the california agricultural worker health survey
DESCRIPTION
The California Agricultural Worker Health Survey. Conducted by the California Institute for Rural Studies Funded by The California Endowment. Investigators and Key Staff. David Lighthall, Executive Director Don Villarejo, Founder & Director Emeritus Bonnie Bade, Co-investigator - PowerPoint PPT PresentationTRANSCRIPT

The California Agricultural Worker Health Survey
Conducted by the California Institute for Rural StudiesFunded by The California
Endowment

Investigators and Key Staff
• David Lighthall, Executive Director• Don Villarejo, Founder & Director Emeritus• Bonnie Bade, Co-investigator• Steve McCurdy, Co-investigator• Richard Mines, Co-investigator• Steve Samuels, Project Statistician• Daniel William III, Project Coordinator• Ann Souter, Senior Site Coordinator

Random Selection of Subjects
• Communities – Five of six agricultural regions represented by randomly selected community sites.
• Dwellings – Enumeration of ALL places (dwellings) in each community where farmworkers are found to reside; then randomly select dwellings to contact.
• Residents – Enumeration of ALL eligible persons in randomly selected dwellings; then random selection of one or more residents to be subjects.

Qualifications of Subjects
• Age 18 years or older• Performed hired farm work in the
previous twelve months• No limit on duration of farm
employment• Livestock & crop work of any type• Exclude off-farm food processing

CAWHS Survey Components
• Main Survey Instrument, In Dwelling, 1 ½ to 2 hours, Interviewer
• Physical Examination, At Clinic, 20 to 30 minutes, Medical Staff, By Appointment, Transportation Provided
• Risk Behavior Instrument, At Clinic, 20 to 30 minutes, Interviewer, Private Room

CAWHS Main Instrument
• Household Composition• Personal Demographics• Health Services Utilization• Self-reported Health Conditions• Doctor-reported Health Conditions• Work History• Income and Living Conditions

CAWHS Main Instrument (continued)
• Workplace Health Conditions• Protective Equipment & Safety
Training• Working With Pesticides in the U.S.A.• Field Sanitation• Work Related Injuries and Injury
Module• Immigration Status

CAWHS Physical Examination
• Biometric• Dental• Skin• Body• Screening• Blood Chemistry• Medical History

Risk Behavior
• Health Habits (alcohol, tobacco)• Domestic Violence• Workplace Violence & Workplace
Risks• Sexual Behaviors• Drug Use• Mental & Psychological Illness• Reproductive Health (female only)




Summary Results, CAWHS, 1999
Dwellings enumerated 11,876
Dwellings contacted 2,989
Dwellings with eligible residents 1,174
Acceptances 968
Response rate 82.4%
Physical exams completed 652
Physical exam participation rate 67.4%
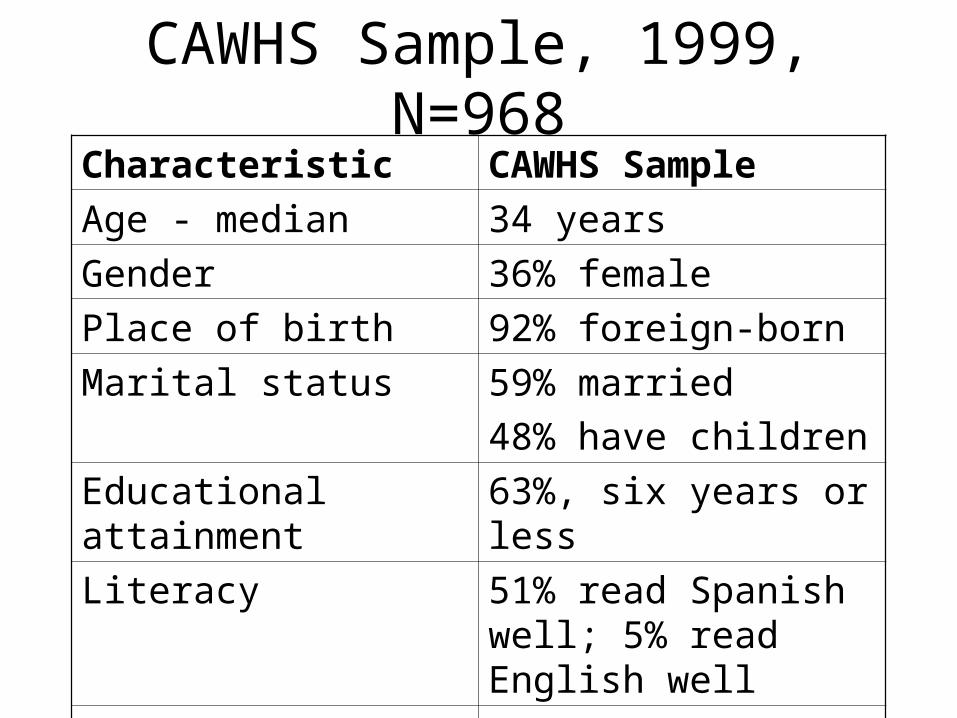
CAWHS Sample, 1999, N=968
Characteristic CAWHS Sample
Age - median 34 years
Gender 36% female
Place of birth 92% foreign-born
Marital status 59% married
48% have children
Educational attainment 63%, six years or less
Literacy 51% read Spanish well; 5% read English well
Income – median 1998 $7,500 - $9,999

