the california family health project: iv. family structure/organization and adult health
TRANSCRIPT

Fam Proc 31:399-419, 1992
The California Family Health Project: IV. FamilyStructure/Organization and Adult Health
LAWRENCE FISHER, Ph.D.a
DONALD C. RANSOM, Ph.D.a
HOWARD E. TERRY, M.A.a
SANDRA BURGE, Ph.D.b
aCenter for the Study of the Family and Health, Department of Family and Community Medicine (AC-9), University of California, SanFrancisco, Box 0900, San Francisco CA 94143.bDepartment of Family Practice, University of Texas Health Science Center at San Antonio.
This research explores the relationships between each of four "domains" of family life and the health of husbands andwives in a community-based sample of 225 families. In this article we report the association between Family Structure/Organization and adult Health. This family domain refers to the architecture of the family or the structural frame ofroles and rules within which the family operates. Interrelationships among 13 self-reported, familyStructure/Organization scales are described, using principle components analysis (PCA) and multidimensional scalinganalysis (MDS). Derived, joint-spouse or couple Structure/Organization variables also were created using inter-batteryfactor analysis. The PCA yielded a poor solution, whereas the MDS yielded a good two-dimensional solution, whichroughly displayed the scales in a circular pattern for both husbands and wives. The analyses indicated that no singledimension or set of separate subdimensions adequately described the Structure/Organization variables. All 13 scalesthen were associated with a battery of 14 adult health scales for husbands and wives separately, using canonicalcorrelation. Different aspects of family Structure/Organization were correlated with health for husbands and wives:Organized Cohesiveness, Sex Role Traditionalism, Role Flexibility and Shared Roles for husbands; and OrganizedCohesiveness and Differentiated Sharing for wives. Different patterns of health scores also emerged by gender, withbehavioral indicators, such as Smoking and Drinking, more salient for husbands, and mood indicators, such as Anxietyand Depression, more salient for wives.
Fam Proc 31:399-419, 1992This is an introduction to the fourth and fifth articles in a series of reports describing the California Family Health
Project, a study of family and health relationships in a community-based sample. We designed this research to identifyfamily variables relevant to family member health, and to explore a set of basic questions that we hope will broaden thebase of family and health theory. Specifically, we sought to explore patterns of relationship between a relatively largenumber of family variables and a relatively large number of health variables to (1) identify primary family and healthvariables for use in health research, (2) provide a framework for describing family and health relationships in ways thatreflect the complexity of family life, and (3) observe differences in patterns of family and health relationships by gender.
Our aim was not to test a particular model or set of hypotheses. Our review of the literature made clear that most studiesof family and health relied on one or two indices, and few included more than one construct, one family domain, or oneaspect of health in the same study. Because the field of family and health relations seemed poised to move rapidly into anew phase of increased activity, we thought that a basic investigation employing a broad-based design and assessmentframework with a relatively large number of family and health variables could provide subsets of family and health linkagesthat we could then use to propose more encompassing models of family and health transaction than are presently available.
This research led us to consider the various ways the family is conceptualized and how health is defined and assessed.Further, it forced us to consider carefully the ways in which complex, multivariate family and health data are analyzed topermit a clear articulation of the data without becoming either overwhelmed by the complexity or yielding tooversimplification of complex family processes. This series of articles chronicles the problems we faced, the decisions wemade, and the family and health linkages we found.
The initial three articles in this series were presented in the issue of Family Process immediately preceding this one. Inthe first article, we reviewed the family and health literature to help us identify "domains" of family life that were relevant tohealth. We identified three levels of family theory to guide us: global theory, which provides lenses for viewing family andhealth relationships abstractly (for example, family systems theory, symbolic interactionism, developmental theory);midrange and dimensional theories, which propose specific processes and defined areas of content for further study (forexample, the Family Paradigm approach, the Double ABC-X Model, the Circumplex Model). Our literature review
_____________________________________________________________________________________________________________
1

suggested a consensus among family investigators about "domains" of family life with greatest relevance to health, althoughdifferent authors applied different terms to similar dimensions.
We used four criteria to establish a domain of family variables in this research: conceptual uniqueness, documentation inthe literature, links with health, and practicality of assessment. With these criteria, we identified and labeled four familydomains that led eventually to the selection of 73 family variables: (1) World View (family beliefs and expectationseightvariables assessed by self-report); (2) Emotion Management (how emotion is acknowledged and responded to33variables assessed by ratings of couple interaction); (3) Structure/Organization (degree of orderliness, pattern and clarity ofroles and rules13 variables assessed by self-report); and (4) Problem Solving (effectiveness and style of problemmanagementassessed by 16 ratings of family interaction).
We defined health broadly to include various aspects of physical, emotional, and social health. We used the RANDHealth Assessment Questionnaire, supplemented by other instruments, to assess 14 health variables, and each is describedbriefly in Appendix IV.1. and Appendix IV.1. (Continued).
To understand more about family and health linkages, we elected to study a community-based rather than a clinical orreferred sample. We reasoned that with this approach we would (1) add to a relatively neglected area of study, (2) define apotentially large universe from which to recruit families for study, and (3) be able to generalize our findings more widelythan is ordinarily possible. We used an anonymous telephone screening technique in a Central California community of500,000 to identify a sample of 225 families. Inclusion criteria for each family were: (1) an adolescent between the ages of13 and 18 in the home, (2) a heterosexual adult couple (not necessarily the biological parents of offspring) in the home forat least 3 years, (3) self-identified Anglo or Hispanic ethnicity, (4) adults who were born in or migrated to the U.S. beforethe age of 6, and (5) no family members who left or returned home in the previous 3 months. The 225 families we recruitedrepresented all but the lowest levels of social class. The average length of adult couple relationship was 17 years, andaverage family income was $44,350. A complete description of the sample is presented in Fisher, Ransom, Terry, et al.(1992).
Each family participated in a home visit and a 3-hour laboratory visit. The adult couple returned to the laboratory for asecond 3-hour visit. In addition to several family and health self-report instruments, the entire family participated in a30-minute, videotaped, family problem-solving game (SIMFAM II), and the adult couple participated in three, 10-minute,videotaped Emotion Management Interaction Tasks (EMITs) that elicited themes of loss, intimacy, or conflict. Each familywas sent a check for $100 at the completion of the protocol.
In this series of reports, we present data on each of the four family domains and health, following a uniform sequence ofdescriptive and associative analyses. In each report, we first describe one family domain and list the variables and scales weused. Second, we describe the association between this domain of family variables and 20 demographic variables (forexample, social class, ethnicity, family size). Third, we use principal components analysis (PCA) and multidimensionalscaling analysis (MDS) to describe the pattern of relationships among the variables in the family domain. Our goals are toobserve the internal "structure" of the variables selected for the family domain, to help us decide which variables to includein analyses with health. Fourth, we use canonical correlation analyses (CA) to associate the domain of family variables with14 health variables for husbands and wives separately. A rationale for the selection of these statistical procedures and abrief description of each is presented in the first article in this series (Fisher et al., 1992).
So far in this series of reports, we have applied this sequence of analyses to two family domains, World View andEmotion Management, and Health. We found that the 14 Health variables and the eight family World View variables couldnot easily be reduced by PCA to a few dimensions that adequately represented the original variables. Therefore, all of thevariables were used in subsequent associative analyses. For the EMIT variables, MDS revealed an ordered, bipolar display:one dimension reflected positive or negative exchanges of affect, and a second reflected overt versus indirect expression ofcouple affect. Variables reflecting husband or wife dominance of the interaction also emerged. The associative analyses forthe World View and Health data indicated strong associations between family Coherence, Religiousness, Optimism, andLife Engagement, and Health for husbands; and family Coherence, Optimism, and Religiousness, and Health for wives.Similar analyses for the EMIT and Health data yielded strong associations between couple Emotional Aversiveness andPositive Conflict Engagement, and Health for husbands; and couple Avoidance/Distance and Health for wives. Differencesbetween husbands and wives in family and health associations were described in each article.
In the two articles presented in this issue, we describe the remaining two domains of family variablesfamilyStructure/Organization and family Problem Solvingand associate them with adult health, following the same sequence ofanalyses employed in the previous articles. Two other articles will be presented in the next issue of this journal: VI reportsthe results of an analysis of all four family domains taken together with health excluded and then included, and VIIsummarizes and integrates the results of the previous articles in this series.
FAMILY STRUCTURE/ORGANIZATION
_____________________________________________________________________________________________________________
2

