the doacs - how and in whom scott c. woller, md · pdf filethe doacs - how and in whom scott...
TRANSCRIPT

TheDOACs-HowandinWhom
ScottC.Woller,MDMedicalDirector,AnticoagulationManagement,IntermountainHealthcareCenralRegion,Co-DirectorVenousThromboemolism
Program,IntermountainMedicalCenter;AssociateProfessor,InternalMedicine,UniversityofUtahSchoolofMedicine;SaltLakeCity,Utah
Objectives:• DiscussandoutlineastrategytoselectamongtheavailableDOAC
medicationsforpatientswithVTEandvariouscharacteristicsandcomorbidities.
• IndicatetheavailablereversalagentsforDOACsandreviewmanagementstrategiestoaddressbleedinginpatientstakingDOACs.
• DescribelimitationstotheunderstandingofDOACinterruption,anddescribeastandardizedapproachtoperi-proceduralinterruptionofDOACs.

Directoralanticoagulants:HowtouseDOACsandinwhom?
ScottC.Woller,MDCo-DirectorThrombosisProgram,IntermountainMedicalCenterAssociateProfessorofClinicalMedicine,UniversityofUtahSchoolofMedicine
ThrombosisGuidelinesSymposiumIntermountainMedicalCenterApril22,2016

Disclosures
PanelistfortheAmericanCollegeofChestPhysicians10theditionGuidelineforAntithromboticTherapyforVTEDisease
PanelistfortheAnticoagulationForumClinicalGuidanceManagementofvenousthromboembolisminitiative
Ihavebeenawardedgrantfundingpaidtomyemployer(IntermountainHealthcare)fromBristol-MeyersSquibb

LearningObjectives• Attheconclusionofthisactivity,participantsshouldbeableto:
• OutlineastrategytoselectamongtheavailableDOACmedicationsforpatientswithVTEandvariouscharacteristicsandcomorbidities.
• IndicatetheavailablereversalagentsforDOACSandreviewmanagementstrategiestoaddressbleedinginpatientstakingDOACs.
• DescribelimitationstotheunderstandingofDOACinterruption,anddescribeastandardizedapproachtotheirperi-proceduralinterruption.

Naminganewclassofmedicines
NOAC: Non Vitamin K Oral AnticoagulantISTHGuidanceStatementJThromb Haemost.2015Jun;13(6):1154-6

TheDirectOralAnticoagulants(DOACs)
http://theuniquesheep.blogspot.com/; http://merchandise.thedoctorwhosite.co.uk/doctor-who-masterpiece-collection-gold-dalek/

TF
Va
VIIa
sciencecodex.com
DOACs

“Acutetherapy”representstheinitialphasewhichoftenincludesahigherdoseorparenteraldrug.
TheminimumdurationofanticoagulanttherapyforDVTorPEisusuallythreemonths,andthisperiodoftreatmentisreferredtoas"long-termtherapy".
Adecisiontotreatpatientsforlongerthan3monthsisreferredtoas"extendedtherapy”.
KearonC.Chest. 2016.doi:10.1016/j.chest.2015.11.026
Nomenclatureofvenousthromboembolismtherapy

TheDirectOralAnticoagulantsRivaroxaban Apixaban Edoxaban Dabigatran
BRANDNAMEPHARMACEUTICAL
Xarleto™
BayerEliquis™
BMS&PfizerSavaysa™
DaiichiSankyoPradaxa™
Boehringer Ingelheim
TARGET FactorXa FactorXa FactorXa FactorIIa
BIOAVAILABILITY(%) ~80 ~50 62 6–7
TIMETOPEAK(h) 2–3 1–2 1-2 1.5
HALF-LIFE(h) 9-13 8-15 9-10 12-14
RENALEXCRETION(%) 33 25 35 >80
EFFECTONaPTT/PT* 1.8/2.6 1.2/~2 yes 2.3/NR
EFFECTONXa 68% NR NR NoEffect
DRUGINTERACTIONS CYP3A4IND/INH CYP3A4INH P-gp INH/CYP3A4 Verapamil/rifampin
Derived from: Crowther. Blood. 2008;111:4871-4879; Garcia, D. Blood. 2010;115:15-20; http://www.eliquis.com/PDF/ELIQUIS%20%C2%AE%20(apixaban)%20SmPC.pdf Schulman ThrombHaemost 2014;111:

