the ahrq and lancet reports on dementia interventions …
TRANSCRIPT

National Institute on Aging (NIA) IMbedded Pragmatic Alzheimer’s Disease (AD) and
AD-Related Dementias (AD/ADRD) Clinical Trials (IMPACT) Collaboratory (NIA U54AG063546)
THE AHRQ AND LANCET REPORTS ON DEMENTIA INTERVENTIONS: INTERPRETATION AND IMPLICATIONS FOR
EMBEDDED PRAGMATIC TRIALS
Presented by: Eric B. Larson, MD, MPH (Lancet Report); Joseph E. Gaugler, PhD (AHRQ Report); & Lis Nielsen, PhD (NIA)
Housekeeping• All participants will be muted
• Enter all questions in the Zoom Q&A or chat box and send to All Panelists and Attendees
• Moderator will curate questions and ask them at the end
• Want to continue the discussion? Look for the associated podcast released about 2 weeks after Grand Rounds.
• Visit impactcollaboratory.org
• Follow us on Twitter: @IMPACTcollab1
• LinkedIn: https://www.linkedin.com/company/65346172 @IMPACT Collaboratory

Eric B. Larson, MD, MPHKaiser Permanente Washington Health Research Institute Senior InvestigatorFormer executive director of Kaiser Permanente Washington Health Research Institute and former vice president for research and health care innovation of Kaiser Permanente WashingtonCore Leader, IMPACT Health Care Systems CoreMember, IMPACT Steering Committee

The Lancet Commission Dementia Report 2020:Perspectives and opportunities to improve care and
evidence-base

Overall Lancet Summary • Well-being is the goal for much of dementia care.• Interventions should be individualized to whole person and
carers.• Evidence supports psychosocial interventions “tailored” to
neuropsychiatric symptoms.• Interventions for carers reduce depression and anxiety & may be
cost-effective.• Keeping people with dementia physically healthy affects
cognition.• Hospitalizations are distressing with poor outcomes and high
costs.

