surgical transgastric debridement of walled off pancreatic necrosis: an option for patients with...
TRANSCRIPT

Surgical transgastric debridement of walled off pancreaticnecrosis: an option for patients with necrotizing pancreatitis
Sujit Kulkarni • Amanda Bogart • James Buxbaum •
Lea Matsuoka • Rick Selby • Dilipkumar Parekh
Received: 25 February 2014 / Accepted: 22 June 2014
� Springer Science+Business Media New York 2014
Abstract
Background Transgastric debridement of walled off
pancreatic necrosis (WOPN) is a surgical treatment option
for patients requiring pancreatic debridement for necro-
tizing pancreatitis. The reported experience with surgical
transgastric pancreatic debridement is limited, however,
the lower incidence of postoperative pancreatic fistulae
with this procedure compared to other options warrants
further evaluation of this technique.
Method Retrospective chart review.
Results Twenty-two patients underwent transgastric
debridement with a cystogastrostomy for clinically symp-
tomatic WOPN from January 1, 2005 to July 31, 2013.
Eight cases were performed laparoscopically and 14 were
performed by an open approach. The mean patient age was
50.9 (50.9 ± 14.5) and the median American Society of
Anesthesiologist score was 3. The most common etiology
for pancreatitis was gallstones and the median time from
attack of pancreatitis to definitive surgical management
was 60 days (range 22–300 days). Median operative time
was 182 min (range 85–327 min) with 100 cc (range
20–500 cc) of blood loss. In seven patients the necrosis
was infected and in 15 patients the necrosis was sterile as
determined by the intraoperative culture of the necrotic
material. The overall significant morbidity (Clavien type 3
or greater) was 13.6 % and the mortality was 0 %. The
incidence of postoperative pancreatic fistula was 0 %. 20
patients (90 %) were symptom free during a median fol-
low-up of 12 months.
Conclusion In selected patients with clinically symp-
tomatic WOPN, surgical transgastric pancreatic debride-
ment appears to be a safe procedure with a low morbidity
and mortality. The low incidence of postoperative pan-
creatic fistulae warrants further evaluation.
Keywords Pancreatic debridement � Walled off
pancreatic necrosis � Necrotizing pancreatitis � Transgastric
debridement
A significant advance in the treatment of necrotizing pan-
creatitis has been the appreciation that delaying surgical
care for 3–4 weeks to allow the pancreatic and peripan-
creatic necrotic material to organize into an area of ‘‘walled
off pancreatic necrosis (WOPN)’’ leads to a substantial
reduction in mortality from the surgery. WOPN, first
described by Connor et al. [1], appears as a heterogeneous
mass with solid and liquid components in a well-formed
wall of fibrous tissue on contrast-enhanced computed
tomography (CT) (Fig. 1). WOPN may cause significant
and life threatening complications such as infection of the
necrosis leading to sepsis, compression of adjacent organs
leading to obstructive jaundice or gastric outlet obstruction
and fistulization or erosion into adjacent organs or vessels
[2]. WOPN may also cause intractable symptoms requiring
treatment such as food intolerance, pain, weight loss, and a
persistent feeling of being unwell [3–6].
S. Kulkarni (&) � L. Matsuoka � R. Selby � D. Parekh
Department of Surgery, Keck School of Medicine, University of
Southern California, 1510 San Pablo Street, Suite 514,
Los Angeles, CA 90033-4612, USA
e-mail: [email protected]
A. Bogart
Keck School of Medicine, University of Southern California,
Los Angeles, CA, USA
J. Buxbaum
Department of Medicine, Keck School of Medicine,
University of Southern California, Los Angeles, CA, USA
123
Surg Endosc
DOI 10.1007/s00464-014-3700-x
and Other Interventional Techniques

Cystogastrostomy is an established treatment option for
the drainage of lesser sac pancreatic pseudocysts [7].
Endoscopic transgastric debridement of pancreatic necrosis
has been reported to be a safe and feasible treatment option
for WOPN [2, 3]. The literature on surgically accessing
WOPN through a transgastric approach is limited. In this
study, we report the largest surgical experience to date
utilizing transgastric access through a cystogastrostomy for
treating WOPN from necrotizing pancreatitis.