MetabolismofDOACs
Nutescu JThromb Thrombolysis(2016)41:15–31Heidbuchel 2013

DRUG RIVAROXABAN APIXABAN EDOXABAN DABIGATRAN
TRIAL EINSTEIN-PE+DVT AMPLIFY HOKUSAI RE-COVERDose 15mg BIDx21d;
20mgQD10mgBDXx7d;
5mgBIDLMMH then60mgQD(30mgCrCl30-50;<60kg)
LMWHthen150mg BIDx6mo.
Comparator/TTR% LWWH+Warf/61% LWWH+Warf/61% LMWH+Warf/63.5% LWWH+Warf/60%
Condition (%) PE61%DVT64% DVT65PE25B10 DVT60PE40B24 DVT70PE20 B10
Enrolled 8281 5395 8240 2539
Design ROL NI RDBNI R DBNI RDBNI
Age/ %♂ 57yrs/55% 57 /61% 55.8 /57% 55yrs/58%
Cancer 5% 2.5% 9.2% 5%
1o Efficacy RecurrentVTE Recur. VTE+VTE death Recur. VTE+VTE death Recur.VTE+death
PrimarySafety MB +CRNMB MB+CRNMB MB+CRNMB Bleeding/ACS/LFT
EfficacyOutcome 2.3v.2.1; RR0.9(0.68-1.2)p<0.003NI
2.3vs.2.7RR0.84(0.6-1.2)p<0.001NI
3.2vs.3.5RR0.89(0.7-1.1)p<0.001NI
2.4v.2.1; RR1.1(0.65-1.84)
MajorBleeding 1.7v.2.2RR0.55(0.38-0.51)p=<0.05sup
0.6vs.1.8 RR0.31(0.17-0.55) p<0.001sup
1.4vs.1.6RR0.84(0.59-1.21)p=0.35sup
1.6v.1.9 RR0.82(ns)
Anybleeding 10.3vs. 11.4% CRB: 4.3 vs.9.7% 21.7%vs.25.6% HR 0.71(0.59-0.85)
Summary Non-inferior;QDdose Non-inferior andsafer Non-inferior,QD Non-inferior
SchulmanNEJM2009;361:2342; EINSTEINInvestigatorsNEJMDec4,2010;AMPLIFYNEJM1Jul2013;HOKUSAINEJM1Sept 2013
DOACsforVTE:TheLong-termTreatmentClinicalTrials
RESOURCESFORAT10GUIDELINESTATEMENT• Dabigatranforlong-termtreatmentofVTE
• RE-COVERNEngl JMed.2009Dec10;361(24):2342-52.• RE-MEDY/RE-SONATENEngl JMed.2013Feb21;368(8):709-18• RE-COVERIITrialInvestigators.Circulation.2014Feb18;129(7):764-72
• Rivaroxabanforacuteandlong-termtreatmentofVTE• PrinsMH,etal.Thromb J.2013Sep20;11(1):21• EINSTEINInvestigators.NEngl JMed.2010Dec23;363(26):2499-510• EINSTEIN–PEInvestigators.NEngl JMed.2012Apr5;366(14):1287-97
• ApixabanforacuteandlongtermtreatmentofVTE• AMPLIFYInvestigators.NEngl JMed.2013Aug29;369(9):799-808.
• Edoxabanforlong-termtreatmentofVTE• Hokusai-VTEInvestigators.NEngl JMed.2013Oct10;369(15):1406-15.
KearonC.Chest. 2016.doi:10.1016/j.chest.2015.11.026
AT10:Choiceofanticoagulantforlong-termtreatmentofDVTandPE:DOACvs.warfarin

AT10Summaryofevidence:RecurrentVTEQUESTION:ShouldaDOACorwarfarinbeusedforacuteandlong-termtreatmentofVTE?
Qualityassessment SummaryofFindingsNOACn(studies)
Riskofbias Overallqualityofevidence
Studyeventrates(%) Relativeeffect(95% CI)
AnticipatedabsoluteeffectsWithLMWHand
VKAWithNOAC Riskw/LMWH
&VKARiskdifferencewith
NOACs(95%CI)
RecurrentVTERIVAROXABAN 8281(2studies)
noseriousriskofbias
⊕⊕⊕⊝MODERATE
duetoimprecision
95/4131 (2.3%)
86/4150 (2.1%)
RR 0.90 (0.68 to 1.2)
23 per 1000 2 fewer per 1000(from 7 fewer
to 5 more)
DABIGATRAN 5107(2studies)
noseriousriskofbias
⊕⊕⊕⊝MODERATE
duetoimprecision
55/2554 (2.2%)2
60/2553 (2.4%)
RR 1.12 (0.77 to 1.62)
22 per 1000 3 more per 1000(from 5 fewer to 13 more)
APIXABAN5244(1study)
noseriousriskofbias
⊕⊕⊕⊝MODERATE
duetoimprecision
71/2635 (2.7%)
59/2609 (2.3%)
RR 0.84 (0.6 to 1.18)
27 per 1000 4 fewer per 1000(from 11 fewer
to 5 more)
EDOXABAN8240(1study)
noseriousriskofbias
⊕⊕⊕⊝MODERATE
duetoimprecision
146/4122 (3.5%)3
130/4118 (3.2%)
RR 0.83 (0.57 to 1.21)
35 per 1000 6 fewer per 1000(from 15 fewer
to 7 more)

