syncope
TRANSCRIPT
Evaluationof Syncope
Dr. Charles Nelson
November 14, 2014
Syncope: A Symptom, not a Diagnosis
• Self-limited loss of consciousness and postural tone
• Relatively rapid onset
• Variable warning symptoms
• Spontaneous, complete, and usually prompt recovery without medical or surgical intervention
Underlying mechanism: Underlying mechanism: transient global cerebral transient global cerebral
hypoperfusion.hypoperfusion.

Syncope Mimics
• Acute intoxication (e.g., alcohol)• Seizures• Sleep disorders• Somatization disorder (psychogenic pseudo-syncope)• Trauma/concussion• Hypoglycemia• Hyperventilation
Brignole M, et al. Europace, 2004;6:467-537.

Syncope: Epidemiological Data
• 40% population, presumed syncope at least once1
• 1-6% of hospital admissions2
• Approx 1% of ED visits per year3,4
• 10% of falls by elderly are believed due to syncope5
• Injuries:
• 6% major morbidity (e.g., fractures, MVA)1
• Minor injury in 29%1
1Kenny RA, et al. eds. The Evaluation and Treatment of Syncope. Futura;2003:23-27.2Kapoor W. Medicine. 1990;69:160-175.
3Brignole M, et al. Europace. 2003;5:293-298.4 Blanc J-J, et al. Eur Heart J. 2002;23:815-820.
5Campbell A, et al. Age and Ageing. 1981;10:264-270.

Syncope & Collapse: Emergency Department US Data 2006
• Emergency Department visits • Primary Diagnosis ~1.13 million• Among all listed diagnoses >1.35 million
• Hospital admission rate, ~36%

• Estimated hospital costs > $5400/hospitalization
• Treating ‘falls’ in older adults1 >$7 billion
Impact of Syncope in USA: Annual Expenditures
1. Benjamin C. Sun, MD, MPP, Jennifer A. Emond, MS, and Carlos A. Camargo, Jr., MD, DrPH “Direct medical costs of syncope-related hospitalizations in the USA Am J Cardiol 2005;95:668-671
2 Kenny RA, Kapoor WN. In: Benditt D, et al. eds. The Evaluation and Treatment of Syncope. Futura;2003:23-27.

Syncope & Collapse: Estimated Hospitalization Costs
Conservative estimates of annual cost:
• Syncope / Collapse - $2.4 billion
• Asthma - $2.8 billion
• HIV - $2.2 billion
• COPD - $1.9 billion
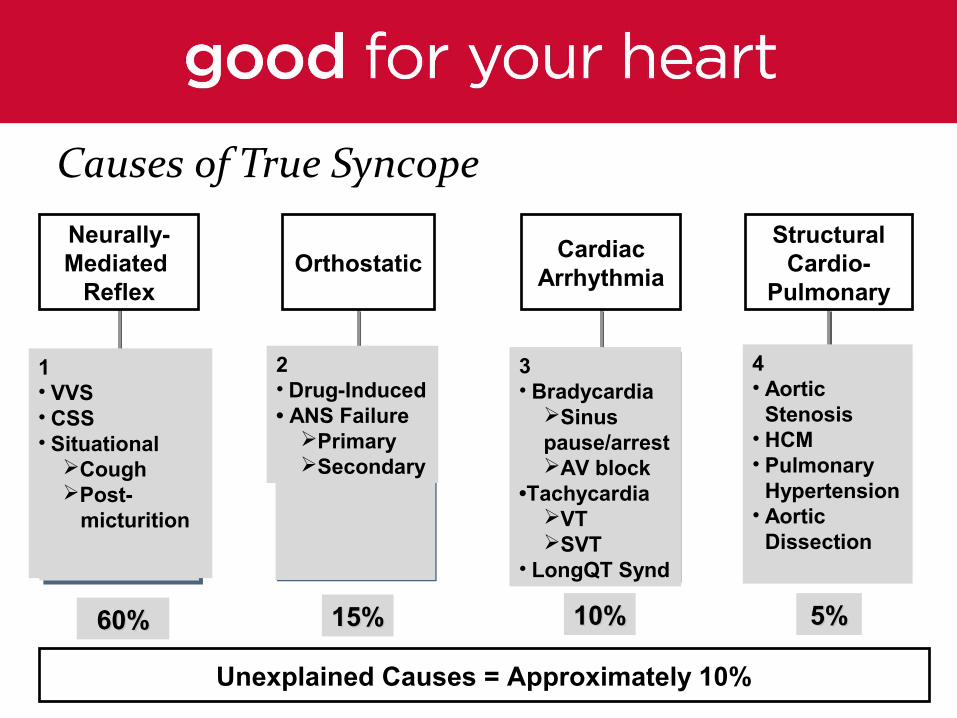
Causes of True Syncope
OrthostaticCardiac
Arrhythmia
StructuralCardio-
Pulmonary
1• VVS• CSS• Situational
CoughPost- micturition
2• Drug-Induced• ANS Failure
PrimarySecondary
3• Bradycardia
Sinus pause/arrestAV block
•TachycardiaVTSVT
• LongQT Synd
4 • Aortic
Stenosis• HCM• Pulmonary
Hypertension• Aortic
Dissection
Neurally-Mediated
Reflex
Unexplained Causes = Approximately 10%
60%60% 15%15% 10%10% 5%5%

