thank you for joining! - healthcarefornewengland.org€¦ · thank you for joining! learning series...
TRANSCRIPT
Thank You for Joining!
Learning Series 2: Improving Dementia Care New England Nursing Home Quality Care Collaborative
Webinar Will Begin Shortly.
Call-In Number: (888) 895-6448
Access Code: 5196001
12/17/2015 1

Learning Series 2: Improving Dementia Care
New England Nursing Home Quality Care Collaborative
(NENHQCC)
Webinar #1
Melissa Miranda, Nursing Home Regional Lead
Margie McLaughlin, MA, Consultant Director of Education for
Healthcentric Advisors and Senior Director of Quality Improvement
at the American Health Care Association [email protected]
Lynn McNicoll, MD, FRCPC, AGSF, Healthcentric Advisors,
Associate Professor of Medicine, Alpert Medical School of Brown
University [email protected]
This material was prepared by the New England Quality Innovation Network-Quality Improvement Organization (NE QIN-QIO), the Medicare Quality Improvement Organization for New England, under
contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy
CMSQIN_C2_201512_0331
December 17, 2015
11:00 am – 12:00 pm
Today’s Objectives: Participants will be able to…
03/24/15 3
Explain the process of identifying a problem, getting to the root cause, and creating a process improvement plan.
Describe components of great dementia care.
Identify key concepts of keeping and growing their staff.
Determine the most likely reasons residents are on antipsychotic medications and recall the steps to implement changes.

573 Nursing Homes Thank you For Participating!
03/05/15 4

Data You’re Receiving:
QIN-QIO Reports
12/17/2015 5
Readmissions
• Facility Readmission Report
• Other provided reports
• Hospital Reports
• Community Reports
Standard Analytic Report (SAR)
• Long-Stay and Short-Stay Quality Measures

New England Nursing Home Quality Care Collaborative:
Learning Series Topics/Timeline www.healthcarefornewengland.org
12/17/2015 6
Series 1: Transitions of Care
Series 2: Improving Dementia Care
Series 3: Improving Your Quality Measures
Series 4: Reserved - Topics to Support Current Issues
Series 5: Reserved - Topics to Support Sustainability
April – November 2015
December 2015 – August 2016
September 2016 – May 2017
June 2017 – February 2018
March 2018 – June 2019
New England Nursing Home Quality Care Collaborative:
Learning Series 2: Improving Dementia Care www.healthcarefornewengland.org
12/17/2015 7
Module 5: Approaches to Maximize Quality of Life
Module 4: Individualize Care
Module 3: Keeping & Growing Your Staff
Module 2: Reducing Antipsychotic Drug Use
Module 1: Critical Elements of Dementia Care
Module 10: Sleep & Falls in Relation to Antipsychotic Drug Use
Module 9: Habilitation Therapy
Module 8: Creating A Therapeutic Environment
Module 7: Improving Mobility
Module 6: Workplace Practice to Enhance Care

Learning Series 2: Mark Your Calendar!
12/17/2015 8
December 17, 2015, Regional Webinar
February 11, 2016, Regional Webinar
April 14, 2016, Regional Webinar
June 9, 2016, Regional Webinar
August 11, 2016, Virtual Outcomes Congress

Important Opportunity!!!
• Prevent Clostridium difficile infection (C.
difficile/ C. diff / CDI)
• Using QAPI approach
• Partnering with the CDC through tracking
• Timeline: Begins in March 2016
• Don’t miss out!!!
12/17/2015 9

THE HOLISTIC APPROACH TO
DEMENTIA CARE
Learning Series 2: Module 1 – Critical Elements of Dementia Care
Margie McLaughlin, MA, Consultant Director of Education for
Healthcentric Advisors and Senior Director of Quality Improvement at the
American Health Care Association

