tecnología para niños con parálisis cerebral y otras discapacidades - dra. deborah gaebler
TRANSCRIPT

Technology for Children with Cerebral Palsy and other Disabilities
Deborah Gaebler-Spira
XIII International ORITEL Conference
Foundational and First General Assembly
of the Latin American Academy on Child
Development and Disability

Grant/Research SupportNIDRR,CPRR,CIHR
Allergan, Merz, CNS Therapeutics
Consultant Nothing to disclose
Speakers Bureau Nothing to disclose
Stock Shareholder Nothing to disclose
Other (identify) Nothing to disclose
Conflict of Interest Disclosures for
Deborah Gaebler-Spira

Rehabilitation Institute of Chicago
3

20121954 1964 1968 1974 2000 2001 2006 2010
RIC: Historical Perspective
4

• Gave examples of robotics
• RIC technology
• Across the ICF
• Give examples of available usable available technology
• Across ICF
Santiago Meeting --------Asunción Meeting
5

• Describe the forces that drive technology
• Identify how technology improves quantification of impairment or body structure and function-use of ultrasound
• Robotic gait technology-enhance for activities-lokomat
• Touch on a few substitution technologies-access to all-Go baby Go
Objectives

Vision has always been to create opportunities through technology
Technology — Vision and Reality

4 Reasons Driving Technology-Robotics
• Technology has the potential to more accurately quantify impairments
• control content and dose of therapy and measure clinical outcomes
• Increase practice-can deliver more therapy –improves cost benefit
• New innovative equipment and treatments-ENGAGE both child, parent’s and clinicians

Health Condition (disorder or disease)
Activities ParticipationBody Functions & Structures-quantification
Environmental Factors
Personal Factors
World Health Organization-International Classification of Function
Interactions between components of the ICF
9

• Physiologic functions of the body
• Anatomical parts of the body
Body Structure and Function
10

Function Depends On
• Interplay of body structure and function-impairments
• Strength, tone, SMC, balance-understanding each and quantifying allows us to target therapy programs
Parse individual deficits contributions

Ultrasonic Evaluation Medial Gastrocnemius
• Non-invasive method to quantify biomechanical properties
• Analyzed both passive and active muscle properties
12

Muscle Fascicle and tendon changes in CPUltrasonography and Biomechanical Evaluations
Soleus MTJCalcaneus
Achilles Tendon
Cross-sectional area ofAchilles Tendon
Proximal Distal Medial Lateral
M ed ia l G astrocn em iu s
M T J
F a s c ic le
A p o n e u ro s is
A t rest
5 cm

GS Fibers in Spastic Hypertonia
Fiber length & pennation
in spastic muscles
M ed ial G astrocn emiu s
M T J
F ascic le
Aponeurosis
N ormal
S troke
F ascic le
Aponeurosis
M T J
-40 -30 -20 -10 0 10 2040
50
60
70
80
NU00
Mu
scle
fib
er
len
gth
@ 5
cm
PF<-- Ankle angle --> DF
-40 -30 -20 -10 0 10 20
35
40
45
50
55
60
FLEX30
Mu
scle
fib
er
len
gth
@ 5
cm
PF<-- Ankle angle --> DF
-40 -30 -20 -10 0 10 20
30
35
40
45
50
55
FLEX60
Mu
scle
fib
er
len
gth
@ 5
cm
PF<-- Ankle angle --> DF
-40 -30 -20 -10 0 10 20
30
35
40
FLEX90
Mu
scle
fib
er
len
gth
@ 5
cm
PF<-- Ankle angle --> DF

Shear wave speed in plantarflexors of individuals with cerebral palsy
Sabrina S.M. Lee1,2, Deborah Gaebler-Spira1,2 , Li-Qun Zhang1,2, William Z. Rymer1,2, Katherine M. Steele3
1 Rehabilitation Institute of Chicago, Chicago, IL, USA2 Northwestern University, Chicago, IL, USA
3 University of Washington, Seattle, WA, USA

• 1) Passive stiffness, 2) neurally-mediated reflex stiffness, 3) active muscle stiffness
• Contracture
• Joint range of motion
• Interventions (e.g. bracing, lengthening surgeries)
Measuring muscle “stiffness”Why does it matter?

