systemic treatment in breast cancer: a primer for radiologists · to facilitate breast-conserving...
TRANSCRIPT
REVIEW
Systemic treatment in breast cancer: a primer for radiologists
Aya Y. Michaels1 & Abhishek R. Keraliya1,2 & Sree Harsha Tirumani1,2 &
Atul B. Shinagare1,2 & Nikhil H. Ramaiya1,2
Received: 29 June 2015 /Revised: 24 September 2015 /Accepted: 21 October 2015 /Published online: 13 November 2015# The Author(s) 2015. This article is published with open access at Springerlink.com
AbstractCytotoxic chemotherapy, hormonal therapy and moleculartargeted therapy are the three major classes of drugs used totreat breast cancer. Imaging modalities such as computed to-mography (CT), magnetic resonance imaging (MRI), 18F-FDG positron emission tomography (PET)/CTand bone scin-tigraphy each have a distinct role in monitoring response anddetecting drug toxicities associated with these treatments. Thepurpose of this article is to elucidate the various systemictherapies used in breast cancer, with an emphasis on the roleof imaging in assessing treatment response and detectingtreatment-related toxicities.
Teaching Points• Cytotoxic chemotherapy is often used in combination withHER2-targeted and endocrine therapies.
• Endocrine and HER2-targeted therapies are recommendedin hormone-receptor- and HER2-positive cases.
• CT is the workhorse for assessment of treatment response inbreast cancer metastases.
• Alternate treatment response criteria can help in interpretingpseudoprogression in metastasis.
• Unique toxicities are associated with cytotoxic chemothera-py and with endocrine and HER2-targeted therapies.
Keywords Breast cancer . Hormonal therapy .
Molecular-targeted therapy . CT .MRI
Introduction
A paradigm shift has occurred over the past few decades in thesystemic (non-surgical and non-radiation) treatment of breastcancer, with treatment regimens evolving from single-agentchemotherapy to those involving hormonal therapy, combina-tion chemotherapy and molecular-targeted therapy (MTT) [1].Much of this evolution can be attributed to a better under-standing of the molecular complexity of breast cancer. Recentstudies have revealed that there are several molecular pheno-types of breast cancer, based on receptor expression [2]. Themajor subtypes of these include luminal A, luminal B, HER2-positive and triple-negative (TN) breast cancer [2]. The risk ofrecurrence, disease management and outcome of these majorsubtypes vary significantly.
Anti-oestrogen therapy is an integral part of hormone re-ceptor (HR)-positive cancers, and acts by inhibiting thegrowth of oestrogen-sensitive tumour cells [1]. In HER2/neu-positive cancer, MTTs directed to the HER2 receptor in-hibit signal transduction pathways involved in oncogenesis[1]. MTTs have also changed the course of treatment intriple-negative breast cancer (TNBC). The increased use ofthese drugs in clinical practice warrants the attention of radi-ologists who must be familiar with the patterns of tumourresponse to systemic therapy and the complications associatedwith them. Accordingly, the purpose of this article is to pro-vide a comprehensive review of the various cytotoxic,hormonal and biologic agents used in breast cancer inneoadjuvant, adjuvant and metastatic settings, with anemphasis on the role of imaging in assessing treatmentresponse and drug toxicities.
* Sree Harsha [email protected]
1 Department of Radiology, Brigham and Women’s Hospital, HarvardMedical School, 75 Francis Street, Boston, MA 02115, USA
2 Department of Imaging, Dana Farber Cancer Institute, HarvardMedical School, 450 Brookline Avenue, Boston, MA 02215, USA
Insights Imaging (2016) 7:131–144DOI 10.1007/s13244-015-0447-4

Systemic treatment in breast cancer: an overview
Systemic treatment in breast cancer includes cytotoxic chemo-therapy, hormonal therapy, molecular-targeted therapy or acombination of these (Table 1). Temporally, systemic treat-ment can be stratified into neoadjuvant, adjuvant and metasta-tic settings, with each having a distinct goal [1]. The objectiveof neoadjuvant treatment is to downgrade the tumour in orderto facilitate breast-conserving surgery and to guide post-operative chemotherapy. Adjuvant therapy is now standardpractice for reducing both systemic and local recurrence, withmost guidelines recommending systemic treatment for node-positive disease and tumours larger than 1 cm, irrespective ofother tumour characteristics.
The commonly used cytotoxic drugs are taxanes (paclitaxeland docetaxel), cyclophosphamide, eribulin, capecitabine, cis-platin and anthracyclines (doxorubicin and epirubicin).Taxanes and anthracyclines are the mainstay in first-line treat-ment of breast cancer in the adjuvant, neoadjuvant and meta-static settings, and are often used with HER2-targeted thera-pies in HER2-positive breast cancer and with hormonal ther-apy in HR-positive breast cancer. Anthracycline-based regi-mens have shown greater efficacy than non-anthracycline
based regimens in HER2-positive tumours [1]. National Com-prehensive Cancer Network (NCCN) guidelines recommendadjuvant cytotoxic chemotherapy for all tumours greater than1 cm, and consideration for use in tumours greater than 0.6 cmor in instances of microinvasion, regardless of molecular char-acteristics [1]. The drugs used in adjuvant therapy can also beused in a neoadjuvant setting, while single-agent therapy ispreferred for metastatic disease in order to reduce toxicity inaggressive regimens.
Hormonal therapy is recommended for most women withHR-positive breast cancer. Tamoxifen, a selective oestrogenreceptor modulator (SERM), acts as an antagonist of theoestrogen receptor (ER) in breast tissue and as agonist in theuterine endometrium [3]. Recently, another class of hormonalagents, called aromatase inhibitors (AIs), has shown superiorefficacy to tamoxifen in the metastatic, neoadjuvant and adju-vant settings in postmenopausal women. Anastrozole,letrozole and exemestane are the three most widely used ofthese drugs. These agents work by reducing the aromatizationof peripheral androgens into oestrogen [4]. Neoadjuvant hor-monal therapy has shown an equivalent to superior responsecompared to neoadjuvant chemotherapy in HR-positive breastcancer. Studies have demonstrated greater rates of breast-
Table 1 Systemic treatment in breast cancer
Drugs Mechanism of action Side effects
Chemotherapy
Anthracycline (doxorubicin and epirubicin) Inhibits DNA and RNA synthesis Cardiotoxicity, typhlitis, bone marrow suppression
Taxanes (paclitaxel and docetaxel) Inhibits mitosis by stabilization ofmicrotubule polymer
Fluid retention, neutropenic enterocolitis andtyphlitis, drug-associated pneumonitis
Cyclophosphamide Interferes with DNA replication byforming intrastrand and interstrandDNA cross-links
Hemorrhagic cystitis, Drug associatedpneumonitis, diarrhoea
Capecitabine Irreversibly inhibits thymidylate synthase Neurotoxicity, mucositis, hand-foot syndrome
Eribulin Inhibits mitosis by interfering withgrowth of microtubule
Neutropenia, diarrhoea, anaemia, peripheralnHER2athy
Hormonal therapy
Tamoxifen Selectively blocks estrogen receptorblockage
Hepatic steatosis and hepatotoxicity,hypercoagulability, endometrial proliferativechanges
Aromatase inhibitors(anastrozole, letrozole, and exemestane)
Blocks estrogen production Osteoporosis, arthralgia
Fulvestrant Estrogen receptor antagonist Elevation of liver enzymes, oedema
Molecular-targeted therapy
Trastuzumab, pertuzumab Interferes with the HER2/neu receptor Cardiotoxicity, pulmonary toxicity
Lapatinib Interrupts the HER2/neu and epidermalgrowth factor receptor (EGFR) pathways
Rash, diarrhoea, liver dysfunction,
Bevacizumab Inhibits vascular endothelial growthfactor (VEGF)
Hepatic steatosis, pancreatitis, cholecystitis,infection
Trastuzumab emtansine Antibody-drug conjugate binds to HER2receptors and enters the cell andreleases the cytotoxic agent emtansine
Hepatotoxicity, thrombocytopenia
132 Insights Imaging (2016) 7:131–144

conserving surgery in postmenopausal oestrogenreceptor-positive breast cancer patients on neoadjuvanthormonal therapy versus neoadjuvant chemotherapy [5].Furthermore, higher rates of breast-conserving surgeryhave been demonstrated in patients treated with AIs ver-sus tamoxifen [6]. Endocrine therapy has a better toxicityprofile and is preferred when chemotherapy cannot betolerated. Another anti-oestrogen agent, fulvestrant, isan ER antagonist, and unlike tamoxifen, has no agonisteffects. Fulvestrant was approved for second-line use inpostmenopausal women with HR-positive metastaticbreast cancer with disease progression following treat-ment with an anti-oestrogen [7]. Luteinizing hormone-releasing hormone (LHRH) agonists (goserelin,leuprolide), progestins (megestrol acetate), androgens(fluoxymesterone) and high-dose oestrogen (ethinyl es-tradiol) are other hormonal therapies used in the adjuvantand metastatic setting in breast cancer [1].