AT10Summaryofevidence:MajorBleedingQUESTION:ShouldaDOACorwarfarinbeusedforacuteandlong-termtreatmentofVTE?
Qualityassessment SummaryofFindingsNOACn(studies)
Riskofbias Overallqualityofevidence
Studyeventrates(%) Relativeeffect(95% CI)
AnticipatedabsoluteeffectsWithLMWHand
VKAWithNOAC Riskwith
LMWHandVKARiskdifferencewith
NOACs(95% CI)
MajorBleedingRIVAROXABAN8246(2studies)
noseriousriskofbias
⊕⊕⊕⊕HIGH
72/4116 (1.7%)4
40/4130 (0.97%)
RR 0.55 (0.38 to 0.81)
17 per 1000 8 fewer per 1000(from 3 fewer to 11
fewer)
DABIGATRAN5107(2studies)
noseriousriskofbias
⊕⊕⊕⊝MODERATE
duetoimprecision
51/2554 (2%)2
37/2553 (1.4%)
RR 0.73 (0.48 to 1.1)
20 per 1000 5 fewer per 1000(from 10 fewer to 2
more)
APIXABAN5365(1study)
noseriousriskofbias
⊕⊕⊕⊕HIGH
49/2689 (1.8%)
15/2676 (0.56%)
RR 0.31 (0.17 to 0.55)
18 per 1000 13 fewer per 1000(from 8 fewer to 15
fewer)
EDOXABAN8240(1study)
noseriousriskofbias
⊕⊕⊕⊝MODERATE
duetoimprecision
66/4122 (1.6%)
56/4118 (1.4%)
RR 0.85 (0.6 to 1.21)
16 per 1000 2 fewer per 1000(from 6 fewer to 3
more)

EvaluationofIndividualswithPulmonaryNodules:GeneralApproachDespitethelackofanantidotefortheDOACs,theriskthatamajorbleedwillbefatalappearstobenohigherthanthatforwarfarin
Theriskofbleeding(particularlyintracranialbleeding)withtheNOACsislessthanwithVKAtherapy
Costandcoveragewillrepresentanimportant“real-world”patientimportantfactorinchoosinglong-termanticoagulant
AT10Choiceofanticoagulantforlong-termtreatmentofDVTandPE:DOACvs.warfarin

EvaluationofIndividualswithPulmonaryNodules:GeneralApproachRecommendedtherapyforVTEtakesintoconsiderationefficacy,safety,andburdenoftreatment.Thisalsocanincludecost.
Isthereevidencetorecommend1DOACoveranother?DOACshavenotbeencomparedhead-to-headforpatient-importantoutcomes.BasedonindirectcomparisonstheseoutcomesappeartobesimilarwithalloftheNOACs
Individualpatientcharacteristics(includingcostandinsurancecoverage)willlikelydrivechoiceofanticoagulantfortheinitial3monthsoftherapy
AT10Choiceofanticoagulantforlong-termtreatmentofDVTandPE:DOACvs.warfarin
EvaluationofIndividualswithPulmonaryNodules:GeneralApproachAT10GuidelineStatement:
AT10Choiceofanticoagulantforlong-termtreatmentofDVTandPE:DOACvs.warfarin
InpatientswithDVTofthelegorPEandnocancer,aslong-term(first3months)anticoagulanttherapy,wesuggestapixabanoredoxabanorrivaroxabanordabigatranoverVKAtherapy (Grade2B).Remarks:Acutetherapywithparenteralanticoagulationisgivenbeforedabigatranandedoxaban.
KearonC.Chest. 2016.doi:10.1016/j.chest.2015.11.026
Forthefirsttimeanalternativetousualcarewithlowmolecularweightheparinandwarfarinhasbeensuggestedforthelong-termtreatmentofPEandDVT.
Fromtheclinicaltrials:
• Needforthrombolytictherapy• AnindicationforanticoagulationforwhichDOACapprovaldoesnotexist• Highriskofbleeding• Significantliverdisease(acuteorchronichepatitis,cirrhosis,orAST/ALT≥3xULN)• Creatinineclearance30mL/min(forapixabanthethresholdwas25mL/min)• Aspirinuse(100mg/day)• Concomitantuseofinteractingmedications• Uncontrolledhypertension
Whoisnot?
WhoisacandidateforaDOACtherapytotreatVTE?
SchulmanS(2013)NEnglJMed368:709–718.EINSTEINInvestigators(2010)NEnglJMed363:2499–2510.AgnelliG(2013)NEngl JMed368:699–708. SchulmanS(2009)NEnglJMed361:2342–2352.SchulmanS(2014)Circulation129:764–772EINSTEIN–PEInvestigators(2012).NEnglJMed366:1287–1297. AgnelliG(2013)NEngl JMed369:799–808.Hokusai-VTEInvestigators(2013)NEnglJMed369:1406–1415.

Fromtheschoolofhardknocks:
• Patientswhostrugglewithcompliance(unlessrelatedtotransportationforINRs)• Warfarinislikelyfavorabletoallowascertainmentofandanticoagulanteffect
• Financialbarrierstolongitudinalcompliance• After1.1yearf/u<50%prescribedDOACpickedupadequatedrugtocover80%days
Whoisnot?
WhoisacandidateforaDOACtherapytotreatVTE?
KearonCAT10Chest2016;Yao,XChestPhysicianVol.11,No.2Feb.2016

