technical manual for the assessment of clinical skills
TRANSCRIPT
Technical Manual for the Assessment of Clinical Skills
2014

Technical Manual for the Assessment of Clinical Skills
Table of Contents
Introduction ......................................................................................................................................... 3
Policies and Procedures for the Assessment of Clinical Skills ...................................................... 4
Background and Overview ................................................................................................................. 5
History ............................................................................................................................................. 5
Purpose ........................................................................................................................................... 5
Certification ...................................................................................................................................... 6
Test Constructions Process and Validity Procedure while Preparing for the Assessment ............................ 9
Validity and Reliability Procedures during the Administration of the Assessment ..................................... 12
Validity and Reliability Procedures during the Evaluation Session ........................................................... 15
Grading Process ................................................................................................................................. 17
Appeals ............................................................................................................................................. 24
Attachment 1 – Assessment of Clinical Skills Protocol ........................................................................... 25
Attachment 2 – Summary of Act ......................................................................................................... 69
Attachment 3 – Competencies for a Beginning Dental Practitioner in Canada ......................................... 74
Attachment 4 – External Evaluation Procedures ................................................................................... 77
Attachment 5 – Publications................................................................................................................ 78
17E November 10, 2015 3 / 78
Introduction
The National Dental Examining Board of Canada (NDEB) was established by an Act of Parliament in 1952
with a mandate to establish the qualifying conditions for a national standard of competence for general
dentists and to issue certificates to dentists who successfully meet this standard. The Act was supported by
all ten provincial licensing authorities and by the Canadian Dental Association (CDA). Since that time, the
NDEB certificate has been accepted by provincial licensing authorities as evidence of having met the national
standard.
High-stakes examinations such as those conducted by the NDEB should be concerned with reliability and
validity because these measures are required in making pass/fail decisions affecting candidates for licensure
or certification. Protection of the public is of foremost concern and the NDEB has the obligation to inform its
ten provincial constituents that it is doing its best to provide the highest quality examination and assessment
program possible. Examination and Assessment policies and procedures provide a guide for the examination
and assessment program. Such policies and procedures assist with establishing and improving reliability and
validity. The Standards for Educational and Psychological Testing {American Educational Research
Association (AERA), American Psychological Association (APA), and the National Council on Measurement in
Education (NCME)} provides standards for testing organizations. This Technical Manual provides a
comprehensive summary of information pertaining to the examinations and assessments developed and
administered by the NDEB, and demonstrates the NDEB’s compliance with accepted international standards.

17E November 10, 2015 4 / 78
Policies and Procedures for the Assessment of Clinical Skills
17E November 10, 2015 5 / 78
Background and Overview
History
In 1906 under the auspices of The Canadian Dental Association (CDA) the Dominion Dental Council
was formed to conduct national written examinations, the successful completion of which would grant the
candidate a Dominion Dental Council certificate. The National Certificate could then be presented to the
Provincial Dental Regulatory Authorities (DRA’s) as evidence of the candidate's ability to meet a basic
national standard of competence. Some DRA’s were prepared to grant licenses to practice on the basis of
the certificate, however, others chose to accept the certificate as an academic base only and required the
candidate to pass additional provincial practical tests.
The Dominion Dental Council proved to be rather ineffective. A name change to The Dental Council of
Canada in 1950 along with attempts to improve the efficiency of the examination mechanism still failed to
attract strong support from the DRA’s. This was in spite of the fact that the DRA’s agreed with the general
concept. They had indicated a desire to be free of provincial licensing examinations, providing a reliable
national examination system could be established.
The following year, 1951, the CDA encouraged the ten DRA’s to develop a satisfactory plan for a National
Examining Board. Its purpose was to provide a facility by which members of the profession could become
eligible, on a national basis, to apply for practice privileges in the province of their choice. The result was
the incorporation of The National Dental Examining Board of Canada (NDEB) in 1952 by an Act of Parliament
of Canada. The Act was supported by all ten DRA’s and by the CDA and this support continues today.
Purpose
According to the Act of Parliament, the NDEB is responsible for the establishment of qualifying conditions for
a national standard of dental competence for general practitioners, for establishing and maintaining an
examination facility to test for this national standard of dental competence and for issuing certificates to
dentists who successfully meet this national standard.
17E November 10, 2015 6 / 78
Structure
The National Dental Examining Board of Canada is composed of twelve members. Each DRA appoints one
member and two members are appointed by the Commission on Dental Accreditation of Canada (CDAC). In
1994, the Board designated representatives from the Royal College of Dentists of Canada (RCDC) and the
CDA. In 2004, the Board designated a representative from the Canadian Dental Regulatory Authorities
Federation (CDRAF) as an official observer and appointed a Public Representative. The full Board meets
annually. The NDEB also has standing committees dealing with examinations, appeals, finances and by-
laws. The NDEB is a non-profit organization supported by fees charged to candidates and participants for
examinations and assessments and certification.
Certification
The NDEB grants certification to candidates from the following groups:
Graduates of Dental Programs accredited by the Commission on Dental
Accreditation of Canada and by the American Dental Association Commission on
Dental Accreditation
Prior to 1971, a graduate of an undergraduate dental program in Canada was required to successfully
complete the NDEB examination (written essay-type) in order to be certified. This policy was changed in
1971, when the NDEB decided to recognize the examinations and evaluation administered by Canadian
faculties of dentistry and issue certificates to current graduates of these faculties without further
examination. The condition for certification established at this time was graduation from an undergraduate
dental program approved by the Commission on Dental Accreditation of Canada.
In 1988 concern was expressed by several DRA’s about the validity of establishing clinical competence solely
by accreditation. This concern was further intensified by the extension of the accreditation cycle from five to
seven years. Therefore, in 1989, the NDEB established a committee "to explore whether the granting of a
certificate on the basis of accreditation alone continues to be acceptable." This committee (Certification
Review Committee or CRC) presented its report at the 1990 NDEB Annual Meeting. The report stated that
certification based on accreditation alone was no longer acceptable, a finding which was further supported in
the Parker Report.
In 1994, the NDEB certification process was modified so that graduates of accredited Canadian dental
programs were required to pass the Written and Objective Structured Clinical (OSCE) Examinations.
As a result of a formal agreement between accrediting organizations, graduates of the United States,
Australia, New Zealand and Ireland dental programs are considered “accredited graduates”. To be certified,
these graduates must pass the Written Examination and the OSCE within a specified period of time.

17E November 10, 2015 7 / 78
The NDEB, through its representatives on the Commission on Dental Accreditation of Canada and through an
appointee on each undergraduate program survey team actively participates in the accreditation process. In
addition, the NDEB gives an annual grant to the Commission to be applied to accreditation costs of
undergraduate dental programs in Canada, the United States, Australia, New Zealand and Ireland.
Certification of Graduates of Non-Accredited Dental Programs
Until December 31, 1999, graduates of non-accredited dental programs were certified either by passing a
certification examination that consisted of the Written Examination and a three part Clinical Examination or
by successfully completing an accredited Qualifying or Degree Completion Program at an accredited
university and then successfully completing the Written Examination and the OSCE.
Since January 1, 2000, graduates of non-accredited dental programs have been required to successfully
complete a Qualifying or Degree Completion Program prior to being eligible to take the NDEB examinations.
With the adoption of the Agreement on Internal Trade in 2009, all professions and trades essentially have
labour mobility (portability) in Canada. In dentistry, after numerous meetings and intense and lengthy
negotiations, the CDRAF unanimously requested that the NDEB implement a new certification process based
on the previous ODQ Equivalency Process and be integrated with the admission process for
Qualifying/Degree Completion Programs. The NDEB Equivalency Process was implemented in 2011. The
Assessment of Clinical Skills is one of three Assessments in the Equivalency Process.
Competencies for a Beginning Dental Practitioner in Canada
In 1993, the NDEB in cooperation with the ACFD, CDA and CDAC conducted a process to establish
“Competencies for the Beginning Dental Practitioner in Canada”. These competencies, which were the first
nationally accepted competencies, were used to establish examination blueprints, guide educational
programs and were included in accreditation standards. They have also been used as a resource for many
national and international processes in dentistry and other professions.
In 2004, the NDEB initiated a review process that resulted in the revision of the competency document
(Appendix B). This document, which has been accepted by the NDEB, the ACFD, CDA and CDAC is used in
the establishment of blueprints for all NDEB Examinations and Assessments.
17E November 10, 2015 8 / 78
Assistance to Other Organizations
The NDEB provides consultation and existing examination related material to the DRA’s on request.
Beginning in 1998, at the request of the DRA’s, the NDEB assisted the ACFD in the administration of the
ACFD Eligibility Examination which was required to apply for Qualifying/Degree Completion Programs. In
2001, formal agreements between the NDEB and the ACFD were signed. These agreements related to the
administration of the ACFD Eligibility Examination and to administrative services provided by the NDEB for
the ACFD. With the implementation of the NDEB Equivalency Process the final ACFD Eligibility Examination
was held in February 2010.
The NDEB also provides examination services on request to any DRA and has formal agreements for
provision of services with l’Ordre des dentistes du Québec.
As directed by the CDRAF, ACFD and NDEB (in collaboration with RCDC) developed the Dental Specialty Core
Knowledge Examination (DSCKE). The DSCKE was administered for the first time in the fall of 2009.
Summary
The NDEB is conscious of its responsibility to certify only candidates who meet the national standard for the
purpose of public protection. The Board has proposed and followed a series of strategic plans.
Each year, the NDEB assesses its certification, examination and assessment procedures and the responses of
the candidates and participants, making adjustments where indicated to improve the validity and reliability of
the examination and assessment. The Examinations Committee annually reviews the standards and
procedures of the respective examinations and assessments and makes recommendations to the Board.
In addition to this ongoing internal review, the NDEB has initiated several external evaluation procedures
over the years.
17E November 10, 2015 9 / 78
Test Constructions Process and Validity Procedure while Preparing
for the Assessment
The primary basis for establishing validity for certification examinations is to show that the process for
examination development is a valid reflection of that part of the professional domain that the examinations
purport to assess. That is, construct validity is about the relationships between the construct (professional
competence) and the instruments. The Assessments in the Equivalency Process are built to be consistent
with the “Competencies for a Beginning Dental Practitioner in Canada”. The content categories reflect both
the educational programs and the demands of practice, and the examinations and assessments are vetted
by practitioners. The content blueprint of the Assessment of Clinical Skills was established on the direction
of the Canadian Dental Regulatory Authorities and is identical to the blueprint of the Assessment of Clinical
Skills administered by l’Ordre des dentistes du Québec from 2001 to 2010. The blueprint was approved by a
joint Examinations Committee meeting of the NDEB and l’ODQ and is shown as IV Assessment Requirements
in the ACS protocol (Attachment 1). The blueprint will be reviewed following the completion of a formal
Task Analysis in 2015.
In addition to the logical basis for asserting construct validity, the NDEB has carried out several studies, both
internal and published, that support validity claims (Appendix 1).
Personnel and Committee Structure
Examinations Committee
The Examinations Committee of the Board consists of nine members appointed by the Board. One of these
members may be the Public Representative. No more than two persons can be recommended to be
members by each of l’Ordre des dentistes du Québec and the Association of Canadian Faculties of Dentistry.
Staff support for the Committee includes the Executive Director, the Examinations Project Manager, the
Examinations Coordinators and the Chief Examiners for the Written Examination; OSCE Examination;
Assessment of Fundamental Knowledge (AFK); Assessment of Clinical Skills(ACS), and, Assessment of
Clinical Judgement(ACJ).
The Examinations Committee ensures that its recommendations will provide for the conducting of
Examinations and Assessments in a manner fair and equitable for all concerned. Each year the Examinations
Committee of the Board:
Reviews the standards and procedures of all Examinations and Assessments and makes recommendations to the Board on all matters concerning the Examinations and Assessments.
Reviews the passing standard for each Examination and Assessment and makes a recommendation to the Board.
Reviews a roster of possible Examiners suggested by representatives of Accredited Programs located in Canada and by the Provincial Dental Regulatory Authorities. The Committee recommends a list of Examiners to permit the Board to appoint a sufficient number of Examiners to develop, construct, validate, administer and evaluate all of the Examinations and Assessments offered to candidates and participants by the Board.
Recommends to the Board, Chief Examiners for each of the Board’s Examinations and Assessments.
17E November 10, 2015 10 / 78
Reviews the protocols for each of the Board’s Examinations and Assessments and submits the protocols to the Board for approval.
Makes decisions under regarding voiding the results of a person’s Examination or Assessment and whether the person has the privilege of repeating the Examination or Assessment.
Suggestions for protocol changes (including the evaluation criteria) are initiated by staff and Chief Examiners
from experience during the administration of the Assessment and from changes in the structure or format of
the Assessment made by the NDEB Examinations Committee.
Examination and Assessment dates are published by policy, well in advance, to permit the staff, candidates
and participants to plan appropriately. Normally, the ACS is offered in June of each year.
Individuals suggested for appointment as examiners by the DRA’s, the Deans and Directors of the dental
programs in Canada and the Canadian Forces Dental Services are reviewed by the Examinations Committee
and subsequently appropriate individuals are recommended to the Board for appointment.
In addition to appointing examiners, on recommendation of the Examinations Committee, the Board
appoints consultants who are recognized for their expertise and/or experience in examination and
assessment development.
The results of the Assessment are reported to the Examinations Committee.
Assessment integrity is maintained by the Committee through the review of Assessment Coordinators’ and
Assessment Supervisors’ reports on irregularities identified during an Assessment session. If a participant is
reported to have compromised the Assessment by cheating or violating the regulations, the Committee has
the authority to void the results of that participant’s Assessment and to prohibit the participant from taking
the Assessment in the future.
Staff Support
The Executive Director/Registrar is responsible for staff supervision and the implementation of all policies
approved by the Board to ensure the process operates efficiently and effectively.
The Chief ACS Examiner is responsible for the development of the Assessment including selection of
Assessment Supervisors, Invigilators, Facilitators, Evaluators, Assessment teeth, calibration (both of
materials and personnel) and review of results.
The Examinations/Assessments Project Manager, in consultation with the Executive Director/Registrar and
Chief Examiner, prepares and administers the Assessment including arrangements with hosting institutions
and staff, preparing protocols, identification cards, correspondence with Assessment Supervisors, Assistant
Assessment Supervisors, Invigilators, Facilitators and Evaluators, and production and translation of
Assessment material. The Examinations/Assessments Project Manager is supported by an Examinations
Coordinator, and Assessments Coordinator and Clerks and Office Administrative Assistant. The
Examinations/Assessments Project Manager contracts with specific personnel at each Assessment centre
who have been trained to assist in the administration of the Assessment of Clinical Skills.

