technological differences in energy wave & focal … brief tech intro.pdf · shockwave therapy...
TRANSCRIPT

Shockwave Therapy
Technological Differences in Energy Wave & Focal Zone Characteristics
between Modalities

First Use in Medicine
• Kidney stone lithotripsy – Mid 70’s
• Advent of minimally invasive medical technology.
• 10yr follow-up on patients found changes in: – MSK & Bone density.
– Considered for use in orthopaedic application
(Herr, 2008)

Type of Devices
Technology Used in Lithotripsy
• Electro-Hydraulic
– MediSpec
– Dornier
• Electro-Magnetic
– Siemens
– Storz
NOTE: Radial pulse is not used in lithotripsy Piezo-electric poor efficacy – Not used

Shockwave Characteristics A Shock Wave = A high-pressure amplitude with the following typical characteristics:
• Sharp impulse with pulse width of 1us (equivalent to 1 MHz)
• Rise time of approximately 40 nano seconds
• Peak pressure higher than 50 Bars
(Gerdesmeyer et al, 2004)

Shockwave Cavitation
Only True shockwave system generates cavitation, penetrating deeper to the treated area, yielding higher efficacy and better clinical results. (Weschel, 2004)
Cavitation bubbles occur directly after the pressure/tension alternating load of the shockwaves has passed in a water medium. Shock wave therapy causes fragmentation of calcium deposits into “crumb” and circulation slowly clears the site. (Gerdesmeyer, 2005, Craig & Miller 2011)
Note: Radial & piezoelectic devices CANNOT produce cavitation as it does not have a liquid medium
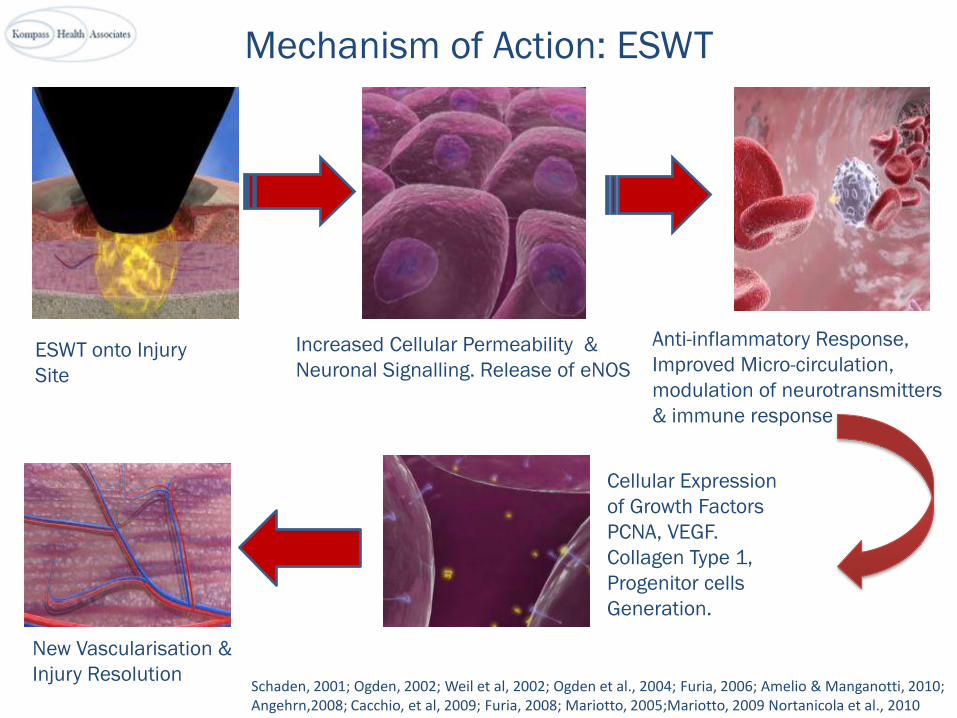
Mechanism of Action: ESWT
ESWT onto Injury
Site
Anti-inflammatory Response,
Improved Micro-circulation,
modulation of neurotransmitters
& immune response
Increased Cellular Permeability &
Neuronal Signalling. Release of eNOS
Cellular Expression
of Growth Factors
PCNA, VEGF.
Collagen Type 1,
Progenitor cells
Generation.
New Vascularisation &
Injury Resolution Schaden, 2001; Ogden, 2002; Weil et al, 2002; Ogden et al., 2004; Furia, 2006; Amelio & Manganotti, 2010; Angehrn,2008; Cacchio, et al, 2009; Furia, 2008; Mariotto, 2005;Mariotto, 2009 Nortanicola et al., 2010