CandidatesforaDOACtherapy:Specialpopulations

Pregnancy
CandidatesforaDOACtherapy:Specialpopulations
XARELTO-PM-ENG-10JUL2014-172618.pdf.http://www.bayerBoehringer Ingelheim CanadaLtd(2014)Pradaxa productmonograph.http://www.boehringeringelheim.ca;imagesfrom:colorbox.com;dailykos.com
+Dabigatranorrivaroxaban=
• Apixabanhasnohumandatainpregnancy,butshowednomaternalorfetalharminanimalstudies
• Edoxabananimalstudiesdemonstratednofetalharm
• DOACexcretioninbreastmilkisnotknown.
Pregnancy
CandidatesforaDOACtherapy:Specialpopulations
dailykos.com
Extremesofweight
CandidatesforaDOACtherapy:Specialpopulations
• Evidenceislimited• Patients<50–60kgwere2–13%ofDOACstudypopulations&
16%ofpatientswere>100kg• 1meta-analysisshowedthatforpatients>100kgrecurrentVTE
riskwas0.9(95%CI0.77-1.06)• Dabigatrandoesnotappeartobeaffectedbyextremesofweight• Weightmayaffectkineticsofanti-Xa’s buttheclinicalsignificance
isunknown. SchulmanNEJM2009;EINSTEINInvestigatorsNEJM2010;AMPLIFYNEJM 2013;HOKUSAINEJM2013;Stangier DJClin Pharmacokinet 2008;FrostJ.thromb Haemost 2009;Upreti VV2013BrJClin Pharmacol;Kubitza D2007 JClin Pharmacol;clipartbest.com;vanEs Blood.2014

Extremesofweight
CandidatesforaDOACtherapy:Specialpopulations
dailykos.com

Elderly
CandidatesforaDOACtherapy:Specialpopulations
• Evidencefromameta-analysisofthePhase3trialsstudyingVTE
• PooledDOACvs.VKAforage≥75yearsforrecurrentVTEorVTE-relateddeath:HR0.56(95%CI0.38-0.82)p=0.003
• PooledDOACvs.VKAforage≥75yearsforMajorbleeding:HR0.49(95%CI0.25-0.96)p=0.04
vanEs N.Blood.2014;pintrest.com

Elderly
CandidatesforaDOACtherapy:Specialpopulations
vanEs N.Blood.2014;pintrest.com

Thrombophilias
CandidatesforaDOACtherapy:Specialpopulations
• Evidenceislimited• Patientswiththrombophilias comprised2-18%ofthoseenrolled
inDOACtrials
• Post-hocdabigatrandatashowsnodifferenceinrecurrentVTE
• Exception:APS--3ongoingstudies• RAPS(Canada),TRAPS(Italy),ASTRO-APS(USA)
SchulmanS(2013)NEnglJMed368:709–718.EINSTEINInvestigators(2010)NEnglJMed363:2499–2510.AgnelliG(2013)NEngl JMed368:699–708. SchulmanS(2009)NEnglJMed361:2342–2352.SchulmanS(2014)Circulation129:764–772EINSTEIN–PEInvestigators(2012).NEnglJMed366:1287–1297. AgnelliG(2013)NEngl JMed369:799–808.Hokusai-VTEInvestigators(2013)NEnglJMed369:1406–1415;SchulmanSetal(2014)ASH56thannualmeetingDec 2014,session332abstract1544

Thrombophilias
CandidatesforaDOACtherapy:Specialpopulations

Thrombophilias
CandidatesforaDOACtherapy:Specialpopulations
APS=

Cancer
CandidatesforaDOACtherapy:Specialpopulations
• NodedicatedRCTevidenceforcancerpatientsexists• Systematicreviewsofthecancersubgroupfromtheclinical
trialssuggestDOACsaresimilartoVKAforVTErecurrenceriskreductionandnodifferenceinMB/CRNMB
• 1meta-analysissuggestedforVTErecurrenceRR0.57(95%CI0.36-0.91;p=0.02)
SchulmanS2013NEJMEINSTEINInvestigators2010NEJM;AgnelliG2013NEJM;SchulmanS2009NEJM;SchulmanS2014Circulation;EINSTEIN–PEInvestigators2012 NEJM;AgnelliG2013NEJM;Hokusai-VTEInvestigators2013NEJM;CastellucciLA.2014JAMA;CarrierM.2014Thromb Res;VedovatiMC.2015Chest;DiMinno MN.2014JThromb Haemost;FranchiniM.2015Thromb Res

