table of contents - university of michiganioe481/ioe481_past_reports/16f04.docx · web viewthe...
TRANSCRIPT

UM Emergency Department Deep-CleansImproving Communication, Coordination, and Tracking Deep-Cleans Between Departments
Final Report
To: Maurits Hughes, Director, UMHS Environmental ServicesMichael Alexander, Senior Business Analyst, UMHS Environmental ServicesSam Clark, Industrial Engineer, Program & Operations Analysis Colby Foster, Management Engineer Fellow, Program & Operations AnalysisMark P. Van Oyen, IOE 481 Professor, [email protected] Duck, Industrial Engineer Expert, [email protected]
From: IOE 481 Fall 2016 Team 4Jessica CernakMichael ShayEmily SnitchlerDavid Walborn
Date: November 29, 2016

TABLE OF CONTENTS
LIST OF FIGURES 3EXECUTIVE SUMMARY 4
Goals & Objectives 4Methodology 4Findings and Conclusions 4
Variation in Deep-Clean Understanding 5Variation in Cleaning and Reporting Practices 5Discontinuous Communication Flow 5Missed Opportunities for Deep-Cleaning 6Minimal Collaboration 6
Recommendations 6INTRODUCTION 7BACKGROUND 7PROJECT MOTIVATIONS 8GOALS & OBJECTIVES 8SCOPE 8METHODOLOGY 8
Observations and Interviews 8Literature Search 9Survey Data 9
Housekeeper Survey Data 9ED Nurse Survey Data 9
Hospital Occupancy Data 9TeleTracking Data 10
FINDINGS & CONCLUSIONS 10Variation in Deep-Clean Understanding 11Variation in Reporting and Cleaning Practices 11
Reporting Practices 11Cleaning Practices 13
Discontinuous Communication Flow 13Missed Opportunities for Deep-Cleaning 14Minimal Collaboration 15
RECOMMENDATIONS 16Retraining 16Identifying EVS Housekeeper Leadership 17Re-Examining Staffing Levels 17Improving Communication 18Tracking Deep-Cleans 19
EXPECTED IMPACT 20REFERENCES 21APPENDIX A: EVS-ED SERVICE-LEVEL AGREEMENT 22APPENDIX B: STANDARD INTERVIEW QUESTIONS 36APPENDIX C: HOUSEKEEPER SURVEY QUESTIONS 37APPENDIX D: NURSE SURVEY QUESTIONS 38
1

APPENDIX E: ED OCCUPANCY DATA ANALYSIS FROM INDUSTRIAL ENGINEER, PROGRAM & OPERATIONS ANALYSIS 39APPENDIX F: PAPER TRACKING EXAMPLE 42
2

LIST OF FIGURES
Figure 1: EVS Housekeepers are using TeleTracking Most of the Time 12Figure 2: Variance Reveals Discrepancies Between Housekeepers’ Standard Procedure 13Figure 3: Largest Gap in Communication between EVS and ED 14Figure 4: Average occupancy is generally lowest from the hours of 5-8AM 15
3