We use the term "family Structure/Organization" to refer to the overall architecture of the family, its degree oforderliness, and the clarity and organization of roles and rules. Although some family investigators consider family size,single-parent status, and other aspects of family membership "structural" variables (Kellam, Ensminger, & Turner, 1977),we draw a distinction between family demographic variables and the organizational patterning of family relations, whilerecognizing that in some ways the two are related.
Research in family sociology and family health psychology has linked several aspects of family Structure/Organizationwith the health and functional status of family members. Examples include family cohesion (for example, Barbarin, Hughes,& Chesler, 1985; Olson, Sprenkle, & Russell, 1979); sex role behavior (Downey, 1984); marital power (Mirowsky, 1985);family privacy (Pittman & Lloyd, 1988); and adaptability or role flexibility (Koch, 1985). Also, most family assessmentinventories include scales that tap various components of family Structure/Organization, for example, FACES (Olson et al.,1979), Family Environment Scale (Moos & Moos, 1981), and Family Assessment Device (Epstein, Baldwin, & Bishop,1983), attesting to the importance placed on this domain when considering issues of health and illness.
In reviewing this research, we were struck by its volume and scope, but also by the lack of a prominent, unifyingstructure from which we might select "representative" variables for use in this research. We found that scales assessingaspects of this domain were the most frequently employed of any in studies of families and health. However, of the fourfamily domains explored in this research, Structure/Organization seemed to us the least well-defined and displayed thegreatest amount of redundancy. Though clinicians and researchers alike recognize the importance ofStructure/Organizational variables, we were unable to find an integrated and overarching framework for this area of familyinvestigation.
To select representative variables for inclusion in our study, we created four groups of frequently used family Structure/Organization variables, based on our review of the literature: (1) interpersonal distance regulation in the family (cohesion,sharing, spouse distance, privacy); (2) degree or kind of internal family organization (orderliness, clarity of rules,organization of the household); (3) sex role traditionalism; and (4) role flexibility. There is nothing sacred about thesegroups of variables, and other investigators might have partitioned this domain differently.
Each of these four aspects of family Structure/Organization has demonstrated substantive links with health in theliterature, and each appeared to be related conceptually to the others. The amount of clinical and theoretical attention paidto how families define and regulate interpersonal distance to balance personal autonomy and family relatedness led us toexpect that this dimension would prove preeminent in relation to health. Kantor and Lehr's (1975) discussion of familydistance regulation, Olson et al.'s (1979) review of family cohesion, Minuchin and colleagues' (Minuchin, Montalvo,Guerney, et al., 1967) description of enmeshment and disengagement, and the inclusion of a number of distance regulationvariables in almost all major family assessment scales suggested the importance placed on this group of variables by familyscholars over the years. At the same time, however, we were less certain how the internal structure of this domain of familyvariables would be described by the data. The four broad content areas might be so interrelated in the minds of familymembers that four clear clusters or components might not emerge. Further, there is sufficient breadth and complexityamong these four areas to lead us to doubt that all four would be combined into one large construct that adequatelyrepresented the Structure/Organization domain.
METHODSDescriptions of the sample, procedures, and health variables were presented in the first article in this series (Fisher et al.,
1992).
Family Structure/Organization ScalesWe identified 13 family Structure/ Organization variables using the four content areas just described and the criteria
outlined in the first article in this series: conceptual distinctness, representativeness in the literature, documentedassociation with health, and practicality of assessment (see Table 1). Our goal was not to select all possible descriptors thatfit the four content areas of family Structure/ Organization; nor did we use any single family perspective or theoreticalorientation to guide variable selection. Instead, this domain was sampled broadly to yield a range of dimensions provenuseful to family scholars previously.
Table 1Family Structure Variables
Scale No. Items Description and Sample Items Lambda Max.*
Adaptability 14 Ability of system to change its power structure, role relationships,and relationship rules in response to situational and developmentalstress:**
.825
_____________________________________________________________________________________________________________
3