17E November 10, 2015 11 / 78
All staff are responsible for carrying out directives from the Examinations Committee as approved by the
Board.
Selection of Assessment Centres
The ACS is held in June and December at participating host Faculties of Dentistry across Canada. A minimum
of 25 participants must register for a location to establish an Assessment centre at that location. At least
one centre must be able to accommodate participants who request a French language ACS.
At least nine months prior to the Assessment, a letter is sent to the Dean/Director of 9 Canadian Faculties of
Dentistry requesting that their school host a site. This letter gives detailed information regarding both the
physical and human resources required in order to host a session and the financial arrangements.
For new ACS sites, the Chief Examiner, the Assessment Supervisor and Assistant Supervisor assigned to the
Assessment Centre and a NDEB staff person perform a site visit and orientation session. During the site visit
the Chief Examiner determines that the school’s dental clinic is acceptable and Assessment equipment is
compatible with the clinic’s equipment. There is variation in the equipment at the different schools but all of
the ACS centres have equipment, lighting and space that meet the standard of a clinical practice.
Requirement Selection
The ACS evaluates a participant’s clinical skills through the completion of dental procedures (requirements)
on a simulated patient (manikin). The NDEB Examinations Committee reviews and revises the requirements
annually and recommends the requirements to the Board as part of a protocol.
Assessment Preparation and Administration
The NDEB performed an in-depth review of commercially available manikins and typodont products prior to
deciding to use the Nissin system distributed in North America by Kilgore International. The NDEB
determined that this product simulates actual patient conditions better than other available systems.
Typodont systems are reviewed every 3 years so that advances in simulations can be integrated into the
Assessment.
In the Assessment protocol, participants are supplied detailed information on all of the simulated teeth used
in the Assessment. Kilgore International will sell teeth to individuals, allowing participants to become
familiar with the simulated teeth used in the ACS. For some of the requirements, Nissin manufactures
custom teeth for the NDEB and these are only available to the NDEB. However, standard versions of these
custom teeth are available for participants to purchase.

17E November 10, 2015 12 / 78
All Assessment teeth are placed in the manikins by NDEB staff in Ottawa. The Chief Examiner checks each
typodont to verify that the appropriate teeth are placed, aligned and occlude properly. One to two weeks
prior to the Assessment, assessment material is shipped to the Assessment centres where it is securely
stored.
Information for Participants
The NDEB website, www.ndeb.ca, has a comprehensive description of the ACS process. The information
includes details of costs, times and locations. It identifies the application process and requirements; the
types of dental procedures on the ACS, details the criteria used in the evaluation process of these
procedures and grade derivation grids. Applicants are informed of the manufacturer of the simulated teeth.
The grading criteria provided on the website are identical to the criteria used by Supervisors, Invigilators and
Evaluators. The website is thorough and available to interested individuals prior to application.
The quality and comprehensiveness of the information on the website about the ACS represents best
practices in transparency and accountability. The objective information available ensures fairness in allowing
participants to prepare and practice the required procedures.
When participants receive confirmation of their ACS application, they are also provided with details of the
equipment available to them at their assigned Assessment centre. This includes a written description and
several photographs of the handpiece coupler compatible with the school’s equipment.
Validity and Reliability Procedures during the Administration of the
Assessment
Personnel
The Chief Examiner and Assistants to the Chief Examiner are appointed by the Board. In consultation with
the Registrar and other NDEB staff, they are responsible for overseeing the preparations for the ACS
administration including; appointing appropriate personnel; assisting with communications between the
NDEB and personnel for each site; selecting the specific teeth used in the Assessment; preparing typodont
teeth for Assessment restorations; drafting Assessment documents; preparing training and calibration
documents including PowerPoint presentations; directing staff on the preparation and assembly of materials
and assuring uniformity of the typodont set ups.
17E November 10, 2015 13 / 78
The following personnel are appointed to be present at each Assessment centre:
Assessment Supervisors and Assistant Supervisors – These are examiners appointed by the Board on the recommendation of a DRA or Faculty of Dentistry who act as Supervisors and Assistant Supervisors. They have advanced training in the ACS process and procedures. These individuals are calibrated and responsible to ensure appropriate training and calibration of Invigilators set up and security of Assessment materials; ensure compliance with standardized Assessment protocols; address any onsite disputes on process; ensure independent Invigilator assessments of infection control and rubber dam requirements and confirm the evaluation of the onsite assessments of infection control and rubber dam requirements.
Invigilators (2-10) –These are examiners appointed by the Board on the recommendation of a DRA or Faculty of Dentistry who act as Invigilators. They are calibrated to set up; monitor the process and evaluate the onsite assessments. In a half day session, held just prior to the ACS, these individuals receive training and are calibrated using standardized PowerPoint presentations. They then prepare the clinic facilities for the ACS. Invigilators are responsible to set up the clinic; monitor participant compliance during the Assessment; report infractions; evaluate infection control and rubber dam placements based on the standardized criteria and assist in securing Assessment materials for transport.
Registered Dental Assistants (2-4) – Dental Assistants are recommended by the host institution. They have knowledge of the clinic and operations, provide access to Faculty sites; obtain and monitor Faculty equipment; support Supervisors and Invigilators in their Assessment functions. Dental assistants do not provide dental assisting services to any of the participants. Dental assistants are trained and delegated tasks by the Assessment Supervisors.
NDEB Staff (1-2) – Staff members of the NDEB are onsite to provide support; ensure compliance with NDEB standardized processes and procedures; secure Assessment material and equipment during transport to and from NDEB offices in Ottawa.
Assessment Coordinator (1) – This is a full time clinical Faculty member, usually the Faculty of Dentistry Clinic Director. They provide onsite pre-Assessment logistical support; provide general support to the Assessment Supervisors; monitor use of Faculty material, supplies and personnel.
Equipment Technician(1-2) – An equipment technician is provided by the Faculty of Dentistry to calibrate equipment prior to the Assessment; assist participants in initial set up; address any malfunctions during the Assessment and provide general support to the Assessment Supervisors.
Training and Calibration
Each category of Assessment personnel receives specific written instructions before the Assessment. On the
day prior to the Assessment, the Assessment Supervisor and Assistant Supervisor conduct training and
calibration sessions for Invigilators and school staff. Strict adherence to the ACS schedule and procedures
for uniform administration of the ACS are emphasized. Assessment Coordinators review any unique features
of equipment or operations of each clinic and discuss safety and emergency protocols.
17E November 10, 2015 14 / 78
Set Up and Verification
On the day prior to the Assessment, all personnel assist in setting up the clinic for the Assessment.
Participants are assigned to specific clinical operatories based on seating charts prepared by the
Examinations Project Manager at the NDEB. NDEB Assessment personnel verify that the typodont ID
number on each manikin matches with the operatory assignment map and that the appropriate participant
photo ID card is visible in each operatory. Assessment Supervisors and Invigilators verify the uniform setup
of each manikin, torso and typodont, including the occlusion.
Participant Registration, Orientation and Set up
On the morning of Day 1 of the Assessment, participants’ identifications are verified with government issued
photo ID and confirmed to match material sent to the NDEB during the application process.
Participants receive a short, scripted orientation session accompanied by a standardized PowerPoint where
ACS procedures and regulations are reviewed. Participants have the opportunity to ask questions of the
Assessment Supervisor and Coordinator.
At the time indicated in the ACS schedule, participants are directed to their pre-assigned operatories in the
clinic. All Assessment personnel are available to assist participants setting up their equipment and ensuring
that equipment is in working order. The equipment technician addresses any technical issues. Participants
are also able to prepare the teeth assigned for practice during this time.
During the Assessment
At the indicated time, the list of requirements for the day is distributed and the Assessment begins.
Supervisors and Invigilators circulate and ensure that anatomically possible operating and patient postures
are maintained throughout the Assessment. Participants are not graded on improper postures, but they are
directed to correct non-anatomically possible positions. If a participant consistently refuses to use
anatomically possible operating and patient posture following three directions they may be stopped and their
grade will be a Fail.
The infection control requirement is observed and graded by examiners throughout the two days of the
Assessment. Violations are noted and recorded on forms pre-printed for each participant. Final grades for
this requirement are tabulated after the Assessment is completed.
The rubber dam requirement is performed at different operatories at times pre-assigned to each participant
throughout the two days of the Assessment. Participants are advised of their assigned time in their Day 1
registration materials. After the completion of the placements, two Invigilators independently grade each
placement. Supervisors verify the placement and the grading to ensure consistency. A photograph of the
placement is taken before the rubber dam is removed in preparation for the next participant,

17E November 10, 2015 15 / 78
Although very few defects with typodont teeth are found, if a defect is identified at any time during the ACS,
Supervisors and Invigilators are trained to determine whether a defect is of such consequence to require
replacement of the tooth and a possible time extension or whether the tooth with the defect should remain
and notes to Evaluators be made on the Participant’s Communication pages.
Participants who experience undue delays because of clinic equipment failures or other circumstances, are
given time extensions by the Supervisors or Invigilators.
At the end of each day, participants are asked to stop working and leave the clinic while typodonts and
Participant Communication pages are collected.
At the end of Day 2, all typodonts and documents are boxed and shipped to Ottawa for grading. Grading
forms used at the centres for the infection control and rubber dam requirements are duplicated, with the
instructions that they be destroyed once the originals are verified to be received intact in Ottawa.
Validity and Reliability Procedures during the Evaluation Session
Personnel
Chief Examiner and Assistants to the Chief Examiner
The Chief Examiner and Assistants ensure appropriate personnel are appointed for the evaluation session;
prepare all training and calibration material including PowerPoint presentations and example requirements
for calibration; direct the text programming of the evaluation computers; draft documents used in evaluation
procedures; direct the set up of the typodonts and documents for evaluation and provide direction to
Facilitators and Evaluators throughout the evaluation session.
Facilitators
These are examiners appointed by the Board on the recommendation of a DRA or Faculty of Dentistry who
act as evaluation Facilitators. Two or more Facilitators are appointed for each requirement. They direct the
calibration session for their assigned requirement; review requirements and grades in cases where
Evaluators have not fully agreed on grades or locations and determine the appropriate final grades and
coordinate discussion between Evaluators on any issues that arise during the evaluation session.
Evaluators
These are examiners appointed by the Board on the recommendation of a DRA or Faculty of Dentistry who
act as Evaluators. Sufficient Evaluators are appointed for each requirement. They evaluate the required
procedures performed by the participants’ and assign grades based on the criteria listed in the ACS Protocol.
17E November 10, 2015 16 / 78
NDEB staff
Full-time staff members of the NDEB are onsite to secure Assessment material and equipment during
transport to and from NDEB offices in Ottawa; set up and take down the calibration and evaluation material;
provide computer support and enter participant grades from the Assessment centres into the central
evaluation computer system.
Training and Calibration
About six weeks prior to the evaluation session, Facilitators and Evaluators are sent specific material related
to the requirement they are assigned to evaluate. Materials include the grading criteria, written guidelines
for evaluation, a typodont and several Assessment teeth for their assigned requirement. Evaluators and
Facilitators are directed to practice the requirement several times themselves so that they are familiar with
how the typodont teeth differ from natural teeth and the challenges that participants face during the
Assessment. Evaluators are also directed to familiarize themselves with the evaluation criteria and
guidelines.
The Evaluation Session starts with an introduction to the process and NDEB and an orientation on the use of
tablet computers for recording evaluations. Each Evaluator has the exclusive use of a tablet style computer
for grading. Then, each requirement’s Facilitators and Evaluators spend two to three hours in calibration and
practice grading activities. Firstly, they review example typodont teeth prepared to illustrate almost all of the
requirement’s possible grades. They then practice grading using 10 examples of completed requirements,
each with a suggested evaluation. They practice entering the evaluations on their tablet computers. The
calibration materials are selected and prepared by the Chief Examiner and verified by the Assistants to the
Chief Examiner.
Once evaluations have started, Facilitators are given extra instruction in the facilitation process and in the
use of the tablet computers for facilitation procedures.
The Evaluation Process
Typodonts and associated Participant Communication pagess are arranged numerically by participant
number, with no indication of the participant name or Assessment centre. Each individual requirement is
graded independently by two Evaluators. If there is not perfect agreement between the two evaluations
(grade, error and location), the Facilitators’ computer will show that facilitation is needed. A Facilitator
reviews the typodont and the evaluations and assigns the appropriate grade, error and location.
In a similar fashion, the written Records of Procedure pages are sorted numerically and independently
graded by two separate Evaluators. Discrepancies in grading are reviewed and final grades assigned by
Facilitators.
Facilitators are advised to look for patterns of grading discrepancies amongst the Evaluators and if such
patterns are noted, to revisit the calibration materials with the Evaluators involved.
17E November 10, 2015 17 / 78
Grading Process
Grading
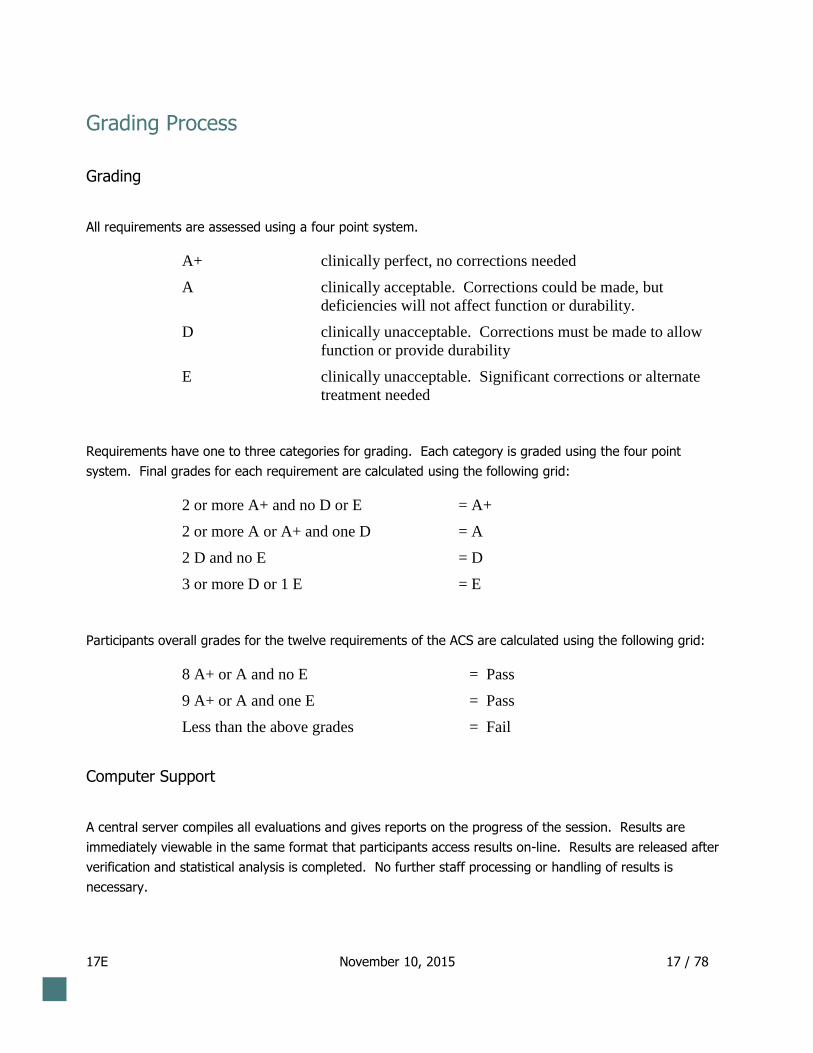
All requirements are assessed using a four point system.
A+ clinically perfect, no corrections needed
A clinically acceptable. Corrections could be made, but
deficiencies will not affect function or durability.
D . clinically unacceptable. Corrections must be made to allow
function or provide durability
E clinically unacceptable. Significant corrections or alternate
treatment needed
Requirements have one to three categories for grading. Each category is graded using the four point
system. Final grades for each requirement are calculated using the following grid:
2 or more A+ and no D or E = A+
2 or more A or A+ and one D = A
2 D and no E = D
3 or more D or 1 E = E
Participants overall grades for the twelve requirements of the ACS are calculated using the following grid:
8 A+ or A and no E = Pass
9 A+ or A and one E = Pass
Less than the above grades = Fail
Computer Support
A central server compiles all evaluations and gives reports on the progress of the session. Results are
immediately viewable in the same format that participants access results on-line. Results are released after
verification and statistical analysis is completed. No further staff processing or handling of results is
necessary.

