ozonoterapia.ozotec.ptozonoterapia.ozotec.pt/wp-content/uploads/2016/12/... · systematic reviews...
TRANSCRIPT
Systematic reviews of wound caremanagement: (5) beds; (6) compression;(7) laser therapy, therapeutic ultrasound,electrotherapy and electromagnetictherapy
N CullumEA NelsonK FlemmingT Sheldon
HTAHealth Technology Assessment NHS R&D HTA Programme
Health Technology Assessment 2001; Vol. 5: No. 9
Review
How to obtain copies of this and other HTA Programme reports.An electronic version of this publication, in Adobe Acrobat format, is available for downloading free ofcharge for personal use from the HTA website (http://www.ncchta.org). A fully searchable CD-ROM isalso available (see below).
Printed copies of HTA monographs cost £20 each (post and packing free in the UK) to both public andprivate sector purchasers from our Despatch Agents, York Publishing Services.
Non-UK purchasers will have to pay a small fee for post and packing. For European countries the cost is£2 per monograph and for the rest of the world £3 per monograph.
You can order HTA monographs from our Despatch Agents, York Publishing Services by:
– fax (with credit card or official purchase order) – post (with credit card or official purchase order or cheque)– phone during office hours (credit card only).
Additionally the HTA website allows you either to pay securely by credit card or to print out yourorder and then post or fax it.
Contact details are as follows:York Publishing Services Email: [email protected] Box 642 Tel: 0870 1616662YORK YO31 7WX Fax: 0870 1616663UK Fax from outside the UK: +44 1904 430868
NHS and public libraries can subscribe at a very reduced cost of £100 for each volume (normallycomprising 30–40 titles). The commercial subscription rate is £300 per volume. Please contact YorkPublishing Services at the address above. Subscriptions can only be purchased for the current orforthcoming volume.
Payment methods
Paying by chequeIf you pay by cheque, the cheque must be in pounds sterling, made payable to York PublishingDistribution and drawn on a bank with a UK address.
Paying by credit cardThe following cards are accepted by phone, fax, post or via the website ordering pages: Delta, Eurocard,Mastercard, Solo, Switch and Visa. We advise against sending credit card details in a plain email.
Paying by official purchase orderYou can post or fax these, but they must be from public bodies (i.e. NHS or universities) within the UK.We cannot at present accept purchase orders from commercial companies or from outside the UK.
How do I get a copy of HTA on CD?
Please use the form on the HTA website (www.ncchta.org/htacd.htm). Or contact York PublishingServices (see contact details above) by email, post, fax or phone. HTA on CD is currently free of chargeworldwide.
The website also provides information about the HTA Programme and lists the membership of the variouscommittees.
HTA
Systematic reviews of wound caremanagement: (5) beds; (6) compression;(7) laser therapy, therapeutic ultrasound,electrotherapy and electromagnetictherapy
N Cullum*
EA NelsonK FlemmingT Sheldon
Department of Health Studies, University of York, UK
* Corresponding author
Competing interests: N Cullum has: received funds from the NHS R&D Programmeto undertake primary research in wound care; received sponsorship of trial-relatededucational meetings from Huntleigh Healthcare and Beiersdorf Ltd. EA Nelson has:conducted one of the trials reviewed; been reimbursed for attending symposia by Smithand Nephew Ltd, ConvaTec and Huntleigh Healthcare
Published May 2001
This report should be referenced as follows:
Cullum N, Nelson EA, Flemming K, Sheldon T. Systematic reviews of wound caremanagement: (5) beds; (6) compression; (7) laser therapy, therapeutic ultrasound,electrotherapy and electromagnetic therapy. Health Technol Assess 2001;5(9).
Health Technology Assessment is indexed in Index Medicus/MEDLINE and Excerpta Medica/EMBASE. Copies of the Executive Summaries are available from the NCCHTA website(see opposite).
NHS R&D HTA Programme
The NHS R&D Health Technology Assessment (HTA) Programme was set up in 1993 to ensurethat high-quality research information on the costs, effectiveness and broader impact of health
technologies is produced in the most efficient way for those who use, manage and provide carein the NHS.
Initially, six HTA panels (pharmaceuticals, acute sector, primary and community care, diagnosticsand imaging, population screening, methodology) helped to set the research priorities for the HTAProgramme. However, during the past few years there have been a number of changes in and aroundNHS R&D, such as the establishment of the National Institute for Clinical Excellence (NICE) andthe creation of three new research programmes: Service Delivery and Organisation (SDO); New andEmerging Applications of Technology (NEAT); and the Methodology Programme.
This has meant that the HTA panels can now focus more explicitly on health technologies(‘health technologies’ are broadly defined to include all interventions used to promote health,prevent and treat disease, and improve rehabilitation and long-term care) rather than settingsof care. Therefore the panel structure has been redefined and replaced by three new panels:Pharmaceuticals; Therapeutic Procedures (including devices and operations); and DiagnosticTechnologies and Screening.
The HTA Programme will continue to commission both primary and secondary research. The HTACommissioning Board, supported by the National Coordinating Centre for Health TechnologyAssessment (NCCHTA), will consider and advise the Programme Director on the best researchprojects to pursue in order to address the research priorities identified by the three HTA panels.
The research reported in this monograph was funded as project number 93/29/01.
The views expressed in this publication are those of the authors and not necessarily those of theHTA Programme or the Department of Health. The editors wish to emphasise that funding andpublication of this research by the NHS should not be taken as implicit support for anyrecommendations made by the authors.
HTA Programme Director: Professor Kent WoodsSeries Editors: Professor Andrew Stevens, Dr Ken Stein, Professor John Gabbay
and Dr Ruairidh MilneMonograph Editorial Manager: Melanie Corris
The editors and publisher have tried to ensure the accuracy of this report but do not accept liabilityfor damages or losses arising from material published in this report. They would like to thank thereferees for their constructive comments on the draft document.
ISSN 1366-5278
© Queen’s Printer and Controller of HMSO 2001
This monograph may be freely reproduced for the purposes of private research and study and may be included in professional journalsprovided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising.
Applications for commercial reproduction should be addressed to HMSO, The Copyright Unit, St Clements House, 2–16 Colegate,Norwich, NR3 1BQ.
Published by Core Research, Alton, on behalf of the NCCHTA.Printed on acid-free paper in the UK by The Basingstoke Press, Basingstoke. G
Criteria for inclusion in the HTA monograph seriesReports are published in the HTA monograph series if (1) they have resulted from workcommissioned for the HTA Programme, and (2) they are of a sufficiently high scientific quality asassessed by the referees and editors.
Reviews in Health Technology Assessment are termed ‘systematic’ when the account of the search,appraisal and synthesis methods (to minimise biases and random errors) would, in theory, permitthe replication of the review by others.
Overview of Parts 1 to 7 .................................. i
Executive summary to Parts 5 to 7 ............... iii
Part 5: pressure-relieving beds,mattresses and cushions for theprevention and treatment ofpressure sores .......................................... 1
Contents to Part 5 ............................................ 3
List of abbreviations ......................................... 5
Executive summary to Part 5 ......................... 7
1 Introduction .................................................. 9Identifying people at risk .............................. 9Types of pressure-relieving intervention ..... 9Aims ................................................................ 10
2 Methods ......................................................... 11Search strategy ............................................... 11Inclusion and exclusion criteria ................... 11Data extraction .............................................. 13Methodological quality .................................. 13Data synthesis ................................................. 13
3 Results ............................................................ 15Studies included in the review ...................... 15Studies excluded from the review ................ 16Prevention of pressure sores ......................... 16Treatment of pressure sores ......................... 21Summary ......................................................... 22
4 Discussion ...................................................... 23
5 Conclusions ................................................... 25Implications for practice ............................... 25Implications for research .............................. 25
Acknowledgements ..................................... 27
References ..................................................... 29
Appendix 1 Databases searched andsearch strategies ............................................. 33
Appendix 2 Advisory panel ....................... 37
Appendix 3 Summary of includedstudies ............................................................. 39
Appendix 4 Quality assessment ofincluded studies ............................................. 71
Appendix 5 Comparisons undertaken inthe included studies ...................................... 75
Part 6: compression for theprevention and treatment ofvenous leg ulcers ................................... 79
Contents to Part 6 ............................................ 81
List of abbreviations ......................................... 83
Executive summary to Part 6 ......................... 85
1 Introduction .................................................. 87Aims ................................................................ 88
2 Methods ......................................................... 89Search strategy ............................................... 89Inclusion and exclusion criteria ................... 89Data extraction .............................................. 90Methodological quality .................................. 90Data synthesis ................................................. 90
3 Results ............................................................ 91Studies included in the review ...................... 91Studies excluded from the review ................ 91Methodological quality of includedstudies ............................................................. 91Presentation of results ................................... 92Application of compression bandages orstockings to prevent breakdown of legs atrisk of venous ulceration ............................... 92Application of compression bandages orstockings to aid venous ulcer healing .......... 92Clinical effectiveness of compressionbandage and stocking systems ...................... 93
Health Technology Assessment 2001; Vol. 5: No. 9
Contents
Cost-effectiveness of compression bandageand stocking systems ...................................... 94
4 Discussion ...................................................... 101
5 Conclusions ................................................... 103Implications for practice ............................... 103Implications for research .............................. 103Methodological recommendations .............. 103Priority research questions ............................ 104
Acknowledgements ..................................... 105
References ..................................................... 107
Appendix 1 Databases searched andsearch strategies ............................................. 111
Appendix 2 Advisory panel ....................... 115
Appendix 3 Summary of includedstudies ............................................................. 117
Appendix 4 Quality assessment ofincluded studies ............................................. 133
Part 7: low-level laser therapy,therapeutic ultrasound,electrotherapy andelectromagnetic therapyfor the treatment of chronicwounds ........................................................... 137
Contents to Part 7 ............................................ 139
List of abbreviations ......................................... 141
Executive summary to Part 7 ......................... 143
1 Introduction .................................................. 145Types of wound .............................................. 145The role of physical therapies in woundhealing ............................................................ 146Aims and objectives ....................................... 147
2 Methods ......................................................... 149Search strategy ............................................... 149Inclusion criteria ............................................ 149Data extraction .............................................. 149Methodological quality .................................. 150Data synthesis ................................................. 150
3 Results ............................................................ 151Quality of included studies ........................... 151Studies excluded from the review ................ 151Low-level laser therapy .................................. 151Therapeutic ultrasound ................................ 152Electrotherapy ................................................ 155Electromagnetic therapy ............................... 159
4 Discussion ...................................................... 161Low-level laser therapy .................................. 161Therapeutic ultrasound ................................ 161Electrotherapy ................................................ 161Electromagnetic therapy ............................... 161Secondary outcome measures ...................... 162
5 Conclusions ................................................... 163Implications for clinical practice .................. 163Implications for future research ................... 163
Acknowledgements ..................................... 165
References ..................................................... 167
Appendix 1 Databases searched andsearch strategies ............................................. 171
Appendix 2 Advisory panel ....................... 175
Appendix 3 Summary of includedstudies ............................................................. 177
Appendix 4 Quality assessment ofincluded studies ............................................. 207
Health Technology Assessment reportspublished to date ......................................... 213
Health Technology AssessmentProgramme ................................................... 219
Contents
T his publication marks the completion of a series ofseven systematic reviews on various aspects of chronic
wound management. Chronic wounds are typicallydefined as those that take more than 6 weeks to heal, andthe majority are leg and foot ulcers, pressure sores andsurgical wounds that break down and/or become infected.Management of chronic wounds usually involves treatingthe underlying cause where possible, for example byreducing pressure and managing the local wound envi-ronment, typically with dressings.
We selected the topics for the seven reviews with referenceto the research available, the views of an expert panel,variation in practice and costs.
We searched 19 electronic databases, several wound carejournals, conference proceedings and bibliographies oftrials retrieved by hand. Experts, manufacturers andcontent experts were asked for additional trials.
Studies were included if they were randomised controlledtrials (RCTs), published or unpublished, that providedobjective outcomes of healing (treatment studies) or inci-dence (prevention studies).
Results
• Thirty-five RCTs of debriding agents were found.There is insufficient evidence to conclude whetherdebridement increases healing or to recommend onedebriding agent over another.
• Ninety-three RCTs of dressings or topical agents wereincluded. There is weak evidence that hydrocolloidsincrease healing of pressure sores compared tomoistened gauze. There is insufficient evidence torecommend any particular agent or dressing for legulcers or chronic surgical wounds.
• From 30 trials we concluded that there is no robustevidence for the use of antimicrobial agents in chronicwounds.
• From 39 RCTs in diabetic foot ulcers we concludedthat there is some evidence that a foot healthprogramme reduces amputation rates and that growthfactors and off-loading increase healing rates.
• Forty-five RCTs of beds, mattresses or cushions forpressure sore prevention or treatment were found. Foamalternatives to standard hospital mattresses reduce theincidence of pressure sores, as can pressure-relievingoverlays on the operating table. One study suggeststhat air-fluidised therapy may increase pressure sorehealing rates.
• From 24 RCTs we concluded that compression ismore effective in healing venous leg ulcers than nocompression, and multilayered high compression ismore effective than single-layer compression. High-compression hosiery was more effective than moderatecompression in preventing ulcer recurrence.
• From 31 RCTs we concluded that there is insufficientreliable evidence on the contribution of laser therapy,therapeutic ultrasound, electrotherapy and electromag-netic therapy to chronic wound healing.
Discussion
This series of reviews has drawn on the availableevidence. There are a number of important areas where notrials have been identified (e.g. the impact of debridementon wound healing, the use of antibiotics for diabetic footulcers).
Studies were generally small and of poor methodologicalquality. Evaluations of the cost-effectiveness of interven-tions were rare. In addition, few studies assessed theimpact of the intervention on patients’ quality of life orrecorded adverse effects of interventions.
Further high-quality trials are required in order to assessthe impact of both new and established wound careinterventions.
Health Technology Assessment 2001; Vol. 5: No. 9
i
Overview of Parts 1 to 7

Background
Chronic wounds such as leg ulcers, diabetic footulcers and pressure sores are common in bothacute and community healthcare settings. Theprevention and treatment of these wounds involvesmany strategies: pressure-relieving beds, mattressesand cushions are universally used as measures forthe prevention and treatment of pressure sores;compression therapy in a variety of forms is widelyused for venous leg ulcer prevention and treat-ment; and a whole range of therapies involvinglaser, ultrasound and electricity is also applied tochronic wounds. This report covers the final threereviews from a series of seven.
Aims
To assess the clinical effectiveness and cost-effectiveness of:
1. pressure-relieving beds, mattresses and cushionsfor pressure sore prevention and treatment
2. compression therapy for the prevention andtreatment of leg ulcers
3. low-level laser therapy, therapeutic ultrasound,electrotherapy and electromagnetic therapy forthe treatment of chronic wounds.
Methods
Data sourcesNineteen electronic databases, includingMEDLINE, CINAHL, EMBASE and the CochraneControlled Trials Register (CENTRAL), weresearched. Relevant journals, conference proceed-ings and bibliographies of retrieved papers werehandsearched. An expert panel was alsoconsulted.
Study selectionRandomised controlled trials (RCTs) which evalu-ated these interventions were eligible for inclusionin this review if they used objective measures ofoutcome such as wound incidence or healing rates.
Results
Beds, mattresses and cushions forpressure sore prevention and treatmentA total of 45 RCTs were identified, of which 40compared different mattresses, mattress overlaysand beds. Only two trials evaluated cushions, oneevaluated the use of sheepskins, and two looked atturning beds/kinetic therapy.
Compression for leg ulcersA total of 24 trials reporting 26 comparisons werewere included (two of prevention and 24 oftreatment strategies).
Low-level laser therapy, therapeuticultrasound, electrotherapy andelectromagnetic therapyFour RCTs of laser (for venous leg ulcers), 10 oftherapeutic ultrasound (for pressure sores andvenous leg ulcers), 12 of electrotherapy (forischaemic and diabetic ulcers, and chronic woundsgenerally) and five of electromagnetic therapy(for venous leg ulcers and pressure sores) wereincluded. Studies were generally small, and of poormethodological quality.
Conclusions• Foam alternatives to the standard hospital foam
mattress can reduce the incidence of pressuresores in people at risk, as can pressure-relievingoverlays on the operating table. One studysuggests that air-fluidised therapy may increasepressure sore healing rates.
• Compression is more effective in healing venousleg ulcers than is no compression, and multi-layered high compression is more effective thansingle-layer compression. High-compressionhosiery was more effective than moderatecompression in preventing ulcer recurrence.
• There is generally insufficient reliable evidenceto draw conclusions about the contribution oflaser therapy, therapeutic ultrasound, electro-therapy and electromagnetic therapy to chronicwound healing.
Health Technology Assessment 2001; Vol. 5: No. 9
iii
Executive summary to Parts 5 to 7

Systematic reviews of wound caremanagement (5): pressure-relieving beds,mattresses and cushions for the preventionand treatment of pressure sores
N Cullum*
EA NelsonT Sheldon
Department of Health Studies, University of York, UK
* Corresponding author
Competing interests: N Cullum has: received funds from the NHS R&D Programmeto undertake primary research in wound care; received sponsorship of trial-relatededucational meetings from Huntleigh Healthcare and Beiersdorf Ltd. EA Nelson has:conducted one of the trials reviewed; been reimbursed for attending symposia by Smithand Nephew Ltd, ConvaTec and Huntleigh Healthcare

List of abbreviations ......................................... 5
Executive summary to Part 5 ......................... 7
1 Introduction .................................................. 9Identifying people at risk .............................. 9Types of pressure-relieving intervention ..... 9Aims ................................................................ 10
2 Methods ......................................................... 11Search strategy ............................................... 11Inclusion and exclusion criteria ................... 11Data extraction .............................................. 13Methodological quality .................................. 13Data synthesis ................................................. 13
3 Results ............................................................ 15Studies included in the review ...................... 15Studies excluded from the review ................ 16Prevention of pressure sores ......................... 16Treatment of pressure sores ......................... 21Summary ......................................................... 22
4 Discussion ...................................................... 23
5 Conclusions ................................................... 25Implications for practice ............................... 25Implications for research .............................. 25
Acknowledgements ..................................... 27
References ..................................................... 29
Appendix 1 Databases searched andsearch strategies ............................................. 33
Appendix 2 Advisory panel ....................... 37
Appendix 3 Summary of includedstudies ............................................................. 39
Appendix 4 Quality assessment ofincluded studies ............................................. 71
Appendix 5 Comparisons undertaken inthe included studies ...................................... 75
Health Technology Assessment 2001; Vol. 5: No. 9
3
Contents to Part 5

Health Technology Assessment 2001; Vol. 5: No. 9
5
List of abbreviations
AP alternating pressure
CI confidence interval
CLP constant low pressure
DARE Database of Abstracts of Reviews of Effectiveness
df degrees of freedom
RCT randomised controlled trial
RR relative risk

Background
Pressure sores (also known as bedsores, pressureulcers, decubitus ulcers) are areas of localiseddamage to the skin and underlying tissue due topressure, shear or friction. They are common inthe elderly and immobile, and costly in financialand human terms. Pressure-relieving beds,mattresses and seat cushions are widely used asaids to the prevention and treatment of pressuresores in both institutional and non-institutionalsettings.
Objectives
This systematic review seeks to answer the followingquestions:
• Do pressure-relieving cushions, beds, mattressoverlays and mattress replacements reduce theincidence of pressure sores compared withstandard support surfaces?
• Do pressure-relieving cushions, beds, mattressoverlays and mattress replacements increase thehealing rate of pressure sores compared withstandard support surfaces?
• Which types of pressure-relieving surface are themost effective for prevention and treatment?
Methods
Data sourcesThe specialised trials register of the CochraneWounds Group (compiled from regular searchesof many electronic databases, including MEDLINE,CINAHL and EMBASE, plus handsearching ofspecialist journals and conference proceedings)was searched for the period up to April 2000. Thereference sections of the obtained studies were alsosearched for further trials.
Study selectionRandomised controlled trials (RCTs), publishedor unpublished, which assessed the effectivenessof beds, mattresses, mattress overlays and seating
cushions for the prevention and/or treatment ofpressure sores, in any patient group in any setting.RCTs were eligible for inclusion if they reportedan objective, clinical outcome measure, such asthe incidence and severity of new pressure sores(in prevention studies) and the healing rates ofexisting pressure sores in treatment studies. Studieswhich only reported proxy outcome measures,such as interface pressure, were excluded.
Data extraction and synthesisTrial data were extracted by one researcher andchecked by a second. The results from each studyare presented as relative risk (for dichotomousvariables) or effect sizes (for continuous variables).Where deemed appropriate, similar studies werepooled in a meta-analysis.
Results
A total of 45 RCTs were identified.
• Foam alternatives to the standard hospital foammattress can reduce the incidence of pressuresores in people at risk of developing pressuresores.
• The relative merits of alternating and constantlow-pressure devices and of the different alter-nating pressure devices for pressure sore preven-tion are unclear.
• Pressure-relieving overlays on the operatingtable have been shown to reduce postoperativepressure sore incidence.
• There is insufficient evidence to draw conclu-sions about the value of seat cushions, limbprotectors, various constant low-pressure devicesand sheepskins as pressure sore preventionstrategies.
• One high-quality trial suggests that air-fluidisedtherapy may improve pressure sore healingrates. There is insufficient evidence to drawconclusions about the value of other beds,mattresses and seat cushions as pressure soretreatments.
Health Technology Assessment 2001; Vol. 5: No. 9
7
Executive summary to Part 5
Conclusions
Implications for practice• In people at high risk of developing pressure
sores, consideration should be given to the useof higher specification foam mattresses ratherthan standard hospital foam mattresses.
• The relative merits of more sophisticatedconstant low-pressure and alternating pressuredevices for the prevention and treatment ofpressure sores are unclear.
• Organisations might consider the use ofpressure relief for high-risk patients in theoperating theatre, as this is associated with areduction in the postoperative incidence ofpressure sores.
• Good evidence from RCTs suggests that air-fluidised supports may improve pressure sorehealing rates.
• Seat cushions have not been adequatelyevaluated.
Recommendations for researchIndependent, well-designed, multicentre RCTsare needed to compare the clinical effectivenessand cost-effectiveness of different types of pressure-relieving devices for patients at different levels ofrisk in a variety of settings. In particular, thisresearch should aim to compare:
• alternating pressure devices with other‘high-tech’ equipment (e.g. low-air-loss andair-fluidised beds) in very high-risk groups
• alternating pressure mattresses with less costlyalternating pressure overlays
• alternating pressure devices with ‘lower tech’alternatives (e.g. different types of high-specification foam mattresses, other constantlow-pressure devices).
Evaluation of alternating pressure is givenhigh priority here on the basis of its wide-spread use in prevention and treatment, andits cost.
Research is needed into valid and reliable methodsof measuring wound healing, of detecting earlyskin damage that is prognostic of pressure soredevelopment, and of the impact of pressure soreson quality of life.
Future research must address the methodologicaldeficiencies associated with much of the researchdescribed in this review. Patients should be trulyrandomised (with concealed allocation), trialsshould be of sufficient size to detect clinicallyimportant differences, and there should be clearcriteria for measuring outcomes which, ideally,should be assessed without knowledge of theintervention received (blinded) or, as a minimum,independently verified. Interventions underevaluation should be thoroughly and clearlydescribed. Researchers should be encouraged todevelop measures to assess patients’ experiencesof pressure-relieving equipment (e.g. comfort).The studies should also have adequate follow-upand appropriate statistical analysis.
Given the high costs associated with the preventionand treatment of pressure sores generally, andof pressure-relieving surfaces specifically, greateremphasis should be given in the future to robusteconomic evaluations.
Executive summary
8
Pressure sores (also known as pressure ulcers,decubitus ulcers and bed sores) are areas of
localised damage to the skin and underlyingtissue, believed to be caused by pressure, shearor friction.1 They usually occur over bony promi-nences such as the base of the spine, hips andheels. Pressure sores occur in both hospital andcommunity settings, most often in the elderly andimmobile (e.g. orthopaedic patients), those withsevere acute illness (e.g. patients in intensive careunits) and in people with neurological deficits (e.g.with spinal cord injuries).
The development of pressure sores is quitecommon. For example, new pressure soresoccurred in 4–10% of patients admitted to a UKdistrict general hospital, depending on the casemix.2 They represent a major burden of sicknessand reduced quality of life for patients and theircarers, and are costly to the NHS. The cost ofpreventing and treating pressure sores in a 600-bed large general hospital has been estimated tobe between £600,000 and £3 million per year.2
It is commonly thought that most pressure soresare avoidable, and a number of initiatives havebeen established to prioritise their prevention.3,4
The 1994–95 NHS Priorities and PlanningGuidance5 encouraged health authorities to setannual targets for an overall reduction in preva-lence of at least 5%. However, target setting inthis area may not be sensible, and the achievementof targets is not straightforward. For example,pressure sore prevalence surveys conducted on thesame 29 wards in a district health authority in 1986and 1989 demonstrated an increase in prevalencefrom 6.8% to 14.2%, despite a large investment inpressure sore prevention equipment during theintervening period.6
A pressure sore can be defined as “a new or estab-lished area of skin and/or tissue discoloration ordamage which persists after the removal ofpressure and which is likely to be due to the effectsof pressure on the tissues”.3 Healthcare profes-sionals attempt to reduce the incidence of severepressure sores by the identification of people athigh risk and the use of prevention strategies suchas pressure-relieving equipment. It is essential thatinitiatives are based on the best available evidence
of clinical effectiveness and cost-effectiveness, andwe have therefore undertaken a systematic reviewof the evidence for the effectiveness of pressure-relieving support surfaces such as beds, mattresses,cushions and repositioning interventions. A system-atic review of the epidemiology of pressure sores isoutside the scope of this review.
Identifying people at risk
Interventions to prevent pressure sores can bevery expensive, and it is important to ensure thatresources are targeted at patients who are at highrisk of developing sores. Various scales have beendeveloped to identify these high-risk patients. Mostscales have been developed in an ad hoc fashion; itis unclear which is the most accurate. There is littleevidence that using a pressure sore risk scale isbetter than clinical judgement or that the use ofsuch a scale improves outcomes. The predictivevalidity of pressure sore risk calculators has beensummarised in a previous systematic review andlittle research has been published since itscompletion.7
Types of pressure-relievingintervention
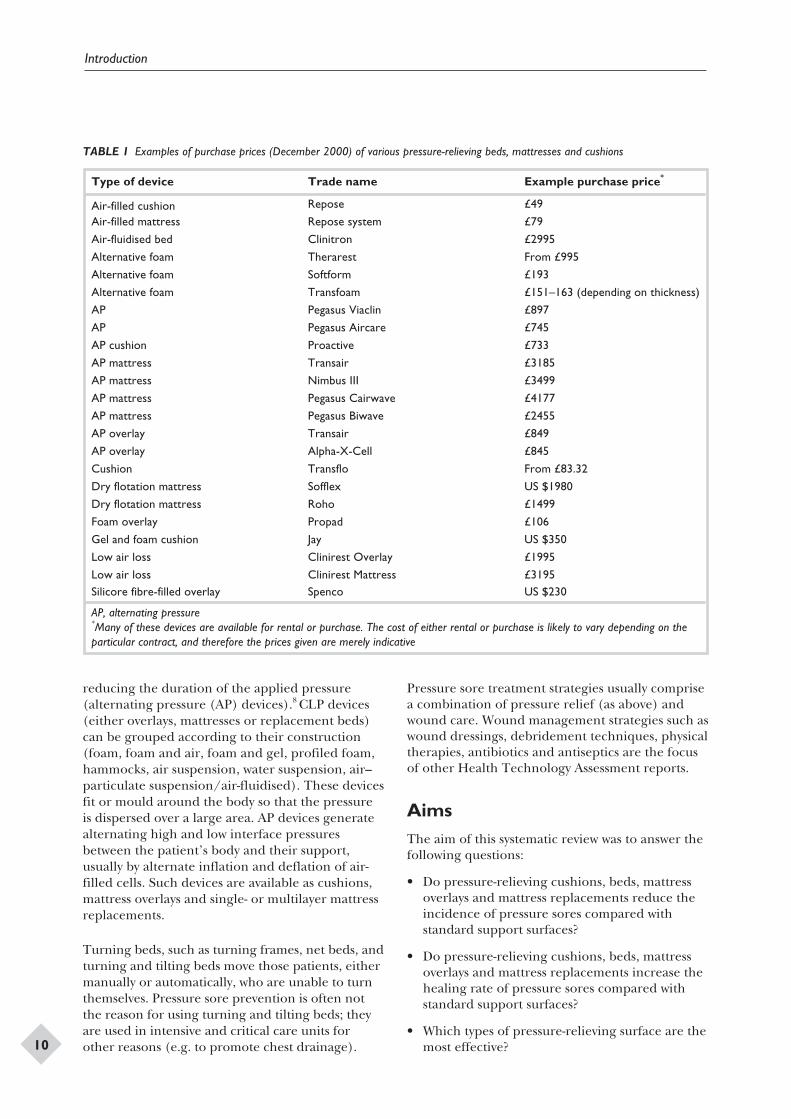
The aim of pressure sore prevention strategies isto reduce the magnitude and/or duration ofpressure between a patient and their supportsurface (the interface pressure). This may beachieved by regular manual repositioning (e.g.2-hourly turning), or by using pressure-relievingsupport surfaces such as cushions, mattress overlays,replacement mattresses or whole bed replacements.The cost of these interventions varies widely; fromover £30,000 for some bed replacements to lessthan £100 for some foam overlays (Table 1). Infor-mation on the relative cost-effectiveness of thisequipment is clearly needed to aid rational use.
Pressure-relieving cushions, beds and mattresseseither mould around the shape of the patient todistribute the patient’s weight over a larger area(constant low-pressure (CLP) devices), or mechani-cally vary the pressure beneath the patient, so
Health Technology Assessment 2001; Vol. 5: No. 9
9
Chapter 1
Introduction
reducing the duration of the applied pressure(alternating pressure (AP) devices).8 CLP devices(either overlays, mattresses or replacement beds)can be grouped according to their construction(foam, foam and air, foam and gel, profiled foam,hammocks, air suspension, water suspension, air–particulate suspension/air-fluidised). These devicesfit or mould around the body so that the pressureis dispersed over a large area. AP devices generatealternating high and low interface pressuresbetween the patient’s body and their support,usually by alternate inflation and deflation of air-filled cells. Such devices are available as cushions,mattress overlays and single- or multilayer mattressreplacements.
Turning beds, such as turning frames, net beds, andturning and tilting beds move those patients, eithermanually or automatically, who are unable to turnthemselves. Pressure sore prevention is often notthe reason for using turning and tilting beds; theyare used in intensive and critical care units forother reasons (e.g. to promote chest drainage).
Pressure sore treatment strategies usually comprisea combination of pressure relief (as above) andwound care. Wound management strategies such aswound dressings, debridement techniques, physicaltherapies, antibiotics and antiseptics are the focusof other Health Technology Assessment reports.
AimsThe aim of this systematic review was to answer thefollowing questions:
• Do pressure-relieving cushions, beds, mattressoverlays and mattress replacements reduce theincidence of pressure sores compared withstandard support surfaces?
• Do pressure-relieving cushions, beds, mattressoverlays and mattress replacements increase thehealing rate of pressure sores compared withstandard support surfaces?
• Which types of pressure-relieving surface are themost effective?
Introduction
10
Type of device Trade name Example purchase price*
Air-filled cushion Repose £49
Air-filled mattress Repose system £79
Air-fluidised bed Clinitron £2995
Alternative foam Therarest From £995
Alternative foam Softform £193
Alternative foam Transfoam £151–163 (depending on thickness)
AP Pegasus Viaclin £897
AP Pegasus Aircare £745
AP cushion Proactive £733
AP mattress Transair £3185
AP mattress Nimbus III £3499
AP mattress Pegasus Cairwave £4177
AP mattress Pegasus Biwave £2455
AP overlay Transair £849
AP overlay Alpha-X-Cell £845
Cushion Transflo From £83.32
Dry flotation mattress Sofflex US $1980
Dry flotation mattress Roho £1499
Foam overlay Propad £106
Gel and foam cushion Jay US $350
Low air loss Clinirest Overlay £1995
Low air loss Clinirest Mattress £3195Silicore fibre-filled overlay Spenco US $230
AP, alternating pressure*Many of these devices are available for rental or purchase. The cost of either rental or purchase is likely to vary depending on theparticular contract, and therefore the prices given are merely indicative
TABLE 1 Examples of purchase prices (December 2000) of various pressure-relieving beds, mattresses and cushions

A systematic review of primary research wasundertaken using the NHS Centre for Reviews
and Dissemination structured guidelines.9
Search strategy
Nineteen electronic research databases weresearched for the period 1966 and June 1998 usinga sensitive search strategy designed in collaborationwith an information specialist at the NHS Centrefor Reviews and Dissemination (appendix 1).Subsequently the Specialist Trials Register of theCochrane Wounds Group (compiled and regularlyupdated from searches of the Cochrane ControlledTrials Register (CENTRAL), MEDLINE, CINAHL,EMBASE, etc.) was searched for the period upto April 2000. The electronic search was supple-mented by a handsearch of five specialist woundcare journals, 12 conference proceedings anda search of systematic reviews held on the NHSCentre for Reviews and Dissemination Database ofAbstracts of Reviews of Effectiveness (DARE). Thebibliographies of all retrieved and relevant publica-tions were searched for further studies. Companieswith an interest in wound care products wereapproached for unreported trials. An advisorypanel of experts in wound management, estab-lished to comment on the review as it progressed,was also asked to identify any additional trials(appendix 2). Relevant economic evaluations weresearched for by adding economic-related searchterms to those used in the search for clinical trials.Authors of trials published between 1985 and 1998were contacted and asked to provide details of anyassociated economic evaluations.
Inclusion and exclusion criteria
Types of studiesRandomised controlled trials (RCTs) comparingbeds, mattresses and cushions, which measuredthe incidence of new pressure sores (in preventionstudies) or pressure sore healing (in treatmentstudies) as objective measures of outcome.
There was no restriction on the basis of thelanguage in which the study reports were writtenor on the basis of publication status.
Studies which used only subjective measures ofoutcome were excluded, as were studies whichreported only proxy measures such as interfacepressure.
Types of participantsPrevention studiesPatients receiving healthcare who were deemed tobe at risk of pressure sore development, in anysetting.
Treatment studiesPatients with existing pressure sores, in any setting.
Types of interventionStudies which evaluated the following interventionsfor pressure sore prevention or treatment wereincluded:
1. Standard foam mattresses.2. Alternative foam mattresses/overlays (e.g.
convoluted foam, cubed foam): these areconformable and aim to redistribute pressureover a larger contact area.
3. Gel-filled mattresses/overlays: mode of actionas above.
4. Fibre-filled mattresses/overlays: mode of actionas above.
5. Air-filled mattresses/overlays: mode of actionas above.
6. Water-filled mattresses/overlays: mode ofaction as above.
7. Bead-filled mattresses/overlays: mode of actionas above.
8. AP mattresses/overlays: the patient lies onair-filled sacs, which sequentially inflateand deflate and relieve pressure at differentanatomical sites for short periods; these devicesmay incorporate a pressure sensor.
9. Air-fluidised beds: warmed air is circulatedthrough fine ceramic beads covered by apermeable sheet; allows support over a largercontact area.
10. Low-air-loss beds: patients are supported ona series of air sacs through which warmed airpasses.
11. Sheepskins: proposed mode of action unclear.12. Turning beds/frames: beds that either aid
manual repositioning of the patient or
Health Technology Assessment 2001; Vol. 5: No. 9
11
Chapter 2
Methods
reposition the patient by motor-driven turningand tilting.
13. Wheelchair cushions: conforming or mechan-ical (e.g. alternating pressure) cushions reducecontact pressure by increasing the surface areain contact with the patient’s body.
14. Operating-table overlays: as above.15. Limb protectors: pads and cushions of
different forms to protect bony prominences.
We classified items 1–7 as ‘low-tech’ surfaces anditems 8–10 as ‘high-tech’ surfaces.
Types of outcome measurePrevention studiesIncidence of new pressure soresMany evaluations have simply measured thepressure on different parts of the body in contactwith the support surface (interface pressure).However, interface pressure is an intermediateor surrogate outcome measure which has seriouslimitations as a proxy for clinical outcome, sincethe process that leads to the development of apressure sore almost certainly involves the complexinterplay of several factors. Unfortunately, becauseit is relatively simple, quick and inexpensive tomeasure, most evaluations only compare interfacepressure. This is also true of Department of Healthcomparative evaluations of mattresses.10 In thisreview we considered only trials which reportedclinical outcome measures.
Some studies, when reporting outcomes of inter-ventions for prevention, did not differentiatebetween people developing grade 1 sores (in whichthe skin is unbroken) and those developing moresevere sores. Studies which compared the inci-dence of pressure sores of grade 2 or greater aremore likely to be reliable (see below for details ofthe grading system). However, we included allstudies, irrespective of whether grade 1 sores weredescribed separately.
Grades of new pressure soresA range of pressure sore grading systems is usedin pressure sore trials. An example of a commonlyused grading system is presented below.
• Grade 1: persistent discoloration of the skin,including non-blanchable erythema;blue/purple/black discoloration.
• Grade 2: partial-thickness skin loss involvingepidermis and dermis.
• Grade 3: full-thickness skin loss involvingdamage to or necrosis of subcutaneous tissues,but not through the underlying fascia and not
extending to the underlying bone, tendon orjoint capsule.
• Grade 4: full-thickness skin loss with extensivedestruction and tissue necrosis extending to theunderlying bone, tendon or joint capsule.
Treatment studiesWhere pressure-relieving interventions areevaluated as aids to the healing of pressure soreswe looked at reported wound healing rates.However, there is no single standard outcomemeasure for wound healing. Both objective andsubjective measures are widely used by researchers,but little effort has been made to determine thevalidity of these measurements.
Most subjective measures, such as visual estimatesof oedema, erythema, granulation, pus and debris,are unlikely to be applied consistently betweenwounds or by different assessors. Unless assessmentis blinded to treatment allocation this method islikely to result in significant biases. Blinding maybe difficult to achieve in wound care trials as manyof the products are easily identified visually and itis usually not feasible to move a patient in order toassess the condition of their pressure-affectedareas. This review excluded studies which reportedonly subjective measures.
Objective measures of healing are usually basedon wound area and/or volume. Planimetry, oftenaided by computer, is the most frequently usedmethod of calculating wound area, althoughother methods such as the measurement of wounddiameter or weight of a tracing drawn around thearea of the wound are also used.
Measurements of wound volume are infrequentlyreported in the literature. These methods areoften cumbersome and their accuracy has notbeen proven.11 Computerised image analysis mayprove to be a useful technique for the assessmentof wound volume in the future, as the equipmentbecomes more affordable and portable.
Even though objective measures reduce oreliminate subjective biases and reduce randommeasurement errors, they cannot address inherentbiases if the patients being compared have woundsof different baseline size.
A change in wound area is often expressed as thepercentage change which, unlike the absolutechange in area, takes into account the initial sizeof the wound. For two wounds healing at the samelinear rate (as measured by diameter reduction)percentage area calculations will show a larger
Methods
12

change for a small wound than for a large wound.The converse is true when the absolute change inarea is measured, since for any unit reduction inwound radius a larger area reduction will occur fora large wound. This has important consequencesfor the validity of trial results where there is poorcomparability in initial wound size at baselinebetween the treatment groups.
In large trials, randomised allocation shouldensure that the mean wound size and variance ineach group is similar. In a small trial, randomallocation is unlikely to result in an even distribu-tion of wound sizes. In a trial where there is poorcomparability between groups for wound size atbaseline, and the outcome is based on the changein area, the result can only be considered valid if itis obtained against the anticipated direction of thebias for wound size, or when the percentage areachange and absolute area change are in the samedirection. If baseline data are not given it is notpossible to determine the direction of bias, andthe validity of the results cannot be determined.
Despite the potential for objective outcomes tobe biased by differences in wound size at baseline,they remain the most reliable assessment of woundhealing since they reduce the biases of the assessor,which cannot be estimated.
All studiesFor all studies, we looked at the following aspects:
• the costs of devices• patient comfort• the durability of devices• the reliability of devices• the acceptability of devices.
Retrieved studies were assessed for relevance by asingle reviewer, and decisions on the final inclu-sion of a study was checked by a second reviewer.Disagreements were resolved by discussion with athird reviewer. Rejected studies were checked by asecond reviewer (one of FS, AF, AN, KF, TS).
Where study details were lacking, the authors wereinvited to provide further information.
Data extraction
Data from included trials were extracted by a singlereviewer into pre-prepared data-extraction tablesand checked by a second reviewer. The followingdata were extracted from each study:
• patient inclusion and exclusion criteria• care setting• key baseline variables by group (e.g. age, sex,
baseline risk, baseline area of existing sores)• a description of the interventions and the
number of patients randomised to eachintervention
• a description of any co-interventions or standardcare
• duration and extent of follow-up• outcomes (e.g. incidence and severity of new
pressure sores; healing rates)• acceptability and reliability of equipment if
reported.
If data were missing from reports attempts weremade to contact the authors to complete theinformation necessary for the critical appraisal. Ifstudies were published more than once, the mostdetailed report was used as the basis for the dataextraction.
Methodological quality
The methodological quality of each trial wasassessed by two researchers independently. Thefollowing quality criteria were used:
• description of inclusion and exclusion criteriaused to derive the sample from the targetpopulation
• description of the a priori sample-sizecalculation
• evidence of allocation concealment atrandomisation
• a description of baseline comparability oftreatment groups
• whether the outcome assessment was stated tobe blinded
• whether incident sores were described byseverity grading as well as frequency (grade 1sores are not breaks in the skin and are subjectto more interrater variation)
• a clear description of the main interventions.
Data synthesis
For each trial the relative risk (RR) was calculatedfor categorical outcomes, such as the numberof patients developing sores and the number ofpressure sores healed. The 95% confidence inter-vals (95% CI) were included when sufficient detailto allow their calculation was provided. The resultsfrom replicated studies were plotted on graphs anddiscussed by narrative review. Unique comparisons
Health Technology Assessment 2001; Vol. 5: No. 9
13

were not plotted and the relative risk is stated inthe text. Individual study details are presented instructured tables. Where there was more thanone trial comparing similar devices using the sameoutcome, and in the absence of obvious method-ological or clinical heterogeneity, statisticalheterogeneity was tested for by using the c2 test. Inthe absence of significant statistical heterogeneity,studies with similar comparisons were pooled usinga fixed-effects model.12 If heterogeneity wasobserved, both random- and fixed-effects models
were used to pool the data. All statistical analysiswas performed using Revman (v3.1.1). Continuousoutcome variables such as change in woundvolume were reported where appropriate andsummarised as the weighted mean differenceacross studies. Where outcomes for continuousvariables were presented as medians without confi-dence intervals, standard deviations or some othermeasure of the precision of the result, the medianwas entered in the analysis table and the data werenot used in the data synthesis.
Methods
14
Studies included in the review
Forty-five relevant RCTs were identified (seeappendix 3). Thirty trials involved patients withoutpre-existing pressure sores (intact skin) in assess-ments of the effectiveness of pressure-relievinginterventions in the prevention of pressure sores.Twelve trials involved patients with pressure soresin assessments of the treatment efficacy of pressure-relieving supports, and three trials involved a mix-ture of patients with and without pre-existing sores.
Three studies evaluated different operating-tablesurfaces;13–15 six evaluated different surfaces inintensive care units;16–21 and seven studies confinedthe evaluation to orthopaedic patients.22–28 Theremaining studies looked at a variety of patients(e.g. those in nursing homes, those on care of theelderly, those on medical and surgical wards).
Only two trials evaluated cushions: one evaluatedthe use of sheepskins and two looked at turning
beds/kinetic therapy. The remaining studiesevaluated different mattresses, mattress overlaysand beds.
A summary of the methodological quality of eachof the trials is given in appendix 4. Methodologicalrigour in RCTs is essential in order to minimisebias. Although the majority (87%) of trialsdiscussed the criteria for including patients, only38% of the reports gave information which madeus confident that patients were truly randomlyallocated,29 and only 9/45 (20%) trials adoptedblinded assessment of outcomes. Small sample sizewas a major limitation of many of the studies; themedian sample size was 80 (range 25–505) andonly 14/45 studies described an a priori samplesize.
Three studies assessed the effectiveness of pressure-relieving interventions for both the preventionand treatment of pressure sores. The results aresummarised according to the type of devices tested.
Health Technology Assessment 2001; Vol. 5: No. 9
15
Chapter 3
Results
Study Reason for exclusion
Bliss and co-workers30 Not an RCT. Patients were allocated in a rota fashion, and the possibility thatknowledge of the next mattress to be allocated might have influenced allocation wasacknowledged. Rotas were changed on the basis of availability of mattresses, etc.
Bliss31 While eight surfaces were evaluated in this prospective trial, not all surfaces were inuse in the trial at any time, and therefore the surfaces were not truly compared withone another contemporaneously. Furthermore, it was possible for patients to bere-randomised back into the study, and this occurred frequently (a total of 457mattress trials were reported in only 238 patients). The data were not presented bypatient; only by mattress trial
Branom and Knox32 No healing data presented
Collins33 Study on two wards; wards, not patients, were randomised
Hawkins34 Not an RCT
Jesurum and co-workers35 Not an RCT
Koo and co-workers36 Not an RCT; a study of interface pressures in healthy volunteers
Marchand and Lidowski37 Not an RCT
Regan and co-workers38 This study reports an audit of pressure sore incidence after implementation of acomprehensive pressure sore policy. Not a prospective RCT
Rosenthal and co-workers39 Not an RCT
Stoneberg and co-workers40 Historical control group
Zernike41 Incidence of pressure sores not reported
TABLE 2 Summary of studies excluded from the review
The implications for prevention and treatment areconsidered separately in chapter 5.
Studies excluded from the review
The studies excluded from the review and thereasons for their exclusion are summarised inTable 2.
Prevention of pressure sores
‘Low-tech’ constant pressure supportsTrials of the standard hospital mattressThis section considers comparisons of thestandard foam hospital mattress with other low-tech, constant-pressure supports.
Seven RCTs comparing ‘standard’ mattresses orsurfaces with low-tech supports for the preventionof pressure sores were identified.24,25,27,42–45 Whencompared with standard hospital mattresses, theincidence and severity of pressure sores in ‘high-risk’ patients were reduced when patients wereplaced on either the Comfortex DeCube mattress,25
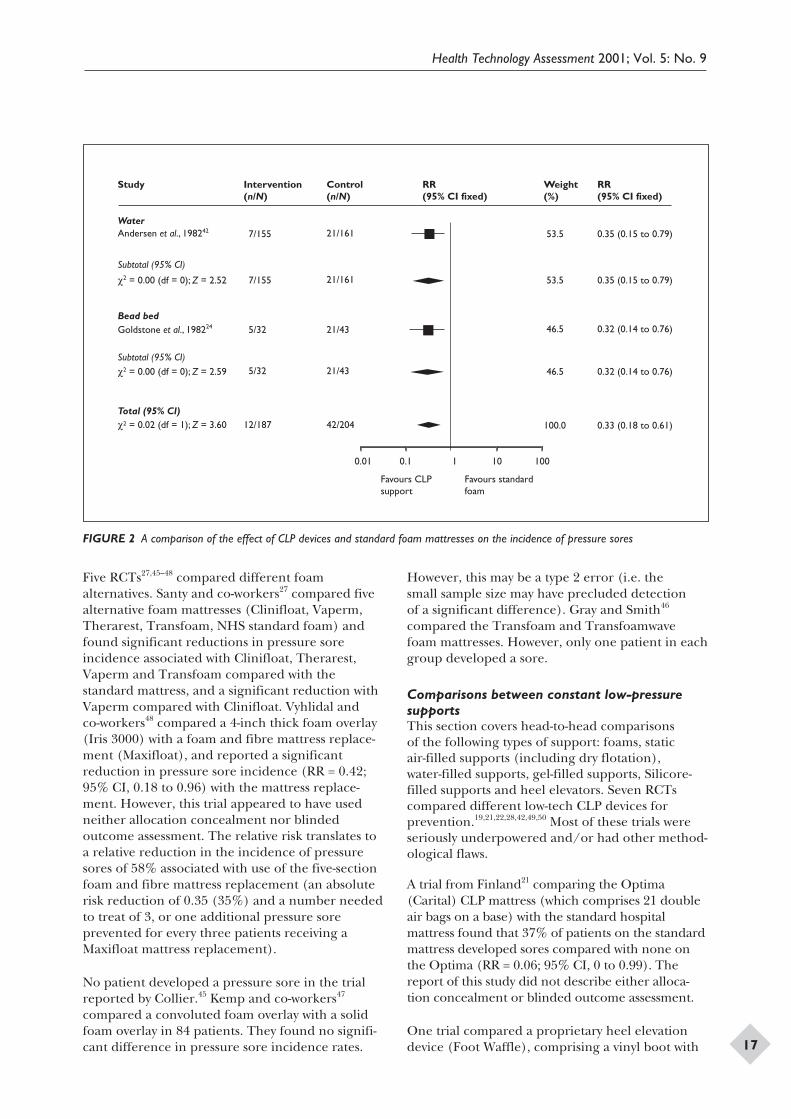
(RR = 0.34; 95% CI, 0.14 to 0.85) the Beaufortbead bed24 (RR = 0.32; 95% CI, 0.14 to 0.76), theSoftform mattress44 (RR = 0.2; 95% CI, 0.09 to0.45) or the water-filled mattress42 (RR = 0.35; 95%CI, 0.15 to 0.79) (Figures 1 and 2). In an unpub-lished British study of older people with hipfractures admitted to orthopaedic trauma wards,patients allocated to receive a NHS standard foammattress (manufactured by Relyon) experienced
over three times the rate of pressure sores asthose using one of a number of foam alternatives(Clinifloat, Therarest, Transfoam, Vaperm – seeappendix 3).27
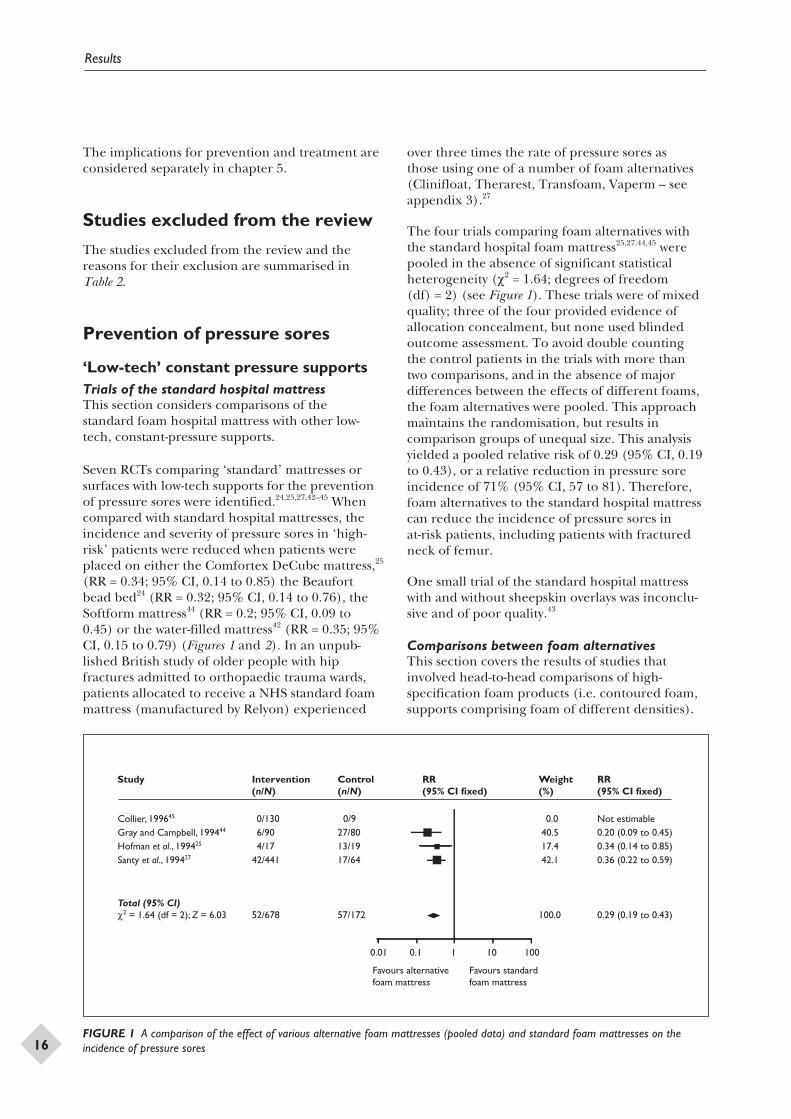
The four trials comparing foam alternatives withthe standard hospital foam mattress25,27,44,45 werepooled in the absence of significant statisticalheterogeneity (c2 = 1.64; degrees of freedom(df) = 2) (see Figure 1). These trials were of mixedquality; three of the four provided evidence ofallocation concealment, but none used blindedoutcome assessment. To avoid double countingthe control patients in the trials with more thantwo comparisons, and in the absence of majordifferences between the effects of different foams,the foam alternatives were pooled. This approachmaintains the randomisation, but results incomparison groups of unequal size. This analysisyielded a pooled relative risk of 0.29 (95% CI, 0.19to 0.43), or a relative reduction in pressure soreincidence of 71% (95% CI, 57 to 81). Therefore,foam alternatives to the standard hospital mattresscan reduce the incidence of pressure sores inat-risk patients, including patients with fracturedneck of femur.
One small trial of the standard hospital mattresswith and without sheepskin overlays was inconclu-sive and of poor quality.43
Comparisons between foam alternativesThis section covers the results of studies thatinvolved head-to-head comparisons of high-specification foam products (i.e. contoured foam,supports comprising foam of different densities).
Results
16
Study Collier, 199645
Gray and Campbell, 199444
Hofman et al., 199425
Santy et al., 199427
Total (95% CI)c2 = 1.64 (df = 2); Z = 6.03
Intervention (n/N) 0/130 6/90 4/1742/441 52/678
Control (n/N) 0/927/8013/1917/64 57/172
RR (95% CI fixed)
Weight (%) 0.0 40.5 17.4 42.1 100.0
RR (95% CI fixed) Not estimable0.20 (0.09 to 0.45)0.34 (0.14 to 0.85)0.36 (0.22 to 0.59) 0.29 (0.19 to 0.43)
0.01 0.1 1 10 100
Favours alternative foam mattress
Favours standard foam mattress
FIGURE 1 A comparison of the effect of various alternative foam mattresses (pooled data) and standard foam mattresses on theincidence of pressure sores
Five RCTs27,45–48 compared different foamalternatives. Santy and co-workers27 compared fivealternative foam mattresses (Clinifloat, Vaperm,Therarest, Transfoam, NHS standard foam) andfound significant reductions in pressure soreincidence associated with Clinifloat, Therarest,Vaperm and Transfoam compared with thestandard mattress, and a significant reduction withVaperm compared with Clinifloat. Vyhlidal andco-workers48 compared a 4-inch thick foam overlay(Iris 3000) with a foam and fibre mattress replace-ment (Maxifloat), and reported a significantreduction in pressure sore incidence (RR = 0.42;95% CI, 0.18 to 0.96) with the mattress replace-ment. However, this trial appeared to have usedneither allocation concealment nor blindedoutcome assessment. The relative risk translates toa relative reduction in the incidence of pressuresores of 58% associated with use of the five-sectionfoam and fibre mattress replacement (an absoluterisk reduction of 0.35 (35%) and a number neededto treat of 3, or one additional pressure soreprevented for every three patients receiving aMaxifloat mattress replacement).
No patient developed a pressure sore in the trialreported by Collier.45 Kemp and co-workers47
compared a convoluted foam overlay with a solidfoam overlay in 84 patients. They found no signifi-cant difference in pressure sore incidence rates.
However, this may be a type 2 error (i.e. thesmall sample size may have precluded detectionof a significant difference). Gray and Smith46
compared the Transfoam and Transfoamwavefoam mattresses. However, only one patient in eachgroup developed a sore.
Comparisons between constant low-pressuresupportsThis section covers head-to-head comparisonsof the following types of support: foams, staticair-filled supports (including dry flotation),water-filled supports, gel-filled supports, Silicore-filled supports and heel elevators. Seven RCTscompared different low-tech CLP devices forprevention.19,21,22,28,42,49,50 Most of these trials wereseriously underpowered and/or had other method-ological flaws.
A trial from Finland21 comparing the Optima(Carital) CLP mattress (which comprises 21 doubleair bags on a base) with the standard hospitalmattress found that 37% of patients on the standardmattress developed sores compared with none onthe Optima (RR = 0.06; 95% CI, 0 to 0.99). Thereport of this study did not describe either alloca-tion concealment or blinded outcome assessment.
One trial compared a proprietary heel elevationdevice (Foot Waffle), comprising a vinyl boot with
Health Technology Assessment 2001; Vol. 5: No. 9
17
Study
WaterAndersen et al., 198242
Subtotal (95% CI)
c2 = 0.00 (df = 0); Z = 2.52
Bead bedGoldstone et al., 198224
Subtotal (95% CI)c2 = 0.00 (df = 0); Z = 2.59
Total (95% CI)c2 = 0.02 (df = 1); Z = 3.60
Intervention (n/N)
7/155
7/155
5/32
5/32
12/187
Control (n/N)
21/161
21/161
21/43
21/43
42/204
RR (95% CI fixed)
Weight (%)
53.5
53.5
46.5
46.5
100.0
RR (95% CI fixed)
0.35 (0.15 to 0.79)
0.35 (0.15 to 0.79)
0.32 (0.14 to 0.76)
0.32 (0.14 to 0.76)
0.33 (0.18 to 0.61)
0.01 0.1 1 10 100
Favours CLP support
Favours standard foam
FIGURE 2 A comparison of the effect of CLP devices and standard foam mattresses on the incidence of pressure sores
a built-in foot cradle, with elevation of the heelsusing a hospital pillow.50 More heel sores devel-oped in the group using the Foot Waffle (6 versus2), although this difference was not statisticallysignificant (the trial involved only 52 patients).
The remaining trials were all unique comparisonsof low power, and none found statistically signifi-cant differences between the surfaces tested.
‘High-tech’ pressure reliefAlternating pressure supportsA variety of AP supports are used in hospital andthe community. The depth of the air cells and themechanical robustness vary between devices, andthese factors may be important in determiningeffectiveness. It is worth emphasising that mostof the RCTs of AP supports did not adequatelydescribe the equipment being evaluated, includingthe size of the air cells.
Eleven RCTs of AP supports for pressure soreprevention were identified: between AP andstandard hospital mattresses in one study;42
between AP and various CLP devices in eightstudies (water,19,42 static air,19,26 Silicore,19,51,52
foam,19,53 various54); and with other AP supportsin two studies.23,55
Alternating pressure compared with thestandard hospital mattressOne RCT reported that the use of AP surfacesreduces the incidence of pressure sores ascompared with standard hospital mattresses(RR = 0.32; 95% CI, 0.14 to 0.74).42 The report
of this large trial (482 patients) gave no indicationthat either allocation concealment or blindedoutcome assessment had been used.
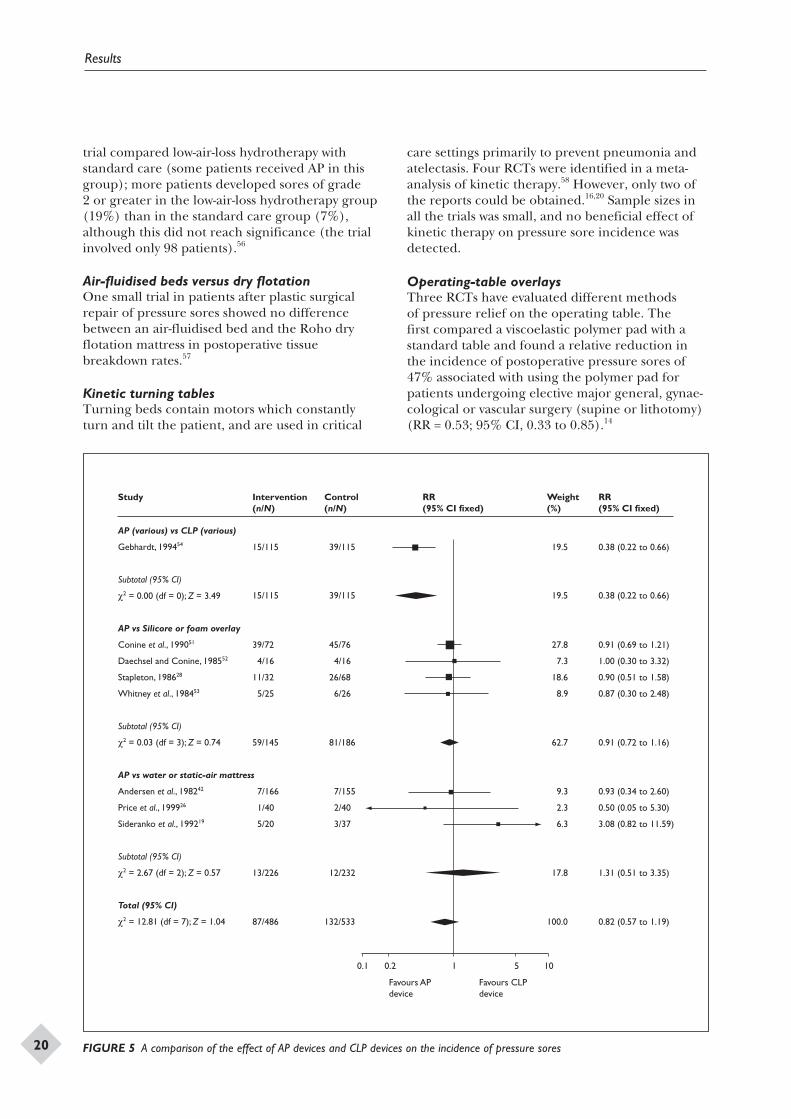
Alternating pressure compared with constantlow pressureEight trials compared AP devices with various CLPdevices, but they obtained conflicting evidence asto the relative effectiveness of these devices. Onestudy compared a range of AP supports with arange of CLP supports in a range of specialities inacute-care settings54 and reported significantlymore pressure sores in patients in the CLP group(34% compared with 13% in the AP group)(RR = 0.38; 95% CI, 0.22 to 0.66). This trial isdifficult to interpret given the wide variety ofsurfaces used in the study. There is currently insuf-ficient evidence to support a class effect for all APdevices and all CLP devices.
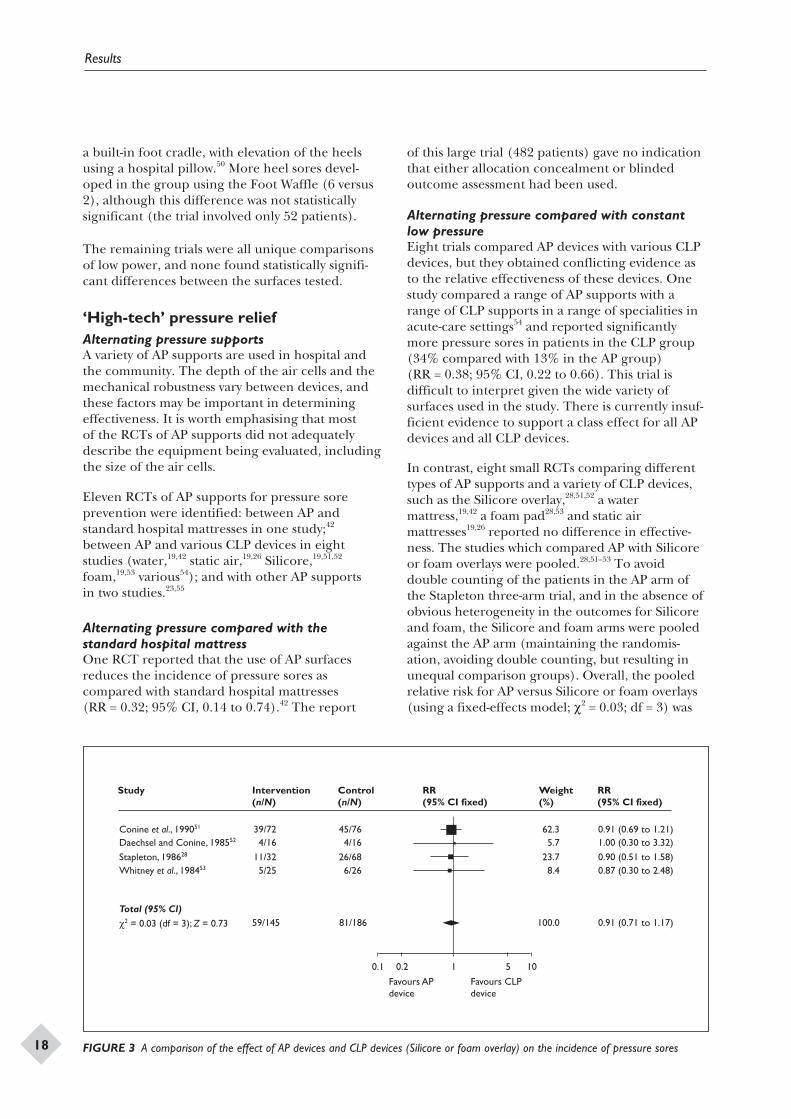
In contrast, eight small RCTs comparing differenttypes of AP supports and a variety of CLP devices,such as the Silicore overlay,28,51,52 a watermattress,19,42 a foam pad28,53 and static airmattresses19,26 reported no difference in effective-ness. The studies which compared AP with Silicoreor foam overlays were pooled.28,51–53 To avoiddouble counting of the patients in the AP arm ofthe Stapleton three-arm trial, and in the absence ofobvious heterogeneity in the outcomes for Silicoreand foam, the Silicore and foam arms were pooledagainst the AP arm (maintaining the randomis-ation, avoiding double counting, but resulting inunequal comparison groups). Overall, the pooledrelative risk for AP versus Silicore or foam overlays(using a fixed-effects model; c2 = 0.03; df = 3) was
Results
18
Study Intervention (n/N)
Control (n/N)
RR (95% CI fixed)
Weight (%)
RR (95% CI fixed)
Conine et al., 199051 39/72 45/76 62.3 0.91 (0.69 to 1.21)Daechsel and Conine, 198552 4/16 4/16 5.7 1.00 (0.30 to 3.32)
Stapleton, 198628 11/32 26/68 23.7 0.90 (0.51 to 1.58)Whitney et al., 198453 5/25 6/26 8.4 0.87 (0.30 to 2.48)
Total (95% CI)59/145 81/186 100.0 0.91 (0.71 to 1.17)c2 = 0.03 (df = 3); Z = 0.73
Favours AP device
Favours CLP device
0.1 0.2 1 5 10
FIGURE 3 A comparison of the effect of AP devices and CLP devices (Silicore or foam overlay) on the incidence of pressure sores
0.91 (95% CI, 0.71 to 1.17), indicating no statisti-cally significant difference between Silicore or foamoverlays and AP (Figure 3).
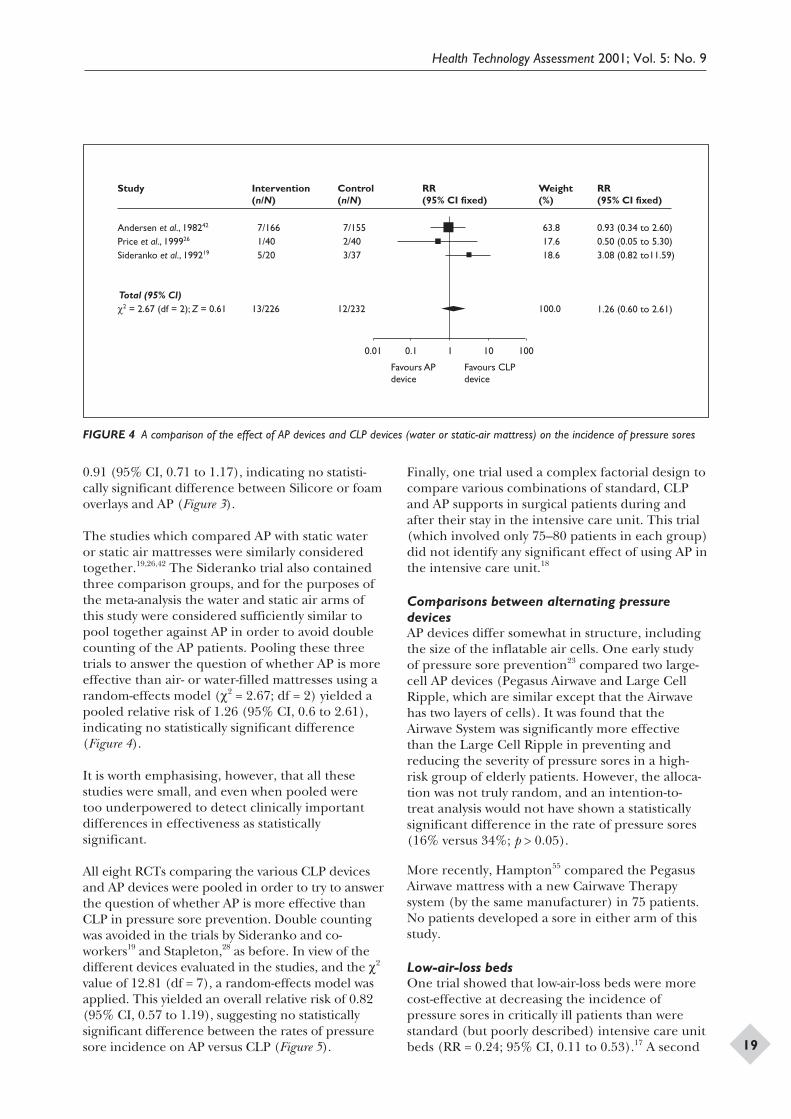
The studies which compared AP with static wateror static air mattresses were similarly consideredtogether.19,26,42 The Sideranko trial also containedthree comparison groups, and for the purposes ofthe meta-analysis the water and static air arms ofthis study were considered sufficiently similar topool together against AP in order to avoid doublecounting of the AP patients. Pooling these threetrials to answer the question of whether AP is moreeffective than air- or water-filled mattresses using arandom-effects model (c2 = 2.67; df = 2) yielded apooled relative risk of 1.26 (95% CI, 0.6 to 2.61),indicating no statistically significant difference(Figure 4).
It is worth emphasising, however, that all thesestudies were small, and even when pooled weretoo underpowered to detect clinically importantdifferences in effectiveness as statisticallysignificant.
All eight RCTs comparing the various CLP devicesand AP devices were pooled in order to try to answerthe question of whether AP is more effective thanCLP in pressure sore prevention. Double countingwas avoided in the trials by Sideranko and co-workers19 and Stapleton,28 as before. In view of thedifferent devices evaluated in the studies, and the c2
value of 12.81 (df = 7), a random-effects model wasapplied. This yielded an overall relative risk of 0.82(95% CI, 0.57 to 1.19), suggesting no statisticallysignificant difference between the rates of pressuresore incidence on AP versus CLP (Figure 5).
Finally, one trial used a complex factorial design tocompare various combinations of standard, CLPand AP supports in surgical patients during andafter their stay in the intensive care unit. This trial(which involved only 75–80 patients in each group)did not identify any significant effect of using AP inthe intensive care unit.18
Comparisons between alternating pressuredevicesAP devices differ somewhat in structure, includingthe size of the inflatable air cells. One early studyof pressure sore prevention23 compared two large-cell AP devices (Pegasus Airwave and Large CellRipple, which are similar except that the Airwavehas two layers of cells). It was found that theAirwave System was significantly more effectivethan the Large Cell Ripple in preventing andreducing the severity of pressure sores in a high-risk group of elderly patients. However, the alloca-tion was not truly random, and an intention-to-treat analysis would not have shown a statisticallysignificant difference in the rate of pressure sores(16% versus 34%; p > 0.05).
More recently, Hampton55 compared the PegasusAirwave mattress with a new Cairwave Therapysystem (by the same manufacturer) in 75 patients.No patients developed a sore in either arm of thisstudy.
Low-air-loss bedsOne trial showed that low-air-loss beds were morecost-effective at decreasing the incidence ofpressure sores in critically ill patients than werestandard (but poorly described) intensive care unitbeds (RR = 0.24; 95% CI, 0.11 to 0.53).17 A second
Health Technology Assessment 2001; Vol. 5: No. 9
19
0.01 0.1 1 10 100
Favours AP device
Favours CLP device
Study Andersen et al., 198242
Price et al., 199926
Sideranko et al., 199219
Total (95% CI)c2 = 2.67 (df = 2); Z = 0.61
Intervention (n/N) 7/166 1/40 5/20
13/226
Control (n/N) 7/155 2/40 3/37
12/232
RR (95% CI fixed)
Weight (%) 63.8 17.6 18.6
100.0
RR (95% CI fixed) 0.93 (0.34 to 2.60)0.50 (0.05 to 5.30)3.08 (0.82 to11.59)
1.26 (0.60 to 2.61)
FIGURE 4 A comparison of the effect of AP devices and CLP devices (water or static-air mattress) on the incidence of pressure sores
trial compared low-air-loss hydrotherapy withstandard care (some patients received AP in thisgroup); more patients developed sores of grade2 or greater in the low-air-loss hydrotherapy group(19%) than in the standard care group (7%),although this did not reach significance (the trialinvolved only 98 patients).56
Air-fluidised beds versus dry flotationOne small trial in patients after plastic surgicalrepair of pressure sores showed no differencebetween an air-fluidised bed and the Roho dryflotation mattress in postoperative tissuebreakdown rates.57
Kinetic turning tablesTurning beds contain motors which constantlyturn and tilt the patient, and are used in critical
care settings primarily to prevent pneumonia andatelectasis. Four RCTs were identified in a meta-analysis of kinetic therapy.58 However, only two ofthe reports could be obtained.16,20 Sample sizes inall the trials was small, and no beneficial effect ofkinetic therapy on pressure sore incidence wasdetected.
Operating-table overlaysThree RCTs have evaluated different methodsof pressure relief on the operating table. Thefirst compared a viscoelastic polymer pad with astandard table and found a relative reduction inthe incidence of postoperative pressure sores of47% associated with using the polymer pad forpatients undergoing elective major general, gynae-cological or vascular surgery (supine or lithotomy)(RR = 0.53; 95% CI, 0.33 to 0.85).14
Results
20
0.1 0.2 1 5 10
Favours AP device
Favours CLP device
Study
AP (various) vs CLP (various)
Gebhardt, 199454
Subtotal (95% CI)
c2 = 0.00 (df = 0); Z = 3.49
AP vs Silicore or foam overlay
Conine et al., 199051
Daechsel and Conine, 198552
Stapleton, 198628
Whitney et al., 198453
Subtotal (95% CI)
c2 = 0.03 (df = 3); Z = 0.74
AP vs water or static-air mattress
Andersen et al., 198242
Price et al., 199926
Sideranko et al., 199219
Subtotal (95% CI)
c2 = 2.67 (df = 2); Z = 0.57
Total (95% CI)
c2 = 12.81 (df = 7); Z = 1.04
Intervention (n/N)
15/115
15/115
39/72
4/16
11/32
5/25
59/145
7/166
1/40
5/20
13/226
87/486
Control (n/N)
39/115
39/115
45/76
4/16
26/68
6/26
81/186
7/155
2/40
3/37
12/232
132/533
RR (95% CI fixed)
Weight (%)
19.5
19.5
27.8
7.3
18.6
8.9
62.7
9.3
2.3
6.3
17.8
100.0
RR (95% CI fixed) 0.38 (0.22 to 0.66)
0.38 (0.22 to 0.66)
0.91 (0.69 to 1.21)
1.00 (0.30 to 3.32)
0.90 (0.51 to 1.58)
0.87 (0.30 to 2.48)
0.91 (0.72 to 1.16)
0.93 (0.34 to 2.60)
0.50 (0.05 to 5.30)
3.08 (0.82 to 11.59)
1.31 (0.51 to 3.35)
0.82 (0.57 to 1.19)
FIGURE 5 A comparison of the effect of AP devices and CLP devices on the incidence of pressure sores
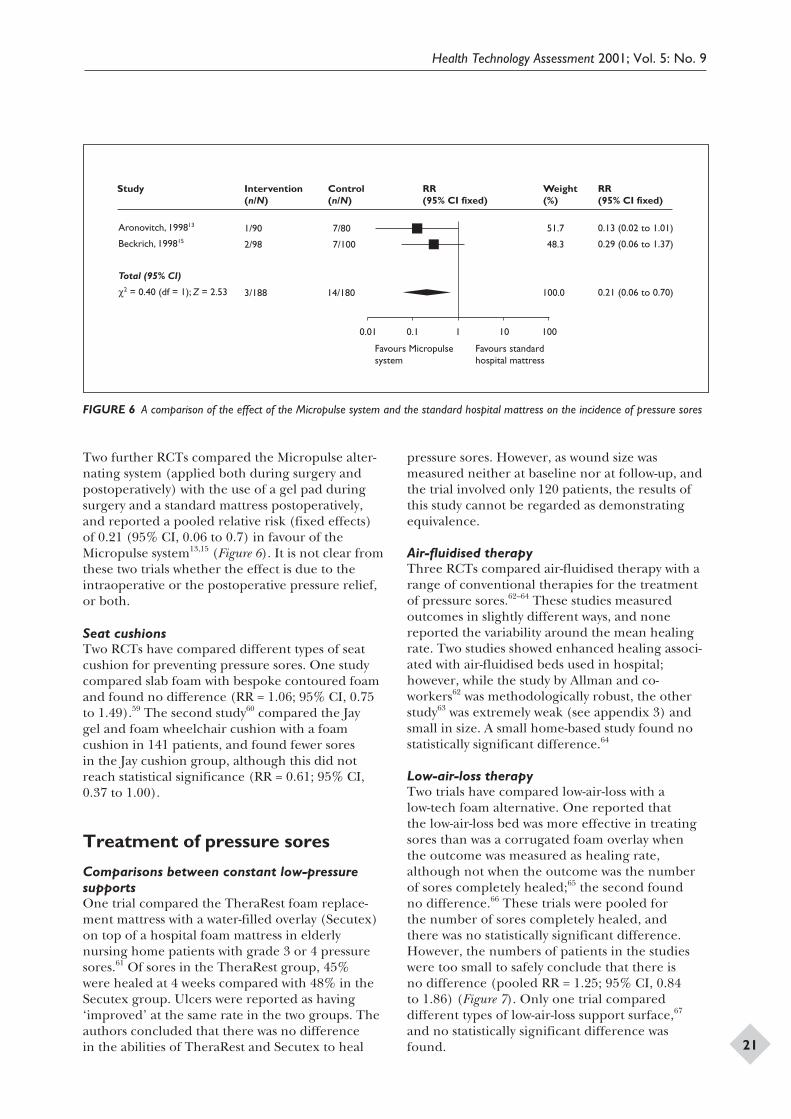
Two further RCTs compared the Micropulse alter-nating system (applied both during surgery andpostoperatively) with the use of a gel pad duringsurgery and a standard mattress postoperatively,and reported a pooled relative risk (fixed effects)of 0.21 (95% CI, 0.06 to 0.7) in favour of theMicropulse system13,15 (Figure 6). It is not clear fromthese two trials whether the effect is due to theintraoperative or the postoperative pressure relief,or both.
Seat cushionsTwo RCTs have compared different types of seatcushion for preventing pressure sores. One studycompared slab foam with bespoke contoured foamand found no difference (RR = 1.06; 95% CI, 0.75to 1.49).59 The second study60 compared the Jaygel and foam wheelchair cushion with a foamcushion in 141 patients, and found fewer soresin the Jay cushion group, although this did notreach statistical significance (RR = 0.61; 95% CI,0.37 to 1.00).
Treatment of pressure sores
Comparisons between constant low-pressuresupportsOne trial compared the TheraRest foam replace-ment mattress with a water-filled overlay (Secutex)on top of a hospital foam mattress in elderlynursing home patients with grade 3 or 4 pressuresores.61 Of sores in the TheraRest group, 45%were healed at 4 weeks compared with 48% in theSecutex group. Ulcers were reported as having‘improved’ at the same rate in the two groups. Theauthors concluded that there was no differencein the abilities of TheraRest and Secutex to heal
pressure sores. However, as wound size wasmeasured neither at baseline nor at follow-up, andthe trial involved only 120 patients, the results ofthis study cannot be regarded as demonstratingequivalence.
Air-fluidised therapyThree RCTs compared air-fluidised therapy with arange of conventional therapies for the treatmentof pressure sores.62–64 These studies measuredoutcomes in slightly different ways, and nonereported the variability around the mean healingrate. Two studies showed enhanced healing associ-ated with air-fluidised beds used in hospital;however, while the study by Allman and co-workers62 was methodologically robust, the otherstudy63 was extremely weak (see appendix 3) andsmall in size. A small home-based study found nostatistically significant difference.64
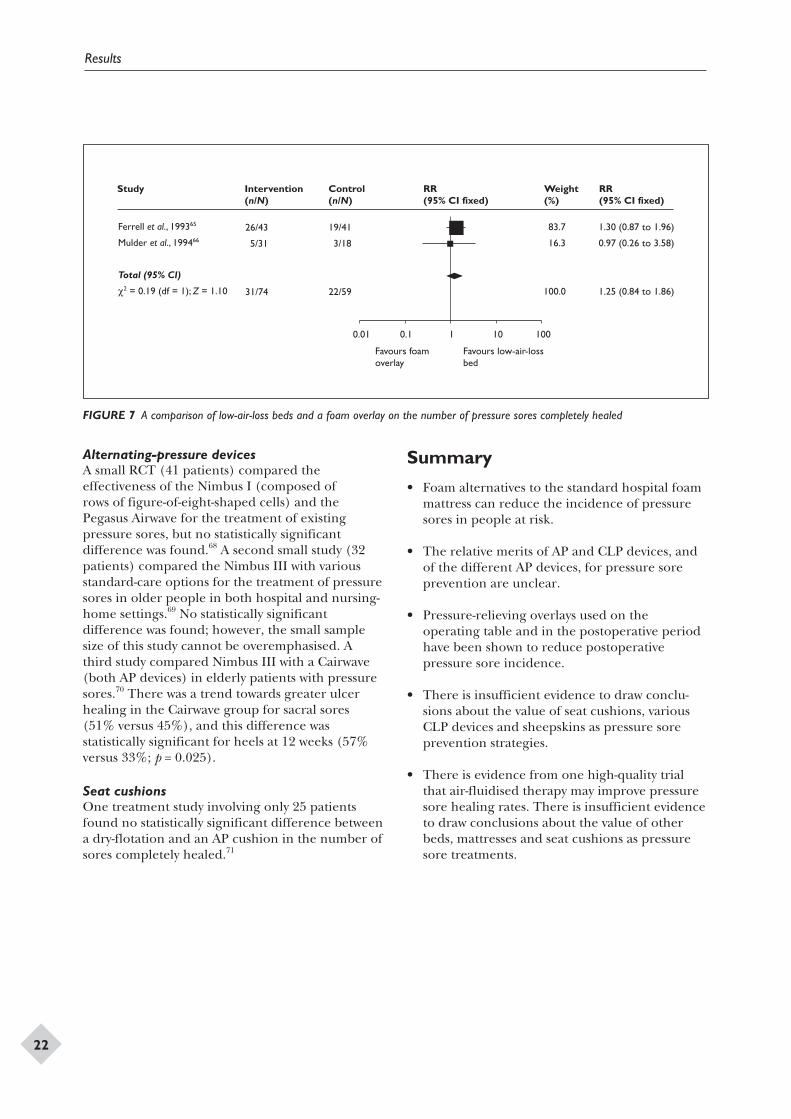
Low-air-loss therapyTwo trials have compared low-air-loss with alow-tech foam alternative. One reported thatthe low-air-loss bed was more effective in treatingsores than was a corrugated foam overlay whenthe outcome was measured as healing rate,although not when the outcome was the numberof sores completely healed;65 the second foundno difference.66 These trials were pooled forthe number of sores completely healed, andthere was no statistically significant difference.However, the numbers of patients in the studieswere too small to safely conclude that there isno difference (pooled RR = 1.25; 95% CI, 0.84to 1.86) (Figure 7). Only one trial compareddifferent types of low-air-loss support surface,67
and no statistically significant difference wasfound.
Health Technology Assessment 2001; Vol. 5: No. 9
21
0.01 0.1 1 10 100
Favours Micropulse system
Favours standard hospital mattress
Study Intervention (n/N)
Control (n/N)
RR (95% CI fixed)
Weight (%)
RR (95% CI fixed)
Aronovitch, 199813
Beckrich, 199815
Total (95% CI)
c2 = 0.40 (df = 1); Z = 2.53
1/90
2/98
3/188
7/80
7/100
14/180
51.7
48.3
100.0
0.13 (0.02 to 1.01)
0.29 (0.06 to 1.37)
0.21 (0.06 to 0.70)
FIGURE 6 A comparison of the effect of the Micropulse system and the standard hospital mattress on the incidence of pressure sores
Alternating-pressure devicesA small RCT (41 patients) compared theeffectiveness of the Nimbus I (composed ofrows of figure-of-eight-shaped cells) and thePegasus Airwave for the treatment of existingpressure sores, but no statistically significantdifference was found.68 A second small study (32patients) compared the Nimbus III with variousstandard-care options for the treatment of pressuresores in older people in both hospital and nursing-home settings.69 No statistically significantdifference was found; however, the small samplesize of this study cannot be overemphasised. Athird study compared Nimbus III with a Cairwave(both AP devices) in elderly patients with pressuresores.70 There was a trend towards greater ulcerhealing in the Cairwave group for sacral sores(51% versus 45%), and this difference wasstatistically significant for heels at 12 weeks (57%versus 33%; p = 0.025).
Seat cushionsOne treatment study involving only 25 patientsfound no statistically significant difference betweena dry-flotation and an AP cushion in the number ofsores completely healed.71
Summary
• Foam alternatives to the standard hospital foammattress can reduce the incidence of pressuresores in people at risk.
• The relative merits of AP and CLP devices, andof the different AP devices, for pressure soreprevention are unclear.
• Pressure-relieving overlays used on theoperating table and in the postoperative periodhave been shown to reduce postoperativepressure sore incidence.
• There is insufficient evidence to draw conclu-sions about the value of seat cushions, variousCLP devices and sheepskins as pressure soreprevention strategies.
• There is evidence from one high-quality trialthat air-fluidised therapy may improve pressuresore healing rates. There is insufficient evidenceto draw conclusions about the value of otherbeds, mattresses and seat cushions as pressuresore treatments.
Results
22
Study Intervention (n/N)
Control (n/N)
RR (95% CI fixed)
Weight (%)
RR (95% CI fixed)
Ferrell et al., 199365
Mulder et al., 199466
Total (95% CI)
c2 = 0.19 (df = 1); Z = 1.10
26/43
5/31
31/74
19/41
3/18
22/59
83.7
16.3
100.0
1.30 (0.87 to 1.96)
0.97 (0.26 to 3.58)
1.25 (0.84 to 1.86)
0.01 0.1 1 10 100
Favours foam overlay
Favours low-air-loss bed
FIGURE 7 A comparison of low-air-loss beds and a foam overlay on the number of pressure sores completely healed

The confidence with which we can draw firmconclusions from the studies detailed in this
review is greatly tempered by the poor quality ofmany of the trials and the lack of replication ofmost comparisons. The clearest conclusion onecan draw is that standard hospital mattresses havebeen consistently out-performed by a range offoam-based, low-pressure mattresses and overlays,and also by higher-tech pressure-relieving bedsand mattresses, both in the prevention and thetreatment of pressure sores. The application ofthis conclusion to current clinical practice is,however, hampered by the fact that the ‘standard’was poorly described in many of these studies, andwhat is standard varies by hospital, country andover time. Nevertheless, the effects of using alter-native foam mattresses are noteworthy in theirconsistency.
None of the trials reviewed provided convincingreassurance that manual repositioning wasprovided equally to each group of participants.This is a possible confounder, as care providerswere not blinded to treatment allocation in anyof the trials and may have moved patients in onegroup more frequently if they perceived a partic-ular mattress to be less effective.
The results of three trials evaluating the use ofpressure-relieving overlays on the operating tablesuggest that these are beneficial in reducing subse-quent pressure sore incidence in high-risk surgicalpatients. These three trials were of reasonableor good quality; in particular, the trial by Nixonand co-workers14 was adequately powered, withallocation concealment and blinded outcomeassessment, lending further weight to the result.At present the most effective means of pressurerelief on the operating table is unclear; Nixon andco-workers14 found a gel-filled overlay to be signifi-cantly better than a standard operating table,while in the other two trials a gel-filled overlayon the operating table was less effective than anAP overlay (the Micropulse system), both intra-and postoperatively. The Micropulse trials areconfounded by their provision of a standardmattress postoperatively in the gel overlay arm, andan AP overlay postoperatively in the Micropulsearm. Thus, while there is clearly a reduction inpressure sore incidence associated with the AP
system, it is not clear whether this is merely a resultof better postoperative pressure relief.
It appears that low-air-loss beds are effective inpreventing pressure sores compared with foammattresses, although the evidence for a treatmenteffect is weak. There are no studies comparinglow-air-loss therapy with AP surfaces and otherhigh-tech low-pressure supports.
Water-filled and bead-filled mattresses were bothassociated with reductions in the incidence ofpressure sores in trials published in the early 1980s.However, the particular products evaluated are nolonger available.
There are tentative indications that two interven-tions may be harmful. First, foot waffle heelelevators were associated with a trebling of theincidence of pressure sores, but this result was notstatistically significant due to the small sample sizeof the study. Secondly, low-air-loss hydrotherapywas evaluated in a trial in which 19% of low-air-losshydrotherapy patients developed sores comparedwith 7% of standard care patients. Again thedifference is not statistically significant, possiblyas a result of the small sample size of the trial(98 patients in total).56
The comparisons that have been undertaken aresummarised in appendix 5. Few comparisons havebeen replicated and, as most of the trials that havebeen undertaken were underpowered, there islittle information from which to draw conclusions.For example, air-fluidised therapy as a preventionstrategy has only been compared with dry flotation,and low-air-loss therapy only with standard care, inone trial, as a treatment. There are clearly manygaps in the knowledge base, and a rational researchagenda could be developed.
Common methodological flaws, such as openrandomisation, lack of baseline comparability, highattrition rates, lack of an intention-to-treat analysisand lack of a blind outcome assessment, furtherreduce the confidence with which we can regardmany of the individual study findings. Future trialsshould address these deficiencies and collect dataon aspects of equipment performance, such asreliability.
Health Technology Assessment 2001; Vol. 5: No. 9
23
Chapter 4
Discussion