Patients and methods
Twenty-two patients with WOPN associated with compli-
cations or intractable symptoms underwent open or
laparoscopic transgastric pancreatic debridement through a
cystogastrostomy from 1/1/2005 and 7/31/2013 at our
institution. Data collection was approved by the University
Institutional Review Board and confidentiality was main-
tained. The selection of laparoscopic versus an open pro-
cedure was at the discretion of the operating surgeon.
Symptoms recorded include persistent abdominal pain
requiring narcotics, inability to tolerate diet, failure to
thrive, repeated hospital admissions for pancreatitis and
persistent feeling of being unwell as described by Rattner
et al. [8]. Patient information collected included age, gen-
der, American Society of Anesthesia (ASA) class, etiology
of necrosis, comorbidities, and prior interventions. Preop-
erative imaging workup included a CT scan and/or mag-
netic resonance imaging (MRI). Operative data collected
included operative time, blood loss, complications, and
cultures. Postoperative data collected included length of
stay, progression of diet, complications, and symptom
resolution (Fig. 2).
Surgical technique
For an open procedure, a small upper midline incision is
performed. An anterior gastrotomy is made where the
WOPN is distorting the stomach. The WOPN cavity is
localized by aspirating the brown or blackish fluid associ-
ated with pancreatic necrosis with an 18 gage needle
through the posterior wall of the stomach. A posterior
gastrotomy is then made with electrocautery to enter the
WOPN cavity and a gastrointestinal stapling device is
utilized to attach the cyst wall to the stomach thereby
establishing a cystogastrostomy and extending the opening
between the stomach and the WOPN cavity. An opening of
approximately 5–10 cm is established between the stomach
and the WOPN cavity. Debridement is achieved using
gentle finger dissection, irrigation, and suction of the
necrotic material. A 30� scope is used to visualize the
cavity and ensure satisfactory debridement and hemostasis.
In hand sewn technique, the posterior stomach wall and
cyst wall are sutured together using 3–0 polypropylene
suture in a continuous manner. The anterior gastrotomy is
then closed.
In the laparoscopic procedure, the abdominal cavity is
entered through a supraumbilical midline incision using
Hasson technique. Two 12 mm ports are placed in the
upper abdomen along the midclavicular lines on the right
and left side. A 5 mm port is placed in the left upper
quadrant. The anterior stomach wall is opened with a
harmonic scalpel. A laparoscopic ultrasound was used to
localize the necrotic area and a laparoscopic needle is used
to aspirate the WOPN cavity. A small posterior gastrotomy
is then performed using hook electrocautery. An endo-
scopic stapler (blue load) is fired to extend the posterior
Fig. 1 CT scan images of pancreatic necrosis
Fig. 2 MRI appearance of pancreatic necrosis (arrow marks solid
component)
Surg Endosc
123

gastrotomy to establish the cystogastrostomy. A bowel-
grasping forceps and suction-irrigator device are used for
debridement. The WOPN cavity is then visualized with the
laparoscope to ensure complete debridement. Necrotic
pancreatic tissue is removed in a plastic bag (Fig. 3).
Hemostasis in the cyst cavity and along the staple line is
ensured. The anterior gastrotomy is closed with an endo-
scopic stapler or 4–0 PDS suture in running fashion. In the
laparoscopic hand-assisted technique, a 5 cm right sub-
costal incision is used for insertion of a Gelport� (Applied
Medical, Rancho Santa Margarita, CA). Two 12 mm ports
are placed in the upper abdomen along the midclavilcular
lines on the right and left side.
Pancreatic fistula
For the purpose of this manuscript, the definition of a
pancreatic fistula followed classification of the Interna-
tional Study Group on Pancreatic Fistula (ISGPF) [9]. If
there is a drain output of any measurable volume of fluid on
or after postoperative day 3 with an amylase level three
times greater than the serum amylase level, then it is
considered as pancreatic fistula. A routine placement of a
drain was avoided both in open or laparoscopic approach.