17E November 10, 2015 18 / 78
Post Evaluation Review
After all evaluations are completed, the Chief Examiner, Assistants to the Chief Examiner and other selected
experienced Evaluators review all of the evaluations. Particular attention is paid to participants who have
received marginal failing grades. The main objective of the review is to ensure that the number of false
negative results from the Assessment is minimal. Favourable consideration is given to those participants who
demonstrate a conservative approach to tooth preparations and those who are judged to have made errors
consistent with those made because of the differences between typodont teeth and natural teeth.
Also, some participants’ grades may be raised to passing grades. The guideline for raising to a passing
grade is a demonstration of skills that could be considered equivalent to that of a new graduate of an
accredited dental program.
Reporting
Detailed results are provided to participants on using the online system. Participants receive an email
notification once results are posted. Participants can log in and view their overall results and the detailed
result for each requirement. A partial example of a participant’s result report follows.

17E November 10, 2015 19 / 78
Partial Example of a Participant’s Result Report
Class II Amalgam Preparation Result: A+
A+: External Outline Form
No errors
A: Internal Form
Minor overpreparation occlusally
Mesial-occlusal
Axial wall too deep: > 1.5 mm
Mesial
Distal
A+: Finish
No errors
Infection Control Result: A+
A+: Infection Control
No violations

17E November 10, 2015 20 / 78
Full Metal Crown Preparation Result: A+
A: Path of Draw and Axial Convergence
Minor undercuts. Manageable by lab.
Mesial
A+: Preservation of Tooth/Structural Durability
No errors
A+: Finish and Margin
No errors

17E November 10, 2015 21 / 78
Provisional Crown Restoration Result: E
D: Margin Contour and Adaptation
Underextended 0.5 – 1.0mm
Distal
D: Morphology and Occlusion
Undercontoured
Distal
D: Polish
Unacceptable roughness
Distal

17E November 10, 2015 22 / 78
Metal-ceramic Crown Preparation Result: A
A: Path of Draw and Axial Convergence
Minor undercuts. Manageable by lab.
Labial
Mesiolabial
D: Preservation of Tooth/Structural Durability
Buccal, mesial, distal reduction 1.5 - 2.5mm
Buccal
Lingual reduction 1.0 - 1.5mm
Mesiolingual
A: Finish and Margin
Located supragingival 0 - 1.0mm
Mesiobuccal
Distolingual
17E November 10, 2015 23 / 78
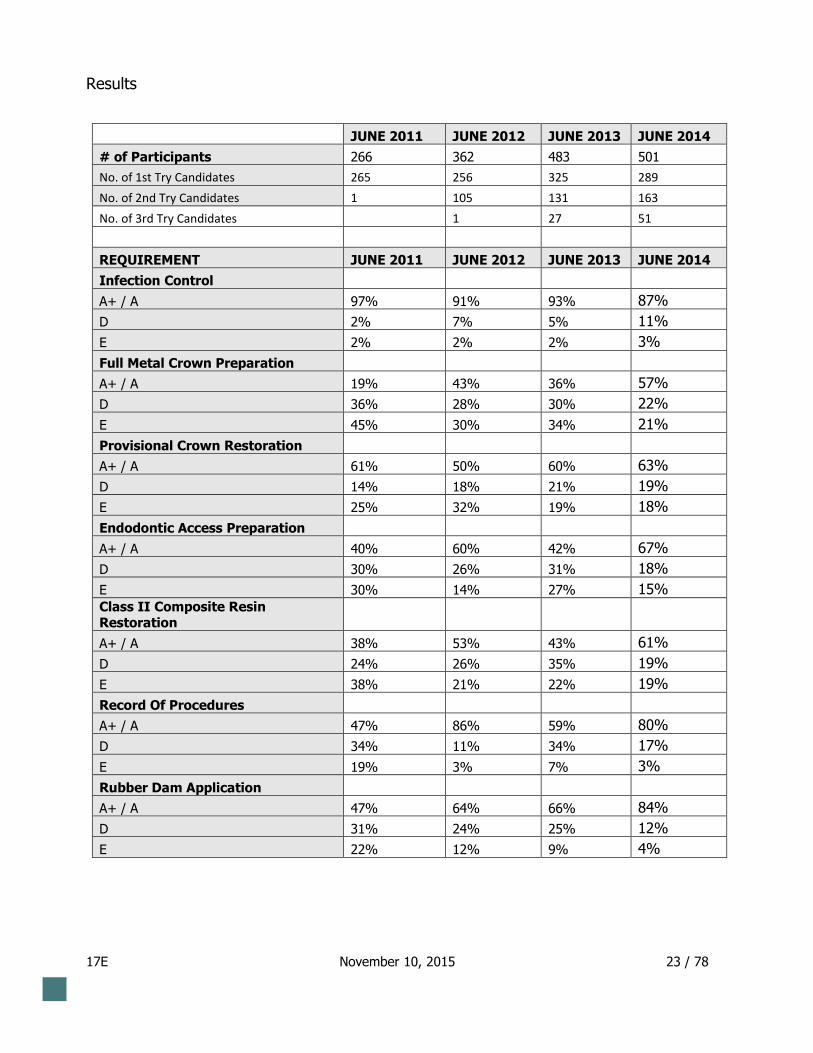
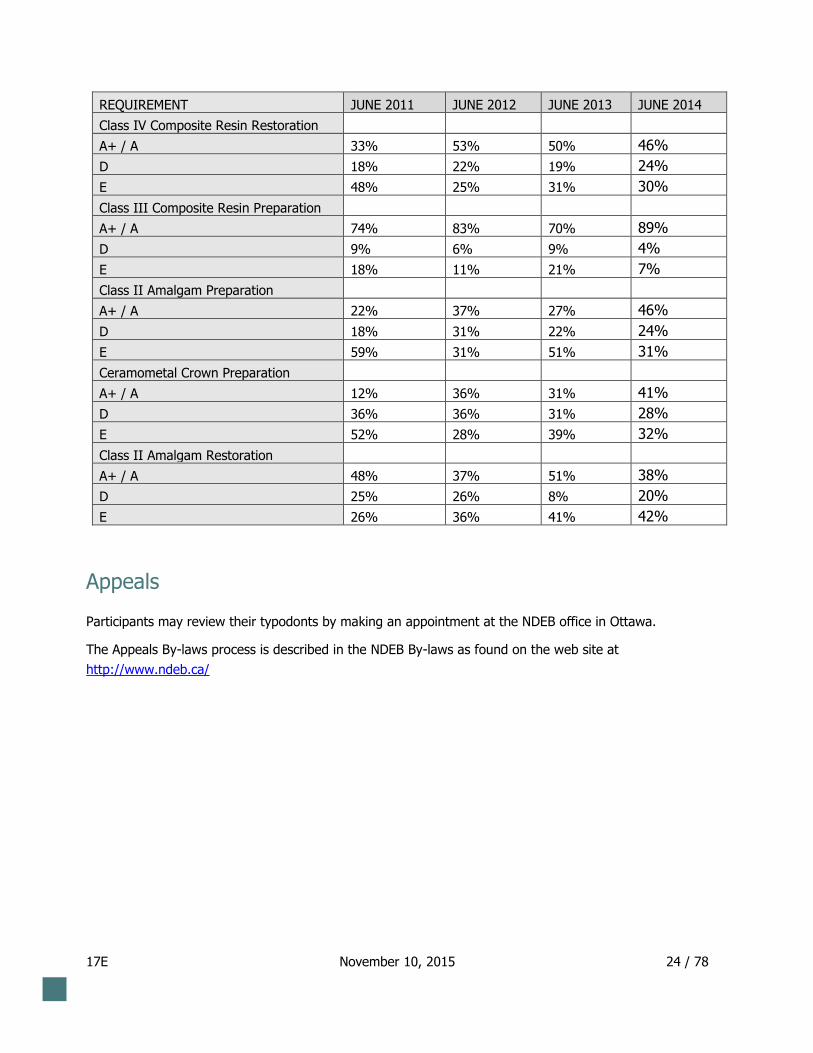
Results
JUNE 2011 JUNE 2012 JUNE 2013 JUNE 2014
# of Participants 266 362 483 501
No. of 1st Try Candidates 265 256 325 289
No. of 2nd Try Candidates 1 105 131 163
No. of 3rd Try Candidates
1 27 51
REQUIREMENT JUNE 2011 JUNE 2012 JUNE 2013 JUNE 2014
Infection Control
A+ / A 97% 91% 93% 87%
D 2% 7% 5% 11%
E 2% 2% 2% 3%
Full Metal Crown Preparation
A+ / A 19% 43% 36% 57%
D 36% 28% 30% 22%
E 45% 30% 34% 21%
Provisional Crown Restoration
A+ / A 61% 50% 60% 63%
D 14% 18% 21% 19%
E 25% 32% 19% 18%
Endodontic Access Preparation
A+ / A 40% 60% 42% 67%
D 30% 26% 31% 18%
E 30% 14% 27% 15% Class II Composite Resin Restoration
A+ / A 38% 53% 43% 61%
D 24% 26% 35% 19%
E 38% 21% 22% 19%
Record Of Procedures
A+ / A 47% 86% 59% 80%
D 34% 11% 34% 17%
E 19% 3% 7% 3%
Rubber Dam Application
A+ / A 47% 64% 66% 84%
D 31% 24% 25% 12%
E 22% 12% 9% 4%
17E November 10, 2015 24 / 78
REQUIREMENT JUNE 2011 JUNE 2012 JUNE 2013 JUNE 2014
Class IV Composite Resin Restoration
A+ / A 33% 53% 50% 46%
D 18% 22% 19% 24%
E 48% 25% 31% 30%
Class III Composite Resin Preparation
A+ / A 74% 83% 70% 89%
D 9% 6% 9% 4%
E 18% 11% 21% 7%
Class II Amalgam Preparation
A+ / A 22% 37% 27% 46%
D 18% 31% 22% 24%
E 59% 31% 51% 31%
Ceramometal Crown Preparation
A+ / A 12% 36% 31% 41%
D 36% 36% 31% 28%
E 52% 28% 39% 32%
Class II Amalgam Restoration
A+ / A 48% 37% 51% 38%
D 25% 26% 8% 20%
E 26% 36% 41% 42%
Appeals
Participants may review their typodonts by making an appointment at the NDEB office in Ottawa.
The Appeals By-laws process is described in the NDEB By-laws as found on the web site at
http://www.ndeb.ca/
17E November 10, 2015 25 / 78
Attachment 1 – Assessment of Clinical Skills Protocol
The National Dental Examining Board of Canada
Le Bureau National d’Examen Dentaire du Canada
EQUIVALENCY PROCESS
ASSESSMENT OF CLINICAL SKILLS
PROTOCOL
June 2014

17E November 10, 2015 26 / 78
The National Dental Examining Board of Canada
Le Bureau National d’Examen Dentaire du Canada
T A B L E O F C O N T E N T S
PAGE
CONTENT AND FORMAT .............................................................................................................. 27
SCHEDULE ....................................................................................................................................... 27
VALIDATION OF REGISTRATION ............................................................................................... 29
ASSESSMENT REQUIREMENTS .................................................................................................. 29
EQUIPMENT, INSTRUMENTS AND SUPPLIES .......................................................................... 31
INSTRUCTIONS ............................................................................................................................... 31
REGULATIONS ................................................................................................................................ 37
Grading Criteria .................................................................................................................................. 39
GRADE DERIVATION GRID FOR INDIVIDUAL REQUIREMENTS ........................................ 64
GRADE DERIVATION GRID FOR PASS/FAIL RESULT ............................................................ 66
RESULTS ........................................................................................................................................... 66
APPEAL ............................................................................................................................................. 68
REPEATS ........................................................................................................................................... 68

27
17E November 10, 2015 27 / 78
ASSESSMENT OF CLINICAL SKILLS
I CONTENT AND FORMAT
During the two day Assessment of Clinical Skills, participants will be evaluated on their performance of
dental procedures on simulated patients (manikins) in a clinical setting.
Each day participants will receive a
1. typodont mounted in a manikin on a dental chair. The typodont will be labelled with the
participant’s ID number.
2. list of teeth for practice preparations.
3. detailed list of required procedures specifying tooth numbers and surfaces.
4. scheduled time to perform the Rubber Dam Requirement (1/2 of participants).
5. Participant Communication form which may be used to provide comments to Evaluators.
II SCHEDULE
DAY 1
Validation of registration 7:30am - 8:00 am
Orientation and instructions 8:00 am - 8:30 am
Set up 8:30 am - 9:00 am
Clinical procedures on simulated patients 9:00 am - 4:30 pm*
28
17E November 10, 2015 28 / 78
DAY 2
Validation of registration 7:30 am - 8:00 am
Set up 8:00 am – 8:30 am
Clinical procedures on simulated patients 8:30 am - 4:30 pm*
* Participants who are scheduled for their Rubber Dam requirement will finish one half hour later.
Participants must exit the clinic and remove all of their equipment and supplies no later than 5:30 each
day.
29
17E November 10, 2015 29 / 78
III VALIDATION OF REGISTRATION
During the validation of registration, participants will be issued an Identification (ID) badge. To receive
the ID badge, participants will be required to show current government photo identification (i.e. a
current passport or driver’s licence) for comparison to the ID badge. The participant’s name on the
government photo identification must match the name used by the participant to register with the NDEB
for the Equivalency Process. Participants who do not provide government photo identification will not
be admitted.
Participants must have their ID card and ID badge visible at all times and must submit them as directed
at the end of the Assessment. Participants who fail to submit their ID card and ID badge may receive an
“E” for all requirements in the Assessment.
IV ASSESSMENT REQUIREMENTS
Participants will be required to perform the following procedures:
Class II amalgam preparation.
Class III composite resin preparation.
Full metal crown preparation.
Metal-ceramic (porcelain fused to metal) crown preparation.
Endodontic access preparation on a molar tooth.
Direct Class II composite resin restoration on a pre-prepared* tooth
Direct Class IV composite resin restoration on a pre-prepared* tooth
Class II amalgam restoration on a pre-prepared* tooth.
30
17E November 10, 2015 30 / 78
Provisional crown restoration for a pre-prepared* metal-ceramic (porcelain fused to metal) crown
preparation on Day 2 of the Assessment. The original unprepared tooth will be in the typodont used
on Day 1 of the Assessment.
Rubber dam application
Participants will also be evaluated on the following:
Record keeping.
Infection control and material hygiene.
* a pre-prepared tooth will be supplied.
31
17E November 10, 2015 31 / 78
V EQUIPMENT, INSTRUMENTS AND SUPPLIES
The dental clinic at the Assessment Centre will provide the following items:
A typodont mounted in a manikin on a dental chair
An overhead dental operating light
An operator stool
Amalgamators
Saliva ejectors
Air/water syringe tips
High volume suction tips
Amalgam waste and sharps disposal containers
Participants must supply ALL OTHER equipment, instruments and supplies needed to complete the
required procedures, including but not limited to:
Handpieces and burs
Curing lights
All restorative materials including amalgam, composite resin and provisional crown materials
Gloves, masks, protective eyewear and appropriate clinic attire
Dental hand instruments
Rubber dam, frames, clamps, forceps and dental floss
Materials to place and finish restorative materials (matrix bands, matrix holders, wedges
polishing supplies, etc.)
Information regarding handpiece configuration (connectors) at each centre will be forwarded to
participants prior to the Assessment.
The dental clinic at the Assessment Centre will not be accessible prior to the Assessment.
VI INSTRUCTIONS
1. At the beginning of each day, the list of requirements for that day will be distributed. Participants
may perform the requirements for the day in any order, except for the application of the rubber dam,
which will have an assigned time for each participant. It is not necessary to use rubber dam to
perform any of the other requirements.

