the cardiovascular system an in-depth look mark h. hyman, md, facp, faadep
TRANSCRIPT
THE CARDIOVASCULAR SYSTEMTHE CARDIOVASCULAR SYSTEMAn In-depth LookAn In-depth Look
MARK H. HYMAN, MD, FACP, FAADEPMARK H. HYMAN, MD, FACP, FAADEP


THE CARDIOVASCULAR SYSTEMTHE CARDIOVASCULAR SYSTEMChapter 3-Heart and AortaChapter 3-Heart and Aorta
Chapter 4-Systemic and Pulmonary Chapter 4-Systemic and Pulmonary ArteriesArteries

THE CARDIOVASCULAR SYSTEMTHE CARDIOVASCULAR SYSTEMChapter 3-Heart and AortaChapter 3-Heart and Aorta

NYHA Functional ClassificationsNYHA Functional Classifications (Table 3-1, pg 26) (Table 3-1, pg 26)
1 - Ordinary Activity - No Symptoms1 - Ordinary Activity - No Symptoms
2 - Greater than Ordinary Activity 2 - Greater than Ordinary Activity Symptoms - Fatigue, Angina Symptoms - Fatigue, Angina
3 - Comfortable At Rest 3 - Comfortable At Rest Symptoms - Ordinary Activity Symptoms - Ordinary Activity
4 - Symptoms At Rest and Worse with4 - Symptoms At Rest and Worse with Ordinary Activity Ordinary Activity
OBJECTIVEOBJECTIVE
MEASUREMENTSMEASUREMENTS

Evaluation of CADEvaluation of CAD
Exercise - treadmill or bicycleExercise - treadmill or bicycle
Thallium Exercise StudyThallium Exercise Study
Exercise Wall Motion - Multi-gatedExercise Wall Motion - Multi-gated
Exercise EchocardiographyExercise Echocardiography
Magnetic Resonance StudyMagnetic Resonance Study
Positron EmissionPositron Emission
Coronary AngiographyCoronary Angiography

Sensitivity and Specificity of Exercise TestsSensitivity and Specificity of Exercise Tests
TestTest Sensitivity Specificity Sensitivity Specificity
Stress ECGStress ECG 68%68% 77% 77%
Spect Thallium-201Spect Thallium-201 9090 89 89
Tc-99 SestamibiTc-99 Sestamibi 8989 90 90
Dipyridamole ThalliumDipyridamole Thallium 8585 87 87
Stress EchoStress Echo 8080 90 90

Stress TestingStress Testing
Peak Level - METsPeak Level - METs
Symptoms and SignsSymptoms and Signs
ArrhythmiasArrhythmias
ST ChangesST Changes
Blood PressureBlood Pressure
MET - Metabolic UnitMET - Metabolic Unit
1 MET = Energy Expenditure of Sitting 1 MET = Energy Expenditure of Sitting at Restat Rest
3.5 cc/Kg/Min3.5 cc/Kg/Min Use Table 3-2 or 3-3 to convert exercise Use Table 3-2 or 3-3 to convert exercise
performance into METs. performance into METs.

Tables 3-2 and 3-3Tables 3-2 and 3-3

3.2-Valve Stenosis - Aortic Impairment3.2-Valve Stenosis - Aortic Impairment Valve Gradient Valve AreaValve Gradient Valve Area
mm Hgmm Hg CM CM22
Aortic ValveAortic Valve
MildMild < 25 < 25 > 1.5> 1.5
ModerateModerate 25 - 50 25 - 50 1.0 – 1.5 1.0 – 1.5
SevereSevere > 50 > 50 < 1.0< 1.0

3.2-Valve Stenosis - Mitral Impairment3.2-Valve Stenosis - Mitral Impairment Valve Gradient Valve AreaValve Gradient Valve Area
mm Hgmm Hg CM CM22
Mitral ValveMitral Valve
MildMild < 5 < 5 > 1.5> 1.5
ModerateModerate 5 - 105 - 10 1.0 – 1.5 1.0 – 1.5
SevereSevere > 10 > 10 < 1.0< 1.0


3.3 CORONARY HEART 3.3 CORONARY HEART
DISEASEDISEASE

Occupational CategoriesOccupational Categories
CarpentryCarpentry 3.5 METs 3.5 METs
MaidMaid 2.5 2.5
PlumbingPlumbing 3.5 3.5
FarmingFarming 8.0 8.0
ForestryForestry 17.017.0
Machine ToolMachine Tool 8.0 8.0
Shoe RepairShoe Repair 2.5 2.5
TypingTyping 1.5 1.5
Problem With CategoriesProblem With Categories
Average energyAverage energy
Peak much higherPeak much higher
Travel exertionTravel exertion
No study on CADNo study on CAD
Time of workTime of work

