temporomandibular disorders and facial pain
TRANSCRIPT
TemporomandibularDisorders and FacialPain
he dentist is commonly perceived as the health care provider withthe most expertise in facial neuropathy, whether it is facial pain oraltered nerve function, as well as disorders of the temporomandib-
ular joints. Dentists receive extensive professional education in facial andtemporomandibular joint anatomy, physiology, and pathologic conditions.Painful disorders of the maxiilofaciai region, whether neurologic or muscu-losbeletal in origin, are common reasons for obtaining a dental opinion.Therefore it is important for dentists to become knowledgable about facialneuropathology and temporomandibular joint disorders,
Chapter 29 presents an overview of facial neuropathology. The neurophys-iology of pain, differential diagnosis of facial pain disorders, and methods ofmanaging various neurogenic facial pain problems are discussed. Then theevaluation and management of altered sensory nerve function arc considered,
lemporomandibular joint physiology and pathology is a broad topic, andentire, comprehensive books exist on this topic. Chapter 30 is a concise, up-to-date discussion of the ever changing field of temporomandibular joint disordersfrom the viewpoint of oral and maxiilofaciai surgeons. The chapter is designedto provide the reader with knowledge of the evaluation and management ofpatients with functional disorders of the temporomandibular joint, includinginternal derangements, ankylosis, and Immunogenic axthritides,
661
Facial Neuropathology
Steven Ganzberg C H A P T E R
CHAPTER OUTLINE
BASICS OF PAIN NEUROPHYSIOLOGYCLASSIFICATION OF OROFACIAL PAINSNEUROPATHIC FACIAL PAINS
Neuropathic Facial Pains Presenting as ToothacheTrigeminal NeuralgiaPretrigeminal NeuralgiaOdontalgia Secondary to Deaffe re rotation (Atypical
Odontalgfa)Other Neuropathic Facial Pains
Postherpetic NeuralgiaNeuroma
Burning Mouth SyndromeOther Cranial Neuralgias
CHRONIC HEADACHEMigraineTension-Type HeadacheCluster Headache
OTHER CHRONIC HEAD PAINS OF DENTAL INTERESTTemporal Arteritis (Giant Cell Arteritis)Indomethacin-Responsive Headaches
EVALUATION OF OROFACIAL PAIN PATIENT
he dentist is frequently called upon to diagnosepain in the oral and maxillofacial region.Although pain in Ihc mouth is most frequently of
odontogenic origin, many facial pains arise from othersources. The diversity of structures in the head and neckregion (e.g., eyes, ears, salivary glands, muscle, joints, sinusmembranes, intracranial blood vessels! can make arriving atan accurate diagnosis quite challenging, Even typicaltoothache symptoms may occur in a healthy tooth second-ary to referred pain or a damaged pain-try remission system.
BASICS OF PAIN NEUROPHYSIOLOGY
Pain is a complex human psychophysiologic experience.The sensory-discriminative aspect enables us to localizeand quantify the pain, but it should be appreciated thattrm unpleasant experience is influenced by such factorsas past experience, cultural behaviors, and emotional and
medical states. As the term implies, the pain experiencehas both psychologic and physiologic aspects. The phys-iologic aspects involve several processes: transductton,transmission, and modulation. The sum total of theseprocesses, when integrated with higher thought andemotional centers, yields the human experience of pain.Transduction refers to activation of specialized nerves,namely A-delta and C fibers, which transmit informationto the spinal cord, or in the case of the trigeminal nerve,to the trigeminal nucleus.
Table 29-1 lists peripheral nerve fibers and their individ-ual characteristics. Chemical, thermal, and mechanicalstimuli can activate the free nerve endings of nnciceptors,the peripheral nerves indicated previously that transmitpain information. Once in the central nervous system(CNS), information regarding pain is transmitted to thelhalamus and hence to cortical centers that process boththe sensory-discriminative and the emotional-affective
662
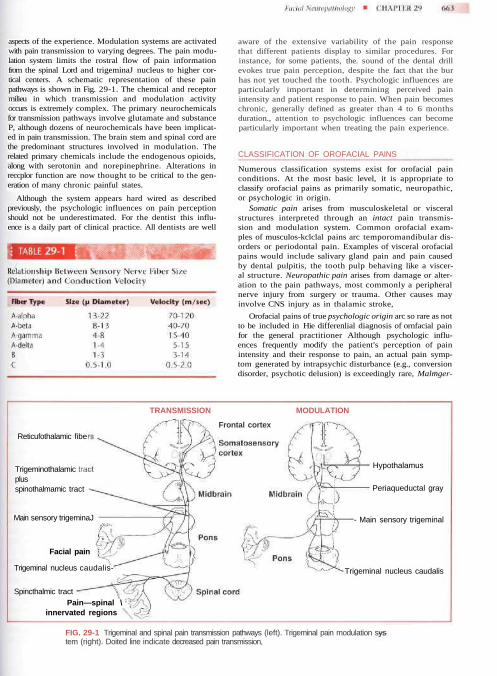
aspects of the experience. Modulation systems are activatedwith pain transmission to varying degrees. The pain modu-lation system limits the rostral flow of pain informationfrom the spinal Lord and trigeminaJ nucleus to higher cor-tical centers. A schematic representation of these painpathways is shown in Fig. 29-1. The chemical and receptormilieu in which transmission and modulation activityoccurs is extremely complex. The primary neurochemicalsfor transmission pathways involve glutamate and substanceP, although dozens of neurochemicals have been implicat-ed in pain transmission. The brain stem and spinal cord arethe predominant structures involved in modulation. Therelated primary chemicals include the endogenous opioids,along with serotonin and norepinephrine. Alterations inreccplor function are now thought to be critical to the gen-eration of many chronic painful states.