Shockwave vs Radial Pulse
Therapy ESWT RWT
Penetration Depth 0-140 mm 0-35 mm
Pressure of Wave Relative To Time
Diagram of Pressure Wave Within Tissue
Pre
ssu
re
Time
Pre
ssu
re
Time
The Radial device (RWT) ie. dolorclast is a cheap alternative and is NOT a shockwave device.
Important Factors for Shockwave Generation
• Size of focal / therapy zone. Effects: – Number of shocks required per Tx.
– Region / area covered during each Tx.
– Impacts of Tx outcomes
• Electrode spacing gap (optimum gap 0.3mm) – Provides a uniform wave
– Bio-physiological impact on tissue
– Impacts Tx outcomes

The Device(S) We Use
• OrthoSpec – OR 3
• OrthoSpec – OR5
All devices are manufactured by MediSpec Ltd.

Small vs. Large Focus Zone
• Energy level up to 0.32/mm2
• Relatively even energy distribution throughout the Therapy Zone
• Does not require imaging (X-Ray or ultrasound) or anesthesia
Typical size at -6dB: Diameter 3mm Height 30mm ED = 0.4 mj / mm 2
Size at -6 dB: Diameter 26mm Height 96 mm ED = 0.29 mj / mm 2
Size at 5 MPa Therapy Zone: Diameter 46mm Height 134 mm ED = 0.20 mj / mm 2
Typical *ESWT System Small Focus Zone
Orthospec™ Large “Therapy
Zone™”
Imaging (X-Ray or ultrasound) and anesthesia are recommended
ED = 0.32 mj / mm 2
Typical size at 5MPa: Diameter 7mm Height 35mm
* Data provided to ISMST by various companies
OrthoSpec vs Other Devices

OrthoSpec Special Patents: 1
Allows for large focal therapeutic region due to unique reflector design combining and elliptical and ellipsoidal reflector

OrthoSpec Special Patents: 2
The Orthospec patented reflector uses both focused and unfocussed wave, resulting in better clinical efficiency

Penetration Depth: OrthoSpec vs Radial
CT Scan of gluteus mimimus region: penetration of focused ESWT (125mm) vs radial (dolorclast 30mm)

• This is why we chose the OrthoSpec Electro-hydraulic device after 18 months of testing all other devices.
• Better long term clinical outcomes and versatility.
ESWT in New Zealand
In 2000 Mr. Bruce Twaddle & I commenced investigation of shockwave devices. Devices tested:
• Reflectron (electro-magnetic) – HMT
• Dolorclast (pneumatic-radial) – EMS
• OrthoSpec OR3 (electro-hydraulic) – MediSpec
In 2002 Mr. Joe Brownlee investigated ESWT using
• Piezosone 100 (piezo-electric) - Wolf

Conclusion
• November 2002 the OrthoSpec was selected because of its superior Tx outcomes compared to the other devices. This is constant with international findings.
• Expertise and leadership of the manufacturer MediSpec in medical shockwave technology.
• Mr. Brownlee’s concluded that the piezo-electric device was ineffective, and did not proceed with it. This is constant with international findings.

