the effects of ankle appliances on lower … · · 2017-12-19the effects of ankle appliances on...
TRANSCRIPT

1 Ankle appliances during back squats
THE EFFECTS OF ANKLE APPLIANCES ON LOWER BODY JOINT ANGLES IN THE SAGITTAL PLANE DURING THE BACK SQUAT
Travis J. Merritt,1 Eric V. Swafford,1 Christopher L. Kliethermes,2 David S. Senchina1
1 Biology Department, Drake University, Des Moines, IA 2 Psychology Department, Drake University, Des Moines, IA
ABSTRACT
Merritt TJ, Swafford EV, Kliethermes CL, Senchina DS. The Effects of Ankle Appliances on Lower Body Joint Angles in the Sagittal Plane during the Back Squat. Journal of Undergraduate
Kinesiology Research 2014; (10)1:1-13. Purpose: Ankle appliances are common prophylactic
measures or treatments for ankle injuries employed in athletics. It is unknown whether ankle appliances might be therapeutically useful to injured athletes gradually returning to exercises such as the back squat. The primary objective of this study was to determine if standard ankle appliances influenced hip, knee, or ankle joint angles in the sagittal plane during standard back
squat. Methods: Twenty-four healthy males (12 college football players and 12 non-football
trained individuals) performed back squats at 50% 1RM in five ankle conditions: shoes with standard tape job, standard lace brace, Figure-8 brace, or ASO brace; and shoes alone (control). Ankle, knee, and hip joint angles were measured by video analysis before, at the bottom of, and after the squat. Subjects self-reported perceived comfort, exertion, and stability
after completing all squats for each condition. Results: No significant differences were seen in
joint angles between any of the appliances or control during any phase; however, significant
differences were seen between football and non-football groups in specific joint time point combinations. While there were no significant differences in self-reports of perceptual measures between ankle appliances or control, non-football subjects indicated a higher exertion score than football subjects. Findings between subject groups are likely explained by back
squat technique differences. Conclusion: Results suggest that common ankle appliances
have negligible effects on movements in the sagittal plane or on perceptions of foot proprioception during the back squat.
Key Words: ankle; ASO brace; brace; Figure-8 brace; hip; knee

2 Ankle appliances during back squats
INTRODUCTION
Ankle injuries are common in athletics (1,2). In collegiate athletics alone, almost 15% of all sports injuries may be related to the ankle (3). Various ankle appliances from braces to taping have been used in a prophylactic and post-injury capacity (4–7). The primary function of these appliances is to reduce range of motion (ROM) in the frontal plane (e.g., inversion and eversion) to promote ankle stability (8,9), which decreases the likelihood of ankle injuries (10). While the effect of ankle appliances on ROM in the frontal plane is fairly clear, their effects on ROM in the sagittal plane effects are less understood (11). Sagittal plane restriction may be deleterious if it causes a decrease in performance, or if restriction at one site (e.g. the ankle) causes biomechanically stressful compensations at other sites (e.g., the knee or hip). Research involving jump-landings shows a decrease in angle displacement at the ankle, knee, and hip in braced conditions compared to non-braced conditions (11–13). Ankle braces or ankle taping have been shown to decrease sagittal ROM in cutting, running, and sidestepping tasks (14–16). On the other hand, other studies utilizing similar movements such as running and volleyball-specific drills, and similar ankle appliances, have shown no effect of sagittal plane ROM (17–20). It has been proposed that differing types of ankle appliances or experimental protocol differences may be the cause for the conflicting data (21). Alternatively, factors such as the type of athlete or type of activity being performed are also possible explanations for the conflicting data. If ankle appliances can reduce sagittal plane movements, then they may have therapeutic benefits for athletes who suffered an ankle injury and are gradually returning to their training programs. No literature exists to address this question. The back squat offers a good model for examining this question because its kinematic chain is largely (though not exclusively) limited to the sagittal plane, and it is an exercise that involves resistance. The purpose of this study was to investigate the effects various ankle appliances had on lower body sagittal plane ROM during the back squat. It was hypothesized that ankle appliances would restrict ankle ROM in the sagittal plane during the back squat sufficiently to prompt a compensatory increase in either knee and/or hip ROM during the standard back squat.
METHODS
Participants This study was approved by the Drake Institutional Review Board as IRB ID 2011-12030. Twenty-four males gave written informed consent and completed the entire protocol. To examine the possible influence of squat technique in this experimental model, the twenty-four subjects were divided into two equal groups: 12 intercollegiate football players (who regularly performed back squats as part of their training regimen) and 12 non-football athletes (for whom back squats were a minor or non-existent training element). Subjects were reminded of proper form for back squats before exercise. To facilitate accurate video detection of body landmarks, subjects were fitted
3 Ankle appliances during back squats
with black compression shirts and shorts (Nike Pro Combat; Nike, Inc.). To control for possible confounding effects due to variation in inter-subject footwear, all subjects were given a new pair of black crew socks (Body Glove, Inc.) and wore identical pairs of either size 11 or 13 athletic shoes (Nike Air Max Skyline; Nike, Inc.); thus, shoe size was an inclusion factor for this study.