• Passive stiffness
– Qualitative measures, estimates of joint stiffness, or groups of muscles (De Vlugt et al., 2010; Roy et al., 2011; Sinkjaer et al., 1994; Katz et al., 1989)
• Elastography (e.g.Debernard et al., 2011; Muthupillai et al., 1995)
• Shear wave elastography (e.g. Bercoff et al.,
2004; Gennisson et al., 2005; Zhao et al. 2009)
Measuring muscle “stiffness” in vivo

Goal - evaluate and compare musclematerial properties
of the more-affected and less-affected limbs of individuals with hemiplegic cerebral palsy-hemiplegic-age ave 9
• Influence of
– muscle and fascicle length
– impairment level
– torque

0 11.5Shear wave velocity (m/s)
More- affected sideLess-affected side
Medial gastrocnemius

Sh
ear
wa
ve v
elo
city
(m
/s)
0
4
8
12
Individual subjects
S1 S2 S3 S4 S5 S6 S7 S8
GMFCS I GMFCS II
More-affectedLess-affected
MG- Maximum plantarflexion MG - Neutral
More-affectedLess-affected
MG - Maximum dorsiflexion
a) c)b)
S1 S2 S3 S4 S5 S6 S7 S8
GMFCS I GMFCS II
S1 S2 S3 S4 S5 S6 S7 S8
GMFCS I GMFCS II
0
4
8
12
0
4
8
12
More-affected side (MG): greater shear wave velocity
More-affected sideLess-affected side
(p = 0.024)14% greater
7/8
6/8
Neutral Dorsiflexion
Shea
r w
ave
velo
city
