the diabetic foot - podiatry m
TRANSCRIPT
THEDIABETIC
FOOT
NOVEMBER/DECEMBER 2004 • PODIATRY MANAGEMENTwww.podiatrym.com 195
encounter. Further, it is commonknowledge that over one-half of allfoot problems that people with dia-betes present with include involve-ment of the skin and/or the toe-nails. This article is designed toclarify these dermatologic entities.
Diabetes mellitus has a signifi-cant effect on the skin and nails.Dermatologic manifestations in dia-betes mellitus are universal, theprevalence approaching 100%. Thefindings range from the initial clini-
Continued on page 196
Welcome to Podiatry Management’s CME Instructional program. Our journal has been approved as a sponsor of Contin-uing Medical Education by the Council on Podiatric Medical Education.
You may enroll: 1) on a per issue basis (at $17.50 per topic) or 2) per year, for the special introductory rate of $109 (yousave $66). You may submit the answer sheet, along with the other information requested, via mail, fax, or phone. In the nearfuture, you may be able to submit via the Internet.
If you correctly answer seventy (70%) of the questions correctly, you will receive a certificate attesting to your earned cred-its. You will also receive a record of any incorrectly answered questions. If you score less than 70%, you can retake the test atno additional cost. A list of states currently honoring CPME approved credits is listed on pg. 206. Other than those entities cur-rently accepting CPME-approved credit, Podiatry Management cannot guarantee that these CME credits will be acceptable byany state licensing agency, hospital, managed care organization or other entity. PM will, however, use its best efforts to ensurethe widest acceptance of this program possible.
This instructional CME program is designed to supplement, NOT replace, existing CME seminars. Thegoal of this program is to advance the knowledge of practicing podiatrists. We will endeavor to publish high quality manuscriptsby noted authors and researchers. If you have any questions or comments about this program, you can write or call us at: Podia-try Management, P.O. Box 490, East Islip, NY 11730, (631) 563-1604 or e-mail us at [email protected].
Following this article, an answer sheet and full set of instructions are provided (p. 206).—Editor
Continuing
Medical Education
IntroductionDiabetic patients presenting
with lower extremity skin problemsare among the most common oc-currences that podiatric physicians
By Kenneth B. Rehm, DPM
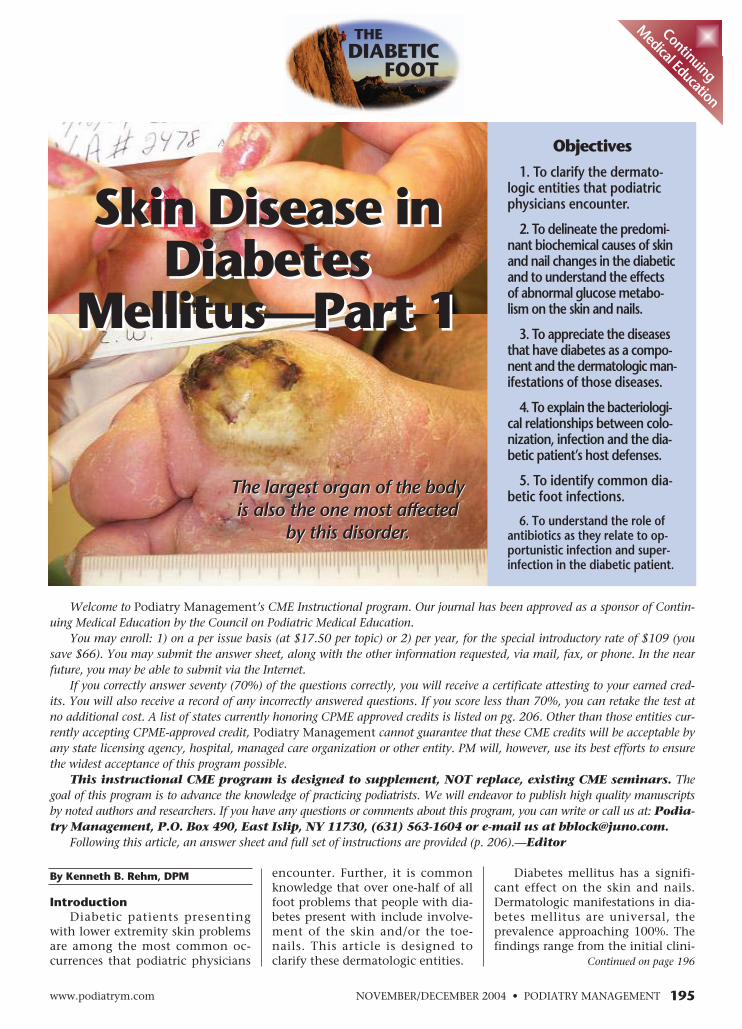
Skin Disease inDiabetes
Mellitus—Part 1
The largest organ of the bodyis also the one most affected
by this disorder.
Objectives
1. To clarify the dermato-logic entities that podiatricphysicians encounter.
2. To delineate the predomi-nant biochemical causes of skinand nail changes in the diabeticand to understand the effectsof abnormal glucose metabo-lism on the skin and nails.
3. To appreciate the diseasesthat have diabetes as a compo-nent and the dermatologic man-ifestations of those diseases.
4. To explain the bacteriologi-cal relationships between colo-nization, infection and the dia-betic patient’s host defenses.
5. To identify common dia-betic foot infections.
6. To understand the role ofantibiotics as they relate to op-portunistic infection and super-infection in the diabetic patient.
Skin Disease inDiabetes
Mellitus—Part 1
The largest organ of the bodyis also the one most affected
by this disorder.

valuable aid in the prevention andtreatment of not only the devastat-ing dermatological effects of thedisease, but the complications ofthe disease ingeneral.
TheBiochemistry ofDermatologicalChanges
The predomi-nant biochemicalcause of diabetic-related changes inthe skin involvesthe attachment ofthe glucosemolecule withmany proteins, includinghemoglobin. This is termed non-enzymatic glycosylation. The resultof this union produces stable cova-lent products, which results in dif-ferent physical and chemical prop-erties than that of the original pro-teins. Most proteins evaluated seemto be involved in this process.
When glucose is in solution, itexists as a stable pyranose ring thatis in equilibrium with the openchain aldehyde form. The NH2group of the protein (either on theepsilon-amino group of the aminoacid lysine or on the alpha-aminogroup of the N-terminal amino
acid) combines withthe double-bondedoxygen of the alde-hyde, resulting in aSchiff base oraldimine. The Schiffbase may reconfigure,resulting in the forma-tion of a ketoamine.
Amador Rearrange-ment
This process iscalled the Amador re-arrangement and theketoamines are termedAmador products. TheAmador products reactwith amino groups onother proteins to formglucose-derived inter-molecular cross-links.This results in colorchanges of collagenthat are confirmed byspectrophotometricmeasurement to corre-
late with diabetes-related complica-tions. Among the advanced gly-colysation end products that havebeen identified in the skin is a yel-
low imidazolecompound andthe amino acidp e n t o s i d i n e ,which has beendemonstrated tocorrelate with ascore of diabeticcompl icat ions .Non-enzymaticglycosylation ofthe red blood cellmembrane isthought to causestiffness in the
erythrocyte of diabetics. Non-enzy-matic glycosylation of collagen re-sults in increased stiffness in colla-gen and resistance to normal enzy-matic degradation.
