swedish organization for global health : the maama...
TRANSCRIPT

Swedish Organization for Global Health : The Maama Project – Annual Report 2014 2
“Every year, 438 women per 100,000 live births die in Uganda due to
birth related problems… However, many of these can be prevented by
simple, evidence based interventions.”
Maternal mortality in Uganda is 68.5 times higher than in Sweden.
Every year, 438 women per 100,000 live births die in Uganda due
to birth related problems and complications1, with infections
responsible for 15% of the deaths.2 Moreover, Uganda has the
fifth highest newborn mortality in Sub-Saharan Africa with 29
deaths per 1,000 live births for infants under 28 days of age.3 The
most common causes of neonatal deaths in Uganda are
complications due to preterm births, asphyxia and infections.4 An
unclean delivery environment is one of the main factors that
contribute to the high rate of infections in both mothers and their
newborns.5 One third of all infant deaths (deaths during the first
year of life), happen during the first month. Even though infant
mortality and under-five mortality are decreasing in Uganda,
newborn mortality has remained constant for the past twenty
years.6
Many maternal and newborn deaths can be prevented by simple,
evidence-based interventions. Evidence shows that 15-32% of
neonatal deaths can be prevented through clean delivery
environment, hygienic cord care, thermal care, early and exclusive
breastfeeding and community-based care for low birth weight.7
Many complications can be prevented by monitoring the health of
the mother and the baby during antenatal and postnatal visits and
through safe motherhood training that can be conducted by
community health workers; health knowledge plays a large role in
newborn survival, with an estimate of 50% of newborn deaths in
rural Uganda being caused to delays in recognizing problems or
making the decision to seek care.8
Increasing attention has been drawn to women's and newborns'
health in view of the post-2015 sustainable development agenda
with the launch of United Nation's Global Strategy for Women's
and Children's Health (2010), the Commission on Life Saving
Commodities for Women and Children (2012) and the Every
Newborn Action Plan by WHO and Unicef. Increased efforts must
be made especially in countries like Uganda that have not
achieved the Millennium Development Goals 4 and 5.
In light of these circumstances, the Swedish Organization for
Global Health, in partnership with the Uganda Development and
Health Associates (UDHA), established the Maama Project, a
scheme to educate expectant and new mothers in rural Uganda
about safe and hygienic childbirth methods and newborn care
with the aim of improving maternal health outcomes and reducing
infant mortality.
The Maama Project: Background The Maama Project was established in 2014 by the Swedish
Organization for Global Health (SOGH) and aims to improve health
outcomes for mothers and children in rural Uganda through
education and advice. Here is why the project was established…
Swedish Organization for Global Health : The Maama Project – Annual Report 2014 3
Mayuge district is a region in southeastern Uganda. It consists of
12 sub-counties and 385 villages. 58.9% of the population is under
18, whereas 4.4% are over 60. The district has an annual
population growth rate of 3.5%. The most recent literacy level
from 2002 was 63%. The fertility rate is 7 children per woman,
higher than the national average. 72% of the rural population
depends on subsistence farming.9
Uganda Development and Health Associates (UDHA), a local NGO,
has been financing a rural health clinic in Maina village, in Buwaya
sub-county of Mayuge district. The health clinic covers Maina
Parish, consisting of four villages with an estimated population of
3,312, of which 900 are women of childbearing age (15-49 years
old)10
. The health clinic is entirely financed by UDHA with the
exception of the salaries for the two nurses, which are covered by
the Ugandan government. The healthcare center provides free
antenatal and postnatal care to all pregnant women in the area.
Currently, only 12% of the women who attend the antenatal clinic
complete all four recommended visits and 64% give birth in health
facilities.11
An estimated 20 women give birth in Maina parish every month.
Most women who access the health facilities for delivery face a
lack of basic materials such as sterile gauze, cotton wool, sterile
cloths, blades and gloves needed to conduct safe deliveries. The
situation has led to general frustration, because pregnant women
are asked to purchase and bring delivery materials with them.