Haskell Work ClassificationHaskell Work Classification
METsMETs ActivityActivity
Very HeavyVery Heavy > 6 > 6 Climb stairsClimb stairs
MediumMedium 4 - 64 - 6 50 lbs50 lbs
LightLight 2 - 42 - 4 20 lbs20 lbs
SedentarySedentary < 2 < 2 SitSit
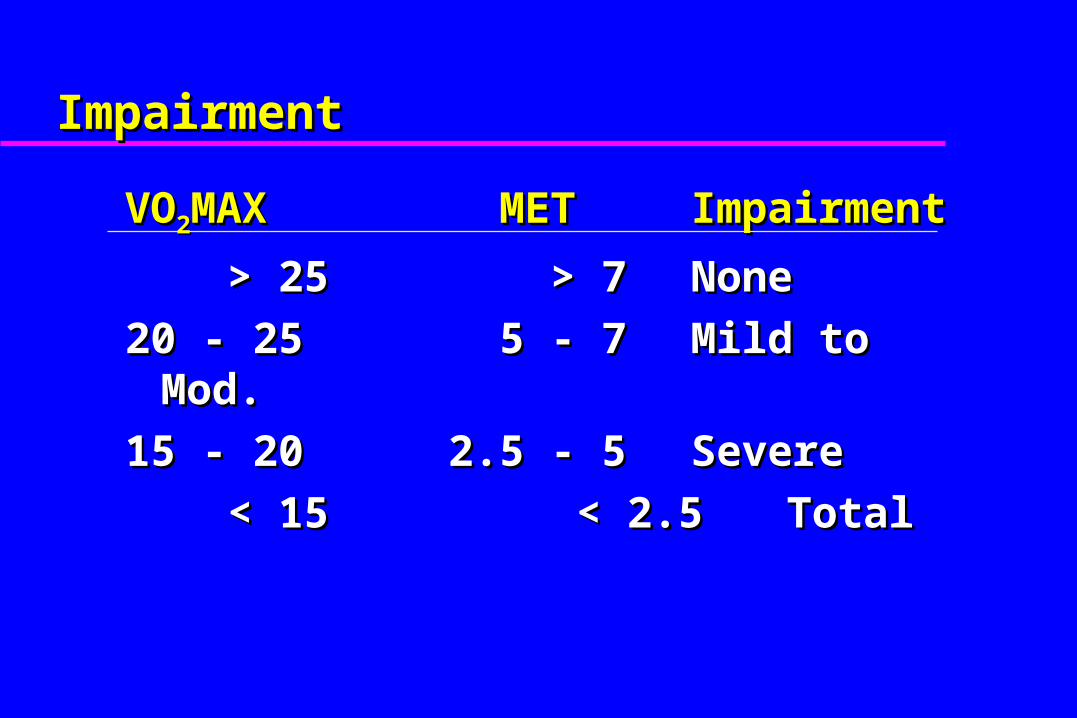
ImpairmentImpairment
VOVO22MAXMAX METMET Impairment Impairment
> 25> 25 > 7 > 7 None None
20 - 2520 - 25 5 - 7 5 - 7 Mild to Mod. Mild to Mod.
15 - 2015 - 20 2.5 - 52.5 - 5 Severe Severe
< 15< 15 < 2.5 < 2.5 Total Total

Cardiac GuidelinesCardiac Guidelines
Peak METsPeak METs Work PreclusionWork Preclusion
> 9> 9 None to No Very Heavy LiftingNone to No Very Heavy Lifting
7 - 97 - 9 No Heavy WorkNo Heavy Work
5 - 75 - 7 To Light WorkTo Light Work
2.5 - 52.5 - 5 To Sedentary WorkTo Sedentary Work
< 2.5< 2.5 TotalTotal
1998 - California1998 - California

Sustained Work - Sustained Work - Percent of Maximal Level Achieved Percent of Maximal Level Achieved
Ilmarinin, 1984Ilmarinin, 1984 30 - 50%30 - 50%
Astrand, 1988Astrand, 1988 40 - 45%40 - 45%
NIOSH GuideNIOSH Guide 33%33%
NIOSH Safety ManualNIOSH Safety Manual 40 - 50%40 - 50%

Sustained Work Sustained Work
During 8 Hour Day During 8 Hour Day
With Breaks With Breaks
Is 40% of Maximum MET LevelIs 40% of Maximum MET Level

Maximum Short Term WorkMaximum Short Term Work
Less than 15 minutesLess than 15 minutes
Once to twice a dayOnce to twice a day
80% of maximal MET level achieved80% of maximal MET level achievedOROR
1-3 minutes maximum MET level 1-3 minutes maximum MET level achievedachieved