Non-Enzymatic GlycosylationTo a minor extent, non-enzy-
matic glycosylation occurs at nor-mal blood sugar levels and could beresponsible for some of the mechan-ical changes of collagen and skin,which are characteristic of the agingprocess. This process, however, is ap-parently accelerated with diabetesmellitus and the resultant changesin solubility and tertiary structure ofproteins could be responsible formany complications of the disease.
Clinically, non-enzymatic glyco-sylation results in alterations of thestructural stability of the skin be-cause of the change in the quality ofthe keratin and collagen formation(figures 3, 4, 7, 8, 14). These alter-ations predispose the diabetic to in-creased callus formation. Althoughkeratin and collagen disturbanceshave been noted in diabetics thatare normoglycemic, they are mostcommonly related to elevated bloodglucose levels making the tissuerigid, inflexible, and more resistantto normal collagenase digestion.Such glycosylated keratin will buildup easier and more abundantly as aresult of repetitive pressures. It willnot shed from the superficial layersof the foot and therefore builds uphyperkeratosis on the plantar walk-ing surface and ultimately causes aplantar ulceration (figures 3, 12, 13).The most destructive lesion in the
Continued on page 197
196 www.podiatrym.comPODIATRY MANAGEMENT • NOVEMBER/DECEMBER 2004
Diabetes Mellitus...
cal presentation to the expres-sions of long-term involvement,
from commonplace to life-threat-ening complications. The clinicaldermatological manifestation of thedisease is directed in various waysbut is thought to be universally in-fluenced by the effect that the at-tachment of glucose to protein hason the structure and function ofthat protein. The increased cross-linking of collagen in diabetic pa-tients is responsible for the fact thatthe skin is commonly thicker in dia-betics than in non-diabetics (figure14). Complex glycosylation end-products are thought to be responsi-ble for the yellowing of the skin andnails (figures 11, 14).
Erythema of the face or theperiungual tissues is thought to bea result of engorgement of the post-capillary venules in the papillarydermis secondary to the increasedviscosity of blood due to stiff redblood cell membranes. An astutewound clinician is able to use theseskin changes as a valid clinical indi-cator of the patient’s current condi-tion, as well as his/her pastmetabolic status and the control ofhis/her hyperglycemic state. Per-ceptive recognition of the subtletiesof this clinical presentation is a
Contin
uing
Medica
l Edu
catio
n
Complex glycosylation
end-products arethought to be
responsible for theyellowing of the skin
and nails.
Figure 1: Moist skin in the webspace predisposes to infection and ulceration.
Figure 2: Candida infection of the webspace.

NOVEMBER/DECEMBER 2004 • PODIATRY MANAGEMENTwww.podiatrym.com 197
In a study of other skin mani-festations of hemochromatosis,there was a high frequency ofichthyosis-like states and koilony-chias, a condition characterized by
a flattened nail that has concavi-ties, also known as a spoon nail. Anassociation with necrobiosis lipoidi-ca and a black keratinous cyst hasbeen reported.
Porphyria Cutanea TardaPorphyria cutanea tarda (PCT)is
a common condition seen in dia-betes mellitus. It is characterizeddermatologically by photosensitivi-ty on exposedareas and bullaeon the dorsum ofthe hands. If bul-lae develop onexposed feet, it isreasonable to as-sume that thismight be a mani-festation of PCT.A feature of PCTis also hypertri-chosis.
MyxedemaMyxedema ,
causing puffinessof the face andpre-tibial edema,can be associatedwith diabetesmellitus.
Lipid Abnormalities
Lipid abnor-malities associat-ed with diabetescan present amyriad of skinchanges includ-ing those associat-ed with lipodys-trophy.
skin of the diabetic is a neuropathicplantar ulceration.
One researcher describes severalsteps in the development of a neu-ropathic plantar ulceration in thediabetic foot.
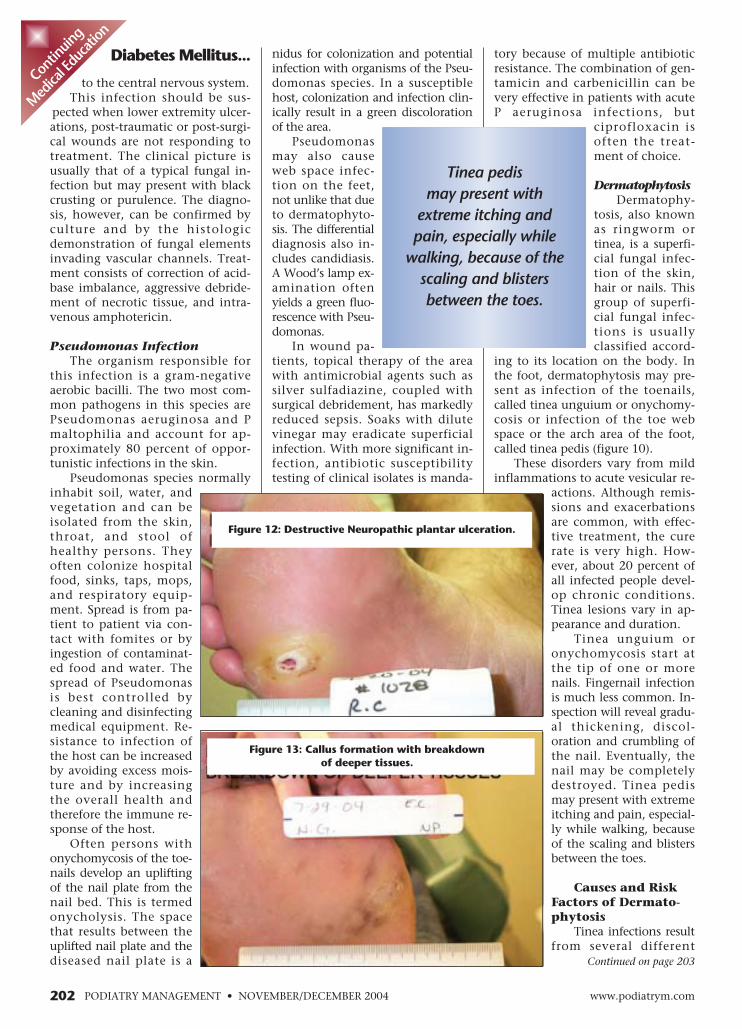
1. The initial hyperkeratotic le-sion (figure 13)
2. A weakening and breakdownof deeper tissues, with continuedrepetitive pressure (figure 4)
3. Eventual cavity formationthat fills with blood (figure 15)
4. Enlargement to the point ofrupturing forming an ulceration(figure 3)
Dermatologic Manifestations ofDiseases Associated WithDiabetes
It is important to realize thatwhen a patient presents with dia-betes and also a dermatologicproblem, that problem may not bedirectly related to the diabetes butto another disease process. Thefollowing are examples of suchdiseases.
Maturity onset diabetes ofyouth syndrome may have an auto-somal dominant inheritance pat-tern. This appears to be common inindividuals from India and in Afro-Americans. The dermatologic asso-ciation with this syndrome is facialflushing that is induced by chlor-propamide and alcohol, the combi-nation found in sherry, amongother alcohol-related substances.This flushing is significant in that itcould be bothersome to the person,but even more important, it seemsto be a marker for other diabeticcomplications.