Lancet 2020 Approach
• Identify evidence for advances with likely greatest impact since 2017 report
• “Triangulation framework”—consistency of evidence from different research lines
• Summarize best evidence using quality systematic reviews, meta-analyses, or individual studies
• Perform systematic literature reviews and meta-analyses where needed
• “Present a synthesis of evidence …balance, strengths, and limitations”
Principles of Intervention in People with Dementia• “People with dementia have complex problems with symptoms in
many domains.”• “Must consider person as a whole,” their context and their close
carers.• “Dementia as an illness which affects cognition by definition affects
the ability to organize activities and people with dementia often need help to do what they enjoy.”
• “Wellbeing is one of the goals of dementia care.”
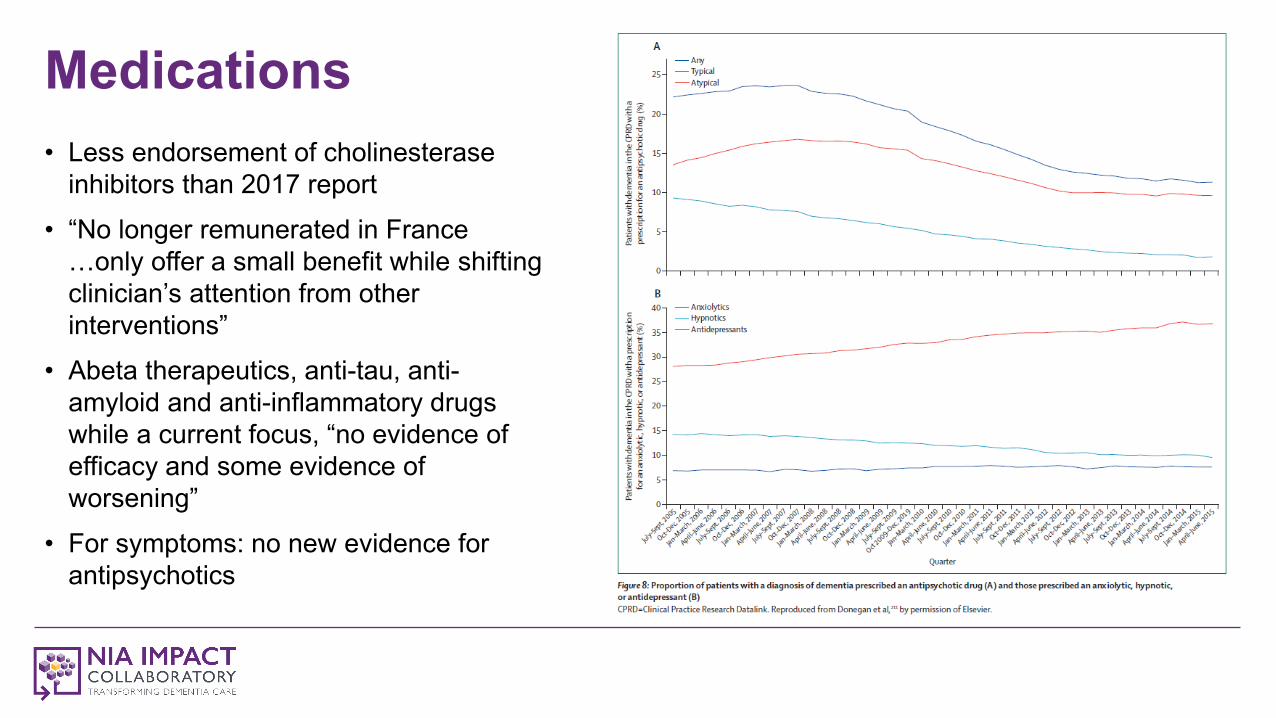
Medications• Less endorsement of cholinesterase
inhibitors than 2017 report• “No longer remunerated in France
…only offer a small benefit while shifting clinician’s attention from other interventions”
• Abeta therapeutics, anti-tau, anti-amyloid and anti-inflammatory drugs while a current focus, “no evidence of efficacy and some evidence of worsening”
• For symptoms: no new evidence for antipsychotics
Training, Exercise, and Physical Activity• Cognitive Training
• Meta-analysis found small statistically significant benefit on overall cognition driven by 2 trials of virtual reality or video games with high risk of bias.
• Cochrane review of 33 trials (2000 participants – high or uncertain risk of bias): Small to moderate effects on overall cognition lasting a few months to 1 year; “no evidence…that cognitive training was better than cognitive stimulation therapy.”
• Exercise and Physical Activity • Dementia and physical activity RCT: Improved fitness but didn’t slow decline.• Reducing Disability in Dementia Study (RDAD): Increased physical activity
days.

Interventions for Neuropsychiatric Symptoms of Dementia• “First line assessment and management of neuropsychiatric
symptoms should focus on basic health: Describe and diagnose symptoms, look for causes such as pain…illness, discomfort, hunger, loneliness, boredom, lack of intimacy and worry that could cause the behaviours and alleviate these while considering risks of harm.”
• “Evidence is slowly accumulating for the effectiveness, at least in the short term, of person centered, evidence based psychosocial interventions”

Examples: Interventions for Neuropsychiatric Symptoms of Dementia• German cluster 6-month RCT of nurse-delivered care
management using a computer assisted assessment to personalize intervention modules:
• Better outcomes vs. usual care on NPI scores**; greater than expected, but effects on quality of life apparent only in persons living with carer.
• An 8-session home-based tailored activity program RCT (to PLWD and family member)
• Reduction in overall neuropsychiatric symptoms, functional independence and pain; not sustained at 4 months.
Agitation – Evidence Growing • Distressing symptom for PLWD (contributes to costs)
• Two new cluster RCTs multi-component interdisciplinary interventions in “care homes” showed reduced agitation
• WHELD study: To improve communication with PLWD w/social sensory experiences or other activities; antipsychotic review and addressed physical problems; lower CMAI scores
• TIME study: Manual based assessment and structured case conferences for tailored plan. Reduced agitation at 8 weeks and 12 weeks
• Another 6-session RCT didn’t reduce agitation but was cost-effective, improving QOL
• Conclusion: Evidence favors multicomponent interventions in care homes. Major knowledge gap: People living at home. Effect sizes as good or better than antipsychotics and no side effects.
Apathy• A new area for me – the opposite of engagement; reduced initiative
and activity.• Conclusions: People engage more in preferred activities – but
require additional support to do so (e.g., pleasant events). • A study in care homes: Engagement does occur in people during
activities in those who attended.• Cochrane review of methylphenidate: Small improvement, low quality
evidence but not on NPI apathy scale.