DEMANDLEVEL
ENERGYREQUIRED
(METS)
WORK LIFTING DEMAND(LBS)
SAMPLEOCCUPATIONS
HOMEACTIVITY
RECREATIONALACTIVITY
PHYSICALCONDITIONING
OCCASIONAL0-33% OF
WORKDAY
FREQUENT34-66% OFWORKDAY
CONSTANT67-100% OF WORKDAY
SEDENTARY 1.5-2.1 10 NONE NONE CLERICALSTORE CLERKBARTENDERTRUCK DRIVERCRANE OPERATOR
WASHING SHAVING DRESSING WRITING WASH DISHESDRIVE CAR
SHUFFLEBOARDHORSESHOEBILLIARDSARCHERYGOLF WITH CART
WALK 2 MPHSTATIONARY BICYCLEVERY LIGHT CALISTHENICS
LIGHT 2.2-3.5 20 10 NONE AND/OROPERATING CONTROLS
WHILE SEATED
LIGHT WELDING,CARPENTRY OR SHELVINGAUTO REPAIRMACHINE ASSEMBLY
RAKING LEAVESWEEDINGPAINTINGCLEAN WINDOWSWAX FLOOR
DANCINGGOLF WALKINGSAILINGHORSEBACKDOUBLES TENNIS
WALK 3-4 MPHCYCLE 6-8MPHLIGHT CALISTHENICS
MEDIUM ORMODERATE
3.6-6.3 20-50 10-25 10 CARPENTRYSHOVELINGPNEUMATIC TOOLS
GARDENINGLAWN MOWINGSLOW CLIMB OF STAIRS
BADMITONSINGLES TENNISSKI DOWNHILLBASKETBALLFOOTBALLICE SKATINGLIGHT BACKPACK
WALK 4-5MPHCYCLE 9-10MPHSWIM BREAST STROKE
HEAVY 6.4-7.5 50-100 25-50 10-20 DITCH DIGGINGPICK & SHOVEL
SAW WOODHEAVY SHOVELING
CANOEINGMOUNTAIN CLIMBINGFENCINGPADDLEBALL
JOG 5 MPHCYCLE 12MPHSWIM CRAWLROWING
VERY HEAVY >7.5 >100 >50 >20 LUMBER JACKHEAVY LABOR
HEAVY SNOW SHOVELINGFAST STAIRS
HANDBALL SQUASHXC SKIING
RUN >6 MPHCYCLE >13 MPHJUMP ROPE

AMA Impairment Classification for CHDAMA Impairment Classification for CHD
ClassClass Impairment Impairment
Class IClass I 0 - 9% 0 - 9%
Class IIClass II 10 - 29%10 - 29%
Class IIIClass III 30 - 49%30 - 49%
Class IVClass IV 50 - 100%50 - 100%

CAD - Class 1: 0-9%CAD - Class 1: 0-9%
Equivocal HistoryEquivocal History
< 50% Blockage< 50% Blockage
EB Scan PositiveEB Scan Positive
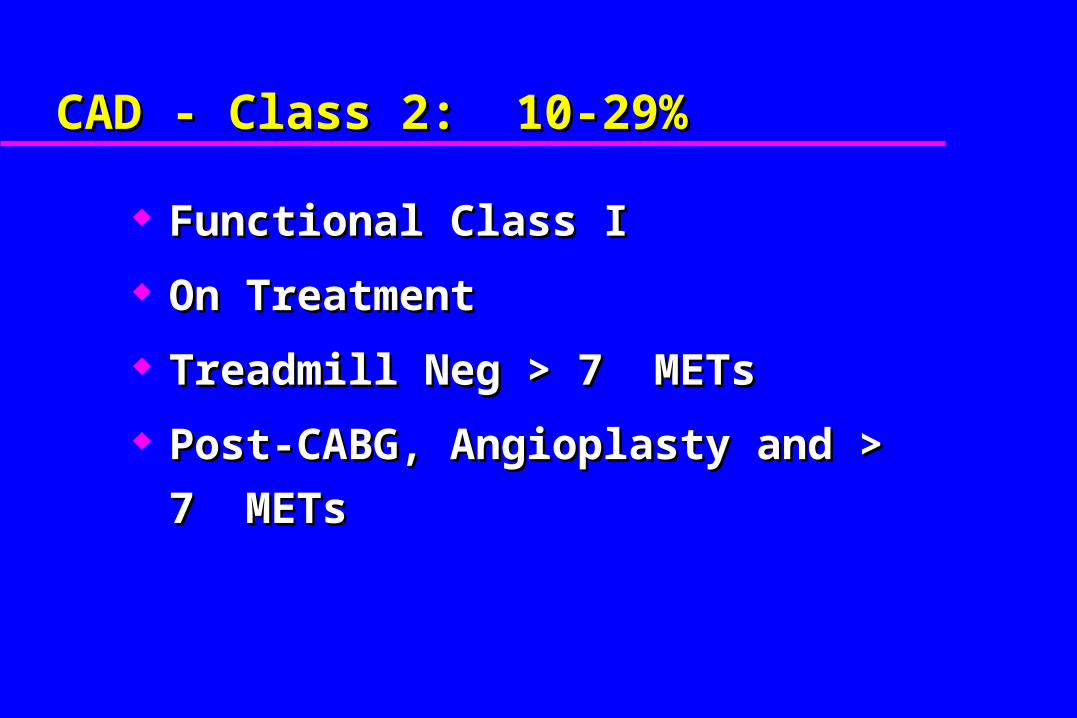
CAD - Class 2: 10-29%CAD - Class 2: 10-29%
Functional Class IFunctional Class I
On TreatmentOn Treatment
Treadmill Neg > 7 METsTreadmill Neg > 7 METs
Post-CABG, Angioplasty and > 7 METsPost-CABG, Angioplasty and > 7 METs