Baseline Testing and Instrumentation One-repetition maximum (1RM) was determined using standard procedures and conversion charts (National Academy of Sports Medicine) before the experiment started. Baseline assessments taken at the time of the experiment included height, weight, body fat percentage, and basal metabolic rate (BMR). Height and weight were determined on a physician’s scale (Health-o-Meter, Sunbeam Products, Inc.) Body fat percentage and BMR were determined with the BodyStat 1500 (Body Stat Inc.) which uses bioelectrical impedance analysis from the hand through the foot.
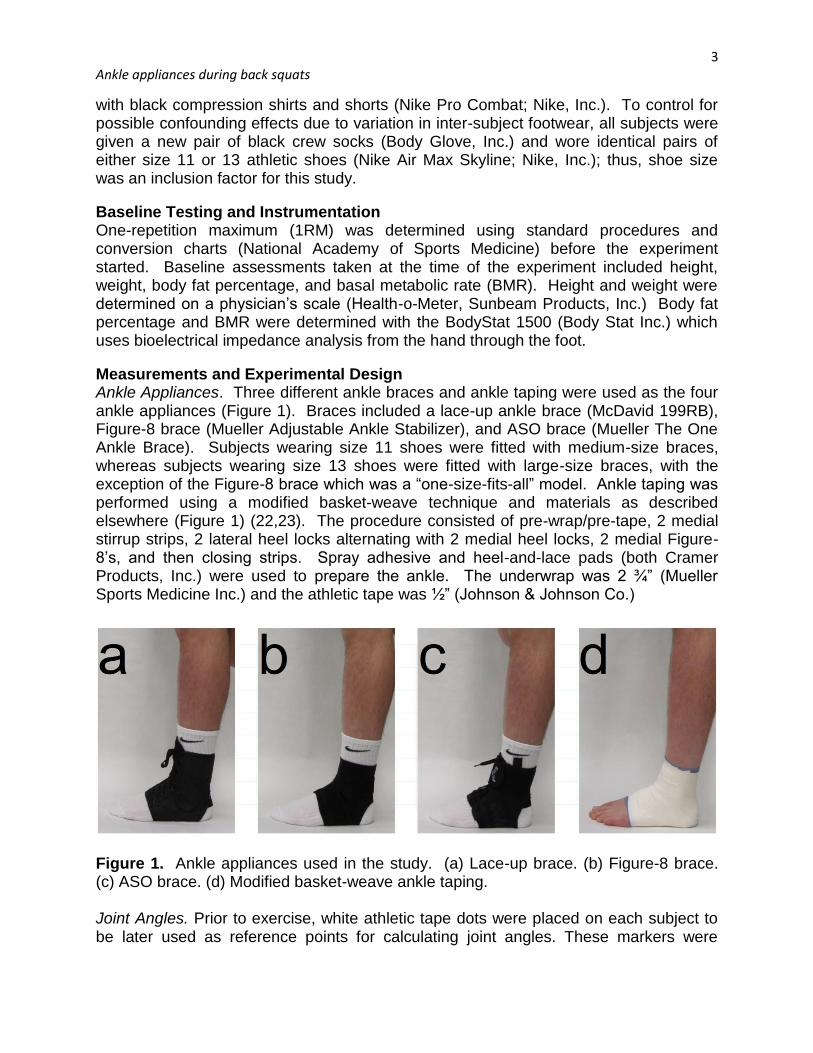
Measurements and Experimental Design Ankle Appliances. Three different ankle braces and ankle taping were used as the four ankle appliances (Figure 1). Braces included a lace-up ankle brace (McDavid 199RB), Figure-8 brace (Mueller Adjustable Ankle Stabilizer), and ASO brace (Mueller The One Ankle Brace). Subjects wearing size 11 shoes were fitted with medium-size braces, whereas subjects wearing size 13 shoes were fitted with large-size braces, with the exception of the Figure-8 brace which was a “one-size-fits-all” model. Ankle taping was performed using a modified basket-weave technique and materials as described elsewhere (Figure 1) (22,23). The procedure consisted of pre-wrap/pre-tape, 2 medial stirrup strips, 2 lateral heel locks alternating with 2 medial heel locks, 2 medial Figure-8’s, and then closing strips. Spray adhesive and heel-and-lace pads (both Cramer Products, Inc.) were used to prepare the ankle. The underwrap was 2 ¾” (Mueller Sports Medicine Inc.) and the athletic tape was ½” (Johnson & Johnson Co.)