Although the system appears hard wired as describedpreviously, the psychologic influences on pain perceptionshould not be underestimated. For the dentist this influ-ence is a daily part of clinical practice. All dentists are well
aware of the extensive variability of the pain responsethat different patients display to similar procedures. Forinstance, for some patients, the. sound of the dental drillevokes true pain perception, despite the fact that the burhas not yet touched the tooth. Psychologic influences areparticularly important in determining perceived painintensity and patient response to pain. When pain becomeschronic, generally defined as greater than 4 to 6 monthsduration., attention to psychologic influences can becomeparticularly important when treating the pain experience.
CLASSIFICATION OF OROFACIAL PAINS
Numerous classification systems exist for orofacial painconditions. At the most basic level, it is appropriate toclassify orofacial pains as primarily somatic, neuropathic,or psychologic in origin.
Somatic pain arises from musculoskeletal or visceralstructures interpreted through an intact pain transmis-sion and modulation system. Common orofacial exam-ples of musculos-kclclal pains arc temporomandibular dis-orders or periodontal pain. Examples of visceral orofacialpains would include salivary gland pain and pain causedby dental pulpitis, the tooth pulp behaving like a viscer-al structure. Neuropathic pain arises from damage or alter-ation to the pain pathways, most commonly a peripheralnerve injury from surgery or trauma. Other causes mayinvolve CNS injury as in thalamic stroke,
Orofacial pains of true psychologic origin arc so rare as notto be included in Hie differenlial diagnosis of ornfacial painfor the general practitioner Although psychologic influ-ences frequently modify the patient's perception of painintensity and their response to pain, an actual pain symp-tom generated by intrapsychic disturbance (e.g., conversiondisorder, psychotic delusion) is exceedingly rare, Malmger-
Reticufothalamic fibe
Trigeminothalamicplusspinothalmamic tract
Main sensory trigeminaJ
TRANSMISSION MODULATION
Frontal cortex
Facial pain
Trigeminal nucleus caudalis-
Spincthalmic tractPain—spinal \ ;
innervated regions
Hypothalamus
Periaqueductal gray
- Main sensory trigeminal
Trigeminal nucleus caudalis
FIG. 29-1 Trigeminal and spinal pain transmission pathways (left). Trigeminal pain modulation system (right). Doited line indicate decreased pain transmission,

ing, a term used to identify behavior in which a patient con-sciously feigns illness or the extent of illness for personalgain, can and does occur, although the literature suggeststhat the incidence is low. However, a denial patient com-plaining of chronic pain should be presumed to have a realpain problem unless definitively proven otherwise.
The term atypical facia! pain is still seen in the litera-ture and used as a diagnosis primarily by physicians andsome dentists; therefore a medical diagnosis code (i.e.,ICD-9 code) is associated with it. When reviewing the lit-erature regarding atypical facial pain, a psychologic causeis frequently implied. Because true psychogenic pain isextremely rare, this term should be abandoned. For thoseundiagnosed facial pains, the appropriate term should befacial pain of unknown cause until a definitive diagnosishas been established. As a practical matter, these patientswill unfortunately continue to be labeled with the diag-nosis of atypical facial pain for coding purposes, but thedentist should he aware that this is a "diagnosis" awaitingfurther clarification.
This chapter covers neuropathic facial pains and com-mon headache disorders. Temporomandibular disordersare discussed in Chapter 30. A glossary of pain terminol-ogy is listed in Box 29-1.
