systems engineering, fieldwork and point-of-care …web2.facs.org/.../d1-s9-greenbergpowerpoint.pdf2...
TRANSCRIPT

Caprice C. Greenberg, MD, MPH, FACS Associate Professor of Surgery
WARF Professor of Surgical Research Director, Wisconsin Surgical Outcomes Research (WiSOR)
University of Wisconsin - Madison
Systems Engineering, Fieldwork and Point-of-Care Research

Take Home Points
• Research at the point of care is critical to improve quality and safety
• A systems view of healthcare is necessary to understand complexity in the work environment
• Simple 6 step process can get you started


Defining Patient Safety
• NPSF – The avoidance, prevention, and amelioration of adverse outcomes or injuries stemming from the processes of healthcare
• IOM - Safety does not reside in a person, device or department but stems from the interactions of components of a system
* IOM, To Err Is Human, 1999

Traditional Thinking in Medicine
Patient Characteristics
Outcomes

Good Outcome Unsafe Process
Time and Progression of Clinical Course or Treatment
Dec
reas
ing
Pat
ient
Saf
ety
Time and Progression of Clinical Course or Treatment
Dec
reas
ing
Pat
ient
Saf
ety
Time and Progression of Clinical Course or Treatment
Dec
reas
ing
Pat
ient
Saf
ety
Baseline Clinical
State
Good Outcome Safe Process
Bad Outcome Unsafe Process
Time and Progression of Clinical Course or Treatment
Dec
reas
ing
Pat
ient
Saf
ety
Bad Outcome Safe Process
Baseline Clinical
State
Baseline Clinical
State
Baseline Clinical
State

Operations/QI v. Research

Six Steps
1 Finding collaborators 2 Identifying a conceptual framework 3 Data collection and sampling strategies 4 Approaches to analysis 5 Presenting results 6 Dissemination and implementation

FINDING COLLABORATORS Step 1


Engineering
• Industrial Engineering
• Systems Engineering
• Human Factors Engineering

Psychology
• Organizational Psychology
• Cognitive Psychology

IOM
• Engineering has the potential to improve both efficiency and quality
• Continuous improvement principles can lead to more efficient, safer, and higher quality

CONCEPTUAL FRAMEWORKS Step 2

A system is a complex assembly of people, information, resources, equipment and procedures working toward a common goal