HemochromatosisHemochromatosis is often
caused by an autosomal-recessivegene. Persons with this genetic syn-drome often have insulin resistanceand diabetes mellitus in associationwith manifestations of iron over-load, such as bronzing of the skin.The sequelae of iron overload arepreventable through simple phle-botomy. It is therefore important toscreen all first-degree relatives ofpatients with hemochromatosis forabnormal iron metabolism by mea-suring transferring saturation andferritin levels.
Diabetes Mellitus... Acanthosis NigricansAcanthosis nigricans
(AN) is characterized by vel-vety to verrucous-like hyperkera-totic, hyperpigmented plaques thatare bilaterally symmetric (figure 5).These plaques are most commonlyfound on the neck, in the flexuralareas and the axillae. The inconsis-tency of cutaneous involvement,however, is striking. The clinical pre-sentation can vary from subtle hy-perpigmented spots and papillarythickening that affect only a fewareas to an aggressive, deeply pig-mented verrucous process that couldinvolve the entire integument in-cluding mucous membranes, palmsand soles. Distinguishing this disor-der from other verrucous-like lesionsis the presence of hyperkeratosis, pa-pillomatosis, areas of acanthosis thatmay alternate with areas of skin at-rophy, and increased melanin in thebasal epidermis as documentedthrough the use of light microscopy.It is this author’s experience that ANcould be stimulated by the develop-
Continued on page 198
Continuing
Medical Education
Hemochromatosis is often caused
by an autosomal-recessive gene.
Figure 3: The fourth stage in the de-velopment of a pressure related plan-
tar ulceration. Notice yellowing of the skin surrounding the ulceration.
Figure 4: Hyperkeratotic lesion with weakening of the deepertissues. Stage 2 in the development of the plantar ulceration.

phy and muscle cramps12. Polycystic ovary disease
(Stein-Leventhal syndrome)
Endocrine disorders associated withinsulin resistance and acanthosisnigricans:
1. Acromegaly2. Ovarian hyperthecosis
3. Addisonism4. Cushing’s Disease5. Hypothyroidism6. Pineal hyperplasia
Medications associated with acan-thosis nigricans and possible in-sulin resistance:
1. Nico-tinic Acid
2. Di-ethylstilbe-strol
3. Gluco-corticoids
CutaneousInfectionsin DiabetesMellitus
Bacteriolo-gy of theSkin
A discus-sion of infec-tions of thediabetic footmust takeinto consid-eration twoi m p o r t a n tpathogenicfeatures: 1)the underly-ing metabol-ic disorderwith its asso-ciated de-g e n e r a t i v ec o m p l i c a -
tions; and 2) the bacteriologic floraof the lower extremity. This discus-sion must consider the microbialecology of the human skin and therelationships between colonization,infection and the diabetic patient’shost defenses against infection.
Non-enzymatic glycosylationand its effect on skin characteristicsand the effect that autonomic neu-ropathy has on the dryness andstiffness of the skin are importanteffects of the underlying metabolicdisorder and participate in the sus-ceptibility for infection (figure 8).
Variations in the bacterial floraof the lower extremity must be dis-cussed to fully understand skinmarkers that relate to diabeticlower extremity infections. Differ-ent areas of the lower extremity arepopulated by different complexand changing bacterial and fungalflora. This is primarily due to thesedifferent environments, each ofwhich predispose to different typesof microbial colonization. On thedry portions of the lower leg andankle, the flora is quite restricted(about 1000 bacteria per squarecentimeter) because of the physicaland chemical conditions on thesurface.
Microbial Growth and SurvivalMicrobial growth and survival
are negatively influenced by thefollowing factors. Lower environ-mental temperatures create a lessthan optimal environment neededfor human pathogens to thrive. Thepresence of metabolic products ofthe skin (e.g., fatty acids) have di-rect antimicrobial chemical effectsand predispose to extremes of pH(especially acidity) and ionicity onthe skin surface. In addition, therelatively arid surface of the dor-sum of the foot and the lower legand ankle allows only those mi-crobes resistant to drying able tothrive.
The increased density and thevariety of organism species in thetoe webs, which is even greaterthan that which is found in the ax-illa (where more than one millionbacteria per square centimeter canbe recovered) attest to the criticalimportance of moisture in bacterialand fungal growth. The toe webstypically are a nidus for the pres-
Continued on page 199
198 www.podiatrym.comPODIATRY MANAGEMENT • NOVEMBER/DECEMBER 2004
Diabetes Mellitus...
ment of a plantar wound andinvolves the wound edges, and
could interfere with its healing.The relationship between insulin
resistance and acanthosis nigricansis well established and especiallyclear. High plasma levels of insulin,stimulated by the non-responsive re-ceptor sites, are thought to con-tribute to the development of AN.Many syndromes associated withAN have been linked to the presenceof some form of insulin resistance.
These include the following:1. Alström syndrome2. Ataxia-telangiectasia3. Bloom syndrome4. Capozucco syndrome5. Crouzon’s disease (craniofa-
cial dysostosis)6. Lawrence-Seip syndrome
(total lipodystrophy)7. Leprechaunism8. Prader-Willi syndrome9. Rabson’s syndrome10. Rud’s syndrome11. Syndrome of acral hypertro-
Contin
uing
Medica
l Edu
catio
n
The relationshipbetween insulinresistance and
acanthosis nigricans iswell established.
Figure 6: Macerated webspace.
Figure 5: Acanthosis Nigricans.

NOVEMBER/DECEMBER 2004 • PODIATRY MANAGEMENTwww.podiatrym.com 199
tremity, especially in diabetics, hasa significant effect on which micro-bial flora will affect it, since manyof the common bacteria and fungi
fail to grow at temperatures muchbelow 37 degrees C and Mycobac-terium marinum and the dermato-phytes can flourish in areas wherethe temperature seldom exceeds 30to 31 degrees C.
ence of Corynebacterium minutissi-mum, Pseudomonas, Herellea, Can-dida, nonlipophilic diphtheroids,and enterobacteria (figure 1). Thiscontrasts markedly with the coccaland lipophilic diptheroid flora ofthe lower calf and ankle. When thefeet are too moist they favor in-creased microbial density as well. Inaddition, this higher microbialdensity of the intertriginous areasresults in a higher surface pH thananywhere else in the body becausethe urea and other nitrogenoussubstances are metabolized, result-ing in ammonia formation. Nor-mally, the low availability of car-bohydrate substrates prevents acidproduction.
Skin pHSince healthy skin has a slightly
acid pH, a more alkaline pH on theskin surface, as is the case with in-creased microbial density and expo-sure to substances with an alkalinepH (such as many commercialcleansers and hand soaps) con-tributes to interruptionsof skin integrity. Oncethe skin integrity is dis-turbed, a homeostatic re-pair mechanism is stimu-lated that causes therapid repair of barrierfunction. Continued ex-posure to a high micro-bial load, alkaline sub-stances, or continued ex-posure to unfavorableenvironmental factorswill slow down repair byinhibiting normal skinacidity.
Interactive FloraThe significance of
interacting flora is exem-plified most on the skinof the toe webs, as is thecase in many diabetics,where combined colo-nization by dermato-phytes, Staphylococcusaureus, and Candida al-bicans intensifies itchingand aggravates the in-flammatory response(fig-ure 1, 2, 6).
The low temperatureof the distal lower ex-
Diabetes Mellitus... Much of what isknown about dermato-phyte fungi on the skincomes from studies relating topatients with fungal infections andotherwise normal skin.
