the 2015 quality of death index - maison de soins ...€¦ · the 2015 quality of death index...
TRANSCRIPT

The 2015 Quality of Death Index Ranking palliative care across the world A report by The Economist Intelligence Unit
Commissioned by

1 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
Contents
Acknowledgements 2
Executive summary 6
About the 2015 Quality of Death Index 9 Anoteondefinitions 10
Introduction 11
Part 1: The 2015 Quality of Death Index—Overall scores 14 Casestudy:Mongolia—Apersonalmission 19 Casestudy:China—Growingawareness 20
Part 2: Palliative and healthcare environment 22 Casestudy:Spain—Theimpactofanationalstrategy 28 Casestudy:SouthAfrica—Raisingthepalliativecareprofile 29
Part 3: Human resources 30 Casestudy:Panama—Palliativecareisprimarycare 34
Part 4: Affordability of care 35 Casestudy:US—Fillinginthegaps 38 Casestudy:UK—Dyingoutofhospital 39
Part 5: Quality of care 40 TheWorldHealthAssemblyresolution 42 Children’spalliativecare 44
Part 6: Community engagement 45 Palliativecareandtherighttodie 48 Casestudy:Taiwan—Leadingtheway 49
Part 7: The 2015 Quality of Death Index—Demand vs supply 51
Conclusion 54
Appendix I: Quality of Death Index FAQ 56
Appendix II: Quality of Death Index Methodology 60
Endnotes 66

2 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
TheQualityofDeathIndexwasdevisedandconstructedbyanEconomistIntelligenceUnit(EIU)researchteamledbyTrishaSuresh.EbunAbarshi,TaniaPastrana,MarcoPellereyandMayecorSarcontributedtoresearchinbuildingtheIndex.SarahMurraywastheauthorofthisreportandDavidLinewastheeditor.MarcoPellereywrotethecountrysummaryappendices.LauraEdigerprovidedadditionalresearch,reportingandwriting.JosephWyattassistedwithproductionandGaddiTamwasresponsibleforlayout.
Forhertimeandadvicethroughoutthisproject,wewouldliketoextendourspecialthankstoCynthiaGoh,chair,AsiaPacificHospicePalliativeCareNetwork.
FortheirsupportandguidanceinconstructionoftheIndexwewouldalsoliketothankStephenConnor,seniorfellowattheWorldwideHospicePalliativeCareAlliance,LilianadeLima,executivedirectoroftheInternationalAssociationforHospiceandPalliativeCare,EmmanuelLuyirika,executivedirectoroftheAfricanPalliativeCareAssociation,andSheilaPayne,emeritusprofessorattheInternationalObservatoryonEndofLifeCareatLancasterUniversity.
Inaddition,duringresearchfortheconstructionoftheIndexandinwritingthisreport,theEIU
interviewedpalliativecareexpertsfromacrosstheworld.Theirtimeandinsightsaregreatlyappreciated.TheEIUtakessoleresponsibilityfortheconstructionoftheIndexandthefindingsofthisreport.
Interviewees, listed alphabetically by country:
GracielaJacob,director,ArgentinianNationalCancerInstitute,Argentina
RobertoWenk,director,ProgramaArgentinodeMedicinaPaliativa-FundaciónFEMEBA,Argentina
AmandaBresnan,executivemanager,policy,programsandresearch,Alzheimer’sAustralia,Australia
LizCallaghan,chiefexecutiveofficer,PalliativeCareAustralia,Australia
TimLuckett,member,ManagingAdvisoryCommittee,ImprovingPalliativeCarethroughClinicalTrials,UniversityofTechnologySydney,Australia
YvonneMcMaster,advocate,PushforPalliative,Australia
MargaretO’Connor,professorofnursing,SwinburneUniversity,Australia
LeenaPelttari,chiefexecutiveofficer,HospiceAustria,Austria
HerbertWatzke,head,president,AustrianSocietyforPalliativeCare,Austria
RumanaDowla,chairperson,BangladeshPalliative&SupportiveCareFoundation,Bangladesh
PaulVandenBerghe,director,FederationPalliativeCareofFlanders,Belgium
JohanMenten,president,ResearchTaskForce,FederationPalliativeCareofFlanders,Belgium
Acknowledgements

3 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
MariaGorettiMaciel,president,NationalAcademyofPalliativeCare,Brazil
IrenaJivkovaHadjiiska,member,BulgarianAssociationforPalliativeCare,Bulgaria
NikolayYordanov,head,PalliativeCareDepartment,InterregionalCancerHospital,Bulgaria
SharonBaxter,executivedirector,CanadianHospicePalliativeCareAssociation,Canada
AnnaTowers,associateprofessor,PalliativeCareDivision,McGillUniversity,Canada
MariaAlejandraPalma,chief,ContinuedandPalliativeCare,DepartmentInternMedicine,UniversityofChileClinicalHospital,UniversityofChile,Chile
MaríaMargaritaReyesD,executivedirector,ClínicaFamilia,Chile
CeciliaSepulveda,senioradviser,CancerControl,ChronicDiseasesPreventionandManagement,WorldHealthOrganization,Chile
ChengWenwu,director,DepartmentofPalliativeCare,FudanUniversityCancerHospital,Shanghai,China
LiWei,founder,SongtangHospice,Beijing,China
NingXiaohong,oncologist,PekingUnionMedicalCollegeHospital,China
ShiBaoxin,director,HospiceCareResearchCentre,TianjinMedicalUniversity,China
WangNaning,nurse,ChineseAssociationforLifeCare,China
JuanCarlosHernandez,president,PalliativeCareAssociationofColombia,Colombia
MartaLeón,chief,PainandPalliativeCareGroup,UniversidaddeLaSabana,Colombia
MaríaAuxiliadoraBrenesFernández,president,CajaCostarricensedeSeguroSocial,Costa Rica
MartinLoučka,director,CentreforPalliativeCare,Czech Republic
OndřejSláma,co-chair,LocalOrganisingCommittee,CzechSocietyforPalliativeMedicine,Czech Republic
Mai-BrittGuldin,postdoctoralresearcher,DepartmentofHealth,AarhusUniversity,Denmark
HelleTimm,director,KnowledgeCentreforRehabilitationandPalliativeCare,Denmark
ToveVejlgaard,consultant,SpecialistPalliativeCareTeam,Vejle,Denmark
GloriaCastillo,doctor,PalliativeCareUnit,SantoDomingo,Dominican Republic
XimenaPozo,coordinatorforpalliativecare,MinistryofPublicHealth,Ecuador
MohammadElShami,directorofpsychiatry,ChildrenCancerHospital57357,Egypt
YosephMamoAzmera,associatedirector,CareandTreatmentofHIV-Aids,UniversityofCaliforniaSanDiego-Ethiopia,Ethiopia
TiinaSurakka,presidentoftheboard,TheFinnishAssociationforPalliativeCare,Finland
EeroVuorinen,president,FinnishAssociationforPalliativeCare,Finland
RégisAubry,president,FrenchNationalObservatoryonEnd-of-LifeCare,France
AnnedelaTour,head,DepartmentofPalliativeCareandChronicPain,CentreHospitalierVDupouy,France
LukasRadbruch,director,DepartmentofPalliativeMedicine,UniversityofAachen,Germany
EdwinaAddo,director,ClinicalServices,OfficeofthePresident,InternationalPalliativeCareResourceCentre,Ghana
MawuliGyakobo,specialist,FamilyMedicineandPublicHealth,DodowaHealthResearchCentre,Ghana
EvaDuarte,director,PalliativeMedicineandSupportCareUnit,SanatorioNuestraSeñoradelPilar,Guatemala
LamWai-man,chairman,HongKongSocietyofPalliativeMedicine,Hong Kong
GáborBenyó,medicaldirector,TábithaHouse,Hungary
SushmaBhatnagar,headofanaesthesiology,painandpalliativeCare,AllIndiaInstituteofMedicalSciences’DrBRAmbedkarInstitute-RotaryCancerHospital,India
MohsenAsadi-Lari,director,OncopathologyResearchCentre,IranUniversityofMedicalSciences,Iran
MazinFaisalAl-Jadiry,doctor,OncologyUnit,ChildrenWelfareTeachingHospital,BaghdadUniversity,Iraq
NettaBentur,associateprofessor,StanleySteyerSchoolforHealthProfessionals,Tel-AvivUniversityandMyers-JDC-BrookdaleInstitute,Israel
AugustoCaraceni,director,VirgilioFlorianiHospiceandPalliativeCareUnit,NationalCancerInstituteofMilan,Italy
CarloPeruselli,president,ItalianSocietyofPalliativeCare,Italy
AdrianaTurriziani,director,HospiceVillaSperanza,Università’CattolicadelSacroCuore,Italy
NaokiIkegami,professoremeritus,KeioUniversity,Japan

4 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
MohammadBushnaq,chairman,JordanPalliativeCareSociety,Jordan
ZipporahAli,executivedirector,KenyaHospicesandPalliativeCareAssociation,Kenya
LucyFinch,co-founder,NdiMoyoHospice,Malawi
RichardLim,chairman,MalaysianHospiceCouncil,Malaysia
CelinaCastañeda,programmecoordinator,PalliativeCarefortheMexicanSocialSecurityInstitute,Mexico
OdontuyaDavaasuren,president,MongolianPalliativeCareSociety,Mongolia
MatiNejmi,coordinator,CenterofPainandPalliativeCare,HôpitalCheikhKhalifaBinZaid,Morocco
WimJ.A.vandenHeuvel,professor,UniversityMedicalCentre,UniversityofGroningen,Netherlands
BregjeOnwuteaka-Philipsen,programmeleader,QualityofCare,InstituteforHealthandCareResearch,Netherlands
KateGrundy,palliativemedicinephysician,ChristchurchHospital,New Zealand
OlaitanSoyannwo,president,SocietyfortheStudyofPain,Nigeria
RosaBuitrago,vicedeanandprofessor,SchoolofPharmacy,UniversityofPanama,Panama
GasparDaCosta,nationalcoordinator,NationalPalliativeCareProgrammeofPanama,Panama
MaryBerenguel,chief,DepartmentofPalliativeMedicineandPainManagement,Oncosalud-AUNA,Peru
MariaFidelisManalo,head,PalliativeCareUnit,CancerCenter,TheMedicalCity,Philippines
WojceechLeppert,chair,DepartmentofPalliativeMedicine,PoznanUniversityofMedicalSciences,Poland
JoséAntónioFerrazGonçalves,medicaldirector,palliativecareunit,PortugueseInstituteofOncology,Portugal
JennyOlivo,president,PuertoRicoHospiceandPalliativeCareAssociation,Puerto Rico
GeorgiyNovikov,chairman,RussianPalliativeCareAcademy,Russia
AlexanderTkachenko,founder,St.PetersburgPediatricPalliativeCareHospital,Russia
VanessaYung,chiefexecutive,SingaporeHospiceCouncil,Singapore
KristinaKrizanova,headdoctor,DepartmentofPalliativeMedicine,NationalOncologyInstitute,Slovakia
LizGwyther,chiefexecutiveofficer,HospiceandPalliativeCareAssociationofSouthAfrica,South Africa
JoanMarston,chiefexecutive,InternationalChildren’sPalliativeCareNetwork,South Africa
YoonjungChang,chief,Hospice&PalliativecareBranch,NationalCancerCenter,South Korea
MariaNabal,head,SupportivePalliativeCareTeam,HospitalUniversitarioArnaudeVilanova,Spain
JavierRocafortGil,formerpresident,SpanishAssociationforPalliativeCare,Spain
NishiraniLankaJayasuriya-Dissanayake,nationalprofessionalofficer,NoncommunicableDiseases,WorldHealthOrganization,Sri Lanka
AjanthaWickremasuriya,chairperson,ShanthaSevanaHospice,Sri Lanka
BertilAxelsson,DepartmentofRadiationSciences,UnitofClinicalResearchCentre,UmeåUniversity,Sweden
PeterStrang,consultant,professor,DepartmentofOncology-Pathology,KarolinskaInstitutet,Sweden
SteffenEychmüller,doctor,CenterofPalliativeCare,BernUniversityHospital,Switzerland
AndreasUllrich,seniormedicalofficer,CancerControl,DepartmentofChronicDiseasesandHealthPromotion,WorldHealthOrganization,Switzerland
Co-ShiChantalChao,professor,MedicalCollege,NationalChengKungUniversity,Taiwan
Ching-YuChen,professoremeritus,NationalTaiwanUniversityHospital,Taiwan
RongchiChen,chairman,LotusHospiceCareFoundation,Taiwan
SharleneCheng,founder,TaiwanResearchNetworkCouncil,TaiwanAcademyofHospicePalliativeMedicine,Taiwan
Sheau-FengHwang,chief,HospicePalliativeCareCenter,TaichungVeteransGeneralHospital,Taiwan
SiewTzuhTang,professor,ChangGungUniversitySchoolofNursing,TaiwanUniversityHospital,Taiwan
YingweiWang,director,HeartLotusHospiceatTzuchiGeneralHospital,Taiwan
EliasJohansenMuganyizi,executivedirector,TanzanianPalliativeCareAssociation,Tanzania
SriviengPairojkul,president,ThaiPalliativeCareSociety,Thailand
KadriyeKahveci,anaesthetist,DepartmentofPalliativeCareCenter,UlusStateHospital,Turkey