Most women in Maina Parish lack the means and access to
purchase these items, leading the women to avoid going to the
health facility or bringing with them the bare minimum of items
that may not be sterile or suitable.
Consequently, Mayuge district was identified as an area that could
significantly benefit from the Maama Project’s aim to improve
access to education and resources that promote and facilitate a
safer birth environment.
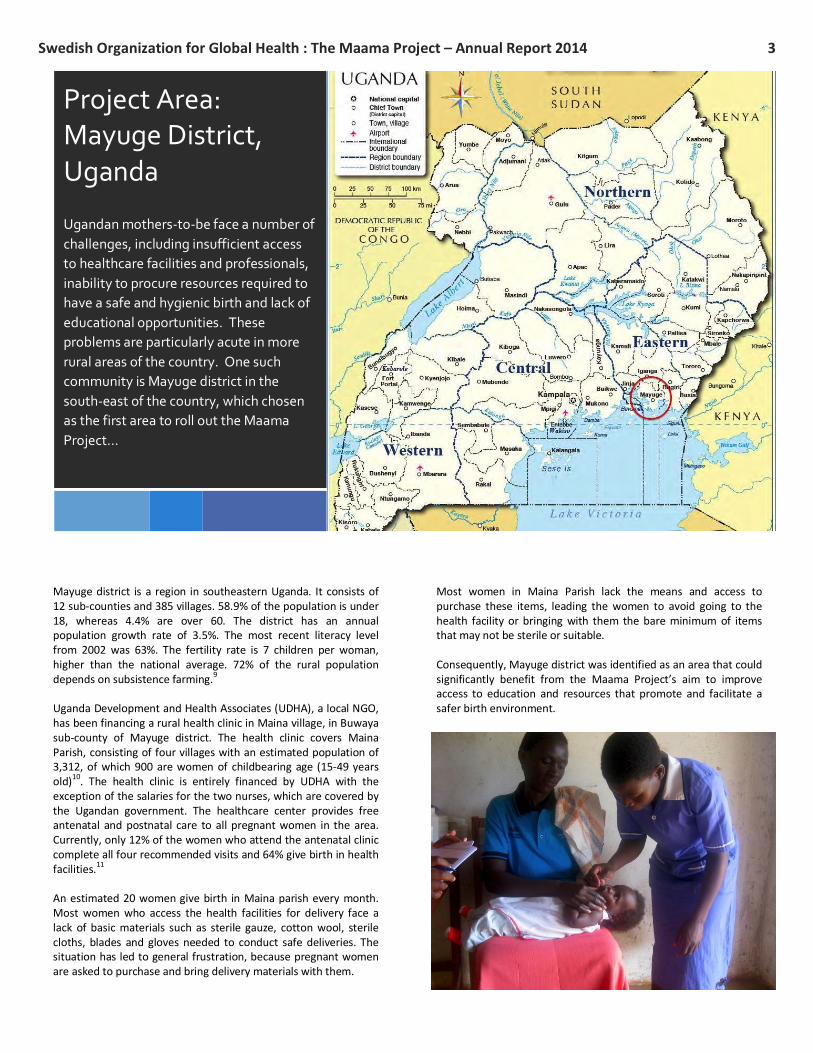
Project Area:
Mayuge District,
Uganda
Ugandan mothers-to-be face a number of
challenges, including insufficient access
to healthcare facilities and professionals,
inability to procure resources required to
have a safe and hygienic birth and lack of
educational opportunities. These
problems are particularly acute in more
rural areas of the country. One such
community is Mayuge district in the
south-east of the country, which chosen
as the first area to roll out the Maama
Project…
Swedish Organization for Global Health : The Maama Project – Annual Report 2014 4
The project consists of the provision of birth kits to pregnant
women, and health training and home visits provided by
community health workers. The community health workers' task is
to identify pregnant women and conduct two home visits where
the woman will be provided information on birth preparedness,
safe motherhood and newborn care. The CHWs also stress the
importance of attending antenatal visits at the health clinic. As an
incentive, a birth kit will be offered free of charge to all women on
their fourth visit. After birth, the community health workers will
visit the mother for three postnatal checkups after 24 hours, 3
days and 7 days.