Preoperatively placed drains are removed at the time of
surgery.
Results
Patient characteristics
The patient characteristics are summarized in Table 1.
Twenty-two patients with WOPN were treated with trans-
gastric debridement through a cystogastrostomy. There
were 13 males and 9 females. The mean patient age was
50.9 (50.9 ± 14.5) and the median ASA score was 3 (range
2–3). Sixteen patients had comorbidities including diabetes
[13], hypertension [5], cirrhosis [1], coronary artery disease
(CAD) [1], and obesity [3]. The cause of pancreatitis was
gallstones in 12, alcoholic in 3, hypertriglyceridemia in 1,
and idiopathic in 6 patients. Eighteen patients did not have
any prior interventions, while two patients had percutane-
ous drains and one patient had endoscopic transgastric
drain. One patient, who underwent prior open debridement
with splenectomy and cholecystectomy, developed a
recurrent peripancreatic fluid collection with necrosis. All
these interventions were performed at the outside hospitals
prior to transfer.
The indications for surgery were based on a prolonged
symptomatic clinical course, which included repeated
readmissions after the developing necrotizing pancreatitis,
persistent feeling of being unwell, abdominal pain, weight
loss and failure to tolerate oral intake. Patients were sur-
gically debrided using the transgastric route at the discre-
tion of the operating surgeon and only patients who did not
have clinical or radiological evidence of infection were
considered. Three out of 22 patients had preoperative organ
failures. Two patients had acute renal failure and acute
respiratory distress syndrome. One patient had renal fail-
ure, respiratory failure, and myocardial infarction. The
majority of the patients had the primary treatment for the
pancreatitis elsewhere and was referred to us afterward.
The median time from attack of pancreatitis to definitive
surgical management was 60 days (range 22–300 days).
Imaging characteristics
CT scan was the most common imaging modality used
(Fig. 1). Two patients had MRI performed because of
contrast allergy (Fig. 2). Median maximal diameter of
WOPN on imaging was 13 cm. Near total necrosis was
seen in seven patients. Left-sided gutter extension of the
necrosis was noted in three patients. Mesenteric extension
along the superior mesenteric vessels was seen in seven