It’s NOT about the drugs!
It’s NOT about finding the right “non-
pharmacological intervention.”
It IS all about well-being!
What it’s all
about . . .
All behaviors are
simply a means of
communication . . .
What are people
communicating?
What it’s all
about . . .
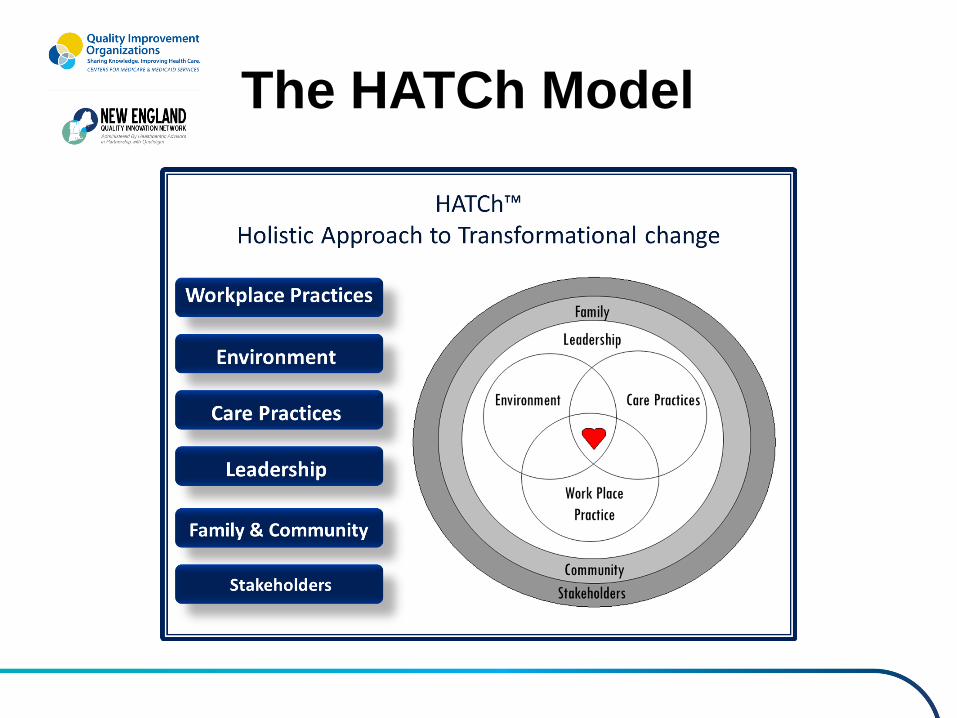
The HATCh Model
What workplace practices contribute
positively to the care of people with
dementia?

Workplace Practice-
As a person with dementia I need :
• A stable staff
• Skilled Staff –“Specialists”-people truly skilled in dementia care with proven competencies
• The same person to care for me daily (familiarity/consistent assignment)
• Confidence and trust in the people who care for me
• A team of professionals who work together on my behalf: row in the same direction

What environmental practices contribute positively to the care of people
with dementia?
Environment
As a person with dementia I need:
• A home
• Safety (I won’t be harmed, get C. diff, get lost)
• Security (I trust the people who care for me; I am never scare; never forced)
• A calm, reassuring and therapeutic environment
• A setting that supports my strengths AND my deficits
• “Special” care not necessarily a special care unit
• A place where I can also rest and sleep

What care practices contribute
positively to the care of people with
dementia?

Care Practices
As a person with dementia I need :
• Only those medications that fully support my well-being
• People who anticipate my needs
• People who watch for clues about my habits and routines
• People who provide for my comfort as well as stimulation
• My dignity-in living and in dying
• To feel useful and have meaningful things to do
• The type of support that keeps me strong and healthy
• To be connected with my family and friends and the things that have always been important to me
• Celebrations and rituals

What leadership practices contribute
positively to the care of people with
dementia?
Leadership
As a person with dementia I need :
As a person with dementia I need:
• A leader who has a vision to transform this workplace into my home
• Leaders who can create a great environment where I can thrive
• Engaged leaders who are working to make life better for me and the staff
• Leaders who have a close relationship to the work and are on the scene
• Leaders to listen to my family/friends and staff

What family & community practices contribute positively to the care of
people with dementia?
Family and Community
As a person with dementia I need :
• Contact and exposure to the people and
places that I love
• My family/friends voice to be heard and
kindness given them
• My family and friends to be included in the
life of the home.

What stakeholders practices contribute
positively to the care of people with dementia?