Trastuzumab (Herceptin) is a monoclonal antibodythat targets cancer cells that over-express a protein calledHER2 that is involved in cell growth, differentiation andblood vessel formation (angiogenesis). Up to 20 % ofwomen with breast cancer have tumours with high levelsof HER2, and many trials have demonstrated betterdisease-free survival with the addition of trastuzumab incombination with standard first-line chemotherapy for thetreatment of HER2-positive breast cancer [8, 9].Pertuzumab is another HER2 receptor inhibitor (HER2dimerization inhibitor) that has been approved by theUnited States Food and Drug Administration (FDA) foruse in metastatic breast cancer. Other targeted agentscurrently being studied in breast cancer include otherHER2-directed agents (lapatinib); HER3 agents, whichinhibit dimerization of the HER2 receptor and thus deac-tivate the tyrosine kinase pathway; vascular endothelialgrowth factor (VEGF) inhibitors (bevacizumab); poly(ADP-ribose) polymerase (PARP) inhibitors; and inhibi-tors of the mammalian target of rapamycin (mTOR) sig-nalling pathway [10, 11]. Lapatinib is an orally activedual tyrosine kinase inhibitor that affects both HER2/neu and epidermal growth factor receptor (EGFR) path-ways. It is being evaluated in patients with refractoryCNS metastases from HER2-positive metastatic breastcancer, given its ability to achieve therapeutic levels incerebrospinal fluid [12]. Studies such as the phase IIICLEOPATRA [Clinical Evaluation Of Pertuzumab andTrastuzumab] trial have demonstrated a benefit inprogression-free survival with the use of a dual anti-HER2 blockade in the metastatic setting over a singleanti-HER2 agent [13]. The NCCN guidelines now rec-ommend trastuzumab and pertuzumab (in combination)in HER2-positive metastatic disease in combination witha taxane [1].
Role of imaging in the assessment of treatmentresponse
Imaging plays a key role in monitoring response to treatment(Table 2). According to the NCCN guidelines, assessment ofdisease is most accurate when an abnormal finding is seriallyfollowed with the same imaging modality. There is no generalconsensus on the optimal frequency of restaging scans. Comput-ed tomography (CT) is generally recommended every 2–4 cyclesin patients on chemotherapy and every 2–6months in patients onendocrine therapy [1]. However, if the patient develops new orworsening signs and symptoms, appropriate imaging should bepursued immediately. Patients enrolled in clinical trials tend to berestaged more frequently to determine drug efficacy.
Multidetector computed tomography (MDCT)
MDCT is theworkhorse for monitoringmetastatic breast cancer.Liver metastases occur in more than 50 % patients with breastcancer, and are seen as hypodense lesions. Restaging MDCTscans following systemic treatment typically show a reductionin size of the hypodense lesions in patients responding to treat-ment (Fig. 1). Non contrast images are useful in finding accuratetumour volume on follow-up MDCT [14]. At our institute, weroutinely perform non-contrast imaging of the abdomen in allbreast cancer patients, as breast cancer metastases can some-times remain occult on the portal venous phase and can be betterfollowed on non-contrast images on restaging scans [14]. Theuse of multiphasic CT with arterial and venous phase imaginghas been shown to increase the detection rate of hypervascularliver metastasis, including those from breast, renal, and thyroidcancers, carcinoid tumours and melanoma [15]. There havebeen no large prospective studies analyzing the diagnostic accu-racy of MDCT in assessing treatment response in liver metasta-sis from breast cancer. The Response Evaluation Criteria inSolid Tumours (RECIST) is the most widely accepted set ofobjective treatment response criteria [16, 17]. A recent retro-spective study by He et al., however, showed that RECISTwas inadequate for assessing response to targeted therapies inbreast cancer liver metastasis. In their study of 39 patients with68 liver lesions, while treatment with cytotoxic chemotherapyshowed a decrease in both size and density of liver metastases,treatment with targeted therapies alone did not, although 2-yearsurvival was better [18].
A classic finding seen in treated breast cancer metastases ishepatic capsular retraction, or Bpseudocirrhosis^ (Fig. 1). Inpatients undergoing chemotherapy, pseudocirrhosis has beendocumented as a form of treatment response, described ascapsular retraction secondary to shrinkage and retraction oftumours. This finding occurs more often in larger than smallerhepatic lesions, suggesting that intrinsic pathologic character-istics such as tumour growth or fibrosis, rather than tumourresponse alone, may contribute to capsular retraction [19].
Insights Imaging (2016) 7:131–144 133
Treatment with molecular-targeted drugs can reduce the en-hancement of hepatic metastatic lesions compared to adjacentl iver parenchyma. This phenomenon, known aspseudoprogression, with the appearance of apparent new le-sions or transient enlargement of existing lesions is frequentlyseen on post-treatment follow-up CT examinations (Fig. 2)[20]. Similarly, lytic osseous metastatic lesions show osteo-blastic response after systemic therapy. Restaging scans mayshow apparent new sclerotic lesions due to osteoblastic treat-ment response, which can be confused as new bone metasta-ses (pseudoprogression) (Fig. 3) [21, 22]. Clinical and bio-chemical correlation (tumours markers) helps to assess treat-ment response in such cases.
Thoracic metastases in breast cancer can involve pulmo-nary parenchyma, airways, pleura and thoracic lymph nodes[23]. Imaging patterns of lung parenchymal metastases frombreast cancer include solitary or multiple lung nodules,endobronchial nodules, lymphangitic carcinomatosis andair–space consolidation. Pleural disease from breast cancerusually manifests as pleural nodularity, thickening and effu-sions. Metastatic parenchymal nodules are generally solid,spheric or ovoid in shape, sharply marginated, and locatedmostly in the periphery of the lung in contrast to other aetiol-ogies such as infection or inflammation [23]. However, a sol-itary pulmonary nodule appearing in a patient with breastcancer is not always suggestive of metastatic disease, as morethan 50 % of the nodules may have aetiologies such as
primary lung tumour or other benign lesions, and histologicalconfirmation is necessary [24]. Pulmonary nodules respond tosystemic treatment with a reduction in size. Cavitation of pul-monary nodules is uncommonly seen as secondary to bothcytotoxic chemotherapy and newer anti-angiogenic agents.To prevent misclassification as disease progression, alterna-tive methods of measuring cavitary lesions (i.e. exclusion ofthe air component during measurement) have been describedin the primary lung cancer literature [25].