NEUROPATHIC FACIAL PAINS
Neuropathic pains arise from an injured pain transmis-sion or modulation system. Surgical intervention or trau-ma Is frequently the cause. For example, trauma to theinfraorbital region may lead to numbness or pain in thedistribution of the infraorbital nerve. In oral and max-illofacial surgery, extraction of mandibular third molarscarries a slight but measurable risk of nerve damage to themandibular or lingual nerves. In the majority of theseeases, damage leads to parcsthcsla, an abnormal sensa-tion in the dermatome of the affected nerve. Typically.,this sensation is one of mild numbness or tingling. Lossof all .sensation may occur when the nerve is transected.In a subset of cases dysesthesiu, an abnormal, unpleasantsensation, can result; it is often described as a burning orsharp electric shocklike sensation. In fact, when a patientcomplains of burning or sharp shocklike pain in the faceor mouth, pain of neuropathic origin should be includedin the differential diagnosis. It should be appreciated thatthe oral cavity is the most common site of amputation, ifone recognizes amputations to include the teeth and thedental pulp (i.e., endodontics). As in phantom limb painafter extremity amputation, "phantom" sensations canalso arise, albeit more rarely, after dental and pulpal trau-ma or extraction. Neuropathic pains may also give rise tothe sensation of tooth pain, which often is a diagnosticdilemma for the dentist. It is customary to refer patientsfor management of these disorders to dentists focusingon orofacial pain diagnosis and management or to thepatient's personal physician or a neurologist.
Neuropathic Facial Pains Presenting as Toothache
Trigeminal neuralgia. The piototypic neuropathicfacial pain is trigeminal neuralgia (TN) (Box 29-2), liter-ally nerve pain arising from the trigeminal nerve.
tfbepaznttt(Vd
Although this could refer to any neuropathic pain oftrigeminal nerve origin, TN or "tic douloureux" (i.e.,painful tic) has specific inclusion criteria. Occurringmost frequently in patients over SO years of age (inci-dence 8:100,000; female-to-male ratio 1.6:1.0), TN usu-ally presents with sharp, electric shocklike pain in theface or mouth. The pain is intense, lasting for brief peri-ods of seconds to 1 minute, after which there is a refrac-ory period during which the pain cannot be reinitiatedor a period of time. At times, a background aching orurning pain is present. Usually a "trigger zone" is pres-nt where mechanical stimuli such as soft touch mayrovoke an attack. Firm pressure to the region is gener-lly not as provocative. Common cutaneous triggerones include the corner of the lips, cheek, a]a of theose, or lateral brow. Any intraoral site may also be arigger zone for TN, including the teeth, gingivae, orongue. Trigger zones in both the V2 and V3 distribu-ions are most common, after which they occur aloneand in decreasing order of incidence) in the V3, V2, andI distributions. The pain of TN illustrates an importantistinction of many neuropathic pains as opposed to
somatic pains—the lack of a typical graded response toincreasing stimulation.. If light stimulation produces apain response oul of proportion to the stimulus, a neu-ropathic process should be considered. This also holdstrue for pain that has a burning or electric shocklikcquality. Sometimes a background aching pain accompa-nies TN, making it quite difficult to distinguish from thepain of acute pulpitis or possibly periapieal periodontltis.Importantly, local anesthetic block of the trigger zonewill arrest the pain of TN for the duration of anesthesiaand sometimes longer, which can lead the dentist toascribe a "dental" cause to the pain complaint.
The cause of TN is not entirely clear, but the consen-sus of opinion is that pressure on the root entry zone ofthe trigeminal nerve by a vascular loop leads to focaldemyelination. This in turn precipitates ectopic or hyper-active discharge of the nerve. The site of demyelinationdetermines the trigeminal division involved and hencethe clinical presentation. Other diseases such as multiplesclerosis, tumors, and fyme disease can produce painsimilar to that produced by TN. The treatment of TN iseither medical or surgical. Medical treatment is generallyundertaken with anticonvulsants.
The classical medication for the condition is carba-mazepine,, but newer anticonvulsants (e.g., gabapenlin,oxcarbazepine) and the antispastic baclofen, are com-monly used as well. Table 29-2 lists commonly used TNand neuropathic facial pain medications. Many of thesemedications have significant, even life-threatening, sideeffects; therefore only dentists focusing on orofaeial paindiagnosis and management use them in dental practice.Surgical treatment includes microvascular decompressionof the offending vascular loop (so-called Janetta proce-dure), GatnmaKnife radiosurgery, percutaneous needleIhcrmal rhizotomy, or balloon compression of the rootentry zone. For the dentist the critical issue is recognizingTN so that un needed dental treatment or extraction isavoided. Unfortunately when the trigger zone is locatedin an intraoral, dental, or periodontal site, unnecessarydental treatment is quite common.
