sussex type 2 diabetes treatment algorithm 2021
TRANSCRIPT

8

1
Sussex Type 2 Diabetes Treatment Algorithm 2021
Type 2 diabetes is a chronic, progressive condition characterised by insulin resistance, reduced pancreatic insulin production and lipid dysregulation. It accounts for 90% of the cases of diabetes in the UK and is associated with overweight and obesity. The condition can lead to several co-morbidities including cardiovascular disease, heart failure, peripheral vascular disease, chronic kidney disease, retinal disease and neuropathy as well as psychological impacts for patients.
Whilst dietary and lifestyle interventions remain the cornerstone of diabetes care, many people go on to develop chronic type 2 diabetes. Management of type 2 diabetes should include a thorough assessment and mitigation of any potential risk factors for the major complications. The NICE 9 Key care processes help guide clinicians to perform reviews comprehensively. In the presence of diabetes and obesity offer the patient a range of dietary interventions including low calorie diet or low carbohydrate diet see https://www.diabetes.org.uk/guide-to-diabetes/enjoy-food/eating-with-diabetes/i-have-type-2-diabetes
Offer the NHS Digital Weight Management Service for people living with diabetes who have a BMI >/= 30 (adjusted to >/= 27.5 in BAME population). See https://www.england.nhs.uk/digital-weight-management/ for details on referral and exclusion criteria.
Once type 2 diabetes is established it is recommended that blood glucose lowering agents are used by all international guidelines. The aim of treatment is to reduce HbA1c to agreed target levels in order to reduce long term complications from diabetes. The current NICE guideline, NG28, which was published in 2015 includes an algorithm for incremental addition of oral or subcutaneous agents depending on individualised HbA1c targets. It does not however provide specific guidance on which agents should be used to help prevent complications, potentially leading to variations in prescribing often informed by clinician’s confidence or experience. It is widely acknowledged by diabetes specialists that the NICE algorithm has become outdated.
Internationally, both the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) produce guidelines that are updated more regularly and take account of the major advances in diabetes trials, in particular, noting the advantages that newer classes of blood glucose lowering agents possess in reducing Major Adverse Cardiovascular Events (MACE), hospitalisation for Heart Failure (hHF), Cardiovascular death and CKD progression.
The Sussex Type 2 Diabetes Treatment Algorithm takes the treatment suggestions from the 2019 ADA/EASD guideline and allocates drug names within each section. Metformin remains the first drug of choice for all patients who can tolerate it. When adding medication to the treatment regime to improve control and reduce risk factors, the suggestion of which drug to use has been made with reference to the drug which has the best evidence within its class. Where there is no difference between drugs within a class, the most cost effective

2
drug has been chosen. The main factors to guide clinician choice include an assessment of any pre-existing complications from diabetes, or patient specific factors that would help guide drug choice. When assessing a patient, it is good practice to establish whether:
1. The patient has any existing atherosclerotic cardiovascular disease (ASCVD)
2. The patient is at very high risk of developing ASCVD (aged 55 and has carotid, coronary or peripheral artery stenosis >50%, or LVH)
3. The patient has Heart Failure with reduced Ejection Fraction (HFrEF- Ejection fraction <40%)
4. The patient has CKD with albuminuria (eGFR >30 and urine albumin >30mg/mmol) 5. The patient needs to avoid or minimise the risk of hypoglycaemia (eg: occupation,
driving) 6. There are compelling reasons why weight gain would be undesirable for the patient 7. If none of the above applies, then the treatment choice for the patient should follow
the most cost effective regime 8. Ethnicity
It should be stressed that addressing cardiovascular risk reduction globally should be undertaken at least annually, including blood pressure, smoking status and lipids. These should all be treated within treatment targets. At each review an assessment of the patient’s current risk factors should be reassessed as these may have changed since the last review. At each review lifestyle and diet advice should be reinforced. If HbA1c remains above the agreed treatment target for that patient, then adjustments should be made every 3-6 months in discussion with the person living with type 2 diabetes. This could include optimising the dose of the current medication or adding a drug of a different class. Drugs that have been ineffective and not led to a measurable improvement in HbA1c should be stopped.
As a supplement to the guideline, we have produced a document entitled ‘Guidance on setting HbA1c targets’. This includes targets that can be individualised depending on patients’ frailty and uses the ADA/ American Geriatric Society recommendations and well as the Quality and Outcomes Framework targets with the aim of relaxing targets and deprescribing for frail patients and patients who are receiving end of life care.
Prescribers should familiarise themselves with the indications and contra-indications as well as interactions listed in the BNF and/or the Electronic Medicines Compendium before initiating therapies. The authors cannot be held liable for any adverse events that occur if medicines are prescribed outside of their licenced indications. Please familiarise yourself with the common side effects and caveats that follow the main guidance. Again, this list is not exhaustive.