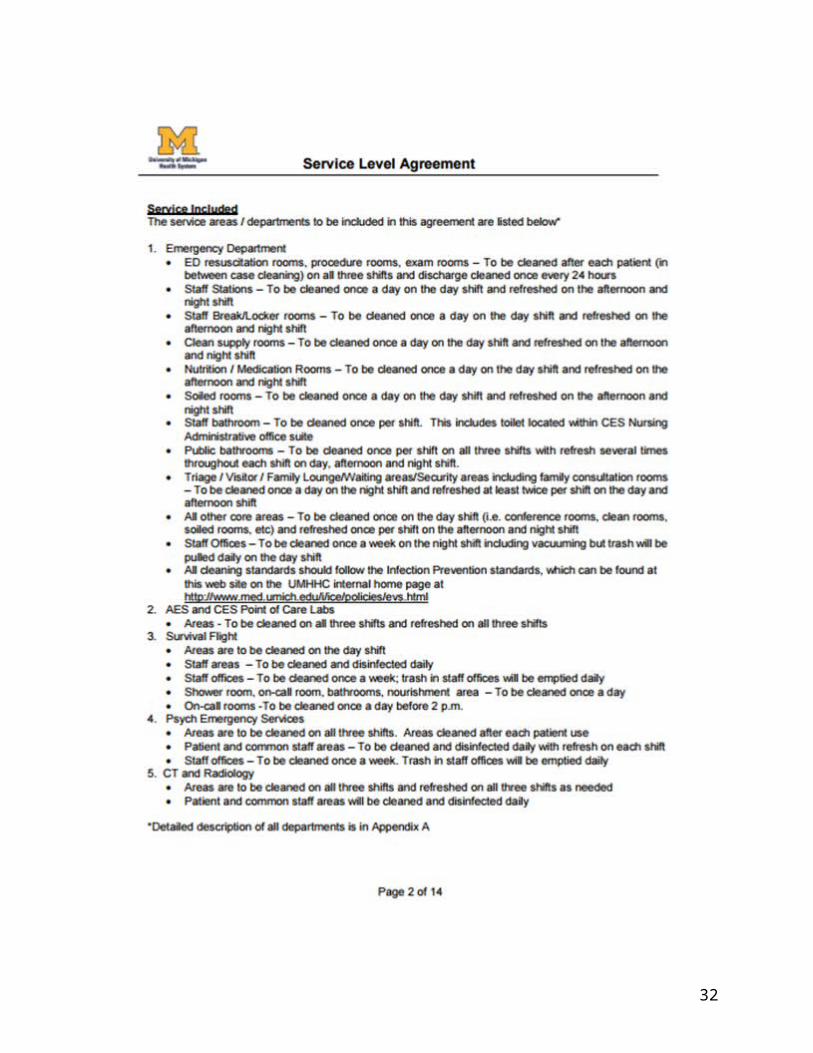
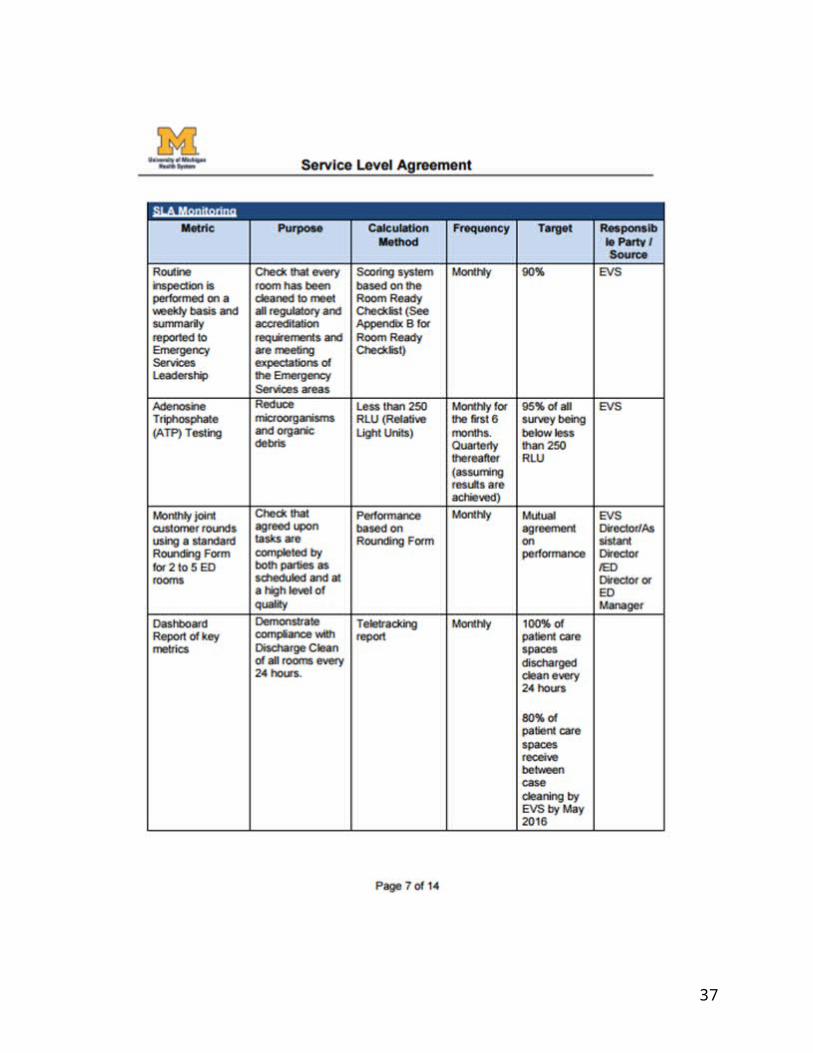
EXECUTIVE SUMMARY The UM Hospital’s Environmental Services (EVS) department is in charge of the cleaning procedures throughout the University of Michigan Health System (UMHS). The Infection Control and Epidemiology (ICE) department at the University of Michigan Hospital System is leading an initiative to reduce the instances of hospital acquired infection. As a part of ICE’s mission, EVS has been charged with deep-cleaning 100% of Emergency Department (ED) rooms every 24 hours. This deep-cleaning goal has been outlined in the Service-Level Agreement between departments. However, there is no communication tool or tracking method currently in place between the ED and EVS to ensure that every room is cleaned once every 24 hours. EVS and the ED asked an IOE 481 team to address the communication and tracking issues preventing every room from being deep-cleaned in 24 hours. After identifying the problem areas, the team has recommended changes for EVS and the ED to help them reach their goal of 100% of ED rooms deep-cleaned every 24 hours.
Goals & Objectives
The primary goal of this project was to help EVS reach its goal of deep-cleaning 100% of ED rooms every 24 hours. In order to accomplish the primary goal, the team has provided the following recommendations: a method to enhance communication between EVS and ED and a method to track deep-cleans.
Methodology
The team utilized five different methods to identify the main issues in the EVS and ED and develop recommendations to facilitate the primary goal.
● Observed and interviewed ED and EVS staff. The team interviewed nurses, nurse techs, Act Team Leaders (ATLs), and housekeepers to understand the current situation and gather ideas regarding current issues and potential solutions.
● Performed literature search. The team examined literature on efficient patient placement, current cleaning methods, and decentralized housekeeping models to aid their recommendations.
● Collected survey data. The team surveyed EVS housekeepers as well as nurses from the ED to grasp the concerns of a larger percentage of the population. The surveys collected qualitative as well as quantitative data.
● Analyzed ED occupancy data. The team obtained data regarding patient stay information from an Industrial Engineer in Program and Operations Analysis. The data was analyzed to interpret specific time intervals in which rooms are available to clean.
● Analyzed TeleTracking data. The team obtained room cleaning times from TeleTracking data. The data was analyzed to reveal information about regular room cleaning procedures.
4
Findings and Conclusions
The team has drawn the following key conclusions:
● Understanding surrounding the definition of deep-clean varies.● Reporting and cleaning practices vary. ● Communication flow between EVS and the ED is discontinuous.● Opportunities to deep-clean rooms are overlooked.● Cross-departmental collaboration is lacking.
Variation in Deep-Clean UnderstandingUnderstanding of the definition of deep-clean differs widely from person to person. The team has observed different uses of the term deep-clean across formal housekeeping training, the ED-EVS Service-Level agreement, and within EVS management.
Variation in Cleaning and Reporting PracticesThe team’s observations have revealed that the procedure of logging in and out of TeleTracking to track room clean time is often neglected. Other times, the procedure of logging in and out of the system is performed in direct sequence to mark the room clean, depicting an inaccurate data set of actual room clean time. The team’s analysis of TeleTracking data supports the inferences drawn from the team’s initial observations that TeleTracking use is inconsistent. The average clean time in TeleTracking data is 16.5 minutes with a standard deviation of 9.1 minutes. The team has determined that the variation of turn time across employees is a result of lack of standardized procedure when using the TeleTracking system.
“Standardizing the Monitoring Process of Inpatient Room Cleaning to Reduce the Spread of Hospital Acquired Infections,” an IOE 481 project performed in Spring 2010, focused primarily on the cleaning process. The report recommended further investigation into standardization: “further investigate the variation in cleaning practices so as to determine what custodial cleaning procedures should be standardized and what should be left to personal preference,” [2]. This aligns with the team’s observations of non-standard cleaning procedures. The team’s findings confirm that the reporting process requires clarification and cleaning practices require standardization.
Discontinuous Communication FlowThrough thorough observation of the existing cleaning processes the team constructed a communication map between EVS and the ED. The flow indicates that no housekeepers directly tell nurses that a room is clean. The results of nurse surveys built upon the need for enhanced communication with 15 out of 38 commenting respondents recommending improved communication. The Fall 2014 IOE 481 project titled “Efficient Patient Placement in the Emergency Department” contained information relating to communication gaps between EVS and the ED. The recommendations cite communication between the ED and EVS as a main disruptor of process flow. This supports the conclusion that communication is a major factor preventing the deep-cleaning of 100% of ED rooms every 24 hours.
5

