the effect of vasopressin in water-loaded hypokalemic patients is prostaglandin-independent
TRANSCRIPT

Prostaglandins & Medicine 7: 465-472, 1981
THE EFFECT OF VASOPRESSIN IN WATER-LOADED HYPOEALEMIC PATIENTS IS PROSTAGLANDIN-INDEPENDENT
Jose A. Rodriguez, Catherine S. Delea, Frederic C. Bartter and Helmy Siragy. Audie L. Murphy Memorial Veterans' Hospital, San Antonio, Texas 78284 (reprint requests to FCB)
ABSTRACT
Potassium-depleted subjects regularly excrete dilute urine with a high free-water clearance which cannot be suppressed either by solute loading or by water deprivation. In man, as in the dog and rat, potassium depletion impairs the ability of the kidney to achieve maxi- mal urinary solute concentration and vasopressin is unsuccessful in overcoming this defect. In man and in the dog, potassium depletion induces a rise in urinary prostaglandin E2, an effect which can be reversed with indomethacin, a cycle-oxygenase inhibitor. To evaluate the role of prostaglandins on the renal action of vasopressin in hypo- kalemia, six subjects with hypokalemia of various etiologies were studied in a control, drug-free condition and again after 3 to 6 days of indomethacin (100 mg/day). Renal clearance studies to measure the maximal free-water excretion in response to an intravenous water load (10 ml/min) and to a superimposed infusion of arginine vasopressin (40 mU/hr) were performed. The results in six patients are as follows: maximal free-water clearance (control) 8.03 2. 0.8 ml/min (mean + S.E.), with the addition of vasopressin, .14 2 0.8; after 3 to 6 days of indomethacin, 8.55 + 1.33; with vasopressin 0.91 + 1.23 ml/min. There was no statistically significant difference between the maximal free water clearance with or without indomethacin. Vasopressin exerted an equally great response in both conditions and prostaglandins did not appear to play a role in free-water formation.
INTRODUCTION
Pnlyuria associated with hypokalemia in human beings has been observed for almost three decades. (1,2,3) Animal experimentation has disclosed that probably more than several mechanisms are operative in its patho- genesis, namely, a> increased thirst with a corresponding increase in water intake, (4,5,6,7) b) decrease in serum concentration of vaso- pressin, (8) c) decrease in renal medullary tonicity, (9,lO) and d) renal tubular resistance to the action of vasopressin. (11)
465

In some clinical conditions characterized by hypokalemia urinary excretion of prostaglandin E2 (12,13,14) is elevated. In vitro and -- in vivo antagonism between the effects of prostaglandin E2 and vaso- -- pressin at the renal tubular level has been reported. (15,16,17)
To evaluate the influence of prostaglandins on the renal effect of vasopressin, we measured free water clearance in normal subjects and in patients with chronic hypokalemia of different etiologies during an intravenous water load and infusion of vasopressin at a constant rate. The intravenous water load was used to suppress endogenous vasopressin secretion and to minimize the effect of changing water intakes. Concurrent administration of fixed amounts of exogenous vasopressin allowed a more accurate evaluation of the renal tubular effects of vasopressin. The studies were repeated during inhibition of prostaglandin synthesis with indomethacin.
MATERIALS AND METHODS
Six patients with polyuria (urine volumes >3000 ml/d) and long-term potassium depletion, as estimated from at least three different serum potassium values below 3.5 mEq/l in a one-month period, and four nor- mal subjects were admitted to a metabolic ward of the Veterans Hospital for study. All subjects were informed in detail about the study and gave written consent. The protocol had been previously approved by the Institutional Review Board and the Research and Development Committee of the Audie L. Murphy Memorial Veterans' Hospi- tal.