Figure 1. Ankle appliances used in the study. (a) Lace-up brace. (b) Figure-8 brace. (c) ASO brace. (d) Modified basket-weave ankle taping. Joint Angles. Prior to exercise, white athletic tape dots were placed on each subject to be later used as reference points for calculating joint angles. These markers were

4 Ankle appliances during back squats
placed on the right side of the body facing the camera so sagittal plane joint angle could be determined. Five locations were marked (Figure 2): distal head of the fifth metatarsal as palpated through the shoe, lateral malleolus of the fibula (ankle), lateral condyle of the tibia (knee), greater trochanter of the femur (hip), and the end of the barbell (as a proxy for the shoulder because the plates obscured visualization of the shoulder directly). Three different angles could be determined using the five marks. For each angle, three different marks were used; lines were drawn between two adjacent markers, and the angle between those lines was computed. The lines for the ankle angle were fifth metatarsal head to lateral malleolus, and lateral malleolus to lateral condyle. The lines for the knee angle were lateral malleolus to lateral condyle, and lateral condyle to greater trochanter. The lines for the hip angle were lateral condyle to greater trochanter, and greater trochanter to barbell marker (representing the lateral edge of the shoulder). Subjects were imaged with the use of a Canon Power Shot A2200 digital video recorder sampling at 32 frames/second. Images were obtained in the sagittal plane. A tripod was used to ensure consistency between images. At the beginning of each film, subjects held a yardstick vertically to the ground as a standard for length. All video analysis was performed with the built-in angle tool of Image J (version 1.45). Angles were measured at three time points during the squat: the start of descent (frame before the break of the knee), hold (lowest point of the squat based on head of femur), and stop of ascent (frame after fullest extension of knee).
Figure 2. Tape marks for calculating joint angles. (a) Lower body markers (from top to bottom): hip marker (on femur greater trochanter), knee marker (on tibia lateral condyle), ankle marker (tibia lateral malleolus), and distal head of the fifth metatarsal as

5 Ankle appliances during back squats
palpated through the shoe. (b) The end of the bar was used to mark the shoulder, as the weight plates obscure the shoulder from being viewed in the sagittal plane. Perceptual. Subjects were asked to rate their perceptions of ankle comfort and stability separately after each set performed in the various ankle appliances using a 10-cm visual analogue scale (VAS; Mills et al. 2010). Subjects were shown a solid line with two terms on either end. They were then asked to make a vertical mark on the line denoting their perceived comfort or stability. The comfort scale was anchored with the terms “very uncomfortable” on the far left and “very comfortable” on the far right; similarly the stability scale had the terms “ very unstable” on the far left and “very stable” on the far right. Subjects were presented a new sheet each time and given the two scales separately to deter any influence between the two. At the same time, subjects were also asked to rate their perceived exertion (RPE) using the standard 6-20 point scale. Procedures After subject preparation, subjects completed six sets of back squats, with each set consisting of three repetitions at 50% 1RM; thus, each subject performed a total of 18 squats during the course of the experiment. Five different ankle conditions were used across the six sets. The first and last (sixth) sets were always fixed as control (shoes only). The second through fifth sets were randomized such that subjects performed squats in shoes plus one of the four ankle appliances as described above. The second through fifth sets were arranged in a counterbalanced fashion to eliminate any potential for treatment order or fatigue effects. Subject movements during the squat were directed verbally by one of the researchers. After donning the barbell and assuming a starting position, a “down” call was given. Subjects descended into the squat and held their thighs parallel to the floor for one second; some of the non-football subjects could not reach this depth, in which case they were brought to the full depth of their squat while still keeping their heels planted. Then, an “up” call was given to return to an upright position. Subjects were told to rack the barbell between repetitions; this procedure was repeated three times for each treatment with a rest period between repetitions to ensure proper recovery between reps. At the end of each set, subjects were asked to complete the comfort VAS, then the stability VAS, then the RPE scale, always in that order. Given the complexity of image analysis, joint angles were determined from only the second repetition of each treatment. Statistical Analyses Two-way analysis of variance (ANOVA) was used with ankle treatment and football/non-football status as the two factors (SPSS PASW 19.0; IBM, Inc.). The joint angle data
was partitioned into 9 groups (3 joints 3 time points) and each joint-time point group was analyzed separately with joint angle being the dependent variable. For the perceptual analysis, the data on comfort, stability, and RPE data was analyzed separately with the subjects’ ranking being the dependent factor. Differences were considered significant at a p<0.05 level.
6 Ankle appliances during back squats
RESULTS
Subject Characteristics
Football players had significantly greater mass (94.0 2.1 kg; p=0.016) and higher BMR
(2398 70 kcal; p=0.023) than the non-football athletes in the study (80.4 3.2 kg and
2142 76 kcal, respectively; Table 1). The two groups were not significantly different in terms of age, height, or body composition. Table 1. Anthropometric characteristics of the subjects. Values are expressed as means ± standard error. BMR=basal metabolic rate.