What is your current immigration status?
0%
10%
20%
30%
40%
50%
60%
US Citizen PermanentResident
Other documented Undocumented Doesn't know /NA

Undocumented Status by Site
0%
10%
20%
30%
40%
50%
60%
Arbuckle Calistoga Cutler Firebaugh Gonzales Mecca Vista

Anemia, Male Subjects with Hemoglobin Concentration below Normal, CAWHS, 1999, N=392
0
0.01
0.02
0.03
0.04
0.05
0.06
0.07
0.08
0.09
20-49 50-69
Age Range
Per
cen
t o
f S
ub
ject
s
TCE CAWHS
CDC-1987

High Serum Cholesterol, by Immigration Status, CAWHS, 1999, N=528
0%
5%
10%
15%
20%
25%
Documented Undocumented
Immigration Status
Perc
ent H
igh
Seru
m
Chol
este
rol
Female
Male
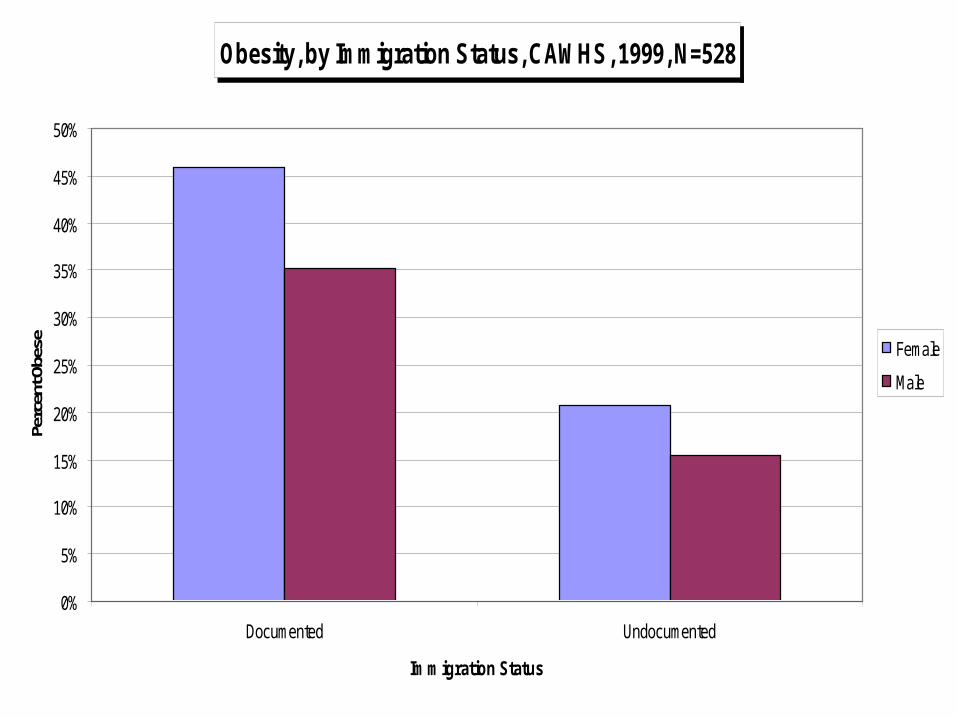
Obesity, by Immigration Status, CAWHS, 1999, N=528
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
Documented Undocumented
Immigration Status
Perc
ent O
bese Female
Male

