tct 2002 scientific sessiontaxus nirx comparative clinical - version 3.02 re 20020916 taxus ii...
TRANSCRIPT

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
TAXUS II International StudyComparative 6 month clinical
QCA & IVUS results
TAXUS NIRx stent system
Slow and Moderate release Paclitaxel formulation Dr Adrian Banning
John Radcliffe Hospital, Oxford
On behalf of the TAXUS II Investigators

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
Paclitaxel (1g/mm2 total loaded) Potent microtubular inhibitor Multifunctional
Slow (SR) and Moderate (MR) release formulationsTransluteTM polymer regulates controlled biphasic release & allows variable elution profile (cf Cypher)
NIRxTM Conformer Stent System Pre-mounted
15mm Conformer stent with 20mm balloon Advance Delivery SystemDiameters 3.0 & 3.5 mm
Paclitaxel (1g/mm2 total loaded) Potent microtubular inhibitor Multifunctional
Slow (SR) and Moderate (MR) release formulationsTransluteTM polymer regulates controlled biphasic release & allows variable elution profile (cf Cypher)
NIRxTM Conformer Stent System Pre-mounted
15mm Conformer stent with 20mm balloon Advance Delivery SystemDiameters 3.0 & 3.5 mm
TAXUS NIRxTMTAXUS NIRxTM
TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
ObjectiveObjective
TAXUS IIEvaluate safety and performance of the two consecutive cohorts for the treatment of
de novo coronary lesions:
Cohort I: Comparing TAXUS slow release randomised 1:1 against bare stent control
Cohort II: Comparing TAXUS moderate release randomised 1:1 against bare stent control
TAXUS IIEvaluate safety and performance of the two consecutive cohorts for the treatment of
de novo coronary lesions:
Cohort I: Comparing TAXUS slow release randomised 1:1 against bare stent control
Cohort II: Comparing TAXUS moderate release randomised 1:1 against bare stent control

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
Study OverviewStudy Overview
• Randomised (1:1)• Triple-blind• International, multi-centre • 536 patients
– TAXUSNIRx SR - 267 – TAXUSNIRx MR - 269
• 30d, 6 mo, 1- 5 year FU• Endpoints:
– Clinical– QCA– IVUS
• Randomised (1:1)• Triple-blind• International, multi-centre • 536 patients
– TAXUSNIRx SR - 267 – TAXUSNIRx MR - 269
• 30d, 6 mo, 1- 5 year FU• Endpoints:
– Clinical– QCA– IVUS
Inclusion Criteria• Standard risk de novo
lesions • Length < 12 mm• RVD > 3.0 & < 3.5mm
Anti-platelet regimen– ASA > 75mg
• Maintained indefinitely
– Clopidogrel• Loading dose 300 mg• 75 mg q.d. for 6 months
Inclusion Criteria• Standard risk de novo
lesions • Length < 12 mm• RVD > 3.0 & < 3.5mm
Anti-platelet regimen– ASA > 75mg
• Maintained indefinitely
– Clopidogrel• Loading dose 300 mg• 75 mg q.d. for 6 months

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
In vitro Release Kinetics Biphasic: 48h burst then slower 10 day low level phase
In vitro Release Kinetics Biphasic: 48h burst then slower 10 day low level phase
• Same total loaded dose - different release rates• Biphasic release - early burst and sustained release phases• 8 fold difference in release rate between SR and MR
• Same total loaded dose - different release rates• Biphasic release - early burst and sustained release phases• 8 fold difference in release rate between SR and MR
0%
5%
10%
15%
0 2 4 6 8 10 12
Time (days)
% P
Tx
rel
ease
d
N = 3
N = 9
Early
Burst
Phase
Sustained Low Level Release Phase
8-10 fold difference
%
Pa
cli
tax
el
Re
lea
se
d
0 2 4 6 8 10 12Days
% P
aclit
axel
rel
ease
d
0%
5%
10
15
Slow Release1g/mm2
Moderate Release1g/mm2