Impact of Syncope on Mortality Risk
• Vasovagal Syncope has low mortality risk– But recurrences are a concern
• Syncope of presumed cardiac cause is associated with high mortality risk– Most evidence suggests that risk is
similar to that of patients without syncope but with similar severity of heart disease
Soteriades ES, Evans JC, Larson MG, et al. Incidence and prognosis of syncope. N Engl J Med. 2002;347(12):878-885. [Framingham Study Population]

Establish cause of syncope with sufficient certainty to:
• Assess prognosis confidently
• Initiate effective preventive treatment
Diagnostic Goal

• EEG, Head CT, Head MRI
carotid dopplers
• May help diagnose seizure
• Reasonable if syncope has
resulted in closed head
injury or if focal neuro
findings
Neurological Tests: Rarely Diagnostic for Syncope
Neurological Tests: Rarely Diagnostic for Syncope
Brignole M, et al. Europace. 2004;6:467-537.

Clinical Features Suggesting Cause of Syncope: ESC Syncope Task Force 2004
• Neurally-mediated Reflex Syncope– Absence of cardiac disease (except CSS)
– Long history of recurrences
– Associated with emotional event, pain, prolonged upright posture, hot
environment, head rotation
– After strenuous exertion
• Orthostatic Syncope– Associated with change to upright posture, prolonged standing, dehydration
– Recent addition of diuretic, vasodilator, etc
– History of neuropathy, diabetes, alcohol abuseCSS=carotid sinus syndrome

Neurally-Mediated Reflex Syncope (NMS)
• Vasovagal Syncope (VVS)• Carotid Sinus Syndrome (CSS)
• Situational Syncope– post-micturition– cough– swallow – defecation– blood drawing– etc.

NMS:Clinical Pathophysiology
• Neurally-mediated physiologic reflex mechanism with two
components:
– Cardioinhibitory ( HR )
– Vasodepressor ( BP )
• Both components are usually present:
– Vasodepressor may be masked in the presence of severe
bradycardia
– Pace or pre-treat with atropine in order to observe
Vasodepressor component
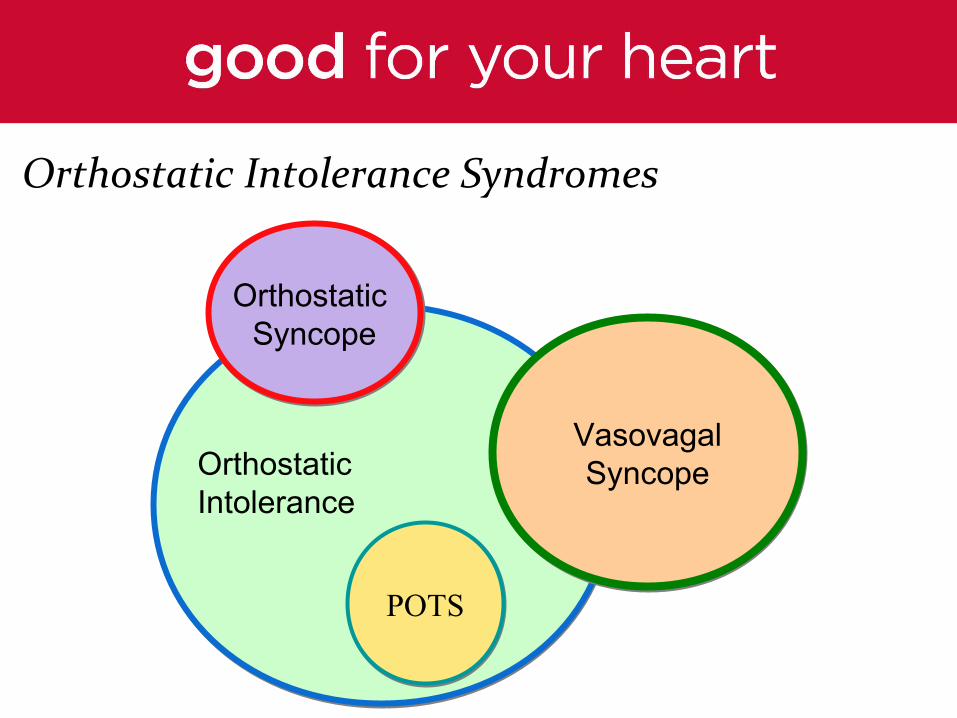
Orthostatic Intolerance Syndromes
Orthostatic Syncope
Orthostatic Syncope
POTSPOTS
VasovagalSyncope
VasovagalSyncopeOrthostatic
Intolerance

