surviving sepsis
DESCRIPTION
Surviving SepsisTRANSCRIPT

SEPSIS

Sepsis : Definition• Sepsis = SIRS + source of infection• SIRS is defined as two or more of the following variables:
• HR > 90 beats per minute• Temperature < 36°C or > 38°C• Tachypnea > 20 breaths per minute or PaCO2 < 32 mmHg • WBC < 4,000 or > 12,000 cells/mm3 or 10 % immature
neutrophils (Bands)
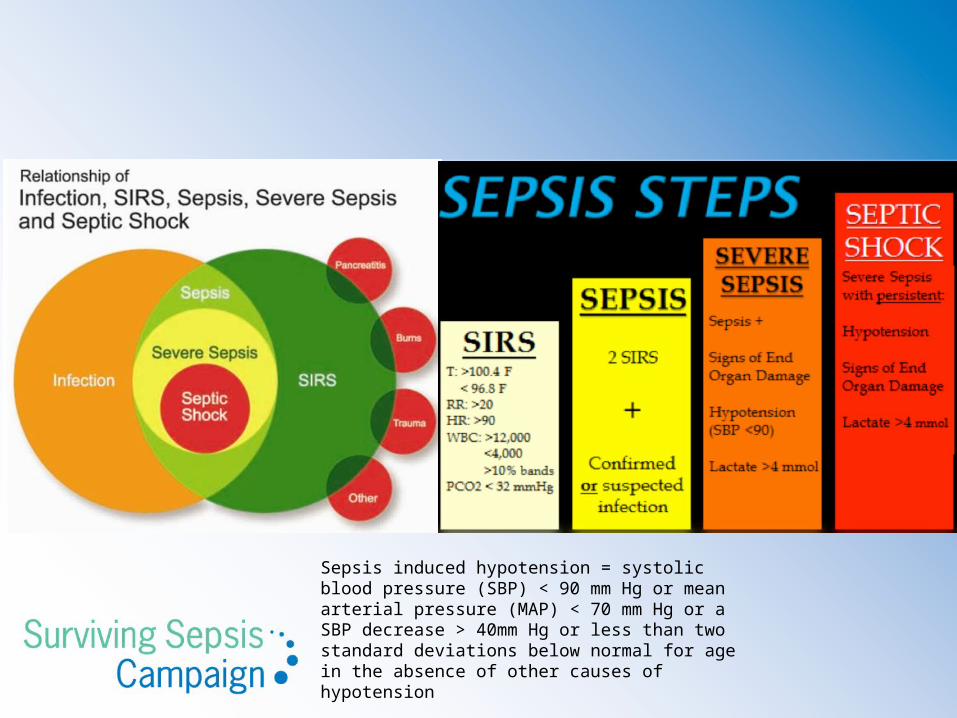
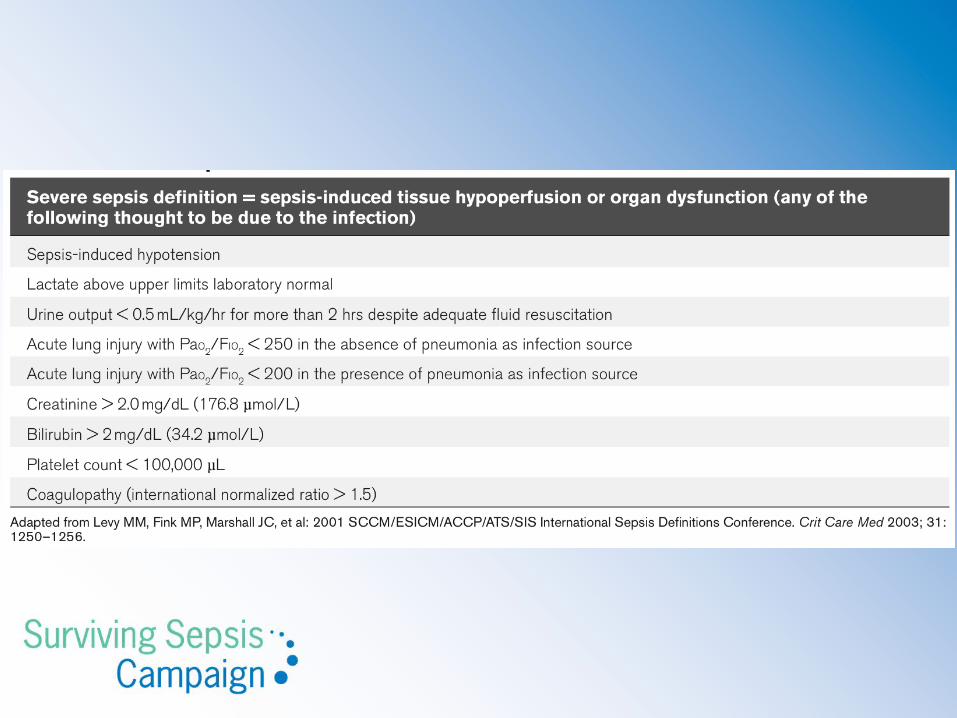
Sepsis induced hypotension = systolic blood pressure (SBP) < 90 mm Hg or mean arterial pressure (MAP) < 70 mm Hg or a SBP decrease > 40mm Hg or less than two standard deviations below normal for age in the absence of other causes of hypotension
Surviving Sepsis
• Severe sepsis and septic shock - leading causes of death among hospitalized patients ~ kills one in four
• Mortality rates attributed to severe sepsis and septic shock are estimated at 25% or greater
• EGDT publication resulted in a 10-12% drop in mortality has been seen nationally over the last decade
Angus DC, Linde-Zwirble WT, Lidicker J, et al. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29:1303–1310.