CAD - Class 3: 30-49%CAD - Class 3: 30-49%
Symptoms of CADSymptoms of CAD
> 50% Blockage> 50% Blockage
5 - 7 METs5 - 7 METs
CAD - Class 4: 50-100%CAD - Class 4: 50-100%
Functional Class 3 - 4Functional Class 3 - 4
< 5 METs< 5 METs

Table 3-6aTable 3-6a

3.4 Congenital Heart Disease3.4 Congenital Heart Disease Uses NYHA Functional Class Table 3-1Uses NYHA Functional Class Table 3-1 Classification by degree of valve Classification by degree of valve
abnormality, heart failure, severity of abnormality, heart failure, severity of pulmonary –systemic flow abnormality, pulmonary –systemic flow abnormality, degree of shuntingdegree of shunting

Congenital Heart Disease Common ExamplesCongenital Heart Disease Common Examples
ASD/VSDASD/VSD Ebsteins AnomalyEbsteins Anomaly Tetrology of FallotTetrology of Fallot Transposition of Great VesselsTransposition of Great Vessels Eisenmengers ComplexEisenmengers Complex

Congenital Heart Disease RatingCongenital Heart Disease Rating

3.5 Cardiomyopathy3.5 Cardiomyopathy Table 3-9 Uses NYHA Functional Class Table 3-9 Uses NYHA Functional Class
and Treatment. Mets Not Usedand Treatment. Mets Not Used
However, it would be better if you use However, it would be better if you use more objective criteria of EF and METS. more objective criteria of EF and METS. See e.g. past California guidelines or SSA See e.g. past California guidelines or SSA Guides.Guides.

Weber Classification of Functional Weber Classification of Functional Impairment in CHF Impairment in CHF
ClassClass SeveritySeverity Peak VO2Peak VO2
AA None to MildNone to Mild >20>20
BB Mild to ModMild to Mod 16-2016-20
CC Mod to SevereMod to Severe 10-1610-16
DD SevereSevere 6-106-10
EE Very SevereVery Severe <2<2

3.6 Pericardial Heart Disease3.6 Pericardial Heart Disease Make sure at MMI as these can relapse Make sure at MMI as these can relapse
and recurand recur If recurrent, demonstrate abnormality If recurrent, demonstrate abnormality
(echo, CT) (echo, CT) Table 3-10 Uses NYHA Functional Class Table 3-10 Uses NYHA Functional Class
and Treatment. Mets Not Usedand Treatment. Mets Not Used However, again, it would be better if you However, again, it would be better if you
use more objective criteria of EF and use more objective criteria of EF and METS.METS.

3.7 Arrhythmia3.7 Arrhythmia Impairment from arrhythmia must be Impairment from arrhythmia must be
combinedcombined with impairment of underlying with impairment of underlying heart disease if presentheart disease if present

Arrhythmia Impairment AMA GuidesArrhythmia Impairment AMA Guides
II - Asymptomatic, Documented Arrhythmia- Asymptomatic, Documented ArrhythmiaNot Malignant, No Organic Heart DiseaseNot Malignant, No Organic Heart Disease
IIII - Asymptomatic, Documented Arrhythmia, Need - Asymptomatic, Documented Arrhythmia, Need Dietary Adjustment, Medication, Organic Dietary Adjustment, Medication, Organic Heart Disease is PresentHeart Disease is Present
IIIIII - Symptoms With Treatment, Infrequent, Active Life- Symptoms With Treatment, Infrequent, Active Life
IVIV - Constant Symptoms; NYHA Class 3-4 - Constant Symptoms; NYHA Class 3-4

REST STOPREST STOP

THE CARDIOVASCULAR SYSTEMTHE CARDIOVASCULAR SYSTEMChapter 4 – Systemic and Pulmonary Chapter 4 – Systemic and Pulmonary
ArteriesArteries

4.1 Hypertensive Cardiovascular Disease4.1 Hypertensive Cardiovascular Disease
This is primarily a numbers gameThis is primarily a numbers game

Classification of HypertensionClassification of HypertensionArch Int Med, 1997 (JNC 6)Arch Int Med, 1997 (JNC 6)
BPBP OptOpt NormNorm Hi-Hi-NormNorm
HBPHBP
II
HBPHBP
IIII
HBPHBP
IIIIII
SystSyst <120<120 <130<130 <139<139 <159<159 <179<179 >180>180
AndAnd AndAnd OrOr OrOr OrOr OrOr
DiastDiast <80<80 <85<85 <89<89 <99<99 <109<109 >110>110

Hypertension - Class 1: 0-9%Hypertension - Class 1: 0-9%
Asymptomatic Stage 1 or 2 Without Asymptomatic Stage 1 or 2 Without MedicationMedicationoror
Normal BP with Medication andNormal BP with Medication and
No End-Organ DamageNo End-Organ Damage