32
17E November 10, 2015 32 / 78
2. Participants are not permitted to remove teeth from typodonts, nor are they permitted to remove
typodonts from the manikins.
3. Participants are not permitted to have extra typodont teeth in the Assessment area.
4. Interocclusal distance on the typodonts is pre-set to a standardized amount. Participants must not
increase the pre-set interocclusal distance. Instructions will be given on occluding the typodonts
without altering the pre-set distance.
5. Participants must wear appropriate clinic attire but this will not be assessed for grading. Open toed
shoes are not allowed in clinics for safety reasons.
6. Participants may use magnification aids but may not use cheek retractors. Participants are
encouraged to take breaks whenever needed.
7. Participants will receive an ‘E’ grade for any requirement in which:
- a procedure is started on a tooth other than one identified for that requirement or identified as a
practice tooth.
- a restorative requirement is completed using an inappropriate material.
- a provisional crown cannot be removed from its preparation or is cracked or broken.
- restorative devices, including matrix bands and wedges are not removed.
8. During the Assessment, participants must demonstrate competency in performing procedures in a
clinical environment. Although there are no criteria for evaluating the posture of a participant,
procedures must be performed in anatomically acceptable positions. Examples of unacceptable
positions include:
- the manikin’s head positioned so that a patient would be uncomfortable
- the manikin’s neck extended so that a patient would be uncomfortable
- the participant leaning on or inappropriately contacting the patient’s torso or head.
Invigilators will direct participants to correct unacceptable positions. Any participant who
continues to work with the manikin in an unacceptable position may be dismissed from the
Assessment and receive an “E” for all requirements.
33
17E November 10, 2015 33 / 78
9. Participants must leave their work areas clean at the end of each day. Any participant who does not
do so may receive an “E” for all requirements. Barriers applied for Day 1 may be left in place for
Day 2.
10. Participants must manage excess amalgam appropriately. Any participant who does not do so may
be dismissed from the Assessment and receive an “E” for all requirements.
11. Participants are responsible for their own instruments and supplies. The NDEB and the Assessment
Centre will not be held responsible for instruments or personal supplies left unattended.
12. Participants are financially responsible for any damage caused to any supplied equipment.
13. The NDEB uses the series 200 typodont and simulated teeth from Kilgore International
(www.kilgoreinternational.com - 1-800-892-9999).
i. Series A21-200 pre-prepared teeth will be provided for the:
• Class II Amalgam Restoration
• Class IV Composite Resin Restoration
• Class II Composite Resin Restoration
• Provisional Crown Restoration
34
17E November 10, 2015 34 / 78
ii. Series S12-200 teeth with simulated enamel, dentin and pulp will be provided for the:
• Endodontic Access Preparation
Simulated enamel and dentin: The simulated enamel and dentin in the crown of the teeth
are white in colour and are made of a uniform composite resin material with no
demarcation between the simulated enamel and dentin. The simulated dentin in the root of
the teeth is made of clear resin. The teeth have been manufactured so that procedures may
be performed using normal pressure with a dental bur and, if desired, finishing can be done
using normal pressure with sharp hand instruments. Fractures may occur if an attempt is
made to remove a large section of tooth structure or if excessive force and/or dull
instruments are used.
Simulated pulp chamber and canals: The simulated dental pulp chamber and canals are
hollow spaces lined with red colouring.
iii. Series A22-200 with simulated enamel, dentin and pulp will be provided for the:
• Full Metal Crown Preparation
• Metal-ceramic Crown Preparation
Simulated enamel: The simulated enamel is white in colour and is made of composite
resin that is harder than the simulated dentin. The teeth have been manufactured so that
procedures may be performed using normal pressure with a dental bur and, if desired,
finishing can be done using normal pressure with sharp hand instruments. Fractures may
occur if an attempt to remove a large section of enamel is made or if excessive force and/or
dull instruments are used.
Simulated dentin: The simulated dentin is light beige and is softer than the simulated
enamel.
Simulated pulp chamber and canals: The simulated dental pulp chamber and canals are
hollow spaces lined with red colouring.
Participants are cautioned not to use mechanical tooth separators and not to be aggressive
with the use of interproximal wedges, as these may cause fractures to the simulated teeth.
35
17E November 10, 2015 35 / 78
iv. Series A27-200 teeth with simulated enamel, dentin and caries will be provided for the:
• Class II Amalgam Preparation
• Class III Composite Resin Preparation
Simulated enamel: The simulated enamel is white in colour and is made of composite
resin that is harder than the simulated dentin and simulated caries. The teeth have been
manufactured so that procedures may be performed using normal pressure with a dental bur
and, if desired, finishing can be done using normal pressure with sharp hand instruments.
Fractures may occur if an attempt to remove a large section of enamel is made or if
excessive force and/ or dull instruments are used.
Simulated dentin: The simulated dentin is yellow in color and is softer than the simulated
enamel.
Simulated caries: The simulated caries in dentin is dark brown in colour and is softer
than the simulated enamel but is of similar hardness to the simulated dentin. In anterior
teeth, there is also a cavitation (hole) in the simulated enamel on the proximal surface.
This cavitation extends through the simulated enamel into the simulated dentin and must be
included as part of the preparation.
Participants are cautioned not to use mechanical tooth separators and not to be aggressive
with the use of interproximal wedges, as these may cause fractures to the simulated teeth.
The manufacturing process for teeth with simulated caries ensures that caries depth and
extent is standardized for each tooth used as part of the Assessment.
As a result of the manufacturing process, there may be a small cement-filled space between
the simulated enamel and the simulated dentin which may appear grey in colour. This is
not simulated caries.
Please Note:
Teeth are slightly softer and more easily abraded than natural teeth.
The use of metal hand instruments in cavity preparations will leave a grey stain.
36
17E November 10, 2015 36 / 78
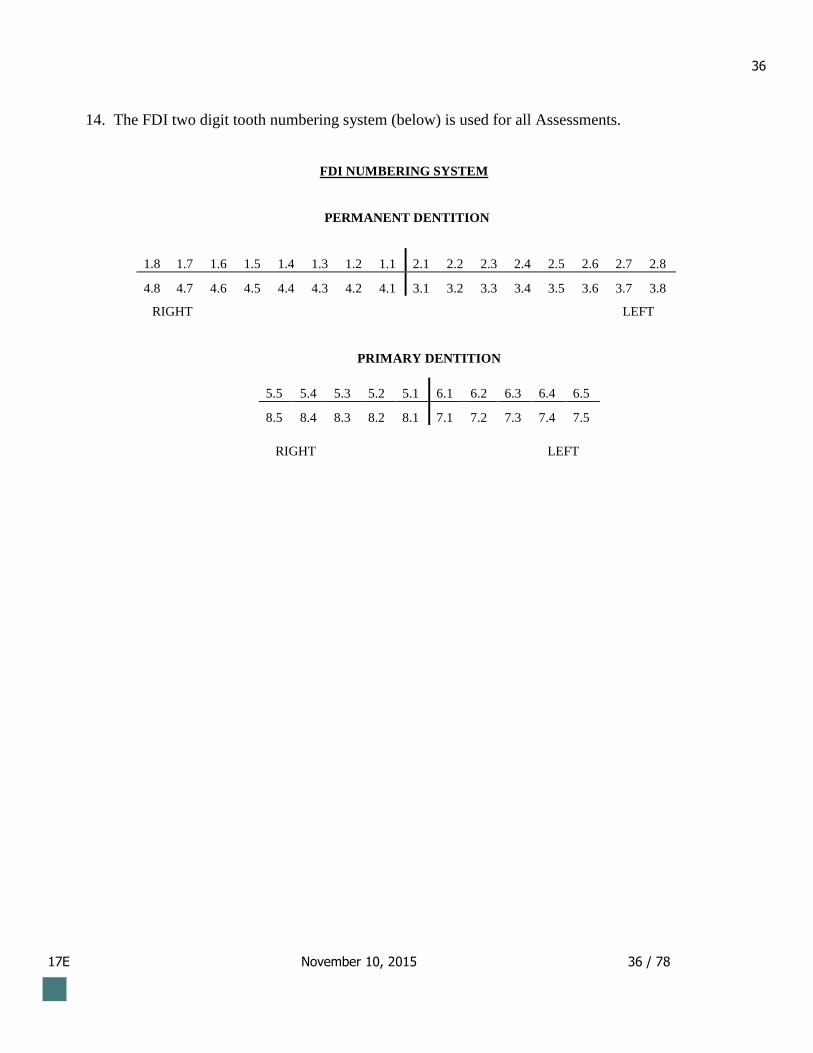
14. The FDI two digit tooth numbering system (below) is used for all Assessments.
FDI NUMBERING SYSTEM
PERMANENT DENTITION
1.8 1.7 1.6 1.5 1.4 1.3 1.2 1.1 2.1 2.2 2.3 2.4 2.5 2.6 2.7 2.8
4.8 4.7 4.6 4.5 4.4 4.3 4.2 4.1 3.1 3.2 3.3 3.4 3.5 3.6 3.7 3.8
RIGHT LEFT
PRIMARY DENTITION
RIGHT LEFT
5.5 5.4 5.3 5.2 5.1 6.1 6.2 6.3 6.4 6.5
8.5 8.4 8.3 8.2 8.1 7.1 7.2 7.3 7.4 7.5
37
17E November 10, 2015 37 / 78
VII REGULATIONS
1. Participants must be punctual for both days of the Assessment. Participants arriving late for an
Assessment may not be admitted. Extra time will not be granted to participants who arrive late.
2. Family or friends must not accompany participants as space at the Assessment centre is provided
ONLY for participants and staff.
3. Participants must not use devices with recording abilities, radios, cameras, cell phones, pagers or
other electronic aids/devices in the Assessment room.
4. Participants may have printed copies of the Assessment of Clinical Skills Protocol in the clinic.
5. The ability of a participant to read, interpret and comply with instructions and other written
material is part of the Assessment. Assessment Supervisors and Invigilators will not answer
questions involving Assessment content.
6. Participants that are unable to attend an examination for religious reasons must request special
consideration for an alternate session to the NDEB office prior to the Registration Deadline Date.
The request must be in writing and must include original documentation confirming the inability to
attend for religious reasons. The NDEB will accommodate requests for alternate sessions, but may
have to offer alternate locations.
7. Participants requiring special Assessment accommodation, including accommodation due to a
diagnosed medical condition must request special consideration in writing to the NDEB office
within two (2) weeks of the registration deadline date. The request must include original
documentation indicating the accommodation measures required. Additional supporting
documentation may be requested by the NDEB office.
8. Consuming food and/or drink (including water) is not allowed in the Assessment room unless
special consideration for medical reasons has been granted by the NDEB office. The request must
include a medical certificate signed by a physician indicating the diagnosis and accommodation
measures required.
9. “Participant Communication” forms must be completed within the Assessment session time.
Additional time will not be allowed.

38
17E November 10, 2015 38 / 78
10. Participants must stop working at the indicated ending time. Participants must exit the clinic
when asked to by Invigilators.
11. Participants must abide by the above Regulations. Participants who do not do so may be given an
“E” for all requirements that day.
12. A participant who considers themself disadvantaged by a personal circumstance beyond the
participant’s control, occurring either immediately before or during the Assessment may, within one
week of this personal circumstance occurring, request that the NDEB make a special consideration
to void the results of the Assessment. The NDEB may grant permission for the participant to
withdraw from the Assessment. The participant may also request special consideration for a refund
of up to 50% of the Assessment fee.
17E November 10, 2015 39 / 78
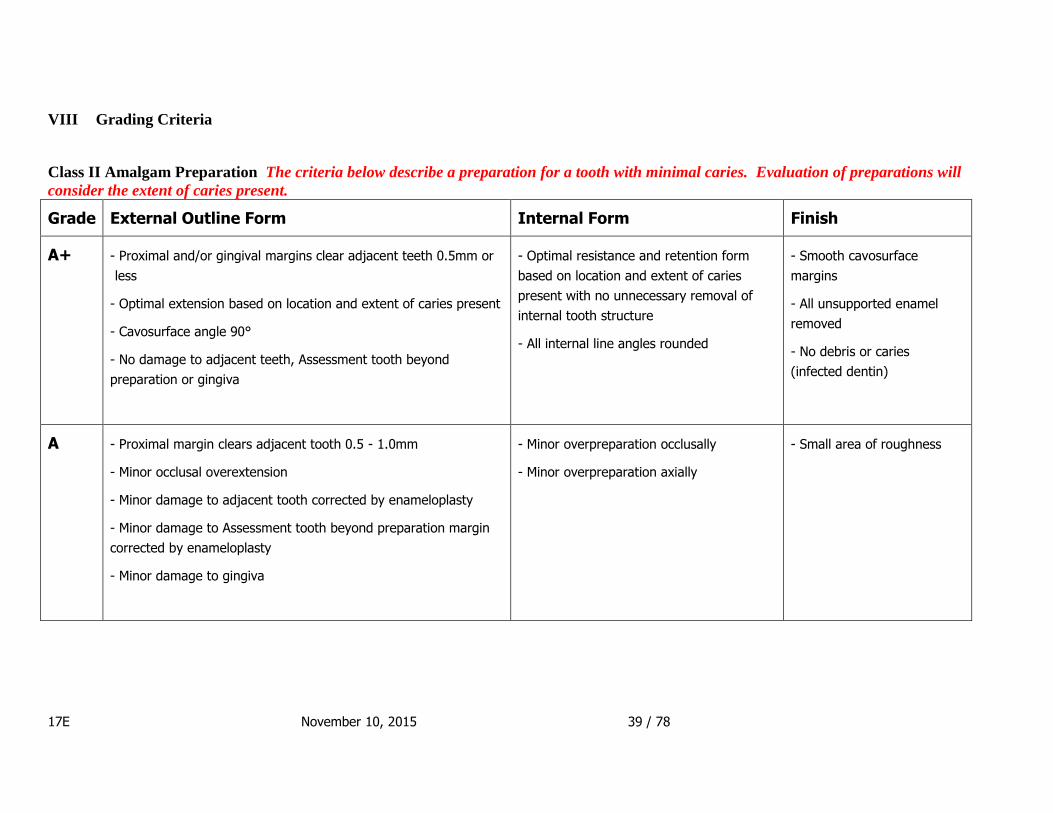
VIII Grading Criteria
Class II Amalgam Preparation The criteria below describe a preparation for a tooth with minimal caries. Evaluation of preparations will
consider the extent of caries present.
Grade External Outline Form Internal Form Finish
A+ - Proximal and/or gingival margins clear adjacent teeth 0.5mm or
less
- Optimal extension based on location and extent of caries present
- Cavosurface angle 90°
- No damage to adjacent teeth, Assessment tooth beyond
preparation or gingiva
- Optimal resistance and retention form
based on location and extent of caries
present with no unnecessary removal of
internal tooth structure
- All internal line angles rounded
- Smooth cavosurface
margins
- All unsupported enamel
removed
- No debris or caries
(infected dentin)
A - Proximal margin clears adjacent tooth 0.5 - 1.0mm
- Minor occlusal overextension
- Minor damage to adjacent tooth corrected by enameloplasty
- Minor damage to Assessment tooth beyond preparation margin
corrected by enameloplasty
- Minor damage to gingiva
- Minor overpreparation occlusally
- Minor overpreparation axially
- Small area of roughness