Cancer
CandidatesforaDOACtherapy:Specialpopulations
SchulmanS2013NEJMEINSTEINInvestigators2010NEJM;AgnelliG2013NEJM;SchulmanS2009NEJM;SchulmanS2014Circulation;EINSTEIN–PEInvestigators2012 NEJM;AgnelliG2013NEJM;Hokusai-VTEInvestigators2013NEJM;CastellucciLA.2014JAMA;CarrierM.2014Thromb Res;VedovatiMC.2015Chest;DiMinno MN.2014JThromb Haemost;FranchiniM.2015Thromb Res;va Es 2015;KearonCAT102016
• AT10statesthat“ForVTEandcancer,wesuggestLMWHoverVKA(Grade2B),dabigatran(Grade2C),rivaroxaban(Grade2C),apixaban(Grade2C),oredoxaban(Grade2C).”
• NocomparisonofDOACwithLMWHtodate• 5ongoingtrials(rivaroxaban=2,apixaban=2,edoxaban=1)
clinicaltrials.govaccessed12MAR2016
Cancer
CandidatesforaDOACtherapy:Specialpopulations
KearonCAT102016
Cancer
CandidatesforaDOACtherapy:Specialpopulations
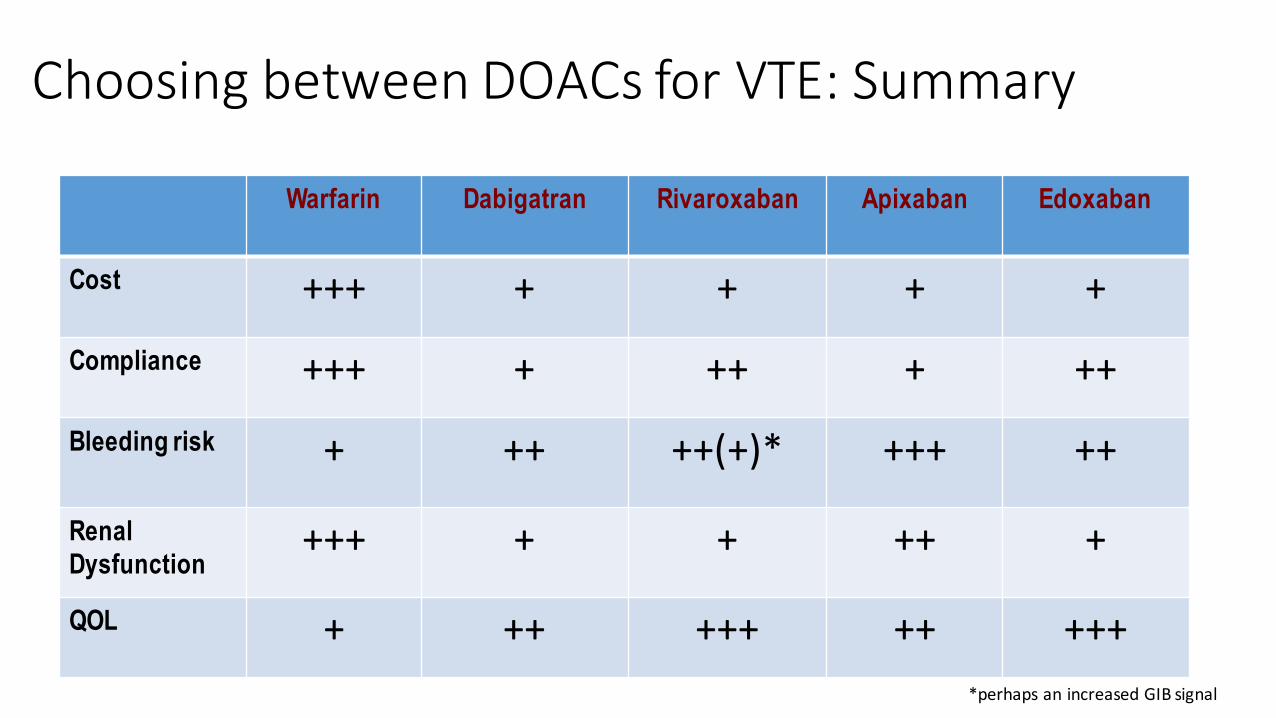
ChoosingbetweenDOACsforVTE:Summary
Warfarin Dabigatran Rivaroxaban Apixaban Edoxaban
Cost +++ + + + +
Compliance +++ + ++ + ++
Bleeding risk + ++ ++(+)* +++ ++
Renal Dysfunction
+++ + + ++ +
QOL + ++ +++ ++ +++*perhapsanincreasedGIBsignal