1. Family members are afraid to say what is their mind.
2. It is difficult to get a rule changed in our family.
Clarity of Leadership 3 Clarity about who makes decisions and what the decisions are: .526
1. It is clear who makes the decision about money in our family.
2. It is easy to know who the leader is in our family.
Cohesion 16 The emotional bonding members have with each other and thedegree of individual au-tonomy a person experiences in the familysystem**
.886
Isolated Problem Solving 3 Solving problems without the support of other family members: .574
1. Family members solve their problems on their own.
2. Family members should handle things themselves if they getinto trouble.
Orderliness 5 Amount of family structure: .784
1. Our family is well organized.
2. Meals are planned in advance in our family.
Organization of HouseholdTasks
3 Organization of household tasks: .707
1. It is hard for family members to keep track of their chores.
2. We all agree as to who does what around the house.
Personal Privacy 6 Amount of personal privacy permitted by the family: .693
1. Everyone has a special place to keep personal things at ourhouse.
2. When a bedroom door is shut, family members knock beforeentering.
Rule Clarity 3 Clarity of norms and sanctions for breaking rules: .711
1. It is hard to know what the rules are in our family because theyare always changing.
2. In our family the kids know what the parents expect of them.
Sex-Role Traditionalism 13 Traditional gender-related role structure: .843
1. Wives, more than husbands, should make most of the decisionsabout childrearing.
2. The needs of a family should come before a woman's personalneeds.
Separate Spouse Activities 6 How much one spouse relies on the other for various concerns andactivities:
.653
1. Financial matters
2. Companionship
Shared Decision Making 4 Number of areas in which family decisions are made jointly: NA***
1. Who makes decisions about husband's job?
2. Who decides if the wife should work?
Sharing 9 Amount of sharing free time, friends, thoughts, and feelings: .770
1. We know very little about each other's friends.
2. We share most interests and hobbies with each other.
Shared Roles 8 Number of specific roles that are shared or occupied by one spouseonly:
NA***
1. Handling the finances
2. Cooking* Lambda Max. refers to the greatest of the six Guttman reliability coefficients; .50 is considered acceptable.** This definition is quoted from Olson et al., 1979.
_____________________________________________________________________________________________________________
4

*** These are non-Likert items. The scale total is the sum of areas of decision making or shared roles listed.
Seven family Structure/Organization scales were taken from the California Family Life Scales, a comprehensive,98-item, self-report inventory developed for this research: Isolated Problem Solving, Orderliness, Rule Clarity, Clarity ofLeadership, Organization of Household Tasks, Personal Privacy, and Sharing. Each scale underwent extensive evaluationboth with this sample and with an additional sample of 255 married adults recruited from church and civic groups. For eachsample, the scales underwent a PCA and separate assessments of internal consistency for males and females. A single, largecomponent for each scale was confirmed through PCA, and Guttman lambda coefficients were computed (see Table 1).1 Ingeneral, the results of the analyses by gender yielded comparable findings so that the same scale could be used for bothhusbands and wives.
In addition to these seven scales, we selected the Adaptability and Cohesion scales from FACES II (Olson, McCubbin,Barnes, et al., 1983). Also selected were four scales, suggested by Bernard Bloom (personal communication), derived fromthe work of Chiriboga and Thurnher (1980), and from Felton, Brown, Lehman, and Liberator (1980): Shared Roles, SharedDecision Making, Separate Spouse Activities, and Sex-Role Traditionalism. These six scales also underwent PCA andreliability analyses to conform with the criteria listed above.
Correlations were run between each of the 13 family Structure/Organization variables and 20 family demographicvariables (for example, education, occupation, family size, length of marriage) by gender. Of the 520 correlations, only 17were above .20, and none exceeded .30. Considering the generally low correlations and our desire to explore theassociation of demographic and family variables by a hypothesis-testing strategy at a later stage, no controls fordemographics were included in the analyses reported here.
Below, we first present the results, by gender, of the PCA and MDS of the 13 family Structure/Organization variables.PCA and MDS are two complementary descriptive procedures for observing the relationships among the family variablesin this domain. They were used to tell us something about the internal structure of the domain and to assist us in decidingwhich family Structure/Organization variables to include in the analyses with health. Next, we report separate canonicalcorrelation analyses (CA) between the family Structure/Organization variables and the 14 adult health variables, separatelyfor husbands and wives. This procedure enabled us to observe patterns of association between family and health variablesfor each gender. Last, we repeat the CAs, this time using derived husband-wife Structure/ Organization scores establishedby inter-battery factor analysis. These analyses allowed us to associate joint-spouse perceptions of familyStructure/Organization and spouse health. Complete data for the variables used in these analyses were available for 172husbands and 160 wives.
RESULTS
PCA And MDS AnalysesWe submitted all 13 family Structure/ Organization variables to a PCA with oblique rotation. Using conventional
criteria, up to five components were justified in the analysis for husbands and for wives, but the general factor structureswere weak in both cases. For husbands, three well-defined components emerged, accounting for only 51% of the variance,and the two additional components were poor doublets or singletons. For wives, two well-defined components emerged,accounting for only 42% of the variance, and the remaining three components were composed of doublets or partialsingletons. The results of the PCAs for husbands and for wives indicated that the family structure variables did not conformwell to a method that reduces the variables into a smaller number of dimensions or subgroups that efficiently andmeaningfully represent the total number of variables.
We next submitted the 13 family Structure/Organization variables to an MDS analysis. A two-dimensional solution wasretained for both husbands (R2 = .92, stress = .15) and wives (R2 = .91, stress = .14; see Figure 1). The MDS clearlyshowed why the results of the PCA were unsatisfying: no clear grouping of variables emerged in the circular-shapeddisplay. Some broad clustering of variables was present, however, with minor variation by gender. The right side of thegraphic displayed a group of family closeness and organization variables. In contrast, variables that reflected spousedistance and isolated problem management were found on the left side. Traditionalism was located in the upper region forboth husbands and wives. The pattern of correlations among the Structure/Organization scores as a whole did not representsignificant bipolarity (that is, consistent negative correlations between variables on opposite sides of the ring). Further,Clarity of Leadership, Personal Privacy, and Sex-Role Traditionalism appeared distant from other variables in the display,corresponding to their presentation as singletons in the PCA described above.
_____________________________________________________________________________________________________________
5