Dental Outcomes, CAWHS, 1999, N=652
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
Decayed teeth Missing/brokenteeth
Gingivitis Other dentalproblems
Dental Outcome
Per
cen
t o
f S
ub
ject
s
Male
Female
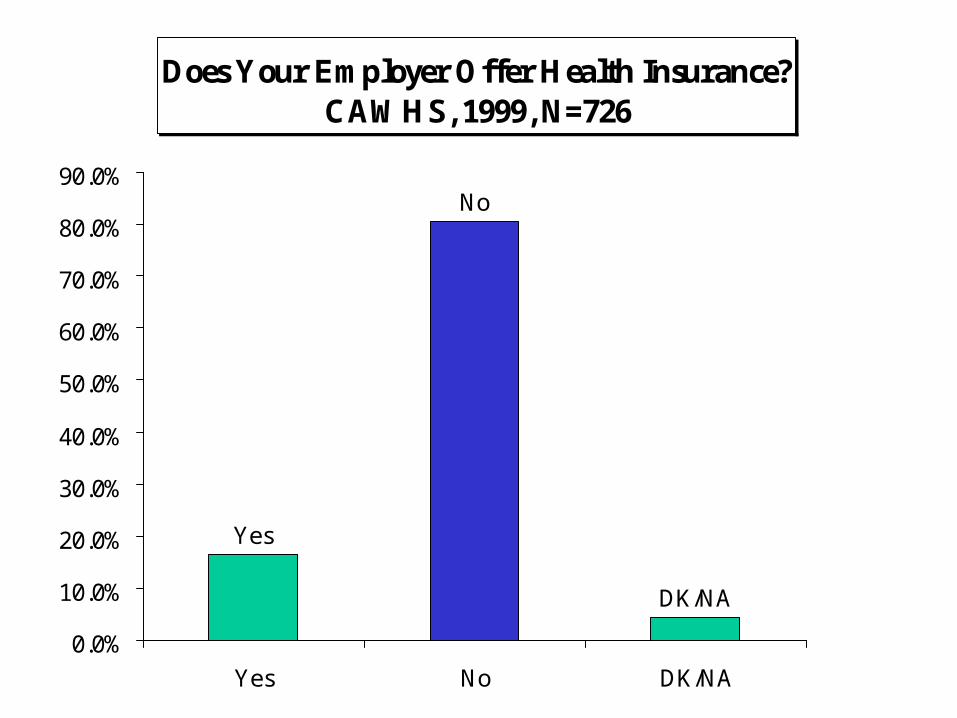
Does Your Employer Offer Health Insurance? CAWHS, 1999, N=726
Yes
No
DK/NA
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
Yes No DK/NA

Most Recent Visit to Doctor or Clinic, CAWHS, 1999, N=971
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
0-5 mo. 6-11 mo. 1-2 years 2-5 years 5+ years Never
Date of most recent visit
Per
cen
t o
f su
bje
cts
Male
Female

Most Recent Dental Care Visit, CAWHS, 1999, N=971
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
0-5 mo. 6-11 mo. 1-2 years 2-5 years 5+ years Never
Date of most recent visit
Per
cen
t o
f su
bje
cts
MaleFemale

Most Recent Eye Care Visit, CAWHS, 1999, N=971
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
0-5 mo. 6-11 mo. 1-2 years 2-5 years 5+ years Never
Date of most recent visit
Pe
rce
nt
of
su
bje
cts
Male
Female
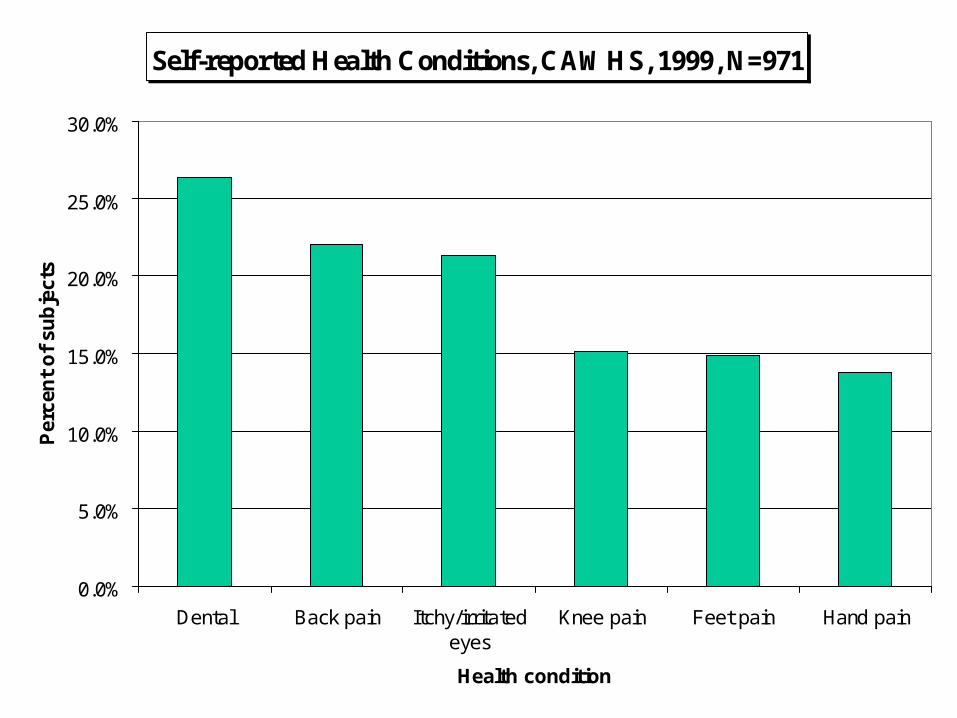
Self-reported Health Conditions, CAWHS, 1999, N=971
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
Dental Back pain Itchy/irritatedeyes
Knee pain Feet pain Hand pain
Health condition
Per
cen
t o
f su
bje
cts