5 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
EllyKatabira,professorofmedicine,MakerereUniversityCollegeofHealthSciences,Uganda
SimonChapman,director,Policy,Intelligence&PublicAffairs,NationalCouncilforPalliativeCare,UK
RichardHarding,director,AfricanProgrammes,CicelySaundersInternational,UK
DavidPraill,formerchiefexecutive,HospiceUK,UK
KatherineSleeman,clinicallecturerinpalliativemedicine,King’sCollegeLondon,UK
MarkSteedman,manager,PhDProgramme,End-of-LifeCareForum,InstituteofGlobalHealthInnovation,ImperialCollegeLondon,UK
RosTaylor,nationaldirector,HospiceCareatHospiceUK,UK
ViktoriiaTymoshevska,director,PublicHealthProgramInitiative,InternationalRenaissanceFoundation,Ukraine
EduardoGarcíaYanneo,chairman,LatinAmericanAssociationforPalliativeCare,Uruguay
IraByock,executivedirectorandchiefmedicalofficer,InstituteforHumanCaring,ProvidenceHealth&Services,US
DavidCasarett,directorofhospiceandpalliativecare,UniversityofPennsylvaniaHealthSystem,US
BarbaraCoombsLee,president,Compassion&Choices,US
MarkLazenby,assistantprofessorofnursing,YaleSchoolofNursing,US
DianeMeier,director,CentretoAdvancePalliativeCare,US
JamesTulsky,chair,DepartmentofPsychosocialOncologyandPalliativeCare,Dana-FarberCancerInstitute,US
HollyYang,assistantdirector,InternationalPalliativeMedicineFellowshipProgram,InstituteofPalliativeMedicine,SanDiegoHospice,US
PatriciaBonilla,programmedirector,NationalCancerInstitute,Venezuela,Venezuela
QuachThanhKhanh,head,PalliativeCareDepartment,HoChiMinhCityOncologyHospital,Vietnam
NjekwaLumbwe,nationalcoordinator,PalliativeCareAllianceofZambia,Zambia
EuniceGaranganga,director,HospiceandPalliativeCareAssociation,Zimbabwe

6 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
Executive summary
Everyonehopesforagooddeath,orrather,“agoodlifetotheveryend”1,butuntilrecentlytherewaslittlededicatedeffortandinvestmenttoprovidetheresourcesandeducationthatwouldmakethatpossible.Publicengagementandpolicyinterventionstoimprovethequalityofdeaththroughtheprovisionofhigh-qualitypalliativecarehavegainedmomentuminrecentyears,andsomecountrieshavemadegreatstridesinimprovingaffordableaccesstopalliativecare.TheEconomistIntelligenceUnit’sQualityofDeathIndex,commissionedbytheLienFoundation,highlightsthoseadvancesaswellastheremainingchallengesandgapsinpolicyandinfrastructure.
ThisisthesecondeditionoftheIndex,updatingandexpandinguponthefirstiteration,whichwaspublishedin2010.Thenewandexpanded2015Indexevaluates80countriesusing20quantitativeandqualitativeindicatorsacrossfivecategories:thepalliativeandhealthcareenvironment,humanresources,theaffordabilityofcare,thequalityofcareandthelevelofcommunityengagement.TobuildtheIndextheEIUusedofficialdataandexistingresearchforeachcountry,andalsointerviewedpalliativecareexpertsfromaroundtheworld.
Inmanycountries,theproportionofolderpeopleinthepopulationisgrowingandnon-
communicablediseasessuchasheartdiseaseandcancerareontherise.Theneedforpalliativecareisalsothereforesettorisesignificantly.Insupplementaryanalysiswecompareexpectedgrowthinthe“demand”forpalliativecaretotheexisting“supply”foreachcountry(asshownintheirIndexrankings).Thedemandanalysisisbasedonforecastsoftheburdenofdisease,old-agedependencyratio,andrateofpopulationageingoverthenext15years.
Despitetheimprovementsthisresearchreveals,muchmoreremainstobedone.Eventop-rankednationscurrentlystruggletoprovideadequatepalliativecareservicesforeverycitizen.Culturalshiftsareneededaswell,fromamindsetthatprioritisescurativetreatmentstoonewhichvaluespalliativecareapproachesthatregarddyingasanormalprocess,andwhichseekstoenhancequalityoflifefordyingpatientsandtheirfamilies.
Keyfindingsofourresearchinclude:
l The UK has the best quality of death, and rich nations tend to rank highest.Asin2010theUKranksfirstinthe2015QualityofDeathIndex,thankstocomprehensivenationalpolicies,theextensiveintegrationofpalliativecareintoitsNationalHealthService,andastronghospicemovement.Italsoearnsthe

7 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
topscoreinqualityofcare.Ingeneral,incomelevelsareastrongindicatoroftheavailabilityandqualityofpalliativecare,withwealthycountriesclusteredatthetopoftheIndex.AustraliaandNewZealandcomesecondandthirdoverall,andfourothercomparativelyrichAsia-Pacificcountriesachieverankingsinthetop20:Taiwanatpositionsix,joinedbySingaporeat12,Japanat14,andSouthKoreaat18.Otherwise,Europeancountriesdominatethetop20,withtheadditionoftheUSandCanadaatpositions9and11,respectively.
l Countries with a high quality of death share several characteristics.Theleadingcountrieshavethefollowingelementsinplace:
• Astrongandeffectivelyimplementednationalpalliativecarepolicyframework;
• Highlevelsofpublicspendingonhealthcareservices;
• Extensivepalliativecaretrainingresourcesforgeneralandspecialisedmedicalworkers;
• Generoussubsidiestoreducethefinancialburdenofpalliativecareonpatients;
• Wideavailabilityofopioidanalgesics;
• Strongpublicawarenessofpalliativecare.
l Less wealthy countries can still improve standards of palliative care rapidly.Althoughmanydevelopingcountriesarestillunabletoprovidebasicpainmanagementduetolimitationsinstaffandbasicinfrastructure,somecountrieswithlowerincomelevelsprovetobeexceptions,demonstratingthepowerofinnovationandindividualinitiative.Forexample,Panamaisbuildingpalliativecareintoitsprimarycareservices,Mongoliahasseenrapidgrowthinhospicefacilitiesandteachingprogrammes,andUgandahasmadehugeadvancesintheavailabilityofopioids.
l National policies are vital for extending access to palliative care.Manyofthetopcountrieshavecomprehensivepolicy
frameworksthatintegratepalliativecareintotheirhealthcaresystems,whetherthroughanationalhealthinsuranceschemeliketheUKorTaiwan,orthroughcancercontrolprogrammessuchasinMongoliaandJapan.Effectivepoliciescancreatetangibleresults:thelaunchofSpain’snationalstrategy,forexample,ledtoa50%increaseinpalliativecareteamsandunifiedregionalapproaches.
l Training for all doctors and nurses is essential for meeting growing demand.Inhigh-rankingcountriessuchastheUKandGermanypalliativecareexpertiseisarequiredcomponentofbothgeneralandspecialisedmedicalqualifications,whileseveraltop-scoringcountrieshaveestablishednationalaccreditationsystems.Countrieswithoutsufficienttrainingresourcesexperienceasevereshortageofspecialists,whilegeneralmedicalstaffmayalsolackthetrainingtouseopioidanalgesicsappropriately.
l Subsidies for palliative care services are necessary to make treatment affordable. Whetherthroughnationalinsuranceorpensionschemesorthroughcharitablefunding(suchasintheUK),withoutfinancialsupportmanypatientsareunabletoaccessadequatecare.Thetopscorersintermsofaffordabilityofcare—Australia,Belgium,Denmark,Ireland,andtheUK—cover80to100%ofpatientcostsforpalliativecare.
l Quality of care depends on access to opioid analgesics and psychological support. Inonly33ofthe80countriesintheindexareopioidpainkillersfreelyavailableandaccessible.Inmanycountriesaccesstoopioidsisstillhamperedbyredtapeandlegalrestrictions,lackoftrainingandawareness,andsocialstigma.Thebestcarealsoincludesinter-disciplinaryteamsthatalsoprovidepsychologicalandspiritualsupportandphysicianswhoinvolvepatientsindecision-makingandaccommodatetheircarechoices.

8 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
l Community efforts are important for raising awareness and encouraging conversations about death.TheDyingMattersCoalitionsetupintheUKbytheNationalCouncilforPalliativeCare,aglobalmovementofinformalmeetingscalledDeathCafés,andtheUS-basedConversationProjectencouragepeopletoopenlydiscusstheirend-of-lifewishesandnormalisetheconversationaboutdying.Useoftelevision,newspapersandsocialmediabygovernmentandnon-profitgroupsinmanycountries—forinstanceBrazil,Greece,andTaiwan—hasalsohelpedtomakeheadwayinmainstreamingawarenessofpalliativecare.
l Palliative care needs investment but offers savings in healthcare costs.Shiftingfromstrictlycurativehealthinterventionstomoreholisticmanagementofpainandsymptomscanreducetheburdenonhealthcaresystemsandlimituseofcostlybutfutiletreatments.Recentresearchhasdemonstratedastatisticallysignificantlinkinuseofpalliativecareandtreatmentcostsavings,afactseveralhigh-rankingcountrieshaverecognisedintheirbidstoexpandpalliativecareservices.
l Demand for palliative care will grow rapidly in some countries that are ill-equipped to meet it.CountrieslikeChina,GreeceandHungarywithlimitedsupplyandrapidlyincreasingdemandwillneedactiveinvestmenttomeetpublicneeds.Moregenerally,
demographicshiftstoanolderpopulation,combinedwiththerisingincidenceofnon-communicablediseaseslikediabetes,dementiaandcancer,willcreateadditionalpressureforcountriesthatalreadystruggletomeetdemand.
TheEIU’s2010Indexsparkedaseriesofpolicydebatesovertheprovisionofpalliativecarearoundtheworld.Sincethen,severalcountrieshavemadesignificantadvancesintermsofnationalpolicy.Colombia,Denmark,Ecuador,Finland,Italy,Japan,Panama,Portugal,Russia,Singapore,Spain,SriLanka,SwedenandUruguayhaveallestablishedneworsignificantlyupdatedguidelines,lawsornationalprogrammes,andcountriessuchasBrazil,CostaRica,TanzaniaandThailandareintheprocessofdevelopingtheirownnationalframeworks.Themomentumbeinggainedonpalliativecareatapolicylevelhasalsobeenstrengthenedbytheinternationalresolutionatthe2014WorldHealthAssemblycallingfortheintegrationofpalliativecareintonationalhealthcaresystems.
Eachcountrywillneedtocraftitsownuniqueapproachbyidentifyingthemostsignificantgaps,addressingregulatoryandresourceconstraints,andformingpartnershipsbetweengovernment,academia,andnonprofitgroups.Approacheswillvarybycontextandculture,butsharetheoverallobjectiveofenablingabetterqualityoflifeforpatientsfacingdeath.

9 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
l Qualityofcare(30%weighting,6indicators)
l Communityengagement(10%weighting,2indicators)
Eachindicatorisallocatedaweightinginitscategory,andeachcategoryisgivenaweightingintheoverallIndex.Parts1to6ofthispaperconsiderinturntheoverallresultsandscoresforeachofthefivecategories.
Thisyear,theEIUalsopreparedasupplementaryassessmentoftheneedforpalliativecareprovision,toenableassessmentofthe“demand”forsuchcarealongsidethequalityof“supply”revealedinthemainIndex.Thisisbasedonthreecategories:
l Theburdenofdiseasesforwhichpalliativecareisnecessary(60%weighting)
l Theold-agedependencyratio(20%)
l Thespeedofageingofthepopulationfrom2015-2030(20%)
TheresultsofthisanalysisarediscussedinPart7.
AmoredetailedexplanationofthemethodologybehindtheIndexandthedemandscorecalculation,andalistoffrequentlyaskedquestionsabouttheconstruction,compositionandlimitationsoftheresearch,areincludedasappendicestothispaper.
In2010,theEIUdevelopedanIndexthatrankedtheavailability,affordabilityandqualityofend-of-lifecarein40countries.TheIndex,whichwascommissionedbytheLienFoundation,aSingaporeanphilanthropicorganisation,consistedof24indicatorsinfourcategories.Thestudygarneredmuchattentionandsparkedaseriesofpolicydebatesovertheprovisionofpalliativeandend-of-lifecarearoundtheworld.Asaresult,theLienFoundationcommissionedanewversionoftheIndextoexpanditsscopeandtakeintoaccountglobaldevelopmentsinpalliativecareinrecentyears.
Inthis,the2015version,thenumberofcountriesincludedhasbeenincreasedfrom40to80.TheIndex,whichfocusesonthequalityandavailabilityofpalliativecaretoadults,isalsostructureddifferentlyfromthe2010version(meaningthedirectcomparisonofscoresbetweenyearsisnotpossible).Now,theIndexiscomposedofscoresin20quantitativeandqualitativeindicatorsacrossfivecategories.Thecategoriesare:
l Palliativeandhealthcareenvironment(20%weighting,4indicators)
l Humanresources(20%weighting,5indicators)
l Affordabilityofcare(20%weighting,3indicators)
About the 2015 Quality of Death Index

10 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
TheQualityofDeathIndexmeasuresthequalityofpalliativecareavailabletoadultsin80countries.Althoughtheterms“palliativecare”and“endoflifecare”aresometimesusedinterchangeably,thelatterisoftentakentomeancaredeliveredonlyinthefinalstagesofaterminalillness.TheIndexisdesignedtomeasurepalliativecareasdefinedbytheWorldHealthOrganization:
“Palliativecareisanapproachthatimprovesthequalityoflifeofpatientsandtheirfamiliesfacingtheproblemsassociatedwithlife-threateningillness,throughthepreventionandreliefofsufferingbymeansofearlyidentificationandimpeccableassessmentandtreatmentofpainandotherproblems,physical,psychosocialandspiritual.Palliativecare:
• providesrelieffrompainandotherdistressingsymptoms;
• affirmslifeandregardsdyingasanormalprocess;
• intendsneithertohastenorpostponedeath;
• integratesthepsychologicalandspiritualaspectsofpatientcare;
• offersasupportsystemtohelppatientsliveasactivelyaspossibleuntildeath;
• offersasupportsystemtohelpthefamilycopeduringthepatientsillnessandintheirownbereavement;
• usesateamapproachtoaddresstheneedsofpatientsandtheirfamilies,includingbereavementcounselling,ifindicated;
• willenhancequalityoflife,andmayalsopositivelyinfluencethecourseofillness;
• isapplicableearlyinthecourseofillness,inconjunctionwithothertherapiesthatareintendedtoprolonglife,suchaschemotherapyorradiationtherapy,andincludesthoseinvestigationsneededtobetterunderstandandmanagedistressingclinicalcomplications.”2
A note on definitions