Pretrigiminal neuralgia. Although a rare condition,pretrigeminal neuralgia (Pre-TNJ has been recognized forquitt some time. The presenting condition is typically anaching dental [lain in a region where physical and radio-graphic examination reveals no abnormality. Local anes-thetic block of the tooth (or extraction site, if applicable)
ia
aiae
pa
f
mc
aolat
arrests pain for the duration of anesthetic action. It hasbeen demonstrated that a number of patients with thiscondition go on to develop typical TN symptoms (i.e.,sharp electric shock pains the area). Pre-TN responds tosimilar treatments as TN, beginning with anticonvulsanttherapy. To avoid unnecessary dental treatment, the den-tist must have a high index of suspicion for secondarydiagnoses for those pains that are inconsistent with phys-cal examination or do not respond in a predictable wayfter treatment. Clinical features of pre-TN are listed in
Box 29-3.Odontalgia secondary to deafferentatiori (atypical
odontalgia). Pain secondary to deaffcremation refers topain that occurs when there has been damage to thefferent pain transmission system- Usually this conditions secondary to trauma or surgery, including extractionnd endodontic treatment. By definition, extraction andndodontics are "dcaffcrcntating" because they both
involve amputation of tissue that contains the nerve sup-ly of a human structure, the tooth. Limb amputation isnother example of a "dcaffcrcntation" procedure. As
with phantom limb pain, a similar picture of oral deaf-erentation pain may occur, but only in a small subset of
patients are the symptoms severe enough to warranttreatment. These pains may be maintained by various
echanisms, some readily appreciated and others quiteomplex and not yet completely understood. Peripheral
hypcraclivity at the site of nerve damage is quite easilyunderstandable. At the site of dental alveolar nerve dam-ge, neuronal hyperactivity leading to persistent painccurs. In this form, the pain is frequently anested withocal anesthetic block. CNS hyperactivity can, however,lso be responsible for persistent pain experienced in theooth site. In this model, peripheral neural damage leads
to changes in the second-order nerve in the trigeminalnucleus that synapsed with the primary peripheral nod-ceptor. Changes occur centrally in which ongoing paintransmission to higher cortical centers can occur despiteminimal or even no peripheral input. Local anestheticblock does not arrest pain in this circumstance.
Additionally, patients may exhibit both forms of com-promise simultaneously (i.e., only a portion of pain maybe arrested by local anesthetic block). Sympathetic nerv-ous system activity has also been shown to augmentsome of these complex neuropathic processes. Clinicalfeatures of deafferentation pains are listed in Box 29-4.Interestingly, for many deafferentation pains, furtherperipheral surgical procedures frequently intensify symp-toms and lead to a broader area of perceived pain. If painsecondary to deafferentation is suspected, further surgicalprocedures-should be undertaken cautiously.
The key to recognizing all of these conditions, andavoiding unnecessary and potentially harmful denialtreatme.nl, frequently lies in obtaining an excellentdescription of the chief complaint, including quality ofpain, duration, alleviating factors and aggravating fac-tors. The history of the complaint and how the symp-toms have changed over time can also be quite valuable.A more complete discussion follows in ihc section onEvaluation of Orofacial Pain Patient.
Other Neuropathic Facial Pains
Although the following pains share common mecha-nisms with those discussed previously, it is appropriate tolist them separately, because they possess some uniquecharacteristics.
Postherpetic neuralgia. Postherpetic neuralgia (PHN)is a potential sequelae of herpes zoster infection. Shingles,or herpes zoster, may occur at any stage in a person's life.Herpes zoster is the clinical manifestation of the reactiva-tion of a lifelong latent infection with varicella zostervirus, usually contracted after an episode of chicken poxin early life. Herpes zoster occurs more commonly in laterlife and in imunocompromised patients. Each year inthe United States shingles strikes at least 850,000 people.Most are over 60 years of age. By age 85, 50% of peoplewill have had a bout. Of those who do, 60% to 70% will
develop P1TN. Varicella zoster virus tends To be reactivat-ed only once in a lifetime, with the incidence of secondattacks being less than 5%. PHN occurs after reactivationof ihc virus, which can lay dormant in the ganglia of aperipheral nerve. Most commonly this is a thoracic nerve,but approximately 10% to 15% of the time the trigeminalnerve is involved, with the VI dermatome affected inapproximately 80% of cases. When reactivated, the virustravels along the nerve and is expressed in that nerve'scutaneous dermatome. For a thoracic nerve, for example,the. patient develops a unilateral patch of vesicular erup-tion closely outlining the classical dermatome for thatnerve. In the ophthalmic division of the trigeminal nerve,the VI dermatome is outlined by rash. In the V2 or V3distribution, both intraoral and cutaneous expression iscommonly seen. The acute phase is quite painful but sub-sides within approximately 2 to 5 weeks. However, a suh-set of patients develops a deaf'farenlation pain that, as dis-cussed previously, can have peripheral, central, or mixedfeatures. The pain is typically burning, aching, or shock-like (consistent with a pain caused by a neuropathic con-dition). Treatment is undertaken with anticonvulsants orthe tricyclic or other antidepiessauts. Tramadol, a mildopioid with mild antidepressant effects, can be a. usefuladjunct. Local injection of painful sites, sympatheticblock, or both is sometimes of value. Most importantly,preventive treatment of PHN with antivirals, analgesics,and frequently corticosteroids very early after rash pres-entation can significantly reduce the expression of PHN,
A related condition, Ramsay Hunt Syndrome, is a her-pes zoster infection of the sensory and motor branches ofIhc facial nerve (VII) and in some cases the auditory nerve(VIII). Symptoms include facial paralysis, vertigo, deafness,and herpctic eruption in the external auditory ineatus
Neuroma. After peripheral nerve transeetion, theproximal portion of the nerve generally forms sprouts inan effort to regain communication with the severed dis-tal component. When sprouting occurs without distalsegment communication, a stump of ncuronai tissue,Schwann cells, and other neural elements can form. Thisstump, or neuroma, can become exquisitely sensitive toboth mechanical and chemical stimuli.