3
Additional Guidance and Caveats Sick Day Rules Counselling Points
Unwell/ Acute Illness Fever, sweats, rigors Vomiting, diarrhoea Unable to eat or drink
Omit/Pause S- SGLT2-i
A- ACEi
D- Diuretics
M- Metformin
A- ARB
N-NSAIDS
Consider? ketones
After 2-3 days
If feeling better restart paused meds
If no better review
If monitoring glucose- increase frequency and check for ketones. If on Insulin or SU may need to adjust dose. Ensure optimal fluid control
ABCD have produced an educational resource for non-specialists to support safe initiation SGLT-2 inhibitors in people with type 2 diabetes-An educational resource for health care professionals who are not diabetes specialists (updated September 2020) | ABCD (Diabetes Care) Ltd
Signs and symptoms of DKA • Excessive thirst • Polyuria • Dehydration • Shortness of breath and laboured breathing • Abdominal pain • Leg cramps • Nausea and vomiting • Mental confusion and drowsiness • Ketones can be detected on the person’s breath (pear-drop smell) or in
the blood or urine

4
Lifestyle Counselling – to be reiterated to patients at every opportunity
Medication review
Reassess needs and complications every 6 months- remember the patient may have changed their risk factors since the last review, eg had and MI which may alter treatment choices. Stop medications that are not effective or have had no effect on HbA1c (unless they were also beneficial for other conditions eg SGLT2-I for heart failure with reduced ejection fraction). Remember to adjust for renal function and liver disease (see next section).
GLP-1 RA
Beware increased risk of retinopathy after starting GLP-
1 RA. Make sure retinal screening up to date.
Beware of the signs of acute pancreatitis- persistent and
severe abdominal pain with or without vomiting.
SGLT2-i
Stop if foot ulcer.
Beware groin gangrene.
Beware euglycaemic DKA.
TZD
Stop if – Heart failure, bladder cancer or DKA.
Beware atypical fractures.
DPP-4i
Don’t use in conjunction with GLP-1 RA.
Beware of the signs of acute
pancreatitis.
SU
Stop and reassess if frequent hypos. Caution low eGFR.
Useful as rescue therapy if
symptomatic or high HbA1c, review once symptoms resolve
+/- target HbA1c achieved.
5
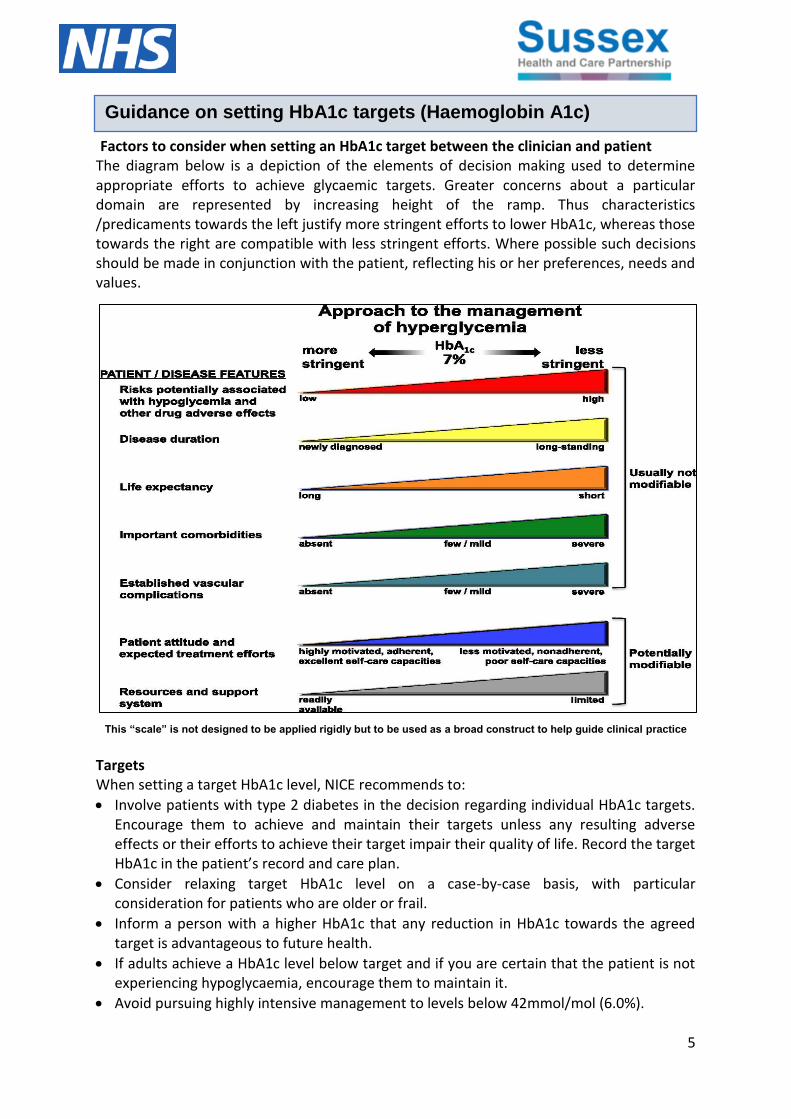
Factors to consider when setting an HbA1c target between the clinician and patient The diagram below is a depiction of the elements of decision making used to determine appropriate efforts to achieve glycaemic targets. Greater concerns about a particular domain are represented by increasing height of the ramp. Thus characteristics /predicaments towards the left justify more stringent efforts to lower HbA1c, whereas those towards the right are compatible with less stringent efforts. Where possible such decisions should be made in conjunction with the patient, reflecting his or her preferences, needs and values.
This “scale” is not designed to be applied rigidly but to be used as a broad construct to help guide clinical practice
Targets When setting a target HbA1c level, NICE recommends to:
Involve patients with type 2 diabetes in the decision regarding individual HbA1c targets. Encourage them to achieve and maintain their targets unless any resulting adverse effects or their efforts to achieve their target impair their quality of life. Record the target HbA1c in the patient’s record and care plan.