Missed Opportunities for Deep-CleaningThe percentage of occupancy in the ED reflects windows of opportunity in which both the ED and EVS are likely to be able to achieve their respective goals. The ED seeks to have as many rooms available as possible to reduce patient wait time, allowing for fast treatment of patients. The goal of EVS is to achieve a deep-clean of each room every 24 hours. When occupancy is lowest from the hours of 5-8AM, both goals are most readily achievable. EVS housekeepers have the most rooms available which they can deep-clean and the ED is able to accommodate incoming patients with low wait times. During the hours of 3-8PM occupancy is highest, presenting challenges to each of these goals.
Minimal CollaborationHousekeeper surveys articulated a need for increased collaboration amongst EVS staff and between EVS and ED staff. 55% of housekeepers who left comments indicated a desire for greater teamwork and clarified expectations. 21% of commenting respondents on nurse surveys supported increased teamwork as well.
Recommendations
The team recommends, first and foremost, that UMHS ED and EVS perform the following tasks:● Retrain staff.● Identify one EVS housekeeper from each shift as a shift leader.● Re-examine staffing levels.● Improve communication between ED staff and EVS staff.● Track when deep-cleans are being performed.
Retraining staff and identifying EVS leadership among the housekeepers will promote communication and teamwork between the ED and EVS, which is essential for reaching the primary goal of having EVS housekeepers deep-clean 100% of ED rooms every 24 hours.
The team recommends re-analyzing staffing levels and the current housekeeper staffing model because the patient stay data indicated that the lowest occupancy times occur during the night shift. Re-examining the current staffing levels could potentially show more windows for opportunity for deep-cleaning and therefore, bring EVS closer toward its primary goal.
The team has also prepared several solutions to bridge the communication gap between the ED and EVS and help EVS track deep-cleans. The solutions include the following: the current paging system, walkie talkies, iPods, and paper tracking.
The current paging system, walkie talkies, and iPods can be used to bridge the communication gap between the EVS and ED. The iPods and paper tracking can be used to track deep-cleans. The idea is that a combination of any of these solutions, along with retraining staff, identifying EVS leadership, and re-examining staffing levels, could be used to help EVS ultimately reach their primary goal of 100% of ED rooms deep-cleaned every 24 hours.
6

INTRODUCTION
The UM Hospital’s Environmental Services (EVS) department is in charge of cleaning procedures throughout the University of Michigan Health System(UMHS), which include the chemicals, cleaning guidelines, schedules, and the housekeeping staff. The Infection Control and Epidemiology (ICE) department at the University of Michigan Hospital System is leading an initiative to reduce the instances of hospital-acquired infections such as Methicillin-Resistant Staphylococcus Aureus (MRSA) and Vancomycin-Resistant Enterococcus (VRE). As a part of ICE’s mission, EVS has been charged with deep-cleaning 100% of Emergency Department (ED) rooms every 24 hours. This goal will ensure that all rooms are sanitary and cleaned to EVS standards for UMHS patients. Currently there is unreliable communication and no tracking method in place between the ED and EVS to ensure that every room is deep-cleaned once every 24 hours. EVS and the ED asked an IOE 481 team to examine the existing cleaning procedures and provide solutions to communication between EVS and ED staff and deep-clean tracking. This final report articulates the methods used to develop recommendations for EVS.
BACKGROUND
The director of Environmental Services estimates that only 40-50% of all Emergency Department rooms receive a deep-clean every 24 hours. This presents a large window of improvement in order to reach the 100% goal promoted by ICE (outlined in the EVS-ED Service-Level agreement in Appendix A). Deep-cleans occur after contact patients, which include skin diseases, flu patients, and tuberculosis patients, as well as terminal patients, or during extended periods of room availability. Deep-cleans are estimated by an EVS area manager to take approximately 30 minutes to complete. Deep-cleaning includes removing trash and linen, high dusting, dust mopping, damp wiping, checking and restocking dispensers, cleaning bathrooms, wet mopping, and inspecting. Environmental Services housekeepers perform deep-cleans, regular case cleans, and regular cleaning of common areas. Each housekeeper is assigned to an Emergency Department Unit consisting of 18-24 beds. ED clerks and nurses page housekeepers when a room needs to be cleaned. ED Nurses and nurse techs may also perform regular cleans based on availability. Housekeepers are expected to complete each room clean within 30 minutes of receiving a page. According to an EVS manager, the ED should be staffed with at least 4 housekeepers at any given time. The ED staff tracks patients from admission to discharge via MiChart, an Electronic Medical Record. If a patient has been discharged from a room, it is marked dirty on MiChart. This prompts an ED staff member to either perform a regular case clean themselves, or page an EVS housekeeper to perform a clean. TeleTracking is a system which stores data regarding a room clean request time, time of clean, and corresponding room for each clean performed by EVS.
7