Vincent, (2004) Annals of Surgery

James Reason
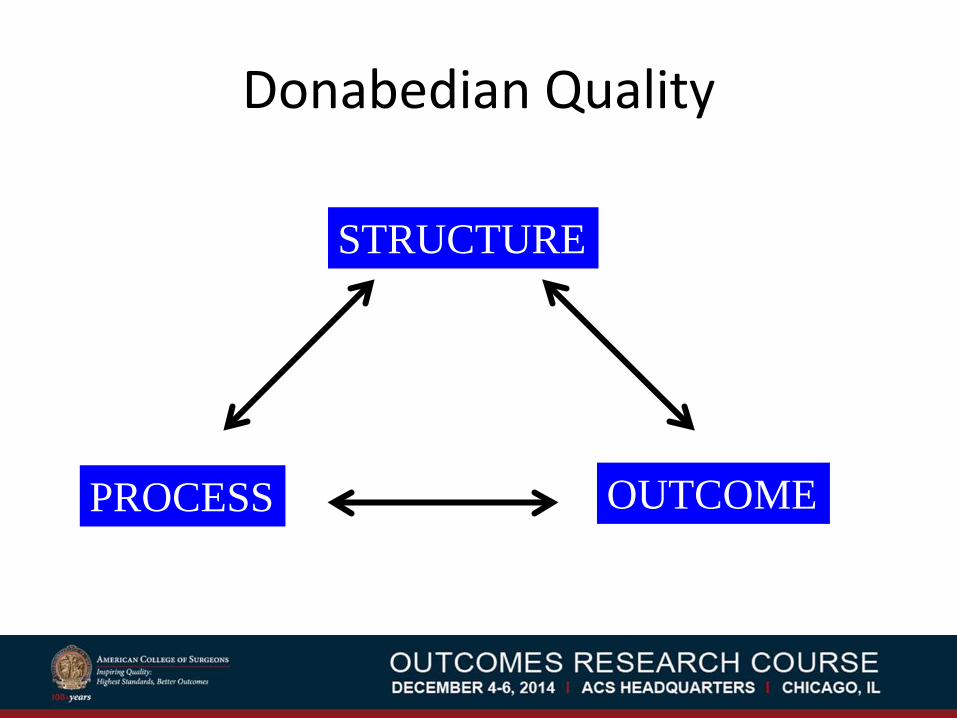
Donabedian Quality
STRUCTURE
PROCESS OUTCOME
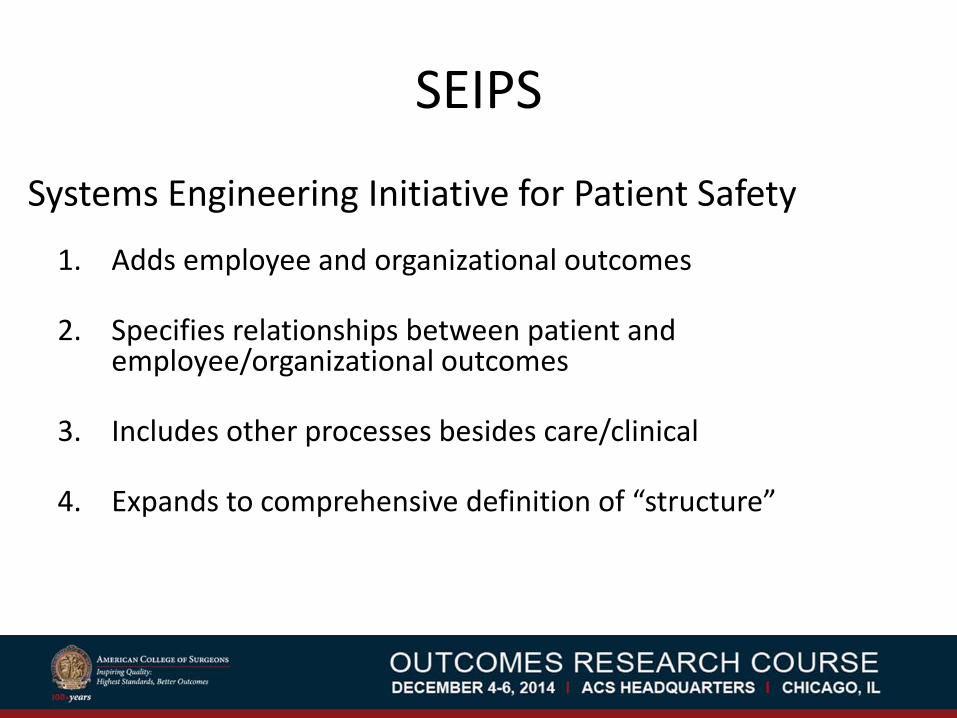
SEIPS
Systems Engineering Initiative for Patient Safety
1. Adds employee and organizational outcomes
2. Specifies relationships between patient and employee/organizational outcomes
3. Includes other processes besides care/clinical
4. Expands to comprehensive definition of “structure”

SEIPS

Our Conceptual Framework
Baseline Risk Profile
Patient Outcome
Individual provider
performance
Team performance
System / organization performance
Expected course
Vulnerability
Resilience
Time

DATA COLLECTION AND SAMPLING Step 3

Types of Data
• Quantitative: anything that can be measured in terms of quantity, amount, intensity, or frequency.
• Qualitative: qualities, processes and meanings of things
• Mixed Methods

Complementary Approaches

• Medical record
• Floor plans to assess flow
• Protocols and policies
• Position descriptions to determine roles
Existing Documentation

• Interviews – Structured – Semi-structured
• Focus Groups
• Questionnaires / Surveys
– Likert scales – Open-ended questions
Frontline Providers

• Ethnography • “Shadowing” • Time and motion studies
• Critical considerations:
– Data collection tools – Content v. domain experts – Training of observers – Sampling strategy
Observational Field Studies