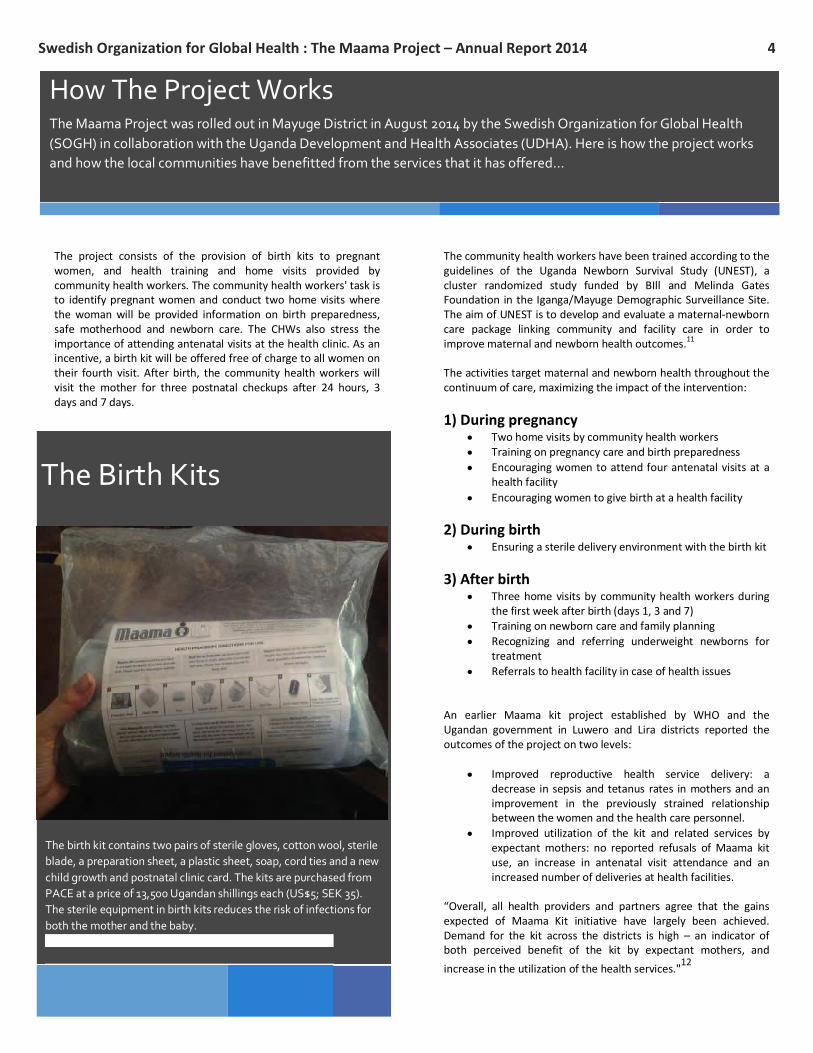
The Birth Kits
The birth kit contains two pairs of sterile gloves, cotton wool, sterile
blade, a preparation sheet, a plastic sheet, soap, cord ties and a new
child growth and postnatal clinic card. The kits are purchased from
PACE at a price of 13,500 Ugandan shillings each (US$5; SEK 35).
The sterile equipment in birth kits reduces the risk of infections for
both the mother and the baby.
The community health workers have been trained according to the
guidelines of the Uganda Newborn Survival Study (UNEST), a
cluster randomized study funded by BIll and Melinda Gates
Foundation in the Iganga/Mayuge Demographic Surveillance Site.