In some departments, MiChart communicates the need for a clean directly to TeleTracking, automatically relaying the information to housekeepers; however, this automated notification functionality is not being used in the ED. Instead, the ATL, nurse, or nurse tech requesting the room clean pages the housekeepers directly. The housekeepers log into TeleTracking via phone at the beginning of the room clean and log out upon completion. This creates a record in TeleTracking, recording which rooms have been cleaned, when they were cleaned, and how long the clean took. Unfortunately, this cleaning data in TeleTracking cannot be used for real-time tracking of deep-cleans because of an inadequate capacity for additional queries on the production server. UMHS will transition to the Epic Electronic Medical Record in March 2017, replacing MiChart and TeleTracking. Neither of these technologies can support real-time tracking of deep-cleans; EVS and the ED need a method for tracking deep-cleans and facilitating communication between EVS housekeepers and ED staff.
PROJECT MOTIVATIONS
The following issues drove the need for this project.
● ICE’s initiative to deep-clean all ED rooms every 24 hours● The creation of the Service-Level agreement between EVS and the ED regarding
cleaning procedures and habits within the ED
GOALS & OBJECTIVES
The primary goal of this project was to help EVS reach its goal of deep-cleaning 100% of ED rooms every 24 hours. In order to accomplish the primary goal, the team has provided the following recommendations: a method to enhance communication between EVS and ED and a method to track deep-cleans.
SCOPE
This project included deep-cleans occurring within the Emergency Department at the University of Michigan Hospital. Modifying the content of a deep-cleaning was not within the scope of this project. The process of regular cleans was not within the scope of this project. The project focused purely on the communication and tracking systems related to deep-cleans in the Emergency Department.
METHODOLOGY
To approach the project goals, the team identified the main barriers preventing the achievement of the goal to accomplish 100% of rooms deep-cleaned in 24 hours. The methodologies used include observations and interviews, literature search, surveys, and data analysis.
Observations and Interviews
The team completed 40 hours of observations and 15 interviews, meeting the goals set forth at the onset of this project. The purpose of the observations and interviews was to develop the
8
team’s understanding of the current communication flow between the ED and EVS staff and to obtain anecdotal evidence to help the team develop appropriate recommendations. Each team member observed staff from the ED and EVS, including nurses, nurse techs, clerks, ATLs, and housekeepers. The interviews were performed informally during the observation hours. The team asked a series of standardized questions as well any other questions that arose from the observations. The standardized interview questions can be found in Appendix B.
Literature Search
The team performed a literature search to gather information on the past state of EVS operations within the ED. The team examined two past IOE 481 projects and a scholarly article from Nursing Management to learn about similar cases at UMHS and other locations. The results from the literature search can be seen in Findings & Conclusions.
Survey Data
Surveys were developed following observations and interviews. The goal of the surveys was to reach a larger percentage of the population and to obtain quantifiable data. The team distributed separate surveys to the housekeepers and nurse staff in the ED. These surveys captured the experiences and opinions of frontline workers in the cleaning process.
Housekeeper Survey DataEVS housekeepers across the morning, afternoon, and night shifts were asked a series of questions relating to communication, tracking, and workload within the ED. Answers were collected from 17 housekeepers working in the Adult Emergency Department between November 11, 2016 and November 14, 2016. The survey questions can be found in Appendix C. ED Nurse Survey DataED nurses across all shifts were asked a set of questions relating to communication and tracking of cleans within the ED. Answers were collected from 47 nurses and nurse techs working in the Adult Emergency Department between November 30, 2016 and December 1, 2016. The survey questions can be found in Appendix D.
Hospital Occupancy Data
The team acquired hospital occupancy data from an Industrial Engineer in Program & Operations Analysis. It contained information about length of stays in the ED. The information included patient arrival date and time to the hospital, arrival time to their first ED room, and ED discharge time. The data also included the patient’s initial ED room and the patient’s reassigned ED room if they were transferred at any point. The data spans 7/1/16 - 9/30/16 and includes information for approximately 20,000 patient visits. In the team’s analysis, patients who were not assigned a room in the ED were excluded. The team only used following fields in their analysis: the time of the first ED room assignment and the ED discharge time. The information regarding patient arrival time and wait time for room assignment is irrelevant to this project. Only the time spent occupying an ED room is necessary, due to its impact on EVS’s ability to clean a room.
9

The data was stratified across each of the three months included (July, August and September of 2016). The team created a matrix in Excel to represent patients occupying (and vacating) rooms in the ED each month. A patient was signified by an increment of 1 during the hours of their stay. The matrix was increased by one during the hour of arrival of a patient to an ED room. The matrix was decremented during the hour a patient was discharged from the ED. The model included three assumptions:
1. Each month began with 0 occupants. After 24 hours of operation, the total occupancy would accurately reflect the number of patients currently in an ED bed. This allows each month to be considered independently.
2. The occupancy information collected represents the status of ED rooms at the end of each hour. The matrix is summed across each arrival and departure column representing 1 hour to give a final value at the end of the hour period.
3. The occupancy percentage averaged across each specific hour interval during the month reflects an accurate trend of patient occupancy in the ED.
By analyzing the patient stay data, the team identified trends in occupancy in the ED. These trends were used to identify the opportune times to deep-clean ED rooms and develop recommendations to help reach the deep-cleaning goal. The team supported the hospital occupancy data analysis described above with further analysis from an Industrial Engineer in Program & Operations Analysis, as shown in Appendix E. The analysis in Appendix E goes beyond the scope of the analysis performed by the team.
TeleTracking Data
The team acquired TeleTracking room clean time data from the Senior Business Analyst in Environmental Services. The sample size of the data was 7,631 room cleans, which took place over 5.5 months (6/1/16-11/17/16). The TeleTracking data contains the following information fields: bed location, room turn time, and employee completing the clean. The team analyzed the average turn time at the individual employee level and summarized the findings in de-identified terms. This analysis was used to evaluate the effectiveness of the TeleTracking system and examine variance in clean performance and clean recording practices.
FINDINGS & CONCLUSIONS
The team has drawn the following key conclusions:
● Understanding surrounding the definition of deep-clean varies.● Reporting and cleaning practices vary. ● Communication flow between EVS and the ED is discontinuous.● Opportunities to deep-clean rooms are overlooked.● Cross-departmental collaboration is lacking.
Combatting these issues will allow EVS and the ED to increase the proportion of ED rooms deep-cleaned every 24 hours.
10

