symptoms of patients & families - critical care · pdf filesymptoms of patients &...
TRANSCRIPT
SYMPTOMS OF PATIENTS & FAMILIES
Pain without words:
Are reactions comparable among patients?
Tuesday, November 12th, 2013
By Céline Gélinas, RN, PhD Assistant Professor
Ingram School of Nursing, McGill University Researcher and Nurse Scientist
Centre for Nursing Research and Lady Davis Institute, Jewish General Hospital
Montréal, Canada [email protected]

Acknowledgements Research team
Darina Tsoller (coordinator) Caroline Arbour, RN, PhD Stephanie Avery, BScN(student) Mélanie Bérubé, RN, NP, PhD(student) Madalina Boitor, RN, PhD(student) Christian Drouin, MScA(student) Christine Echegaray-Benites, RN, MScA(N) Esther Garceau, BScN(student) Oxana Kapoustina, RN, MScA(N) Jade Remy, CEPI, BScN Melody Ross, CEPI, MScA(student) Brandy Vanderbyl, MScA(student)
Funding agencies
Key collaborators
Jane Topolovec-Vranic, PhD (co-PI) Kathleen Puntillo, RN, DNSc, FAAN Manon Choinière, PhD Andrew Baker, MD Michael Cusimano, MD, PhD Anne-Sylvie Ramelet, RN, PhD David Streiner, PhD

What is pain?
Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage (IASP, 1979)
Alternative definition for non-verbal patients:
«Behavioral alterations caused by pain are valuable forms of self-report and should be considered as alternative measures of pain» (Anand & Craig, 1996)
“The inability to communicate verbally does not negate the possibility that an individual is experiencing pain and is in need of appropriate pain-relieving treatment” (IASP, 2011)

The picture of pain in the ICU Pain is a major stressor for critically ill patients (Rotondi et al., 2002)
Pain is experienced by ICU patients either at rest (Chanques et al., 2007) or during nociceptive procedures (Puntillo et al., 2001)
Incomplete or absence of pain assessments have been associated with longer ICU stay, longer MV duration, and increased mortality in the ICU (Kastrup et al., 2009; Payen et al., 2009)
Many ICU patients are unable to self-report…
In such situations, the use of a valid behavioral pain scale is recommended by the ASPMN (Herr et al., 2011) and SCCM (Barr et al., 2013)
BPS (Payen et al., 2001) or CPOT (Gélinas et al., 2006)
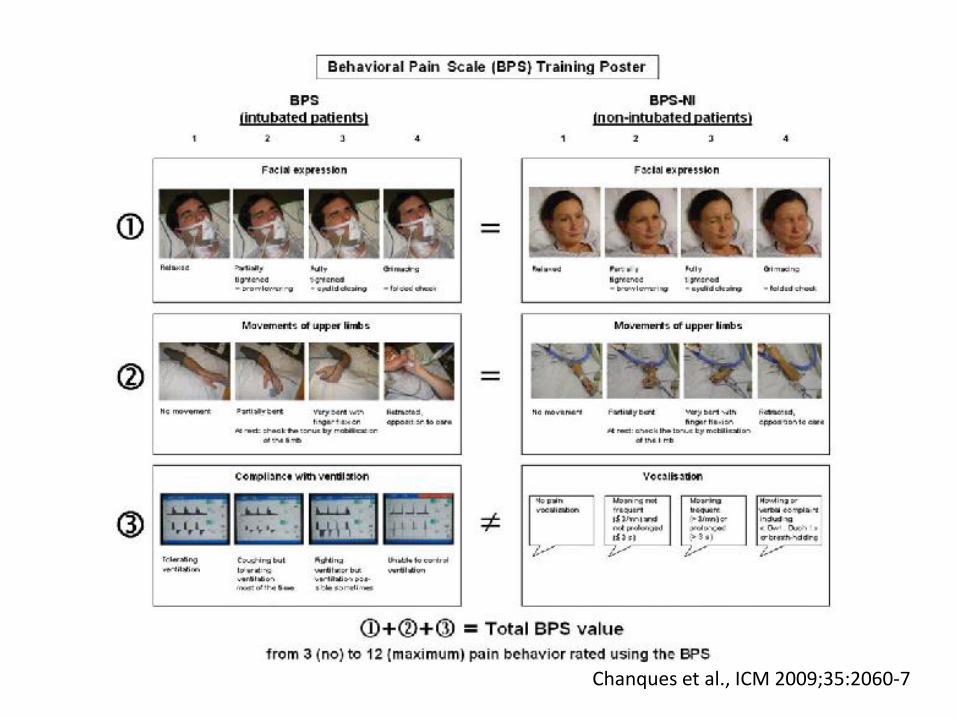
Chanques et al., ICM 2009;35:2060-7