The aim of UNEST is to develop and evaluate a maternal-newborn
care package linking community and facility care in order to
improve maternal and newborn health outcomes.11
The activities target maternal and newborn health throughout the
continuum of care, maximizing the impact of the intervention:
1) During pregnancy Two home visits by community health workers
Training on pregnancy care and birth preparedness
Encouraging women to attend four antenatal visits at a
health facility
Encouraging women to give birth at a health facility
2) During birth Ensuring a sterile delivery environment with the birth kit
3) After birth Three home visits by community health workers during
the first week after birth (days 1, 3 and 7)
Training on newborn care and family planning
Recognizing and referring underweight newborns for
treatment
Referrals to health facility in case of health issues
An earlier Maama kit project established by WHO and the
Ugandan government in Luwero and Lira districts reported the
outcomes of the project on two levels:
Improved reproductive health service delivery: a
decrease in sepsis and tetanus rates in mothers and an
improvement in the previously strained relationship
between the women and the health care personnel.
Improved utilization of the kit and related services by
expectant mothers: no reported refusals of Maama kit
use, an increase in antenatal visit attendance and an
increased number of deliveries at health facilities.
“Overall, all health providers and partners agree that the gains
expected of Maama Kit initiative have largely been achieved.
Demand for the kit across the districts is high – an indicator of
both perceived benefit of the kit by expectant mothers, and
increase in the utilization of the health services."12
How The Project Works
The Maama Project was rolled out in Mayuge District in August 2014 by the Swedish Organization for Global Health
(SOGH) in collaboration with the Uganda Development and Health Associates (UDHA). Here is how the project works
and how the local communities have benefitted from the services that it has offered…
Swedish Organization for Global Health : The Maama Project – Annual Report 2014 5
The Maama Project aims to build a community-based
approach to improving healthcare outcomes for
expectant and new mothers and their infants.
The project has five main objectives that it seeks to
achieve…
Project Objectives
1. Strengthen and invest in care during labor,
birth and the first day and week of life
The birth kits will enable the women to have a hygienic delivery,
reducing the risk of infection for the mother and the baby. The
services offered by the clinic will be complemented by CHW home
visits during pregnancy and after birth.
2. Improve the quality of maternal and newborn
care
Birth kits are a cost-effective way to make a delivery safer when
the health facility suffers from a lack of resources and equipment.
The availability of local CHWs will enable women to access
information on issues related to health and pregnancy and receive
advice on when and where to seek help for health issues. The
CHWs encourage the women to attend antenatal visits, making it
possible to monitor the health of the woman and her baby.
3. Reach every woman and newborn to reduce
inequities
The community health worker visits and birth kits are free and the
birth kits are offered to every pregnant woman on their fourth
antenatal visit. Women living further away from the clinic are also
reached as the CHWs conduct home visits at every house in their
home villages.
4. Harness the power of parents, families and
communities
The local community leaders are working closely with the project
and have given it their full approval. All community health workers
have been recruited from the local villages and are respected by
their community. The training of the CHWs, interactions with
beneficiaries and monitoring of the project are all conducted
entirely in Lusoga, the local language in the area.
5. Count every newborn through measurement,
program tracking and accountability
Monitoring and evaluation is conducted on CHW training,
activities, and services to mothers including monitoring of
deliveries and birth outcomes. Baseline data has been collected in
order to measure program success.

Swedish Organization for Global Health : The Maama Project – Annual Report 2014 6
2014 Project Outcomes to Date Monthly data and reports are collected to ensure that the impact of the project in Mayuge district can be evaluated.
The first five months of the project from August 2014 to December 2014 have already demonstrated the impact that
the project has had…
0
5
10
15
20
25
Visit 1 Visit 2 Visit 3 Visit 4
Av
erg
ae
Mo
nth
ly V
isit
s
Antenatal Visits
Pre-Project (May 13 -
Jun 14)
Project (Aug 14 - Dec
14)
0
20
40
60
80
100
120
140
Aug-14 Sep-14 Oct-14 Nov-14 Dec-14
Nu
mb
er
of
Vis
its
Women Reached by CHWs by
District
Mwezi
Maina
Kyete
Girigiri
CHWs in the four subregions of
Mayuge district have been responsible
for 531 visits to women who are either
expecting or of child-rearing age. As
well as their role in educating mothers,
CHWs have also been able to reach out
to fathers within the community and
encourage them to support their wives
by helping them with transport
arrangements or procurement of items
to help with a hygienic and safe
delivery.