Variation in Deep-Clean Understanding
Understanding of the definition of deep-clean differs widely from person to person. The team has observed different uses of the term deep-clean across formal housekeeping training, the ED-EVS Service-Level agreement, and within EVS management. The definition of deep-clean is expounded upon in the ED-EVS Service Level Agreement where a deep-clean has 8 primary steps. These steps include:
1. High dust all equipment and surfaces2. Damp wipe furnishing, stretcher, headwall, monitor, computer workstation and horizontal
surfaces with a facility approved germicidal disinfectant solution. Bleach to be used only for cleaning room occupied by patient in Contact Precautions Droplet (CPD)
3. Clean public bathroom and room sink using a facility approved disinfectant4. Empty, clean, and reline waste basket and soiled linen hampers and remove trash and
soiled linen to a soil location5. Restock supplies (i.e. toilet paper, paper towels, hand soap, alcohol foam, hand sanitizer,
sharps containers, pharmacy boxes, etc.)6. Dust mop floors7. Wet mop floors using disinfectant. Use wet floor signs at all times when mopping floors8. Inspect walls and ceilings (which includes ceiling air vents and light fixtures) for soiling
and clean with facility approved disinfectant
Variation in Reporting and Cleaning Practices
Reporting PracticesThe team’s observations have revealed that TeleTracking is not always properly utilized by housekeeping staff. Often, the procedure of logging in and out of TeleTracking to track room clean time is completely neglected. Other times, the procedure of logging in and out of the system is performed in direct sequence to mark the room clean, depicting an inaccurate data set of actual room clean time.
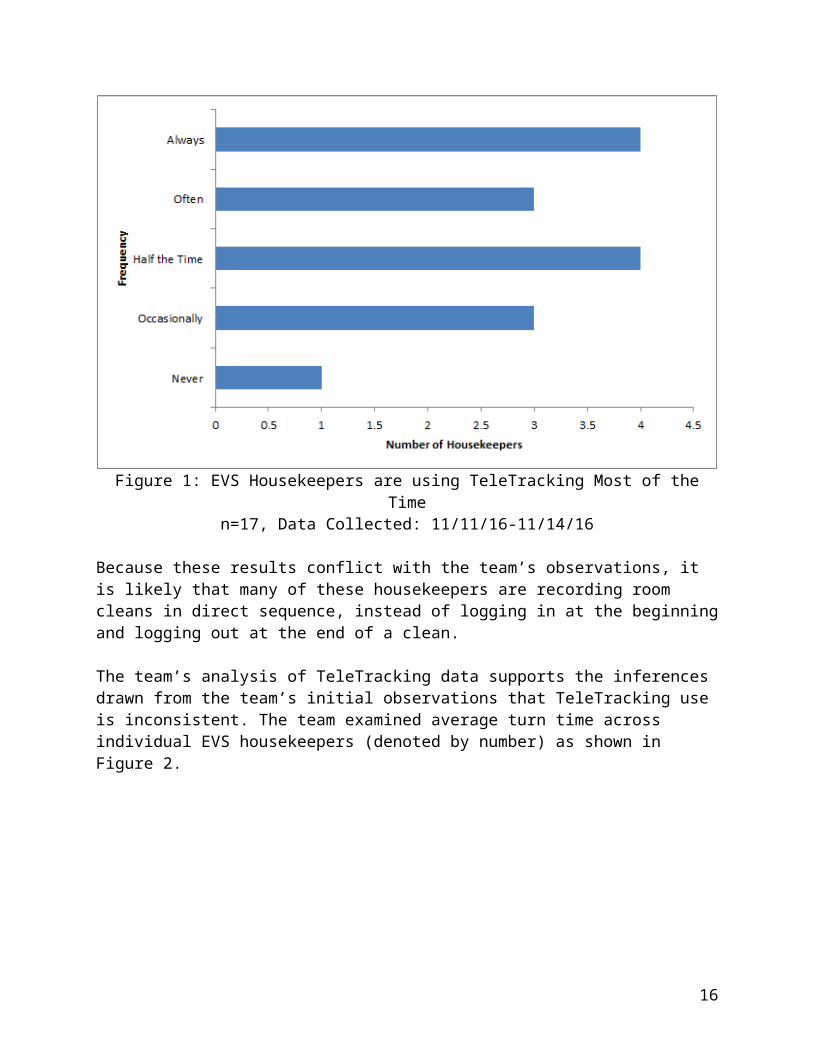
Survey responses were received from 17 EVS housekeepers, representing approximately half of the total populations of ED housekeepers. Of these 17 housekeepers, 5 worked the day shift, 4 worked the night shift, and 8 worked the evening shift. 13 out of 17 housekeepers use TeleTracking half the time or more, in contrast to the team’s observational data. This distribution can be seen in Figure 1 below.
11

Figure 1: EVS Housekeepers are using TeleTracking Most of the Timen=17, Data Collected: 11/11/16-11/14/16
Because these results conflict with the team’s observations, it is likely that many of these housekeepers are recording room cleans in direct sequence, instead of logging in at the beginning and logging out at the end of a clean.
The team’s analysis of TeleTracking data supports the inferences drawn from the team’s initial observations that TeleTracking use is inconsistent. The team examined average turn time across individual EVS housekeepers (denoted by number) as shown in Figure 2.
12

Figure 2: Variance Reveals Discrepancies Between Housekeepers’ Standard Proceduren=7631 room cleans, Data Collected 6/1/16 - 11/17/16
The average turn time in TeleTracking data is 16.5 minutes with a standard deviation of 9.1 minutes. The figure clearly shows this variance. The team has determined that the variation of turn time across employees is a result of lack of standardized procedure when using the TeleTracking system. This information coupled with the team’s qualitative results confirm that employees do not all follow the same standard procedure using the system.
Cleaning PracticesThe team observed that ED room cleans may be abbreviated if a patient needs to use the room quickly, creating inconsistency in clean time. Additionally, the team observed each EVS housekeeper employing different cleaning processes. This further contributes to variation in clean times.
“Standardizing the Monitoring Process of Inpatient Room Cleaning to Reduce the Spread of Hospital Acquired Infections,” an IOE 481 project performed in Spring 2010, focused primarily on the cleaning process. The project included important information about work policies and the relationship between EVS and ICE. The report recommended further investigation into standardization: “further investigate the variation in cleaning practices so as to determine what custodial cleaning procedures should be standardized and what should be left to personal preference,” [2]. This aligns with the team’s observations of non-standard cleaning procedures.
The team’s findings confirm that the reporting process requires clarification and cleaning practices require standardization. Further training and clarification will improve the accuracy and informative nature of the data for future analysis.
Discontinuous Communication Flow
Through thorough observation of the existing cleaning processes the team constructed a communication map between EVS and the ED. The flow is shown in Figure 3 with a dotted
13