_____________________________________________________________________________________________________________
6

Figure 1.MDS configuration for husbands' and wives' Structure/Organization data.
Looking at Figure 1, it is clear that additional sampling of this family domain would have been helpful. We selectedfamily Structure/Organization variables from the broad content areas described earlierwe did not select variables basedon a systematic sampling of a well-defined and fully partitioned family construct (see Canter, 1985). Although adequate forour current needs, additional sampling will be helpful in future research.
In sum, using these self-report scales with this community-based sample, we did not find either a single overarchingdimension or several relatively uncorrelated sub-dimensions that could be used to reduce the 13 familyStructure/Organization variables. We decided, therefore, to include all 13 family Structure/Organization variables in thecanonical analyses with Health, as described below.
Canonical Correlation AnalysesCanonical correlation allowed us to correlate linear composites (called canonical variates) of one set of variables (in this
case, family Structure/Organization scales) with linear composites of a second set of variables (in this case, Health scales),when both were taken together. The benefit of CA is that it provides a correlation between two groups of variables, just as aPearson coefficient provides a measure of the correlation between two individual variables. The first pair of canonicalvariates represents the highest correlation between any two linear composites. The next pair is based on the residualvariance and represents the next highest correlation between any two linear composites, and so on. Thus, each pair ofcanonical variates is independent of the others.
We present below the structure matrix for each analysis, along with codes to reflect the weight and complementarystructure matrices.2 We describe and label each canonical variate by listing those variables that are most highly "loaded" oneach, similar to defining a component in PCA. This enables us to observe the statistical linking of subsets of variablesacross the domains of family Structure/Organization and Health.
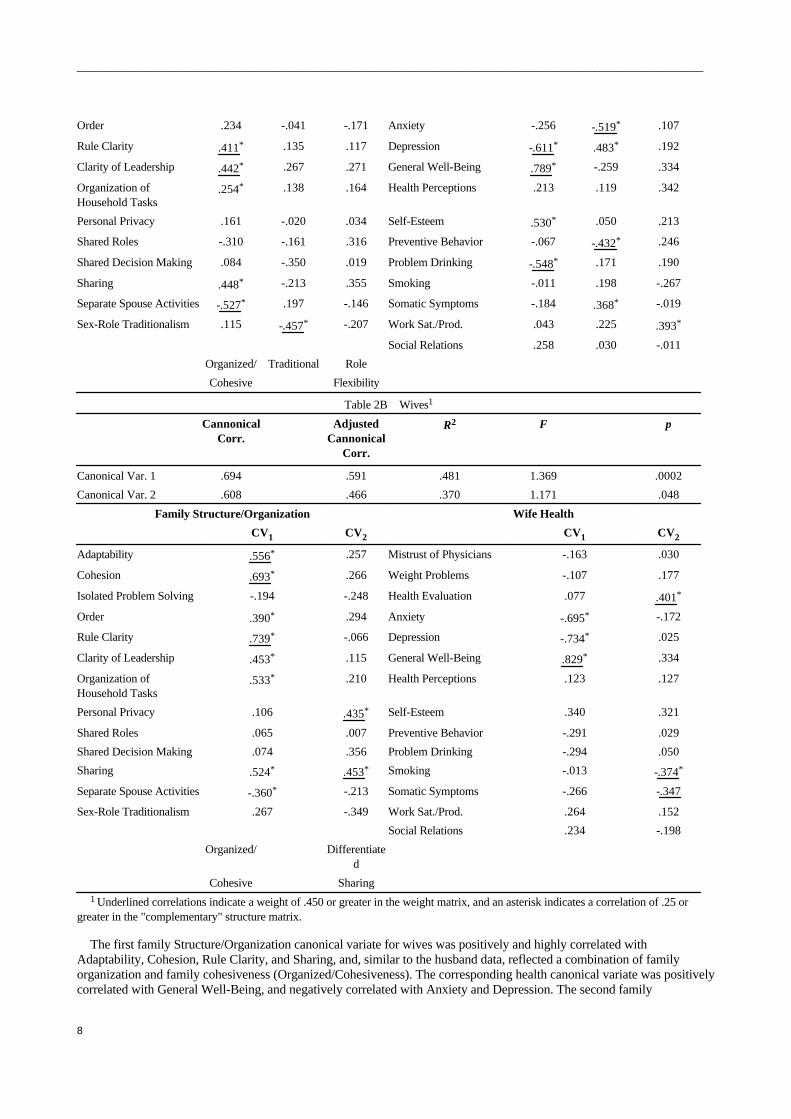
Individual CAsThree significant pairs of canonical variates were found for husbands and two were found for wives. The CA statistics
and structure matrixes are presented in Table 2A for husbands and 2B for wives (zero-order correlations among thevariables are available from the first author). For husbands, the first family Structure/Organization canonical variatedisplayed high positive correlations with family Cohesion, Sharing, Clarity of Leadership, and Rule Clarity, and highnegative correlations with Separate Spouse Activities, suggesting what we call an Organized/ Cohesive family pattern. Thecorresponding health canonical variate was positively correlated with General Well-Being and Self-Esteem, and negativelycorrelated with Depression and Problem Drinking. The second canonical variate for husbands displayed high positivecorrelations with Adaptability and Sex-Role Traditionalism, suggesting a Traditional family style. Its corresponding healthcanonical variate was negatively correlated with Anxiety and Depression, and positively correlated with PreventiveBehaviors. The third family Structure/Organization canonical variate for husbands displayed the highest positive correlationwith Adaptability. The pattern of associations with this canonical variate presents a configuration of scores that suggestsfamily Role Flexibility. The corresponding health canonical variate was positively correlated primarily with WorkSatisfaction/Productiveness.
Table 2Person-Level Family Structure/Organization and Health CA: CA Statistics and Structure Matrix
Table 2AHusbands1
Canonical Corr. AdjustedCanonical Corr.
R2 F p
Canonical Var. 1 .681 .565 .464 1.533 .0001
Canonical Var. 2 .619 .477 .383 1.360 .0005
Canonical Var. 3 .579 .449 .336 1.230 .0197
Family Structure/Organization Husband Health
CV1 CV2 CV3 CV1 CV2 CV3
Adaptability .325* -.406* .411* Mistrust of Physicians .367* .092 -.349
Cohesion .677* -.164 .316 Weight Problems .035 .015 .179
Isolated Problem Solving -.331 -.365 -.127 Health Evaluation .167 -.041 .062
_____________________________________________________________________________________________________________
7
Order .234 -.041 -.171 Anxiety -.256 -.519* .107
Rule Clarity .411* .135 .117 Depression -.611* .483* .192
Clarity of Leadership .442* .267 .271 General Well-Being .789* -.259 .334
Organization ofHousehold Tasks
.254* .138 .164 Health Perceptions .213 .119 .342
Personal Privacy .161 -.020 .034 Self-Esteem .530* .050 .213
Shared Roles -.310 -.161 .316 Preventive Behavior -.067 -.432* .246
Shared Decision Making .084 -.350 .019 Problem Drinking -.548* .171 .190
Sharing .448* -.213 .355 Smoking -.011 .198 -.267
Separate Spouse Activities -.527* .197 -.146 Somatic Symptoms -.184 .368* -.019
Sex-Role Traditionalism .115 -.457* -.207 Work Sat./Prod. .043 .225 .393*
Social Relations .258 .030 -.011
Organized/ Traditional Role
Cohesive Flexibility
Table 2BWives1
CannonicalCorr.
AdjustedCannonical
Corr.
R2 F p
Canonical Var. 1 .694 .591 .481 1.369 .0002
Canonical Var. 2 .608 .466 .370 1.171 .048
Family Structure/Organization Wife Health
CV1 CV2 CV1 CV2
Adaptability .556* .257 Mistrust of Physicians -.163 .030
Cohesion .693* .266 Weight Problems -.107 .177
Isolated Problem Solving -.194 -.248 Health Evaluation .077 .401*
Order .390* .294 Anxiety -.695* -.172
Rule Clarity .739* -.066 Depression -.734* .025
Clarity of Leadership .453* .115 General Well-Being .829* .334
Organization ofHousehold Tasks
.533* .210 Health Perceptions .123 .127
Personal Privacy .106 .435* Self-Esteem .340 .321
Shared Roles .065 .007 Preventive Behavior -.291 .029
Shared Decision Making .074 .356 Problem Drinking -.294 .050
Sharing .524* .453* Smoking -.013 -.374*
Separate Spouse Activities -.360* -.213 Somatic Symptoms -.266 -.347
Sex-Role Traditionalism .267 -.349 Work Sat./Prod. .264 .152
Social Relations .234 -.198
Organized/ Differentiated
Cohesive Sharing1 Underlined correlations indicate a weight of .450 or greater in the weight matrix, and an asterisk indicates a correlation of .25 or
greater in the "complementary" structure matrix.
The first family Structure/Organization canonical variate for wives was positively and highly correlated withAdaptability, Cohesion, Rule Clarity, and Sharing, and, similar to the husband data, reflected a combination of familyorganization and family cohesiveness (Organized/Cohesiveness). The corresponding health canonical variate was positivelycorrelated with General Well-Being, and negatively correlated with Anxiety and Depression. The second family
_____________________________________________________________________________________________________________
8