Critical-Care Pain Observation Tool
(CPOT; Gélinas et al., AJCC 2006; 15:420-7)
© Gélinas, 2013
Facial Expressions
Relaxed
0
Tense
1
Grimacing
2
Body Movements
Absence of movements or
normal position
0
Protection
1
Agitation
2
Muscle Tension Relaxed
0
Tense, rigid
1
Very tense/rigid
2
Compliance with the
Ventilator (intubated)
Tolerating ventilator or movements
0
Coughing but tolerating
1
Fighting ventilator
2
Vocalization (extubated)
Normal or silent
0
Sighing or moaning
1
Crying out or sobbing
2
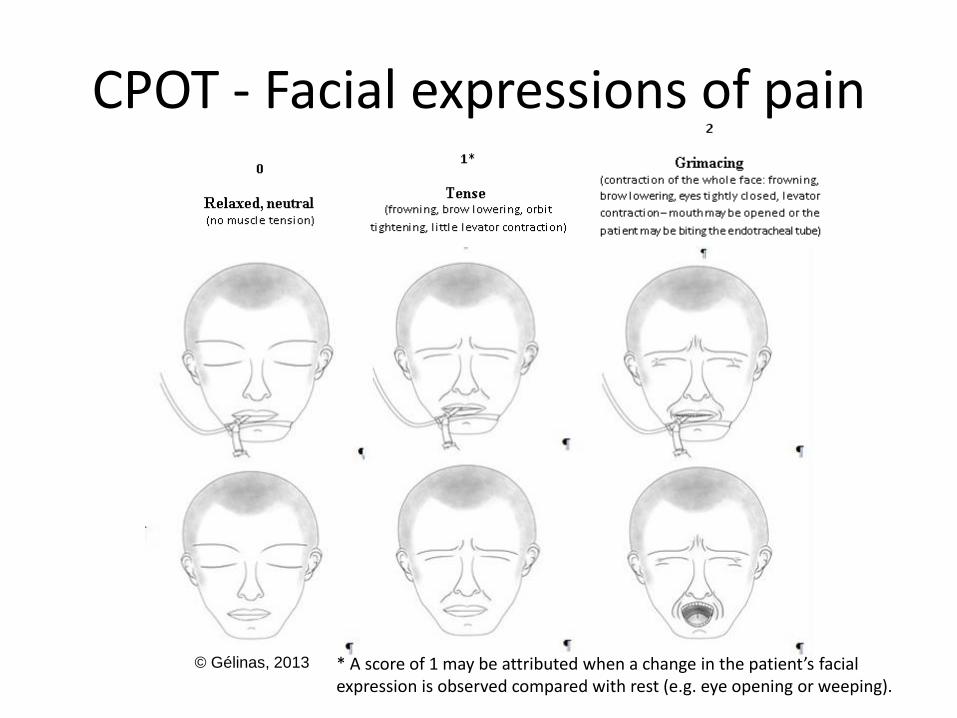
CPOT - Facial expressions of pain
© Gélinas, 2013 * A score of 1 may be attributed when a change in the patient’s facial expression is observed compared with rest (e.g. eye opening or weeping).