Hypertension - Class 2: 10-29%Hypertension - Class 2: 10-29%
Abnormal UrineAbnormal Urine
But No Renal ImpairmentBut No Renal Impairment
Retinal ChangeRetinal Change
No Symptoms; Stage1 or 2 with medsNo Symptoms; Stage1 or 2 with meds
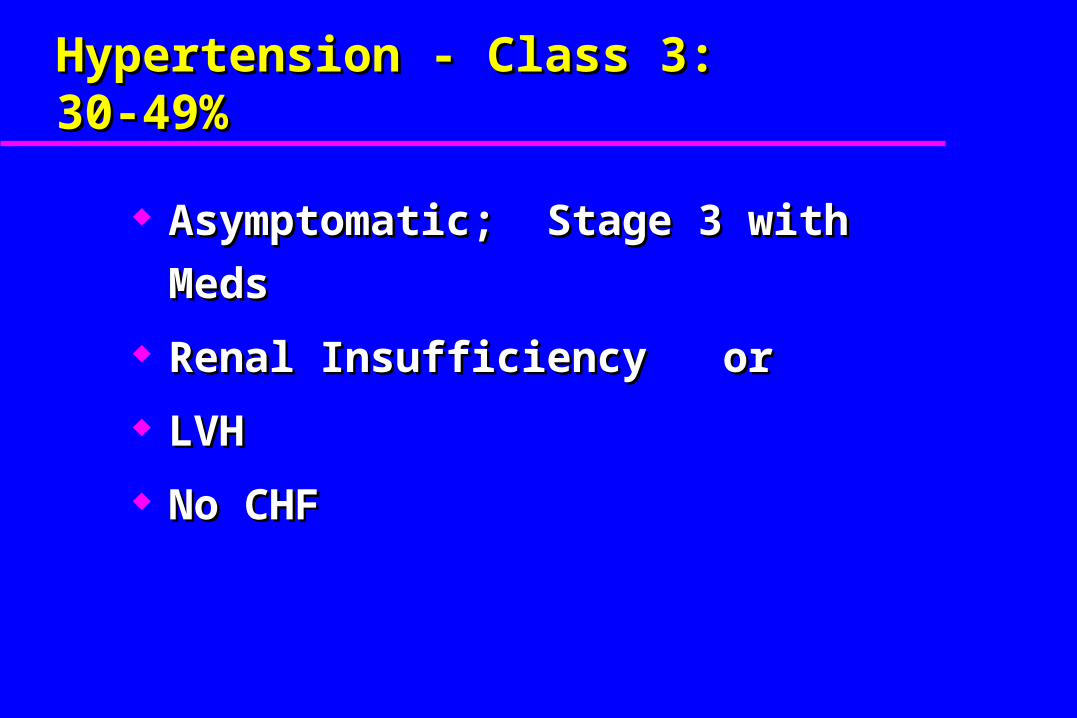
Hypertension - Class 3: 30-49%Hypertension - Class 3: 30-49%
Asymptomatic; Stage 3 with MedsAsymptomatic; Stage 3 with Meds
Renal Insufficiency orRenal Insufficiency or
LVH LVH
No CHFNo CHF

Hypertension – Class 4 50-100%Hypertension – Class 4 50-100%
Stage 1-3 with Medication andStage 1-3 with Medication and Renal Disease orRenal Disease or Hypertensive Cerebrovascular Damage Hypertensive Cerebrovascular Damage
oror LVH, CHFLVH, CHF

Pulmonary HypertensionPulmonary Hypertension
Findings of Right Heart FailureFindings of Right Heart Failure Pulmonary Artery PressurePulmonary Artery Pressure
– Class 1 40-50 mm HgClass 1 40-50 mm Hg– Class 2 51-75 mmHg Class 2 51-75 mmHg – Class 3 >75Class 3 >75 mm Hgmm Hg– Class 4 >76 mm Hg or functional class 3-4Class 4 >76 mm Hg or functional class 3-4

4.2 Diseases of the Aorta4.2 Diseases of the Aorta Functional Classification for Aortic Functional Classification for Aortic
Symptoms such as dyspnea, wheezing, Symptoms such as dyspnea, wheezing, coughcough
At risk or had surgeryAt risk or had surgery

4.4 Peripheral Vascular Disease-4.4 Peripheral Vascular Disease-Upper ExtremityUpper Extremity
ClaudicationClaudication Physical findings especially of edema or Physical findings especially of edema or
ulcerationsulcerations Finger-brachial indicesFinger-brachial indices AmputationAmputation

4.4 Peripheral Vascular Disease-4.4 Peripheral Vascular Disease-Lower ExtremityLower Extremity
Claudication (distance)Claudication (distance) Do Claudication Treadmill StudyDo Claudication Treadmill Study
Physical findings especially of edema or Physical findings especially of edema or ulcerations ulcerations
Ankle-brachial indices are not mentioned Ankle-brachial indices are not mentioned but should be donebut should be done
AmputationAmputation
Additional Points CardiovascularAdditional Points Cardiovascular
3 areas of importance 3 areas of importance for Heart Diseasefor Heart Disease1.1. Risk FactorsRisk Factors
2.2. StressStress
3.3. ApportionmentApportionment