It is interesting to note thatthere can be dermatophytosis with-out clinical evidence of skin disease.In one study, foot scrapings fromrecruits demonstrated that 18.6%had colonization of one or moreof three fungal species (Trichophy-ton mentagrophytes, T. rubrum, orEpidermophyton floccosum) with-out any clinical evidence of disease.Similarly, in one study of 100 gener-ally well-controlled diabetics, 70were found to have dermatophyto-sis of the inter-digital areas of thefeet.
Environmental FactorsWeight bearing, body chem-
istry, poor circulation, trauma tothe feet, and the environment thatis created inside our shoes predis-pose a person with diabetes to cer-tain bacteriological problems. Theamount of fatty acids secreted by
the sebaceous glands isless and this low fattyacid concentration maypredispose the person toringworm infection. Ifthe feet are cool, toomoist and contain moredebris factors (dry skin,subungual debris, skinscaling) then dermato-phyte and atypical my-cobacterial infectionsbecome common-place.Interdigital dermatophy-tosis is a predisposingfactor for the occurrenceof bacterial infection be-cause the resultant epi-dermal fissures and ero-sions create portals ofentry for the pyogeniccocci, leading to celluli-tis and “infectious” gan-grene of the digits.In the diabetic patient,even minor trauma canlead to stasis and ulcera-tion, followed by pene-tration of potentiallypathogenic skin fungiand bacterial and thenby overt infection. If the
Continuing
Medical Education
The toe webs typicallyare a nidus for the
presence ofCorynebacteriumminutissimum,Pseudomonas,
Herellea, Candida,nonlipophilic
diphtheroids, andenterobacteria.
Figure 7: Ulcerated callus.
Figure 8: Left plantar surface, dry and cracked, rightafter treatment with conditioning cream.
Continued on page 200

tion are found to be reduced. Thepresence of these immodeficienciesappear to be correlated, at least inpart, to adequate glycemic control.
Other accompaniments of dia-betes that predispose to infectiouscomplications are poor granulomaformation andprolonged persis-tence of abscesses.Also, diabetic pa-tients tend tohave a higher car-rier rate of Staphy-lococcus aureuson the skin. Thisvirulent pathogencan become infec-tious when theprotective skinbarrier is broken.Trauma, various types of skin disor-ders discussed in this paper, as wellas fungal skin and nail infectionsthat disproportionately plaque thediabetic patient all create potentialsites for bacterial invasion by the le-sions that cause breaks in the pro-tective skin barrier.
A skin infection in a personwith immunopathy, such as a dia-betic, is potentially disastrous (fig-ure 9). This morbidity is intensifiedby the unique anatomy of the foot.A skin infection can travel to thestructures in the various compart-ments, tendon sheaths, and neu-rovascular bundles to favor itsspread. These compartments are
bound by rigid fa-cial and bonystructures, suchthat the edemaand pressure ofthe infectiousmaterials cancause an extremeelevation of com-partment pres-sures, causing is-chemic necrosisand possible gan-grenous changesof these confinedtissues. The etiol-ogy of gangrene
in any part of the foot is often dueto the infectious process.
Clinical DiagnosisThe clinical diagnosis of a foot
infection is as important as the mi-crobiologic presentation because
all skin lesions are colonized withmicroorganisms; and infection ofthe skin, or cellulitis, requires thepresence of purulent secretions ortwo or more signs or symptoms ofinflammation (erythema, edema,and calor). Many patients, but not
all, with sensoryneuropathy donot report anypain with the in-fection. Infectionshould be sus-pected at the firstappearance of alocal foot prob-lem, whether it ispain, swelling,ulceration, sinustract formation,or crepitation.
Cellulitis may be accompanied bysystemic signs and symptoms ormetabolic disorder, such as severe hy-perglycemia, ketosis, or azotemia. In-fection should always be consideredeven when the local signs of cellulitisare less severe than might be expect-ed. Benign appearing ulcerationswith no outward signs of inflamma-tion may be associated with underly-ing osteomyelitis. In addition, morethan half of all patients with diabeticfoot infections lack a fever, elevatedwhite blood cell count, or elevatederythrocyte sedimentation rate.Therefore even though the clinicaland/or the systemic signs and symp-toms may be mild, the diabetic pa-tient may be suffering from a poten-tially very serious infection. Alwayshave a high index of suspicion.
Common Diabetic FootInfections
There are several infectionswhich can be of concern in personswith diabetes mellitus. There iscontroversy whether these are morecommon in the diabetic popula-tion; nevertheless, they are com-mon and may be life and/or limb-threatening and are an importantpart of any discussion on skin dis-ease in diabetes mellitus.
Candida InfectionsThe incidence of Candida infec-
tion in the hands and feet appearsto be relatively the same in the dia-betic and the non-diabetic popula-tion. When it does occur, its pre-
Continued on page 201
200 www.podiatrym.comPODIATRY MANAGEMENT • NOVEMBER/DECEMBER 2004
Diabetes Mellitus...
skin, especially on the plan-tar surface of the feet, loses its
integrity, becomes dry, cracked,fissured and hard, the foot then isat increased risk for damage, sores,lesions, ulcers, and therefore alltypes of infections. Therefore, pre-venting the feet from becomingcontaminated with debris, too wetor too dry, thereby maintainingthe balance of proper lubrication,skin conditioning, and hygiene,becomes an essential part of pre-venting foot infection (figure 8).
VirusesThere is little information on
the density or variety of virusesfound on healthy skin, since theyare difficult to identify in the ab-sence of skin lesions. Virus replica-tion would presumably be restrict-ed to the deeper layers of the skinbecause viruses are obligate para-sites of living cells, and there are noliving cells in the upper layers ofthe skin. The viruses, however, thatparasitize bacteria, called bacterio-phages, must be present in signifi-cant numbers within the residentbacterial flora (e.g., S. aureus andcutaneous diphtheroids).
Predisposing FactorsPredisposing factors, such as
metabolic derangements, faultywound healing, neuropathy, vascu-lopathy and im-munologic distur-bances allow theperson with dia-betes to be moreprone to foot in-fection than then o n - d i a b e t i c .Among the de-fects in the hostimmune responseassociated withdiabetes mellitusis an impairmentof polymor-phonuclear leuko-cyte function, in-cluding abnormalities of migration,phagocytosis, intracellular killing,and chemotaxis. Also, ketosis im-pairs leucocyte function. In addi-tion, there is evidence that the cel-lular immune responses as well asmonocyte and complement func-
Contin
uing
Medica
l Edu
catio
n
The etiology of gangrene in
any part of the foot is often due to theinfectious process.
Diabetic patients whose blood sugar
is uncontrolled and who may be in
ketosis are sometimespredisposed to a fungal
infection calledmucormycosis.

NOVEMBER/DECEMBER 2004 • PODIATRY MANAGEMENTwww.podiatrym.com 201
Thirdly, Candida infection ofthe hands and feet can show up asan abnormality of the nail plate.This can literally be indistinguish-able from a fungus infection of thenail and the only way to differenti-ate the two is to do a nail plate cul-ture. These cultures are positive forCandida approximately five percentof the time. Even then, it is neces-sary to ascertain whether Candidais a contaminant or secondary toanother causative organism.