Table I: Diagnosis and Serum Potassium
SEX AGE DIAGNOSIS
1) F 51 2) M 56 3) F 22 4) F 22
5) M 48 6) M 14 7) M 46
8) M 41
9) I? 42 10) F 36
NORMAL NORMAL NORMAL NORMAL
Mean + S.E. PRIMARY ALDOSTERONIS~ BARTTER'S SYNDROME HYPERTENSION; DITJRETIC-
INDUCED HYPOEALEMIA "CYPTOGENIC" RENAL POTASSIUM LOSS
DIURETIC ABUSE LAXATIVE ABUSE
Mean 2 S.E.
SERUM POTASSIUM mEq/l
4.2 4.7 4.0 4.0
4.2 + 0.1 2T9 2.0
3.2
2.2
3.2 2.9
2.7 + 0.2
466
The patients were given a diet constant in sodium (150 mEq/d) and potassium (70 mEq/d). Body weight was measured daily and urine was collected in twenty-four hour pools. The patients were asked to dis- continue all medications one week prior to the study.
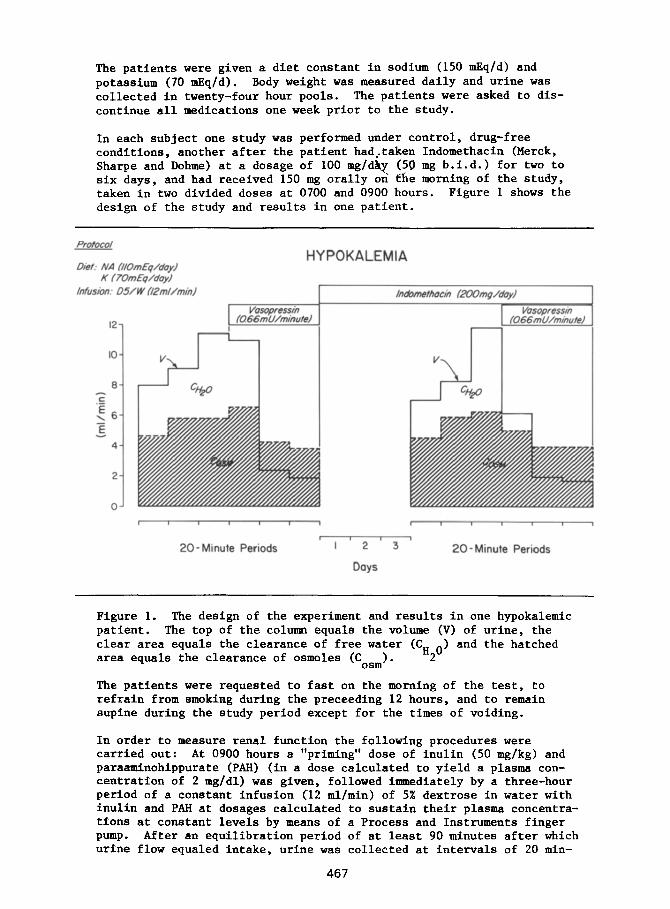
In each subject one study was performed under control, drug-free conditions, another after the patient had,taken Indomethacin (Merck, Sharpe and Dohme) at a dosage of 100 mg/d&y (56 mg b.i.d.) for two to six days, and had received 150 mg orally on the morning of the study, taken in two divided doses at 0700 and 0900 hours. Figure 1 shows the design of the study and results in one patient.
Diet: NA /I/OmEq/dayJ K f ?OmEq/dayJ
/ni?sion: &F/W fJ2mUminJ
12
IO
8
z E
\6
E 4
2
0
HY POKALEMIA
r
I 1 1 I I , 1
20- Minute Periods '1'2'3' 20 -Minute Periods
Doys
Figure 1. The design of the experiment and results in one hypokalemic patient. The top of the column equals the volume (V) of urine, the clear area equals the clearance of free water (CP o> and the hatched area equals the clearance of osmoles (Cosm). 2
The patients were requested to fast on the morning of the test, to refrain from smoking during the preceeding 12 hours, and to remain supine during the study period except for the times of voiding.