11 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
Introduction
Asgovernmentsacrosstheworldworktoimprovelifefortheircitizens,theymustalsoconsiderhowtohelpthemdiewell.Itisachallengenottobeunderestimated.Inmanycountries,olderpeoplemakeupanever-growingproportionofthepopulation.Meanwhile,theprevalenceofnon-communicablediseases,suchasheartdisease,diabetes,dementiaandcancer,isincreasingrapidly.Takentogether,thismeansthattheneedforpalliativecareissettorisesharply.
“We’veseenunprecedentedchangesinthewaytheworldpopulationismoving,withmorepeopleovertheageof65thanundertheageoffive,”saysStephenConnor,seniorfellowattheWorldwideHospicePalliativeCareAlliance(WHPCA).“That’sneverhappenedinhumanhistorybeforeandit’sgoingtocontinuetogetmorepronounced.”
Yetmanycountriesremainwoefullyill-equippedtoprovideappropriateservicestothesecitizens.Despiteimprovementsinrecentyearsandgreaterattentiontotheissue,just34countrieshaveabove-average3scoresinthe2015QualityofDeathIndex.Togethertheseaccountforjust15%ofthetotaladultpopulationofthecountriesintheIndex(whichthemselvesaccountfor85%oftheglobaladultpopulation)4,meaningthevastmajorityofadultslackaccesstogood
palliativecare.(Givenbetterpalliativecareisgenerallyavailableinrichercountrieswitholderpopulations,thisrisesto27%ofthepopulationaged65orover.TheIndexcovers91%oftheglobalpopulationofthoseagedover65.5)Separately,theWHPCAestimatesthatgloballyunder10%ofthosewhorequirepalliativecareactuallyreceiveit.6
EventhosecountriesthatdowellintheQualityofDeathIndexcannotmeetalltheneedsofthoserequiringpalliativecare,withevidenceofshortfallscontinuingtoemergeinnationsthat—inrelativeterms—havehighlysophisticatedservices.
TaketheUK,whichtopstheoverallIndex.InMay2015,aninvestigationbytheParliamentaryandHealthServiceOmbudsmanintocomplaintsaboutend-of-lifecarehighlighted12casesitsaidillustratedproblemsitsawregularlyinitscasework.7Failingsincludedpoorsymptomcontrol,poorcommunicationandplanning,notrespondingtotheneedsofthedying,inadequateout-of-hoursservicesanddelaysindiagnosisandreferralsfortreatment.
ThefactthattheUK,anacknowledgedleaderinpalliativecare,isstillnotprovidingadequateservicesforeverycitizenunderlinesthechallengefacingallcountries.Becausewhile
Thebiggestproblemthatpersistsisthatourhealthcaresystemsaredesignedtoprovideacutecarewhenwhatweneedischroniccare.That’sstillthecasealmosteverywhereintheworld.
Stephen Connor, senior fellow, Worldwide Hospice Palliative Care Alliance

12 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
greaternumbersofpeoplearelivinglonger,theyarenotnecessarilydoingsoingoodhealth.Oftentheymayhaveseveralillnesses,makingtheprocessofdyingmoredrawn-outanddemandingincreasinglycomplexformsoftreatment.
Thisplacesaheavyburdenonhealthcaresystems,mostofwhicharestrugglingtoadapt—andoneofthehardestshiftstomakeiscultural.“Thebiggestproblemthatpersistsisthatourhealthcaresystemsaredesignedtoprovideacutecarewhenwhatweneedischroniccare,”saysDrConnor.“That’sstillthecasealmosteverywhereintheworld.”
ThisisalsotrueintheUS,anothercountrythatperformswellintheIndex.“Ourhealthsystemsfocusondiagnosingandtreatingdiseasesandaredemonstrablynegligentinmeetingtheneedsofpatientsandfamiliesgoingthroughthesedifficultexperiences,”saysIraByock,executivedirectorandchiefmedicalofficeroftheInstituteforHumanCaringatProvidenceHealth&Servicesandauthorofthebook,The Best Care Possible.
Theironyisthatascountriesstruggletocopewithrisinghealthcarecosts,palliativecarecouldbeamorecost-effectivewayofmanagingtheneedsofanageingpopulation.Onerecentliteraturereviewfoundthatpalliativecarewasfrequentlyfoundtobecheaperthanalternativeformsofcareandthat,inmostcases,thecostdifferencewasstatisticallysignificant.8Anotherrecentstudyfoundthattheearlierpalliativecarewasadministeredtopatientswithanadvancedcancerdiagnosis,thegreaterthepotentialcostsavings.Ifpalliativecaretreatmentwasintroducedwithintwodaysofdiagnosisthisledtosavingsof24%comparedwithnointervention;itsintroductionwithinsixdayssaved14%.9
Yet,despiteevidenceofitseconomicbenefits,atinyproportionofhealthcareresearchgoesintoresearchonpalliativecare(about0.2%ofthefundsawardedforcancerresearchintheUKin2010,forexample,andjust1%oftheUSNationalCancerInstitute’stotal2010appropriation10).
“Akeyfactorlimitingresearchisthatit’sreallypoorlyfunded,”saysKatherineSleeman,clinicallecturerinpalliativemedicineatKing’sCollegeLondon.“Thisissomethingthatarguablywillaffecteverysinglepersonandyetweinvestalmostnothingintryingtoworkouthowtodoitbetter.”
Moreworrying,manydevelopingcountriesareunabletoofferbasicpainmanagement,leavingmillionsofpeopledyinganagonisingdeath.
Nevertheless,evidenceofinnovationiscomingfromunexpectedquarters.MongoliaandPanama(inpositions28and31respectivelyintheIndex),areshowingthatevenlesswealthycountriescanincreasetheavailabilityandqualityofcare,relativelyquickly.
Andwhenitcomestotheavailabilityofmorphine,Ugandahasmadestrikingadvancesinpaincontrolthroughapublic-privatepartnershipbetweenthehealthministryandHospiceAfricaUganda,apioneeringinstitutionfoundedbyAnneMerriman—anomineeforthe2014NobelPeacePrize.“Thegovernmentnowsupportstheavailabilityoforalmorphinetoanyonewhoneedsitforfree,”explainsEmmanuelLuyirika,executivedirectoroftheAfricanPalliativeCareAssociation.
Somedevelopingcountriescanmoveforwardrelativelyrapidlybecauseoftheabsenceofentrenchedsystems,saysMarkSteedman,PhDprogrammemanagerfortheEnd-of-LifeCareForumatImperialCollegeLondon’sInstituteofGlobalHealthInnovation.“Wethinkthereareplaceswherethere’salotofpotential,”hesays.“Whenyou’restartingfromzeroyoucanleapfrogalotoftheproblems.”
RichardHarding,whodevelopedtheAfricanprogrammeforCicelySaundersInternational(anNGOfocusedonresearchonandeducationaboutpalliativecare)atKing’sCollegeLondon,seesthisprincipleatworkinAfrica.“Africancountrieshavesucceededindeliveringhighqualityeffectivepalliativecareinthefaceoflow
Thisissomethingthatarguablywillaffecteverysinglepersonandyetweinvestalmostnothingintryingtoworkouthowtodoitbetter.
Katherine Sleeman, clinical lecturer in palliative medicine, King’s College London

13 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
resourcesandoverwhelmingneed,”hesays.“Andhigh-andmiddle-incomecountrieswouldbewisetolearnlessonsfromthem.”
Whenlookingmorebroadly,SheilaPayne,emeritusprofessorattheInternationalObservatoryonEndofLifeCareatLancasterUniversity,seesprogressbeingmade.“There’sageneraltrendinwhichwe’removingfromthepioneerstageinmanycountriestopeopleseeinghowtheycanembedpalliativecareinhealthcaresystems,”shesays.“That’sreallyimportantbecausethat’saboutsustainability.”
Inamajorstepforward,theWorldHealthAssembly—WHA,theforumthroughwhichtheWorldHealthOrganizationisgoverned—lastyearpublishedaresolutiononpalliativecarecallingonmemberstatestointegrateitintonationalhealthcaresystems(seetheboxinPart5).“Thatsetsthepolicycontextandlegitimisesgovernmentsgettingengaged,”saysDrPayne.“Inthepolicycontext,that’sabigdevelopment.”
Inaddition,initsglobalactionplanforthepreventionandcontrolofnon-communicablediseasesfor2013–2020,theWHOhasincludedpalliativecareamongthepolicyareasproposedtomemberstates.TheWHOisalsoshiftingitsfocustoplacemoreattentiononnon-communicablediseases.
ThequestionthatliesaheadishowquicklyandeffectivelymemberstatescanputinplacemeasuresthatcanmeettherecommendationsoftheWHAresolutionandincreaseaccesstoopioidsandpalliativecare.Andwhiledevelopingcountriesneedtoscaleuppromisingpioneerprogrammes,countriesthatalreadyhavesophisticatedpalliativecareprovisionneedtofindwaystomeetthegrowingdemandsofarapidlyageingpopulation.
However,somearguethat,evenwithoutlargeinvestments,significantimprovementscanbemadeinpalliativecare.“Thethingsthatmakeabetterdeatharesosimple,”saysRosTaylor,nationaldirectorforhospicecareatHospiceUK.“It’sbasicknowledgeaboutgoodpaincontrolandconversationswithpeopleaboutthethingsthatmatter—thatcouldtransformmanymoredeaths.”
Forpolicymakers,majorissuestoconsiderareavailabilityofcare,humanresourcesandtraining,affordabilityofcare,qualityofcareandcommunityengagementthroughpublicawarenesscampaignsandsupportvolunteers.Theseissuesarecoveredbythefivecategoriesinthe2015QualityofDeathIndex.Ineach,theIndexlooksathowcountriesmeasureupagainstothernations,aswellasagainsttheirregionalpeersandthosewithsimilarincomelevels.

14 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
The 2015 Quality of Death Index—overall scores1
Inassessingtheresultsofthe2015QualityofDeathIndex,itisnosurprisetofindthatwealthycountriesdominatethetopofthelist,whiletheirpoorercounterpartsareclusteredtogetherinitslowersections.Infact,incomelevelsareastrongindicatoroftheavailabilityandqualityofpalliativecare.However,thereareexceptionstothisrule,ofteninplaceswhereanindividualischampioningthecauseorwherecertaincircumstances—thespreadofHIV-Aids
insomeAfrican,countries,forexample—havebeencatalystsforinnovationandinvestment.
Aswasthecasein2010,theUKtopstheIndex,followedbyAustraliaandNewZealand(whichtooksecondandthirdin2010).TheUK’sleadingpositionreflectstheattentionpaidtopalliativecareinbothpublicandnon-profitsectors.Withastronghospicemovement—muchofitsupportedbycharitablefunding—palliative
2015 Quality of Death Index—Overall scores
Figure 1.1
0 20 40 60 80 100

15 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
2015 Quality of Death Index—Overall scores
Figure 1.2
Rank Country
IraqBangladeshPhilippines
NigeriaMyanmar
Dominican RepublicGuatemala
IranBotswana
ChinaEthiopiaUkraine
ColombiaIndia
MalawiSri LankaRomania
KenyaBulgaria
ZambiaSaudi Arabia
ZimbabweVietnam
GreeceEgypt
SlovakiaTanzania
IndonesiaMorocco
GhanaKazakhstan
PeruRussiaTurkey
Puerto RicoVenezuela
ThailandMexico
BrazilHungaryEcuadorUruguayMalaysia
JordanCuba
UgandaSouth Africa
Czech RepublicArgentina
PanamaLithuania
Costa RicaMongolia
ChilePoland
IsraelPortugal
SpainHong Kong
ItalyFinland
DenmarkSouth Korea
AustriaSweden
SwitzerlandJapan
NorwaySingapore
CanadaFrance
USNetherlands
GermanyTaiwan
BelgiumIreland
New ZealandAustralia
UK
12.514.115.316.917.117.2
20.921.222.823.325.125.526.726.827.027.128.330.030.130.330.831.331.932.932.933.233.433.633.834.334.836.037.238.240.040.140.242.342.542.744.046.146.546.746.847.848.551.852.553.654.057.357.758.658.759.860.863.466.6
71.173.373.573.774.875.476.176.377.477.677.879.480.880.982.083.184.585.887.6
91.693.9
8079787776757473727170696867666564636261605958
=56=56
55545352515049484746454443424140393837363534333231302928272625242322212019181716151413121110
987654321
andend-oflifecarearebothpartofanationalstrategythatisleadingtomoreservicesbeingprovidedinNationalHealthServicehospitals,asthecountryworkstointegratehospicecaremoredeeplyintothehealthcaresystem.11 “Peoplehavewokenuptothefactthatwemaybeabletosavemoneyoverallforsocietybyinvestingindyingbetter,”saysDrSleeman.
WhileAustraliaandNewZealandareinthetopthree,fourotherAsia-Pacificcountriesmakeitintothetop20,withTaiwanatpositionsix,Singaporeatposition12,Japanatposition14andSouthKoreaatposition18.Forthesecountries,governmentengagementhasbeencrucial.Amongotherfactors,Taiwanbenefitsfromthecountry’sNationalHealthInsurance,whichdeterminesinsurancecoverageandthelevelofreimbursementforspecificservices.12 Japan(whichperformedrelativelypoorlyinthe2010Index,atposition23of40)isinstitutinganewcancercontrolprogramme,whichisexpectedtopromptanincreasedfocusonpalliativecarefromtheearlystagesofthediseasealongwiththeincorporationofpalliativecarecentresintothenationalbudget.13
AndinSingapore,whichisgrapplingwitharapidlyageingpopulation,caringforpeopletowardstheendoftheirliveshasrisenuptheagendaforhealthcarepolicymakers.SingaporerecentlydevelopedanationalpalliativecarestrategyandtheMinistryofHealthisworkingbothtoincreasethenumberofservicesavailableandtoempowerindividualstomaketheirowndecisionsonend-of-lifecare.14
However,whiletheEuropean,Asia-PacificandNorthAmericancountriesinthetopoftheIndexbenefitfromrelativelyhighlevelsofgovernmentsupport,severallesswealthycountrieswithlesswelldevelopedhealthcaresystemsstandout.TheseincludeChile,Mongolia,CostaRicaandLithuania,whichappearinthetop30,atpositions27,28,29and30respectively.