Stakeholders
As a person with dementia I need :
• You to understand the impact your
decisions have on me care
• You to appreciate the toll this is taking on
my family
• Policy makers to budget based on my
needs
Chapter 2
Reducing Antipsychotic
Drugs
• Philosophy of care focused on well being
• Being fluent in Alzheimer’s
• Drug free/minimal
• Reduced Noise
• Shift Change
• Redefined “activity”
• A process to enhance sleeping & waking
• Restructured bathing
Creating a
Therapeutic
Environment

ANCHORING YOUR ANTIPSYCHOTIC
DRUG REDUCTION PLAN WITH QAPI
QAPI: Applying the Process and Tools
03/05/15 27

Two views
Old School
• Recognize a problem
• Top Down
• Implement a change
• Deal with the consequences
• Hit or miss success
New World
• Data indicates a weakness
• Collaborative
• Consider the possibilities based on best known practices
• Work the process for best outcomes
• Succeed!
03/05/15 28

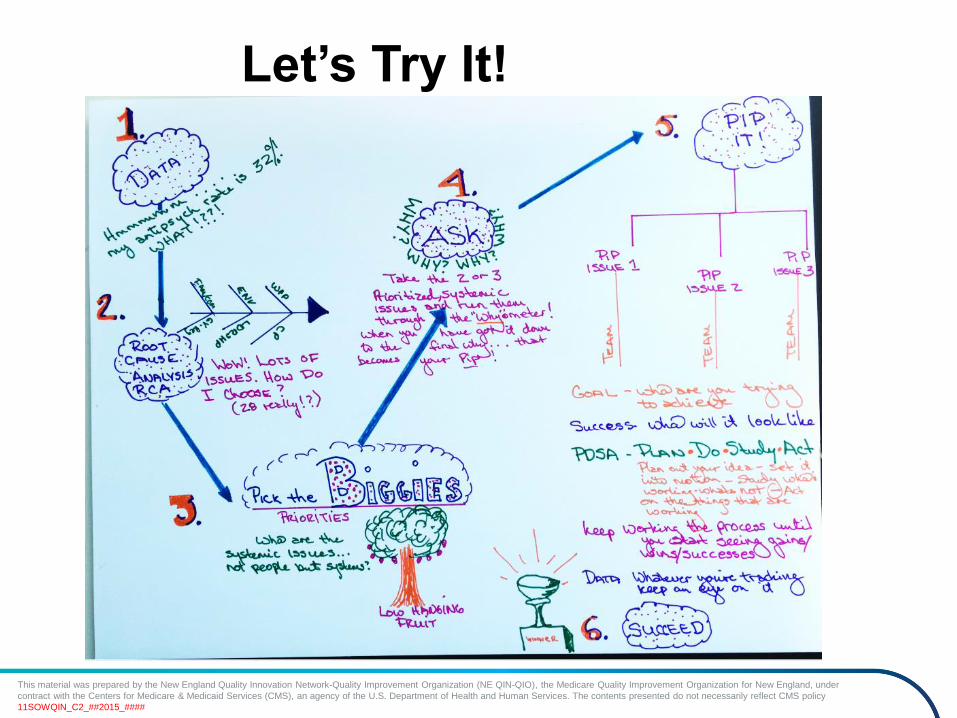
The Formal Process
• Data>
>Root Cause Analysis
>Prioritize
>ASK- why? Why? WHY?
>PIP IT
>Succeed
03/05/15 29

This material was prepared by the New England Quality Innovation Network-Quality Improvement Organization (NE QIN-QIO), the Medicare Quality Improvement Organization for New England, under
contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy
11SOWQIN_C2_##2015_####
Real Life Process
This material was prepared by the New England Quality Innovation Network-Quality Improvement Organization (NE QIN-QIO), the Medicare Quality Improvement Organization for New England, under
contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy
11SOWQIN_C2_##2015_####
Let’s Try It!

Real Life
12/05/15 32

The Resources are in Here to guide
Your Process
03/05/15 33

REDUCING ANTIPSYCHOTIC DRUG USE
Janice Lexton, DNP, RN-BC
Quality Assurance Nurse
Lutheran Home of Southbury, Southbury, CT
12/17/2015 34
Problem Identified
• High utilization of antipsychotic
medications in residents with dementia
• The Casper Report indicated a 23% use of
antipsychotic medications for long stay
residents (4/1/15-6/30/15)
• 27 residents were on this class of
medication

Root Cause Analysis
• Gradual Dose Reductions (GDRs) had not
been attempted in more than 6 months.
• No process to evaluate those residents on
an antipsychotic medication on a regular
basis.
• Staff unaware of facility statistics.
• Staff’s fear to change “what isn’t broken.”
12/17/2015 36
The Changes Made
• Moved from in the office morning report to
walking clinical rounds daily.
• Met monthly as an interdisciplinary team.
• Held staff meetings to disseminate the
plan and goals for improvement.
• Staff and family education key to success.
12/17/2015 37

The Changes Made
• Discussion of:
• Why the medication was in use and can a
GDR occur?
• Can the antipsychotic medication be
discontinued or changed to another class
of medication?