Cut-off scores for significant pain
CPOT>2 (see ROC: Gélinas et al., 2009)
BPS>5 (Payen et al., 2007)

Impact of their use in ICU practice
CPOT (Gélinas et al., 2011; Rose et al., 2013) ↑ documentation of pain assessments
Changes in analgesic and sedative use
ICU nurses reported that it helped them assess pain more effectively, but inter-professional communication of pain assessment findings was identified as an area for improvement
BPS (Chanques et al., 2006; Radtke et al., 2012) ↑ documentation of pain assessments
↓ incidence of pain
Changes in analgesic and sedative use
↓ MV duration and nosocomial infections
Training: To plan carefully
See CPOT teaching video at
http://pointers.audiovideoweb.com/stcasx/il83win10115/CPOT2011-
WMV.wmv/play.asx
Funded and created by
Kaiser Permanente Northern California Nursing Research

Clinical Practice Recommendations Concerning Pain
Assessment in the Patient Unable to Self-Report American Society for Pain Management Nursing (Herr et al., PMN 2011; 12:230-50)
Attempt to obtain the patient’s self-report of pain – Gold standard A simple yes or no = valid self-report
Look for behavioral changes Use a standardized and valid behavioral pain scale
The family can help to identify pain behaviors
Sources of pain = “Assume pain is present”
Attempt an intervention for pain relief
1
2
3
4

Clinical Practice Recommendations Concerning Pain
Assessment in the Patient Unable to Self-Report American Society for Pain Management Nursing (Herr et al., PMN 2011; 12:230-50)
Be cautious when interpreting a behavioral score!
self-report score
Allows the detection of the presence/absence of pain
Allows the assessment of intervention effectiveness
Related to changes observed in behaviors