Additional Points CardiovascularAdditional Points Cardiovascular
Risk Factors for Heart Disease:Risk Factors for Heart Disease:– CigarettesCigarettes– DyslipidemiaDyslipidemia– DiabetesDiabetes– HypertensionHypertension– ObesityObesity– Family HistoryFamily History– ExerciseExercise

Additional Points CardiovascularAdditional Points Cardiovascular Risk Factors for Heart Disease:Risk Factors for Heart Disease:
– C-Reactive ProteinC-Reactive Protein– Lipoprotein (a)Lipoprotein (a)– Apolipoprotein EApolipoprotein E– HomocysteineHomocysteine– sICAM-1(Soluble Intracellular Adhesion Molecule 1, also sICAM-1(Soluble Intracellular Adhesion Molecule 1, also
called sCD40 Ligand)called sCD40 Ligand)– OCP/HRT in womenOCP/HRT in women– StressStress– Caffeine-in CYP1A2 1F slow metabolizerCaffeine-in CYP1A2 1F slow metabolizer
– PMPM2.5 2.5 fine particulate air pollutionfine particulate air pollution

Additional Points CardiovascularAdditional Points Cardiovascular
Risk Factors for Heart Disease:Risk Factors for Heart Disease:– HypergammaglobulinemiaHypergammaglobulinemia– Hypercoagulable state-Factor V Leiden, Hypercoagulable state-Factor V Leiden,
Antiphospholipid Antibody, Protein C/S Antiphospholipid Antibody, Protein C/S deficiency, Antithrombin IIIdeficiency, Antithrombin III
– MyeloperoxidaseMyeloperoxidase– Gene polymorphisms- ESR alpha, Gene polymorphisms- ESR alpha,
VEGF(Vascular Endothelial Growth VEGF(Vascular Endothelial Growth Factors, e.g. Placental Growth Factor)Factors, e.g. Placental Growth Factor)
– Adiponectin LevelAdiponectin Level

Archives Int Med, Vol. 165, No. 2 1/24/05, p.141

Additional Points CardiovascularAdditional Points CardiovascularUSPSTF issued reports that the some of the more common nontraditional USPSTF issued reports that the some of the more common nontraditional
risk factors do increase risk, but there is insufficient evidence about risk factors do increase risk, but there is insufficient evidence about usage and treatment for:usage and treatment for:
CRPCRP ABIABI Leukocyte CountLeukocyte Count Fasting BGFasting BG Periodontal DiseasePeriodontal Disease Carotid IMTCarotid IMT CAC ScoreCAC Score HomocysteineHomocysteine Lipoprotein (a)Lipoprotein (a)
Annals Internal Medicine, 3 reports, 10/6/09;151 Annals Internal Medicine, 3 reports, 10/6/09;151

Additional Points CardiovascularAdditional Points Cardiovascular
Risk Factors for Heart DiseaseRisk Factors for Heart Disease– The Zutphen Elderly Study in Arch The Zutphen Elderly Study in Arch
Int Med, 2 reports, 2/27/06Int Med, 2 reports, 2/27/06
– Cocoa (Chocolate) lowers risk, Cocoa (Chocolate) lowers risk, probably due to flavan-3-ols, part of probably due to flavan-3-ols, part of the flavanoids familythe flavanoids family
– Dispositional optimism ( a Dispositional optimism ( a generalized positive future’s outcome generalized positive future’s outcome expectation) lowers riskexpectation) lowers risk

Additional Points CardiovascularAdditional Points Cardiovascular
Risk Factors for Heart DiseaseRisk Factors for Heart Disease– Also, Taubert in JAMA 7/4/07Also, Taubert in JAMA 7/4/07
– Cocoa , as dark chocolate, lowers BP Cocoa , as dark chocolate, lowers BP and raises nitric oxide levelsand raises nitric oxide levels
– Therefore, Hyman says, (not simon Therefore, Hyman says, (not simon says), yes to chocolate!says), yes to chocolate!

Additional Points CardiovascularAdditional Points Cardiovascular
Stress and Heart DiseaseStress and Heart Disease– The following discussion is more The following discussion is more
developed in the literature for heart developed in the literature for heart disease and hypertension, but also disease and hypertension, but also applies generally to arrhythmiasapplies generally to arrhythmias
– There is a poor correlation between There is a poor correlation between patient complaints of palpitations patient complaints of palpitations and actual arrhythmia. Ref Barskyand actual arrhythmia. Ref Barsky

Additional Points CardiovascularAdditional Points Cardiovascular
Stress and Heart DiseaseStress and Heart Disease– 2 types of stress based on the 2 types of stress based on the
time frame involved:time frame involved:
» AcuteAcute
» ChronicChronic