The clinical presentation of nail
sentation may be influenced by thepresence of diabetes. It usually pre-sents in one of three ways in the di-abetic patient.
Firstly, Candida causes parony-chia, usually of the fingernails, butcan occur on the toenails. It oftenbegins at the unguilabia as erythe-ma, edema, and separation of medi-al and lateral margins of the nailfrom the skin. Further infection ofthe yeast organism involves theproximal nail fold andsubsequent separation ofthe nail from the cuticle.Moisture trapped in thedefects created encour-ages further growth ofyeast and repeatedepisodes of erythemaand edema. A secondarybacterial infection canoccur, as evidenced by apurulent discharge andpain, if the patient hasadequate sensation. Thediagnosis of a yeast in-fection can be estab-lished by performing aKOH preparation on ex-truded serous material.
Secondly, Candidainfection can affect theweb spaces of the handsand the feet. The spacebetween the 3rd and 4thfinger and between the4th and 5th toes is mostcommonly affected (fig-ure 2). Occlusion of theskin in these areascaused by apposing sur-faces of the skin of thetoes or fingers allowsthis area to retain mois-ture, and serves as anidus for the growth ofyeast. The increased sug-ars and their metabolicby-products further en-courage its growth. Clin-ically, this infection ap-pears as a white macerat-ed patch of skin, oftenwith central peeling.Candida infection of thetoe web spaces is oftenmistaken for a dermato-phyte infection, whichcan be differentiated bya KOH preparation.
Diabetes Mellitus... yeast or fungus infectionis the same. There is rarelyprimary involvement of live tis-sue, but the nail folds can becomereactively inflamed, callused and sec-ondarily infected with bacteria. Therecan be subungual debris and reactivehypertrophy of tissue. The nail platebecomes thickened, discolored withdistal whitening or yellowing. Theconsistency can change and becomepowdery or brittle.
One must appreciate that the pri-mary nail plate Candida infection
does not pose a special riskin diabetics in and of itself.When the nail plate getsabnormally thickened andis able to cause a callusednail groove, or to becomeingrown or to causeparonychia with a sec-ondary bacterial infection,this poses a very signifi-cant risk for the personwith loss of protective sen-sation and/or diabetes.This is especially truewhen one considers thatpersons with diabetes mel-litus often suffer a compro-mised immune response(i.e., immunopathy).
Mucormycosis Infections
Diabetic patientswhose blood sugar is un-controlled and who maybe in ketosis are some-times predisposed to afungal infection calledmucormycosis becauseof the decreased abilityof their neutrophils tophagocytize and adhereto endothelial walls. Fur-thermore, the acidosisand hyperglycemia pro-vide an excellent envi-ronment for this fungusto grow. The presence ofsystemic or local acidosisis an important risk fac-tor for infection, no mat-ter what causes the aci-dosis. Traumatized or ul-cerated skin can be thesite of involvement. Der-mal infections frequent-ly metastasize via theblood stream and spread
Continuing
Medical Education
Figure 9: Deep diabetic skin infection.
Figure 10: Onychomycosis.
Figure 11: Yellowing of great toenail.
Continued on page 202
nidus for colonization and potentialinfection with organisms of the Pseu-domonas species. In a susceptiblehost, colonization and infection clin-ically result in a green discolorationof the area.
Pseudomonasmay also causeweb space infec-tion on the feet,not unlike that dueto dermatophyto-sis. The differentialdiagnosis also in-cludes candidiasis.A Wood’s lamp ex-amination oftenyields a green fluo-rescence with Pseu-domonas.
In wound pa-tients, topical therapy of the areawith antimicrobial agents such assilver sulfadiazine, coupled withsurgical debridement, has markedlyreduced sepsis. Soaks with dilutevinegar may eradicate superficialinfection. With more significant in-fection, antibiotic susceptibilitytesting of clinical isolates is manda-
tory because of multiple antibioticresistance. The combination of gen-tamicin and carbenicillin can bevery effective in patients with acuteP aeruginosa infections, but
ciprofloxacin isoften the treat-ment of choice.
DermatophytosisDermatophy-
tosis, also knownas ringworm ortinea, is a superfi-cial fungal infec-tion of the skin,hair or nails. Thisgroup of superfi-cial fungal infec-tions is usuallyclassified accord-
ing to its location on the body. Inthe foot, dermatophytosis may pre-sent as infection of the toenails,called tinea unguium or onychomy-cosis or infection of the toe webspace or the arch area of the foot,called tinea pedis (figure 10).
These disorders vary from mildinflammations to acute vesicular re-
actions. Although remis-sions and exacerbationsare common, with effec-tive treatment, the curerate is very high. How-ever, about 20 percent ofall infected people devel-op chronic conditions.Tinea lesions vary in ap-pearance and duration.
Tinea unguium oronychomycosis start atthe tip of one or morenails. Fingernail infectionis much less common. In-spection will reveal gradu-al thickening, discol-oration and crumbling ofthe nail. Eventually, thenail may be completelydestroyed. Tinea pedismay present with extremeitching and pain, especial-ly while walking, becauseof the scaling and blistersbetween the toes.
Causes and RiskFactors of Dermato-phytosis
Tinea infections resultfrom several different
202 www.podiatrym.comPODIATRY MANAGEMENT • NOVEMBER/DECEMBER 2004
Diabetes Mellitus...
to the central nervous system.This infection should be sus-
pected when lower extremity ulcer-ations, post-traumatic or post-surgi-cal wounds are not responding totreatment. The clinical picture isusually that of a typical fungal in-fection but may present with blackcrusting or purulence. The diagno-sis, however, can be confirmed byculture and by the histologicdemonstration of fungal elementsinvading vascular channels. Treat-ment consists of correction of acid-base imbalance, aggressive debride-ment of necrotic tissue, and intra-venous amphotericin.
Pseudomonas InfectionThe organism responsible for
this infection is a gram-negativeaerobic bacilli. The two most com-mon pathogens in this species arePseudomonas aeruginosa and Pmaltophilia and account for ap-proximately 80 percent of oppor-tunistic infections in the skin.
Pseudomonas species normallyinhabit soil, water, andvegetation and can beisolated from the skin,throat, and stool ofhealthy persons. Theyoften colonize hospitalfood, sinks, taps, mops,and respiratory equip-ment. Spread is from pa-tient to patient via con-tact with fomites or byingestion of contaminat-ed food and water. Thespread of Pseudomonasis best controlled bycleaning and disinfectingmedical equipment. Re-sistance to infection ofthe host can be increasedby avoiding excess mois-ture and by increasingthe overall health andtherefore the immune re-sponse of the host.
Often persons withonychomycosis of the toe-nails develop an upliftingof the nail plate from thenail bed. This is termedonycholysis. The spacethat results between theuplifted nail plate and thediseased nail plate is a
Contin
uing
Medica
l Edu
catio
n
Tinea pedis may present with
extreme itching andpain, especially while
walking, because of thescaling and blistersbetween the toes.
Figure 13: Callus formation with breakdown of deeper tissues.
Figure 12: Destructive Neuropathic plantar ulceration.
Continued on page 203

NOVEMBER/DECEMBER 2004 • PODIATRY MANAGEMENTwww.podiatrym.com 203
deep in the nail and nail bed.Tinea versicolor may be treated
with selenium sulfide lotion or keto-conazole shampoo. Occasionally, thequestion arises as to whether a con-current bacterial infection is compli-cating a fungal infection. This situa-tion most com-monly occurs inpersons who havean immunopathy,such as diabetics.The lesions usuallyresolve using oralantibiotics, alongwith the antifun-gal treatments in-stituted.