Magnetic resonance Imaging (MRI)
Breast MRI In the neoadjuvant setting, breast magnetic res-onance (MR) imaging is a useful tool for monitoring responseto chemotherapy, and is superior to clinical examination, ul-trasound andmammography [26]. The tumour size correlationcoefficient between MRI and pathologic analysis is very high(more than 0.9) compared to that of clinical examination andmammography (around 0.7) [26]. MRI has demonstrated highsensitivity (96 %) and accuracy (89 %) for the detection ofresidual disease after neoadjuvant chemotherapy [27]. Variousstudies have shown that the accuracy of MRI in this settingvaries with the molecular subtype of breast cancer, the patternof enhancement on pre-treatment MRI and the nuclear grade[27]. MRI has demonstrated higher accuracy in assessingtreatment response and size changes in tumours withHER2+ or triple-negative status, and lower accuracy with
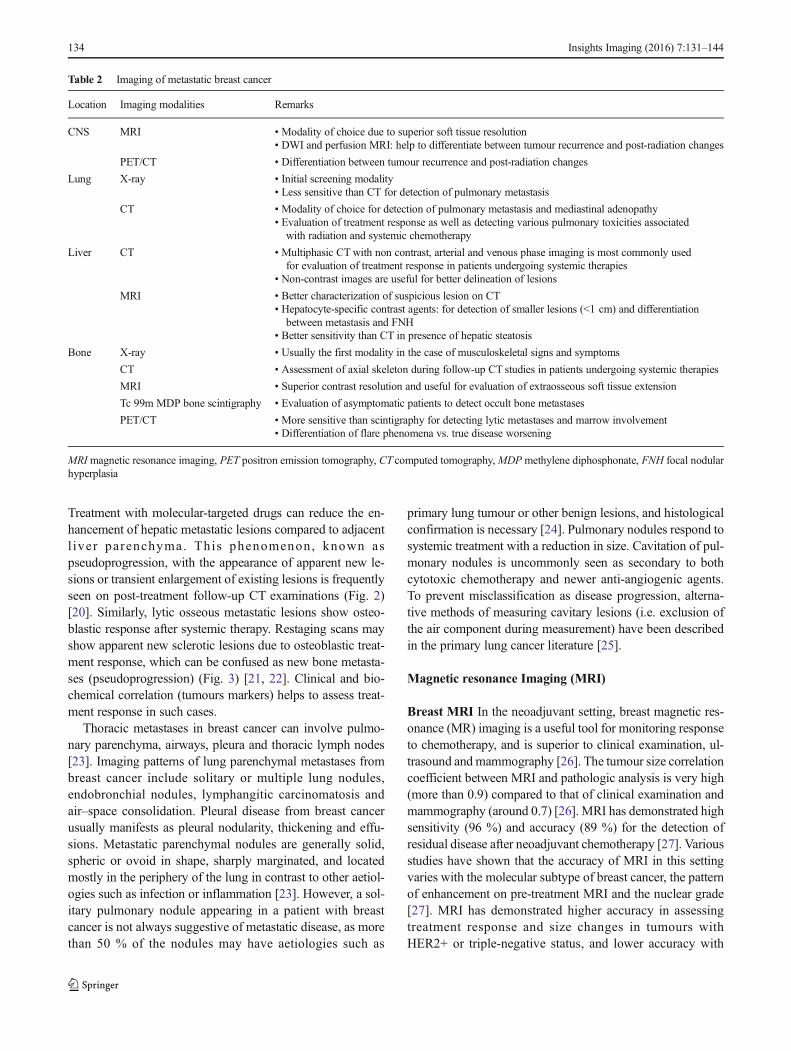
Table 2 Imaging of metastatic breast cancer
Location Imaging modalities Remarks
CNS MRI • Modality of choice due to superior soft tissue resolution• DWI and perfusion MRI: help to differentiate between tumour recurrence and post-radiation changes
PET/CT • Differentiation between tumour recurrence and post-radiation changes
Lung X-ray • Initial screening modality• Less sensitive than CT for detection of pulmonary metastasis
CT • Modality of choice for detection of pulmonary metastasis and mediastinal adenopathy• Evaluation of treatment response as well as detecting various pulmonary toxicities associated
with radiation and systemic chemotherapy
Liver CT • Multiphasic CTwith non contrast, arterial and venous phase imaging is most commonly usedfor evaluation of treatment response in patients undergoing systemic therapies
• Non-contrast images are useful for better delineation of lesions
MRI • Better characterization of suspicious lesion on CT• Hepatocyte-specific contrast agents: for detection of smaller lesions (<1 cm) and differentiation
between metastasis and FNH• Better sensitivity than CT in presence of hepatic steatosis
Bone X-ray • Usually the first modality in the case of musculoskeletal signs and symptoms
CT • Assessment of axial skeleton during follow-up CT studies in patients undergoing systemic therapies
MRI • Superior contrast resolution and useful for evaluation of extraosseous soft tissue extension
Tc 99m MDP bone scintigraphy • Evaluation of asymptomatic patients to detect occult bone metastases
PET/CT • More sensitive than scintigraphy for detecting lytic metastases and marrow involvement• Differentiation of flare phenomena vs. true disease worsening
MRI magnetic resonance imaging, PET positron emission tomography, CT computed tomography,MDP methylene diphosphonate, FNH focal nodularhyperplasia
134 Insights Imaging (2016) 7:131–144
luminal-type breast cancer, low nuclear grade and diffuse non-mass-like enhancement on initial MRI [27, 28]. Dynamiccontrast-enhanced MRI, in addition to morphological analy-sis, offers the advantage of evaluating enhancement kinetics,
which correlate with angiogenic changes in response to neo-adjuvant therapy (Fig. 4) [29].
Liver MRI Superior soft tissue characterization renders MRimaging particularly helpful in the evaluation of liver
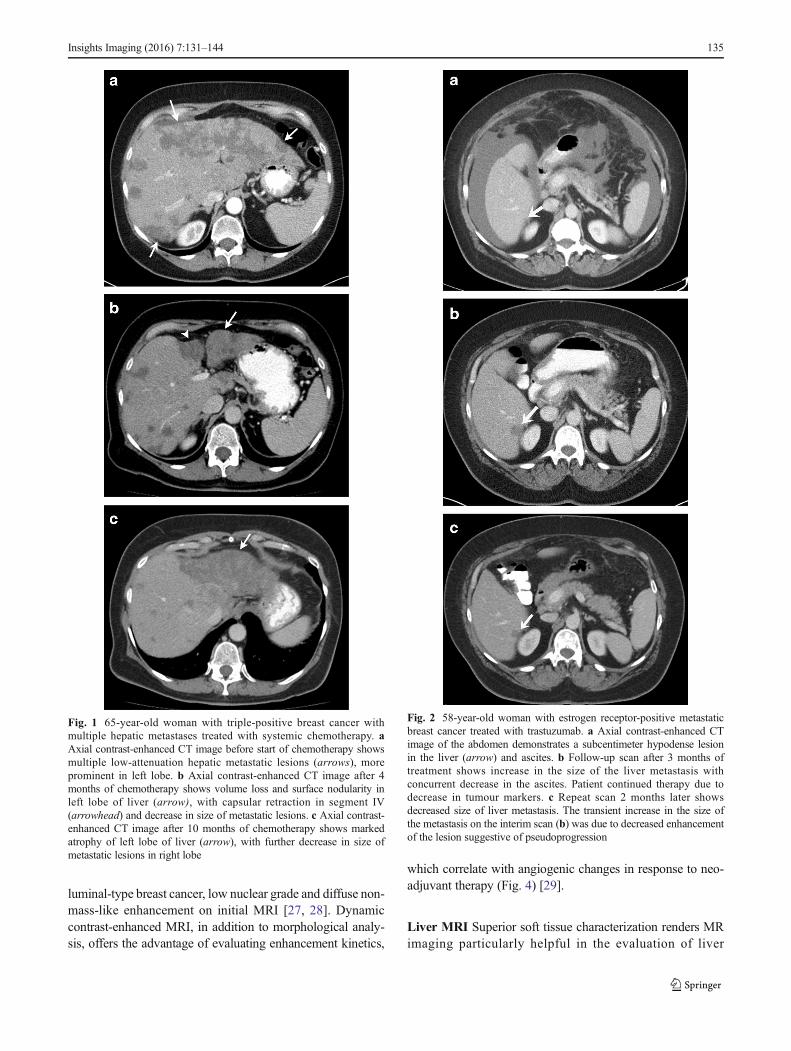
Fig. 1 65-year-old woman with triple-positive breast cancer withmultiple hepatic metastases treated with systemic chemotherapy. aAxial contrast-enhanced CT image before start of chemotherapy showsmultiple low-attenuation hepatic metastatic lesions (arrows), moreprominent in left lobe. b Axial contrast-enhanced CT image after 4months of chemotherapy shows volume loss and surface nodularity inleft lobe of liver (arrow), with capsular retraction in segment IV(arrowhead) and decrease in size of metastatic lesions. c Axial contrast-enhanced CT image after 10 months of chemotherapy shows markedatrophy of left lobe of liver (arrow), with further decrease in size ofmetastatic lesions in right lobe
Fig. 2 58-year-old woman with estrogen receptor-positive metastaticbreast cancer treated with trastuzumab. a Axial contrast-enhanced CTimage of the abdomen demonstrates a subcentimeter hypodense lesionin the liver (arrow) and ascites. b Follow-up scan after 3 months oftreatment shows increase in the size of the liver metastasis withconcurrent decrease in the ascites. Patient continued therapy due todecrease in tumour markers. c Repeat scan 2 months later showsdecreased size of liver metastasis. The transient increase in the size ofthe metastasis on the interim scan (b) was due to decreased enhancementof the lesion suggestive of pseudoprogression
Insights Imaging (2016) 7:131–144 135
metastases. Dynamic contrast-enhanced MRI has greater than90 % sensitivity in the identification of hepatic metastases,compared to contrast-enhanced CT at around 80 % [30].Hepatocyte-specific contrast agents, including gadoxetatedisodium (Eovist/Primovist; Bayer HealthCare, Leverkusen,Germany) and gadobenate dimeglumine (MultiHance; BraccoDiagnostics Inc., Princeton, NJ, USA), are excreted through acombination of biliary and renal routes [31]. Gadoxetatedisodium has approximately 50% biliary excretion in patientswith normal liver and renal function, and the addition of ahepatobiliary phase in dynamic-contrast MRI has shown in-creased sensitivity (more than 10 %) in detecting metastaticlesions over dynamic MRI alone (Fig. 5) [32]. These agentsare particularly useful in detecting small metastases, less than1 cm in size [33], and for differentiation of metastatic lesionsfrom focal nodular hyperplasia (FNH) [34]. In the assessmentof treatment response, MRI with in-phase and out-of-phase
imaging can be more effective for the evaluation of lesionsin the setting of chemotherapy-induced hepatic steatosis,which can obscure liver metastases [20]. Diffusion-weightedMRI has been shown in a few studies to predict early responseto treatment in breast cancer [35].