Structure/Organization canonical variate for wives was highly correlated with Privacy and Sharing. We called thiscanonical variate Differentiated Sharing, reflecting a balance of personal separateness and family communality. Thecorresponding canonical variate for health was correlated positively with Health Evaluation, and negatively with Smokingand Somatic Symptoms.
In sum, for husbands, family Organized/ Cohesiveness was correlated positively with General Well-Being, andnegatively with Depression and Problem Drinking; Sex-Role Traditionalism was correlated negatively with Anxiety andDepression; and Role Flexibility was correlated positively with Work Satisfaction/Productiveness. For wives,Organized/Cohesiveness was correlated positively with General Well-Being and negatively with Anxiety and Depression,and Differentiated Sharing was correlated positively with physical Health Evaluation.
Couple CAsWe also constructed husband-wife scores, which reflected the salience of the Structure/Organization variables for each
couple, through inter-battery factor analysis (Cudek, 1982). This procedure determines if similar dimensions exist in two ormore groups of scores, while maintaining the logical integrity of self-report data (Fisher, Kokes, Ransom, et al., 1985;,Ransom, Fisher, Phillips, et al., 1990). In this case, a battery is composed of a group of husband scores and a group of wifescores, consisting of the same Structure/Organization scales. Because our goal was to explore patterns of relationshipsamong scores, we accepted the solution in which the largest number of well-defined factors occurred. This resulted in sevenwell-defined factors that neatly contained the same Structure/Organization scales for husbands and wives (homologousstructure): Flexible Closeness, Orderliness, Shared Roles, Clarity of Leadership, Clarity of Roles and Tasks, SeparateSpouse Activities, and Shared Decision Making.3 The matrix of loadings and our descriptive labels for each factor arepresented in Table 3. These seven factors next were submitted to a CA with husband health and a CA with wife health, andthe CA statistics and structure matrixes, with codes reflecting the "complementary" structure and weight matrices, arepresented in Table 4A and Table 4B, respectively.
Table 3Inter-Battery Factor Analysis of Family Structure/Organization Data
Oblique Rotation: 7 Factor Inter-Battery Factor Analytic Solution
1 2 3 4 5 6 7
Husbands
Adaptability .688 .076 .077 -.053 .045 .087 .012
Cohesion .429 .055 -.061 .065 .378 -.053 .108
Isolation .031 -.376 -.073 -.092 -.005 -.042 -.051
Order .138 .758 -.158 -.131 .045 -.108 -.027
Rule Clarity -.011 .199 .083 .162 .434 .107 -.162
Clarity of Leadership -.087 .142 -.009 .502 .027 -.024 -.064
Household Tasks .025 .099 -.112 .012 .502 -.107 -.042
Personal Privacy .289 .026 .011 .009 .000 .057 .093
Shared Roles .060 .039 .787 -.073 -.072 .010 -.061
Shared Decisions .038 -.060 .100 -.049 .082 .013 .588
Sharing .329 .075 .029 .404 .198 -.142 .222
Sep. Spouse
Activities .015 -.050 -.062 .155 -.176 .619 -.063
Sex-Role
Traditionalism .111 -.228 -.078 .322 -.121 -.168 -.275
Wives
Adaptability .650 .003 .002 -.092 .093 .018 -.048
Cohesion .478 .007 -.072 .005 .325 -.228 .033
Isolation -.061 -.023 -.205 -.066 -.037 .237 -.043
Order .066 .744 -.078 .102 .023 -.099 -.061
Rule Clarity -.029 .047 .095 .247 .285 -.099 -.278
_____________________________________________________________________________________________________________
9