17E November 10, 2015 40 / 78
D - Proximal margin does not clear adjacent tooth
- Proximal margin clears adjacent tooth 1.0 - 1.5mm
- Proximal wall flared
- Unacceptable isthmus junction
- Buccal-lingual width too wide
- Buccal-lingual width too narrow
- Minor damage to adjacent tooth
- Minor damage to Assessment tooth beyond preparation margin
- Unacceptable damage to gingiva
- Pulpal floor too deep 2.5 - 3.0mm
- Pulpal floor too shallow 1.0 - 1.5mm
- Axial wall too deep 1.5 - 3.0mm
- Axial wall too shallow < 0.5mm
- Unnecessary removal of tooth structure
- Divergent walls
- Sharp line angle
- Undefined line angle
- Unacceptable roughness
- Unacceptable unsupported
enamel
- Presence of debris
E - Proximal margin clears adjacent tooth > 1.5mm
- Significant occlusal overextension
- Significant occlusal underextension
- Major damage to adjacent tooth
- Major damage to Assessment tooth beyond preparation margin
- Excessive damage to gingiva
- Pulpal floor too deep > 3.0mm
- Pulpal floor too shallow < 1.0mm
- Axial wall too deep > 3.0mm
- Excessive overpreparation. Alternate
design or RCT required
- Excessive roughness
- Excessive unsupported
enamel
- Caries remaining on axial or
pulpal
- Caries remaining at
dentinoenamel junction
17E November 10, 2015 41 / 78
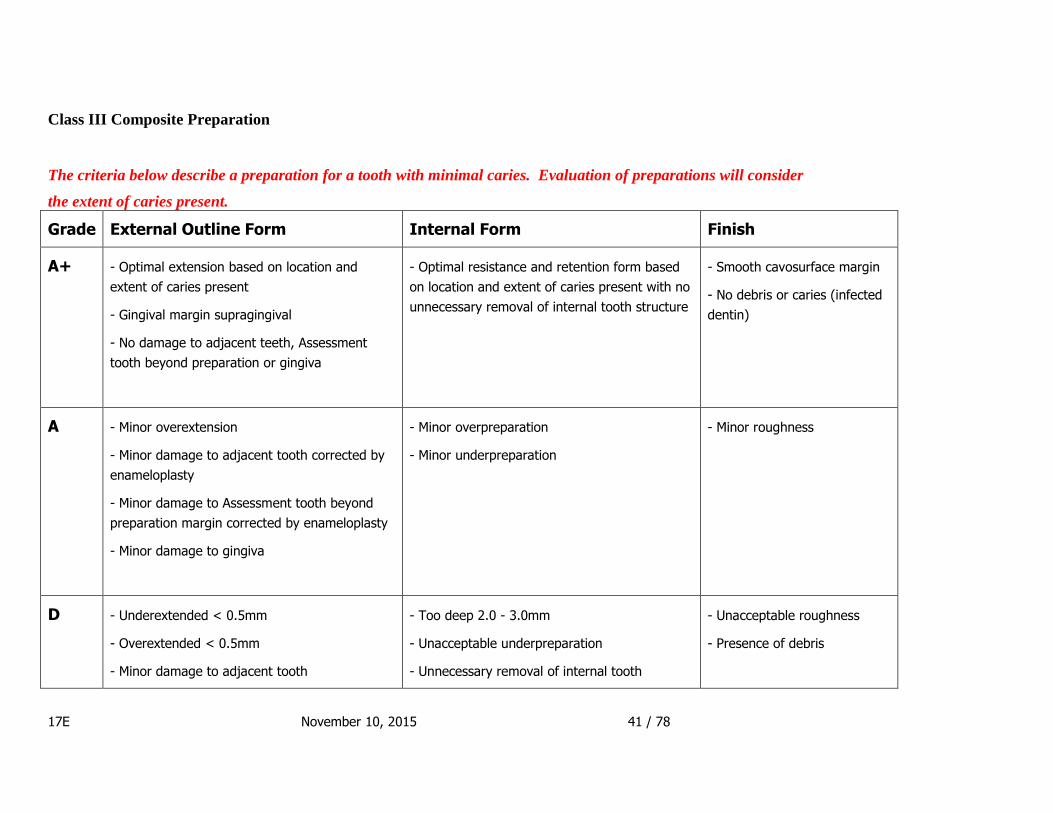
Class III Composite Preparation
The criteria below describe a preparation for a tooth with minimal caries. Evaluation of preparations will consider
the extent of caries present.
Grade External Outline Form Internal Form Finish
A+ - Optimal extension based on location and
extent of caries present
- Gingival margin supragingival
- No damage to adjacent teeth, Assessment
tooth beyond preparation or gingiva
- Optimal resistance and retention form based
on location and extent of caries present with no
unnecessary removal of internal tooth structure
- Smooth cavosurface margin
- No debris or caries (infected
dentin)
A - Minor overextension
- Minor damage to adjacent tooth corrected by
enameloplasty
- Minor damage to Assessment tooth beyond
preparation margin corrected by enameloplasty
- Minor damage to gingiva
- Minor overpreparation
- Minor underpreparation
- Minor roughness
D - Underextended < 0.5mm
- Overextended < 0.5mm
- Minor damage to adjacent tooth
- Too deep 2.0 - 3.0mm
- Unacceptable underpreparation
- Unnecessary removal of internal tooth
- Unacceptable roughness
- Presence of debris
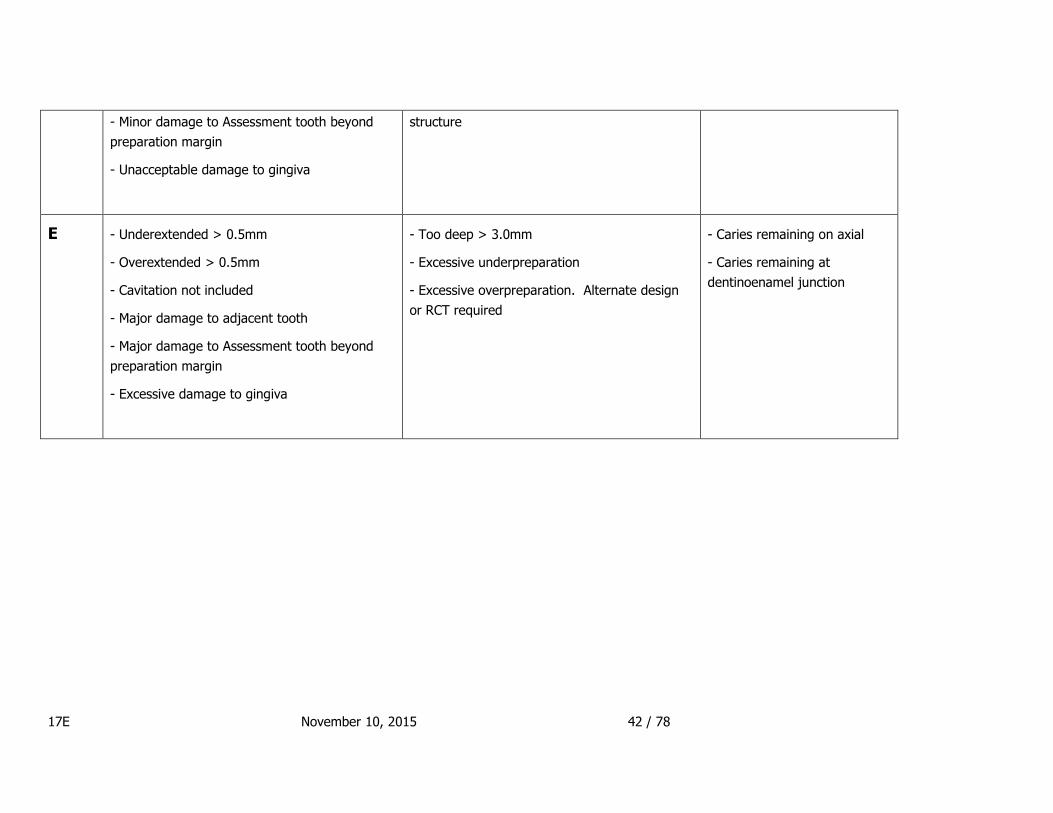
17E November 10, 2015 42 / 78
- Minor damage to Assessment tooth beyond
preparation margin
- Unacceptable damage to gingiva
structure
E - Underextended > 0.5mm
- Overextended > 0.5mm
- Cavitation not included
- Major damage to adjacent tooth
- Major damage to Assessment tooth beyond
preparation margin
- Excessive damage to gingiva
- Too deep > 3.0mm
- Excessive underpreparation
- Excessive overpreparation. Alternate design
or RCT required
- Caries remaining on axial
- Caries remaining at
dentinoenamel junction

17E November 10, 2015 43 / 78
Full Metal Crown Preparation
Clearance will be measured from opposing teeth in maximal intercuspation and excursions.
Grad
e
Path of Draw and Axial
Convergence
Preservation of Tooth Vitality &
Structural Durability
Finish and Margin
A+ - Preparation allows the fabrication of a
restoration with optimal retention and
contour
- No undercuts
- Axial convergence 6° - 10°
- Optimal preparation has been performed to permit
fabrication of a functional restoration
- Axial reduction 0.5 – 1.0mm
- Clearance 1.5mm
- Margin width 0.5mm
- No sharp angles
- No damage to adjacent teeth
- Margin optimally placed, defined, smooth and
identifiable
- Margin smooth, continuous and has no steps
- Positioned 0.5mm supragingival
- Preparation walls are smooth
- No damage to gingiva
A - Minor undercuts. Manageable by lab
- Axial convergence 10° - 20°
- Axial reduction 1.0-1.5mm
- Clearance >1.0 but < 1.5mm
or >1.5 but < 2.0mm
- Minor damage to adjacent tooth corrected by
enameloplasty
- Margin continuous with minor irregularity
- Located supragingival < 0.5mm or 0.6 - 1.0mm
- Located subgingival < 0.5mm
- Minor damage to gingiva
D - Will not draw. Modification required.
- Axial convergence 20° - 25°
- Axial reduction < 0.5mm
- Clearance 0.5 – 1.0mm or 2.0 – 3.0mm
- Sharp cusp
- Indistinct, discontinuous or rough
- Located supragingival 1.0 - 2.0mm
- Located sub-gingival 0.5 - 1.0mm

17E November 10, 2015 44 / 78
- Sharp line angle
- Minor damage to adjacent tooth
- Incorrect form
- Unsupported enamel (lipping)
- Unacceptable roughness of axial wall
- Unacceptable damage to gingiva
E - Will not draw. Major modification
required.
- Axial convergence >25°
- Axial reduction – no reduction or >1.5mm
- Clearance < 0.5 or > 3.0mm
- Pulpal blush or exposure
- Major damage to adjacent tooth
- Alternative preparation or RCT needed
- Excessively indistinct, discontinuous or rough
- No discernible margin
- Located supragingival > 2.0mm
- Located subgingival > 1.0mm
- Excessively unsupported enamel (lipping)
- Excessive damage to gingiva