Brain MRI MRI is the best modality for localizing brainmetastases and assessing response to treatment (Fig. 6). Inpatients with a good prognosis, local control with surgeryand/or radiation treatment (either stereotactic or whole-brainradiation therapy) can be pursued. Measuring the response isoften difficult, as the appearance of post-treatment changescan mimic recurrent or residual pathology. Determiningwhether a ring-enhancing lesion at the site of the treated tu-mour represents treatment response (radiation necrosis orgranulation tissue surrounding a resection cavity) versus re-currence can be particularly challenging. The chronology ofthe appearance of the lesion can be helpful, as radiation ne-crosis typically appears within 4 months and resolves after 2–3 years [36]. Advanced MRI techniques such as diffusion andperfusion MRI are helpful for differentiating between tumourrecurrence and post-treatment changes [37]. Recurrent tu-mours show restricted diffusion, whereas post-treatmentchanges have high signal intensity on apparent diffusion co-efficient (ADC) maps. Metastatic lesions on perfusion MRwill typically demonstrate increased relative cerebral bloodvolume (rCBV), while radiation necrosis usually shows de-creased rCBV [36].
18F-FDG PET/CT
Positron emission tomography (PET)/CT is a useful diagnos-tic modality in the event of equivocal findings on conventionalstaging techniques, especially in patients with locally ad-vanced or metastatic disease [1]. In the neoadjuvant setting,a decrease in maximum standardized uptake value (SUVmax)of 60 % from baseline has shown up to 96 % specificity inpredicting pathologic complete response (pCR) after just onecourse of chemotherapy (Fig. 7) [38]. This contributes impor-tant prognostic information, as patients with pCR have signif-icantly higher disease-free and overall survival rates than non-responders. PET/CT is also valuable for detecting metabolicchanges following treatment with antineoplastic agents. Priorto PET/CT, methods for monitoring therapeutic effectivenesswere limited to physical exam or conventional imaging, thusrelying on physical and morphological information. PET/CTis effective for monitoring physiological response after onetreatment, prior to pathologic confirmation at the time of sur-gery, and thus decisions regarding the continuation or modifi-cation of therapy can be made early in the treatment course[39]. The pooled sensitivity and specificity of FDG-PET/CTin predicting histopathologic response in primary breast can-cer is 81 and 79 %, respectively [40]. Similar to that of MRI,
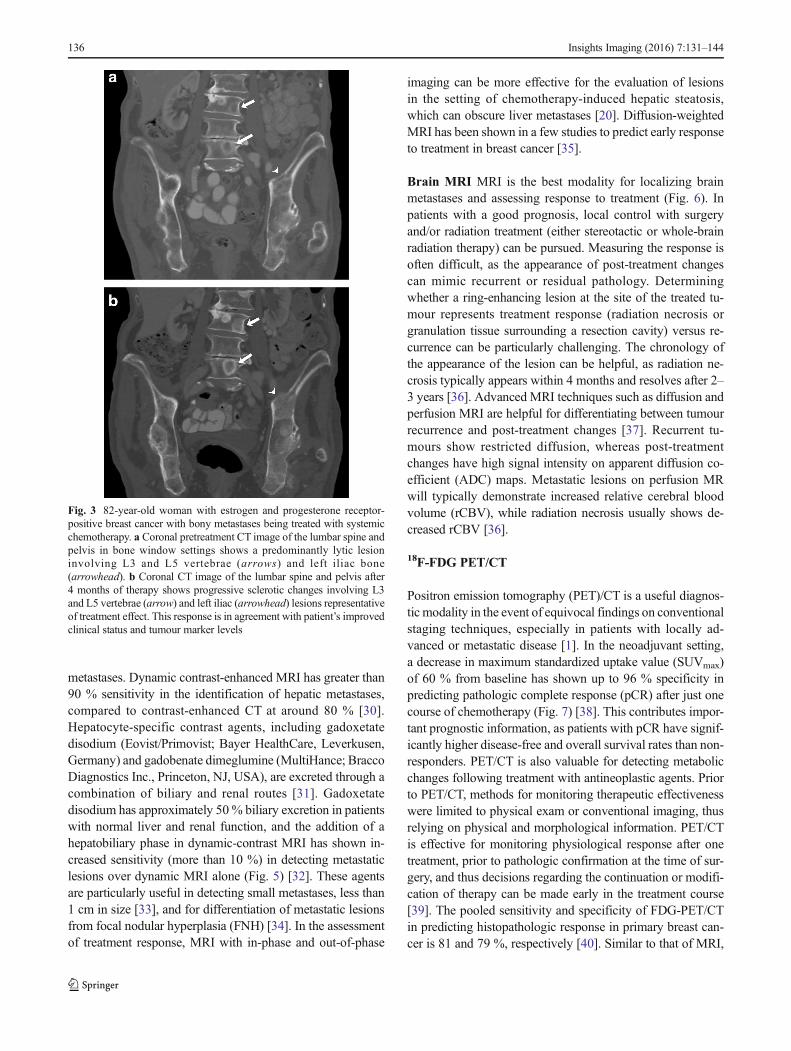
Fig. 3 82-year-old woman with estrogen and progesterone receptor-positive breast cancer with bony metastases being treated with systemicchemotherapy. a Coronal pretreatment CT image of the lumbar spine andpelvis in bone window settings shows a predominantly lytic lesioninvolving L3 and L5 vertebrae (arrows) and left iliac bone(arrowhead). b Coronal CT image of the lumbar spine and pelvis after4 months of therapy shows progressive sclerotic changes involving L3and L5 vertebrae (arrow) and left iliac (arrowhead) lesions representativeof treatment effect. This response is in agreement with patient’s improvedclinical status and tumour marker levels
136 Insights Imaging (2016) 7:131–144

the performance of FDG-PET/CT in predicting pathologiccomplete response is better in HER2-positive and triple-negative tumours than in the luminal subtype [40]. In themetastatic setting, the sensitivity and specificity of FDG-PET/CT is 93 and 82 %, respectively [41]. The degree ofreduction in FDG uptake in metastatic lesions after the firstcycle of chemotherapy has been shown in some studies todifferentiate responders from non-responders [41]. In evalua-tion of osseous metastasis, FDG-PET/CT can help in identi-fying viable metastases, as treated metastases become FDG-negative but remain osteoblastic on CT [41]. In cases of brainmetastasis, FDG-PET is useful for differentiating betweenpost-radiation necrosis and tumour recurrence [42]. One studyfound that dual-phase FDG-PET imaging of the brain wassuperior to the standard single-phase FDG-PET in differenti-ating recurrent metastasis from post-treatment necrosis [43].