The Changes Made
• Reviewed the process of starting a new
antipsychotic medication before any MD
orders are obtained.
• Reviewed the process of medication
reconciliation on admission. Looking
closely at whether an antipsychotic
medication was started in the hospital.
12/17/2015 39
The Changes Made
• Use of non-pharmacological alternatives:
Music & Memory program
12/17/2015 40
The Results
• June 2015: 23% (27 residents)
• August 2015: 16.3% (19 residents)
• October 2015: 15% (18 residents)
• November 2015: 12% (14 residents)
• December 2015: 9.4% (11 residents)
State Average: 19.87%,
National Average: 18.7%
The Results
• Residents more alert, participating in
facility activities: walking program, rock
and rolling program.
• Staff proud of the achievements to date.
12/17/2015 42
Conclusion
• It takes a TEAM approach to succeed
• Slow and steady wins the race…
• Build on small successes: identify the “low
hanging fruit”
• Next steps:
Continue to reduce and eliminate the
remaining 11 residents on antipsychotics
with the use of personalized care
approaches.
REDUCING ANTIPSYCHOTIC
DRUG USE
Lynn McNicoll, MD, Consultant Physician Faculty for
Healthcentric Advisors and Associate Professor of Medicine
at Alpert Medical School of Brown University
12/17/2015 44
Learning Series 2: Module 2


The Problem of Dementia
In 2000, 5 million adults with dementia
In 2050, 13 million adults with dementia
Costs in 2010, $172 Billion
70% of adults with dementia die in nursing homes
42% of nursing home residents have dementia
Special Care Units may provide better care?
Variability in care prevails despite some standards – e.g. the underlying prescribing culture of a nursing home may determine if and what type of antipsychotic is prescribed

Between Scylla and Charybdis
Greek mythology proverb meaning “having to choose between two evils” Antipsychotics are bad,
benzodiazepines are no better and perhaps also antidepressants How do you weigh the impact on
the unit of aggressive and disruptive behavior over the risk to the individual? Most difficult dementia patients
end up in the nursing home

FDA
Use of antipsychotics to treat dementia and behavioral problems is NOT FDA approved
Why are antipsychotics BAD?
BLACK BOX WARNING: increases mortality likely from cardiovascular death and within 30 days
Increases risk for gait instability and falls
Metabolic syndrome (diabetes, weight gain)
Anticholinergic properties (constipation, urinary retention, etc.)
Dopaminergic properties (parkinsonism)
Tardive dyskinesia and neuroleptic malignant syndrome

Why are antipsychotics BAD? CATIE-AD trial – risperdal and olanzapine found
to have modest improvements in inappropriate behavior but high discontinuation rate due to side effects
Meta-analysis of 16 placebo-controlled trials showed increase death among those on antipsychotics (3.5% vs 2.3%)
Benzodiazepines have shown similar rate of increased mortality
Atypicals (second generation) may be better than typical (e.g. Haloperidol) antipsychotics

Potential Benefit of Antipsychotic Medications in Advanced Dementia
Reduce anxiety and behavioral problems in some limited residents with advanced dementia
Improve quality of life for some residents with advanced dementia with behavioral problems
Calmer and safer environment in dementia units
However, no robust evidence to support this use in the medical literature
There is much controversy!

Other Issues with Antipsychotics 17% had daily doses exceeding recommended levels
18% had both inappropriate indications and high dosing (Breisach, 2005)
Likelihood of a person with dementia getting antipsychotic was directly correlated with a NH antipsychotic prescribing rate, even after adjusting for confounder (Chen, 2010)
So facility and physician variation EXISTS
State to state variation EXISTS as well (Hawaii 13% to MA 28% using Q3 2012 data)