Clarity of Leadership -.012 .130 .094 .597 .039 .063 .023
Household Tasks .067 .067 -.057 .073 .524 -.029 .007
Personal Privacy .518 .006 .058 .076 -.253 -.028 -.121
Shared Roles .025 -.133 .764 .012 -.027 -.047 .012
Shared Decisions -.007 .053 -.093 .040 -.141 -.069 .570
Sharing .439 -.039 .016 .193 .199 -.165 .187
Sep. Spouse
Activities .107 -.030 .043 -.075 .134 .643 .030
Sex-Role
Traditionalism .091 -.158 -.232 .537 .075 -.044 -.049
Factor Labels FlexibleCloseness
Orderliness Shared Roles Clarity ofLeadership
Clarity ofRules & Task
SeparateSpouse Actvts
SharedDecisionMaking
Table 4Couple-Level Family Structure/Organization and Health CA: CA Statistics and Structure Matrix
Table 4AHusbands1
Canonical Corr. AdjustedCanonical Corr.
R2 F p
Canonical Var. 1 .617 .526 .381 1.798 .0001
Canonical Var. 2 .481 .526 .231 1.440 .0108
Family Structure/Organization Husband Health
CV1 CV2 CV1 CV2
Flexible Closeness .458 .450* Mistrust of Physicians .204 -.471*
Orderliness .028 .018 Weight Problems .295 -.227
Shared Roles -.202 .861* Health Evaluation .190 .388
Clarity of Leadership .590* .058 Anxiety -.252 .081
Clarity of Rules & Tasks .483* .289 Depression -.580* .196
Separate Spouse Activities -.700* .100 General Well-Being .672* .124
Shared Decision Making -.075 .241 Health Perceptions .093 .386
Self-Esteem .304 .076
Preventive Behaviors -.125 .400
Problem Drinking -.611* -.185
Smoking -.264 -.210
Somatic Symptoms -.330 -.342
Work Sat./Prod. .262 .518*
Social Relations .284 -.214
Organized/ Shared
Cohesive Roles
Table 4BWives1
Canonical Corr. AdjustedCanonical Corr.
R2 F p
Canonical Var. 1 .642 .567 .412 1.826 .0001
Canonical Var. 2 .485 .315 .235 1.355 .0279
Family Structure/Organization Wife Health
_____________________________________________________________________________________________________________
10

CV1 CV2 CV1 CV2
Flexible Closeness .740* .472* Mistrust of Physicians -.121 .181
Orderliness .294 .217 Weight Problems .021 -.044
Shared Roles .095 .357 Health Evaluation .116 .216
Clarity of Leadership .542* -.257 Anxiety -.625* -.077
Clarity of Rules & Tasks .536* -.247 Depression -.748* .010
Separate Spouse Activities -.474* .466* General Well-Being .817* -.065
Shared Decision Making -.264 .084 Health Perceptions .214 .384
Self-Esteem .626* .597*
Preventive Behaviors -.191 .385
Problem Drinking -.144 -.153
Smoking .036 -.045
Somatic Symptoms -.387* -.349
Work Sat./Prod. .437* -.132
Social Relations .287 -.223
Organized/ Differentiated
Cohesive Sharing1 Underlined correlations indicate a weight of .450 or greater in the weight matrix, and an asterisk indicates a correlation of .25 or
greater in the "complementary" structure matrix.
Two significant canonical variates emerged in the association of joint-spouse family Structure/Organization factors andhusband health. The first canonical variate was correlated positively with Flexible Closeness, Clarity of Leadership, Clarityof Roles and Tasks, and was correlated negatively with Separate Spouse Activities. This canonical variate reflected a globalconstruct composed of family organization and family cohesion, similar to Organized/Cohesiveness found in the previousanalyses. The corresponding health canonical variate was positively correlated primarily with General Well-Being andnegatively correlated with Depression and Problem Drinking, a pattern of association also similar to the individual CAfindings for husbands. The second family Structure/Organization canonical variate for husbands was highly and positivelycorrelated with Shared Roles (r = 0.86) and moderately correlated with Flexible Closeness (r = 0.45). Because of therelative size of the correlations, we called this canonical variate Shared Roles. The corresponding health canonical variatewas correlated positively with Work Satisfaction/Productiveness, Mistrust of Physicians, and Preventive Behaviors. It isinteresting that Anxiety for husbands was not associated with any family Structure/Organization canonical variate in thecouple analyses, whereas a substantial correlation was found in the individual score analysis.
Two canonical variates also emerged in the analysis of the joint-spouse family Structure/Organization data and wifehealth. The first canonical variate for family Structure/Organization was correlated positively with Flexible Closeness,Clarity of Leadership, and Clarity of Roles and Tasks, and was correlated negatively with Separate Spouse Activities.Again, this group of variables was similar to Organized/Cohesiveness, described in the individual analyses. Thecorresponding health canonical variate was correlated positively primarily with General Well-Being, Self-Esteem, WorkSatisfaction/Productiveness, and negatively with Anxiety, Depression, and Somatic Symptoms. The second familyStructure/Organization canonical variate for wives was correlated positively with Flexible Closeness and Separate SpouseActivities, and was similar in description to the Differentiated Sharing canonical variate found in the individual scoreanalyses. Its corresponding health canonical variate was correlated positively with Self-Esteem and other physical healthindicators (Health Perceptions and Preventive Behaviors), and negatively with Somatic Symptoms.
DISCUSSION
Descriptive AnalysesThe results of the PCA and MDS analyses support the usefulness of exploring a broad pattern of relationships among
family Structure/Organization variables. Although the roughly circular MDS solution is suggestive, the presence of gaps inthe display points to the need to expand and refine the number of variables included. For example, the large space betweenShared Roles/Shared Decision Making and Separate Spouse Activities for husbands might be filled by a scale reflectingpersonal autonomy within the family without isolation.
_____________________________________________________________________________________________________________
11