Orthostatic Hypotension- Etiology
• Drug-induced (very common)
– Diuretics, Vasodilators
• Primary autonomic failure
– Multiple system atrophy, Parkinsonism
• Secondary autonomic failure
– Diabetes, Alcohol, Amyloid

Clinical/ECG Features For Cardiac Syncope• Presence of severe structural heart disease
• Family history of sudden death
• Syncope during exertion or while supine
• Palpitations at time of syncope
• Heart failure / LV Dysfunction
• ECG / Monitor findings of:
– Baseline Wide QRS Complex
– Mobitz 1 second degree AVB
– Sinus bradycardia <50 bpm
– Documented Non Sustained or Sustained VT
– Preexcitation, Long QT, t wave inversion
– Bifasicular blockAdapted from ESC Syncope Guidelines– Update 2004
Syncope Due to Structural CV Disease
• Acute MI / Ischemia • Acquired coronary artery disease
– Congenital coronary artery anomalies• Hypertrophic Cardiomyopathy (HCM)• Arrhythmogenic RV Dysplasia (ARVD)• Acute aortic dissection• Acute pulmonary embolus/pulmonary hypertension• Valvular abnormalities
– Aortic stenosis– Mitral stenosis
• Atrial myxoma• Intra-cardiac thrombus (ball-valve thrombus)

Syncope Due to Cardiac Arrhythmias
• Bradyarrhythmias
– Sinus arrest, exit block
– High grade or acute complete AV block
• Tachyarrhythmias
– Atrial fibrillation/flutter with rapid ventricular rate (e.g., WPW syndrome)
– Paroxysmal SVT or VT
– Torsades de pointes (e.g., long QT syndrome)

The Initial Evaluation: 4 Key Questions
• Did the patient suffer ‘true’ Transient Loss of Consciousness (TLOC)?
• Was TLOC due to syncope or mimic?
• Is heart disease present?
• Does the medical history (including observations by witnesses) suggest a specific diagnosis?
Occasionally may need to be admitted
•No heart disease but sudden onset of palpitations shortly before syncope or high suspicion of cardiac syncope
•Other sig condition associated with though not cause of syncope
•Syncope in supine position,
•Frequent recurrent episodes, injuries
Hospital Admission for Diagnosis or Treatment
ESC Syncope Task Force 2004

Diagnostic Testing
• Exertional syncope or exertional symptoms: stress test
• Signs or symptoms CHF, murmurs: echo
• Palpitations or tachycardia preceeding event: holter or
event
• Abnormal ekg (heart block, bifasicular block): holter or
ILR
• Suspected (but uncertain) NMS: tilt test
• Pts that are orthostatic do not need tilt test

When do not need refer to specialist
• No need to refer when cause for syncope is certain,
and no evidence of significant heart disease.
• No need to refer if diagnosis is uncertain, but
episode did not result in significant injury and is not
recurrent.

When to refer to specialist
• When initial evaluation or testing indicates underlying significant
heart disease (abnormal ekg or echo)
• When need tilt testing to confirm cause of syncope
• When syncope is recurrent in spite of treatment for suspected
cause
• When cause is uncertain and syncope is recurrent
• Anytime you have a question that you cant answer or are not
sure how to proceed in evaluating the patient.
Feedback and Questions

Treatment Strategies for Orthostatic Intolerance• Patient education, injury avoidance
• Hydration
– fluids, salt, diet
– minimize caffeine/alcohol
• Sleeping with head of bed elevated
• Tilt Training, leg crossing, arm tensing
• Support hose, abdominal binders
• Drug therapies
– fludrocortisone, midodrine, erythropoietin