Football Non-Football
Age (yr) 19.6 ± 0.3 23.0 ± 1.7 Height (cm) 182.0 ± 2.1 183.3 ± 1.6 Weight (kg) 94.0 ± 4.1* 80.4 ± 3.2 % body fat 14.6 ± 1.3 14.8 ± 1.3 BMR (kcal) 2398 ± 70* 2142 ± 76
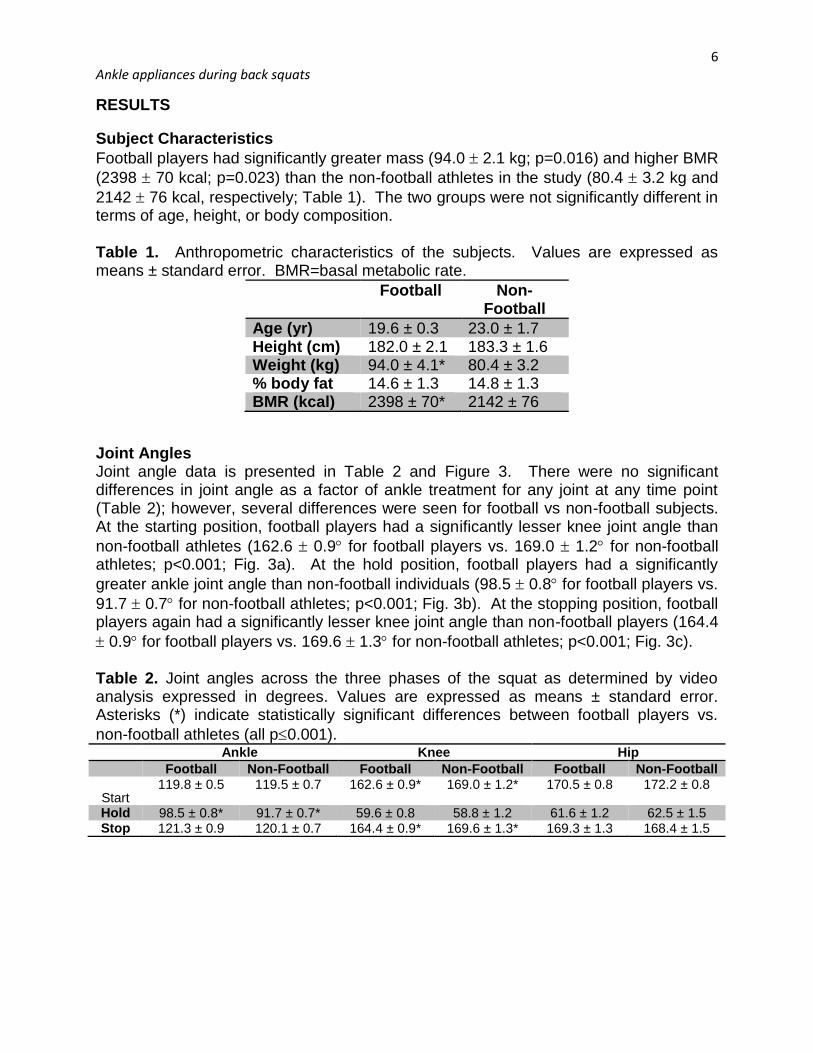
Joint Angles Joint angle data is presented in Table 2 and Figure 3. There were no significant differences in joint angle as a factor of ankle treatment for any joint at any time point (Table 2); however, several differences were seen for football vs non-football subjects. At the starting position, football players had a significantly lesser knee joint angle than
non-football athletes (162.6 0.9 for football players vs. 169.0 1.2 for non-football athletes; p<0.001; Fig. 3a). At the hold position, football players had a significantly
greater ankle joint angle than non-football individuals (98.5 0.8 for football players vs.
91.7 0.7 for non-football athletes; p<0.001; Fig. 3b). At the stopping position, football players again had a significantly lesser knee joint angle than non-football players (164.4
0.9 for football players vs. 169.6 1.3 for non-football athletes; p<0.001; Fig. 3c). Table 2. Joint angles across the three phases of the squat as determined by video analysis expressed in degrees. Values are expressed as means ± standard error. Asterisks (*) indicate statistically significant differences between football players vs.
non-football athletes (all p0.001). Ankle Knee Hip
Football Non-Football Football Non-Football Football Non-Football
Start 119.8 ± 0.5 119.5 ± 0.7 162.6 ± 0.9* 169.0 ± 1.2* 170.5 ± 0.8 172.2 ± 0.8
Hold 98.5 ± 0.8* 91.7 ± 0.7* 59.6 ± 0.8 58.8 ± 1.2 61.6 ± 1.2 62.5 ± 1.5 Stop 121.3 ± 0.9 120.1 ± 0.7 164.4 ± 0.9* 169.6 ± 1.3* 169.3 ± 1.3 168.4 ± 1.5
7 Ankle appliances during back squats
Figure 3. Joint angles during the start (top), hold (middle), and stop (bottom) phases of the back squat expressed in degrees. Dark bars represent football players and light bars represent non-football trained individuals. Values are expressed as means ± standard error, with shaded bars representing football players and unshaded bars representing non-football athletes. Asterisks (*) indicate statistically significant
differences between football players vs. non-football athletes (p0.05).