99mTc methylene diphosphonate (MDP) bonescintigraphy
Bone is the most common site of breast cancer metastasis.Bone scintigraphy is the most widely used modality for de-tecting bone metastases, and demonstrates osteoblastic activ-ity as areas of increased radiotracer uptake. However, certaincharacteristic false-negative and false-positive findings onscintigraphy should be kept in mind in assessing treatmentresponse. Scintigraphy sometimes demonstrates an apparent
worsening of abnormalities, known as the Bflare phenomenon,^ characterized by increased activity in known lesions or newlesions during the first 3 months after treatment as a result ofbone repair (Fig. 8) [44]. This finding should not be confusedwith progression of disease, and should be followed up withanother bone scan in 4 to 6 months. A finding that persistsbeyond 6 months, however, is more likely indicative of dis-ease progression. The apparent worsening or new scleroticosseous lesions should be interpreted with caution, and shouldnot be considered new or progressive disease, particularly inthe setting of improving tumour markers and clinical statusand the absence of other bone progression. The concept ofincreased osteoblastic healing reaction was introduced as acriterion for treatment response by the M.D. Anderson CancerCenter in 2004 [45]. In the revised criteria, CT and MRI areincluded as imaging modalities for assessing treatment re-sponse in bony metastases. The appearance of peripheral scle-rosis around initial lytic lesions or sclerosis of previously un-detectable lesions on CTor radiographs is considered a partialresponse. The rapid regression of lesions on scintigraphy wasexcluded as a partial response, as this finding may representprogression of lytic bony lesions. Bone scintigraphy is notsensitive for lytic osseous metastases given the low amountor absence of osteoblastic activity in these lesions. 18F-FDGPET is more sensitive than scintigraphy in detecting lytic me-tastases and marrow involvement [46]. The recently proposedPERCIST (PET Response Criteria in Solid Tumours)
Fig. 4 36-year-old woman withinvasive lobular carcinoma in theright breast. a Axial contrast-enhanced T1-weighted MR imagebefore start of neoadjuvantchemotherapy shows diffuse skinthickening and edema involvingthe right breast, with multipleenhancing masses (arrowheads)and enlarged right axillary lymphnodes (arrow). b, c Correspondingcolor map and enhancementkinetic curve demonstrate intenseenhancement and washoutconsistent with malignancy.d Axial contrast-enhanced T1-weightedMR image after 4monthsof therapy shows intervalresolution of skin thickeningand breast masses, with markeddecrease in size of axillary lymphnodes (arrow). e, f Correspondingcolor map and enhancement curvedemonstrate nearly completeresolution of the breast massand axillary modes
Insights Imaging (2016) 7:131–144 137
guidelines involve the role of FDG PET in treatment response,with an emphasis on change in tumour metabolism after ther-apy over anatomically based criteria [47].
Complications associated with treatment: the roleof imaging
Cytotoxic agents
CT is also helpful in monitoring treatment-related complica-tions. Pulmonary toxicity is a common drug-related compli-cation seen with taxanes and methotrexate. CT findings in-clude pulmonary infiltrates presenting in early onset as bilat-eral reticular, ground-glass or consolidative opacities, pulmo-nary oedema, and pleural effusions, and as fibrosis in latedisease (Fig. 9) [48]. Pulmonary infiltrates, however, are anon-specific finding, and can also result from disease progres-sion and infection; thus clinical factors should also be takeninto consideration.
Neutropenic enterocolitis and typhlitis (neutropenic entero-colitis of the cecum) are the most common GI side effects ofchemotherapy, and are associated with several cytotoxic
breast cancer drugs including doxorubicin, docetaxel, pacli-taxel and platinum agents. CT findings include colonic wallthickening and oedema and/or necrosis, pericolonic fatstranding, ascites, pneumatosis intestinalis, and free air inthe setting of bowel necrosis and perforation. While mostfrequently seen in the right colon, any colonic or small bowelsegment can be involved. Because rapidly dividing GI muco-sal cells are also vulnerable to cytotoxic agents, GI ulceration,which may further lead to perforation, is another treatmentcomplication most commonly associated with doxorubicinand taxanes. Pneumatosis intestinalis may be observed withcyclophosphamide, doxorubicin, cisplatin and docetaxel [49].
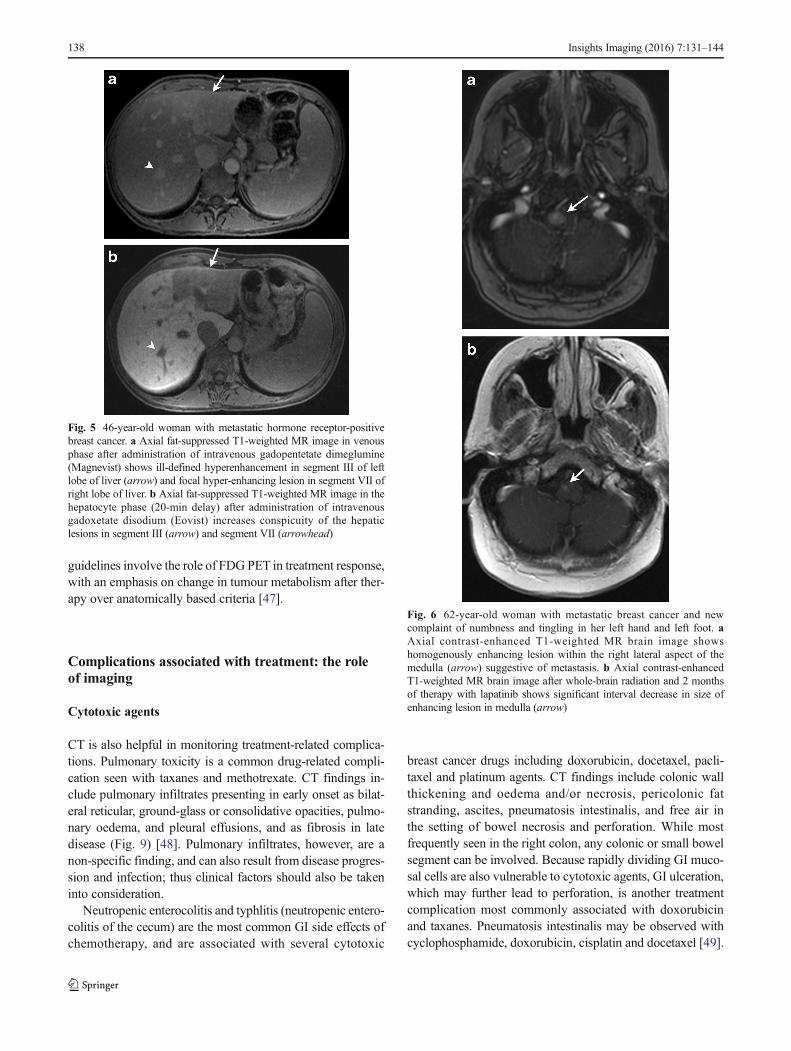
Fig. 5 46-year-old woman with metastatic hormone receptor-positivebreast cancer. a Axial fat-suppressed T1-weighted MR image in venousphase after administration of intravenous gadopentetate dimeglumine(Magnevist) shows ill-defined hyperenhancement in segment III of leftlobe of liver (arrow) and focal hyper-enhancing lesion in segment VII ofright lobe of liver. b Axial fat-suppressed T1-weighted MR image in thehepatocyte phase (20-min delay) after administration of intravenousgadoxetate disodium (Eovist) increases conspicuity of the hepaticlesions in segment III (arrow) and segment VII (arrowhead)
Fig. 6 62-year-old woman with metastatic breast cancer and newcomplaint of numbness and tingling in her left hand and left foot. aAxial contrast-enhanced T1-weighted MR brain image showshomogenously enhancing lesion within the right lateral aspect of themedulla (arrow) suggestive of metastasis. b Axial contrast-enhancedT1-weighted MR brain image after whole-brain radiation and 2 monthsof therapy with lapatinib shows significant interval decrease in size ofenhancing lesion in medulla (arrow)
138 Insights Imaging (2016) 7:131–144

Fig. 7 36-year-old woman withinvasive lobular carcinoma in theright breast (same patient as inFig. 4). a Coronal maximum-intensity projection (MIP) 18F-FDG PET image also performedprior to start of treatment showsmultiple FDG-avid nodules in theright breast, with right axillary,subpectoral, cervical, mediastinal,and bilateral hilarlymphadenopathy. Also note theFDG-avid focus in the sacrumsuggestive of osseous metastasis.b Coronal maximum-intensityprojection (MIP) 18F-FDG PETimage after 6 months of therapyshows significant decrease inFDG-avid lesions suggestive ofresponse to therapy
Fig. 8 61-year-old woman with breast cancer and osseous metastasesbeing treated with capecitabine. a Pretreatment bone scan showsmultifocal abnormal radiotracer uptake in calvarium, multiple thoracicand lumbar vertebrae, and bilateral iliac bones. Focal uptake in left 9thrib (arrowhead) corresponds to recent traumatic fracture. b Post-treatment bone scan after 2 months of therapy shows slight increase inthe intensity and extent of radiotracer uptake in the multiple knownmetastases, uptake in calvarium, multiple thoracic, and lumbar
vertebrae and bilateral iliac bones. Given the improvement in tumourmarkers, this finding was regarded as response to treatment with ascintigraphic flare phenomenon. Uptake in left 9th rib is decreased(arrowhead). c Post-treatment bone scan after 4 months of therapyshows interval decrease in the intensity and extent of radiotracer uptakein the multiple known metastases. Focal uptake in right 10th rib (arrow)corresponds to a new traumatic fracture
Insights Imaging (2016) 7:131–144 139

Fluid retention, likely due to capillary protein leakage, hasbeen seen in patients treated with docetaxel, and may manifestas peripheral oedema and as pleural and pericardial effusions[50]. Platinum-based agents carry an increased risk of throm-bus formation [51]. Hemorrhagic cystitis is a well-knowncomplication of cyclophosphamide, manifesting radiological-ly as diffuse thickening and nodularity of the bladder wallsecondary to urothelial toxicity. This complication usually oc-curs early in treatment and is preventable with hydration andconcurrent treatment with mesna, which neutralizes the toxicmetabolic products within the bladder [52].