16 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
2015 Quality of Death Index—Ranking by region
Figure 1.3
Country
IraqNigeria
IranBotswana
EthiopiaMalawiKenya
ZambiaSaudi Arabia
ZimbabweEgypt
TanzaniaMorocco
GhanaJordan
UgandaSouth Africa
IsraelUkraine
RomaniaBulgaria
GreeceSlovakia
KazakhstanRussiaTurkey
HungaryCzech Republic
LithuaniaPoland
PortugalSpainItaly
FinlandDenmark
AustriaSweden
SwitzerlandNorwayFrance
NetherlandsGermanyBelgiumIreland
UKBangladeshPhilippines
MyanmarChinaIndia
Sri LankaVietnam
IndonesiaThailandMalaysia
MongoliaHong Kong
South KoreaJapan
SingaporeTaiwan
New ZealandAustralia
Dominican RepublicGuatemala
ColombiaPeru
Puerto RicoVenezuela
MexicoBrazil
EcuadorUruguay
CubaArgentina
PanamaCosta Rica
ChileCanada
US
12.516.9
21.222.825.127.030.030.330.831.332.933.433.834.3
46.747.848.5
59.825.528.330.132.933.234.837.238.2
42.751.854.0
58.760.863.4
71.173.373.574.875.476.177.479.480.982.084.585.8
93.914.115.317.1
23.326.827.1
31.933.6
40.246.5
57.766.6
73.776.377.6
83.187.6
91.617.2
20.926.7
36.040.040.142.342.544.046.146.8
52.553.6
57.358.6
77.880.8
Amer
icas
Asia
-Pac
ific
Euro
peM
iddl
e Ea
st &
Afr
ica
Mongoliaisanimpressivecase.ThedrivingforcebehindtheincreaseinpalliativecareinthecountryisOdontuyaDavaasuren,adoctorwhoishelpingtobuildanationalpalliativecareprogramme,pushingtochangeprescriptionregulationstomakegenericopioidsavailable,trainingpalliativecarespecialists,andworkingtoincludeeducationonpalliativecareinthecurriculafordoctors,nursesandsocialworkers.“She’sabrilliantteacher,leaderandvisionary,”saystheWHPCA’sDrConnor.“Andleadershipiscriticaltoanychangeprocessinanywhereintheworld.”
Bycontrast,somecountriesthatmightbeexpectedtoperformmorestrongly,giventheirrapidrecenteconomicgrowth,rankatlowpositionsintheIndex.IndiaandChinaperformpoorlyoverall,atpositions67and71intheIndex.Inthelightofthesizeoftheirpopulations,thisisworrying.
InChina’scase,arapidlyageingdemographicpresentsadditionalchallenges.TheadoptionofpalliativecareinChinahasbeenslow,withacurativeapproachdominatinghealthcarestrategies.Thismaybeabouttochange,asrecentshiftsinpolicy,mainlyatthemunicipallevel,indicategreatergovernmentsupportandinvestmentinhospiceandpalliativecareservices.
RegionalvariationsarepresentintheIndex,andtherearesurpriseshere,too.IntheAmericas,theUSandCanadatopthelist,asmightbeexpected.ButChileisinthirdplace,makingitaleaderinLatinAmerica—withthehighestnumberofpalliativecareservicesintheregion.15Chile’spositionintheIndexreflectstheeffortsmadetoincorporatepalliativecareintohealthcareservicesandtodeveloppoliciesforaccesstoopioidssincethecountrylauncheditspalliativecareprogrammein1996.16,17

17 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
Correlation with per-capita GDP(2013, US$, ppp)
Figure 1.4
Quality of Death overall score (100=best)
Income per capita (US$, PPP, 2013)
R2 = 0.652
0
20
40
60
80
100
0 10000 20000 30000 40000 50000 60000 70000 80000 90000
Singapore
US
NorwaySwitzerland
Hong Kong
Saudi Arabia
UKAustralia
IrelandNew Zealand Belgium
Taiwan
France
Germany
NetherlandsCanadaJapanSouth Korea
Italy
Sweden
AustriaDenmark
Finland
SpainIsrael
PortugalPolandChile
LithuaniaCzech Republic
Puerto Rico
Mongolia
Costa Rica
South Africa
Jordan
Ecuador
PeruEgypt Bulgaria
Romania
IranBotswana
China
ColombiaSri Lanka
UkraineEthiopiaMalawi India
ZimbabweTanzania
Ghana
Vietnam
Indonesia
Bangladesh
PhilippinesMyanmar
NigeriaGuatemala
Iraq
Dominican Republic
Cuba
UgandaPanamaArgentina
Malaysia
HungaryMexicoVenezuela
Turkey
ThailandBrazil
RussiaKazakhstan
Greece
Slovakia
UruguayMorocco
Zambia
Kenya
Incomelevelscorrelatequitestronglywithrelativesuccessindeliveringpalliativecareservices(asFigure1.4demonstrates).Thetop10countriesintheIndexareallhigh-incomecountries,althoughwithinthehighincomegroup,somecountriesexperiencingeconomicdifficulties—suchasGreece(equal56thplace)andRussia(48th)—canbefoundamongthepoorerperformingnations(Figure1.5).
Withinregionsasimilarprincipleapplies.Israel(ahighincomecountry)andSouthAfrica(amiddle-incomecountry)earnthefirstandsecondhighestscoresamongthe18MiddleEasternandAfricancountries.Meanwhile,fourofthelastfivecountriesintheIndex—Myanmar,Nigeria,thePhilippinesandBangladesh—arelow-income
countries.However,somecountriesdonotperformaswellasonemightexpect,giventheirwealth.ThisisthecaseforSingapore,forexample,whichdoesnotmakeitintothetop10,andHongKong,whichisonlyatposition22intheIndex.
InthecaseofSingapore,thegovernmentisworkingtocatchupfollowingyearswhenitinvestedrelativelylittleinpalliativecare.“Singaporehasoneofthefastestageingpopulationsintheworldbutuntilabout25yearsago,wehadayoungpopulation,”saysCynthiaGoh,chairoftheAsiaPacificHospicePalliativeCareNetwork.“Sowebuiltupaprettygoodacutecaresystem,butwhenitcomestochronicdiseasesandendoflife,thereisalotofcatchinguptodo.”

18 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
2015 Quality of Death Index—Ranking by income group
Figure 1.5
Country
BangladeshPhilippines
NigeriaMyanmar
GuatemalaEthiopiaUkraine
IndiaMalawi
Sri LankaKenya
ZambiaZimbabwe
VietnamEgypt
TanzaniaIndonesia
MoroccoGhana
UgandaMongolia
IraqDominican Republic
IranBotswana
ChinaColombiaRomaniaBulgaria
KazakhstanPeru
TurkeyVenezuela
ThailandMexico
BrazilHungaryEcuador
MalaysiaJordan
CubaSouth Africa
ArgentinaPanama
Costa RicaSaudi Arabia
GreeceSlovakia
RussiaPuerto Rico
UruguayCzech Republic
LithuaniaChile
PolandIsrael
PortugalSpain
Hong KongItaly
FinlandDenmark
South KoreaAustriaSweden
SwitzerlandJapan
NorwaySingapore
CanadaFrance
USNetherlands
GermanyTaiwan
BelgiumIreland
New ZealandAustralia
UK
14.115.316.917.1
20.925.125.526.827.027.130.030.331.331.932.933.433.633.834.3
47.857.7
12.517.2
21.222.823.3
26.728.330.1
34.836.038.240.140.242.342.542.744.046.546.746.848.5
52.553.6
57.330.832.933.2
37.240.0
46.151.854.0
58.658.759.860.863.466.6
71.173.373.573.774.875.476.176.377.477.677.879.480.880.982.083.184.585.887.6
91.693.9
Hig
h in
com
eM
iddl
e in
com
eLo
w in
com
e
Note: Low income countries are those that had 2013 GNI per capita of less than US$4,125; middle income countries more than US$4,125 but less than US$12,746; and high income countries more than US$12,746.
ThediscrepanciesthatemergebetweenincomeandIndexperformanceandthepresenceofoutlierssuchasMongoliaareinthemselvesenlightening.Theyservetodemonstratethattherearenosimpleanswersforcountrieswhenitcomestoprovidingthecarethatissoessentialfortheirageinganddyingcitizens.
Acomplexrangeoffactors—economic,social,culturalandpolitical—needtobetakenintoaccountbeforepalliativecarecanbedeliveredeffectively.Byfactoringineverythingfromcertificationsforspecialistpalliativecareworkerstotheavailabilityofopioidanalgesics,thefollowingfivecategoriesthattogetherconstitutetheIndexprovideinsightsintowhysomecountriesaresucceedingwhileothersarefailing.
19 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
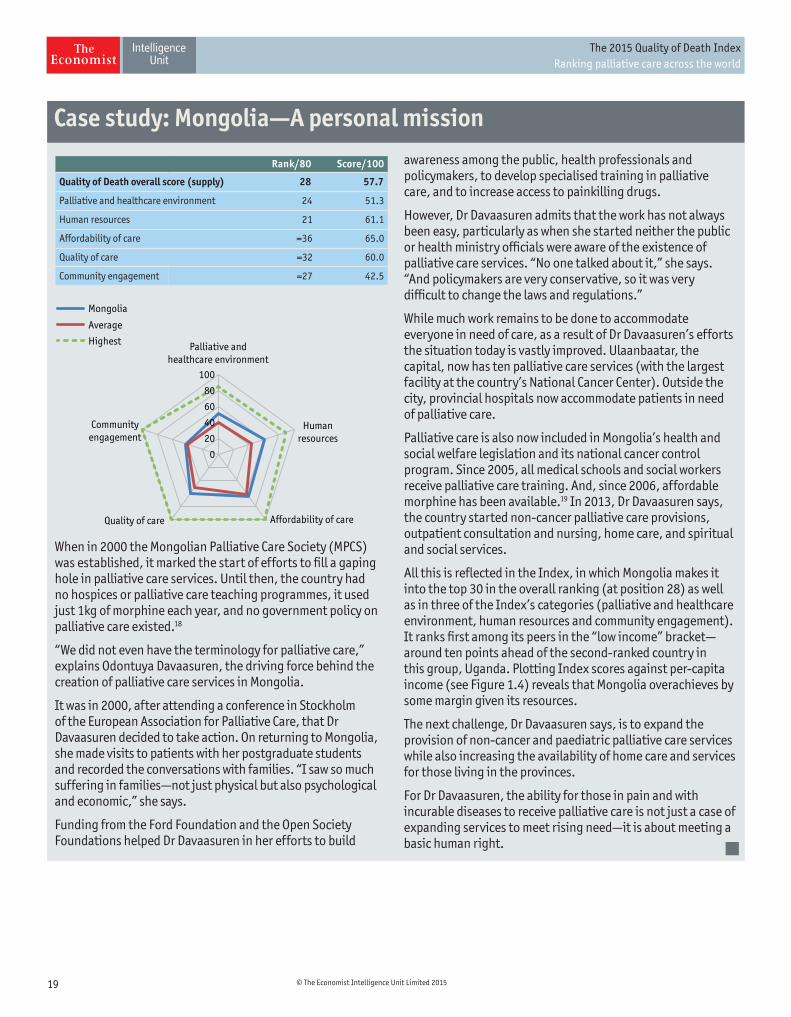
Whenin2000theMongolianPalliativeCareSociety(MPCS)wasestablished,itmarkedthestartofeffortstofillagapingholeinpalliativecareservices.Untilthen,thecountryhadnohospicesorpalliativecareteachingprogrammes,itusedjust1kgofmorphineeachyear,andnogovernmentpolicyonpalliativecareexisted.18
“Wedidnotevenhavetheterminologyforpalliativecare,”explainsOdontuyaDavaasuren,thedrivingforcebehindthecreationofpalliativecareservicesinMongolia.
Itwasin2000,afterattendingaconferenceinStockholmoftheEuropeanAssociationforPalliativeCare,thatDrDavaasurendecidedtotakeaction.OnreturningtoMongolia,shemadevisitstopatientswithherpostgraduatestudentsandrecordedtheconversationswithfamilies.“Isawsomuchsufferinginfamilies—notjustphysicalbutalsopsychologicalandeconomic,”shesays.
FundingfromtheFordFoundationandtheOpenSocietyFoundationshelpedDrDavaasureninhereffortstobuild
awarenessamongthepublic,healthprofessionalsandpolicymakers,todevelopspecialisedtraininginpalliativecare,andtoincreaseaccesstopainkillingdrugs.
However,DrDavaasurenadmitsthattheworkhasnotalwaysbeeneasy,particularlyaswhenshestartedneitherthepublicorhealthministryofficialswereawareoftheexistenceofpalliativecareservices.“Noonetalkedaboutit,”shesays.“Andpolicymakersareveryconservative,soitwasverydifficulttochangethelawsandregulations.”
Whilemuchworkremainstobedonetoaccommodateeveryoneinneedofcare,asaresultofDrDavaasuren’seffortsthesituationtodayisvastlyimproved.Ulaanbaatar,thecapital,nowhastenpalliativecareservices(withthelargestfacilityatthecountry’sNationalCancerCenter).Outsidethecity,provincialhospitalsnowaccommodatepatientsinneedofpalliativecare.
PalliativecareisalsonowincludedinMongolia’shealthandsocialwelfarelegislationanditsnationalcancercontrolprogram.Since2005,allmedicalschoolsandsocialworkersreceivepalliativecaretraining.And,since2006,affordablemorphinehasbeenavailable.19In2013,DrDavaasurensays,thecountrystartednon-cancerpalliativecareprovisions,outpatientconsultationandnursing,homecare,andspiritualandsocialservices.
AllthisisreflectedintheIndex,inwhichMongoliamakesitintothetop30intheoverallranking(atposition28)aswellasinthreeoftheIndex’scategories(palliativeandhealthcareenvironment,humanresourcesandcommunityengagement).Itranksfirstamongitspeersinthe“lowincome”bracket—aroundtenpointsaheadofthesecond-rankedcountryinthisgroup,Uganda.PlottingIndexscoresagainstper-capitaincome(seeFigure1.4)revealsthatMongoliaoverachievesbysomemargingivenitsresources.
Thenextchallenge,DrDavaasurensays,istoexpandtheprovisionofnon-cancerandpaediatricpalliativecareserviceswhilealsoincreasingtheavailabilityofhomecareandservicesforthoselivingintheprovinces.
ForDrDavaasuren,theabilityforthoseinpainandwithincurablediseasestoreceivepalliativecareisnotjustacaseofexpandingservicestomeetrisingneed—itisaboutmeetingabasichumanright.
Case study: Mongolia—A personal mission
Rank/80 Score/100
Quality of Death overall score (supply) 28 57.7
Palliative and healthcare environment 24 51.3
Human resources 21 61.1
Affordability of care =36 65.0
Quality of care =32 60.0
Community engagement =27 42.5
Palliative andhealthcare environment
Humanresources
Affordability of careQuality of care
Communityengagement
Mongolia
Average
Highest
0
20
40
60
80
100