8 Ankle appliances during back squats
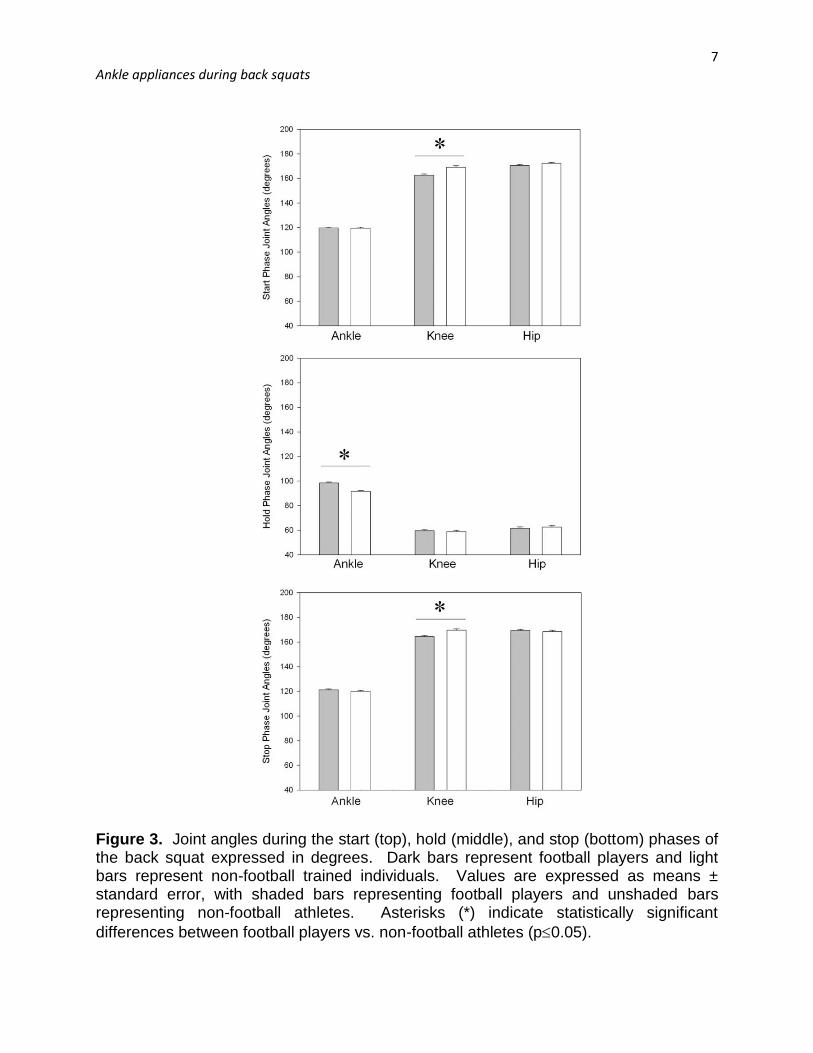
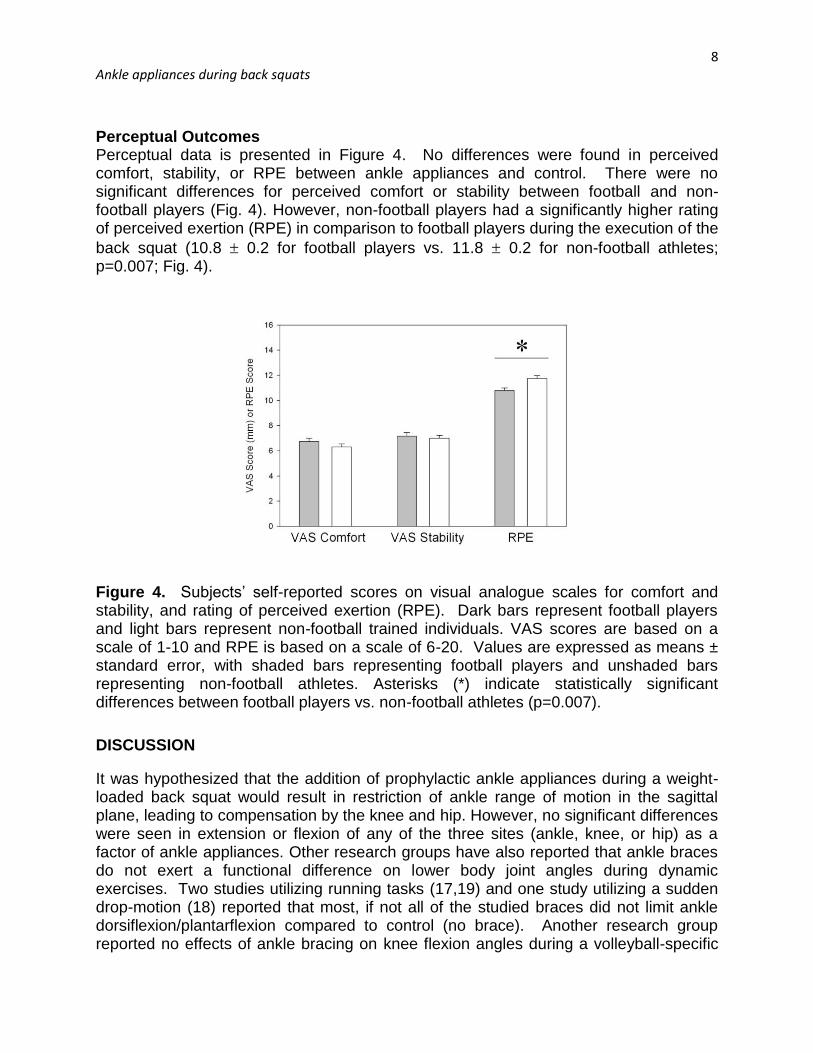
Perceptual Outcomes Perceptual data is presented in Figure 4. No differences were found in perceived comfort, stability, or RPE between ankle appliances and control. There were no significant differences for perceived comfort or stability between football and non-football players (Fig. 4). However, non-football players had a significantly higher rating of perceived exertion (RPE) in comparison to football players during the execution of the
back squat (10.8 0.2 for football players vs. 11.8 0.2 for non-football athletes; p=0.007; Fig. 4).