Medical Care 50(11);2012
TYPICAL
ATYPICAL

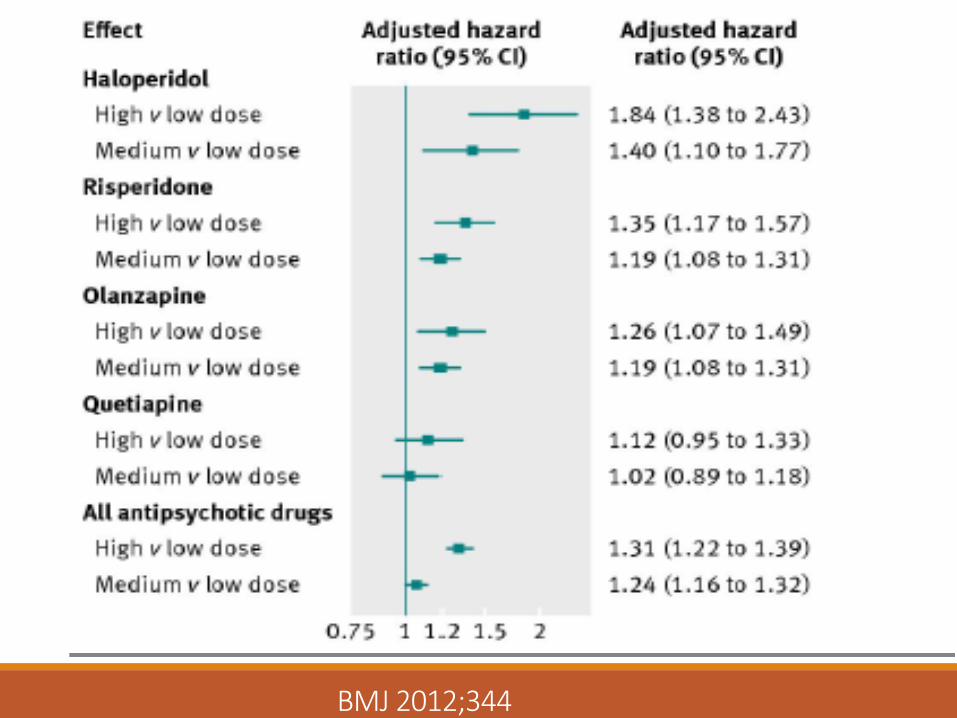
BMJ 2012;344
BMJ 2012;344
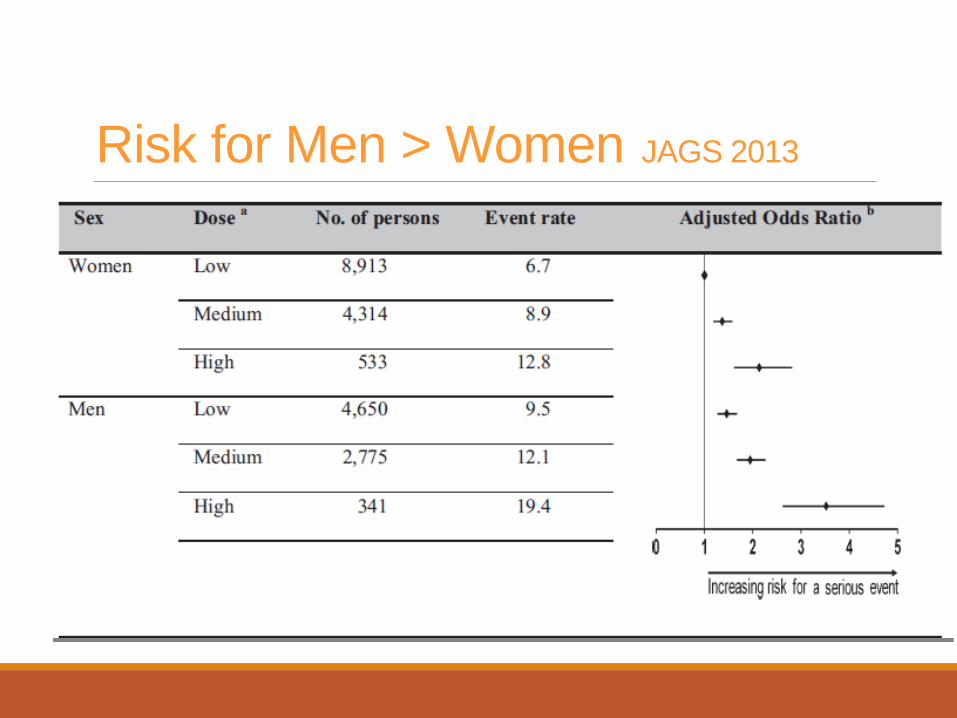
Risk for Men > Women JAGS 2013

