temporomandibular joint degeneration in alport's syndrome
TRANSCRIPT

Temporomandibular Joint Degeneration in Alport'sSyndrome: Review of Literature and Case Report
David GIngrass, DDSAssistant ProfessorDepartment of Oral
and Maxillofacial SurgeryMedical College of WisconsinMilwaukee. Wisconsin 53226
A case of Alport's syndrome and coincidental temporomandibularjoint degenerative disease is reported. Aiport's syndrome is anunusuai genetic disease that uitimateiy resuits in renai failure andhas a high incidence of sensorineurai hearing loss. The patient pre-sented had complaints of facial and joint pain that mimicked whatis currently termed temporomandibular disorder, includingheadache, tinnitus, joint pain, and temporal swelling. The signifi-cance of renal osteodystrophy is briefly reviewed as it pertains tothis dinical presentation. The clinician must be alert to the manypotentiai causes of degeneration of the temporomandibular joint,one of which may be metabolic in origin.J OROFACIALPAIN 1993;7:307-310.
A lport's syndrome comprises progressive hereditary nephritiswith sensory neural bearing loss. Described in 1927 byAlport, the exact mechanism that destroys the kidney
remains unclear, although a defect in the glomeruiar basementmembrane bas heen suggested.'"* The inheritance of the syndromeis unclear as well, hut it is most commonly described as being auto-somal dominant. There is a male predominance, with end-stagerenal failure being reached when the patient is between 20 and 40years of age.
Tbe first symptom is usually hematuria, often appearing in child-hood, coupled with proteinuria. The usual course is one of slowdeterioration of renai function. The sensorineurai hearing loss mayoccut at any age, and it primarily affects the high tones and is pro-gressive. A spectrum of ocular dysfunction has been reported,which includes perinuclear anterior Ienticonus, perimacular andretinal flecks, and possibly arcus juveniles." Finally, thrombocy-topenia has heen reported to be somewhat common.'
Case Report
A 46-year-old white woman was referred to the Oral andMaxillofacial Surgery Department by her otorhinolatyngologist forevaluation of "TMJ syndrome." The patient's chief complaint wasone of facial and jaw pain. In particular, the pain was located overthe temporomandibular joints (TMJs) with radiation to the angleof the mandible. The facial pain was accentuated with chewing andeating. The patient also complained of swelling on both sides of herhead and associated temporal headaches.
Her past history demonstrated a diagnosis of Alport's syndromeat age 25, with chronic dialysis-dependent renal failure, bilateral
Journal of Orofaciai Pain 307

Gingrass
sensorineural hearing loss, and ocular dysfunction,A familial patrern has been demonsrrated, as hersister ha.s the same disease to some degree.
Clinical examination demonstrated that theskull was increased in irs overall size and that therewas mild patchy alopecia. The patienr's glassescaused skin indentarions in the temples bilaterally.Hearing was decreased to rhe poinr where rheexaminer had ro repeat many of the clinical ques-tions and speak in excessively loud tones. TheTMJ examination showed thar the verrical openingwas approximately 50 mm, without deviarion. Softcrepitus was presenr upon palpation over the leftTMJ, with mild pain. The right TMJ did notdemonstrate significant pain or noise, Lareral andprotrusive excursions were essentially normal.Oral examinarion revealed 1- to 2-mm apertog-
Fig ] Waters view of skull showingincreased radiopacity.
nathia and excessive occlusal wear throughour.The dentition was otherwise in a good state ofrepair. Palpation of che facial musculature demon-strated bilateral atrophy of the temporaiis muscles,hut the remaining facial muscle examination wasunremarkable.
Radiologie examination included skull films anda panoramic radiograph. Skull films showed a clas-sic "salt and pepper" appearance with increasedradiopaciry of rhe calvarium {Fig 1). The panoram-ic radiograph showed radiopacity in the maxillaand mandible and loss of the lamina dura sur-rounding the dentition. The mandibular condyiesexhibited degenerative joint disease, with rhe ero-sion and pirting being worse on rhe left than theright (Fig 2).
Multiple diagnoses, including Alporr's syn-drome, renal osreodysrrophy, degenerative jointdisease, bruxism, and a skeleral malocclusion,were rendered.
Discussion
In our review of the literature, no case of TMJinvolvement has been reported with Alport's syn-drome. The incidence of degenerative TMJ istherefore unknown in rhis syndrome. The obviousunderlying pathology of Alport's syndrome is renalfailure and its associated systemic changes. Renalosteodysrrophy is a generic rerm used to describevarious osseous diseases in uremic parients. In1973, Sellers et al° reporred on two cases of condy-lar degeneration in which rhe patients were afflict-ed wirh severe renal failure and osteodystrophy.This appears to be the first report of condylardegeneration secondary to renal osteodystrophy.