Figure 4. Subjects’ self-reported scores on visual analogue scales for comfort and stability, and rating of perceived exertion (RPE). Dark bars represent football players and light bars represent non-football trained individuals. VAS scores are based on a scale of 1-10 and RPE is based on a scale of 6-20. Values are expressed as means ± standard error, with shaded bars representing football players and unshaded bars representing non-football athletes. Asterisks (*) indicate statistically significant differences between football players vs. non-football athletes (p=0.007).
DISCUSSION
It was hypothesized that the addition of prophylactic ankle appliances during a weight-loaded back squat would result in restriction of ankle range of motion in the sagittal plane, leading to compensation by the knee and hip. However, no significant differences were seen in extension or flexion of any of the three sites (ankle, knee, or hip) as a factor of ankle appliances. Other research groups have also reported that ankle braces do not exert a functional difference on lower body joint angles during dynamic exercises. Two studies utilizing running tasks (17,19) and one study utilizing a sudden drop-motion (18) reported that most, if not all of the studied braces did not limit ankle dorsiflexion/plantarflexion compared to control (no brace). Another research group reported no effects of ankle bracing on knee flexion angles during a volleyball-specific
9 Ankle appliances during back squats
task (20). Coupled with the present findings, the data collectively suggest that ankle braces may not significantly limit extension/flexion angles of lower body segments, particularly for movements in the sagittal plane, and that the phenomenon is apparent across different activities and populations (age, gender). By contrast, other research groups have reported that braces may reduce ankle, knee, and/or hip flexion during various tasks (11–16). In some cases, restriction may be observed pre-exercise but disappears quickly once activity starts (24). Regarding the hip specifically, only one other study (15) examined the effects of ankle restriction on hip ROM in the sagittal plane, but they used a twenty minute running bout and ankle taping alone, so their results may not be directly comparable to the present study. Subjects self-reported no perceptual differences between appliances. Compared to ROM studies, far less is known about ankle appliances and perception, although research has shown that addition of appliances results in little to no decreases in performance (25) or oxygen consumption (15) regardless of perceptions or specific appliance. Subjects in the present study reported no differences in comfort or stability between different appliances, yet another research group found an inverse relationship between ankle brace comfort and ankle brace stability when they compared three different types of ankle brace during sudden forced inversion movement (26). The sudden, uncontrolled (from the subject’s perspective) movement of the latter study compared to the gradual, controlled movement employed in the present study likely explains the discrepancy. Both athletes and non-athletes tend to perceive braces as either comparable (23) or superior (27) to ankle taping within injury recovery or prevention contexts. Ankle taping may lose much of its restrictive effects during exercise whereas braces tend to maintain restriction (28–33), and ankle taping requires more time and funds than bracing (5,34). The present study may thus corroborate the current literature suggesting that ankle braces may be an equal, if not superior alternative to traditional ankle taping. The only significant differences observed in the present study were football versus non-football subjects. Joint angle differences were found between the two groups when the squat was broken down by phase. In the upright position (Start and Stop phases), football players had less knee extension than the non-football group, and in the hold position (Hold phase) football players had less ankle dorsiflexion. Squat technique differences or differences in flexibility may explain these discrepancies. Knee angle differences are possibly explained by the football subjects starting and stopping in a more neutral spine position (versus leaning forward) with slight hip flexion (“hip-hinge”) which results in greater knee flexion; by contrast, individuals less well-trained in back squat technique may have more forward trunk lean through the eccentric movement (35) resulting in greater ankle dorsiflexion, similar to what has been demonstrated in restricted versus unrestricted squat technique (36–38). Also, non-football subjects indicated higher RPE than football subjects, which may be expected given that football subjects would more readily perceive the 50% 1RM to be easier as relative submaximal lifting capacities are greater for resistance training-habituated individuals (39).