Self-reported Workplace Health Conditions, CAWHS, 1999, N=968
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
Type of health condition
Per
cen
t o
f su
bje
cts

Employer Type
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%

Have you received pesticide safety training?, CAWHS, 1999
Yes
No
DK/NA
0%
10%
20%
30%
40%
50%
60%
Yes No DK/NA

Have you ever received pesticide safety training? (by study site)
0%20%40%60%80%
100%
Yes
No
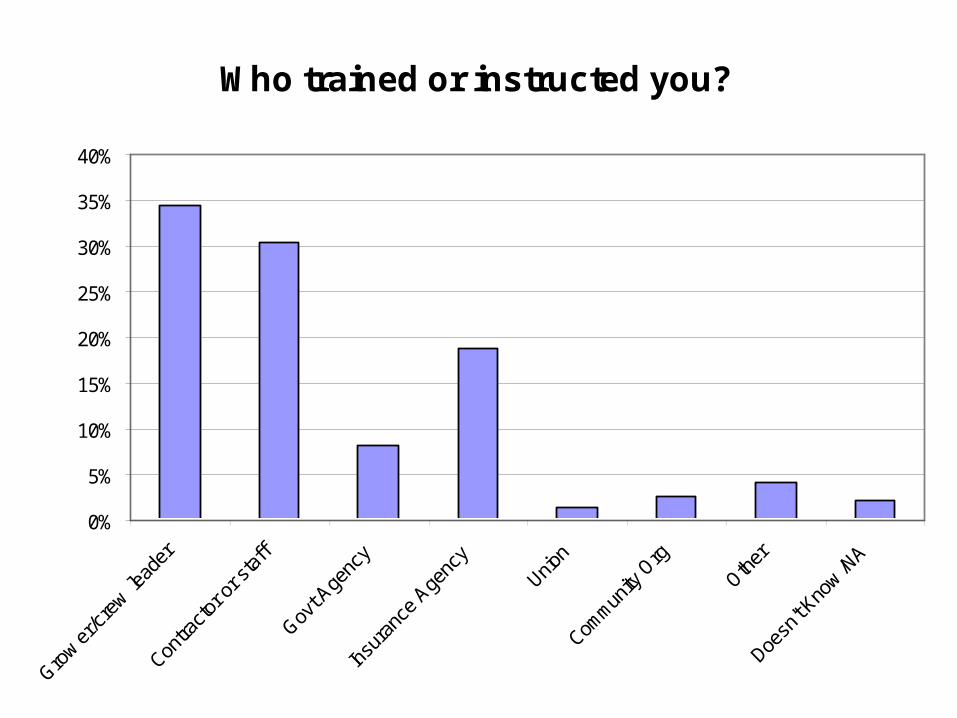
Who trained or instructed you?
0%
5%
10%
15%
20%
25%
30%
35%
40%