Implications for practice
• In people at high risk of pressure sore develop-ment, consideration should be given to the useof higher specification foam mattresses ratherthan standard hospital foam mattresses.
• The relative merits of higher-tech CLP andAP for prevention and treatment are unclear.Organisations should consider the use ofpressure relief for high-risk patients in theoperating theatre, as this is associated with areduction in the postoperative incidence ofpressure sores.
• Air-fluidised supports may improve pressuresore healing rates.
• Seat cushions have not been adequatelyevaluated.
Implications for research
Independent, well-designed, multicentre RCTs areneeded to compare the clinical effectiveness andcost-effectiveness of different types of pressure-relieving devices for patients at different levels ofrisk in a variety of settings. Particular gaps in theavailable information, which are evident fromappendix 5, include comparisons of:
• AP devices with other high-tech equipment(such as low-air-loss and air-fluidised beds)for pressure sore prevention in very high-riskgroups
• AP mattresses with less costly AP overlays
• AP devices with lower-tech alternatives (suchas different types of high-specification foammattresses and other CLP devices).
The evaluation of AP devices is given particularemphasis as they are viewed as standard preventiveinterventions in some areas and not others, andvary widely in cost (from less than £1000 to morethan £4000).
Research is needed into valid and reliable methodsof measuring wound healing, of detecting earlyskin damage, which is prognostic of pressure soredevelopment, and of the impact of pressure soreson quality of life.
Future research must address the methodologicaldeficiencies associated with much of the researchdescribed in this review. Patients should be trulyrandomised (with concealed allocation), trialsshould be of sufficient size to detect clinicallyimportant differences, and there should be clearcriteria for measuring outcomes, which ideallyshould be assessed without knowledge of theintervention received (blinded). Interventionsunder evaluation should be thoroughly and clearlydescribed. Researchers should be encouraged todevelop measures to assess patients’ experiences ofpressure-relieving equipment (e.g. comfort). Thestudies should also have adequate follow-up andappropriate statistical analysis.
Given the high costs associated with the preventionand treatment of pressure sores generally, and ofpressure-relieving surfaces specifically, greateremphasis should be given in the future to robusteconomic evaluations.
Health Technology Assessment 2001; Vol. 5: No. 9
25
Chapter 5
Conclusions


Health Technology Assessment 2001; Vol. 5: No. 9
27
This study was commissioned by the NHS R&DHTA programme. The authors are indebted to
the HTA referees for their perseverance in readingthis report and the quality of their comments.The views expressed in this report are those ofthe authors, who are responsible for any errors.
The authors are extremely grateful to: JulieGlanville and Alison Fletcher for early assistancewith the search, location and collection of theliterature; to Fujian Song and Jon Deeks, whoparticipated in early versions of this review; and toSally Bell-Syer, Roz Thompson (Trial Search
Coordinator and Secretary, respectively, of theCochrane Wounds Group) and Kate Flemming forhelp in the ongoing search and retrieval of RCTs,contact with authors, maintenance of the WoundsGroup trials register and data checking. We arealso grateful to our expert panel (appendix 2) fortheir helpful comments on the review protocol andearly drafts.
Early versions of this review have appeared as anEffective Healthcare bulletin7 and as a CochraneReview72 (this review will be maintained in theCochrane Library).
Acknowledgements

1. Allman RM. Pressure ulcers among the elderly.N Engl J Med 1989;320:850–3.
2. Clark M, Watts S. The incidence of pressure soresduring a National Health Service Trust Hospitalduring 1991. J Adv Nurs 1994;20:33–6.
3. Department of Health. Pressure sores: a key qualityindicator. London: Department of Health; 1993.
4. NHS Executive. Pressure sores: a preventableproblem. London: NHS Executive; 1994. VFMUpdate No. 12.
5. NHS Management Executive. Priorities and plan-ning guidance 1994–5. Leeds: NHS ME. ReportNo. EL (93)54.
6. Clark M, Cullum N. Matching patient need forpressure sore prevention with the supply ofpressure redistributing mattresses. J Adv Nurs1992;17:310–16.
7. Effective Health Care. The prevention andtreatment of pressure sores. Effective Health Care1995;2(Pt 1):1–16.
8. Bliss MR, Thomas JM. Clinical trials with budgetaryimplications: establishing randomised trials ofpressure-relieving aids. Professional Nurse 1993;8(Pt 5):292–6.
9. NHS Centre for Reviews and Dissemination.Undertaking systematic reviews of effectiveness.York: University of York; 1996. Report No. 4.
10. Medical Devices Directorate. Foam mattresses.London: Medical Devices Directorate; 1993.Evaluation PS1. p. 1–24.
11. Brown-Etris M, Pribble J, LaBreque J. Evaluation oftwo wound measurement methods in a multicentrecontrolled study. Ostomy Wound Management 1994;40(Pt 7):44–8.
12. Clarke M, Oxman AD, editors. Summarising effectsacross studies. Cochrane Reviewers’ Handbook 4.0[updated July 1999]; Section 8.3. Oxford: UpdateSoftware; 2000. Cochrane Library [database on CDROM], issue 1.
13. Aronovitch SA. A comparative, randomized,controlled study to determine safety and efficacy ofpreventive pressure ulcer systems: preliminaryanalysis. Adv Wound Care 1998;11(Pt 3 Suppl):15–16.
14. Nixon J, McElvenny D, Mason S, Brown J, Bond S.A sequential randomised controlled trial
comparing a dry visco-elastic polymer pad andstandard operating table mattress in the preventionof postoperative pressure sores. Int J Nurs Stud1998;35:193–203.
15. Beckrich K. Personal communication: Micropulse.A 7-day comparative, parallel randomised singlecentre study to determine the safety and efficacyof the Micropulse system for the prevention ofpressure ulcers in patients undergoing cardio-thoracic procedures. 1998.
16. Gentilello L, Thompson DA, Tonnesen AS,Hernandez D, Kapadia AS, Allen SJ, et al. Effectof a rotating bed on the incidence of pulmonarycomplications in critically ill patients. Crit Care Med1998;16(Pt 8):783–6.
17. Inman KJ, Sibbald WJ, Rutledge FS, Clark BJ.Clinical utility and cost-effectiveness of an airsuspension bed in the prevention of pressureulcers. JAMA 1993;269:1139–43.
18. Laurent S. Effectiveness of pressure decreasingmattresses in cardiovascular surgery patients: acontrolled clinical trial. Proceedings of the 3rdEuropean Conference for Nurse Managers; 1997;Brussels.
19. Sideranko S, Quinn A, Burns K, Froman RD. Effectsof position and mattress overlay on sacral and heelpressures in a clinical population. Res Nurs Health1992;15(Pt 4):245–51.
20. Summer WR, Curry P, Haponik EF, Nelson S,Elston R. Continuous mechanical turning ofintensive care unit patients shortens length of stayin some diagnostic groups. J Crit Care 1989;4(Pt 2):45–53.
21. Takala J, Varmavuo S, Soppi E. Prevention ofpressure sores in acute respiratory failure: arandomised controlled trial. Clin Intensive Care1996;7:228–35.
22. Cooper PJ, Gray DG, Mollison J. A randomisedcontrolled trial of two pressure reducing surfaces.J Wound Care 1998;7(Pt 8):374–6.
23. Exton-Smith AN, Overstall PW, Wedgwood J,Wallace G. Use of the ‘air wave system’ to preventpressure sores in hospital. Lancet 1982;i(Pt 8284):1288–90.
24. Goldstone LA, Norris M, O’Reilly M, White J.A clinical trial of a bead bed system for theprevention of pressure sores in elderly orthopaedicpatients. J Adv Nurs 1982;7(Pt 6):545–8.
Health Technology Assessment 2001; Vol. 5: No. 9
29
References
25. Hofman A, Geelkerken RH, Wille J, Hamming JJ,Hermans J, Breslau PJ. Pressure sores and pressure-decreasing mattresses: controlled clinical trial.Lancet 1994;343(Pt 8897):568–71.
26. Price P, Bale S, Newcombe R, Harding K.Challenging the pressure sore paradigm. J WoundCare 1999;8(Pt 4):187–90.
27. Santy JE, Bulter MK, Whyman JD. A comparisonstudy of 6 types of hospital mattress to determinewhich most effectively reduces the incidence ofpressure sores in elderly patients with hip fracturesin a District General Hospital. Northern andYorkshire Regional Health Authority; 1994.Unpublished report.
28. Stapleton M. Preventing pressure sores – anevaluation of three products. Geriatr Nurs (London)1986;6(Pt 2):23–5.
29. Schulz KF, Chalmers I, Hayes RJ, Altman DG.Empirical evidence of bias: dimensions ofmethodological quality associated with estimatesof treatment effects in controlled trials. JAMA1995;273:408–12.
30. Bliss MR, McLaren R, Exton-Smith AN. Mattressesfor preventing pressure sores in geriatric patients.Med Bull Ministry Health 1966;25:238–67.
31. Bliss MR. Preventing pressure sores in elderlypatients: a comparison of seven mattress overlays[published erratum appears in Age Ageing1995;24:543]. Age Ageing 1995;24:297–302.
32. Branom R, Knox L. Proceedings of the 31st Wound,Ostomy and Continence Conference; 1999 June;Minneapolis.
33. Collins F. The contribution made by an armchairwith integral pressure-reducing cushion in theprevention of pressure sore incidence in theelderly, acutely ill patient. J Tissue Viability 1999;9(Pt 4):133–7.
34. Hawkins JE. The effectiveness of pressure-reducingtable pads as an intervention to reduce the risk ofinteroperatively acquired pressure sores. MilitaryMed 1997;162:759–61.
35. Jesurum J, Joseph K, Davis JM. Balloons, beds, andbreakdown. Effects of low-air loss therapy on thedevelopment of pressure ulcers in cardiovascularsurgical patients with intra-aortic balloon pumpsupport. Crit Care Nurs Clin North Am 1996;8(Pt 4):423–40.
36. Koo TKK, Mak AFT, Lee YL. Evaluation of an activeseating system for pressure relief. Assist 1995;7:119–28.
37. Marchand AC, Lidowski H. Reassessment of the useof genuine sheepskin for pressure ulcer preventionand treatment. Decubitus 1993;6(Pt 1):44–7.
38. Regan MB, Byers BH, Mayrovitz HN. Efficacy of acomprehensive pressure ulcer prevention programin an extended care facility. Adv Wound Care 1995;8(Pt 3):51–5.
39. Rosenthal MJ, Felton RM, Hileman DL, Lee M,Friedman M, Navach JH. A wheelchair cushiondesigned to redistribute sites of sitting pressure.Arch Phys Med Rehab 1996;77:278–82.
40. Stoneberg C, Pitcock N, Myton C. Pressure sores inthe homebound: one solution. Am J Nurs 1986;86(Pt 4):426–8.
41. Zernike W. Heel pressure relieving devices: howeffective are they? Aust J Adv Nurs 1997;14(Pt 4):12–19.
42. Andersen KE, Jensen O, Kvorning SA, Bach E.Decubitus prophylaxis: a prospective trial on theefficiency of alternating-pressure air-mattressesand water-mattresses. Acta Dermatol Venereol 1982;63(Pt 3):227–30.
43. Ewing MR, Garrow C, Presley TA, Ashley C, KisellaNM. Further experiences in the use of sheep skinsas an aid in nursing. Austr Nurse J 1964;Sept:215–19.
44. Gray DG, Campbell M. A randomised clinical trialof two types of foam mattresses. J Tissue Viability1994;4:128–32.
45. Collier ME. Pressure-reducing mattresses. J WoundCare 1996;5(Pt 5):207–11.
46. Gray DG, Smith M. Comparison of a new foammattress with the standard hospital mattress.J Wound Care 2000;9(Pt 1):29–31.
47. Kemp MG, Kopanke D, Tordecilla L, Fogg L, ShottS, Matthiesen V, et al. The role of support surfacesand patient attributes in preventing pressure ulcersin elderly patients. Res Nurs Health 1993;16(Pt 2):89–96.
48. Vyhlidal SK, Moxness D, Bosak KS, Van-Meter FG,Bergstrom N. Mattress replacement or foamoverlay? A prospective study on the incidence ofpressure ulcers. Appl Nurs Res 1997;10(Pt 3):111–20.
49. Lazzara DJ, Buschmann MT. Prevention of pressureulcers in elderly nursing home residents: are specialsupport surfaces the answer? Decubitus 1991;4(Pt 4):42–6.
50. Tymec AC, Pieper B, Vollman K. A comparison oftwo pressure-relieving devices on the prevention ofheel pressure ulcers. Adv Wound Care 1997;10(Pt 1):39–44.
51. Conine TA, Daechsel D, Lau MS. The role ofalternating air and Silicore overlays in preventingdecubitus ulcers. Int J Rehab Res 1990;13(Pt 1):57–65.
52. Daechsel D, Conine TA. Special mattresses:effectiveness in preventing decubitus ulcers in
References
30
chronic neurologic patients. Arch Phys Med Rehab1985;66(Pt 4):246–8.
53. Whitney JD, Fellows BJ, Larson E. Do mattressesmake a difference? J Gerontol Nurs 1984;10(Pt 9):20–5.
54. Gebhardt K. A randomized trial of alternatingpressure (AP) and constant low pressure (CLP)supports for the prevention of pressure sores.J Tissue Viability 1994;4(Pt 3):93.
55. Hampton S. Evaluation of the new Cairwavetherapy system in one hospital trust. Br J Nurs1997;6(Pt 3):167–70.
56. Bennett RG, Baran PJ, DeVone L, Bacetti H, KristoE, Tayback M, et al. Low air loss hydrotherapyversus standard care for incontinent hospitalisedpatients. JAGS 1998;46:569–76.
57. Economides NG, Skoutakis VA, Carter CA, SmithVH. Evaluation of the effectiveness of two supportsurfaces following myocutaneous flap surgery. AdvWound Care: J Prev Healing 1995;8(Pt 1):49–53.
58. Choi SC, Nelson LD. Kinetic therapy in critically illpatients: combined results based on meta-analysis.J Crit Care 1992;7:57–62.
59. Lim R, Sirett R, Conine TA, Daechsel D. Clinical trialof foam cushions in the prevention of decubitusulcers in elderly patients. J Rehab Res 1988;25:19–26.
60. Conine TA, Hershler C, Daechsel D, Peel C,Pearson A. Pressure ulcer prophylaxis in elderlypatients using polyurethane foam or Jay wheelchaircushions. Int J Rehab Res 1994;17(Pt 2):123–37
61. Groen HW, Groenier KH, Schuling J. Comparativestudy of a foam mattress and a water mattress.J Wound Care 1999;8(Pt 7):333–5.
62. Allman RM, Keruly JC, Smith CR. Cost effectivenessof air-fluidized beds versus conventional therapy forpressure sores. Clin Res 1987;35(Pt 3):A728.
63. Munro BH, Brown L, Heitman BB. Pressure ulcers:one bed or another? Geriatr Nurs NY 1989;10(Pt 4):190–2.
64. Strauss MJ, Gong J, Gary BD, Kalsbeek WD, Spear S.The cost of home air-fluidized therapy for pressuresores. A randomized controlled trial. J Fam Pract1991;33(Pt 1):52–9.
65. Ferrell BA, Osterweil D, Christenson P. Arandomized trial of low-air-loss beds for treatmentof pressure ulcers [published erratum appears inJAMA 1993;269(Pt 21):2739] [see comments].JAMA 1993;269(Pt 4):494–7.
66. Mulder GD, Taro N, Seeley JE, Andrews K. A studyof pressure ulcer response to low air loss beds vsconventional treatment. J Geriatr Dermatol 1994;2(Pt 3):87–91.
67. Caley L, Jones S, Freer J, Muller JS. Randomizedprospective trial of two types of low-air-loss therapy.1994. Unpublished conference paper.
68. Devine B. Alternating pressure air mattresses in themanagement of established pressure sores. J TissueViability 1995;5(Pt 3):94–8.
69. Evans D, Land L, Geary A. A clinical evaluationof the Nimbus 3 alternating pressure mattressreplacement system. J Wound Care 2000;9(Pt 4):181–6.
70. Russell L, Reynolds TM, Carr J, Evans A, Holmes M.Randomised controlled trial of two pressure-relieving systems. J Wound Care 2000;9(Pt 2):52–5.
71. Clark M, Donald IP. A randomised controlledtrial comparing the healing of pressure soresupon two pressure-redistributing seat cushions. In:Proceedings of the 7th European Conference onAdvances in Wound Management. London: EMAPHealthcare Ltd; 1999; p. 122–5.
72. Cullum N, Deeks, Sheldon T, Song, Fletcher A.Beds, mattresses and cushions for preventing andtreating pressure sores. Oxford: Update Software;2000. Cochrane Review, Cochrane Library, issue 1.
Health Technology Assessment 2001; Vol. 5: No. 9
31

The review was compiled using RCTs from theCochrane Wounds Group Specialist Trials
Register. The Wounds Group Trials Register wassearched for the period up to April 2000 and hasbeen assembled and maintained as described below.
Electronic searches
MEDLINEMEDLINE (SilverPlatter version 4.0) has beensearched for RCTs and controlled clinical trialsfrom 1966 to December 1997 using a mixture offree text terms and MeSH headings: Since January1998 it has been unnecessary to search MEDLINEas this is searched centrally by the UK CochraneCentre for all trials and the results are transferredto CENTRAL/CCTR. Since January 1998,CENTRAL/CDSR has been searched instead ofMEDLINE for all issues of the Cochrane Library.The search strategy used was as follows:
1. decubitus ulcer/ or foot ulcer/2. leg ulcer/ or varicose ulcer/3. pilonidal cyst/4. skin ulcer/5. diabetic foot/6. ((plantar or diabetic or heel or venous or stasis
or arterial) adj ulcer$).tw.7. ((decubitus or foot or diabetic or ischaemic or
pressure) adj ulcer$).tw.8. ((pressure or bed) adj sore$).tw.9. ((pilonidal adj cyst) or (pilonidal adj sinus) or
bedsore$).tw.10. ((diabetic adj foot) or (cavity adj wound)).tw.11. ((varicose or leg or skin) adj ulcer$).tw.12. (decubitus or (chronic adj wound$)).tw.13. ((sinus adj wound$) or (cavity adj wound$)).tw.14. or/1–1315. debridement/ or biological dressings/ or
bandages/16. occlusive dressings/ or clothing/ or wound
healing/17. antibiotics/ or growth substances/ or platelet-
derived growth factor/18. fibroblast growth factor/ or electrical
stimulation therapy.ti,ab,sh.19. lasers/ or nutrition/ or surgery/ or surgery,
plastic/20. surgical flaps/ or skin transplantations/ or
homeopathy/ or homeopathic/
21. acupuncture therapy/ or acupuncture/ oralternative medicine/
22. alternative medicine/ or massage/ or iloprost/or alginates/
23. zinc/ or zinc oxide/ or ointments/ or anti-infective agents/
24. dermatologic agents/ or colloids/ or cushions/or wheelchairs/
25. beds/ or wound dressings/26. (debridement or dressing$ or compress$ or
cream$ or (growth adj factor$)).tw.27. (pressure-relie$ or (recombinant adj protein$)
or bandag$ or stocking$).tw.28. (antibiotic$ or (electric adj therapy) or laser$
or nutrition$ or surg$).tw.29. (homeopath$ or acupuncture or massage or
reflexology or ultrasound).tw.30. (iloprost or alginate$ or zinc or paste$ or
ointment$ or hydrocolloid$).tw.31. ((compression adj therapy) or (compression
adj bandag$) or wrap$).tw.32. (bed$ or mattress$ or wheelchair$ or (wheel
adj chair) or cushion$).tw.33. ((wound adj dressing$) or vitamin$ or bind$ or
gauze$ or heals or healing).tw.34. (diet or lotion$ or infect$ or reduc$ or (wound
adj healing)).tw.35. (treat$ or prevent$ or epidemiol$ or aetiol$ or
etiol$ or therap$ or prevalence orincidence).tw.
36. or/15–3537. 14 and 3638. random allocation/ or randomized controlled
trials/39. controlled clinical trials/ or clinical trials phase
I/ or clinical trials phase II/40. clinical trials phase III/ or clinical trials phase
IV/ or clinical trials overviews/41. single-blind method/ or double-blind method/42. publication bias/ or review/ or review, academic/43. review tutorial/ or meta-analysis/ or systematic
review/44. ((random$ adj controlled adj trial$) or
(prospective adj random$)).tw.45. ((random adj allocation) or random$ or
(clinical adj trial$) or control$).tw.46. ((standard adj treatment) or compar$ or
single-blind$ or double-blind$).tw.47. (blind$ or placebo$ or systematic$ or (system-
atic adj review)).tw.
Health Technology Assessment 2001; Vol. 5: No. 9
33
Appendix 1
Databases searched and search strategies
48. (randomized controlled trial or clinicaltrial).pt. or comparative study.sh.
49. or/38–4850. 37 and 4951. limit 50 to human52. burns/ or wounds, gunshot/ or corneal ulcer/
or exp dentistry/53. peptic ulcer/ or duodenal ulcer/ or stomach
ulcer/54. ((peptic adj ulcer) or (duodenal adj ulcer) or
traum$).tw.55. ((aortocaval adj fistula) or (arteriovenous adj
fistula)).tw.56. (bite adj wound$).tw.57. or/52–5658. 51 not 57
CENTRAL/CDSRThe CENTRAL/CDSR was searched on theCochrane Library CD-ROM. The search strategyused was as follows:
1. ((DECUBITUS and ULCER*) or (VARICOSEand ULCER*))
2. ((LEG or LEGS) and ULCER*)3. ((FOOT or FEET) and ULCER*)4. ((LEG or LEGS) and VARICOSE)5. (SKIN and ULCER*)6. SKIN-ULCER*:ME7. ((FOOT or FEET) and DIABETIC)8. ((((((PLANTAR or DIABETIC) or HEEL) or
VENOUS) or STASIS) or ARTERIAL) andULCER*)
9. ((ISCHEMIC or PRESSURE) and ULCER*)10. ((BED or BEDS) near (SORE or SORES))11. (PRESSURE near (SORE or SORES))12. (PILONIDAL and CYST*)13. (PILONIDAL and SINUS*)14. (PILONIDAL and ABSCES*)15. ((WOUND or WOUNDS) and CAVITY)16. ((WOUND or WOUNDS) and SINUS*)17. ((WOUND or WOUNDS) and CHRONIC)18. ((WOUND or WOUNDS) and DECUBITUS)19. WOUND-INFECTION*:ME20. ((WOUND or WOUNDS) and MALIGNANT)21. WOUND-HEALING*:ME22. WOUNDS-GUNSHOT*:ME23. ((GUN or GUNS) or GUNSHOT)24. WOUNDS-STAB*:ME25. LACERATION*26. SURGICAL-WOUND-DEHISCENCE*:ME27. BITES-AND-STINGS*2:ME28. ((BITE or BITES) or BITING)29. TRAUMATOLOGY*:ME30. BURNS*:ME31. (WOUND* and BURN*)32. (BURN* or SCALD*)
33. ((SITE or SITES) near DONOR)34. SELF-MUTILATION*:ME35. ((STAB or STABS) or STABBING)36. SOFT-TISSUE-INJURIES*:ME37. (((((((((((#1 or #2) or #3) or #4) or #5) or #6)
or #7) or #8) or #9) or #10) or #11) or #12)38. (((((((((((#13 or #14) or #15) or #16) or #17)
or #18) or #19) or #20) or #21) or #22) or #23)or #24)
39. (((((((((((#25 or #26) or #27) or #28) or #29)or #30) or #31) or #32) or #33) or #34) or #35)or #36)
40. (#37 or #38 OR #39)41. DENTAL42. (#40 not #41)43. CORNEAL44. (#42 not 43)45. DUODENAL-ULCER*1:ME46. (#44 not #45)47. CORNEAL-ULCER*1:ME48. (#46 not #47)49. CORNEAL-DISEASES*:ME50. (#48 not #49)51. ACNE52. (#50 not #51)53. BEDNET54. (#52 not #53)
CINAHLCINAHL (SilverPlatter version 4.0) was searchedfor the period from its inception to July 1999. Thesearch strategy used was as follows:
1. (pressure-ulcer* or foot-ulcer* or leg-ulcer* orskin-ulcer*) in de
2. (diabetic-foot* or diabetic-neuropathies*) in de3. ((diabetic-angiopathies*) in de) or diabetes-
mellitus/complications/ all age subheadings4. (pilonidal-cyst* or surgical-wound-infection*)
in de5. (plantar or diabetic or heel or venous or stasis
or (arterial near ulcer*)) in ti,ab6. (decubitus or foot or diabetic or ischaemic or
(pressure near ulcer*)) in ti,ab7. (pressure or (bed near sore*))in ti,ab8. ((pilonidal near cyst) or (pilonidal near sinus)
or bedsore) in ti,ab9. (diabetic near foot) or ((cavity near wound)in
ti,ab)10. (varicose or leg or (skin near ulcer*)) in ti,ab11. ((decubitus or chronic) near wound*) in ti,ab12. (sinus near wound*) or ((cavity near wound*)
in ti,ab)13. ((burn near wound*) or (gunshot near wound*)
or (bite near wound*) or trauma) in ti,ab14. #1 or #2 or #3 or #4 or #5 or #6 or #7 or #8 or
#9 or #10 or #11 or #12 or #13
Appendix 1
34
15. (clinical-trials or single-blind-studies or double-blind-studies) in de
16. (control-group or placebos or meta-analysis) in de17. (random* near clinical near trial*) or
((prospective near random*) in ti,ab)18. ((random near allocation) or random* or
controlled-clinical-trial* or control) in ti,ab19. (comparison group* or (standard near
treatment) or compar*)in ti,ab20. (single-blind* or (single near blind) or double-
blind or (double near blind)) in ti,ab21. (blind* or placebo* or systematic or (systematic
near review)) in ti,ab22. ((meta analysis or meta-analysis) or (trial* or
prospective)) in ti,ab23. ((clinical-trials) or (comparative-studies)) in de24. #15 or #16 or #17 or #18 or #19 or #20 or #21
or #22 or #2325. #14 and #2426. explode dentistry/ all topical subheadings/ all
age subheadings27. (peptic-ulcer*) or (duodenal-ulcer*) or
((corneal-ulcer*)in de)28. (peptic near ulcer) or (duodenal near ulcer)
or ((corneal near ulcer) in ti,ab)29. dentist* in de30. #26 or #27 or #28 or #2931. #25 not #30
Other databasesOther databases that were searched, from theearliest date available until 1997, were:
• EMBASE (SilverPlatter version 4.0)• ISI Science Citation Index (on BIDS)• BIOSIS (on EDINA)• British Diabetic Association Database• CISCOM (Complementary Medicine Database
of the RCCM)• Conference Proceedings (on BIDS)• Dissertation Abstracts• Royal College of Nursing Database (CD-ROM)• British Nursing Index (on ARC) to December
1998.
Handsearching
JournalsThe following wound care specialist journals werebeing prospectively handsearched for all RCTs:
• CARE – Science and Practice, 1979–90 (later,Journal of Tissue Viability, searched until present)
• Decubitus, 1987–93• Journal of Tissue Viability, 1991–present• Journal of Wound Care, 1991–present• Phlebology, 1986–present.
Conference proceedingsWound care conference proceedings that werehandsearched for RCTs were as follows:
• Proceedings of the 1st European Conference onAdvances in Wound Management, September1991, Cardiff, UK
• Proceedings of the 2nd European Conferenceon Advances in Wound Management, October1992, Harrogate, UK
• Proceedings of the 3rd European Conferenceon Advances in Wound Management, October1993, Harrogate, UK
• Proceedings of the 4th European Conference onAdvances in Wound Management, September1994, Copenhagen, Denmark
• Proceedings of the 5th European Conference onAdvances in Wound Management, November1995, Harrogate, UK
• Proceedings of the 6th European Conference onAdvances in Wound Management, October1996, Amsterdam, The Netherlands
• Proceedings of the 7th European Conference onAdvances in Wound Management, November1997, Harrogate, UK
• Proceedings of the 8th European Conference onAdvances in Wound Management, April 1998,Madrid, Spain
• 3rd Annual Symposium on Advanced WoundCare, March 1990, Orlando, FL, USA
• 4th Annual Symposium on Advanced WoundCare, April 1991, San Francisco, CA, USA
• 5th Annual Symposium on Advanced WoundCare, April 1992, New Orleans, USA
• 8th Annual Symposium on Advanced WoundCare & Medical Research Forum on WoundRepair, April 1995, San Diego, CA, USA
• 9th Annual Symposium on Advanced WoundCare, April 1996, Atlanta, GA, USA
• Proceedings of: Going into the ‘90s: ThePharmacist and Wound Care, September 1992,London, UK
• Proceedings of the Second Joint British/SwedishAngiology Meeting, 1991, London, UK
• Symposium on Venous Leg Ulcers, 1985,London, UK
• Venous Forum of the Royal Society of Medicine,16 April 1999, Leeds, UK.
Other strategies
Identification of unpublished studiesSeveral databases were searched (up toDecember 1997) in an attempt to identifyunpublished studies. The databases includedthe following:
Health Technology Assessment 2001; Vol. 5: No. 9
35

• CRIB (Current Research in Britain)• DHS Database• SIGLE• UK National Research Register.
Experts in the field of wound care were contactedto enquire about ongoing and recently published
trials in the field of wound care. In addition,manufacturers of wound care materials werecontacted for details of the trials they wereconducting.
Citations within the reviews and papers obtainedwere scrutinised to identify additional studies.
Appendix 1
36
Dr Mary Bliss Homerton Hospital, London
Carol Dealey Southern Birmingham Community Health NHS Trust
Krzys Gebhardt St George’s Hospital, London
Peter Lowthian Watford
Jane Nixon St James’s University Hospital, Leeds
Dr John Young St Luke’s Hospital, Bradford
Health Technology Assessment 2001; Vol. 5: No. 9
37
Appendix 2
Advisory panel