In order to measure renal function the following procedures were carried out: At 0900 hours a "priming" dose of inulin (50 mg/kg) and paraaminohippurate (PAH) (in a dose calculated to yield a plasma con- centration of 2 mg/dl) was given, followed immediately by a three-hour period of a constant infusion (12 ml/min) of 5;6 dextrose in water with inulin and PAH at dosages calculated to sustain their plasma concentra- tions at constant levels by means of a Process and Instruments finger Pump. After an equilibration period of at least 90 minutes after which urine flow equaled intake, urine was collected at intervals of 20 min-
467

utes each and blood was collected at the mid-points of the periods. Three control periods were obtained in order to measure the clearances of inulin, PAh, sodium, potassium, chloride, and osmolality and to estimate "free" water clearance (CH20). Following these three periods, 0.66 mU/min of vasopressin (Aqueous Pitressin, Parke-Davis) were added to :he solution to be infused and three additional 20- minute clearance periods were obtained.
Alkali-stable inulin was estimated by the method of Walser and Orloff (18) and PAH bjr the method of Bratton and ?larshall. (19) Sodium and potassium wert estimated by an internal-standard flame photometer. Chloride was estimated by a Cotlove titrimeter, osmoles by an osmo- meter from changes in vapor pressure.
The following calculations were made: Clearance (C) of a substance equals W/P where U equals urinary concentration, V equals volume of urine per minute, and P equals plasma concentration. The clearance of inulin yieius an estimate of glomerular filtration rate, that of PAH an estimate of renal plasma flow. The clearance of free water (CH 0)
2 = v =
stu ent's t co moles.
tes f. All data were statistically analyzed by
RESULTS
The serum potassium (mean + s.e.m.) was 4.2 + 0.1 mEq/l in normal and 2.7 + 0.2 mEq/l in potassium-depleted subjects. Indomethacin did not change serum potassium or sodium in either group of subjects.
Glomerular filtration rate during water loading did not change signifi- cantly from control values when vasopressin was given nor when vaso- pressin was given with the indomethacin in either normal or hypokalemic subjects with medication. Renal plasma flow showed a statistically significant difference in the hypokalemic subjects only when vaso- pressin was given to the indomethacin-treated subjects (488 2 41 ml/min with indamethacin versus 304 + 72 ml/min with indomethacin plus vaso- pressi/f;, P = ~0.025).
-
In normai subjects, the 24-hour urinary osmolality was 232 + 9.5 mOsm/ kg. During the water loading, urine osmolality reached 113 + 28 mOsm/ kg. Vasopressin induced a maximal urinary osmolality of 413 + 97 mOsm/ kg (v < .005> that was not further increased significantly with indo- methacin treatment (487 5 116 mOsm/kg). In hypokalemic subjects, the 24-hour urinary osmolality was 237 + 40 mOsm/kg and was not significant- ly different from that of normal subjects. During water loading urinary osmolality was 104 + 26 mOsm/kg. Maximal urinary osmolality was 316 + 57 mOsm/kg with vasopressin alone (p < .005) and 384 &- 61 mOsm/kg with the addition of indomethacin (difference not statistically signifi- cant).
Vasopressin produced a highly significant decrease in fractional free water clearance (CE2G/GF'R X 100) in normal (p < 0.025) as well as in hypokalemic subjects (p < 0.001) and of the same magnitude in both groups. When prostaglandin synthesis was inhibited with indomethacin,
468

no significant difference was observed in the response to vasopressin in normal or hypokalemic subjects.
Table II. Effect of Vasopressin, Indomethacin and both on Fractional Free H 0 Clearance during water loading in normal and Hypoka emit z subjects.