Preventionof Dermato-phytosis
Nurturing the protective barrier ofthe skin by preventing excess mois-ture accumulation while keeping theskin conditioned and free from de-bris, scaling and cracking are firststeps in preventing dermatophyte in-fections of the feet. Excess moisture inthe skin favors the growth of fungi.
fungi. Transmission canoccur directly throughcontact with infected le-sions or indirectlythrough contact with con-taminated articles such asshoes, towels or showerstalls. Another predispos-ing factor is the warmmoist environment of theshoe, exacerbated bysweating and warmweather, which encouragefungus growth. Some ofthe fungi involved inthese conditions primarilyinfect animals, but theymay also be transmittedfrom animals to humans.Cats may have an infec-tion, but may not be sus-pected until lesions appearon their owners.
Diagnosis of Der-matophytosis
Diagnosis must ruleout other possible causesof the signs and symp-toms, which may includeeczema, psoriasis, and con-tact dermatitis. A microscopic exami-nation of some lesion scrapings usual-ly confirms tinea infection. This iscalled a KOH (potassium hydroxide)preparation. Culture of the affectedarea, which may take weeks, mayhelp identify the infecting organism.
Treatment of Dermatophy-tosis
Topical antifungal preparationsshould be effective in treatingsmall, uncomplicated tinea infec-tions of the skin. These include top-ical clotrimazole and miconazole(available over the counter) andterbinafine cream. Sometimes, oralantifungal medication may be re-quired if the condition is severe.Medications may include griseoful-vin, itraconazole, terbinafine andfluconazole. Corticosteroids maysometimes be used for the treat-ment of severely inflamed or wide-spread lesions, such as those thatoccasionally occur on the soles ofthe feet. Fungal infections involv-ing the nails (onychomycosis) mayrequire oral treatment as well, be-cause the dermatophyte is found
Diabetes Mellitus... Cleaningthe skin with anatural oil-basedcleanser is importantas it removes the debristhat may contain con-taminant fungus andthat chokes and blocksthe pores that are re-sponsible for the secre-tions that favor an opti-mal pH of the skin.Avoid soaps with a highpH as they will dry theskin and eliminate itsacid mantle protectivelayer on the surface. Aslightly acidic ph (4-6)helps deter colonizationby non-resident bacteriaand other pathogens be-cause these organismscan survive in a narrowpH range near neutral.
Dry the skin carefullyafter bathing and let itdry before dressing.Wear appropriate foot-wear that allows the skinto breath and preventexcess moisture reten-tion. Socks that wickaway excess moisture
and leather shoes that can breatheare important tools in fungal infec-tion protection.
Tinea PedisTinea pedis should be aggres-
sively managed in the person withdiabetes mellitusand neurovascu-lar compromise.Toe web space in-fection may causefissuring and in-flammation thatmight serve as aportal of entry forsecondary bacte-rial infection inthe immune-c o m p r o m i s e d ,uncontrolled orneurovascularly
compromised diabetic patient. It isimportant to note that the oxygendemand of the subsequent infec-tion and inflammation may exceedthe ability of the diabetic microcir-culation, possibly leading to necro-sis and gangrene.
Continued on page 204
Continuing
Medical Education
Tinea pedis should be aggressivelymanaged in the personwith diabetes mellitus
and neurovascularcompromise.
Figure 14: Increased callus formation with yellowing skin.
Figure 15: Cavity that fills with blood.

and immunologic health of thebody. These may be compromisedor altered by disease, such as dia-betes; trauma, such as ulcerations orinjury; or by procedures and agentsused for diagnosis and/or treatment,such as the indiscriminate use ofantibiotics, immunosuppressivemedications, or cytotoxic drugs.Host defense mechanisms can alsobe altered by age, burns, neoplasms,other metabolic disorders besidesdiabetes, irradiation, foreign bodies,corticosteroids, or diagnostic ortherapeutic instrumentation.
When infections occur in thissetting or if antimicrobial therapyalters the normal relationship be-tween the human host and the mi-crobe, this is often called an oppor-tunistic infection. In these cases, thepatient is predisposed to infectionfrom endogenous microflora that isnot pathogenic or from ordinaryharmless, saprophytic organismsthat are acquired by contact withother patients, hospital personnel,or even equipment such as cathetersand various mechanical devices. Theorganisms involved may be bacteria,fungi, viruses, or other parasites, de-pending on the particular alterationin the host’s defenses, and are oftenpart of the normal flora of the skinsurface and resistant to multiple an-tibiotics. These infections that resultrange from minor to fatal, and oftenpose serious challenges to the pa-tient and the physician.
AntibioticsAntibiotics, especially in the di-
abetic and others with impairedhost defense mechanism, should beused with extreme caution. The rea-son is that they alter the normalmicroflora of the mucous mem-branes, GI tract and the skin andtherefore then encourage coloniza-tion by new organisms. This colo-nization is harmless unless it resultsin invasion by indigenous or envi-ronmental organisms that have be-come resistant to the antibioticbeing used. This is called superin-fection and occurs mostly as a re-sult of treatment with broad-spec-trum antibiotics. Superinfectionsusually appear on the 4th or 5thday of therapy and may be respon-sible for conversion of a benign,self-limited disease into a very seri-ous, prolonged or even fatal infec-
tion. The diagnosis of superinfec-tion is certain only when the speci-men is cultured from the blood,CSF, or fluid from a body cavity ordeep wound.
It is logical that if non-pathogenic, normally benign or-ganisms can cause such serious in-fections, then given the potentiallyimmune compromised situation ofa person with diabetes, pathogenicbacteria can wreak havoc as well. ■
References1. Dockery GL, Crawford ME. Cutaneous
Disorders of the Lower Extremity Text W.B.Saunders Company Pages 178-183
2. Bowker JH, Pfeifer MH Levin andO’Neals THE DIABETIC FOOT sixth editionText Mosby Pages 197-208
3. Chakrabarty A, Norman RA, PhillipsTJ Cutaneous Manifestations of Diabetes.Wounds 14(8): 267-274, 2002.
4. Sibald GR, et al. Skin and diabetes.Endocrinol Metab Clin North Am 1996;25:463-72
5. Miller F III. Management of diabeticfoot ulcers. J Cut Med Surg 1998;3(suppl1):13-7
6. Caputo M, Cavanagh P, Ulbrecht J,et al. Assessment and management of footdisease in patients with diabetes. N Eng JMed 1994; 331:854-60
7. Meurer M, Szeimies RM. Diabetesmellitus and skin diseases. Curr Probl1991;20:11-23
8. Fitzpatrick TB, Johnson RA, Wolff K(eds). Color Atlas and Synopsis of ClinicalDermatology, Fourth Edition. McGraw-Hill,2001:120-22.
9. Drugge R, Dunn HA. The ElectronicTextbood of Dermatology The Internet Der-matology Society Incorporated, 1995-2000
10. West KM: Epidemiology of diabetesand its vascular lesions. New York, 1978, El-sevier North-Holland Inc., p 353.
11. Haroon TS: Diabetes and skin—a re-view. Scott Med J 19:257-267, 1974
12. Bernstein JE: Cutaneous manifesta-tions of diabetes mellitus. Curr ConceptsSkin Disord 1:3, 1980
204 www.podiatrym.comPODIATRY MANAGEMENT • NOVEMBER/DECEMBER 2004
Diabetes Mellitus...