MonitoringofDOACs
youtube.com

MonitoringofDOACsDOACmonitoringisnotroutinelyrecommended
DetectclinicallyrelevantlevelsofDOACs• Urgentoremergentinvasiveprocedure• Hemorrhage• Neuraxial anesthesia• Majortrauma• Potentialthrombolysisinacutethromboembolism
Derived from:BurnettAEJThromb Thrombolysis(2016)41:206–232
MonitoringofDOACsDOACmonitoringisnotroutinelyrecommended
Detectexpectedon-therapylevelsofDOACs• Eventontherapy• Questionssurroundingadherence
Derived from:BurnettAEJThromb Thrombolysis(2016)41:206–232
MonitoringofDOACsDOACmonitoringisnotroutinelyrecommended
DetectofexcessivelevelsofDOACs• Hemorrhage• Overdose• Hepatic/renalimpairment• Druginteractions
Derived from:BurnettAEJThromb Thrombolysis(2016)41:206–232
MonitoringofDOACsDOACmonitoringisnotroutinelyrecommended
MostcircumstancesthatwouldtriggeradesiretomonitoreffectareurgentMajorBleeding:• Supportivecare• Administrationofbloodproducts• Asapplicable,administrationofantidote
Derived from:BurnettAEJThromb Thrombolysis(2016)41:206–232
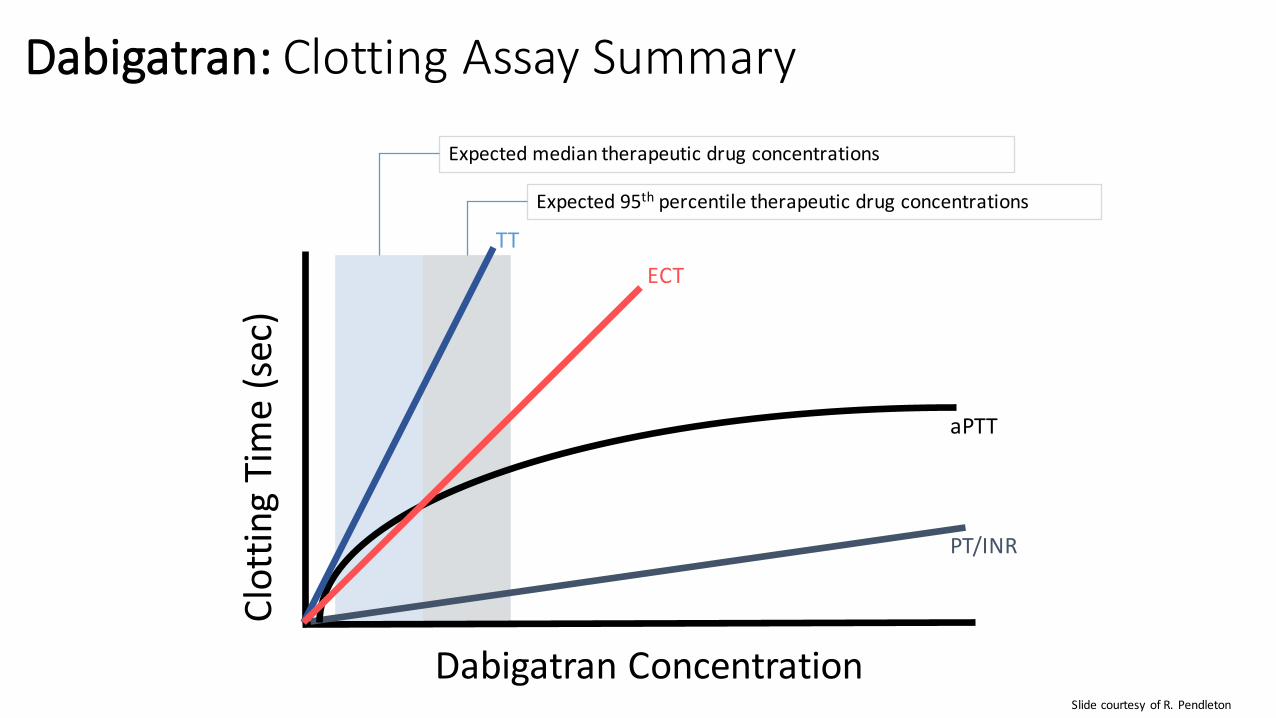
Dabigatran: ClottingAssaySummary
DabigatranConcentration
Clottin
gTime(sec)
PT/INR
aPTT
TTECT
Expectedmediantherapeuticdrugconcentrations
Expected95th percentiletherapeuticdrugconcentrations
SlidecourtesyofR.Pendleton

EvaluationofanticoagulanteffectofDabigatran
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
100 200 300 400 500 600 700 800 900
DabigatraneffectonaPTT
aPTT
ratio
DabigatranConcentration(ng/mL)Derived fromvanRynThromb Haemost 2010;103:1116

MonitoringofDOACs:SummaryDOACmonitoringisnotroutinelyrecommended
ItmaybeoccasionallyhelpfultoascertainaqualitativeaffectofDOACsPTT(dabigatran)PT(rivaroxaban,?apixaban)
Quantitativemeasurementmaybecomemorewidelyavailable• dTT,ECT(dabigatran)DOACanti-Xa (apixaban,rivaroxaban,edoxaban)• LMWHanti-Xa (apixaban,rivaroxaban,edoxaban)
Theclinicalvalueofmonitoringmaybeuncertain
Derived from:BurnettAEJThromb Thrombolysis(2016)41:206–232

MonitoringofDOACs:SummaryAssess for on-therapy
(quantitative)Interpretation Assess for on-therapy
(qualitative)Qualitative
assessment for drug
dabigatran dTT,ECT NLTTexcludes
PTT NL maybeunreliable
rivaroxaban Anti-Xa* NLanti-Xaexcludes
PT NLlikelyexcludes
apixaban Anti-Xa* NLanti-Xaexcludes
-- --
edoxaban Anti-Xa* NLanti-Xaexcludes
-- --
*Standardchromogenicanti-Xa calibratedtoUFHorLMWHmaybeused asaqualitativealternative DerivedfromBurnettJThromb Thrombolysis (2016)41:206

ReversalofDOACeffectIstherearoleforreversalagentsfortheDOACs?
• Shortt1/2
• ClinicaltrialsdemonstratethatregardlessoftheabsenceofanantidoteclinicallyimportantbleedingappearsnomorefrequentlyandmayoccurlesswithDOACscomparedwithVKA
BurnettAEJThromb Thrombolysis(2016)41:206–232;WuCThromb Res.2015;Castellucci LA, JAMA2014;Chai-Adisaksopha C.Blood2014