SUBJECTS CONTROL VASOPRESSIN INDOMETHACIN VASOPRESSIN + INDOMETHACIN
mllmin mlfmin ml/min mllmin
NORMAL 6.85 + 1.5 -0.35 + 0.66 6.12 + 0.66 -0.63 + 0.22 - - - N= 4 p < 0.025 p < 0.025
y"f=EFC 8.03 - + 0.8 0.14 - + 0.83 8.55 - + 1.33 0.91 - + 1.23
p < 0.001 p < 0.001
DISCUSSION
Potassium-depleted animals as well as human beings are unable to con- centrate their urine to the extent that normal subjects can when challenged by hydropenia. Reports that mechanisms other than renal tubular resistance to the action of vasopressin could be involved in this defect prompted us to study subjects not in hydropenia but in an overhydrated state, so as to minimize the influence of non-renal factors on the effectiveness of exogenous vasopressin in hypokalemic and normal subjects.
We found that the effect of vasopressin on renal water reabsorption is similar in normal and in hypokalemic subjects. This lack of renal resistance to vasopressin in our hypokalemic patients suggests that attention should be given to the non-renal factors, e.g., vasopressin secretion and water intake, in the impairment of urinary concentration observed in hypokalemia in man.
Inhibition of prostaglandin synthesis with indomethacin did not change the effect of vasopressin on free water clearance in either group studied. This is in agreement with previous findings by Berl and associates (20) in the rat,
In man, the dose and duration of the effect of vasopressin could be critfcal for the demonstration of the antagonism between prostaglandins and vasopressin. Large doses of vasopressin, especially if administer- ed as a bolus, could %ncrease prostaglandin synthesis and limit its own effect. (21,22) If vasopressin were given in physiologic doses at a constant rate, over longer periods of time, this antagonism would pro- bably not be apparent and the results would be similar to those in the subjects studied here.
469

Although we did not measure urinary prostaglandins in this study, there is ample evidence in the literature (12,13,14,23) that urinary pros- taglandins are increased in hypokalemia. More important to the study is the evidence of suppression of prostaglandin synthesis in the normal and hypokalemic subjects. Indomethacin at the dosage in which it was administered has been shown in many studies to give a significant inhibition of prostaglandin synthesis. (13,14,24) In the patients in whom we measured urinary aldosterone and plasma renin activity (data not shown) in the control state and on day 2 of indomethacin, there was a signfficant decrease in both variables when indomethacin was given, a fact which contributes indirect evidence of the effective suppression of prostaglandins. (25,26)
Ih summary, the action of vasopressin on the renal ability to reab- sorb free water in man seems to be independent of prostaglandins. Its effect is simflar in normal and hypokalemic subjects, a fact which suggests a role for extra-renal factors in the polyuria of hypokalemia.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
REFERENCES
Schwartz WB and Reloan AS. Metabolic and renal studies in chronic potassium depletion resulting from overuse of laxatives. Journal of Clinical Investigation 32:258, 1953.
Rubini m. Water excretion in potassium - deficient man. Journal of Clinical Investigation 40:2215, 1961.
Relman AS and Schwartz WB. The nephropathy of potassium depletion: A clinical and pathological entity. New England Journal of Medi- cine 255:195, 1956.
Smith SG and Lasater T. A diabetes insipidus-like condition produced in dogs on potassium-deficient diet. Proceedings of the Society for Experimental Biology and Medicine 74~427, 1950.
Brockaw A. Renal hypertrophy and polydipsia in potassium deficient rats. Amertcan Journal of Physiology 172:333, 1953.
Hollander W, Winters RW, Williams F, Bradley J, Oliver J, Welt LG. Defect in renal reabsorption of water assocfated with potassium depletion in rats. American Journal of Physiology 189:557, 1957.
Berl T, Linas SL, Aisenbrey GA, Anderson RJ. On the mechanism of polyuria in potassium depletion. Journal of Clinical Investigation 60:620, 1977.
Rutecki G, Greenspan R, Cox JW, Robertson G, Ferris TF. Studies of the diabetes insipidus with K deficiency. Clinical Research 27: 499, 1979.