Areas for Improvement in Dementia Care –> The Low Lying Fruit Residents with advanced dementia who are no
longer able to produce violent or aggressive behaviors
Use of antipsychotics for disruptive behaviors (crying, yelling) and not aggressive or dangerous behaviors
Use of antipsychotics for anxiety or depression without proper trial of SSRI or mood stabilizers or non-pharmacological strategies
The Low Lying Fruit Continued Continued use of antipsychotics started for
reversible episodes of delirium or psychotic depression Continued use of antipsychotics started prior to
nursing home admission Infrequently used PRN antipsychotics can
probably be discontinued Use for psychotic symptoms that are not
problematic to the patient (e.g. non-violent hallucinations)

Potential Unintended Consequences of Focusing on the Rate of Antipsychotic Use
If the medication has been successful in an individual patient and attempts at reduction have failed, stopping the medication may produce more harm than good
NH may start to refuse residents who are already on antipsychotics
More frequent ED referrals for agitation or behavior problems rather than addressing the issue internally
How to address this problem
KNOW YOUR DATA: Review all residents on antipsychotic medications for alternatives (pharmacological AND non-pharmacological)
Do NOT replace antipsychotics with benzodiazepines or other potentially equally harmful medications (e.g. trazodone)
Do NOT suddenly stop antipsychotics in residents who have been on the medication for a long time, consider a slow weaning trial (sudden withdrawal or rapid weaning can cause withdrawal psychosis)

How to address this problem
Learn proper strategies for holistic, individualized care of the resident with dementia e.g. HATCH model
Guideline-based multifactorial interventions have been proven to work
Work with you team including your pharmacists, physicians and consultants
Resources 1. Antipsychotic Reduction Resident Prioritization Tool
2. Hand in Hand from CMS
3. Nhqualitycampaign.org
4. NE QIN-QIO website ◦ http://www.healthcarefornewengland.org/

Conclusions The goal should always be to provide dementia care
without antipsychotics – the goal should be 0%
There are always opportunities to improve antipsychotic rates
Improving the education, approach and culture towards antipsychotic use is essential to reduce antipsychotic medication rates

Thank you – Questions?

References 1. Huybrechts et al. Differential risk of death in older residents in
nursing homes prescribed specific antipsychotic drugs. BMJ 2012;344
2. Aparasu et al. Risk of death in dual-eligible nursing home residents using typical and atypical antipsychotic agents. Medical Care 2012; 50(11);961.
3. Gellad et al. Use of antipsychotics among older residents of VA nursing homes. Medical Care 2012;50(11);954.
4. Huybrechts et al. Variation of antipsychotic treatment choice across US nursing homes. Journal of Clinical Psychopharmacology. 2012;32(1);11-7.

References 5. Huybrechts et al. Risk of death and hospital admission for major
medical events after initiation of psychotropic medications in older adults. CMAJ 2011;183(7);411.
6. Cadigan et al. The quality of advanced dementia care in the nursing home: the role of special care units. Medical Care 2012;50(10);856.
7. Kopke et al. Effect of guideline-based multicomponent intervention on use of physical restraints in nursing homes: a randomized control trial. JAMA 2012; 307(20);2177.
8. Rochon et al. Older men with dementia are at greater risk than women of serious events after initiating antipsychotic therapy. JAGS 2013;61;55.
KEEPING & GROWING YOUR
STAFF
Learning Series 2: Module 3 – Staff Stability
Margie McLaughlin, MA, Consultant Director of Education for
Healthcentric Advisors and Senior Director of Quality Improvement at the
American Health Care Association