ReversalofDOACeffectIstherearoleforreversalagentsfortheDOACs?
EvidenceagainsttheroutineneedforDOACmonitoring• AT10summaryofbleedingrisk
• Real-worldexperienceDresdenregistryof1776patientsfollowed1.1years• 1082bleedingeventsoccurringin762patientswereevaluated• 3.4%experiencedmajorbleeding(ISTHcriteria)
• 62%treatedconservatively• 38%requiredsurgeryoranintervention
• FFPorPCCgivenin6patients(norFVII given)• 1deathataweek
• Conclusion:Inreallife,ratesofrivaroxaban-relatedMBmaybelower&atleastnotworsethanVKA
Beyer-Westendorf J.Blood.2014;124(6):955-962)

ReversalofDOACeffectIstherearoleforreversalagentsfortheDOACs?
• InVTEpatients:• Theper-100patientyearincidencerateofmajorbleedingofDOACvs.VKA:0.35(95%CI,0.17-0.68,p=0.0023).
• INallDOACs:
WuCThromb Res.2015;Castellucci LA, JAMA2014;Chai-Adisaksopha C.Blood2014

ReversalofDOACeffectIstherearoleforreversalagentsfortheDOACs?
• INallDOACs:
WuCThromb Res.2015;Castellucci LA, JAMA2014;Chai-Adisaksopha C.Blood2014

ReversalofDOACeffectIstherearoleforreversalagentsfortheDOACs?
• INallDOACs:
WuCThromb Res.2015;Castellucci LA, JAMA2014;Chai-Adisaksopha C.Blood2014
ReversalofDOACs

ReversalofDOACs:Idarucizumab
NEngl JMed2015;373:511-20.
� “Idarucizumab completelyreversedtheanticoagulanteffectofdabigatranwithinminutes”
� FDAApprovedOctober16,2015

Andexanet alpha
https://www.youtube.com/watch?v=LFf1WRGNZhg/ FromNEJM.org
RecombinantcompetitiveinhibitorofFactorXa

Andexanet AlfafortheReversalofXa Inhibitors
-94
100
-21
11
-92
96
-18
7
anti-Xaactivity Thrombinrestoration
RESULTS
apixaban placebo rivaroxaban placebo2
Siegal DMNEJM2015;373:2413
%

ReversalofDOACs:Aripazine (PER977)
http://cardiac-safety.org/wp-content/uploads/2014/11/3.-James-Costin_Perosphere.pdf accessed18Nov2015
Smallwatersolublemoleculethatnon-covalentlybendsthebindingsiteofallanticoagulants

ReversalofDOACs:Aripazine (PER977)
http://cardiac-safety.org/wp-content/uploads/2014/11/3.-James-Costin_Perosphere.pdf accessed18Nov2015
Perioperativeinterruption:TheDOACs
• About2.5MAmericansrequirelong-termanticoagulation
• About10%requireinterruptionannually
• Generally,interrupt4-5half-livesbeforeHBRprocedure
• OKtointerrupt2-3half-livesbeforeLBRprocedure
• Half-lifeincreasesascreatinineclearancedeclinesAndersonMClev.Clin JMed,2014, 8;629;