patients. Eight patients had splenic vein thrombosis. Two
out of those eight patients also had portal vein thrombosis
with varices. We were unable to calculate CT severity
index because of lack of availability of initial imaging
studies performed at the outside hospitals.
Perioperative data and outcomes
The perioperative data and outcomes are summarized in
Table 2. Eight out of 22 patients underwent laparoscopic
transgastric debridement and six out of eight laparoscopic
cases were performed totally laparoscopically. Hand-
assisted technique with Gelport� was used in two cases.
Fig. 3 Laparoscopic pancreatic debridement
Surg Endosc
123

Ta
ble
1P
atie
nt
char
acte
rist
ics
Pat
ien
tA
ge
Gen
der
AS
A
clas
s
Eti
olo
gy
Sy
mp
tom
sC
om
orb
idit
ies
Pre
-op
org
an
fail
ure
Pri
or
inte
rven
tio
ns
Tim
eto
surg
ery
(day
s)
Fo
llo
w-u
p
(mo
nth
s)
11
9M
3Id
iop
ath
icP
,IT
PO
,W
LO
bes
ity
No
No
55
6
26
5F
3Id
iop
ath
icP
,IT
PO
,W
LH
TN
No
No
55
10
34
2F
3B
ilia
ryP
,IT
PO
,W
LN
on
eN
oN
o5
61
9
45
2M
3B
ilia
ryP
,IT
PO
,W
LD
MN
oN
o6
01
9
54
5M
2H
yp
er-t
rig
lyce
rid
emia
P,
ITP
O,
WL
DM
No
No
22
20
62
5M
2B
ilia
ryP
,IT
PO
,W
L,
FD
MN
oN
o6
72
0
77
7F
3B
ilia
ryP
,IT
PO
HT
N,
DM
,o
bes
ity
No
Per
cuta
neo
us
dra
in6
81
9
86
2M
2B
ilia
ryP
,IT
PO
,W
LD
MN
oN
o3
81
8
94
9F
2Id
iop
ath
icP
,IT
PO
,W
L,
FD
MN
oP
ercu
tan
eou
sd
rain
37
13
10
37
F2
Idio
pat
hic
P,
ITP
O,
WL
,F
No
ne
No
No
12
01
6
11
57
F2
Bil
iary
P,
ITP
O,
WL
,F
DM
No
No
53
14
12
39
M3
Bil
iary
P,
ITP
O,
WL
No
ne
No
Pan
crea
tic
deb
rid
emen
t6
01
2
13
52
F2
Bil
iary
P,
ITP
O,
WL
No
ne
No
No
30
14
14
43
M3
Alc
oh
ol
P,
ITP
O,
WL
DM
No
No
30
01
2
15
63
M3
Alc
oh
ol
P,
ITP
O,
FH
TN
,D
MN
oN
o3
86
16
50
F3
Bil
iary
P,
ITP
O,
FD
MY
esN
o7
11
2
17
44
M2
Alc
oh
ol
P,
ITP
O,
WL
,F
Cir
rho
sis
No
No
27
06
18
57
M3
Bil
iary
P,
ITP
O,
WL
DM
No
No
73
7
19
71
M3
Idio
pat
hic
P,
ITP
O,
WL
No
ne
No
No
46
6
20
43
M3
Idio
pat
hic
P,
ITP
O,
WL
,F
DM
,H
TN
,o
bes
ity
Yes
Yes
76
4
21
55
M2
Bil
iary
P,
ITP
ON
on
eN
oN
o6
02
22
72
F3
Bil
iary
P,
ITP
O,
WL
DM
,H
TN
,C
AD
Yes
Yes
75
2
Pp
ain
,IT
PO
inab
ilit
yto
tole
rate
per
ora
lin
tak
e,W
Lw
eig
ht
loss
,F
fev
er,
DM
dia
bet
esm
elli
tus,
HT
Nh
yp
erte
nsi
on
Surg Endosc
123
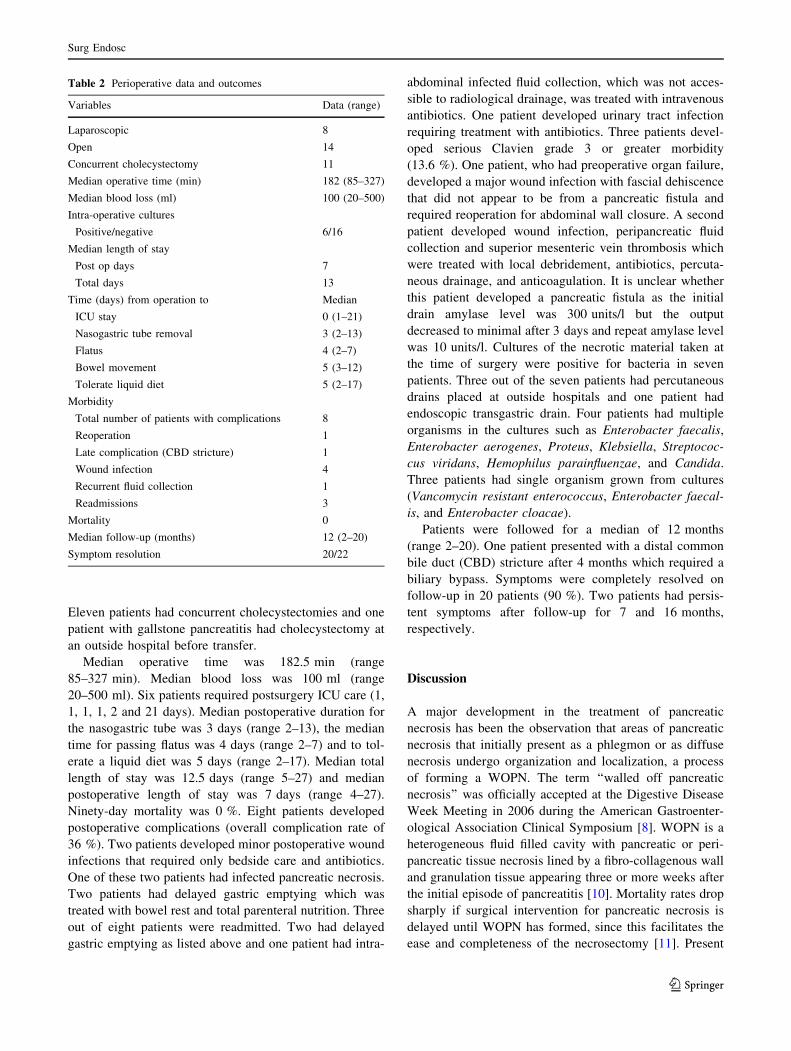
Eleven patients had concurrent cholecystectomies and one
patient with gallstone pancreatitis had cholecystectomy at
an outside hospital before transfer.