Consider relaxing target HbA1c level on a case-by-case basis, with particular consideration for patients who are older or frail.
Inform a person with a higher HbA1c that any reduction in HbA1c towards the agreed target is advantageous to future health.
If adults achieve a HbA1c level below target and if you are certain that the patient is not experiencing hypoglycaemia, encourage them to maintain it.
Avoid pursuing highly intensive management to levels below 42mmol/mol (6.0%).
Guidance on setting HbA1c targets (Haemoglobin A1c)
53
6
Patient decision aids can help adults with type 2 diabetes think about their options for controlling their blood glucose to try to reduce the long-term risks of diabetes. NICE patient decision aids can be found here. (NICE NG28 resources)
Individualised care
Adopt an individualised approach to diabetes care that is tailored to the needs and circumstances of adults with type 2 diabetes, taking into account their personal preferences. An example of individualised treatment options is to consider the ABCD approach-
Age – less stringent HbA1c targets with decreasing life expectancy.
Body weight. Be aware of which drugs affect body weight – weight neutral – metformin and DPP4i (gliptins), weight gain – insulins, pioglitazone, sulphonylureas, weight loss – SGLT I and GLP1 RAs.
Complications – co-incident complications will impact drug selection e.g. patient with eGFR< 30ml/min/1.73m2 should avoid metformin.
Duration – disease duration is a consideration when setting HbA1c levels. The shorter the disease duration the greater the cardiovascular protection offered by strict glycaemic control. Once disease duration is 10-12 years the beneficial effects of strict glycaemic control may be lost or reversed.
Reassess the person’s needs and circumstances at each review and consider discontinuing any medicines that are not effective.
The table below is based on targets suggested by the American Diabetes Association and the American Geriatrics Society. They suggest the following targets, based on frailty and co-morbidity (Diabetes Care 2012;35:2650). It should be noted that this is for guidance only and has not yet been adopted by NICE. QOF targets are included for comparison.

7
Health status Target HbA1c (adapted from
ADA)
QOF Target
threshold
Target BP Lipid modification for primary prevention
Healthy
Reasonable life expectancy
58 58
140/90 (NICE 2019)
140/80 (QOF)
130/80 if renal disease or stroke
Statins indicated if Qrisk2 score >10%
Moderate Frailty
Several co-morbidities
Limited functional ability
Mild to moderate cognitive impairment
64 Review sulphonylureas and insulin. Avoid hypoglycaemia
75 140/90 (no target set for QOF)
Benefits of statins uncertain
Severe Frailty
End-stage chronic disease
In long-term care/ limited functional ability
Moderate to severe cognitive impairment
70 Review sulphonylureas and insulin. Avoid hypoglycaemia
75 150/90 (no target set for QOF)
Statins not indicated
End of life and palliative care
No Target Avoid symptomatic hyperglycaemia
No target No target Statins not indicated