20 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
TheadoptionofapalliativecareapproachinChinahasbeenslow,withmosthealthcareresourcesfocusedoncurativetreatment.AlthoughthenationalMinistryofHealthofficiallyendorsedtheestablishmentofpalliativecaredepartmentsinhospitalsin2008,20publicawarenessofandaccesstopalliativecareisstilllimited.OutsideofChina’s400specialisedcancerhospitals,thereareonlyahandfulofcharityhospitalsandcommunityhealthcentresthatofferpalliativecareservicestopatients.
China’soverallrankof71stoutof80countriesreflectsthislimitedavailabilityandthepoorqualityofpalliativecareingeneral.Serviceaccessibilitystandsatlessthan1%withmosthospicesconcentratedintheurbanareasofShanghai,BeijingandChengdu;thereisnonationalstrategyorguidelines;useandavailabilityofopioidsislimited;andpatient-doctorcommunicationispoor.21Inaddition,ifcareisnotcoveredbycharitabledonationsthefinancialburdenonpatientscanbequitehigh.AswithmostmedicaltreatmentsinChina,publicsubsidiesdonotfullycoverthecostandpatientcontributionsarerequired.
Arecentshiftingovernmentpolicy,mainlyatthemunicipallevel,signalsatrendofgreatersupportandinvestmentinhospicecareservices.CitieslikeShanghai,ShenzhenandTianjinhavesetnewtargetsandpoliciestoincreaseaccess
topalliativecare.Shanghaiplannedtoadd1,000bedsforhospicepatientsbytheendof2014,someinhospitalsandsomeincommunity-basedhealthcarecentres,22andTianjinrecentlyaddedhospicecaretotheofficiallistofgovernment-fundedsocialservices.23
ShiBaoxin,directoroftheHospiceCareResearchCenteratTianjinMedicalUniversity,saysthatdespiteimprovedawarenessandexpansionofpalliativecareinChinaoverthepast20years,it’sstillearlydays.“It’shardforhospicecaretodevelopmainlybecauseofthelackofeducationaboutdeath,”DrShisays,addingthatthisalsomakeseffectivepsychologicaltreatmentofdyingpatientsmorechallenging.
Thislackofawarenessextendstomedicalprofessionals.NingXiaohong,anoncologistatPekingUnionMedicalCollegeHospital,saysthatteachingofpalliativecareconceptsinmedicaltrainingisextremelylimited,whichmeansthatmostpracticingprofessionalshaveneverbeenexposedtoessentialconceptsortechniques.Inresponse,DrNingisdevelopinganonlinecourseonpalliativecaretobeusedonanannualbasis.
ChengWenwu,directoroftheDepartmentofPalliativeCareatFudanUniversityCancerHospital,agreesthatthelackofprofessionalknowledgeandlowpublicawarenessmeanthatbothpatientsanddoctorsfocusoncurativetreatments,anddon’tthinkaboutpalliativecareoptions.However,publicawarenessisgraduallyincreasing,spreadviaTVandnewspapersandalsowordofmouth.DrNingreportsanincreaseinthelastfewyears,andsaysshenowseessomepatientsathercliniccominginwithquestionsaboutpalliativecareoptions.
Withoutgovernmentsubsidies,financialcostsareamajorchallenge,aspalliativecareisgenerallynotsupportedthroughthenationalhealthsecuritysystem.SongtangHospiceinBeijingwasoneoftheearliestpalliativecareinstitutions,foundedin1987,andcurrentlycaresforaround320patients.Whilethecostsofcarearerelativelylow,onaverageRMB1,000-2,000(US$160-320)permonth,patientsstillstruggletoaffordit,saysLiWei,thehospital’sfounder.
Inadditiontofinancialbarriers,culturalbeliefsalsohinderthewidespreaduseofpalliativecare.AccordingtoDrLi,most
Case study: China—Growing awareness
Rank/80 Score/100
Quality of Death overall score (supply) 71 23.3
Palliative and healthcare environment 69 21.1
Human resources 70 21.0
Affordability of care =65 37.5
Quality of care 69 16.3
Community engagement =45 25.0
Palliative andhealthcare environment
Humanresources
Affordability of careQuality of care
Communityengagement
China
Average
Highest
0
20
40
60
80
100
Thebiggestchallengeistochangepeople’sminds,toletthemknowthatsocietycantakegoodcareoftheirparentsinthelatestagesofillnessandhelpthemdiewithdignity.
Li Wei, founder, Songtang Hospice, Beijing

21 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
Chinesestillfollowthetraditionof“raisingchildrentocareforyouinoldage,”andmanyfamiliesfeelthattooutsourcecareofrelatives,evenintheirfinaldays,isunfilial.
“Thebiggestchallengeistochangepeople’sminds,toletthemknowthatsocietycantakegoodcareoftheirparentsinthelatestagesofillnessandhelpthemdiewithdignity,”DrLisays.Theimpactoftheone-childpolicy,oftenleavingindividualscaringfortwoparentsandfourgrandparents,willleadtoevenmoredemandforoutsideresourcestoprovidesupport.
ThemostinnovativeaspectsofprovidingpalliativecareinChinaarenottechnical,butcultural.AccordingtoDrShi,“WefollowtheWesternideasforhospicetreatment,butour
mainimprovementistoapplyChinesetraditionalculturetopsychologicalcounseling,forexamplewedoresearchtounderstandhowpeopleofdifferentclassesandagesthinkofdeath,tofigureouthowtohelpthempsychologically.”
Meanwhile,SongtangHospicehasworkedwithmanyvolunteerswhoprovidepsychologicalandemotionalsupporttopatients,intheprocesseducatingcommunitymembersaboutpalliativecare.Publicawarenessisalsogrowingthroughscatteredsocialmediaefforts,suchasanonlinecampaignon”ChoiceandDignity”foundedbythechildrenofseniorCommunistPartymembers,whichencouragesvisitorstosignlivingwills.24

22 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
Palliative and healthcare environment2
Giventheavalancheofdemandheadingtowardsgovernmentsaroundtheworld,animportantindicatorofcountries’successindeliveringpalliativecareistheextenttowhichservicesareavailable—whetherinhospices,hospitals,carehomesorpeople’sownhomes.Toassessthis,theIndexusesarangeofindicators,includinganation’soverallspendingonhealthcare,thepresenceandstrengthofgovernmentpoliciesonpalliativecare,theavailabilityofresearch-basedpolicyevaluationandthecapacitytodeliverpalliativecareservices.25
Inthiscategory,inwhichtheUKtopsthelist,sixofthetop10countriesareEuropean,alongwithAustralia,Taiwan,theUSandNewZealand.Regionally,somesurprisesemerge.AmongAsia-Pacificcountries,itisnotablethatVietnamandMongoliamakeitintothetop10.AndintheAmericas,whileasexpectedtheUSandCanadatopthelist,Chileisinfourthplace.This,saysEduardoYanneo,chairmanoftheMontevideo-basedLatinAmericanAssociationforPalliativeCare,is“becauseithasoneoftheoldestnationalprogrammesintheregion,withgovernmentsupportsincethebeginning.”
Notallhigh-incomecountriesperformwellintheIndex.HongKongisrelativelylowintheoverallrankingofthiscategory,atposition28—lowerthanPanama(atposition25),amiddle-incomecountry,andMongolia(atposition24),alow-incomecountry.HongKongscoresrelativelypoorlyintermsofoverallhealthcarespending,theavailabilityofresearch-based
policyevaluationanditscapacitytodeliverpalliativecareservices.
Nationalpoliciesplayavitalroleinextendingaccesstopalliativecare.Asaresult,thepresenceandeffectivenessofgovernmentpoliciesreceivesa50%weightinginthiscategory(andbecausethiscategoryisgivena20%weightingintheoverallIndex,thisindicatorrepresents10%oftheentireQualityofDeathscore).
Whilechangesinmethodologyandscopemeandirectcomparisonswiththe2010Indexarenotpossible,severalcountrieshavemadepolicyadvancesthatarereflectedinahigherrankinginthe2015Index.Singaporewasatposition18in2010—roughlymidwaydownthe40-countrylist—andisnowatposition12outof80countries,havingdevelopedanationalpalliativecarestrategythatwasacceptedin2012andisnowbeingimplemented.
India,whichwasatthebottomofthelistinthe2010Index,isataslightlyhigherpositionin2015—at51—reflectingastrongerindicationofgovernmentcommitment.WhilethebudgetallocationforIndia’s2012NationalProgramforPalliativeCarewaswithdrawn,elementsofthestrategyremainsinplaceand,asaresult,someteachingprogrammesareemergingacrossthecountry.Moreover,recentlegislativechangeshavemadeiteasierfordoctorstoprescribemorphineinIndia.
23 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
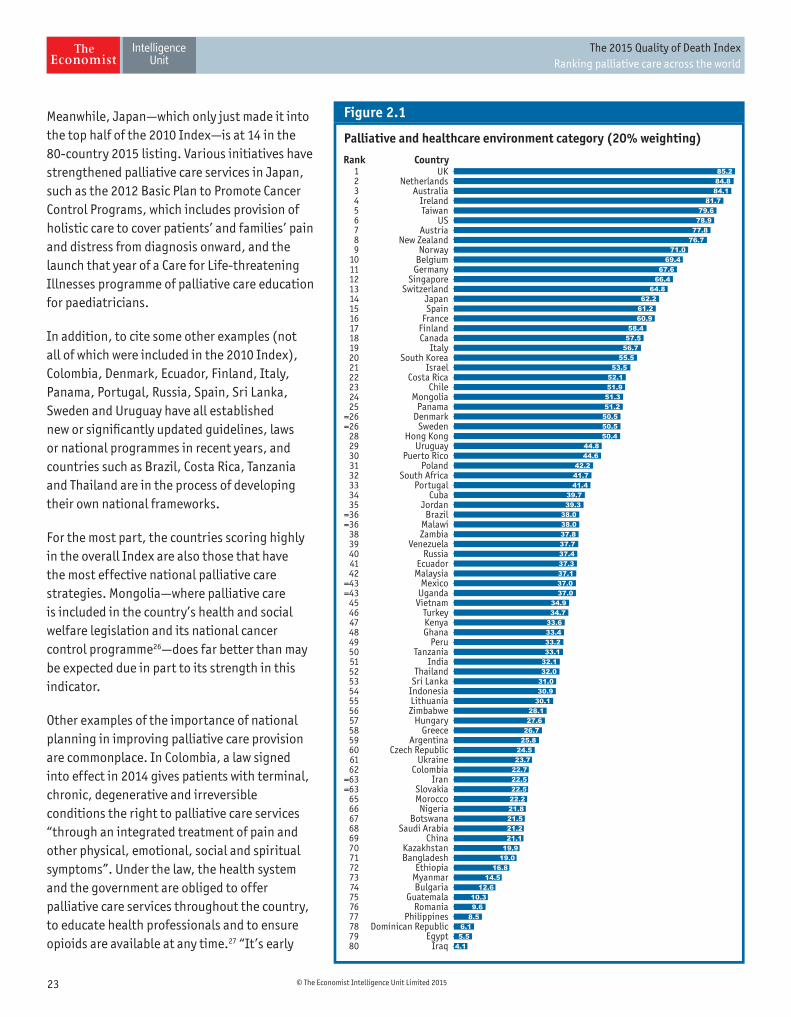
Meanwhile,Japan—whichonlyjustmadeitintothetophalfofthe2010Index—isat14inthe80-country2015listing.VariousinitiativeshavestrengthenedpalliativecareservicesinJapan,suchasthe2012BasicPlantoPromoteCancerControlPrograms,whichincludesprovisionofholisticcaretocoverpatients’andfamilies’painanddistressfromdiagnosisonward,andthelaunchthatyearofaCareforLife-threateningIllnessesprogrammeofpalliativecareeducationforpaediatricians.
Inaddition,tocitesomeotherexamples(notallofwhichwereincludedinthe2010Index),Colombia,Denmark,Ecuador,Finland,Italy,Panama,Portugal,Russia,Spain,SriLanka,SwedenandUruguayhaveallestablishedneworsignificantlyupdatedguidelines,lawsornationalprogrammesinrecentyears,andcountriessuchasBrazil,CostaRica,TanzaniaandThailandareintheprocessofdevelopingtheirownnationalframeworks.
Forthemostpart,thecountriesscoringhighlyintheoverallIndexarealsothosethathavethemosteffectivenationalpalliativecarestrategies.Mongolia—wherepalliativecareisincludedinthecountry’shealthandsocialwelfarelegislationanditsnationalcancercontrolprogramme26—doesfarbetterthanmaybeexpecteddueinparttoitsstrengthinthisindicator.
Otherexamplesoftheimportanceofnationalplanninginimprovingpalliativecareprovisionarecommonplace.InColombia,alawsignedintoeffectin2014givespatientswithterminal,chronic,degenerativeandirreversibleconditionstherighttopalliativecareservices“throughanintegratedtreatmentofpainandotherphysical,emotional,socialandspiritualsymptoms”.Underthelaw,thehealthsystemandthegovernmentareobligedtoofferpalliativecareservicesthroughoutthecountry,toeducatehealthprofessionalsandtoensureopioidsareavailableatanytime.27“It’searly
Palliative and healthcare environment category (20% weighting)
Figure 2.1
Rank Country
IraqEgypt
Dominican RepublicPhilippines
RomaniaGuatemala
BulgariaMyanmarEthiopia
BangladeshKazakhstan
ChinaSaudi Arabia
BotswanaNigeria
MoroccoSlovakia
IranColombia
UkraineCzech Republic
ArgentinaGreece
HungaryZimbabweLithuaniaIndonesiaSri LankaThailand
IndiaTanzania
PeruGhanaKenyaTurkey
VietnamUgandaMexico
MalaysiaEcuador
RussiaVenezuela
ZambiaMalawi
BrazilJordan
CubaPortugal
South AfricaPoland
Puerto RicoUruguay
Hong KongSweden
DenmarkPanama
MongoliaChile
Costa RicaIsrael
South KoreaItaly
CanadaFinlandFranceSpainJapan
SwitzerlandSingapore
GermanyBelgiumNorway
New ZealandAustria
USTaiwanIreland
AustraliaNetherlands
UK
4.15.56.18.59.610.312.614.516.819.019.921.121.221.521.822.222.522.522.723.724.525.826.727.628.130.130.931.032.032.133.133.233.433.634.734.937.037.037.137.337.437.737.838.038.039.339.741.441.742.244.644.8
50.450.550.551.251.351.952.153.555.556.757.558.460.961.262.264.866.467.669.471.0
76.777.878.979.681.784.184.885.2
80797877767574737271706968676665
=63=63
626160595857565554535251504948474645
=43=43
4241403938
=36=36
3534333231302928
=26=26
25242322212019181716151413121110
987654321