arrow representing the major gap in communication. No housekeepers directly tell nurses that a room is clean.
Figure 3: Largest Gap in Communication between EVS and ED
The results of nurse surveys built upon the need for enhanced communication with 39.5% of commenting respondents recommending improved communication. The responses from surveyed nurses suggested two-way communication, EVS tracking boards, and teaching housekeepers how to use MiChart.
The Fall 2014 IOE 481 project titled “Efficient Patient Placement in the Emergency Department” contained information relating to communication gaps between EVS and the ED. The first relevant recommendation from this project describes the time between patient discharge and beginning room cleaning. The recommendation advises “standardizing the signal of a dirty bed to EVS. This signal could be using papers, the tracking board, or any other method as long as it is consistent and quick,” [1]. The second recommendation describes the process that occurs between the end of a room clean and the admission of a new patient into a room: “the team recommends reducing this time by standardizing the signal of a clean bed to the ATL,” [1]. These recommendations cite communication between the ED and EVS as a main disruptor of process flow. This supports the conclusion that communication is a major factor preventing the deep-cleaning of 100% of ED rooms every 24 hours drawn from the IOE 481 team’s observations. Additionally, the report revealed that ED staff recommended that EVS staff should receive access to the ED tracking board.
Missed Opportunities for Deep-Cleaning
In examining the Hospital Occupancy data, a general trend was exhibited across all three months of patient stay data. Figure 4 below details the percent capacity of ED rooms occupied by hour.
14

Figure 4: Average occupancy is generally lowest from the hours of 5-8AMn= 17,971 Patient Visits, Data Collected 7/01/16 - 9/30/16
The percentage of occupancy in the ED reflects windows of opportunity in which both the ED and EVS are likely to be able to achieve their respective goals. The ED seeks to have as many rooms available as possible to reduce patient wait time, allowing for fast treatment of patients. The goal of EVS is to achieve a deep-clean of each room every 24 hours. When occupancy is lowest, specifically from the hours of 5-8AM, both goals are most readily achievable. EVS housekeepers have the most rooms available which they can deep-clean and the ED is able to accommodate incoming patients with low wait times.
During the hours of 3-8PM, occupancy is highest. This presents challenges to each of these goals. Namely, the ED cannot accommodate as many new patients, forcing patient wait time to increase. As patients fill rooms at an increasing rate, EVS housekeepers are challenged by a limited amount of time to clean each room, as well as a limited selection of rooms to deep-clean. Rooms which have not been deep-cleaned in the 24 hour period are more likely to be occupied during these peak hours, thus preventing the achievement of the aforementioned EVS goal.
A similar analysis from an Industrial Engineer in Program & Operations Analysis found in Appendix E, Figure E1 supports the team’s findings about the general trend in hospital occupancy data. The data analysis continued to show occupancy trends for each area of the ED: East A, East B, EC3, Main, South, and West. Both the team’s and the Industrial Engineer’s analysis should be used to help assist in the creation of staffing models to maximize EVS ability to deep clean 100% of rooms in 24 hours.
Minimal Collaboration
Housekeeper surveys articulated a need for increased collaboration amongst EVS staff and between EVS and ED staff. The most impactful housekeeper survey responses were found to the
15
last two questions. Housekeepers were asked about opportunities for improvement and solutions to persistent problems. 55% of housekeepers who left comments indicated a desire for greater teamwork and clarified expectations. 21% of commenting respondents to nurse surveys supported increased teamwork as well.
“Strike a Balance with Decentralized Housekeeping,” an article from Nursing Management, describes the initial state at Santa Rosa Memorial Hospital much like that at UMHS. By decentralizing the housekeepers and making them valuable members of the patient-care teams, Santa Rosa Memorial Hospital was able to create dialogue and collaboration between the housekeeping and nursing departments to foster mutual trust and respect [3]. In their new roles, “service partners felt positive about several aspects of the decentralization, including better communication and teamwork and increased understanding of roles between nursing staff and the service partners. They appreciated nurse managers’ support and accessibility,” [3]. This unique problem-solving approach lends a new perspective to the issues Environmental Services is encountering in the Emergency Department.
RECOMMENDATIONS
The main goal of the UMHS ED is to give patients the most efficient and safe care as possible. To do this, the ED staff focuses on getting patients in and out of ED rooms as quickly as possible. This often means that ED nurses will clean their own rooms with the sanitary wipes and EVS staff will only be contacted to pull linens or trash. On the other hand, the EVS staff focuses on performing their daily tasks as well as making sure all rooms are as clean as possible.
While both the ED staff and the EVS staff are working towards making UMHS as efficient and safe as possible for ED patients, the main goals of the two departments conflict. To achieve the goal set by ICE of deep-cleaning 100% of ED rooms every 24 hours, it is essential that both the EVS and ED staff align their goals and work together.
The following recommendations must be implemented to achieve the primary goal of 100% of ED rooms deep-cleaned every 24 hours.
● Retrain staff.● Identify one EVS housekeeper from each shift as a shift leader.● Re-examine staffing levels.● Improve communication between ED staff and EVS staff.● Track when deep-cleans are being performed.
Retraining
The main goal of the UMHS ED is to give patients the most efficient and safe care as possible. To do this, the ED staff focuses on getting patients in and out of ED rooms as quickly as possible. This often means that ED nurses will clean their own rooms with the sanitary wipes and EVS staff will only be contacted to pull linens or trash. On the other hand, the EVS staff focuses on performing all of their daily tasks as well as making sure all rooms are as clean as possible.
16