8
Dapagliflozin can be initiated for heart
failure but not glucose control
Guidance on blood glucose lower therapies in diabetes for those with renal and hepatic disease
[Type a quote from the document or the summary of an interesting point. You can position the text box
DPP-4 INHIBITORS: DIPEPTIDYLPEPTIDASE-4 INHIBITORS (SITAGLIPTIN, SAXAGLIPTIN, LINAGLIPTIN, VILDAGLIPTIN, ALOGLIPTIN)
Inhibits dipeptidylpeptidase-4 to increase insulin secretion and lower glucagon secretion.
Preparation Dose
Dose adjustments
Moderate renal impairment (eGFR= mL/min/1.73 m2)
Severe renal impairment (eGFR= mL/min/1.73 m2)
Hepatic Impairment:
Alogliptin* 25 mg once daily eGFR 30 50:
12.5 mg once daily
eGFR <30: 6.25 mg once daily;
Use with caution
No dose adjustment necessary if mild/moderate impairment. Use with caution Therapeutic experience in severe hepatic impairment is limited and therefore use is not recommended by manufacturer.
Linagliptin 5 mg once daily N/A
Sitagliptin 100 mg once daily eGFR 30 45: 50 mg once daily
eGFR <30: 25 mg once daily
Saxagliptin 5 mg once daily
eGFR <45: 2.5mg once daily
Vildagliptin 50 mg twice daily 50 mg once daily in the morning when used in combination with a sulfonylurea
eGFR <50: 50 mg once daily
Should not be used in people with hepatic impairment
Contraindications: Ketoacidosis
Pregnancy and breast-feeding: Avoid
Cautions: Potentiates the hypoglycaemic effects of insulin and sulfonylureas (see page 32/65) People with a history of pancreatitis.
Class side effects: Headache/dizziness Please see individual drug monograph in the BNF for a complete side-effect profile
Monitoring requirements: Discontinue if symptoms of acute pancreatitis (persistent, severe abdominal pain)
Vildagliptin associated with liver toxicity; seek medical attention if nausea, vomiting, abdominal pain, fatigue, and dark urine develops. Monitor liver enzymes 3 month interval for first year, periodically after.
Additional information: *Alogliptin not licensed for monotherapy
TYPE 2 DIABETES ORAL HYPOGLYCAEMIC AGENTS (2)
THIAZOLIDINEDIONES (PIOGLITAZONE)
Reduces peripheral insulin resistance, leading to a reduction of blood-glucose concentration.
Preparation Dose Dose adjustments
Renal Impairment Hepatic Impairment:
Pioglitazone
Initially 15 30 mg once daily, adjusted according to response up to 45 mg once daily with or without food. Elderly - initiate with lowest possible dose and increase gradually.
No dose adjustment is necessary
Should not be used in people with hepatic impairment (Therapy with pioglitazone should not be initiated if the ALT is > 2.5 times the upper limit of normal or with any other evidence of liver disease.)
Contraindications: Cardiac failure / Hx of cardiac failure (NYHA stages I to IV) hepatic impairment diabetic ketoacidosis current bladder cancer or a history of bladder cancer uninvestigated macroscopic haematuria
Pregnancy and breast-feeding: Avoid
Cautions: Potentiates the hypoglycaemic effects of insulin and sulfonylureas (see page 32/65)
Side effects: Bone fracture (particularly in women); Increased risk of infection; numbness; visual impairment; weight increased
Monitoring requirements: Review treatment after 3 6 months and regularly thereafter
Liver function tests prior to commencing therapy, and periodically thereafter Whilst on pioglitazone, if ALT levels are increased to 3 times upper limit of normal, liver enzyme levels should be reassessed as soon as possible. If ALT levels remain > 3 X the upper limit of normal, therapy should be discontinued Weight
Additional information: Important safety information Please see hyperlinks for more detailed advice
MHRA/CHM advice: Pioglitazone cardiovascular safety (December 2007 and January 2011) People should be informed on the signs and symptoms of DKA, discontinue treatment with the SGLT2 inhibitor immediately if DKA is suspected or diagnosed
Pioglitazone: risk of bladder cancer (July 2011) Pioglitazone should not be used in people with active bladder cancer or a past history of bladder cancer, or in those who have uninvestigated macroscopic haematuria.
Weight gain which may be due to fat accumulation, and in some cases associated with fluid retention. In some cases weight increase may be a symptom of cardiac failure, therefore weight should be closely monitored.