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
TAXUS II Global InvestigatorsTAXUS II Global Investigators
Banning, Adrian
Belardi, Jorge
Benit, Edouard
Bilodeau, Luc
Bonnier, Edouard
Camenzind, Edoardo
Chan, Charles
Colombo, Antonio
Dawkins, Keith
Drzewiecki, Janusz
Dudek, Dariusz
Figulla, Hans
Fort, Stephen
Grube, Eberhard
Guagliumi, Giulio
Hamburger, Jaap
Hauptmann, Karl
Kelbaek, Henning
LeBlanche, Jean-Michel
Banning, Adrian
Belardi, Jorge
Benit, Edouard
Bilodeau, Luc
Bonnier, Edouard
Camenzind, Edoardo
Chan, Charles
Colombo, Antonio
Dawkins, Keith
Drzewiecki, Janusz
Dudek, Dariusz
Figulla, Hans
Fort, Stephen
Grube, Eberhard
Guagliumi, Giulio
Hamburger, Jaap
Hauptmann, Karl
Kelbaek, Henning
LeBlanche, Jean-Michel
Meredith, Ian
Muenzel, Thomas
Neinaber, Christoph
Nordrehaug, Jan
Pfisterer, Matthias
Ormiston, John
Reeves, Francois
Roy, Louis
Rutsch, Wolfgang
Ruzyllo, Witold
Schiele, Francois
Silber, Sigmund
Siminiak, Tomasz
Strauss, Bradley
Urbaszek, Wilhelm
Webb, John
Whitbourn, Robert
Zmudka, Krzysztof
Meredith, Ian
Muenzel, Thomas
Neinaber, Christoph
Nordrehaug, Jan
Pfisterer, Matthias
Ormiston, John
Reeves, Francois
Roy, Louis
Rutsch, Wolfgang
Ruzyllo, Witold
Schiele, Francois
Silber, Sigmund
Siminiak, Tomasz
Strauss, Bradley
Urbaszek, Wilhelm
Webb, John
Whitbourn, Robert
Zmudka, Krzysztof
Real world experience (15 countries, 38 sites) Randomized, triple blinded study with 536 pts >95% Angiographic and >87% IVUS FU
Real world experience (15 countries, 38 sites) Randomized, triple blinded study with 536 pts >95% Angiographic and >87% IVUS FU

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
Study ManagementStudy Management
Angiographic & IVUS: Cardialysis
Core Analysis: Rotterdam, The Netherlands
CEC: 7 independent members
DMC: 4 independent members
Study Coordination: PPD Development
Paris, France
Central Lab: COVANCE Bioanalytical Services
Indianapolis, Indiana
Industry Sponsor: Boston Scientific Corporation
Angiographic & IVUS: Cardialysis
Core Analysis: Rotterdam, The Netherlands
CEC: 7 independent members
DMC: 4 independent members
Study Coordination: PPD Development
Paris, France
Central Lab: COVANCE Bioanalytical Services
Indianapolis, Indiana
Industry Sponsor: Boston Scientific Corporation

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
DemographicsNo Significant Differences Between Groups
DemographicsNo Significant Differences Between Groups
61.0
15.0
27.0
36.0
42.0
15.0
59.8 + 9.7
78.0
Combined Control (%)
(n=270)
63.0
11.0
21.0
35.0
35.0
11.0
61.5 + 10.5
70.0
TAXUSNIRx SR
(%)
(n=131)
60.0Hypertension17.0Diabetes24.0Smoker30.0Unstable Angina39.0Prior MI17.0Prior Intervention59.3 + 10.1Age76.0Male
TAXUSNIRx MR
(%)
(n=135)