(m
/s)
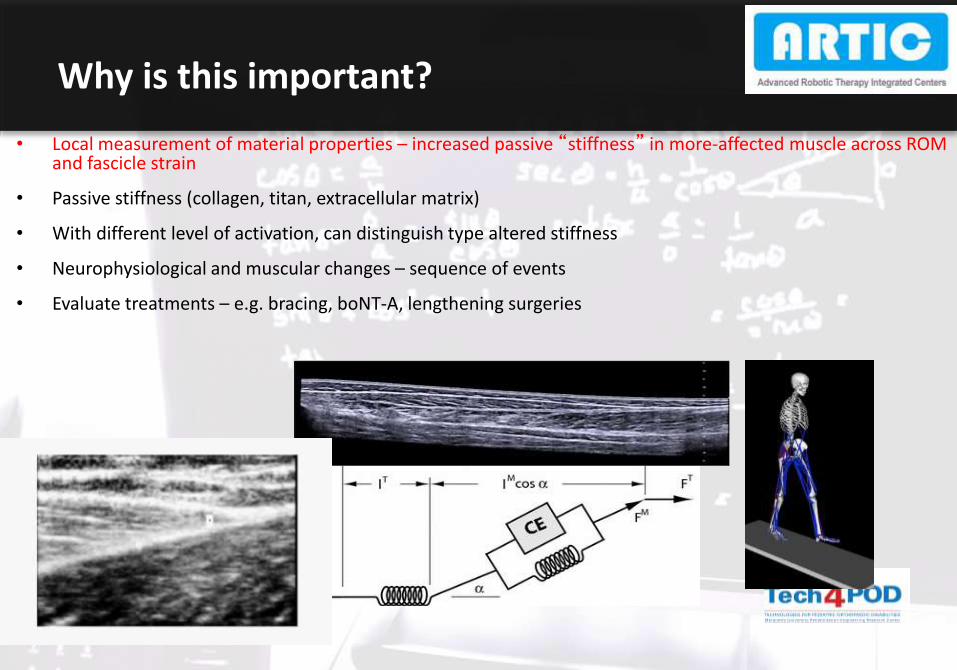
Why is this important?
• Local measurement of material properties – increased passive “stiffness” in more-affected muscle across ROM and fascicle strain
• Passive stiffness (collagen, titan, extracellular matrix)
• With different level of activation, can distinguish type altered stiffness
• Neurophysiological and muscular changes – sequence of events
• Evaluate treatments – e.g. bracing, boNT-A, lengthening surgeries
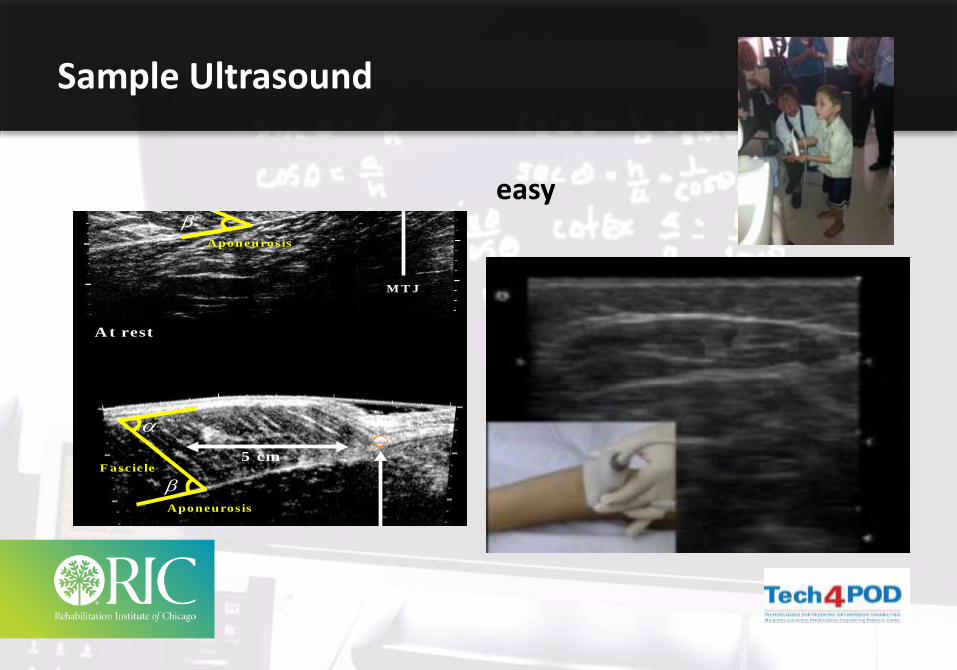
Sample Ultrasound
M ed ial G astrocn emiu s
M T J
F ascic le
Aponeurosis
A t rest
S timu lation
F ascic le
Aponeurosis
M T J
5 cm
5 cm
easy

Health Condition (disorder or disease)
Activities-motor learning
ParticipationBody Functions
& Structures
Environmental Factors
Personal Factors
International Classification of Function
Interactions between components of the ICF
23

Execution of a task or action by an individual
CP — walking, feeding , transfers, dressing-school work
Activities — backdrop of development
24

Technologies to address activities
• Activities Walkingtask-specific repetition, sensory feedback and feedback about performance are thought to enhance the effects of practice