The pain is commonly burning or shocklikc. Fre-quently a positive Tinel's sign is present. In this test, tap-
CHAPTER 29
ping over the suspected neuroma produces sharp shoot-ing electric shocklike pain. Damage to the mandibular orlingual nerve after third molar surgery is another sourcefor neuroma formation. Some oral and maxillofacial sur-geons provide microneurosurgical treatment, which canbe beneficial for some patients.
Although it is difficult to predict which patients will ben-efit from nerve repair, It is clear that neurosurgical inter-vention should be accomplished within 3 to 6 months toimprove the likelihood of success. Again the commonalityof symptom presentation in multiple nerve injury modelssuggests the importance of eliciting the patient's descrip-tion of pain when facing a diagnostic dilemma.
Burning mouth syndrome. In this condition thepatient perceives a burning or aching sensation in all or partof the oral cavity. The tongue is the most frequentlyinvolved site. Perceived dry mouth and altered taste is com-mon. The cause is unknown but a defect in pain modula-tion may be the most promising theory. Most sufferers arepostmenopausal women, although hormone replacementtherapy does not consistently affect symptoms. Approxi-mately 50% of patients improve without treatment over a2-year period, indicating the importance of placebo-con-trolled trials when scientifically testing any treatmentmodality. The predominant treatment approach is wilhanticonvulsants or antidepressants, although neitheravenue, even in combination, shows consistent results.
Other cranial neuralgias. As with TN, any of the cra-nial nerves (CNs) with a sensory component appears capa-ble of a "neuralgic" presentation. The most common of theother CNs to present this way is the glossopharyngealnerve (IX). The presenting symptom is typically sharp,electric shocklike pain on swallowing with a trigger zone inthe oropharynx or the base of the tongue. Pain is usuallyexperienced in the throat or tongue but may be referred tothe lower jaw. The facial nerve (VII) has a small somaticcomponent on the anterior wall of the external auditorymeatus in which shncklike pains are experienced (some-times associated with symptoms of tinnitus, dysguisca, anddisequilibrium). The vagus nerve (X) also has the potentiallor neuralgic activity manifesting as pain in the laryngealregion shooting deep to the mandibular ramus or even tothe region of the MJ. Most often treatment of cranial neu-ralgias, like TN, involves the use of anticonvulsants; how-ever, in some cases intracranial surgery is necessary.
CHRONIC HEADACHE
Headache has many causes and is one of the most com-mon complaints made to the primary care physician.When headaches recur regularly, the majority will bediagnosed as one of the primary (no other cause)headaches: migraine, tension-type headache, or clusterheadache. Although most headaches are centered in theOrbits and temples, many may present in the lower halfof the face, teeth, or jaws.
Migraine
Migraine is a common headache afflicting approximately18% of woman and 8% of men. The first migraine
headache typically occurs in the teenage years or in youngadulthood taut may begin in very young children as well,before puberty, migraine occurs equally in both sexes.After puberty the ratio changes so that women are at leasttwice as likely as men to suffer with migraine. Migraineheadaches are unilateral in approximately 40% of cases.An "aura" may develop several minutes to 1 hour beforeheadache onset in approximately 4U% of patients. Theaura is a neurologic disturbance, frequently expressed asflashing or shimmering lights or a partial loss of vision.
Complicated auras may produce transient hemiparesis,aphasia, or blindness. Upwards of 8G% of migraineursdevelop nausea and photophobia (intolerance to light)during attacks. Migraines typically last A to 72 hours. TheInternational Headache Society (THS) criteria for migraineare listed in Boxes 29-5 and 29-6. Headache triggersinclude menstruation, stress, certain vasoactive foods ordrugs and certain musculoskeletal disorders that producepain in the trigeminal system (e.g., temporomandibular

disorders [TMDsJ). The mechanism for migraine headache,although not completely understood, appears to involveneurogenic inflammation of intracranial blood vessels sec-ondary to newotransmitlcr imbalance in certain brainstem centers. It is a referred pain process, and the intracra-nial vessel involved determines the site of perceived pain(e.g., the orbit, temple, jaw, vertex of the head). Preventivetreatment is directed at normalizing neuretransmitterimbalance with antidepressants, anticonvulsants, beta-blockcrs, and other drugs. Biofeedback and other therapiesare also helpful. Treatment of acute attacks is with the"triptans" (e.g., sumatriptan-Imitrex, zolmitriptan-Zomig,rizatriptan-Maxalt, naratriptan-Amerge, almotriptan-Axert), ergots, nonsteroidal antiinflammatory drugs(NSAIDs), opioid analgesics, antiemetics, and other agents.