Eigler JOC, Salassa RM, Bahn RC, Owen CA, Jr. Renal distribution of sodium in potassium-depleted and vitamin D intoxicated rats. American Journal of Physiology 202:1115, 1962.
Gottschalk CW, Mylles M, Jones NF, Winters RW, Welt LG. Osmolality of renal tubular fluids in potassium-depleted rodents. Clinical Science 29:249, 1965.
470

11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
Camey S, Rayson B, Morgan T. A study in vitro of the concentra- -- ting defect associated with hypokalemia and hypercalcemia. Pflugers Archives 366:11, 1976.
Galvez OG, Bay WH, Robert8 BW, Ferris TF. The hemodynamic effects of potassium defztciency in the dog. Circulation Research 40 (Supplement I):l, 1977.
Gill JR, Jr, Frolich JC, Bowden RE, Taylor AA, Keiser HR, Seyberth HW, Oates JA, Bartter FC. Bartter's syndrome: A disorder char- acterized by high urinary prostaglandins and a dependence of hyperreninemia on prostaglandin synthesis. American Journal of Medicine 61:43, 1976.
Fichman M, Telfer N, Zia P, Speckart LP, Golub M, Rude R. Role of prostaglandins in the pathogenesis of Bartter's syndrome. American Journal of Medicine 60:785, 1976.
Anderson RJ, Berl T, McDonald KM, Schrier RW. Evidence for an in - vivo antagonism between vasopressin and prostaglandin in the
nnumqalian kidney. Journal of Clinical Investigation 56:420, 1975.
Berl T, Raz A, Wald H, Horowitz J, Czaczkes W. Prostaglandin syn- thesis inhihition and the action of vasopressin: studies in man and rat. American Journal of Physiology F232:529, 1977.
Orloff J, Handler JS, Bergstrom S. on the permeability response of
Effect of prostaglandin (PGEl) toad bladder to vasopressin, theo-
phylline and adenosine 3', 5'-monophosphate. Nature, London, 205:397, 1965.
Walser M, Davidson DG, Orloff J. The renal clearance of alkali stable inulin. Journal of Clinical Investigation 34:1520, 1955.
Bratton AC, Marshall EK. A new coupling component for sulfanila- mide determination. Journal of Biology and Chemistry 128:537, 1939.
Berl T, Aisenbrey GA, Linas SL. Renal concentrating defect in the hypokaleraic rat is prostaglandin independent. American Journal of Physiology F238:37, 1980.
Zusman RM, Keiser HR, Handler JS. Vasopressin-stimulated prosta- glandin E biosynthesis in the toad urinary bladder. Effect on water flow. Journal of Clinical Investigation 60:1339, 1977.
Grantham JJ, Orloff J. Effect of prostaglandin El on the pemeabil- ity response of the isolated collecting tubule to vasopressin, adenosine 3', 5' monophosphate and theophylline. Journal of Clini- cal Investigation 47:1154, 1968.
Gill JR, Bartter FC. Evidence for a prostaglandin-independent defect in chloride reabsorption in the loop of Henle as a proximal cause of Bartter's syndrome. American Journal of Medicine 65:766, 1978.
Bowden RE, Gill JR, Jr, Radfar N, Taylor AA, Keiser HR. Effect of different prostaglandin synthetase inhibitors on immunoreactive prostaglandin E excretion in Bartter's syndrome. Journal of the American Medical Association 239:117, 1978.
471

25. Werning C, Vetter W, Weidmann P, Schweikart HV, Steil D, Siegenthaler W. Effect of prostaglandin E on renin in the dog. American Journal of Physiology 220:852, 19jl.
26. Yun JC, Kelly GD, Bartter FC, Smith GW. Role of prostaglandins in the control of renin secretion in the dog (II). Life Sciences 23:945, 1978.
472