products as the most important source of human gastrointestinal infections arising from food.”
Spinach outbreak, USA, 2006
• Cases of E. coli O157 in 26 different states in USA reported eating fresh spinach (95% of cases)– 183 cases– 92 hospitalised– 29 had HUS– 1 person died
• E. coli O157 with a PFGE pattern matching the outbreak strain isolated from three open packages of fresh spinach consumed by cases (1 from New Mexico, 1 from Utah, and 1 from Pennsylvania)
• Spinach grown in California was implicated in the outbreak – same strain found in feral swine nr spinach fields
Jay et al. Emerg Infect Dis. 2007 Dec;13(12):1908-11.
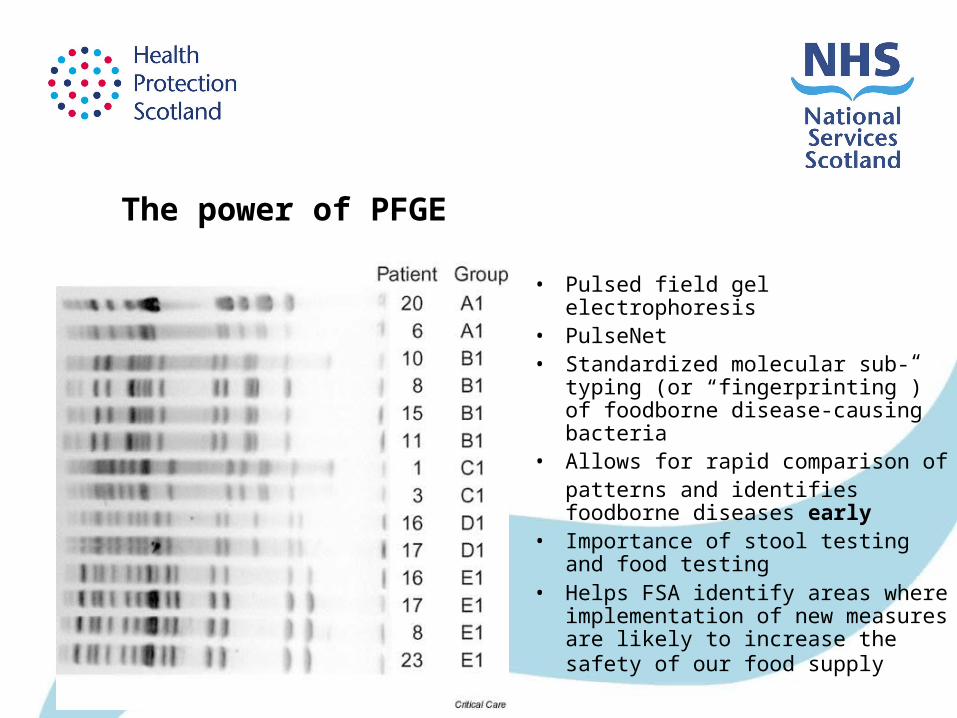
The power of PFGE
• Pulsed field gel electrophoresis• PulseNet• Standardized molecular sub-
typing (or “fingerprinting”) of foodborne disease-causing bacteria
• Allows for rapid comparison of patterns and identifies foodborne diseases early
• Importance of stool testing and food testing
• Helps FSA identify areas where implementation of new measures are likely to increase the safety of our food supply

Morrison’s outbreak, Paisley - 2007
• 9 cases associated with meat delicatessen• All cases confirmed phage type 2• 1 fatality - 66-year old female• No other cases associated with consumption of
cold cooked meats from Morrison’s UK-wide• Hypothesis - cross-contamination of various cold
cooked meats at the particular delicatessen • Fatal accident enquiry

Aberdeen outbreak, 2007
• 9 confirmed cases associated with hotel and social club• 1 case hospitalised• EHOs investigated kitchen and routines• Microbiological sampling of foodstuffs including cold
cooked meats, coleslaw, salad leaves• All samples negative for E. coli O157• 7 out of 10 people from club consumed cold meat
platter• Descriptive epidemiology estimates salad part of
platter as being suspect vehicle – previously washed in salted water – now washed in disinfectant solution
• PFGE not used hence descriptive


Unpasteurised cheese
• Precedent of Listeria in Lanark Blue• Are all unpasteurised cheeses labelled
so?• Cheese boards in restaurants – labelling?• Cluster of cases of haemolytic uraemic
syndrome due to unpasteurised cheese– Deschenes et al. (1996) Pediatr
Nephrol, 10

How are the VTECs being transmitted?
• 50% of cases unknown transmission• EHO reports of farm contact (p< 0.001)• EHO reports of person-person spread (p<
0.001)• Small no. of reports of food as source of
infection (pre-2007) – not statistically significant
• Private water supplies – theoretical but actual?