For the dentist knowledge of migraine is important,because temporomandibular disorders may precipitate amigraine attack in a migraine-prone patient. Likewise,cervical spine and cervical muscular disorders may pre-cipitate migraine. It is also important for the dentist torecognize that cervical and masticatory muscle hyperac-tivity often occurs during a migraine headache. Migrainemay therefore be a perpetuating factor in some TMDs ora reason for misdiagnosis. Although toothache and jawpains are not a common expression of migraine, a num-ber of cases have been reported in the literature and areseen with some frequency by pain specialists. Whenmigraine is a cause of jaw or face pain, the key to thediagnosis is recognizing lhal nausea, sonophobia, andphotophobia are not accompaniments of masticatorymusculoskeletal disorders or jaw and tooth pain of den-tal origin.
Tension-Type Headache
Ihe majority of patients who report to the physician witha chief complaint of headache will be diagnosed withtension-type headache. The name can be misleadingbecause "muscle tension" or "tension from stress" is notalways present, either alone or in combination. Tension-type headache is common in the general population, andmost people will experience at least one tension-typeheadache at some point.
I .hronic tension-type headache is more common inwoman than men. The headache is generally bilateral. It isfrequently bitcmporal or frontal-temporal in distribution.Patients commonly describe their pain as though theirhead is "in a vice" or a "squeezing hatband" is around theirhead. Headache can occur with or without "pcricranialmuscle tenderness" (i.e., tenderness to palpation of themasticatory and occipital muscles). To be defined as chron-ic tension-type headache, symptoms must be presentgreater than 15 days per month. The HIS criteria lor ten-sion-type headache are listed in Treatment oftension-type headache is commonly with tricyclic or otherantidepressants. When tension-type headache occurs inmigraineuis, migraine treatments are usually beneficial.
Psychosocial factors arc often a contributing factorinfluencing tension-type headache. In this situation cog-nitive-behavioral and other psychologic therapies are fre-quently beneficial.
im
p
hml2mtapeL
For the dentist, it is important to distinguish tension-type headache from masticatory myofascial pain. Thiscan be confusing, because both conditions have similarsymptoms. It is significant that in myofascial pain, pres-sure to various head or neck muscles refers to the site ofhead pain, whereas in tension-type headache, pressureidentifies the site of pain. Importantly for either condi-tion, Identifying the site of pain does not always implythe source of pain. Additionally, in tension-typeheadache, pain does not proportionally increase withincreasing pressure to the headache site nor refer pain toother areas.
Cluster Headache
Cluster headache is an overwhelmingly unilateral headpain typically centered around the eye and temporalregions. The pain is intense, frequently described as aslabbing sensation (i.e., as if an ice pick was being driveninto the eye). Some component of para sympathetic over-activity is present (commonly lacrimation, conjunctiva]njection, ptosis, or rhinorrhea). Headaches last 15 to 180
inutes and may occur once or multiple times per day,commonly with precise regularity (e.g., awakening the
atient at the same time night after night). Theheadaches occur in "clusters" such that they may be pres-ent for some months and then remit for several monthsor even years. Alcohol ingestion consistently triggerseadache but only during cluster episodes. As opposed toost other chronic headaches, men are much more like-
y to suffer from cluster headache than women (Box
Box 29-7. 9-8). INS criteria are listed in Box 29-9. Treatment, as inigraine, is either preventive or symptomatic. Preventivereatment is accomplished with verapamil, lithium salts,nliconvulsants, corticosteroids, and certain ergot com-ounds. Symptomatic treatment is with "triptans,"rgots, and analgesics. Oxygen inhalation at 7 to 10/min may be an effective abortive treatment.

ing 70% of patients and is the presenting symptom in onethird of patients. Jaw claudication (i.e., increasing weak-ness and pain in the jaw or tongue with ongoing mastica-tion) may lead the patient to visit the dentist for diagno-sis. Any older patient reporting jaw or face pain not obvi-ously of odontogenic origin and whose symptoms suggesttemporal arteritis should be referred for an erythrocytesedimentation rate (ESR) test—a standard laboratoryblood test. Although a negative test does not rule out tem-
hita
t
poral arteritis, a significantly elevated ESR may help con-firm the diagnosis. A temporal artery biopsy may also beobtained, but again a negative test does not conclusivelyrule out the condition. Treatment is with high-dose corti-costeroids, frequently for many months, and early treat-ment is necessary to avoid blindness caused by extensionof the disease process to the ophthalmic artery.