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
TAXUS IIBaseline Lesion Characteristics
TAXUS IIBaseline Lesion Characteristics
Combined Control
(n=270)
TAXUSNIRx SR
(n=131)
TAXUSNIRx MR
(n=135 )
P-value
SR vs. Combined
Control
P-value MR vs.
Combined Control
P-value SR vs.
MR
RVD (mm) 2.75 + 0.5 2.78 + 0.4 2.72 + 0.5 0.5996 0.4442 0.2656
MLD (mm) 1.0 + 0.4 1.0 + 0.3 0.9 + 0.3 0.2385 0.4895 0.1063
Diameter Stenosis (%) 64.7 + 11.1 63.3 + 9.6 64.9 + 10.3 0.2108 0.8434 0.2088
Lesion Length mm) 10.6 + 4.1 10.5 + 3.9 10.2 + 4.8 0.8968 0.3125 0.4498
Well matched RVD at 2.75mm and Lesion Length at 10.5mmWell matched RVD at 2.75mm and Lesion Length at 10.5mm

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
Stent DistributionPredominantly Single Stents Implanted
Stent DistributionPredominantly Single Stents Implanted
0.5298
0.5298
0.6480
P-value
SR vs. Control
4 (6)
94 (127)
1 (2)
15.7+3.1
50% (70)
50% (69)
96%
TAXUSNIRx MR (n=135)
1.0000
1.0000
0.3557
P-value MR vs. Control
0.628454% (72)50% (140) 3.5
0.628446% (62)50% (138) 3.0
Study Stent Distribution
0.766795%94%Clinical Procedural Success
5 (6) 4% (12) 2
93 (122)94% (254) 1
2 (3) 1% (4) None
Study Stents (per pt)
15.7+3.2Study Stent Length, mm (per pt)
TAXUSNIR SR (n=131)
P-value SR vs.
MR
Combined Control(n=270)

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
Early Clinical EventsNo differences in SR, MR or Controls
Early Clinical EventsNo differences in SR, MR or Controls
One peri-procedural stent thrombosis of 266 TAXUS stents placedOne peri-procedural stent thrombosis of 266 TAXUS stents placed
0.0%0.8%0.0% < 1 day
0.0%0.0%0.0% 30 days - 180 days
2.0 %(3) 2.0% (3)4.0% (12)30-day MACE
2.0% (3)Periprocedural MACE
Stent Thrombosis
TAXUSNIRx SR(n=131)
Combined Control (n=270)
TAXUSNIRx MR(n=135)
4.0% 2.0% (3)
1 day - 30 days 0.0%0.0%
MI (n)
Death (n) (1)
(11) (2) (3)
(0) (0)
0.0%

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
1.0000
0.7572
0.0080
0.0262
0.1567
1.0000
1.0000
0.0035
P-value
SR vs. Combined
Control
1.0 (1)
2.3 (3)
3.1 (4)
6.2 (8)
2.3 (3)
0.0
0.0
7.8 (10)
TAXUSNIRx MR
(n=135)Rate %/ (n)
1.0000
1.0000
0.0010
0.0059
0.4029
1.0000
1.0000
0.0019
P-value MR vs.
Combined Control
1.00003.1 (4)2.7 (7) TVR Remote
1.00000.8 (1)0.8 (2) CABG
0.74904.6 (6)13.3 (35) TLR
1.00008.5 (11)19.8 (52)6-Month MACE
0.8078
0.6838
P-value SR vs.
MR
7.7 (10)
1.5 (2)
0.0
0.0
TAXUSNIRx SR
(n=131)Rate % / (n)
16.0 (42) TVR - Overall
4.6 (12) Non Q-Wave MI
0.8 (2) Q-Wave MI
0.4 (1) Death
Combined Control(n=270)
Rate % / (n)
TAXUS II 6 mo. Major Adverse Cardiac Events
TAXUS II 6 mo. Major Adverse Cardiac Events
N/A
N/A
Improvements in SR and MRImprovements in SR and MR