OnychomycosisDermatophyte infection of the
toenails (onychomycosis) shouldnot be taken casually in the diabeticpatient. Onychomycotic toenailsbecome hard, brittle, deformed andthickened and can precipitate sub-ungual and periungual debris, aswell as incurvated, ingrown toe-nails. This, in turn can cause irrita-tion, trauma, and infection of thetissues surrounding the toenail. At-tentive hygienic and conditioningcare and debridement of the toe-nails and surrounding skin is essen-tial for preventing infection in thisarea. Recently, the FDA approvedboth itraconazole treatment (200mg/day for one week a month for 4months) and terbinafine (250mg/day for 3 months) for the treat-ment of onychomycosis. Thesetreatments pose no additional riskto the diabetic patient.
Bacterial, Opportunistic andSuperinfection in theCompromised Host
Infections are risky in diabeticsas they can cause necrosis of the tis-sues, edema, and ablation of localcirculation, causing gangrene. Hy-perglycemia and immunopathy pre-dispose diabetics to infection. Thesigns of localized infection or celluli-tis are redness (erythema), edema(swelling), calor (increase in temper-ature), pus (purulent drainage) andpain. Even in the patient with lossof sensation, pain can be perceived.The spread of infection is caused bythe pressure of the purulence, some-times causing as much as 25 poundsper square inch of pressure. Thespreading erythema is a sign ofspreading infection.
Non-pathogenic organisms canbecome colonized and progress tobecoming infectious. This canoccur in patients whose host de-fense mechanisms are compro-mised. In the hospital setting, theyfrequently occur as a result of colo-nization of antibiotic-resistant or-ganisms. The use of catheters andmechanical devices are often theculprit in these types of infections.
Host Defense MechanismsHost defense mechanisms de-
pend on the physiologic, anatomic
Contin
uing
Medica
l Edu
catio
n
Dr. Rehm, board-certified in dia-betic woundcare, practices inSan Diego, CA.He lectures na-tionally and of-fers seminars forpodiatrists andother profes-sionals. Dr.Rehm is Director of the Diabetic Foot andWound Treatment Centers in San Diego,and a Fellow, American ProfessionalWound Care Association.

NOVEMBER/DECEMBER 2004 • PODIATRY MANAGEMENTwww.podiatrym.com 205
all of the following except:A) Development of a functionalsympathectomy in the cervicalplexusB) Engorgement of the post-capillary venulesC) Increased viscosity of thebloodD) Stiff red blood cellmembranes
6) The predominant biochemicalcause of diabetic-related changesin the skin involves:
A) Non-enzymatic lipoxidationB) Non-enzymaticglycosylationC) Enzymatic glucoxylationD) Covalent enzymatization
7) Color changes of collagen indiabetes-related complicationsinvolve all of the following except:
A) NH2 group of the proteinB) Schiff baseC) Amador productsD) Unstable pyruvate ring
8) Advanced glycosylation end-products that have been identifiedin the skin include:
A) The amino acid pentosidineB) “Café au lait” imidazolecompoundsC) Glucose-loaded ketoaminicbaseD) Beta-amino group l-terminalamino acids
9) Which of the following is nottrue regarding non-enzymaticglycosylation:
A) Causes increased stiffness ofthe red blood cellB) Causes decreased resistanceto normal enzymaticdegradationC) Causes increased stiffness incollagenD) Predisposes the diabetic toincreased callus formation
1) Which of the followingstatements are true?
A) Dermatologic complicationsin diabetes are rare, but seriousB) 30 % of all skin problems indiabetics put a patient at riskfor serious ulcerationC) Diabetic skin problems areusually life-threateningD) Dermatologicmanifestations in diabetesmellitus are universal, theprevalence approaching 100%
2) The dermatologic manifestationof diabetes mellitus is universallyinfluenced by which of thefollowing?
A) The attachment of glucoseto proteinB) The attachment of proteinto insulinC) The attachment of proteinto glucagonD) The attachment of collagento insulin by-products
3) The skin is commonly thicker indiabetics because of:
A) The increased lactic acidmetabolism end-productsB) The decrease inglycosylation end-productsC) The increased cross-linkingof collagenD) Engorgement of the post-capillary venules
4) Complex glycosylation endproducts have their greatest effecton which of the following?
A) Erythema of the faceB) Lower extremity post-traumatic fatty depositsC) Yellowing of the skin andnailsD) Ketosis and glycemiccontrol
5) Erythema of the periungualtissues is thought to be a result of
10) The most destructive lesion inskin of the diabetic is
A) A mosaic virus-relatedverrucaB) Porokeratosis plantarisdiscretaC) Neuropathic plantarulcerationD) Heloma molle
11) Which is not part of the normaldevelopment of a neuropathic plan-tar ulceration in the diabetic foot?
A) A deep puncture woundB) The initial hyperkeratoticlesionC) Weakening and breakdownof deeper cutaneous tissuesD) Eventual cavity formationthat fills with blood
12) The following are not diseasesassociated with diabetes mellitus:
A) HemochromatosisB) Porphyria cutanea tardaC) Wilson’s diseaseD) Acanthosis nigricans
13) High plasma levels of insulin,stimulated by the non-responsivereceptor sites, are linked to whichof the following:
A) MyxedemaB) Primary lipidemiasC) Cutaneous infectionsD) Leprechaunism
14) All of the following areassociated with insulin resistanceexcept:
A) DHEAB) GlucocorticoidsC) DiethystilbestrolD) Nicotinic acid
15) The microbial ecology of thehuman skin involves the following:
A) Cutaneous levels of PABA in the granular layer of theepidermis
Continuing
Medical Education
E X A M I N A T I O N
See answer sheet on page 207.
Continued on page 206
206
B) Carotinization of the dermal epidermaljunctionC) The relationship between colonization,infection and host defensesD) Rapid epidermolysis of the basementmembrane
16) Susceptibility for cutaneous infection involves allof the following except:
A) The ratio of melanocytes to total skin areaB) the dryness and stiffness of the skinC) The underlying metabolic disordersD) The effect of autonomic neuropathy
17) Which statement is true?A) On the moist portion of the lower leg andankle, the flora is quite restrictedB) Criteria for restricted flora requires 40,000bacteria per square centimeterC) Fatty acids in the skin have directantimicrobial effectsD) When the feet are too moist they favordecreased microbial density
18) Higher microbial density of the intertriginousareas results in:
A) Decreased ammonia formationB) Increased acid productionC) Higher surface pHD) Prevention of the metabolism of urea
19) Which of the following is not true regardingCandida infection?
A) the incidence in the hands and feet appearsto be relatively the same in the diabetic and thenon-diabetic populationB) Candida can cause paronychia of thefingernailsC) Pilonidal cysts are often related to candidainfection in the diabetic populationD) Candida often begins at the unguilabia aserythema, edema and separation of nail margins
20) All of the following are common causes ofinfections in the diabetic except:
A) H. pylorisB) MucormycosisC) PseudomonasD) Dermatophytosis
E X A M I N A T I O N
(cont’d)
See answer sheet on page 207.