Indomethacin-Responsive HeadachesA number of head pains respond primarily or exclusive-ly to the NSAID, indomethacin. One of these headaches,chronic paroxysmal hemicrania, is similar in presenta-tion to cluster headache, although the attacks are shortlived (lasting several minutes) and occur many times perday. Unlike cluster headaches, women are more oftenaffected than men. Again toothache may be the initialpresentation. Exertional headaches, as in weightliftingor during intercourse, may also produce intense, rapid-onset headache responsive to indomethacin. Hypnicheadache, waking the patient from sleep generally with-
Dentists must be aware that frequently clustereadache produces pain in the posterior maxilla, mimick-ng severe dentoalveolar pain in the posterior maxillaryeeth. The pain is frequently stabbing and intense,lthough background aching may occur. Unnecessary
dental therapy is, unfortunately, common. Common fea-ures can distinguish a toothache secondary to cluster
headache from a toothache produced by a dental problem:• Rapid emergence and discontinuation of symptoms
unlike typical toothache• Toothache precipitated by alcohol ingestion• Toothache accompanied by unilateral rhinorrhea or
other parasympathetic symptoms• Toothache that occurs with regular periodicity
OTHER CHRONIC HEAD PAINSOF DENTAL lNTEREST_____________________
Temporal Arteritis (Giant Cell Arteritis)Temporal arteritis, more properly termed giant cell arteritis,is literally an inflammation (i.e., vasculitis) of the cranialarterial tree that can affect any or all vessels of the aorticarch and its branches. The condition is most prevalent inthose over 50 years of age. The inflammation is secondaryto a giant cell granulomatous reaction. Polymyalgiarheumatica, the most common nonarticular rheumato-logic condition causing diffuse muscle inflammation, isfrequently a co-morbid condition. Dull aching or throb-bing temporal or head pain is a common complaint affect-
in 2 to 4 hours of sleep onset and lasting 15 minutes to3 hours, is frequently indomethacin responsive, buthypnic headache is not accompanied by symptoms ofparasympathetic overactivity.
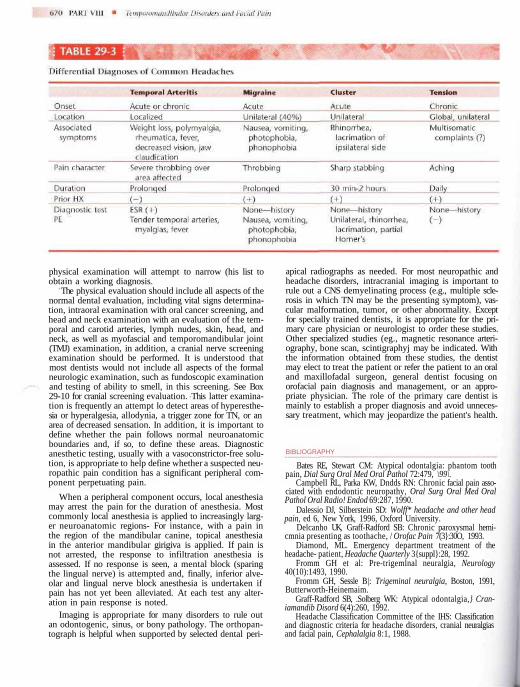
EVALUATION OF OROFACIAL PAIN PATIENTEvaluation of the dental patient who presents with jaw orface pain of nonodontogenic origin is an important skillfor the dentist to master. Obtaining an accurate history isthe most important component of information gathering.For chronic headache disorders and many neuropathicdisorders, such as TN, pre-TN, and other cranial neural-gias, as well as burning mouth syndrome, generally noabnormality is found on physical examination; thereforethe clinician must rely on the verbal history to arrive at anaccurate diagnosis. Chronic headache disorders based onsymptom description are presented in Table 29-3.
The pain history should include the chief complaint,including the current description of pain quality (e.g.,aching, throbbing, burning, shocklike, paroxysmal, orsome combination), intensity, when it occurs, how longit lasts, if it changes in character over time, precipitatingfactors, and alleviating factors. The history of the presentillness should include date of onset, circumstances sur-rounding onset, how the pain evolved over time, diag-nostic tests undertaken, diagnoses rendered, what treat-ments were instituted in the past, and the response tothose treatments. Finally, a comprehensive medical anddental history should be taken. Most commonly a shortdifferential diagnostic list can be made at this time. The
physical examination will attempt to narrow (his list toobtain a working diagnosis.