NB: All information presented is in line with the Summaries of Product Characteristics (SPC) of each drug or the BNF.
Date of preparation: October 2020. For review: April 2021 35
DPP-4 INHIBITORS: DIPEPTIDYLPEPTIDASE-4 INHIBITORS (SITAGLIPTIN, SAXAGLIPTIN, LINAGLIPTIN, VILDAGLIPTIN, ALOGLIPTIN)
Inhibits dipeptidylpeptidase-4 to increase insulin secretion and lower glucagon secretion.
Preparation Dose
Dose adjustments
Moderate renal impairment (eGFR= mL/min/1.73 m2)
Severe renal impairment (eGFR= mL/min/1.73 m2)
Hepatic Impairment:
Alogliptin* 25 mg once daily eGFR 30 50:
12.5 mg once daily
eGFR <30: 6.25 mg once daily;
Use with caution
No dose adjustment necessary if mild/moderate impairment. Use with caution Therapeutic experience in severe hepatic impairment is limited and therefore use is not recommended by manufacturer.
Linagliptin 5 mg once daily N/A
Sitagliptin 100 mg once daily eGFR 30 45: 50 mg once daily
eGFR <30: 25 mg once daily
Saxagliptin 5 mg once daily
eGFR <45: 2.5mg once daily
Vildagliptin 50 mg twice daily 50 mg once daily in the morning when used in combination with a sulfonylurea
eGFR <50: 50 mg once daily
Should not be used in people with hepatic impairment
Contraindications: Ketoacidosis
Pregnancy and breast-feeding: Avoid
Cautions: Potentiates the hypoglycaemic effects of insulin and sulfonylureas (see page 32/65) People with a history of pancreatitis.
Class side effects: Headache/dizziness Please see individual drug monograph in the BNF for a complete side-effect profile
Monitoring requirements: Discontinue if symptoms of acute pancreatitis (persistent, severe abdominal pain)
Vildagliptin associated with liver toxicity; seek medical attention if nausea, vomiting, abdominal pain, fatigue, and dark urine develops. Monitor liver enzymes 3 month interval for first year, periodically after.
Additional information: *Alogliptin not licensed for monotherapy
TYPE 2 DIABETES ORAL HYPOGLYCAEMIC AGENTS (2)
THIAZOLIDINEDIONES (PIOGLITAZONE)
Reduces peripheral insulin resistance, leading to a reduction of blood-glucose concentration.
Preparation Dose Dose adjustments
Renal Impairment Hepatic Impairment:
Pioglitazone
Initially 15 30 mg once daily, adjusted according to response up to 45 mg once daily with or without food. Elderly - initiate with lowest possible dose and increase gradually.
No dose adjustment is necessary
Should not be used in people with hepatic impairment (Therapy with pioglitazone should not be initiated if the ALT is > 2.5 times the upper limit of normal or with any other evidence of liver disease.)
Contraindications: Cardiac failure / Hx of cardiac failure (NYHA stages I to IV) hepatic impairment diabetic ketoacidosis current bladder cancer or a history of bladder cancer uninvestigated macroscopic haematuria
Pregnancy and breast-feeding: Avoid
Cautions: Potentiates the hypoglycaemic effects of insulin and sulfonylureas (see page 32/65)
Side effects: Bone fracture (particularly in women); Increased risk of infection; numbness; visual impairment; weight increased
Monitoring requirements: Review treatment after 3 6 months and regularly thereafter
Liver function tests prior to commencing therapy, and periodically thereafter Whilst on pioglitazone, if ALT levels are increased to 3 times upper limit of normal, liver enzyme levels should be reassessed as soon as possible. If ALT levels remain > 3 X the upper limit of normal, therapy should be discontinued Weight
Additional information: Important safety information Please see hyperlinks for more detailed advice
MHRA/CHM advice: Pioglitazone cardiovascular safety (December 2007 and January 2011) People should be informed on the signs and symptoms of DKA, discontinue treatment with the SGLT2 inhibitor immediately if DKA is suspected or diagnosed
Pioglitazone: risk of bladder cancer (July 2011) Pioglitazone should not be used in people with active bladder cancer or a past history of bladder cancer, or in those who have uninvestigated macroscopic haematuria.
Weight gain which may be due to fat accumulation, and in some cases associated with fluid retention. In some cases weight increase may be a symptom of cardiac failure, therefore weight should be closely monitored.
NB: All information presented is in line with the Summaries of Product Characteristics (SPC) of each drug or the BNF.
Date of preparation: October 2020. For review: April 2021 35