Contin
uing
Medica
l Edu
catio
n
PM’sCPME Program
Welcome to the innovative Continuing EducationProgram brought to you by Podiatry ManagementMagazine. Our journal has been approved as asponsor of Continuing Medical Education by theCouncil on Podiatric Medical Education.
Now it’s even easier and more convenientto enroll in PM’s CE program!
You can now enroll at any time during the yearand submit eligible exams at any time during yourenrollment period.
PM enrollees are entitled to submit ten examspublished during their consecutive, twelve–monthenrollment period. Your enrollment period beginswith the month payment is received. For example,if your payment is received on September 1, 2003,your enrollment is valid through August 31, 2004.
If you’re not enrolled, you may also submit anyexam(s) published in PM magazine within the pasttwelve months. CME articles and examinationquestions from past issues of Podiatry Man-agement can be found on the Internet athttp://www.podiatrym.com/cme. All lessonsare approved for 1.5 hours of CE credit. Please readthe testing, grading and payment instructions to de-cide which method of participation is best for you.
Please call (631) 563-1604 if you have any ques-tions. A personal operator will be happy to assist you.
Each of the 10 lessons will count as 1.5 credits;thus a maximum of 15 CME credits may beearned during any 12-month period. You may se-lect any 10 in a 24-month period.
The Podiatry Management Magazine CMEprogram is approved by the Council on PodiatricEducation in all states where credits in instruction-al media are accepted. This article is approved for1.5 Continuing Education Contact Hours (or 0.15CEU’s) for each examination successfully completed.
PM’s CME program is valid in all statesexcept Kentucky.
www.podiatrym.com
Home Study CME credits nowaccepted in Pennsylvania
PODIATRY MANAGEMENT

Over, please
Please print clearly...Certificate will be issued from information below.
Name _______________________________________________________________________Soc. Sec. #______________________________Please Print: FIRST MI LAST
Address_____________________________________________________________________________________________________________
City__________________________________________________State_______________________Zip________________________________
Charge to: _____Visa _____ MasterCard _____ American Express
Card #________________________________________________Exp. Date____________________
Note: Credit card payment may be used for fax or phone-in grading only.
Signature__________________________________Soc. Sec.#______________________Daytime Phone_____________________________
State License(s)___________________________Is this a new address? Yes________ No________
Check one: ______ I am currently enrolled. (If faxing or phoning in your answer form please note that $2.50 will be charged to your credit card.)
______ I am not enrolled. Enclosed is a $17.50 check payable to Podiatry Management Magazine for each exam submitted. (plus $2.50 for each exam if submitting by fax or phone).
______ I am not enrolled and I wish to enroll for 10 courses at $109.00 (thus saving me $66 over the cost of 10 individual exam fees). I understand there will be an additional fee of $2.50 for any exam I wish to submit via fax or phone.
Note: If you are mailing your answer sheet, you must completeall info. on the front and back of this page and mail with yourcheck to: Podiatry Management, P.O. Box 490, East Islip,NY 11730. Credit cards may be used only if you are faxing orphoning in your test answers.
TESTING, GRADING AND PAYMENT INSTRUCTIONS(1) Each participant achieving a passing grade of 70% or
higher on any examination will receive an official computer formstating the number of CE credits earned. This form should be safe-guarded and may be used as documentation of credits earned.
(2) Participants receiving a failing grade on any exam will benotified and permitted to take one re-examination at no extra cost.
(3) All answers should be recorded on the answer formbelow. For each question, decide which choice is the best an-swer, and circle the letter representing your choice.
(4) Complete all other information on the front and back ofthis page.
(5) Choose one out of the 3 options for testgrading: mail-in,fax, or phone. To select the type of service that best suits yourneeds, please read the following section, “Test Grading Options”.
TEST GRADING OPTIONSMail-In GradingTo receive your CME certificate, complete all information
and mail with your check to:Podiatry Management
P.O. Box 490, East Islip, NY 11730There is no charge for the mail-in service if you have already
enrolled in the annual exam CPME program, and we receive this
E N R O L L M E N T F O R M & A N S W E R S H E E T
✄
207
Continuing
Medical Education
exam during your current enrollment period. If you are not en-rolled, please send $17.50 per exam, or $109 to cover all 10exams (thus saving $66 over the cost of 10 individual exam fees).
Facsimile GradingTo receive your CPME certificate, complete all information and
fax 24 hours a day to 1-631-563-1907. Your CPME certificate willbe dated and mailed within 48 hours. This service is available for$2.50 per exam if you are currently enrolled in the annual 10-examCPME program (and this exam falls within your enrollment period),and can be charged to your Visa, MasterCard, or American Express.
If you are not enrolled in the annual 10-exam CPME pro-gram, the fee is $20 per exam.
Phone-In GradingYou may also complete your exam by using the toll-free ser-
vice. Call 1-800-232-4422 from 10 a.m. to 5 p.m. EST, Mondaythrough Friday. Your CPME certificate will be dated the same dayyou call and mailed within 48 hours. There is a $2.50 charge forthis service if you are currently enrolled in the annual 10-examCPME program (and this exam falls within your enrollment peri-od), and this fee can be charged to your Visa, Mastercard, Ameri-can Express, or Discover. If you are not currently enrolled, the feeis $20 per exam. When you call, please have ready:
1. Program number (Month and Year)2. The answers to the test3. Your social security number4. Credit card information
In the event you require additional CPME information,please contact PMS, Inc., at 1-631-563-1604.
Enrollment/Testing Informationand Answer Sheet
✄
208 www.podiatrym.comPODIATRY MANAGEMENT • NOVEMBER/DECEMBER 2004
LESSON EVALUATION
Please indicate the date you completed this exam
_____________________________
How much time did it take you to complete the lesson?
______ hours ______minutes
How well did this lesson achieve its educational objectives?
_______Very well _________Well
________Somewhat __________Not at all
What overall grade would you assign this lesson?
A B C D
Degree____________________________
Additional comments and suggestions for future exams:
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
EXAM #12/04Skin Disease in
Diabetes Mellitus—Part 1(Rehm)
1. A B C D
2. A B C D
3. A B C D
4. A B C D
5. A B C D
6. A B C D
7. A B C D
8. A B C D
9. A B C D
10. A B C D
11. A B C D
12. A B C D
13. A B C D
14. A B C D
15. A B C D
16. A B C D
17. A B C D
18. A B C D
19. A B C D
20. A B C D
Circle:
LESSON EVALUATION
Please indicate the date you completed this exam
_____________________________
How much time did it take you to complete the lesson?
______ hours ______minutes
How well did this lesson achieve its educational objectives?
_______Very well _________Well
________Somewhat __________Not at all
What overall grade would you assign this lesson?
A B C D
Degree____________________________
Additional comments and suggestions for future exams:
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
EXAM #11/04Optimizing Wound Prevention
and Healing (Donohue, Goss, LaVan,Weingarten, and Abboud)
1. A B C D
2. A B C D
3. A B C D
4. A B C D
5. A B C D
6. A B C D
7. A B C D
8. A B C D
9. A B C D
10. A B C D
11. A B C D
12. A B C D
13. A B C D
14. A B C D
15. A B C D
16. A B C D
17. A B C D
18. A B C D
19. A B C D
20. A B C D
Circle:
E N R O L L M E N T F O R M & A N S W E R S H E E T (cont’d)Con
tinuin
g
Medica
l Edu
catio
n