Clinical Practice Recommendations Concerning Pain
Assessment in the Patient Unable to Self-Report American Society for Pain Management Nursing (Herr et al., PMN 2011; 12:230-50)
Be cautious with vital signs!
Have not been found to be valid for assessing pain
No change No pain
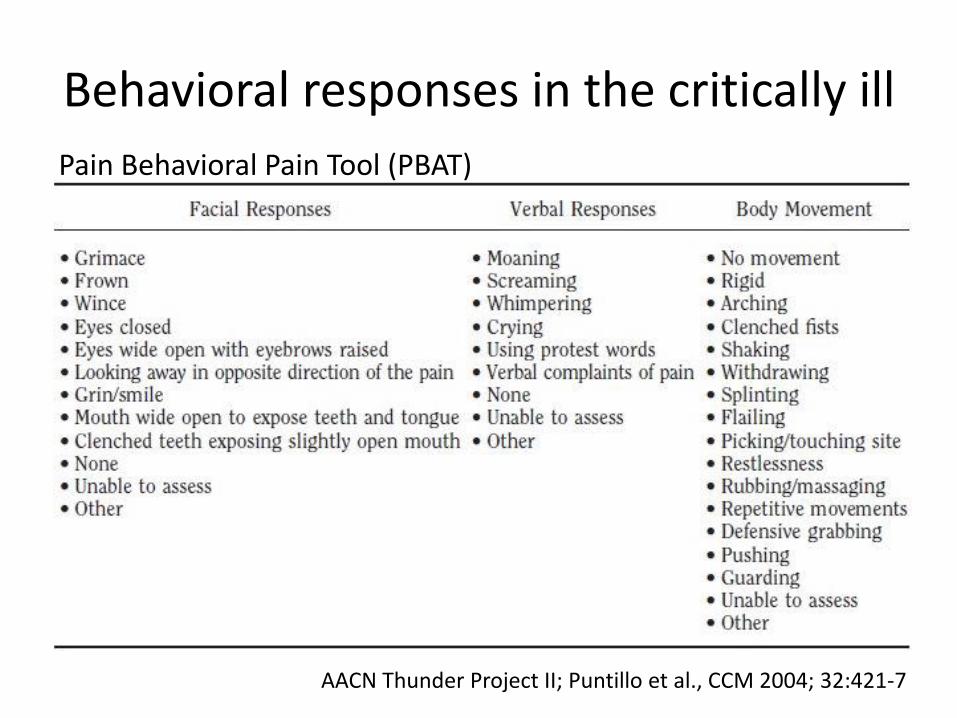
Behavioral responses in the critically ill
Pain Behavioral Pain Tool (PBAT)
AACN Thunder Project II; Puntillo et al., CCM 2004; 32:421-7
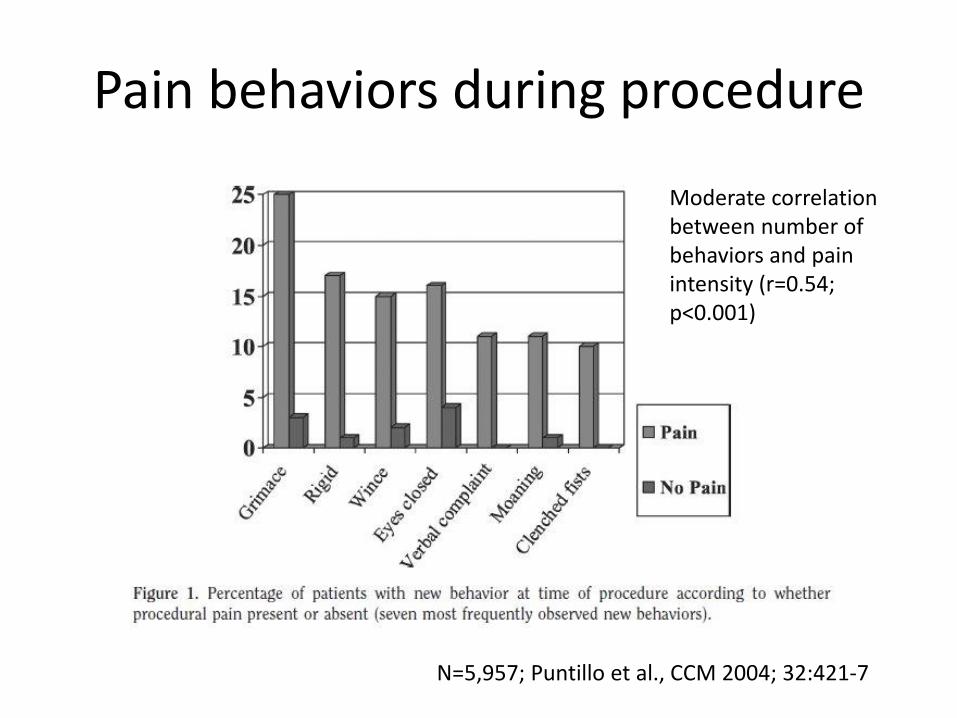
Pain behaviors during procedure
N=5,957; Puntillo et al., CCM 2004; 32:421-7
Moderate correlation between number of behaviors and pain intensity (r=0.54; p<0.001)
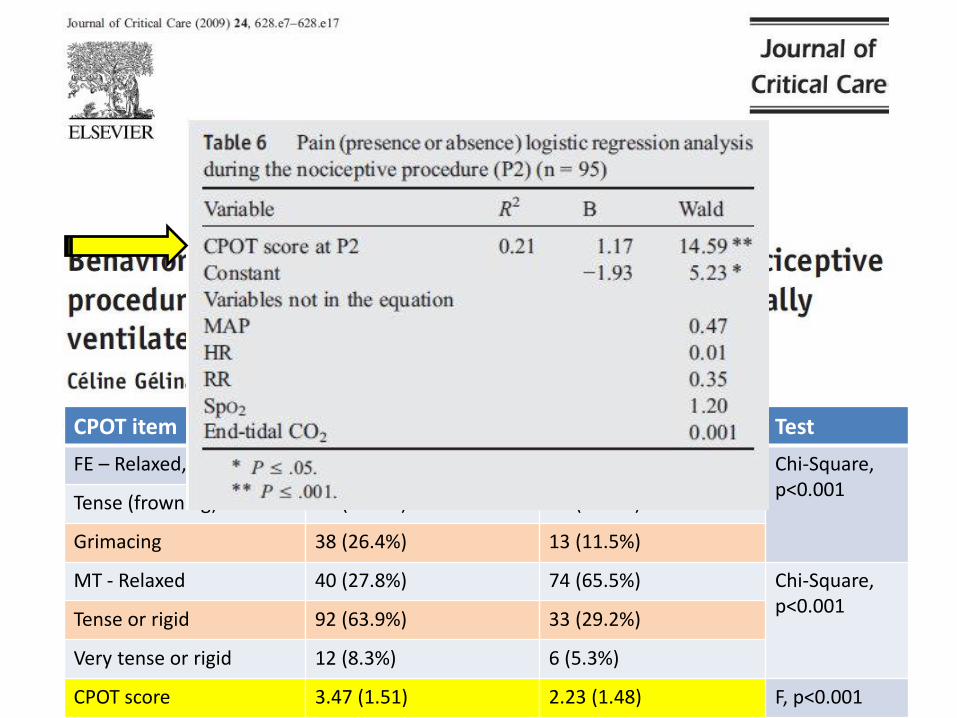
CPOT item Conscious (n=144) Unconscious (n=113) Test
FE – Relaxed, neutral 16 (11.1%) 35 (31%) Chi-Square, p<0.001
Tense (frowning) 90 (62.5%) 65 (57.5%)
Grimacing 38 (26.4%) 13 (11.5%)
MT - Relaxed 40 (27.8%) 74 (65.5%) Chi-Square, p<0.001
Tense or rigid 92 (63.9%) 33 (29.2%)
Very tense or rigid 12 (8.3%) 6 (5.3%)
CPOT score 3.47 (1.51) 2.23 (1.48) F, p<0.001