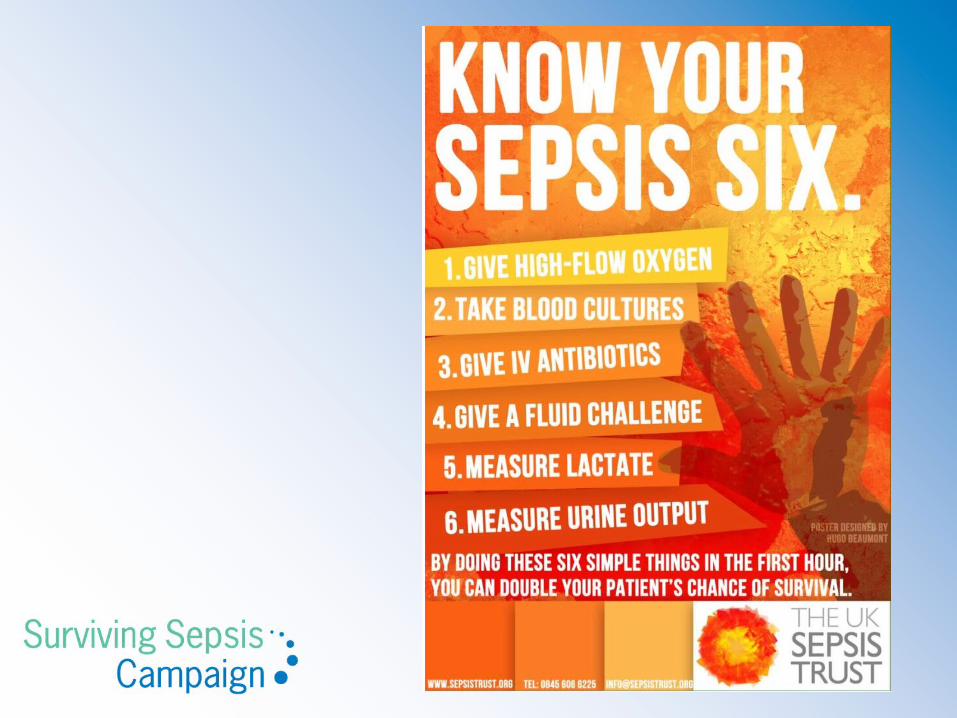
TO BE COMPLETED WITHIN 3 HOURS:
1) Measure lactate level2) Obtain blood cultures prior to administration of antibiotics3) Administer broad spectrum antibiotics4) Administer 30 mL/kg crystalloid for hypotension or lactate 4mmol/L

Goals during the first 6 hrs

Why measure lactate?
• Diagnose severe sepsis with elevated lactate as a diagnosis of tissue hypoperfusion
• Trigger for quantitative resuscitation if lactate is 4 mg/dL or more

• Lactic Acid Can be Tricky...
• during states of low perfusion when there is cellular metabolic failure
• > 2 = severe sepsis; > 4 = tissue hypoxia
• Can be mildly elevated by other conditions:• Cirrhosis,lymphoma,renal failure, ketosis, short gut
syndrome, metformin, nitroprusside, retrovirals