Carers and Carer Distress• Carer distress associated with increased use and costs of health
services.• 6-year follow-up of 8 session STrAtegies for RelaTives intervention
(START): A manual-based coping intervention delivered by supervised psychology graduates found continuing effectiveness for depression, risk of “case-level depression”, and 3 times lower costs c/w those not receiving intervention.
• Caregiver depression rather than symptoms of PLWD associated with ED use for PLWD.

Functioning• U.K. RCT of 14 sessions of cognitive rehab focused on individual goal
attainment (home-based with OT/nurse) reported increased goal attainment at 3 & 9 months, but no improvement in QOL, mood, self efficacy, cognition, carer stress, health status; and was not cost-effective.
• Meta-analysis: “All interventions which had improved functioning in PLWD in the community have been individual rather than group interventions.”
• Physiotherapists for exercise (2 studies) • Individualized cognitive rehab (2 studies) • In home activities focused OT (3 studies): “Reduced functional decline compared
to controls
Depression and Sleep• Depression: Two new systematic reviews of antidepressants
reported moderate-quality evidence that antidepressant treatment for PLWD does not lead to better control of symptomatology.
• Sleep: No evidence that medication for sleep in dementia is effective and considerable evidence for harm (earlier death, increased hospitalization and falls)
• “Testing of non-pharmacological interventions is ongoing”

People with Dementia Have Other Illnesses• 70-80% of those diagnosed in primary care have at least 2 other chronic
illnesses; Multimorbidity is associated with faster functional decline, worse QOL for PLWD and their family carers
• Hospitalization is 1.4-4 times more common c/w similar illnesses; systematic review and meta-analysis (included 34 studies, 277432 people) showed “admissions often for conditions that might be manageable in the community”
• Early detection of physical illness (pain, falls, diabetes incontinence and sensory impairment) is important
• No intervention has successfully reduced number of hospital admissions of community dwelling PLWD (c/w interventions like education, exercise, rehab and telemedicine which have reduced admissions for PLW/OD)

Delirium and Dementia/Physical Illness and Frailty• Co-occurrence common, especially in those over 80 years • Delirium associated with dramatic increase in risk.• Most research on delirium prevention has been in people w/o dementia. • But Hospital Elder Life Program (HELP), a delirium-prevention program, reduced
incidence and includes those cognitively impaired.• No definitive evidence that any medication improves delirium. Cholinesterase
inhibitors, antipsychotics and sedating benzodiazepines are ineffective and the latter are associated with mortality and morbidity.
• MIGHT prevention and advances in delirium management “offer a means of dementia prevention”?
• Likewise, given the link of very old age, frailty, dementia, MIGHT therapy focusing on age-related process that underpin many diseases of late life reduce the incidence and severity of dementia?

“End of Life Care” (or Late-in-Life care) in Dementia• Trajectory is unpredictable; only a quarter of those dying with dementia have severe dementia. • One RCT testing decision aids re: care goals led to increased palliative care content in care plans.• Another prospective study (U.K.) showed high levels of agitation (54%) and pain (61% on
movement) in PLWD (advanced) in care homes.• Capacity to make abstract decisions, including about the future, might be lost early in dementia. • “Advance care planning designed to empower people with dementia and improve quality of dying
might theoretically be something everyone should do before developing dementia.” • Agreement of proxies with stated end-of-life treatment preferences of people with dementia is only
low to moderate. Advanced care plan might reduce uncertainty and “perceptions of quality of care.”

Some Key Takeaways from 2020 Lancet Report• Well-being is the goal of much dementia care:
• How well do we measure this or set this as our goal – in caring and in research?
• People with dementia have complex problems and symptoms in many domains.
• Interventions should be individualized, whole persons and include family carers.
• Evidence supports psychosocial interventions tailored to individual needs to manage neuropsychiatric symptoms.
• Evidence-based interventions for carers can reduce depressive and anxiety symptoms over years and are cost effective.
• Keeping people with dementia physically healthy is important for their cognition and well being.
• Avoiding hospitalizations is worthwhile as is prevention of delirium – a big opportunity for IMPACT and other pragmatic research programs. There is much opportunity for improvement, especially post-COVID
• Advance care planning including possibly establishing preferences before dementia impairs judgement and decision making should be promoted.