17E November 10, 2015 45 / 78
Metal-ceramic Crown Preparation
Clearance will be measured from opposing teeth in maximal intercuspation and excursions.
Grade Path of Draw and
Axial Convergence
Preservation of Tooth Vitality & Structural Durability Finish & Margin
A+
- Preparation allows the
fabrication of a
restoration with optimal
retention and contour
- No undercuts
- Axial convergence 6° -
10°
- Optimal preparation has been performed to permit the fabrication of an
esthetic and functional restoration
- Reduction: Labial, mesial, distal 1.2mm
Lingual 0.5mm (area to be restored by metal only)
1.0mm (area to be restored by metal and porcelain)
Incisal 2.0mm
- Clearance 2.0mm
- Width of margin: Labial 1.2mm - 1.5mm
Lingual 0.5mm
- Preparation is smooth and has no sharp areas
- No damage to adjacent teeth
- Margin is optimally placed, defined
and identifiable
- Margin is smooth, continuous and
has no steps
- Margin positioned 0.5mm
supragingival
- Preparation walls are smooth
- No damage to gingiva
A - Minor undercuts.
Manageable by lab
- Axial convergence 10°-
20°
- Reduction: Labial, mesial, distal 1.2 - 1.5mm
Lingual under reduced < 0.2 mm from optimal
over reduced < 0.5mm from optimal
Incisal 2.1-2.5mm
- Clearance 2.1- 2.5mm
- Minor damage to adjacent tooth corrected by enameloplasty
- Margin continuous with minor
irregularity
- Located supragingival < 0.5mm or
0.6 - 1.0mm
- Located subgingival < 0.5mm
- Minor damage to gingiva
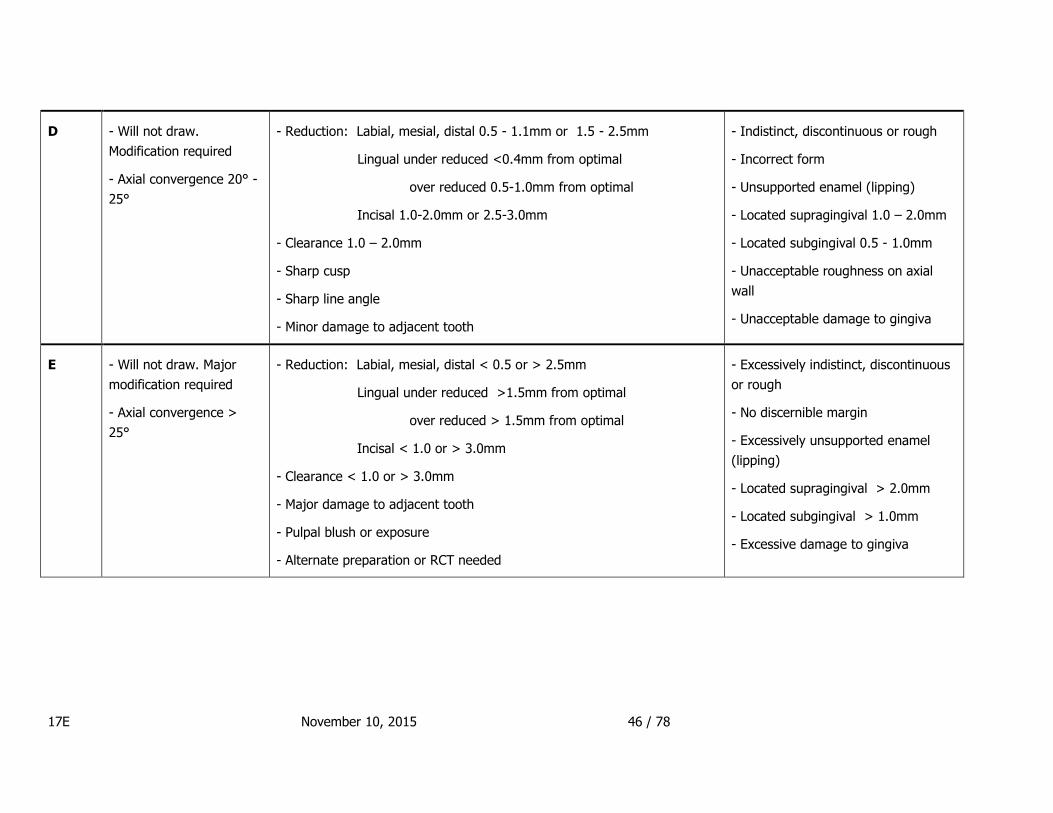
17E November 10, 2015 46 / 78
D - Will not draw.
Modification required
- Axial convergence 20° -
25°
- Reduction: Labial, mesial, distal 0.5 - 1.1mm or 1.5 - 2.5mm
Lingual under reduced <0.4mm from optimal
over reduced 0.5-1.0mm from optimal
Incisal 1.0-2.0mm or 2.5-3.0mm
- Clearance 1.0 – 2.0mm
- Sharp cusp
- Sharp line angle
- Minor damage to adjacent tooth
- Indistinct, discontinuous or rough
- Incorrect form
- Unsupported enamel (lipping)
- Located supragingival 1.0 – 2.0mm
- Located subgingival 0.5 - 1.0mm
- Unacceptable roughness on axial
wall
- Unacceptable damage to gingiva
E
- Will not draw. Major
modification required
- Axial convergence >
25°
- Reduction: Labial, mesial, distal < 0.5 or > 2.5mm
Lingual under reduced >1.5mm from optimal
over reduced > 1.5mm from optimal
Incisal < 1.0 or > 3.0mm
- Clearance < 1.0 or > 3.0mm
- Major damage to adjacent tooth
- Pulpal blush or exposure
- Alternate preparation or RCT needed
- Excessively indistinct, discontinuous
or rough
- No discernible margin
- Excessively unsupported enamel
(lipping)
- Located supragingival > 2.0mm
- Located subgingival > 1.0mm
- Excessive damage to gingiva
17E November 10, 2015 47 / 78
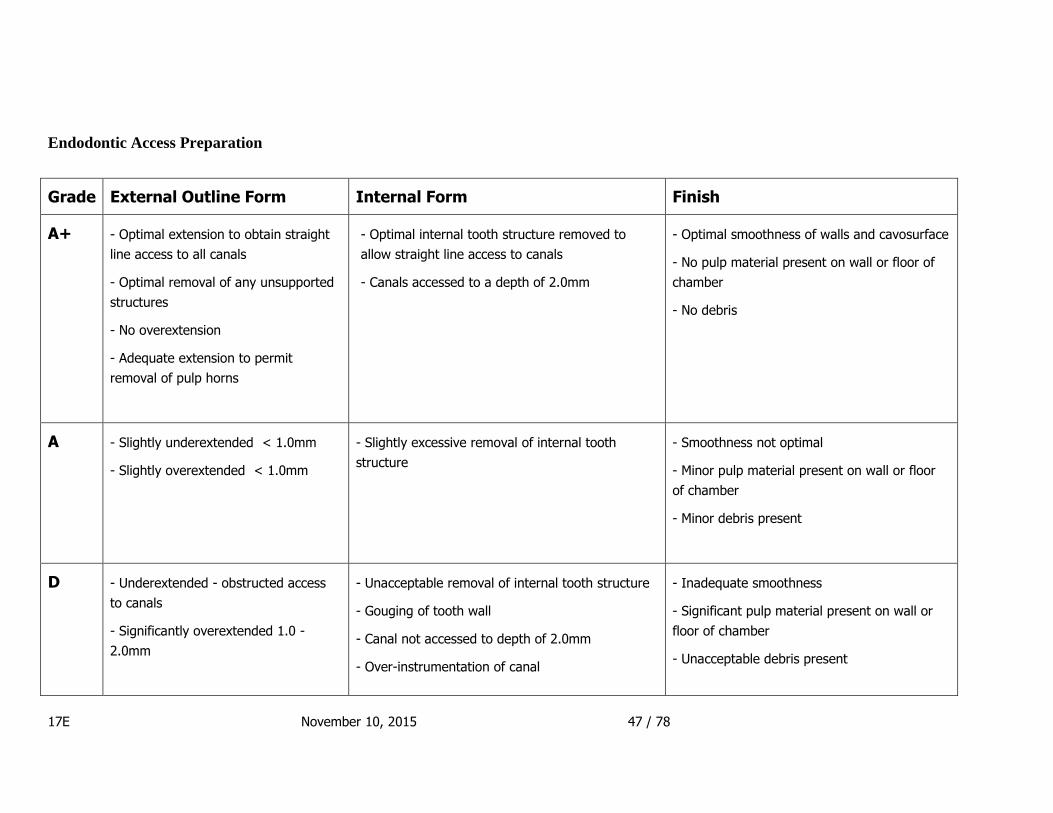
Endodontic Access Preparation
Grade External Outline Form Internal Form Finish
A+ - Optimal extension to obtain straight
line access to all canals
- Optimal removal of any unsupported
structures
- No overextension
- Adequate extension to permit
removal of pulp horns
- Optimal internal tooth structure removed to
allow straight line access to canals
- Canals accessed to a depth of 2.0mm
- Optimal smoothness of walls and cavosurface
- No pulp material present on wall or floor of
chamber
- No debris
A - Slightly underextended < 1.0mm
- Slightly overextended < 1.0mm
- Slightly excessive removal of internal tooth
structure
- Smoothness not optimal
- Minor pulp material present on wall or floor
of chamber
- Minor debris present
D - Underextended - obstructed access
to canals
- Significantly overextended 1.0 -
2.0mm
- Unacceptable removal of internal tooth structure
- Gouging of tooth wall
- Canal not accessed to depth of 2.0mm
- Over-instrumentation of canal
- Inadequate smoothness
- Significant pulp material present on wall or
floor of chamber
- Unacceptable debris present

17E November 10, 2015 48 / 78
E - Chamber not accessed
- Excessively underextended > 2.0mm
- Excessively overextended > 2.0mm
- Excessive removal of internal tooth structure
- Perforation
- Canal not accessed
- Excessive gouging of wall
- Excessive over-instrumentation of canal
- Separated instrument in canal
- Excessive roughness
- Excessive pulp material present on wall or
floor of chamber
- Debris obscuring chamber or canal
17E November 10, 2015 49 / 78
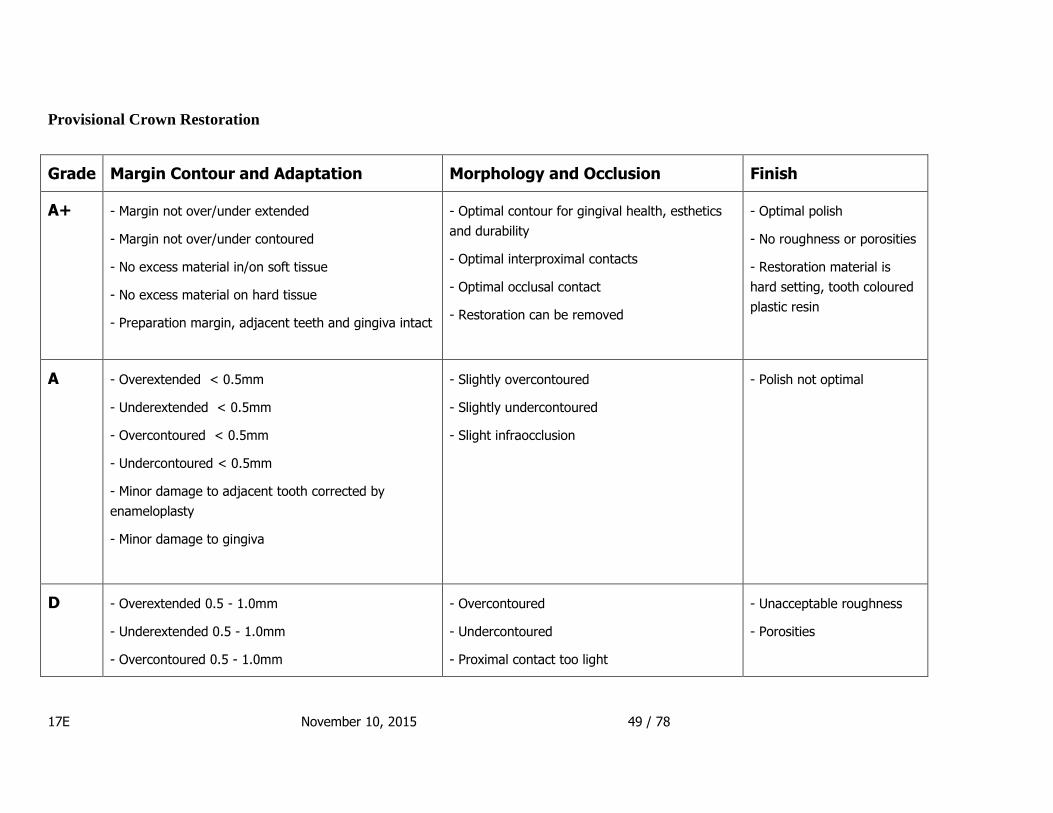
Provisional Crown Restoration
Grade Margin Contour and Adaptation Morphology and Occlusion Finish
A+ - Margin not over/under extended
- Margin not over/under contoured
- No excess material in/on soft tissue
- No excess material on hard tissue
- Preparation margin, adjacent teeth and gingiva intact
- Optimal contour for gingival health, esthetics
and durability
- Optimal interproximal contacts
- Optimal occlusal contact
- Restoration can be removed
- Optimal polish
- No roughness or porosities
- Restoration material is
hard setting, tooth coloured
plastic resin
A - Overextended < 0.5mm
- Underextended < 0.5mm
- Overcontoured < 0.5mm
- Undercontoured < 0.5mm
- Minor damage to adjacent tooth corrected by
enameloplasty
- Minor damage to gingiva
- Slightly overcontoured
- Slightly undercontoured
- Slight infraocclusion
- Polish not optimal
D - Overextended 0.5 - 1.0mm
- Underextended 0.5 - 1.0mm
- Overcontoured 0.5 - 1.0mm
- Overcontoured
- Undercontoured
- Proximal contact too light
- Unacceptable roughness
- Porosities

17E November 10, 2015 50 / 78
- Undercontoured 0.5 - 1.0mm
- Excess material in/ on soft tissue
- Excess material on hard tissue
- Damage to preparation margin
- Minor damage to adjacent tooth
- Unacceptable damage to gingiva
- Proximal contact too occlusal
- Proximal contact too gingival
- Proximal contact too tight
- No proximal contact < 0.5mm open
- Supraocclusion < 1.0mm
- Infraocclusion < 1.0mm
E - Overextended > 1.0mm
- Underextended > 1.0mm
- Overcontoured > 1.0mm
- Undercontoured > 1.0mm
- Excessive amount of excess material in/on soft tissue
- Excessive amount of excess material on hard tissue
- Major damage to adjacent tooth
- Excessive damage to gingiva
- Needs major revision or new provisional
- Significantly overcontoured
- Significantly undercontoured
- No proximal contact > 0.5mm open
- Supraocclusion > 1.0mm
- Infraocclusion > 1.0mm
- Restoration cannot be removed
- Restoration submitted broken or cracked
- Restoration broken or cracked due to
excessive occlusion or lack of structural integrity
- Excessive roughness
- Excessive porosity
- Inappropriate restorative
material

17E November 10, 2015 51 / 78
Class II Composite Resin Restoration
These criteria do not include shade matching, which is NOT part of the evaluation.
Grade Restoration Quality and Finish
Margin Contours and Function
A+ - Uniform smoothness
- Uniform polish matching tooth
surface
- No contamination of resin (no
stain or inclusions)
- Junction of tooth/ restoration not detectable
or slightly detectable with explorer
- No excess resin past preparation margin
- No damage to adjacent teeth, Assessment
tooth or gingiva
- Physiologic tooth contours of occlusal and proximal
surfaces optimally restored
- Optimal proximal contact restored
- No excess resin in/on soft tissue
- No excess resin on hard tissue
A - Areas needing more polish
- Minor contamination of resin not
affecting durability or esthetics
- Minor amount of resin beyond preparation
margin
- Minor damage to adjacent tooth corrected
by enameloplasty
- Minor damage to Assessment tooth
corrected by enameloplasty
- Minor damage to gingiva
- Undercontoured < 0.5mm
- Overcontoured < 0.5mm
- Proximal contact slightly too occlusal
- Proximal contact slightly too gingival
- Proximal contact slightly too broad
- Slight marginal ridge disharmony
D - Unacceptable roughness,
scratches or voids
- Porosities
- Contamination of resin that
- Deficiency/void at margin < 0.5mm
- Excess resin beyond preparation margin
requiring correction
- Undercontoured 0.5 - 1.0mm
- Overcontoured 0.5 – 1.0mm
- Poor occlusal morphology

17E November 10, 2015 52 / 78
needs correction
- Minor damage to adjacent tooth
- Minor damage to Assessment tooth
- Unacceptable damage to gingiva
- Light proximal contact
- Proximal contact too occlusal
- Proximal contact too gingival
- Proximal contact too broad/concave
- Proximal contact too tight/rough
- Marginal ridge disharmony < 1.0mm
- Excess resin in/on soft tissue
- Excess resin on hard tissue
- Excessive occlusal contact
E - Excessive roughness, scratches
or voids
- Excessive porosities
- Excessive contamination of resin
requiring replacement of entire
restoration.
- Incomplete polymerization
- Deficiency/void at margin > 0.5mm
- Excessive amount of excess resin beyond
preparation margin
- Major damage to adjacent tooth
- Major damage to Assessment tooth
- Excessive damage to gingiva
- Undercontoured > 1.0mm
- Overcontoured > 1.0mm
- Lack of physiologic contour
- No proximal contact
- Floss will not pass through proximal contact
- Marginal ridge disharmony > 1.0mm
- Excessive amount of excess resin in /on soft tissue
- Excessive amount of excess resin on hard tissue
- Restoration fractured or loose

17E November 10, 2015 53 / 78
Class IV Composite Resin Restoration
These criteria do not include shade matching, which is NOT part of the evaluation.
Grade Restoration Quality and Polish Margin Contours and Function
A+ - Uniform smoothness
- Uniform polish matching tooth surface
- No contamination of resin (no stains or
inclusions)
- Junction of tooth/ restoration not detectable or
slightly detectable with explorer
- No excess beyond preparation margin
- No damage to adjacent teeth, Assessment
tooth or gingiva
- Physiologic tooth contours restored
- Optimal proximal contact restored
- No excess resin in/on soft tissue
- No excess resin on hard tissue
- Appropriate occlusal contact
A - Areas needing more polish
- Minor contamination of resin not
affecting durability or esthetics
- Minor excess resin beyond preparation margin
- Minor damage to adjacent tooth corrected by
enameloplasty
- Minor damage to Assessment tooth corrected
by enameloplasty
- Minor damage to gingiva
- Undercontoured < 0.5mm
- Overcontoured < 0.5mm
- Proximal contact slightly too incisal
- Proximal contact slightly too gingival
- Proximal contact slightly too broad
D - Unacceptable roughness, scratches or
voids
- Porosities
- Contamination of resin that requires
correction
- Deficiency/void at margin < 0.5mm
- Excess resin beyond preparation margin
requiring correction
- Minor damage to adjacent tooth
- Minor damage to Assessment tooth
- Undercontoured 0.5 - 1.0mm
- Overcontoured 0.5 – 1.0mm
- Light proximal contact
- Proximal contact too incisal
- Proximal contact too gingival