Audio - Video Capture

Video v. Live Observation
• Complete record
• Extract, count, correlate as salient issues evolve
• Larger number of observers
• Self-evaluation and reflection

Limitations to Video • Expensive
• Can be intrusive
• Can limit range of settings
• Analysis is time-consuming
• Discoverability, confidentiality, privacy
• Requires a cultural shift

APPROACHES TO ANALYSIS Step 5

Examples • Systems analysis
• Time and motion analysis
• Root cause analysis
• Failure modes and effects analysis
• Statistical process control charts

Usability Studies

RATE
• Event Tracker List – Time stamps events intrinsic to every
operation • Event Tracker Counter
– Environmental disruptions/interruptions – Start/stop times for specific events
• Flag performance or factor examples * Guerlain S, Shin T, Guo H, Calland JF (2002) Team performance data capture and analysis system. In: Proceedings of HFES 46th Annual Meeting, Baltimore



MVTA

Motion Analysis

Identify objects of interest
Image source: Mayo SPARC
• Identify objects • Code behaviors • Temporal coding • Analyze
sequences • Link with
outcomes
Montague, E., *Xu, J., *Asan, O., *Chen, P., Chewning, B., Barrett, B., (2011) An illustration of modeling eye gaze patterns in doctor-patient interaction with lag sequential analysis, Human Factors: The Journal of the Human Factors and Ergonomics Society, 53(5), 502-16.

PRESENTING RESULTS, DISSEMINATION AND IMPLEMENTATION
Step 5 and 6

Convey Your Message
• Quantitative – Descriptive statistics – Counts – Tables and figures
• Qualitative – Illustrative examples and quotes – Compare and contrast cases – Diagrams

DISSEMINATION IMPLEMENTATION
Goal Active spread of information Active intervention
Characteristics Less structured More theory and frameworks exist
Level Policy Institution and provider
Target Community and population Specific individuals and small groups
* Adapted from Ross Bronson. Training Institute for D& I Research in Health

STUDY EXAMPLES

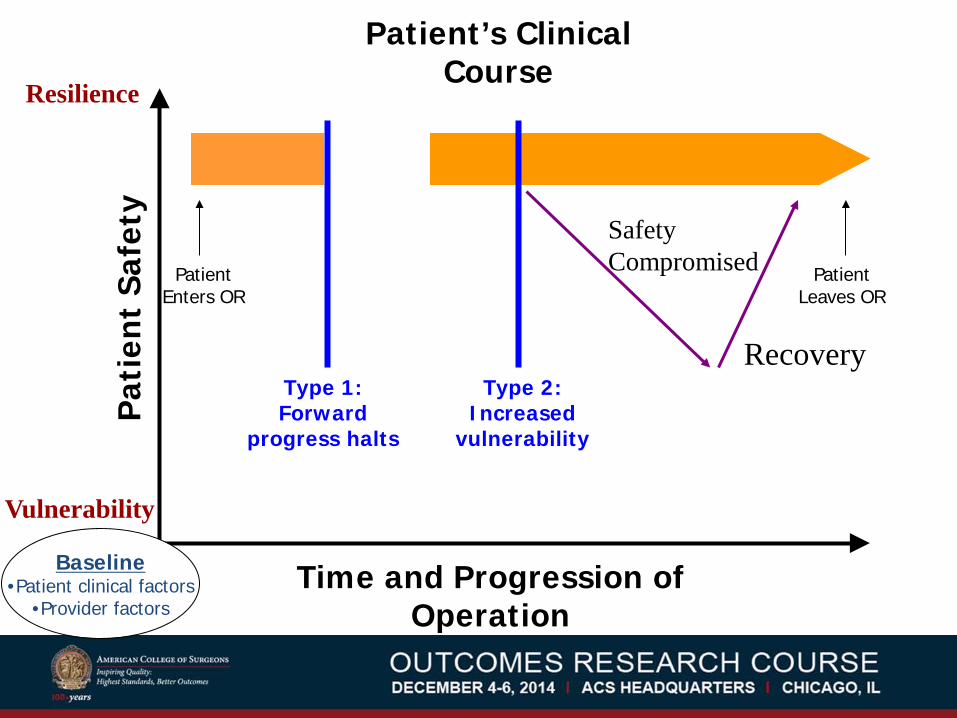
Study #1: Protecting Patients from an Unsafe System
Deviations and Resilience
in the OR
Hu et al., Annals of Surgery (2012); 256(2): 203 – 210
Pat
ient
Saf
ety
Time and Progression of Operation
Baseline •Patient clinical factors
•Provider factors
Type 2: Increased
vulnerability
Type 1: Forward
progress halts
Patient Enters OR
Patient Leaves OR
Patient’s Clinical Course
Safety Compromised
Recovery
Resilience
Vulnerability