Appendix 3
Summary of included studies
Health Technology Assessment 2001; Vol. 5: No. 9
39
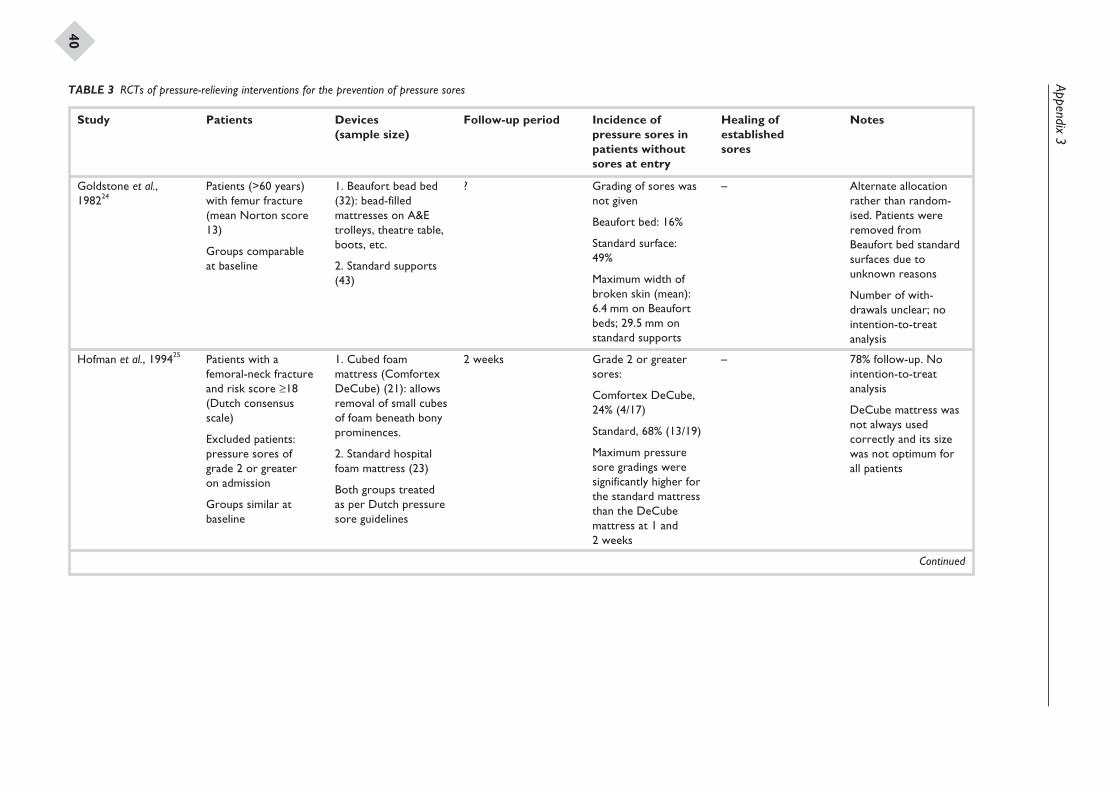
Appendix3
40
Study Patients Devices(sample size)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
Goldstone et al.,198224
Patients (>60 years)with femur fracture(mean Norton score13)
Groups comparableat baseline
1. Beaufort bead bed(32): bead-filledmattresses on A&Etrolleys, theatre table,boots, etc.
2. Standard supports(43)
? Grading of sores wasnot given
Beaufort bed: 16%
Standard surface:49%
Maximum width ofbroken skin (mean):6.4 mm on Beaufortbeds; 29.5 mm onstandard supports
– Alternate allocationrather than random-ised. Patients wereremoved fromBeaufort bed standardsurfaces due tounknown reasons
Number of with-drawals unclear; nointention-to-treatanalysis
Hofman et al., 199425 Patients with afemoral-neck fractureand risk score ≥18(Dutch consensusscale)
Excluded patients:pressure sores ofgrade 2 or greateron admission
Groups similar atbaseline
1. Cubed foammattress (ComfortexDeCube) (21): allowsremoval of small cubesof foam beneath bonyprominences.
2. Standard hospitalfoam mattress (23)
Both groups treatedas per Dutch pressuresore guidelines
2 weeks Grade 2 or greatersores:
Comfortex DeCube,24% (4/17)
Standard, 68% (13/19)
Maximum pressuresore gradings weresignificantly higher forthe standard mattressthan the DeCubemattress at 1 and2 weeks
– 78% follow-up. Nointention-to-treatanalysis
DeCube mattress wasnot always usedcorrectly and its sizewas not optimum forall patients
Continued
TABLE 3 RCTs of pressure-relieving interventions for the prevention of pressure sores
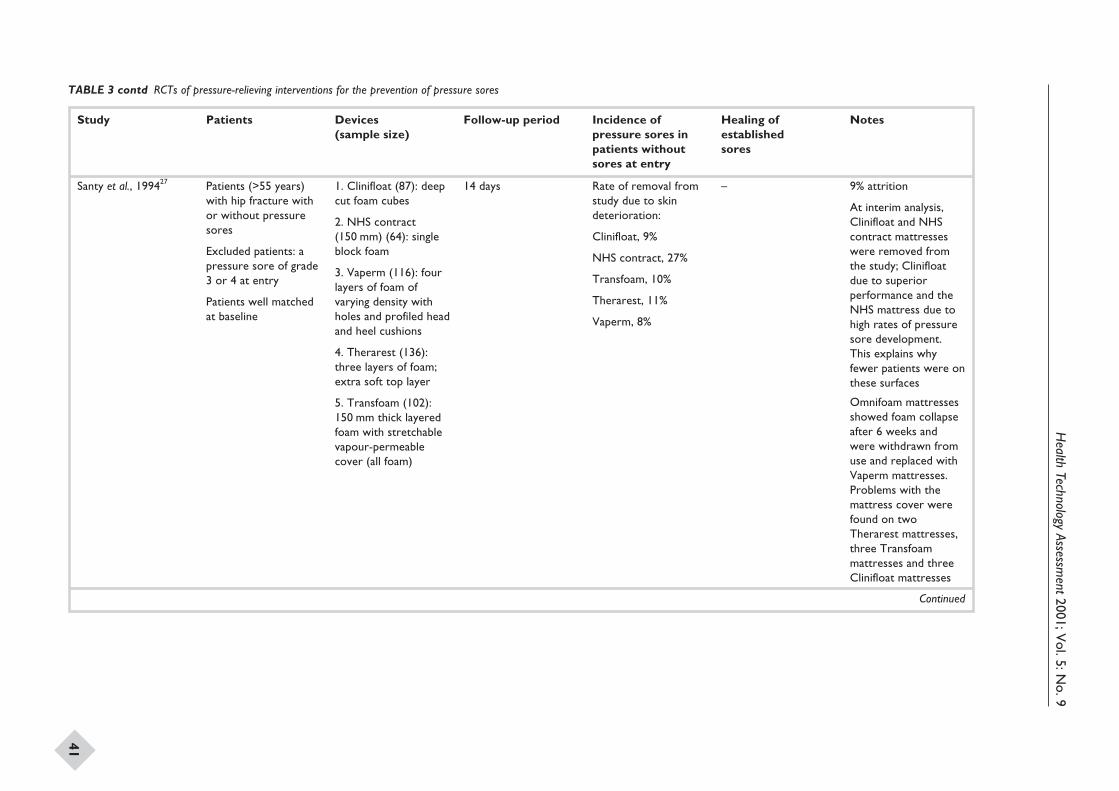
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
41
Study Patients Devices(sample size)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
Santy et al., 199427 Patients (>55 years)with hip fracture withor without pressuresores
Excluded patients: apressure sore of grade3 or 4 at entry
Patients well matchedat baseline
1. Clinifloat (87): deepcut foam cubes
2. NHS contract(150 mm) (64): singleblock foam
3. Vaperm (116): fourlayers of foam ofvarying density withholes and profiled headand heel cushions
4. Therarest (136):three layers of foam;extra soft top layer
5. Transfoam (102):150 mm thick layeredfoam with stretchablevapour-permeablecover (all foam)
14 days Rate of removal fromstudy due to skindeterioration:
Clinifloat, 9%
NHS contract, 27%
Transfoam, 10%
Therarest, 11%
Vaperm, 8%
– 9% attrition
At interim analysis,Clinifloat and NHScontract mattresseswere removed fromthe study; Clinifloatdue to superiorperformance and theNHS mattress due tohigh rates of pressuresore development.This explains whyfewer patients were onthese surfaces
Omnifoam mattressesshowed foam collapseafter 6 weeks andwere withdrawn fromuse and replaced withVaperm mattresses.Problems with themattress cover werefound on twoTherarest mattresses,three Transfoammattresses and threeClinifloat mattresses
Continued
TABLE 3 contd RCTs of pressure-relieving interventions for the prevention of pressure sores
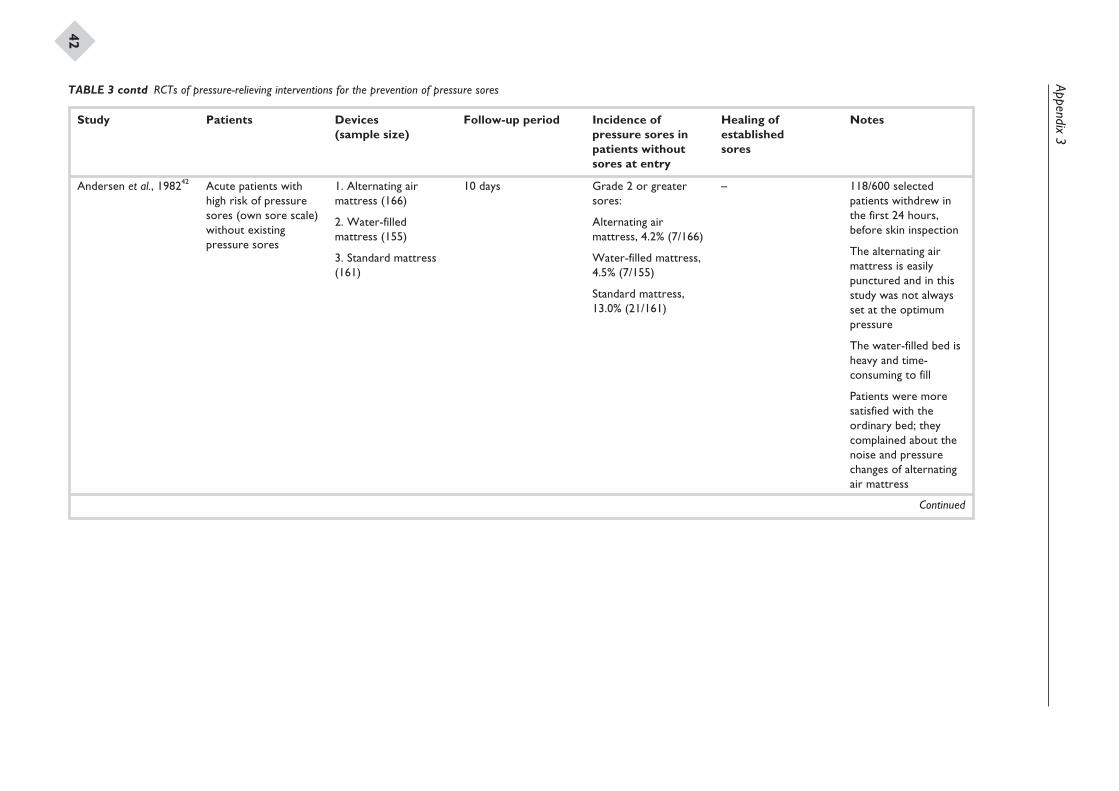
Appendix3
42
Study Patients Devices(sample size)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
Andersen et al., 198242 Acute patients withhigh risk of pressuresores (own sore scale)without existingpressure sores
1. Alternating airmattress (166)
2. Water-filledmattress (155)
3. Standard mattress(161)
10 days Grade 2 or greatersores:
Alternating airmattress, 4.2% (7/166)
Water-filled mattress,4.5% (7/155)
Standard mattress,13.0% (21/161)
– 118/600 selectedpatients withdrew inthe first 24 hours,before skin inspection
The alternating airmattress is easilypunctured and in thisstudy was not alwaysset at the optimumpressure
The water-filled bed isheavy and time-consuming to fill
Patients were moresatisfied with theordinary bed; theycomplained about thenoise and pressurechanges of alternatingair mattress
Continued
TABLE 3 contd RCTs of pressure-relieving interventions for the prevention of pressure sores
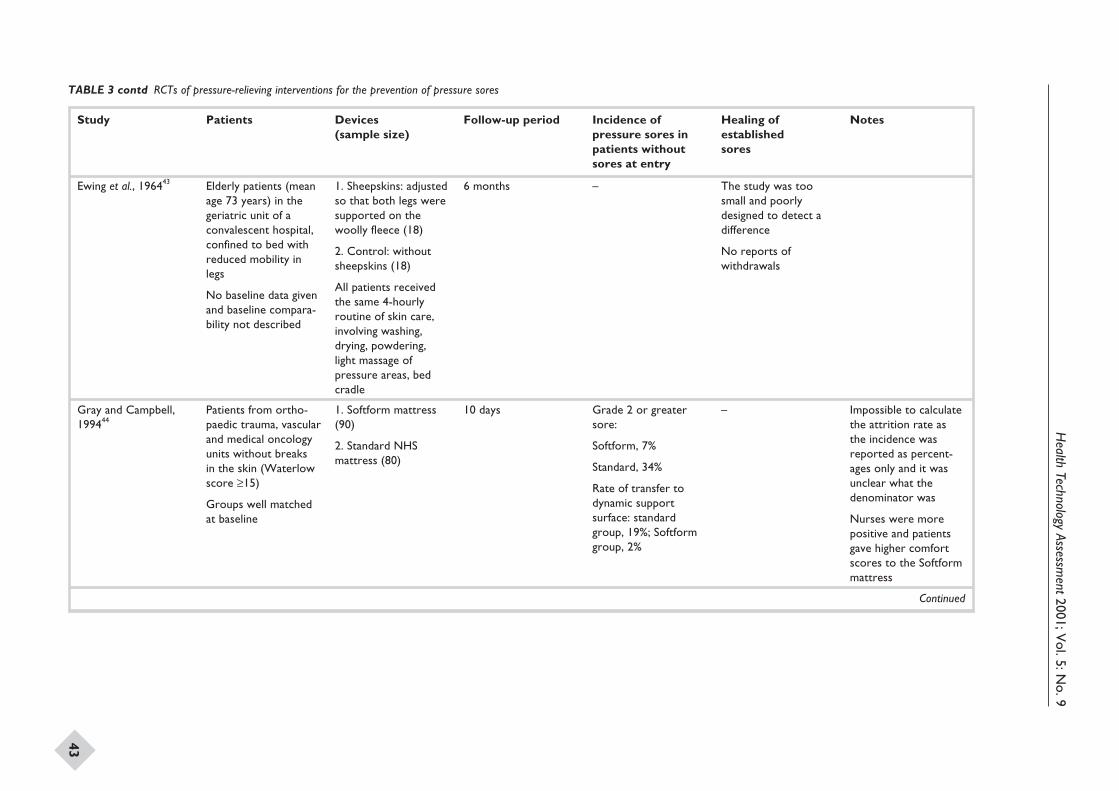
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
43
Study Patients Devices(sample size)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
Ewing et al., 196443 Elderly patients (meanage 73 years) in thegeriatric unit of aconvalescent hospital,confined to bed withreduced mobility inlegs
No baseline data givenand baseline compara-bility not described
1. Sheepskins: adjustedso that both legs weresupported on thewoolly fleece (18)
2. Control: withoutsheepskins (18)
All patients receivedthe same 4-hourlyroutine of skin care,involving washing,drying, powdering,light massage ofpressure areas, bedcradle
6 months – The study was toosmall and poorlydesigned to detect adifference
No reports ofwithdrawals
Gray and Campbell,199444
Patients from ortho-paedic trauma, vascularand medical oncologyunits without breaksin the skin (Waterlowscore ≥15)
Groups well matchedat baseline
1. Softform mattress(90)
2. Standard NHSmattress (80)
10 days Grade 2 or greatersore:
Softform, 7%
Standard, 34%
Rate of transfer todynamic supportsurface: standardgroup, 19%; Softformgroup, 2%
– Impossible to calculatethe attrition rate asthe incidence wasreported as percent-ages only and it wasunclear what thedenominator was
Nurses were morepositive and patientsgave higher comfortscores to the Softformmattress
Continued
TABLE 3 contd RCTs of pressure-relieving interventions for the prevention of pressure sores
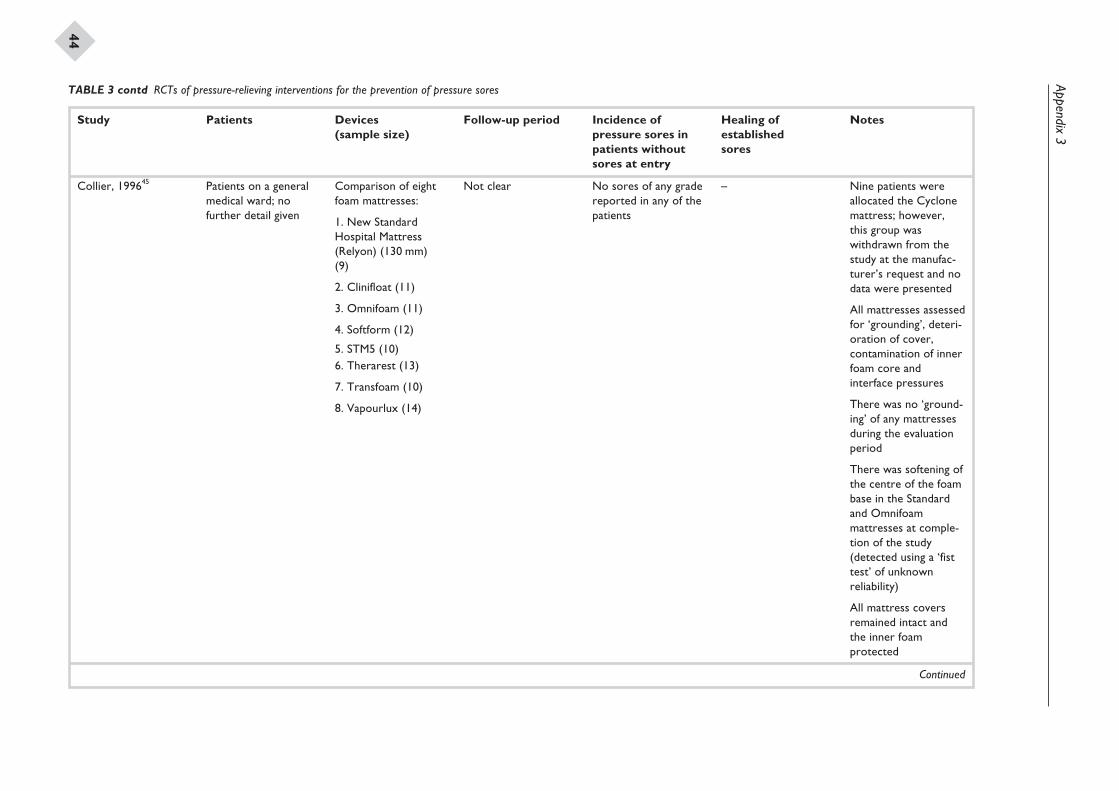
Appendix3
44
Study Patients Devices(sample size)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
Collier, 199645 Patients on a generalmedical ward; nofurther detail given
Comparison of eightfoam mattresses:
1. New StandardHospital Mattress(Relyon) (130 mm)(9)
2. Clinifloat (11)
3. Omnifoam (11)
4. Softform (12)
5. STM5 (10)6. Therarest (13)
7. Transfoam (10)
8. Vapourlux (14)
Not clear No sores of any gradereported in any of thepatients
– Nine patients wereallocated the Cyclonemattress; however,this group waswithdrawn from thestudy at the manufac-turer’s request and nodata were presented
All mattresses assessedfor ‘grounding’, deteri-oration of cover,contamination of innerfoam core andinterface pressures
There was no ‘ground-ing’ of any mattressesduring the evaluationperiod
There was softening ofthe centre of the foambase in the Standardand Omnifoammattresses at comple-tion of the study(detected using a ‘fisttest’ of unknownreliability)
All mattress coversremained intact andthe inner foamprotected
Continued
TABLE 3 contd RCTs of pressure-relieving interventions for the prevention of pressure sores
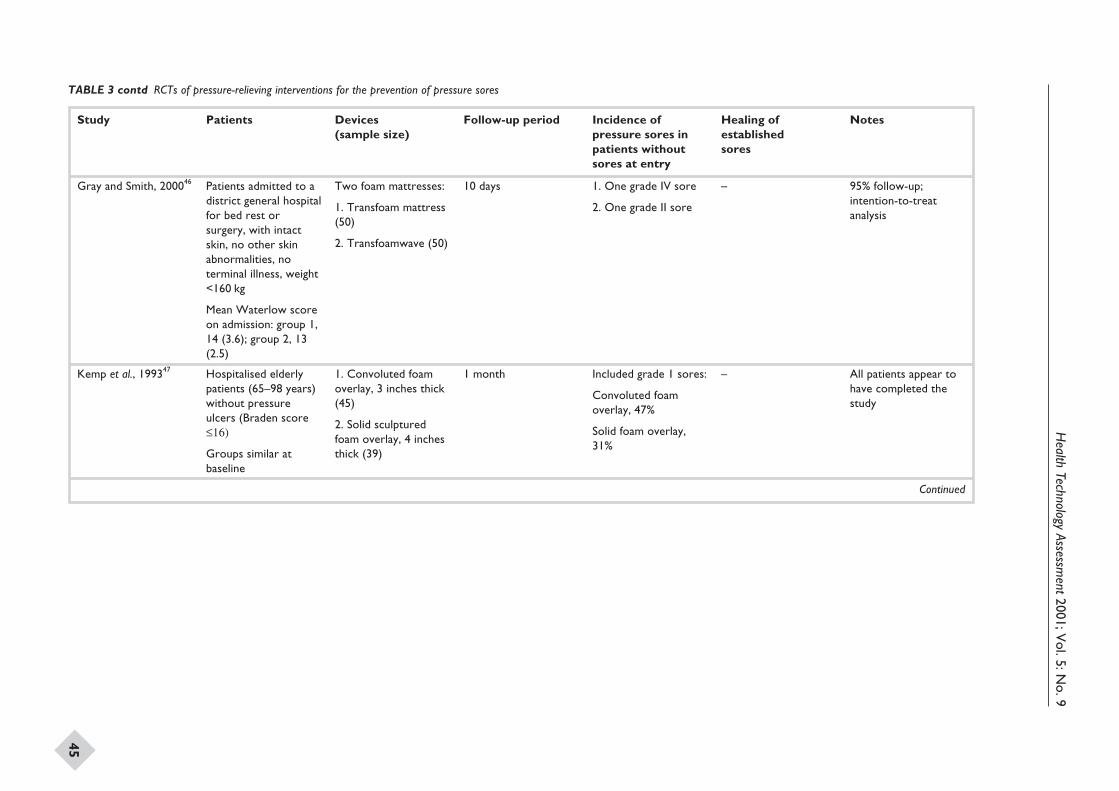
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
45
Study Patients Devices(sample size)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
Gray and Smith, 200046 Patients admitted to adistrict general hospitalfor bed rest orsurgery, with intactskin, no other skinabnormalities, noterminal illness, weight<160 kg
Mean Waterlow scoreon admission: group 1,14 (3.6); group 2, 13(2.5)
Two foam mattresses:
1. Transfoam mattress(50)
2. Transfoamwave (50)
10 days 1. One grade IV sore
2. One grade II sore
– 95% follow-up;intention-to-treatanalysis
Kemp et al., 199347 Hospitalised elderlypatients (65–98 years)without pressureulcers (Braden score£16)
Groups similar atbaseline
1. Convoluted foamoverlay, 3 inches thick(45)
2. Solid sculpturedfoam overlay, 4 inchesthick (39)
1 month Included grade 1 sores:
Convoluted foamoverlay, 47%
Solid foam overlay,31%
– All patients appear tohave completed thestudy
Continued
TABLE 3 contd RCTs of pressure-relieving interventions for the prevention of pressure sores
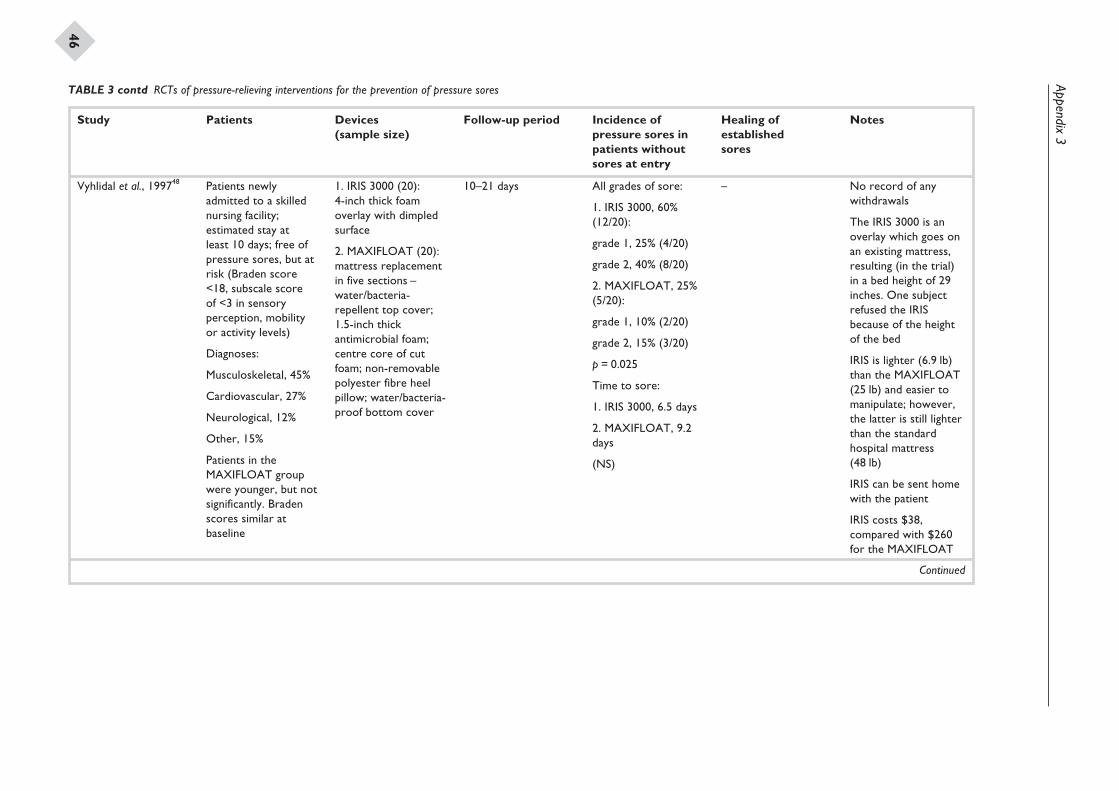
Appendix3
46
Study Patients Devices(sample size)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
Vyhlidal et al., 199748 Patients newlyadmitted to a skillednursing facility;estimated stay atleast 10 days; free ofpressure sores, but atrisk (Braden score<18, subscale scoreof <3 in sensoryperception, mobilityor activity levels)
Diagnoses:
Musculoskeletal, 45%
Cardiovascular, 27%
Neurological, 12%
Other, 15%
Patients in theMAXIFLOAT groupwere younger, but notsignificantly. Bradenscores similar atbaseline
1. IRIS 3000 (20):4-inch thick foamoverlay with dimpledsurface
2. MAXIFLOAT (20):mattress replacementin five sections –water/bacteria-repellent top cover;1.5-inch thickantimicrobial foam;centre core of cutfoam; non-removablepolyester fibre heelpillow; water/bacteria-proof bottom cover
10–21 days All grades of sore:
1. IRIS 3000, 60%(12/20):
grade 1, 25% (4/20)
grade 2, 40% (8/20)
2. MAXIFLOAT, 25%(5/20):
grade 1, 10% (2/20)
grade 2, 15% (3/20)
p = 0.025
Time to sore:
1. IRIS 3000, 6.5 days
2. MAXIFLOAT, 9.2days
(NS)
– No record of anywithdrawals
The IRIS 3000 is anoverlay which goes onan existing mattress,resulting (in the trial)in a bed height of 29inches. One subjectrefused the IRISbecause of the heightof the bed
IRIS is lighter (6.9 lb)than the MAXIFLOAT(25 lb) and easier tomanipulate; however,the latter is still lighterthan the standardhospital mattress(48 lb)
IRIS can be sent homewith the patient
IRIS costs $38,compared with $260for the MAXIFLOAT
Continued
TABLE 3 contd RCTs of pressure-relieving interventions for the prevention of pressure sores
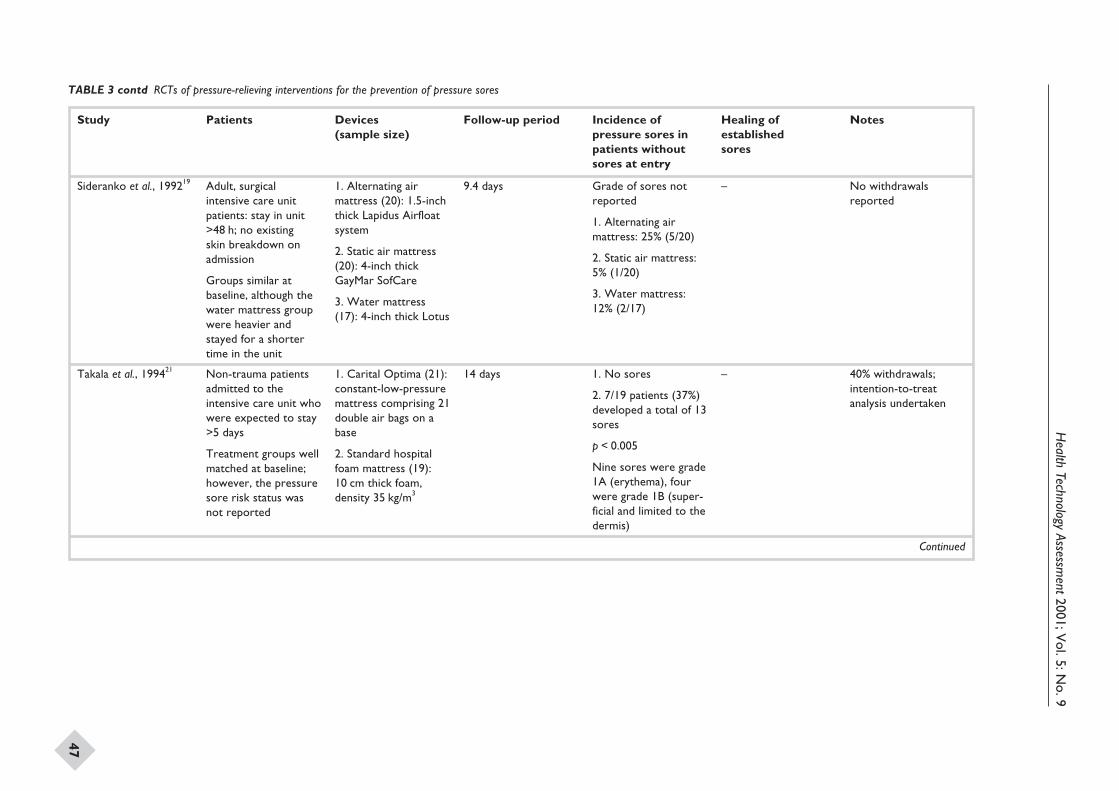
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
47
Study Patients Devices(sample size)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
Sideranko et al., 199219 Adult, surgicalintensive care unitpatients: stay in unit>48 h; no existingskin breakdown onadmission
Groups similar atbaseline, although thewater mattress groupwere heavier andstayed for a shortertime in the unit
1. Alternating airmattress (20): 1.5-inchthick Lapidus Airfloatsystem
2. Static air mattress(20): 4-inch thickGayMar SofCare
3. Water mattress(17): 4-inch thick Lotus
9.4 days Grade of sores notreported
1. Alternating airmattress: 25% (5/20)
2. Static air mattress:5% (1/20)
3. Water mattress:12% (2/17)
– No withdrawalsreported
Takala et al., 199421 Non-trauma patientsadmitted to theintensive care unit whowere expected to stay>5 days
Treatment groups wellmatched at baseline;however, the pressuresore risk status wasnot reported
1. Carital Optima (21):constant-low-pressuremattress comprising 21double air bags on abase
2. Standard hospitalfoam mattress (19):10 cm thick foam,density 35 kg/m3
14 days 1. No sores
2. 7/19 patients (37%)developed a total of 13sores
p < 0.005
Nine sores were grade1A (erythema), fourwere grade 1B (super-ficial and limited to thedermis)
– 40% withdrawals;intention-to-treatanalysis undertaken
Continued
TABLE 3 contd RCTs of pressure-relieving interventions for the prevention of pressure sores
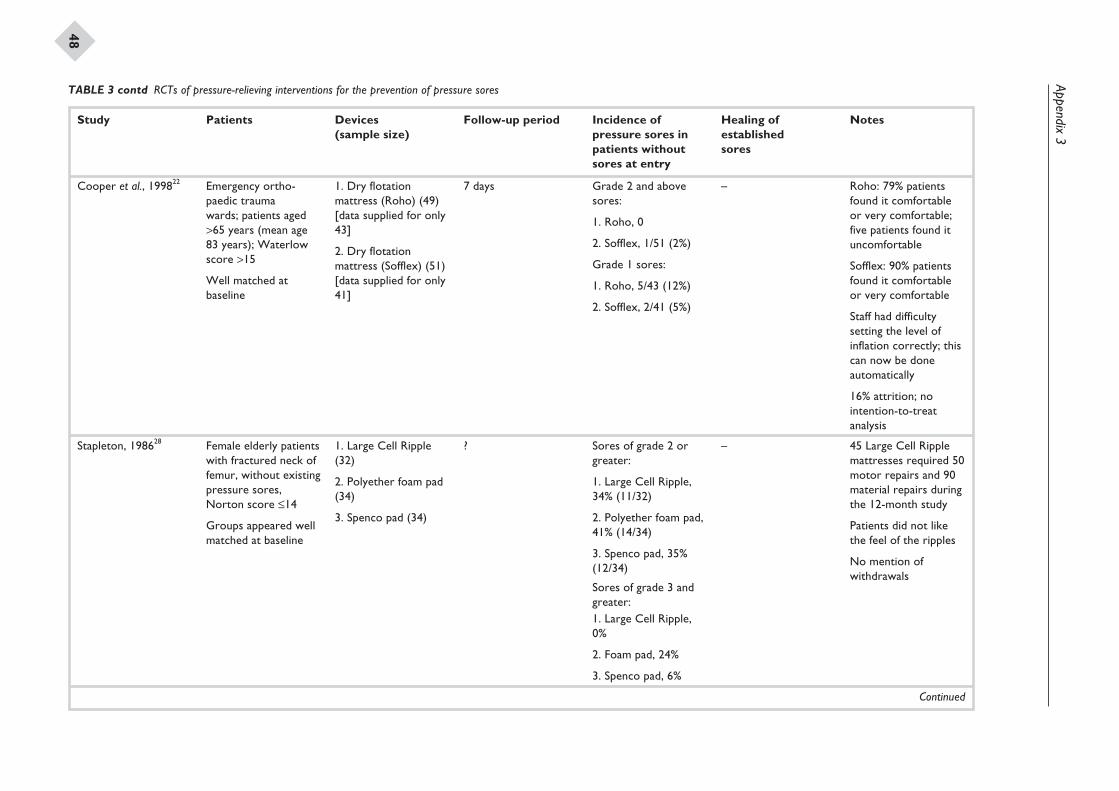
Appendix3
48
Study Patients Devices(sample size)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
Cooper et al., 199822 Emergency ortho-paedic traumawards; patients aged>65 years (mean age83 years); Waterlowscore >15
Well matched atbaseline
1. Dry flotationmattress (Roho) (49)[data supplied for only43]
2. Dry flotationmattress (Sofflex) (51)[data supplied for only41]
7 days Grade 2 and abovesores:
1. Roho, 0
2. Sofflex, 1/51 (2%)
Grade 1 sores:
1. Roho, 5/43 (12%)
2. Sofflex, 2/41 (5%)
– Roho: 79% patientsfound it comfortableor very comfortable;five patients found ituncomfortable
Sofflex: 90% patientsfound it comfortableor very comfortable
Staff had difficultysetting the level ofinflation correctly; thiscan now be doneautomatically
16% attrition; nointention-to-treatanalysis
Stapleton, 198628 Female elderly patientswith fractured neck offemur, without existingpressure sores,Norton score £14
Groups appeared wellmatched at baseline
1. Large Cell Ripple(32)
2. Polyether foam pad(34)
3. Spenco pad (34)
? Sores of grade 2 orgreater:
1. Large Cell Ripple,34% (11/32)
2. Polyether foam pad,41% (14/34)
3. Spenco pad, 35%(12/34)
Sores of grade 3 andgreater:1. Large Cell Ripple,0%
2. Foam pad, 24%
3. Spenco pad, 6%
– 45 Large Cell Ripplemattresses required 50motor repairs and 90material repairs duringthe 12-month study
Patients did not likethe feel of the ripples
No mention ofwithdrawals
Continued
TABLE 3 contd RCTs of pressure-relieving interventions for the prevention of pressure sores
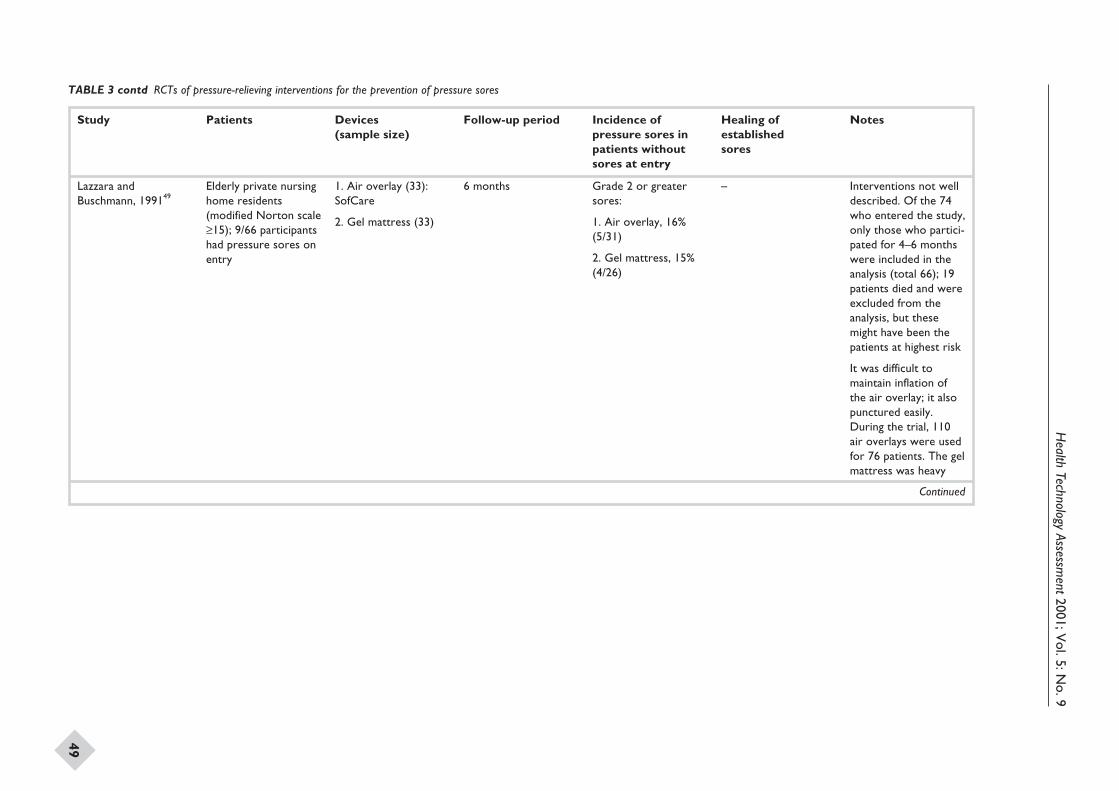
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
49
Study Patients Devices(sample size)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
Lazzara andBuschmann, 199149
Elderly private nursinghome residents(modified Norton scale≥15); 9/66 participantshad pressure sores onentry
1. Air overlay (33):SofCare
2. Gel mattress (33)
6 months Grade 2 or greatersores:
1. Air overlay, 16%(5/31)
2. Gel mattress, 15%(4/26)
– Interventions not welldescribed. Of the 74who entered the study,only those who partici-pated for 4–6 monthswere included in theanalysis (total 66); 19patients died and wereexcluded from theanalysis, but thesemight have been thepatients at highest risk
It was difficult tomaintain inflation ofthe air overlay; it alsopunctured easily.During the trial, 110air overlays were usedfor 76 patients. The gelmattress was heavy
Continued
TABLE 3 contd RCTs of pressure-relieving interventions for the prevention of pressure sores
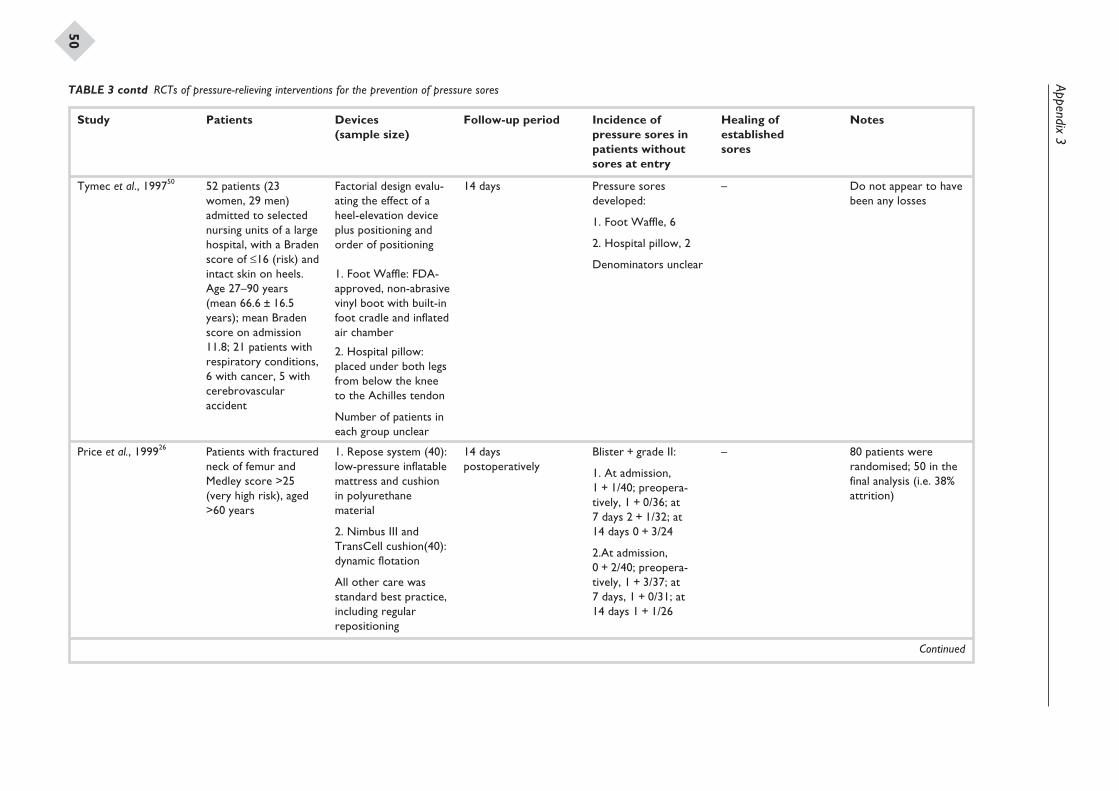
Appendix3
50
Study Patients Devices(sample size)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
Tymec et al., 199750 52 patients (23women, 29 men)admitted to selectednursing units of a largehospital, with a Bradenscore of £16 (risk) andintact skin on heels.Age 27–90 years(mean 66.6 ± 16.5years); mean Bradenscore on admission11.8; 21 patients withrespiratory conditions,6 with cancer, 5 withcerebrovascularaccident
Factorial design evalu-ating the effect of aheel-elevation deviceplus positioning andorder of positioning
1. Foot Waffle: FDA-approved, non-abrasivevinyl boot with built-infoot cradle and inflatedair chamber
2. Hospital pillow:placed under both legsfrom below the kneeto the Achilles tendon
Number of patients ineach group unclear
14 days Pressure soresdeveloped:
1. Foot Waffle, 6
2. Hospital pillow, 2
Denominators unclear
– Do not appear to havebeen any losses
Price et al., 199926 Patients with fracturedneck of femur andMedley score >25(very high risk), aged>60 years
1. Repose system (40):low-pressure inflatablemattress and cushionin polyurethanematerial
2. Nimbus III andTransCell cushion(40):dynamic flotation
All other care wasstandard best practice,including regularrepositioning
14 dayspostoperatively
Blister + grade II:
1. At admission,1 + 1/40; preopera-tively, 1 + 0/36; at7 days 2 + 1/32; at14 days 0 + 3/24
2.At admission,0 + 2/40; preopera-tively, 1 + 3/37; at7 days, 1 + 0/31; at14 days 1 + 1/26
– 80 patients wererandomised; 50 in thefinal analysis (i.e. 38%attrition)
Continued
TABLE 3 contd RCTs of pressure-relieving interventions for the prevention of pressure sores
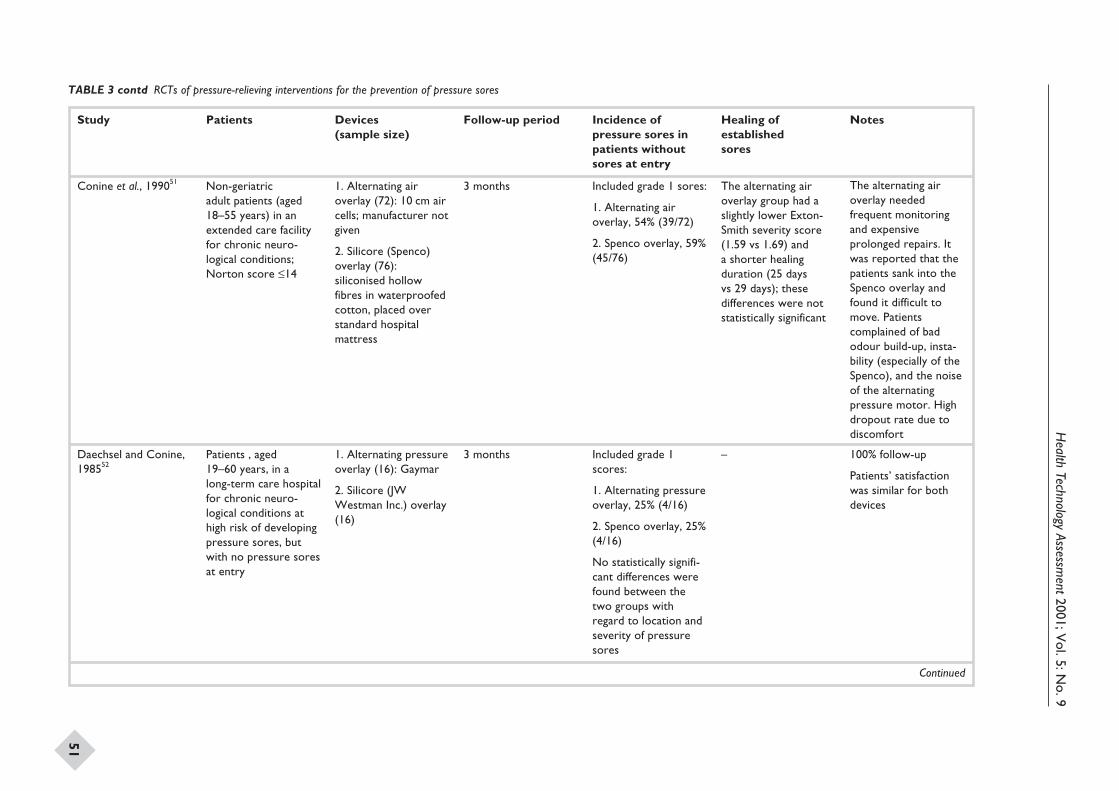
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
51
Study Patients Devices(sample size)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
Conine et al., 199051 Non-geriatricadult patients (aged18–55 years) in anextended care facilityfor chronic neuro-logical conditions;Norton score £14
1. Alternating airoverlay (72): 10 cm aircells; manufacturer notgiven
2. Silicore (Spenco)overlay (76):siliconised hollowfibres in waterproofedcotton, placed overstandard hospitalmattress
3 months Included grade 1 sores:
1. Alternating airoverlay, 54% (39/72)
2. Spenco overlay, 59%(45/76)
The alternating airoverlay group had aslightly lower Exton-Smith severity score(1.59 vs 1.69) anda shorter healingduration (25 daysvs 29 days); thesedifferences were notstatistically significant
The alternating airoverlay neededfrequent monitoringand expensiveprolonged repairs. Itwas reported that thepatients sank into theSpenco overlay andfound it difficult tomove. Patientscomplained of badodour build-up, insta-bility (especially of theSpenco), and the noiseof the alternatingpressure motor. Highdropout rate due todiscomfort
Daechsel and Conine,198552
Patients , aged19–60 years, in along-term care hospitalfor chronic neuro-logical conditions athigh risk of developingpressure sores, butwith no pressure soresat entry
1. Alternating pressureoverlay (16): Gaymar
2. Silicore (JWWestman Inc.) overlay(16)
3 months Included grade 1scores:
1. Alternating pressureoverlay, 25% (4/16)
2. Spenco overlay, 25%(4/16)
No statistically signifi-cant differences werefound between thetwo groups withregard to location andseverity of pressuresores
– 100% follow-up
Patients’ satisfactionwas similar for bothdevices
Continued
TABLE 3 contd RCTs of pressure-relieving interventions for the prevention of pressure sores
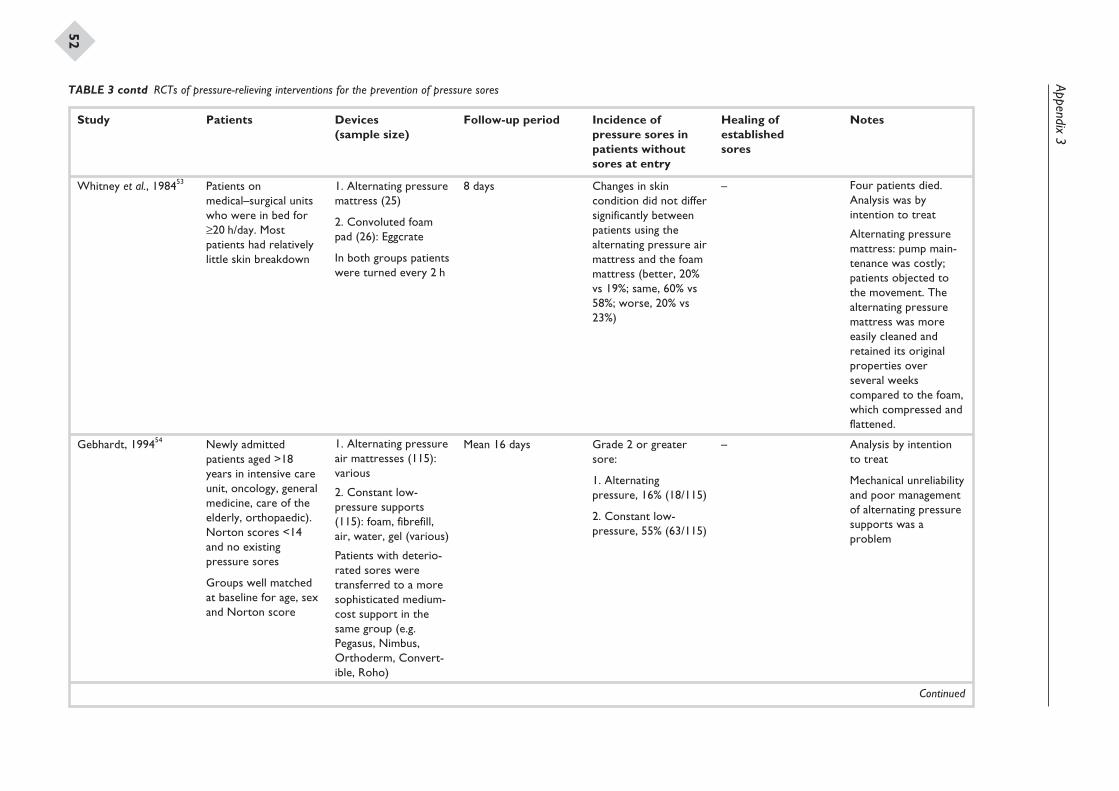
Appendix3
52
Study Patients Devices(sample size)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
Whitney et al., 198453 Patients onmedical–surgical unitswho were in bed for≥20 h/day. Mostpatients had relativelylittle skin breakdown
1. Alternating pressuremattress (25)
2. Convoluted foampad (26): Eggcrate
In both groups patientswere turned every 2 h
8 days Changes in skincondition did not differsignificantly betweenpatients using thealternating pressure airmattress and the foammattress (better, 20%vs 19%; same, 60% vs58%; worse, 20% vs23%)
– Four patients died.Analysis was byintention to treat
Alternating pressuremattress: pump main-tenance was costly;patients objected tothe movement. Thealternating pressuremattress was moreeasily cleaned andretained its originalproperties overseveral weekscompared to the foam,which compressed andflattened.
Gebhardt, 199454 Newly admittedpatients aged >18years in intensive careunit, oncology, generalmedicine, care of theelderly, orthopaedic).Norton scores <14and no existingpressure sores
Groups well matchedat baseline for age, sexand Norton score
1. Alternating pressureair mattresses (115):various
2. Constant low-pressure supports(115): foam, fibrefill,air, water, gel (various)
Patients with deterio-rated sores weretransferred to a moresophisticated medium-cost support in thesame group (e.g.Pegasus, Nimbus,Orthoderm, Convert-ible, Roho)
Mean 16 days Grade 2 or greatersore:
1. Alternatingpressure, 16% (18/115)
2. Constant low-pressure, 55% (63/115)
– Analysis by intentionto treat
Mechanical unreliabilityand poor managementof alternating pressuresupports was aproblem
Continued
TABLE 3 contd RCTs of pressure-relieving interventions for the prevention of pressure sores
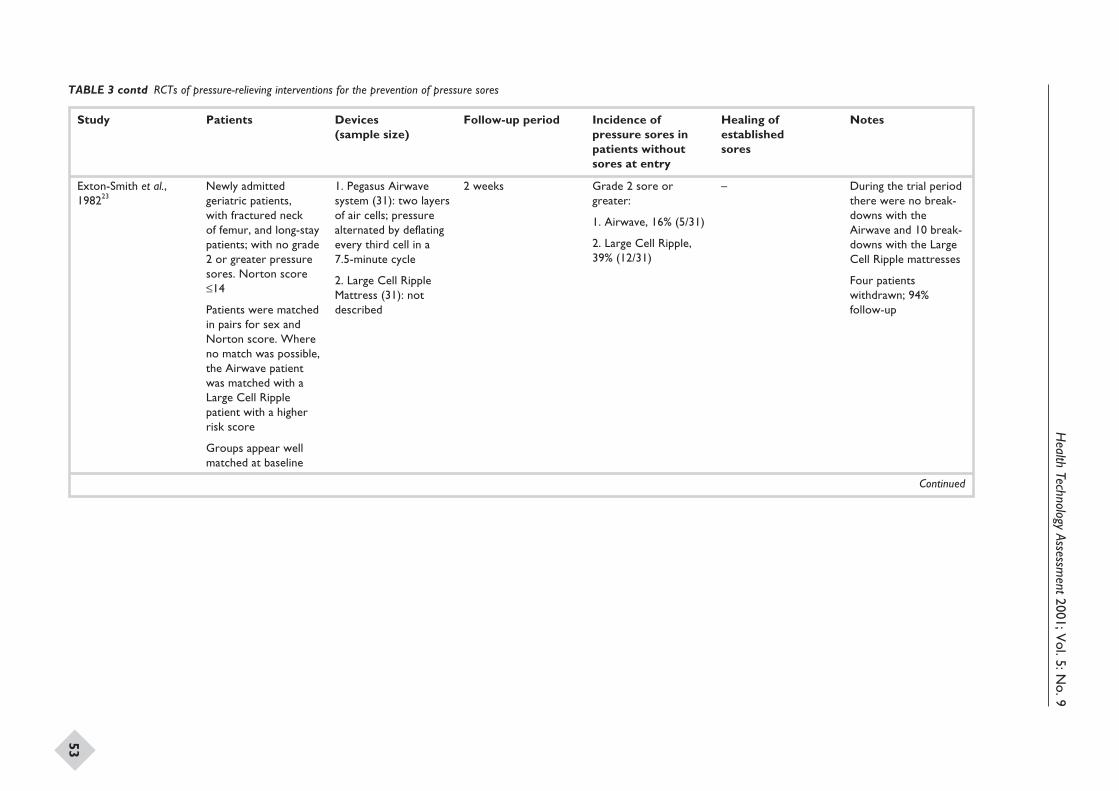
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
53
Study Patients Devices(sample size)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
Exton-Smith et al.,198223
Newly admittedgeriatric patients,with fractured neckof femur, and long-staypatients; with no grade2 or greater pressuresores. Norton score£14
Patients were matchedin pairs for sex andNorton score. Whereno match was possible,the Airwave patientwas matched with aLarge Cell Ripplepatient with a higherrisk score
Groups appear wellmatched at baseline
1. Pegasus Airwavesystem (31): two layersof air cells; pressurealternated by deflatingevery third cell in a7.5-minute cycle
2. Large Cell RippleMattress (31): notdescribed
2 weeks Grade 2 sore orgreater:
1. Airwave, 16% (5/31)
2. Large Cell Ripple,39% (12/31)
– During the trial periodthere were no break-downs with theAirwave and 10 break-downs with the LargeCell Ripple mattresses
Four patientswithdrawn; 94%follow-up
Continued
TABLE 3 contd RCTs of pressure-relieving interventions for the prevention of pressure sores
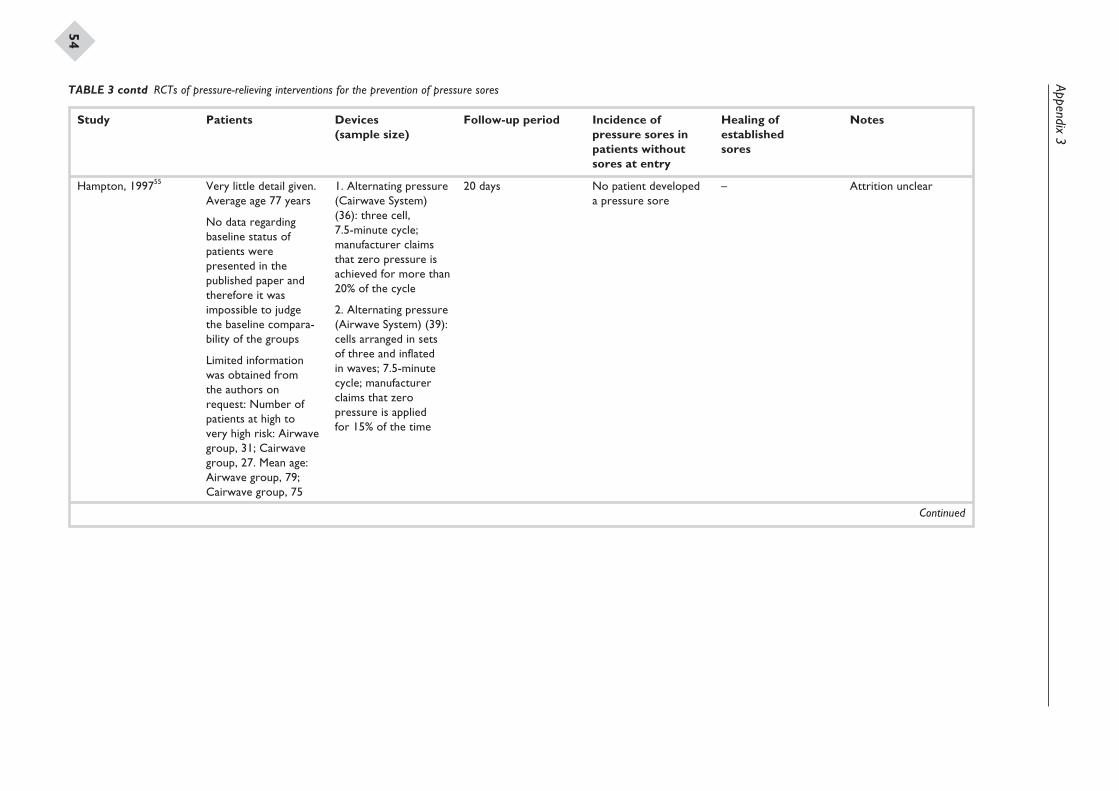
Appendix3
54
Study Patients Devices(sample size)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
Hampton, 199755 Very little detail given.Average age 77 years
No data regardingbaseline status ofpatients werepresented in thepublished paper andtherefore it wasimpossible to judgethe baseline compara-bility of the groups
Limited informationwas obtained fromthe authors onrequest: Number ofpatients at high tovery high risk: Airwavegroup, 31; Cairwavegroup, 27. Mean age:Airwave group, 79;Cairwave group, 75
1. Alternating pressure(Cairwave System)(36): three cell,7.5-minute cycle;manufacturer claimsthat zero pressure isachieved for more than20% of the cycle
2. Alternating pressure(Airwave System) (39):cells arranged in setsof three and inflatedin waves; 7.5-minutecycle; manufacturerclaims that zeropressure is appliedfor 15% of the time
20 days No patient developeda pressure sore
– Attrition unclear
Continued
TABLE 3 contd RCTs of pressure-relieving interventions for the prevention of pressure sores
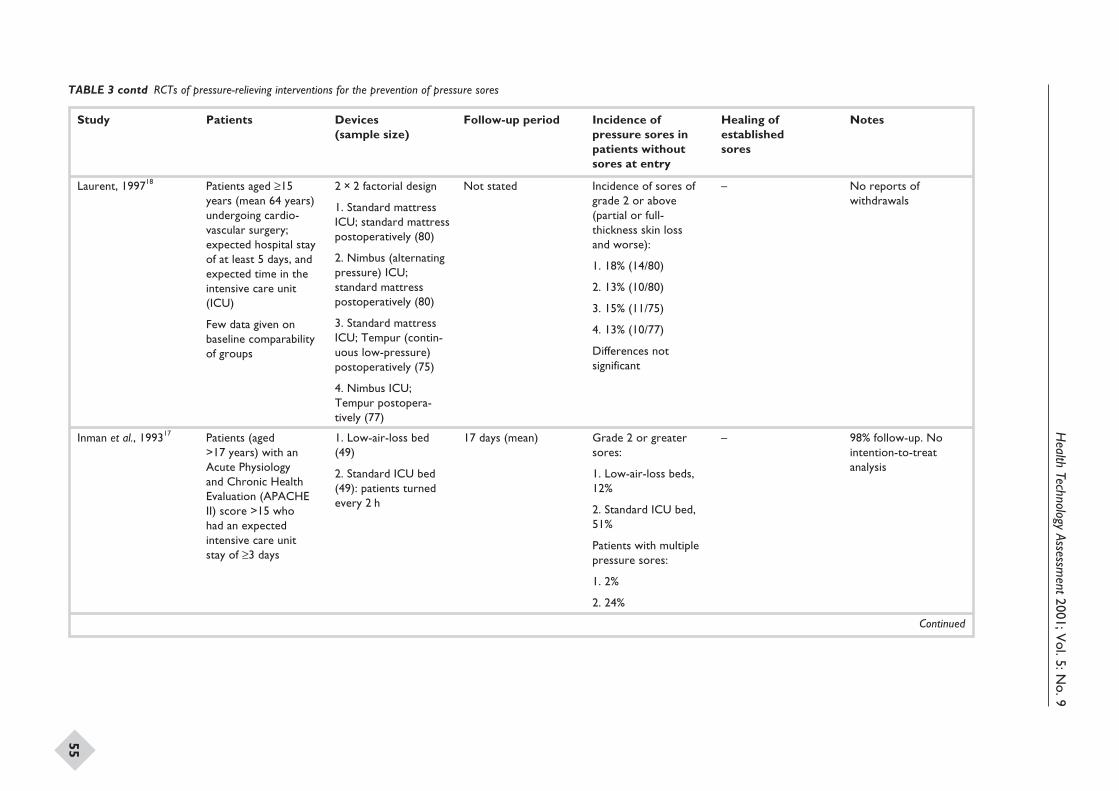
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
55
Study Patients Devices(sample size)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
Laurent, 199718 Patients aged ≥15years (mean 64 years)undergoing cardio-vascular surgery;expected hospital stayof at least 5 days, andexpected time in theintensive care unit(ICU)
Few data given onbaseline comparabilityof groups
2 × 2 factorial design
1. Standard mattressICU; standard mattresspostoperatively (80)
2. Nimbus (alternatingpressure) ICU;standard mattresspostoperatively (80)
3. Standard mattressICU; Tempur (contin-uous low-pressure)postoperatively (75)
4. Nimbus ICU;Tempur postopera-tively (77)
Not stated Incidence of sores ofgrade 2 or above(partial or full-thickness skin lossand worse):
1. 18% (14/80)
2. 13% (10/80)
3. 15% (11/75)
4. 13% (10/77)
Differences notsignificant
– No reports ofwithdrawals
Inman et al., 199317 Patients (aged>17 years) with anAcute Physiologyand Chronic HealthEvaluation (APACHEII) score >15 whohad an expectedintensive care unitstay of ≥3 days
1. Low-air-loss bed(49)
2. Standard ICU bed(49): patients turnedevery 2 h
17 days (mean) Grade 2 or greatersores:
1. Low-air-loss beds,12%
2. Standard ICU bed,51%
Patients with multiplepressure sores:
1. 2%
2. 24%
– 98% follow-up. Nointention-to-treatanalysis
Continued
TABLE 3 contd RCTs of pressure-relieving interventions for the prevention of pressure sores
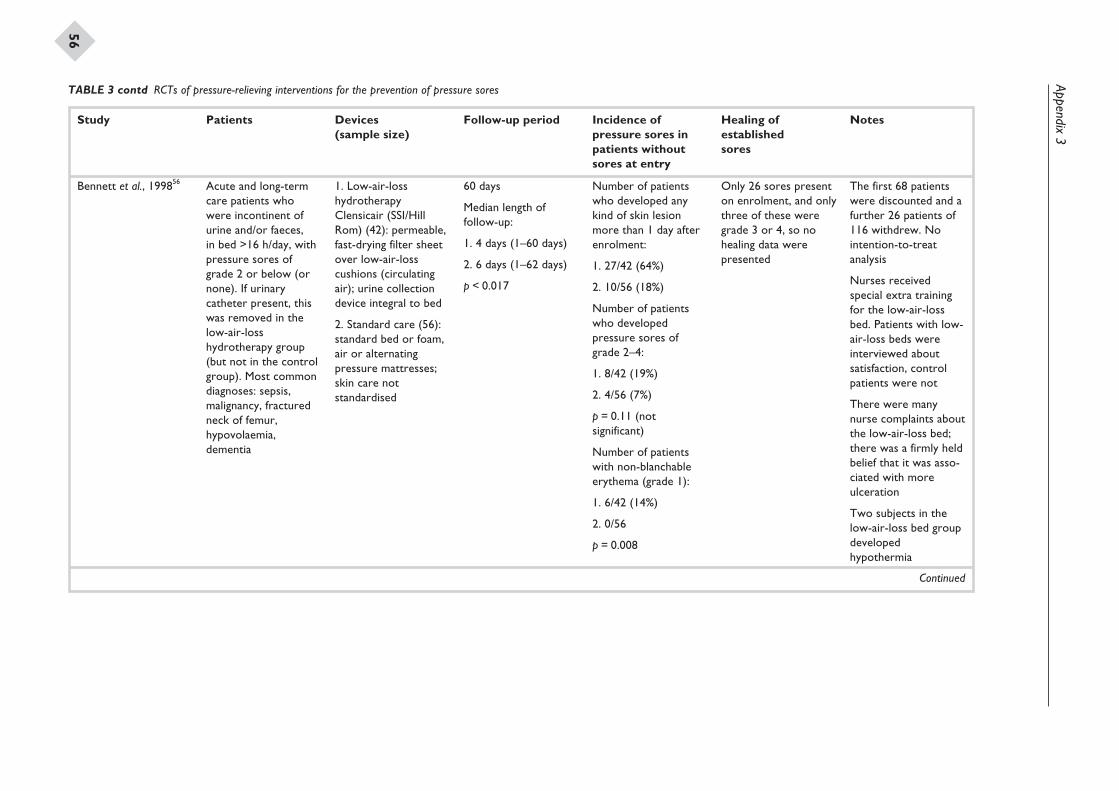
Appendix3
56
Study Patients Devices(sample size)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
Bennett et al., 199856 Acute and long-termcare patients whowere incontinent ofurine and/or faeces,in bed >16 h/day, withpressure sores ofgrade 2 or below (ornone). If urinarycatheter present, thiswas removed in thelow-air-losshydrotherapy group(but not in the controlgroup). Most commondiagnoses: sepsis,malignancy, fracturedneck of femur,hypovolaemia,dementia
1. Low-air-losshydrotherapyClensicair (SSI/HillRom) (42): permeable,fast-drying filter sheetover low-air-losscushions (circulatingair); urine collectiondevice integral to bed
2. Standard care (56):standard bed or foam,air or alternatingpressure mattresses;skin care notstandardised
60 days
Median length offollow-up:
1. 4 days (1–60 days)
2. 6 days (1–62 days)
p < 0.017
Number of patientswho developed anykind of skin lesionmore than 1 day afterenrolment:
1. 27/42 (64%)
2. 10/56 (18%)
Number of patientswho developedpressure sores ofgrade 2–4:
1. 8/42 (19%)
2. 4/56 (7%)
p = 0.11 (notsignificant)
Number of patientswith non-blanchableerythema (grade 1):
1. 6/42 (14%)
2. 0/56
p = 0.008
Only 26 sores presenton enrolment, and onlythree of these weregrade 3 or 4, so nohealing data werepresented
The first 68 patientswere discounted and afurther 26 patients of116 withdrew. Nointention-to-treatanalysis
Nurses receivedspecial extra trainingfor the low-air-lossbed. Patients with low-air-loss beds wereinterviewed aboutsatisfaction, controlpatients were not
There were manynurse complaints aboutthe low-air-loss bed;there was a firmly heldbelief that it was asso-ciated with moreulceration
Two subjects in thelow-air-loss bed groupdevelopedhypothermia
Continued
TABLE 3 contd RCTs of pressure-relieving interventions for the prevention of pressure sores
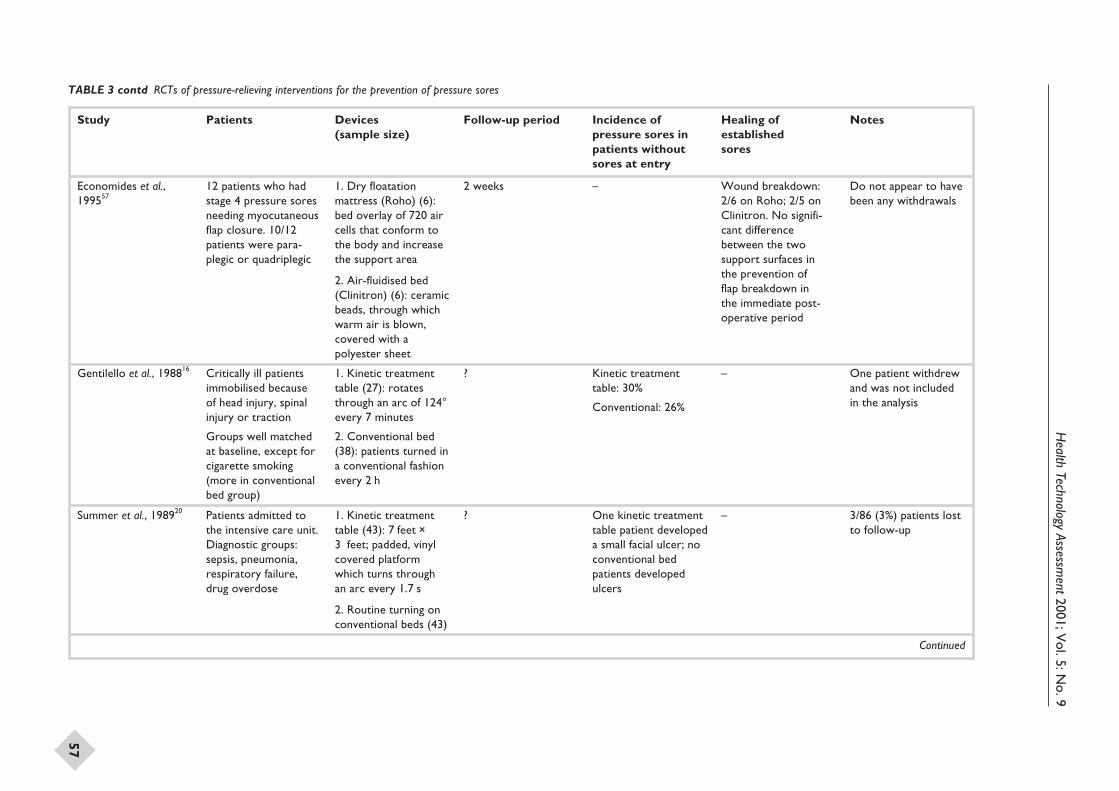
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
57
Study Patients Devices(sample size)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
Economides et al.,199557
12 patients who hadstage 4 pressure soresneeding myocutaneousflap closure. 10/12patients were para-plegic or quadriplegic
1. Dry floatationmattress (Roho) (6):bed overlay of 720 aircells that conform tothe body and increasethe support area
2. Air-fluidised bed(Clinitron) (6): ceramicbeads, through whichwarm air is blown,covered with apolyester sheet
2 weeks – Wound breakdown:2/6 on Roho; 2/5 onClinitron. No signifi-cant differencebetween the twosupport surfaces inthe prevention offlap breakdown inthe immediate post-operative period
Do not appear to havebeen any withdrawals
Gentilello et al., 198816 Critically ill patientsimmobilised becauseof head injury, spinalinjury or traction
Groups well matchedat baseline, except forcigarette smoking(more in conventionalbed group)
1. Kinetic treatmenttable (27): rotatesthrough an arc of 124°every 7 minutes
2. Conventional bed(38): patients turned ina conventional fashionevery 2 h
? Kinetic treatmenttable: 30%
Conventional: 26%
– One patient withdrewand was not includedin the analysis
Summer et al., 198920 Patients admitted tothe intensive care unit.Diagnostic groups:sepsis, pneumonia,respiratory failure,drug overdose
1. Kinetic treatmenttable (43): 7 feet ×3 feet; padded, vinylcovered platformwhich turns throughan arc every 1.7 s
2. Routine turning onconventional beds (43)
? One kinetic treatmenttable patient developeda small facial ulcer; noconventional bedpatients developedulcers
– 3/86 (3%) patients lostto follow-up
Continued
TABLE 3 contd RCTs of pressure-relieving interventions for the prevention of pressure sores
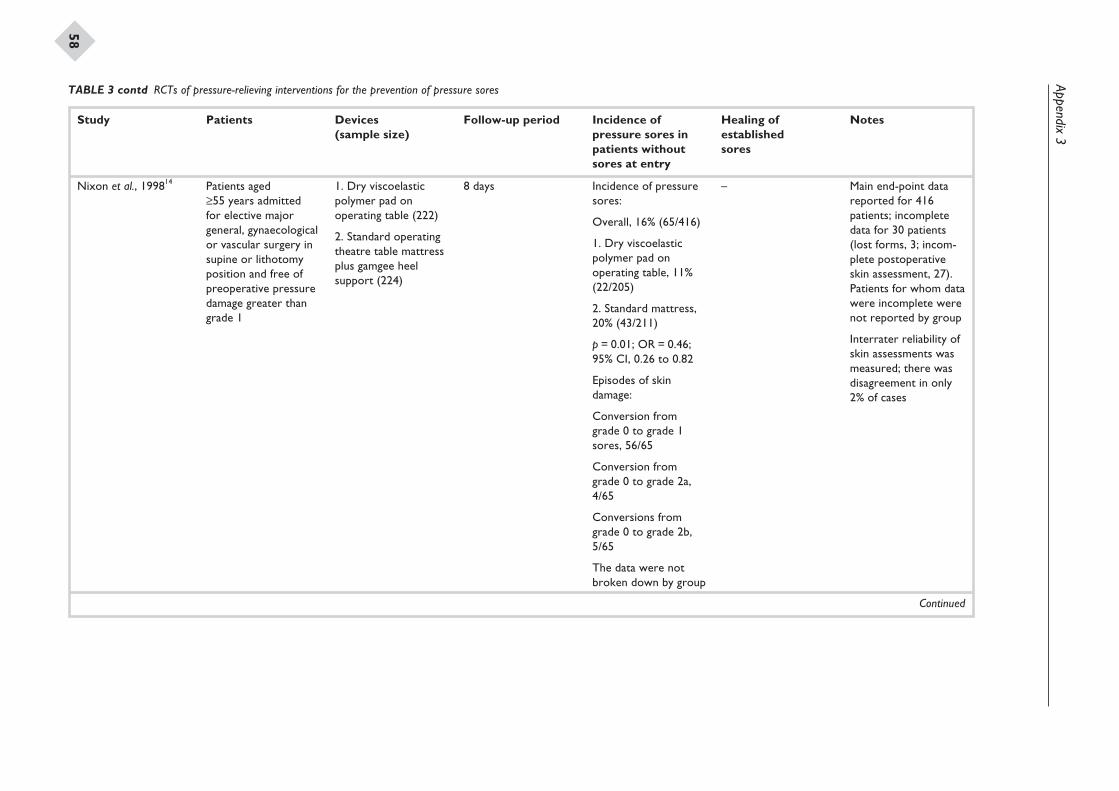
Appendix3
58
Study Patients Devices(sample size)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
Nixon et al., 199814 Patients aged≥55 years admittedfor elective majorgeneral, gynaecologicalor vascular surgery insupine or lithotomyposition and free ofpreoperative pressuredamage greater thangrade 1
1. Dry viscoelasticpolymer pad onoperating table (222)
2. Standard operatingtheatre table mattressplus gamgee heelsupport (224)
8 days Incidence of pressuresores:
Overall, 16% (65/416)
1. Dry viscoelasticpolymer pad onoperating table, 11%(22/205)
2. Standard mattress,20% (43/211)
p = 0.01; OR = 0.46;95% CI, 0.26 to 0.82
Episodes of skindamage:
Conversion fromgrade 0 to grade 1sores, 56/65
Conversion fromgrade 0 to grade 2a,4/65
Conversions fromgrade 0 to grade 2b,5/65
The data were notbroken down by group
– Main end-point datareported for 416patients; incompletedata for 30 patients(lost forms, 3; incom-plete postoperativeskin assessment, 27).Patients for whom datawere incomplete werenot reported by group
Interrater reliability ofskin assessments wasmeasured; there wasdisagreement in only2% of cases
Continued
TABLE 3 contd RCTs of pressure-relieving interventions for the prevention of pressure sores
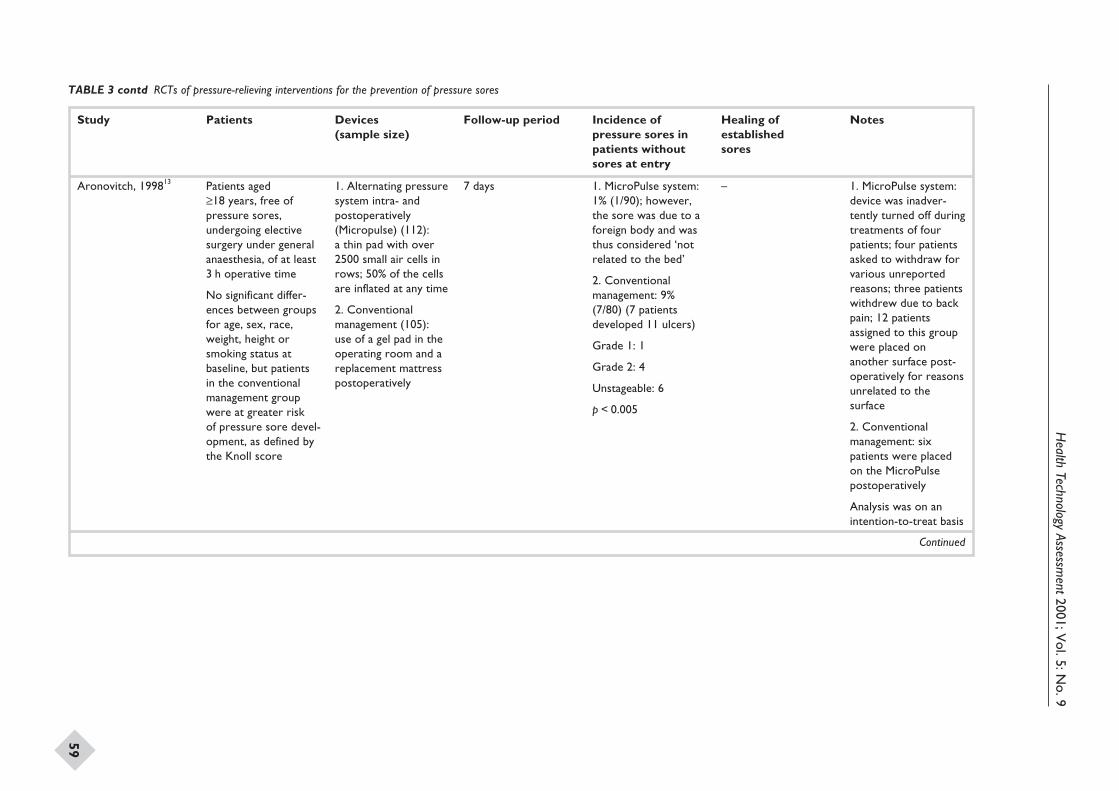
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
59
Study Patients Devices(sample size)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
Aronovitch, 199813 Patients aged≥18 years, free ofpressure sores,undergoing electivesurgery under generalanaesthesia, of at least3 h operative time
No significant differ-ences between groupsfor age, sex, race,weight, height orsmoking status atbaseline, but patientsin the conventionalmanagement groupwere at greater riskof pressure sore devel-opment, as defined bythe Knoll score
1. Alternating pressuresystem intra- andpostoperatively(Micropulse) (112):a thin pad with over2500 small air cells inrows; 50% of the cellsare inflated at any time
2. Conventionalmanagement (105):use of a gel pad in theoperating room and areplacement mattresspostoperatively
7 days 1. MicroPulse system:1% (1/90); however,the sore was due to aforeign body and wasthus considered ‘notrelated to the bed’
2. Conventionalmanagement: 9%(7/80) (7 patientsdeveloped 11 ulcers)
Grade 1: 1
Grade 2: 4
Unstageable: 6
p < 0.005
– 1. MicroPulse system:device was inadver-tently turned off duringtreatments of fourpatients; four patientsasked to withdraw forvarious unreportedreasons; three patientswithdrew due to backpain; 12 patientsassigned to this groupwere placed onanother surface post-operatively for reasonsunrelated to thesurface
2. Conventionalmanagement: sixpatients were placedon the MicroPulsepostoperatively
Analysis was on anintention-to-treat basis
Continued
TABLE 3 contd RCTs of pressure-relieving interventions for the prevention of pressure sores
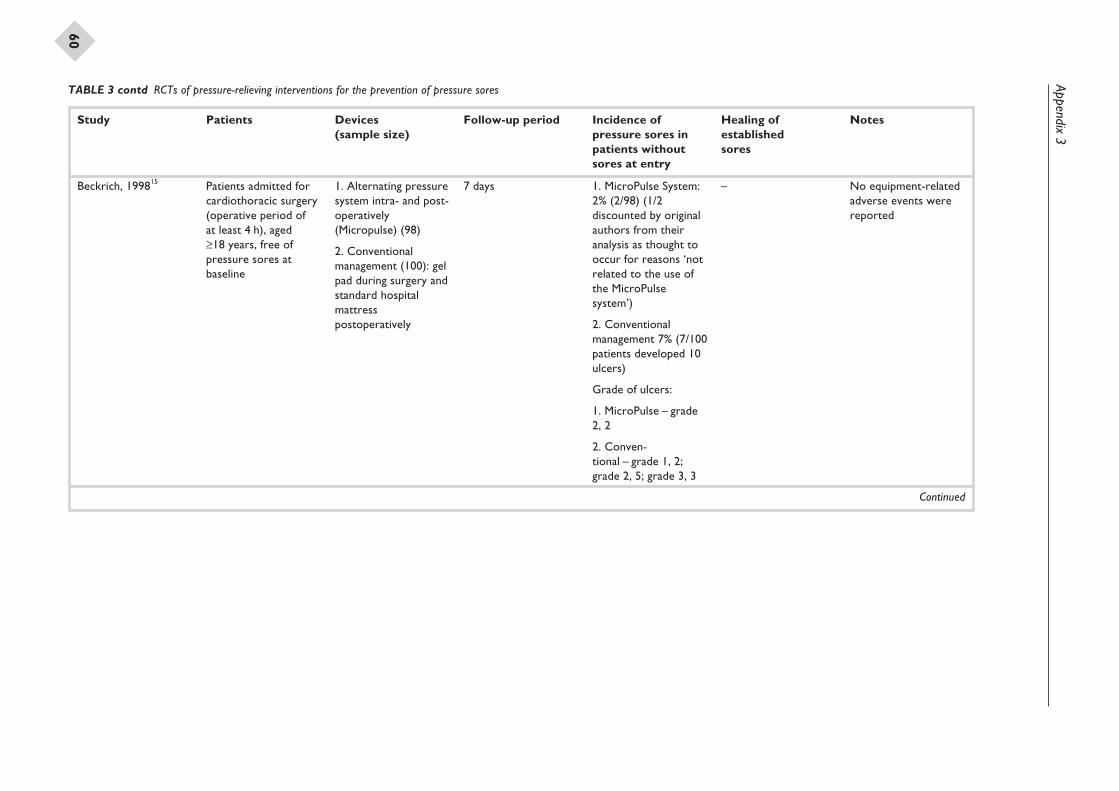
Appendix3
60
Study Patients Devices(sample size)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
Beckrich, 199815 Patients admitted forcardiothoracic surgery(operative period ofat least 4 h), aged≥18 years, free ofpressure sores atbaseline
1. Alternating pressuresystem intra- and post-operatively(Micropulse) (98)
2. Conventionalmanagement (100): gelpad during surgery andstandard hospitalmattresspostoperatively
7 days 1. MicroPulse System:2% (2/98) (1/2discounted by originalauthors from theiranalysis as thought tooccur for reasons ‘notrelated to the use ofthe MicroPulsesystem’)
2. Conventionalmanagement 7% (7/100patients developed 10ulcers)
Grade of ulcers:
1. MicroPulse – grade2, 2
2. Conven-tional – grade 1, 2;grade 2, 5; grade 3, 3
– No equipment-relatedadverse events werereported
Continued
TABLE 3 contd RCTs of pressure-relieving interventions for the prevention of pressure sores
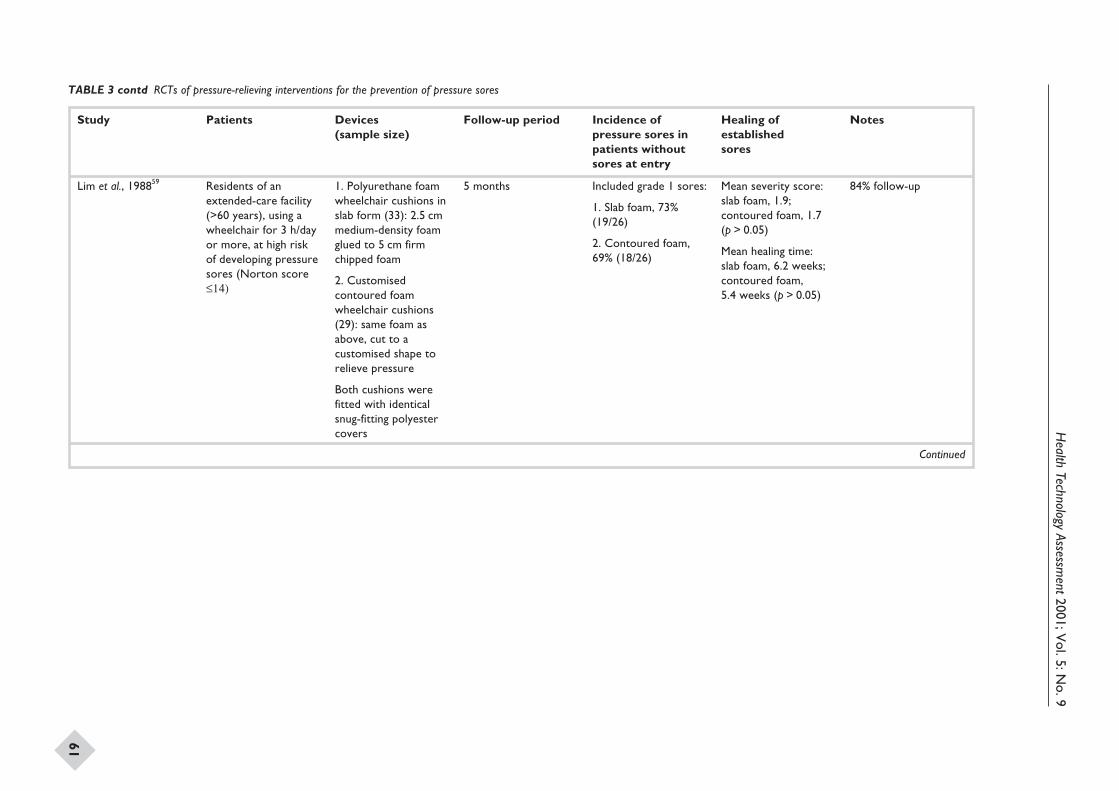
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
61
Study Patients Devices(sample size)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
Lim et al., 198859 Residents of anextended-care facility(>60 years), using awheelchair for 3 h/dayor more, at high riskof developing pressuresores (Norton score£14)
1. Polyurethane foamwheelchair cushions inslab form (33): 2.5 cmmedium-density foamglued to 5 cm firmchipped foam
2. Customisedcontoured foamwheelchair cushions(29): same foam asabove, cut to acustomised shape torelieve pressure
Both cushions werefitted with identicalsnug-fitting polyestercovers
5 months Included grade 1 sores:
1. Slab foam, 73%(19/26)
2. Contoured foam,69% (18/26)
Mean severity score:slab foam, 1.9;contoured foam, 1.7(p > 0.05)
Mean healing time:slab foam, 6.2 weeks;contoured foam,5.4 weeks (p > 0.05)
84% follow-up
Continued
TABLE 3 contd RCTs of pressure-relieving interventions for the prevention of pressure sores
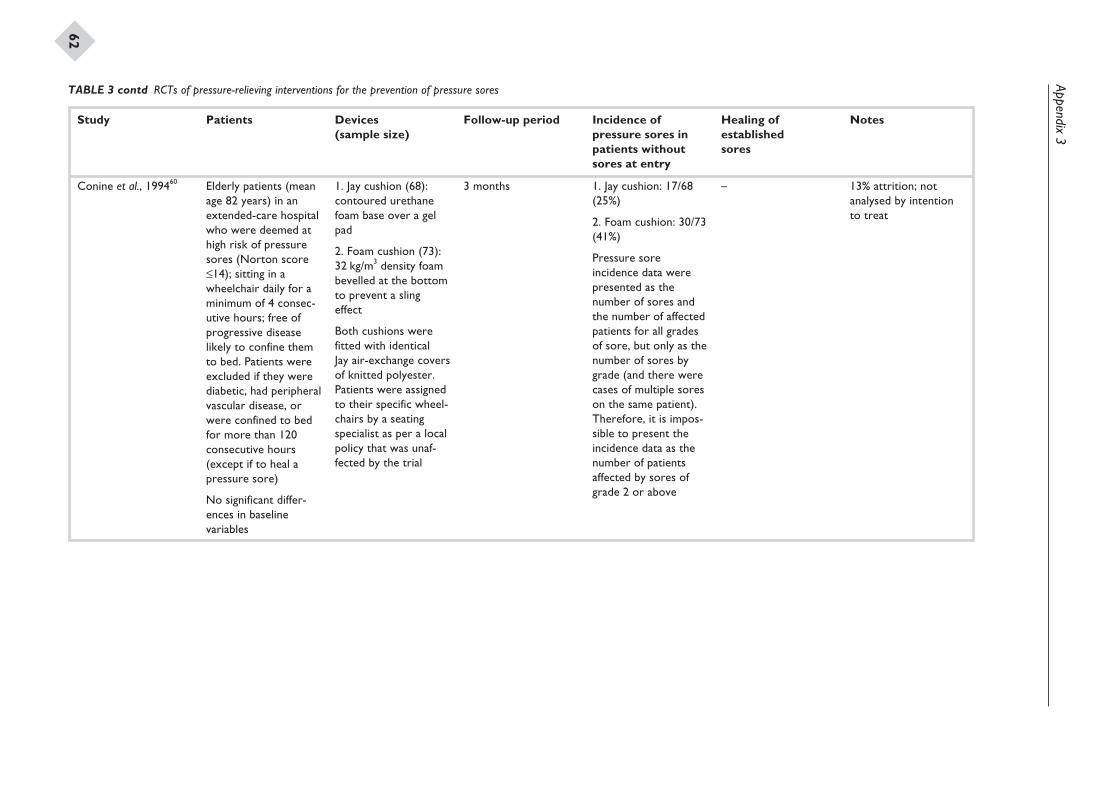
Appendix3
62
Study Patients Devices(sample size)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
Conine et al., 199460 Elderly patients (meanage 82 years) in anextended-care hospitalwho were deemed athigh risk of pressuresores (Norton score£14); sitting in awheelchair daily for aminimum of 4 consec-utive hours; free ofprogressive diseaselikely to confine themto bed. Patients wereexcluded if they werediabetic, had peripheralvascular disease, orwere confined to bedfor more than 120consecutive hours(except if to heal apressure sore)
No significant differ-ences in baselinevariables
1. Jay cushion (68):contoured urethanefoam base over a gelpad
2. Foam cushion (73):32 kg/m3 density foambevelled at the bottomto prevent a slingeffect
Both cushions werefitted with identicalJay air-exchange coversof knitted polyester.Patients were assignedto their specific wheel-chairs by a seatingspecialist as per a localpolicy that was unaf-fected by the trial
3 months 1. Jay cushion: 17/68(25%)
2. Foam cushion: 30/73(41%)
Pressure soreincidence data werepresented as thenumber of sores andthe number of affectedpatients for all gradesof sore, but only as thenumber of sores bygrade (and there werecases of multiple soreson the same patient).Therefore, it is impos-sible to present theincidence data as thenumber of patientsaffected by sores ofgrade 2 or above
– 13% attrition; notanalysed by intentionto treat
TABLE 3 contd RCTs of pressure-relieving interventions for the prevention of pressure sores
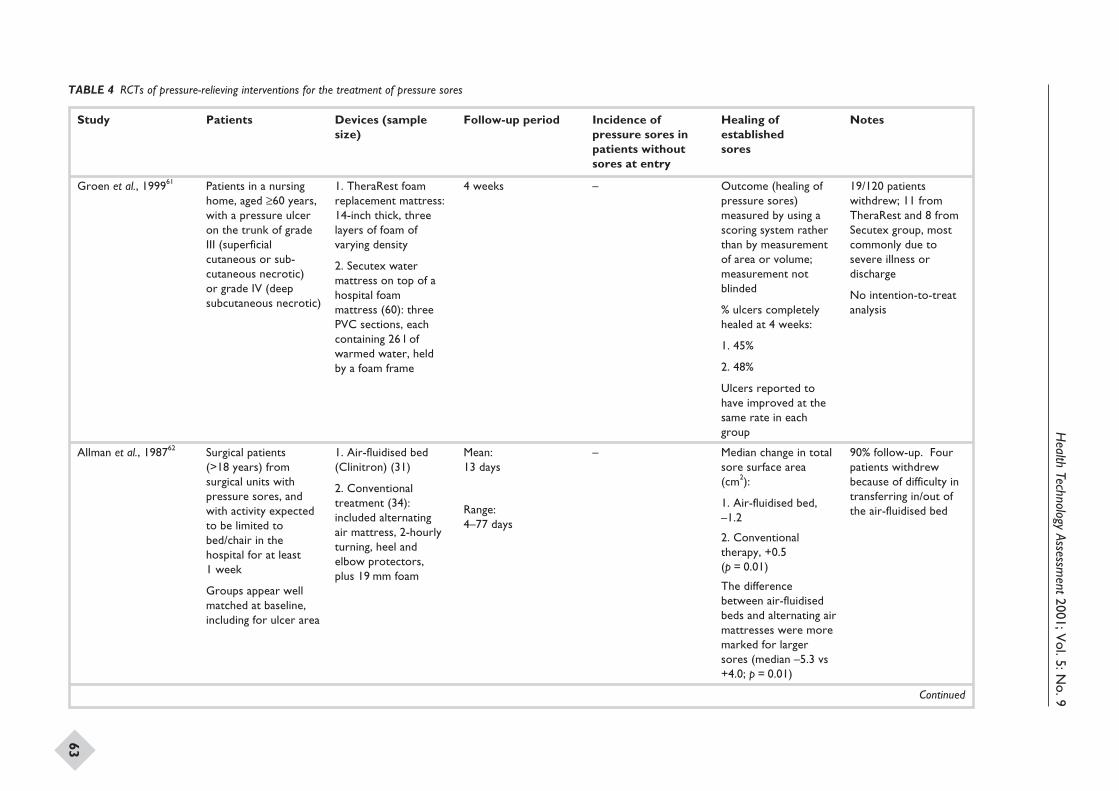
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
63
Study Patients Devices (samplesize)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
Groen et al., 199961 Patients in a nursinghome, aged ≥60 years,with a pressure ulceron the trunk of gradeIII (superficialcutaneous or sub-cutaneous necrotic)or grade IV (deepsubcutaneous necrotic)
1. TheraRest foamreplacement mattress:14-inch thick, threelayers of foam ofvarying density
2. Secutex watermattress on top of ahospital foammattress (60): threePVC sections, eachcontaining 26 l ofwarmed water, heldby a foam frame
4 weeks – Outcome (healing ofpressure sores)measured by using ascoring system ratherthan by measurementof area or volume;measurement notblinded
% ulcers completelyhealed at 4 weeks:
1. 45%
2. 48%
Ulcers reported tohave improved at thesame rate in eachgroup
19/120 patientswithdrew; 11 fromTheraRest and 8 fromSecutex group, mostcommonly due tosevere illness ordischarge
No intention-to-treatanalysis
Allman et al., 198762 Surgical patients(>18 years) fromsurgical units withpressure sores, andwith activity expectedto be limited tobed/chair in thehospital for at least1 week
Groups appear wellmatched at baseline,including for ulcer area
1. Air-fluidised bed(Clinitron) (31)
2. Conventionaltreatment (34):included alternatingair mattress, 2-hourlyturning, heel andelbow protectors,plus 19 mm foam
Mean:13 days
Range:4–77 days
– Median change in totalsore surface area(cm2):
1. Air-fluidised bed,–1.2
2. Conventionaltherapy, +0.5(p = 0.01)
The differencebetween air-fluidisedbeds and alternating airmattresses were moremarked for largersores (median –5.3 vs+4.0; p = 0.01)
90% follow-up. Fourpatients withdrewbecause of difficulty intransferring in/out ofthe air-fluidised bed
Continued
TABLE 4 RCTs of pressure-relieving interventions for the treatment of pressure sores
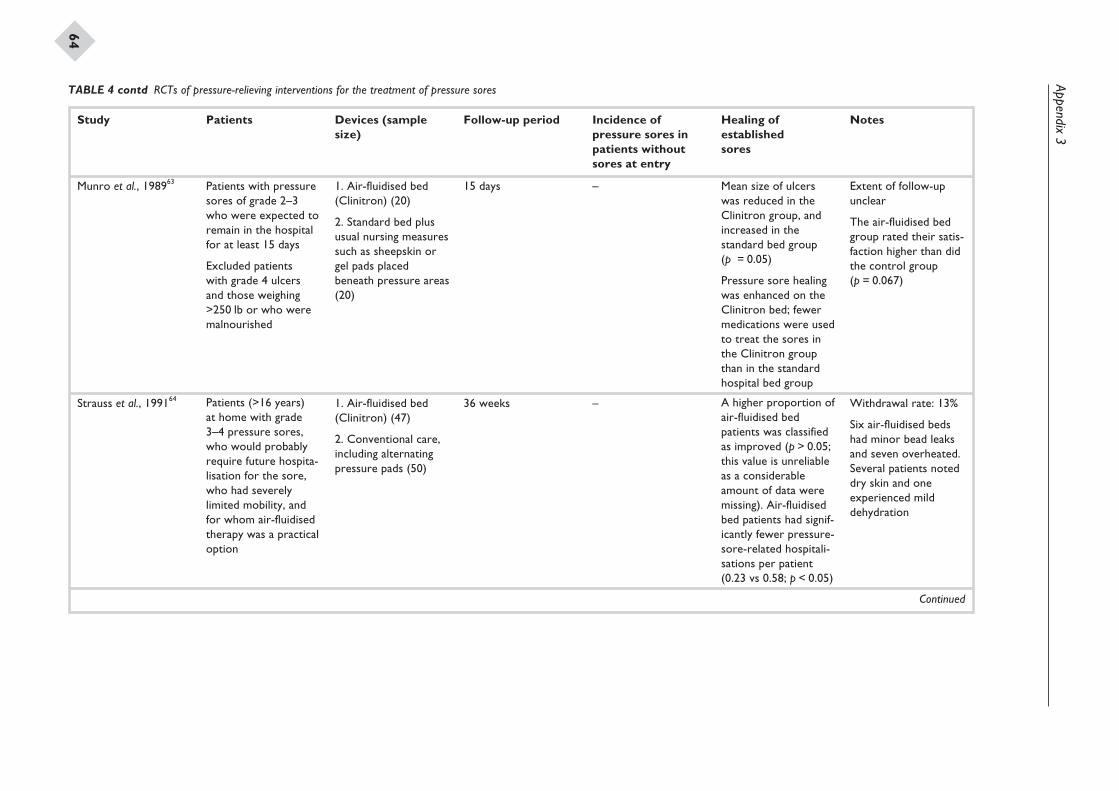
Appendix3
64
Study Patients Devices (samplesize)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
Munro et al., 198963 Patients with pressuresores of grade 2–3who were expected toremain in the hospitalfor at least 15 days
Excluded patientswith grade 4 ulcersand those weighing>250 lb or who weremalnourished
1. Air-fluidised bed(Clinitron) (20)
2. Standard bed plususual nursing measuressuch as sheepskin orgel pads placedbeneath pressure areas(20)
15 days – Mean size of ulcerswas reduced in theClinitron group, andincreased in thestandard bed group(p = 0.05)
Pressure sore healingwas enhanced on theClinitron bed; fewermedications were usedto treat the sores inthe Clinitron groupthan in the standardhospital bed group
Extent of follow-upunclear
The air-fluidised bedgroup rated their satis-faction higher than didthe control group(p = 0.067)
Strauss et al., 199164 Patients (>16 years)at home with grade3–4 pressure sores,who would probablyrequire future hospita-lisation for the sore,who had severelylimited mobility, andfor whom air-fluidisedtherapy was a practicaloption
1. Air-fluidised bed(Clinitron) (47)
2. Conventional care,including alternatingpressure pads (50)
36 weeks – A higher proportion ofair-fluidised bedpatients was classifiedas improved (p > 0.05;this value is unreliableas a considerableamount of data weremissing). Air-fluidisedbed patients had signif-icantly fewer pressure-sore-related hospitali-sations per patient(0.23 vs 0.58; p < 0.05)
Withdrawal rate: 13%
Six air-fluidised bedshad minor bead leaksand seven overheated.Several patients noteddry skin and oneexperienced milddehydration
Continued
TABLE 4 contd RCTs of pressure-relieving interventions for the treatment of pressure sores
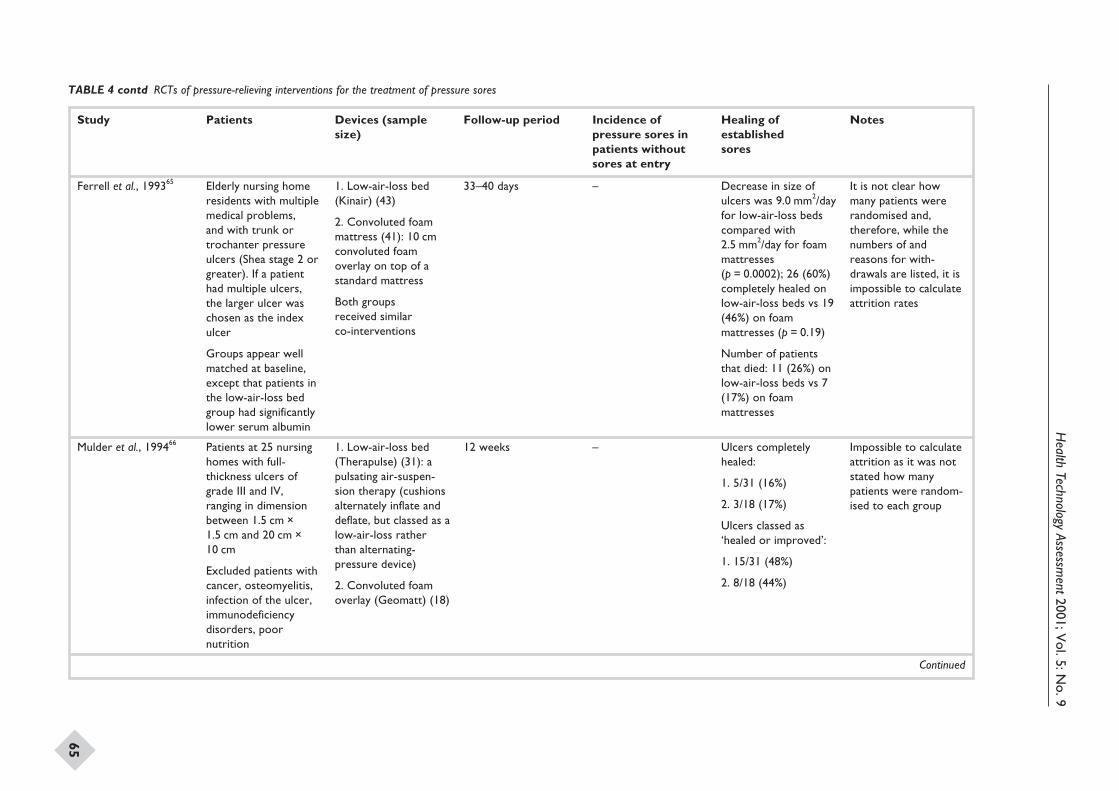
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
65
Study Patients Devices (samplesize)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
Ferrell et al., 199365 Elderly nursing homeresidents with multiplemedical problems,and with trunk ortrochanter pressureulcers (Shea stage 2 orgreater). If a patienthad multiple ulcers,the larger ulcer waschosen as the indexulcer
Groups appear wellmatched at baseline,except that patients inthe low-air-loss bedgroup had significantlylower serum albumin
1. Low-air-loss bed(Kinair) (43)
2. Convoluted foammattress (41): 10 cmconvoluted foamoverlay on top of astandard mattress
Both groupsreceived similarco-interventions
33–40 days – Decrease in size ofulcers was 9.0 mm2/dayfor low-air-loss bedscompared with2.5 mm2/day for foammattresses(p = 0.0002); 26 (60%)completely healed onlow-air-loss beds vs 19(46%) on foammattresses (p = 0.19)
Number of patientsthat died: 11 (26%) onlow-air-loss beds vs 7(17%) on foammattresses
It is not clear howmany patients wererandomised and,therefore, while thenumbers of andreasons for with-drawals are listed, it isimpossible to calculateattrition rates
Mulder et al., 199466 Patients at 25 nursinghomes with full-thickness ulcers ofgrade III and IV,ranging in dimensionbetween 1.5 cm ×1.5 cm and 20 cm ×10 cm
Excluded patients withcancer, osteomyelitis,infection of the ulcer,immunodeficiencydisorders, poornutrition
1. Low-air-loss bed(Therapulse) (31): apulsating air-suspen-sion therapy (cushionsalternately inflate anddeflate, but classed as alow-air-loss ratherthan alternating-pressure device)
2. Convoluted foamoverlay (Geomatt) (18)
12 weeks – Ulcers completelyhealed:
1. 5/31 (16%)
2. 3/18 (17%)
Ulcers classed as‘healed or improved’:
1. 15/31 (48%)
2. 8/18 (44%)
Impossible to calculateattrition as it was notstated how manypatients were random-ised to each group
Continued
TABLE 4 contd RCTs of pressure-relieving interventions for the treatment of pressure sores
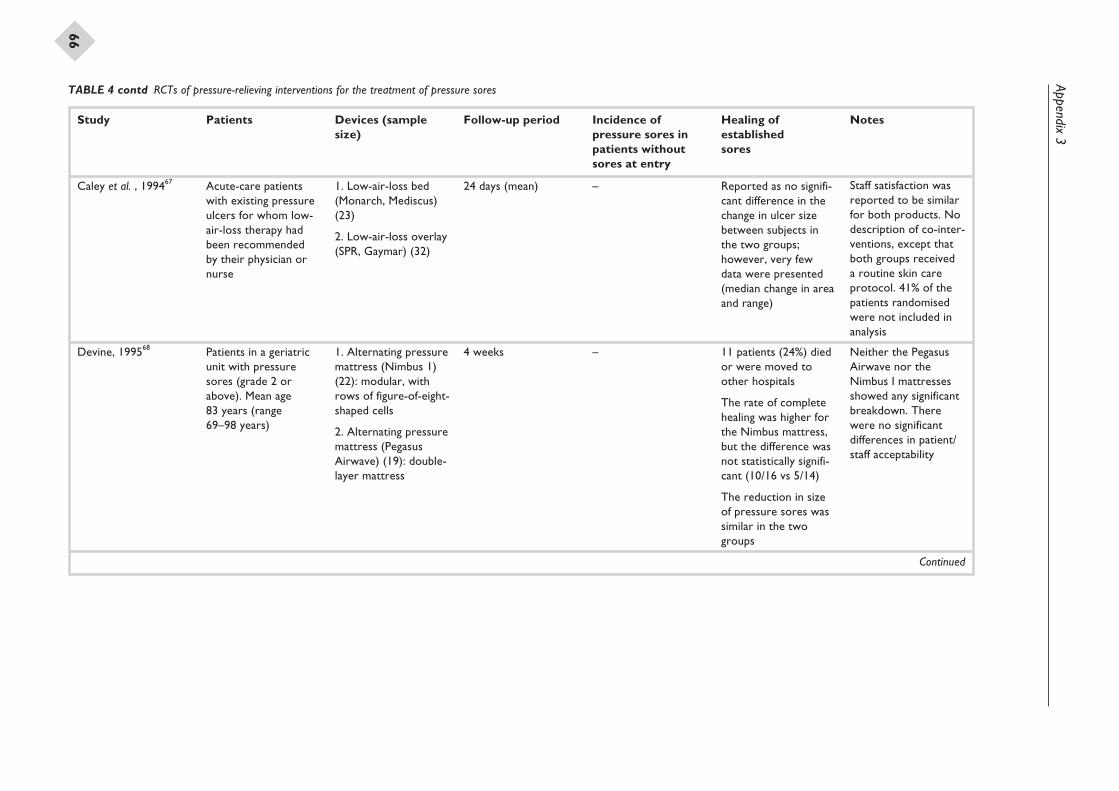
Appendix3
66
Study Patients Devices (samplesize)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
Caley et al. , 199467 Acute-care patientswith existing pressureulcers for whom low-air-loss therapy hadbeen recommendedby their physician ornurse
1. Low-air-loss bed(Monarch, Mediscus)(23)
2. Low-air-loss overlay(SPR, Gaymar) (32)
24 days (mean) – Reported as no signifi-cant difference in thechange in ulcer sizebetween subjects inthe two groups;however, very fewdata were presented(median change in areaand range)
Staff satisfaction wasreported to be similarfor both products. Nodescription of co-inter-ventions, except thatboth groups receiveda routine skin careprotocol. 41% of thepatients randomisedwere not included inanalysis
Devine, 199568 Patients in a geriatricunit with pressuresores (grade 2 orabove). Mean age83 years (range69–98 years)
1. Alternating pressuremattress (Nimbus 1)(22): modular, withrows of figure-of-eight-shaped cells
2. Alternating pressuremattress (PegasusAirwave) (19): double-layer mattress
4 weeks – 11 patients (24%) diedor were moved toother hospitals
The rate of completehealing was higher forthe Nimbus mattress,but the difference wasnot statistically signifi-cant (10/16 vs 5/14)
The reduction in sizeof pressure sores wassimilar in the twogroups
Neither the PegasusAirwave nor theNimbus I mattressesshowed any significantbreakdown. Therewere no significantdifferences in patient/staff acceptability
Continued
TABLE 4 contd RCTs of pressure-relieving interventions for the treatment of pressure sores
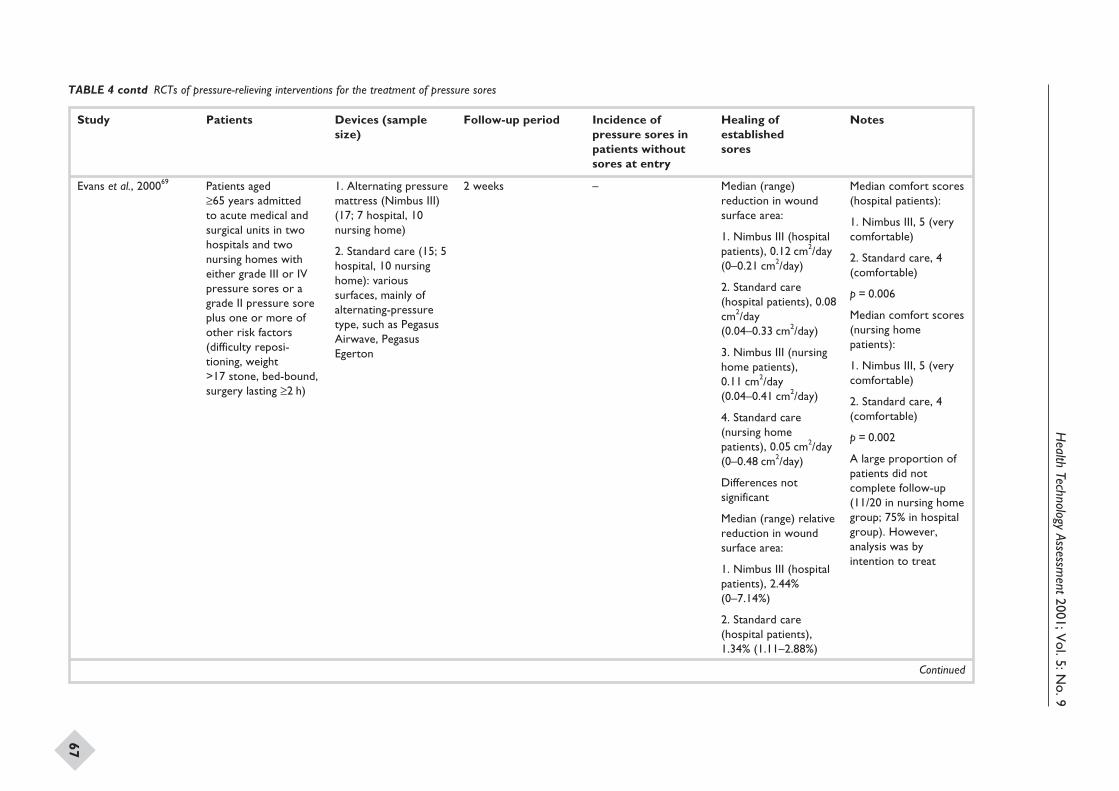
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
67
Study Patients Devices (samplesize)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
Evans et al., 200069 Patients aged≥65 years admittedto acute medical andsurgical units in twohospitals and twonursing homes witheither grade III or IVpressure sores or agrade II pressure soreplus one or more ofother risk factors(difficulty reposi-tioning, weight>17 stone, bed-bound,surgery lasting ≥2 h)
1. Alternating pressuremattress (Nimbus III)(17; 7 hospital, 10nursing home)
2. Standard care (15; 5hospital, 10 nursinghome): varioussurfaces, mainly ofalternating-pressuretype, such as PegasusAirwave, PegasusEgerton
2 weeks – Median (range)reduction in woundsurface area:
1. Nimbus III (hospitalpatients), 0.12 cm2/day(0–0.21 cm2/day)
2. Standard care(hospital patients), 0.08cm2/day(0.04–0.33 cm2/day)
3. Nimbus III (nursinghome patients),0.11 cm2/day(0.04–0.41 cm2/day)
4. Standard care(nursing homepatients), 0.05 cm2/day(0–0.48 cm2/day)
Differences notsignificant
Median (range) relativereduction in woundsurface area:
1. Nimbus III (hospitalpatients), 2.44%(0–7.14%)
2. Standard care(hospital patients),1.34% (1.11–2.88%)
Median comfort scores(hospital patients):
1. Nimbus III, 5 (verycomfortable)
2. Standard care, 4(comfortable)
p = 0.006
Median comfort scores(nursing homepatients):
1. Nimbus III, 5 (verycomfortable)
2. Standard care, 4(comfortable)
p = 0.002
A large proportion ofpatients did notcomplete follow-up(11/20 in nursing homegroup; 75% in hospitalgroup). However,analysis was byintention to treat
Continued
TABLE 4 contd RCTs of pressure-relieving interventions for the treatment of pressure sores
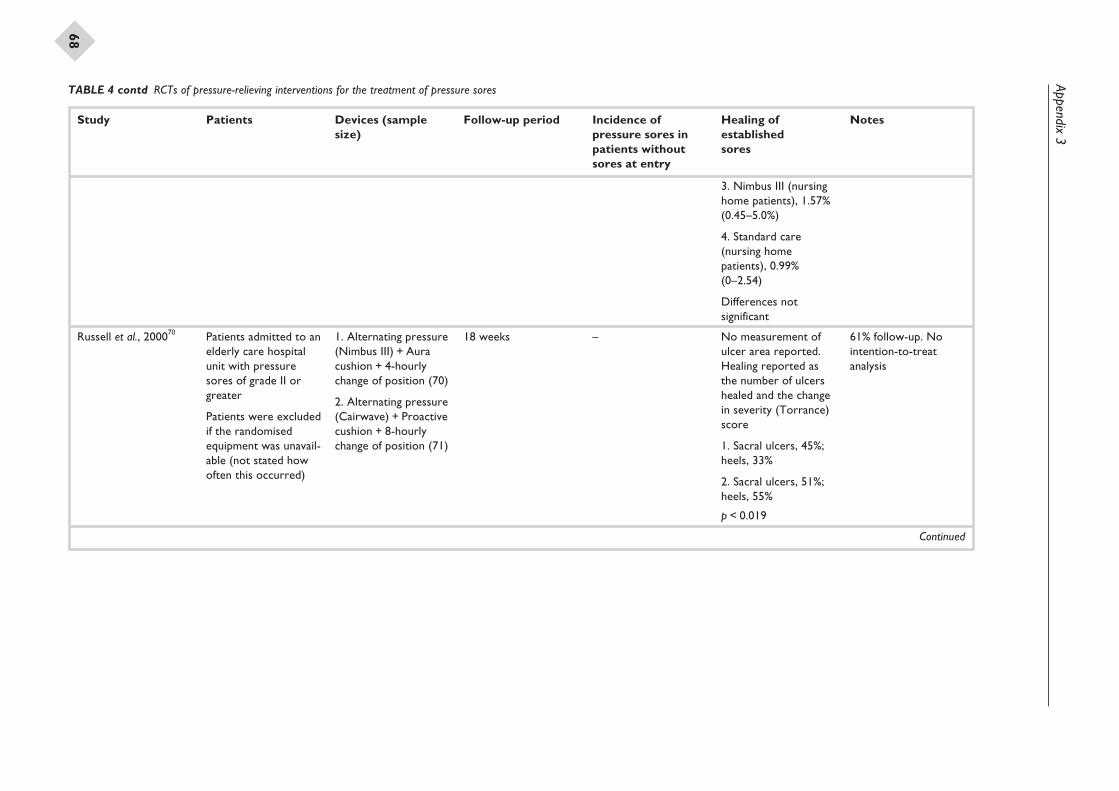
Appendix3
68
Study Patients Devices (samplesize)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
3. Nimbus III (nursinghome patients), 1.57%(0.45–5.0%)
4. Standard care(nursing homepatients), 0.99%(0–2.54)
Differences notsignificant
Russell et al., 200070 Patients admitted to anelderly care hospitalunit with pressuresores of grade II orgreater
Patients were excludedif the randomisedequipment was unavail-able (not stated howoften this occurred)
1. Alternating pressure(Nimbus III) + Auracushion + 4-hourlychange of position (70)
2. Alternating pressure(Cairwave) + Proactivecushion + 8-hourlychange of position (71)
18 weeks – No measurement ofulcer area reported.Healing reported asthe number of ulcershealed and the changein severity (Torrance)score
1. Sacral ulcers, 45%;heels, 33%
2. Sacral ulcers, 51%;heels, 55%
p < 0.019
61% follow-up. Nointention-to-treatanalysis
Continued
TABLE 4 contd RCTs of pressure-relieving interventions for the treatment of pressure sores
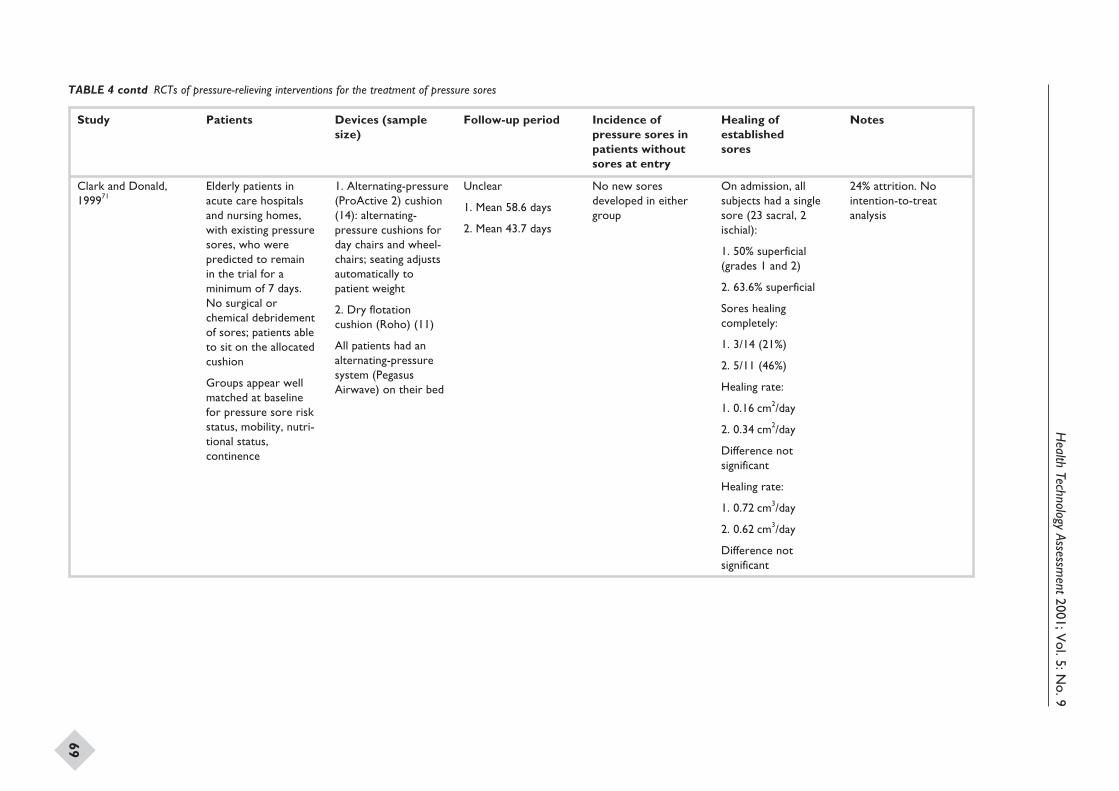
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
69
Study Patients Devices (samplesize)
Follow-up period Incidence ofpressure sores inpatients withoutsores at entry
Healing ofestablishedsores
Notes
Clark and Donald,199971
Elderly patients inacute care hospitalsand nursing homes,with existing pressuresores, who werepredicted to remainin the trial for aminimum of 7 days.No surgical orchemical debridementof sores; patients ableto sit on the allocatedcushion
Groups appear wellmatched at baselinefor pressure sore riskstatus, mobility, nutri-tional status,continence
1. Alternating-pressure(ProActive 2) cushion(14): alternating-pressure cushions forday chairs and wheel-chairs; seating adjustsautomatically topatient weight
2. Dry flotationcushion (Roho) (11)
All patients had analternating-pressuresystem (PegasusAirwave) on their bed
Unclear
1. Mean 58.6 days
2. Mean 43.7 days
No new soresdeveloped in eithergroup
On admission, allsubjects had a singlesore (23 sacral, 2ischial):
1. 50% superficial(grades 1 and 2)
2. 63.6% superficial
Sores healingcompletely:
1. 3/14 (21%)
2. 5/11 (46%)
Healing rate:
1. 0.16 cm2/day
2. 0.34 cm2/day
Difference notsignificant
Healing rate:
1. 0.72 cm3/day
2. 0.62 cm3/day
Difference notsignificant
24% attrition. Nointention-to-treatanalysis
TABLE 4 contd RCTs of pressure-relieving interventions for the treatment of pressure sores
Appendix 4
Quality assessment of included studies
Health Technology Assessment 2001; Vol. 5: No. 9
71
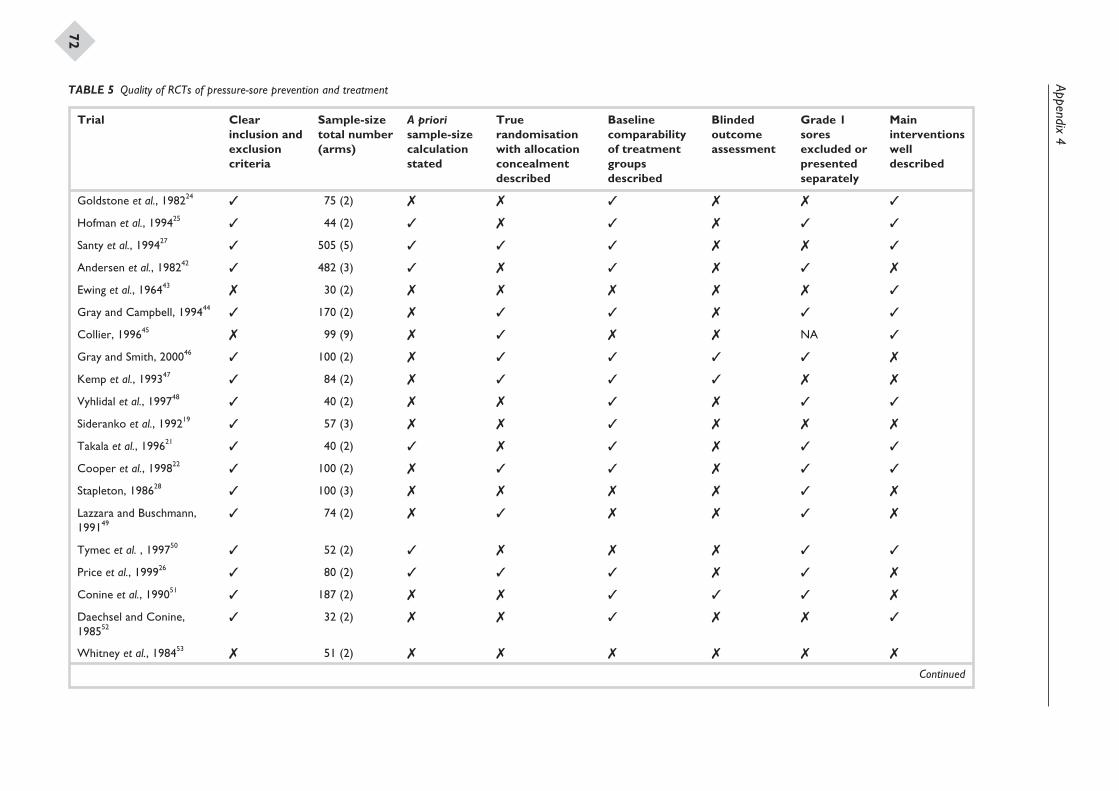
Appendix4
72
Trial Clearinclusion andexclusioncriteria
Sample-sizetotal number(arms)
A priorisample-sizecalculationstated
Truerandomisationwith allocationconcealmentdescribed
Baselinecomparabilityof treatmentgroupsdescribed
Blindedoutcomeassessment
Grade 1soresexcluded orpresentedseparately
Maininterventionswelldescribed
Goldstone et al., 198224 3 75 (2) 7 7 3 7 7 3
Hofman et al., 199425 3 44 (2) 3 7 3 7 3 3
Santy et al., 199427 3 505 (5) 3 3 3 7 7 3
Andersen et al., 198242 3 482 (3) 3 7 3 7 3 7
Ewing et al., 196443 7 30 (2) 7 7 7 7 7 3
Gray and Campbell, 199444 3 170 (2) 7 3 3 7 3 3
Collier, 199645 7 99 (9) 7 3 7 7 NA 3
Gray and Smith, 200046 3 100 (2) 7 3 3 3 3 7
Kemp et al., 199347 3 84 (2) 7 3 3 3 7 7
Vyhlidal et al., 199748 3 40 (2) 7 7 3 7 3 3
Sideranko et al., 199219 3 57 (3) 7 7 3 7 7 7
Takala et al., 199621 3 40 (2) 3 7 3 7 3 3
Cooper et al., 199822 3 100 (2) 7 3 3 7 3 3
Stapleton, 198628 3 100 (3) 7 7 7 7 3 7
Lazzara and Buschmann,199149
3 74 (2) 7 3 7 7 3 7
Tymec et al. , 199750 3 52 (2) 3 7 7 7 3 3
Price et al., 199926 3 80 (2) 3 3 3 7 3 7
Conine et al., 199051 3 187 (2) 7 7 3 3 3 7
Daechsel and Conine,198552
3 32 (2) 7 7 3 7 7 3
Whitney et al., 198453 7 51 (2) 7 7 7 7 7 7
Continued
TABLE 5 Quality of RCTs of pressure-sore prevention and treatment
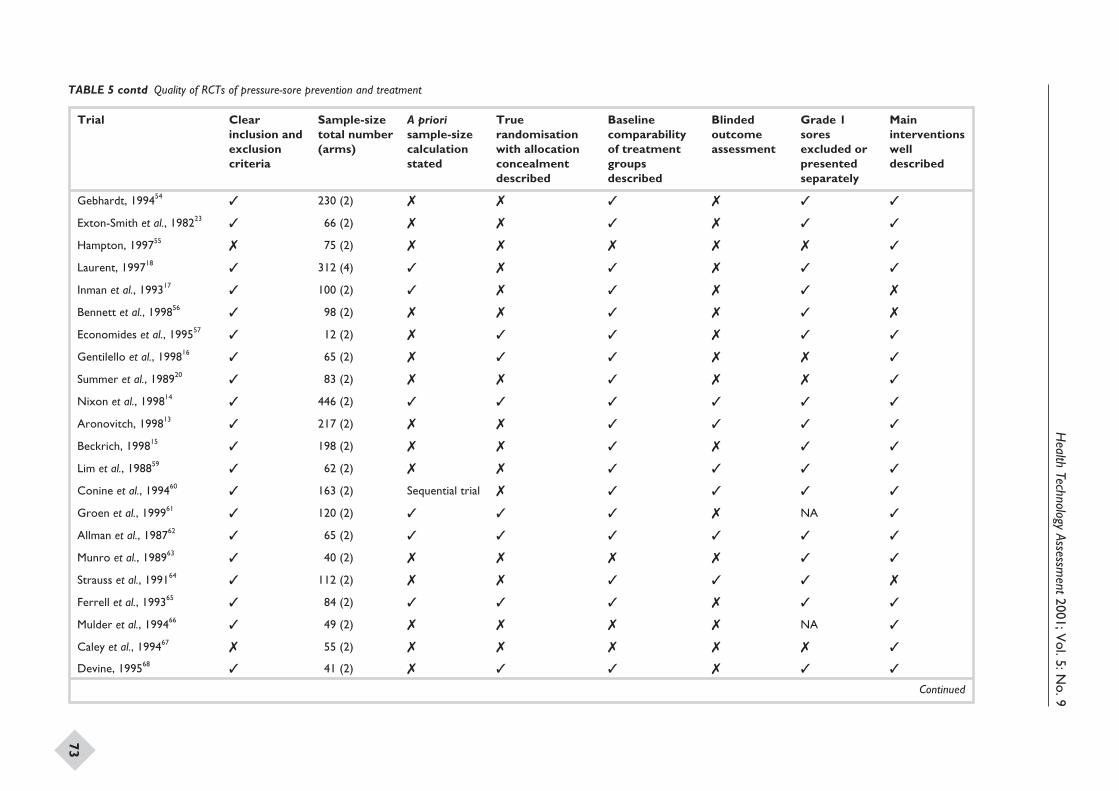
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
73
Trial Clearinclusion andexclusioncriteria
Sample-sizetotal number(arms)
A priorisample-sizecalculationstated
Truerandomisationwith allocationconcealmentdescribed
Baselinecomparabilityof treatmentgroupsdescribed
Blindedoutcomeassessment
Grade 1soresexcluded orpresentedseparately
Maininterventionswelldescribed
Gebhardt, 199454 3 230 (2) 7 7 3 7 3 3
Exton-Smith et al., 198223 3 66 (2) 7 7 3 7 3 3
Hampton, 199755 7 75 (2) 7 7 7 7 7 3
Laurent, 199718 3 312 (4) 3 7 3 7 3 3
Inman et al., 199317 3 100 (2) 3 7 3 7 3 7
Bennett et al., 199856 3 98 (2) 7 7 3 7 3 7
Economides et al., 199557 3 12 (2) 7 3 3 7 3 3
Gentilello et al., 199816 3 65 (2) 7 3 3 7 7 3
Summer et al., 198920 3 83 (2) 7 7 3 7 7 3
Nixon et al., 199814 3 446 (2) 3 3 3 3 3 3
Aronovitch, 199813 3 217 (2) 7 7 3 3 3 3
Beckrich, 199815 3 198 (2) 7 7 3 7 3 3
Lim et al., 198859 3 62 (2) 7 7 3 3 3 3
Conine et al., 199460 3 163 (2) Sequential trial 7 3 3 3 3
Groen et al., 199961 3 120 (2) 3 3 3 7 NA 3
Allman et al., 198762 3 65 (2) 3 3 3 3 3 3
Munro et al., 198963 3 40 (2) 7 7 7 7 3 3
Strauss et al., 199164 3 112 (2) 7 7 3 3 3 7
Ferrell et al., 199365 3 84 (2) 3 3 3 7 3 3
Mulder et al., 199466 3 49 (2) 7 7 7 7 NA 3
Caley et al., 199467 7 55 (2) 7 7 7 7 7 3
Devine, 199568 3 41 (2) 7 3 3 7 3 3
Continued
TABLE 5 contd Quality of RCTs of pressure-sore prevention and treatment
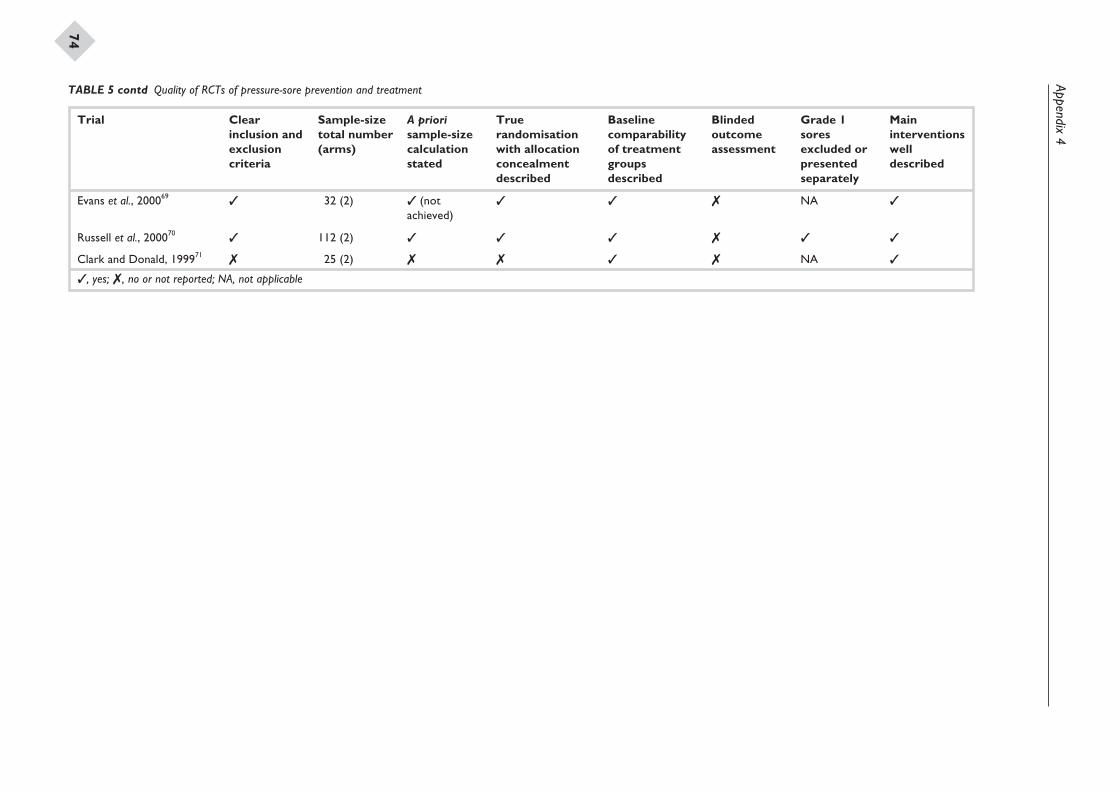
Appendix4
74
Trial Clearinclusion andexclusioncriteria
Sample-sizetotal number(arms)
A priorisample-sizecalculationstated
Truerandomisationwith allocationconcealmentdescribed
Baselinecomparabilityof treatmentgroupsdescribed
Blindedoutcomeassessment
Grade 1soresexcluded orpresentedseparately
Maininterventionswelldescribed
Evans et al., 200069 3 32 (2) 3 (notachieved)
3 3 7 NA 3
Russell et al., 200070 3 112 (2) 3 3 3 7 3 3
Clark and Donald, 199971 7 25 (2) 7 7 3 7 NA 3
, yes; , no or not reported; NA, not applicable
TABLE 5 contd Quality of RCTs of pressure-sore prevention and treatment
Appendix 5
Comparisons undertaken in the included studies
Health Technology Assessment 2001; Vol. 5: No. 9
75
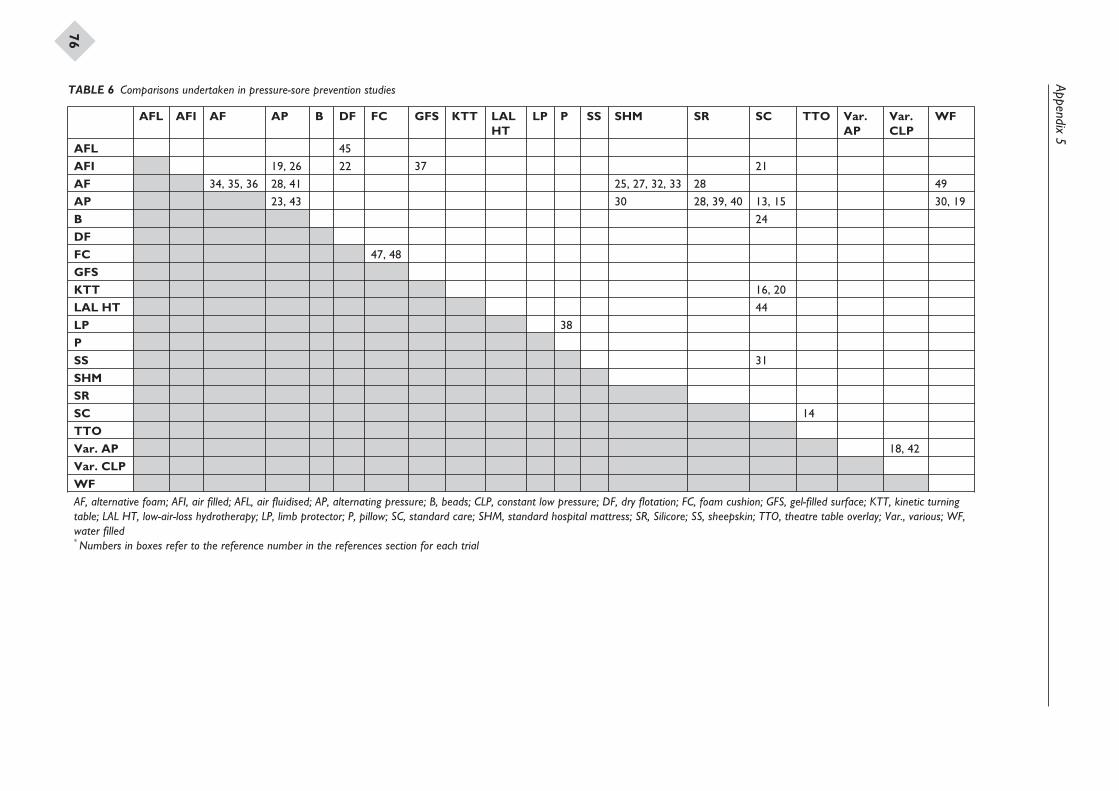
Appendix5
76
AFL AFI AF AP B DF FC GFS KTT LALHT
LP P SS SHM SR SC TTO Var.AP
Var.CLP
WF
AFL 45
AFI 19, 26 22 37 21
AF 34, 35, 36 28, 41 25, 27, 32, 33 28 49
AP 23, 43 30 28, 39, 40 13, 15 30, 19
B 24
DF
FC 47, 48
GFS
KTT 16, 20
LAL HT 44
LP 38
P
SS 31
SHM
SR
SC 14
TTO
Var. AP 18, 42
Var. CLP
WFAF, alternative foam; AFI, air filled; AFL, air fluidised; AP, alternating pressure; B, beads; CLP, constant low pressure; DF, dry flotation; FC, foam cushion; GFS, gel-filled surface; KTT, kinetic turningtable; LAL HT, low-air-loss hydrotherapy; LP, limb protector; P, pillow; SC, standard care; SHM, standard hospital mattress; SR, Silicore; SS, sheepskin; TTO, theatre table overlay; Var., various; WF,water filled* Numbers in boxes refer to the reference number in the references section for each trial
TABLE 6 Comparisons undertaken in pressure-sore prevention studies
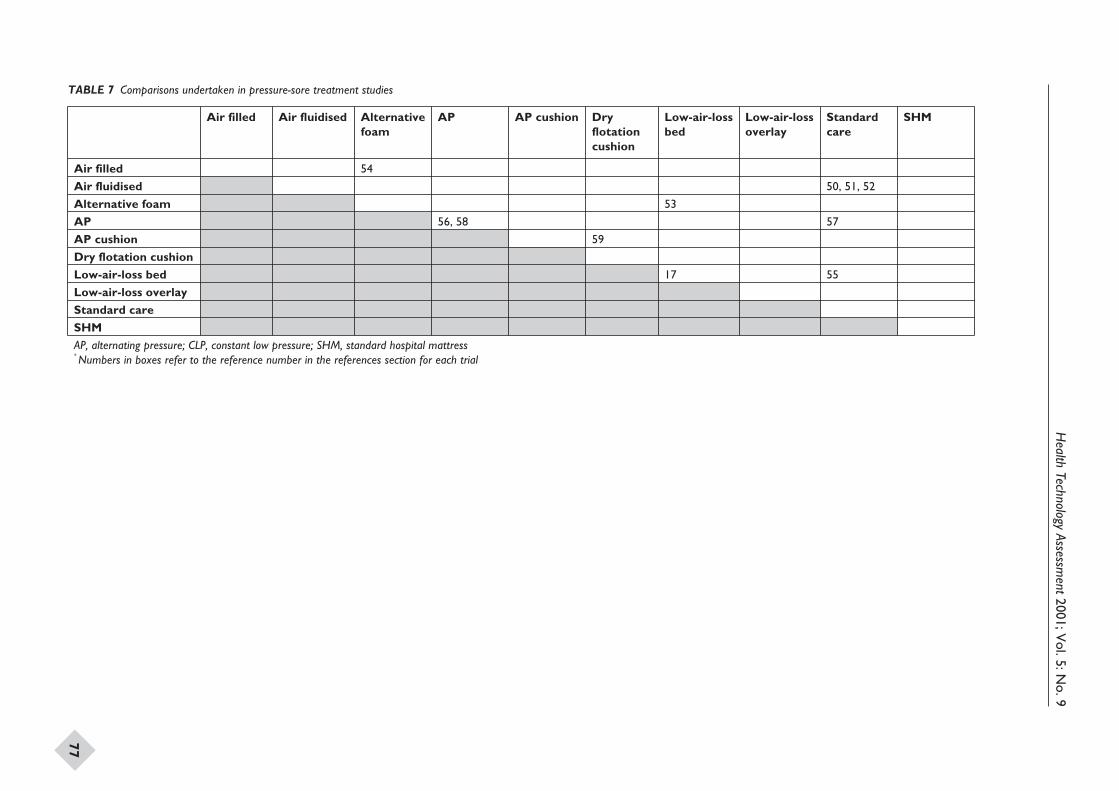
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
77
Air filled Air fluidised Alternativefoam
AP AP cushion Dryflotationcushion
Low-air-lossbed
Low-air-lossoverlay
Standardcare
SHM
Air filled 54
Air fluidised 50, 51, 52
Alternative foam 53
AP 56, 58 57
AP cushion 59
Dry flotation cushion
Low-air-loss bed 17 55
Low-air-loss overlay
Standard care
SHMAP, alternating pressure; CLP, constant low pressure; SHM, standard hospital mattress* Numbers in boxes refer to the reference number in the references section for each trial
TABLE 7 Comparisons undertaken in pressure-sore treatment studies
Systematic reviews of wound caremanagement (6): compression for theprevention and treatment of venous legulcers
N Cullum*
EA Nelson
Centre for Evidence Based Nursing, Department of Health Studies,University of York, UK
* Corresponding author
Competing interests: N Cullum has: received funds from the NHS R&D Programmeto undertake primary research in wound care; received sponsorship of trial-relatededucational meetings from Huntleigh Healthcare and Beiersdorf Ltd. EA Nelson has:conducted one of the trials reviewed; been reimbursed for attending symposia by Smithand Nephew Ltd, ConvaTec and Huntleigh Healthcare

List of abbreviations ......................................... 83
Executive summary to Part 6 ......................... 85
1 Introduction .................................................. 87Aims ................................................................ 88
2 Methods ......................................................... 89Search strategy ............................................... 89Inclusion and exclusion criteria ................... 89Data extraction .............................................. 90Methodological quality .................................. 90Data synthesis ................................................. 90
3 Results ............................................................ 91Studies included in the review ...................... 91Studies excluded from the review ................ 91Methodological quality of includedstudies ............................................................. 91Presentation of results ................................... 92Application of compression bandages orstockings to prevent breakdown of legs atrisk of venous ulceration ............................... 92Application of compression bandages orstockings to aid venous ulcer healing .......... 92Clinical effectiveness of compressionbandage and stocking systems ...................... 93
Cost-effectiveness of compression bandageand stocking systems ...................................... 94
4 Discussion ...................................................... 101
5 Conclusions ................................................... 103Implications for practice ............................... 103Implications for research .............................. 103Methodological recommendations .............. 103Priority research questions ............................ 104
Acknowledgements ..................................... 105
References ..................................................... 107
Appendix 1 Databases searched andsearch strategies ............................................. 111
Appendix 2 Advisory panel ....................... 115
Appendix 3 Summary of includedstudies ............................................................. 117
Appendix 4 Quality assessment ofincluded studies ............................................. 133
Health Technology Assessment 2001; Vol. 5: No. 9
81
Contents to Part 6

Health Technology Assessment 2001; Vol. 5: No. 9
83
List of abbreviations
ABPI ankle/brachial pressure index
CCT controlled clinical trial
CI confidence interval
df degrees of freedom
RCT randomised controlled trial
RR relative risk