In press in PMN, available online
N=10 moderate to severe critically ill TBI patients with altered LOC
New behaviors observed in 5 or more TBI patients during turning
Frowning Levator contraction Eye opening Eye weeping Eyebrow raising
CPOT developments
Adaptation of the CPOT content for brain-injured ICU patients with altered LOC (Funded by CIHR and FRQ-S; Gélinas, Topolovec-Vranic et al. with Dr. Kathleen Puntillo)
Phase 1 – Item generation
Phase 2 – Content validation
Phase 3 – Validation of CPOT-Neuro at the ICU bedside

Phase 1: Different brain-injured patient groups under observation
Elective brain surgery group (N=43)
Mainly conscious, awake, and stable
Use of original CPOT was found to be valid (Echegaray-Benites, Kapoustina & Gélinas, under review)
Neuro medical group (N=53)
TBI group (target N=95, now at 91)
Gélinas, Topolovec-Vranic et al.
Nociceptive and non-nociceptive procedures

Conscious post-op brain surgery
Video used with permission

Phase 1: TBI group
Some findings from 84 critically ill TBI patients
Mostly men (76.2%)
Mean age of 54 years (SD=22.7)
Mild (23.7%), moderate (33.8%) and severe (42.5%) TBI
Frontal region (51.8%), fall as a main cause (51.2%)
Conscious – GCS >13 (n=14, 16.7%)
Reduced LOC – GCS 9-12 (n=35, 41.7%)
Unconscious – GCS <8 (n=35, 41.7%)
Conscious TBI exhibited more behaviors (mean=5.8) compared to those with reduced LOC (mean=4.0) and unconsciousness (mean=2.0) (p<0.001)
Gélinas, Topolovec-Vranic et al. Picture reproduced with permission
New behaviors observed during turning
Frowning (39.3%) Eye opening (36.9%) Mouth opening (21.4%) Limb movements (21.4%) Eye weeping (13.1%)
Were mainly absent Grimacing (84.5%) Muscle rigidity (86.9%)
Severe TBI patient with altered LOC
Video used with permission