24 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
Figure 2.2: Presence and effectiveness of government-led national palliative care strategy5 4 3 2 1
Thereisacomprehensivestrategyforthedevelopmentandpromotionofnationalpalliativecare.Ithasaclearvision,clearlydefinedtargets,anactionplanandstrongmechanismsinplacetoachievetargets.Infederal-structurecountries,therearestrongandclearlydefinedstrategiesthatindividualstatesmustfollow.Thesemechanismsandmilestonesareregularlyreviewedandupdated.
Thereisawell-defined,government-ledstrategyforthedevelopmentandpromotionofnationalpalliativecare.Ithasaclearvisionandspecificmilestones.Therearemechanismsinplaceandguidelinesonimplementation.Itismostlywellimplemented,eveninfederal-structurecountries.
Thereisagovernment-ledstrategyforthedevelopmentandpromotionofnationalpalliativecare.Thishasabroadvision,andlooselydefinedmilestones(nospecifictargets).Therearelimitedmechanismsinplacethataimtoachievemilestones.Infederal-structurecountries,statesarenotmandatedtofollowthenationalstrategy;i.e.itisonlyprescriptiveinnature
Thereisagovernment-ledstrategyforthedevelopmentandpromotionofnationalpalliativecare.However,itismerelyastatementofbroadintent.Itdoesnotcontainaclearvisionorspecificmilestonestoachieve.Therearenoclearmechanismsinplacetoachievethestrategy.
Thereisnogovernment-ledstrategyforthedevelopmentandpromotionofnationalpalliativecare.
Australia Singapore Austria Japan Brazil Portugal Argentina Iran Bulgaria Guatemala
Ireland Taiwan Belgium Mongolia Canada PuertoRico Bangladesh Kazakhstan Dominican Iraq
Netherlands UK Chile Norway CostaRica Russia Botswana Lithuania Republic Philippines
NewZealand Finland Panama Cuba SouthAfrica China Morocco Egypt Romania
France SouthKorea Denmark SriLanka Colombia Myanmar
Germany Spain Ecuador Sweden Czech Nigeria
HongKong Switzerland Ghana Tanzania Republic SaudiArabia
Israel US India Thailand Ethiopia Slovakia
Italy Indonesia Turkey Greece Ukraine
Jordan Uganda Hungary
Kenya Uruguay
Malawi Venezuela
Malaysia Vietnam
Mexico Zambia
Peru Zimbabwe
Poland
days,”saysDrPayne.“Buttherearethingshappeningtherethatshowgreatpromise.”
InSpain,itwasthe2007launchofanationalstrategythatledtoanincreaseof50%inthenumberofpalliativecareteamsandunifiedregionalapproachestopalliativecare,accordingtoJavierRocafortGil,formerpresidentoftheSpanishAssociationforPalliativeCare.28
Therelationshipbetweenhealthcarespendingandavailabilityofpalliativecareismorecomplex.(Inthiscategory,governmentspendingonhealthcare—whichisusedasaproxyforpalliative
carespending,forwhichcomparabledataarenotalwaysavailable—isgivena20%weighting,sorepresents4%oftheoverallIndex;Figure2.3.)Forexample,whiletheUSisattopofthelistwhenitcomestohealthcarespending(equivalentto17.9%ofGDPin2012),itisonlyatposition6inthiscategoryoftheIndex.AndwhiletheUKtopsthelistinthiscategory,itfallstoposition17lookingathealthcarespendingalone(9.4%ofGDP).
Singaporeisanevenmoredramaticoutlier,sinceitsCentralProvidentFund—acomprehensivesocialsecuritysystembasedon

25 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
asavingsplanthatiscompulsoryforallworkingresidents—coversalargeproportionofnationalhealthcarecosts,withindividualspayingforhealthcareoutoftheirfund.However,inrecentyears,fallingbirthratesandsmallerfamilyunitshavemeantthat,whenitcomestocaringfortheelderlyanddying,thetraditionalsystemofcarebyrelativeshasbrokendown.Asaresult,Singaporehashadtoraiseitshealthcarespending.Thegovernmenthasincreasedhealthcarecoveragefortheelderlywhilethenationalhealthcareinsuranceprogrammehasbeenenhanced,dramaticallyimprovingaffordability.
Thediscrepanciesreflectdifferencesinthewaypalliativecareisdeliveredaroundtheworld.Forwhilegovernmentsareresponsibleinsomeplaces,avarietyoforganisations,fromphilanthropicgroupstoreligiousinstitutions,extendthereachofthoseservicesinmanycountries.
Correlation with spending on healthcare (% of GDP, 2012)
Figure 2.3
Quality of Death overall score (100=best)
Healthcare spending (% of GDP, 2012)
R2 = 0.463
ZimbabweSri Lanka
Saudi ArabiaIndonesia
Malaysia
ThailandVenezuela
PeruGhana
Kazakhstan
Egypt
IndiaEthiopia
MyanmarBangladesh
IraqPhilippines
Dominican Republic
NigeriaGuatemala
UkraineMalawi
Zambia
Vietnam
MoroccoRussiaPuerto RicoTurkey
Brazil
SlovakiaTanzania
Israel
ChileLithuania Czech Republic Argentina
Cuba
Costa Rica
SpainPortugal
Singapore
TaiwanIreland
AustraliaUK
New Zealand
South Korea
Italy
Norway
Sweden DenmarkAustria
SwitzerlandNetherlandsFranceGermany
Belgium
USJapan
Finland
Panama
PolandMongolia
Greece
Ecuador
Hong Kong
Mexico
Bulgaria
ColombiaChina
RomaniaKenya
Botswana Iran
0
20
40
60
80
100
0 2 4 6 8 10 12 14 16 18 20
South AfricaJordanUruguay
Uganda
Hungary
Canada
TheUS,forexample,hasahighlevelofspendingonpalliativecarethroughthegovernment-fundedreimbursementforhospicecarethroughMedicare,thefederalprogrammeprovidinghealthinsurancecoveragetoallindividualsovertheageof65.
IntheUK,thehospicemovement,whichdeliversmuchofthecountry’spalliativecare,isfundedlargelythroughcharitabledonations.InSingapore,too,thecharitablesectorwasbehindthehospicemovement.“Agroupofvolunteersidentifiedagapintheservices,anditwasagapthegovernmentatthetimewasn’tpreparedtoworkon,”explainsDrGoh.However,shesays,whilethevoluntarysectorcontinuestoruntheservices,thegovernmentnowfundsthem,providingapproximately30-60%oftheirfinancialrequirements.

26 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
Capacity to deliver palliative care* (%)
Figure 2.4
Rank Country
EthiopiaNigeria
MoroccoEgypt
VietnamVenezuelaIndonesiaMyanmarSri Lanka
IranBangladesh
Dominican RepublicIraq
BrazilPeru
GhanaChina
ThailandMexico
ColombiaIndia
Saudi ArabiaTurkey
CubaEcuador
KazakhstanPanamaUkraine
GuatemalaTanzania
MalawiRussia
ZambiaBotswanaZimbabwe
UgandaKenya
JordanPhilippines
PortugalCzech Republic
GreeceSlovakia
ArgentinaRomania
ChileSouth Korea
MongoliaBulgaria
South AfricaHong Kong
IsraelFinland
JapanHungary
ItalyUruguayMalaysia
FranceDenmark
SingaporePoland
SwitzerlandPuerto Rico
LithuaniaSpain
SwedenNew Zealand
TaiwanBelgium
GermanyIrelandCanada
Costa RicaNorway
NetherlandsAustralia
UKUS
Austria
000.10.10.10.10.10.10.10.10.10.20.30.30.30.30.30.40.40.40.40.50.50.50.60.70.80.91.01.01.01.31.81.82.02.02.52.62.82.93.1
4.24.34.34.44.55.65.65.76.27.08.310.211.012.312.5
15.416.416.817.519.6
22.923.024.024.325.5
30.932.5
39.039.339.740.240.842.342.642.844.2
46.652.0
63.6
=79=79=70=70=70=70=70=70=70=70=70
69=64=64=64=64=64=60=60=60=60=57=57=57
56555453
=50=50=50
49=47=47=45=45
444342414039
=37=37
3635
=33=33
3231302928272625242322212019181716151413121110
987654321
Similarly,ofthelargenetworkofhospicesinSouthAfrica,mostarenon-governmentalorganisations,withchurchesalsoprovidingservices.SouthAfricahasdevelopedahighlyintegratedmodelofpalliativecarethroughitshospicemovement,saysDrHarding.“Theirhospicesdon’tjustfocusonend-of-lifecare,”hesays.“TheyareoutinthecommunityprovidingTBcontrol,familyeducation,diagnosis,infectioncontrolandgoingintoclinicstoprovidebasicHIVcare.”
Yetevenincountriesthathaverobustpoliciesandfundingforpalliativecare,gapsinprovisionexist—gapsthatmayincreasewiththeriseintheproportionofoldercitizensinthecomingyears.
InAustralia,whichrankssecondintheoverallIndexandthirdinthepalliativeandhealthcareenvironmentcategory,responsibilityforhealthcareisdevolvedtothestates,whichcanleadtoinconsistencyincaredelivery.
“Thereisn’tanequitablespreadoffundingacrossthecountry,”saysLizCallaghan,chiefexecutiveofPalliativeCareAustralia(PCA).“You’dhopeitwouldbebasedonwhatthepopulationneeds.Everyonetalksaboutit,butthat’sveryfaraway.Insomestatesfundingforpalliativecareisextremelylowsothemultidisciplinaryteammightbejustadoctorandanurse.”
Butwhileincreasedgovernmentfundingforhealthcaremightseemtobetheanswer,thismaynotalwaysbethecase.IntheUS,tighterscrutinyofhealthcarespendingbybothgovernmentandprivateinsurerscouldactuallybeaforcedrivingincreaseduseofpalliativecare,asitbecomesclearthatpalliativecareisacost-effectivealternativetohospitaladmissions.
Aspartofthis,healthsystems’andhospitals’reimbursementsareincreasinglybeingtiedtoqualitymeasures,includingwhetherpatientsarereadmittedwithin30days.InPennsylvania,
*Thisisaproxyindicatortomeasurethepercentageofpeoplewhodiedinacountryinoneyearthatwouldhavebeabletoreceivepalliativecare,giventhecountry’sexistingresources.Somecountriespublishstatisticsonthenumberofdeathsthatusedpalliativecare,butdataisnotuniformlyavailableforall80countriesintheIndex.Asanapproximation,weuseanestimationofthecapacityofpalliativecareservicesavailable(i.e.ofspecialisedprovidersofpalliativecare,includingthosethatadmitpatientsandprovideservicesathomeandinfacilities)basedonWHPCAdata,anddividebythenumberofdeathsinagivenyear.