Background
Leg ulceration is a common, recurring conditionwhich affects around three in every 2000 adults inthe UK. Most people with leg ulcers are elderlywomen. There is a considerable cost to the patientin terms of pain, social isolation and quality of life.The health service provides nursing and medicalcare, as well as dressings, bandages and drug treat-ments. Most leg ulcers are associated with venousdisease and this is treated by preventing venoushypertension through the application of externalgraduated compression.
There are many methods of applying externalgraduated compression, such as elasticatedbandages, Unna’s boots (non-compliant, plaster-type bandages), multilayer elastic compressionbandages, short stretch bandages and elastomerichosiery (stockings).
Objectives
To assess the clinical effectiveness and cost-effectiveness of compression bandaging andstockings in the prevention and treatment ofvenous leg ulcers. The research questions were:
• Does the application of compression bandagesor stockings to legs at risk of venous ulcerationprevent skin breakdown?
• If compression prevents recurrence, what is theoptimal level of compression?
• Does the application of compression bandagesor stockings aid the healing of venous ulcers?
• What is the optimum level of compression?• Which compression bandage or stocking system
is the most clinically effective for healing venousulcers?
• Which system is the most cost-effective inhealing venous ulcers?
Methods
Data sourcesSearches were made of 19 databases (includingMEDLINE, CINAHL, EMBASE and CENTRAL),
and journals, conference proceedings and bibliog-raphies were handsearched. Manufacturers of com-pression bandages and stockings and an advisorypanel were contacted for unpublished studies.Searches were completed in December 1999.
Study selectionRandomised trials that evaluated compressionbandaging or stockings, either for the preventionof or as a treatment for venous leg ulcers, wereincluded in the review. There was no restrictionon date or language. Ulcer incidence and healingwere the primary endpoints. Prevention trialswere only included if they provided data on ulcerincidence. Healing trials were only included if theyprovided objective data on the rate of ulcer healingor the number of ulcers healing in the trial period.
Data extraction and synthesisDetails of eligible studies were extracted andsummarised using a data extraction sheet. Dataextraction was verified independently by tworeviewers.
Results
Twenty four trials reporting 26 comparisons wereincluded in the review (two in ulcer prevention,24 in ulcer treatment). High compression wasmore effective than moderate compression inpreventing ulceration (one trial), and one trialfound no difference in healing rates between twomeans of applying moderate compression.
Compression was more effective in healing ulcersthan was no compression (4/6 trials). Whenmultilayered systems were compared, elasticcompression was more effective at healing ulcersthan was non-elastic compression (five trials).There was no difference in healing rates betweenfour-layer bandaging and other high-compressionmultilayered systems (three trials). There wasno difference in healing rates between differentelastomeric multilayered systems (four trials).Multilayered high-compression was more effectivein healing ulcers than was single-layer compression(four trials). Compression stockings for healingwere evaluated in two trials. One found a high-
Health Technology Assessment 2001; Vol. 5: No. 9
85
Executive summary to Part 6
compression stocking plus a thrombostocking tobe more effective than a short stretch bandage.A second small trial reported no difference inoutcome between a compression stocking andUnna’s boot.
There were insufficient data to draw conclusionsabout the relative cost-effectiveness of differentregimens.
Conclusions
Prevention of recurrence of legulcerationThere is evidence from one large trial that high-compression stockings are more effective atpreventing recurrence of leg ulcers than aremoderate-compression stockings.
Healing of ulcersCompression increases ulcer healing ratescompared with no compression. Multilayeredsystems are more effective than single-layeredsystems. High compression is more effective thanlow compression, but there are no clear differencesin the effectiveness of different types of highcompression (e.g. Unna’s boot, compressionhosiery, multilayer high-compression elastomericregimens, short-stretch bandages).
Implications for researchPriority questions that have not been answered bythe research published to date are:
• At what level of the ankle/brachial pressureindex is it safe to apply compression?
• What is the most reliable method of identifyingthose venous leg ulcer patients with concurrentdiabetes or rheumatoid arthritis who wouldbenefit from compression?
• Which are the most effective multilayered high-compression regimens in terms of cost andquality of life?
• Which are the most effective non-elastomericcompression regimens in terms of cost andquality of life?
• What contribution can self-care and lay caremake towards improving quality of life inpatients with venous leg ulcers?
• What are the most effective ways of deliveringcompression to prevent recurrence of venousulcers once healed (e.g. one high compressionsock or stocking compared to two socks orstockings, each applying moderatecompression)?
• What is an acceptable rate of adverse events forthe widely used compression regimens?
Methodological issues that need to be addressed infuture trials are:
• Trial numbers should be based on an a priorisample-size calculation so that clinicallyimportant differences can be detected asstatistically significant.
• Patients receiving different interventions shouldbe comparable at the start of the trial. Thismay require paired randomisation or stratifiedrandomisation in order to ensure that factorswhich may influence healing are equallydistributed between treatment groups.
• Assessment of outcomes should be blind totreatment.
• To ensure the inclusion of all clinical trials insystematic reviews, prospective registration ofresearch studies should become mandatory.
• Contemporaneous economic evaluations shouldbe conducted in future trials.
• A complete and thorough description of themethod of application of compression and anyconcurrent treatments, including dressings,should be given in trial reports.
• Ulcer healing should be expressed as both arelative and an absolute change in area.
• For each patient, a single reference ulcer shouldbe selected. Multiple ulcers on a patient shouldnot be included in the analysis as individualulcers are not independent unless specialisedstatistical analysis is performed to separateout the effects of the intervention (i.e. matchedpairs analysis). Survival-rate analysis shouldbe adopted for all studies that assess ulcerincidence or healing.
Executive summary
86

The prevalence of active leg ulceration in theUK has been estimated at 1.5/1000,1,2 and a
similar rate has been reported in Australia.3 Preva-lence increases with age, and is higher in women.Leg ulceration is typically a chronic recurringcondition, with 45% of patients in a Scottish studyreporting episodes of ulceration for more than 10years.1 There is a considerable cost both to thepatient4 and to the health service.5 Most leg ulcersare associated with venous disease, and a historyof a deep vein thrombosis is widely regarded as apredisposing factor to venous insufficiency andhence venous ulceration. However, the aetiology ofleg ulceration remains poorly understood. Venousinsufficiency has been shown to be associated withincreased hydrostatic pressure in the veins of theleg, and it is in an attempt to reverse this and aidvenous return that external compression, invarious forms, is applied as a therapy for venous legulcers.
Various forms of bandaging have been appliedover the years. In the seventeenth century,compression was applied as rigid lace-up stockings,while elasticated bandages were first produced inthe middle of the nineteenth century.6 At presentthere is wide variation in the management ofvenous leg ulcers. In the USA, Unna’s boot (anon-compliant, plaster-type bandage) is favoured;in the UK, multilayer elastic compression is widelyused; while in mainland Europe and Australiathe inelastic, short stretch bandaging is common.This review summarises the evidence for theeffectiveness of the different forms of compressionbandaging and compression stockings for venousleg ulcers. Devices that apply intermittent orpulsed compression to the limb were specificallyexcluded from this review.
There are many ways of applying compression(e.g. a single layer of bandage, multiple layers ofbandages, compression stockings, combinationsof bandages and/or stockings). The interpretationof comparisons between compression systems iscomplicated by the lack of internationally agreedperformance standards; for example, the classi-fication systems for compression stockings aredifferent in the UK and in mainland Europe. Inthe UK, performance indicators for bandages andcompression stockings have been developed.7
Stockings are classified according to the amount offorce required to extend them and hence the levelof compression they can apply to a limb (Table 1).
Bandages are categorised as retention, supportor compression, depending on their performancein standardised laboratory tests. Compressionbandages are further subdivided according to theamount of force required to extend them, andtherefore the level of compression which they canapply to a limb (Table 2). It is important to notethat the laboratory performance or classificationof a bandage may not reflect its performance inclinical use, as this is dependent on the techniqueof application and operator training.
Compression systems consisting of combinations ofcompression layers (stockings and/or bandages),sometimes incorporating an initial layer of pastebandage or orthopaedic wool, are commonly used.A number of these are listed in Box 1.
The use of compression to enhance venous returnand aid the healing of venous ulcers is not withoutrisk. The external application of very high pres-sures will reduce the blood supply to the skin and
Health Technology Assessment 2001; Vol. 5: No. 9
87
Chapter 1
Introduction
Class Support level Compression exerted Uses
1 Light 14–17 mmHg at the ankle Treatment of varicose veins
2 Medium 18–24 mmHg at the ankle Treatment of more severe varicosities;prevention of venous leg ulcers
3 Strong 25–35 mmHg at the ankle Treatment of severe chronic hypertension andsevere varicose veins; prevention of venous legulcers
TABLE 1 Classification of compression hosiery in the UK
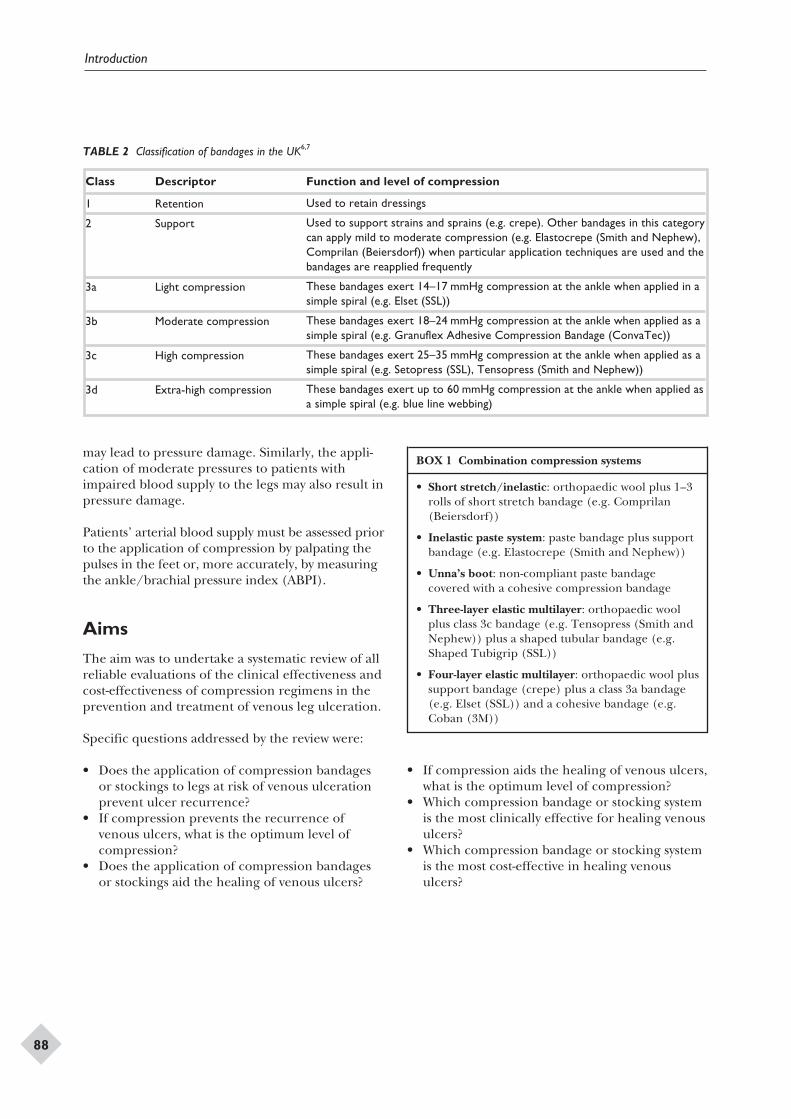
may lead to pressure damage. Similarly, the appli-cation of moderate pressures to patients withimpaired blood supply to the legs may also result inpressure damage.
Patients’ arterial blood supply must be assessed priorto the application of compression by palpating thepulses in the feet or, more accurately, by measuringthe ankle/brachial pressure index (ABPI).
Aims
The aim was to undertake a systematic review of allreliable evaluations of the clinical effectiveness andcost-effectiveness of compression regimens in theprevention and treatment of venous leg ulceration.
Specific questions addressed by the review were:
• Does the application of compression bandagesor stockings to legs at risk of venous ulcerationprevent ulcer recurrence?
• If compression prevents the recurrence ofvenous ulcers, what is the optimum level ofcompression?
• Does the application of compression bandagesor stockings aid the healing of venous ulcers?
• If compression aids the healing of venous ulcers,what is the optimum level of compression?
• Which compression bandage or stocking systemis the most clinically effective for healing venousulcers?
• Which compression bandage or stocking systemis the most cost-effective in healing venousulcers?
Introduction
88
Class Descriptor Function and level of compression
1 Retention Used to retain dressings
2 Support Used to support strains and sprains (e.g. crepe). Other bandages in this categorycan apply mild to moderate compression (e.g. Elastocrepe (Smith and Nephew),Comprilan (Beiersdorf)) when particular application techniques are used and thebandages are reapplied frequently
3a Light compression These bandages exert 14–17 mmHg compression at the ankle when applied in asimple spiral (e.g. Elset (SSL))
3b Moderate compression These bandages exert 18–24 mmHg compression at the ankle when applied as asimple spiral (e.g. Granuflex Adhesive Compression Bandage (ConvaTec))
3c High compression These bandages exert 25–35 mmHg compression at the ankle when applied as asimple spiral (e.g. Setopress (SSL), Tensopress (Smith and Nephew))
3d Extra-high compression These bandages exert up to 60 mmHg compression at the ankle when applied asa simple spiral (e.g. blue line webbing)
TABLE 2 Classification of bandages in the UK6,7
• Short stretch/inelastic: orthopaedic wool plus 1–3rolls of short stretch bandage (e.g. Comprilan(Beiersdorf))
• Inelastic paste system: paste bandage plus supportbandage (e.g. Elastocrepe (Smith and Nephew))
• Unna’s boot: non-compliant paste bandagecovered with a cohesive compression bandage
• Three-layer elastic multilayer: orthopaedic woolplus class 3c bandage (e.g. Tensopress (Smith andNephew)) plus a shaped tubular bandage (e.g.Shaped Tubigrip (SSL))
• Four-layer elastic multilayer: orthopaedic wool plussupport bandage (crepe) plus a class 3a bandage(e.g. Elset (SSL)) and a cohesive bandage (e.g.Coban (3M))
BOX 1 Combination compression systems
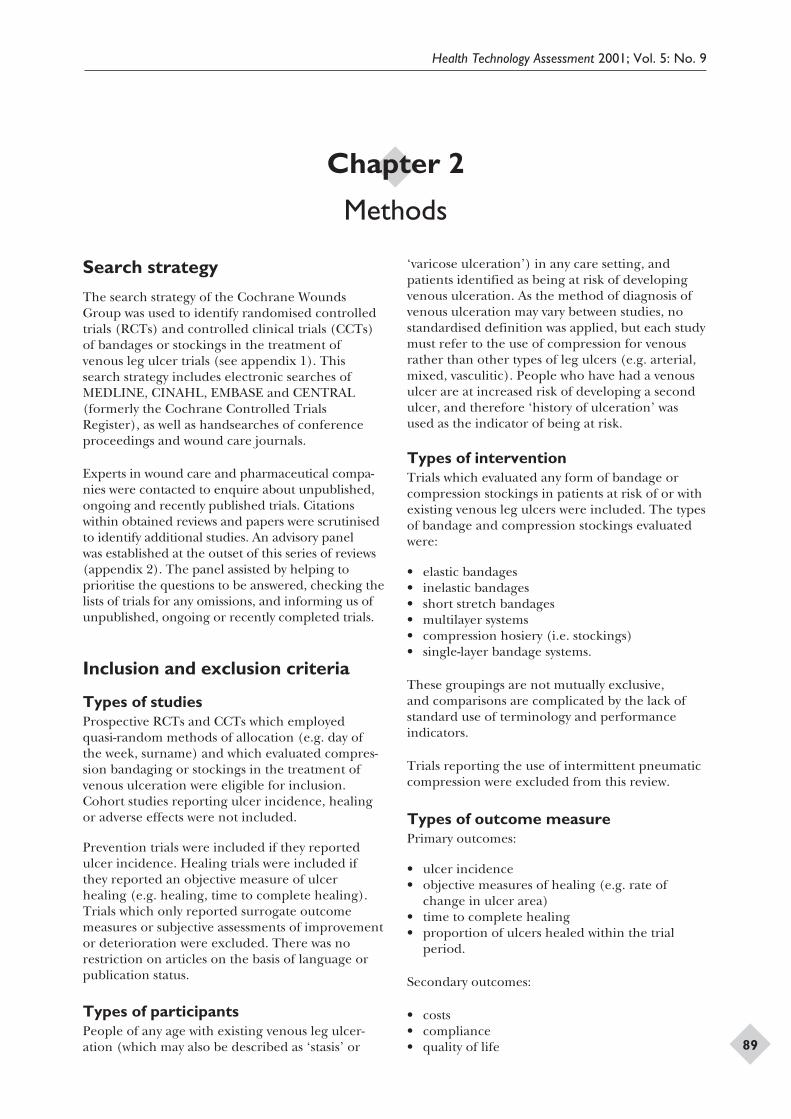
Search strategy
The search strategy of the Cochrane WoundsGroup was used to identify randomised controlledtrials (RCTs) and controlled clinical trials (CCTs)of bandages or stockings in the treatment ofvenous leg ulcer trials (see appendix 1). Thissearch strategy includes electronic searches ofMEDLINE, CINAHL, EMBASE and CENTRAL(formerly the Cochrane Controlled TrialsRegister), as well as handsearches of conferenceproceedings and wound care journals.
Experts in wound care and pharmaceutical compa-nies were contacted to enquire about unpublished,ongoing and recently published trials. Citationswithin obtained reviews and papers were scrutinisedto identify additional studies. An advisory panelwas established at the outset of this series of reviews(appendix 2). The panel assisted by helping toprioritise the questions to be answered, checking thelists of trials for any omissions, and informing us ofunpublished, ongoing or recently completed trials.
Inclusion and exclusion criteria
Types of studiesProspective RCTs and CCTs which employedquasi-random methods of allocation (e.g. day ofthe week, surname) and which evaluated compres-sion bandaging or stockings in the treatment ofvenous ulceration were eligible for inclusion.Cohort studies reporting ulcer incidence, healingor adverse effects were not included.
Prevention trials were included if they reportedulcer incidence. Healing trials were included ifthey reported an objective measure of ulcerhealing (e.g. healing, time to complete healing).Trials which only reported surrogate outcomemeasures or subjective assessments of improvementor deterioration were excluded. There was norestriction on articles on the basis of language orpublication status.
Types of participantsPeople of any age with existing venous leg ulcer-ation (which may also be described as ‘stasis’ or
‘varicose ulceration’) in any care setting, andpatients identified as being at risk of developingvenous ulceration. As the method of diagnosis ofvenous ulceration may vary between studies, nostandardised definition was applied, but each studymust refer to the use of compression for venousrather than other types of leg ulcers (e.g. arterial,mixed, vasculitic). People who have had a venousulcer are at increased risk of developing a secondulcer, and therefore ‘history of ulceration’ wasused as the indicator of being at risk.
Types of interventionTrials which evaluated any form of bandage orcompression stockings in patients at risk of or withexisting venous leg ulcers were included. The typesof bandage and compression stockings evaluatedwere:
• elastic bandages• inelastic bandages• short stretch bandages• multilayer systems• compression hosiery (i.e. stockings)• single-layer bandage systems.
These groupings are not mutually exclusive,and comparisons are complicated by the lack ofstandard use of terminology and performanceindicators.
Trials reporting the use of intermittent pneumaticcompression were excluded from this review.
Types of outcome measurePrimary outcomes:
• ulcer incidence• objective measures of healing (e.g. rate of
change in ulcer area)• time to complete healing• proportion of ulcers healed within the trial
period.
Secondary outcomes:
• costs• compliance• quality of life
Health Technology Assessment 2001; Vol. 5: No. 9
89
Chapter 2
Methods
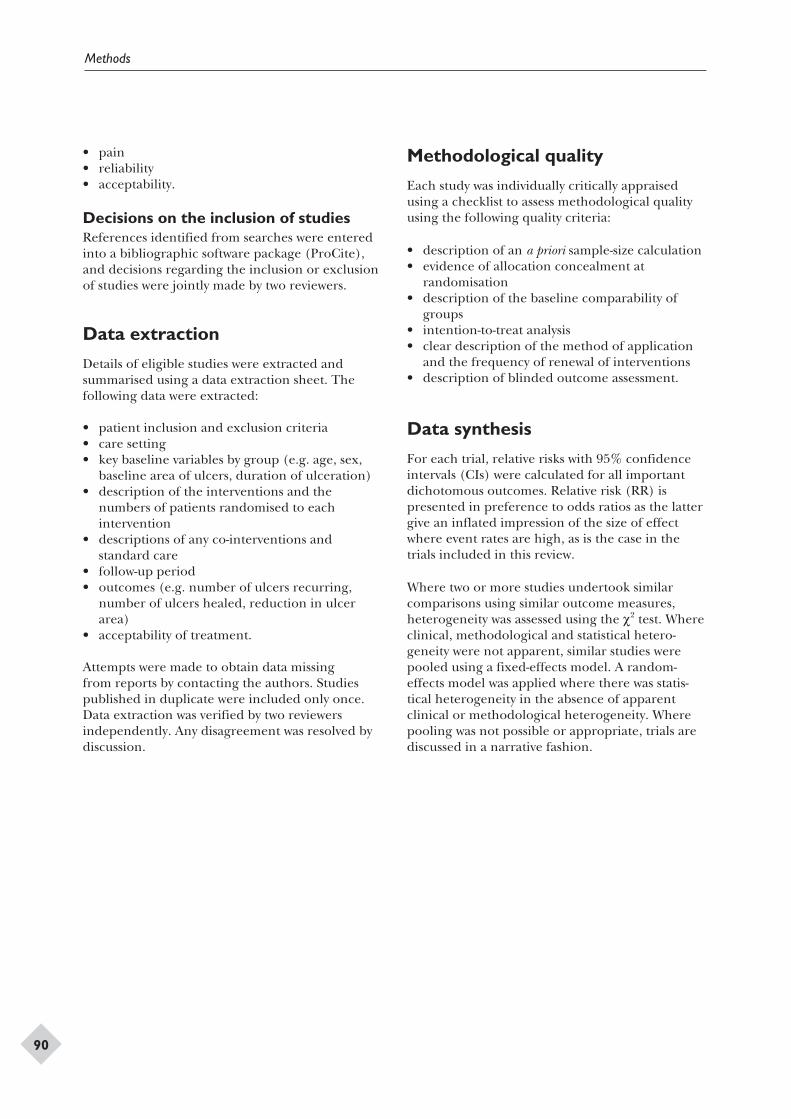
• pain• reliability• acceptability.
Decisions on the inclusion of studiesReferences identified from searches were enteredinto a bibliographic software package (ProCite),and decisions regarding the inclusion or exclusionof studies were jointly made by two reviewers.
Data extraction
Details of eligible studies were extracted andsummarised using a data extraction sheet. Thefollowing data were extracted:
• patient inclusion and exclusion criteria• care setting• key baseline variables by group (e.g. age, sex,
baseline area of ulcers, duration of ulceration)• description of the interventions and the
numbers of patients randomised to eachintervention
• descriptions of any co-interventions andstandard care
• follow-up period• outcomes (e.g. number of ulcers recurring,
number of ulcers healed, reduction in ulcerarea)
• acceptability of treatment.
Attempts were made to obtain data missingfrom reports by contacting the authors. Studiespublished in duplicate were included only once.Data extraction was verified by two reviewersindependently. Any disagreement was resolved bydiscussion.
Methodological quality
Each study was individually critically appraisedusing a checklist to assess methodological qualityusing the following quality criteria:
• description of an a priori sample-size calculation• evidence of allocation concealment at
randomisation• description of the baseline comparability of
groups• intention-to-treat analysis• clear description of the method of application
and the frequency of renewal of interventions• description of blinded outcome assessment.
Data synthesis
For each trial, relative risks with 95% confidenceintervals (CIs) were calculated for all importantdichotomous outcomes. Relative risk (RR) ispresented in preference to odds ratios as the lattergive an inflated impression of the size of effectwhere event rates are high, as is the case in thetrials included in this review.
Where two or more studies undertook similarcomparisons using similar outcome measures,heterogeneity was assessed using the c2 test. Whereclinical, methodological and statistical hetero-geneity were not apparent, similar studies werepooled using a fixed-effects model. A random-effects model was applied where there was statis-tical heterogeneity in the absence of apparentclinical or methodological heterogeneity. Wherepooling was not possible or appropriate, trials arediscussed in a narrative fashion.
Methods
90
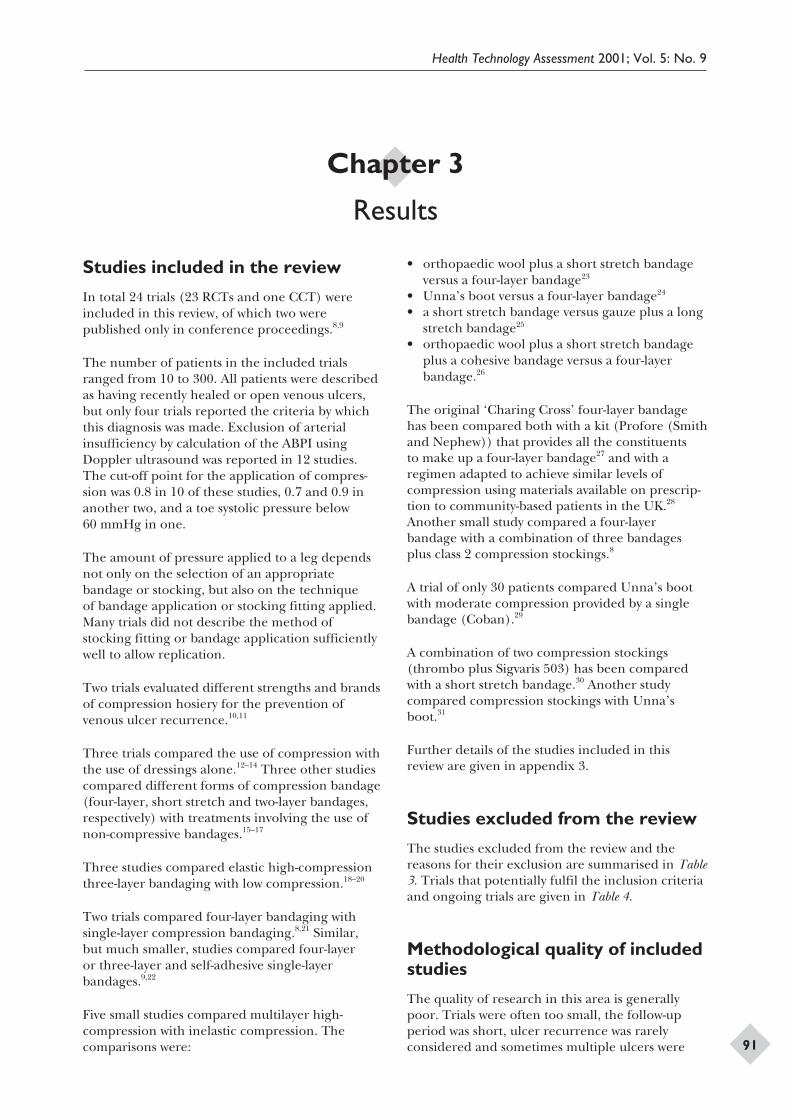
Studies included in the review
In total 24 trials (23 RCTs and one CCT) wereincluded in this review, of which two werepublished only in conference proceedings.8,9
The number of patients in the included trialsranged from 10 to 300. All patients were describedas having recently healed or open venous ulcers,but only four trials reported the criteria by whichthis diagnosis was made. Exclusion of arterialinsufficiency by calculation of the ABPI usingDoppler ultrasound was reported in 12 studies.The cut-off point for the application of compres-sion was 0.8 in 10 of these studies, 0.7 and 0.9 inanother two, and a toe systolic pressure below60 mmHg in one.
The amount of pressure applied to a leg dependsnot only on the selection of an appropriatebandage or stocking, but also on the techniqueof bandage application or stocking fitting applied.Many trials did not describe the method ofstocking fitting or bandage application sufficientlywell to allow replication.
Two trials evaluated different strengths and brandsof compression hosiery for the prevention ofvenous ulcer recurrence.10,11
Three trials compared the use of compression withthe use of dressings alone.12–14 Three other studiescompared different forms of compression bandage(four-layer, short stretch and two-layer bandages,respectively) with treatments involving the use ofnon-compressive bandages.15–17
Three studies compared elastic high-compressionthree-layer bandaging with low compression.18–20
Two trials compared four-layer bandaging withsingle-layer compression bandaging.8,21 Similar,but much smaller, studies compared four-layeror three-layer and self-adhesive single-layerbandages.9,22
Five small studies compared multilayer high-compression with inelastic compression. Thecomparisons were:
• orthopaedic wool plus a short stretch bandageversus a four-layer bandage23
• Unna’s boot versus a four-layer bandage24
• a short stretch bandage versus gauze plus a longstretch bandage25
• orthopaedic wool plus a short stretch bandageplus a cohesive bandage versus a four-layerbandage.26
The original ‘Charing Cross’ four-layer bandagehas been compared both with a kit (Profore (Smithand Nephew)) that provides all the constituentsto make up a four-layer bandage27 and with aregimen adapted to achieve similar levels ofcompression using materials available on prescrip-tion to community-based patients in the UK.28
Another small study compared a four-layerbandage with a combination of three bandagesplus class 2 compression stockings.8
A trial of only 30 patients compared Unna’s bootwith moderate compression provided by a singlebandage (Coban).29
A combination of two compression stockings(thrombo plus Sigvaris 503) has been comparedwith a short stretch bandage.30 Another studycompared compression stockings with Unna’sboot.31
Further details of the studies included in thisreview are given in appendix 3.
Studies excluded from the review
The studies excluded from the review and thereasons for their exclusion are summarised in Table3. Trials that potentially fulfil the inclusion criteriaand ongoing trials are given in Table 4.
Methodological quality of includedstudies
The quality of research in this area is generallypoor. Trials were often too small, the follow-upperiod was short, ulcer recurrence was rarelyconsidered and sometimes multiple ulcers were
Health Technology Assessment 2001; Vol. 5: No. 9
91
Chapter 3
Results

incorrectly regarded as independent. Severalpapers did not report the method of bandageapplication, the experience of staff and otheraspects of bandage use and patient mobility.The same system applied by different staff underdifferent circumstances may result in the attain-ment of widely different pressures, thus makinginterpretation of results difficult.
The quality indicators of the included trials aresummarised in appendix 4.
Presentation of results
Results of dichotomous variables are presented asrelative risks with 95% CIs. The relative risk hasbeen used rather than the odds ratio as event ratesare high in the included trials and odds ratioswould give an inflated impression of the magnitudeof effect.40 Relative risk is the ulcer healing ratein the experimental group divided by the ulcerhealing rate in the control group, and indicates thelikelihood of ulcer healing with an experimentalbandage compared with a comparison bandage.As, by definition, the risk of an ulcer healing in thecontrol group is 1, then the relative-risk reductionassociated with using the experimental bandage is1 – RR. The relative risk indicates the relativebenefit of a therapy, but not the actual benefit (i.e.it does not take into account the number of peoplein whom the ulcer would have healed anyway).The absolute risk reduction can be calculated bysubtracting the healing rate in the experimentalgroup from the healing rate in the control group.The absolute risk reduction tells us how muchthe increase in healing is due to the bandageitself. The relative benefit increase is the propor-tional increase in the rate of a good event, such ashealing, between experimental and control partici-pants, expressed as a percentage. Thus a healingrate of 30% with a control bandage, increased to50% with an experimental bandage, translates intoan absolute risk reduction of 30–50 (= –20%; or arelative benefit increase of 20%).
The results are presented with reference to theoriginal questions posed in the review.
Application of compressionbandages or stockings to preventbreakdown of legs at risk ofvenous ulceration
No studies were identified that compared ulcerincidence in people with and without compression.The trial by Harper and co-workers,10 however,suggests that there may be a dose response tocompression, and this may be indirect evidencethat compression reduces ulcer recurrence (Figure 1(for convienience, figures are grouped together atthe end of the chapter)). However, 5-year follow-updata from this trial have still to be reported.
Optimum level of compressionOne trial10 (300 patients followed up for 3–5 years)compared ulcer recurrence rates in patientsallocated to class 2 (18–25 mmHg pressure atankle) or class 3 (25–35 mmHg pressure at theankle). A lower recurrence rate was found inthe high-compression group compared with themoderate compression group (32% versus23%). Compliance was higher in the moderate-compression group, and there may be a trade-offbetween compression and compliance. The 5-yearfollow-up data from this trial are not yet available.Franks and co-workers11 compared two brands ofmoderate strength stockings (class 2) and foundno statistically significant difference in the ulcerrecurrence rate (see Figure 1).
Application of compressionbandages or stockings to aidvenous ulcer healing
In total, six RCTs investigated this aspect (Figure 2).Three trials compared the use of compression
Results
92
Study Reason for exclusion
Cameron and co-workers32 Historical control; non-randomised trial
Cherry33 Healing not measured as an outcome
Eriksson34 Essentially a comparison between dressings (paste or hydrocolloid)
Sabolinski and co-workers35 Both groups received compression; comparison was of dressings
Sironi and co-workers36 Insufficient details givenWalker and Faria37 Have abstract only; author did not reply to request for more information
TABLE 3 Summary of studies excluded from the review
(provided by Unna’s boot) with the use of dress-ings alone. Two of these found a statisticallysignificantly higher proportion of healed ulcerswhen compression was used.12,13 A third small studyshowed a non-statistically significant increase inhealing with Unna’s boot.14
Three other studies, which compared differentforms of compression (four-layer, short stretchand two-layer bandages) with treatments usingnon-compressive bandages, showed that healingimproved with compression.15–17
The results of these six trials were not pooled,as very different comparisons were presented.However, all the trials found greater healing withcompression, although this difference was signifi-cant in only four of the six trials. Overall, there isreasonable evidence that venous ulcers heal morerapidly with compression than without.
What is the optimum level ofcompression?As none of the studies measured the amount ofpressure applied by the bandages or stockingsin use, the dose–response relationship betweencompression and ulcer healing is unknown and
there is no basis for recommending a particularlevel of pressure.
Clinical effectiveness ofcompression bandage and stockingsystems
Elastic compression versus inelasticcompressionThree RCTs compared elastic high-compressionthree-layer bandaging with multilayered low com-pression (Figure 3).18–20 The results of these studieswere pooled (c2 (test for heterogeneity) = 2.11;degrees of freedom (df) = 2) showing an overallstatistically significant relative benefit increase forhealing for the high-compression bandaging of54% (95% CI, 19 to 99).
Multilayer high compression versussingle-layer compressionFour RCTs were identified (Figure 4). Two RCTsshowed four-layer bandaging to increase thepercentage of ulcers healed at 24 and 12 weeks,compared with single-layer compression bandaging(Granuflex Adhesive Compression Bandage21 and
Health Technology Assessment 2001; Vol. 5: No. 9
93
Study Description
Trials that potentially fulfil the inclusion criteria
Olofsson and co-workers41 A comparison of two regimens for treating venous leg ulcers:
1. in a specialist clinic with one bandage2. in the usual setting with the usual bandage
Awaiting further information from the authors to determine what ‘usualcare’ was
Moody42 A comparison of short stretch and elastomeric bandages in the treatmentof venous leg ulcers. There were insufficient data in the journal article toinclude the study in this review. The author has been contacted severaltimes for additional information, but this has not been forthcoming
Freak and McCollum (unpublished,Manchester)
An RCT of four-layer versus short stretch bandages which wasabandoned after approximately 48 patients had been enrolled. Furtherinformation about this trial is being sought from the investigators
Ongoing trials
Burnand, St Thomas’ Hospital, London Comparison of four-layer and multilayered elastomeric bandaging usingSetopress in treating venous leg ulcers. Recruitment has been completed,but no results have been reported to date
Cullum, University of York VenUS bandaging trial (an HTA commissioned trial, coordinated fromthe University of York). Comparison of four-layer and short stretchbandaging in the treatment of venous leg ulcers in the community (400patients, 12 months follow-up). Recruitment was started in 1999; resultswill be reported in early 2002
TABLE 4 Trials that potentially fulfil the inclusion criteria and ongoing trials
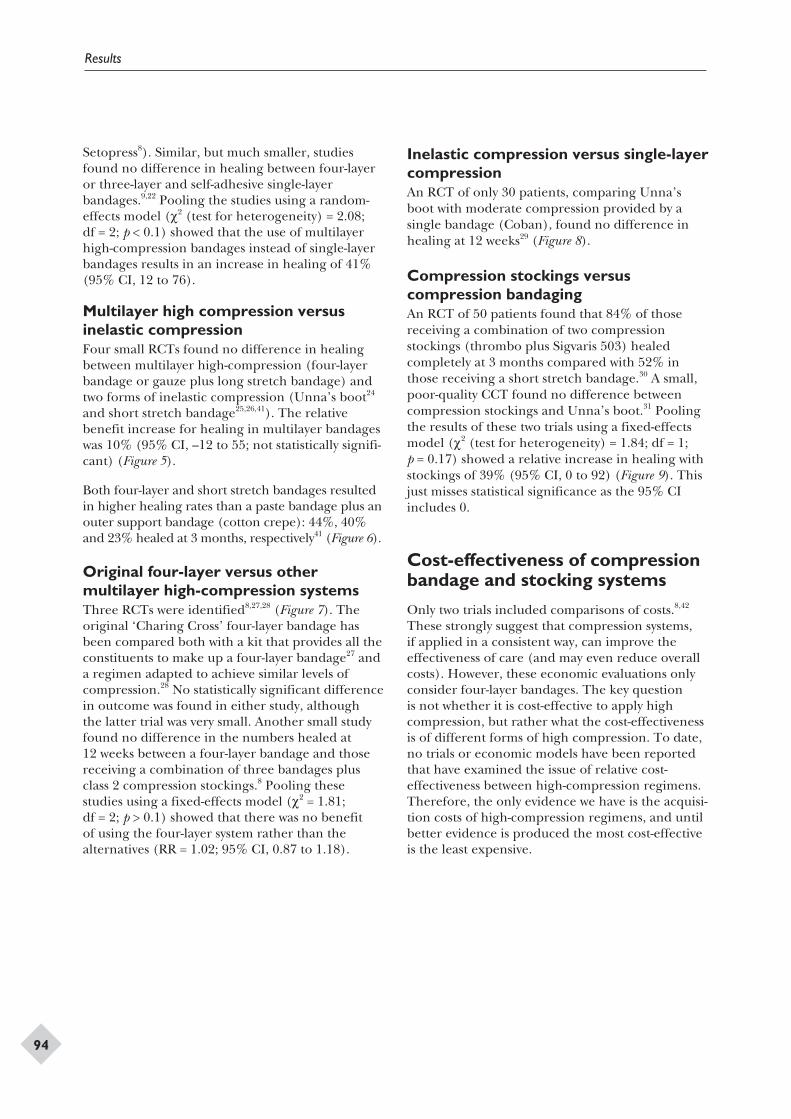
Setopress8). Similar, but much smaller, studiesfound no difference in healing between four-layeror three-layer and self-adhesive single-layerbandages.9,22 Pooling the studies using a random-effects model (c2 (test for heterogeneity) = 2.08;df = 2; p < 0.1) showed that the use of multilayerhigh-compression bandages instead of single-layerbandages results in an increase in healing of 41%(95% CI, 12 to 76).
Multilayer high compression versusinelastic compressionFour small RCTs found no difference in healingbetween multilayer high-compression (four-layerbandage or gauze plus long stretch bandage) andtwo forms of inelastic compression (Unna’s boot24
and short stretch bandage25,26,41). The relativebenefit increase for healing in multilayer bandageswas 10% (95% CI, –12 to 55; not statistically signifi-cant) (Figure 5).
Both four-layer and short stretch bandages resultedin higher healing rates than a paste bandage plus anouter support bandage (cotton crepe): 44%, 40%and 23% healed at 3 months, respectively41 (Figure 6).
Original four-layer versus othermultilayer high-compression systemsThree RCTs were identified8,27,28 (Figure 7). Theoriginal ‘Charing Cross’ four-layer bandage hasbeen compared both with a kit that provides all theconstituents to make up a four-layer bandage27 anda regimen adapted to achieve similar levels ofcompression.28 No statistically significant differencein outcome was found in either study, althoughthe latter trial was very small. Another small studyfound no difference in the numbers healed at12 weeks between a four-layer bandage and thosereceiving a combination of three bandages plusclass 2 compression stockings.8 Pooling thesestudies using a fixed-effects model (c2 = 1.81;df = 2; p > 0.1) showed that there was no benefitof using the four-layer system rather than thealternatives (RR = 1.02; 95% CI, 0.87 to 1.18).
Inelastic compression versus single-layercompressionAn RCT of only 30 patients, comparing Unna’sboot with moderate compression provided by asingle bandage (Coban), found no difference inhealing at 12 weeks29 (Figure 8).
Compression stockings versuscompression bandagingAn RCT of 50 patients found that 84% of thosereceiving a combination of two compressionstockings (thrombo plus Sigvaris 503) healedcompletely at 3 months compared with 52% inthose receiving a short stretch bandage.30 A small,poor-quality CCT found no difference betweencompression stockings and Unna’s boot.31 Poolingthe results of these two trials using a fixed-effectsmodel (c2 (test for heterogeneity) = 1.84; df = 1;p = 0.17) showed a relative increase in healing withstockings of 39% (95% CI, 0 to 92) (Figure 9). Thisjust misses statistical significance as the 95% CIincludes 0.
Cost-effectiveness of compressionbandage and stocking systems
Only two trials included comparisons of costs.8,42
These strongly suggest that compression systems,if applied in a consistent way, can improve theeffectiveness of care (and may even reduce overallcosts). However, these economic evaluations onlyconsider four-layer bandages. The key questionis not whether it is cost-effective to apply highcompression, but rather what the cost-effectivenessis of different forms of high compression. To date,no trials or economic models have been reportedthat have examined the issue of relative cost-effectiveness between high-compression regimens.Therefore, the only evidence we have is the acquisi-tion costs of high-compression regimens, and untilbetter evidence is produced the most cost-effectiveis the least expensive.
Results
94
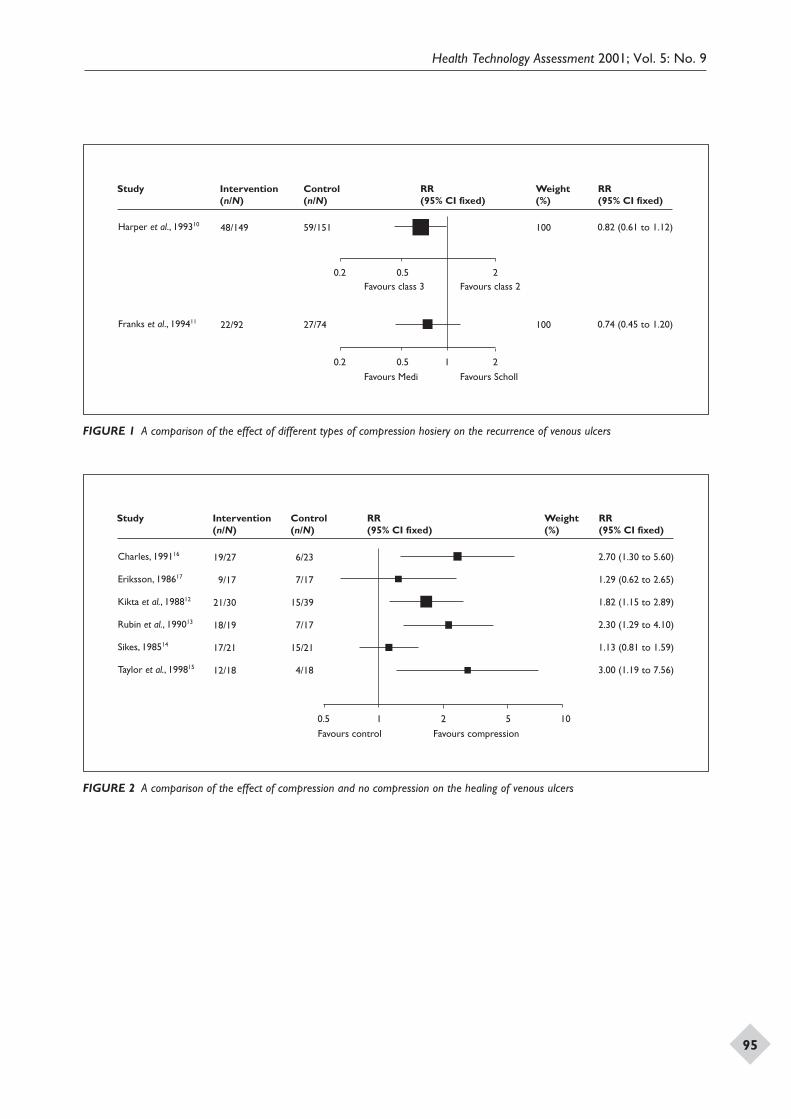
Health Technology Assessment 2001; Vol. 5: No. 9
95
Study Intervention (n/N)
Control (n/N)
RR (95% CI fixed)
RR (95% CI fixed)
Harper et al., 199310
Franks et al., 199411
48/149
22/92
59/151
27/74
Weight (%)
100
100
0.82 (0.61 to 1.12)
0.74 (0.45 to 1.20)
0.2 0.5 1 2
0.2 0.5 2
Favours Medi Favours Scholl
Favours class 3 Favours class 2
FIGURE 1 A comparison of the effect of different types of compression hosiery on the recurrence of venous ulcers
Study Intervention (n/N)
Control (n/N)
RR (95% CI fixed)
RR (95% CI fixed)
Charles, 199116
Eriksson, 198617
Kikta et al., 198812
Rubin et al., 199013
Sikes, 198514
Taylor et al., 199815
19/27
9/17
21/30
18/19
17/21
12/18
6/23
7/17
15/39
7/17
15/21
4/18
Weight (%)
2.70 (1.30 to 5.60)
1.29 (0.62 to 2.65)
1.82 (1.15 to 2.89)
2.30 (1.29 to 4.10)
1.13 (0.81 to 1.59)
3.00 (1.19 to 7.56)
0.5 1 52 10
Favours control Favours compression
FIGURE 2 A comparison of the effect of compression and no compression on the healing of venous ulcers
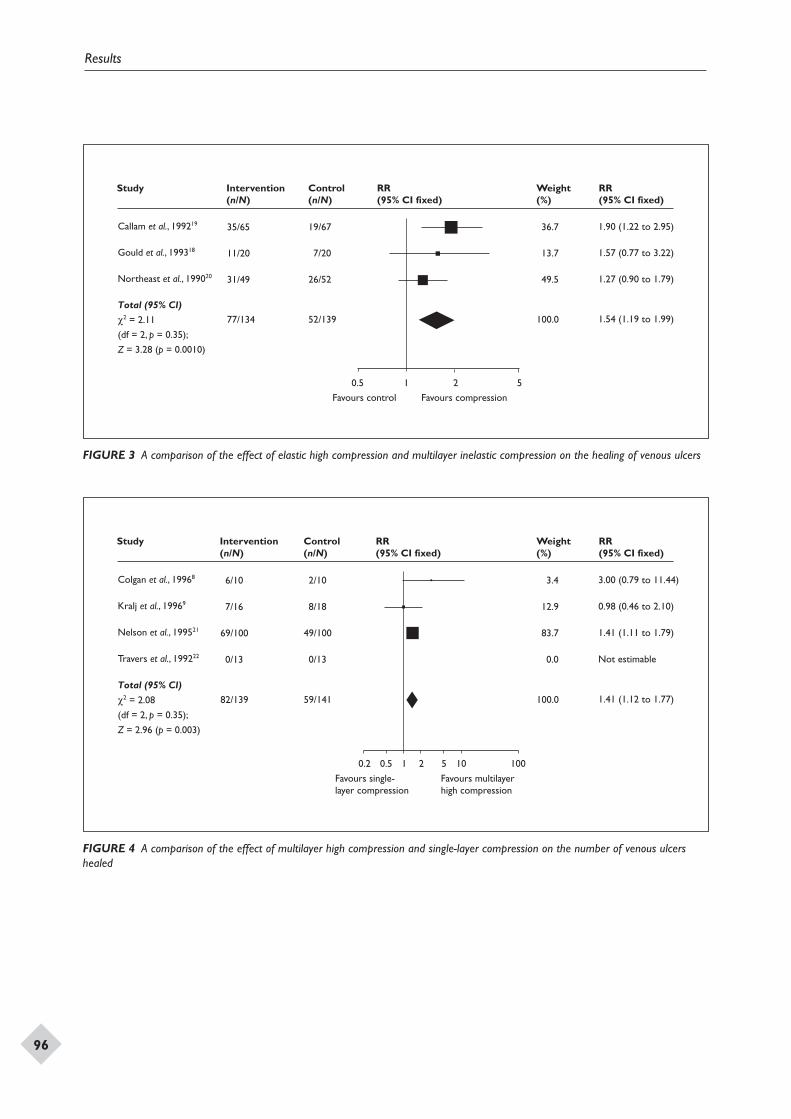
Results
96
Study Intervention (n/N)
Control (n/N)
RR (95% CI fixed)
RR (95% CI fixed)
Callam et al., 199219
Gould et al., 199318
Northeast et al., 199020
Total (95% CI)
c2 = 2.11
(df = 2, p = 0.35);
Z = 3.28 (p = 0.0010)
35/65
11/20
31/49
77/134
19/67
7/20
26/52
52/139
Weight (%)
36.7
13.7
49.5
100.0
1.90 (1.22 to 2.95)
1.57 (0.77 to 3.22)
1.27 (0.90 to 1.79)
1.54 (1.19 to 1.99)
0.5 1 2 5
Favours control Favours compression
FIGURE 3 A comparison of the effect of elastic high compression and multilayer inelastic compression on the healing of venous ulcers
Study Intervention (n/N)
Control (n/N)
RR (95% CI fixed)
RR (95% CI fixed)
Colgan et al., 19968
Kralj et al., 19969
Nelson et al., 199521
Travers et al., 199222
Total (95% CI)
c2 = 2.08
(df = 2, p = 0.35);
Z = 2.96 (p = 0.003)
6/10
7/16
69/100
0/13
82/139
2/10
8/18
49/100
0/13
59/141
Weight (%)
3.4
12.9
83.7
0.0
100.0
3.00 (0.79 to 11.44)
0.98 (0.46 to 2.10)
1.41 (1.11 to 1.79)
Not estimable
1.41 (1.12 to 1.77)
0.50.2 1 2 5 10 100
Favours single-layer compression
Favours multilayerhigh compression
FIGURE 4 A comparison of the effect of multilayer high compression and single-layer compression on the number of venous ulcershealed
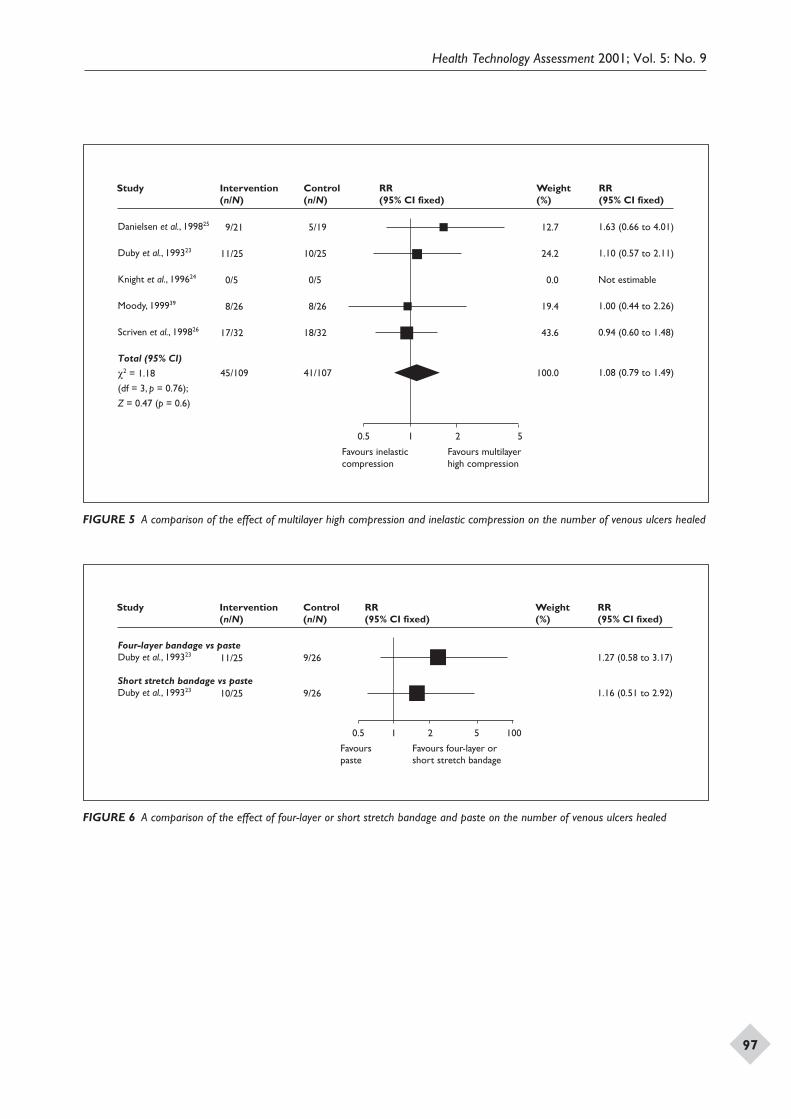
Health Technology Assessment 2001; Vol. 5: No. 9
97
Study Intervention (n/N)
Control (n/N)
RR (95% CI fixed)
RR (95% CI fixed)
Danielsen et al., 199825
Duby et al., 199323
Knight et al., 199624
Moody, 199939
Scriven et al., 199826
Total (95% CI)
c2 = 1.18
(df = 3, p = 0.76);
Z = 0.47 (p = 0.6)
9/21
11/25
0/5
8/26
17/32
45/109
5/19
10/25
0/5
8/26
18/32
41/107
Weight (%)
12.7
24.2
0.0
19.4
43.6
100.0
1.63 (0.66 to 4.01)
1.10 (0.57 to 2.11)
Not estimable
1.00 (0.44 to 2.26)
0.94 (0.60 to 1.48)
1.08 (0.79 to 1.49)
Favours inelasticcompression
Favours multilayerhigh compression
0.5 1 2 5
FIGURE 5 A comparison of the effect of multilayer high compression and inelastic compression on the number of venous ulcers healed
Study Intervention (n/N)
Control (n/N)
RR (95% CI fixed)
RR (95% CI fixed)
Four-layer bandage vs pasteDuby et al., 199323
Short stretch bandage vs pasteDuby et al., 199323
11/25
10/25
9/26
9/26
Weight (%)
1.27 (0.58 to 3.17)
1.16 (0.51 to 2.92)
Favours paste
Favours four-layer or short stretch bandage
0.5 1 2 5 100
FIGURE 6 A comparison of the effect of four-layer or short stretch bandage and paste on the number of venous ulcers healed
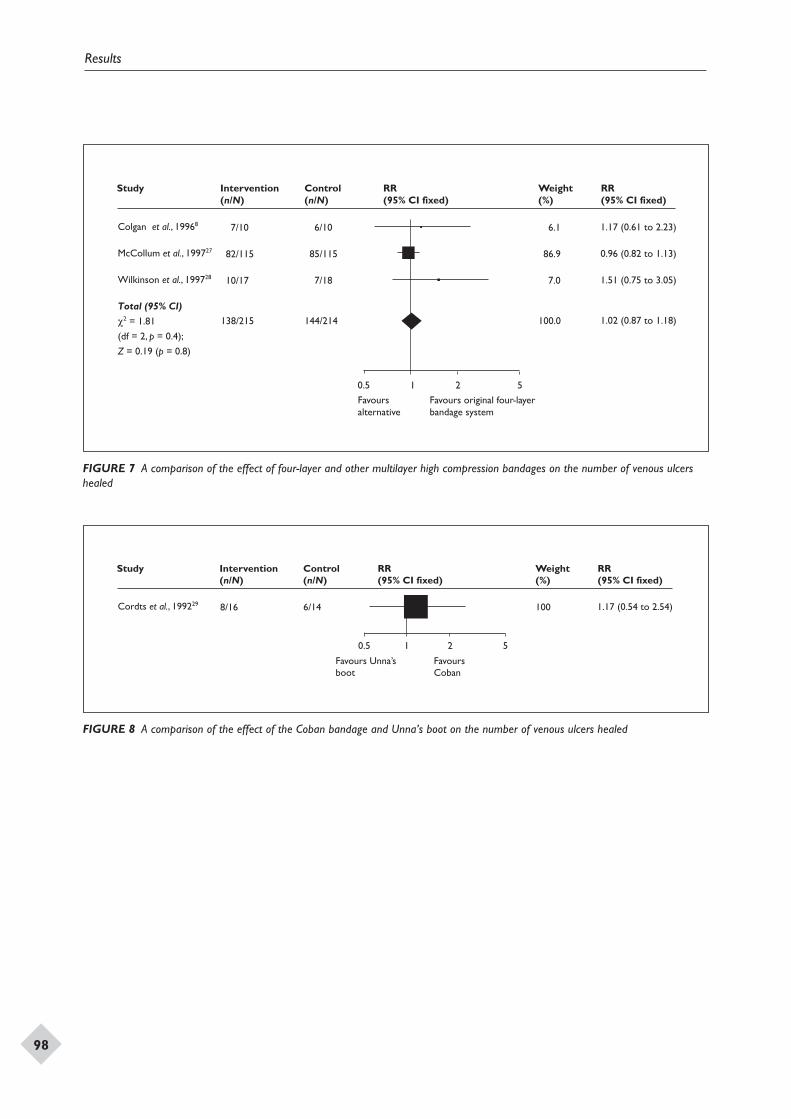
Results
98
Study Intervention (n/N)
Control (n/N)
RR (95% CI fixed)
RR (95% CI fixed)
Colgan et al., 19968
McCollum et al., 199727
Wilkinson et al., 199728
Total (95% CI)
c2 = 1.81
(df = 2, p = 0.4);
Z = 0.19 (p = 0.8)
7/10
82/115
10/17
138/215
6/10
85/115
7/18
144/214
Weight (%)
6.1
86.9
7.0
100.0
1.17 (0.61 to 2.23)
0.96 (0.82 to 1.13)
1.51 (0.75 to 3.05)
1.02 (0.87 to 1.18)
0.5 1 2 5
Favours alternative
Favours original four-layerbandage system
FIGURE 7 A comparison of the effect of four-layer and other multilayer high compression bandages on the number of venous ulcershealed
Study Intervention (n/N)
Control (n/N)
RR (95% CI fixed)
RR (95% CI fixed)
Cordts et al., 199229 8/16 6/14
Weight (%)
100 1.17 (0.54 to 2.54)
Favours Unna’sboot
Favours Coban
0.5 1 2 5
FIGURE 8 A comparison of the effect of the Coban bandage and Unna’s boot on the number of venous ulcers healed
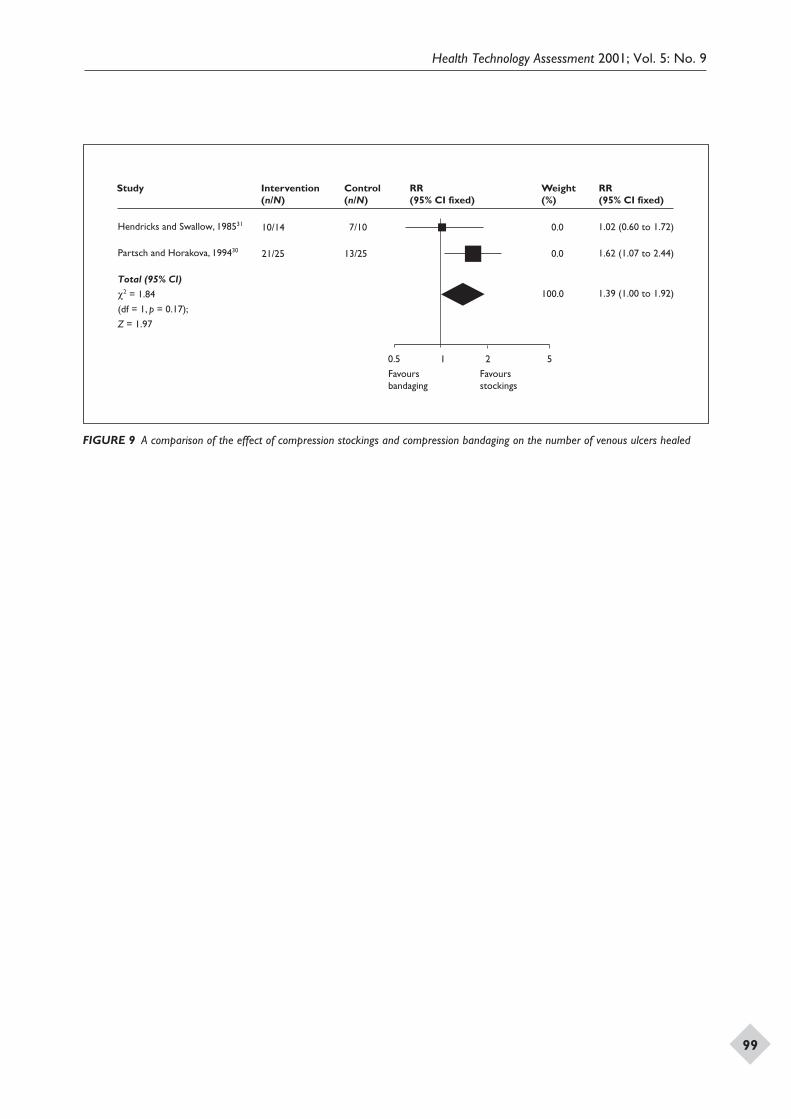
Health Technology Assessment 2001; Vol. 5: No. 9
99
Study Intervention (n/N)
Control (n/N)
RR (95% CI fixed)
RR (95% CI fixed)
Hendricks and Swallow, 198531
Partsch and Horakova, 199430
Total (95% CI)
c2 = 1.84
(df = 1, p = 0.17);
Z = 1.97
10/14
21/25
7/10
13/25
Weight (%)
0.0
0.0
100.0
1.02 (0.60 to 1.72)
1.62 (1.07 to 2.44)
1.39 (1.00 to 1.92)
0.5 1 2 5
Favours bandaging
Favours stockings
FIGURE 9 A comparison of the effect of compression stockings and compression bandaging on the number of venous ulcers healed
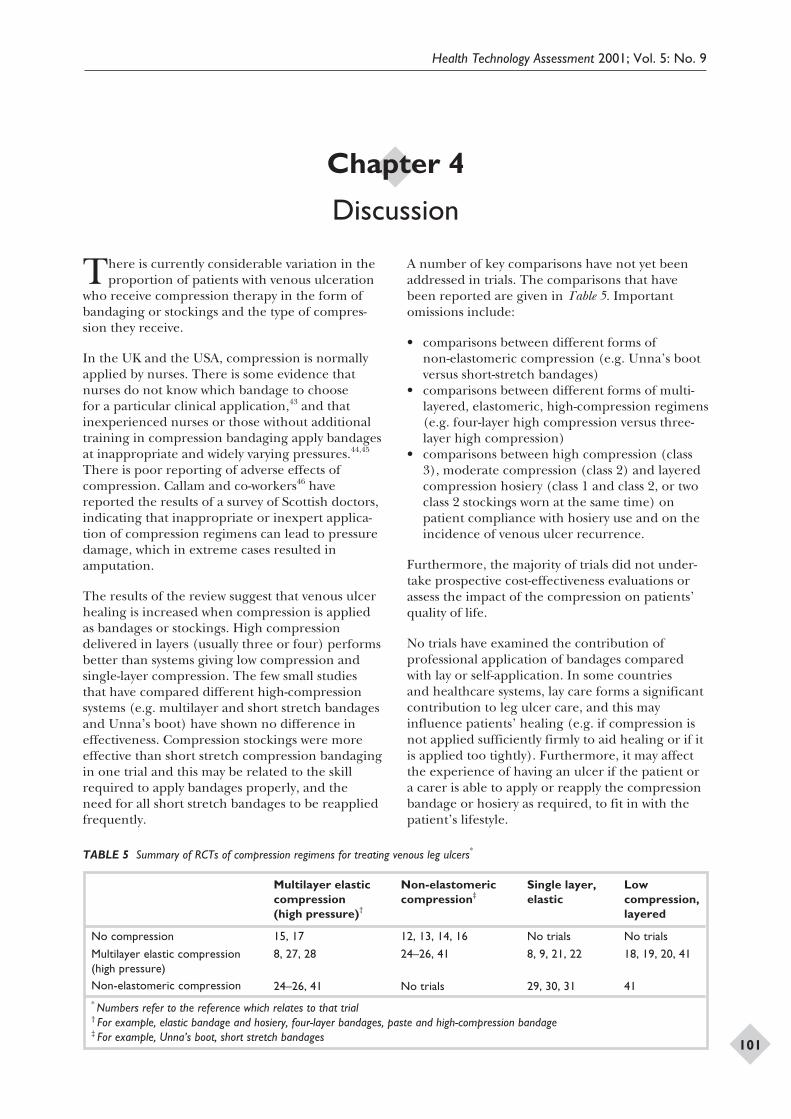
There is currently considerable variation in theproportion of patients with venous ulceration
who receive compression therapy in the form ofbandaging or stockings and the type of compres-sion they receive.
In the UK and the USA, compression is normallyapplied by nurses. There is some evidence thatnurses do not know which bandage to choosefor a particular clinical application,43 and thatinexperienced nurses or those without additionaltraining in compression bandaging apply bandagesat inappropriate and widely varying pressures.44,45
There is poor reporting of adverse effects ofcompression. Callam and co-workers46 havereported the results of a survey of Scottish doctors,indicating that inappropriate or inexpert applica-tion of compression regimens can lead to pressuredamage, which in extreme cases resulted inamputation.
The results of the review suggest that venous ulcerhealing is increased when compression is appliedas bandages or stockings. High compressiondelivered in layers (usually three or four) performsbetter than systems giving low compression andsingle-layer compression. The few small studiesthat have compared different high-compressionsystems (e.g. multilayer and short stretch bandagesand Unna’s boot) have shown no difference ineffectiveness. Compression stockings were moreeffective than short stretch compression bandagingin one trial and this may be related to the skillrequired to apply bandages properly, and theneed for all short stretch bandages to be reappliedfrequently.
A number of key comparisons have not yet beenaddressed in trials. The comparisons that havebeen reported are given in Table 5. Importantomissions include:
• comparisons between different forms ofnon-elastomeric compression (e.g. Unna’s bootversus short-stretch bandages)
• comparisons between different forms of multi-layered, elastomeric, high-compression regimens(e.g. four-layer high compression versus three-layer high compression)
• comparisons between high compression (class3), moderate compression (class 2) and layeredcompression hosiery (class 1 and class 2, or twoclass 2 stockings worn at the same time) onpatient compliance with hosiery use and on theincidence of venous ulcer recurrence.
Furthermore, the majority of trials did not under-take prospective cost-effectiveness evaluations orassess the impact of the compression on patients’quality of life.
No trials have examined the contribution ofprofessional application of bandages comparedwith lay or self-application. In some countriesand healthcare systems, lay care forms a significantcontribution to leg ulcer care, and this mayinfluence patients’ healing (e.g. if compression isnot applied sufficiently firmly to aid healing or if itis applied too tightly). Furthermore, it may affectthe experience of having an ulcer if the patient ora carer is able to apply or reapply the compressionbandage or hosiery as required, to fit in with thepatient’s lifestyle.
Health Technology Assessment 2001; Vol. 5: No. 9
101
Chapter 4
Discussion
Multilayer elasticcompression(high pressure)†
Non-elastomericcompression‡
Single layer,elastic
Lowcompression,layered
No compression 15, 17 12, 13, 14, 16 No trials No trials
Multilayer elastic compression(high pressure)
8, 27, 28 24–26, 41 8, 9, 21, 22 18, 19, 20, 41
Non-elastomeric compression 24–26, 41 No trials 29, 30, 31 41* Numbers refer to the reference which relates to that trial† For example, elastic bandage and hosiery, four-layer bandages, paste and high-compression bandage‡ For example, Unna’s boot, short stretch bandages
TABLE 5 Summary of RCTs of compression regimens for treating venous leg ulcers*

The majority of trials have used a hand-heldDoppler to measure the ABPI and only includedpatients with an ABPI of at least 0.7. In addition,studies usually excluded patients with concurrentdiseases that may compromise peripheral arterialcirculation, such as diabetes and rheumatoidarthritis. The application of compression to avenous leg ulcer in a patient with minimally
compromised arterial circulation, representedby an ABPI reading of around 0.8, appears to bebeneficial (this is a tentative conclusion because ofthe poor reporting of adverse events in trials andcohort studies). The balance between harm andbenefit, depending on the degree of arterial impair-ment, needs to be determined as it may be differentfor the various types of compression regimen.
Discussion
102

Implications for practice
High compression is more effective than moderatecompression in the prevention of ulcer recurrence.Compliance is lower with high-compression stock-ings, and patients should be prescribed the firmestclass stocking that they will wear.
Compression treatment increases the healing ofulcers compared with no compression. Highcompression is more effective than low compres-sion, but should only be used in the absence ofsignificant arterial disease. It is not clear whichof the high-compression systems (three-layer,four-layer, short stretch, high-compression hosiery,Unna’s boot) is the most cost-effective.
Implications for research
Much of the research concerning ulcer treatmentis of poor quality. In the trials reviewed, samplesizes were rarely sufficient to detect clinicallyimportant effects, and poor baseline comparabilityof the groups introduced bias. In addition, ourpoor understanding of the biological processesinvolved in healing may influence the ability of astudy to detect significant differences in healingrates. Several important messages can be identifiedfor future studies.
Recruitment numbers should be based on an apriori sample-size calculation. In most trials thesample size was too small to find a statisticallysignificant difference between treatment groups.In order to recruit sufficient patient numbers,multicentre trials should be considered. Theselarge trials have been undertaken in other areas ofhealthcare, and although the field of wound carepresents its own difficulties, there is no reason whysuch trials should not be performed. If these trialsare to be commissioned they will require a stronginfrastructure for providing support andpromoting collaboration.
Methodological recommendations
• A truly objective outcome measure should beused, or wound healing should be expressed
as both percentage and absolute change inarea.
• Unwanted effects of compression (e.g. pressuredamage, sensitivity to the components of thefabrics used, the impact of compression on thepatient’s ability to wear their usual footwear)should be fully reported.
• For each patient a single reference ulcer shouldbe selected. Multiple ulcers on a patient shouldnot be included in the analysis, since individualulcers are not independent unless specialisedstatistical analysis is performed to separate outthe effects of the intervention (i.e. matched-pairs analysis).
• Experimental groups should be comparable atbaseline. In small RCTs, randomisation alonewill not achieve comparability. In such situationspatients should be paired by baseline characteris-tics, and then the individuals of each pair shouldbe randomised to treatment. Such randomisationis particularly important if ulcers of mixedaetiology are to be assessed in the same trial.
• Head-to-head comparisons are required andshould use interventions that are recommendedfor similar patients and ulcers (e.g. ambulantpatients, moderately exuding ulcers).
• A complete and thorough description of concur-rent treatments, including primary and secondarydressings, should be given in trial reports.
• Assessment of outcomes should, where possible,be blind to treatment.
• Survival-rate analysis should be adopted for allstudies that assess ulcer healing.
• Studies to determine the biological mechanisminvolved in ulcer healing are needed. A betterunderstanding of the healing process will leadto the development of validated outcomemeasures.
• To prevent publication bias and ensure theinclusion of unpublished trials in systematicreviews, prospective registration of research
Health Technology Assessment 2001; Vol. 5: No. 9
103
Chapter 5
Conclusions
studies should become mandatory. Thoseinvolved in primary research should also maketheir data available to those undertaking system-atic reviews, particularly in those trials whereparticipants have given their written consent onthe understanding that their involvement willadd to medical knowledge.
• Contemporaneous economic evaluations shouldbe conducted in future trials.
Priority research questions
• At what level of ABPI is it safe to applycompression?
• What is the most reliable method of identifyingvenous leg ulcer patients with concurrentdiabetes or rheumatoid arthritis who wouldbenefit from compression?
• What are the most effective multilayer high-compression regimens with respect to cost-effectiveness and quality of life?
• What are the most effective non-elastomericcompression regimens with respect to cost-effectiveness and quality of life?
• What contribution can self-care or lay care maketowards improving the quality of life in patientswith venous leg ulcers?
• What are the most effective ways of deliveringcompression to prevent recurrence of venousulcers once healed (e.g. one high-compressionsock or stocking compared with two socks orstockings, each applying moderatecompression)?
• What is an acceptable rate of adverse events forthe widely used compression regimens?
Conclusions
104

This study was commissioned by the NHS R&DHTA programme. The authors are indebted to
the HTA referees for their perseverance in readingthis report and the quality of their comments. Theviews expressed in this report are those of theauthors, who are responsible for any errors.
We are extremely grateful to Professor TrevorSheldon of the University of York for his guidanceand good humour throughout this review. DrAlison Fletcher contributed to this review bysearching, data extraction and checking, andproject management. Sally Bell-Syer contributedto this review by searching, data extractionand checking and database management. RozThompson contributed to the review by managingthe citation database, expeditious documentacquisition and administrative support.
The assistance of the Information Staff, notablyJulie Glanville, of the NHS Centre for Reviews and
Dissemination, University of York, is gratefullyacknowledged.
We are extremely grateful to the members of theadvisory panel (appendix 2) who gave generouslyof their time and expertise. Andrew Herxheimer,Gillian Leng, Stephen Blair and Charles McCollumalso provided useful feedback. We would also liketo thank Georg Waernhjelm, who kindly translateda Swedish paper for us.
A less detailed version of this review haspreviously appeared in print.47 It was alsopublished as an Effective Health Care Bulletinand a Cochrane Review.48 The latter two publica-tions included reviews of assessment, intermittentpneumatic compression, organisation of careand prevention of ulcer recurrence. This reviewwill be maintained (updated in the light of users’comments and new trial data) in the CochraneLibrary.
Health Technology Assessment 2001; Vol. 5: No. 9
105
Acknowledgements

1. Callam MJ, Ruckley CV, Harper DR, Dale JJ.Chronic ulceration of the leg: extent of theproblem and provision of care. Br Med J 1985;290:1855–6.
2. Lees TA, Lambert D. Prevalence of lower limbulceration in an urban health district. Br J Surg1992;79(Pt 10):1032–4.
3. Baker SR, Stacey MC, Jopp-McKay AG, Hoskin SE,Thompson PJ. Epidemiology of chronic venousulcers. Br J Surg 1991;78:864–7.
4. Charles H. The impact of leg ulcers on patients’quality of life. Professional Nurse 1995;10:571–4.
5. Bosanquet N. Costs of venous ulcers: frommaintenance therapy to investment programmes.Phlebology 1992;(Suppl 1):44–6.
6. Thomas S. Compression bandages. In: Cullum N,Roe BH, editors. Leg ulcers: nursing management.Harrow: Scutari; 1995.
7. British Standards Institution. British Standard 7505:elastic properties of extensible bandages. MiltonKeynes: BSI, 1995.
8. Colgan MP, Teevan M, McBride C, O’Sullivan L,Moore D, Shanik G. Cost comparisons in themanagement of venous ulceration. In: Proceedingsof the 5th European Conference on Advances inWound Management. London: MacmillanMagazines; 1996. p. 103.
9. Kralj B, Kosicek M. A randomised comparativetrial of single-layer and multi-layer bandages inthe treatment of venous leg ulcers. In: Leaper DJ,Cherry GW, Dealey C, Lawrence JC, Turner TD,editors. Proceedings of the 6th EuropeanConference on Advances in Wound Management.London: Macmillan Magazines; 1996. p. 158–60.
10. Harper DR, Nelson EA, Gibson B, Brown D,Ruckley CV. A prospective, controlled, randomizedtrial of class 2 and class 3 elastic compression in theprevention of venous ulceration. In: Cherry GW,Gottrup F, Lawrence JC, Moffatt CJ, Turner TD,editors. Proceedings of the 5th EuropeanConference on Advances in Wound Management.London: Macmillan Magazines; 1996. p. 55.
11. Franks PJ, Oldroyd MI, Dickson D, Sharp EJ,Moffatt CJ. Risk factors for leg ulcer recurrence:a randomized trial of two types of compressionstocking. Age Ageing 1995;24(Pt 6):490–4.
12. Kikta MJ, Schuler JJ, Meyer JP, et al. A prospective,randomized trial of Unna’s boots versus hydroactivedressing in the treatment of venous stasis ulcers.J Vasc Surg 1988;7:478–83.
13. Rubin JR, Alexander J, Plecha EJ, Marman C.Unna’s boot vs polyurethane foam dressings forthe treatment of venous ulceration. A randomizedprospective study. Arch Surg 1990;125(Pt 4):489–90.
14. Sikes E. Evaluation of a transparent dressing inthe treatment of stasis ulcers of the lower limb.J Enterostomal Ther 1985;12(Pt 4):116–20.
15. Taylor AD, Taylor RJ, Marcuson RW. Prospectivecomparison of healing rates and therapy costsfor conventional and four layer high compressionbandaging treatments of venous leg ulcers.Phlebology 1998;13:20–4.
16. Charles H. Compression healing of ulcers. J DistrictNurs 1991;4:6–7.
17. Eriksson G. Comparison of two occlusive bandagesin the treatment of venous leg ulcers. Br J Dermatol1986;114:227–30.
18. Gould DJ, Campbell S, Harding EF. Short stretchvs. long stretch bandages in the management ofchronic venous leg ulcers. Phlebology 1993;8:43.
19. Callam MJ, Harper DR, Dale JJ, et al. Lothian andForth Valley leg ulcer healing trial. Part 1: elasticversus non-elastic bandaging in the treatment ofchronic leg ulceration. Phlebology 1992;7(Pt 4):136–41.
20. Northeast ADR, Layer GT, Wilson NM, Browse NL,Burnand KG. Increased compression expeditesvenous ulcer healing. R Soc Med Venous Forum 1990.
21. Nelson EA, Harper DR, Ruckley CV, Prescott RJ,Gibson B, Dale JJ. A randomised trial of singlelayer and multi-layer bandages in the treatment ofchronic venous ulceration. Phlebology 1995;(Suppl 1):915–16.
22. Travers JP, Dalziel KL, Makin GS. Assessment ofa new one-layer adhesive bandaging method inmaintaining prolonged limb compression andeffects on venous ulcer healing. Phlebology 1992;7(Pt 2):59–63.
23. Duby T, Cherry G, Hoffman D, Cameron J, Dobloff-Brown D, Ryan T. A randomized trial in thetreatment of venous leg ulcers comparing shortstretch bandages, four layer bandage system, and a
Health Technology Assessment 2001; Vol. 5: No. 9
107
References
long stretch-paste bandage system. WoundsCompendium Clin Res Pract 1993;5(Pt 6):276–9.
24. Knight CA, McCulloch J. A comparative studybetween two compression systems in thetreatment of venous insufficiency in leg ulcers.In: Proceedings of the Symposium on AdvancedWound Care and Medical Research Forum onWound Repair; 1996; Wayne, PN. p. 117.
25. Danielsen L, Madsen SM, Henriksen L. Venousleg ulcer healing: a randomized prospective studyof long-stretch versus short-stretch compressionbandages. Phlebology 1998;13:59–63.
26. Scriven JM, Taylor LE, Wood AJ, Bell PR, NaylorAR, London NJ. A prospective randomised trialof four-layer versus short stretch compressionbandages for the treatment of venous leg ulcers.Ann R Coll Surg Engl 1998;80(Pt 3):215–20.
27. McCollum CN, Ellison DA, Groarke L, et al.Randomised trial comparing Profore and theoriginal four layer bandage. In: Proceedings of theConference of the European Wound ManagementAssociation. London: Macmillan; 1997. p. 8.
28. Wilkinson E, Buttfield S, Cooper S, Young E. Trialof two bandaging systems for chronic venous legulcers. J Wound Care 1997;6(Pt 7):339–40.
29. Cordts PR, Hanrahan LM, Rodriguez AA, WoodsonJ, LaMorte WW, Menzoian JO. A prospective,randomized trial of Unna’s boot versus DuodermCGF hydroactive dressing plus compression in themanagement of venous leg ulcers. J Vasc Surg1992;15(Pt 3):480–6.
30. Partsch H, Horakova MA. Compression stockingsfor the treatment of venous leg ulcers. Wien MedWochenschr 1994;144(Pt 10–11):242–9.
31. Hendricks WM, Swallow RT. Management of stasisleg ulcers with Unna’s boots versus elastic supportstockings. J Am Acad Dermatol 1985;12(Pt 1):90–8.
32. Cameron J, Hofman D, Poore S, Duby T, Cherry G,Ryan T. A comparative study of two bandagesystems. In: Proceedings of the 3rd EuropeanConference on Advances in Wound Management.London: Macmillan; 1994. p. 168.
33. Cherry G. Clinical comparison of a new compres-sion bandage. Nursing Stand 1990;8(Suppl):8–11.
34. Eriksson G. Comparison of two occlusive bandagesin the treatment of venous leg ulcers. Br J Dermatol1986;114:227–30.
35. Sabolinski M, Borchard G, Mulder G. Cost benefitanalysis of living skin equivalent versus graduated,multi-layered compression therapy for thetreatment of venous skin ulcers. Diabetes 1995;44(Suppl 1):107.
36. Sironi G, Losa S, DiLuca G, Pezzoni F. Treatmentof venous leg ulcers with Intrasite gel, OpsiteFlexigrid, Allevyn hydrocellular dressing andFlexobande (elastic compression bandage) invascular surgery. A protocol for clinical evaluations.In: Proceedings of the 3rd European Conferenceon Advances in Wound Management. London:Macmillan Magazines; 1994. p. 164.
37. Walker P, Faria DT. Evaluation of a three layerbandage system versus a four layer bandage systemin venous leg ulcers. In: Symposium on AdvancedWound Care and Medical Research Forum onWound Repair. Wayne: Health ManagementPublications; 1996. p. 121.
38. Olofsson B, Ljunghall K, Nordin-Bjorklund K,Sorensen S, Leppert J. [Two therapeutic models invenous leg ulcers are compared: better results withoptimized compression.] Lakartidningen 1996;93(Pt51–52):4752–4.
39. Moody M. Comparison of Rosidal K and Surepressin the treatment of venous leg ulcers. Br J Nurs1999;6:345–55.
40. Deeks J. Odds ratios should be used only in casecontrol studies and logistic regression analyses.BrMed J 1998;317:1155–6.
41. Duby T, Hofman D, Cameron J, Dobloff Brown D,Cherry G, Ryan T. A randomized trial in thetreatment of venous leg ulcers comparing shortstretch bandages, four layer bandage system, anda long stretch-paste bandage system. WoundsCompendium Clin Res Pract 1993;5(Pt 6):276–9.
42. Taylor A. A prospective study to compare healingrates and associated treatment costs for currentmanagement of venous leg ulcers in the communityand a four-layer compression bandage regime. In:Proceedings of the 4th European Conference onAdvances in Wound Management. London:Macmillan Magazines; 1995. p. 199–200.
43. Magazinovic N, Phillips-Turner J, Wilson GV.Assessing nurses’ knowledge of bandages andbandaging. J Wound Care 1993;2(Pt 2):97–101.
44. Logan RA, Thomas S, Harding EF. A comparisonof sub-bandage pressures produced by experiencedand inexperienced bandagers. J Wound Care 1992;1(Pt 2):23–6.
45. Stockport JC, Groarke L, Ellison DA, McCollum C.Single-layer and multilayer bandaging in thetreatment of venous leg ulcers. J Wound Care 1997;6(Pt 10):485–8.
46. Callam MJ, Harper DR, Dale JJ, Ruckley CV.Arterial disease in chronic leg ulceration: anunderestimated hazard? Lothian and Forth Valleyleg ulcer study. Br Med J 1987;294:929–31.
References
108

47. Fletcher A, Cullum N, Sheldon TA. A systematicreview of compression treatment for venous legulcers. Br Med J 1997;315:576–80.
48. Cullum N, Nelson EA, Fletcher A, Sheldon TA.Compression therapy for venous leg ulcers. Oxford.Update Software. Cochrane Library. 2000(1).
Health Technology Assessment 2001; Vol. 5: No. 9
109

MEDLINE
MEDLINE was searched for RCTs for the period1966 to December 1999 using a mixture of freetext terms and the following MeSH headings:
WOUND INFECTIONPILONIDAL CYSTWOUNDS AND INJURIESWOUND HEALINGLEG ULCERVARICOSE ULCERSKIN ULCERDECUBITUS
The MEDLINE search strategy used was as follows:
1. decubitus ulcer/ or foot ulcer/2. leg ulcer/ or varicose ulcer/3. pilonidal cyst/4. skin ulcer/5. diabetic foot/6. ((plantar or diabetic or heel or venous or stasis
or arterial) adj ulcer$).tw.7. ((decubitus or foot or diabetic or ischaemic or
pressure) adj ulcer$).tw.8. ((pressure or bed) adj sore$).tw.9. ((pilonidal adj cyst) or (pilonidal adj sinus) or
bedsore$).tw.10. ((diabetic adj foot) or (cavity adj wound)).tw.11. ((varicose or leg or skin) adj ulcer$).tw.12. (decubitus or (chronic adj wound$)).tw.13. ((sinus adj wound$) or (cavity adj
wound$)).tw.14. or/1–1315. debridement/ or biological dressings/ or
bandages/16. occlusive dressings/ or clothing/ or wound
healing/17. antibiotics/ or growth substances/ or platelet-
derived growth factor/18. fibroblast growth factor/ or electrical
stimulation therapy.ti,ab,sh.19. lasers/ or nutrition/ or surgery/ or surgery,
plastic/20. surgical flaps/ or skin transplantations/ or
homeopathy/ or homeopathic/21. acupuncture therapy/ or acupuncture/ or
alternative medicine/
22. alternative medicine/ or massage/ or iloprost/or alginates/
23. zinc/ or zinc oxide/ or ointments/ or anti-infective agents/
24. dermatologic agents/ or colloids/ or cushions/or wheelchairs/
25. beds/ or wound dressings/26. (debridement or dressing$ or compress$ or
cream$ or (growth adj factor$)).tw.27. (pressure-relie$ or (recombinant adj protein$)
or bandag$ or stocking$).tw.28. (antibiotic$ or (electric adj therapy) or laser$
or nutrition$ or surg$).tw.29. (homeopath$ or acupuncture or massage or
reflexology or ultrasound).tw.30. (iloprost or alginate$ or zinc or paste$ or
ointment$ or hydrocolloid$).tw.31. ((compression adj therapy) or (compression
adj bandag$) or wrap$).tw.32. (bed$ or mattress$ or wheelchair$ or (wheel
adj chair) or cushion$).tw.33. ((wound adj dressing$) or vitamin$ or bind$ or
gauze$ or heals or healing).tw.34. (diet or lotion$ or infect$ or reduc$ or (wound
adj healing)).tw.35. (treat$ or prevent$ or epidemiol$ or aetiol$
or etiol$ or therap$ or prevalence orincidence).tw.
36. or/15–3537. 14 and 3638. random allocation/ or randomized controlled
trials/39. controlled clinical trials/ or clinical trials phase
I/ or clinical trials phase II/40. clinical trials phase III/ or clinical trials phase
IV/ or clinical trials overviews/41. single-blind method/ or double-blind method/42. publication bias/ or review/ or review,
academic/43. review tutorial/ or meta-analysis/ or systematic
review/44. ((random$ adj controlled adj trial$) or
(prospective adj random$)).tw.45. ((random adj allocation) or random$ or
(clinical adj trial$) or control$).tw.46. ((standard adj treatment) or compar$ or
single-blind$ or double-blind$).tw.47. (blind$ or placebo$ or systematic$ or
(systematic adj review)).tw.
Health Technology Assessment 2001; Vol. 5: No. 9
111
Appendix 1
Databases searched and search strategies
48. (randomized controlled trial or clinicaltrial).pt. or comparative study.sh.
49. or/38–4850. 37 and 4951. limit 50 to human52. burns/ or wounds, gunshot/ or corneal ulcer/
or exp dentistry/53. peptic ulcer/ or duodenal ulcer/ or stomach
ulcer/54. ((peptic adj ulcer) or (duodenal adj ulcer) or
traum$).tw.55. ((aortocaval adj fistula) or (arteriovenous adj
fistula)).tw.56. (bite adj wound$).tw.57. or/52–5658. 51 not 57
CINAHL
The CINAHL search strategy used was as follows:
1. pressure ulcer/ or foot ulcer/ or leg ulcer/ orskin ulcer/
2. diabetic foot/ or diabetic neuropathies/3. diabetic angiopathies/ or diabetes mellitus/co4. pilonidal cyst/ or surgical wound infection/5. ((plantar or diabetic or heel or venous or stasis
or arterial) adj ulcer$).tw.6. ((decubitus or foot or diabetic or ischaemic or
pressure) adj ulcer$).tw.7. ((pressure or bed) adj sore$).tw.8. ((pilonidal adj cyst) or (pilonidal adj sinus) or
bedsore).tw.9. ((diabetic adj foot) or (cavity adj wound)).tw.10. ((varicose or leg or skin) adj ulcer$).tw.11. (decubitus or (chronic adj wound$)).tw.12. ((sinus adj wound$) or (cavity adj
wound$)).tw.13. or/1–1214. debridement/ or biological dressings/ or
occlusive dressings/15. (bandages.ti,sh,ab,it. and ‘Bandages and
Dressings’/) or16. compression garments/ or antibiotics/17. electric stimulation/ or Laser Surgery/ or
lasers/th lasers/ or Nutrition Care (SabaHHCC)/ or diet therapy/ or NutritionTherapy (Iowa NIC)/
18. surgery, reconstructive/ or surgery, plastic/ orsurgical flaps/
19. surgical stapling/ or skin transplantation/ oralternative therapies/
20. acupuncture/ or massage/ or zinc/ orointments/
21. antiinfective agents, local/ or antibiotics/ ordermatologic agents/
22. dermatology nursing/ or colloids/ or beds andmattresses/
23. flotation beds/ or wheelchairs/ orpositioning:wheelchair/ orpositioning:therapy/
24. patient positioning/ or positioning/ or woundcare/ or wound healing/
25. (debridement or dressing$ or compress$ orcream$).tw.
26. ((growth adj factor$) or pressure relie$ or(recombinant adj protein$) or bandag$).tw.
27. (stocking$ or antibiotic$ or (electric adjtherapy) or laser$ or nutrition$ or surg$).tw.
28. (iloprost or alginate$ or zinc or paste$ orointment$ or hydrocolloid$).tw.
29. ((compression adj therapy) or (compressionadj bandag$) or wrap$).tw.
30. (bed$ or mattress$ or wheelchair$ or (wheeladj chair) or cushion$).tw.
31. ((wound adj dressing$) or vitamin$ or bind$ orgauze$ or heals or healing).tw.
32. (diet or lotion$ or infect$ or reduc$ or etiol$or (wound adj healing)).tw.
33. (treat$ or prevent$ or epidemiol$ or aetiol$ ortherap$ or prevalence or incidence).tw.
34. ‘Bandages and Dressings’/ or skintransplantation/ or homeopathy/ orointments/ or ‘beds and mattresses’/
35. or/14–3436. 13 and 3537. clinical trials/ or single-blind studies/ or
double-blind studies/38. control group/ or placebos/ or meta analysis/39. ((random$ adj clinical adj trial$) or
(prospective adj random$)).tw.40. ((random adj allocation) or random$ or
controlled clinical trial$ or control).tw.41. (comparison group$ or (standard adj
treatment) or compar$).tw.42. (single-blind$ or (single adj blind) or double-
blind or (double adj blind)).tw.43. (blind$ or placebo$ or systematic or
(systematic adj review)).tw.44. (meta analysis or meta-analysis).tw. or (trials or
trial or prospective).tw.45. (clinical trials).sh. or (comparative studies).sh.46. or/37–4547. 36 and 4648. burns/ or wounds, gunshot/ or corneal ulcer/
or exp dentistry/49. peptic ulcer/ or duodenal ulcer/50. ((peptic adj ulcer) or (duodenal adj ulcer) or
trauma).tw.51. (burn$ or (gunshot adj wound$) or (corneal
adj ulcer) or dentist$ or (bite adj wound)).tw.52. or/48–5153. 47 not 52
Appendix 1
112