Hg 2 Patioratnic: radiograph showing increased radiopacity and degenerationof mandibular condyles.
308 Volume 7, Number 3, 1993
Gingrass
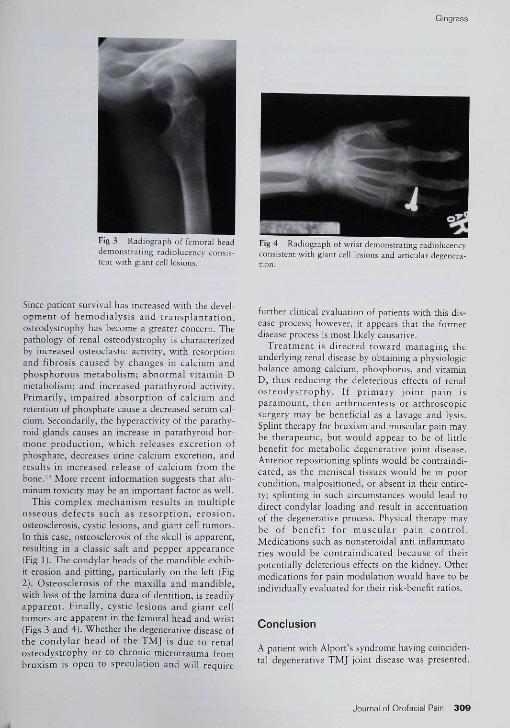
Fig 3 Radiograph of femoral headdemonstrating radiolucency consis-tent with giant cell lesions.
Fig 4 Radiograph of wrist demonstrating radiolucencyconsistent with giant cell lesions and articular degenera-tion.
Since patient survival has increased with the devel-opment of hemodialysis and transplantation,osteodystrophy has become a greater concern. Thepathology of renal osteodystrophy is characterizedby increased osteoclastic activity, with résorptionand fibrosis caused by changes in calcium andphosphorous metabolism; abnormal vitamin Dmetabolism; and increased parathyroid activity.Primarily, impaired absorption of calcium andretention of phosphate cause a decreased serum cal-cium. Secondarily, the hyperactivity of the parathy-roid glands causes an increase in parathyroid hor-mone production, which releases excretion ofphosphate, decreases urine calcium excretion, andresults in increased release of calcium from thebone."'' More recent information suggests that alu-minum toxicity may be an important factor as well.
This complex mechanism results in multipleosseous defects such as résorption, erosion,oste o sclerosis, cystic lesions, and giant cell tumors.In this case, osteosclerosis of the skull is apparent,resulting in a classic salt and pepper appearance(Fig 1). The condylar heads of the mandible exhib-it erosion and pitting, particularly on the left (Fig2). Osteosclerosis of the maxilla and mandible,with loss of the lamina dura of dentition, is readilyapparent. Finally, cystic lesions and giant celltumors are apparent in the femoral head and wrist(Figs 3 and 4|. Whether the degenerative disease ofthe condylar head of the TMJ is due to renalosteodystrophy or to chronic microtrauma frombruxism is open to speculation and will require
further clinical evaluation of patients with this dis-ease process; however, it appears that the formerdisease process is most likely causative.
Treatment is directed toward managing theunderlying renal disease by obtaining a physiologicbalance among calcium, phosphorus, and vitaminD, thus reducing the deleterious effects of renalosteodystrophy. If primary joint pain isparamount, then arthrocentesis or arthroscopicsurgery may be beneficial as a lavage and lysis.Splint therapy for bruxism and muscular pain maybe therapeutic, but would appear to be of littlebenefit for metabolic degenerative joint disease.Anterior repositioning splints would be contraindi-cated, as the meniscal tissues would be in poorcondition, malpositioned, or absent in their entire-ty; splinting in such circumstances would lead todirect condylar loading and result in accentuationof the degenerative process. Physical therapy maybe of benefit for muscular pain control.Medications such as nonsteroidal anti-inflammato-ries would be contraindicated because of theirpotentially deleterious effects on the kidney. Othermedications for pain modulation would have to beindividually evaluated for their risk-benefit ratios.
Conclusion
A patient with Alport's syndrome having coinciden-tal degenerative TMJ joint disease was presented.
Journal of Orofacial Pain 3 0 9

Gingrass
This patient's symptoms were similar to those ofother individuals who complain of pain and dys-function in the area of the TMJ, The examiningpractitioner should he aware of the primary under-lying defect in Alport's syndrome of end-stagerenal disease, and that renal osteodystrophy mayproduce a spectrum of osseous changes, includingfrank degeneration of articular surfaces, which willalter conventtonal treatment protocols.