The AHRQ and Lancet Reports on Dementia Interventions: Interpretation and Implications for Embedded Pragmatic Trials
Joseph E. Gaugler, PhDRobert L. Kane Endowed Chair in Long-Term Care & AgingDirector, Center for Healthy Aging & InnovationUniversity of MinnesotaCo-Lead, Implementation Core, NIA IMPACT Collaboratory

Aims• Brief Overview: Butler M, Gaugler JE, Talley KMC, et al. Care
Interventions for People Living With Dementia and Their Caregivers. Comparative Effectiveness Review No. 231. (Prepared by the Minnesota Evidence-based Practice Center under Contract No. 290-2015-00008-I.) AHRQ Publication No. 20-EHC023. Rockville, MD: Agency for Healthcare Research and Quality; August 2020. Posted final reports are located on the Effective Health Care Program search page. DOI: https://doi.org/10.23970/AHRQEPCCER231.
• Disclaimer: My role• How do we advance dementia care science?

Disclaimer: This presentation is based on a report of research conducted by the Minnesota Evidence-based Practice Center (EPC). The findings and conclusions in this document are those of the authors who are responsible for its contents. Statements in the presentation should not be construed as an official position of AHRQ or of the U.S. Department of Health and Human Services. No author has any affiliation or financial conflict of interest.
Contract Support: By the Agency for Healthcare Research and Quality (AHRQ Contract Number HHSA290201500008I)
Investigators• Mary Butler, PhD, MBA• Joseph E. Gaugler, PhD• Kristine Talley, PhD, RN, GNP-BC• Priyanka Desai, PhD, MHP• Sue Duval, PhD• Mary Forte, DC, PhD
• Weiwen Ng, PhD Candidate• Edward Ratner, MD• Jayati Saha, PhD, MPH• Tetyana Shippee, PhD• Brittin Wagner, PhD• Lobsang Yeshi, MS

OVERVIEW OF AHRQ REPORT’S METHODS
AND FINDINGS

Objective“To understand the evidence base for care interventions for people living with dementia (PLWD) and their caregivers, and to assess the potential for broad dissemination and implementation of that evidence” (Butler et al., 2020, p. vii)

Data Sources“Ovid Medline, Ovid Embase, Ovid PsycINFO, CINAHL, and the Cochrane Central Register of Controlled Trials (CENTRAL) to identify randomized controlled trials, nonrandomized controlled trials, and quasi-experimental designs published and indexed in bibliographic databases through March 2020” (Butler et al., 2020, p. vii)