The PCA and MDS analyses also suggest that the family Structure/Organization domain is not well represented by asingle, large dimension, by a series of independent dimensions, or by one or two variables taken out of context. Theproximity of Adaptability and Cohesion in the display for both husbands and wives provides us with an instructive example.If, indeed, the goal is to assess family Structure/Organization at all comprehensively, we are persuaded by our findings tobegin with a larger and more discriminating set of variables than is typically used in current family and health research(Fisher, Terry, & Ransom, 1990).
Associative AnalysesThe degree of association between self-reports of family Structure/Organization and personal health is considerable, and
suggests the salience of this family domain for any broad, theoretical understanding of family and health relations. Forhusbands, the cumulative percent of variance accounted for by the three canonical variates is 54%, and for wives the twocanonical variates jointly account for 44% of the variance. Likewise, the cumulative percent of variance accounted for inthe couple analyses is 56% for husbands and 62% for wives. Considerably higher associations are found for wives betweenfamily variables and health in the couple analyses, compared to the individual analyses, suggesting the importance andpotential of the under-explored terrain of family appraisals that are salient to both spouses.
We also identified several family Structural/Organization constructs that are linked with adult health (see Figure 2). Forhusbands, Organized Cohesiveness, Sex-Role Traditionalism, and Role Flexibility are important correlates of health in theindividual analyses, and Organized Cohesiveness and Shared Roles emerge in the couple analyses. For wives, OrganizedCohesiveness and Differentiated Sharing are identified in both the person and couple canonical analyses. Althoughcontinued exploration of these variables with other samples is needed, these variable groups provide us with a useful stepin the identification and ordering of important family Structure/Organization variables that are related to family memberhealth.
_____________________________________________________________________________________________________________
12

Figure 2.Summary table: Structure/Organization and Health canonical analyses for husbands and wives.
Organized Cohesiveness is a particularly interesting Structure/Organization composite, given the recent history of familyassessment. Families are frequently scaled along separate dimensions of family organization and family closeness orcohesion. Our data suggest that the joint relationship of these two family qualities takes on new meaning. Why, in oursample, do these two conventionally distinct descriptors of family Structure/Organization covary so closely with thereported health and well-being of both husbands and wives? One possibility is that families in the community, such as those
_____________________________________________________________________________________________________________
13

in our sample, have busy lifestyles, hectic schedules, and competing personal demands. Our experience with these familiessuggests that considerable energy is required to maintain family structures that sustain feelings of closeness and cohesionamong family members. Without such structuring, a sense of "family" may become diluted, leading to less contact amongfamily members, diminished feelings of family support and personal well-being, and less confidence in one's health thanwould be the case otherwise. From this perspective, the joint operation of family closeness and family organization providesa conceptually intriguing complex with implications for health.
Differentiated Sharing is another composite of family Structure/Organization scores that covaries with health for wives.This variable group is composed of two positively correlated scores: Family Privacy, reflecting family support for beingalone and having "personal space," and Family Sharing, referring to family support for shared activities with other familymembers. Their joint association with the same canonical variate suggests a linkage between family support for sharedfamily activities and family respect for the individuality of each family member. Together they represent a strongdimensional correlate of health for wives. Respect for personal boundaries within the context of shared family relationshipshas been proposed as central to an optimal family climate. In clinical settings, we have observed considerable tensionbetween the need for clear personal boundaries and the demands of family life. It is significant that in our study the salienceof this pattern of scores holds only for wives. It is probably no surprise that the often contradictory demands of traditionalfamily and work roles, and the difficulty in setting aside time for personal needs and wishes, is more salient for wives thanfor husbands.
The variable groups we identified in this study reflect what appear to be key features of family Structure/Organizationwith salience for self-reported health in this community-based sample. The major family canonical correlates represent (1)the structural unity and integration of family members (Organized Cohesiveness), (2) the content of family roles(Traditional versus non-Traditional), (3) the ability to share and alter family roles (Shared Roles and Role Flexibility), and(4) the family's support for a balance between personal and family spheres of behavior and experience (DifferentiatedSharing).
These findings support our initial expectations about the importance of family distance regulation for self-appraisedhealth, especially for wives. Family cohesion is a major contributor to Organized Cohesiveness, and Personal Privacy andFamily Sharing are also indices of primary distance regulation. Distance regulation variables also reach significance withhealth for husbands, but they do so in conjunction with three other content areas: organization, traditionalism, and roleflexibility. Because Sex-Role Traditionalism and Shared Roles are positively associated with Health, and Role Flexibility isnegatively associated with Health, it appears that predictable and traditional family role structures, in which husbands havea generally dominant and customary position with few opportunities for unexpected shifts or changes in responsibilities, arepositively associated with husband health.
Gender differences are also evident in the patterns of health variables correlated with family Structure/Organizationscores. The salient health indices for husbands in the individual analysis are Anxiety, Depression, General Well-Being, andProblem Drinking; whereas, in the couple analysis, Work Satisfaction/Productiveness is more prominent. The pattern ofhealth variables for wives in the individual analysis includes a similar set of well-being and mood indicators, but alsoincludes Somatic Symptoms. Unlike husbands, no associations with Work Satisfaction/Productiveness or ProblemDrinking occurs for wives. The same general pattern of differences between husbands and wives is revisited in the coupleanalysis, with Health Perceptions and Somatic Symptoms for wives. As we reported in the analysis of the World Viewdomain and adult health (Ransom, Fisher, & Terry, 1992), drinking and smoking emerge as behavioral health indicators forhusbands, whereas anxiety, somatic symptoms, and a sense of somatic wellbeing emerge for wives.
More health variables are associated with family Structure/Organization in the couple analyses than in the individualanalyses for wives. This suggests the broader health implications of this family domain for wives than for husbands. Thequality of family organization of tasks and roles, family responsiveness, and a sense of family sharingprimary andtraditional arenas of women's work and emotional investmentare salient for more aspects of a general health construct forwives than for husbands. This finding also fits the observation made by Verbrugge (1985) in her review of the potentialcauses of gender differences in health. She suggests that although prior health care, biological risks, health reporting, andcaretaker effects are contributory, the bulk of gender differences in health can best be attributed to "acquired risks"(day-to-day conflicts in primary roles, competing demands of home and work) and psychosocial factors (the perception andevaluation of symptoms). Our findings in the analyses of both the family Structure/Organization domain and Health, and theWorld View domain and Health conform well with Verbrugge's observations.
Our findings suggest several important questions to address in future research. First, we have not explored the impact ofdifferences in perceptions about family Structure/Organization between spouses, and the effects of these differences ontheir respective states of health. Do couples tend to agree or disagree about these primary aspects of the family? Do theyhave different basic pictures of the family in terms of the patterning of variables we have been discussing here? Coupletypes, similar to those constructed by Fitzpatrick (1988), could be derived, and implications for the health of each spousecould be explored. Second, we have not introduced the potential differences that stress might have on the relationship
_____________________________________________________________________________________________________________
14