27 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
forexample,Medicaid—thefederallyfundedhealthcareprogrammeforlow-incomeAmericans—doesnotreimbursehealthcareprovidersforall30-dayreadmissions.
“IfwetakecareofaMedicaidpatientandtheycomeback,thecostofthesecondreadmissionisonus,”saysDavidCasarett,directorofhospiceandpalliativecareattheUniversityofPennsylvaniaHealthSystem.“Sotheattentionto30-dayreadmissionsisstartingtodrivealotofinterestinpalliativecare.”
Thepreferenceofmanypeopletodieathomeisanotherreasonhospiceinfrastructureneedstobebalancedwiththeavailabilityofoutpatientpalliativecare.Andascountriesarefacedwithrapidlyageingpopulationsandhealthcareresourcesbecomemoretightlystretched,moreandmorepalliativecarewillneedtotakeplaceoutsideformalhospiceorhospitalsettings.
You’dhope[palliativecarefunding]wouldbebasedonwhatthepopulationneeds.Everyonetalksaboutit,butthat’sveryfaraway.
Liz Callaghan, chief executive, Palliative Care Australia
“Everyoneisgettingolder,deathsarebecomingmorecomplicated,thenumberofdeathsperyearisincreasingandhospicesonlycatertoabout6%ofalldeaths,”saysDrSleeman.“Sothere’snowaywe’lleverhaveenoughin-patientbeds.”Aproxyindicatormeasuringthecapacitytodeliverpalliativecare,basedontheservicesavailablecomparedtothenumberofdeaths(Figure2.4),illustratesthescaleofthechallengefacingmostcountries,withthehighest(Austria)stillreachingjust64%andthemajorityofcountries—allbut28—under10%.29
DrSleemanarguesthatcarehomesandpeople’shomesshouldbethefocusfortheextensionofpalliativecareservices.“Itmeansputtinglessemphasisonaunitcateringtoonly22peopleatatimebuttakingskillsandprofessionalsintothecommunity,”shesays.“That’sthefuture.”

28 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
ThedevelopmentsinpalliativecareinSpainthatfollowedthe2007launchofanationalpalliativecarestrategy30demonstratewhatcanbeachievedwhenstandardsareco-ordinatedacrossanation.
Thecountryhaslonghadpocketsofexcellence:inCatalonia,extensivepalliativecareserviceshavebeenavailablesince1990throughtheCatalanHealthCareSystem,withmorethan95%oftheregioncoveredbypalliativecareservicesby2005.31 Butinacountrywherehealthcarefallsundertheauthorityof17regionalhealthsystems,unifyingapproachestopalliativecarehasdonemuchtoincreaseaccesstoservices.
“ItwasthedeterminantforthedevelopmentofpalliativecareinSpain,”saysJavierRocafortGil,formerpresidentoftheSpanishAssociationforPalliativeCare.“Thestrategyensuredthateveryregionalministryofhealthwouldworktogetherinthesamemanner.”
Since2007,anotherimportantdevelopmentinpalliativecaredevelopmenthasbeentheinvolvementof“laCaixa”bankingfoundation,whichhassupportedtheintegrationof29psychologicalandspiritualcareteamsintothecountry’spalliativecarenetwork.
Evenbeforethelaunchofthenationalstrategy,Spain—whichisatposition23intheoverallIndexand15inthepalliativeandhealthcareenvironmentcategory—hadfromthe1990sdevelopedastrongnetworkofhomecareservices.
“It’scultural,becauseinSpainpeoplewanttodieathome,”saysProfessorRocafortGil,whoisnowmedicaldirectorattheFundaciónVianorteLagunaatMadrid’sUniversidadFranciscodeVitoria.“Butit’salsobecauseprimarycareisverystrong—muchoftheinitialdevelopmentinspecialistpalliativecareinSpainwasinprimarycareteams.”
AndwhileSpainhasonlytwodedicatedhospices,servicesverysimilartothosefoundathospicesareavailableatthecountry’smedium-andlong-termstayhospitals.
However,despiteitsstrengthinmanyareasofpalliativecare,Spainstillhasworktodo.“Weareclosetohavingthenumberofunitsinhomecareandhospitalteamsweneed,”explainsProfessorRocafortGil.“Butwearestillfarfromhavingenoughunitsforchildren.”
Moreover,whileatuniversitiesmorethanhalfofmedicalstudentsnowundertakebasicandintermediarypalliativecareprogrammes,accreditationforspecialistpalliativecareteamsisstilllacking.This,saysProfessorRocafortGil,willrequirefurtherregulation.Andwhilelawspassedin2003and2004giveeverySpanishcitizentherighttoreceivepalliativecareathomeorinhospital,onlythreeregions—Andalusia,AragonandNavarra—havethekindofdetailedlegislationcoveringpalliativecarethathearguesshouldbeimplementedacrossthewholecountry.
Spain’sstrengthsandweaknesseshighlightthefactthat,evenincountriesthathavebroadaccesstohigh-qualityservices,theinterplayofpolicy,legislationandtrainingremainscriticalifserviceprovisionistomeetrisingdemandforcare.
Case study: Spain—The impact of a national strategy
Rank/80 Score/100
Quality of Death overall score (supply) 23 63.4
Palliative and healthcare environment 15 61.2
Human resources 36 42.6
Affordability of care =25 75.0
Quality of care 24 78.8
Community engagement =33 40.0
Palliative andhealthcare environment
Humanresources
Affordability of careQuality of care
Communityengagement
Spain
Average
Highest
0
20
40
60
80
100
29 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
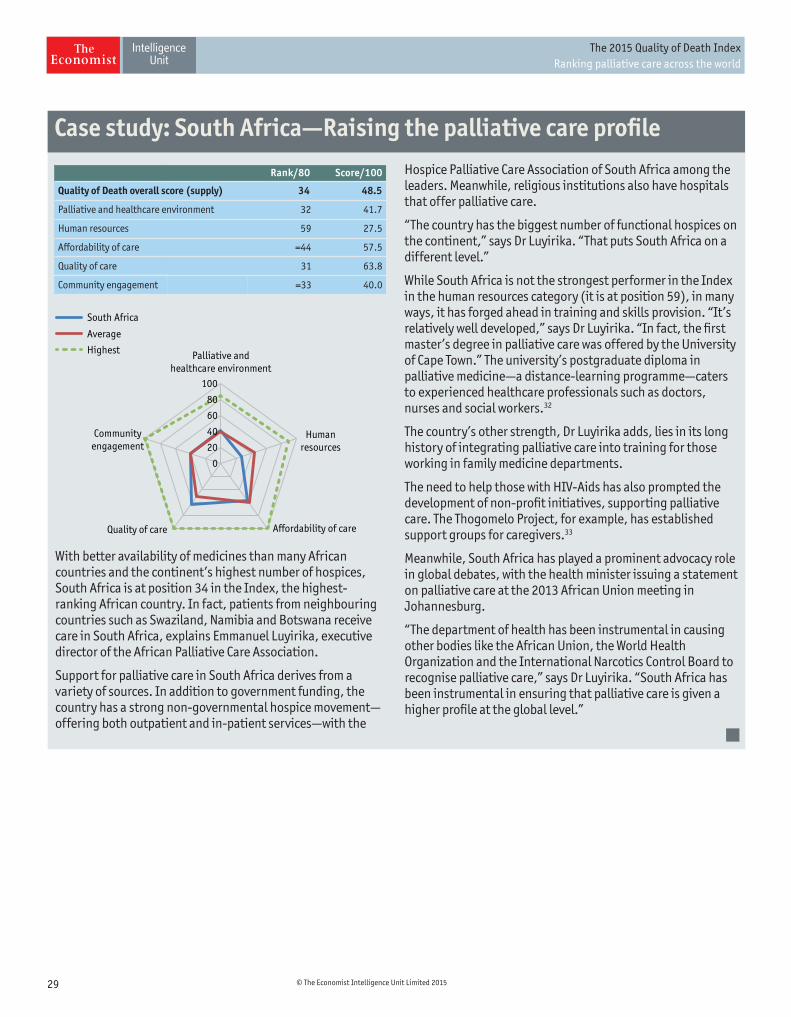
WithbetteravailabilityofmedicinesthanmanyAfricancountriesandthecontinent’shighestnumberofhospices,SouthAfricaisatposition34intheIndex,thehighest-rankingAfricancountry.Infact,patientsfromneighbouringcountriessuchasSwaziland,NamibiaandBotswanareceivecareinSouthAfrica,explainsEmmanuelLuyirika,executivedirectoroftheAfricanPalliativeCareAssociation.
SupportforpalliativecareinSouthAfricaderivesfromavarietyofsources.Inadditiontogovernmentfunding,thecountryhasastrongnon-governmentalhospicemovement—offeringbothoutpatientandin-patientservices—withthe
HospicePalliativeCareAssociationofSouthAfricaamongtheleaders.Meanwhile,religiousinstitutionsalsohavehospitalsthatofferpalliativecare.
“Thecountryhasthebiggestnumberoffunctionalhospicesonthecontinent,”saysDrLuyirika.“ThatputsSouthAfricaonadifferentlevel.”
WhileSouthAfricaisnotthestrongestperformerintheIndexinthehumanresourcescategory(itisatposition59),inmanyways,ithasforgedaheadintrainingandskillsprovision.“It’srelativelywelldeveloped,”saysDrLuyirika.“Infact,thefirstmaster’sdegreeinpalliativecarewasofferedbytheUniversityofCapeTown.”Theuniversity’spostgraduatediplomainpalliativemedicine—adistance-learningprogramme—caterstoexperiencedhealthcareprofessionalssuchasdoctors,nursesandsocialworkers.32
Thecountry’sotherstrength,DrLuyirikaadds,liesinitslonghistoryofintegratingpalliativecareintotrainingforthoseworkinginfamilymedicinedepartments.
TheneedtohelpthosewithHIV-Aidshasalsopromptedthedevelopmentofnon-profitinitiatives,supportingpalliativecare.TheThogomeloProject,forexample,hasestablishedsupportgroupsforcaregivers.33
Meanwhile,SouthAfricahasplayedaprominentadvocacyroleinglobaldebates,withthehealthministerissuingastatementonpalliativecareatthe2013AfricanUnionmeetinginJohannesburg.
“ThedepartmentofhealthhasbeeninstrumentalincausingotherbodiesliketheAfricanUnion,theWorldHealthOrganizationandtheInternationalNarcoticsControlBoardtorecognisepalliativecare,”saysDrLuyirika.“SouthAfricahasbeeninstrumentalinensuringthatpalliativecareisgivenahigherprofileatthegloballevel.”
Case study: South Africa—Raising the palliative care profile
Rank/80 Score/100
Quality of Death overall score (supply) 34 48.5
Palliative and healthcare environment 32 41.7
Human resources 59 27.5
Affordability of care =44 57.5
Quality of care 31 63.8
Community engagement =33 40.0
Palliative andhealthcare environment
Humanresources
Affordability of careQuality of care
Communityengagement
South Africa
Average
Highest
0
20
40
60
80
100

30 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
Human resources3 Therisingneedforpalliativecaremeanscountrieswillneedtospendmoreequippingdoctorsandnursestoprovideit.Partofthismeansprovidingappropriatetrainingforend-of-lifecareworkersinmedicalschools.However,tomeetgrowingdemand,thistrainingalsoneedstobeincorporatedintotheteachingforalldoctorsandnurses,withpalliativecareexpertisearequiredcomponentofbothgeneralandspecialisedmedicalqualifications.
InthiscategoryoftheIndex,countriesareassessedontheavailabilityofspecialistsinpalliativecareandpractitionerswithgeneralmedicalknowledgeofpalliativecare;thepresenceofcertificationsforpalliativecare;andthenumberofdoctorsandnursesforevery1,000palliativecare-relateddeaths(togaugetheburdenrelativetotheneedforpalliativecare).
Ofthese,theavailabilityofspecialisedpalliativecareworkersisgiventhehighestweighting,at40%ofthiscategory(and8%oftheoverallIndex,asthehumanresourcescategoryisweighted20%oftheoverallIndex;Figure3.2).Countriesthatscore5inthisindicatorhaveprofessionallyornationallyaccreditedspecialisttrainingfortheircorepalliativecareteams.Bycontrast,ascoreof1indicatesanabsenceofcertificationoraccreditationandasevereshortageofpalliativecareprofessionals.
Generalmedicalknowledgeofpalliativecareisalsoimportant(accountingfor30%ofthiscategory),withscoresof5awardedtocountrieswhereallnursesanddoctorshaveagood
understandingofpalliativecare,andpalliativecareiscompulsoryindoctorandnursetrainingschoolsandhealthcareprofessionalsreceiveprofessionaltrainingthroughouttheircareers.Forthosescoring1,thereisnosuchknowledgeortrainingavailable.
Inthiscategory,atthetopofthelistisAustralia,followedbytheUKandGermany.SingaporeandTaiwanmakeitintothetop10inthisindicator,butAsia’spoorer,morepopulousnationsdoworse.India,forexample,hasashortageofspecialisedcareprofessionalsandaccreditationforpalliativecareisnotyetthenorm.However,thecountryisworkingtowardschangingthis,accordingtoSushmaBhatnagar,headofanaesthesiology,painandpalliativecareattheAllIndiaInstituteofMedicalSciences’DrBRAmbedkarInstitute-RotaryCancerHospital.
DrBhatnagarhighlightsvariousteachingprogrammesthathaveemergedacrossIndiasincethegovernmentintroducedanationalpalliativecarepolicyin2012.ThisincludesamajornationalinitiativelaunchedbytheIndianAssociationofPalliativeCare.“Theyareorganisingessentialcoursesinpalliativecareinalmostall30centres,”saysDrBhatnagar.“Soit’sgoodnewsforthecountry.”
Meanwhile,incountriesthatperformwellinthiscategory,someseeroomforimprovement.WhileAustraliaisinfirstplace,forexample,YvonneMcMaster,aretiredpalliativecaredoctor
Ifevery[healthprofessional]haspalliativecareintheirbasiceducation,thennoonewillcomeoutnotunderstandingpainmanagement,howtocommunicatewithpatientsandfamiliesorthatpsychological,socialandspiritualcarearepartofpalliativecare,notanoptionalextra.
Sheila Payne, emeritus professor at the International Observatory on End of Life Care at Lancaster University