Methods (Butler et al., 2020, p. vii)• Non-pharmacological interventions targeting PLWD, their informal or
formal caregivers, or health systems were searched. • Rigorous AHRQ Evidence Practice Center standards were applied to
screen abstracts and extract study data • Eligible studies included randomized controlled trials and quasi-
experimental observational studies enrolling people with Alzheimer’s disease or related dementias or their informal or formal caregivers.
• Narrative summary of results for studies not judged to be NIH Stage Model 0 to 2 (pilot or small sample size studies) or to have high risk of bias.
Categorization• To support readiness for broad dissemination decisions, used NIH
Stage Model (Onken et al,. 2014) as a framework for categorizing studies to focus on those best designed to look for real-world effects.
• Modified PRECIS-2 (Loudon et al., 2015) tool to assist with assessment
• Stage 0-2 categorized as pilot• Stage 3 categorized as “explanatory”• Stage 4 categorized as “pragmatic”
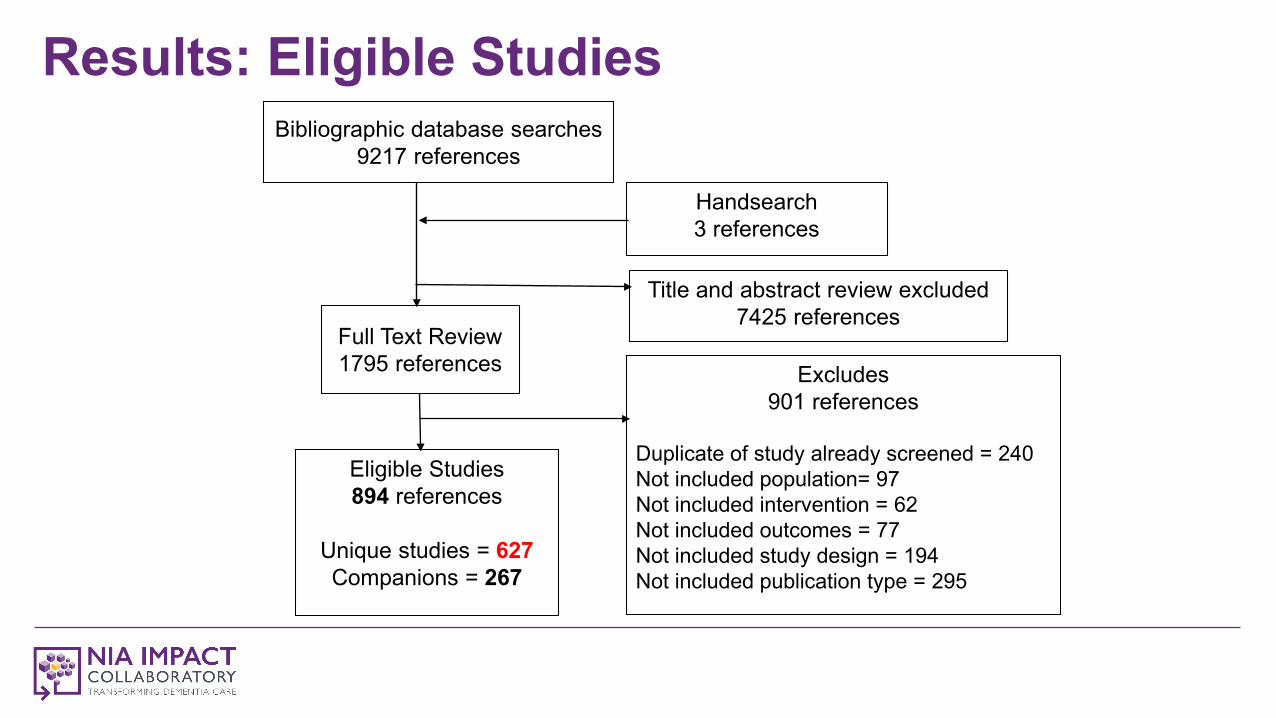
Results: Eligible Studies
Title and abstract review excluded7425 references
Eligible Studies894 references
Unique studies = 627Companions = 267
Full Text Review1795 references Excludes
901 references
Duplicate of study already screened = 240Not included population= 97Not included intervention = 62Not included outcomes = 77Not included study design = 194Not included publication type = 295
Handsearch3 references
Bibliographic database searches 9217 references
Results: Eligible Studies• 100 studies in the analytic set: the set of studies not judged to be
pilots or have a high potential for bias that might have interfered with the ability of the study to answer its research question.
• 527 studies in the evidence map: the set of studies that did not undergo synthesis. Summarizes what has been studied and facilitates identifying future research needs.
Results• Current available Stage III or IV evidence cannot yet provide clear
answers about which interventions (or interventions components) offer consistent benefits.
• Low-strength evidence for collaborative care models• Low-strength evidence for REACH II
• On-going research funded post-2015 with stronger rigor/reporting requirements may help resolve some questions

IMPLICATIONS FOR DEMENTIA CARE
SCIENCE

Compare and Contrast• Contrast: Question/Scope
• AHRQ question: “What is the evidence for interventions ready for broad dissemination?”
• Lancet Commission 2020 report: “identify the evidence for advances likely to have the greatest impact” since its 2017 report
• “What is ready” versus “what to do”• Contrast: Method
• AHRQ: Use of rigorous AHRQ review methods, NIH Stage Model, and qualitative synthesis due to study heterogeneity
• Lancet: Narrative review supplemented by some systematic search activities, used a “triangulation framework evaluating the consistency of evidence from different lines of research and used that as the basis to evaluate evidence”

Implications: Moving Forward (Gaugler, Jutkowitz, & Gitlin, 2020)• What is our philosophy?• Advancing implementation science
• NIH Stage Model as concept, process, and nomenclature• NIA IMPACT Collaboratory• a priori planning
• Engagement of persons living with dementia and their family caregivers• Aligning measures with treatment and personal goals
• INTERDEM• LINC-AD• Goal Attainment Scaling (e.g., Reuben & Jennings, 2019)
• Achieving greater understanding of intervention benefits and mechanisms• Reporting
• Categorization challenges• Taxonomy approaches