How was the training or instruction delivered?
0%
10%
20%
30%
40%
50%
60%

Contact with Pesticides (17.5% Total)
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
Sprayed or blow n Spilled While cleaning
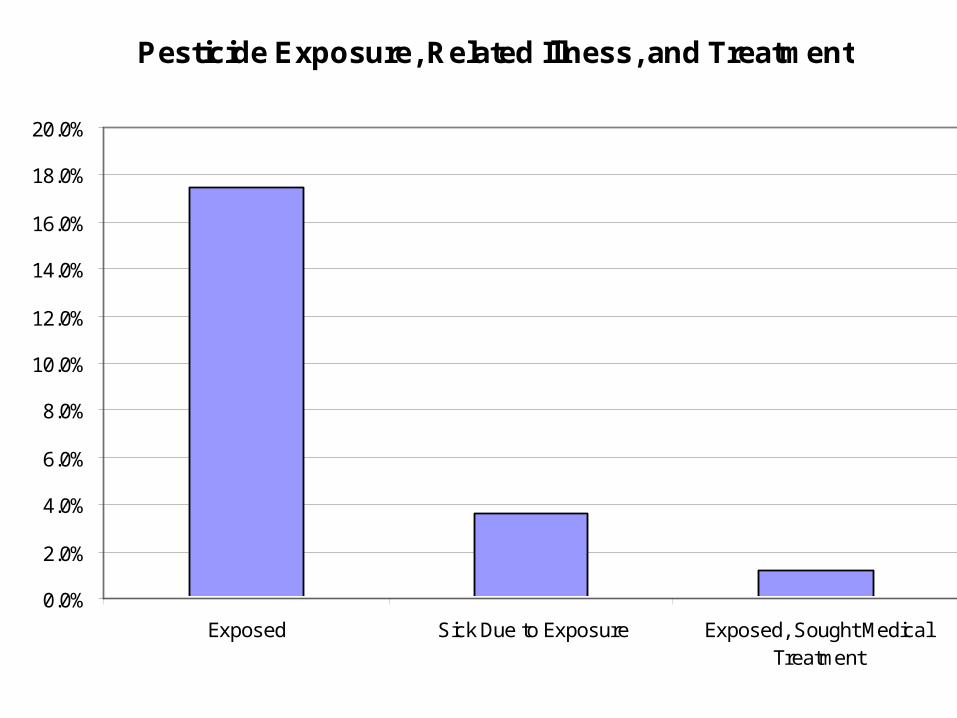
Pesticide Exposure, Related Illness, and Treatment
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
18.0%
20.0%
Exposed Sick Due to Exposure Exposed, Sought MedicalTreatment

Does Your Employer Provide These EVERYDAY? N=968
Clean drinking water and disposable cups
Yes - both 80%
Yes - water only 5%
No water, no cups 12%
Toilets Yes 88%
No 11%
Wash water Yes 82%
No 16%

Job Injury with Workers Compensation Payments-Ever, CAWHS, 1999, N=652
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
Yes No Don't know Not answered
Su
bje
cts
(p
erc
en
t)

Injured while working on a farm in past twelve months? California Hired Farmworker Health Needs Assessment, 1999
Yes5%
No93%
DK/NA2%

Employer Has Insurance to Pay You if You Are Injured on the Job and Can't Work, CAWHS, 1999,
N=706
YesNo
DK/NA
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
Yes No DK/NA

Conclusions: Occupational Safety and Health
1. High level of non-compliance with Worker Protection Standard pesticide training regulations.
2. For workers who are trained, the quality of WPS training is questionable: Multiple sources of training with a high proportion of workers receiving inadequate training.
3. Evidence that lateral, airborne pesticide drift is common, suggesting weak compliance with WPS pesticide application rules.
4. Overall, WPS appears relatively ineffective.5. High rates of musculoskeletal complaints:
66% reported chronic M-S pain in past year.6. Clear evidence of need for better eye
protection: 22% report chronic eye irritation.

Conclusions: Access to Care and Chronic Disease
1. Strikingly high proportions of workers who have rarely or never been to doctor, dentist, or optom.
2. Major problems of access to preventative and primary care: Dental, musculoskeletal (back, etc.), vision are perhaps the most serious.
3. Little affordable employer-provided health insurance, low levels of MediCal participation.
4. Cultural traditions of health care are being confronted by emergence of new chronic diseases tied to dietary changes in Mexico and the U.S.
5. Genetic predisposition (diabetes) and high rates of obesity increase long-term risk to heart disease, hypertension, stroke, and diabetes.
6. Looming long-term health costs for county and state health system if access to preventative and primary care is not dramatically improved.