31 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
andadvocateforpalliativecare,identifiesgapsinhumanresourcesinfrastructure.
ShecitesthecaseofNewSouthWales,whichishometoone-thirdofAustralia’spopulation.“IntheruralandregionalareasoutsidetheSydneymetropolitancluster,mostpalliativecareisdonebynurses,”shesays.“ThereareonlyfourspecialistdoctorsinNewSouthWalesoutsidetheSydneyarea.Andeventhoughmorearebeingtrainedthefundingisn’tbeingprovidedforthepositions.”
DespiteFrance’spositionat10thinthiscategory,gapsintrainingstillexist.Forexample,whilemaster’sdegreesinpalliativecareareavailablefordoctorsoncetheyhavequalified,littleattentionispaidtoitduringtheirinitialtraining.“Fordoctors,thereareonly10hoursinalloftheirtrainingtostudypalliativecare,”saysAnnedelaTour,headofthedepartmentofpalliativecareandchronicpainattheCentreHospitalierVDupouy.Sheaddsthatnurseshavenorecognitionintermsofsalaryorstatusforhavingaspecialisationinpalliativecare.
Uruguayperformsrelativelywellinthiscategory,comingwithinthetop25countriesandinthetopthreeintheAmericas.YetDrYanneo,oftheLatinAmericanAssociationforPalliativeCare,highlightsweaknesses.Themainproblem,hesays,isthatthegovernment’sinitialhumanresourcesfocushasnotledtothedevelopmentofarobustpalliativecarediscipline.“Unfortunately,theseeffortsdidnothavesufficient,timelyandadequatesupportfromuniversityandgovernmentauthorities,”hesays.
Infact,hepointsto“improvingeducationandcertificationinthediscipline”asoneofthebiggestchallengesfacedbymostLatinAmericancountries.
ThisshouldbeapriorityforChile,saysCeciliaSepulveda,formerheadoftheNationalCancerControlProgrammeatChile’sministryof
Human resources category (20% weighting)
Figure 3.1
Rank Country
BangladeshIraqIran
MyanmarBulgaria
PhilippinesEthiopia
KenyaBotswanaIndonesia
ChinaVietnam
GuatemalaIndiaPeru
Puerto RicoDominican Republic
TanzaniaZimbabwe
GreeceKazakhstan
South AfricaNigeriaTurkey
Sri LankaRussia
RomaniaColombiaSlovakiaEcuador
MalawiSaudi Arabia
EgyptGhana
MoroccoThailand
VenezuelaUkrainePanama
Costa RicaMalaysia
CubaHungaryPortugal
SpainZambiaMexico
BrazilChile
PolandJordan
ArgentinaLithuania
ItalyCzech Republic
UruguayUganda
IsraelNetherlands
MongoliaHong Kong
DenmarkFinland
BelgiumJapan
SwitzerlandUS
South KoreaAustriaSweden
FranceTaiwan
SingaporeNorwayCanada
New ZealandIreland
GermanyUK
Australia
1.34.0
11.511.611.612.8
17.918.819.619.721.021.322.122.322.523.024.425.125.825.927.027.527.928.830.031.031.333.834.034.435.135.436.136.337.139.539.839.841.641.641.741.942.142.342.643.245.446.247.449.449.450.751.351.552.252.654.0
57.559.661.162.162.462.6
66.067.569.470.271.271.471.671.672.274.075.578.0
81.486.187.988.2
92.3
807978
=76=76
75747372717069686766656463626160595857565554535251504948474645
=43=43=41=41
403938373635343332
=30=30
292827262524232221201918171615141312
=10=10
987654321

32 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
Figure 3.2: Availability of specialised palliative care workers5 4 3 2 1
Therearesufficientspecialisedpalliativecareprofessionals,includingdoctors,nurses,psychologists,socialworkersetc.Voluntaryworkersshouldhaveparticipatedinacourseofinstructionforvoluntaryhospiceworkers.Thespecialistpalliativecaretrainingforthecorecareteamisaccreditedbynationalprofessionalboards.
Thereisanadequatenumberofspecialisedpalliativecareprofessionals,butinsomesupportfunctions(psychologists,socialworkersetc),thereareshortages.Specialistpalliativetrainingisaccreditedbynationalprofessionalboards,butthiscanbeinconsistentattimes.
Therearespecialisedpalliativecareprofessionalsbutthereareshortagesofphysicians,nursesandothersupportstaff.Specialistpalliativecaretrainingisgenerallynotaccreditedbynationalprofessionalboards.
Thereisashortageofspecialisedpalliativecareprofessionals,andaccreditationofspecialistpalliativecaretrainingisnotthenorm.
Thereisasevereshortageofspecialisedpalliativecareprofessionalsandaccreditationisnon-existent.
Australia UK Austria Netherlands Argentina Lithuania Botswana Myanmar Bangladesh Iraq
Germany Belgium NewZealand Brazil Mexico China Nigeria Bulgaria Philippines
Canada Norway Chile Mongolia Colombia Panama Iran
Finland Singapore CostaRica Morocco Dominican Peru
France SouthKorea Cuba Poland Republic PuertoRico
HongKong Sweden Czech Portugal Ethiopia Romania
Ireland Switzerland Republic Spain Ghana Rusia
Italy Taiwan Denmark Thailand Greece SaudiArabia
Japan US Ecuador Uganda Guatemala Slovakia
Egypt Ukraine India SouthAfrica
Hungary Uruguay Indonesia SriLanka
Israel Venezuela Jordan Tanzania
Kazakhstan Turkey
Kenya Vietnam
Malawi Zambia
Malaysia Zimbabwe
health.“There’snospecialistpalliativecareofficiallyrecognisedbyuniversitiesandmedicalsocieties,”shesays.“Wealsoneedtohavedifferentlevelsoftraining—oneisspecialised;theotherisforthefamilydoctors,sotheycanprovidepalliativecareaspartofprimarycare.Thatisnotthereyet,althoughtherearesomeinitiativestotrytomoveinthatdirection.”DrYanneoagrees.“Perhapsthegreatestdeficiencyinthiscountryisthelackofadvancededucationinthediscipline,”hesays.
Forsome,thepriorityshouldbetostartincludingpalliativecareinthebasiceducation
ofeverysinglehealthprofessional.“Itmighttakealongtimetomakethechange,”saysDrPayne.“Butifeveryonehaspalliativecareintheirbasiceducation,thennoonewillcomeoutnotunderstandingpainmanagement,howtocommunicatewithpatientsandfamiliesorthatpsychological,socialandspiritualcarearepartofpalliativecare,notanoptionalextra.”
IntheUS—whichfallsoutsidethetop10inthiscategory,atposition14—medicalschoolsshouldberequiredtotraindoctorstoassessandtreatpainandtocommunicatemoreeffectively

33 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
withpatientsandfamiliesabouttreatmentdecisions,arguesDrByock.Hebelievesacademicinstitutionsshouldbetestingdoctorsontheseskillsaspartofgainingtheirmedicaldegrees.
“Butthey’vemadeonlyincrementalimprovementsinmedicaltrainingandeducationoverthepast10years,”hesays.“Therehavebeensomeimprovementsbutthosearesmallcomparedtowhat’sneeded.”
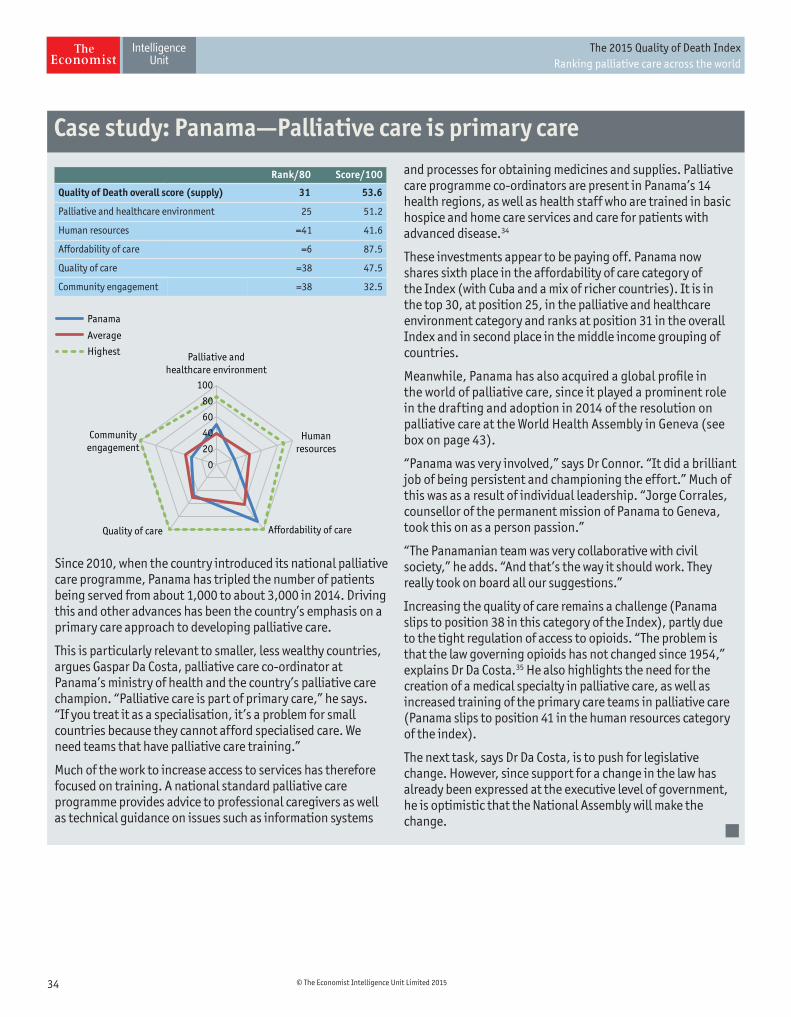
34 © The Economist Intelligence Unit Limited 2015
The 2015 Quality of Death Index Ranking palliative care across the world
Since2010,whenthecountryintroduceditsnationalpalliativecareprogramme,Panamahastripledthenumberofpatientsbeingservedfromabout1,000toabout3,000in2014.Drivingthisandotheradvanceshasbeenthecountry’semphasisonaprimarycareapproachtodevelopingpalliativecare.
Thisisparticularlyrelevanttosmaller,lesswealthycountries,arguesGasparDaCosta,palliativecareco-ordinatoratPanama’sministryofhealthandthecountry’spalliativecarechampion.“Palliativecareispartofprimarycare,”hesays.“Ifyoutreatitasaspecialisation,it’saproblemforsmallcountriesbecausetheycannotaffordspecialisedcare.Weneedteamsthathavepalliativecaretraining.”
Muchoftheworktoincreaseaccesstoserviceshasthereforefocusedontraining.Anationalstandardpalliativecareprogrammeprovidesadvicetoprofessionalcaregiversaswellastechnicalguidanceonissuessuchasinformationsystems
andprocessesforobtainingmedicinesandsupplies.Palliativecareprogrammeco-ordinatorsarepresentinPanama’s14healthregions,aswellashealthstaffwhoaretrainedinbasichospiceandhomecareservicesandcareforpatientswithadvanceddisease.34
Theseinvestmentsappeartobepayingoff.PanamanowsharessixthplaceintheaffordabilityofcarecategoryoftheIndex(withCubaandamixofrichercountries).Itisinthetop30,atposition25,inthepalliativeandhealthcareenvironmentcategoryandranksatposition31intheoverallIndexandinsecondplaceinthemiddleincomegroupingofcountries.
Meanwhile,Panamahasalsoacquiredaglobalprofileintheworldofpalliativecare,sinceitplayedaprominentroleinthedraftingandadoptionin2014oftheresolutiononpalliativecareattheWorldHealthAssemblyinGeneva(seeboxonpage43).
“Panamawasveryinvolved,”saysDrConnor.“Itdidabrilliantjobofbeingpersistentandchampioningtheeffort.”Muchofthiswasasaresultofindividualleadership.“JorgeCorrales,counsellorofthepermanentmissionofPanamatoGeneva,tookthisonasapersonpassion.”
“ThePanamanianteamwasverycollaborativewithcivilsociety,”headds.“Andthat’sthewayitshouldwork.Theyreallytookonboardalloursuggestions.”
Increasingthequalityofcareremainsachallenge(Panamaslipstoposition38inthiscategoryoftheIndex),partlyduetothetightregulationofaccesstoopioids.“Theproblemisthatthelawgoverningopioidshasnotchangedsince1954,”explainsDrDaCosta.35Healsohighlightstheneedforthecreationofamedicalspecialtyinpalliativecare,aswellasincreasedtrainingoftheprimarycareteamsinpalliativecare(Panamaslipstoposition41inthehumanresourcescategoryoftheindex).
Thenexttask,saysDrDaCosta,istopushforlegislativechange.However,sincesupportforachangeinthelawhasalreadybeenexpressedattheexecutivelevelofgovernment,heisoptimisticthattheNationalAssemblywillmakethechange.
Case study: Panama—Palliative care is primary care
Rank/80 Score/100
Quality of Death overall score (supply) 31 53.6
Palliative and healthcare environment 25 51.2
Human resources =41 41.6
Affordability of care =6 87.5
Quality of care =38 47.5
Community engagement =38 32.5
Palliative andhealthcare environment
Humanresources
Affordability of careQuality of care
Communityengagement
Panama
Average
Highest
0
20
40
60
80
100