Staff Stability
• Turnover has a significant effect on quality
• Centers frequently review turnover data but infrequently realize how much money is associated with that figure.
• Example: A nursing home choosing between operating at the 25th percentile versus the 75th percentile of turnover, i.e. between 38% and 78%, would experience a cost saving of $668,252.
Why this is
Critical?
How much!!??
The costs of turnover in nursing homes
Dana B. Mukamel, Ph.D., Professor and Senior Fellow, William D. Spector, Ph.D, Senior Social Scientist, Rhona Limcangco, Ph.D., Ying Wang, M.S., Zhanlian
Feng, Ph.D., Assistant Professor, and Vincent Mor, Ph.D., Professor & Chair
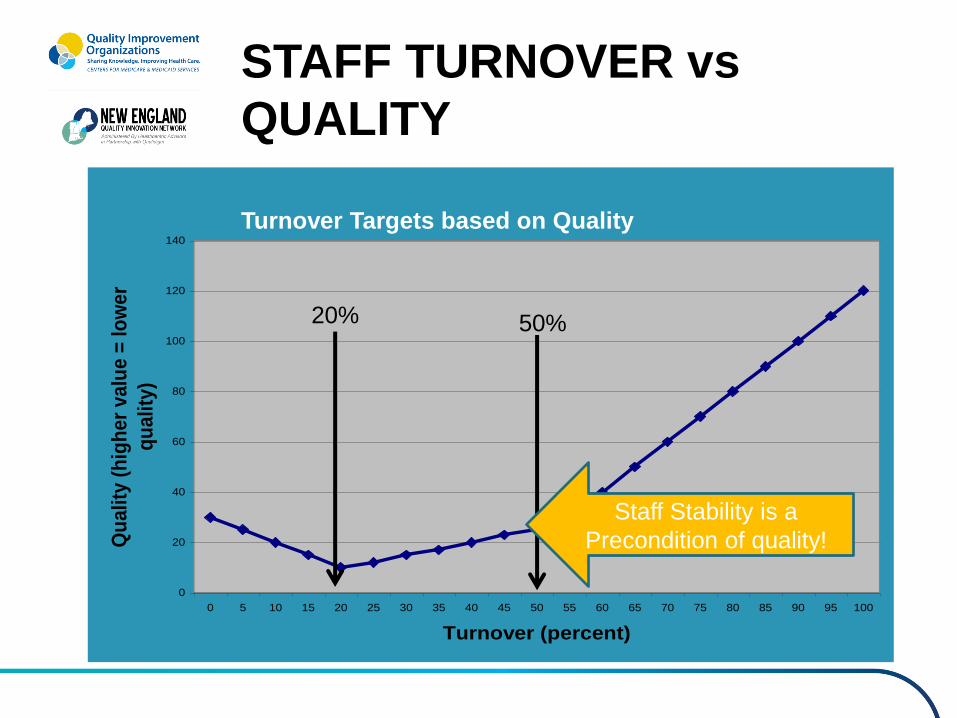
STAFF TURNOVER vs
QUALITY
Figure 1: Hypothesized Quality-Turnover Relationship
0
20
40
60
80
100
120
140
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 95 100
Turnover (percent)
Qu
ali
ty (
hig
he
r v
alu
e =
lo
we
r
qu
ali
ty)
Turnover Targets based on Quality
50% 20%
Staff Stability is a
Precondition of quality!
Increased Turnover =
Decreased Quality
• Contractures
• Physical restraints
• Catheter use
• Pressure ulcers
• Psychoactive drugs
• Quality of care deficiencies
Castle, et al 2006
Increased Turnover =
Decreased Quality
• CNA’s report the task neglected when short staffed:
• Range of Motion
• Hydration
• Feeding
• Bathing
Castle, et al 2000

Study of High & Low
Turnover Homes
• From the work of Susan C.
Eaton
• Recognized five essential
elements that dominated
low turnover organizations

What a difference management makes! Five Management Practices Associated with
High Retention, Attendance and Performance
High quality
leadership at
all levels of
the
organization
Valuing staff
day-to-day in
policy and
practice, word
and deed
High
performance,
high
commitment
HR policies
Work systems
aligned with
and serving
organizational
goals
Sufficiency
of staff and
resources
to care
humanely
Eaton, 2002

Next Steps
• Identify at least one QAPI Opportunities
– Complete the QAPI Self Assessment
• Access learning modules on QAPI and other topics to get started or to re-educate your staff – not just clinical staff!
– www.healthcarefornewengland.org
– Watch for Series 2 Modules, Jan 2016
• Call your state team to learn about affinity groups in your area and/or to talk through your QAPI plans…
12/17/2015 74

03/05/15 75
Contact your Nursing Home
Quality Improvement State Lead
03/05/15 76
• Connecticut
Florence Johnson:
• Maine
Sharon Emerson:
• Massachusetts
Sarah Dereniuk:
• New Hampshire
Pamela Heckman:
• Rhode Island
Nelia Silva Odom:
• Vermont
Gail Harbour:
Care Transitions Regional Lead
Nursing Home Regional Lead