Other databases
• ISI Science Citation Index (on BIDS)• BIOSIS (on SilverPlatter)• British Diabetic Association Database• CISCOM (database of the Research Council for
Complementary Medicine)• Cochrane Controlled Trials Register (Central)• Cochrane Database of Systematic Reviews
(CDSR)• Cochrane Wounds Group register of trials• Current Research in Britain (CRIB)• Database of Abstract of Reviews of Effectiveness
(DARE)
• Dissertation Abstracts• DHSS Data (on Knight-Ridder Datastar)• EconLit• EMBASE (on Knight-Ridder Datastar)• Index to Scientific and Technical Proceedings
(searched on BIDS)• National Research Register (to locate ongoing
research in NHS)• NHS Economic Evaluation Database
(NHS Centre for Reviews and Dissemination)• Royal College of Nursing Database
(CD-ROM)• System for Information on Grey Literature in
Europe (SIGLE) (on Blaise Line)
Health Technology Assessment 2001; Vol. 5: No. 9
113


Dr Mary Bliss Department of Medicine for the Elderly, Homerton Hospital, London
Professor Nick Bosanquet Department of General Medicine, Imperial College School of Medicine,London
Professor Andrew Boulton Department of Medicine, Manchester Royal Infirmary, Manchester
Dr Richard Bull Department of Dermatology, Homerton Hospital, London
Mr Michael Callam Department of Vascular Surgery, Bedford Hospital, Bedford
Mrs Carol Dealey Moseley Hall Hospital, Birmingham
Professor Peter Friedman Department of Dermatology, Royal Liverpool University Hospital, Liverpool
Mr Brian Gilchrist Department of Nursing Studies, King’s College, London
Dr Keith Harding Wound Healing Research Unit, University of Wales College of Medicine,University Department of Surgery, Cardiff
Mrs Deborah Hofman Department of Dermatology, Churchill Hospital, Oxford
Mrs Vanessa Jones Wound Healing Research Unit, University of Wales College of Medicine,University Department of Surgery, Cardiff
Dr Christina Lindholm Department of Nursing Research, Uppsala University Hospital, Uppsala
Dr Raj Mani Department of Medical Physics, Southampton University Hospital,Southampton
Ms Andrea Nelson Department of Nursing, University of Liverpool, Liverpool
Dr Steve Thomas Surgical Materials Testing Laboratory, Bridgend General Hospital, MidGlamorgan
Dr Ewan Wilkinson Buckinghamshire Health Authority, Aylesbury
Health Technology Assessment 2001; Vol. 5: No. 9
115
Appendix 2
Advisory panel

Appendix 3
Summary of included studies
Health Technology Assessment 2001; Vol. 5: No. 9
117
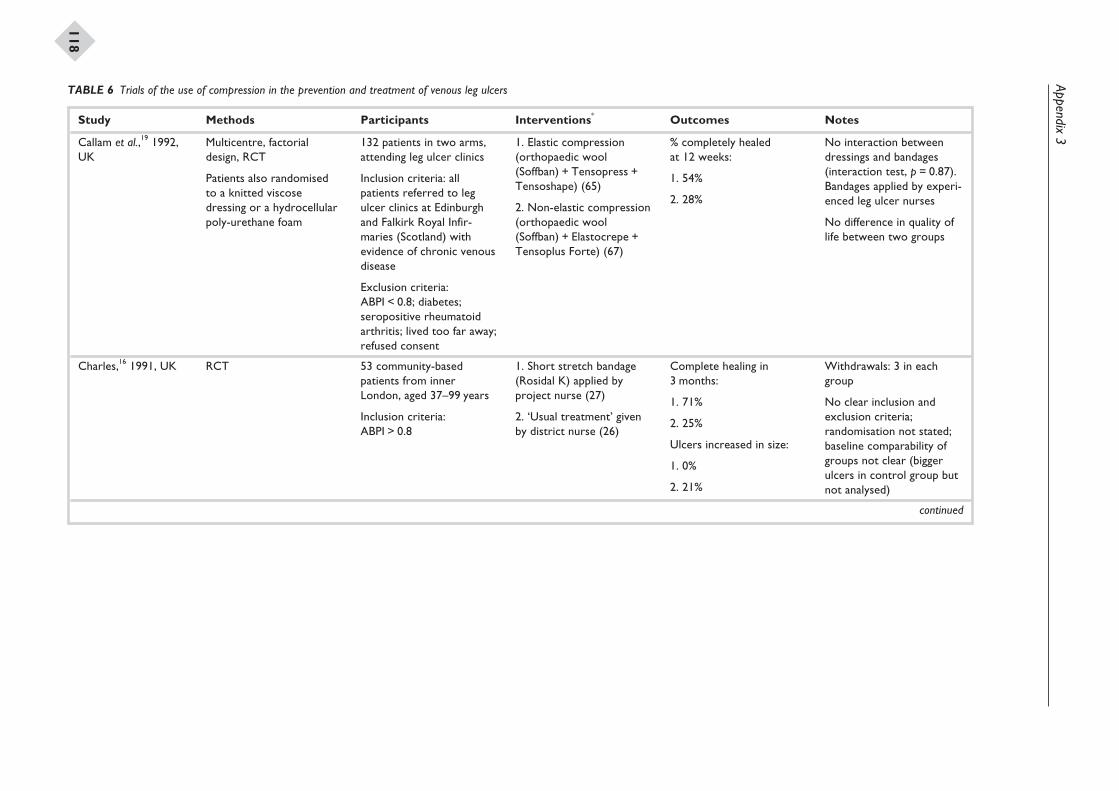
Appendix3
118
Study Methods Participants Interventions* Outcomes Notes
Callam et al.,19 1992,UK
Multicentre, factorialdesign, RCT
Patients also randomisedto a knitted viscosedressing or a hydrocellularpoly-urethane foam
132 patients in two arms,attending leg ulcer clinics
Inclusion criteria: allpatients referred to legulcer clinics at Edinburghand Falkirk Royal Infir-maries (Scotland) withevidence of chronic venousdisease
Exclusion criteria:ABPI < 0.8; diabetes;seropositive rheumatoidarthritis; lived too far away;refused consent
1. Elastic compression(orthopaedic wool(Soffban) + Tensopress +Tensoshape) (65)
2. Non-elastic compression(orthopaedic wool(Soffban) + Elastocrepe +Tensoplus Forte) (67)
% completely healedat 12 weeks:
1. 54%
2. 28%
No interaction betweendressings and bandages(interaction test, p = 0.87).Bandages applied by experi-enced leg ulcer nurses
No difference in quality oflife between two groups
Charles,16 1991, UK RCT 53 community-basedpatients from innerLondon, aged 37–99 years
Inclusion criteria:ABPI > 0.8
1. Short stretch bandage(Rosidal K) applied byproject nurse (27)
2. ‘Usual treatment’ givenby district nurse (26)
Complete healing in3 months:
1. 71%
2. 25%
Ulcers increased in size:
1. 0%
2. 21%
Withdrawals: 3 in eachgroup
No clear inclusion andexclusion criteria;randomisation not stated;baseline comparability ofgroups not clear (biggerulcers in control group butnot analysed)
continued
TABLE 6 Trials of the use of compression in the prevention and treatment of venous leg ulcers
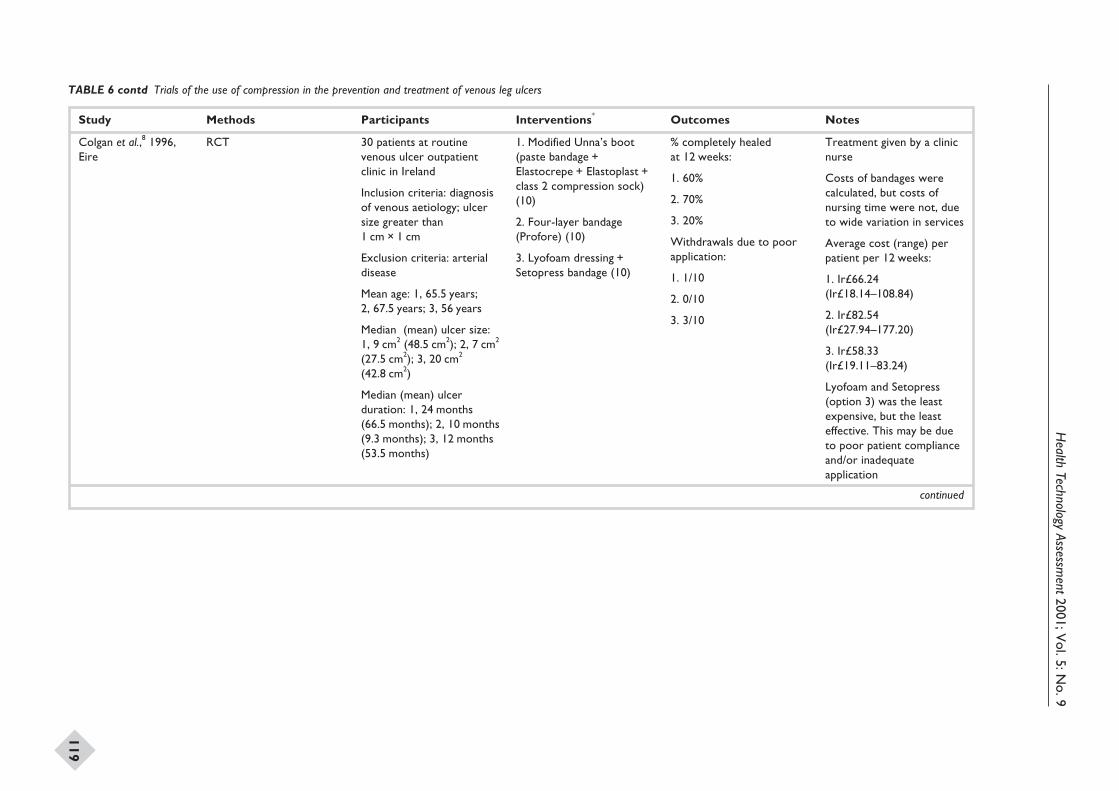
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
119
Study Methods Participants Interventions* Outcomes Notes
Colgan et al.,8 1996,Eire
RCT 30 patients at routinevenous ulcer outpatientclinic in Ireland
Inclusion criteria: diagnosisof venous aetiology; ulcersize greater than1 cm × 1 cm
Exclusion criteria: arterialdisease
Mean age: 1, 65.5 years;2, 67.5 years; 3, 56 years
Median (mean) ulcer size:1, 9 cm2 (48.5 cm2); 2, 7 cm2
(27.5 cm2); 3, 20 cm2
(42.8 cm2)
Median (mean) ulcerduration: 1, 24 months(66.5 months); 2, 10 months(9.3 months); 3, 12 months(53.5 months)
1. Modified Unna’s boot(paste bandage +Elastocrepe + Elastoplast +class 2 compression sock)(10)
2. Four-layer bandage(Profore) (10)
3. Lyofoam dressing +Setopress bandage (10)
% completely healedat 12 weeks:
1. 60%
2. 70%
3. 20%
Withdrawals due to poorapplication:
1. 1/10
2. 0/10
3. 3/10
Treatment given by a clinicnurse
Costs of bandages werecalculated, but costs ofnursing time were not, dueto wide variation in services
Average cost (range) perpatient per 12 weeks:
1. Ir£66.24(Ir£18.14–108.84)
2. Ir£82.54(Ir£27.94–177.20)
3. Ir£58.33(Ir£19.11–83.24)
Lyofoam and Setopress(option 3) was the leastexpensive, but the leasteffective. This may be dueto poor patient complianceand/or inadequateapplication
continued
TABLE 6 contd Trials of the use of compression in the prevention and treatment of venous leg ulcers
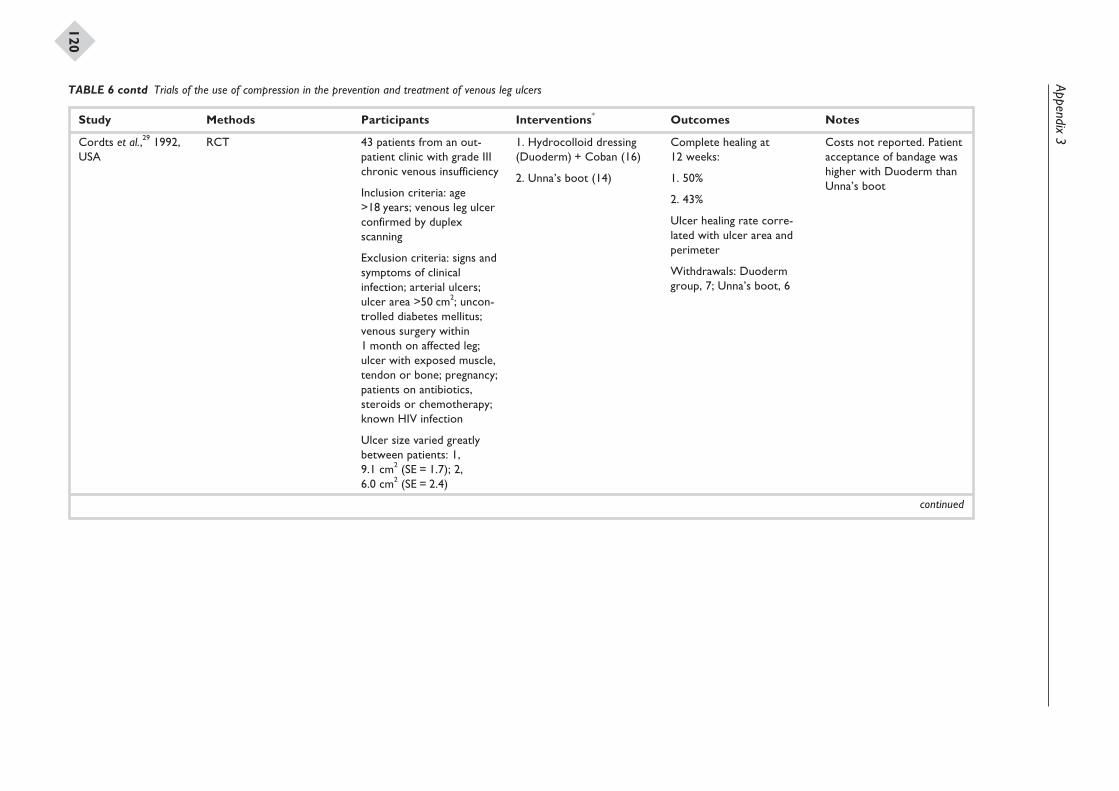
Appendix3
120
Study Methods Participants Interventions* Outcomes Notes
Cordts et al.,29 1992,USA
RCT 43 patients from an out-patient clinic with grade IIIchronic venous insufficiency
Inclusion criteria: age>18 years; venous leg ulcerconfirmed by duplexscanning
Exclusion criteria: signs andsymptoms of clinicalinfection; arterial ulcers;ulcer area >50 cm2; uncon-trolled diabetes mellitus;venous surgery within1 month on affected leg;ulcer with exposed muscle,tendon or bone; pregnancy;patients on antibiotics,steroids or chemotherapy;known HIV infection
Ulcer size varied greatlybetween patients: 1,9.1 cm2 (SE = 1.7); 2,6.0 cm2 (SE = 2.4)
1. Hydrocolloid dressing(Duoderm) + Coban (16)
2. Unna’s boot (14)
Complete healing at12 weeks:
1. 50%
2. 43%
Ulcer healing rate corre-lated with ulcer area andperimeter
Withdrawals: Duodermgroup, 7; Unna’s boot, 6
Costs not reported. Patientacceptance of bandage washigher with Duoderm thanUnna’s boot
continued
TABLE 6 contd Trials of the use of compression in the prevention and treatment of venous leg ulcers
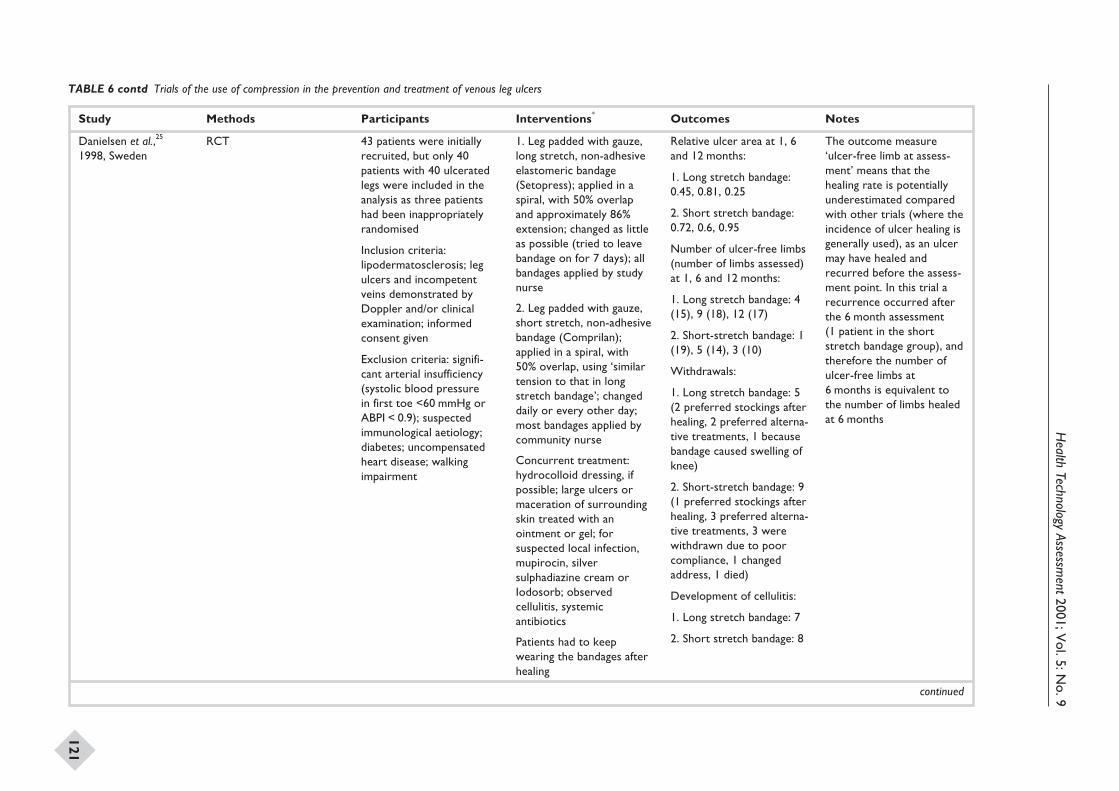
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
121
Study Methods Participants Interventions* Outcomes Notes
Danielsen et al.,25
1998, SwedenRCT 43 patients were initially
recruited, but only 40patients with 40 ulceratedlegs were included in theanalysis as three patientshad been inappropriatelyrandomised
Inclusion criteria:lipodermatosclerosis; legulcers and incompetentveins demonstrated byDoppler and/or clinicalexamination; informedconsent given
Exclusion criteria: signifi-cant arterial insufficiency(systolic blood pressurein first toe <60 mmHg orABPI < 0.9); suspectedimmunological aetiology;diabetes; uncompensatedheart disease; walkingimpairment
1. Leg padded with gauze,long stretch, non-adhesiveelastomeric bandage(Setopress); applied in aspiral, with 50% overlapand approximately 86%extension; changed as littleas possible (tried to leavebandage on for 7 days); allbandages applied by studynurse
2. Leg padded with gauze,short stretch, non-adhesivebandage (Comprilan);applied in a spiral, with50% overlap, using ‘similartension to that in longstretch bandage’; changeddaily or every other day;most bandages applied bycommunity nurse
Concurrent treatment:hydrocolloid dressing, ifpossible; large ulcers ormaceration of surroundingskin treated with anointment or gel; forsuspected local infection,mupirocin, silversulphadiazine cream orIodosorb; observedcellulitis, systemicantibiotics
Patients had to keepwearing the bandages afterhealing
Relative ulcer area at 1, 6and 12 months:
1. Long stretch bandage:0.45, 0.81, 0.25
2. Short stretch bandage:0.72, 0.6, 0.95
Number of ulcer-free limbs(number of limbs assessed)at 1, 6 and 12 months:
1. Long stretch bandage: 4(15), 9 (18), 12 (17)
2. Short-stretch bandage: 1(19), 5 (14), 3 (10)
Withdrawals:
1. Long stretch bandage: 5(2 preferred stockings afterhealing, 2 preferred alterna-tive treatments, 1 becausebandage caused swelling ofknee)
2. Short-stretch bandage: 9(1 preferred stockings afterhealing, 3 preferred alterna-tive treatments, 3 werewithdrawn due to poorcompliance, 1 changedaddress, 1 died)
Development of cellulitis:
1. Long stretch bandage: 7
2. Short stretch bandage: 8
The outcome measure‘ulcer-free limb at assess-ment’ means that thehealing rate is potentiallyunderestimated comparedwith other trials (where theincidence of ulcer healing isgenerally used), as an ulcermay have healed andrecurred before the assess-ment point. In this trial arecurrence occurred afterthe 6 month assessment(1 patient in the shortstretch bandage group), andtherefore the number ofulcer-free limbs at6 months is equivalent tothe number of limbs healedat 6 months
continued
TABLE 6 contd Trials of the use of compression in the prevention and treatment of venous leg ulcers
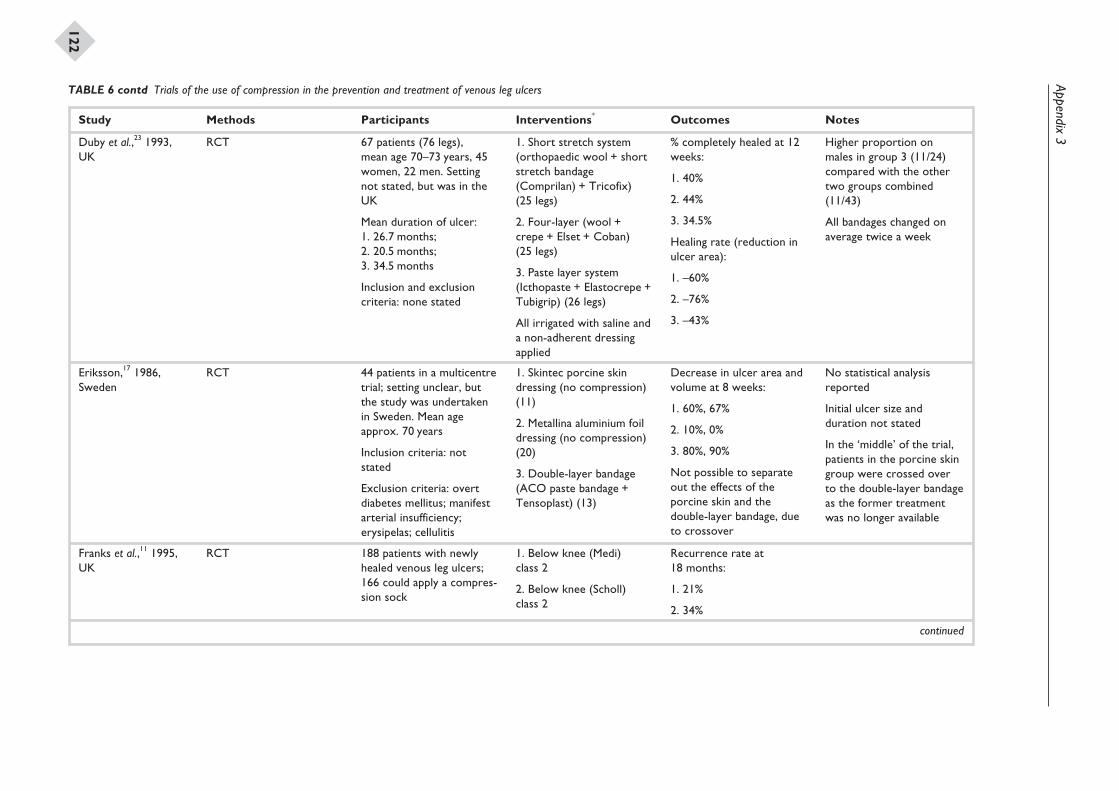
Appendix3
122
Study Methods Participants Interventions* Outcomes Notes
Duby et al.,23 1993,UK
RCT 67 patients (76 legs),mean age 70–73 years, 45women, 22 men. Settingnot stated, but was in theUK
Mean duration of ulcer:1. 26.7 months;2. 20.5 months;3. 34.5 months
Inclusion and exclusioncriteria: none stated
1. Short stretch system(orthopaedic wool + shortstretch bandage(Comprilan) + Tricofix)(25 legs)
2. Four-layer (wool +crepe + Elset + Coban)(25 legs)
3. Paste layer system(Icthopaste + Elastocrepe +Tubigrip) (26 legs)
All irrigated with saline anda non-adherent dressingapplied
% completely healed at 12weeks:
1. 40%
2. 44%
3. 34.5%
Healing rate (reduction inulcer area):
1. –60%
2. –76%
3. –43%
Higher proportion onmales in group 3 (11/24)compared with the othertwo groups combined(11/43)
All bandages changed onaverage twice a week
Eriksson,17 1986,Sweden
RCT 44 patients in a multicentretrial; setting unclear, butthe study was undertakenin Sweden. Mean ageapprox. 70 years
Inclusion criteria: notstated
Exclusion criteria: overtdiabetes mellitus; manifestarterial insufficiency;erysipelas; cellulitis
1. Skintec porcine skindressing (no compression)(11)
2. Metallina aluminium foildressing (no compression)(20)
3. Double-layer bandage(ACO paste bandage +Tensoplast) (13)
Decrease in ulcer area andvolume at 8 weeks:
1. 60%, 67%
2. 10%, 0%
3. 80%, 90%
Not possible to separateout the effects of theporcine skin and thedouble-layer bandage, dueto crossover
No statistical analysisreported
Initial ulcer size andduration not stated
In the ‘middle’ of the trial,patients in the porcine skingroup were crossed overto the double-layer bandageas the former treatmentwas no longer available
Franks et al.,11 1995,UK
RCT 188 patients with newlyhealed venous leg ulcers;166 could apply a compres-sion sock
1. Below knee (Medi)class 2
2. Below knee (Scholl)class 2
Recurrence rate at18 months:
1. 21%
2. 34%
continued
TABLE 6 contd Trials of the use of compression in the prevention and treatment of venous leg ulcers
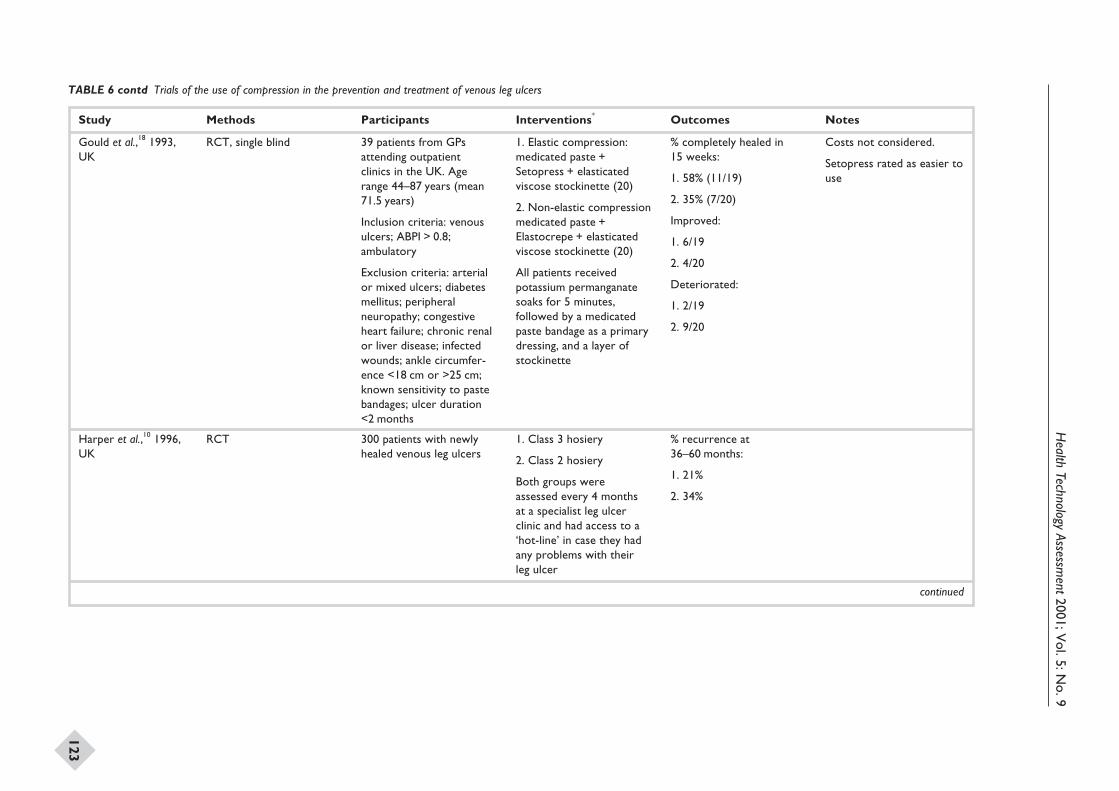
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
123
Study Methods Participants Interventions* Outcomes Notes
Gould et al.,18 1993,UK
RCT, single blind 39 patients from GPsattending outpatientclinics in the UK. Agerange 44–87 years (mean71.5 years)
Inclusion criteria: venousulcers; ABPI > 0.8;ambulatory
Exclusion criteria: arterialor mixed ulcers; diabetesmellitus; peripheralneuropathy; congestiveheart failure; chronic renalor liver disease; infectedwounds; ankle circumfer-ence <18 cm or >25 cm;known sensitivity to pastebandages; ulcer duration<2 months
1. Elastic compression:medicated paste +Setopress + elasticatedviscose stockinette (20)
2. Non-elastic compressionmedicated paste +Elastocrepe + elasticatedviscose stockinette (20)
All patients receivedpotassium permanganatesoaks for 5 minutes,followed by a medicatedpaste bandage as a primarydressing, and a layer ofstockinette
% completely healed in15 weeks:
1. 58% (11/19)
2. 35% (7/20)
Improved:
1. 6/19
2. 4/20
Deteriorated:
1. 2/19
2. 9/20
Costs not considered.
Setopress rated as easier touse
Harper et al.,10 1996,UK
RCT 300 patients with newlyhealed venous leg ulcers
1. Class 3 hosiery
2. Class 2 hosiery
Both groups wereassessed every 4 monthsat a specialist leg ulcerclinic and had access to a‘hot-line’ in case they hadany problems with theirleg ulcer
% recurrence at36–60 months:
1. 21%
2. 34%
continued
TABLE 6 contd Trials of the use of compression in the prevention and treatment of venous leg ulcers
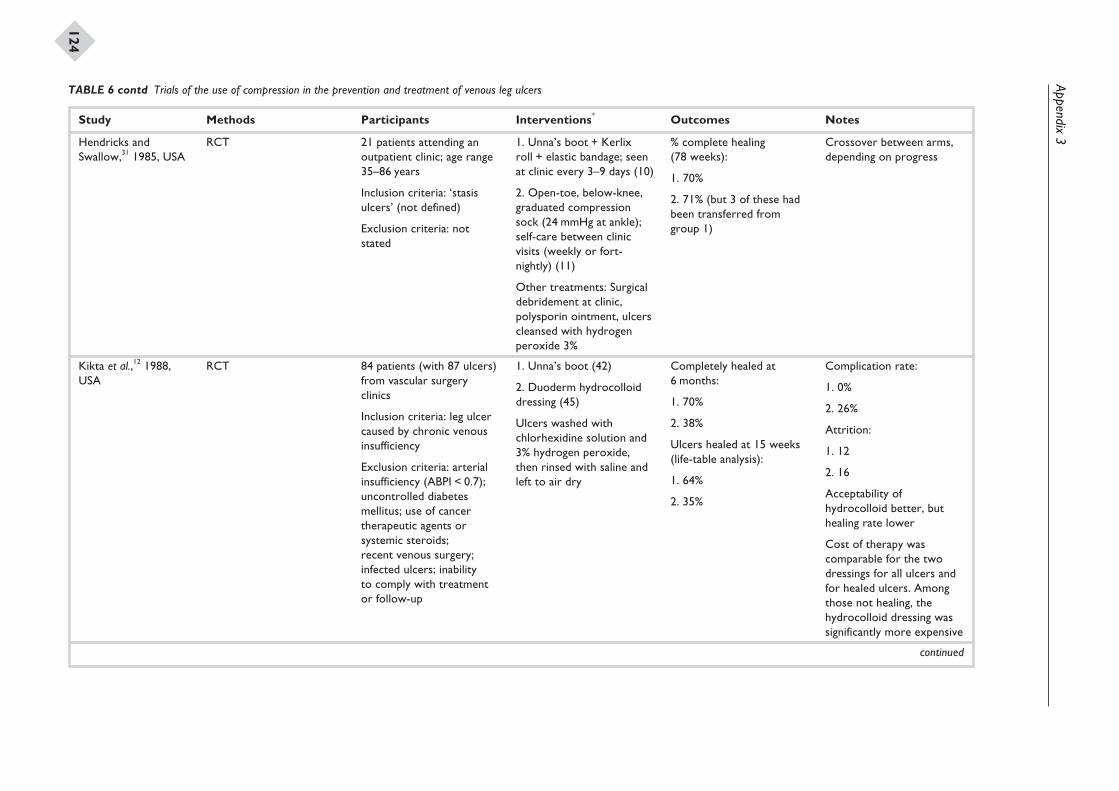
Appendix3
124
Study Methods Participants Interventions* Outcomes Notes
Hendricks andSwallow,31 1985, USA
RCT 21 patients attending anoutpatient clinic; age range35–86 years
Inclusion criteria: ‘stasisulcers’ (not defined)
Exclusion criteria: notstated
1. Unna’s boot + Kerlixroll + elastic bandage; seenat clinic every 3–9 days (10)
2. Open-toe, below-knee,graduated compressionsock (24 mmHg at ankle);self-care between clinicvisits (weekly or fort-nightly) (11)
Other treatments: Surgicaldebridement at clinic,polysporin ointment, ulcerscleansed with hydrogenperoxide 3%
% complete healing(78 weeks):
1. 70%
2. 71% (but 3 of these hadbeen transferred fromgroup 1)
Crossover between arms,depending on progress
Kikta et al.,12 1988,USA
RCT 84 patients (with 87 ulcers)from vascular surgeryclinics
Inclusion criteria: leg ulcercaused by chronic venousinsufficiency
Exclusion criteria: arterialinsufficiency (ABPI < 0.7);uncontrolled diabetesmellitus; use of cancertherapeutic agents orsystemic steroids;recent venous surgery;infected ulcers; inabilityto comply with treatmentor follow-up
1. Unna’s boot (42)
2. Duoderm hydrocolloiddressing (45)
Ulcers washed withchlorhexidine solution and3% hydrogen peroxide,then rinsed with saline andleft to air dry
Completely healed at6 months:
1. 70%
2. 38%
Ulcers healed at 15 weeks(life-table analysis):
1. 64%
2. 35%
Complication rate:
1. 0%
2. 26%
Attrition:
1. 12
2. 16
Acceptability ofhydrocolloid better, buthealing rate lower
Cost of therapy wascomparable for the twodressings for all ulcers andfor healed ulcers. Amongthose not healing, thehydrocolloid dressing wassignificantly more expensive
continued
TABLE 6 contd Trials of the use of compression in the prevention and treatment of venous leg ulcers
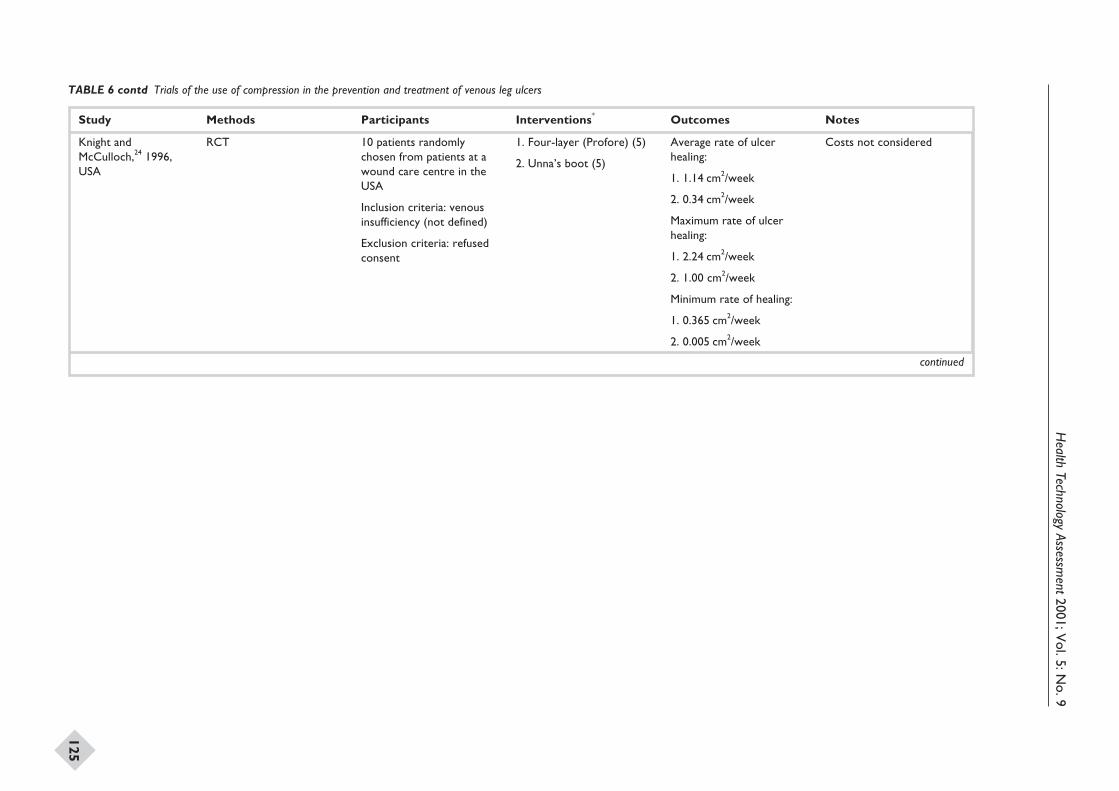
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
125
Study Methods Participants Interventions* Outcomes Notes
Knight andMcCulloch,24 1996,USA
RCT 10 patients randomlychosen from patients at awound care centre in theUSA
Inclusion criteria: venousinsufficiency (not defined)
Exclusion criteria: refusedconsent
1. Four-layer (Profore) (5)
2. Unna’s boot (5)
Average rate of ulcerhealing:
1. 1.14 cm2/week
2. 0.34 cm2/week
Maximum rate of ulcerhealing:
1. 2.24 cm2/week
2. 1.00 cm2/week
Minimum rate of healing:
1. 0.365 cm2/week
2. 0.005 cm2/week
Costs not considered
continued
TABLE 6 contd Trials of the use of compression in the prevention and treatment of venous leg ulcers
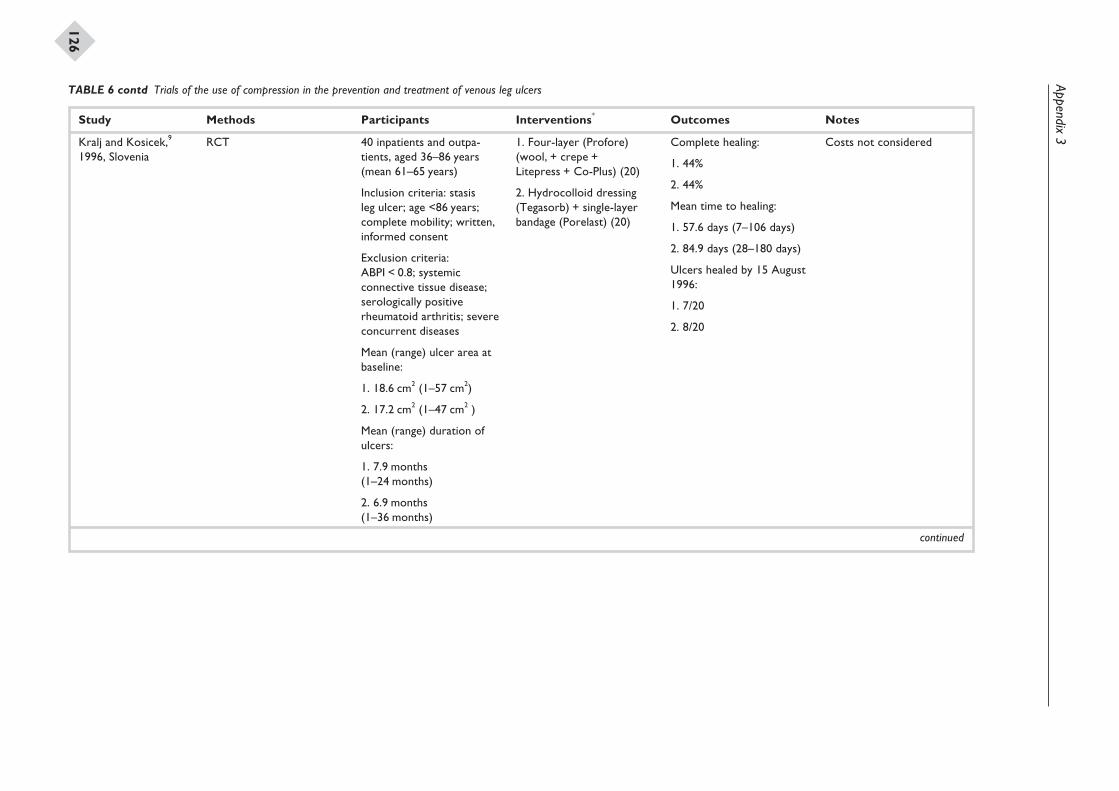
Appendix3
126
Study Methods Participants Interventions* Outcomes Notes
Kralj and Kosicek,9
1996, SloveniaRCT 40 inpatients and outpa-
tients, aged 36–86 years(mean 61–65 years)
Inclusion criteria: stasisleg ulcer; age <86 years;complete mobility; written,informed consent
Exclusion criteria:ABPI < 0.8; systemicconnective tissue disease;serologically positiverheumatoid arthritis; severeconcurrent diseases
Mean (range) ulcer area atbaseline:
1. 18.6 cm2 (1–57 cm2)
2. 17.2 cm2 (1–47 cm2 )
Mean (range) duration ofulcers:
1. 7.9 months(1–24 months)
2. 6.9 months(1–36 months)
1. Four-layer (Profore)(wool, + crepe +Litepress + Co-Plus) (20)
2. Hydrocolloid dressing(Tegasorb) + single-layerbandage (Porelast) (20)
Complete healing:
1. 44%
2. 44%
Mean time to healing:
1. 57.6 days (7–106 days)
2. 84.9 days (28–180 days)
Ulcers healed by 15 August1996:
1. 7/20
2. 8/20
Costs not considered
continued
TABLE 6 contd Trials of the use of compression in the prevention and treatment of venous leg ulcers
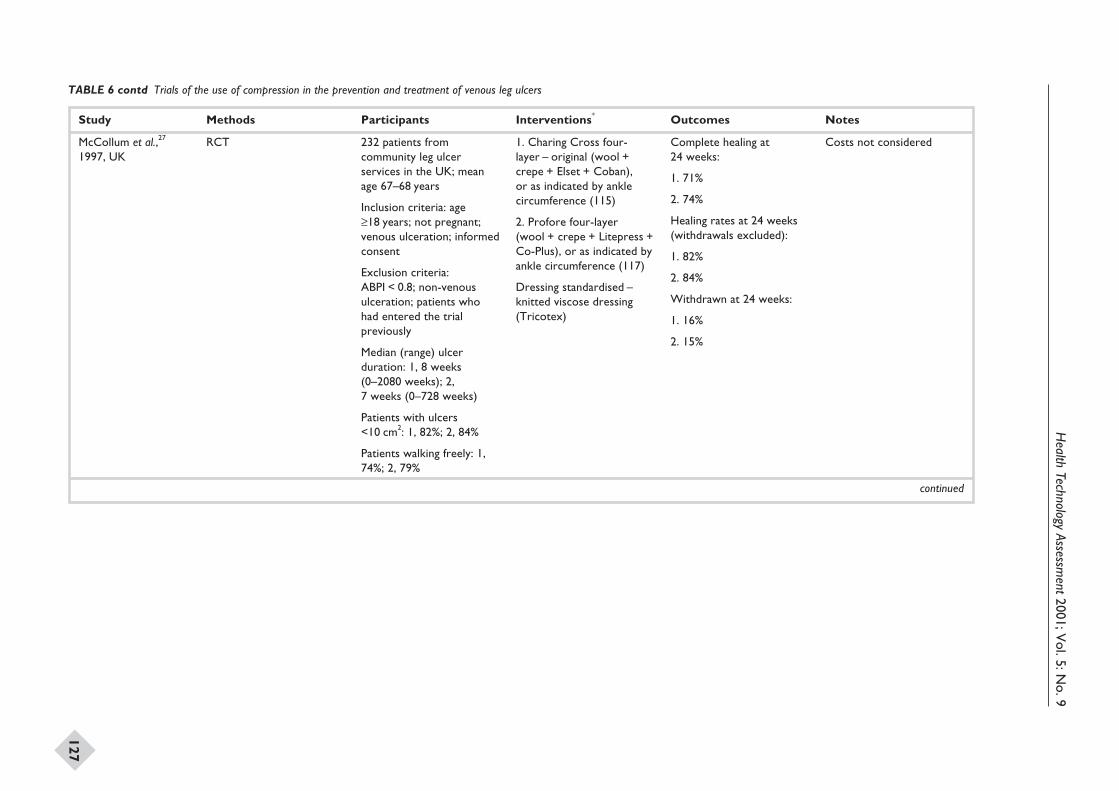
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
127
Study Methods Participants Interventions* Outcomes Notes
McCollum et al.,27
1997, UKRCT 232 patients from
community leg ulcerservices in the UK; meanage 67–68 years
Inclusion criteria: age≥18 years; not pregnant;venous ulceration; informedconsent
Exclusion criteria:ABPI < 0.8; non-venousulceration; patients whohad entered the trialpreviously
Median (range) ulcerduration: 1, 8 weeks(0–2080 weeks); 2,7 weeks (0–728 weeks)
Patients with ulcers<10 cm2: 1, 82%; 2, 84%
Patients walking freely: 1,74%; 2, 79%
1. Charing Cross four-layer – original (wool +crepe + Elset + Coban),or as indicated by anklecircumference (115)
2. Profore four-layer(wool + crepe + Litepress +Co-Plus), or as indicated byankle circumference (117)
Dressing standardised –knitted viscose dressing(Tricotex)
Complete healing at24 weeks:
1. 71%
2. 74%
Healing rates at 24 weeks(withdrawals excluded):
1. 82%
2. 84%
Withdrawn at 24 weeks:
1. 16%
2. 15%
Costs not considered
continued
TABLE 6 contd Trials of the use of compression in the prevention and treatment of venous leg ulcers
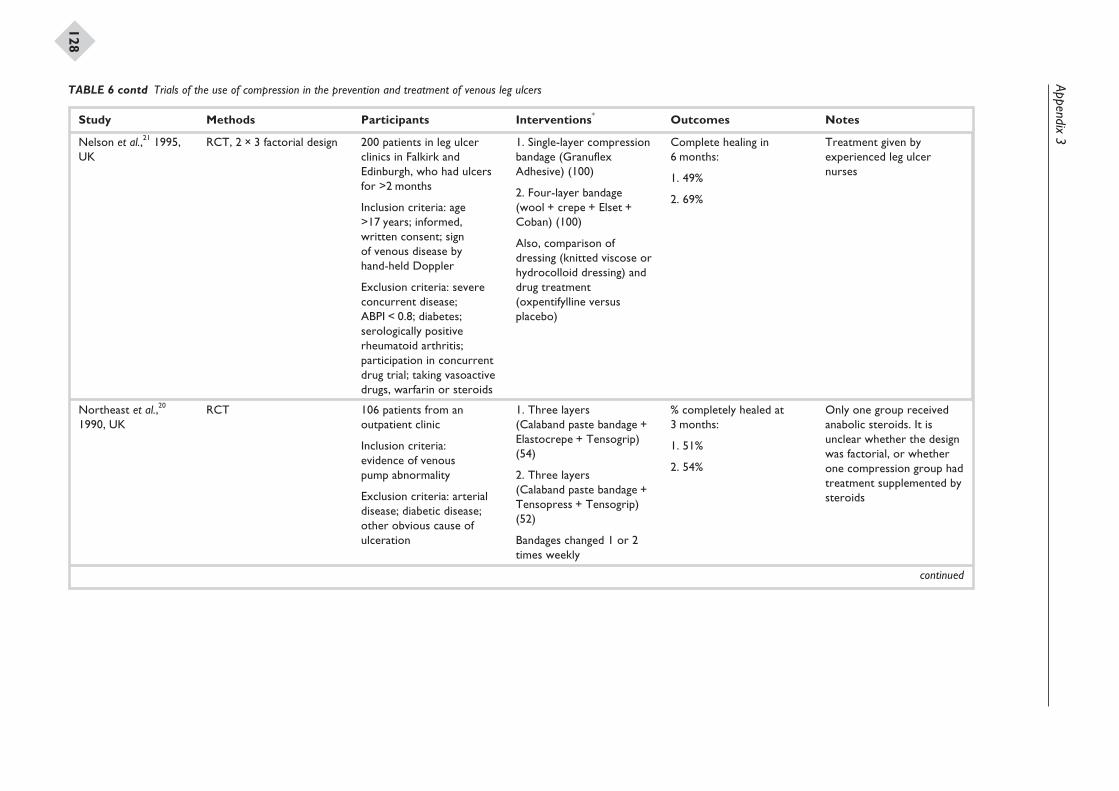
Appendix3
128
Study Methods Participants Interventions* Outcomes Notes
Nelson et al.,21 1995,UK
RCT, 2 × 3 factorial design 200 patients in leg ulcerclinics in Falkirk andEdinburgh, who had ulcersfor >2 months
Inclusion criteria: age>17 years; informed,written consent; signof venous disease byhand-held Doppler
Exclusion criteria: severeconcurrent disease;ABPI < 0.8; diabetes;serologically positiverheumatoid arthritis;participation in concurrentdrug trial; taking vasoactivedrugs, warfarin or steroids
1. Single-layer compressionbandage (GranuflexAdhesive) (100)
2. Four-layer bandage(wool + crepe + Elset +Coban) (100)
Also, comparison ofdressing (knitted viscose orhydrocolloid dressing) anddrug treatment(oxpentifylline versusplacebo)
Complete healing in6 months:
1. 49%
2. 69%
Treatment given byexperienced leg ulcernurses
Northeast et al.,20
1990, UKRCT 106 patients from an
outpatient clinic
Inclusion criteria:evidence of venouspump abnormality
Exclusion criteria: arterialdisease; diabetic disease;other obvious cause ofulceration
1. Three layers(Calaband paste bandage +Elastocrepe + Tensogrip)(54)
2. Three layers(Calaband paste bandage +Tensopress + Tensogrip)(52)
Bandages changed 1 or 2times weekly
% completely healed at3 months:
1. 51%
2. 54%
Only one group receivedanabolic steroids. It isunclear whether the designwas factorial, or whetherone compression group hadtreatment supplemented bysteroids
continued
TABLE 6 contd Trials of the use of compression in the prevention and treatment of venous leg ulcers
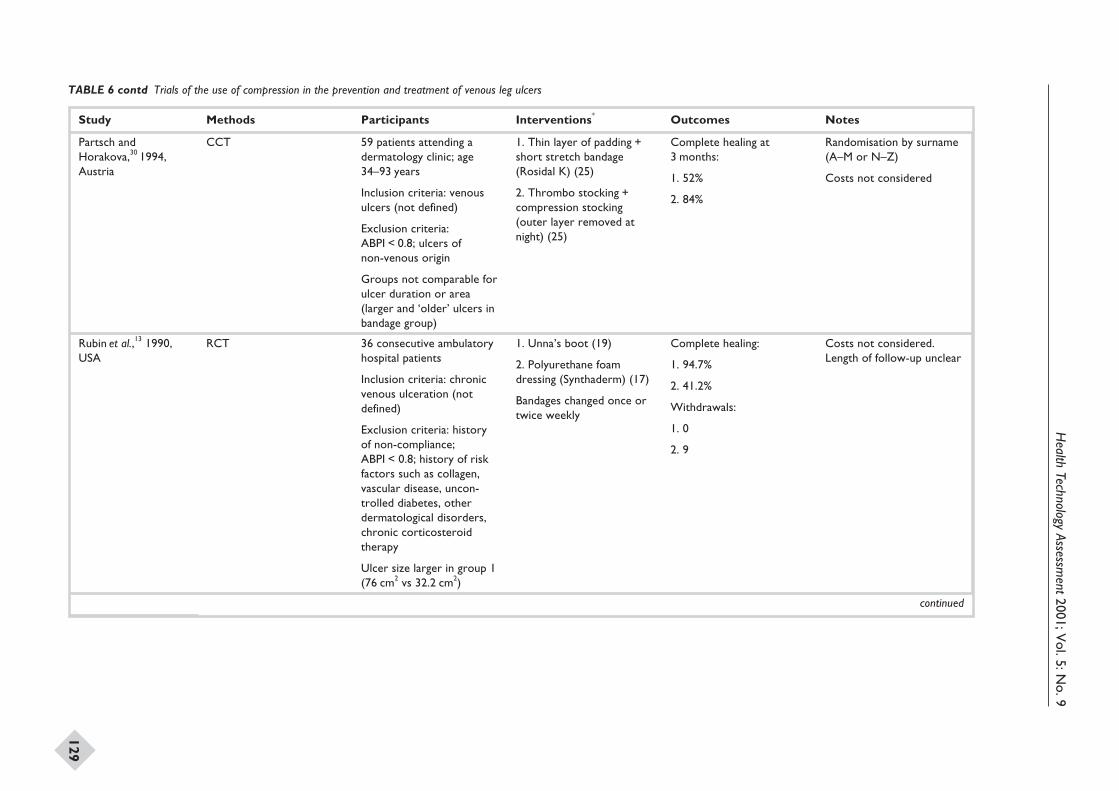
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
129
Study Methods Participants Interventions* Outcomes Notes
Partsch andHorakova,30 1994,Austria
CCT 59 patients attending adermatology clinic; age34–93 years
Inclusion criteria: venousulcers (not defined)
Exclusion criteria:ABPI < 0.8; ulcers ofnon-venous origin
Groups not comparable forulcer duration or area(larger and ‘older’ ulcers inbandage group)
1. Thin layer of padding +short stretch bandage(Rosidal K) (25)
2. Thrombo stocking +compression stocking(outer layer removed atnight) (25)
Complete healing at3 months:
1. 52%
2. 84%
Randomisation by surname(A–M or N–Z)
Costs not considered
Rubin et al.,13 1990,USA
RCT 36 consecutive ambulatoryhospital patients
Inclusion criteria: chronicvenous ulceration (notdefined)
Exclusion criteria: historyof non-compliance;ABPI < 0.8; history of riskfactors such as collagen,vascular disease, uncon-trolled diabetes, otherdermatological disorders,chronic corticosteroidtherapy
Ulcer size larger in group 1(76 cm2 vs 32.2 cm2)
1. Unna’s boot (19)
2. Polyurethane foamdressing (Synthaderm) (17)
Bandages changed once ortwice weekly
Complete healing:
1. 94.7%
2. 41.2%
Withdrawals:
1. 0
2. 9
Costs not considered.Length of follow-up unclear
continued
TABLE 6 contd Trials of the use of compression in the prevention and treatment of venous leg ulcers
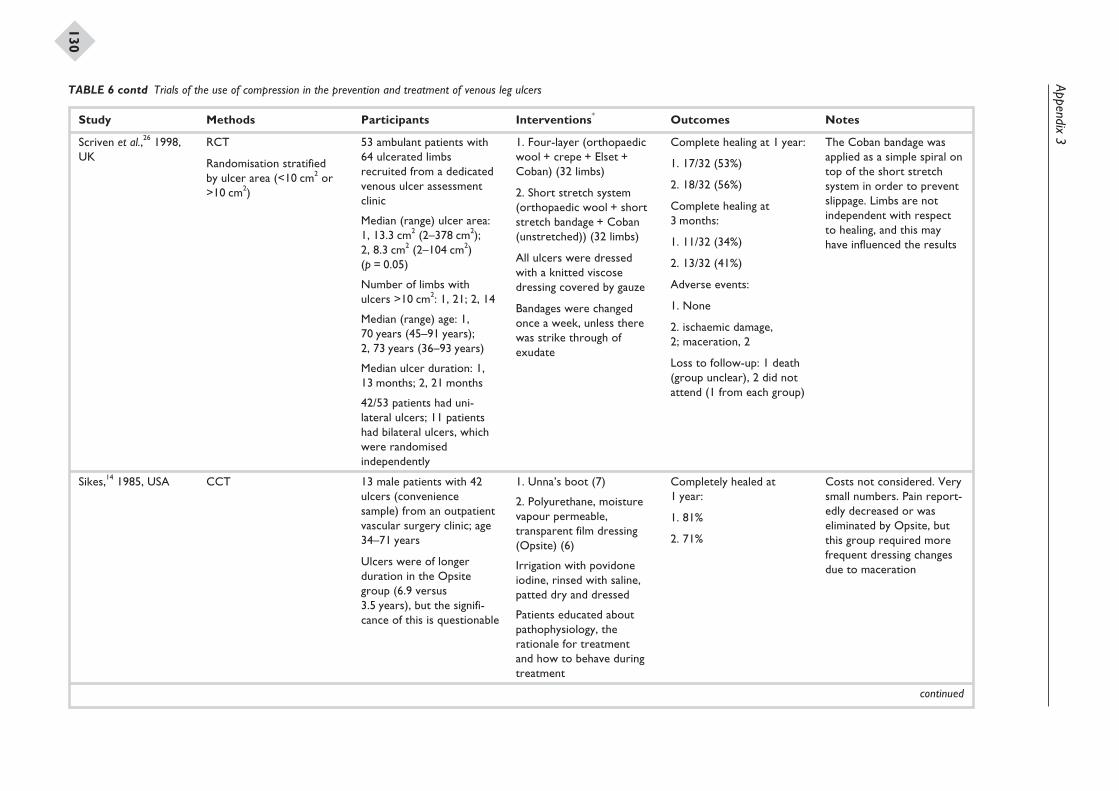
Appendix3
130
Study Methods Participants Interventions* Outcomes Notes
Scriven et al.,26 1998,UK
RCT
Randomisation stratifiedby ulcer area (<10 cm2 or>10 cm2)
53 ambulant patients with64 ulcerated limbsrecruited from a dedicatedvenous ulcer assessmentclinic
Median (range) ulcer area:1, 13.3 cm2 (2–378 cm2);2, 8.3 cm2 (2–104 cm2)(p = 0.05)
Number of limbs withulcers >10 cm2: 1, 21; 2, 14
Median (range) age: 1,70 years (45–91 years);2, 73 years (36–93 years)
Median ulcer duration: 1,13 months; 2, 21 months
42/53 patients had uni-lateral ulcers; 11 patientshad bilateral ulcers, whichwere randomisedindependently
1. Four-layer (orthopaedicwool + crepe + Elset +Coban) (32 limbs)
2. Short stretch system(orthopaedic wool + shortstretch bandage + Coban(unstretched)) (32 limbs)
All ulcers were dressedwith a knitted viscosedressing covered by gauze
Bandages were changedonce a week, unless therewas strike through ofexudate
Complete healing at 1 year:
1. 17/32 (53%)
2. 18/32 (56%)
Complete healing at3 months:
1. 11/32 (34%)
2. 13/32 (41%)
Adverse events:
1. None
2. ischaemic damage,2; maceration, 2
Loss to follow-up: 1 death(group unclear), 2 did notattend (1 from each group)
The Coban bandage wasapplied as a simple spiral ontop of the short stretchsystem in order to preventslippage. Limbs are notindependent with respectto healing, and this mayhave influenced the results
Sikes,14 1985, USA CCT 13 male patients with 42ulcers (conveniencesample) from an outpatientvascular surgery clinic; age34–71 years
Ulcers were of longerduration in the Opsitegroup (6.9 versus3.5 years), but the signifi-cance of this is questionable
1. Unna’s boot (7)
2. Polyurethane, moisturevapour permeable,transparent film dressing(Opsite) (6)
Irrigation with povidoneiodine, rinsed with saline,patted dry and dressed
Patients educated aboutpathophysiology, therationale for treatmentand how to behave duringtreatment
Completely healed at1 year:
1. 81%
2. 71%
Costs not considered. Verysmall numbers. Pain report-edly decreased or waseliminated by Opsite, butthis group required morefrequent dressing changesdue to maceration
continued
TABLE 6 contd Trials of the use of compression in the prevention and treatment of venous leg ulcers
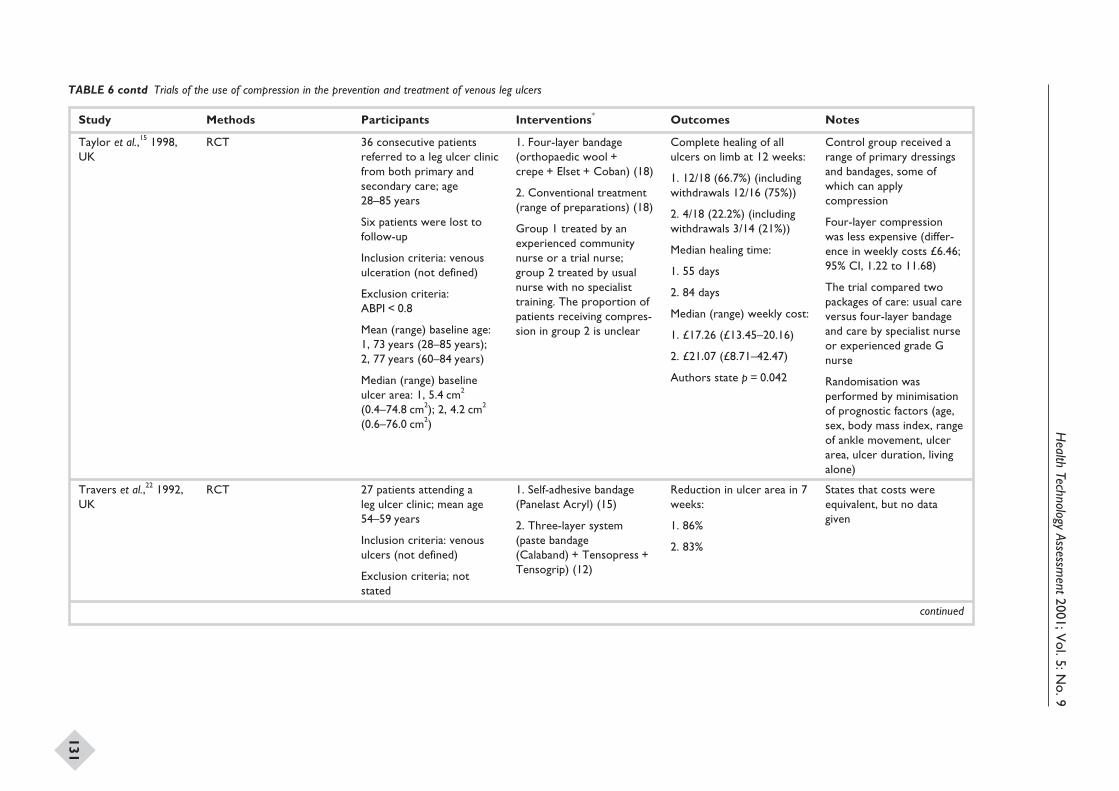
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
131
Study Methods Participants Interventions* Outcomes Notes
Taylor et al.,15 1998,UK
RCT 36 consecutive patientsreferred to a leg ulcer clinicfrom both primary andsecondary care; age28–85 years
Six patients were lost tofollow-up
Inclusion criteria: venousulceration (not defined)
Exclusion criteria:ABPI < 0.8
Mean (range) baseline age:1, 73 years (28–85 years);2, 77 years (60–84 years)
Median (range) baselineulcer area: 1, 5.4 cm2
(0.4–74.8 cm2); 2, 4.2 cm2
(0.6–76.0 cm2)
1. Four-layer bandage(orthopaedic wool +crepe + Elset + Coban) (18)
2. Conventional treatment(range of preparations) (18)
Group 1 treated by anexperienced communitynurse or a trial nurse;group 2 treated by usualnurse with no specialisttraining. The proportion ofpatients receiving compres-sion in group 2 is unclear
Complete healing of allulcers on limb at 12 weeks:
1. 12/18 (66.7%) (includingwithdrawals 12/16 (75%))
2. 4/18 (22.2%) (includingwithdrawals 3/14 (21%))
Median healing time:
1. 55 days
2. 84 days
Median (range) weekly cost:
1. £17.26 (£13.45–20.16)
2. £21.07 (£8.71–42.47)
Authors state p = 0.042
Control group received arange of primary dressingsand bandages, some ofwhich can applycompression
Four-layer compressionwas less expensive (differ-ence in weekly costs £6.46;95% CI, 1.22 to 11.68)
The trial compared twopackages of care: usual careversus four-layer bandageand care by specialist nurseor experienced grade Gnurse
Randomisation wasperformed by minimisationof prognostic factors (age,sex, body mass index, rangeof ankle movement, ulcerarea, ulcer duration, livingalone)
Travers et al.,22 1992,UK
RCT 27 patients attending aleg ulcer clinic; mean age54–59 years
Inclusion criteria: venousulcers (not defined)
Exclusion criteria; notstated
1. Self-adhesive bandage(Panelast Acryl) (15)
2. Three-layer system(paste bandage(Calaband) + Tensopress +Tensogrip) (12)
Reduction in ulcer area in 7weeks:
1. 86%
2. 83%
States that costs wereequivalent, but no datagiven
continued
TABLE 6 contd Trials of the use of compression in the prevention and treatment of venous leg ulcers
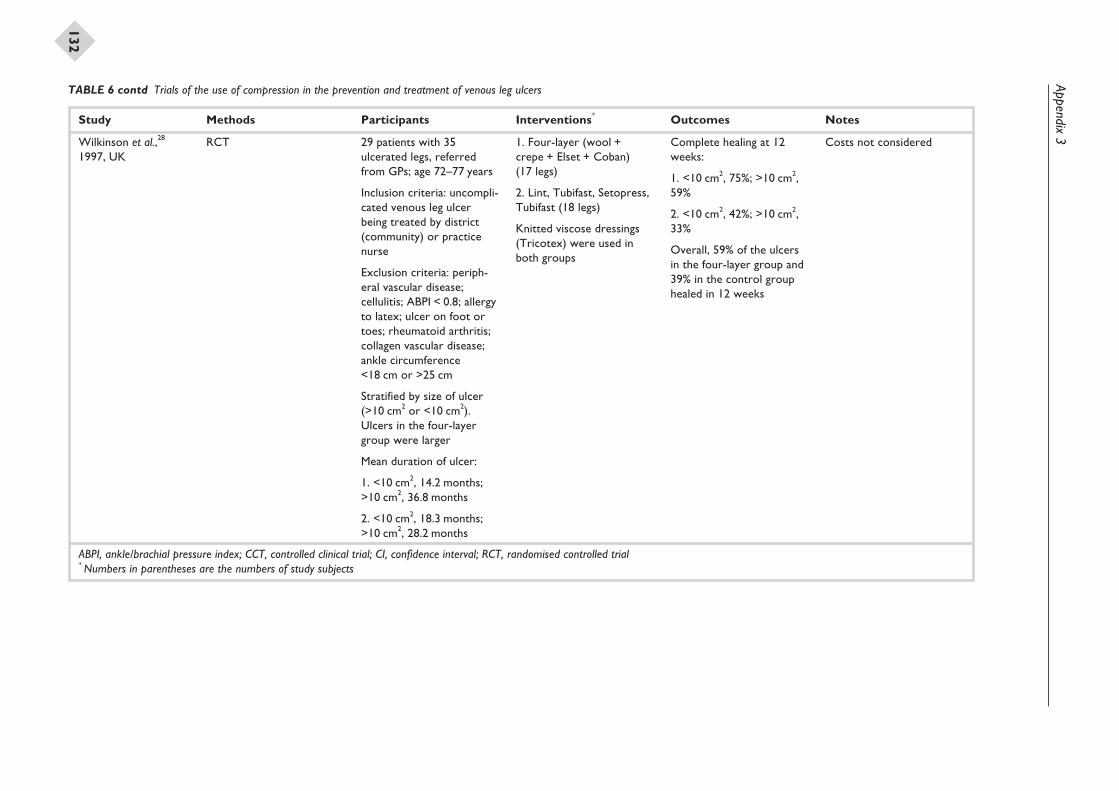
Appendix3
132
Study Methods Participants Interventions* Outcomes Notes
Wilkinson et al.,28
1997, UKRCT 29 patients with 35
ulcerated legs, referredfrom GPs; age 72–77 years
Inclusion criteria: uncompli-cated venous leg ulcerbeing treated by district(community) or practicenurse
Exclusion criteria: periph-eral vascular disease;cellulitis; ABPI < 0.8; allergyto latex; ulcer on foot ortoes; rheumatoid arthritis;collagen vascular disease;ankle circumference<18 cm or >25 cm
Stratified by size of ulcer(>10 cm2 or <10 cm2).Ulcers in the four-layergroup were larger
Mean duration of ulcer:
1. <10 cm2, 14.2 months;>10 cm2, 36.8 months
2. <10 cm2, 18.3 months;>10 cm2, 28.2 months
1. Four-layer (wool +crepe + Elset + Coban)(17 legs)
2. Lint, Tubifast, Setopress,Tubifast (18 legs)
Knitted viscose dressings(Tricotex) were used inboth groups
Complete healing at 12weeks:
1. <10 cm2, 75%; >10 cm2,59%
2. <10 cm2, 42%; >10 cm2,33%
Overall, 59% of the ulcersin the four-layer group and39% in the control grouphealed in 12 weeks
Costs not considered
ABPI, ankle/brachial pressure index; CCT, controlled clinical trial; CI, confidence interval; RCT, randomised controlled trial* Numbers in parentheses are the numbers of study subjects
TABLE 6 contd Trials of the use of compression in the prevention and treatment of venous leg ulcers
Appendix 4
Quality assessment of included studies
Health Technology Assessment 2001; Vol. 5: No. 9
133
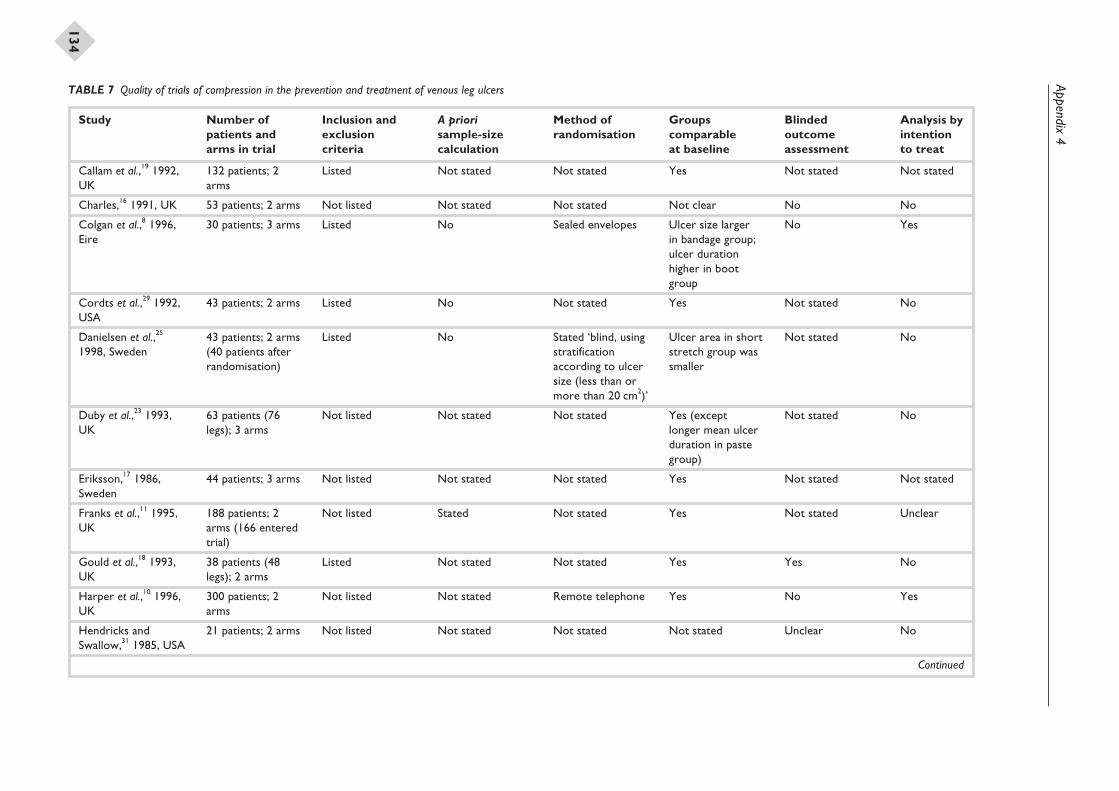
Appendix4
134
Study Number ofpatients andarms in trial
Inclusion andexclusioncriteria
A priorisample-sizecalculation
Method ofrandomisation
Groupscomparableat baseline
Blindedoutcomeassessment
Analysis byintentionto treat
Callam et al.,19 1992,UK
132 patients; 2arms
Listed Not stated Not stated Yes Not stated Not stated
Charles,16 1991, UK 53 patients; 2 arms Not listed Not stated Not stated Not clear No No
Colgan et al.,8 1996,Eire
30 patients; 3 arms Listed No Sealed envelopes Ulcer size largerin bandage group;ulcer durationhigher in bootgroup
No Yes
Cordts et al.,29 1992,USA
43 patients; 2 arms Listed No Not stated Yes Not stated No
Danielsen et al.,25
1998, Sweden43 patients; 2 arms(40 patients afterrandomisation)
Listed No Stated ‘blind, usingstratificationaccording to ulcersize (less than ormore than 20 cm2)’
Ulcer area in shortstretch group wassmaller
Not stated No
Duby et al.,23 1993,UK
63 patients (76legs); 3 arms
Not listed Not stated Not stated Yes (exceptlonger mean ulcerduration in pastegroup)
Not stated No
Eriksson,17 1986,Sweden
44 patients; 3 arms Not listed Not stated Not stated Yes Not stated Not stated
Franks et al.,11 1995,UK
188 patients; 2arms (166 enteredtrial)
Not listed Stated Not stated Yes Not stated Unclear
Gould et al.,18 1993,UK
38 patients (48legs); 2 arms
Listed Not stated Not stated Yes Yes No
Harper et al.,10 1996,UK
300 patients; 2arms
Not listed Not stated Remote telephone Yes No Yes
Hendricks andSwallow,31 1985, USA
21 patients; 2 arms Not listed Not stated Not stated Not stated Unclear No
Continued
TABLE 7 Quality of trials of compression in the prevention and treatment of venous leg ulcers
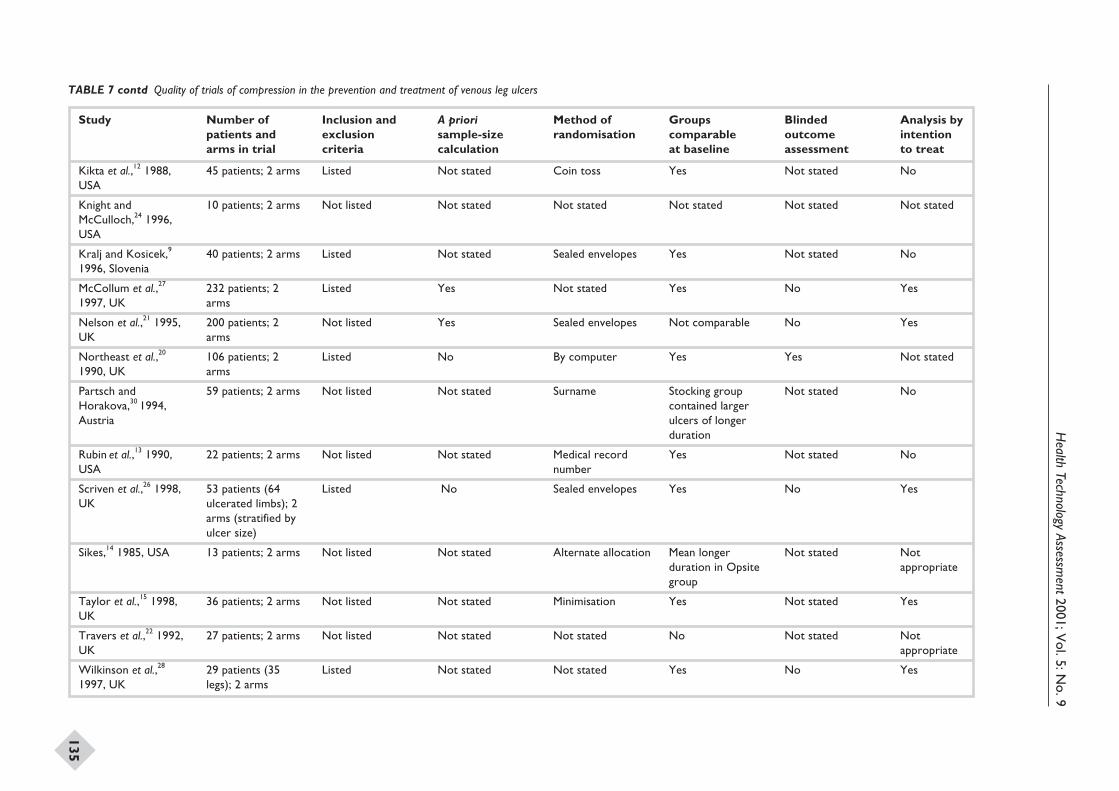
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
135
Study Number ofpatients andarms in trial
Inclusion andexclusioncriteria
A priorisample-sizecalculation
Method ofrandomisation
Groupscomparableat baseline
Blindedoutcomeassessment
Analysis byintentionto treat
Kikta et al.,12 1988,USA
45 patients; 2 arms Listed Not stated Coin toss Yes Not stated No
Knight andMcCulloch,24 1996,USA
10 patients; 2 arms Not listed Not stated Not stated Not stated Not stated Not stated
Kralj and Kosicek,9
1996, Slovenia40 patients; 2 arms Listed Not stated Sealed envelopes Yes Not stated No
McCollum et al.,27
1997, UK232 patients; 2arms
Listed Yes Not stated Yes No Yes
Nelson et al.,21 1995,UK
200 patients; 2arms
Not listed Yes Sealed envelopes Not comparable No Yes
Northeast et al.,20
1990, UK106 patients; 2arms
Listed No By computer Yes Yes Not stated
Partsch andHorakova,30 1994,Austria
59 patients; 2 arms Not listed Not stated Surname Stocking groupcontained largerulcers of longerduration
Not stated No
Rubin et al.,13 1990,USA
22 patients; 2 arms Not listed Not stated Medical recordnumber
Yes Not stated No
Scriven et al.,26 1998,UK
53 patients (64ulcerated limbs); 2arms (stratified byulcer size)
Listed No Sealed envelopes Yes No Yes
Sikes,14 1985, USA 13 patients; 2 arms Not listed Not stated Alternate allocation Mean longerduration in Opsitegroup
Not stated Notappropriate
Taylor et al.,15 1998,UK
36 patients; 2 arms Not listed Not stated Minimisation Yes Not stated Yes
Travers et al.,22 1992,UK
27 patients; 2 arms Not listed Not stated Not stated No Not stated Notappropriate
Wilkinson et al.,28
1997, UK29 patients (35legs); 2 arms
Listed Not stated Not stated Yes No Yes
TABLE 7 contd Quality of trials of compression in the prevention and treatment of venous leg ulcers

Systematic reviews of wound caremanagement (7): low-level laser therapy,therapeutic ultrasound, electrotherapyand electromagnetic therapy for thetreatment of chronic wounds
K Flemming*
N Cullum
Centre for Evidence Based Nursing, Department of Health Studies,University of York, UK
* Corresponding author
Competing interests: N Cullum has: received funds from the NHS R&D Programmeto undertake primary research in wound care; received sponsorship of trial-relatededucational meetings from Huntleigh Healthcare and Beiersdorf Ltd

List of abbreviations ......................................... 141
Executive summary to Part 7 ......................... 143
1 Introduction .................................................. 145Types of wound .............................................. 145The role of physical therapies in woundhealing ............................................................ 146Aims and objectives ....................................... 147
2 Methods ......................................................... 149Search strategy ............................................... 149Inclusion criteria ............................................ 149Data extraction .............................................. 149Methodological quality .................................. 150Data synthesis ................................................. 150
3 Results ............................................................ 151Quality of included studies ........................... 151Studies excluded from the review ................ 151Low-level laser therapy .................................. 151Therapeutic ultrasound ................................ 152Electrotherapy ................................................ 155Electromagnetic therapy ............................... 159
4 Discussion ...................................................... 161
Low-level laser therapy .................................. 161Therapeutic ultrasound ................................ 161Electrotherapy ................................................ 161Electromagnetic therapy ............................... 161Secondary outcome measures ...................... 162
5 Conclusions ................................................... 163Implications for clinical practice .................. 163Implications for future research ................... 163
Acknowledgements ..................................... 165
References ..................................................... 167
Appendix 1 Databases searched andsearch strategies ............................................. 171
Appendix 2 Advisory panel ....................... 175
Appendix 3 Summary of includedstudies ............................................................. 177
Appendix 4 Quality assessment ofincluded studies ............................................. 207
Health Technology Assessment 2001; Vol. 5: No. 9
139
Contents to Part 7

Health Technology Assessment 2001; Vol. 5: No. 9
141
List of abbreviations
CI confidence interval
df degrees of freedom*
GaAs gallium arsenide
HeNe helium–neon
PEMF pulsed electromagnetic field
RCT randomised controlled trial
RR relative risk
SD standard deviation
* Used only in tables and figures