Expansion of the Use of ESWT in Medicine

Advances in Shockwave Medicine • Cardiology (Vasyuk et al., 2010)
• Complex Ulcers (Schaden et al., 2007; Sagginni et al, 2008; Moretti et al., 2009;
Mittermyer et al, 2011)
• Erectile dysfunction (Yardi et al., 2010; Yardi et al., 2012; Gruenwald et al, 2012)
• Dystonia (Trompetto et al, 2009; Amelio et al., 2010)
• Neuropathy (Craig K & Walker M, 2012; Craig et al, 2011)
• Complex Pain (Nortanicola et al., 2009; Craig, 2011; D’Agostino et al, 2011; Craig K,
D’agostino, & Perez R., 2012)
Note: Radial & piezoelectric devices are NOT used in these areas.

Electrohydraulic Devices Across Disciplines
E3000 & EM1000 Extracorporeal Shock wave lithotripters
UROLOGY Cardiospec SWT for cardiac ischemic diseases
CARDIOLOGY
Orthospec Orthopedic Shock wave system
ORTHOPEDICS
ED1000 SWT for erectile dysfunction
VASCULAR

Reference
• Herr H. (2008). ’Crushing the Stone’: a brief history of lithotripsy, the first minimally invasive surgery. British Journal of Urology International, 102(4) 432 - 435.
• Schaden, W., Fisher, A. & Sailler, A. (2001). Extracorporeal Shockwave Therapy of Nonunion or Delayed Osseous Union. Clinical Orthopaedics and Related Research, 387; 90 – 94.
• Ogden, J. A., Alvarez, R. G. & Marlow, M. E. (2002). Shockwave Therapy for Chronic Proximal Plantar Fasciitis: A Meta Analysis. Foot and Ankle International 23 (4) 301 – 308.
• Ogden, J. A., Alvarez, R. G., Levitt, R. L ., Johnson, J. E. & Marlow, M. E. (2004). Electrohydraulic High-Energy Shock-Wave Treatment for Chronic Plantar Fasciitis. Journal of Bone and Joint Surgery 86-A (10) 2216 – 2228.
• Amelio, E. & Manganotti, P. (2010). EFFECT OF SHOCK WAVE STIMULATION ON HYPERTONIC PLANTAR FLEXOR MUSCLE IN PATIENTS WITH CEREBRAL PALSY: A PLACEBO-CONTROLLED STUDY. Journal of Rehabilitative Medicine 42 (4) 339 -343.
• Angehrn, F., Kuhn, C., Sonnabend, O. & Voss, A. (2008). Impact of extracorporeal shock waves on the human skin with cellulite: A case study of an unique instance. Clinical Interventions in Ageing, 3 (1) 175 – 182.
• Cacchio, A., Giordano, L., Colafarina, O., Rompe, J. D., Tavernese, E., Ioppolo, F., Flamini, S., Spacca, G. & Santilli, V. (2009). Extracorporeal Shock-Wave Therapy Compared with Surgery for Hypertonic Long-Bone Nonunions. The Journal of Bone and Joint Surgery, 91 2589 – 2597.
• Furia, J. P. (2008). Jigh Energy Extracorporeal Shock Wave Therapy as a Treatment for Chronic Non-insertional Achilles Tendinopathy. The American Journal of Sports Medicine 36(3) 502 – 508.
• Mariotto et al. (2005). Extracorporeal shock waves: From lithotripsy to anti-inflammatoryaction by NO production. Nitric Oxide, 12; 89 – 96.