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
Six month Binary Restenosis Decreased in stented segment not in edges
Six month Binary Restenosis Decreased in stented segment not in edges
3.41.6 2.3
19.0
2.3
4.73.1
1.6 2.30.0
5.0
10.0
15.0
20.0
25.0
Re
ste
no
sis
%
Combined Control TAXUS SR TAXUS MR
Stented SegmentProximal Edge Distal Edge5mm 5mm
P<0.0001P<0.0001
n=128n=263 n=128n=127n=261 n=128 n=127n=262 n=128
P<0.0001P<0.0001
P=0.500P=0.500
P=1.000P=1.000P=1.000P=1.000
P=0.509P=0.509P =0.515P =0.515
P=0.758P=0.758 P=1.000P=1.000

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
2.3% (3/128)1.6% (2/127) 3.1% (8/262)Distal Edge
2.3% (3/128)1.6% (2/127) 3.4 % (9/261)Proximal Edge
22.0% (58/264)
18.6% (49/263)
19.0% (50/263)
Combined Control
(n=270)
8.6% (11/128)
0.8% ( 1/128)
4.7% (6/128)
TAXUSNIRx MR
(n=135 )
5.5% (7/128)Total Analysis Segment
1.5% (2/128)
If confounders excluded
2.3% ( 3/128)Stented Segment
TAXUSNIRx SR
(n=131)
6 mo. Restenosis Rates Improvements for TAXUS SR and MR
6 mo. Restenosis Rates Improvements for TAXUS SR and MR
Stented Segment: All stents (study and non-study) used to treat target lesion
Total Analysis Segment: Stented segment + 5 mm proximal and distal edge
Stented Segment: All stents (study and non-study) used to treat target lesion
Total Analysis Segment: Stented segment + 5 mm proximal and distal edge
TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
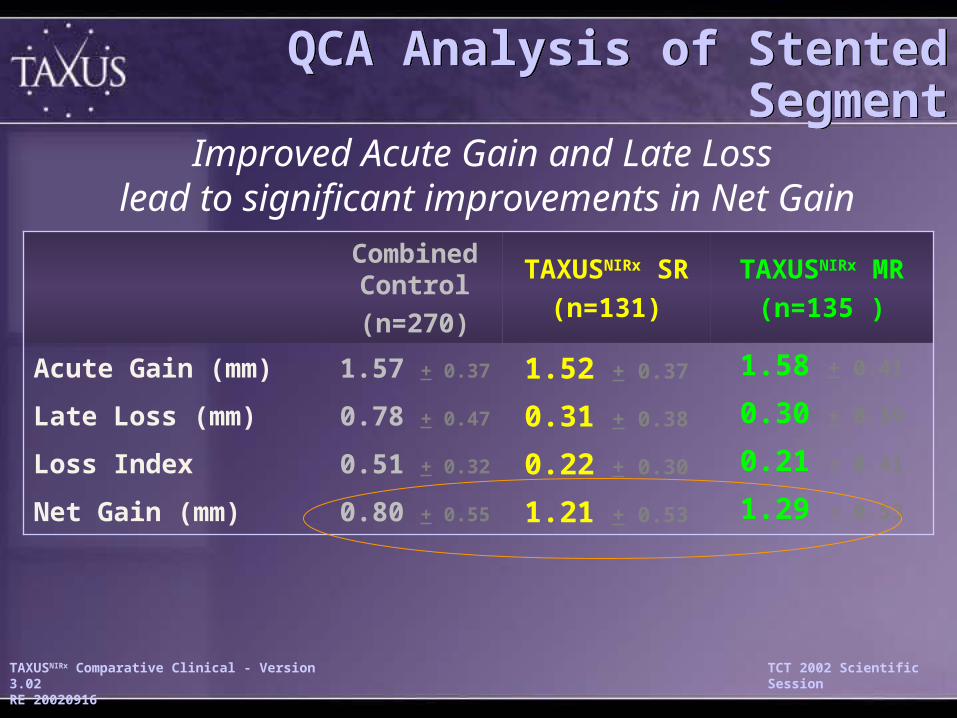
QCA Analysis of Stented SegmentQCA Analysis of Stented Segment
0.80 + 0.55
0.51 + 0.32
0.78 + 0.47
1.57 + 0.37
Combined Control
(n=270)
1.29 + 0.53
0.21 + 0.41
0.30 + 0.39
1.58 + 0.41
TAXUSNIRx MR
(n=135 )
1.21 + 0.53Net Gain (mm)
0.22 + 0.30Loss Index
0.31 + 0.38Late Loss (mm)
1.52 + 0.37Acute Gain (mm)
TAXUSNIRx SR
(n=131)
Improved Acute Gain and Late Loss lead to significant improvements in Net Gain