Haemolytic uraemic syndrome (HUS)
• Characterised by microangiopathic haemolytic anaemia with red blood cell destruction and fever
• Variable neurological involvement• Variable renal impairment• Acute onset, often fatal and difficult to
diagnose• 85-90% cases associated with VTEC

Aims of ENSHURE
• Clinically driven system• Combines info on short-term and long-term outcomes,
clinical management and treatment of HUS/TTP• Provides data to enable future prevention and
management including» Epidemiology» Clinical parameters» Social outcomes of infection

Clinical markers for HUS and TTP
Clinical markers HUS TTP Significance
Length of stay in hospital (days)
14 +/- 1.5 21 +/- 3 P< 0.02
Lactate Dehydrogenase (LDH)
4864 +/- 588
2411 +/- 512
P= 0.006
Serum albumin 27.4 +/- 0.9 32.7 +/- 1.7 P= 0.017
C-reactive protein (CRP)
56.3 +/- 9.2 80 +/- 25.4 P= 0.305
Neutrophil count 14.9 +/- 1.0 12.2 +/- 1.2 P= 0.238
White blood cell (WBC) count
19.8 +/- 1.1 14 +/- 1.1 P= 0.021
Anuria (days) 10.4 +/- 2.5 8.1 +/- 1.6 P= 0.692

Treatment and initial outcomes of HUS
• Treatment of HUS cases with NSAIDs sig. associated with renal impairment and death (p< 0.001)
• Treatment of HUS cases with antibiotics sig. associated with dialysis dependence (p< 0.03)
• 71% ‘recovered’• 14% had renal impairment
- half of these are dialysis-dependent• 8% had neurological impairment• 7% deaths

How did the illness affect patients/relatives?
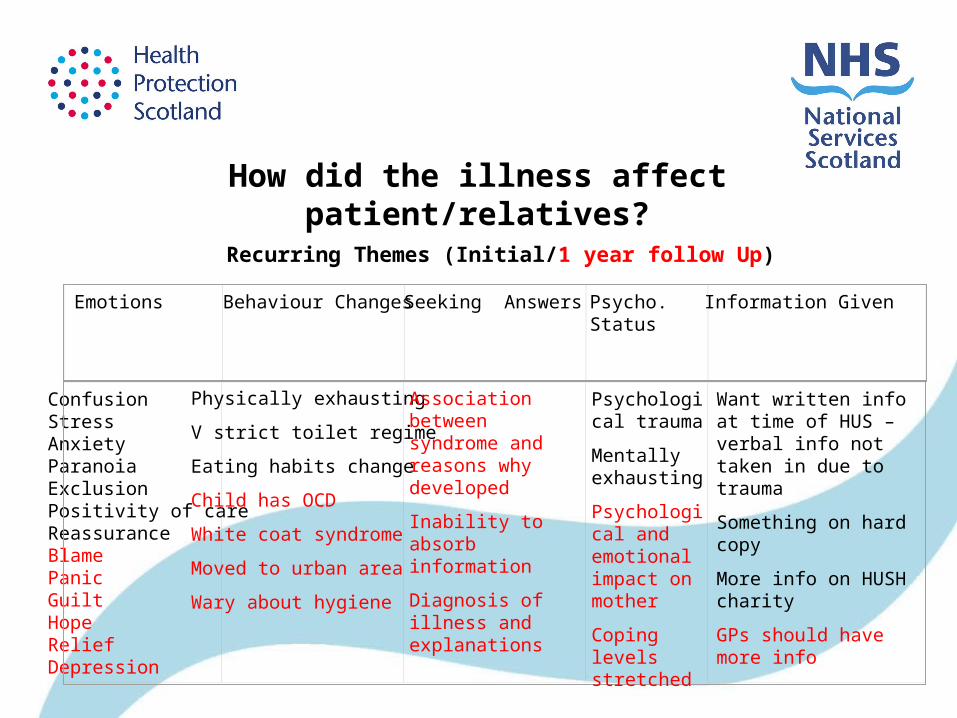
How did the illness affect patient/relatives?
Recurring Themes (Initial/1 year follow Up)
Emotions Behaviour ChangesSeeking Answers Psycho. Status
Information Given
ConfusionStressAnxietyParanoiaExclusionPositivity of careReassuranceBlamePanicGuiltHopeReliefDepression
Physically exhausting
V strict toilet regime
Eating habits change
Child has OCD
White coat syndrome
Moved to urban area
Wary about hygiene
Association between syndrome and reasons why developed
Inability to absorb information
Diagnosis of illness and explanations
Psychological trauma
Mentally exhausting
Psychological and emotional impact on mother
Coping levels stretched
Want written info at time of HUS – verbal info not taken in due to trauma
Something on hard copy
More info on HUSH charity
GPs should have more info

Conclusions
• VTEC/HUS surveillance less artefactual – enhanced system
• Farm/rural contact important mode of transmission of VTEC
• Foodborne E. coli O157 still poses a public health threat
• Ready-to-eat produce unlikely source of infection• Severity of HUS illness and psychological effects
upon family are devastating• Vigilance over potential sources for testing - PFGE

Patient presents with diarrhoea
Is it likely to be infectious?
Is it grossly bloody?
Is the patient:
• Under 15 years of age
• Over 60 years of age
• Suffering severe abdominal pain
• Contact of a likely case
Has the ID physician/paediatrician advised admission?
Admit to hospital
No
No
No
No
No
Yes
Yes
Consider sending stool and enquireabout associated cases and biologically
plausible exposures
Almost certainly not E coli O157
Probably not E coliO157
Yes
Send stool and report to PHPU
Unlikely to result in HUS but observe for 24 hours
Yes
Yes
Consult with ID physician/paediatricianover risk of HUS developing
Follow consultant advice
Patient presents with diarrhoea
Is it likely to be infectious?
Is it grossly bloody?
Is the patient:
• Under 15 years of age
• Over 60 years of age
• Suffering severe abdominal pain
• Contact of a likely case
Has the ID physician/paediatrician advised admission?
Admit to hospital
No
No
No
No
No
Yes
Yes
Consider sending stool and enquireabout associated cases and biologically
plausible exposures
Almost certainly not E coli O157
Probably not E coliO157
Yes
Send stool and report to PHPU
Unlikely to result in HUS but observe for 24 hours
Yes
Yes
Consult with ID physician/paediatricianover risk of HUS developing
Follow consultant advice