Additional Points CardiovascularAdditional Points Cardiovascular
Stress and Heart Disease Stress and Heart Disease AcuteAcute: : – sudden, severe, significant episodes sudden, severe, significant episodes
of stress, as with physical exertion, of stress, as with physical exertion, may precipitate an increase in may precipitate an increase in blood pressure, arrhythmias, blood pressure, arrhythmias, angina or actual heart/brain angina or actual heart/brain infarctioninfarction

Additional Points CardiovascularAdditional Points Cardiovascular
Stress and Heart Disease Stress and Heart Disease ChronicChronic: : – when you are saying chronic stress when you are saying chronic stress
contributes to cardiovascular disease, contributes to cardiovascular disease, you are saying it is one of the risk you are saying it is one of the risk factors just listed. Therefore, as with factors just listed. Therefore, as with any risk factor, there has to be data to any risk factor, there has to be data to support the effectsupport the effect

Additional Points CardiovascularAdditional Points Cardiovascular
Stress and Heart Disease Stress and Heart Disease ChronicChronic: : – first, as with any risk factor, it must be first, as with any risk factor, it must be
present on a relatively constant, daily basis present on a relatively constant, daily basis to contribute to disease formation, to contribute to disease formation, aggravation or accelerationaggravation or acceleration
– you do not smoke one cigarette and develop you do not smoke one cigarette and develop lung cancerlung cancer
– you do not have altered lipids one day and you do not have altered lipids one day and have atherosclerosis the next dayhave atherosclerosis the next day

Additional Points CardiovascularAdditional Points Cardiovascular
Stress and Heart Disease Stress and Heart Disease ChronicChronic: : – This is an area of intense research. The most This is an area of intense research. The most
prominent contributors to the field are:prominent contributors to the field are:» Karasek, Theorell-Job StrainKarasek, Theorell-Job Strain» Siegrist, Peter-Effort RewardSiegrist, Peter-Effort Reward» Schnall, Landsbergis, Baker and Belkic-Threat Schnall, Landsbergis, Baker and Belkic-Threat
AvoidantAvoidant» Alfredsson, Hall, HlatkyAlfredsson, Hall, Hlatky

Additional Points CardiovascularAdditional Points Cardiovascular
Stress and Heart Disease Stress and Heart Disease ChronicChronic: : – Karasek identified job strain/stress as the Karasek identified job strain/stress as the
combination of high psychological demands and combination of high psychological demands and low decision latitude, the “Demand Control” modellow decision latitude, the “Demand Control” model
– Psychological demands=quantity of work+ mental Psychological demands=quantity of work+ mental requirements+time constraints, i.e. working fast requirements+time constraints, i.e. working fast and hardand hard
– Decision latitude=ability to make decisions about Decision latitude=ability to make decisions about your own work+creativity+skill use, i.e. low control, your own work+creativity+skill use, i.e. low control, low autonomy, little skill use low autonomy, little skill use

Additional Points CardiovascularAdditional Points Cardiovascular
Stress and Heart Disease Stress and Heart Disease ChronicChronic: : – Karasek investigated these parameters with Karasek investigated these parameters with
the JCQ-Job Content Questionnairethe JCQ-Job Content Questionnaire


Additional Points CardiovascularAdditional Points Cardiovascular
Stress and Heart Disease Stress and Heart Disease ChronicChronic::– Siegrist offered an alternative model, though Siegrist offered an alternative model, though
having many similar characteristics to having many similar characteristics to Karasek, called the “Effort Reward” modelKarasek, called the “Effort Reward” model
– Here the job strain/stress is a product of high Here the job strain/stress is a product of high job effort with low social rewardjob effort with low social reward

Additional Points CardiovascularAdditional Points Cardiovascular
Stress and Heart Disease Stress and Heart Disease ChronicChronic::– Belkic provides an excellent review in this Belkic provides an excellent review in this
area. She is a clinician and not an area. She is a clinician and not an epidemiologist.epidemiologist.
– Her questionnaire OSI-Occupational Stress Her questionnaire OSI-Occupational Stress Index is available for generic use and for a Index is available for generic use and for a few specific occupationsfew specific occupations
– In particular, the one occupation that has In particular, the one occupation that has consistently shown a pattern of increased consistently shown a pattern of increased heart disease risk is commercial bus driversheart disease risk is commercial bus drivers

Additional Points CardiovascularAdditional Points Cardiovascular
Stress and Heart Disease Stress and Heart Disease ChronicChronic::– Work by many including Alfredsson suggest Work by many including Alfredsson suggest
that shift work at poor hours may be an that shift work at poor hours may be an important marker of job strain that leads to important marker of job strain that leads to increased riskincreased risk

Additional Points CardiovascularAdditional Points Cardiovascular
Stress and Heart Disease Stress and Heart Disease ChronicChronic::– Probably best thought of as job strain has Probably best thought of as job strain has
it’s strongest impact in patients from lower it’s strongest impact in patients from lower SES group who display hostility, anger, time SES group who display hostility, anger, time urgency/impatience(TUI), depression, urgency/impatience(TUI), depression, anxietyanxiety