References
1, Yoshikawa K, Ito 11, Matsuyama S, Hazikano 11, Okada S,Matsuo T, Hereditary nephritis in children with and with-out characterisric glomecular basement membrane alter-ations, CIm Nephrol 1988;30:122-127,
2, Grunfeld JP, Charbonneau R, Grateau C, Noel LH,Alport's syndrome and related hereditary nephropathies,ContrNephrol 19SS;Ê1:32-9O,
3, Cecil R, Renal diseases. In: Beeson PB, McDermott W,Wyngaarden JB (eds). Textbook of Medicine, ed !5 ,Philadelphia: Saunders, 1979;1316-1462,
4, Setala K, Ruusuvaara P, Alport syndrome with hereditarymacular degeneration. Acta Oph thai mol 1989;67:409-^14,
5, Thomas HS, Bauer JH, Hereditary nephritis, deafness andthrombocytópenla. Mo Med 1984;8l(ál:305-307,311,
6, Sellers A, Winficld AC, Massry SG, Resorption o! condy-loid process of mandible. Arch Intern Med 1973;13 l(May|:72 7-728,
7, Fournier A, Sebert JL, Moriniere P, Grégoire 1, de FremontJF, Tahiri Y, et al. Renal osteodystrophyí Pa tho physio logyand treatment. Hormone Res T984;2n:44-5S,
S, Giovannctti S, Barsotti C, Crer?. N, Krafr K, Treatment andprevention of uremic csteodystrophy, Conrr Nephrol 1589;72:66-72,
Resumen
La Degeneración de la Articulación Temporomandibularen el Síndrome de Alport
Se reporta el caso de un paciente afectado por jn Síndrome deAlport y por la enfermedad degenerativa de la articulación tem-poromandibular El síndrome de Alport es una enfermedad genéti-ca inusual que finalmente produce una falla renal y trene una inci-dencia alta de sordera neurosensorial. El paciente se quejaba dedoior en la cara y en ia articulación, el cual imitaba la los síntomasque se alribuyen cornentemerte a los desórdenes temporo-mandibulares, incluyendo las cefaleas, tinitus, dolor articular y lahinchazón temporal. Se describe brevemente ei significado de iaosteodistrofia renal en lo que se refiere a esta presentación clíni-ca, Ei ciinico debe estar pendiente de ias numerosas causas quepueden producir la degeneración de la articulación temporo-mandibular, una de las cuales puede tener un origen metabólico
Zusammenfassung
Degenerative Veränderungen des Kiefergeletikes beimAlport' Syndrom: Literatur-Review und Fallpràsentation
Der Autor beschreibt einen Faii von Alport' Syndrom, einherge-hend mit der Degeneration des Kiefergelenkes. Das Alport'Syndrom ist eine seltene erbliche Erkrankung, die letïtendlichzum Nierenversagen und ztir Innenohrschwerhörigkeit fuhrenkann Die Patientin klagte über Gesichts- und Kiefergei-enksschmerzen, ähnlich wie sie bei einer Myoarthropathie desKausystems auftreten, ausserdem über Kopfschmerzen undtemporaie Schwellung, Die Bedeutung einer renalenOsteodystrophie wird erklärt. Der Kliniker muss bei degerieratlv-en Veränderungen des Kiefergelenkes auch an solchemetabolise he Ursachen denken.
A.NNOUNCEMENT
Graduate Program in Temporomandibular Disorders and Oroíacíal Pain
The Dep r̂tinent of Diagnostic and Surgical Sciences at the Univetsity of Minnesota is accepting applications for graduate training at a MS orPhD level in Temporomandibular Disorders and Orofaciai Pain, This program begins |uly 1 of each year and will provide participants withdidactic and clinical training in the diagnosis and management of acute and chronic temporomandibulat disorder and orofaciai pain prob-lems.
Each student is required to complete a series of courses designed to provide a background in the neurosciences, anatomy and pbysiolo-gy of the head and neck; the pathophysiology of chronic ororacial pain disorders; clinical techniques of evaluation, diagnosis, and man-agement of chronic orofaciai pain; and research melhodobëy. Through primary management of patients in the TM) and CraniofaciaiPain Clinic as well as clinical rotations in areas of medicine, dentistry, and psychology, the student gains a broad understanding of eval-uation and management of tbese disorders. In addition, a multideparlmental research project for an MS or PhD thesis is required.
The University of Minnesota is committed to the policy that all persons shall have equal access to its programs, facilities, andemployment without regard to race, religion, color, sex, national origin, handicap, or veterans status,Tbe interviews for applicants to this program are tentatively scheduled for November 12, 1993, If interested, pli-ase send s letter ofintent, curriculum vitae, and three letters of recommendation by October i , 1993 to:
]ames R, Fricton, DDS, MSUniversity of MinnesotaSchool of Dentistry515 SE Delaware Street6-320 Moos TowerMinneapolis, MN ,'55455