Implications for NIA-funded Research
Lis Nielsen, PhDDirector, Division of Behavioral and Social Research, National Institute on Aging

Behavioral and Social Research on Alzheimer’s Disease

Dementia Care Summits 2017 & 2020
• Identified opportunities for strengthening our fields• 2017 Summit informed AD/ADRD research milestones• 2020 Summit gaps and opportunities currently being finalized• https://www.nia.nih.gov/2020-dementia-care-summit

Impetus for the AHRQ/NASEM project• Research on care/caregiving in the Alzheimer’s and related
dementias field is expanding.• Some programs to improve care and caregiving have already been
disseminated.• A rigorous, independent review of which care/caregiving-related
interventions are effective and ready for widespread dissemination was needed.
Overall goals of the AHRQ/NASEM project
• Take stock of the current state of knowledge• Inform decision making about which care interventions for
individuals with dementia and their caregivers are ready for dissemination and implementation on a broad scale.

A Collaborative Effort
AHRQ-EPC: Systematic Evidence Review
National Academies Committee: Development of Recommendations
NIA: Next steps

Why engage two independent organizations?• AHRQ offers a highly-refined systematic evidence review process
that has been trusted by governmental organizations for its comprehensiveness and independence

Why engage two independent organizations?• AHRQ offers a highly-refined systematic evidence review process
that has been trusted by governmental organizations for its comprehensiveness and independence
• NASEM offers an external, independent committee that can consider: The EPC’s findings on our current state of knowledge; The EPC’s findings in a larger context (of ongoing research, etc.); and Whether dissemination & implementation is justifiable. How the existing evidence and other evidence considered in the review
may inform specific research priorities.

NASEM Committee’s Ongoing Work• Use the EPC findings as a guide to determine the balance for the
NASEM recommendations (“what to tell the public” and “research gaps” identified)
• Prioritize implementable guidance to the NIA re: actions needed in future award solicitations, peer review changes, etc.

Issues Identified by AHRQ Evidence Review• Why an intervention works • Intervention fidelity • Real-world implementation • Fitting complex interventions
into complex systems • Meaningful classification of
interventions
• Quality of life• Progressive nature of
dementia• Focus on dyadic populations• Interventions for diverse
populations• Consideration of broader
research context
What’s so hard about delivering interventions with fidelity? What can be done?
CHALLENGES• Specialized background may
be required• Training cannot be assumed
to work
SOLUTIONS• Determine essential
ingredients• Consider ease of
implementability at the outset
• Develop and test scalable training procedures
NIH Stage Model guides our planning and points to solutions.

2016 & 2017• Quality of care for in LTSS settings PLWD
at end of life (R03, R01)• Pragmatic trials for dementia care (R01,
R21/R33)• Socially assistive robots for PLWD and
caregivers (R41/R42, R43/R44)• Informal and formal caregiving reissue
(R21, R01)
2018 • Pragmatic trials for dementia care in LTSS settings (R61/R33)
• Assistive technology for PLWD and caregivers (R41/R42, R43/R44)
• Dementia care and caregiver support interventions (R01)
2015• Informal and formal
caregiving (R01, R21)
2019 & 2020• High-priority research topics: Dementia
care and caregiving• Special interest: Dementia care workforce• Interpersonal processes in AD clinical
interactions and care partnerships (R01)• Dementia care HCBS (R01, R21)• Preliminary testing of interventions
• Dementia care RoybalCenters (P30)
• AD/ADRD Collaboratory(U54)
• AD Demography and Aging Centers (P30)
• High-priority AD care network (R24)
2018 Centers & Networks

R21 or R61 Phase• Operationalize intervention, including
interventions addressing disparities • Evidence identifying mechanism of action • Determine feasibility • Validating training interventions for care
providers• Partner with healthcare providers and pilot test• Develop and test inexpensive methods and
deliver intervention R33 Phase• Adequately powered to test effectiveness
NIA initiatives to promote intervention development
• Adapt, modify, or refine the intervention to increase potency and scalability of the intervention
• Adequately powered to test efficacy • Mechanism of action • Fidelity of delivery in the community• Create and test training interventions for care
providers• Produce preliminary data for Stage IV
pragmatic trials
Dementia Care and Caregiver Support Interventions (R01)
RFA-AG-18-030 (Stage I-III)
Pragmatic Trials for Dementia Care in LTSS Settings
RFA-AG-17-065/064 and PAR-18-585 (Stage I/IV)