Hormones
Patients receiving treatment with tamoxifen have an increasedprevalence of endometrial hyperplasia, endometrial polypsand endometrial carcinoma (Fig. 10). Transvaginal ultrasound(US) and hysterosonography are useful tools for endometrialassessment, which is especially helpful in women treated withtamoxifen. While the agonistic effects of tamoxifen on estro-gen receptors are beneficial in some tissues—for example, in
lowering serum cholesterol and protecting against bone lossand cardiovascular disease—its proliferative effects on theuterine endometrium increase the risk of endometrial cancer[53]. On transvaginal US, endometrial carcinomas are typical-ly diffusely or partially echogenic. As many patients treatedon tamoxifen have endometrial thickening and underlyingadenomyosis, poorly defined endometrial thickening is not aspecific sign. Hysterosonography may be of further help inidentifying an irregular, inhomogeneous mass or focal thick-ening in the endometrium [54]. Lack of distensibility of theendometrial cavity may also suggest carcinoma. MRI is usefulfor the characterization of endometrial abnormalities associat-ed with tamoxifen therapy [55].
Tamoxifen causes hypercoagulability, increasing the risk ofthromboembolic phenomena and catheter-related thrombosis(Fig. 8) [56].
Fig. 10 72-year-old woman with metastatic hormone receptor-positivebreast cancer being treated with tamoxifen. a Sagittal contrast-enhancedCT image of the pelvis shows irregular thickening of the endometriallining (arrow) suggestive of endometrial hyperplasia. b Coronalcontrast-enhanced CT image of the pelvis during routine restagingstudy shows hypodense filling defect (arrow) in descending branch ofright pulmonary artery suggestive of pulmonary embolism. The patienthad no complaints of chest pain
Fig. 9 69-year-old woman with metastatic hormone receptor-positive,HER2/neu-positive breast cancer being treated with paclitaxel. Axialcontrast-enhanced lung window CT image before (a) and after (b)treatment with paclitaxel shows interval appearance of patchy ground-glass opacities in upper lobes of lungs (arrow in b) suggestive of drug-associated pneumonitis. Also note the decreased size of left axillarylymph node (arrowheads in a and b) suggestive of treatment response
140 Insights Imaging (2016) 7:131–144
Fatty liver is seen in up to 30 % of patients treated withtamoxifen (Fig. 11), and can be present as early as 3 monthsafter initiation of treatment and can persist for more than4 years after discontinuation [57]. Risk factors for hepaticchanges associated with tamoxifen include preexisting condi-tions such as diabetes, obesity and hepatic steatosis. Fatty livermay rarely progress to steatohepatitis and cirrhosis. On ultra-sound, hepatic steatosis presents as an echogenic liver, whileon CT, the liver appears hypodense in comparison to thespleen (Fig. 9). On CT, fatty infiltration of the liver may ob-scure the presence of hypodense metastases. MR is helpful, asin-phase and out-of-phase imaging will demonstrate intracel-lular fatty deposition with signal dropout on out-of-phase se-quences [58].
In postmenopausal women, the primary source ofoestrogen is through conversion from adrenal androgen byaromatase. AIs prevent the conversion of androgens to estro-gens, thereby causing a relatively rapid reduction in circulat-ing oestrogen and an acceleration of bone loss at more thantwice the rate of physiologic postmenopausal loss [59]. Reg-ular bone marrow density monitoring is thus highly recom-mended. Bisphosphonates are the first line of therapy for theprevention and treatment of aromatase inhibitor-associated
bone loss, as women on AIs are at increased risk of fractures[59].
Molecular-targeted therapies
MTTs have class-specific and drug-specific toxicities. m-TORinhibitors such as everolimus are associated with drug-induced pneumonitis manifesting radiologically as ground-glass and consolidative opacities [48]. Radiation recall pneu-monitis refers to an inflammatory reaction in the lungs withinthe previously treated radiation field after the start of chemo-therapy, and can be seen occasionally with HER2 inhibitors(Fig. 12) [60]. Trastuzumab has been associated withcardiotoxicity, especially when administered with or afterdoxorubicin. The incidence of cardiac dysfunction in patientsreceiving trastuzumab ranges from 2 to 28 % [61]. The mostcommon manifestation of trastuzumab cardiotoxicity is anasymptomatic decrease in left ventricular ejection fraction(LVEF) [62]. In contrast to doxorubicin-associatedcardiotoxicity, trastuzumab-induced cardiotoxicity is not relat-ed to cumulative dose and is often reversible with discontinu-ation of treatment [63]. Multiple-gated acquisition (MUGA)scan and echocardiogram are used for determination of LVEF
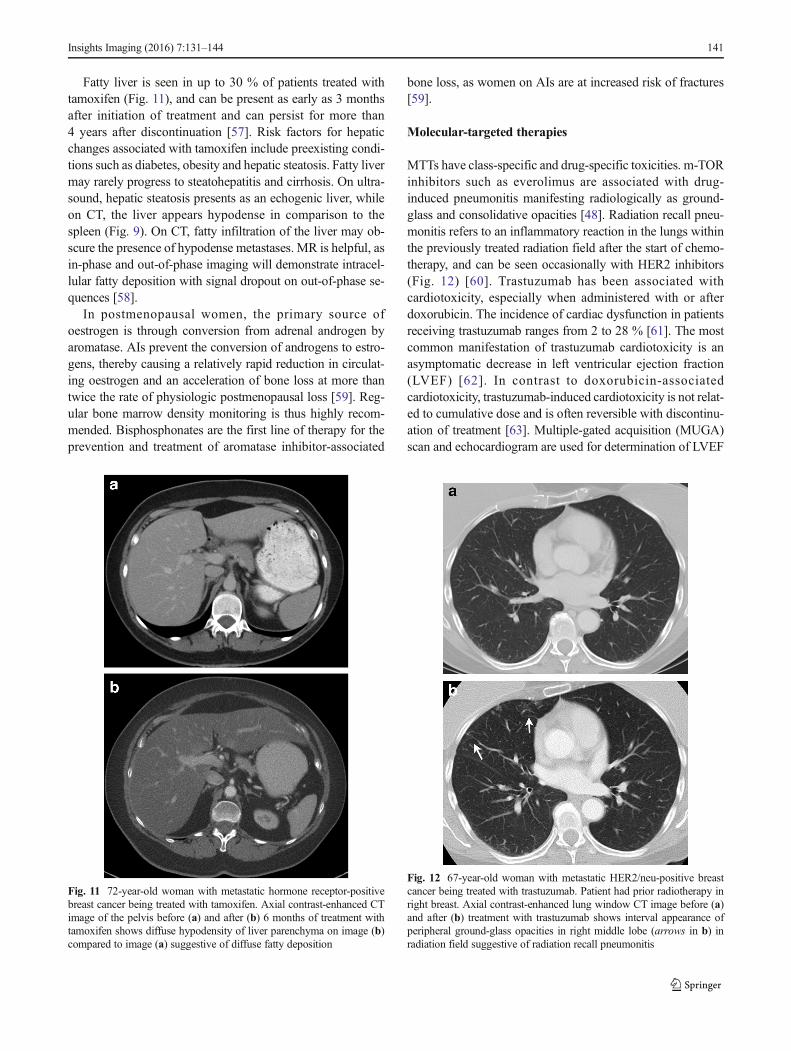
Fig. 12 67-year-old woman with metastatic HER2/neu-positive breastcancer being treated with trastuzumab. Patient had prior radiotherapy inright breast. Axial contrast-enhanced lung window CT image before (a)and after (b) treatment with trastuzumab shows interval appearance ofperipheral ground-glass opacities in right middle lobe (arrows in b) inradiation field suggestive of radiation recall pneumonitis
Fig. 11 72-year-old woman with metastatic hormone receptor-positivebreast cancer being treated with tamoxifen. Axial contrast-enhanced CTimage of the pelvis before (a) and after (b) 6 months of treatment withtamoxifen shows diffuse hypodensity of liver parenchyma on image (b)compared to image (a) suggestive of diffuse fatty deposition
Insights Imaging (2016) 7:131–144 141

in breast cancer patients before and after chemotherapy [64].The biochemical marker troponin I is also useful for monitor-ing cardiotoxicity as well as for identifying patients who are atrisk for cardiotoxicity and less likely to recover [65]. Treat-ment discontinuation is recommended in patients with a great-er than 16 % drop in LVEF compared to baseline or a declinein LVEF to below the lower limit of normal, and in patientswho develop symptomatic cardiac failure [66]. Adverseeffects of lapatinib include fatigue, nausea, rash, diarrhoea,neutropenia, hepatotoxicity, interstitial lung disease andpneumonitis [67].