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
Comparative TAXUS II Clinical SummaryComparative TAXUS II Clinical Summary
• Matched demographics in combined control, SR & MR
• Excellent control outcomes
• At 6 mo, SR & MR superior compared with combined
control
– MACE reduced by >60%
– TVR reduced by >60% due to TLR being reduced by >60%
– Beneficial edge effects on 6 mo. MLD and late loss
• Only 1/266 late TLR in regions treated by TAXUSNIRx
• SR and MR excellent with comparable late MACE rates
• Matched demographics in combined control, SR & MR
• Excellent control outcomes
• At 6 mo, SR & MR superior compared with combined
control
– MACE reduced by >60%
– TVR reduced by >60% due to TLR being reduced by >60%
– Beneficial edge effects on 6 mo. MLD and late loss
• Only 1/266 late TLR in regions treated by TAXUSNIRx
• SR and MR excellent with comparable late MACE rates

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
21.85
7.85 7.84
0
10
20
30
40
50
CombinedControl
TAXUS SR
TAXUS MR
n=270 n=131 n=135
+ 17.5
+9.9 + 9.7
IVUS Primary Endpoint Met Reduced 6 mo. % In-Stent Net Volume Obstruction
IVUS Primary Endpoint Met Reduced 6 mo. % In-Stent Net Volume Obstruction
P=0.997
P<0.0001
No difference in SR vs. MRNo difference in SR vs. MR
Superior SR & MR vs. ControlSuperior SR & MR vs. Control
P<0.0001

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
Stent Volume (mm3)Stent Volume (mm3)
130.68 128.8 132.45
0
100
200
Combined Control TAXUS SR TAXUS MR
+41.17
Stent Volume (mm3) at 6 mo. FUNo change in Stent Volume for all groupsStent Volume (mm3) at 6 mo. FUNo change in Stent Volume for all groups
+42.44 +48.81
n=244 n=118 n=118
P=0.670
P=0.718
P=0.520

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
Vessel Volume (mm3)Vessel Volume (mm3)
258.6 266.79 273.63
0
100
200
300
400
Combined Control TAXUS SR TAXUS MR
+76.48
Vessel Volume (mm3) at 6 mo. FUNo change in Vessel Volume for all groups Vessel Volume (mm3) at 6 mo. FU
No change in Vessel Volume for all groups
+89.66 +97.55
n=214 n=110 n=104
P=0.414
P=0.142
P=0.558

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
29.1
10.25 11.2
0.0
10.0
20.0
30.0
40.0
50.0
Combined Control TAXUS SR TAXUS MR
+28.23
+13.26
Neointimal Hyperplasia (mm3) at 6 monthsReduced for TAXUS SR & MR vs control
Neointimal Hyperplasia (mm3) at 6 monthsReduced for TAXUS SR & MR vs control
+17.29
n=244 n=118 n=118
P<0.0001
P=0.742
P<0.0001