“Launchpad” for development and implementation of Stage IV Pragmatic Clinical Trialsembedded within healthcare systems
“Incubator” to conduct Stage 0 Through IV Clinical Trials to lay the groundwork for larger dementia care provider behavioral interventions.
NIA investments in dementia care and caregiving intervention development infrastructure


Multiple entry points
Training Research Resources
Early Stage Pilots
Later Stage Pilots
FOAs & NOSIs

Training opportunities• RCMAR scientists and pilot proposals• AD/ADRD institutional training programs• Diversity and re-entry supplements• Other NIA career or fellowship opportunities
Use research resources• AD/ADRD Demography and Economics of Aging Centers
• Center for Advancing Sociodemographic and Economic Study of Alzheimer’s Disease and Related Dementias (USC)
• Hopkins' Economics of Alzheimer's Disease and Services Center• Center to Accelerate Population Research in Alzheimer’s (Michigan)
• BSR-supported data infrastructure

Early stage intervention development pilots• Roybal Centers pilot opportunities• Example research ideas appropriate for this stage:
• Stage I and Stage III research on the development and testing of training materials to teach individuals in the community to deliver an efficacious intervention with fidelity
• Stage II or Stage III research to determine the governing principles/mechanisms of behavior change of an efficacious intervention
• Stage II or Stage III research to determine the essential ingredients/critical components of an efficacious intervention

Later stage pragmatic trials• IMPACT pilot opportunities• Example research ideas appropriate for this stage
• Stage IV research to test the effectiveness of interventions to improve patient, physician, or healthcare system performance that can be easily delivered with fidelity that have been shown to have some degree of evidence of efficacy, such as simple default interventions, simple nudge interventions, 100% technology-based interventions, de-prescribing interventions

Dementia care/caregiving-specific FOAs & NOSIs• Dementia care workforce (R01/R21) (NOT-AG-20-026)• Preliminary testing of interventions (Stage I, II, III) (NOT-OD-20-106)• Dementia care and caregiver high priority topics (NOT-AG-18-
056/057)• Late-stage clinical trials of non-pharmacological interventions (PAR-
18-878)• Interventions to mitigate cognitive decline in PLWD (PA-18-347)
Future Opportunities• NIA approved concepts provide hints of future
• Active NIA/BSR opportunities updated as new initiatives are published
• Subscribe to the NIA blog for real-time announcements

NIA supports research to generate evidenceThe NIA mission is to support and conduct research on aging, foster the development of scientists, and provide research resources. Including intervention research to elucidate what works, why, for whom, and under what circumstances
• Use-inspired basic research on the principles that account for an intervention’s effects• Implementation research tackling whether principle-based interventions can be
delivered with fidelity in real world contexts
It is the mission of other agencies and organizations to deliver services.

Summary • NIA regularly solicits input from the research community and public to
inform our programs in AD/ADRD science
• The Care Interventions for People With Dementia and their Caregivers AHRQ Evidence Review draft and final reports raised serious concerns
• Numerous NIA funding opportunities – many predating the AHRQ report –address similar issues confronting the field
• Existing infrastructure and opportunities offer multiple entry points for researchers at all levels, and new opportunities are always on the horizon

AHRQ and NASEM Key Dates & Links• Link to final AHRQ report (Summer 2020):
https://effectivehealthcare.ahrq.gov/products/care-interventions-pwd/report
• The NASEM committee is still deliberating its recommendations, and the Committee’s final public session was held in September
• Final NASEM report expected in early 2021
• Link to NASEM ACTIVITY:https://www.nationalacademies.org/our-work/care-interventions-for-individuals-with-dementia-and-their-caregivers---phase-two#sectionProjectScope

Q&A• Enter all questions in the Zoom Q&A or chat box and send to All Panelists and
Attendees• Moderator will curate questions • Want to continue the discussion? Look for the associated podcast released about 2
weeks after Grand Rounds.• Visit impactcollaboratory.org• Follow us on Twitter: @IMPACTcollab1• LinkedIn: https://www.linkedin.com/company/65346172 @IMPACT Collaboratory