• Total of 24 deviations identified in 8 cases – 5 delays (Type 1) – 14 safety-compromising (Type 2) – 5 combined Type 1 & 2
• One every 1.5 hours of operative time
Quantitative Results

Description: • 16 minutes after incision, a beeping noise
starts. It lasts about 10 minutes. • All anesthesia and nursing personnel become
absorbed in trying to figure out what’s beeping.
• Unclear if it is a monitor or malfunctioning equipment
Qualitative Results


Quantitative Results
Contributing Factors % Involving
Mitigating or Compensatory Factors
% Involving
Individual Provider
Knowledge/Training Leadership
25 17
Monitoring/Vigilance Knowledge/Training Decision-Making Leadership
63 17 17 38
Team Communication Coordination
33 46
Communication Coordination Cooperation
50 33 33
System Equipment (Failure) Organizational Structure
17 29

Resilience
• The ability to anticipate, cope with, recover and learn from unforeseen challenges
• Understand gaps in system operation and expert strategies to bridge – Recognition of variation in workload during a case and
willingness to forego poorly timed breaks – Interim count at timing of handoffs – Competing goals resolved with cross-disciplinary
communication and collaborative problem solving
* Nemeth, Wears, Woods, Hollnagel, Cook. Minding the Gaps: Creating Resilience in Healthcare

Approach to Education
Error Prevention • Current approach to
improving surgical safety
• Erratic people degrade an otherwise safe system
• Increased standardization and tighter coupling
Resilience • Alternative approach
based on error mitigation
• Practitioners primary source of resilience in imperfect system
• Requires adaptability and flexibility
* Patterson, Woods, Roth, Cook, Wears, Render. J Patient Safety (2006) 2(1): 1-6

Study #2: A Prospective Study of Patient Safety in
the Operating Room
Christian et al. Surgery (2006); 139: 159-173.


Emerging Themes
• Communication and Information Flow – Generalized vulnerability
– Multiple points in the peri-operative period
– Significant impact on case progression
• Workload and Competing Tasks – Poor synchronization with case progression
– Counting introduced strain on the system

SNT-SNC1C2C3
[2][1]
2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 1 2 3 4 5 6 7 8 9 10 11 12 13 14
Counting Protocol
SCR
Repeat Counting Protocol
[2] [2] [1] [1] [2] [2] [1] [2] [2]
Time(min)
[1,2] [1,2] [1,2][1,2]
[1,2][1]
Near Miss Near Miss
Temporal Relationships

Study #3: Validating risk-adjusted surgical
outcomes: Site visit assessment of process and structure
Daley et al., JACS (1997); 185:341-51

Study Overview
• Validation of NSQIP included site visits
• Structured protocol for data collection
• Observers were dept. chiefs, RN, MD
• Identify characteristics of outlier status
• Predict high vs. low outlier status
• Exit interview to member-check results *

NSQIP Qualitative Results
• High outliers had: – Less spacious physical layout
– Higher per diem RN staffing & lower skill level
• Low outliers had: – Strong relationship with medicine and cardiology
– More interaction between surgeons and RNs
– More clinical pathways and practice guidelines

NSQIP Results and Implications
• Correctly identified 17 of 20 institutions as high or low outlier status
• Convincing evidence that differences exist in the quality of surgical care
• Risk-adjusted outcomes reliably discriminate quality of care

Take Home Points
• Research at the point of care is critical to improve quality and safety
• A systems view of healthcare is necessary to understand complexity in the work environment
• Simple 6 step process can get you started