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
Summary of key IVUS findingsSummary of key IVUS findings
Blinded, randomized study of 536 patients provides largest IVUS data set in
DES field with paired FU
Comprehensive IVUS (pre, post & 6 mo. FU) data set for TAXUS & large
control group shows:
1) Stent volumes stable for TAXUS (SR & MR) & Controls
2) Vessel volumes stable for TAXUS (SR & MR) & Controls
3) Improved TAXUS SR & MR volumetric indices
neointimal hyperplasia reduced
% net volume obstruction reduced
No differences between SR & MR
4) IVUS improvements concordant with QCA gains
Blinded, randomized study of 536 patients provides largest IVUS data set in
DES field with paired FU
Comprehensive IVUS (pre, post & 6 mo. FU) data set for TAXUS & large
control group shows:
1) Stent volumes stable for TAXUS (SR & MR) & Controls
2) Vessel volumes stable for TAXUS (SR & MR) & Controls
3) Improved TAXUS SR & MR volumetric indices
neointimal hyperplasia reduced
% net volume obstruction reduced
No differences between SR & MR
4) IVUS improvements concordant with QCA gains

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
Cumulative Frequency Distribution of Percent Diameter Stenosis by QCA
Cumulative Frequency Distribution of Percent Diameter Stenosis by QCA
Per
cen
tile
0
20
40
60
80
100
% Diameter Stenosis
-10 0 10 20 30 40 50 60 70 80 90 100
Pre procedureNo differences
PostprocedureNo differences Control
Improved % DS SR & MR at 6-mo
SR MR
TAXUS SR
TAXUS MR
Control
TAXUS SR
TAXUS MR
Control

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
0
10
20
30
40
-1.0
-0.8
-0.6
-0.4
-0.2 0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
1.8
2.0
2.2
2.4
2.6P
erc
en
tag
e o
f P
ati
en
ts
Taxus SR Taxus MR Control
6 mo. Late Loss within Stented SegmentImproved in TAXUS SR and MR vs. Combined Control
6 mo. Late Loss within Stented SegmentImproved in TAXUS SR and MR vs. Combined Control
TAXUS SR & MR– Left shift towards reduced late loss for TAXUS SR & MR
– Tighter frequency distribution for TAXUS vs. Control
TAXUS SR & MR– Left shift towards reduced late loss for TAXUS SR & MR
– Tighter frequency distribution for TAXUS vs. Control
TAXUS lower frequency of high late loss
NegativeLate lossSimilar toControl
TAXUS SR0.30 + 0.36
TAXUS MR0.26 + 0.34
Control0.78 + 0.47

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
Stent segmentStent segment
Incompete AppositionIncompete Apposition

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
Fates of Incomplete Apposition
Baseline
Incomplete Apposition
Baseline
Incomplete Apposition
Preserved
Incomplete Apposition
Preserved
Incomplete Apposition
Healed/Resolved
Incomplete Apposition
Healed/Resolved
Incomplete Apposition

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
Follow-up IA (+ remodeling)
BaselineBaseline
Follow-up IA(remodeling)Follow-up IA(remodeling)
Follow-up IA(no remodeling)Follow-up IA
(no remodeling)
TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
Incomplete Apposition in TAXUS IISummary
Incomplete Apposition in TAXUS IISummary
Late acquired mal-apposition • Incidence of 5.3% in control (bare stent)• Incidence in TAXUS (SR 8.5% & MR 9.6%)
not significantly different from control • No correlation with MACE incidence
Late acquired mal-apposition • Incidence of 5.3% in control (bare stent)• Incidence in TAXUS (SR 8.5% & MR 9.6%)
not significantly different from control • No correlation with MACE incidence