• Lange observed 31 physical and occupational therapy sessions at 7 different settings
• Average number of repetitions of task specific , functional movement was 32
• Animal studies use 600 repetitions per session to induce plasticity
Can you increase practice at home?
Practice Intensity
26
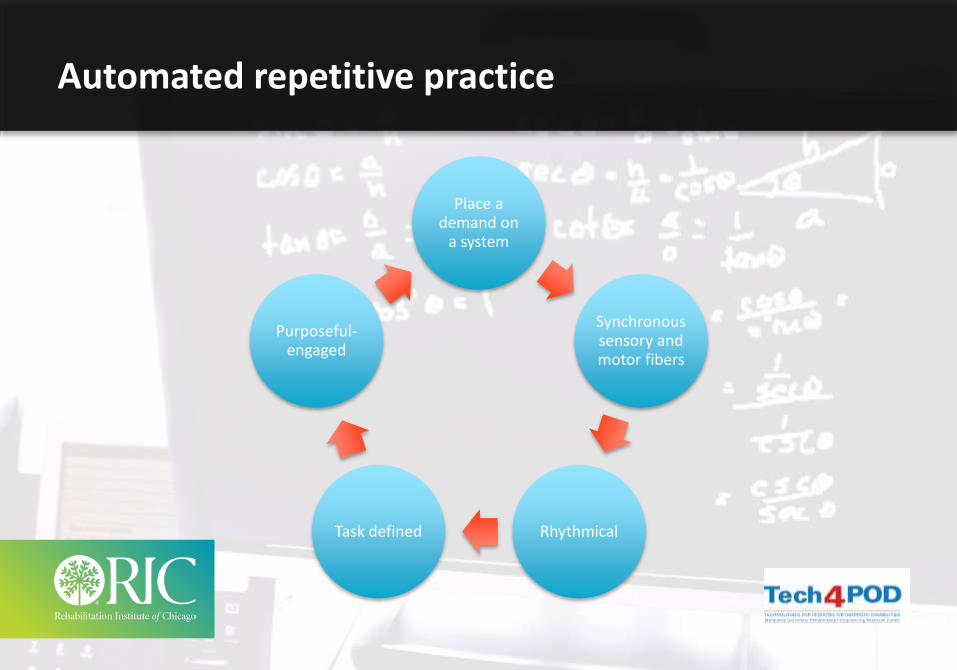
Place a demand on
a system
Synchronous sensory and motor fibers
RhythmicalTask defined
Purposeful-engaged
Automated repetitive practice

Goal — To Walk Further and Quicker, Participate in Playground
• N.R. — 6 y/o adopted, CP spastic diplegia, mild component of dystonia
• GMFC-3
• FMS-2,2,1
• Described as slow and wandering
• On oral baclofen 10 mg TID, artane 2 mg TID
• Hamstrings interfering, with stride length
• Botulinum toxin A to SM,ST 3 weeks prior

Lokomat training
29
3/week for 4 weeks20-40 minutes with Lokomat partial supported bodyweight

Results
• Pre
• 6 minute -97 meters
• 10 meters- 35 sec
• Gmfm-41
• Tripping-2-3
• Post
• 6 minute-155 meters
• 10 meters-26 sec
• Gmfm-41
• Tripping-0

• Lokomat with pediatric legs shared by adult/pediatric PT services
• 4 sessions/wk for 30-50minutes/session; 12 sessions/pt
• Since 2008 treated over 200+ pediatric patients with CP
• Gait training CPT code 97116
RIC Clinical Experience

RIC Outcomes Reveal
• BWSTT using Lokomat improved overall function, as measured by the 6 minute walk test and 10 meter walk test
• GMFM Domains (A/B/E) improved in GMFCS IV
• GMFM domains D/E approaching significance
• Motor ‘learning’ effect in children with cp participating in daily BWSTT –maintenance of effect after study completion
• Effects of TT better in higher level GMFCS patients
• UNCLEAR on role !

Practical Recommendations for use of Lokomat
33Aurich 2015 J of Neuropediatrics


• Training schedules highly variable
• positive outcomes GMFM-D,E
• Standing, walking speed, 10 meter walk distance 6 minute
• Most improvement in younger and engaged
• No adverse effects
• Questions still remain-Can we work together and contribute to the combined data base?
Literature to Support RAGT-5 studies
35

Artic Mission-possible collaboration
• Collect data to develop guidelines as well as to answer scientific questions with regards to the use of robotic devices in rehabilitation
• to improve patient outcome through a sophisticated use of the devices