While both the ED staff and the EVS staff are working towards making UMHS as efficient and safe as possible for ED patients, the main goals of the two departments conflict. To achieve the goal set by ICE of deep-cleaning 100% of ED rooms every 24 hours, it is essential that both the EVS and ED staff align their goals and work together. The team recommends that both the EVS and ED staff undergo retraining to facilitate communication and understanding between departments.
For the EVS staff training, it is crucial that the housekeepers understand how to use the whiteboard and MiChart. When observing, the team discovered that several housekeepers did not know how to use MiChart, so they relied solely on pages from the ED staff. Others proactively examined the ED whiteboards to quickly and efficiently address room-cleaning needs. The team also recommends that the EVS staff be retrained on proper deep-cleaning procedures and the importance of performing deep-cleans whenever time permits. After training, the team recommends attaching a laminated checklist of the eight steps of a deep-clean to each housekeeper cart to constantly remind housekeeping staff of the proper techniques.
The team recommends holding a workshop with both the ED housekeepers as well as the ED staff that discusses the ED-EVS Service Level Agreement, emphasizes the importance of deep-cleans, and the stresses the importance of interdepartmental communication.
Identifying EVS Housekeeper Leadership
To promote communication between the ED and EVS, the team recommends that each shift of housekeepers has one designated housekeeper as the leader. This leader will be expected to participate in nurse huddles as well as conduct huddles with all of the housekeepers in the ED. The leader will act as the spokesperson for the housekeepers. In terms of reaching the primary goal, the housekeeper shift leader will be able to notify the ED nurses when a room needs to go offline for a deep-clean. Currently at the nursing change of shift huddle, staff is updated on the status of their ‘handwashing goal’. In a similar fashion, transparency of deep-cleaning results can be shared to help increase urgency and motivation towards the 100% goal. This key statistic should be included in change of shift huddles.
Re-Examining Staffing Levels
Staffing levels were outside the scope of this project; however, several ED staff and housekeepers said that more housekeepers could be beneficial. The team’s analysis of the hospital occupancy data suggested that the greatest window of opportunity for deep-cleans is between 5-8 AM. A future IOE 481 project should focus on time studies to determine if the ED is staffed adequately as well as potential re-configuration of the current housekeeper scheduling model. The graphs in Appendix E indicate slight differences in room availability from unit to unit in the ED. These graphs may influence EVS housekeeper scheduling within each unit.
Improving Communication
The following paragraphs outline different methods that could be implemented to improve interdepartmental and intradepartmental communication. A combination of these methods could
17

potentially be used to reach the primary goal. The methods include the current paging system, walkie talkies, and iPods.
Communicating via PagersHousekeepers rate the current paging system at a 6.5/10 for efficiency, according to the housekeeper survey results. Given this information, it is clear that the paging system is not the only reason that 100% of deep-cleans are not happening every day. Benefits of the current paging system include the following: it already exists, so it will not cost extra to continue implementing it; pages allow housekeepers to have a written record of their requests; and housekeepers do not mind this system and they will not need additional training on this matter. The team believes that the staff retraining will promote communication, and thus, new technology may not be necessary at this point in time. Cons of the paging system include the following: it does not promote two-way communication because housekeepers cannot respond to pages via pager; and nurses have reported significant lag time between when a page is sent and when a housekeeper starts cleaning a room. This lag time can be broken into two parts: the time between when a page is received and when a housekeeper reads it; and the time between when a page is read and when the housekeeper takes action to fulfill the pager request. Despite the cons, the paging system is still a viable option and should be considered.
Communicating va Walkie TalkiesAn alternative solution for the housekeepers to utilize for communication is a set of walkie talkies. Each Housekeeper on shift would have their own walkie talkie, as would either a clerk or nurse tech in each area of the ED. When a room needs to be cleaned, the nurse tech or ED clerk would send out the request orally over the walkie talkie. The benefits of utilizing walkie talkies include: low cost, two-way communication between departments, zero lag time in request acknowledgement, and collaboration between EVS workers.
By receiving clean requests over the walkie talkies, the housekeepers will not have to stop what they are doing to view the request like they currently have to with the paging system, reducing lag time. Another benefit of utilizing walkie talkies is that they will enable two-way communication between departments. Nurses can tell the EVS workers what condition the room is in and what priority the clean is. In response, housekeepers could tell them when they finish or give them updates on their estimated time remaining. This would help avoid patients arriving before housekeepers have left the room as well as delays in utilizing a room that is now clean during busy hours. Moreover, the walkie talkies will enable the housekeepers to talk to each other and work together. This will be particularly advantageous when one housekeeper receives multiple requests in a short period of time, developing a queue. With the walkie talkies a housekeeper that has a queue can radio for support from nearby coworkers that may not be as busy.
The cons of utilizing the walkie talkies are that there will not be a written record for housekeepers and that they increase noise in the ED. These cons could be mitigated by equipping housekeepers with paper to write requests on as well as earpieces to reduce noise.
Communicating via iPods
18

Ideally, iPods could be utilized to promote communication as well as track deep-cleans. If each housekeeper had an iPod, it would be equipped with the following two applications: a messaging application and a tracking application. The deep-clean tracking functionality will be discussed in detail in the following section. The benefits of having iPods as a communication device include the following: two-way communication via a messaging app and a written record of requests for housekeepers. The messaging app will bridge the gap in communication by allowing housekeepers to send a message to the nursing staff as soon as a room is done being cleaned. In this model, the computers in the ED that display MiChart would also have the messaging app open so that they can easily see when a room is done being cleaned and switch its status on MiChart.
The cons of iPods include that they are resource-intensive, they have a high risk for theft, and housekeepers could use the messaging app for personal use. Not only are iPods expensive, but the housekeepers would have to be trained how to use the messaging app and monitored to prevent usage of the app for personal reasons outside of work. To avoid theft, the team recommends locking the iPods to the cart. The biggest con of the iPod system is that, according to the Senior Business Analyst of EVS, the iPods might not be compatible with Epic. If this is the case, it would not make sense to utilize iPods for solely communication purposes. If the new Epic system does find a way to allow tracking in the ED, the iPods would be ideal because they provide a solution to communication as well as tracking.
Tracking Deep-Cleans
The following paragraphs outline different methods that could be implemented to track the performance of deep-cleans. These methods can be used individually, in conjunction with each other, or in conjunction with any combination of the communication methods previously outlined to help EVS reach its primary goal. The methods include paper tracking and iPods.
Tracking via PaperThe purpose of the paper trackers is to provide a real time tracking method and that can drive work. Each unit would have a dedicated paper near the white board listing the room numbers in that unit. Next to the room numbers are three additional columns for the shifts (Appendix F). Every time a worker deep-cleans a room they mark the time they completed it under their shift. By doing so, both housekeepers and nurses can see which rooms have not been cleaned yet and need to be flagged when they become available. This would be especially useful in the AM and midnight shifts. For the midnight shift, housekeepers and nurses can see which rooms have not been cleaned all day, and therefore need to be cleaned during their shift in order to achieve the departmental goal. During the AM shift, as the sheets are changed, the EVS leader can identify which rooms are overdue for a clean and can tell both nurses and fellow housekeepers during their huddles. By doing so, both parties will be on the same page and can work together to get those overdue rooms deep-cleaned as soon as possible. Additionally, the data from these sheets can be input into excel each day quickly using a macro. This would either be able to replace TeleTracking or work in conjunction as a second data collection method in order to track the long term performance of the EVS departments regarding deep-clean percentages.
19