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
TAXUS Angiographic Aneurysm Incidence Summary
TAXUS Angiographic Aneurysm Incidence Summary
SR Cohortn=4
SR Cohortn=4
MR Cohortn=4
MR Cohortn=4
TAXUSTAXUS ControlControl3
1283
1281
1341
134
TAXUSTAXUS ControlControl1
1281
1283
1303
130
Incidence (%)Incidence (%) 2.32.3 0.70.7 0.80.8 2.32.3
Diabetics (%) Diabetics (%) 0.00.0 0.00.0 0.00.0 0.00.0
TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
Comparative IVUS & QCA TAXUS II For TAXUS SR & MR vs. Combined ControlComparative IVUS & QCA TAXUS II For TAXUS SR & MR vs. Combined Control
IVUS• >60% improvement IVUS volumetric indices • Stable vessel & stent volumes comparable to control
QCA Binary Restenosis Rates reduced• Improvements of at least 60% for all RVDs• Optimal placement may reduce confounding restenosis (gap & bare
stents)
QCA parameters by 40%-60% for MLD & Late Loss• Beneficial edge effect by MLD & LL• Beneficial improvements for Diabetics
No significant differences in excellent outcomes between TAXUS SR & TAXUS MR
IVUS• >60% improvement IVUS volumetric indices • Stable vessel & stent volumes comparable to control
QCA Binary Restenosis Rates reduced• Improvements of at least 60% for all RVDs• Optimal placement may reduce confounding restenosis (gap & bare
stents)
QCA parameters by 40%-60% for MLD & Late Loss• Beneficial edge effect by MLD & LL• Beneficial improvements for Diabetics
No significant differences in excellent outcomes between TAXUS SR & TAXUS MR

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
Key practice messagesKey practice messages
• Drug eluting stents will reduce (but not abolish) restenosis within the stent but…
• Must optimise stent deployment• Must cover all the atheroma (mind the edges)• Do not leave gaps between stents (overlap not a problem) • Don’t mix your stents
(Drugs & bare metal might not mix)
• Drug eluting stents will reduce (but not abolish) restenosis within the stent but…
• Must optimise stent deployment• Must cover all the atheroma (mind the edges)• Do not leave gaps between stents (overlap not a problem) • Don’t mix your stents
(Drugs & bare metal might not mix)

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
Key practice messagesKey practice messages
More IVUS / pressure wire assessment
More IIb/IIIa Inhibitor use
Longer stented segments
particularly in small vessels and diabetics
-Taxus 6
More IVUS / pressure wire assessment
More IIb/IIIa Inhibitor use
Longer stented segments
particularly in small vessels and diabetics
-Taxus 6

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
Taxus 6Taxus 6
• Lesions - >18 mm and <40mm length– Randomised 1:1 with bare stents– >2.5m and <3.75 diameter– De Novo Lesions– Express stent– Moderate release polymer
– 9 month QCA and IVUS follow up
• Lesions - >18 mm and <40mm length– Randomised 1:1 with bare stents– >2.5m and <3.75 diameter– De Novo Lesions– Express stent– Moderate release polymer
– 9 month QCA and IVUS follow up

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
Taxus 6Taxus 6
• 47 centres in Europe• Co-PI, Prof Grubbe and Dr K Dawkins• 448 pts enrolled Dec 28th 2002
– Banning/Channon 28 pts– Dawkins 19 pts– Thomas 7 pts– Adam DeBelder 5 pts
– United Kingdom 13% total study
• 47 centres in Europe• Co-PI, Prof Grubbe and Dr K Dawkins• 448 pts enrolled Dec 28th 2002
– Banning/Channon 28 pts– Dawkins 19 pts– Thomas 7 pts– Adam DeBelder 5 pts
– United Kingdom 13% total study

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session
AcknowledgementsAcknowledgements
• Co investigator - Prof Keith Channon
• Medical study team– C McKenna, G Niccoli, P Heck, F Khan, – D Nicholson
• Cath lab, cardiology ward and DCU– Nurses, techs, radiographers (N Searle)– K Lucas
• Colleagues referred pts – (OO, DS, JB, MH, DL, MP, RC-W)
• Co investigator - Prof Keith Channon
• Medical study team– C McKenna, G Niccoli, P Heck, F Khan, – D Nicholson
• Cath lab, cardiology ward and DCU– Nurses, techs, radiographers (N Searle)– K Lucas
• Colleagues referred pts – (OO, DS, JB, MH, DL, MP, RC-W)

TAXUSNIRx Comparative Clinical - Version 3.02RE 20020916
TCT 2002 Scientific Session