Blood Cultures

Diagnosis• Recommend at least two blood cultures be obtained before antimicrobial therapy is
administered , volume >10ml
• As long as such cultures do not cause significant delay (>45 minutes) in antimicrobial administration,
• With at least one drawn percutaneously and one drawn through each vascular access device, unless the device was recently (<48 hr.) inserted
• Cultures of other sites (preferably quantitative where appropriate), such as urine, cerebrospinal fluid, wounds, respiratory secretions, or other body fluids that may be the source of infection , should also be obtained before antimicrobial therapy if doing so does not cause significant delay in antibiotic administration (grade 1C)

Antibiotic Therapy
• We recommend that intravenous antibiotic therapy be started as early as possible and within the first hour of recognition of septic shock (1B) and severe sepsis without septic shock (1C).
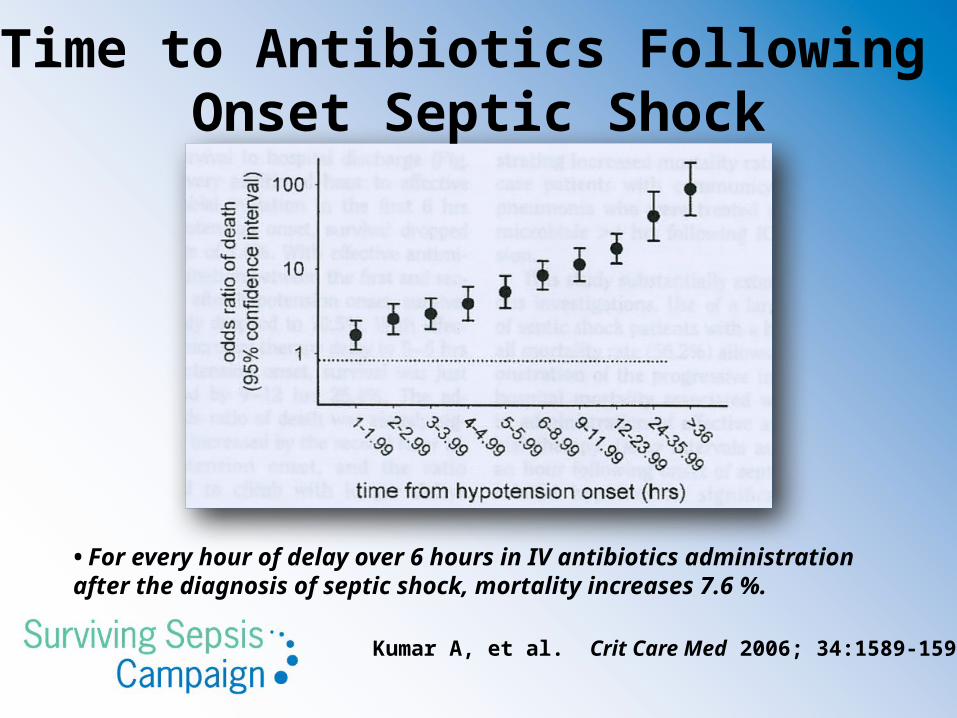
Kumar A, et al. Crit Care Med 2006; 34:1589-1596
Time to Antibiotics Following Onset Septic Shock
• For every hour of delay over 6 hours in IV antibiotics administration after the diagnosis of septic shock, mortality increases 7.6 %.
Antibiotic Therapy• Initial empiric anti-infective therapy – activity against all likely pathogens and
adequate concentrations into suspected or potential sources of infection (1B)
• Reassess antibiotic regimen daily for de-escalation (1B)
• For patients with severe infections associated with respiratory failure and septic shock, combination therapy with an extended spectrum beta-lactam and either an aminoglycoside or a fluoroquinolone is for P. aeruginosa bacteremia (grade 2B).
• A combination of beta-lactam and macrolide for patients with septic shock from bacteremic Streptococcus pneumoniae infections (grade 2B).