between patterns of family Structure/Organization and the reported health of spouses. For example, some patterns or stylesof family Structure/Organization may mediate the effects of stress better than others.
CONCLUSIONOur findings demonstrate that the domain of family Structure/Organization, as defined here, is highly associated with
patterns of health scores for both husbands and wives in this community-based sample. These patterns vary in specific waysby gender. The results suggest that this area of family and health association is worthy of continued exploration. In the nextarticle in this series we explore the association of a fourth family domain: family problem solving and the health ofhusbands and wives.
REFERENCES
1. Barbarin, O. A., Hughes, D. and Chesler, M. A., (1985). Stress, coping, and marital functioning among parents ofchildren with cancer. Journal of Marriage and the Family 47: 473-480.
2. Canter, D. (Ed.), (1985). Facet theory: Approaches to social research. New York: Springer-Verlag. 3. Chiriboga, D. A. and Thurnher, M., (1980). Marital lifestyles and adjustment to separation. Journal of Divorce 3:
379-390. 4. Cudek, R., (1982). Methods for estimating between-battery factors. Multivariate Behavioral Research 17: 47-68. 5. Downey, A. M., (1984). The relationship of sex-role orientation to self-perceived health status in middle-aged
adults. Sex Roles 11: 211-224. 6. Epstein, N. B., Baldwin, L. M. and Bishop, D. S., (1983). The McMaster Family Assessment Device. Journal of
Marital and Family Therapy 9: 171-180. 7. Felton, B. J., Brown, P., Lehman, S. and Liberator, P., (1980). The coping function of sex-role attitudes during
marital disruption. Journal of Health and Social Behavior 21: 240-248. 8. Fisher, L., Kokes, R. F., Ransom, D. C., Phillips, S. L. and Rudd, P., (1985). Alternative strategies for creating
"relational" family data. Family Process 24: 213-224. 9. Fisher, L., Ransom, D. C., Terry, H. E., Lipkin, M. and Weiss, R., (1992). The California Family Health Project: I.
Introduction and description of adult health. Family Process 31: 231-250. 10. Fisher, L., Terry, H. E. and Ransom, D. C., (1990). Advancing a family perspective in health research: Models
and methods. Family Process 29: 177-189. 11. Fitzpatrick, M. A., (1988). Between husbands and wives: Communication in marriage. Beverly Hills CA: Sage
Publications. 12. Kantor, D. and Lehr, W., (1975). Inside the family: Toward a theory of family process. San Francisco:
Jossey-Bass. 13. Kellam, S. G., Ensminger, M. E. and Turner, R. J., (1977). Family structure and the mental health of children:
Concurrent and longitudinal community-wide studies. Archives of General Psychiatry 34: 1012-1022. 14. Koch, A., (1985). A strategy for prevention: Role flexibility and affective reactivity as factors in family coping.
Family Systems Medicine 3: 70-81. 15. Minuchin, S., Montalvo, B., Guerney, B. G., Jr., Rosman, B. L. and Schumer, F., (1967). Families of the slums:
An exploration of their structure and treatment. New York: Basic Books. 16. Mirowsky, J., (1985). Depression and marital power. American Journal of Sociology 91: 557-592. 17. Moos, R. and Moos, B. S., (1981). Family Environment Scale: Manual. Palo Alto CA: Consulting Psychologists
Press. 18. Olson, D. H., McCubbin, H. I., Barnes, H., Larsen, A., Muxen, M. and Wilson, M., (1983). Families: What makes
them work. Beverly Hills CA: Sage Publications. 19. Olson, D. H., Sprenkle, D. H. and Russell, C. S., (1979). Circumplex Model of Marital and Family Systems: I.
Cohesion and adaptability dimensions, family types, and clinical applications. Family Process 18: 3-28. 20. Pittman, J. F. and Lloyd, S. A., (1988). Quality of family life, social support, and stress. Journal of Marriage and
the Family 50: 53-67. 21. Ransom, D. C., Fisher, L., Phillips, S., Kokes, R. F. and Weiss, R., (1990). The logic of measurement in family
research (pp. 48-66). In T.W. Draper & A.C. Marcus (eds.), Family variables: Conceptualization, measurement,and use. Newbury Park CA: Sage Publications.
22. Ransom, D. C., Fisher, L. and Terry, H. E., (1992). The California Family Health Project: II. Family world viewand adult health. Family Process 31: 251-267.
23. Verbrugge, L. M., (1985). Gender and health: An update on hypotheses and evidence. Journal of Health andSocial Behavior 26: 156-182.
_____________________________________________________________________________________________________________
15

Manuscript received September 10, 1990; Revisions submitted August 14, 1991; Accepted April 27, 1992.
1Items were included only if they met criteria in both samples: substantial loadings on the principal component, high correlationsbetween the item and the scale score total with that item excluded, and substantive contribution to "internal consistency." Acomplete list of items, loadings, etc. for these 13 scales is available upon request from the first author.
2The structure matrix is composed of correlations between each canonical variate and each contributing variable(within-domain). The "complementary" structure matrix contains correlations between each canonical variate and the variablesfrom the opposing variable group (cross-domain). The weight matrix reflects the relative contribution of each variable in theprediction of the respective canonical variates. Each matrix, then, presents a different perspective on the association of one set ofvariables with the other.
3χ2 = 50. 4 (p < .057; df = 36); reliability of solution = .91; and an absolute off-diagonal residual of .06.
_____________________________________________________________________________________________________________
16

_____________________________________________________________________________________________________________
17

_____________________________________________________________________________________________________________
18