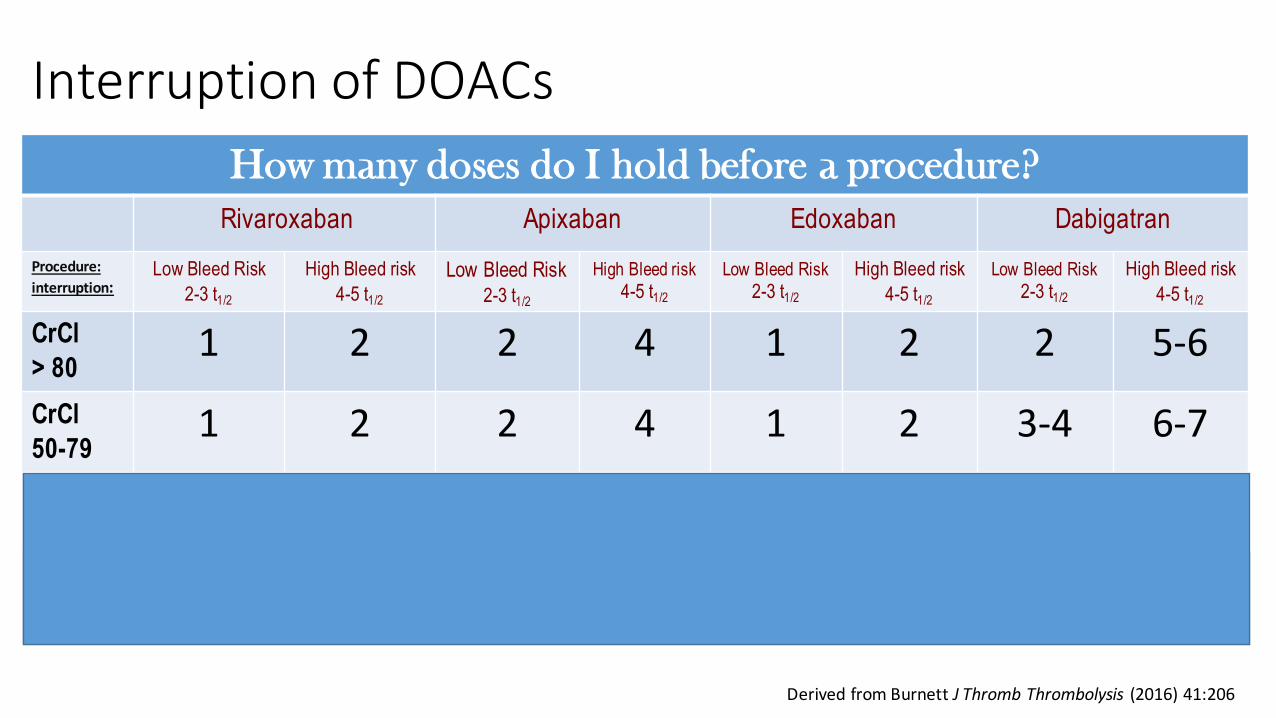
InterruptionofDOACsHow many doses do I hold before a procedure?
Rivaroxaban Apixaban Edoxaban DabigatranProcedure:interruption:
Low Bleed Risk2-3 t1/2
High Bleed risk4-5 t1/2
Low Bleed Risk2-3 t1/2
High Bleed risk4-5 t1/2
Low Bleed Risk2-3 t1/2
High Bleed risk4-5 t1/2
Low Bleed Risk2-3 t1/2
High Bleed risk4-5 t1/2
CrCl> 80
1 2 2 4 1 2 2 5-6CrCl50-79
1 2 2 4 1 2 3-4 6-7CrCl30-49
1 2 3-4 6-7 1 2 4-5 7-8CrCl15-29
1-2 2-3 3-4 6-7 2 3-4 5-7 9-12
DerivedfromBurnettJThromb Thrombolysis (2016)41:206
InterruptionofDOACsHow many doses do I hold before a procedure?
Rivaroxaban Apixaban Edoxaban DabigatranProcedure:interruption:
Low Bleed Risk2-3 t1/2
High Bleed risk4-5 t1/2
Low Bleed Risk2-3 t1/2
High Bleed risk4-5 t1/2
Low Bleed Risk2-3 t1/2
High Bleed risk4-5 t1/2
Low Bleed Risk2-3 t1/2
High Bleed risk4-5 t1/2
CrCl> 80
1 2 2 4 1 2 2 5-6CrCl50-79
1 2 2 4 1 2 3-4 6-7CrCl30-49
1 2 3-4 6-7 1 2 4-5 7-8CrCl15-29
1-2 2-3 3-4 6-7 2 3-4 5-7 9-12
DerivedfromBurnettJThromb Thrombolysis (2016)41:206

InterruptionofDOACsHow many doses do I hold before a procedure?
Rivaroxaban Apixaban Edoxaban DabigatranProcedure:interruption:
Low Bleed Risk2-3 t1/2
High Bleed risk4-5 t1/2
Low Bleed Risk2-3 t1/2
High Bleed risk4-5 t1/2
Low Bleed Risk2-3 t1/2
High Bleed risk4-5 t1/2
Low Bleed Risk2-3 t1/2
High Bleed risk4-5 t1/2
CrCl> 80
1 2 2 4 1 2 2 5-6CrCl50-79
1 2 2 4 1 2 3-4 6-7CrCl30-49
1 2 3-4 6-7 1 2 4-5 7-8CrCl15-29
1-2 2-3 3-4 6-7 2 3-4 5-7 9-12
DerivedfromBurnettJThromb Thrombolysis (2016)41:206

InterruptionofDOACsHow many doses do I hold before a procedure?
Rivaroxaban Apixaban Edoxaban DabigatranProcedure:interruption:
Low Bleed Risk2-3 t1/2
High Bleed risk4-5 t1/2
Low Bleed Risk2-3 t1/2
High Bleed risk4-5 t1/2
Low Bleed Risk2-3 t1/2
High Bleed risk4-5 t1/2
Low Bleed Risk2-3 t1/2
High Bleed risk4-5 t1/2
CrCl> 80
1 2 2 4 1 2 2 5-6CrCl50-79
1 2 2 4 1 2 3-4 6-7CrCl30-49
1 2 3-4 6-7 1 2 4-5 7-8CrCl15-29
1-2 2-3 3-4 6-7 2 3-4 5-7 9-12
DerivedfromBurnettJThromb Thrombolysis (2016)41:206
Follow-upforpatientsonaDOAC
• Follow-upvisitsshouldfocuson3objectives:• EnsuringproperDOAC• Maximizingadherence• Minimizingbleeding.
• A(adherence)• B(bleeding)• C(creatinineclearance)• D(druginteractions)• E(examination)• F(follow-up)
GladstoneDJAnnInternMed.2015;163:382-385.

Follow-upforpatientsonaDOAC
http://thrombosiscanada.ca
GladstoneDJAnnInternMed.2015;163:382-385.

SummaryDOACsareeffectiveandsafeforthelong-termtreatmentofVTE
Forthe1st timeamajorguidelinerecommendsatreatmentotherthanVKAforVTEPatientsshouldbeconsideredonacasebycasebasisforthe1st lineuseofDOACs
BewareofDOACuseamongspecialpopulations
RoutinemonitoringofDOACsisnotrecommended
ReversalagentsfortheDOACsarehere(withmoretocome)
Anticoagulantsaredangerousdrugsthatrequirethoughtfuluseandfollow-up