Objectives
To evaluate the evidence of the effectiveness oflow-level laser therapy, therapeutic ultrasound,electrotherapy and electromagnetic therapy inthe treatment of chronic wounds.
Methods
Data sourcesNineteen electronic databases, includingMEDLINE, EMBASE, CINAHL and the CochraneWounds Group’s specialised trials register, andwound care journals were searched for the periodup to December 1999. Organisations, manufac-turers, researchers and healthcare professionalsconcerned with wound care were contacted foradditional trials. The reference sections of theobtained studies were also searched for furthertrials.
Study selectionRandomised controlled trials (RCTs), published orunpublished, which assessed the effectiveness oflow-level laser therapy, therapeutic ultrasound,electrotherapy or electromagnetic therapy in thetreatment of chronic wounds were included inthe review. Studies in any language were eligiblefor inclusion. Studies were only included if theyreported either the proportion of wounds healedwithin a certain time period or the percentage orabsolute change in wound area. Decisions on therelevance of primary studies were made independ-ently by two reviewers.
Data extraction and synthesisDetails of the studies were extracted and summa-rised using a data-extraction sheet. If data weremissing from a report, an attempt was made tocontact the authors to obtain missing information.Studies published in duplicate were included onlyonce. Data extraction was undertaken by onereviewer and checked for accuracy by a second.
Data were assessed on the following aspects ofquality: use of clear inclusion and exclusioncriteria; adequacy of allocation concealment;baseline comparability of treatment groups for
important variables (e.g. wound size); use of inten-tion-to-treat analysis; extent of loss to follow-up;and use of blinded outcome assessment
The studies included in the review were combinedby narrative overview, with a quantitative summaryof the results of similar trials where appropriate.This involved meta-analysis of outcome data usingthe Cochrane Revman software. For each trial withimportant dichotomous outcomes (e.g. number ofulcers healed), the relative risk and the 95% confi-dence intervals were calculated.
Results
Low-level laser therapy for thetreatment of venous leg ulcersOnly four studies met the inclusion criteria. Theonly suggestion of therapeutic benefit was shownin one small RCT where a combination of laserand infrared light led to a significant improvementin the healing rates of venous ulcers. However, theresults of this trial and the others included in thissection were drawn from small studies withoutclear inclusion criteria for venous leg ulcers andof poor baseline comparability. As such, the resultsshould be viewed with caution.
Therapeutic ultrasound for thetreatment of venous leg ulcersThere was no clear evidence of a benefit of treatingvenous leg ulcers with therapeutic ultrasound, asthe seven small trials eligible for inclusion in thereview were inconclusive.
Therapeutic ultrasound for thetreatment of pressure soresThree studies were eligible for inclusion. Theresults of these studies do not suggest a benefitassociated with therapeutic ultrasound in thehealing of pressure sores. The trials included inthis section involved small numbers of patients,different regimens of therapeutic ultrasound anddifferent follow-up periods. The trials also hadinadequate staging of pressure sores and baselinecomparisons. The results should therefore beviewed with caution.
Health Technology Assessment 2001; Vol. 5: No. 9
143
Executive summary to Part 7
Electrotherapy for the treatment ofchronic woundsThe results suggest that there may be some benefitassociated with electrotherapy in the healing ofchronic wounds. This suggestion is made withcaution, as there are only three small trials with atotal of 63 patients involved, making it impossibleto determine clinically important effects.
Electrotherapy for the treatment ofischaemic ulcersThe results were difficult to interpret as the fivetrials eligible for inclusion in this section weresmall and mostly of poor quality. Those trials thathad better methodological quality were biased forbaseline ulcer area. As such, no recommendationscan be made for practice.
Electrotherapy for diabetic ulcersThe one small trial identified demonstrated nosignificant benefit of the use of electrotherapy totreat diabetic ulcers.
Electrotherapy for pressure soresThe three trials identified suggest a benefit associ-ated with using electrotherapy to treat pressuresores. However, this suggestion is drawn fromthree small studies with a total of 140 patients, andtherefore the results should be viewed with cautionas it is difficult to determine clinically importanteffects from such small samples.
Electromagnetic therapy for thetreatment of venous leg ulcersThe three small, poor-quality trials identifiedprovide no evidence of a benefit of electromagnetictherapy for the treatment of venous leg ulcers.
Electromagnetic therapy for thetreatment of pressure soresTwo small, poor-quality studies were identified.These provided no clear evidence of a benefit ofelectromagnetic therapy in the treatment ofpressure sores.
Conclusions
Implications for clinical practiceThere is generally insufficient evidence to statewhether the use of any of the therapies identifiedfor this review are beneficial or not in thetreatment of any of the chronic wounds studied.
Recommendations for researchThis review found that for two of the interventionsthere is a suggestion of benefit. These therapiesshould have research priority:
• therapeutic ultrasound for venous leg ulcers• electrotherapy for chronic wounds including
pressure sores.
Within all studies examining the effectiveness ofthe therapies outlined in this review, researchmethodology could be significantly improved, andcommissioning groups may wish to consider thefollowing aspects for future research:
• The number of patients in a trial should bebased on an a priori sample-size calculation.
• A truly objective outcome measure should beused, or wound healing should be expressed asboth percentage and absolute change in area.
• For each patient a single reference woundshould be selected.
• Experimental groups should be comparable atbaseline.
• Wherever possible, each therapy should becompared with sham therapy.
• A complete and thorough description of concur-rent treatments, including secondary dressings,should be given in trial reports.
• Assessment of outcomes should ideally be blindto treatment or be completely objective.
• Survival-rate analysis should be adopted in allstudies that assess wound healing.
• Future trials should include cost-effectivenessand quality-of-life assessments, as well asobjective measures of the effectiveness ofphysical therapies.
• Economic evaluations should be incorporated intrials that are sufficiently large in order to detectappropriate economic and clinical outcomes.
• In order to prevent publication bias and ensurethe inclusion of unpublished trials in systematicreviews, those involved in primary researchshould make their data available to those under-taking systematic reviews.
Executive summary
144
This report is one of a series of systematicreviews aimed at identifying effective interven-
tions for the prevention and treatment of chronicwounds. This report focuses specifically on theeffectiveness of the following therapies for thetreatment of chronic wounds:
• low-level laser therapy• therapeutic ultrasound• electrotherapy• electromagnetic therapy.
The following were selected for this review as theyare the most common chronic wounds encoun-tered in clinical practice:
• venous leg ulcers• pressure sores• diabetic ulcers• ischaemic ulcers.
The interventions for the review were selectedthrough consultation with the advisory panel (seeappendix 2), the National Coordinating Centre forHealth Technology Assessment, and on the basis ofcurrent practice, clinical variation and uncertainty.
Types of wound
Venous leg ulcersThe prevalence of active leg ulceration in the UKhas been estimated at 1.5 in 1000,1,2 and a similarrate has been reported in Australia.3 Prevalenceincreases with age, and is higher among women.Leg ulceration is typically a chronic recurringcondition, with 45% of patients in a Scottish studyreporting episodes of ulceration for more than10 years.4 There is a considerable cost both to thepatient5 and to the health service.6 Most leg ulcersare associated with venous disease, and a historyof a deep vein thrombosis is widely regarded as apredisposing factor to venous insufficiency andhence to venous ulceration. However, the aetiologyof leg ulceration remains poorly understood.Venous insufficiency has been shown to be associ-ated with increased hydrostatic pressure in theveins of the leg, and it is in an attempt to reversethis and aid venous return that external
compression in various forms is applied as atherapy for venous leg ulcers.7 However, whilecompression therapy is the mainstay of venousulcer therapy, various other interventions,including dressings, are used as an adjunct tocompression or in the absence of compressionwhere compression is contraindicated (e.g. in thepresence of arterial disease).
Pressure soresPressure sores (also known as bed sores, decubitusulcers and pressure ulcers) are areas of localiseddamage to the skin and underlying tissue caused bypressure, shear or friction. They usually occur overbony prominences such as the sacrum, heels, hipsand elbows, and most often in immobile elderlypeople (e.g. elderly orthopaedic patients), patientswith severe acute illnesses (e.g. patients in intensivecare units) and in people with neurologicalproblems (e.g. people with spinal cord injuries).
Pressure sores have been recorded as occurring in4–10% of patients admitted to a UK district generalhospital (the precise rate depends on the case mix)and in an unknown proportion of patients in thecommunity. These sores represent a major burdenof sickness and reduced quality of life for patientsand their carers, and are costly to health serviceproviders.
Pressure sores present as a continuum of tissuedamage, from unbroken skin with sustained rednessafter the release of pressure (non-blanchingerythema) to the destruction of muscle and bone.
The treatment of pressure sores covers four mainstrategies:
• local treatment of the wound using dressingsand other topical applications
• pressure relief, using beds, mattresses orcushions, or by repositioning the patient
• treating concurrent conditions that may delayhealing (e.g. poor nutrition, infection)
• the use of physical therapies, such as electricalstimulation, ultrasound and laser therapy.
In a Dutch Consensus Report (1985),64 ultrasoundwas described as “potentially useful in individualcases of Grade IIIa pressure sore”, although a
Health Technology Assessment 2001; Vol. 5: No. 9
145
Chapter 1
Introduction

survey in The Netherlands found that only approxi-mately 25% of nursing-home doctors and nursesregarded ultrasound as “effective or very effective”for treating pressure sores.8
Diabetic ulcersFoot ulceration in diabetes (type 1, formerly calledinsulin-dependent diabetes mellitus; and type 2,formerly called non-insulin-dependent diabetesmellitus) is a major contribution to the morbidityand mortality of the disease, and is thought toaffect 15% of all people with diabetes at some timeduring their life.9 There is some uncertainty as tothe true incidence and prevalence, as much of thetreatment is delivered in the community andoutpatient departments, where data collection ispatchy and surveillance limited. The cost to theNHS is thought to be about £12.9 million peryear.10 In the USA, diabetic foot ulcerationaccounts for $350 million of hospital costs and50% of non-traumatic lower-limb amputations.
Population-based studies have identified trendsin hospital admissions, the incidence of footulceration and the risk factors for diabetic footulceration. Other studies have identified that thereis a positive correlation between diabetic foot ulcer-ation and the rate of non-traumatic amputation.11
Aetiology of foot ulceration in diabetesThe pathway to foot ulceration in diabetes involves acomplex combination of peripheral vascular disease(reduced blood supply) and peripheral neuropathy(reduced sensation and/or change in lower-limbmovement). Decreased pain sensation and muscularspatial awareness (proprioception) due to neurop-athy lead to abnormal loading of the foot, and thisin turn leads to areas of increased pressure on theplantar (base) aspects of the foot (e.g. metatarsalheads, base of the toes). These increased footpressures lead to the formation of thick, hard skin(callus) that can then lead to further increased footpressure in the affected areas. If left untreated, thiscan lead to tissue damage.
Ischaemic ulcersLeg ulceration affects around 1% of the populationin industrialised countries. The major causes ofulceration include venous insufficiency, diabetesand arterial disease. Although the majority of legulcers are due to venous disease, a significantnumber (around 25%) of patients have arterialinsufficiency.12,13
Arterial (ischaemic) leg ulcers are due toinadequate blood supply to the skin. This may be
caused by an embolism blocking the arteryor to a narrowing of the arteries to the legs(atherosclerosis).
It is essential to differentiate between arterial andvenous ulcers, as the compression therapy recom-mended for venous ulcers14 may lead to skinnecrosis, and potentially to amputation, if appliedto an arterial leg ulcer.15
The key to treatment is improvement in the bloodsupply, and therefore surgery is often required inorder to bypass or clear the blockage or narrowingin the arteries. In a number of patients surgery maynot be possible due to:
• patient preference• patient age and general health• diffuse, distal arterial disease where the vessels
to be reconstructed are very small.
In this instance the role of other therapies(e.g. laser therapy, therapeutic ultrasound,electrotherapy, electromagnetic therapy)which are used in place of surgery needs to beevaluated.
For all the chronic wound types discussed hereinthere is general professional uncertainty as toeffective forms of treatment, thus warranting asystematic review.
The role of physical therapies inwound healing
Low-level laser therapyResearch into the role of low-level laser therapybegan in the late 1960s, in Eastern Europe.16
The research into low-level laser therapy hasconcentrated on three areas: cellular function,animal studies and human trials.17 Much of theresearch undertaken in humans has concentratedon soft-tissue wound healing. Lasers work at alocal cellular and humoral level on variousbiological systems. Increased numbers offibroblasts, mast cells and degranulation havebeen observed, together with increased activityof succinic acid dehydrogenase in the tissuessurrounding the wound rim. Local prostaglandinchanges and increased epithelial activity havealso been noted.18 It is hypothesised that byexposing impaired cells to the photon energyproduced by low-level laser therapy, repairmay be enhanced via proliferation or cellularmigration.19
Introduction
146

There are a number of different types of laser usedfor medical purposes, including crystalline lasermedium, semiconductor lasers, liquid lasers andgas lasers. For wound healing, gas lasers such ashelium–neon (HeNe) and gallium arsenide (GaAs)are used for biostimulation and are the main typesof laser on the market. The HeNe laser was the firstlaser available and is reported to have beneficialeffects in both wound healing and dentistry. TheHeNe laser has the advantage that it emits redlight, which is visible and therefore the blink reflexprotects the eyes from it. The GaAs laser has mostcommonly been used for the treatment of pain andinflammation, and is less suited to wound healing,as it has the deepest tissue penetration of thecommon therapeutic lasers. Lower doses are usedthan with the HeNe laser. The GaAs laser has thedisadvantage that its light is invisible, and thereforeeye protection is required.20
Laser therapy is widely used as a treatment forchronic wounds21 and is often applied by health-care professionals. However, its role in promotingulcer healing as an adjunct to, or in the absenceof, other proven therapies such as compressionremains unclear.
Therapeutic ultrasoundThe mechanisms by which ultrasound is thoughtto affect wound healing have been reviewed.22,23
Briefly, the cellular effects of ultrasound can bedivided into thermal and non-thermal.22 The lowerintensities of ultrasound used therapeutically meanthat any beneficial effects are likely to be due tonon-thermal mechanisms.23 Non-thermal effectsinclude the production of standing waves, acousticstreaming, microstreaming and cavitation. Someof these effects may be beneficial, while others areharmful; standing waves may cause the arrest ofblood flow, while cavitation may cause bubbleformation within the bloodstream.22 Careful choiceof exposure time and intensity and continuousmovement of the ultrasound applicator aims tominimise these effects.
In a number of trials, therapeutic ultrasound hasbeen delivered using different pulse widths, poweroutput from the probe and frequencies.
ElectrotherapyElectrical stimulation has been used for decadesas a treatment for chronic wounds24 and is oftenapplied by healthcare professionals. However, itsrole in promoting ulcer healing as an adjunct to,or in the absence of, other proven therapies suchas compression remains unclear.
Research into the role of electricity in woundhealing has been undertaken since at least the1940s.25 Experimental animal studies have shownthat electrical potentials over the wound duringhealing are initially positive, becoming negativeafter the fourth day of healing.26 It has beenconcluded that the proliferative phase of healingis related to a negative electrical potential overthe wound. However, some studies have experi-mented with positive wound electrodes, and otherswith alternating or reversing the polarity of theelectrode during healing. It is hypothesised thatelectrical stimulation influences the migratory,proliferative and synthetic functions of fibroblasts,and also results in increased expression of growthfactors.26 It seems likely that a moist wound envi-ronment is essential to maintain endogenous orapplied current flow.
Electromagnetic therapyElectromagnetic therapy is distinct from mostother forms of electrotherapy in that it is a fieldeffect and not a direct electrical effect or aform of radiation. It is often termed pulsedelectromagnetic field (PEMF) to distinguish itfrom short-wave diathermy, which uses eithercapacitance or induction to produce indirectheating of tissues and can be thought of as a fieldeffect.27
Aims and objectives
AimThe aim was to undertake a systematic review ofthe evidence of the effectiveness of low-level lasertherapy; therapeutic ultrasound, electrotherapyand electromagnetic therapy in the treatmentof chronic wounds. This series of reviews hasregarded leg and foot ulcers, pressure sores, cavitywounds and surgical wounds healing by secondaryintention as chronic wounds.
ObjectivesThis review sought to answer the following generalquestions:
• Do low-level laser therapy, therapeutic ultra-sound, electrotherapy and electromagnetictherapy increase the healing of chronic wounds?
• If yes, what is the optimum treatment regimenwith each therapy?
More specifically, for each therapy this reviewsought to answer the following questions:
Health Technology Assessment 2001; Vol. 5: No. 9
147

Laser therapy• Does low-level laser therapy stimulate chronic
wound healing?
• If yes, what is the optimum treatment regimen,in terms of source, energy and power?
Therapeutic ultrasound• Does therapeutic ultrasound stimulate chronic
wound healing?
• If yes, what is the optimum treatment regimen,in terms of duration, pulses, power output fromthe probe, ultrasound frequency, and the lengthand frequency of treatment?
Electrotherapy• Does electrotherapy stimulate chronic wound
healing?
• If yes, what is the optimum treatment regimen,in terms of polarity, waveform, current density,and the duration and frequency of treatments?
Electromagnetic therapy• Does electromagnetic therapy stimulate chronic
wound healing?
• If yes, what is the optimum treatment regimen,in terms of polarity, waveform, current density,and the duration and frequency of treatments?
Introduction
148
Search strategy
The search strategy is presented in detail inappendix 1. Briefly, 19 electronic databases,including MEDLINE, EMBASE, CINAHL and thespecialised trials register of the Cochrane WoundsGroup, and wound care journals were searched forthe period up to December 1999. Organisations,manufacturers, researchers and healthcare profes-sionals concerned with wound care were contactedfor additional trials. The reference sections of theobtained studies were also searched for furthertrials.
Inclusion criteria
Types of studiesProspective randomised controlled trials (RCTs)comparing the therapies outlined below wereeligible for inclusion. The size (and hence power)of a study was not an inclusion criterion becausesample size itself is not a measure of quality orvalidity. Leaving the review open to small studiesleaves the possibility of pooling similar smallstudies to increase precision.
Low-level laser therapy• Low-level laser therapy versus sham or no laser
therapy
• head-to-head comparisons of different regimensof laser therapy (e.g. variations in source, energypower, frequency).
Therapeutic ultrasound• Therapeutic ultrasound versus sham ultrasound
or no ultrasound
• different regimens of ultrasound stimulation(e.g. variations in duration of pulses, poweroutput, frequency).
Electrotherapy• Electrical stimulation versus sham or no
stimulation
• different regimens of electrical stimulation (e.g.variations in current, waveform, frequency).
Electromagnetic therapy• Electromagnetic stimulation versus sham or no
electromagnetic therapy
• different regimens of electromagnetic stimula-tion (e.g. variations in current, waveform,frequency).
Types of participantsPatients of any age and in any care setting anddescribed as having a chronic wound were included.As the means of diagnosis of venous ulceration candiffer between trials and is usually not described, itwas not possible to apply a standard definition.
Types of outcome measureThe primary outcome was regarded as woundhealing. Some measures of wound healing aresubjective (e.g. whether a wound is ‘improved’);we only included studies which incorporatedobjective measures of healing, such as the rate ofchange in ulcer area, time to complete healingand/or the proportion of ulcers healed within thetrial period.
Financial costs, quality of life, adverse effects andpain were regarded as secondary outcome measures,and these data were extracted if presented.
All studiesTitles and abstracts of studies identified from eachsearch were assessed against the criteria by onereviewer (KAF) for their relevance and design.Full versions of articles were obtained if from thisinitial assessment it was deemed possible that theinclusion criteria were satisfied. Rejected articleswere checked by another reviewer (NC).
The full text of papers was checked for eligibility(by KAF). This was repeated independently byanother reviewer (NC) in order to provide verifica-tion. Any disagreement was resolved by discussion.
Data extraction
Details of the studies were extracted and summa-rised using a data extraction sheet. If data weremissing from reports, attempts were made to
Health Technology Assessment 2001; Vol. 5: No. 9
149
Chapter 2
Methods
contact the authors to obtain missing information.Studies published in duplicate were included onlyonce. Data extraction was undertaken by onereviewer (KAF) and checked for accuracy by asecond (NC). Data were extracted from each studyon the following criteria (appendix 3):
• inclusion and exclusion criteria• method of randomisation• setting• treatment and control group interventions• baseline characteristics of patients (by treatment
group)• extent and duration of follow-up• results.
Methodological quality
Each study was appraised using a standard checklistto assess the validity of the methods used. Datawere extracted on the following aspects of quality:
• use of clear inclusion and exclusion criteria• adequacy of allocation concealment• baseline comparability of treatment groups for
important variables (e.g. wound size)
• use of intention-to-treat analysis• extent of loss to follow-up• use of blinded outcome assessment.
Retrieved trials that did not meet the inclusioncriteria are given in Table 1.
Data synthesis
The method used to synthesise the studiesdepended on the quality, design and heterogeneityof the studies identified. Clinical heterogeneity wasexplored by examining influential factors, such asthe parameters of the physical therapy used, thecare setting and co-interventions (e.g. compressiontherapy). Statistical heterogeneity was tested bymeans of a c2 test. For each trial, the relative riskand the 95% confidence intervals (CI) were calcu-lated for all important, dichotomous outcomes(e.g. the number of patients developing newpressure sores). Relative risk (RR) is presentedin preference to odds ratios as the latter give aninflated impression of the size of effect where eventrates are high, as was the case in these trials.28
Where synthesis was inappropriate, a narrativeoverview was undertaken.
Methods
150
Study Comparison Reason for exclusion
Goldin et al., 198129 Electrotherapy versus sham electrotherapy Not chronic wounds
Jivegard et al., 199530 Electrotherapy versus standard care Not a wound healing study
Katelaris et al., 198731 Electrotherapy Not an RCT
Muirhead et al., 199132 Electromagnetic therapy versus standard care Not chronic wounds
Santoianni et al., 198433 HeNe laser versus standard care Patients acted as their own internal control
TABLE 1 Summary of studies excluded from the review
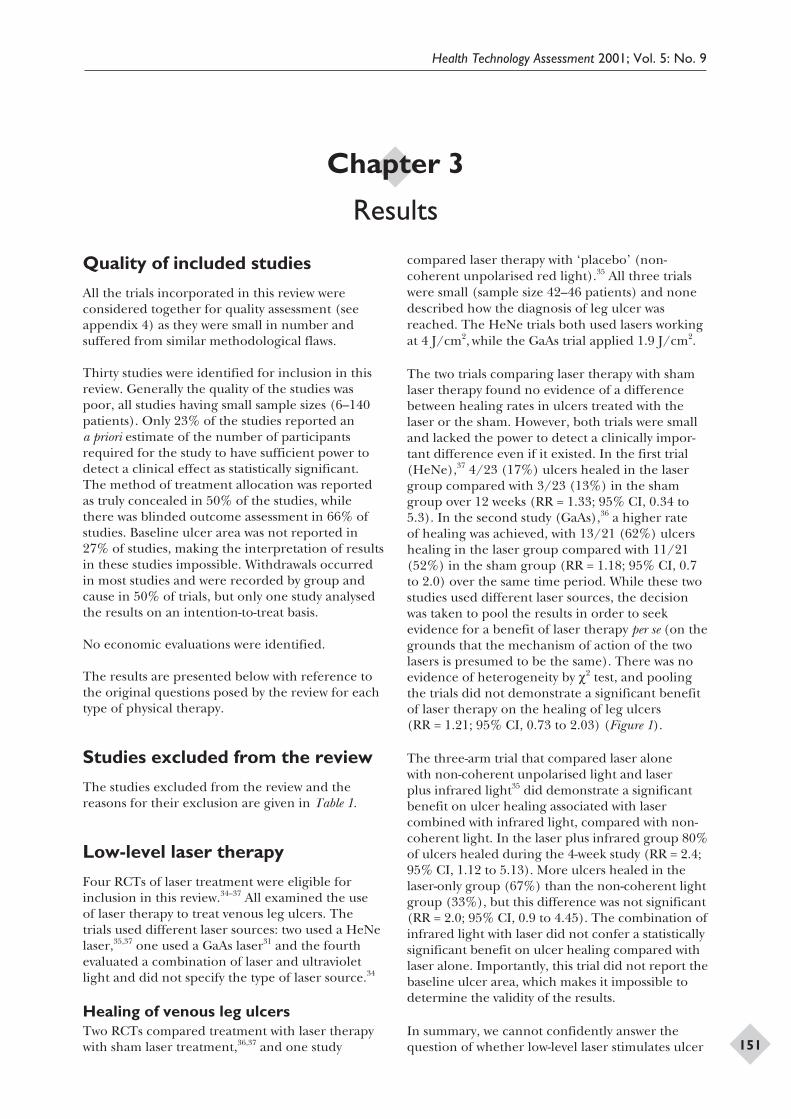
Quality of included studies
All the trials incorporated in this review wereconsidered together for quality assessment (seeappendix 4) as they were small in number andsuffered from similar methodological flaws.
Thirty studies were identified for inclusion in thisreview. Generally the quality of the studies waspoor, all studies having small sample sizes (6–140patients). Only 23% of the studies reported ana priori estimate of the number of participantsrequired for the study to have sufficient power todetect a clinical effect as statistically significant.The method of treatment allocation was reportedas truly concealed in 50% of the studies, whilethere was blinded outcome assessment in 66% ofstudies. Baseline ulcer area was not reported in27% of studies, making the interpretation of resultsin these studies impossible. Withdrawals occurredin most studies and were recorded by group andcause in 50% of trials, but only one study analysedthe results on an intention-to-treat basis.
No economic evaluations were identified.
The results are presented below with reference tothe original questions posed by the review for eachtype of physical therapy.
Studies excluded from the review
The studies excluded from the review and thereasons for their exclusion are given in Table 1.
Low-level laser therapy
Four RCTs of laser treatment were eligible forinclusion in this review.34–37 All examined the useof laser therapy to treat venous leg ulcers. Thetrials used different laser sources: two used a HeNelaser,35,37 one used a GaAs laser31 and the fourthevaluated a combination of laser and ultravioletlight and did not specify the type of laser source.34
Healing of venous leg ulcersTwo RCTs compared treatment with laser therapywith sham laser treatment,36,37 and one study
compared laser therapy with ‘placebo’ (non-coherent unpolarised red light).35 All three trialswere small (sample size 42–46 patients) and nonedescribed how the diagnosis of leg ulcer wasreached. The HeNe trials both used lasers workingat 4 J/cm2, while the GaAs trial applied 1.9 J/cm2.
The two trials comparing laser therapy with shamlaser therapy found no evidence of a differencebetween healing rates in ulcers treated with thelaser or the sham. However, both trials were smalland lacked the power to detect a clinically impor-tant difference even if it existed. In the first trial(HeNe),37 4/23 (17%) ulcers healed in the lasergroup compared with 3/23 (13%) in the shamgroup over 12 weeks (RR = 1.33; 95% CI, 0.34 to5.3). In the second study (GaAs),36 a higher rateof healing was achieved, with 13/21 (62%) ulcershealing in the laser group compared with 11/21(52%) in the sham group (RR = 1.18; 95% CI, 0.7to 2.0) over the same time period. While these twostudies used different laser sources, the decisionwas taken to pool the results in order to seekevidence for a benefit of laser therapy per se (on thegrounds that the mechanism of action of the twolasers is presumed to be the same). There was noevidence of heterogeneity by c2 test, and poolingthe trials did not demonstrate a significant benefitof laser therapy on the healing of leg ulcers(RR = 1.21; 95% CI, 0.73 to 2.03) (Figure 1).
The three-arm trial that compared laser alonewith non-coherent unpolarised light and laserplus infrared light35 did demonstrate a significantbenefit on ulcer healing associated with lasercombined with infrared light, compared with non-coherent light. In the laser plus infrared group 80%of ulcers healed during the 4-week study (RR = 2.4;95% CI, 1.12 to 5.13). More ulcers healed in thelaser-only group (67%) than the non-coherent lightgroup (33%), but this difference was not significant(RR = 2.0; 95% CI, 0.9 to 4.45). The combination ofinfrared light with laser did not confer a statisticallysignificant benefit on ulcer healing compared withlaser alone. Importantly, this trial did not report thebaseline ulcer area, which makes it impossible todetermine the validity of the results.
In summary, we cannot confidently answer thequestion of whether low-level laser stimulates ulcer
Health Technology Assessment 2001; Vol. 5: No. 9
151
Chapter 3
Results
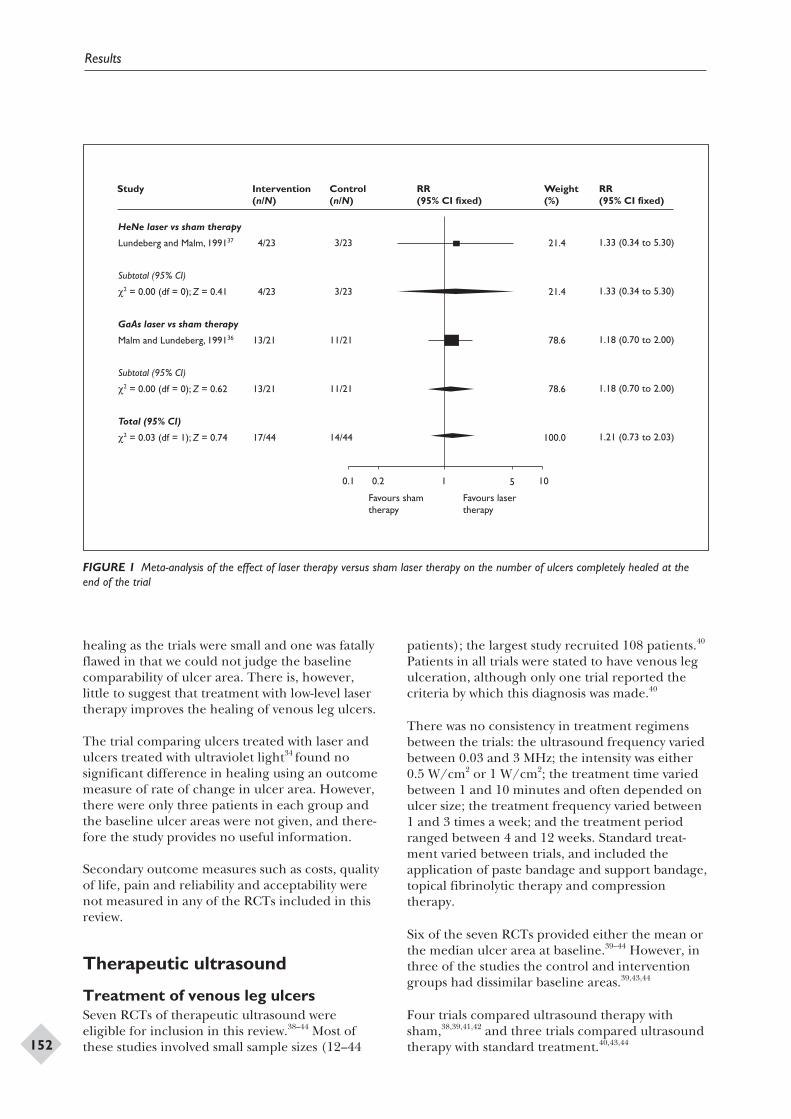
healing as the trials were small and one was fatallyflawed in that we could not judge the baselinecomparability of ulcer area. There is, however,little to suggest that treatment with low-level lasertherapy improves the healing of venous leg ulcers.
The trial comparing ulcers treated with laser andulcers treated with ultraviolet light34 found nosignificant difference in healing using an outcomemeasure of rate of change in ulcer area. However,there were only three patients in each group andthe baseline ulcer areas were not given, and there-fore the study provides no useful information.
Secondary outcome measures such as costs, qualityof life, pain and reliability and acceptability werenot measured in any of the RCTs included in thisreview.
Therapeutic ultrasound
Treatment of venous leg ulcersSeven RCTs of therapeutic ultrasound wereeligible for inclusion in this review.38–44 Most ofthese studies involved small sample sizes (12–44
patients); the largest study recruited 108 patients.40
Patients in all trials were stated to have venous legulceration, although only one trial reported thecriteria by which this diagnosis was made.40
There was no consistency in treatment regimensbetween the trials: the ultrasound frequency variedbetween 0.03 and 3 MHz; the intensity was either0.5 W/cm2 or 1 W/cm2; the treatment time variedbetween 1 and 10 minutes and often depended onulcer size; the treatment frequency varied between1 and 3 times a week; and the treatment periodranged between 4 and 12 weeks. Standard treat-ment varied between trials, and included theapplication of paste bandage and support bandage,topical fibrinolytic therapy and compressiontherapy.
Six of the seven RCTs provided either the mean orthe median ulcer area at baseline.39–44 However, inthree of the studies the control and interventiongroups had dissimilar baseline areas.39,43,44
Four trials compared ultrasound therapy withsham,38,39,41,42 and three trials compared ultrasoundtherapy with standard treatment.40,43,44
Results
152
Study Intervention (n/N)
Control (n/N)
RR (95% CI fixed)
Weight (%)
RR (95% CI fixed)
HeNe laser vs sham therapy
Lundeberg and Malm, 199137
Subtotal (95% CI)
c2 = 0.00 (df = 0); Z = 0.41
GaAs laser vs sham therapy
Malm and Lundeberg, 199136
Subtotal (95% CI)
c2 = 0.00 (df = 0); Z = 0.62
Total (95% CI)
c2 = 0.03 (df = 1); Z = 0.74
4/23
4/23
13/21
13/21
17/44
3/23
3/23
11/21
11/21
14/44
21.4
21.4
78.6
78.6
100.0
1.33 (0.34 to 5.30)
1.33 (0.34 to 5.30)
1.18 (0.70 to 2.00)
1.18 (0.70 to 2.00)
1.21 (0.73 to 2.03)
0.1 0.2 1 5 10
Favours sham therapy
Favours laser therapy
FIGURE 1 Meta-analysis of the effect of laser therapy versus sham laser therapy on the number of ulcers completely healed at theend of the trial

Healing of venous leg ulcersThe first study42 compared active and shamultrasound over an 8-week period. There wasno difference in baseline ulcer size between thetreatment and control groups. Six of 19 ulcers(32%) healed in the intervention group, comparedwith 4/19 (21%) ulcers in the control group(RR = 1.5; 95% CI, 0.5 to 4.48); this difference isnot statistically significant.
In a study of slightly longer duration41 it wasreported that 10/22 (45%) ulcers healed over12 weeks in the ultrasound group compared with8/22 (36%) ulcers in the sham group (RR = 1.25;95% CI, 0.61 to 2.56).
A further study39 compared ultrasound with shamover an 8-week period using the percentage changein ulcer area as the outcome measure. However,the ulcers were larger at baseline in the ultrasoundgroup, which for this outcome favours small ulcers(the sham group). Ulcers in the ultrasound groupshowed a mean decrease in ulcer area of 35.3%(standard deviation (SD) = 30.06) compared with7.0% (SD = 36.7) in the sham group. The outcomemeasure used is against the direction of bias, andtherefore the results are more convincing.
The fourth trial38 compared ultrasound with shamover 4 weeks. However, it failed to report baselineulcer area and involved only 25 patients. There-fore, imbalance between groups at baseline ishighly likely. Outcomes were reported as the meanpercentage of initial ulcer area: 66.4 ± 8.8% forulcers treated with ultrasound compared with91.6 ± 8.9% for ulcers treated with sham. Whilethis difference is reported as statistically significant(p < 0.05), the result cannot be interpreted due tothe lack of information about baseline ulcer area.
Three trials compared ultrasound therapy withstandard treatment.40,43,44 The largest trial40
reported good comparability between groups forbaseline ulcer area, but only 76% follow-up wasachieved. In this trial 25/41 (61%) ulcers healedin the ultrasound group at 12 weeks compared with17/41 (41%) in the standard treatment group(RR = 1.47; 95% CI, 0.95 to 2.28).
Ultrasound was compared with standard therapyin a trial of only 12 patients.43 Ulcers were largerat baseline in the control group, which for anoutcome of percentage decrease in ulcer areabiases the study in favour of the small ulcers (i.e.the ultrasound group). The mean percentagedecrease in ulcer area was 55% at 12 weeks in the
ultrasound group compared with 16% in thestandard therapy group (p < 0.007). While thedifference is significant it cannot be interpreteddue to the biased distribution of baseline ulcerarea.
The final study44 compared ultrasound withstandard therapy in 37 patients. The meanpercentage change in initial ulcer area at the endof the study was 41.5% in the ultrasound groupand 9.5% in the standard therapy group. However,the baseline ulcer area was larger in the standardtherapy group, and therefore the outcomemeasure favours the ultrasound group, which hadsmaller ulcers. One ulcer completely healed in theultrasound group compared to none in the controlgroup.
The four studies40–42,44 which measured similaroutcomes (i.e. the number of ulcers healed at theend of the trial) were tested for heterogeneity, andthis was non-significant (c2 = 0.34). The notabledifference between these trials lies in the dissimilarcomparison groups: sham ultrasound41,42 andstandard therapy.40,44 Despite this, we pooled theresults of these four trials (fixed-effects model)while acknowledging that the trials without a shamgroup may exaggerate any perceived treatmenteffect. This resulted in a borderline statisticallysignificant result in favour of ultrasound (RR =1.44; 95% CI, 1.01 to 2.05) (Figure 2). The differ-ence in the pooled result remained significantwhen a random-effects model was applied (therandom-effects model includes both within- andbetween-studies variation in the assessment of theuncertainty of the meta-analysis and is thereforemore conservative). If one study44 (which wasbiased in favour of ultrasound, and in which onlyone patient healed) is removed from the analysisthe difference is no longer significant (RR = 1.41;95% CI, 0.99 to 2.02) (fixed-effects model).
The remaining three studies used continuousoutcome measures and could not be includedin the meta-analysis. The direction of effect wasconsistently in favour of ultrasound in these trials.However, none reached statistical significance.
Secondary outcome measures such as costs, qualityof life, pain, and reliability and acceptability werenot measured in any of the RCTs included in thisreview.
There is insufficient evidence about the effect oftherapeutic ultrasound on venous leg ulcers since,despite the existence of seven RCTs (274 patientsin total), the results of each of which tended to
Health Technology Assessment 2001; Vol. 5: No. 9
153
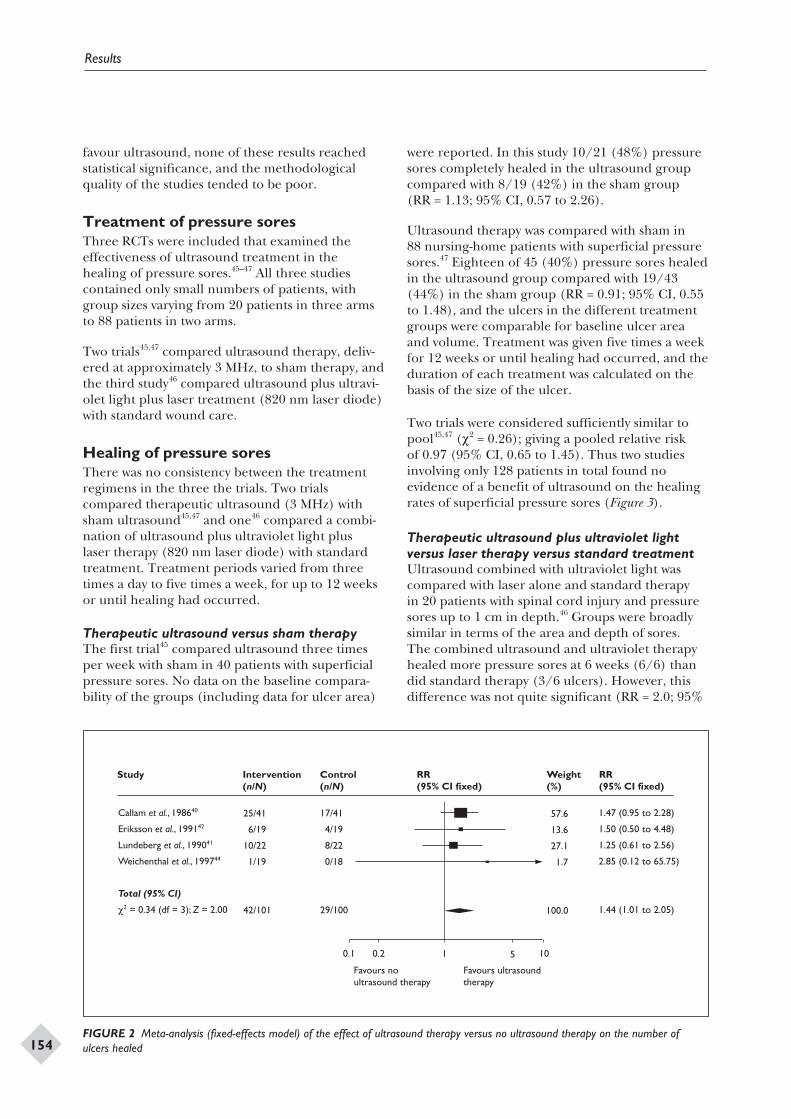
favour ultrasound, none of these results reachedstatistical significance, and the methodologicalquality of the studies tended to be poor.
Treatment of pressure soresThree RCTs were included that examined theeffectiveness of ultrasound treatment in thehealing of pressure sores.45–47 All three studiescontained only small numbers of patients, withgroup sizes varying from 20 patients in three armsto 88 patients in two arms.
Two trials45,47 compared ultrasound therapy, deliv-ered at approximately 3 MHz, to sham therapy, andthe third study46 compared ultrasound plus ultravi-olet light plus laser treatment (820 nm laser diode)with standard wound care.
Healing of pressure soresThere was no consistency between the treatmentregimens in the three the trials. Two trialscompared therapeutic ultrasound (3 MHz) withsham ultrasound45,47 and one46 compared a combi-nation of ultrasound plus ultraviolet light pluslaser therapy (820 nm laser diode) with standardtreatment. Treatment periods varied from threetimes a day to five times a week, for up to 12 weeksor until healing had occurred.
Therapeutic ultrasound versus sham therapyThe first trial45 compared ultrasound three timesper week with sham in 40 patients with superficialpressure sores. No data on the baseline compara-bility of the groups (including data for ulcer area)
were reported. In this study 10/21 (48%) pressuresores completely healed in the ultrasound groupcompared with 8/19 (42%) in the sham group(RR = 1.13; 95% CI, 0.57 to 2.26).
Ultrasound therapy was compared with sham in88 nursing-home patients with superficial pressuresores.47 Eighteen of 45 (40%) pressure sores healedin the ultrasound group compared with 19/43(44%) in the sham group (RR = 0.91; 95% CI, 0.55to 1.48), and the ulcers in the different treatmentgroups were comparable for baseline ulcer areaand volume. Treatment was given five times a weekfor 12 weeks or until healing had occurred, and theduration of each treatment was calculated on thebasis of the size of the ulcer.
Two trials were considered sufficiently similar topool45,47 (c2 = 0.26); giving a pooled relative riskof 0.97 (95% CI, 0.65 to 1.45). Thus two studiesinvolving only 128 patients in total found noevidence of a benefit of ultrasound on the healingrates of superficial pressure sores (Figure 3).
Therapeutic ultrasound plus ultraviolet lightversus laser therapy versus standard treatmentUltrasound combined with ultraviolet light wascompared with laser alone and standard therapyin 20 patients with spinal cord injury and pressuresores up to 1 cm in depth.46 Groups were broadlysimilar in terms of the area and depth of sores.The combined ultrasound and ultraviolet therapyhealed more pressure sores at 6 weeks (6/6) thandid standard therapy (3/6 ulcers). However, thisdifference was not quite significant (RR = 2.0; 95%
Results
154
Study Intervention (n/N)
Control (n/N)
RR (95% CI fixed)
Weight (%)
RR (95% CI fixed)
Callam et al., 198640
Eriksson et al., 199142
Lundeberg et al., 199041
Weichenthal et al., 199744
Total (95% CI)
c2 = 0.34 (df = 3); Z = 2.00
25/41
6/19
10/22
1/19
42/101
17/41
4/19
8/22
0/18
29/100
57.6
13.6
27.1
1.7
100.0
1.47 (0.95 to 2.28)
1.50 (0.50 to 4.48)
1.25 (0.61 to 2.56)
2.85 (0.12 to 65.75)
1.44 (1.01 to 2.05)
0.1 0.2 1 5 10
Favours no ultrasound therapy
Favours ultrasound therapy
FIGURE 2 Meta-analysis (fixed-effects model) of the effect of ultrasound therapy versus no ultrasound therapy on the number ofulcers healed
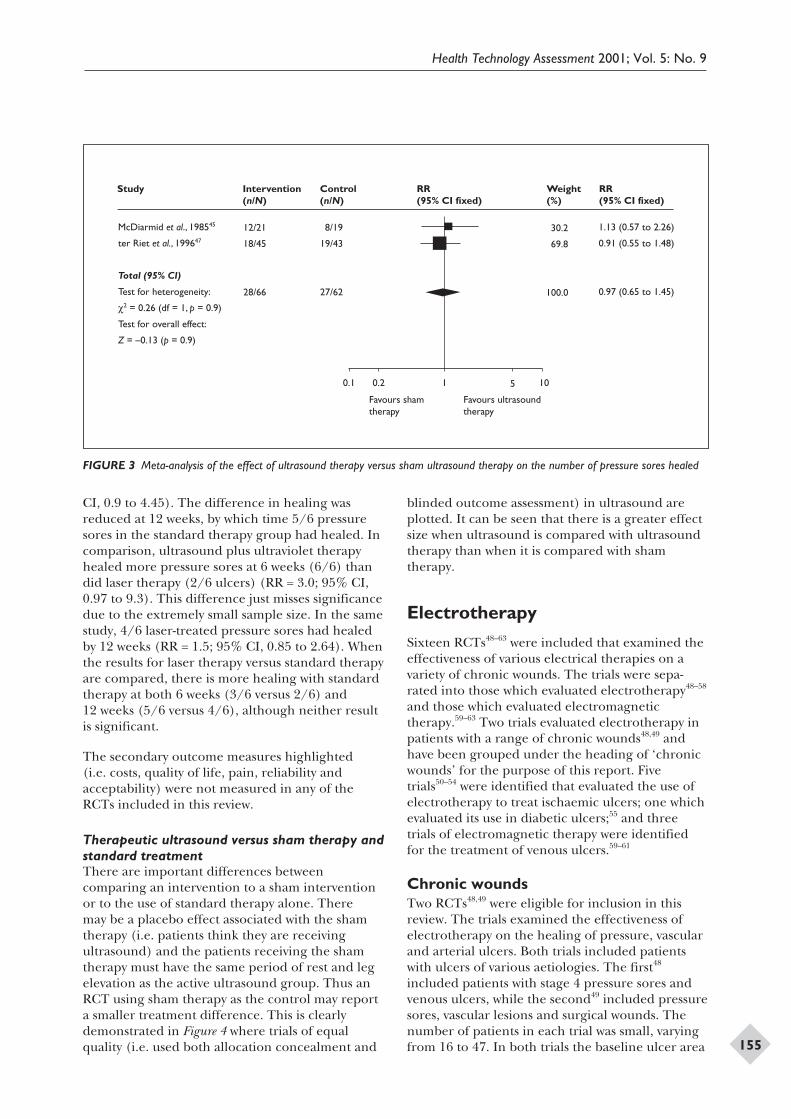
CI, 0.9 to 4.45). The difference in healing wasreduced at 12 weeks, by which time 5/6 pressuresores in the standard therapy group had healed. Incomparison, ultrasound plus ultraviolet therapyhealed more pressure sores at 6 weeks (6/6) thandid laser therapy (2/6 ulcers) (RR = 3.0; 95% CI,0.97 to 9.3). This difference just misses significancedue to the extremely small sample size. In the samestudy, 4/6 laser-treated pressure sores had healedby 12 weeks (RR = 1.5; 95% CI, 0.85 to 2.64). Whenthe results for laser therapy versus standard therapyare compared, there is more healing with standardtherapy at both 6 weeks (3/6 versus 2/6) and12 weeks (5/6 versus 4/6), although neither resultis significant.
The secondary outcome measures highlighted(i.e. costs, quality of life, pain, reliability andacceptability) were not measured in any of theRCTs included in this review.
Therapeutic ultrasound versus sham therapy andstandard treatmentThere are important differences betweencomparing an intervention to a sham interventionor to the use of standard therapy alone. Theremay be a placebo effect associated with the shamtherapy (i.e. patients think they are receivingultrasound) and the patients receiving the shamtherapy must have the same period of rest and legelevation as the active ultrasound group. Thus anRCT using sham therapy as the control may reporta smaller treatment difference. This is clearlydemonstrated in Figure 4 where trials of equalquality (i.e. used both allocation concealment and
blinded outcome assessment) in ultrasound areplotted. It can be seen that there is a greater effectsize when ultrasound is compared with ultrasoundtherapy than when it is compared with shamtherapy.
Electrotherapy
Sixteen RCTs48–63 were included that examined theeffectiveness of various electrical therapies on avariety of chronic wounds. The trials were sepa-rated into those which evaluated electrotherapy48–58
and those which evaluated electromagnetictherapy.59–63 Two trials evaluated electrotherapy inpatients with a range of chronic wounds48,49 andhave been grouped under the heading of ‘chronicwounds’ for the purpose of this report. Fivetrials50–54 were identified that evaluated the use ofelectrotherapy to treat ischaemic ulcers; one whichevaluated its use in diabetic ulcers;55 and threetrials of electromagnetic therapy were identifiedfor the treatment of venous ulcers.59–61
Chronic woundsTwo RCTs48,49 were eligible for inclusion in thisreview. The trials examined the effectiveness ofelectrotherapy on the healing of pressure, vascularand arterial ulcers. Both trials included patientswith ulcers of various aetiologies. The first48
included patients with stage 4 pressure sores andvenous ulcers, while the second49 included pressuresores, vascular lesions and surgical wounds. Thenumber of patients in each trial was small, varyingfrom 16 to 47. In both trials the baseline ulcer area
Health Technology Assessment 2001; Vol. 5: No. 9
155
Study Intervention (n/N)
Control (n/N)
RR (95% CI fixed)
Weight (%)
RR (95% CI fixed)
McDiarmid et al., 198545
ter Riet et al., 199647
Total (95% CI)
Test for heterogeneity:
c2 = 0.26 (df = 1, p = 0.9)
Test for overall effect:
Z = –0.13 (p = 0.9)
12/21
18/45
28/66
8/19
19/43
27/62
30.2
69.8
100.0
1.13 (0.57 to 2.26)
0.91 (0.55 to 1.48)
0.97 (0.65 to 1.45)
0.1 0.2 1 5 10
Favours sham therapy
Favours ultrasound therapy
FIGURE 3 Meta-analysis of the effect of ultrasound therapy versus sham ultrasound therapy on the number of pressure sores healed
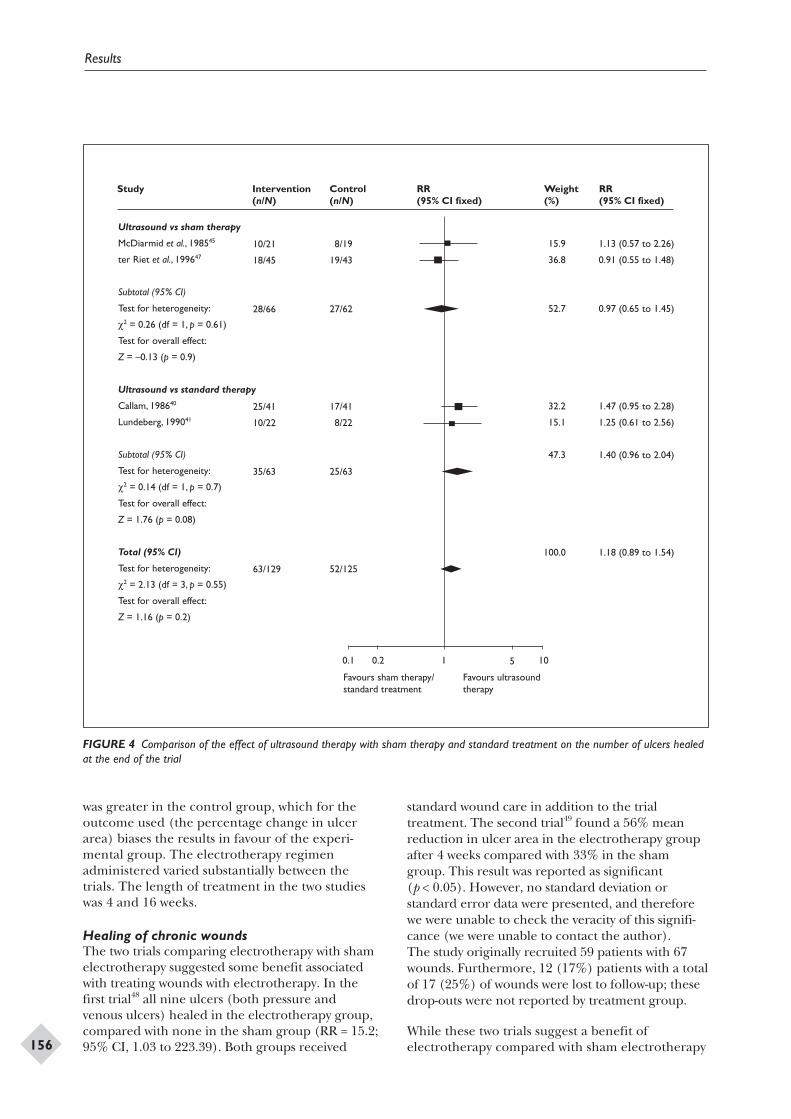
was greater in the control group, which for theoutcome used (the percentage change in ulcerarea) biases the results in favour of the experi-mental group. The electrotherapy regimenadministered varied substantially between thetrials. The length of treatment in the two studieswas 4 and 16 weeks.
Healing of chronic woundsThe two trials comparing electrotherapy with shamelectrotherapy suggested some benefit associatedwith treating wounds with electrotherapy. In thefirst trial48 all nine ulcers (both pressure andvenous ulcers) healed in the electrotherapy group,compared with none in the sham group (RR = 15.2;95% CI, 1.03 to 223.39). Both groups received
standard wound care in addition to the trialtreatment. The second trial49 found a 56% meanreduction in ulcer area in the electrotherapy groupafter 4 weeks compared with 33% in the shamgroup. This result was reported as significant(p < 0.05). However, no standard deviation orstandard error data were presented, and thereforewe were unable to check the veracity of this signifi-cance (we were unable to contact the author).The study originally recruited 59 patients with 67wounds. Furthermore, 12 (17%) patients with a totalof 17 (25%) of wounds were lost to follow-up; thesedrop-outs were not reported by treatment group.
While these two trials suggest a benefit ofelectrotherapy compared with sham electrotherapy
Results
156
Study Intervention (n/N)
Control (n/N)
RR (95% CI fixed)
Weight (%)
RR (95% CI fixed)
Ultrasound vs sham therapy
McDiarmid et al., 198545
ter Riet et al., 199647
Subtotal (95% CI)
Test for heterogeneity:
c2 = 0.26 (df = 1, p = 0.61)
Test for overall effect:
Z = –0.13 (p = 0.9)
Ultrasound vs standard therapy
Callam, 198640
Lundeberg, 199041
Subtotal (95% CI)
Test for heterogeneity:
c2 = 0.14 (df = 1, p = 0.7)
Test for overall effect:
Z = 1.76 (p = 0.08)
Total (95% CI)
Test for heterogeneity:
c2 = 2.13 (df = 3, p = 0.55)
Test for overall effect:
Z = 1.16 (p = 0.2)
10/21
18/45
28/66
25/41
10/22
35/63
63/129
8/19
19/43
27/62
17/41
8/22
25/63
52/125
15.9
36.8
52.7
32.2
15.1
47.3
100.0
1.13 (0.57 to 2.26)
0.91 (0.55 to 1.48)
0.97 (0.65 to 1.45)
1.47 (0.95 to 2.28)
1.25 (0.61 to 2.56)
1.40 (0.96 to 2.04)
1.18 (0.89 to 1.54)
0.1 0.2 1 5 10
Favours sham therapy/standard treatment
Favours ultrasound therapy
FIGURE 4 Comparison of the effect of ultrasound therapy with sham therapy and standard treatment on the number of ulcers healedat the end of the trial

or no electrotherapy in healing chronic ulcers, thetrials were small, were biased for baseline area andlacked the power to detect clinically importantdifferences. Importantly, one study49 incorporatedpatients with multiple wounds, but regarded thewound as the unit of analysis. This approach isflawed because separate wounds on the samepatient cannot be regarded as independent.
It is not possible to identify an optimum protocolfor the use of electrotherapy as there was no consis-tency in the electrotherapy treatment regimensused in the three trials.
Venous leg ulcersNo RCTs of the use of electrotherapy in treatingvenous leg ulcers were identified.
Ischaemic ulcersFive studies examined electrotherapy as atreatment for ischaemic ulcers.50–54 These studieswere published between 1969 and 1997, and thetreatment regimens used varied. Two studies50,51
included patients with two ulcers, randomising oneulcer to the intervention group and one ulcer tothe control group. The other studies randomisedindividuals, not wounds, to the treatment orcontrol groups. Only one study53 reported thebaseline ulcer area. It is also a feature of each ofthese studies that they had small sample sizes,varying from 12 to 66 patients.
Healing of ischaemic ulcersThree trials have compared the use of electro-therapy with various standard therapies50–52 and onehas compared electrotherapy with sham treatment.53
The fifth study54 studied patients with non-reconstructable Fontaine stage 4 ulcers or gangrene.
In the first study comparing electrotherapy withstandard therapies,50 6/8 (75%) ulcers healed inthe electrotherapy group compared with none inthe standard therapy group (RR = 13.0; 95% CI,0.85 to 198.15). In this study both groups receivedstandard therapy of debridement where required,and cleansing with an antibacterial detergent.Details of the baseline ulcer area were not providedby the authors. Each patient had two ulcers andtherefore acted as their own control. It is note-worthy also that the average age of patients in thisstudy was 25.8 years (10–41 years). Most studiesexamining chronic ulceration involve populationsover the age of 60 years.
Patients were also used as their own controls in astudy comparing electrotherapy combined with
standard therapy against standard therapy alone.51
The objective outcome for the study was thepercentage ulcer area healed at 12 weeks in thesix patients recruited to the study. The electro-therapy group had a mean healing of 74%,compared with 27% in the standard therapy group.No variance or baseline ulcer area data werereported, which makes interpretation of the resultsimpossible.
In the most recent study comparing electrotherapyand standard treatment52 no ulcers healed in eithergroup. The results of this study are confoundedby the fact that the 15 patients receiving electro-therapy were also treated with a variety of topicalmeasures. These differed from the those givento the patients in the standard treatment group,although little detail about the standard regimenwas reported. At end of treatment (5 weeks), ulcersin the electrotherapy group had a mean reductionin volume of 4.24 cm3 (SD = 1.32) versus a meanreduction of 1.76 cm3 (SD = 1.14) in the controlgroup (p < 0.01). This difference is in the samedirection as the bias in baseline volume (whereexperimental ulcers were larger), and thereforethe results are impossible to interpret.
The fourth study53 compared electrotherapy withsham electrotherapy in 59 patients with 67 wounds.The primary outcome measure was the percentageof initial wound size at the end of the 4-week studyperiod. The electrotherapy group had 44% ofinitial wound size at the end of the trial, comparedwith 67% of initial wound size in the control group(p < 0.02). However, the smaller mean baselinearea in the intervention group favours the outcomemeasure used (i.e. the percentage reduction inwound size), thus biasing the results. It is alsoworth noting that 20% of the patients recruitedinto the study and 25% of the wounds were lost tofollow-up, although these losses were not reportedby group.
A fifth study54 compared electrotherapy incombination with intravenous prostaglandintherapy to prostaglandin therapy alone in non-reconstructable ulcers classed as Fontaine stage 4.The presence of gangrene for more than 4 weekswas also an inclusion criterion. This study foundthat 31/45 (69%) ulcers healed in the combinedelectrotherapy and prostaglandin group comparedwith 7/41 (17%) of ulcers in the prostaglandingroup (RR = 4.03; 95% CI, 2.00 to 8.15). However,no details of baseline area were reported.
Overall, the results of these trials are difficult tointerpret as those trials of reasonable quality (i.e.
Health Technology Assessment 2001; Vol. 5: No. 9
157
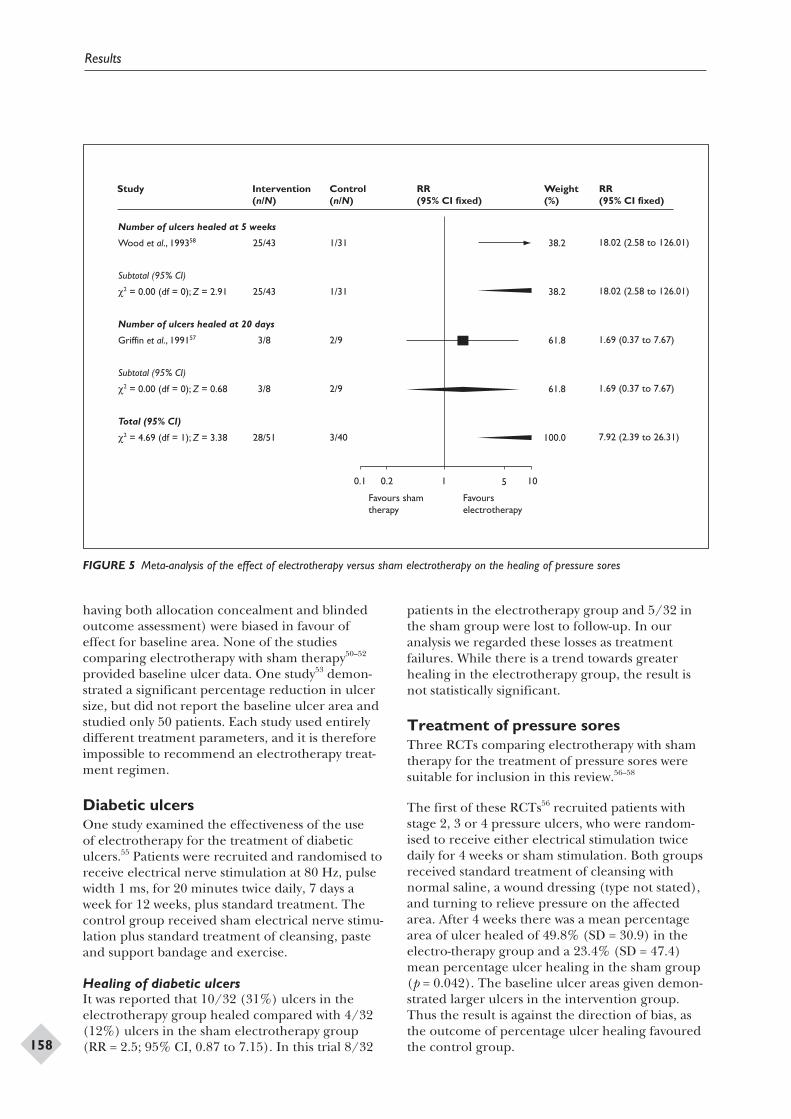
having both allocation concealment and blindedoutcome assessment) were biased in favour ofeffect for baseline area. None of the studiescomparing electrotherapy with sham therapy50–52
provided baseline ulcer data. One study53 demon-strated a significant percentage reduction in ulcersize, but did not report the baseline ulcer area andstudied only 50 patients. Each study used entirelydifferent treatment parameters, and it is thereforeimpossible to recommend an electrotherapy treat-ment regimen.
Diabetic ulcersOne study examined the effectiveness of the useof electrotherapy for the treatment of diabeticulcers.55 Patients were recruited and randomised toreceive electrical nerve stimulation at 80 Hz, pulsewidth 1 ms, for 20 minutes twice daily, 7 days aweek for 12 weeks, plus standard treatment. Thecontrol group received sham electrical nerve stimu-lation plus standard treatment of cleansing, pasteand support bandage and exercise.
Healing of diabetic ulcersIt was reported that 10/32 (31%) ulcers in theelectrotherapy group healed compared with 4/32(12%) ulcers in the sham electrotherapy group(RR = 2.5; 95% CI, 0.87 to 7.15). In this trial 8/32
patients in the electrotherapy group and 5/32 inthe sham group were lost to follow-up. In ouranalysis we regarded these losses as treatmentfailures. While there is a trend towards greaterhealing in the electrotherapy group, the result isnot statistically significant.
Treatment of pressure soresThree RCTs comparing electrotherapy with shamtherapy for the treatment of pressure sores weresuitable for inclusion in this review.56–58
The first of these RCTs56 recruited patients withstage 2, 3 or 4 pressure ulcers, who were random-ised to receive either electrical stimulation twicedaily for 4 weeks or sham stimulation. Both groupsreceived standard treatment of cleansing withnormal saline, a wound dressing (type not stated),and turning to relieve pressure on the affectedarea. After 4 weeks there was a mean percentagearea of ulcer healed of 49.8% (SD = 30.9) in theelectro-therapy group and a 23.4% (SD = 47.4)mean percentage ulcer healing in the sham group(p = 0.042). The baseline ulcer areas given demon-strated larger ulcers in the intervention group.Thus the result is against the direction of bias, asthe outcome of percentage ulcer healing favouredthe control group.
Results
158
Study Intervention (n/N)
Control (n/N)
RR (95% CI fixed)
Weight (%)
RR (95% CI fixed)
Number of ulcers healed at 5 weeks
Wood et al., 199358
Subtotal (95% CI)
c2 = 0.00 (df = 0); Z = 2.91
Number of ulcers healed at 20 days
Griffin et al., 199157
Subtotal (95% CI)
c2 = 0.00 (df = 0); Z = 0.68
Total (95% CI)
c2 = 4.69 (df = 1); Z = 3.38
25/43
25/43
3/8
3/8
28/51
1/31
1/31
2/9
2/9
3/40
38.2
38.2
61.8
61.8
100.0
18.02 (2.58 to 126.01)
18.02 (2.58 to 126.01)
1.69 (0.37 to 7.67)
1.69 (0.37 to 7.67)
7.92 (2.39 to 26.31)
0.1 0.2 1 5 10
Favours sham therapy
Favours electrotherapy
FIGURE 5 Meta-analysis of the effect of electrotherapy versus sham electrotherapy on the healing of pressure sores

The second study57 examined only 17 male patientswith spinal cord injury and a pressure sore. Partici-pants were randomised to receive electrotherapyplus standard treatment or sham therapy plusstandard treatment. The standard treatmentconsisted of wound cleansing and dressing. In thistrial 3/8 (37.5%) ulcers healed in the electro-therapy group compared with 2/9 (22%) in thecontrol group (RR = 1.69; 95% CI, 0.37 to 7.67).
The final study of this type58 compared electro-therapy with sham therapy for the treatment ofchronic pressure ulcers. Both groups receivedstandard treatment of wound cleansing, moistdressing and whirlpool baths. After 8 weeks25/43 (58%) ulcers in the electrotherapy grouphad healed, compared with only 1/31 (3%) inthe sham therapy group (RR = 18.02; 95% CI,2.58–126.01). As the ulcers were larger at baselinein the intervention group, this result is against thedirection of bias.
Two studies50,51 were considered sufficiently similarto pool (c2 = 2.16) and gave a pooled relative riskof 7.91 (95% CI, 3.32 to 18.85) (Figure 5). Thisdemonstrates a statistically significant increase inthe healing of pressure sores treated with electro-therapy compared with sham therapy. However, asthis result is drawn from two small studies with atotal of 91 patients, the results should be inter-preted with caution.
Electromagnetic therapy
Electromagnetic therapy is distinct from otherforms of electrotherapy in that it provides a fieldeffect rather than a direct electrical effect or aform of radiation.
Treatment of venous leg ulcersThree RCTs of electromagnetic therapy for thetreatment of venous leg ulcers were includedin this review.59–61 Each trial contained a smallnumber of patients, varying from 19 patients inthree arms to 44 patients in two arms. Differenttreatment parameters and standard concomitanttherapies were used in each trial, and treatmentwas given over 50–90 days. Each trial provideddetailed baseline data of the ulcers.
Healing of venous leg ulcersTwo trials compared electromagnetic therapywith sham therapy59,60 and one trial61 comparedelectromagnetic therapy with standard topicaltreatments.
The first study59 compared electromagnetic therapywith sham therapy given over a period of 90 days.Twelve of 18 (66%) ulcers healed in the electro-magnetic therapy group compared with 6/19(32%) in the sham therapy group (RR = 2.11; 95%CI, 1.01 to 4.42). If the four (18%) patients fromthe electromagnetic therapy group and three(14%) patients from the sham therapy group whowere lost to follow-up are regarded as treatmentfailures, the difference is not significant (RR = 2.0;95% CI, 0.92 to 4.37). In the second study,60 2/10(20%) venous ulcers healed in the electromagnetictherapy group, compared with 2/9 (22%) in thesham therapy group (RR = 0.9; 95% CI, 0.16 to5.13) after a 50-day period All patients receivedcompression therapy, and had ulcer dressingsapplied by community staff. No drop-outs werereported in this study.
The results of these two studies were pooled usinga fixed-effects model. Overall, more ulcers treatedwith electrotherapy healed than did those treatedwith sham therapy, but this difference was notsignificant (RR = 1.79; 95% CI, 0.91 to 3.51).
In a third study,61 pulsed electromagnetic therapywas compared with standard care. All patientsreceived compression therapy. On average, ulcersin the electrotherapy group had decreased in sizeby 47% at 8 weeks, while in the control groupulcers increased in size by 49% over the same timeperiod (p < 0.0002, analysis of variance). The ulcerswere matched at baseline for size.
Overall, these three small, poor-quality trialsprovide no good evidence of a positive benefit ofelectromagnetic therapy for the healing of venousleg ulcers. Each of the RCTs included in this reviewdelivered electromagnetic therapy using a varietyof electrical and magnetic parameters, overdifferent time periods and with differing treatmentregimens. It is therefore impossible to identify anoptimum regimen from these trials.
Treatment of pressure soresTwo studies of the use of electromagnetic therapyfor the treatment of pressure sores were includedin the review.62,63
The first of these studies62 was a three-arm study,comparing electromagnetic therapy with electro-magnetic therapy in combination with standardtherapy and with standard therapy alone. At theend of the 2-week treatment period 17/20 (85%)ulcers had healed in the electrotherapy groupcompared with no ulcers in either of the other two
Health Technology Assessment 2001; Vol. 5: No. 9
159

groups (n = 5 and 5) (RR = 10; 95% CI, 0.7 to143.7). However, this trial was extremely small, andthe process of randomisation was not described,despite the unequal distribution between groups.
The second study63 was a straight comparisonbetween electromagnetic therapy and shamtherapy in 30 male patients with a spinal cordinjury and a grade 2 or 3 pressure sore. Differentoutcomes were presented for the two grades ofpressure sore. After 1 week in the stage 2 pressuresores the median area of ulcer healed was 84% inthe electromagnetic therapy group and 40% in thesham therapy group (p = 0.01). As the stage 2pressure sores were significantly smaller at baseline
in the electrotherapy group than in the shamgroup, this result goes with the direction of bias, asthe outcome (percentage healing) favours smallerulcers. For stage 3 pressure sores, 3/5 (60%) soreshealed in the electromagnetic therapy groupcompared with none in the sham therapy group(RR = 7; 95% CI, 0.45 to 108.26).
These two studies were small and of questionablevalidity, and therefore they provide no clearevidence of a benefit of electromagnetic therapyon pressure sore healing. Secondary outcomemeasures such as financial costs, quality of life,pain and acceptability were not measured in any ofthe RCTs included in this review.
Results
160
Low-level laser therapy
Treatment of venous leg ulcersThere is insufficient evidence to suggest a benefitof treating venous ulcers with low-level lasertherapy. The only suggestion of a therapeuticbenefit was given in one small RCT where thecombination of laser and infrared light led to asignificant improvement in the healing rates ofvenous ulcers.42 However, the results of this trialand the others included in this review were drawnfrom small studies and no clear inclusion criteriafor venous leg ulcers were given and there waspoor baseline comparability between study arms.Thus the results of the trials included in this reviewshould be viewed with caution.
Therapeutic ultrasound
Treatment of venous leg ulcersThere is no clear, reliable evidence of a benefitof treating venous leg ulcers with therapeuticultrasound. Only seven small trials were includedin this review, with a total of 269 patients. Thus it isimpossible to determine clinically important effectsof this treatment modality.
Treatment of pressure soresThe results of the studies included in this reviewdo not suggest a benefit associated with therapeuticultrasound in the healing of pressure sores. All thetrials included involved small numbers of patients,different regimens of therapeutic ultrasound anddiffering follow-up periods. The trials also hadinadequate staging of pressure sores and baselinecomparisons. Thus the results should be viewedwith caution.
Electrotherapy
Treatment of chronic woundsThe two small trials identified suggest a benefitassociated with electrotherapy compared with shamelectrotherapy or no electrotherapy to heal chroniculcers. However, the trials were biased for baselinearea and lacked the power to detect clinically
important differences. Importantly, one study49
incorporated patients with multiple wounds,but regarded the wound as the unit of analysis.This approach is flawed, because separate woundson the same patient cannot be regarded asindependent. As such, it is impossible to drawconclusions about the effectiveness ofelectrotherapy to treat chronic wounds.
Treatment of ischaemic ulcersThe results of the five studies eligible for inclusionin this section of the review are difficult tointerpret as the trials were small and mostly of poorquality. Those trials that had superior methodolog-ical quality were biased for baseline ulcer area. Assuch, no recommendations for practice can bemade.
Treatment of diabetic ulcersThe one trial identified demonstrated no signifi-cant difference in ulcer healing between theintervention and control groups. The numberof ulcers healing in both groups was very small.Therefore, no significant benefit was demonstratedfor the use of electrotherapy to treat diabeticulcers.
Treatment of pressure soresThe three trials identified suggest a benefit associ-ated with using electrotherapy to treat pressuresores. However, this suggestion is drawn from threesmall studies with a total of only 140 patients, andtherefore the results should be viewed withcaution.
Electromagnetic therapy
Treatment of venous leg ulcersOnly three small trials with a total of 92 patientswere identified. These trials provided no evidenceof a benefit of electromagnetic therapy for venousleg ulcers.
Treatment of pressure soresTwo small trials, with a total of 55 patients, wereidentified. These provide no clear evidence ofa benefit of electromagnetic therapy for thetreatment of pressure sores.
Health Technology Assessment 2001; Vol. 5: No. 9
161
Chapter 4
Discussion
Secondary outcome measuresNone of the secondary outcome measures high-lighted at the start of the review (i.e. financial
costs, quality of life, adverse effects, pain) wereaddressed in any of the trials included in thereview. It is therefore impossible to provide anyconclusions on these issues.
Discussion
162
Implications for clinical practice
There is insufficient evidence to state whether theuse of any of the physical therapies identified forthis review are beneficial or not in the treatment ofany of the chronic wounds studied.
Implications for future research
Further research is required to clarify the relation-ship between the various physical therapies andchronic wound healing. The most promisingphysical therapies for further investigation areultrasound for the treatment of venous leg ulcersand electrotherapy for the treatment of pressuresores. Future research should include detailedreporting of co-interventions (e.g. wound dress-ings, and compression for venous leg ulcers,pressure relief for pressure sores), as these mayaffect healing and details of their use are essentialfor the interpretation of results.
In all the studies included in this review theresearch methodology could be significantlyimproved, and commissioning groups may wishto consider the following aspects for futureresearch.
• The number of patients in a trial should bebased on an a priori sample-size calculation.
• A truly objective outcome measure should beused, or wound healing should be expressed as
both a percentage and an absolute change inwound area.
• A single reference wound should be selected foreach patient.
• Experimental groups should be comparable atbaseline.
• Wherever possible, each therapy should becompared with sham therapy.
• A complete and thorough description of concur-rent treatments, including secondary dressings,should be given in trial reports.
• Assessment of outcomes should ideally be blindto treatment or be completely objective.
• Survival-rate analysis should be done in allstudies that assess wound healing.
• Cost-effectiveness and quality-of-life assessmentsshould be included in addition to objectivemeasures of effectiveness of physical therapies.
• Economic evaluations should be incorporatedin trials that are sufficiently large to detectappropriate economic and clinical outcomes.
To prevent publication bias and ensure the inclusionof unpublished trials in systematic reviews, thoseinvolved in primary research should make their dataavailable to those undertaking systematic reviews.
Health Technology Assessment 2001; Vol. 5: No. 9
163
Chapter 5
Conclusions


This study was commissioned by the NHS R&DHTA programme. The authors are indebted to
the HTA referees for their perseverance in readingthis report and the quality of their comments.The views expressed in this report are those ofthe authors, who are responsible for any errors.
The authors are extremely grateful to RozThompson and Sally Bell-Syer (Secretary andTrial Search Coordinator, respectively, of theCochrane Wounds Group) for help withsearching and careful maintenance of the TrialsRegister.
Health Technology Assessment 2001; Vol. 5: No. 9
165
Acknowledgements

1. Callam MJ, Ruckley CV, Harper DR, Dale JJ.Chronic ulceration of the leg: extent of theproblem and provision of care. Br Med J 1985;290:1855–6.
2. Lees TA, Lambert D. Prevalence of lower limbulceration in an urban health district B J Surg1992;79:1032–4.
3. Baker SR, Stacey MC, Singh G, Hoskin SE,Thompson PJ. Aetiology of chronic leg ulcers. Eur JVasc Surg 1991;6:245–51.
4. Callam M. Chronic leg ulceration: the Lothianand Forth Valley Leg Ulcer Study [ChM thesis].Dundee: University of Dundee; 1989.
5. Charles H. The impact of leg ulcers on patients’quality of life. Prof Nurse 1995;10:571–4.
6. Bosanquet N. Costs of venous ulcers – frommaintenance therapy to investment programs.Phlebology 1992;7:44–6.
7. Cullum N, Fletcher AW, Nelson EA, Sheldon TA.Compression bandages and stockings in thetreatment of venous leg ulcers. Oxford: UpdateSoftware; 1998. Cochrane review, Cochrane Library,Issue 3.
8. Riet ter G. Vitamin C and ultrasound in thetreatment of pressure ulcers (dissertation).Maastricht: University of Limburg; 1994.
9. Reiber GE. The epidemiology of diabetic footproblems. Diabetic Med 1996;13(Suppl 1):S6–11.
10. Kings Fund. Counting the cost. The real impact ofnon-insulin dependent diabetes. London: KingsFund Policy Unit; 1996.
11. Moss SE, Klein R, Klein BE. The prevalence andincidence of lower extremity amputation in adiabetic population. Arch Int Med 1992;152:610–16.
12. Callam MJ, Ruckley CV, Harper DV, Dale JJ.Chronic ulceration of the leg: extent of theproblem and provision of care. Br Med J 1985;290:1855–6.
13. Andersson E, Hansson C, Swanbeck G. Legand foot ulcer prevalence and investigation ofperipheral arterial and venous circulation in arandomized elderly population – an epidemiologicsurvey and clinical investigation. Acta DermatolVenerol 1993;73:57–61.
14. Cullum NA, Fletcher AW, Nelson EA, Sheldon TA.Compression bandages and stockings in the
treatment of venous leg ulcers. Oxford: UpdateSoftware. Cochrane Library, Issue 4.
15. Callam MJ, Ruckley CV, Dale JJ, Harper DR.Hazards of compression treatment of the leg: anestimate from Scottish surgeons. Br Med J 1987;295:1382.
16. Mester E. Mester AF, Mester A. The biomedicaleffects of laser application. Lasers Surg Med 1988;5:607–14.
17. Basford JR. Low-energy laser therapy: controversiesand new research findings. Lasers Surg Med 1989;9:1–5.
18. James J. Laser therapy on trial Primary Health Care1994;4(Pt 10):18–20.
19. James J. Low-power laser therapy. In: Proceedingsof the 5th European Conference on Advances inWound Management. London: Macmillan; 1996.p. 119–21.
20. Swedish Laser-Medical Society. http://www.laser.nu/lllt/faq1.htm; 1998.
21. Basford JR. Low intensity laser therapy: still not anestablished clinical tool. Lasers Surg Med 1995;16:331–42.
22. Dyson M. Non-thermal cellular effects ofultrasound. Br J Cancer 1982;45(Pt 5 Suppl):165–71.
23. Dyson M. Mechanisms involved in therapeuticultrasound. Physiotherapy 1987;73:116–20.
24. Hewitt GK. Chronic leg ulcers Physiotherapy1956;42:43–5.
25. Burr HS, Taffel M, Harvey SC. An electrometricstudy of the healing wound in man. Yale J Biol Med1940;12:483–5.
26. Weiss DS, Kirsner R, Eaglstein WH. Electricalstimulation and wound healing. Arch Dermatol1990;126(Pt 2):222–5.
27. Stiller MJ, Pak GH, Shupack JL, Thaler S, Kenny C,Jondreau L. A portable pulsed electromagneticfield (PEMF) device to enhance healing ofrecalcitrant venous ulcers: a double-blind, placebo-controlled clinical trial. Br J Dermatol 1992;127:147–54.
28. Deeks J. Odds ratios should be used only in casecontrol studies and logistic regression analyses. BrMed J 1998;317:1155–6.
Health Technology Assessment 2001; Vol. 5: No. 9
167
References
29. Goldin JH, Broadbent NRG, Nancarrow JD,Marshall T. The effects of Diapulse on the healingof wounds: a double blind randomised controlledtrial in man. Br J Plastic Surg 1981:34;267–70.
30. Jivegard LEH, Augustinsson LE, Holm J, Risberg B,Ortenwall P. Effects of spinal cord stimulationin patients with inoperable severe lower limbischaemia: a prospective randomised controlledtrial. Eur J Endovasc Surg 1995;9:421–5.
31. Katelaris PM, Fletcher JP, Little M, McEntyre RJ,Jeffcoate KW. Electrical stimulation in thetreatment of chronic venous ulceration. Austr NZ JSurg 1987;57:605–7.
32. Muirhead RJ, Place D, Buswell WA, Heselting J.Pulsed electromagnetic energy and pre-tibiallacerations: a randomised clinical trial. Arch EmergMed 1991;8:152–60.
33. Santoianni P, Monfrecola G, Martellotta D, Ayala F.Inadequate effect of helium–neon laser on venousleg ulcers. Photodermatology 1984;1:245–9.
34. Crous L, Malherbe C. Laser and ultraviolet lightirradiation in the treatment of chronic ulcers.Physiotherapy 1988;44:73–7.
35. Bilhari I, Mester AR. The biostimulative effect oflow level laser therapy of long-standing cruralulcers using helium neon laser, helium neon plusinfrared lasers, and noncoherent light: preliminaryreport of a randomized double-blind comparativestudy. Laser Ther 1989;1(Pt 2):97–8.
36. Malm M, Lundeberg T. Effect of low power galliumarsenide laser on healing of venous ulcers. Scand JPlastic Reconstruct Surg Hand Surg 1991;25(Pt 3):249–51.
37. Lundeberg T, Malm M. Low-power HeNe lasertreatment of venous leg ulcers. Ann Plastic Surg1991;27(Pt 6):537–9.
38. Dyson M, Franks C, Suckling J. Stimulation ofhealing of varicose ulcers by ultrasound. Ultrasonics1976;14:232–6.
39. Roche C, West J. A controlled trial investigating theeffect of ultrasound on venous ulcers referred fromgeneral practitioners. Physiotherapy 1984;70:475–7.
40. Callam MJ, Dale JJ, Ruckley CV, Harper DR. Trialof ultrasound in the treatment of chronic legulceration. In: Negus D, Jantet G, editors.Phlebology ‘85. London: Libbey; 1986. p. 625–6.
41. Lundeberg T, Nordstrom F, Brodda-Jansen G,Eriksson SV, Kjartansson J, Samuelson UE. Pulsedultrasound does not improve healing of venousulcers. Scand J Rehab Med 1990;22:195–7.
42. Eriksson SV, Lundeberg T, Malm M. A placebocontrolled trial of ultrasound therapy in chronic legulceration. Scand J Rehab Med 1991;23:211–13.
43. Peschen M, Vanscheidt W. Low frequencyultrasound of chronic venous leg ulcers as part ofan out-patient treatment. In: Proceedings of the 5thEuropean Conference on Advances in WoundManagement. London: Macmillan; 1996. p. 271.
44. Weichenthal M, Mohr P, Stegmann W, BrietbartEW. Low-frequency ultrasound treatment ofchronic venous ulcers. Wound Repair Regeneration1997;5(Pt 1):18–22.
45. McDiarmid T, Burns PN, Lewith GT, Machin D.Ultrasound in the treatment of pressure sores.Physiotherapy 1985;71:66–70.
46. Nussbaum EL, Biemann I, Mustard B. Comparisonof ultrasound/ultraviolet-C and laser for treatmentof pressure ulcers in patients with spinal cordinjury. Phys Ther 1994;74(Pt 9):812–25.
47. ter Riet G, Kessels AGH, Knipschild P. Arandomized clinical trial of ultrasound in thetreatment of pressure ulcers. Phys Ther 1996;76(Pt 12):1301–11.
48. Kloth LC, Feedar JA. Acceleration of woundhealing with high voltage, monophasic, pulsedcurrent [published erratum appears in Phys Ther1989;69(Pt 8):702]. Phys Ther 1988;68:503–8.
49. Mulder GD. Treatment of open-skin wounds withelectric stimulation. Arch Phys Med Rehab 1991;72:375–7.
50. Wolcott LE, Wheeler PC, Hardwicke HM,Rowley BA. Accelerated healing of skin ulcer byelectrotherapy: preliminary clinical results. SouthMed J 1969;62:795–801.
51. Gault WR, Gatens Jr PF. Use of low intensity directcurrent in management of ischaemic skin ulcers.Phys Ther 1976;56:265–9.
52. Carley P, Wainapel SF. Electrotherapy foracceleration of wound healing: low intensity directcurrent. Arch Phys Med Rehab 1985;66(Pt 7):443–6.
53. Feedar JA, Kloth LC, Gentzkow GD. Chronic dermalulcer healing enhanced with monophasic pulsedelectrical stimulation. Phys Ther 1991;71:639–49.
54. Claeys LGV, Horsch S. Effects of spinal cordstimulation on ischaemic inflammatory pain andwound healing in patients with peripheral arterialocclusive disease. Pain Digest 1997;7:200–3.
55. Lundeberg TCM, Eriksson SV, Malm M. Electricalnerve stimulation improves healing of diabeticulcers. Ann Plastic Surg 1992;29(Pt 4):328–31.
56. Gentzkow GD, Pollack SV, Kloth LC, Stubbs HA.Improved healing of pressure ulcers usingDermapulse, a new electrical stimulation device.Wounds: Compend Clin Res Pract 1991;3(Pt 5):158–70.
57. Griffin JW, Tooms RE, Mendius RA, Clifft JK,Vander Zwaag R, el-Zeky F. Efficacy of high voltage
References
168
pulsed current for healing of pressure ulcers inpatients with spinal cord injury. Phys Ther 1991;71:433–42, discussion 442–4.
58. Wood JM, Evans PE III, Schallreuter KU, WymanMD, Jacobson E, Sufit R, et al. A multicentre studyon the use of pulsed low-intensity direct current forhealing chronic stage II and stage III decubitusulcers [see comments]. Arch Dermatol 1993;129:999–1009.
59. Ieran M, Zaffuto S, Bagnacani M, Annovi M,Moratti A, Cadossi R. Effect of low frequencypulsing electromagnetic fields on skin ulcers ofvenous origin in humans: a double-blind study.J Orthopaed Res 1990;8:276–82.
60. Kenkre JE, Hobbs FD, Carter YH, Holder RL,Holmes EP. A randomized controlled trial ofelectromagnetic therapy in the primary caremanagement of venous leg ulceration. FamilyPract 1996;13(Pt 3):236–41.
61. Stiller MJ, Pak GH, Shupack JL, Thaler S, Kenny C,Jondreau L. A portable pulsed electromagneticfield (PEMF) device to enhance healing ofrecalcitrant venous ulcers: a double-blind, placebo-controlled clinical trial. Br J Dermatol 1992;127:147–54.
62. Comorosan S, Vascilco R, Arghiropol M, Paslaru L,Jieanu V, Stelea S. The effect of Diapulse therapyon the healing of decubitus ulcer. Romanian JPhysiol 1993;30:1–2, 41–5.
63. Salzberg CA, Cooper-Vastola SA, Perez F, ViehbeckMG, Byrne DW. The effects of non-thermal pulsedelectromagnetic energy on wound healing ofpressure ulcers in spinal cord-injured patients: arandomized, double-blind study. Ostomy WoundManagement 1995;41:42–4, 46, 48.
64. Central Begeleidingsorgaan voor de IntercollegialeToetsing. Consensus bijeenkomst: behandelingDecubitus. Utrecht: CBO; 1985.
Health Technology Assessment 2001; Vol. 5: No. 9
169

The review was compiled using RCTs from theCochrane Wounds Group Specialist Trials
Register. Multiple and repeated searches have beencarried out since 1995, and our searching has, tosome extent, been validated by searches carried outby BMJ Publishing Ltd for the publication ClinicalEvidence. It is not possible at this stage to present aflowchart describing search yields and exclusions,as the search has been ongoing for so many yearsand initially was part of a larger search coveringeight related wound management topics.
The Wounds Group Trials Register was searchedup to April 2000 and has been assembled andmaintained as described in the following sections.
Electronic searches
MEDLINEMEDLINE (SilverPlatter version 4.0) was beensearched for RCTs and controlled clinical trialsfrom 1966 to December 1997, using a mixtureof free text terms and MeSH headings: FromJanuary 1998 it was unnecessary to searchMEDLINE as this is searched centrally by the UKCochrane Centre for all trials and the results aretransferred to CENTRAL/CCTR. Since January1998, CENTRAL/CDSR was searched instead ofMEDLINE for all issues of the Cochrane Library.
The search strategy used was as follows:
1. decubitus ulcer/ or foot ulcer/2. leg ulcer/ or varicose ulcer/3. pilonidal cyst/4. skin ulcer/5. diabetic foot/6. ((plantar or diabetic or heel or venous or stasis
or arterial) adj ulcer$).tw.7. ((decubitus or foot or diabetic or ischaemic or
pressure) adj ulcer$).tw.8. ((pressure or bed) adj sore$).tw.9. ((pilonidal adj cyst) or (pilonidal adj sinus) or
bedsore$).tw.10. ((diabetic adj foot) or (cavity adj wound)).tw.11. ((varicose or leg or skin) adj ulcer$).tw.12. (decubitus or (chronic adj wound$)).tw.13. ((sinus adj wound$) or (cavity adj
wound$)).tw.
14. or/1–1315. debridement/ or biological dressings/ or
bandages/16. occlusive dressings/ or clothing/ or wound
healing/17. antibiotics/ or growth substances/ or platelet-
derived growth factor/18. fibroblast growth factor/ or electrical
stimulation therapy.ti,ab,sh.19. lasers/ or nutrition/ or surgery/ or surgery,
plastic/20. surgical flaps/ or skin transplantations/ or
homeopathy/ or homeopathic/21. acupuncture therapy/ or acupuncture/ or
alternative medicine/22. alternative medicine/ or massage/ or iloprost/
or alginates/23. zinc/ or zinc oxide/ or ointments/ or anti-
infective agents/24. dermatologic agents/ or colloids/ or cushions/
or wheelchairs/25. beds/ or wound dressings/26. (debridement or dressing$ or compress$ or
cream$ or (growth adj factor$)).tw.27. (pressure-relie$ or (recombinant adj protein$)
or bandag$ or stocking$).tw.28. (antibiotic$ or (electric adj therapy) or laser$
or nutrition$ or surg$).tw.29. (homeopath$ or acupuncture or massage or
reflexology or ultrasound).tw.30. (iloprost or alginate$ or zinc or paste$ or
ointment$ or hydrocolloid$).tw.31. ((compression adj therapy) or (compression
adj bandag$) or wrap$).tw.32. (bed$ or mattress$ or wheelchair$ or (wheel
adj chair) or cushion$).tw.33. ((wound adj dressing$) or vitamin$ or bind$ or
gauze$ or heals or healing).tw.34. (diet or lotion$ or infect$ or reduc$ or (wound
adj healing)).tw.35. (treat$ or prevent$ or epidemiol$ or aetiol$ or
etiol$ or therap$ or prevalence or incidence).tw.36. or/15–3537. 14 and 3638. random allocation/ or randomized controlled
trials/39. controlled clinical trials/ or clinical trials phase
I/ or clinical trials phase II/40. clinical trials phase III/ or clinical trials phase
IV/ or clinical trials overviews/
Health Technology Assessment 2001; Vol. 5: No. 9
171
Appendix 1
Databases searched and search strategies
41. single-blind method/ or double-blind method/42. publication bias/ or review/ or review,
academic/43. review tutorial/ or meta-analysis/ or systematic
review/44. ((random$ adj controlled adj trial$) or
(prospective adj random$)).tw.45. ((random adj allocation) or random$ or
(clinical adj trial$) or control$).tw.46. ((standard adj treatment) or compar$ or
single-blind$ or double-blind$).tw.47. (blind$ or placebo$ or systematic$ or
(systematic adj review)).tw.48. (randomized controlled trial or clinical
trial).pt. or comparative study.sh.49. or/38–4850. 37 and 4951. limit 50 to human52. burns/ or wounds, gunshot/ or corneal ulcer/
or exp dentistry/53. peptic ulcer/ or duodenal ulcer/ or stomach
ulcer/54. ((peptic adj ulcer) or (duodenal adj ulcer) or
traum$).tw.55. ((aortocaval adj fistula) or (arteriovenous adj
fistula)).tw.56. (bite adj wound$).tw.57. or/52–5658. 51 not 57
CENTRAL/CDSRThe CENTRAL/CSDR was searched on theCochrane Library CD-ROM. The search strategyused was as follows:
1. ((DECUBITUS and ULCER*) or (VARICOSEand ULCER*))
2. ((LEG or LEGS) and ULCER*)3. ((FOOT or FEET) and ULCER*)4. ((LEG or LEGS) and VARICOSE)5. (SKIN and ULCER*)6. SKIN-ULCER*:ME7. ((FOOT or FEET) and DIABETIC)8. ((((((PLANTAR or DIABETIC) or HEEL) or
VENOUS) or STASIS) or ARTERIAL) andULCER*)
9. ((ISCHEMIC or PRESSURE) and ULCER*)10. ((BED or BEDS) near (SORE or SORES))11. (PRESSURE near (SORE or SORES))12. (PILONIDAL and CYST*)13. (PILONIDAL and SINUS*)14. (PILONIDAL and ABSCES*)15. ((WOUND or WOUNDS) and CAVITY)16. ((WOUND or WOUNDS) and SINUS*)17. ((WOUND or WOUNDS) and CHRONIC)18. ((WOUND or WOUNDS) and DECUBITUS)
19. WOUND-INFECTION*:ME20. ((WOUND or WOUNDS) and MALIGNANT)21. WOUND-HEALING*:ME22. WOUNDS-GUNSHOT*:ME23. ((GUN or GUNS) or GUNSHOT)24. WOUNDS-STAB*:ME25. LACERATION*26. SURGICAL-WOUND-DEHISCENCE*:ME27. BITES-AND-STINGS*2:ME28. ((BITE or BITES) or BITING)29. TRAUMATOLOGY*:ME30. BURNS*:ME31. (WOUND* and BURN*)32. (BURN* or SCALD*)33. ((SITE or SITES) near DONOR)34. SELF-MUTILATION*:ME35. ((STAB or STABS) or STABBING)36. SOFT-TISSUE-INJURIES*:ME37. (((((((((((#1 or #2) or #3) or #4) or #5) or
#6) or #7) or #8) or #9) or #10) or #11) or#12)
38. (((((((((((#13 or #14) or #15) or #16) or #17)or #18) or #19) or #20) or #21) or #22) or #23)or #24)
39. ((((((((((((#25 or #26) or #27) or #28) or#29) or #30) or #31) or #32) or #33) or #34) or#35) or #36)
40. (#37 or #38 OR #39)41. DENTAL42. (#40 not #41)43. CORNEAL44. (#42 not 43)45. DUODENAL-ULCER*1:ME46. (#44 not #45)47. CORNEAL-ULCER*1:ME48. (#46 not #47)49. CORNEAL-DISEASES*:ME50. (#48 not #49)51. ACNE52. (#50 not #51)53. BEDNET54. (#52 not #53)
CINAHLThe Cumulative Index of Nursing and AlliedHealth Literature (CINAHL) (SilverPlatter version4.0) was been searched for the period from itsinception to July 1999. The search strategy usedwas as follows:
1. (pressure-ulcer* or foot-ulcer* or leg-ulcer* orskin-ulcer*) in de
2. (diabetic-foot* or diabetic-neuropathies*)in de
3. ((diabetic-angiopathies*) in de) or diabetes-mellitus/complications/ all age subheadings
Appendix 1
172
4. (pilonidal-cyst* or surgical-wound-infection*)in de
5. (plantar or diabetic or heel or venous or stasisor (arterial near ulcer*)) in ti,ab
6. (decubitus or foot or diabetic or ischaemic or(pressure near ulcer*)) in ti,ab
7. (pressure or (bed near sore*))in ti,ab8. ((pilonidal near cyst) or (pilonidal near sinus)
or bedsore) in ti,ab9. (diabetic near foot) or ((cavity near wound)in
ti,ab)10. (varicose or leg or (skin near ulcer*)) in
ti,ab11. ((decubitus or chronic) near wound*) in
ti,ab12. (sinus near wound*) or ((cavity near wound*)
in ti,ab)13. ((burn near wound*) or (gunshot near
wound*) or (bite near wound*) or trauma) inti,ab
14. #1 or #2 or #3 or #4 or #5 or #6 or #7 or #8 or#9 or #10 or #11 or #12 or #13
15. (clinical-trials or single-blind-studies or double-blind-studies) in de
16. (control-group or placebos or meta-analysis)in de
17. (random* near clinical near trial*) or((prospective near random*) in ti,ab)
18. ((random near allocation) or random* orcontrolled-clinical-trial* or control) in ti,ab
19. (comparison group* or (standard neartreatment) or compar*)in ti,ab
20. (single-blind* or (single near blind) or double-blind or (double near blind)) in ti,ab
21. (blind* or placebo* or systematic or(systematic near review)) in ti,ab
22. ((meta analysis or meta-analysis) or (trial* orprospective)) in ti,ab
23. ((clinical-trials) or (comparative-studies))in de
24. #15 or #16 or #17 or #18 or #19 or #20 or #21or #22 or #23
25. #14 and #2426. explode dentistry/ all topical subheadings/ all
age subheadings27. (peptic-ulcer*) or (duodenal-ulcer*) or
((corneal-ulcer*)in de)28. (peptic near ulcer) or (duodenal near ulcer)
or ((corneal near ulcer) in ti,ab)29. dentist* in de30. #26 or #27 or #28 or #2931. #25 not #30
Other databasesOther databases that were searched from theearliest date available until 1997 are:
• EMBASE (SilverPlatter version 4.0)• ISI Science Citation Index (on BIDS)• BIOSIS (on EDINA)• British Diabetic Association Database• CISCOM (Complementary Medicine Database
of the RCCM)• Conference Proceedings (on BIDS)• Dissertation Abstracts• Royal College of Nursing Database (CD-ROM)• British Nursing Index (on ARC), to December
1998
Handsearching
JournalsThe following wound care specialist journals arebeing prospectively handsearched for all RCTs asfollows:
• CARE – Science and Practice, 1979–1990 (laterJournal of Tissue Viability, searched until present)
• Decubitus, 1987–1993• Journal of Tissue Viability, 1991–present• Journal of Wound Care, 1991–present• Phlebology, 1986–present.
Conference proceedingsWound care conference proceedings that havebeen handsearched for RCTs are:
• Proceedings of the 1st European Conference onAdvances in Wound Management, September1991, Cardiff, UK
• Proceedings of the 2nd European Conferenceon Advances in Wound Management, October1992, Harrogate, UK
• Proceedings of the 3rd European Conferenceon Advances in Wound Management, October1993, Harrogate, UK
• Proceedings of the 4th European Conference onAdvances in Wound Management, September1994, Copenhagen, Denmark
• Proceedings of the 5th European Conference onAdvances in Wound Management, November1995, Harrogate, UK
• Proceedings of the 6th European Conference onAdvances in Wound Management, October1996, Amsterdam, The Netherlands
• Proceedings of the 7th European Conference onAdvances in Wound Management, November1997, Harrogate, UK
• Proceedings of the 8th European Conference onAdvances in Wound Management, April 1998,Madrid, Spain
Health Technology Assessment 2001; Vol. 5: No. 9
173