The Maama Project has contributed to a
significant increase in expectant
mothers in the project areas attending
antenatal appointments. This has been
particularly remarkable in respect of
fourth visit attendances, which have
increased by 760%. Expectant mothers
attending a fourth antenatal visit not
only benefit from critical checks on both
their own and their child’s health, but
are also able to take advantage of the
free clean birth kit.

Swedish Organization for Global Health : The Maama Project – Annual Report 2014 7
0%
20%
40%
60%
80%
100%
% o
f B
irth
s
Birth Locations
Non-Health Facility
Births
Health Facility Births
2014 Project Outcomes to Date
(continued)
0
5
10
15
20
25
30
Aug-14 Sep-14 Oct-14 Nov-14 Dec-14Nu
mb
er
of
Bir
th K
its
Dis
trib
ute
d
Birth Kit Distribution
One of the main goals of the Maama Project
is to encourage women to give birth in a
healthcare facility where they can benefit
from medical professionals and avoid the
risks associated with home births. Although
transportation issues often present
problems in more rural parts of the
community, 63% of births in the project
duration took place in healthcare facilities, in
line with the national average. This is an
area, therefore, that CHW will continue to
target as they seek to encourage women to
give birth in the safest possible
environment.
A total of 87 birth kits have been
distributed to expectant mothers,
relieving them of the financial burden of
buying their own sanitary birth
materials. In turn, this has helped those
mothers minimize the risk of infection
during birth and help rebalance some of
the financial inequalities that exist
between the different communities
within the project area.
Swedish Organization for Global Health : The Maama Project – Annual Report 2014 8
The training of Community Healthcare Workers (CHWs) is a key cornerstone of
the Maama Project. To date, ten CHWs have been trained to deliver advice to
new and expectant mothers. Here is what they have to say about their
experiences….
‘’The best part of being a CHW is being known as a helper. I learnt that health centers contribute a
lot to the well being of the community’. Mothers have no bad reactions on the visits and birth kits
but call for the project to continue running.’’
Naigoma Zam, CHW, Mwezi B
‘’The best part of being a CHW is that you learn to solve your own problems because of the
different training you get from different organizations. I learnt that human health at home is
everyone’s responsibility. Mothers have appreciated the visits and birth kits and there is also
increased male involvement in child birth planning in some homes.’’
Naigaga Zaina, CHW, Girigiri
“The best part of being a CHW is that you act as a role model to the community so there is a lot of
respect if you also work well. I learnt to maintain sanitation and hygiene at home through the
training I got from different people. Mothers are so happy with the home visits and the birth kits
given to them. The information passed out to the community has helped both mother and father
to be involved in birth preparedness.”
Namalero Tabisa, CHW, Mwezi A
“The best part of being a CHW is that you acquire some knowledge that you didn’t have and you
are always informed about all health policies. I learnt basic techniques of counseling and gained
confidence to talk in public. Mothers are positive to both home visits and the birth kits, they also
give thanks to UDHA for remembering their community and giving them that type of help. The
community has benefited a lot. Before this project, fathers could not be bothered helping mothers
to prepare for birth but as of now fathers even fetch water for their pregnant wives and also buy
most of the necessary materials for birth.”
Mirembe Agness, CHW, Maina
Community Healthcare Workers (CHWs)

Swedish Organization for Global Health : The Maama Project – Annual Report 2014 9
As well as dispensing valuable advice,
CHWs can also perform a wider role
within their communities. Here is a story
about how one CHW went beyond the call
of duty…
Scovia Wandera is one of the Community Health Workers trained by the
Maama Project in Mwezi village to give advice to expectant mothers about
accessing antenatal services, preparing for childbirth, giving birth in a formal
health center and caring for infants and young children.