17E November 10, 2015 54 / 78
- Unacceptable damage to gingiva - Proximal contact too broad/ concave
- Proximal contact too tight/rough
- Excess resin in/on soft tissue
- Excess resin on hard tissue
- Excessive occlusal contact
E - Excessive roughness, scratches or voids
- Excessive porosities
- Excessive contamination of resin
requiring replacement of entire
restoration.
- Incomplete polymerization
- Deficiency/void at margin > 0.5mm
- Excessive amount of excess resin beyond
preparation margin
- Major damage to adjacent tooth
- Major damage to Assessment tooth
- Excessive damage to gingiva
- Undercontoured > 1.0mm
- Overcontoured > 1.0mm
- Lack of physiologic contour
- No proximal contact
- Floss will not pass through proximal contact
- Excessive amount of excess resin in /on soft tissue
- Excessive amount of excess resin on hard tissue
- Restoration fractured or loose

17E November 10, 2015 55 / 78
Class II Amalgam Restoration
Grade Surface quality Margin Contours and Function
A+ - Uniform smoothness - Junction of tooth/restoration not detectable with
explorer
- No debris/loose amalgam in soft tissue
- No damage to adjacent teeth, Assessment tooth or
gingiva
- Physiologic tooth contours of occlusal and
proximal surfaces optimally restored
- Optimal proximal contact restored
- Optimal occlusal contact
A - Some areas of roughness - Margin slightly detectable
- Minor damage to adjacent tooth corrected by
enameloplasty
- Minor damage to Assessment tooth corrected by
enameloplasty
- Minor damage to gingiva
- Slightly undercontoured
- Slightly overcontoured
- Proximal contact slightly too occlusal
- Proximal contact slightly too gingival
- Proximal contact slightly too broad
- Slight marginal ridge disharmony
D - Roughness or scratches
requiring correction
- Excess amalgam at margin < 0.5mm
- Disharmony of amalgam-enamel margin < 0.5mm on
occlusal
- Debris/loose amalgam in soft tissue
- Undercontoured < 0.5mm
- Overcontoured < 0.5mm
- Poor occlusal morphology

17E November 10, 2015 56 / 78
- Minor damage to adjacent tooth
- Minor damage to Assessment tooth
- Unacceptable damage to gingiva
- Light proximal contact
- Proximal contact too occlusal
- Proximal contact too gingival
- Proximal contact too broad/concave
- Proximal contact too tight/rough
- Marginal ridge disharmony < 1.0mm
- Excessive occlusal contact
E - Excessive roughness or
scratches
- Deep or excessive voids
other than at margin
- Restoration must be
replaced because of surface
quality
- Excess amalgam at margin > 0.5mm
- Deficiency/void at margin requiring replacement of
restoration
- Excessive debris/loose amalgam in soft tissue
- Major damage to adjacent tooth
- Major damage to Assessment tooth
- Excessive damage to gingiva
- Undercontoured > 0.5mm
- Overcontoured > 0.5mm
- No proximal contact
- Marginal ridge disharmony > 1.0mm
- Restoration fractured or loose

17E November 10, 2015 57 / 78
Grade Rubber Dam Application
A+
- Appropriate and stable clamp
- Clamp secured with an appropriate length of dental floss
- Orientation provides an unrestricted airway
- Dam inverted on all isolated teeth
- All punch holes in appropriate positions
- Dam, frame and clamp positioned for optimal access, safety, moisture control
and patient comfort
A
- Dam is inverted on teeth in operative area only
- Dam is through contacts in operative area only, not affecting moisture control
- Minor correction to ligature required
- Minor deviations in punch hole locations
- Minor tears or holes not affecting moisture control in operative area
- Dam needs minor adjustment for proper
Access
Safety
Moisture control
Patient comfort
- Frame needs minor adjustment for proper
Access
Safety
Moisture control
Patient comfort
- Clamp needs minor adjustment for proper
Access

17E November 10, 2015 58 / 78
Safety
Moisture control
Patient comfort
- Floss needs minor adjustment for proper
Access
Safety
Moisture control
Patient comfort

17E November 10, 2015 59 / 78
D
One or two of the following deficiencies:
- Unnecessary trauma to gingiva or teeth
- Unstable clamp
- Unsecured or inadequately secured clamp
- Inappropriate ligature
- Patient airway compromised
- Dam caught on wings of clamp
- Inappropriate number of teeth isolated
- Frame incorrectly oriented
- Dam not inverted in operative area
- Dam not through all interproximal contact points
- Punch holes improperly positioned
- Tears or holes compromising moisture control
- Dam must be altered for proper
Access
Safety
Moisture control
Patient comfort
- Frame must be altered for proper
Access
Safety
Moisture control
Patient comfort
- Clamp must be altered for proper
Access
Safety
Moisture control
Patient comfort
- Floss must be altered for proper

17E November 10, 2015 60 / 78
Access
Safety
Moisture control
Patient comfort
E
Three or more of the above deficiencies or:
- Dam not placed in allotted time
- Improper position/placement of dam, frame, clamp or floss not allowing
treatment on indicated tooth
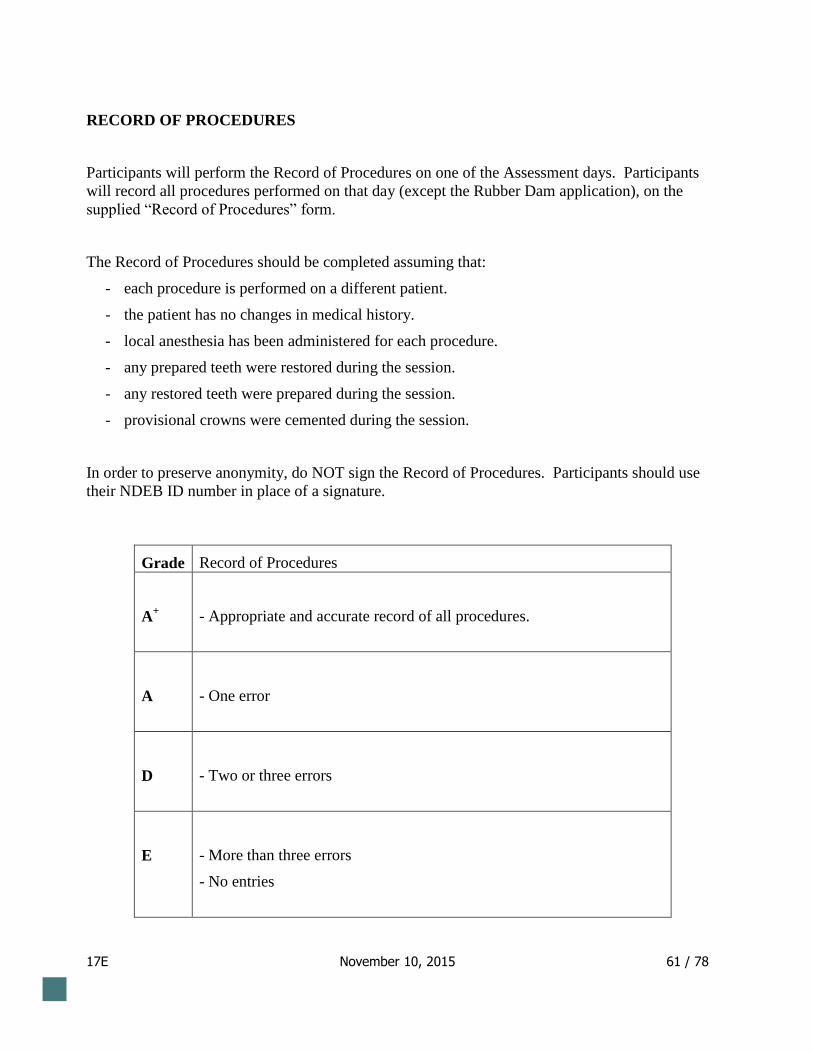
17E November 10, 2015 61 / 78
RECORD OF PROCEDURES
Participants will perform the Record of Procedures on one of the Assessment days. Participants
will record all procedures performed on that day (except the Rubber Dam application), on the
supplied “Record of Procedures” form.
The Record of Procedures should be completed assuming that:
- each procedure is performed on a different patient.
- the patient has no changes in medical history.
- local anesthesia has been administered for each procedure.
- any prepared teeth were restored during the session.
- any restored teeth were prepared during the session.
- provisional crowns were cemented during the session.
In order to preserve anonymity, do NOT sign the Record of Procedures. Participants should use
their NDEB ID number in place of a signature.
Grade Record of Procedures
A+
- Appropriate and accurate record of all procedures.
A
- One error
D
- Two or three errors
E
- More than three errors
- No entries

17E November 10, 2015 62 / 78
Errors on Record of Procedures:
Incorrect or incomplete record of procedures.
No or inappropriate date.
No or inappropriate record of updating medical history.
No or inappropriate record of type, quantity or location of local anesthesia.
No or incorrect tooth number identified.
No or incorrect restored surfaces identified.
No or inappropriate type and/or brand of restorative / provisional material or cement identified.
17E November 10, 2015 63 / 78
Incorrect technique or improper use of material identified.
No shade recorded.
No cementation of provisional restoration recorded.
Record not written in ink.
Record not legible.
Inappropriate correction of entry (original entry not visible through correction).
No ID number or ID number in inappropriate location.
INFECTION CONTROL
Participants will perform all requirements as if they were working on actual patients.
Infection control and material hygiene procedures will be observed by Assessment
Invigilators. Participants will NOT be informed of any recorded violations.
It will be assumed that all instruments are sterile at the beginning of each day.
If an instrument or treatment material is dropped during a procedure, a participant must notify
an Invigilator who will ask the participant to describe how the situation should be handled in
actual patient treatment and give permission to pick up the instrument or material.
The following modifications to infection control procedures for the purposes of this
Assessment:
- participants are allowed to wear treatment gloves while:
loosening the clamp that allows the patient’s head position to be adjusted and
adjusting the head.
using the amalgamators.
walking to and from the Rubber Dam Requirement operatories.
- participants do not need to wear treatment gloves while mixing, placing and removing
putty materials used in the making of stents.

17E November 10, 2015 64 / 78
Grade Infection Control
A+ - No violations of infection control or material hygiene errors
A - One infection control violation or material hygiene errors
D - Two infection control violations or material hygiene errors
E - Three or more infection control violations or material hygiene errors
Infection control and material hygiene errors include:
- Gloves not worn.
- Gloves worn outside of the operatory.
- Gloves have holes or tears.
- Unacceptable infection control procedures involving gloves such as wearing treatment
gloves when retrieving an article from a non-sterile area such as a storage bin or
cabinet or touching masks, glasses or hair.
- Mask not worn or not worn appropriately.
- Use of contaminated instruments or materials.
- No barriers placed on equipment touched with treatment gloves.
- Contamination of operating area or instruments.
- Eye protection not used.
- Hair not appropriately controlled.
- Unacceptable amalgam handling and disposal.
- Unacceptable handling and disposal of sharps.
- Safety of patient or operator is jeopardized by handling or placement of materials or
instruments.
- No or insufficient cooling water used with high speed handpiece.
IX GRADE DERIVATION GRID FOR INDIVIDUAL REQUIREMENTS

17E November 10, 2015 65 / 78
Each requirement is evaluated in one or three criteria categories.
Each category receives the lowest assigned grade of A+, A, D, or E.
1. Requirements with one criterion category
The grade assigned for these requirements will be determined as described in the
evaluation criteria.

17E November 10, 2015 66 / 78
2. Requirements with three criteria categories
The grade assigned for these requirements will be determined by the grades assigned in
the criteria categories.
A grade of A+
will be assigned for a requirement if 2 A+
and no D or E is assigned in any
category.
A grade of A will be assigned for a requirement if no more than 1 D and no E is assigned
in any criteria category.
A grade of D will be assigned for a requirement if 2 D’s and no E are assigned in any
criteria category.
A grade of E will be assigned for a requirement if 1 E or 3 D’s are assigned in any
criteria category.
X GRADE DERIVATION GRID FOR PASS/FAIL RESULT ( 12 requirements)
In order to pass the Assessment of Clinical Skills, on the 12 requirements, a participant must
obtain:
8 or more grades of A / A+ and no E grade
OR
9 or more grades of A / A+ and no more than 1 E grade
XI RESULTS
Participants will receive a grade for each requirement as determined by using the evaluation
criteria for the requirement and the “Grade Derivation Grid”. The final result for each
participant will be determined using the “Final Result” Grade Derivation Grid.
17E November 10, 2015 67 / 78
The results of the Assessment of Clinical Skills will be posted on a secure website that will be
accessible using the secure code you selected at the time of initial registration. Posting of
results will normally be done within 6 weeks and an e-mail notification of the posting will be
sent to participants.
The results of the Assessment of Clinical Skills will be sent to universities in Canada offering
a Qualifying or Degree Completion Program.
Results will not be released by telephone, fax or email.