• 3rd Annual Symposium on Advanced WoundCare, March 1990, Orlando, FL, USA
• 4th Annual Symposium on Advanced WoundCare, April 1991, San Francisco, CA, USA
• 5th Annual Symposium on Advanced WoundCare, April 1992, New Orleans, LA, USA
• 8th Annual Symposium on Advanced WoundCare & Medical Research Forum on WoundRepair, April 1995, San Diego, CA, USA
• 9th Annual Symposium on Advanced WoundCare, April 1996, Atlanta, GA, USA
• Proceedings of Going into the ‘90s: The Phar-macist and Wound Care, September 1992,London, UK
• Proceedings of the Second Joint British/SwedishAngiology Meeting, 1991, London, UK
• Symposium on Venous Leg Ulcers, 1985,London, UK
• Venous Forum of the Royal Society of Medicine,April 1999, Leeds, UK
Other strategies
Identification of unpublished studiesSeveral databases were searched (up to December1997) in an attempt to identify unpublishedstudies. These include:
• Current Research in Britain (CRIB)• DHS Database• SIGLE• UK National Research Register.
Experts in the field of wound care were contactedto enquire about ongoing and recently publishedtrials in the field of wound care. In addition,manufacturers of wound care materials werecontacted for details of the trials they areconducting. Citations within obtained reviewsand papers were scrutinised to identify additionalstudies.
Appendix 1
174

Dr Mary Bliss Department of Medicine for the Elderly, Homerton Hospital, London(now retired)
Professor Andrew Boulton Department of Medicine, Manchester Royal Infirmary, Manchester
Professor Nick Bosanquet Department of General Medicine, Imperial College School of Medicine,London
Dr Richard Bull Department of Dermatology, Homerton Hospital, London
Mr Michael Callam Department of Vascular Surgery, Bedford Hospital, Bedford
Carol Dealey Moseley Hall Hospital, Birmingham
Professor Peter Friedman Department of Dermatology, Royal Liverpool University Hospital, Liverpool(now Southampton)
Mr Brian Gilchrist Department of Nursing Studies, King’s College, London
Dr Keith Harding Wound Healing Research Unit, University of Wales College of Medicine,University Department of Surgery, Cardiff
Deborah Hofman Dermatology Department, Churchill Hospital, Oxford
Vanessa Jones Wound Healing Research Unit, University Department of Surgery, Cardiff
Christina Lindholm Department of Nursing Research, Uppsala University Hospital, Uppsala
Dr Raj Mani Southampton University Hospital, Medical Physics Department,Southampton
Andrea Nelson Department of Nursing, University of Liverpool (now Department ofHealth Studies, University of York)
Dr Steve Thomas Surgical Materials Testing Laboratory, Bridgend, Mid Glamorgan
Dr Ewan Wilkinson Bucks Health Authority, Aylesbury
Health Technology Assessment 2001; Vol. 5: No. 9
175
Appendix 2
Advisory panel

Appendix 3
Summary of included studies
Health Technology Assessment 2001; Vol. 5: No. 9
177
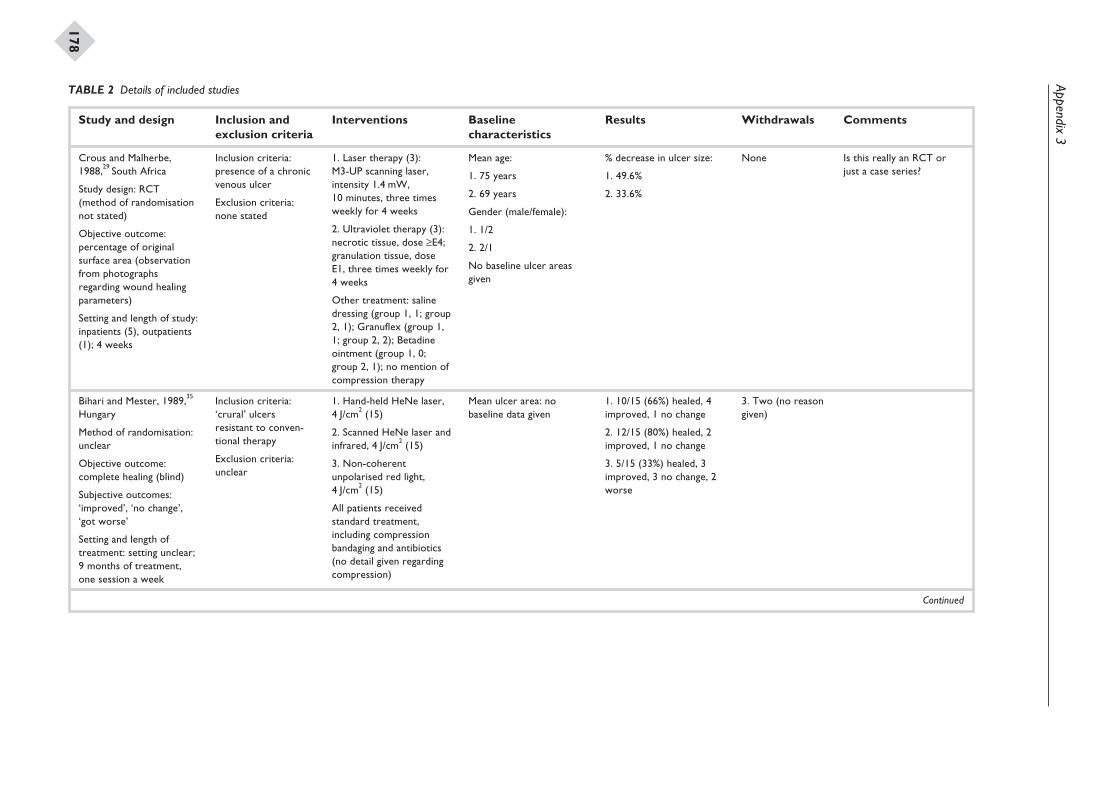
Appendix3
178
Study and design Inclusion andexclusion criteria
Interventions Baselinecharacteristics
Results Withdrawals Comments
Crous and Malherbe,1988,29 South Africa
Study design: RCT(method of randomisationnot stated)
Objective outcome:percentage of originalsurface area (observationfrom photographsregarding wound healingparameters)
Setting and length of study:inpatients (5), outpatients(1); 4 weeks
Inclusion criteria:presence of a chronicvenous ulcer
Exclusion criteria:none stated
1. Laser therapy (3):M3-UP scanning laser,intensity 1.4 mW,10 minutes, three timesweekly for 4 weeks
2. Ultraviolet therapy (3):necrotic tissue, dose ≥E4;granulation tissue, doseE1, three times weekly for4 weeks
Other treatment: salinedressing (group 1, 1; group2, 1); Granuflex (group 1,1; group 2, 2); Betadineointment (group 1, 0;group 2, 1); no mention ofcompression therapy
Mean age:
1. 75 years
2. 69 years
Gender (male/female):
1. 1/2
2. 2/1
No baseline ulcer areasgiven
% decrease in ulcer size:
1. 49.6%
2. 33.6%
None Is this really an RCT orjust a case series?
Bihari and Mester, 1989,35
Hungary
Method of randomisation:unclear
Objective outcome:complete healing (blind)
Subjective outcomes:‘improved’, ‘no change’,‘got worse’
Setting and length oftreatment: setting unclear;9 months of treatment,one session a week
Inclusion criteria:‘crural’ ulcersresistant to conven-tional therapy
Exclusion criteria:unclear
1. Hand-held HeNe laser,4 J/cm2 (15)
2. Scanned HeNe laser andinfrared, 4 J/cm2 (15)
3. Non-coherentunpolarised red light,4 J/cm2 (15)
All patients receivedstandard treatment,including compressionbandaging and antibiotics(no detail given regardingcompression)
Mean ulcer area: nobaseline data given
1. 10/15 (66%) healed, 4improved, 1 no change
2. 12/15 (80%) healed, 2improved, 1 no change
3. 5/15 (33%) healed, 3improved, 3 no change, 2worse
3. Two (no reasongiven)
Continued
TABLE 2 Details of included studies
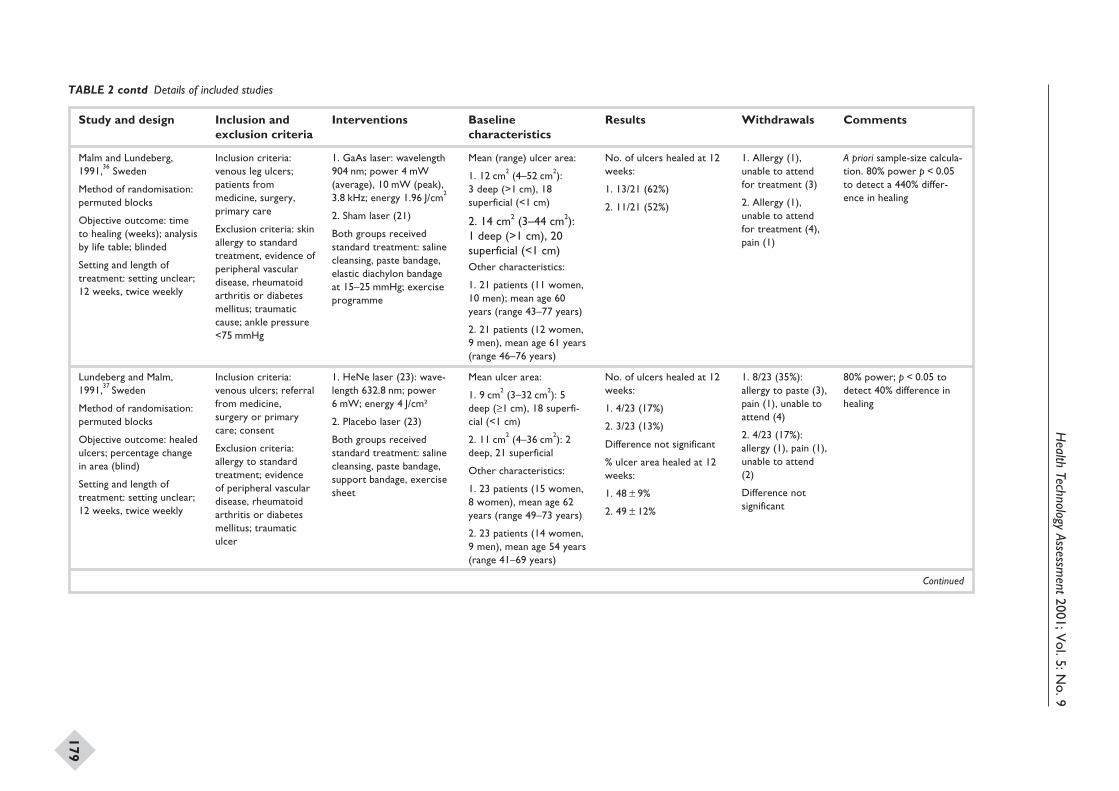
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
179
Study and design Inclusion andexclusion criteria
Interventions Baselinecharacteristics
Results Withdrawals Comments
Malm and Lundeberg,1991,36 Sweden
Method of randomisation:permuted blocks
Objective outcome: timeto healing (weeks); analysisby life table; blinded
Setting and length oftreatment: setting unclear;12 weeks, twice weekly
Inclusion criteria:venous leg ulcers;patients frommedicine, surgery,primary care
Exclusion criteria: skinallergy to standardtreatment, evidence ofperipheral vasculardisease, rheumatoidarthritis or diabetesmellitus; traumaticcause; ankle pressure<75 mmHg
1. GaAs laser: wavelength904 nm; power 4 mW(average), 10 mW (peak),3.8 kHz; energy 1.96 J/cm2
2. Sham laser (21)
Both groups receivedstandard treatment: salinecleansing, paste bandage,elastic diachylon bandageat 15–25 mmHg; exerciseprogramme
Mean (range) ulcer area:
1. 12 cm2 (4–52 cm2):3 deep (>1 cm), 18superficial (<1 cm)
2. 14 cm2 (3–44 cm2):1 deep (>1 cm), 20superficial (<1 cm)Other characteristics:
1. 21 patients (11 women,10 men); mean age 60years (range 43–77 years)
2. 21 patients (12 women,9 men), mean age 61 years(range 46–76 years)
No. of ulcers healed at 12weeks:
1. 13/21 (62%)
2. 11/21 (52%)
1. Allergy (1),unable to attendfor treatment (3)
2. Allergy (1),unable to attendfor treatment (4),pain (1)
A priori sample-size calcula-tion. 80% power p < 0.05to detect a 440% differ-ence in healing
Lundeberg and Malm,1991,37 Sweden
Method of randomisation:permuted blocks
Objective outcome: healedulcers; percentage changein area (blind)
Setting and length oftreatment: setting unclear;12 weeks, twice weekly
Inclusion criteria:venous ulcers; referralfrom medicine,surgery or primarycare; consent
Exclusion criteria:allergy to standardtreatment; evidenceof peripheral vasculardisease, rheumatoidarthritis or diabetesmellitus; traumaticulcer
1. HeNe laser (23): wave-length 632.8 nm; power6 mW; energy 4 J/cm²
2. Placebo laser (23)
Both groups receivedstandard treatment: salinecleansing, paste bandage,support bandage, exercisesheet
Mean ulcer area:
1. 9 cm2 (3–32 cm2): 5deep (≥1 cm), 18 superfi-cial (<1 cm)
2. 11 cm2 (4–36 cm2): 2deep, 21 superficial
Other characteristics:
1. 23 patients (15 women,8 women), mean age 62years (range 49–73 years)
2. 23 patients (14 women,9 men), mean age 54 years(range 41–69 years)
No. of ulcers healed at 12weeks:
1. 4/23 (17%)
2. 3/23 (13%)
Difference not significant
% ulcer area healed at 12weeks:
1. 48 ± 9%
2. 49 ± 12%
1. 8/23 (35%):allergy to paste (3),pain (1), unable toattend (4)
2. 4/23 (17%):allergy (1), pain (1),unable to attend(2)
Difference notsignificant
80% power; p < 0.05 todetect 40% difference inhealing
Continued
TABLE 2 contd Details of included studies
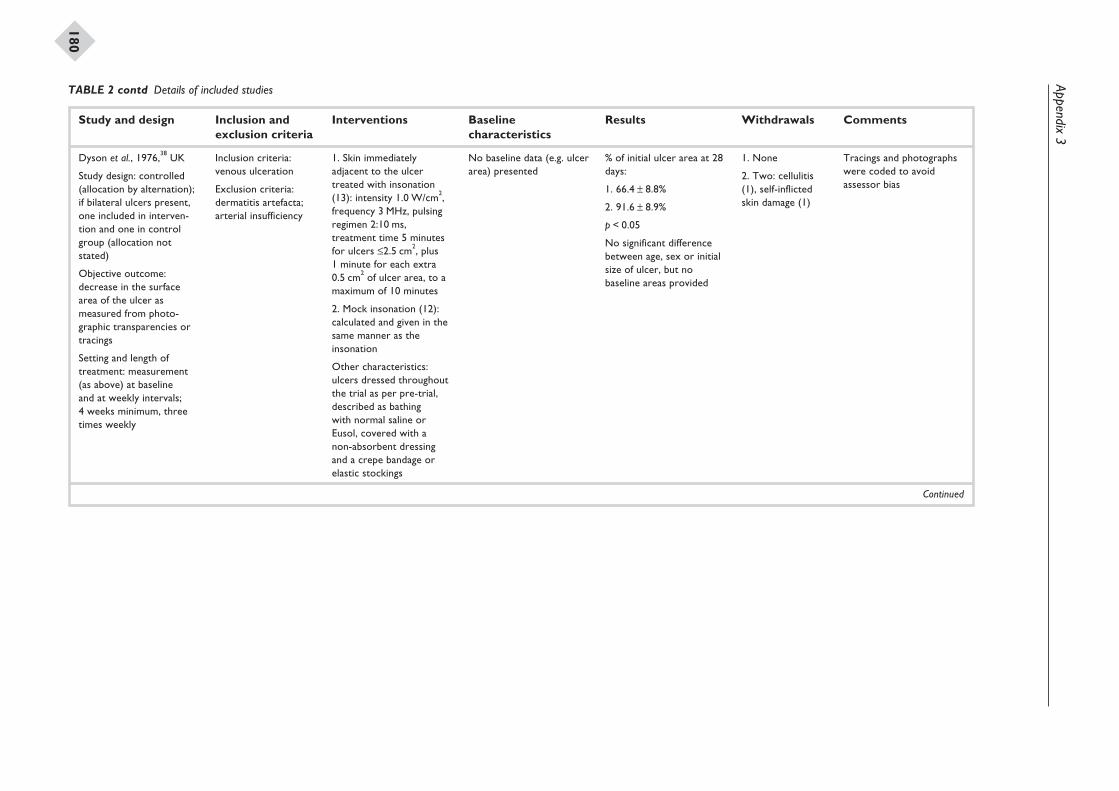
Appendix3
180
Study and design Inclusion andexclusion criteria
Interventions Baselinecharacteristics
Results Withdrawals Comments
Dyson et al., 1976,38 UK
Study design: controlled(allocation by alternation);if bilateral ulcers present,one included in interven-tion and one in controlgroup (allocation notstated)
Objective outcome:decrease in the surfacearea of the ulcer asmeasured from photo-graphic transparencies ortracings
Setting and length oftreatment: measurement(as above) at baselineand at weekly intervals;4 weeks minimum, threetimes weekly
Inclusion criteria:venous ulceration
Exclusion criteria:dermatitis artefacta;arterial insufficiency
1. Skin immediatelyadjacent to the ulcertreated with insonation(13): intensity 1.0 W/cm2,frequency 3 MHz, pulsingregimen 2:10 ms,treatment time 5 minutesfor ulcers £2.5 cm2, plus1 minute for each extra0.5 cm2 of ulcer area, to amaximum of 10 minutes
2. Mock insonation (12):calculated and given in thesame manner as theinsonation
Other characteristics:ulcers dressed throughoutthe trial as per pre-trial,described as bathingwith normal saline orEusol, covered with anon-absorbent dressingand a crepe bandage orelastic stockings
No baseline data (e.g. ulcerarea) presented
% of initial ulcer area at 28days:
1. 66.4 ± 8.8%
2. 91.6 ± 8.9%
p < 0.05
No significant differencebetween age, sex or initialsize of ulcer, but nobaseline areas provided
1. None
2. Two: cellulitis(1), self-inflictedskin damage (1)
Tracings and photographswere coded to avoidassessor bias
Continued
TABLE 2 contd Details of included studies
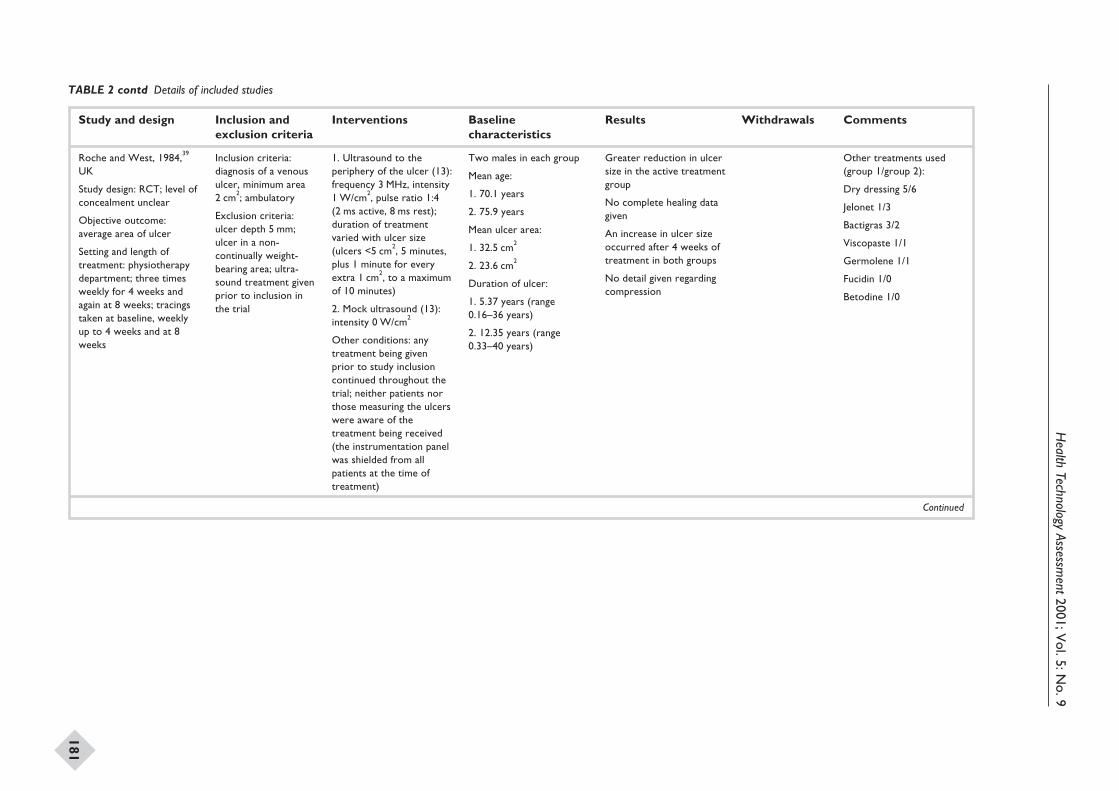
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
181
Study and design Inclusion andexclusion criteria
Interventions Baselinecharacteristics
Results Withdrawals Comments
Roche and West, 1984,39
UK
Study design: RCT; level ofconcealment unclear
Objective outcome:average area of ulcer
Setting and length oftreatment: physiotherapydepartment; three timesweekly for 4 weeks andagain at 8 weeks; tracingstaken at baseline, weeklyup to 4 weeks and at 8weeks
Inclusion criteria:diagnosis of a venousulcer, minimum area2 cm2; ambulatory
Exclusion criteria:ulcer depth 5 mm;ulcer in a non-continually weight-bearing area; ultra-sound treatment givenprior to inclusion inthe trial
1. Ultrasound to theperiphery of the ulcer (13):frequency 3 MHz, intensity1 W/cm2, pulse ratio 1:4(2 ms active, 8 ms rest);duration of treatmentvaried with ulcer size(ulcers <5 cm2, 5 minutes,plus 1 minute for everyextra 1 cm2, to a maximumof 10 minutes)
2. Mock ultrasound (13):intensity 0 W/cm2
Other conditions: anytreatment being givenprior to study inclusioncontinued throughout thetrial; neither patients northose measuring the ulcerswere aware of thetreatment being received(the instrumentation panelwas shielded from allpatients at the time oftreatment)
Two males in each group
Mean age:
1. 70.1 years
2. 75.9 years
Mean ulcer area:
1. 32.5 cm2
2. 23.6 cm2
Duration of ulcer:
1. 5.37 years (range0.16–36 years)
2. 12.35 years (range0.33–40 years)
Greater reduction in ulcersize in the active treatmentgroup
No complete healing datagiven
An increase in ulcer sizeoccurred after 4 weeks oftreatment in both groups
No detail given regardingcompression
Other treatments used(group 1/group 2):
Dry dressing 5/6
Jelonet 1/3
Bactigras 3/2
Viscopaste 1/1
Germolene 1/1
Fucidin 1/0
Betodine 1/0
Continued
TABLE 2 contd Details of included studies
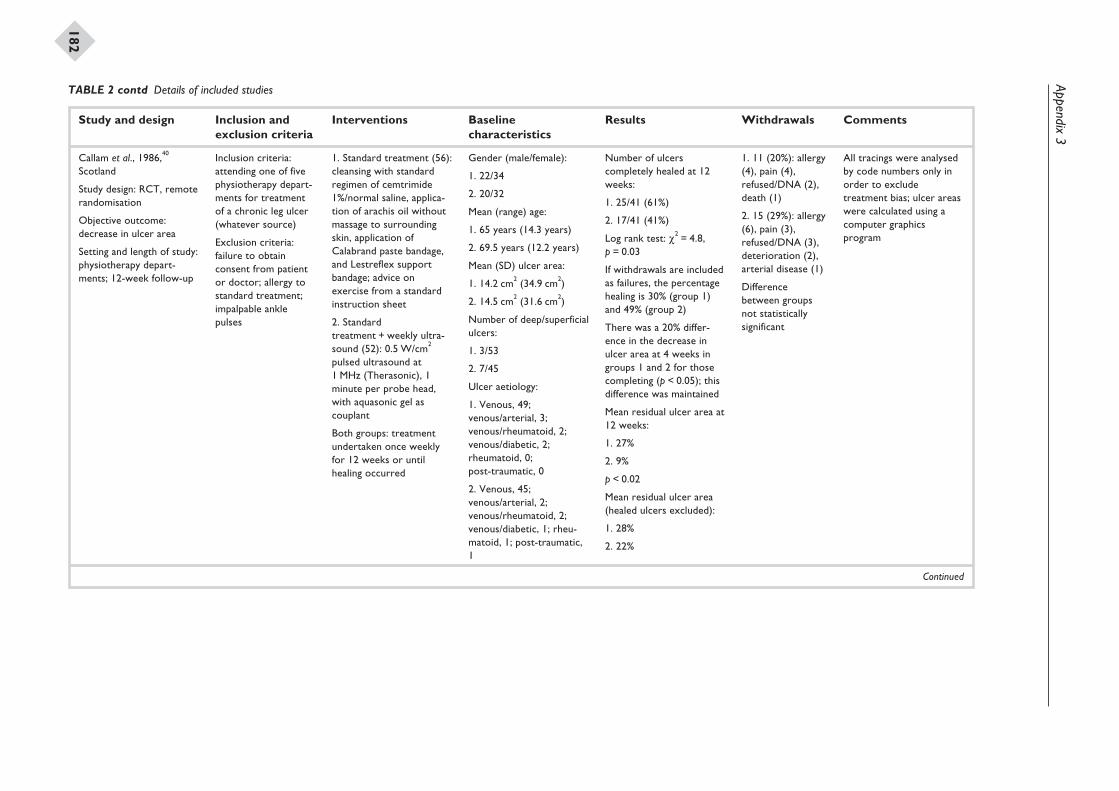
Appendix3
182
Study and design Inclusion andexclusion criteria
Interventions Baselinecharacteristics
Results Withdrawals Comments
Callam et al., 1986,40
Scotland
Study design: RCT, remoterandomisation
Objective outcome:decrease in ulcer area
Setting and length of study:physiotherapy depart-ments; 12-week follow-up
Inclusion criteria:attending one of fivephysiotherapy depart-ments for treatmentof a chronic leg ulcer(whatever source)
Exclusion criteria:failure to obtainconsent from patientor doctor; allergy tostandard treatment;impalpable anklepulses
1. Standard treatment (56):cleansing with standardregimen of cemtrimide1%/normal saline, applica-tion of arachis oil withoutmassage to surroundingskin, application ofCalabrand paste bandage,and Lestreflex supportbandage; advice onexercise from a standardinstruction sheet
2. Standardtreatment + weekly ultra-sound (52): 0.5 W/cm2
pulsed ultrasound at1 MHz (Therasonic), 1minute per probe head,with aquasonic gel ascouplant
Both groups: treatmentundertaken once weeklyfor 12 weeks or untilhealing occurred
Gender (male/female):
1. 22/34
2. 20/32
Mean (range) age:
1. 65 years (14.3 years)
2. 69.5 years (12.2 years)
Mean (SD) ulcer area:
1. 14.2 cm2 (34.9 cm2)
2. 14.5 cm2 (31.6 cm2)
Number of deep/superficialulcers:
1. 3/53
2. 7/45
Ulcer aetiology:
1. Venous, 49;venous/arterial, 3;venous/rheumatoid, 2;venous/diabetic, 2;rheumatoid, 0;post-traumatic, 0
2. Venous, 45;venous/arterial, 2;venous/rheumatoid, 2;venous/diabetic, 1; rheu-matoid, 1; post-traumatic,1
Number of ulcerscompletely healed at 12weeks:
1. 25/41 (61%)
2. 17/41 (41%)
Log rank test: c2 = 4.8,p = 0.03
If withdrawals are includedas failures, the percentagehealing is 30% (group 1)and 49% (group 2)
There was a 20% differ-ence in the decrease inulcer area at 4 weeks ingroups 1 and 2 for thosecompleting (p < 0.05); thisdifference was maintained
Mean residual ulcer area at12 weeks:
1. 27%
2. 9%
p < 0.02
Mean residual ulcer area(healed ulcers excluded):
1. 28%
2. 22%
1. 11 (20%): allergy(4), pain (4),refused/DNA (2),death (1)
2. 15 (29%): allergy(6), pain (3),refused/DNA (3),deterioration (2),arterial disease (1)
Differencebetween groupsnot statisticallysignificant
All tracings were analysedby code numbers only inorder to excludetreatment bias; ulcer areaswere calculated using acomputer graphicsprogram
Continued
TABLE 2 contd Details of included studies
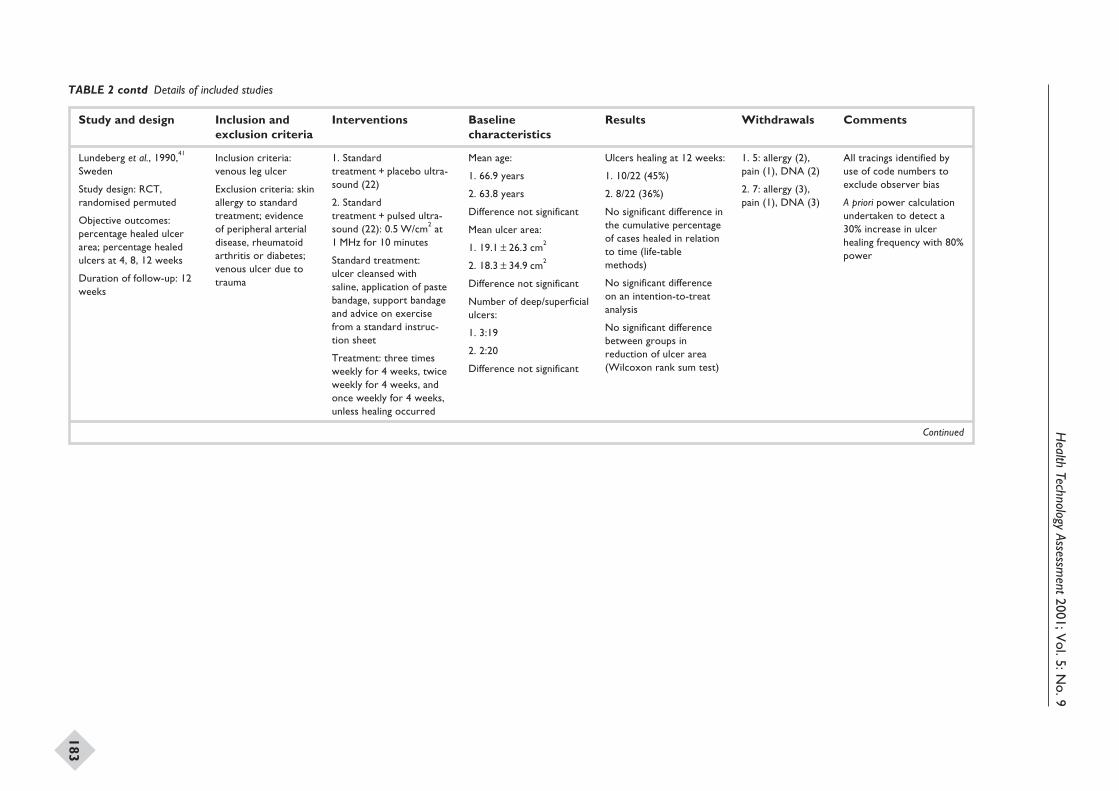
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
183
Study and design Inclusion andexclusion criteria
Interventions Baselinecharacteristics
Results Withdrawals Comments
Lundeberg et al., 1990,41
Sweden
Study design: RCT,randomised permuted
Objective outcomes:percentage healed ulcerarea; percentage healedulcers at 4, 8, 12 weeks
Duration of follow-up: 12weeks
Inclusion criteria:venous leg ulcer
Exclusion criteria: skinallergy to standardtreatment; evidenceof peripheral arterialdisease, rheumatoidarthritis or diabetes;venous ulcer due totrauma
1. Standardtreatment + placebo ultra-sound (22)
2. Standardtreatment + pulsed ultra-sound (22): 0.5 W/cm2 at1 MHz for 10 minutes
Standard treatment:ulcer cleansed withsaline, application of pastebandage, support bandageand advice on exercisefrom a standard instruc-tion sheet
Treatment: three timesweekly for 4 weeks, twiceweekly for 4 weeks, andonce weekly for 4 weeks,unless healing occurred
Mean age:
1. 66.9 years
2. 63.8 years
Difference not significant
Mean ulcer area:
1. 19.1 ± 26.3 cm2
2. 18.3 ± 34.9 cm2
Difference not significant
Number of deep/superficialulcers:
1. 3:19
2. 2:20
Difference not significant
Ulcers healing at 12 weeks:
1. 10/22 (45%)
2. 8/22 (36%)
No significant difference inthe cumulative percentageof cases healed in relationto time (life-tablemethods)
No significant differenceon an intention-to-treatanalysis
No significant differencebetween groups inreduction of ulcer area(Wilcoxon rank sum test)
1. 5: allergy (2),pain (1), DNA (2)
2. 7: allergy (3),pain (1), DNA (3)
All tracings identified byuse of code numbers toexclude observer bias
A priori power calculationundertaken to detect a30% increase in ulcerhealing frequency with 80%power
Continued
TABLE 2 contd Details of included studies
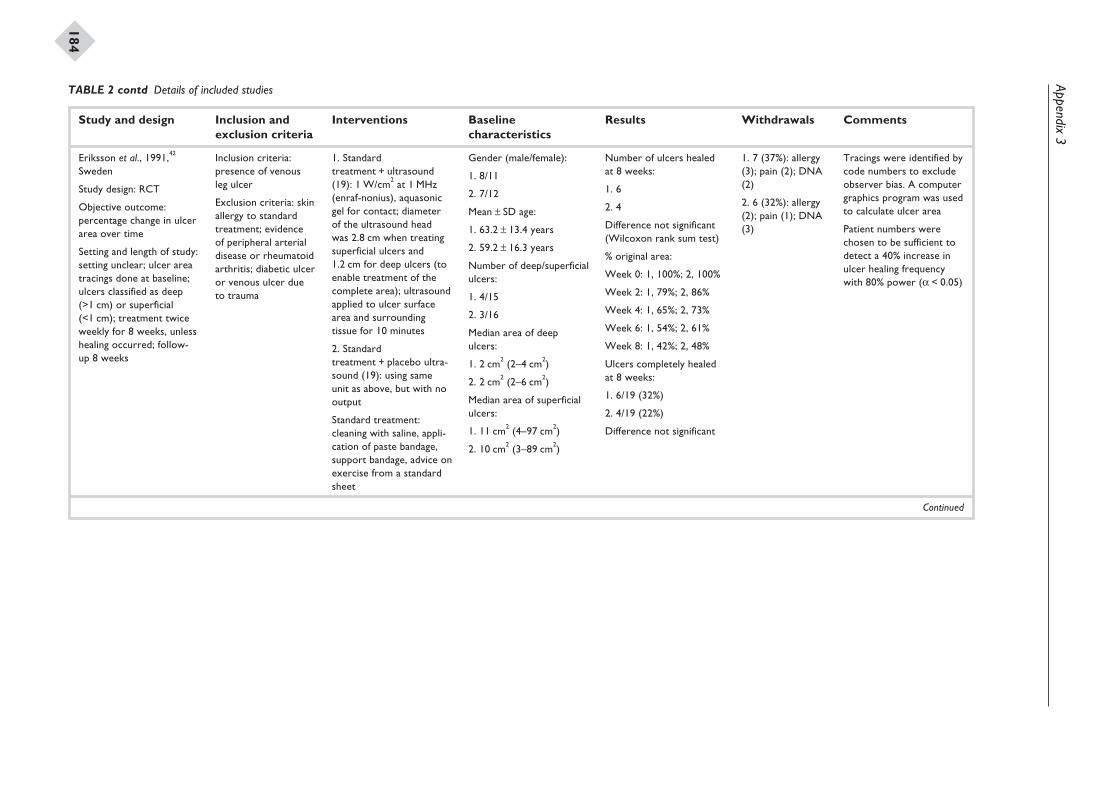
Appendix3
184
Study and design Inclusion andexclusion criteria
Interventions Baselinecharacteristics
Results Withdrawals Comments
Eriksson et al., 1991,42
Sweden
Study design: RCT
Objective outcome:percentage change in ulcerarea over time
Setting and length of study:setting unclear; ulcer areatracings done at baseline;ulcers classified as deep(>1 cm) or superficial(<1 cm); treatment twiceweekly for 8 weeks, unlesshealing occurred; follow-up 8 weeks
Inclusion criteria:presence of venousleg ulcer
Exclusion criteria: skinallergy to standardtreatment; evidenceof peripheral arterialdisease or rheumatoidarthritis; diabetic ulceror venous ulcer dueto trauma
1. Standardtreatment + ultrasound(19): 1 W/cm2 at 1 MHz(enraf-nonius), aquasonicgel for contact; diameterof the ultrasound headwas 2.8 cm when treatingsuperficial ulcers and1.2 cm for deep ulcers (toenable treatment of thecomplete area); ultrasoundapplied to ulcer surfacearea and surroundingtissue for 10 minutes
2. Standardtreatment + placebo ultra-sound (19): using sameunit as above, but with nooutput
Standard treatment:cleaning with saline, appli-cation of paste bandage,support bandage, advice onexercise from a standardsheet
Gender (male/female):
1. 8/11
2. 7/12
Mean ± SD age:
1. 63.2 ± 13.4 years
2. 59.2 ± 16.3 years
Number of deep/superficialulcers:
1. 4/15
2. 3/16
Median area of deepulcers:
1. 2 cm2 (2–4 cm2)
2. 2 cm2 (2–6 cm2)
Median area of superficialulcers:
1. 11 cm2 (4–97 cm2)
2. 10 cm2 (3–89 cm2)
Number of ulcers healedat 8 weeks:
1. 6
2. 4
Difference not significant(Wilcoxon rank sum test)
% original area:
Week 0: 1, 100%; 2, 100%
Week 2: 1, 79%; 2, 86%
Week 4: 1, 65%; 2, 73%
Week 6: 1, 54%; 2, 61%
Week 8: 1, 42%; 2, 48%
Ulcers completely healedat 8 weeks:
1. 6/19 (32%)
2. 4/19 (22%)
Difference not significant
1. 7 (37%): allergy(3); pain (2); DNA(2)
2. 6 (32%): allergy(2); pain (1); DNA(3)
Tracings were identified bycode numbers to excludeobserver bias. A computergraphics program was usedto calculate ulcer area
Patient numbers werechosen to be sufficient todetect a 40% increase inulcer healing frequencywith 80% power (a < 0.05)
Continued
TABLE 2 contd Details of included studies
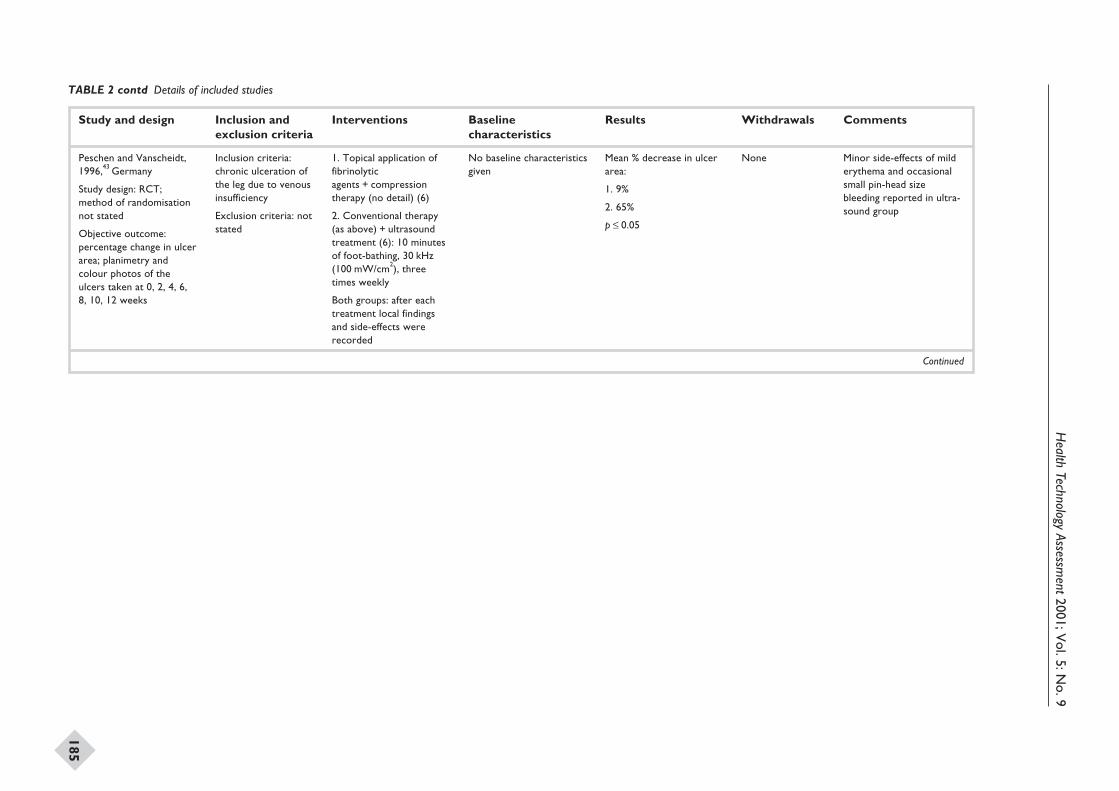
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
185
Study and design Inclusion andexclusion criteria
Interventions Baselinecharacteristics
Results Withdrawals Comments
Peschen and Vanscheidt,1996,43 Germany
Study design: RCT;method of randomisationnot stated
Objective outcome:percentage change in ulcerarea; planimetry andcolour photos of theulcers taken at 0, 2, 4, 6,8, 10, 12 weeks
Inclusion criteria:chronic ulceration ofthe leg due to venousinsufficiency
Exclusion criteria: notstated
1. Topical application offibrinolyticagents + compressiontherapy (no detail) (6)
2. Conventional therapy(as above) + ultrasoundtreatment (6): 10 minutesof foot-bathing, 30 kHz(100 mW/cm2), threetimes weekly
Both groups: after eachtreatment local findingsand side-effects wererecorded
No baseline characteristicsgiven
Mean % decrease in ulcerarea:
1. 9%
2. 65%
p £ 0.05
None Minor side-effects of milderythema and occasionalsmall pin-head sizebleeding reported in ultra-sound group
Continued
TABLE 2 contd Details of included studies
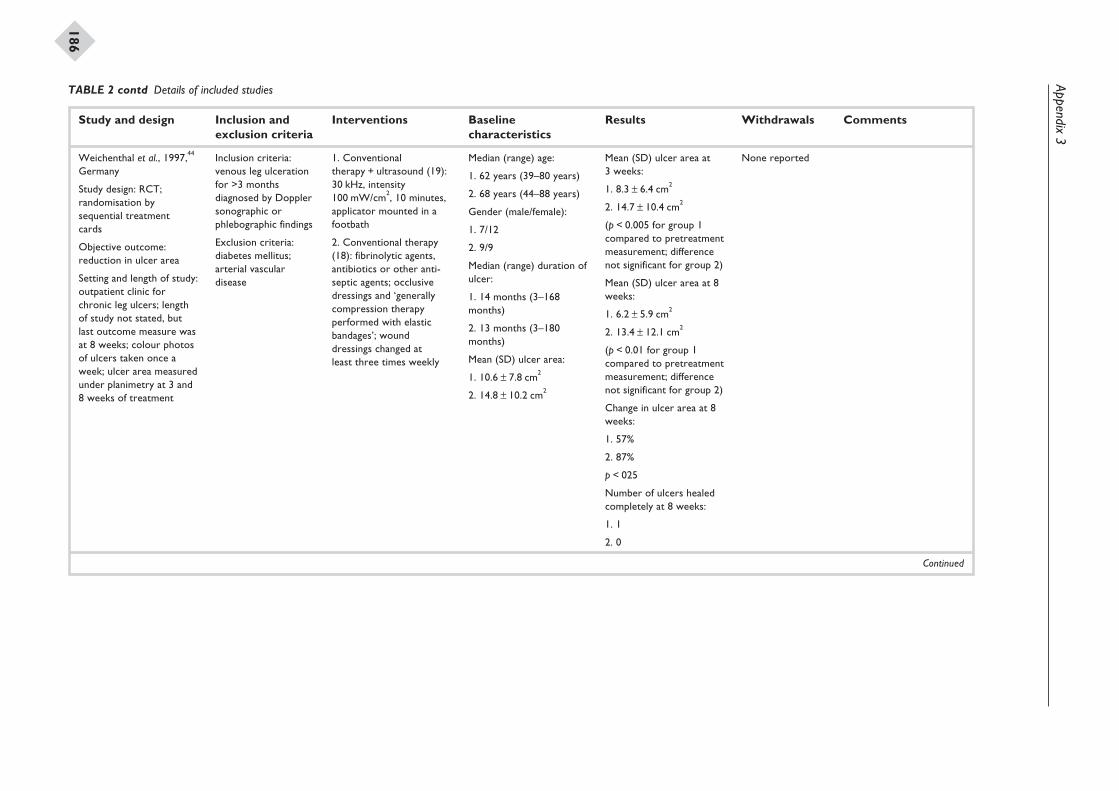
Appendix3
186
Study and design Inclusion andexclusion criteria
Interventions Baselinecharacteristics
Results Withdrawals Comments
Weichenthal et al., 1997,44
Germany
Study design: RCT;randomisation bysequential treatmentcards
Objective outcome:reduction in ulcer area
Setting and length of study:outpatient clinic forchronic leg ulcers; lengthof study not stated, butlast outcome measure wasat 8 weeks; colour photosof ulcers taken once aweek; ulcer area measuredunder planimetry at 3 and8 weeks of treatment
Inclusion criteria:venous leg ulcerationfor >3 monthsdiagnosed by Dopplersonographic orphlebographic findings
Exclusion criteria:diabetes mellitus;arterial vasculardisease
1. Conventionaltherapy + ultrasound (19):30 kHz, intensity100 mW/cm2, 10 minutes,applicator mounted in afootbath
2. Conventional therapy(18): fibrinolytic agents,antibiotics or other anti-septic agents; occlusivedressings and ‘generallycompression therapyperformed with elasticbandages’; wounddressings changed atleast three times weekly
Median (range) age:
1. 62 years (39–80 years)
2. 68 years (44–88 years)
Gender (male/female):
1. 7/12
2. 9/9
Median (range) duration ofulcer:
1. 14 months (3–168months)
2. 13 months (3–180months)
Mean (SD) ulcer area:
1. 10.6 ± 7.8 cm2
2. 14.8 ± 10.2 cm2
Mean (SD) ulcer area at3 weeks:
1. 8.3 ± 6.4 cm2
2. 14.7 ± 10.4 cm2
(p < 0.005 for group 1compared to pretreatmentmeasurement; differencenot significant for group 2)
Mean (SD) ulcer area at 8weeks:
1. 6.2 ± 5.9 cm2
2. 13.4 ± 12.1 cm2
(p < 0.01 for group 1compared to pretreatmentmeasurement; differencenot significant for group 2)
Change in ulcer area at 8weeks:
1. 57%
2. 87%
p < 025
Number of ulcers healedcompletely at 8 weeks:
1. 1
2. 0
None reported
Continued
TABLE 2 contd Details of included studies
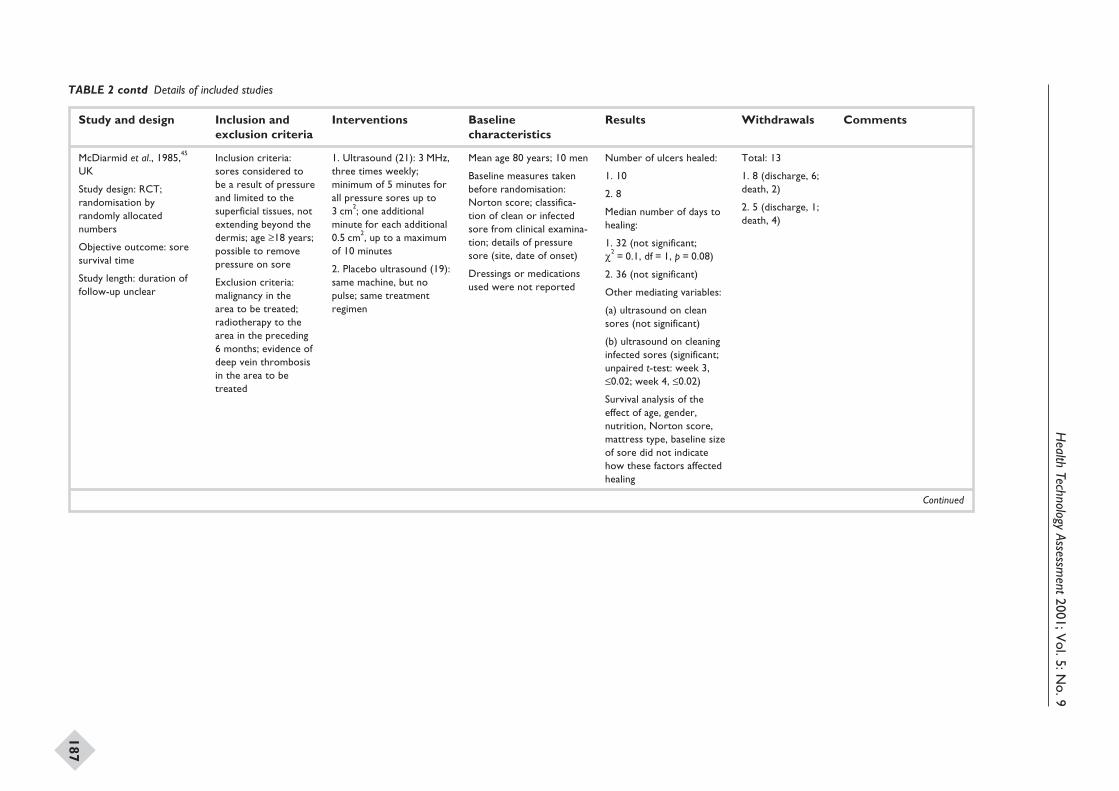
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
187
Study and design Inclusion andexclusion criteria
Interventions Baselinecharacteristics
Results Withdrawals Comments
McDiarmid et al., 1985,45
UK
Study design: RCT;randomisation byrandomly allocatednumbers
Objective outcome: soresurvival time
Study length: duration offollow-up unclear
Inclusion criteria:sores considered tobe a result of pressureand limited to thesuperficial tissues, notextending beyond thedermis; age ≥18 years;possible to removepressure on sore
Exclusion criteria:malignancy in thearea to be treated;radiotherapy to thearea in the preceding6 months; evidence ofdeep vein thrombosisin the area to betreated
1. Ultrasound (21): 3 MHz,three times weekly;minimum of 5 minutes forall pressure sores up to3 cm2; one additionalminute for each additional0.5 cm2, up to a maximumof 10 minutes
2. Placebo ultrasound (19):same machine, but nopulse; same treatmentregimen
Mean age 80 years; 10 men
Baseline measures takenbefore randomisation:Norton score; classifica-tion of clean or infectedsore from clinical examina-tion; details of pressuresore (site, date of onset)
Dressings or medicationsused were not reported
Number of ulcers healed:
1. 10
2. 8
Median number of days tohealing:
1. 32 (not significant;c2 = 0.1, df = 1, p = 0.08)
2. 36 (not significant)
Other mediating variables:
(a) ultrasound on cleansores (not significant)
(b) ultrasound on cleaninginfected sores (significant;unpaired t-test: week 3,£0.02; week 4, £0.02)
Survival analysis of theeffect of age, gender,nutrition, Norton score,mattress type, baseline sizeof sore did not indicatehow these factors affectedhealing
Total: 13
1. 8 (discharge, 6;death, 2)
2. 5 (discharge, 1;death, 4)
Continued
TABLE 2 contd Details of included studies
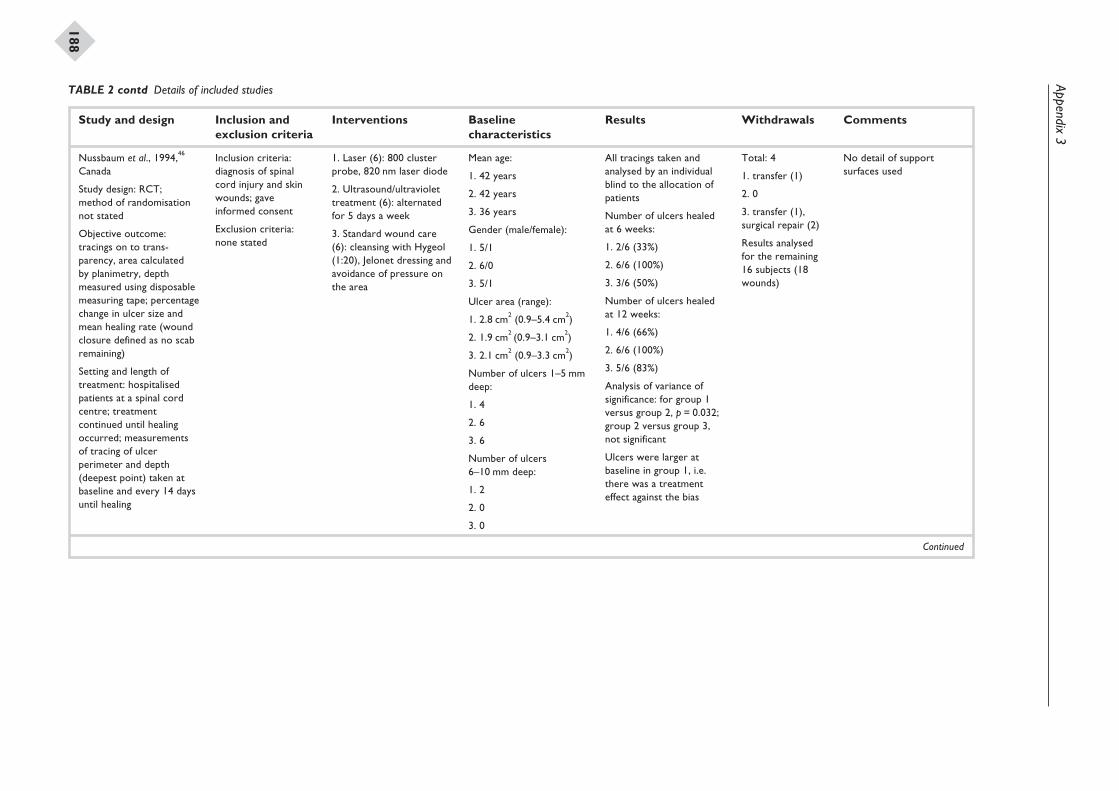
Appendix3
188
Study and design Inclusion andexclusion criteria
Interventions Baselinecharacteristics
Results Withdrawals Comments
Nussbaum et al., 1994,46
Canada
Study design: RCT;method of randomisationnot stated
Objective outcome:tracings on to trans-parency, area calculatedby planimetry, depthmeasured using disposablemeasuring tape; percentagechange in ulcer size andmean healing rate (woundclosure defined as no scabremaining)
Setting and length oftreatment: hospitalisedpatients at a spinal cordcentre; treatmentcontinued until healingoccurred; measurementsof tracing of ulcerperimeter and depth(deepest point) taken atbaseline and every 14 daysuntil healing
Inclusion criteria:diagnosis of spinalcord injury and skinwounds; gaveinformed consent
Exclusion criteria:none stated
1. Laser (6): 800 clusterprobe, 820 nm laser diode
2. Ultrasound/ultraviolettreatment (6): alternatedfor 5 days a week
3. Standard wound care(6): cleansing with Hygeol(1:20), Jelonet dressing andavoidance of pressure onthe area
Mean age:
1. 42 years
2. 42 years
3. 36 years
Gender (male/female):
1. 5/1
2. 6/0
3. 5/1
Ulcer area (range):
1. 2.8 cm2 (0.9–5.4 cm2)
2. 1.9 cm2 (0.9–3.1 cm2)
3. 2.1 cm2 (0.9–3.3 cm2)
Number of ulcers 1–5 mmdeep:
1. 4
2. 6
3. 6
Number of ulcers6–10 mm deep:
1. 2
2. 0
3. 0
All tracings taken andanalysed by an individualblind to the allocation ofpatients
Number of ulcers healedat 6 weeks:
1. 2/6 (33%)
2. 6/6 (100%)
3. 3/6 (50%)
Number of ulcers healedat 12 weeks:
1. 4/6 (66%)
2. 6/6 (100%)
3. 5/6 (83%)
Analysis of variance ofsignificance: for group 1versus group 2, p = 0.032;group 2 versus group 3,not significant
Ulcers were larger atbaseline in group 1, i.e.there was a treatmenteffect against the bias
Total: 4
1. transfer (1)
2. 0
3. transfer (1),surgical repair (2)
Results analysedfor the remaining16 subjects (18wounds)
No detail of supportsurfaces used
Continued
TABLE 2 contd Details of included studies
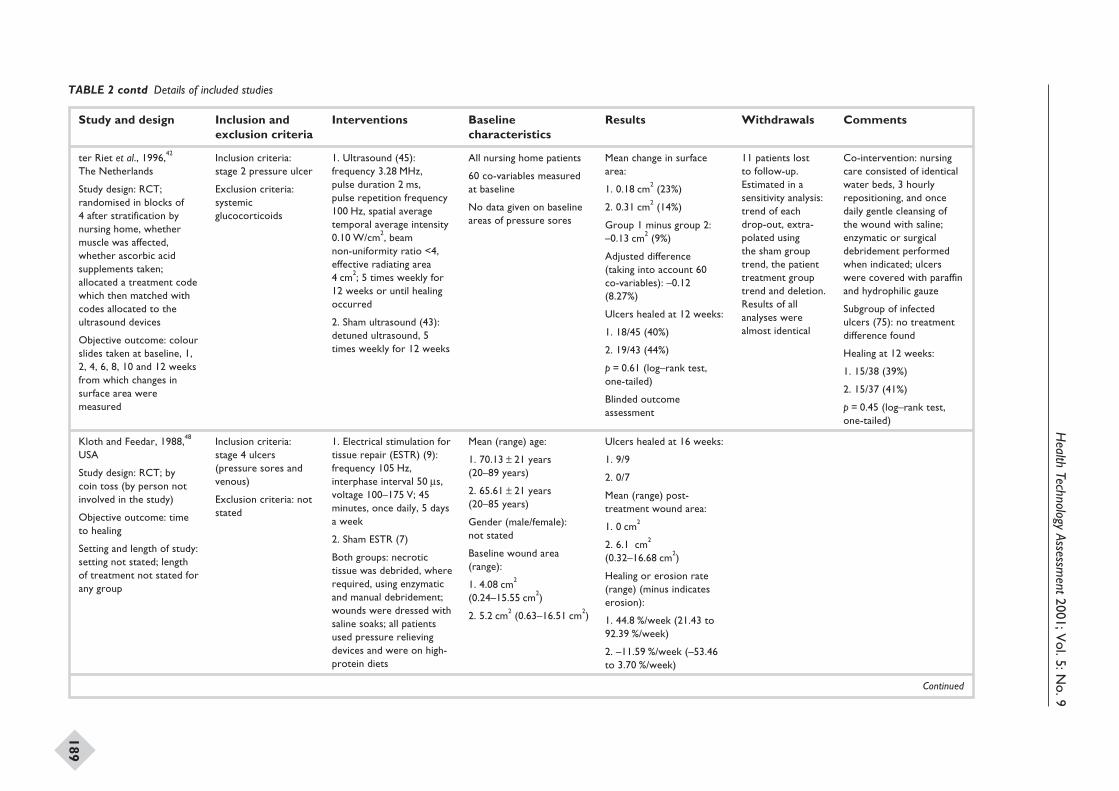
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
189
Study and design Inclusion andexclusion criteria
Interventions Baselinecharacteristics
Results Withdrawals Comments
ter Riet et al., 1996,42
The Netherlands
Study design: RCT;randomised in blocks of4 after stratification bynursing home, whethermuscle was affected,whether ascorbic acidsupplements taken;allocated a treatment codewhich then matched withcodes allocated to theultrasound devices
Objective outcome: colourslides taken at baseline, 1,2, 4, 6, 8, 10 and 12 weeksfrom which changes insurface area weremeasured
Inclusion criteria:stage 2 pressure ulcer
Exclusion criteria:systemicglucocorticoids
1. Ultrasound (45):frequency 3.28 MHz,pulse duration 2 ms,pulse repetition frequency100 Hz, spatial averagetemporal average intensity0.10 W/cm2, beamnon-uniformity ratio <4,effective radiating area4 cm2; 5 times weekly for12 weeks or until healingoccurred
2. Sham ultrasound (43):detuned ultrasound, 5times weekly for 12 weeks
All nursing home patients
60 co-variables measuredat baseline
No data given on baselineareas of pressure sores
Mean change in surfacearea:
1. 0.18 cm2 (23%)
2. 0.31 cm2 (14%)
Group 1 minus group 2:–0.13 cm2 (9%)
Adjusted difference(taking into account 60co-variables): –0.12(8.27%)
Ulcers healed at 12 weeks:
1. 18/45 (40%)
2. 19/43 (44%)
p = 0.61 (log–rank test,one-tailed)
Blinded outcomeassessment
11 patients lostto follow-up.Estimated in asensitivity analysis:trend of eachdrop-out, extra-polated usingthe sham grouptrend, the patienttreatment grouptrend and deletion.Results of allanalyses werealmost identical
Co-intervention: nursingcare consisted of identicalwater beds, 3 hourlyrepositioning, and oncedaily gentle cleansing ofthe wound with saline;enzymatic or surgicaldebridement performedwhen indicated; ulcerswere covered with paraffinand hydrophilic gauze
Subgroup of infectedulcers (75): no treatmentdifference found
Healing at 12 weeks:
1. 15/38 (39%)
2. 15/37 (41%)
p = 0.45 (log–rank test,one-tailed)
Kloth and Feedar, 1988,48
USA
Study design: RCT; bycoin toss (by person notinvolved in the study)
Objective outcome: timeto healing
Setting and length of study:setting not stated; lengthof treatment not stated forany group
Inclusion criteria:stage 4 ulcers(pressure sores andvenous)
Exclusion criteria: notstated
1. Electrical stimulation fortissue repair (ESTR) (9):frequency 105 Hz,interphase interval 50 ms,voltage 100–175 V; 45minutes, once daily, 5 daysa week
2. Sham ESTR (7)
Both groups: necrotictissue was debrided, whererequired, using enzymaticand manual debridement;wounds were dressed withsaline soaks; all patientsused pressure relievingdevices and were on high-protein diets
Mean (range) age:
1. 70.13 ± 21 years(20–89 years)
2. 65.61 ± 21 years(20–85 years)
Gender (male/female):not stated
Baseline wound area(range):
1. 4.08 cm2
(0.24–15.55 cm2)
2. 5.2 cm2 (0.63–16.51 cm2)
Ulcers healed at 16 weeks:
1. 9/9
2. 0/7
Mean (range) post-treatment wound area:
1. 0 cm2
2. 6.1 cm2
(0.32–16.68 cm2)
Healing or erosion rate(range) (minus indicateserosion):
1. 44.8 %/week (21.43 to92.39 %/week)
2. –11.59 %/week (–53.46to 3.70 %/week)
Continued
TABLE 2 contd Details of included studies
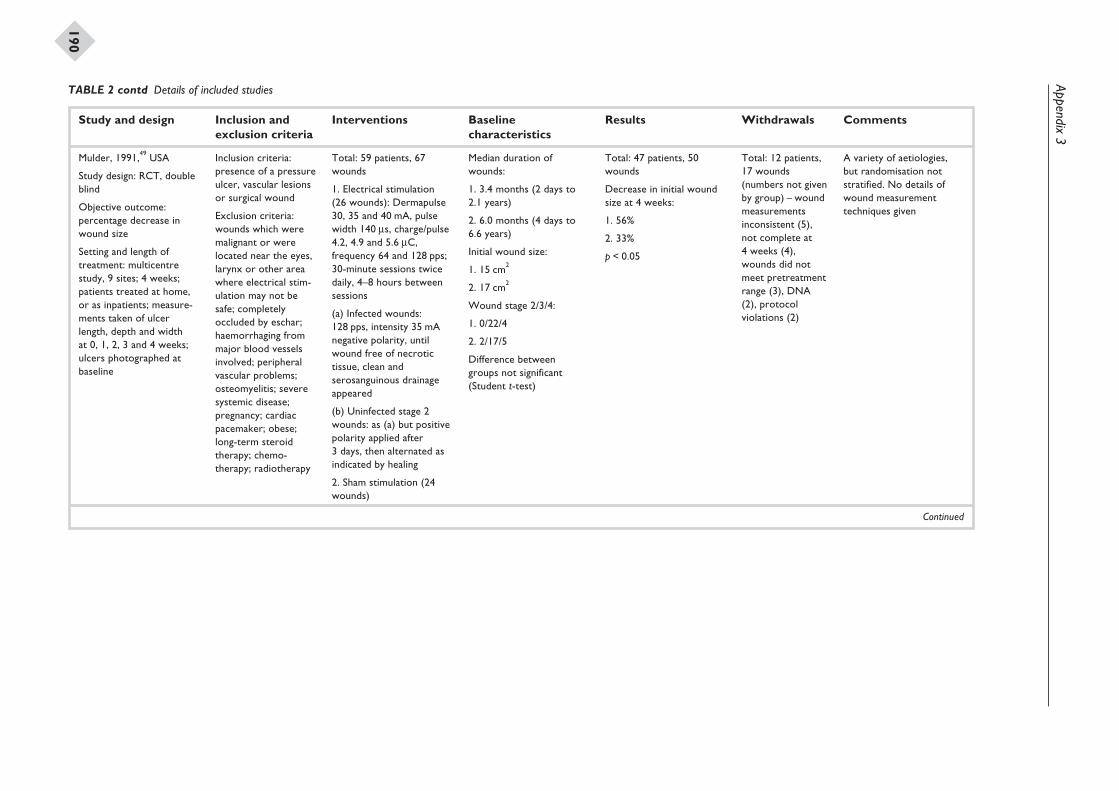
Appendix3
190
Study and design Inclusion andexclusion criteria
Interventions Baselinecharacteristics
Results Withdrawals Comments
Mulder, 1991,49 USA
Study design: RCT, doubleblind
Objective outcome:percentage decrease inwound size
Setting and length oftreatment: multicentrestudy, 9 sites; 4 weeks;patients treated at home,or as inpatients; measure-ments taken of ulcerlength, depth and widthat 0, 1, 2, 3 and 4 weeks;ulcers photographed atbaseline
Inclusion criteria:presence of a pressureulcer, vascular lesionsor surgical wound
Exclusion criteria:wounds which weremalignant or werelocated near the eyes,larynx or other areawhere electrical stim-ulation may not besafe; completelyoccluded by eschar;haemorrhaging frommajor blood vesselsinvolved; peripheralvascular problems;osteomyelitis; severesystemic disease;pregnancy; cardiacpacemaker; obese;long-term steroidtherapy; chemo-therapy; radiotherapy
Total: 59 patients, 67wounds
1. Electrical stimulation(26 wounds): Dermapulse30, 35 and 40 mA, pulsewidth 140 ms, charge/pulse4.2, 4.9 and 5.6 mC,frequency 64 and 128 pps;30-minute sessions twicedaily, 4–8 hours betweensessions
(a) Infected wounds:128 pps, intensity 35 mAnegative polarity, untilwound free of necrotictissue, clean andserosanguinous drainageappeared
(b) Uninfected stage 2wounds: as (a) but positivepolarity applied after3 days, then alternated asindicated by healing
2. Sham stimulation (24wounds)
Median duration ofwounds:
1. 3.4 months (2 days to2.1 years)
2. 6.0 months (4 days to6.6 years)
Initial wound size:
1. 15 cm2
2. 17 cm2
Wound stage 2/3/4:
1. 0/22/4
2. 2/17/5
Difference betweengroups not significant(Student t-test)
Total: 47 patients, 50wounds
Decrease in initial woundsize at 4 weeks:
1. 56%
2. 33%
p < 0.05
Total: 12 patients,17 wounds(numbers not givenby group) – woundmeasurementsinconsistent (5),not complete at4 weeks (4),wounds did notmeet pretreatmentrange (3), DNA(2), protocolviolations (2)
A variety of aetiologies,but randomisation notstratified. No details ofwound measurementtechniques given
Continued
TABLE 2 contd Details of included studies
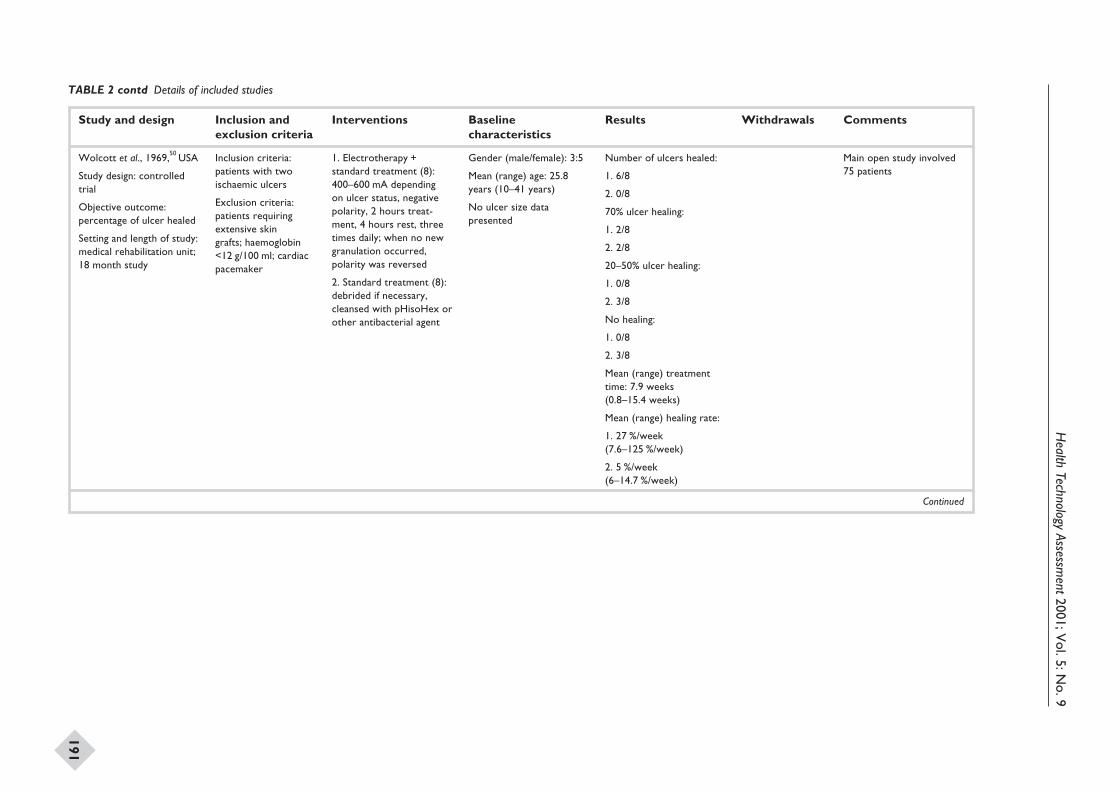
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
191
Study and design Inclusion andexclusion criteria
Interventions Baselinecharacteristics
Results Withdrawals Comments
Wolcott et al., 1969,50 USA
Study design: controlledtrial
Objective outcome:percentage of ulcer healed
Setting and length of study:medical rehabilitation unit;18 month study
Inclusion criteria:patients with twoischaemic ulcers
Exclusion criteria:patients requiringextensive skingrafts; haemoglobin<12 g/100 ml; cardiacpacemaker
1. Electrotherapy +standard treatment (8):400–600 mA dependingon ulcer status, negativepolarity, 2 hours treat-ment, 4 hours rest, threetimes daily; when no newgranulation occurred,polarity was reversed
2. Standard treatment (8):debrided if necessary,cleansed with pHisoHex orother antibacterial agent
Gender (male/female): 3:5
Mean (range) age: 25.8years (10–41 years)
No ulcer size datapresented
Number of ulcers healed:
1. 6/8
2. 0/8
70% ulcer healing:
1. 2/8
2. 2/8
20–50% ulcer healing:
1. 0/8
2. 3/8
No healing:
1. 0/8
2. 3/8
Mean (range) treatmenttime: 7.9 weeks(0.8–15.4 weeks)
Mean (range) healing rate:
1. 27 %/week(7.6–125 %/week)
2. 5 %/week(6–14.7 %/week)
Main open study involved75 patients
Continued
TABLE 2 contd Details of included studies
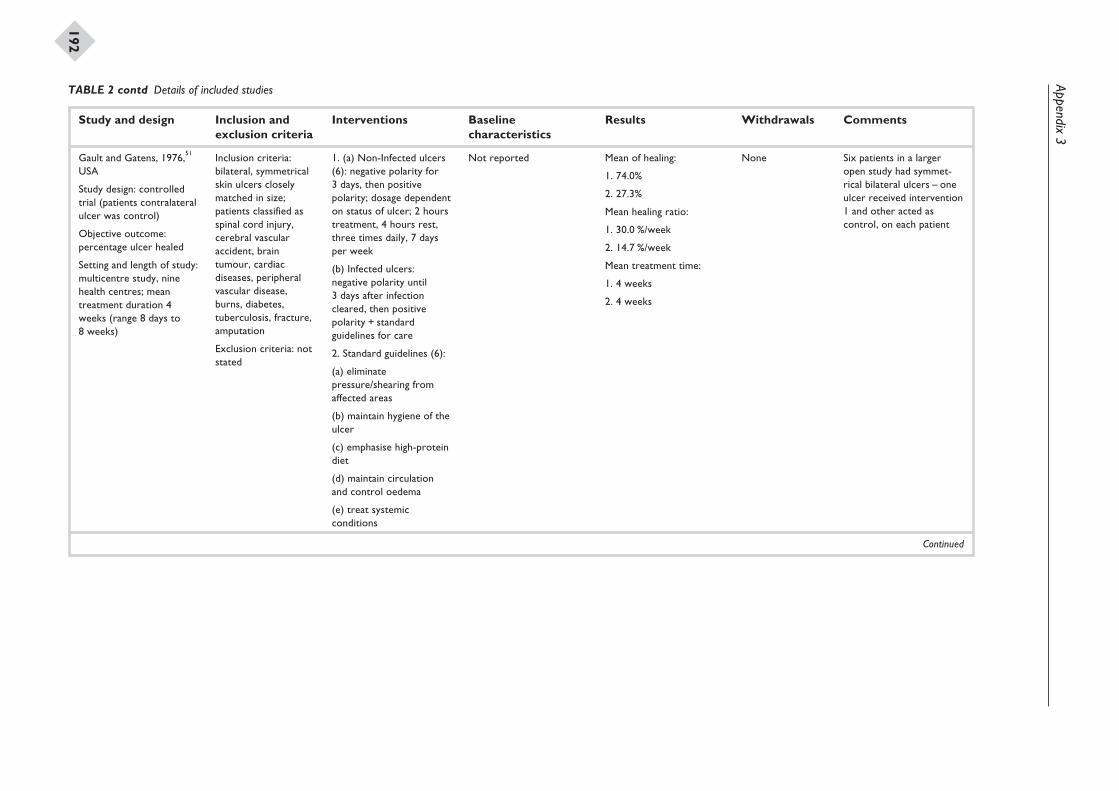
Appendix3
192
Study and design Inclusion andexclusion criteria
Interventions Baselinecharacteristics
Results Withdrawals Comments
Gault and Gatens, 1976,51
USA
Study design: controlledtrial (patients contralateralulcer was control)
Objective outcome:percentage ulcer healed
Setting and length of study:multicentre study, ninehealth centres; meantreatment duration 4weeks (range 8 days to8 weeks)
Inclusion criteria:bilateral, symmetricalskin ulcers closelymatched in size;patients classified asspinal cord injury,cerebral vascularaccident, braintumour, cardiacdiseases, peripheralvascular disease,burns, diabetes,tuberculosis, fracture,amputation
Exclusion criteria: notstated
1. (a) Non-Infected ulcers(6): negative polarity for3 days, then positivepolarity; dosage dependenton status of ulcer; 2 hourstreatment, 4 hours rest,three times daily, 7 daysper week
(b) Infected ulcers:negative polarity until3 days after infectioncleared, then positivepolarity + standardguidelines for care
2. Standard guidelines (6):
(a) eliminatepressure/shearing fromaffected areas
(b) maintain hygiene of theulcer
(c) emphasise high-proteindiet
(d) maintain circulationand control oedema
(e) treat systemicconditions
Not reported Mean of healing:
1. 74.0%
2. 27.3%
Mean healing ratio:
1. 30.0 %/week
2. 14.7 %/week
Mean treatment time:
1. 4 weeks
2. 4 weeks
None Six patients in a largeropen study had symmet-rical bilateral ulcers – oneulcer received intervention1 and other acted ascontrol, on each patient
Continued
TABLE 2 contd Details of included studies
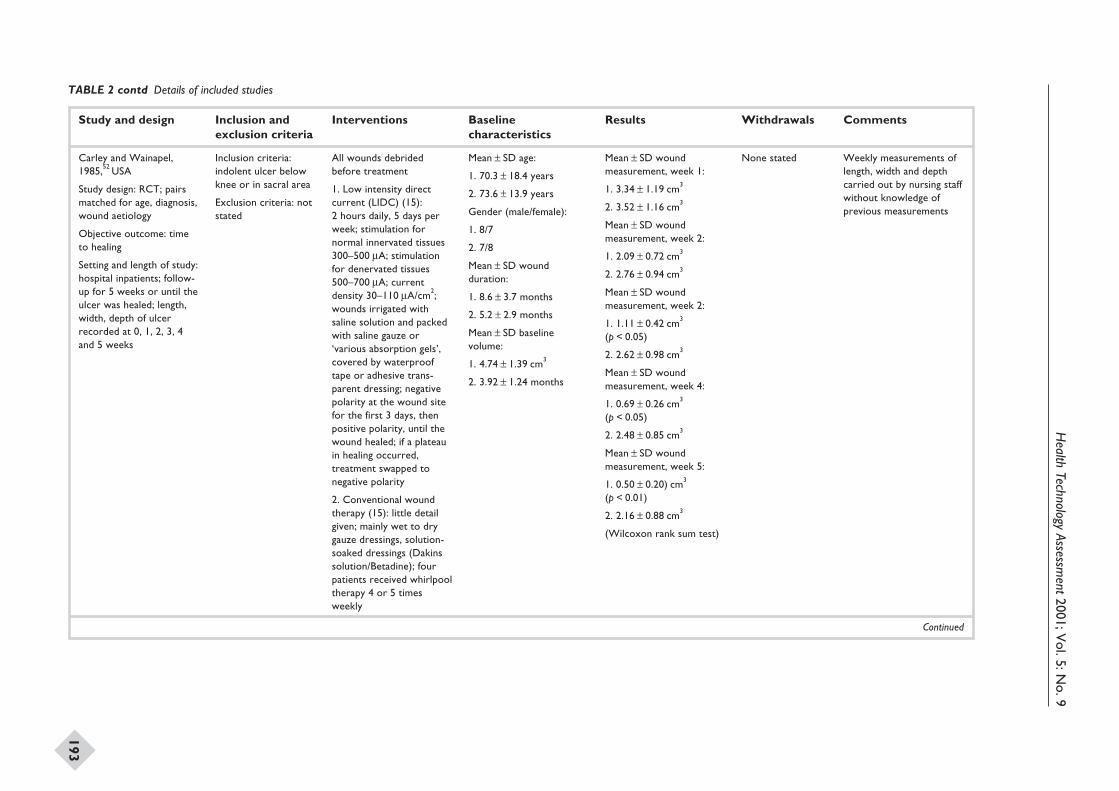
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
193
Study and design Inclusion andexclusion criteria
Interventions Baselinecharacteristics
Results Withdrawals Comments
Carley and Wainapel,1985,52 USA
Study design: RCT; pairsmatched for age, diagnosis,wound aetiology
Objective outcome: timeto healing
Setting and length of study:hospital inpatients; follow-up for 5 weeks or until theulcer was healed; length,width, depth of ulcerrecorded at 0, 1, 2, 3, 4and 5 weeks
Inclusion criteria:indolent ulcer belowknee or in sacral area
Exclusion criteria: notstated
All wounds debridedbefore treatment
1. Low intensity directcurrent (LIDC) (15):2 hours daily, 5 days perweek; stimulation fornormal innervated tissues300–500 mA; stimulationfor denervated tissues500–700 mA; currentdensity 30–110 mA/cm2;wounds irrigated withsaline solution and packedwith saline gauze or‘various absorption gels’,covered by waterprooftape or adhesive trans-parent dressing; negativepolarity at the wound sitefor the first 3 days, thenpositive polarity, until thewound healed; if a plateauin healing occurred,treatment swapped tonegative polarity
2. Conventional woundtherapy (15): little detailgiven; mainly wet to drygauze dressings, solution-soaked dressings (Dakinssolution/Betadine); fourpatients received whirlpooltherapy 4 or 5 timesweekly
Mean ± SD age:
1. 70.3 ± 18.4 years
2. 73.6 ± 13.9 years
Gender (male/female):
1. 8/7
2. 7/8
Mean ± SD woundduration:
1. 8.6 ± 3.7 months
2. 5.2 ± 2.9 months
Mean ± SD baselinevolume:
1. 4.74 ± 1.39 cm3
2. 3.92 ± 1.24 months
Mean ± SD woundmeasurement, week 1:
1. 3.34 ± 1.19 cm3
2. 3.52 ± 1.16 cm3
Mean ± SD woundmeasurement, week 2:
1. 2.09 ± 0.72 cm3
2. 2.76 ± 0.94 cm3
Mean ± SD woundmeasurement, week 2:
1. 1.11 ± 0.42 cm3
(p < 0.05)
2. 2.62 ± 0.98 cm3
Mean ± SD woundmeasurement, week 4:
1. 0.69 ± 0.26 cm3
(p < 0.05)
2. 2.48 ± 0.85 cm3
Mean ± SD woundmeasurement, week 5:
1. 0.50 ± 0.20) cm3
(p < 0.01)
2. 2.16 ± 0.88 cm3
(Wilcoxon rank sum test)
None stated Weekly measurements oflength, width and depthcarried out by nursing staffwithout knowledge ofprevious measurements
Continued
TABLE 2 contd Details of included studies
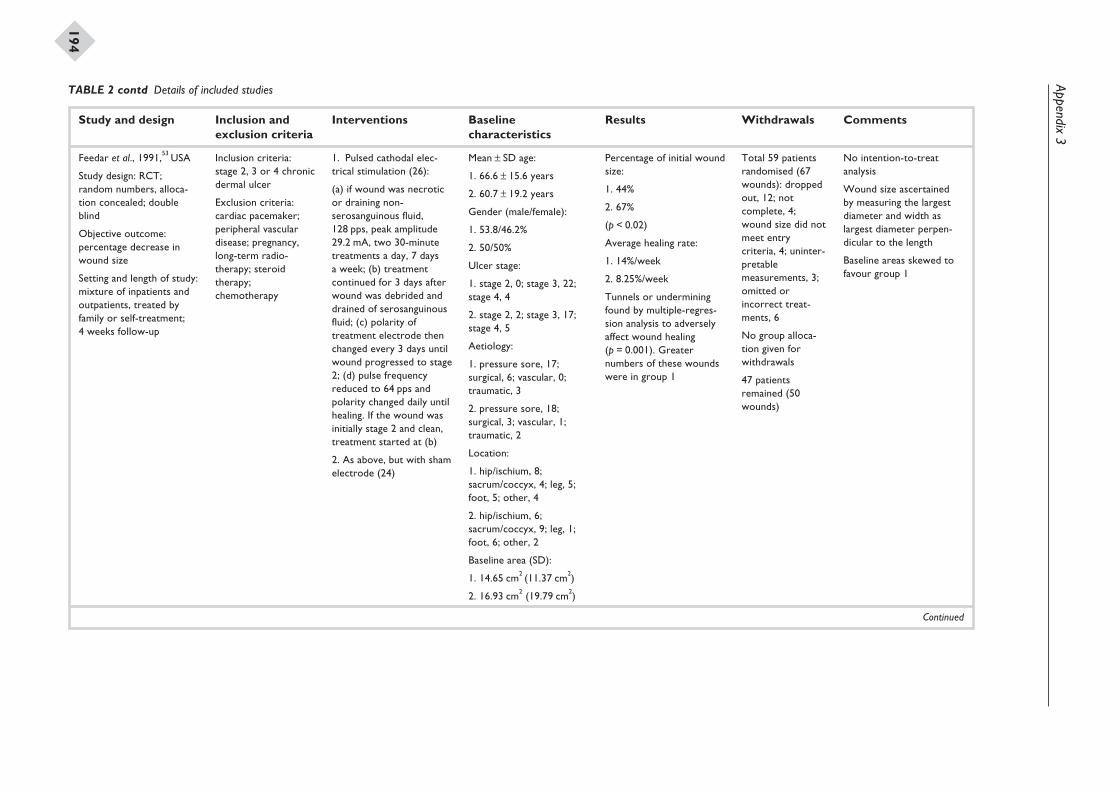
Appendix3
194
Study and design Inclusion andexclusion criteria
Interventions Baselinecharacteristics
Results Withdrawals Comments
Feedar et al., 1991,53 USA
Study design: RCT;random numbers, alloca-tion concealed; doubleblind
Objective outcome:percentage decrease inwound size
Setting and length of study:mixture of inpatients andoutpatients, treated byfamily or self-treatment;4 weeks follow-up
Inclusion criteria:stage 2, 3 or 4 chronicdermal ulcer
Exclusion criteria:cardiac pacemaker;peripheral vasculardisease; pregnancy,long-term radio-therapy; steroidtherapy;chemotherapy
1. Pulsed cathodal elec-trical stimulation (26):
(a) if wound was necroticor draining non-serosanguinous fluid,128 pps, peak amplitude29.2 mA, two 30-minutetreatments a day, 7 daysa week; (b) treatmentcontinued for 3 days afterwound was debrided anddrained of serosanguinousfluid; (c) polarity oftreatment electrode thenchanged every 3 days untilwound progressed to stage2; (d) pulse frequencyreduced to 64 pps andpolarity changed daily untilhealing. If the wound wasinitially stage 2 and clean,treatment started at (b)
2. As above, but with shamelectrode (24)
Mean ± SD age:
1. 66.6 ± 15.6 years
2. 60.7 ± 19.2 years
Gender (male/female):
1. 53.8/46.2%
2. 50/50%
Ulcer stage:
1. stage 2, 0; stage 3, 22;stage 4, 4
2. stage 2, 2; stage 3, 17;stage 4, 5
Aetiology:
1. pressure sore, 17;surgical, 6; vascular, 0;traumatic, 3
2. pressure sore, 18;surgical, 3; vascular, 1;traumatic, 2
Location:
1. hip/ischium, 8;sacrum/coccyx, 4; leg, 5;foot, 5; other, 4
2. hip/ischium, 6;sacrum/coccyx, 9; leg, 1;foot, 6; other, 2
Baseline area (SD):
1. 14.65 cm2 (11.37 cm2)
2. 16.93 cm2 (19.79 cm2)
Percentage of initial woundsize:
1. 44%
2. 67%
(p < 0.02)
Average healing rate:
1. 14%/week
2. 8.25%/week
Tunnels or underminingfound by multiple-regres-sion analysis to adverselyaffect wound healing(p = 0.001). Greaternumbers of these woundswere in group 1
Total 59 patientsrandomised (67wounds): droppedout, 12; notcomplete, 4;wound size did notmeet entrycriteria, 4; uninter-pretablemeasurements, 3;omitted orincorrect treat-ments, 6
No group alloca-tion given forwithdrawals
47 patientsremained (50wounds)
No intention-to-treatanalysis
Wound size ascertainedby measuring the largestdiameter and width aslargest diameter perpen-dicular to the length
Baseline areas skewed tofavour group 1
Continued
TABLE 2 contd Details of included studies
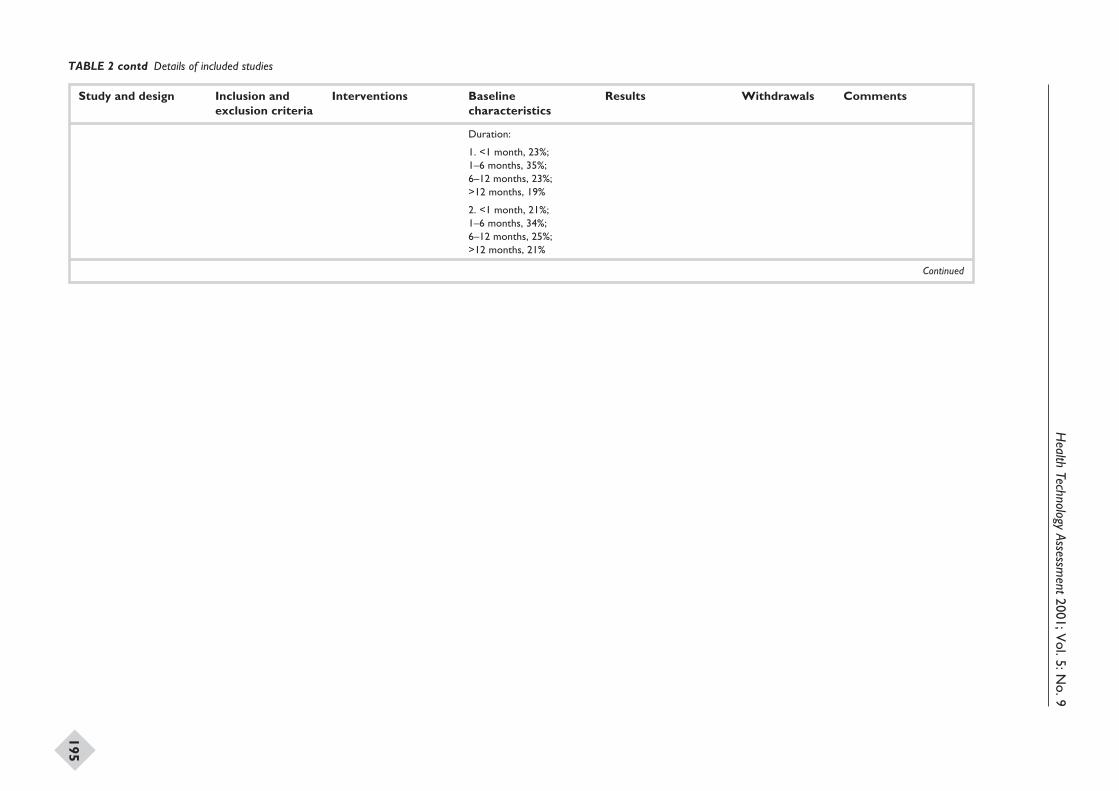
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
195
Study and design Inclusion andexclusion criteria
Interventions Baselinecharacteristics
Results Withdrawals Comments
Duration:
1. <1 month, 23%;1–6 months, 35%;6–12 months, 23%;>12 months, 19%
2. <1 month, 21%;1–6 months, 34%;6–12 months, 25%;>12 months, 21%
Continued
TABLE 2 contd Details of included studies
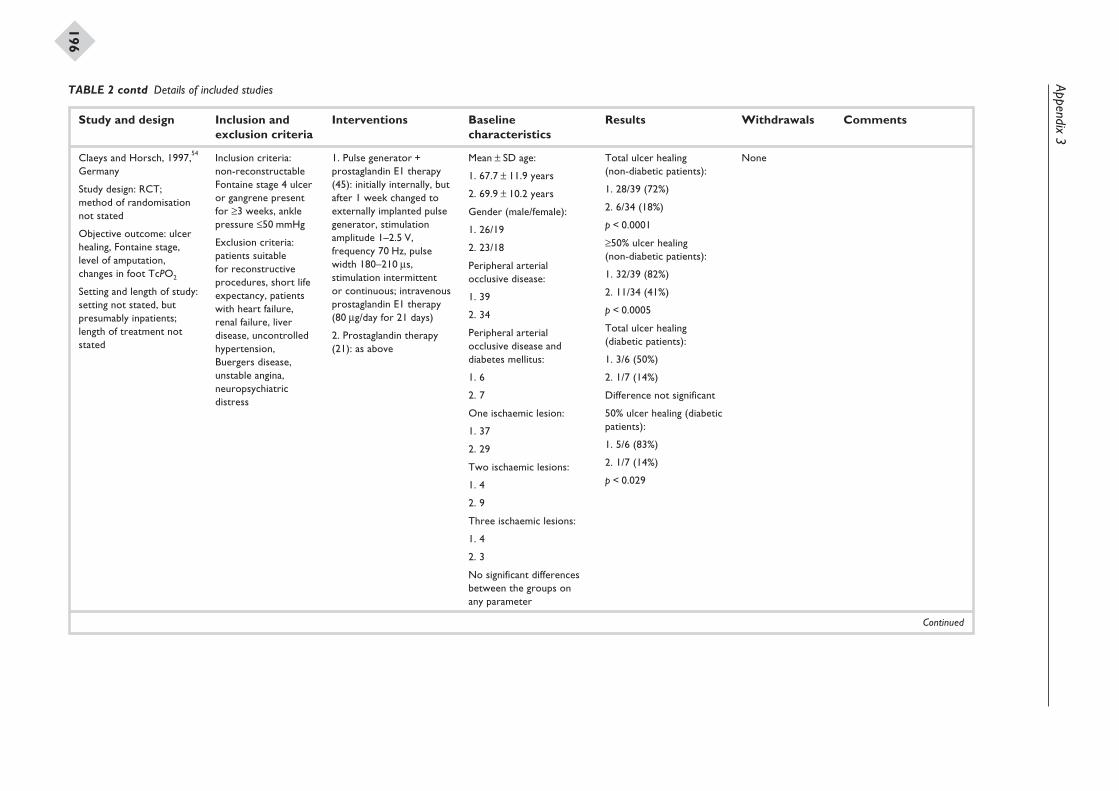
Appendix3
196
Study and design Inclusion andexclusion criteria
Interventions Baselinecharacteristics
Results Withdrawals Comments
Claeys and Horsch, 1997,54
Germany
Study design: RCT;method of randomisationnot stated
Objective outcome: ulcerhealing, Fontaine stage,level of amputation,changes in foot TcPO2
Setting and length of study:setting not stated, butpresumably inpatients;length of treatment notstated
Inclusion criteria:non-reconstructableFontaine stage 4 ulceror gangrene presentfor ≥3 weeks, anklepressure £50 mmHg
Exclusion criteria:patients suitablefor reconstructiveprocedures, short lifeexpectancy, patientswith heart failure,renal failure, liverdisease, uncontrolledhypertension,Buergers disease,unstable angina,neuropsychiatricdistress
1. Pulse generator +prostaglandin E1 therapy(45): initially internally, butafter 1 week changed toexternally implanted pulsegenerator, stimulationamplitude 1–2.5 V,frequency 70 Hz, pulsewidth 180–210 ms,stimulation intermittentor continuous; intravenousprostaglandin E1 therapy(80 mg/day for 21 days)
2. Prostaglandin therapy(21): as above
Mean ± SD age:
1. 67.7 ± 11.9 years
2. 69.9 ± 10.2 years
Gender (male/female):
1. 26/19
2. 23/18
Peripheral arterialocclusive disease:
1. 39
2. 34
Peripheral arterialocclusive disease anddiabetes mellitus:
1. 6
2. 7
One ischaemic lesion:
1. 37
2. 29
Two ischaemic lesions:
1. 4
2. 9
Three ischaemic lesions:
1. 4
2. 3
No significant differencesbetween the groups onany parameter
Total ulcer healing(non-diabetic patients):
1. 28/39 (72%)
2. 6/34 (18%)
p < 0.0001
≥50% ulcer healing(non-diabetic patients):
1. 32/39 (82%)
2. 11/34 (41%)
p < 0.0005
Total ulcer healing(diabetic patients):
1. 3/6 (50%)
2. 1/7 (14%)
Difference not significant
50% ulcer healing (diabeticpatients):
1. 5/6 (83%)
2. 1/7 (14%)
p < 0.029
None
Continued
TABLE 2 contd Details of included studies
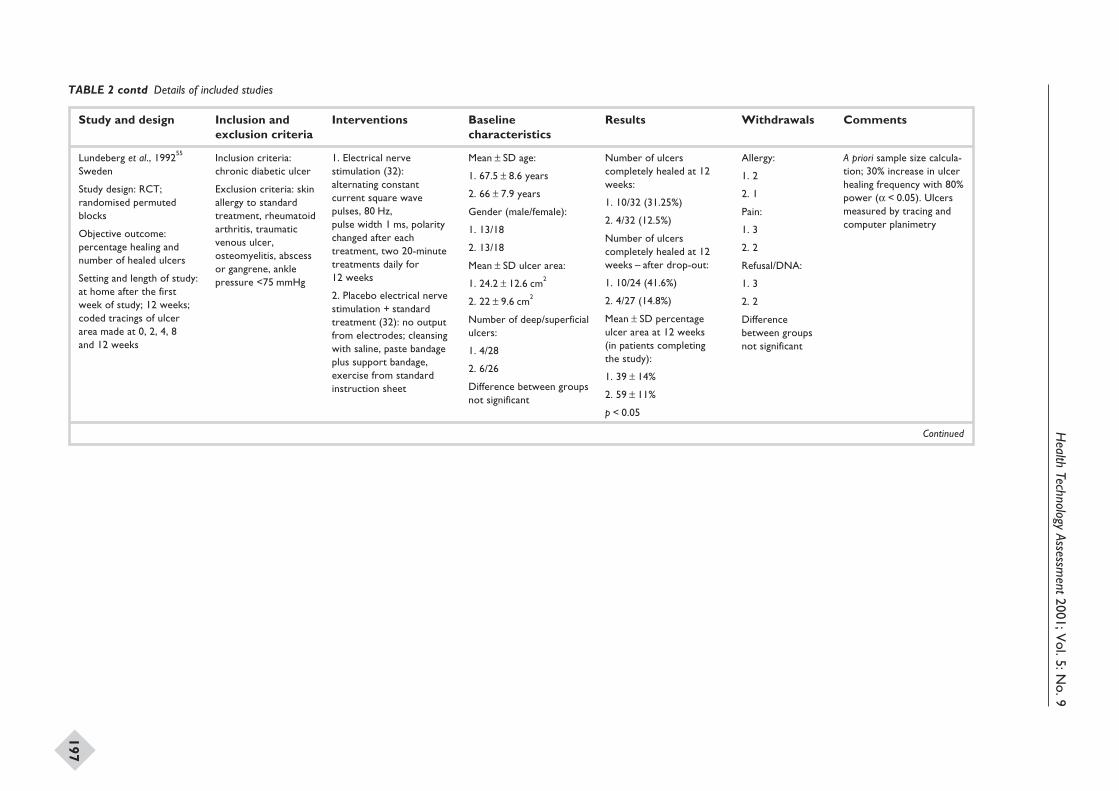
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
197
Study and design Inclusion andexclusion criteria
Interventions Baselinecharacteristics
Results Withdrawals Comments
Lundeberg et al., 199255
Sweden
Study design: RCT;randomised permutedblocks
Objective outcome:percentage healing andnumber of healed ulcers
Setting and length of study:at home after the firstweek of study; 12 weeks;coded tracings of ulcerarea made at 0, 2, 4, 8and 12 weeks
Inclusion criteria:chronic diabetic ulcer
Exclusion criteria: skinallergy to standardtreatment, rheumatoidarthritis, traumaticvenous ulcer,osteomyelitis, abscessor gangrene, anklepressure <75 mmHg
1. Electrical nervestimulation (32):alternating constantcurrent square wavepulses, 80 Hz,pulse width 1 ms, polaritychanged after eachtreatment, two 20-minutetreatments daily for12 weeks
2. Placebo electrical nervestimulation + standardtreatment (32): no outputfrom electrodes; cleansingwith saline, paste bandageplus support bandage,exercise from standardinstruction sheet
Mean ± SD age:
1. 67.5 ± 8.6 years
2. 66 ± 7.9 years
Gender (male/female):
1. 13/18
2. 13/18
Mean ± SD ulcer area:
1. 24.2 ± 12.6 cm2
2. 22 ± 9.6 cm2
Number of deep/superficialulcers:
1. 4/28
2. 6/26
Difference between groupsnot significant
Number of ulcerscompletely healed at 12weeks:
1. 10/32 (31.25%)
2. 4/32 (12.5%)
Number of ulcerscompletely healed at 12weeks – after drop-out:
1. 10/24 (41.6%)
2. 4/27 (14.8%)
Mean ± SD percentageulcer area at 12 weeks(in patients completingthe study):
1. 39 ± 14%
2. 59 ± 11%
p < 0.05
Allergy:
1. 2
2. 1
Pain:
1. 3
2. 2
Refusal/DNA:
1. 3
2. 2
Differencebetween groupsnot significant
A priori sample size calcula-tion; 30% increase in ulcerhealing frequency with 80%power (a < 0.05). Ulcersmeasured by tracing andcomputer planimetry
Continued
TABLE 2 contd Details of included studies
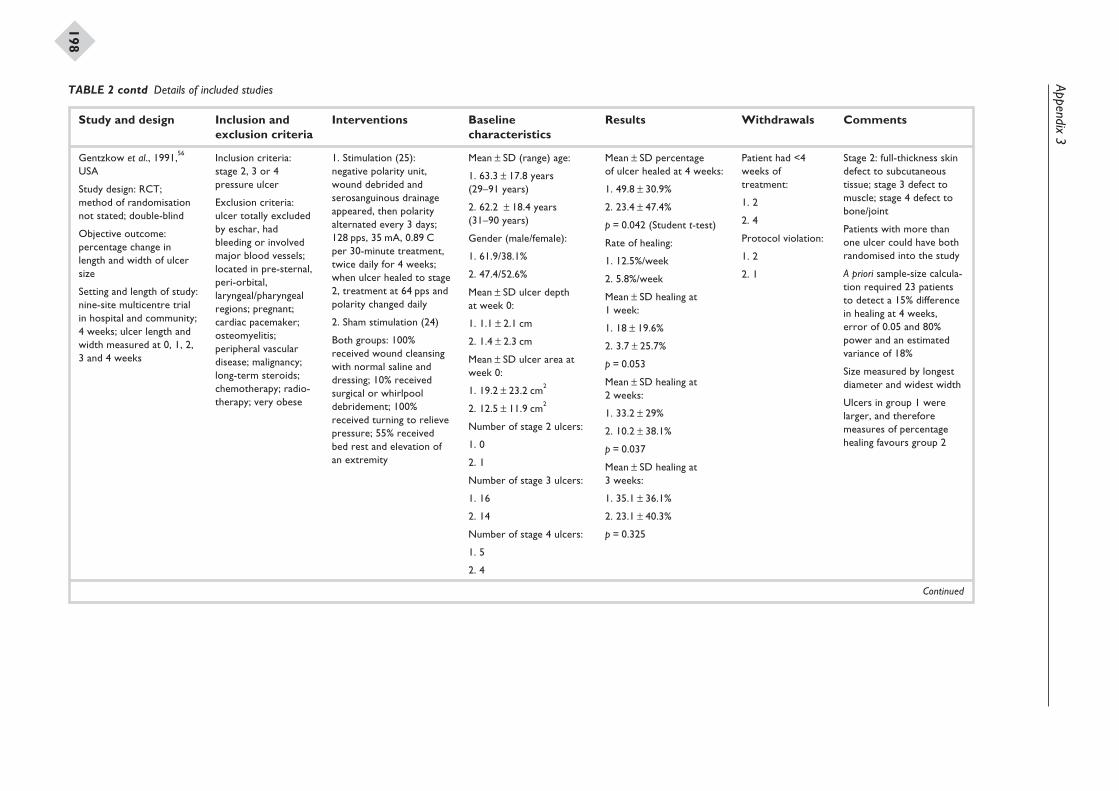
Appendix3
198
Study and design Inclusion andexclusion criteria
Interventions Baselinecharacteristics
Results Withdrawals Comments
Gentzkow et al., 1991,56
USA
Study design: RCT;method of randomisationnot stated; double-blind
Objective outcome:percentage change inlength and width of ulcersize
Setting and length of study:nine-site multicentre trialin hospital and community;4 weeks; ulcer length andwidth measured at 0, 1, 2,3 and 4 weeks
Inclusion criteria:stage 2, 3 or 4pressure ulcer
Exclusion criteria:ulcer totally excludedby eschar, hadbleeding or involvedmajor blood vessels;located in pre-sternal,peri-orbital,laryngeal/pharyngealregions; pregnant;cardiac pacemaker;osteomyelitis;peripheral vasculardisease; malignancy;long-term steroids;chemotherapy; radio-therapy; very obese
1. Stimulation (25):negative polarity unit,wound debrided andserosanguinous drainageappeared, then polarityalternated every 3 days;128 pps, 35 mA, 0.89 Cper 30-minute treatment,twice daily for 4 weeks;when ulcer healed to stage2, treatment at 64 pps andpolarity changed daily
2. Sham stimulation (24)
Both groups: 100%received wound cleansingwith normal saline anddressing; 10% receivedsurgical or whirlpooldebridement; 100%received turning to relievepressure; 55% receivedbed rest and elevation ofan extremity
Mean ± SD (range) age:
1. 63.3 ± 17.8 years(29–91 years)
2. 62.2 ± 18.4 years(31–90 years)
Gender (male/female):
1. 61.9/38.1%
2. 47.4/52.6%
Mean ± SD ulcer depthat week 0:
1. 1.1 ± 2.1 cm
2. 1.4 ± 2.3 cm
Mean ± SD ulcer area atweek 0:
1. 19.2 ± 23.2 cm2
2. 12.5 ± 11.9 cm2
Number of stage 2 ulcers:
1. 0
2. 1
Number of stage 3 ulcers:
1. 16
2. 14
Number of stage 4 ulcers:
1. 5
2. 4
Mean ± SD percentageof ulcer healed at 4 weeks:
1. 49.8 ± 30.9%
2. 23.4 ± 47.4%
p = 0.042 (Student t-test)
Rate of healing:
1. 12.5%/week
2. 5.8%/week
Mean ± SD healing at1 week:
1. 18 ± 19.6%
2. 3.7 ± 25.7%
p = 0.053
Mean ± SD healing at2 weeks:
1. 33.2 ± 29%
2. 10.2 ± 38.1%
p = 0.037
Mean ± SD healing at3 weeks:
1. 35.1 ± 36.1%
2. 23.1 ± 40.3%
p = 0.325
Patient had <4weeks oftreatment:
1. 2
2. 4
Protocol violation:
1. 2
2. 1
Stage 2: full-thickness skindefect to subcutaneoustissue; stage 3 defect tomuscle; stage 4 defect tobone/joint
Patients with more thanone ulcer could have bothrandomised into the study
A priori sample-size calcula-tion required 23 patientsto detect a 15% differencein healing at 4 weeks,error of 0.05 and 80%power and an estimatedvariance of 18%
Size measured by longestdiameter and widest width
Ulcers in group 1 werelarger, and thereforemeasures of percentagehealing favours group 2
Continued
TABLE 2 contd Details of included studies

Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
199
Study and design Inclusion andexclusion criteria
Interventions Baselinecharacteristics
Results Withdrawals Comments
Duration of ulcer £12months:
1. 85%
2. 66.7%
Duration of ulcer >12months:
1. 15%
2. 33.3%
Continued
TABLE 2 contd Details of included studies
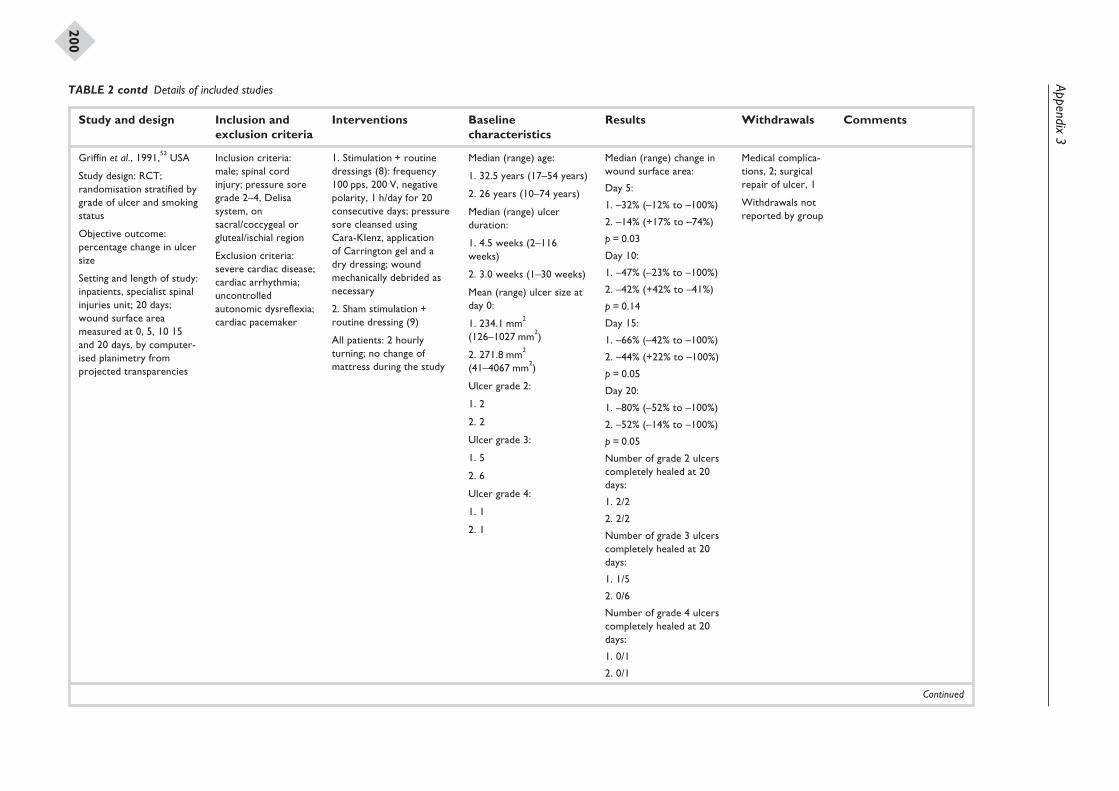
Appendix3
200
Study and design Inclusion andexclusion criteria
Interventions Baselinecharacteristics
Results Withdrawals Comments
Griffin et al., 1991,52 USA
Study design: RCT;randomisation stratified bygrade of ulcer and smokingstatus
Objective outcome:percentage change in ulcersize
Setting and length of study:inpatients, specialist spinalinjuries unit; 20 days;wound surface areameasured at 0, 5, 10 15and 20 days, by computer-ised planimetry fromprojected transparencies
Inclusion criteria:male; spinal cordinjury; pressure soregrade 2–4, Delisasystem, onsacral/coccygeal orgluteal/ischial region
Exclusion criteria:severe cardiac disease;cardiac arrhythmia;uncontrolledautonomic dysreflexia;cardiac pacemaker
1. Stimulation + routinedressings (8): frequency100 pps, 200 V, negativepolarity, 1 h/day for 20consecutive days; pressuresore cleansed usingCara-Klenz, applicationof Carrington gel and adry dressing; woundmechanically debrided asnecessary
2. Sham stimulation +routine dressing (9)
All patients: 2 hourlyturning; no change ofmattress during the study
Median (range) age:
1. 32.5 years (17–54 years)
2. 26 years (10–74 years)
Median (range) ulcerduration:
1. 4.5 weeks (2–116weeks)
2. 3.0 weeks (1–30 weeks)
Mean (range) ulcer size atday 0:
1. 234.1 mm2
(126–1027 mm2)
2. 271.8 mm2
(41–4067 mm2)
Ulcer grade 2:
1. 2
2. 2
Ulcer grade 3:
1. 5
2. 6
Ulcer grade 4:
1. 1
2. 1
Median (range) change inwound surface area:
Day 5:
1. –32% (–12% to –100%)
2. –14% (+17% to –74%)
p = 0.03
Day 10:
1. –47% (–23% to –100%)
2. –42% (+42% to –41%)
p = 0.14
Day 15:
1. –66% (–42% to –100%)
2. –44% (+22% to –100%)
p = 0.05
Day 20:
1. –80% (–52% to –100%)
2. –52% (–14% to –100%)
p = 0.05
Number of grade 2 ulcerscompletely healed at 20days:
1. 2/2
2. 2/2
Number of grade 3 ulcerscompletely healed at 20days:
1. 1/5
2. 0/6
Number of grade 4 ulcerscompletely healed at 20days:
1. 0/1
2. 0/1
Medical complica-tions, 2; surgicalrepair of ulcer, 1
Withdrawals notreported by group
Continued
TABLE 2 contd Details of included studies
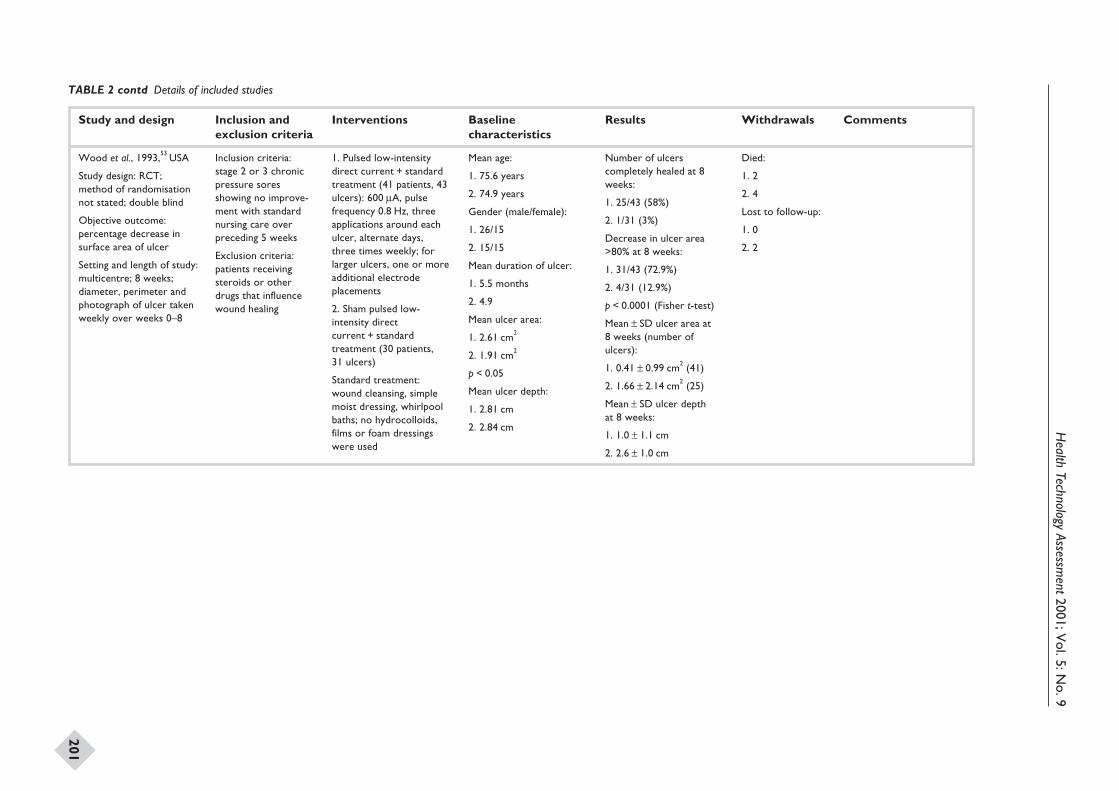
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
201
Study and design Inclusion andexclusion criteria
Interventions Baselinecharacteristics
Results Withdrawals Comments
Wood et al., 1993,53 USA
Study design: RCT;method of randomisationnot stated; double blind
Objective outcome:percentage decrease insurface area of ulcer
Setting and length of study:multicentre; 8 weeks;diameter, perimeter andphotograph of ulcer takenweekly over weeks 0–8
Inclusion criteria:stage 2 or 3 chronicpressure soresshowing no improve-ment with standardnursing care overpreceding 5 weeks
Exclusion criteria:patients receivingsteroids or otherdrugs that influencewound healing
1. Pulsed low-intensitydirect current + standardtreatment (41 patients, 43ulcers): 600 mA, pulsefrequency 0.8 Hz, threeapplications around eachulcer, alternate days,three times weekly; forlarger ulcers, one or moreadditional electrodeplacements
2. Sham pulsed low-intensity directcurrent + standardtreatment (30 patients,31 ulcers)
Standard treatment:wound cleansing, simplemoist dressing, whirlpoolbaths; no hydrocolloids,films or foam dressingswere used
Mean age:
1. 75.6 years
2. 74.9 years
Gender (male/female):
1. 26/15
2. 15/15
Mean duration of ulcer:
1. 5.5 months
2. 4.9
Mean ulcer area:
1. 2.61 cm2
2. 1.91 cm2
p < 0.05
Mean ulcer depth:
1. 2.81 cm
2. 2.84 cm
Number of ulcerscompletely healed at 8weeks:
1. 25/43 (58%)
2. 1/31 (3%)
Decrease in ulcer area>80% at 8 weeks:
1. 31/43 (72.9%)
2. 4/31 (12.9%)
p < 0.0001 (Fisher t-test)
Mean ± SD ulcer area at8 weeks (number ofulcers):
1. 0.41 ± 0.99 cm2 (41)
2. 1.66 ± 2.14 cm2 (25)
Mean ± SD ulcer depthat 8 weeks:
1. 1.0 ± 1.1 cm
2. 2.6 ± 1.0 cm
Died:
1. 2
2. 4
Lost to follow-up:
1. 0
2. 2
TABLE 2 contd Details of included studies
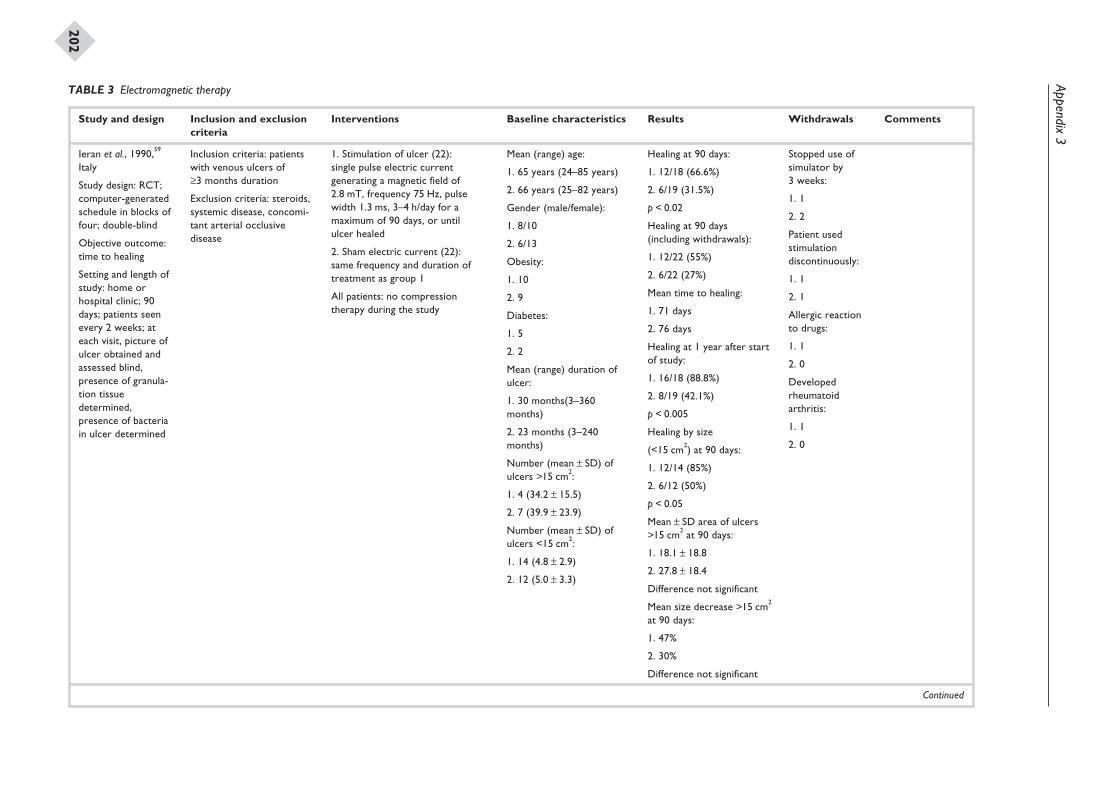
Appendix3
202
Study and design Inclusion and exclusioncriteria
Interventions Baseline characteristics Results Withdrawals Comments
Ieran et al., 1990,59
Italy
Study design: RCT;computer-generatedschedule in blocks offour; double-blind
Objective outcome:time to healing
Setting and length ofstudy: home orhospital clinic; 90days; patients seenevery 2 weeks; ateach visit, picture ofulcer obtained andassessed blind,presence of granula-tion tissuedetermined,presence of bacteriain ulcer determined
Inclusion criteria: patientswith venous ulcers of≥3 months duration
Exclusion criteria: steroids,systemic disease, concomi-tant arterial occlusivedisease
1. Stimulation of ulcer (22):single pulse electric currentgenerating a magnetic field of2.8 mT, frequency 75 Hz, pulsewidth 1.3 ms, 3–4 h/day for amaximum of 90 days, or untilulcer healed
2. Sham electric current (22):same frequency and duration oftreatment as group 1
All patients: no compressiontherapy during the study
Mean (range) age:
1. 65 years (24–85 years)
2. 66 years (25–82 years)
Gender (male/female):
1. 8/10
2. 6/13
Obesity:
1. 10
2. 9
Diabetes:
1. 5
2. 2
Mean (range) duration ofulcer:
1. 30 months(3–360months)
2. 23 months (3–240months)
Number (mean ± SD) ofulcers >15 cm2:
1. 4 (34.2 ± 15.5)
2. 7 (39.9 ± 23.9)
Number (mean ± SD) ofulcers <15 cm2:
1. 14 (4.8 ± 2.9)
2. 12 (5.0 ± 3.3)
Healing at 90 days:
1. 12/18 (66.6%)
2. 6/19 (31.5%)
p < 0.02
Healing at 90 days(including withdrawals):
1. 12/22 (55%)
2. 6/22 (27%)
Mean time to healing:
1. 71 days
2. 76 days
Healing at 1 year after startof study:
1. 16/18 (88.8%)
2. 8/19 (42.1%)
p < 0.005
Healing by size
(<15 cm2) at 90 days:
1. 12/14 (85%)
2. 6/12 (50%)
p < 0.05
Mean ± SD area of ulcers>15 cm2 at 90 days:
1. 18.1 ± 18.8
2. 27.8 ± 18.4
Difference not significant
Mean size decrease >15 cm2
at 90 days:
1. 47%
2. 30%
Difference not significant
Stopped use ofsimulator by3 weeks:
1. 1
2. 2
Patient usedstimulationdiscontinuously:
1. 1
2. 1
Allergic reactionto drugs:
1. 1
2. 0
Developedrheumatoidarthritis:
1. 1
2. 0
Continued
TABLE 3 Electromagnetic therapy
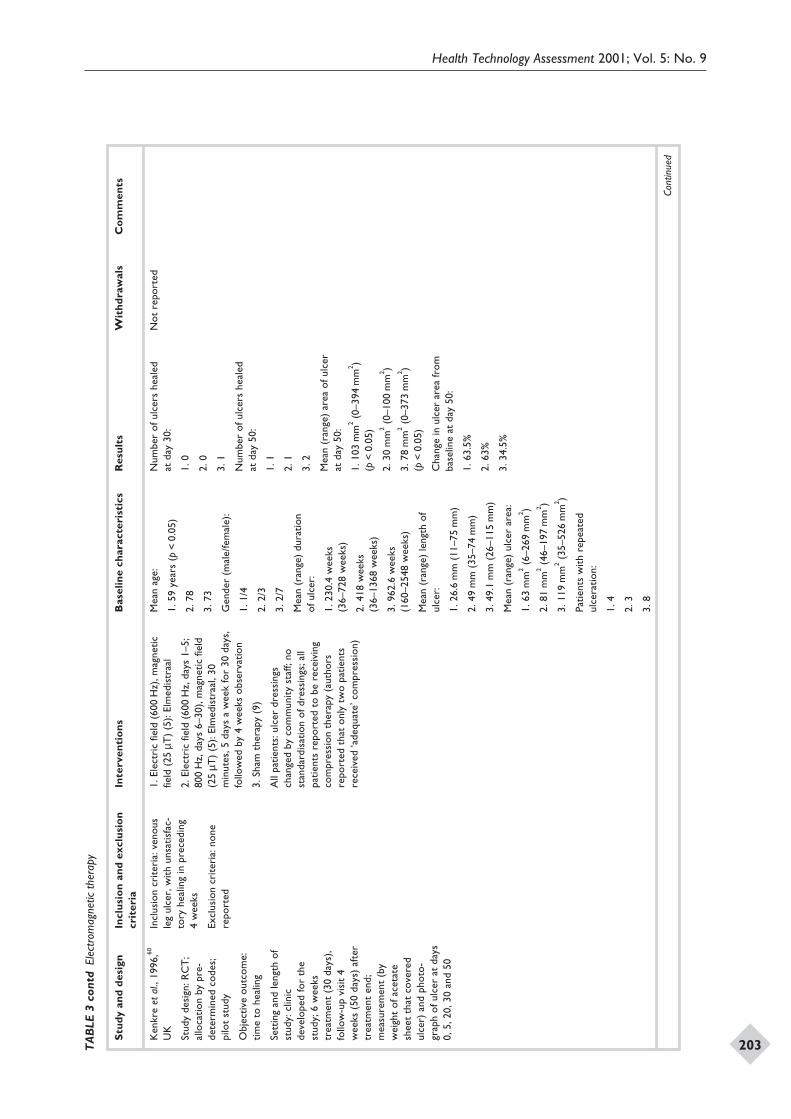
Health Technology Assessment 2001; Vol. 5: No. 9
203
Stu
dy
and
des
ign
Incl
usi
on
and
excl
usi
on
crit
eria
Inte
rven
tio
ns
Bas
elin
ech
arac
teri
stic
sR
esu
lts
Wit
hd
raw
als
Co
mm
ents
Ken
kre
etal
.,19
96,60
UK
Stud
yde
sign
:RC
T;
allo
catio
nby
pre-
dete
rmin
edco
des;
pilo
tst
udy
Obj
ectiv
eou
tcom
e:tim
eto
heal
ing
Sett
ing
and
leng
thof
stud
y:cl
inic
deve
lope
dfo
rth
est
udy;
6w
eeks
trea
tmen
t(3
0da
ys),
follo
w-u
pvi
sit
4w
eeks
(50
days
)af
ter
trea
tmen
ten
d;m
easu
rem
ent
(by
wei
ght
ofac
etat
esh
eet
that
cove
red
ulce
r)an
dph
oto-
grap
hof
ulce
rat
days
0,5,
20,3
0an
d50
Incl
usio
ncr
iteri
a:ve
nous
leg
ulce
r,w
ithun
satis
fac-
tory
heal
ing
inpr
eced
ing
4w
eeks
Excl
usio
ncr
iteri
a:no
nere
port
ed
1.El
ectr
icfie
ld(6
00H
z),m
agne
ticfie
ld(2
5µT
)(5
):El
med
istr
aal
2.El
ectr
icfie
ld(6
00H
z,da
ys1–
5;80
0H
z,da
ys6–
30),
mag
netic
field
(25
µT)
(5):
Elm
edis
traa
l,30
min
utes
,5da
ysa
wee
kfo
r30
days
,fo
llow
edby
4w
eeks
obse
rvat
ion
3.Sh
amth
erap
y(9
)
All
patie
nts:
ulce
rdr
essi
ngs
chan
ged
byco
mm
unity
staf
f;no
stan
dard
isat
ion
ofdr
essi
ngs;
all
patie
nts
repo
rted
tobe
rece
ivin
gco
mpr
essi
onth
erap
y(a
utho
rsre
port
edth
aton
lytw
opa
tient
sre
ceiv
ed‘a
dequ
ate’
com
pres
sion
)
Mea
nag
e:
1.59
year
s(p
<0.
05)
2.78
3.73
Gen
der
(mal
e/fe
mal
e):
1.1/
4
2.2/
3
3.2/
7
Mea
n(r
ange
)du
ratio
nof
ulce
r:
1.23
0.4
wee
ks(3
6–72
8w
eeks
)
2.41
8w
eeks
(36–
1368
wee
ks)
3.96
2.6
wee
ks(1
60–2
548
wee
ks)
Mea
n(r
ange
)le
ngth
oful
cer:
1.26
.6m
m(1
1–75
mm
)
2.49
mm
(35–
74m
m)
3.49
.1m
m(2
6–11
5m
m)
Mea
n(r
ange
)ul
cer
area
:
1.63
mm
2(6
–269
mm
2 )
2.81
mm
2(4
6–19
7m
m2 )
3.11
9m
m2
(35–
526
mm
2 )
Patie
nts
with
repe
ated
ulce
ratio
n:
1.4
2.3
3.8
Num
ber
oful
cers
heal
edat
day
30:
1.0
2.0
3.1
Num
ber
oful
cers
heal
edat
day
50:
1.1
2.1
3.2
Mea
n(r
ange
)ar
eaof
ulce
rat
day
50:
1.10
3m
m2
(0–3
94m
m2 )
(p<
0.05
)
2.30
mm
2(0
–100
mm
2 )
3.78
mm
2(0
–373
mm
2 )(p
<0.
05)
Cha
nge
inul
cer
area
from
base
line
atda
y50
:
1.63
.5%
2.63
%
3.34
.5%
Not
repo
rted
Cont
inue
d
TA
BLE
3co
ntd
Elec
trom
agne
ticth
erap
y
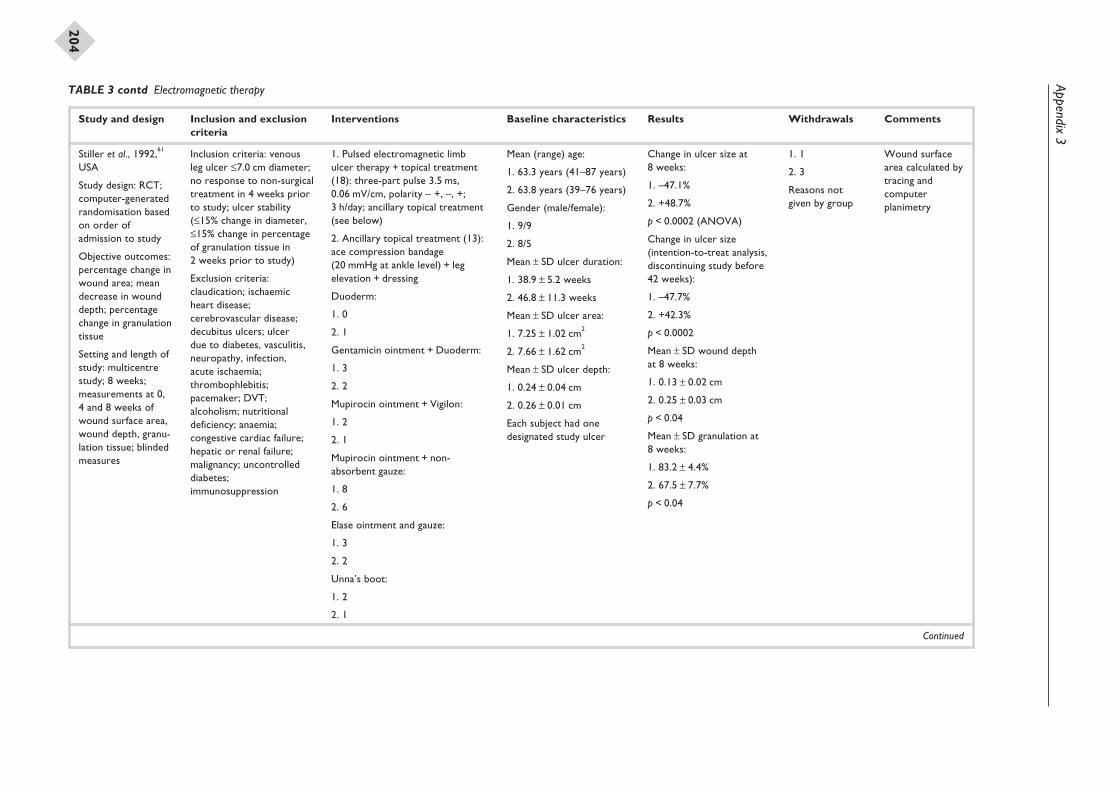
Appendix3
204
Study and design Inclusion and exclusioncriteria
Interventions Baseline characteristics Results Withdrawals Comments
Stiller et al., 1992,61
USA
Study design: RCT;computer-generatedrandomisation basedon order ofadmission to study
Objective outcomes:percentage change inwound area; meandecrease in wounddepth; percentagechange in granulationtissue
Setting and length ofstudy: multicentrestudy; 8 weeks;measurements at 0,4 and 8 weeks ofwound surface area,wound depth, granu-lation tissue; blindedmeasures
Inclusion criteria: venousleg ulcer £7.0 cm diameter;no response to non-surgicaltreatment in 4 weeks priorto study; ulcer stability(£15% change in diameter,£15% change in percentageof granulation tissue in2 weeks prior to study)
Exclusion criteria:claudication; ischaemicheart disease;cerebrovascular disease;decubitus ulcers; ulcerdue to diabetes, vasculitis,neuropathy, infection,acute ischaemia;thrombophlebitis;pacemaker; DVT;alcoholism; nutritionaldeficiency; anaemia;congestive cardiac failure;hepatic or renal failure;malignancy; uncontrolleddiabetes;immunosuppression
1. Pulsed electromagnetic limbulcer therapy + topical treatment(18): three-part pulse 3.5 ms,0.06 mV/cm, polarity – +, –, +;3 h/day; ancillary topical treatment(see below)
2. Ancillary topical treatment (13):ace compression bandage(20 mmHg at ankle level) + legelevation + dressing
Duoderm:
1. 0
2. 1
Gentamicin ointment + Duoderm:
1. 3
2. 2
Mupirocin ointment + Vigilon:
1. 2
2. 1
Mupirocin ointment + non-absorbent gauze:
1. 8
2. 6
Elase ointment and gauze:
1. 3
2. 2
Unna’s boot:
1. 2
2. 1
Mean (range) age:
1. 63.3 years (41–87 years)
2. 63.8 years (39–76 years)
Gender (male/female):
1. 9/9
2. 8/5
Mean ± SD ulcer duration:
1. 38.9 ± 5.2 weeks
2. 46.8 ± 11.3 weeks
Mean ± SD ulcer area:
1. 7.25 ± 1.02 cm2
2. 7.66 ± 1.62 cm2
Mean ± SD ulcer depth:
1. 0.24 ± 0.04 cm
2. 0.26 ± 0.01 cm
Each subject had onedesignated study ulcer
Change in ulcer size at8 weeks:
1. –47.1%
2. +48.7%
p < 0.0002 (ANOVA)
Change in ulcer size(intention-to-treat analysis,discontinuing study before42 weeks):
1. –47.7%
2. +42.3%
p < 0.0002
Mean ± SD wound depthat 8 weeks:
1. 0.13 ± 0.02 cm
2. 0.25 ± 0.03 cm
p < 0.04
Mean ± SD granulation at8 weeks:
1. 83.2 ± 4.4%
2. 67.5 ± 7.7%
p < 0.04
1. 1
2. 3
Reasons notgiven by group
Wound surfacearea calculated bytracing andcomputerplanimetry
Continued
TABLE 3 contd Electromagnetic therapy
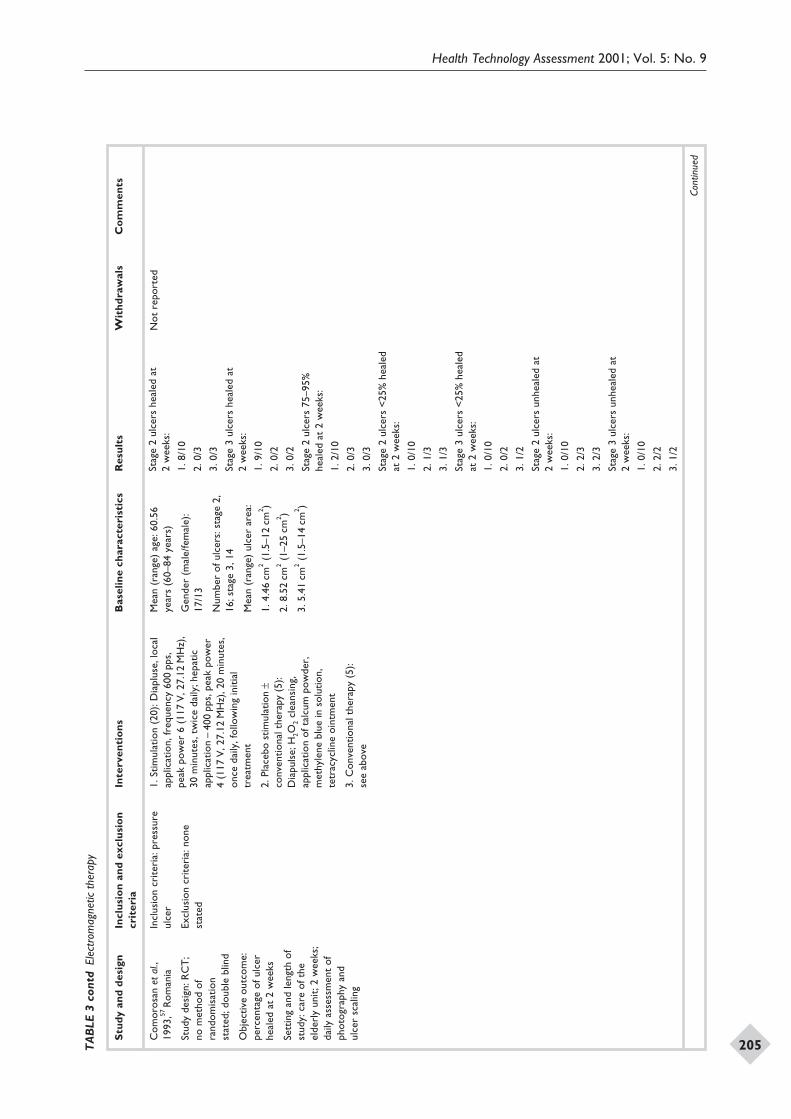
Health Technology Assessment 2001; Vol. 5: No. 9
205
Stu
dy
and
des
ign
Incl
usi
on
and
excl
usi
on
crit
eria
Inte
rven
tio
ns
Bas
elin
ech
arac
teri
stic
sR
esu
lts
Wit
hd
raw
als
Co
mm
ents
Com
oros
anet
al.,
1993
,57R
oman
ia
Stud
yde
sign
:RC
T;
nom
etho
dof
rand
omis
atio
nst
ated
;dou
ble
blin
d
Obj
ectiv
eou
tcom
e:pe
rcen
tage
oful
cer
heal
edat
2w
eeks
Sett
ing
and
leng
thof
stud
y:ca
reof
the
elde
rly
unit;
2w
eeks
;da
ilyas
sess
men
tof
phot
ogra
phy
and
ulce
rsc
alin
g
Incl
usio
ncr
iteri
a:pr
essu
reul
cer
Excl
usio
ncr
iteri
a:no
nest
ated
1.St
imul
atio
n(2
0):D
iapl
use,
loca
lap
plic
atio
n,fr
eque
ncy
600
pps,
peak
pow
er6
(117
V,2
7.12
MH
z),
30m
inut
es,t
wic
eda
ily;h
epat
icap
plic
atio
n–
400
pps,
peak
pow
er4
(117
V,2
7.12
MH
z),2
0m
inut
es,
once
daily
,fol
low
ing
initi
altr
eatm
ent
2.Pl
aceb
ost
imul
atio
n±
conv
entio
nalt
hera
py(5
):D
iapu
lse;
H2O
2cl
eans
ing,
appl
icat
ion
ofta
lcum
pow
der,
met
hyle
nebl
uein
solu
tion,
tetr
acyc
line
oint
men
t
3.C
onve
ntio
nalt
hera
py(5
):se
eab
ove
Mea
n(r
ange
)ag
e:60
.56
year
s(6
0–84
year
s)
Gen
der
(mal
e/fe
mal
e):
17/1
3
Num
ber
oful
cers
:sta
ge2,
16;s
tage
3,14
Mea
n(r
ange
)ul
cer
area
:
1.4.
46cm
2(1
.5–1
2cm
2 )
2.8.
52cm
2(1
–25
cm2 )
3.5.
41cm
2(1
.5–1
4cm
2 )
Stag
e2
ulce
rshe
aled
at2
wee
ks:
1.8/
10
2.0/
3
3.0/
3
Stag
e3
ulce
rshe
aled
at2
wee
ks:
1.9/
10
2.0/
2
3.0/
2
Stag
e2
ulce
rs75
–95%
heal
edat
2w
eeks
:
1.2/
10
2.0/
3
3.0/
3
Stag
e2
ulce
rs<
25%
heal
edat
2w
eeks
:
1.0/
10
2.1/
3
3.1/
3
Stag
e3
ulce
rs<
25%
heal
edat
2w
eeks
:
1.0/
10
2.0/
2
3.1/
2
Stag
e2
ulce
rsun
heal
edat
2w
eeks
:
1.0/
10
2.2/
3
3.2/
3
Stag
e3
ulce
rsun
heal
edat
2w
eeks
:
1.0/
10
2.2/
2
3.1/
2
Not
repo
rted
Cont
inue
d
TA
BLE
3co
ntd
Elec
trom
agne
ticth
erap
y
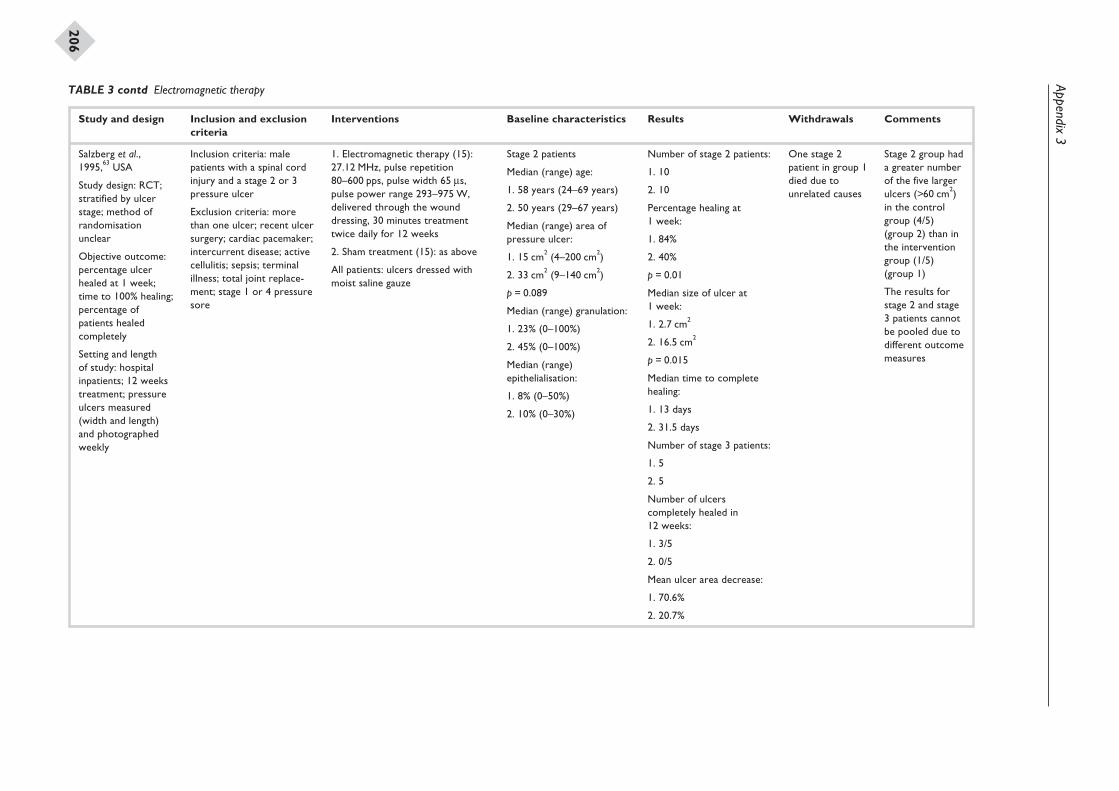
Appendix3
206
Study and design Inclusion and exclusioncriteria
Interventions Baseline characteristics Results Withdrawals Comments
Salzberg et al.,1995,63 USA
Study design: RCT;stratified by ulcerstage; method ofrandomisationunclear
Objective outcome:percentage ulcerhealed at 1 week;time to 100% healing;percentage ofpatients healedcompletely
Setting and lengthof study: hospitalinpatients; 12 weekstreatment; pressureulcers measured(width and length)and photographedweekly
Inclusion criteria: malepatients with a spinal cordinjury and a stage 2 or 3pressure ulcer
Exclusion criteria: morethan one ulcer; recent ulcersurgery; cardiac pacemaker;intercurrent disease; activecellulitis; sepsis; terminalillness; total joint replace-ment; stage 1 or 4 pressuresore
1. Electromagnetic therapy (15):27.12 MHz, pulse repetition80–600 pps, pulse width 65 ms,pulse power range 293–975 W,delivered through the wounddressing, 30 minutes treatmenttwice daily for 12 weeks
2. Sham treatment (15): as above
All patients: ulcers dressed withmoist saline gauze
Stage 2 patients
Median (range) age:
1. 58 years (24–69 years)
2. 50 years (29–67 years)
Median (range) area ofpressure ulcer:
1. 15 cm2 (4–200 cm2)
2. 33 cm2 (9–140 cm2)
p = 0.089
Median (range) granulation:
1. 23% (0–100%)
2. 45% (0–100%)
Median (range)epithelialisation:
1. 8% (0–50%)
2. 10% (0–30%)
Number of stage 2 patients:
1. 10
2. 10
Percentage healing at1 week:
1. 84%
2. 40%
p = 0.01
Median size of ulcer at1 week:
1. 2.7 cm2
2. 16.5 cm2
p = 0.015
Median time to completehealing:
1. 13 days
2. 31.5 days
Number of stage 3 patients:
1. 5
2. 5
Number of ulcerscompletely healed in12 weeks:
1. 3/5
2. 0/5
Mean ulcer area decrease:
1. 70.6%
2. 20.7%
One stage 2patient in group 1died due tounrelated causes
Stage 2 group hada greater numberof the five largerulcers (>60 cm2)in the controlgroup (4/5)(group 2) than inthe interventiongroup (1/5)(group 1)
The results forstage 2 and stage3 patients cannotbe pooled due todifferent outcomemeasures
TABLE 3 contd Electromagnetic therapy
Appendix 4
Quality assessment of included studies
Health Technology Assessment 2001; Vol. 5: No. 9
207
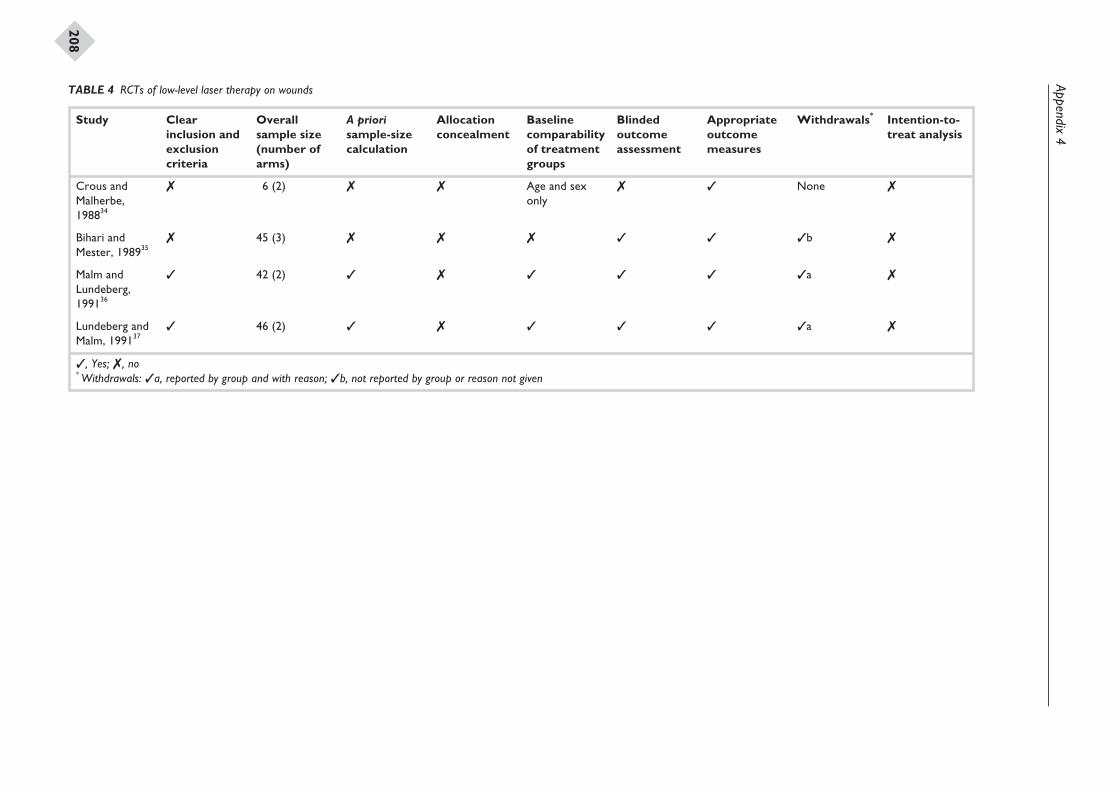
Appendix4
208
Study Clearinclusion andexclusioncriteria
Overallsample size(number ofarms)
A priorisample-sizecalculation
Allocationconcealment
Baselinecomparabilityof treatmentgroups
Blindedoutcomeassessment
Appropriateoutcomemeasures
Withdrawals* Intention-to-treat analysis
Crous andMalherbe,198834
7 6 (2) 7 7 Age and sexonly
7 3 None 7
Bihari andMester, 198935
7 45 (3) 7 7 7 3 3 3b 7
Malm andLundeberg,199136
3 42 (2) 3 7 3 3 3 3a 7
Lundeberg andMalm, 199137
3 46 (2) 3 7 3 3 3 3a 7
, Yes; , no* Withdrawals: a, reported by group and with reason; b, not reported by group or reason not given
TABLE 4 RCTs of low-level laser therapy on wounds
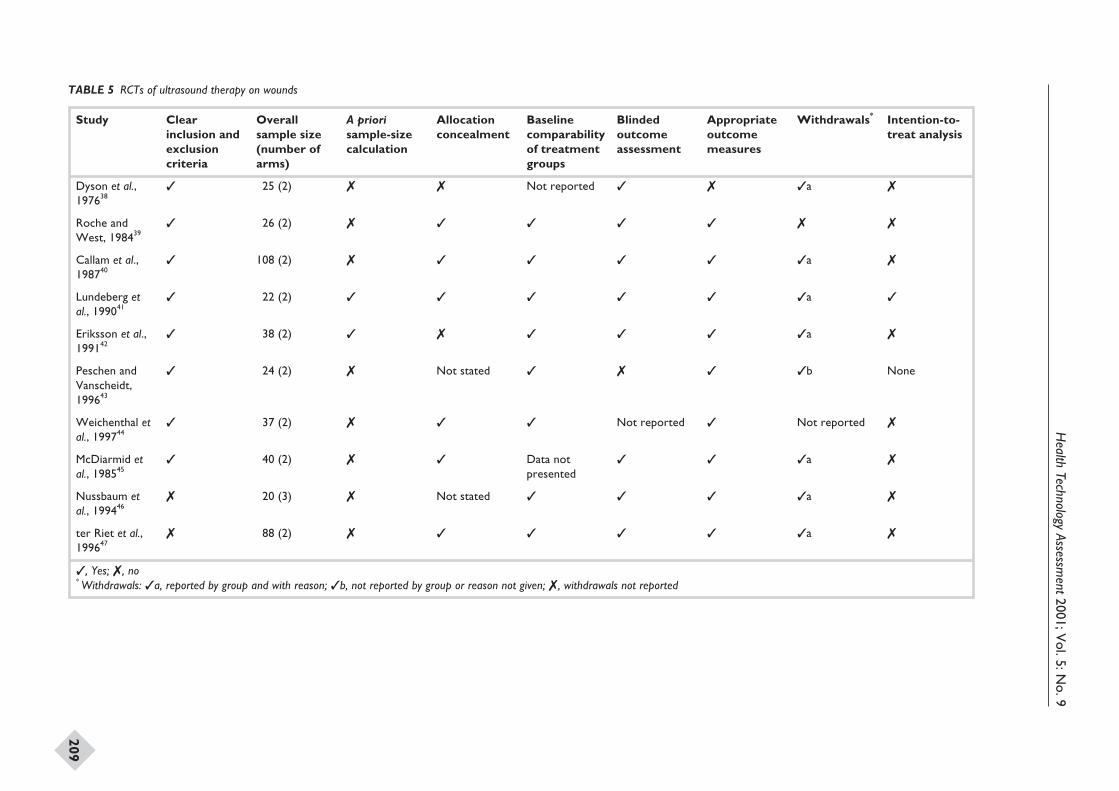
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
209
Study Clearinclusion andexclusioncriteria
Overallsample size(number ofarms)
A priorisample-sizecalculation
Allocationconcealment
Baselinecomparabilityof treatmentgroups
Blindedoutcomeassessment
Appropriateoutcomemeasures
Withdrawals* Intention-to-treat analysis
Dyson et al.,197638
3 25 (2) 7 7 Not reported 3 7 3a 7
Roche andWest, 198439
3 26 (2) 7 3 3 3 3 7 7
Callam et al.,198740
3 108 (2) 7 3 3 3 3 3a 7
Lundeberg etal., 199041
3 22 (2) 3 3 3 3 3 3a 3
Eriksson et al.,199142
3 38 (2) 3 7 3 3 3 3a 7
Peschen andVanscheidt,199643
3 24 (2) 7 Not stated 3 7 3 3b None
Weichenthal etal., 199744
3 37 (2) 7 3 3 Not reported 3 Not reported 7
McDiarmid etal., 198545
3 40 (2) 7 3 Data notpresented
3 3 3a 7
Nussbaum etal., 199446
7 20 (3) 7 Not stated 3 3 3 3a 7
ter Riet et al.,199647
7 88 (2) 7 3 3 3 3 3a 7
, Yes; , no* Withdrawals: a, reported by group and with reason; b, not reported by group or reason not given; , withdrawals not reported
TABLE 5 RCTs of ultrasound therapy on wounds
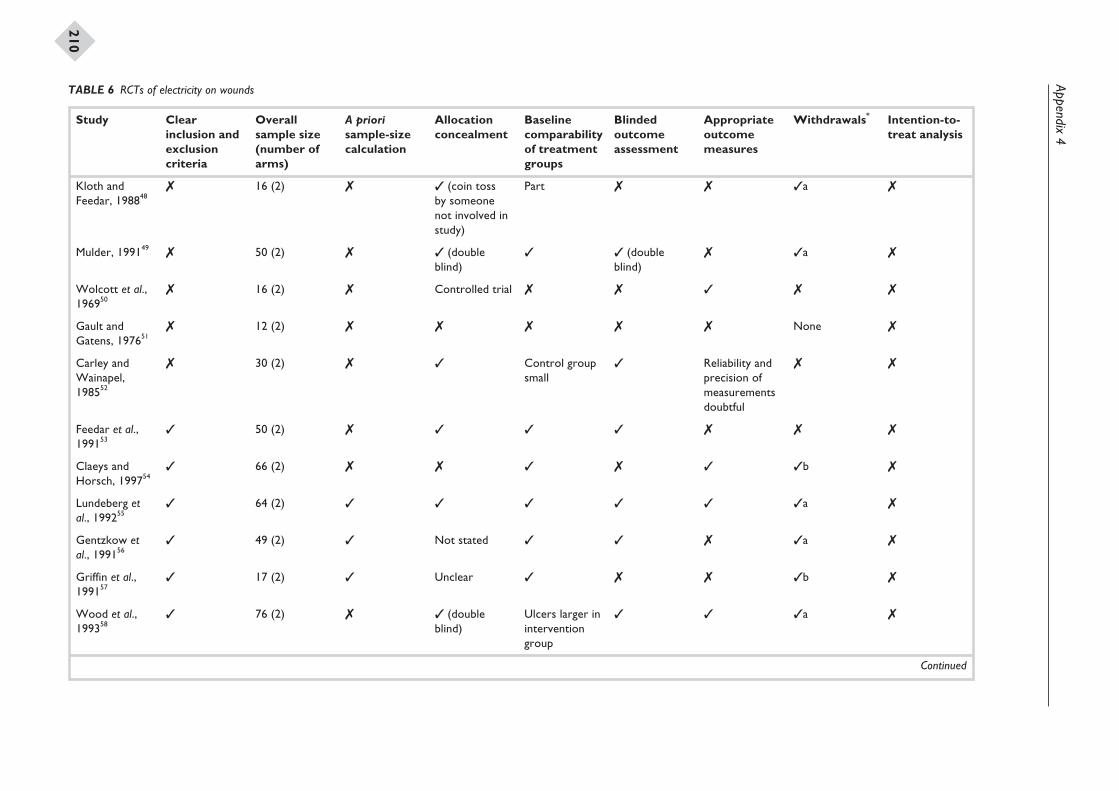
Appendix4
210
Study Clearinclusion andexclusioncriteria
Overallsample size(number ofarms)
A priorisample-sizecalculation
Allocationconcealment
Baselinecomparabilityof treatmentgroups
Blindedoutcomeassessment
Appropriateoutcomemeasures
Withdrawals* Intention-to-treat analysis
Kloth andFeedar, 198848
7 16 (2) 7 3 (coin tossby someonenot involved instudy)
Part 7 7 3a 7
Mulder, 199149 7 50 (2) 7 3 (doubleblind)
3 3 (doubleblind)
7 3a 7
Wolcott et al.,196950
7 16 (2) 7 Controlled trial 7 7 3 7 7
Gault andGatens, 197651
7 12 (2) 7 7 7 7 7 None 7
Carley andWainapel,198552
7 30 (2) 7 3 Control groupsmall
3 Reliability andprecision ofmeasurementsdoubtful
7 7
Feedar et al.,199153
3 50 (2) 7 3 3 3 7 7 7
Claeys andHorsch, 199754
3 66 (2) 7 7 3 7 3 3b 7
Lundeberg etal., 199255
3 64 (2) 3 3 3 3 3 3a 7
Gentzkow etal., 199156
3 49 (2) 3 Not stated 3 3 7 3a 7
Griffin et al.,199157
3 17 (2) 3 Unclear 3 7 7 3b 7
Wood et al.,199358
3 76 (2) 7 3 (doubleblind)
Ulcers larger ininterventiongroup
3 3 3a 7
Continued
TABLE 6 RCTs of electricity on wounds
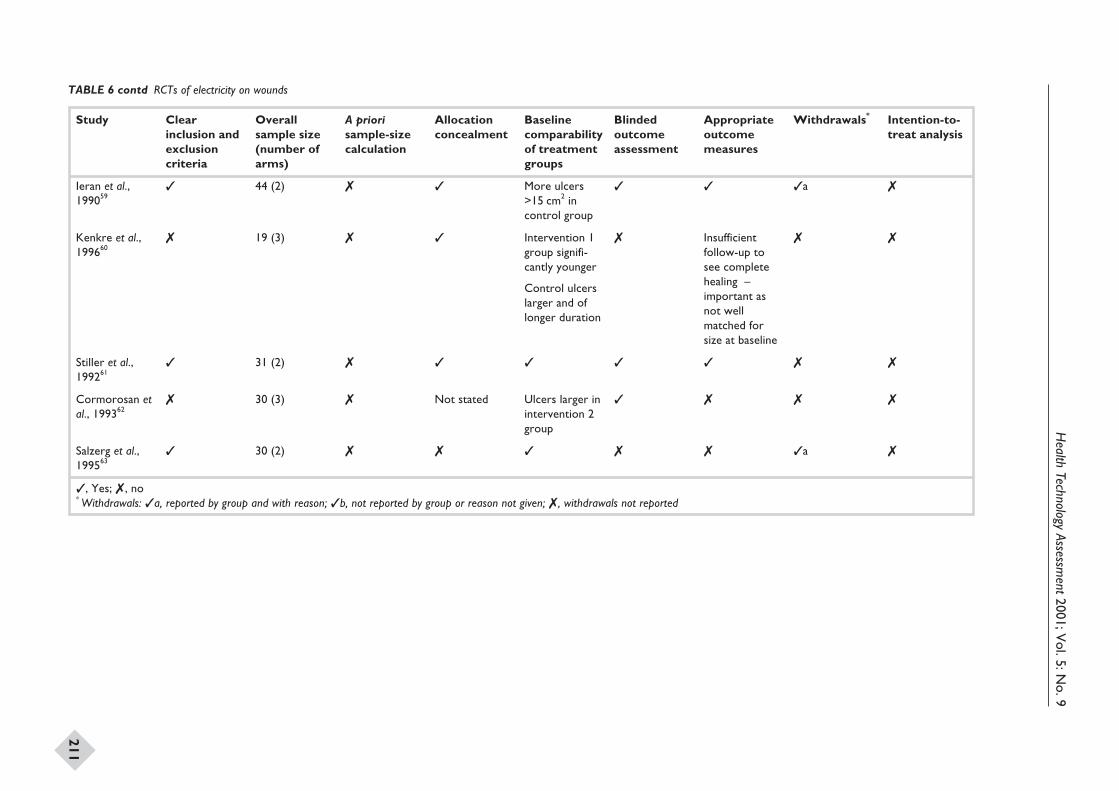
Health
TechnologyAssessm
ent2001;Vol.5:N
o.9
211
Study Clearinclusion andexclusioncriteria
Overallsample size(number ofarms)
A priorisample-sizecalculation
Allocationconcealment
Baselinecomparabilityof treatmentgroups
Blindedoutcomeassessment
Appropriateoutcomemeasures
Withdrawals* Intention-to-treat analysis
Ieran et al.,199059
3 44 (2) 7 3 More ulcers>15 cm2 incontrol group
3 3 3a 7
Kenkre et al.,199660
7 19 (3) 7 3 Intervention 1group signifi-cantly younger
Control ulcerslarger and oflonger duration
7 Insufficientfollow-up tosee completehealing –important asnot wellmatched forsize at baseline
7 7
Stiller et al.,199261
3 31 (2) 7 3 3 3 3 7 7
Cormorosan etal., 199362
7 30 (3) 7 Not stated Ulcers larger inintervention 2group
3 7 7 7
Salzerg et al.,199563
3 30 (2) 7 7 3 7 7 3a 7
, Yes; 7, no* Withdrawals: a, reported by group and with reason; b, not reported by group or reason not given; , withdrawals not reported
TABLE 6 contd RCTs of electricity on wounds
Health Technology Assessment 2001; Vol. 5: No. 9
219Current and past membership details of all HTA ‘committees’ are available from the HTA website (see inside front cover for details)
continued
Health Technology AssessmentProgramme
Prioritisation Strategy GroupMembers
ChairProfessor Kent WoodsDirector,NHS HTA Programme, &Professor of TherapeuticsLeicester Royal Infirmary
Professor Bruce CampbellConsultant General SurgeonRoyal Devon & Exeter Hospital
Professor Shah EbrahimProfessor of Epidemiologyof AgeingUniversity of Bristol
Dr John ReynoldsClinical DirectorAcute General Medicine SDUOxford Radcliffe Hospital
Dr Ron ZimmernDirector, Public HealthGenetics UnitStrangeways ResearchLaboratories, Cambridge
HTA Commissioning BoardMembers
Programme DirectorProfessor Kent WoodsDirector, NHS HTAProgramme, &Professor of TherapeuticsLeicester Royal Infirmary
ChairProfessor Shah EbrahimProfessor of Epidemiologyof AgeingUniversity of Bristol
Deputy ChairProfessor Jon NichollDirector, Medical CareResearch UnitUniversity of Sheffield
Professor Douglas AltmanDirector, ICRF MedicalStatistics GroupUniversity of Oxford
Professor John BondDirector, Centre for HealthServices ResearchUniversity of Newcastle-upon-Tyne
Ms Christine ClarkFreelance Medical WriterBury, Lancs
Professor Martin EcclesProfessor ofClinical EffectivenessUniversity of Newcastle-upon-Tyne
Dr Andrew FarmerGeneral Practitioner &NHS R&DClinical ScientistInstitute of Health SciencesUniversity of Oxford
Professor Adrian GrantDirector, Health ServicesResearch UnitUniversity of Aberdeen
Dr Alastair GrayDirector, Health EconomicsResearch CentreInstitute of Health SciencesUniversity of Oxford
Professor Mark HaggardDirector, MRC Instituteof Hearing ResearchUniversity of Nottingham
Professor Jenny HewisonSenior LecturerSchool of PsychologyUniversity of Leeds
Professor Alison KitsonDirector, Royal College ofNursing Institute, London
Dr Donna LampingHead, Health ServicesResearch UnitLondon School of Hygiene& Tropical Medicine
Professor David NealProfessor of SurgeryUniversity of Newcastle-upon-Tyne
Professor Gillian ParkerNuffield Professor ofCommunity CareUniversity of Leicester
Dr Tim PetersReader in Medical StatisticsUniversity of Bristol
Professor Martin SeversProfessor in ElderlyHealth CareUniversity of Portsmouth
Dr Sarah Stewart-BrownDirector, Health ServicesResearch UnitUniversity of Oxford
Professor Ala SzczepuraDirector, Centre for HealthServices StudiesUniversity of Warwick
Dr Gillian VivianConsultant in NuclearMedicine & RadiologyRoyal Cornwall Hospitals TrustTruro
Professor Graham WattDepartment ofGeneral PracticeUniversity of Glasgow
Dr Jeremy WyattSenior FellowHealth KnowledgeManagement CentreUniversity College London
Health Technology Assessment Programme
220
continued
Current and past membership details of all HTA ‘committees’ are available from the HTA website (see inside front cover for details)
Diagnostic Technologies & Screening PanelMembers
ChairDr Ron ZimmernDirector, Public HealthGenetics UnitStrangeways ResearchLaboratoriesCambridge
Dr Philip J AyresConsultant in Epidemiology& Public HealthThe Leeds Teaching HospitalsNHS Trust
Mrs Stella BurnsideChief Executive, AltnagelvinHospitals Health & SocialServices TrustLondonderryNorthern Ireland
Dr Paul O CollinsonConsultant ChemicalPathologist & Senior LecturerSt George’s Hospital, London
Dr Barry CooksonDirector, Laboratory ofHospital InfectionPublic Health LaboratoryService, London
Professor Howard CuckleProfessor of ReproductiveEpidemiologyUniversity of Leeds
Dr Carol DezateuxSenior Lecturer in PaediatricEpidemiologyInstitute of Child HealthLondon
Professor Adrian K DixonProfessor of RadiologyAddenbrooke’s HospitalCambridge
Mr Steve Ebdon-JacksonHead, Diagnostic Imaging &Radiation Protection TeamDepartment of Health, London
Dr Tom FaheySenior Lecturer in GeneralPracticeUniversity of Bristol
Dr Andrew FarmerGeneral Practitioner &NHS Clinical ScientistInstitute of Health SciencesUniversity of Oxford
Mrs Gillian FletcherAntenatal Teacher & TutorNational Childbirth TrustReigate
Professor Jane FranklynProfessor of MedicineUniversity of Birmingham
Dr JA Muir GrayJoint Director, NationalScreening CommitteeNHS Executive, Oxford
Dr Peter HowlettExecutive Director –DevelopmentPortsmouth HospitalsNHS Trust
Professor Alistair McGuireProfessor of Health EconomicsCity University, London
Mrs Kathlyn SlackProfessional SupportDiagnostic Imaging &Radiation Protection TeamDepartment of Health,London
Mr Tony TesterChief Officer, SouthBedfordshire CommunityHealth CouncilLuton
Pharmaceuticals PanelMembers
ChairDr John ReynoldsClinical Director –Acute General Medicine SDUOxford Radcliffe Hospital
Dr Felicity J GabbayManaging Director,Transcrip LtdMilford-on-Sea, Hants
Mr Peter GolightlyDirector, Trent DrugInformation ServicesLeicester Royal Infirmary
Dr Alastair GrayDirector, Health EconomicsResearch CentreInstitute of Health SciencesUniversity of Oxford
Mrs Jeannette HoweSenior Principal PharmacistDepartment of Health, London
Dr Andrew MortimoreConsultant in Public HealthMedicineSouthampton & South WestHants Health Authority
Mr Nigel OffenHead of Clinical QualityNHS Executive – EasternMilton Keynes
Professor Robert PevelerProfessor of Liaison PsychiatryRoyal South Hants HospitalSouthampton
Mrs Marianne RiggeDirector, College of HealthLondon
Dr Frances RotblatManager, Biotechnology GroupMedicines Control AgencyLondon
Mr Bill SangChief ExecutiveSalford Royal HospitalsNHS Trust
Dr Eamonn SheridanConsultant in Clinical GeneticsSt James’s University HospitalLeeds
Mrs Katrina SimisterNew Products ManagerNational Prescribing CentreLiverpool
Dr Ross TaylorSenior LecturerDepartment of GeneralPractice & Primary CareUniversity of Aberdeen
Dr Richard TinerMedical DirectorAssociation of the BritishPharmaceutical IndustryLondon
Professor JeniferWilson-BarnettHead, Florence NightingaleDivision of Nursing& MidwiferyKing’s College, London
Mr David J WrightChief ExecutiveInternational GlaucomaAssociation, London
Health Technology Assessment 2001; Vol. 5: No. 9
221Current and past membership details of all HTA ‘committees’ are available from the HTA website (see inside front cover for details)
Therapeutic Procedures PanelMembers
ChairProfessor Bruce CampbellConsultant General SurgeonRoyal Devon & Exeter Hospital
Professor John BondProfessor ofHealth Services ResearchUniversity of Newcastle-upon-Tyne
Ms Judith BrodieHead of CancerSupport ServiceCancer BACUP, London
Ms Tracy BuryHead of Research& DevelopmentChartered Society ofPhysiotherapy, London
Mr Michael ClancyConsultant in A&E MedicineSouthampton General Hospital
Professor Collette CliffordProfessor of NursingUniversity of Birmingham
Dr Katherine DartonInformation UnitMIND – The Mental HealthCharity, London
Mr John DunningConsultant CardiothoracicSurgeonPapworth Hospital NHS TrustCambridge
Mr Jonothan EarnshawConsultant Vascular SurgeonGloucestershire Royal Hospital
Professor David FieldProfessor of Neonatal MedicineThe Leicester Royal InfirmaryNHS Trust
Professor FD Richard HobbsProfessor of Primary Care& General PracticeUniversity of Birmingham
Mr Richard JohansonConsultant & Senior LecturerNorth Staffordshire InfirmaryNHS Trust, Stoke-on-Trent
Dr Duncan KeeleyGeneral PractitionerThame, Oxon
Dr Phillip LeechPrincipal Medical OfficerDepartment of Health, London
Professor James LindesayProfessor of Psychiatry forthe ElderlyUniversity of Leicester
Professor Rajan MadhokDirector of Health Policy& Public HealthEast Riding & HullHealth Authority
Dr Mike McGovernBranch HeadDepartment of HealthLondon
Dr John C PounsfordConsultant PhysicianFrenchay Healthcare TrustBristol
Dr Mark SculpherSenior Research Fellow inHealth EconomicsUniversity of York
Dr Ken SteinConsultant in PublicHealth MedicineNorth & East Devon HealthAuthority, Exeter
Expert Advisory NetworkMembers
Professor John BrazierDirector of Health EconomicsUniversity of Sheffield
Mr Shaun BroganChief Executive, RidgewayPrimary Care GroupAylesbury, Bucks
Mr John A CairnsDirector, Health EconomicsResearch UnitUniversity of Aberdeen
Dr Nicky CullumReader in Health StudiesUniversity of York
Professor Pam EnderbyChair of CommunityRehabilitationUniversity of Sheffield
Mr Leonard R FenwickChief ExecutiveFreeman HospitalNewcastle-upon-Tyne
Ms Grace GibbsDeputy Chief ExecutiveWest MiddlesexUniversity Hospital
Dr Neville GoodmanConsultant AnaesthetistSouthmead Hospital, Bristol
Professor Robert E HawkinsCRC Professor & Director ofMedical OncologyChristie Hospital NHS TrustManchester
Professor Allen HutchinsonDirector of Public Health &Deputy Dean, ScHARRUniversity of Sheffield
Professor David MantProfessor of General PracticeInstitute of Health SciencesUniversity of Oxford
Professor Alexander MarkhamDirectorMolecular Medicine UnitSt James’s University HospitalLeeds
Dr Chris McCallGeneral PractitionerCorfe Mullen, Dorset
Dr Peter MooreFreelance Science WriterAshtead, Surrey
Dr Sue MossAssociate Director, CancerScreening Evaluation UnitInstitute of Cancer ResearchSutton, Surrey
Mrs Julietta PatnickNational CoordinatorNHS Cancer ScreeningProgrammes, Sheffield
Professor Jennie PopayProfessor of Sociology &Community HealthUniversity of Salford
Professor Chris PriceProfessor ofClinical BiochemistrySt Bartholomew’s & TheRoyal London School ofMedicine & Dentistry
Mr Simon RobbinsChief ExecutiveCamden & IslingtonHealth Authority, London
Dr William RosenbergSenior Lecturer &Consultant in MedicineUniversity of Southampton
Dr Sarah Stewart-BrownDirector, Health ServicesResearch UnitUniversity of Oxford
Dr Gillian VivianConsultant in NuclearMedicine & RadiologyRoyal Cornwall Hospitals TrustTruro
Mrs Joan WebsterFormer ChairSouthern DerbyshireCommunity Health CouncilNottingham


Health Technology Assessm
ent 2001;Vol.5:No.9
Wound care:beds,com
pression,physical therapies
Copies of this report can be obtained from:
The National Coordinating Centre for Health Technology Assessment,Mailpoint 728, Boldrewood,University of Southampton,Southampton, SO16 7PX, UK.Fax: +44 (0) 23 8059 5639 Email: [email protected]://www.ncchta.org ISSN 1366-5278
FeedbackThe HTA programme and the authors would like to know
your views about this report.
The Correspondence Page on the HTA website(http://www.ncchta.org) is a convenient way to publish
your comments. If you prefer, you can send your comments to the address below, telling us whether you would like
us to transfer them to the website.
We look forward to hearing from you.