One of the women impacted by the Maama Project in Mwezi was Monica
Kagoya, who first met Scovia when she was five months pregnant with her
fourth child. Monica had recently moved to a more remote area in the region
and was concerned that she wouldn’t be able to access healthcare facilities
due to a lack of transportation. However, through Scovia’s advice and
incentive of the free clean birth kit, Monica was encouraged to attend her
remaining antenatal visits during her pregnancy to ensure that she was
prepared adequately for the birth.
However, one night between her third and fourth antenatal visits, Monica
began the onset of early labor. Her family was too far away from the health
center to be transported there, so Monica called upon her trusted neighbor
Scovia to give her some assistance. Scovia was able to use her training to
support Monica and help her give birth successfully to a boy that she called
Kirabo or ‘gift’. Monica said that she felt that Scovia’s assistance was
invaluable and felt that the experience was like giving birth in a hospital.
Although Scovia’s role is as a local educator rather than a midwife, Kirabo’s
birth demonstrates the trusted position that CHWs hold within their
communities and the invaluable role that they can play in supplementing
existing healthcare resources in areas where demand often outstrips supply.
- Attribution
’The best part of being a CHW is that you gain respect from the community if you help the people. I
learnt that all people offering help to the community need appropriate training before helping because
you deal with different people, cases and problems. Mothers are always positive to the visits and feel
they are being helped a lot when we give them the birth kits. The community has benefited from the
project, especially mothers because before they had no access to information or encouragement to go
to health care facilities. However, now that they have got CHWs, they get informed on everything and
move some distances to go for antenatal classes at Maina or Mayuge.”
Scovia Wandera, CHW, Mwezi

Swedish Organization for Global Health (SOGH)
Address: Katarina Västra Kyrkogata 4, 116 25 Stockholm, Sweden
Email: [email protected]
Website: http://www.sogh.se
Organization-No. 802490-6664
Report compiled by Chris Barstow
References:
1 gapminder.org
2 World Health Organization (WHO). “Making Pregnancy Safer: A health sector strategy for
reducing maternal and perinatal morbidity and mortality.” (Unpublished) (2000). 3 Ministry of Health, Government of Uganda (2008). Situation analysis of newborn health in Uganda.
4 Ministry of Health. Situation analysis of newborn health in Uganda: current status and opportunities to improve care and survival. Kampala: Government of Uganda.
Save the Children, UNICEF,WHO; 2008. 5 WHO. “Care of the Umbilical Cord: A Review of the Evidence.” http://www.who/int.rht/
documents/MSM98-4/MSM-98-4.htm (1 June 2000). 6 Ministry of Health. Situation analysis of newborn health in Uganda: current status and opportunities to improve care and survival. Kampala: Government of Uganda.
Save the Children, UNICEF,WHO; 2008. 7 Bhutta, Z. A., Darmstadt, G. L., Hasan, B. S., & Haws, R. A. (2005). Community-based interventions for improving perinatal and neonatal health outcomes in
developing countries: a review of the evidence. Pediatrics,115(Supplement 2), 519-617. 8 Waiswa P, Källander K, Peterson S et al. Using the three delays model to understand why newborn babies die in eastern Uganda. Trop Med and Int Health, 2010, 15:
964-972. 9 Mayuge District (2009). Higher Local Government Statistical Abstract. http://www.ubos.org/onlinefiles/uploads/ubos/2009_HLG_%20Abstract_printed/Mayuge.pdf
10 Mayuge District (2009). Higher Local Government Statistical Abstract. http://www.ubos.org/onlinefiles/uploads/ubos/2009_HLG_%20Abstract_printed/Mayuge.pdf
11Baseline data collected in June 2014.
12 Information brief about the Uganda newborn survival study (UNEST).
http://www.healthynewbornnetwork.org/sites/default/files/resources/WHAT%20IS%20UNEST.pdf