10 Ankle appliances during back squats
This study has some limitations. First, by using the back squat the ankle was kept fixed to a position on the floor. This limits full ankle range of motion in the sagittal plane. Further research should be done to monitor joint angles during cutting maneuvers to identify the role of ankle appliances during more lateral movements. Second, the effects of ankle appliances on muscular activity were not noted, though some research suggests that ankle bracing may reduce energy loads at the ankle by transferring them to the knee and hip (21). Future research could use a similar experimental model as the present study but include electromyographic (EMG) readings from thigh and leg muscles. Third, 50% of 1RM may not have been enough weight to elicit any substantial differences in the football players. CONCLUSIONS In conclusion, ankle appliances had no effect on lower body joint angles during the back squat and the addition of these appliances had little to no difference in comfort or stability of the subject. The back squat is an exercise that largely restricts the body’s motion to the sagittal plane; thus, the results may indicate that ankle appliances do not hinder functional ROM for lower body joints in other exercise or sport-specific motions largely restricted to the sagittal plane (such as many of the maneuvers made by football defensive lineman, often performed in crouched or squatted positions).
ACKNOWLEDGEMENTS
The authors would like to thank all of the subjects who donated their time for the study. Students in the Bio 133L Kinesiology Lab, Fall 2012, helped with data collection and subject recruitment. TJM and DSS wrote the majority of the paper with contributions from EVS and CLK. Address for correspondence: David S. Senchina, PhD. Biology Department, Drake University, 2507 University Ave., Des Moines, IA, 50311. Tel. 1 515 271 2956; Fax 1 515 271 3702; e-mail: [email protected].

11 Ankle appliances during back squats
REFERENCES
1. Czajka CM, Tran E, Cai AN, Dipreta JA. Ankle Sprains and Instability. Med Clin North Am. 2014 Mar;98(2):313–29.
2. Kaminski TW, Hertel J, Amendola N, Docherty CL, Dolan MG, Hopkins JT, et al. National Athletic Trainers’ Association position statement: conservative management and prevention of ankle sprains in athletes. J Athl Train. 2013 Aug;48(4):528–45.
3. Hootman JM, Dick R, Agel J. Epidemiology of collegiate injuries for 15 sports: summary and recommendations for injury prevention initiatives. J Athl Train. 2007 Jun;42(2):311–9.
4. Kerkhoffs GM, van den Bekerom M, Elders LAM, van Beek PA, Hullegie WAM, Bloemers GMFM, et al. Diagnosis, treatment and prevention of ankle sprains: an evidence-based clinical guideline. Br J Sports Med. 2012 Sep;46(12):854–60.
5. Mickel TJ, Bottoni CR, Tsuji G, Chang K, Baum L, Tokushige KAS. Prophylactic bracing versus taping for the prevention of ankle sprains in high school athletes: a prospective, randomized trial. J Foot Ankle Surg. 2006 Dec;45(6):360–5.
6. Tiemstra JD. Update on acute ankle sprains. Am Fam Physician. 2012 Jun 15;85(12):1170–6.
7. Trojian TH, Mohamed N. Demystifying preventive equipment in the competitive athlete. Curr Sports Med Rep. 2012 Dec;11(6):304–8.
8. Forbes H, Thrussell S, Haycock N, Lohkamp M, White M. The effect of prophylactic ankle support during simulated soccer activity. J Sport Rehabil. 2013 Aug;22(3):170–6.
9. You SH, Granata KP, Bunker LK. Effects of circumferential ankle pressure on ankle proprioception, stiffness, and postural stability: a preliminary investigation. J Orthop Sports Phys Ther. 2004 Aug;34(8):449–60.
10. Faraji E, Daneshmandi H, Atri AE, Onvani V, Namjoo FR. Effects of prefabricated ankle orthoses on postural stability in basketball players with chronic ankle instability. Asian J Sports Med. 2012 Dec;3(4):274–8.
11. DiStefano LJ, Padua DA, Brown CN, Guskiewicz KM. Lower extremity kinematics and ground reaction forces after prophylactic lace-up ankle bracing. J Athl Train. 2008 Jun;43(3):234–41.
12. McCaw ST, Cerullo JF. Prophylactic ankle stabilizers affect ankle joint kinematics during drop landings. Med Sci Sports Exerc. 1999 May;31(5):702–7.
13. Simpson KJ, Yom JP, Fu Y-C, Arnett SW, O’Rourke S, Brown CN. Does wearing a prophylactic ankle brace during drop landings affect lower extremity kinematics and ground reaction forces? J Appl Biomech. 2013 Apr;29(2):205–13.
14. Gudibanda A, Wang Y. Effect of the ankle stabilizing orthosis on foot and ankle kinematics during cutting maneuvers. Res Sports Med Print. 2005 Jun;13(2):111–26.
15. Paulson S, Braun WA. Prophylactic ankle taping: influence on treadmill-running kinematics and running economy. J Strength Cond Res. 2014 Feb;28(2):423–9.
16. Stoffel KK, Nicholls RL, Winata AR, Dempsey AR, Boyle JJW, Lloyd DG. Effect of ankle taping on knee and ankle joint biomechanics in sporting tasks. Med Sci Sports Exerc. 2010 Nov;42(11):2089–97.
17. DeClercq DL. Ankle bracing in running: the effect of a Push type medium ankle brace upon movements of the foot and ankle during the stance phase. Int J Sports Med. 1997 Apr;18(3):222–8.