DatabaseSimple looking for partners

Data Status
• 7 centers are already contributing data• 1 center has recently received IRB/Ethical approval• 2 centers are awaiting IRB approval• 1 center contributes administratively
Nu
mb
ers
in a
rro
ws
sho
w im
pro
vem
ent
fro
m M
arch
to
May
2
015

• Transfer of skills from TT to OG is ‘hardly definitive’
• BWS limits ‘dynamic’ trunk control
• Restricted degrees of freedom
• Altered gait dynamics and passive training ‘patterns’ limit skill acquisition
• Minimal to modest functional outcomes in ambulation
• Stroke literature points to importance of daily # steps and speed of TT
D. Damiano 11’; J. Moore 10’
What does the Literature ‘tell us’ about current RGT

Defining Levels of Activity
Tudor-Locke 2008, 2013

41
81 youth with CP, aged 10-13 years, GMFCS I to III (Bjornson et al. 2007)

42
Pedometers to sensors- to monitor steps
Unobtrusive Sensing and Wearable Devices-REAL WORLD DATA

Engagement-Participation

Health Condition (disorder or disease)
ActivitiesParticipation-Substitution
Body Functions & Structures
Environmental Factors
Personal Factors
International Classification of Function
Interactions between components of the ICF
44

Involvement of a life situation
Cp-home, -school, sports, arts
Participation-backdrop of culture and community

Rehabilitation
• Stem cell, influence environmental of the injured site (or prevent 2 damage)
• Plasticity-motor learningNeural
recovery
• The over exuberant non-injured pathways enlarge, IPS lateral pathways or “other slower” tracks take over
• Plasticity
Compensation
• Eye gaze, power chair, Brain computer interface — wireless technology
Substitution

Mind-controlled exoskeleton kicks off World Cup

The problem
• Self-produced mobility plays a crucial role in a child’s cognitive and psychosocial development (Piaget 1952, Erikson 1963, Paulsson and Christofferson 1984, Verburg et al. 1984, Butler 1986).
• linked to the development of spatial cognition, emotional skills, self-awareness, increased independence, and the emergence of new capacities to cope with environmental stressors.
• inability to move independently has a significant negative impact on cognitive, perceptual, and/or motor development (Zubek et al. 1963, Tatlow 1980, Brinker and Lewis 1982, Verburg 1987)

The problem
• Mobility devices such as motorized wheelchairs require a certain level of cognitive ability and maturity to operate
• When do is the child ready for a wheelchair?
• Wheelchairs introduced at school age
• Providing daily mobility between the ages of 1 and 5 is critical, given that significant learning, brain and behavioral development is dependent on mobility during this time.

The problem
• How much does a wheelchair cost? A LOT
• How much do they weigh? A LOT
• issues
– How often do you replace?
– Battery malfunction?
– Insurance approval?
– Slow response?
– Social issues?

The solution
• At the University of Delaware, Cole Galloway launched the GoBabyGo project in 2006 with Sunil Agrawal.
• Goal to provide mobility to kids who have trouble moving on their own.
• “Modifying off-the-shelf toy racecars to provide mobility to children with crawling and walking problems, empowering them to be part of the action at home, in the daycare center, and on the playground.”

Go baby Go

• "Interacting with kids and adults out in the world and gaining a little independence are crucial to early development. The disability no longer causes them to miss out on playtime or making friends—now they are able to participate. Other kids see the girl in the Barbie car and say, 'Wow, can I play with you?‘”
- Cole Galloway, PhD

• Consistent—
• Can create intermittent reinforcement
• Can program for perfect practice
• Can be fun and tied to gaming
• Can provide feedback precise to follow progress
• Open worlds
Robotics

The Promise of Recovery
• Parent’s perception of therapy is key, though studies and meta analysis do not support large changes in motor prognosis with current ongoing therapy, common experience is parent’s perceive MORE is better, and generally expect more
• Are the expected outcomes of technology at the same level as parental expectations

Before we had machines we had relationships