17E November 10, 2015 68 / 78
XII APPEAL
Within three months of the release of results, a participant who has failed the Assessment of
Clinical Skills may make a submission in writing to the Board setting out the grounds for
requesting to have the results changed. Any such application for review must be accompanied
by the filing fee.
This submission must clearly identify the individual requirement results to be reviewed and
must set out the grounds for requesting to have the grade(s) changed. The NDEB Appeals
Committee will review the participant’s submission, all related correspondence, grading
sheets and the participant’s submitted typodont teeth.
Results of the Assessment review will be released on a participant’s secure online profile.
Participants will receive an email notification of the posting.
XIII REPEATS
A participant may take the Assessment of Clinical Skills three (3) times.
ACS Protocol 2014 FINAL-1.docx
17E November 10, 2015 69 / 78
Attachment 2 – Summary of Act
A Summary of the Act relating to The National Dental Examining Board of Canada
originally established in 1952 and revised in 1973.
Preamble to 1952 Act
Whereas the persons hereinafter named have by their petition prayed that it be enacted as hereinafter set
forth and it is expedient to grant the prayer of the petition: Therefore Her Majesty, by and with the advice
and consent of the Senate and House of Commons of Canada, enacts as follows:
Preamble to 1973 Revision
Whereas The National Dental Examining Board of Canada, hereinafter called "the Board", has by its petition
prayed that it be enacted as hereinafter set forth, and it is expedient to grant the prayer of the petition:
Therefore Her Majesty, by and with the advice and consent of the Senate and House of Commons of
Canada, enacts as follows:
1973 Section 1: Name in French
The Board may use, in the transaction of its business, either the name The National Dental Examining Board
of Canada or the name Le Bureau national d'examen dentaire du Canada, or both of such names as and
when it so elects. It may sue or be sued in either or both of such names, and any transaction, contract or
obligation entered into or incurred by the Board in either or both of the said names shall be valid and
binding on the Board.
1973 Section 2: Existing rights saved
Nothing contained in section 1 shall in any way alter or affect the rights or liabilities of the Board, except as
therein expressly provided, or in any way affect any proceeding or judgment now pending, either by or in
favour of or against the Board, which, notwithstanding the provisions of section 1, may be prosecuted,
continued, completed and enforced as if this Act had not been passed.
Incorporation and Composition (in the 1952 Act)
1. Harold M. Cline, doctor of dental surgery, of the city of Vancouver in the province of British Columbia, Gustave Ratte, doctor of dental surgery, of the city of Quebec in the province of Quebec, and Don W. Gullett, doctor of dental surgery, of the city of Toronto, in the province of Ontario, together with such persons as may hereafter become members of the Board as hereinafter provided, are incorporated under the name of "The National Dental Examining Board of Canada", hereinafter called "the Board”.
17E November 10, 2015 70 / 78
2. The persons named in section one of this Act shall be provisional members of the Board with power to organize the Board as in this Act provided.
3. The head office of the Board shall be at the city of Toronto, in the province of Ontario, or at such other place as the Board may determine by by-law from time to time.
4. (1) The Board shall be composed of
(a) one member appointed as its representative by the appropriate licensing body of each
province in Canada;
and
(b) two members appointed by the Council on Dental Education of the Canadian Dental
Association.
(2) The term of office for each member of the Board shall be three years, except in respect of the
members appointed to constitute the first Board.
(3) The term of office for one-half of the members of the first Board shall be two years and for
the other one-half shall be four years; the members constituting each such one-half shall be
chosen by lot in such manner as the Board may determine.
(4) A member of the Board on the expiration of his term of office, if properly qualified, shall be
eligible for reappointment.
(5) If the appropriate licensing body of any province fails to appoint a member of the Board
within a reasonable time a vacancy occurs, the Secretary of the Board shall notify such licensing
body and require such licensing body to make such appointment and certify the result to the
Board within one month of the date of service of the notice.
(6) All members of the Board shall continue in office until their successors are appointed or until
expiration of their term of office if their successors are appointed before the expiration of such
term of office.
5. (1) The appropriate licensing body of any province may at any time upon twelve month's notice to the Board, withdraw from participation in and recognition of the activities of the Board, and such licensing body shall not thereafter, so long as such withdrawal continues, be entitled to appoint any representative to the Board.
(2) The Board may upon the application of any licensing body which has so withdrawn, restore
the participation and representation of such licensing body.
17E November 10, 2015 71 / 78
Purposes of the Board (revised by 1973 Act)
“6. The purposes of the Board shall be
(a) to establish qualifying conditions for a single national standard certificate of qualification for
general practitioner dentists;
(b) to establish qualifying conditions for national standard certificates of qualification for dental
specialists subject to the approval of The Royal College of Dentists of Canada;
(c) to ensure that the rules and regulations governing examinations will be acceptable to all
participating licensing bodies and provide for the conducting of examinations in a manner fair
and equitable for all concerned; and
(d) to promote enactment, with the consent and at the instance of the provincial licensing
bodies, of provincial legislation necessary or desirable to supplement the provisions of this Act."
Powers of the Board (revised by 1973 Act)
“7. The Board shall have power to
(a) establish qualifications for general practitioner dentists to ensure that the qualifications may
be recognized by the appropriate licensing bodies in all provinces of Canada;
(b) establish, subject to the approval of the Royal College of Dentists of Canada, qualifications
for dental specialists, to ensure that, in each case the qualifications may be recognized by the
appropriate licensing bodies in all provinces of Canada;
(c) establish the conditions under which a general practitioner dentist ay obtain and hold a
certificate of qualification;
(d) establish subject to the approval of The Royal College of Dentists of Canada, the conditions
under which a dental specialist may obtain and hold a certificate of qualification;
(e) prescribe compulsory examinations as evidence of qualifications for registration, subject to
the rights of The Royal College of Dentists of Canada as hereinafter set forth;
(f) establish and maintain a body of examiners to hold examinations and to recommend the
granting of certificates of qualification to general practitioner dentists;
(g) establish and maintain a body of examiners appointed by The Royal College of Dentists of
Canada to hold examinations and make recommendations concerning the granting of certificates
of qualification of properly trained dental specialists;
(h) issue certificates of qualification to general practitioner dentists and dental specialists in
accordance with the recommendation of the examiners;

17E November 10, 2015 72 / 78
(i) establish a register for Canada of general practitioner dentists and dental specialists who have
been granted certificates of qualification by the Board;
(j) delete from the register the name of any person whose provincial registration has been cancelled
or suspended and to restore such name to the register if and when such cancellation or suspension
is reversed, or the period of suspension is terminated; and (k) publish and revise the register from
time to time."
Bylaws (1952 Act)
8. (1) The Board may make such by-laws and regulations, not contrary to law or the provisions of
this Act, as it may deem necessary or advisable for
(a) the government and management of its business and affairs;
(b) the selection and election or appointment and remuneration of officers and employees
and prescription of their respective powers and duties;
(c) the imposition and collection of dues or fees; and
(d) the carrying into effect of the purposes of the Board and its powers under this Act.
(2) The Board may, from time to time alter or repeal all or any of such by-laws or regulations as
it may see fit.
(3) No such by-law or regulation shall be enacted, altered or repealed except with the
concurrence of two-thirds of the representatives on the Board of the provincial licensing bodies
then represented on the Board.
Property (1952 Act)
9. The Board may acquire, own, hold, deal with and dispose of, subject to the provisions of
applicable provincial laws, any real and personal estate and property rights and privileges necessary
or expedient for the purposes of the Board.
Ability to borrow money (1952 Act)
10. The Board shall have power to
(a) borrow money on the credit of the Board when required for the purposes of the Board
and to give security for any sum or sums of money so borrowed;
and
(b) draw, make, accept and endorse all bills of exchange and promissory notes necessary
for the purposes of the Board under the hands of such officers as may be designated by the
by-laws and in no case shall it be necessary that the seal of the Board be affixed thereto nor

17E November 10, 2015 73 / 78
shall the signing officers be individually responsible therefore, provided that nothing herein
shall be construed to authorize the Board to issue notes or bills of exchange payable to
bearer or intended to be circulated as money or as notes or bills of a bank.
Certificate of Qualification for Specialists (revised 1973 Act)
"11. (1) The Board shall issue its certificate of qualification to all Fellows of The Royal College of
Dentists of Canada who are dental specialists, and whose specialties are recognized by the Canadian
Dental Association and who make application for such a certificate within five years from the date on
which this Act comes into force.
(2) In the event of the dissolution of The Royal College of Dentists of Canada, all powers
conferred upon it herein shall become vested in The National Dental Examining Board. Any
reference in this Act to The Royal College of Dentists of Canada or The National Dental
Examining Board shall include their successors or assigns."
17E November 10, 2015 74 / 78
Attachment 3 – Competencies for a Beginning Dental Practitioner in
Canada
A competent beginning dental practitioner in Canada must be able to provide oral health care for the benefit
of individual patients and communities in a culturally sensitive manner.
Competency assumes that all behaviours are supported by foundation knowledge and skills in biomedical,
behavioural and clinical dental science and by professional behaviour. Beginning dental practitioners in
Canada must be able to apply foundation knowledge and skills to justify their decisions and actions and to
evaluate outcomes. Therefore, foundation knowledge, skills and professional behaviour are understood to be
a part of every competency.
Competency also assumes that all behaviours are performed to an acceptable level and that the practitioner
can evaluate their quality and effectiveness. Competency cannot be achieved without the ability to self-
evaluate. Moreover, there are no degrees of competence: a dentist is either competent or not competent.
The competencies below refer to general dental practice and include the management of patients of all ages
including those with special needs. It is assumed that all oral health care is provided in an ethical manner,
in accordance with legal requirements at the national and provincial level.
A beginning dental practitioner in Canada must be competent to:
1. recognize the determinants of oral health in individuals and populations and the role of dentists in health promotion, including the disadvantaged.
2. recognize the relationship between general health and oral health.
3. evaluate the scientific literature and justify management recommendations based on the level of evidence available.
4. communicate effectively with patients, parents or guardians, staff, peers, other health professionals and the public.
5. identify the patient’s chief complaint/concern and obtain the associated history.
6. obtain and interpret a medical, dental and psychosocial history, including a review of systems as necessary, and evaluate physical or psychosocial conditions that may affect dental management.
7. maintain accurate and complete patient records in a confidential manner.
8. prevent the transmission of infectious diseases by following current infection control guidelines.
9. perform a clinical examination.
10. differentiate between normal and abnormal hard and soft tissues of the maxillofacial complex.
11. prescribe and obtain the required diagnostic tests, considering their risks and benefits.
12. perform a radiographic examination.

17E November 10, 2015 75 / 78
13. interpret the findings from a patient's history, clinical examination, radiographic examination and from other diagnostic tests and procedures.
14. recognize and manage the anxious or fearful dental patient.
15. recognize signs of abuse and/or neglect and make appropriate reports.
16. assess patient risk (including, but not limited to, diet and tobacco use) for oral disease or injuries.
17. develop a problem list and establish diagnoses.
18. determine the level of expertise required for treatment and formulate a written request for consultation and/or referral when appropriate.
19. develop treatment options based on the evaluation of all relevant data.
20. discuss the findings, diagnoses, etiology, risks, benefits and prognoses of the treatment options, with a view to patient participation in oral health management.
21. develop an appropriate comprehensive, prioritized and sequenced treatment plan.
22. present and discuss the sequence of treatment, estimated fees, payment arrangements, time requirements and the patient’s responsibilities for treatment.
23. obtain informed consent including the patient’s written acceptance of the treatment plan and any modifications.
24. modify the treatment plan as required during the course of treatment.
25. provide education regarding the risks and prevention of oral disease and injury to encourage the adoption of healthy behaviors.
26. provide therapies for the prevention of oral disease and injury.
27. recognize and institute procedures to minimize occupational hazards related to the practice of dentistry.
28. achieve local anesthesia for dental procedures and manage related complications.
29. determine the indications and contraindications for the use of drugs used in dental practice, their dosages and routes of administration and write prescriptions for drugs used in dentistry.
30. manage dental emergencies.
31. recognize and manage systemic emergencies which may occur in dental practice.
32. manage conditions and diseases of the periodontium, provide periodontal treatment when indicated and monitor treatment outcomes.
33. assess the risk, extent and activity of caries and recommend appropriate non-surgical and surgical therapy.
34. manage dental caries, tooth defects and esthetic problems and, when restoration is warranted, use techniques that conserve tooth structure and preserve pulp vitality to restore form and function.
35. manage patients with orofacial pain and/or dysfunction.
36. manage surgical procedures related to oral soft and hard tissues and their complications
37. manage trauma to the orofacial complex.
38. manage conditions and pathology of the pulp and provide endodontic treatment when indicated.
17E November 10, 2015 76 / 78
39. manage abnormalities of orofacial growth and development and treat minor orthodontic problems.
40. recognize and manage functional and non-functional occlusion.
41. select and, where indicated, prescribe appropriate biomaterials for patient treatment.
42. manage partially and completely edentulous patients with prosthodontic needs including the provision of fixed, removable and implant prostheses.
43. make records required for use in the laboratory fabrication of dental prostheses and appliances.
44. design a dental prosthesis or appliance, write a laboratory prescription and evaluate laboratory products.
45. apply accepted principles of ethics and jurisprudence to maintain standards and advance knowledge and skills.
46. apply basic principles of practice administration, financial and personnel management to a dental practice.
47. demonstrate professional behaviour that is ethical, supercedes self-interest, strives for excellence, is committed to continued professional development and is accountable to individual patients, society and the profession.
Definition
To “manage” the oral health care needs of a patient is assumed to include all actions performed by a health
care provider that are designed to alter the course of a patient’s condition. Such actions may include
providing education, advice, treatment by the dentist, treatment by the dentist after consultation with
another health care professional, referral of a patient to another health care professional, monitoring
treatment provided, but also may include providing no treatment or observation. “Manage” assumes the use
of the least invasive therapy necessary to gain a successful outcome in accordance with patient wishes

17E November 10, 2015 77 / 78
Attachment 4 – External Evaluation Procedures
A Report by the Commissioner of Examinations. Malcolm G. Taylor, Ph.D.-1966
A Study of the Accreditation Mechanism - 1983
Workshop on Preclinical and Clinical Examinations - 1985
1989/90 Certification Review Committee (CRC) to explore whether the granting of a certificate on the basis
of accreditation alone continues to be acceptable
A Report of NDEB by-laws and policies by the Honourable W.D. Parker - 1990
A psychometric analysis of examination evaluation methods by Dr. A. Rothman - 1991
Symposium - 1992
A Workshop on Clinical Competencies - 1993
A Consensus Conference on Certification of Graduates of Dental Programs accredited by the ADA
Commission of Dental Accreditation - 1995
Conference on Competency in Oral Health Care, Education & Practice – 2000
NDEB Program Evaluation – André Boulais – 2001
Strategic Plan for 2006 – 2010
Review and Validation of Statistical Procedures – Mr. Thomas Maguire – 2004
CDA/DCF Teaching Conference: Review of Competencies for a Beginning Dental Practitioner in Canada -
2004
Written Examination Standard Setting Study - Chad W. Buckendahl – July 2007
OSCE Examination Standard Setting Study - Chad W. Buckendahl – February 2008
17E November 10, 2015 78 / 78
Attachment 5 – Publications
Chambers DW, Gerrow JD. Manual for Developing and Formatting Competency Statements. J Dent Educ,
58(5): 361, May 1994.
Gerrow JD, Boyd MB, Doyle MG, Scott D. Clinical Evaluation in Prosthodontics: Practical Methods to Improve
Validity and Reliability, J Prosthet Dent 75(6):675, June 1996.
Boyd MA, Gerrow JD, Chambers DW, Henderson BJ. Competencies for Dental Licensure in Canada. J Dent
Educ, 60(10):842, October 1996.
Boyd MA, Gerrow JD. Certification of Competence: A National Standard for Dentistry in Canada. J Can Dent
Assoc, 62(12):928, December 1996.
Gerrow JD, Boyd MA, Duquette P, Bentley KA. Results of the National Dental Examining Board of Canada’s
Written Examination and Implications for Licensure. J Dent Educ 6 (12): 921, December 1997.
Gerrow JD, Chambers DW, Henderson BJ. Boyd MA. Competencies for a Beginning Dental Practitioner in
Canada. J Can Dent Assoc, 64(2):94, February 1998.
Gerrow JD, Boyd MA, Donaldson D, Watson PA, Henderson BJ. Modifications to the National Dental
Examining Board of Canada’s Certification Process. J Can Dent Assoc, 64(2):98, February 1998.
Gerrow JD, Boyd MB, Scott D, Boulais AP. Use of Discriminant and Regression Analysis to Improve
Certification Board Examinations. J Dent Educ, 63(6):459, June 1999.
Gerrow JD, Boyd MA, Scott D. Portability of licensure in Canada based on accreditation and certification. J
Am Coll Dent, 70(1): 8, May 2003.
Gerrow JD, Murphy HJ, Boyd MA, Scott D. Concurrent validity of written and OSCE components of the
Canadian dental certification examinations. J Dent Educ, 67(8): 896, August 2003.
Gerrow JD, Murphy HJ Boyd MA, Scott D. An Analysis of the Contribution of a Patient-Based Component to
a Clinical Licensure Examination. JADA 137:1434, October 2006.
Gerrow JD Murphy HJ Boyd MA. A Validity Survey of Competencies for the Beginning Dental Practitioner in
Canada. J Dent Educ 70(10):1076, October 2006.
Gerrow JD Murphy HJ Boyd MA. Review and Revision of the Competencies for a Beginning Dental
Practitioner in Canada. J Can Dent Assoc 73(2):157, 2007.