Severe TBI patient with altered LOC
Video used with permission

Cerebral stroke with altered LOC
Video used with permission
What to remember
Brain-injured ICU patients with altered LOC seem to present atypical behavioral responses to pain which would necessitate some modification of the content of existing scales
By the mean time, we should follow clinical recommendations and guidelines and look for behavioral changes when a patient is exposed to procedures known to be painful and intervene accordingly
“ “ “ “
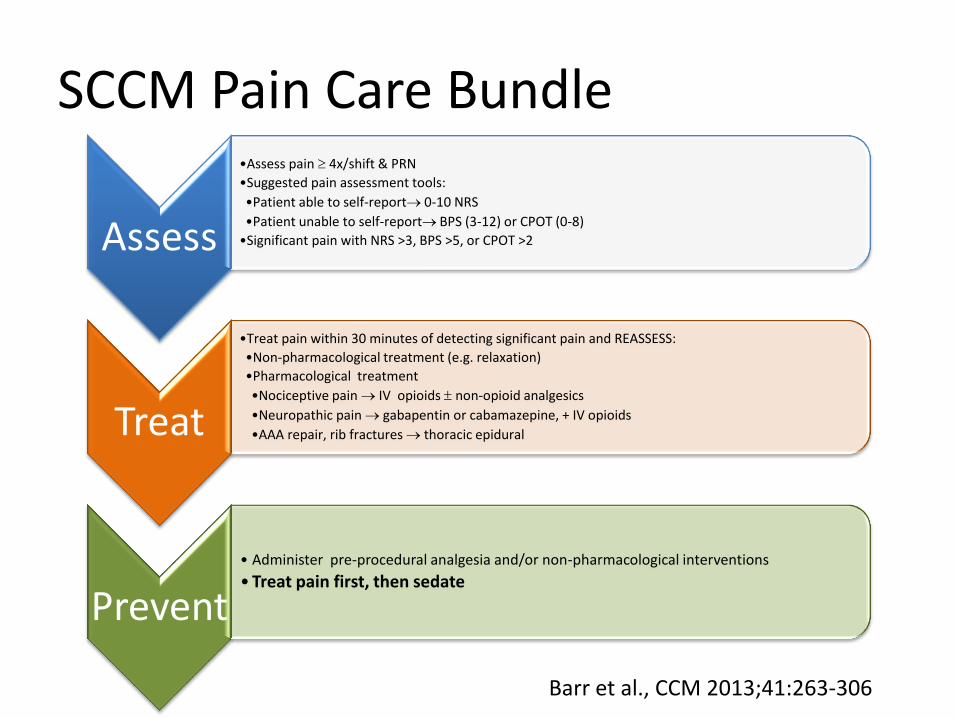
SCCM Pain Care Bundle
Assess
•Assess pain 4x/shift & PRN
•Suggested pain assessment tools:
•Patient able to self-report 0-10 NRS
•Patient unable to self-report BPS (3-12) or CPOT (0-8)
•Significant pain with NRS >3, BPS >5, or CPOT >2
Treat
•Treat pain within 30 minutes of detecting significant pain and REASSESS:
•Non-pharmacological treatment (e.g. relaxation)
•Pharmacological treatment
•Nociceptive pain IV opioids non-opioid analgesics
•Neuropathic pain gabapentin or cabamazepine, + IV opioids
•AAA repair, rib fractures thoracic epidural
Prevent
• Administer pre-procedural analgesia and/or non-pharmacological interventions
• Treat pain first, then sedate
Barr et al., CCM 2013;41:263-306

A source of inspiration
The most practical lesson that can be given to nurses is to teach them what to observe and how to observe
Florence Nightingale