• Mariotto et al (2009). Extracorporeal Shock Wave Therapy in Inflammatory Diseases: Molecular Mechanism that Triggers Anti-Inflammatory Action. Current Medicinal Chemistry, 16; 2366 – 2372.
• Gerdesmeyer et al. (2005). Effects of extracorporeal shockwaves. Ultrasound in Med. & Biol. 31(1) 115 – 119.
• Craig K & Miller, A (2011). ESWT an option for chronic tendinopathy management: a clinical perspective. New Zealand Pain Publication Summer 2011.
• Vasyuk, Y. A., Hadzegova, A. B., Shkolnik, E. L., Kopeleva, M. V., Krikunova, O. V., Iouchtchouk, E. N., Aronova, E. M. & Ivanova, S. V. (2010). Initial Clinical Experience With Extracorporeal Shock Wave Therapy in Treatment of Ischemic Heart Failure. Original Research.
• Schaden, W., Thiele, R., Kölpl, C., Pusch, M., Nissan, A., Attinger, C. E., Maniscalo-The berge, M. E., Peoples, G. E., Elster, E. A. & Stojadinovic , A. (2007). Shock Wave Therapy for Acute and Chronic Soft Tissue Wounds: A Feasibility Study, 143 (1) 1 – 12.
• Saginni R, Figus A, Troccola A et al. EXTRACORPOREAL SHOCK WAVE THERAPY FOR MANAGEMENT OF CHRONIC ULCERS IN THE LOWER EXTREMITIES. Ultrasound in Med. & Biol. 2008; 34( 8):1261–1271
• Moretti B, Notarnicola A, Maggio G, Moretti L, Pascone M et, al. The management of neuropathic ulcers of the foot in diabetes by shock wave therapy. BMC Musculoskeletal Disorders. 2009; 10:54
• Mittermayr R, Hartinger J, Antonic V, et al. Extracorporeal Shock Wave Therapy (ESWT) Minimizes Ischemic Tissue Necrosis Irrespective of Application Time and Promotes Tissue Revascularization by Stimulating Angiogenesis. Ann Surg 2011;253:1024–1032.
• Yardi, Y., Appel, B., Jacob, G., Massarwi, O. & Gruenwald, I. (2010). Can low-intensity Extracorporeal Shockwave Therapy Improve Erectile Function? A 6-Month Follow-up Pilot Study in Patients with Organic Erectile Dysfunction. European Urology, 58: 243 –248.

• Yardi et al., (2012). Does Low Intensity Extracorporeal Shock Wave Therapy Have a Physiological Effect on Erectile Function? Short-Term Results of a Randomized, Double-Blind, Sham Controlled Study. The Journal of Urology, 187; 1769 – 1775.
• Grunewald et al. (2012). Low-Intensity Extracorporeal Shock Wave Therapy—A Novel Effective Treatment for Erectile Dysfunction in Severe ED Patients Who Respond Poorly to PDE5 Inhibitor Therapy. Journal of Sexual Medicine 9; 259 – 264.
• Trompetto, C., Avanzino, L., Bove, M., Marinelli, L., Molfetta, L., Trentini, R. & Abbruzzese, G. (2009). External shock waves therapy in dystonia: preliminary results. European Journal of Neurology, 16 (4) 517 – 521.
• Craig, K. & Walker, M. (2012). Medical Shockwaves for the treatment of peripheral neuropathic pain in a Type II diabetic: a case report. New Zealand Pain Society Publication, Winter Issue, 7 – 16.
• Craig, K., D’Agostino, C., Poratt, D., Lewis, G. & Hing, W. (2012). Original Exploratory Case Study: Utilization of ESWT to Restore Peripheral Vibrosensory Perception in a non-Sensitive Type I Diabetic Foot. Paper Presented at the 15th International Society for Medical Shockwave Treatment Congress, Cartagena, Columbia. (Article in Press: Journal of Diabetes and Its Complications).
• Notarnicola, A., Moretti, L., Tafuri, S., Panella, A., Filipponi, M., Casalino, A., Panella, M. & Moretti, B. (2010). Shockwave therapy in the management of complex regional pain syndrome in medial femoral condyle of the knee. Ultrasound in Medicine & Biology, 36 (6) 874 – 879.
• Craig K (2011). Medical shockwaves a treatment option for complex and neuropathic pain syndromes? A compilation of case reports. Presented at the 32nd Australian/New Zealand Pain Conference, Wellington, New Zealand.
• D’Agostino C, et al. (2011). ESWT In Pillar Pain After Carpal Tunnel Release: A Preliminary Study. Ultrasound in Med & Biol, 37(10) 1603 – 1608.
• Craig K, D’Agostino C. & Perez R. (2012). ESWT for complex regional pain syndrome? A 52 week case-series follow-up. (Article in Press: European Journal of Pain).