Additional Points CardiovascularAdditional Points Cardiovascular
Stress and Heart Disease Stress and Heart Disease ChronicChronic::– Do not underestimate the potential effects of Do not underestimate the potential effects of
stress. In the Schnall Cornell work, stress stress. In the Schnall Cornell work, stress had a relative risk = to cholesterol, cigs, etc. had a relative risk = to cholesterol, cigs, etc. In their work, job strain, age and BMI were In their work, job strain, age and BMI were the only reliable predictors of hypertensionthe only reliable predictors of hypertension
– The average effect of job strain seems to be The average effect of job strain seems to be 7mm Hg, may be as high as 12mm Hg7mm Hg, may be as high as 12mm Hg

Additional Points CardiovascularAdditional Points Cardiovascular
Stress and Heart Disease Stress and Heart Disease ChronicChronic::– References include:References include:
» Karasek book Karasek book Healthy Work; Healthy Work; articles are many including articles are many including J Occ Health Psych, 1998,3,4,322; website at Dept of J Occ Health Psych, 1998,3,4,322; website at Dept of Work Environment, Umass Lowell Work Environment, Umass Lowell www.uml.edu
» Theorell J Occ Health Psych 1996,1,1,9Theorell J Occ Health Psych 1996,1,1,9
» Shnall at Shnall at www.workhealth.org –the Job Stress Network –the Job Stress Network
» European Heart NetworkEuropean Heart Network
» JAMA 10/22/03, 290,16,2190JAMA 10/22/03, 290,16,2190
» Belkic in Scand J Work Environ Health 2004,30,3,85Belkic in Scand J Work Environ Health 2004,30,3,85

Additional Points CardiovascularAdditional Points Cardiovascular
ApportionmentApportionment: : – if the effect is only transient, such as an anginal if the effect is only transient, such as an anginal
episode or a brief rise in blood pressure, then episode or a brief rise in blood pressure, then this is a classic temporary exacerbation, i.e. no this is a classic temporary exacerbation, i.e. no impairment or disability, no apportionmentimpairment or disability, no apportionment
– recall that any factor, to be considered as part recall that any factor, to be considered as part of the apportionment, must be present on a of the apportionment, must be present on a relatively constant, daily basis to contribute to relatively constant, daily basis to contribute to disease formation, aggravation or accelerationdisease formation, aggravation or acceleration

Additional Points CardiovascularAdditional Points Cardiovascular
Apportionment PERMITTEDApportionment PERMITTED: : – Pre-existing disabilityPre-existing disability
– The natural progression of disease would have caused The natural progression of disease would have caused
a disability by this point in timea disability by this point in time
– Prior disability not manifest, as when a patient is not Prior disability not manifest, as when a patient is not
testing himselftesting himself
– Prior documented work restrictionPrior documented work restriction

Additional Points CardiovascularAdditional Points Cardiovascular
Apportionment NOT PERMITTEDApportionment NOT PERMITTED: : – Temporary DisabilityTemporary Disability
– DeathDeath
– Non-Disabling DiseaseNon-Disabling Disease
– Retroactive Work RestrictionRetroactive Work Restriction
– A totally rehabilitated injuryA totally rehabilitated injury

Additional Points CardiovascularAdditional Points Cardiovascular ApportionmentApportionment: :
– Causation a major consideration. If there is an industrial injury that Causation a major consideration. If there is an industrial injury that
happened in a patient with risk factors for cardiovascular disease, e.g. happened in a patient with risk factors for cardiovascular disease, e.g.
Diabetes, cigarette use; then apportion the final disability to these Diabetes, cigarette use; then apportion the final disability to these
factors which caused part of the formation of the diagnosed factors which caused part of the formation of the diagnosed
hypertension or heart diseasehypertension or heart disease
– this is almost, though not always, saying that the natural progression this is almost, though not always, saying that the natural progression
of disease would have caused impairment/disability by this point in of disease would have caused impairment/disability by this point in
time, absent the industrial injurytime, absent the industrial injury

Additional Points CardiovascularAdditional Points Cardiovascular
ApportionmentApportionment: : – the counter argument of apportionment to causation, the counter argument of apportionment to causation,
or to natural progression of disease, is that the or to natural progression of disease, is that the
industrial injury commenced the actual disability and industrial injury commenced the actual disability and
hence the disability is completely industrialhence the disability is completely industrial
– there are some jurisdictions that may contain worker there are some jurisdictions that may contain worker
compensation language supporting different positions compensation language supporting different positions

Additional Points CardiovascularAdditional Points Cardiovascular
ApportionmentApportionment: :
– rememberremember
» this is your best medical opinionthis is your best medical opinion
» you are asked to give your opinion based on reasonable you are asked to give your opinion based on reasonable
medical probability, i.e. > 50% likelihoodmedical probability, i.e. > 50% likelihood
» if you keep doing this properly, you are sure to anger a if you keep doing this properly, you are sure to anger a
lawyer, which is your real job, and joy, in lifelawyer, which is your real job, and joy, in life

THANK YOUTHANK YOU