Conclusions
Systemic treatment for breast cancer includes a combinationof cytotoxic, hormonal and molecular-targeted therapies invarious stages of treatment. The assessment of response tothese agents on restaging scans has significant a impact onthe patient’s treatment course. Imaging modalities such asCT, MRI, FDG-PET/CT and bone scintigraphy each have adistinct role in monitoring response to various treatment strat-egies. Familiarity with the response patterns on imaging andtoxicities associated with these therapies can enhance the keyrole played by radiologists in patient management.
Compliance with ethical standards
Disclosures The investigator A.B.S was awarded a Radiological Soci-ety of North America (RSNA) research grant beginning July, 2014. Theremaining authors have nothing to disclosure.
Open Access This article is distributed under the terms of the CreativeCommons At t r ibut ion 4 .0 In te rna t ional License (h t tp : / /creativecommons.org/licenses/by/4.0/), which permits unrestricted use,distribution, and reproduction in any medium, provided you give appro-priate credit to the original author(s) and the source, provide a link to theCreative Commons license, and indicate if changes were made.
References
1. (2014) National Clinical Practice Guidelines in Oncology (NCCNguidelines): Breast cancer-version 3.2014. Available via http://www.nccn.org/professionals/physician_gls/f_guidelines.asp#site
2. Chikarmane SA, Tirumani SH, Howard SA, Jagannathan JP, DiPiroPJ (2015) Metastatic patterns of breast cancer subtypes: what radi-ologists should know in the era of personalized cancer medicine.Clin Radiol 70:1–10
3. Jordan VC (2006) Tamoxifen (ici46,474) as a targeted therapy totreat and prevent breast cancer. Br J Pharmacol 147(Suppl 1):S269–S276
4. Rugo HS (2008) The breast cancer continuum in hormone-receptor-positive breast cancer in postmenopausal women: evolv-ing management options focusing on aromatase inhibitors. AnnOncol 19:16–27
5. Semiglazov VF, Semiglazov VV, Dashyan GA et al (2007) Phase 2randomized trial of primary endocrine therapy versus chemothera-py in postmenopausal patients with estrogen receptor-positivebreast cancer. Cancer 110:244–254
6. Cataliotti L, Buzdar AU, Noguchi S et al (2006) Comparison ofanastrozole versus tamoxifen as preoperative therapy in postmeno-pausal women with hormone receptor-positive breast cancer: thepre-operative BArimidex^ compared to Tamoxifen (PROACT) tri-al. Cancer 106:2095–2103
7. Croxtall JD, McKeage K (2011) Fulvestrant: a review of its use inthe management of hormone receptor-positive metastatic breastcancer in postmenopausal women. Drugs 71:363–380
8. Joensuu H, Bono P, Kataja V et al (2009) Fluorouracil, epirubicin,and cyclophosphamide with either docetaxel or vinorelbine, with orwithout trastuzumab, as adjuvant treatments of breast cancer: finalresults of the finher trial. J Clin Oncol 27:5685–5692
9. Spielmann M, Roche H, Delozier T et al (2009) Trastuzumab forpatients with axillary-node-positive breast cancer: results of theFNCLCC-PACS 04 trial. J Clin Oncol 27:6129–6134
10. Kelly CM, Buzdar AU (2013) Using multiple targeted therapies inoncology: considerations for use, and progress to date in breastcancer. Drugs 73:505–515
11. Abdel-Razeq H, Marei L (2011) Current neoadjuvant treatmentoptions for HER2-positive breast cancer. Biologics 5:87–94
12. Lin NU, Dieras V, Paul D et al (2009) Multicenter phase ii study oflapatinib in patients with brain metastases from HER2-positivebreast cancer. Clin Cancer Res 15:1452–1459
13. Swain SM,Kim SB, Cortes J et al (2013) Pertuzumab, trastuzumab,and docetaxel for HER2-positivemetastatic breast cancer (cleopatrastudy): overall survival results from a randomised, double-blind,placebo-controlled, phase 3 study. Lancet Oncol 14:461–471
14. Zimmerman P, Lu DS, Yang LY, Chen S, Sayre J, Kadell B (2000)Hepatic metastases from breast carcinoma: comparison ofnoncontrast, arterial-dominant, and portal-dominant phase spiralCT. J Comput Assist Tomogr 24:197–203
15. Sica GT, Ji H, Ros PR (2000) CT and MR imaging of hepaticmetastases. AJR Am J Roentgenol 174:691–698
16. Therasse P, Arbuck SG, Eisenhauer EA et al (2000) New guidelinesto evaluate the response to treatment in solid tumors. HER2eanOrganization for Research and Treatment of Cancer, NationalCancer Institute of the United States, National Cancer Institute ofCanada. J Natl Cancer Inst 92:205–216
17. Eisenhauer EA, Therasse P, Bogaerts J et al (2009) New responseevaluation criteria in solid tumours: revised RECIST guideline (ver-sion 1.1). Eur J Cancer 45:228–247
18. He H, Cai C, Charnsangavej C et al (2015) Contrast-enhancedcomputed tomography evaluation of hepatic metastases in breastcancer patients before and after cytotoxic chemotherapy or targetedtherapy. Can Assoc Radiol J. doi:10.1016/j.carj.2015.03.005
19. Lee SL, Chang ED, Na SJ et al (2014) Pseudocirrhosis of breastcancer metastases to the liver treated by chemotherapy. Cancer ResTreat 46:98–103
20. Shinagare AB, Jagannathan JP, Krajewski KM, Ramaiya NH(2013) Liver metastases in the era of molecular targeted therapy:new faces of treatment response. AJR Am J Roentgenol 201:W15–W28
21. Tateishi U, Gamez C, Dawood S, Yeung HW, Cristofanilli M,Macapinlac HA (2008) Bone metastases in patients with metastaticbreast cancer: morphologic and metabolic monitoring of responseto systemic therapy with integrated PET/CT. Radiology 247:189–196
22. Stattaus J, Hahn S, Gauler T et al (2009) Osteoblastic response as ahealing reaction to chemotherapy mimicking progressive disease inpatients with small cell lung cancer. Eur Radiol 19:193–200
23. Jung JI, Kim HH, Park SH et al (2004) Thoracic manifestations ofbreast cancer and its therapy. Radiographics 24:1269–1285
142 Insights Imaging (2016) 7:131–144
24. Tanaka K, Shimizu K, Ohtaki Yet al (2013) Diagnosis and surgicalresection of solitary pulmonary nodules in patients with breast can-cer. Mol Clin Oncol 1:117–123
25. Nishino M, Jagannathan JP, Ramaiya NH, Van den Abbeele AD(2010) Revised recist guideline version 1.1: what oncologists wantto know and what radiologists need to know. AJRAm J Roentgenol195:281–289
26. Weatherall PT, Evans GF, Metzger GJ, Saborrian MH, Leitch AM(2001) MRI vs. histologic measurement of breast cancer followingchemotherapy: comparison with x-ray mammography and palpa-tion. J Magn Reson Imaging 13:868–875
27. Ko ES, Han BK, Kim RB et al (2013) Analysis of factors thatinfluence the accuracy of magnetic resonance imaging forpredicting response after neoadjuvant chemotherapy in locally ad-vanced breast cancer. Ann Surg Oncol 20:2562–2568
28. McGuire KP, Toro-Burguete J, Dang H et al (2011) MRI stagingafter neoadjuvant chemotherapy for breast cancer: does tumor biol-ogy affect accuracy? Ann Surg Oncol 18:3149–3154
29. Lobbes M, Prevos R, Smidt M (2012) Response monitoring ofbreast cancer patients receiving neoadjuvant chemotherapy usingbreast MRI – a review of current knowledge. J Cancer Ther Res 1:34