• A specific anatomical diagnosis of infection requiring consideration for emergent source control be sought and diagnosed or excluded as rapidly as possible, and intervention be undertaken for source control within the first 12 hr after the diagnosis is made, if feasible (grade 1C).
Source control

Fluid therapy1. Crystalloids (1B)2. Albumin (2C)3. Avoid HES (1B)4. Initial fluid challenge in sepsis-
induced tissue hypoperfusion (hypotension or elevated lactate) with suspicion of hypovolemia to be a minimum of 30ml/kg of crystalloids
5. More rapid administration and greater amounts of fluid, may be needed in some patients (1B)
SURVIVING SEPSIS CAMPAIGN BUNDLES
TO BE COMPLETED WITHIN 6 HOURS:
5) Apply vasopressors (for hypotension that does not respond to initial fluid resuscitation to maintain a mean arterial pressure [MAP] 65 mm Hg)
6) In the event of persistent arterial hypotension despite volume resuscitation (septicshock) or initial lactate ≥ 4 mmol/L (36 mg/dL):- Measure central venous pressure (CVP)*- Measure central venous oxygen saturation (ScvO2)*7) Remeasure lactate if initial lactate was elevated*
*Targets for quantitative resuscitation included in the guidelines are CVP of 8 mm Hg,ScvO2 of 70%, and normalization of lactate

Resuscitation of Sepsis Induced Tissue Hypoperfusion
• Requirement for vasopressors after fluid challenge
• Lactate ≥ 4 mg/dL
• Recommend MAP is 65 mmHg - Grade 1C

Vasopressors
(1) Norepinephrine (1B) - Dopamine increases MAP and cardiac output - increase
in stroke volume and heart rate.
- Norepinephrine increases MAP due to its
vasoconstrictive effects, with little change in heart rate
and less increase in stroke volume compared with
dopamine.
(2) Epinephrine (2B)

Vasopressors
– Dopamine, generally avoided unless• Relative or absolute bradycardia and low risk of tachyarrhythmias (2C)
– Phenylephrine, unless• Norepinephrine associated with serious arrhythmias• Cardiac output is known to be high and blood pressure target difficult to achieve• As salvage therapy
• Dobutaminea) myocardial dysfunction as suggested by elevated cardiac filling pressures and low
cardiac output, or (b) ongoing signs of hypoperfusion despite achieving adequate intravascular volume
and adequate mean arterial pressure

Initial Resuscitation of Sepsis Induced Tissue Hypoperfusion
Recommend Insertion central venous catheterRecommended goals :• Central venous pressure: 8–12 mm Hg
• Higher with altered ventricular compliance or increased intrathoracic pressure
• In mechanically ventilated patients or those with known preexisting decreased ventricular compliance, a higher target CVP of 12 to 15mm Hg should be achieved to account for the impediment in filling
• intravascular volume status and response to fluids, a low CVP generally can be relied upon as supporting positive response to fluid loading
Grade 1C
• The determinants of SvO2 include CO, oxygen demand, hemoglobin, and arterial oxygen saturation
• reflecting the balance between oxygen delivery (DO2) and consumption (VO2).
• Normal SvO2 is 70–75%. • In sepsis SvO2 may be elevated secondary to maldistribution of flow
(blood returning to the venous circulation without opportunity for oxygen transfer)
• recent data showing that lactate clearance in sepsis is non-inferior to continuous ScVO2 monitoring (Jones, JAMA, 2010)
Central venous oxygen saturation (ScvO2) monitoring
• 2015 - ProCESS ProMISe ARISE - 3 trials that do not demonstrate superiority of required use of CVP monitoring and central venous oxygen saturation (ScvO2) in all patients with septic shock
• esp those who have received timely antibiotics and fluid resuscitation compared with controls or in all patients with lactate >4 mmol/L

Lactate Clearance
• In patients with elevated lactate levels as a marker of tissue hypoperfusion we suggest targeting resuscitation to normalize lactate as rapidly as possible (grade 2C).

Other Recommendations
• Glucose control: commence insulin once 2 readings of >180mg/dl
• DVT prophylaxis: should receive daily VTE prophylaxis - LMWH (Grade 1b) & compression stockings / intermittent compression device
• Stress ulcer prophylaxis: H2 blocker or PPI (Grade 1b)
Blood products
• Red blood cell transfusion occur only when hemoglobin concentration decreases to <7.0 g/dL to target a hemoglobin concentration of 7.0 –9.0 g/dL in adults (grade 1B)
• FFP not be used in the absence of bleeding or planned invasive procedures (grade 2D)
• Platelets prophylactically when counts are <10,000/mm3 (10 x 109/L) in the absence of apparent bleeding. (grade 2D)