9
Information taken from North West London Guide with permission. For review July 2022

10
Information taken from North West London Guide with permission. For review July 2022

11
Information taken from North West London Guide with permission. For review July 2022

12
Information taken from North West London Guide with permission. For review July 2022

13
Information taken from North West London Guide with permission. For review July 2022

14
Abbreviations: T2DM; type 2 diabetes mellitus; eGFR, estimated glomerular filtration rate; SGLT-2i, sodiumglucose cotransporter-2 inhibitor; DPP-4i, dipeptidyl peptidase 4 inhibitor (gliptin); SU, sulfonylurea; TZD, thiazolidinedione; BMI, body mass index; GLP-1RA, glucagon-like peptide-1 receptor agonist; CVD, cardiovascular disease; eCVD, established cardiovascular disease; MI, myocardial infarction; Cana, canagliflozin; Dapa, dapagliflozin; Empa, empagliflozin; HF, heart failure; CKD, chronic kidney disease; HbA1c , haemoglobin A1C; BD, twice daily; ACEi, Angiotensin-converting enzyme inhibitors; ARB, Angiotensin II receptor blocker; NSAID, Non-steroidal anti-inflammatory drug; DKA, diabetic ketoacidosis; uACR, urine albumin creatinine ratio; HFrEF, Heart Failure with reduced Ejection Fraction References:
1. National Institute for Health & Care Excellence. Type 2 diabetes in adults: management https://www.nice.org.uk/guidance/ng28 2. American Diabetes Association, Diabetes Care 2020 Jan; 43(Supplement 1): S98-S110
3. DiRECT; Lancet 2018; 391: 541–51 https://doi.org/10.1016/S0140-6736(17)33102-1 4. FDA Drug Safety Communication: FDA adds warnings about heart failure risk to labels of type 2 diabetes medicines containing saxagliptin
and alogliptin https://bit.ly/2ZZCNni 5. Pioglitazone to be avoided in patients with heart failure. PROactive; Lancet. 2005 Oct 8;366(9493):1279-89 https://doi.org/10.1016/S0140-
6736(05)67528-9 8. REWIND (Dulaglutide CVOT); Lancet 2019; 394: 121–30; DOI: https://doi.org/10.1016/S0140-6736(19)31149-3 6. REWIND (Dulaglutide CVOT); Lancet 2019; 394: 121–30; DOI: https://doi.org/10.1016/S0140-6736(19)31149-3 7. EMPA-REG; N Engl J Med 2015; 373:2117-2128; DOI: https://doi.org/10.1056/NEJMoa1504720 8. CANVAS; N Engl J Med 2017; 377:644-657; DOI: https://doi.org/10.1056/NEJMoa1611925 9. Circulation. 2019 May 28;139(22):2516-2527; DOI: https://doi.org/10.1161/CIRCULATIONAHA.119.039996 10. SUSTAIN 6; N Engl J Med. 2016 Nov 10;375(19):1834-1844 DOI: https://doi.org/10.1056/NEJMoa1607141 11. LEADER; N Engl J Med 2016; 375:311-322; DOI: https://doi.org/10.1056/NEJMoa1603827 12. DAPA HF; September 19, 2019; DOI: https://doi.org/10.1056/NEJMoa1911303 13. CREDENCE; N Engl J Med 2019; 380:2295-2306; DOI: https://doi.org/10.1056/NEJMoa1811744 14. SGLT-2 inhibitors or GLP-1 receptor agonists for adults with type 2 diabetes: a clinical practice guideline ; BMJ 2021
DOI: https://doi.org/10.1136/bmj.n1091 15. North West London, Hounslow CCG. North West London Diabetes Guidelines (hounslowccg.nhs.uk) 16. Management of Type 2 Diabetes in Adults, Medway and Swale CCG, 2019
Authors: Dr Dan Jenkinson (GP Lead, Diabetes Care for You), Hannah Syed (Diabetes Lead Pharmacist, East Sussex Healthcare NHS Trust), Dr Chathanath Binodh (Clinical Lead Diabetes, East Sussex) and Dr Jude Gunasegaram (Clinical Lead Long Term Conditions, West Sussex CCG) with thanks to the North West London Diabetes Clinical Reference Group for permission to use parts of their guideline, and to our Sussex Diabetes Teams for their endorsement and support. Review date July 2022