30. Bottcher J, Hansch A, Pfeil A et al (2013) Detection and classifica-tion of different liver lesions: comparison of gd-eob-dtpa-enhancedMRI versus multiphasic spiral CT in a clinical single centre inves-tigation. Eur J Radiol 82:1860–1869
31. Guglielmo FF, Mitchell DG, Gupta S (2014) Gadolinium contrastagent selection and optimal use for body MR imaging. Radiol ClinN Am 52:637–656
32. Lee KH, Lee JM, Park JH et al (2013) MR imaging in patients withsuspected liver metastases: value of liver-specific contrast agentgadoxetic acid. Korean J Radiol 14:894–904
33. Shimada K, Isoda H, Hirokawa Y, Arizono S, Shibata T, Togashi K(2010) Comparison of gadolinium-eob-dtpa-enhanced anddiffusion-weighted liver MRI for detection of small hepatic metas-tases. Eur Radiol 20:2690–2698
34. Ringe KI, Husarik DB, Sirlin CB, Merkle EM (2010) Gadoxetatedisodium-enhanced MRI of the liver: part 1, protocol optimizationand lesion appearance in the noncirrhotic liver. AJR Am JRoentgenol 195:13–28
35. Thoeny HC, Ross BD (2010) Predicting and monitoring cancertreatment response with diffusion-weighted MRI. J Magn ResonImaging 32:2–16
36. Shah R, Vattoth S, Jacob R et al (2012) Radiation necrosis in thebrain: imaging features and differentiation from tumor recurrence.Radiographics 32:1343–1359
37. Al-Okaili RN, Krejza J, Wang S, Woo JH, Melhem ER (2006)Advanced MR imaging techniques in the diagnosis of intraaxialbrain tumors in adults. Radiographics 26(Suppl 1):S173–S189
38. Rousseau C, Devillers A, Sagan C et al (2006) Monitoring of earlyresponse to neoadjuvant chemotherapy in stage ii and iii breastcancer by [18f]fluorodeoxyglucose positron emission tomography.J Clin Oncol 24:5366–5372
39. Berriolo-Riedinger A, Touzery C, Riedinger JM et al (2007)[18F]FDG-PET predicts complete pathological response of breastcancer to neoadjuvant chemotherapy. Eur J Nucl MedMol Imaging34:1915–1924
40. Humbert O, Cochet A, Coudert B et al (2015) Role of positronemission tomography for the monitoring of response to therapy inbreast cancer. Oncologist 20:94–104
41. Avril N, Sassen S, Roylance R (2009) Response to therapy in breastcancer. J Nucl Med 50(Suppl 1):55S–63S
42. Chao ST, Suh JH, Raja S, Lee SY, Barnett G (2001) The sensitivityand specificity of FDG PET in distinguishing recurrent brain tumorfrom radionecrosis in patients treated with stereotactic radiosurgery.Int J Cancer 96:191–197
43. Horky LL, Hsiao EM, Weiss SE, Drappatz J, Gerbaudo VH (2011)Dual phase FDG-PET imaging of brain metastases provides supe-rior assessment of recurrence versus post-treatment necrosis. JNeurooncol 103:137–146
44. Lecouvet FE, Talbot JN, Messiou C et al (2014) Monitoring theresponse of bone metastases to treatment with magnetic resonanceimaging and nuclear medicine techniques: a review and positionstatement by the HER2ean Organisation for Research andTreatment of Cancer Imaging Group. Eur J Cancer 50:2519–2531
45. Hamaoka T, Madewell JE, Podoloff DA, Hortobagyi GN, Ueno NT(2004) Bone imaging in metastatic breast cancer. J Clin Oncol 22:2942–2953
46. Malhotra P, Berman CG (2002) Evaluation of bone metastases inlung cancer. Improved sensitivity and specificity of PET over bonescanning. Cancer Control 9(254):259–260
47. Wahl RL, Jacene H, Kasamon Y, Lodge MA (2009) From RECISTto PERCIST: evolving considerations for PET response criteria insolid tumors. J Nucl Med 50(Suppl 1):122S–150S
48. Torrisi JM, Schwartz LH, Gollub MJ, Ginsberg MS, Bosl GJ,Hricak H (2011) CT findings of chemotherapy-induced toxicity:what radiologists need to know about the clinical and radiologicmanifestations of chemotherapy toxicity. Radiology 258:41–56
49. Cronin CG, O’Connor M, Lohan DG et al (2009) Imaging of thegastrointestinal complications of systemic chemotherapy. ClinRadiol 64:724–733
50. Park SI, Jeon WH, Jeung HJ, Kim GC, Kim DK, Sim YJ (2014)Clinical features of docetaxel chemotherapy-related lymphedema.Lymphat Res Biol 12:197–202
51. Shahab N, Haider S, Doll DC (2006) Vascular toxicity of antineo-plastic agents. Semin Oncol 33:121–138
52. Lawson M, Vasilaras A, De Vries A, Mactaggart P, Nicol D (2008)Urological implications of cyclophosphamide and ifosfamide.Scand J Urol Nephrol 42:309–317
53. Swerdlow AJ, Jones ME (2005) Tamoxifen treatment for breastcancer and risk of endometrial cancer: a case–control study. J NatlCancer Inst 97:375–384
54. Fong K, Causer P, Atri M, Lytwyn A, Kung R (2003) TransvaginalUS and hysterosonography in postmenopausal women with breastcancer receiving tamoxifen: correlation with hysteroscopy andpathologic study. Radiographics 23:137–150, discussion 151–135
55. Ochi J, Hayakawa K, Moriguchi Y, Urata Y, Yamamoto A, KawaiK (2010) Uterine changes during tamoxifen, toremifene, and othertherapy for breast cancer: evaluation with magnetic resonance im-aging. Jpn J Radiol 28:430–436
56. Erman M, Abali H, Oran B et al (2004) Tamoxifen-induced tissuefactor pathway inhibitor reduction: a clue for an acquiredthrombophilic state? Ann Oncol 15:1622–1626
57. Rodriguez-Frias EA, Lee WM (2007) Cancer chemotherapy II:atypical hepatic injuries. Clin Liver Dis 11:663–676, viii
58. Pilleul F, Chave G, Dumortier J, Scoazec JY, Valette PJ (2005) Fattyinfiltration of the liver. Detection and grading using dual T1 gradi-ent echo sequences on clinical MR system. Gastroenterol Clin Biol29:1143–1147
59. Hadji P, Aapro MS, Body JJ et al (2011) Management of aromataseinhibitor-associated bone loss in postmenopausal women withbreast cancer: practical guidance for prevention and treatment.Ann Oncol 22:2546–2555
60. Lee HE, Jeong NJ, Lee Y et al (2014) Radiation recall dermatitisand pneumonitis induced by trastuzumab (herceptin®). Int JDermatol 53:e159–e160
61. Yeh ET, Bickford CL (2009) Cardiovascular complications of can-cer therapy: incidence, pathogenesis, diagnosis, and management. JAm Coll Cardiol 53:2231–2247
62. Huszno J, LesD, Sarzyczny-Slota D, Nowara E (2013) Cardiac sideeffects of trastuzumab in breast cancer patients—single center ex-periences. Contemp Oncol (Pozn) 17:190–195
Insights Imaging (2016) 7:131–144 143

63. Guarneri V, Lenihan DJ, Valero V et al (2006) Long-term cardiactolerability of trastuzumab in metastatic breast cancer: the M.D.Anderson Cancer Center experience. J Clin Oncol 24:4107–4115
64. Perez EA, Rodeheffer R (2004) Clinical cardiac tolerability oftrastuzumab. J Clin Oncol 22:322–329
65. Cardinale D, Colombo A, Torrisi R et al (2010) Trastuzumab-induced cardiotoxicity: clinical and prognostic implications of tro-ponin I evaluation. J Clin Oncol 28:3910–3916
66. Romond EH, Perez EA, Bryant J et al (2005) Trastuzumab plusadjuvant chemotherapy for operable HER2-positive breast cancer.N Engl J Med 353:1673–1684
67. de Azambuja E, Holmes AP, Piccart-Gebhart M et al (2014)Lapatinib with trastuzumab for HER2-positive early breast cancer(NeoALTTO): survival outcomes of a randomised, open-label,multicentre, phase 3 trial and their association with pathologicalcomplete response. Lancet Oncol 15:1137–1146
144 Insights Imaging (2016) 7:131–144