18. Kernozek T, Durall CJ, Friske A, Mussallem M. Ankle bracing, plantar-flexion angle, and ankle muscle latencies during inversion stress in healthy participants. J Athl Train. 2008 Mar;43(1):37–43.
12 Ankle appliances during back squats
19. Lindley TR, Kernozek TW. Taping and semirigid bracing may not affect ankle functional range of motion. J Athl Train. 1995 Jun;30(2):109–12.
20. West T, Ng L, Campbell A. The effect of ankle bracing on knee kinetics and kinematics during volleyball-specific tasks. Scand J Med Sci Sports. 2013 Dec;24(6):958-63.
21. Gardner JK, McCaw ST, Laudner KG, Smith PJ, Stafford LN. Effect of ankle braces on lower extremity joint energetics in single-leg landings. Med Sci Sports Exerc. 2012 Jun;44(6):1116–22.
22. Faganel PP, Drake TC, Dahl-Miller AR, Senchina DS. Height variations in football shoes (cleats) for running backs and receivers may not alter ankle spatting effects in football field drills. J Undergrad Res. 2013;4(1):6–10.
23. Reuter G, Dahl A, Senchina D. Ankle spatting compared to bracing or taping during maximal-effort sprint drills. Int J Exerc Sci. 2011;4(1):49–64.
24. Verhagen EA, van der Beek AJ, van Mechelen W. The effect of tape, braces and shoes on ankle range of motion. Sports Med. 2001;31(9):667–77.
25. Putnam AR, Bandolin SN, Krabak BJ. Impact of ankle bracing on skill performance in recreational soccer players. PM R. 2012 Aug;4(8):574–9.
26. Ubell ML, Boylan JP, Ashton-Miller JA, Wojtys EM. The effect of ankle braces on the prevention of dynamic forced ankle inversion. Am J Sports Med. 2003 Dec;31(6):935–40.
27. Lardenoye S, Theunissen E, Cleffken B, Brink PR, de Bie RA, Poeze M. The effect of taping versus semi-rigid bracing on patient outcome and satisfaction in ankle sprains: a prospective, randomized controlled trial. BMC Musculoskelet Disord. 2012;13:81.
28. Cordova ML, Ingersoll CD, LeBlanc MJ. Influence of ankle support on joint range of motion before and after exercise: a meta-analysis. J Orthop Sports Phys Ther. 2000 Apr;30(4):170–7; discussion 178–82.
29. Fleet K, Galen S, Moore C. Duration of strength retention of ankle taping during activities of daily living. Injury. 2009 Mar;40(3):333–6.
30. Lohkamp M, Craven S, Walker-Johnson C, Greig M. The influence of ankle taping on changes in postural stability during soccer-specific activity. J Sport Rehabil. 2009 Nov;18(4):482–92.
31. Meana M, Alegre LM, Elvira JLL, Aguado X. Kinematics of ankle taping after a training session. Int J Sports Med. 2008 Jan;29(1):70–6.
32. Paris DL, Kokkaliaris J, Vardaxis V. Ankle ranges of motion during extended activity periods while taped and braced. J Athl Train. 1995 Sep;30(3):223–8.
33. Purcell SB, Schuckman BE, Docherty CL, Schrader J, Poppy W. Differences in ankle range of motion before and after exercise in 2 tape conditions. Am J Sports Med. 2009 Feb;37(2):383–9.
34. Kemler E, van de Port I, Backx F, van Dijk CN. A systematic review on the treatment of acute ankle sprain: brace versus other functional treatment types. Sports Med Auckl NZ. 2011 Mar 1;41(3):185–97.
35. Sands WA, Wurth JJ, Hewit JK. The National Strength and Conditioning Association’s (NCSA) Basics of Strength and Conditioning Manual [Internet]. Colorado Springs, Colorado: National Strength and Conditioning Association; 2012 [cited 2014 Apr 1]. 105 p. Available from: http://www.nsca.com/uploadedFiles/NSCA/Resources/PDF/Publications/Basics_of_Strength_and_Conditioning/BasicsManual_FINAL_201210.pdf
36. Fry AC, Smith JC, Schilling BK. Effect of knee position on hip and knee torques during the barbell squat. J Strength Cond Res. 2003 Nov;17(4):629–33.
37. List R, Gülay T, Stoop M, Lorenzetti S. Kinematics of the trunk and the lower extremities during restricted and unrestricted squats. J Strength Cond Res. 2013 Jun;27(6):1529–38.

13 Ankle appliances during back squats
38. McKean MR, Dunn PK, Burkett BJ. Quantifying the movement and the influence of load in the back squat exercise. J Strength Cond Res. 2010 Jun;24(6):1671–9.
39. Pick J, Becque MD. The Relationship Between Training Status and Intensity on Muscle Activation and Relative Submaximal Lifting Capacity During the Back Squat. J Strength Cond Res. 2000;14(2):175–81.
Disclaimer The opinions expressed in the Journal of Undergraduate Kinesiology Research are those of the authors and are not attributable to the Journal of Undergraduate Kinesiology Research, the editorial staff or Western State Colorado University.