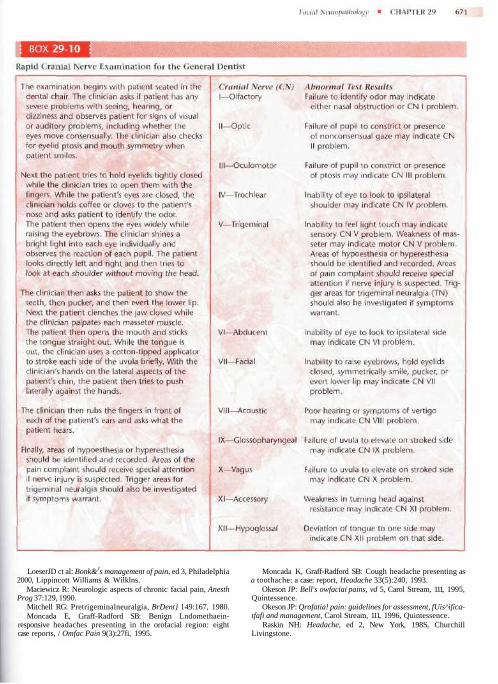
The physical evaluation should include all aspects of thenormal dental evaluation, including vital signs determina-tion, intraoral examination with oral cancer screening, andhead and neck examination with an evaluation of the tem-poral and carotid arteries, lymph nudes, skin, head, andneck, as well as myofascial and temporomandibular joint(TMJ) examination, in addition, a cranial nerve screeningexamination should be performed. It is understood thatmost dentists would not include all aspects of the formalneurologic examination, such as fundoscopic examinationand testing of ability to smell, in this screening. See Box29-10 for cranial screening evaluation. This latter examina-tion is frequently an attempt lo detect areas of hyperesthe-sia or hyperalgesia, allodynia, a trigger zone for TN, or anarea of decreased sensation. In addition, it is important todefine whether the pain follows normal neuroanatomicboundaries and, if so, to define these areas. Diagnosticanesthetic testing, usually with a vasoconstrictor-free solu-tion, is appropriate to help define whether a suspected neu-ropathic pain condition has a significant peripheral com-ponent perpetuating pain.
When a peripheral component occurs, local anesthesiamay arrest the pain for the duration of anesthesia. Mostcommonly local anesthesia is applied to increasingly larg-er neuroanatomic regions- For instance, with a pain inthe region of the mandibular canine, topical anesthesiain the anterior mandibular girigiva is applied. If pain isnot arrested, the response to infiltration anesthesia isassessed. If no response is seen, a mental block (sparingthe lingual nerve) is attempted and, finally, inferior alve-olar and lingual nerve block anesthesia is undertaken ifpain has not yet been alleviated. At each test any alter-ation in pain response is noted.
Imaging is appropriate for many disorders to rule outan odontogenic, sinus, or bony pathology. The orthopan-tograph is helpful when supported by selected dental peri-
apical radiographs as needed. For most neuropathic andheadache disorders, intracranial imaging is important torule out a CNS demyelinating process (e.g., multiple scle-rosis in which TN may be the presenting symptom), vas-cular malformation, tumor, or other abnormality. Exceptfor specially trained dentists, it is appropriate for the pri-mary care physician or neurologist to order these studies.Other specialized studies (eg., magnetic resonance arteri-ography, bone scan, scintigraphyj may be indicated. Withthe information obtained from these studies, the dentistmay elect to treat the patient or refer the patient to an oraland maxillofadal surgeon, general dentist focusing onorofacial pain diagnosis and management, or an appro-priate physician. The role of the primary care dentist ismainly to establish a proper diagnosis and avoid unneces-sary treatment, which may jeopardize the patient's health.
BIBLIOGRAPHY
Bates RE, Stewart CM: Atypical odontalgia: phantom toothpain, Dial Surg Oral Med Oral Pathol 72:479, \99\.
Campbell RL, Parka KW, Dndds RN: Chronic facial pain asso-ciated with endodontic neuropathy, Oral Surg Oral Med OralPathol Oral Radio! Endod 69:287, 1990.
Dalessio DJ, Silberstein SD: Wolff* headache and other headpain, ed 6, New York, 1996, Oxford University.
Delcanho UK, Graff-Radford SB: Chronic paroxysmal hemi-cmnia presenting as toothache, / Orofac Pain 7(3}:30O, 1993.
Diamond, ML. Emergency department treatment of theheadache- patient, Headache Quarterly 3{suppl}:28, 1992.
Fromm GH et al: Pre-trigemlnal neuralgia, Neurology40(10):1493, 1990.
Fromm GH, Sessle B|: Trigeminal neuralgia, Boston, 1991,Butterworth-Heinemaim.
Graff-Radford SB, .Solberg WK: Atypical odontalgia,} Cran-iamandib Disord 6(4):260, 1992.
Headache Classification Committee of the IHS: Classificationand diagnostic criteria for headache disorders, cranial neuralgiasand facial pain, Cephalalgia 8:1, 1988.
LoeserJD ct al: Bonk&Js management of pain, ed 3, Philadelphia2000, Lippincott Williams & Wilklns.
Maciewicz R: Neurologic aspects of chronic facial pain, AnesthProg 37:129, 1990.
Mitchell RG: Pretrigeminalneuralgia, BrDent} 149:167, 1980.Moncada E, Graff-Radford SB: Benign Lndomethaein-
responsive headaches presenting in the orofacial region: eightcase reports, / Omfac Pain 9(3):27fi, 1995.
Moncada K, Graff-Radford SB: Cough headache presenting asa toothache: a case: report, Headache 33(5):240, 1993.
Okeson JP: Bell's owfaciai pains, vd 5, Carol Stream, 111, 1995,Quintessence.
Okeson JP: Qrofatia! pain: guidelines for assessment, fUis^ifica-tfafi and management, Carol Stream, 111, 1996, Quintessence.
Raskin NH: Headache, ed 2, New York, 198Sr ChurchillLivingstone.