Tracking via iPodsTracking would ideally be done through iPods. The pros of this method are that it would take less time to enter a clean via iPod than it takes to login/logout via TeleTracking and it could potentially provide an easy tracking method compatible with Epic. As mentioned in the previous section, it is unclear currently whether Epic will allow a deep-clean tracking functionality within the ED. According to the Senior Business Analyst at EVS, Epic may not have all of the ED rooms enabled for EVS, so staff would not be able to login to rooms that aren’t enabled. Additionally, once Epic is fully implemented in the hospital, the TeleTracking system will be deleted.
On the other hand, if Epic does find a way to enable all ED rooms for EVS services, the team recommends contracting a student group from the EECS department at the University of Michigan to design an application to allow housekeepers to track deep-cleans via iPod. This app could take the following inputs and enter them into a database: housekeeper ID number, room number, time of day, and whether the clean was a deep-clean or not. This would allow the data to differentiate between the types of cleans being performed (which is not a functionality of TeleTracking).
EXPECTED IMPACT
The IOE 481 team anticipates that retraining and identifying EVS leadership will encourage communication and future improvement efforts between the ED and EVS. These recommendations should also work towards strengthening the relationship between EVS housekeepers and ED staff.
The assortment of solutions provided will allow EVS to more accurately assess deep-clean performance within the ED. Any combination of the communication and tracking solutions will permit EVS to develop a baseline for performance and make concrete steps towards increasing the portion of ED rooms deep-cleaned every 24 hours.
The team’s analysis on staffing levels can be leveraged by future project teams to develop an appropriate and efficient staffing model for EVS housekeepers.
20

REFERENCES
[1] Anshul Mehta, Austin Timmer, Sarah Tommelein, and Timothy Vervaeke, “Efficient Patient Placement in the Emergency Department,” Univ. of Michigan, Ann Arbor, MI, Dec. 9, 2014.
[2] Melissa Chen, Michelle Delaney, Lantei Takona, and Yiwen Xu, “Standardizing the Monitoring Process of Inpatient Room Cleaning to Reduce the Spread of Hospital Acquired Infections,” Univ. of Michigan, Ann Arbor, MI, Apr. 23, 2010.
[3] Robin Hagenstad, Carol Weis and Kathy Brophy. Strike a balance with decentralized housekeeping. Nursing Management. 31(6), pp. 39-43. 2000. Available: http://search.proquest.com/docview/231433137?accountid=35396.
21

22

APPENDIX A: EVS-ED SERVICE-LEVEL AGREEMENT
23
24

25

26

27

28

29

30

31
32

33

34

35

36
APPENDIX B: STANDARD INTERVIEW QUESTIONS
1. What is your role?2. How do you feel about the pager system?3. What is a deep-clean?4. If you perform deep-cleans, how often do you perform them?5. If you perform deep-cleans, on average how long do they take?6. What issues do you see in the existing cleaning process?7. What ideas do you have to resolve these issues?
37

APPENDIX C: HOUSEKEEPER SURVEY QUESTIONS
Housekeeper Survey
1. Which area of the ED do you work in?a. Mainb. C&W
2. What shift do you work on?a. Daysb. Afternoonsc. Midnight
3. Please rate how often you feel overwhelmed (with workload or work requests) during your shift by circling one of the following options:
a. never overwhelmed b. occasionally overwhelmedc. overwhelmed half the timed. often overwhelmede. always overwhelmed
4. How often do you log a room into TeleTracking immediately before beginning a clean and log out immediately after finishing a clean? Please circle one option.
a. Neverb. Occasionallyc. Half the timed. Oftene. Always
5. Please rate the pager system currently used on a scale of 1 (inefficient and ineffective) to 10 (very efficient and effective).
For the purposes of this survey a deep-clean is defined as a discharge clean performed solely by an EVS housekeeper that includes high-dusting, damp-wiping bed and main touchpoints, cleaning sink, pulling trash and linens, restocking supplies, dust mopping floors, wet mopping floors, and inspecting the walls and ceilings.
6. How many times per 24 hours do you perform a deep-clean? 7. Estimate the percentage of your shift that you spend performing deep-cleans compared to
other activities.8. How many times a shift do you get a request from a nurse for a room needing a deep-
clean?9. What opportunities for improvement/issues do you see in the room cleaning process?10. What ideas do you have for solutions to these issues?
38

APPENDIX D: NURSE SURVEY QUESTIONS
Nurse Survey
1. What role (if any) do you play in the room cleaning process?
2. How many times during a given hour do you instruct an EVS housekeeper to clean a room?
3. How do you communicate cleaning instructions to EVS staff? (circle all that apply)a. Pager (or phone)b. Word of Mouthc. Other: _________
4. How often do you send a request for a room needing a deep-clean? For the purposes of this survey a deep-clean is defined as a discharge clean performed solely by an EVS housekeeper that includes high-dusting, damp-wiping bed and main touchpoints, cleaning sink, pulling trash and linens, restocking supplies, dust mopping floors, wet mopping floors, and inspecting the walls and ceilings.
a. Neverb. Occasionallyc. Half the timed. Oftene. Always
5. How many times per 24 hours do you think a room receives a deep-clean?
6. What opportunities for improvement/issues do you see in the room cleaning process?
7. What ideas do you have for solutions to these issues?
39

APPENDIX E: ED OCCUPANCY DATA ANALYSIS FROM INDUSTRIAL ENGINEER, PROGRAM & OPERATIONS ANALYSIS
Figure E1: Analysis of Total ED Occupancy
Figure E2: Analysis of East A ED Occupancy
Figure E3: Analysis of East B ED Occupancy
40

Figure E4: Analysis of EC3 Occupancy
Figure E5: Analysis of Main ED Occupancy
Figure E6: Analysis of Resus ED Occupancy
41

Figure E7: Analysis of South ED Occupancy
Figure E8: Analysis of West ED Occupancy
42

APPENDIX F: PAPER TRACKING EXAMPLE - START OF MIDNIGHT SHIFT
Day Evening Night
41 9:15
42 5:10
43 12:30
44
45
46 11:45
47 7:30
48
49
50 2:00
51 10:00
52
53 3:12
54
55 11:00
56 9:30
57
58 6:15
59
60
61 6:45
62
63
64 10:10
65
66
67
East
ED
43

44