Median operative time was 182.5 min (range
85–327 min). Median blood loss was 100 ml (range
20–500 ml). Six patients required postsurgery ICU care (1,
1, 1, 1, 2 and 21 days). Median postoperative duration for
the nasogastric tube was 3 days (range 2–13), the median
time for passing flatus was 4 days (range 2–7) and to tol-
erate a liquid diet was 5 days (range 2–17). Median total
length of stay was 12.5 days (range 5–27) and median
postoperative length of stay was 7 days (range 4–27).
Ninety-day mortality was 0 %. Eight patients developed
postoperative complications (overall complication rate of
36 %). Two patients developed minor postoperative wound
infections that required only bedside care and antibiotics.
One of these two patients had infected pancreatic necrosis.
Two patients had delayed gastric emptying which was
treated with bowel rest and total parenteral nutrition. Three
out of eight patients were readmitted. Two had delayed
gastric emptying as listed above and one patient had intra-
abdominal infected fluid collection, which was not acces-
sible to radiological drainage, was treated with intravenous
antibiotics. One patient developed urinary tract infection
requiring treatment with antibiotics. Three patients devel-
oped serious Clavien grade 3 or greater morbidity
(13.6 %). One patient, who had preoperative organ failure,
developed a major wound infection with fascial dehiscence
that did not appear to be from a pancreatic fistula and
required reoperation for abdominal wall closure. A second
patient developed wound infection, peripancreatic fluid
collection and superior mesenteric vein thrombosis which
were treated with local debridement, antibiotics, percuta-
neous drainage, and anticoagulation. It is unclear whether
this patient developed a pancreatic fistula as the initial
drain amylase level was 300 units/l but the output
decreased to minimal after 3 days and repeat amylase level
was 10 units/l. Cultures of the necrotic material taken at
the time of surgery were positive for bacteria in seven
patients. Three out of the seven patients had percutaneous
drains placed at outside hospitals and one patient had
endoscopic transgastric drain. Four patients had multiple
organisms in the cultures such as Enterobacter faecalis,
Enterobacter aerogenes, Proteus, Klebsiella, Streptococ-
cus viridans, Hemophilus parainfluenzae, and Candida.
Three patients had single organism grown from cultures
(Vancomycin resistant enterococcus, Enterobacter faecal-
is, and Enterobacter cloacae).
Patients were followed for a median of 12 months
(range 2–20). One patient presented with a distal common
bile duct (CBD) stricture after 4 months which required a
biliary bypass. Symptoms were completely resolved on
follow-up in 20 patients (90 %). Two patients had persis-
tent symptoms after follow-up for 7 and 16 months,
respectively.
Discussion
A major development in the treatment of pancreatic
necrosis has been the observation that areas of pancreatic
necrosis that initially present as a phlegmon or as diffuse
necrosis undergo organization and localization, a process
of forming a WOPN. The term ‘‘walled off pancreatic
necrosis’’ was officially accepted at the Digestive Disease
Week Meeting in 2006 during the American Gastroenter-
ological Association Clinical Symposium [8]. WOPN is a
heterogeneous fluid filled cavity with pancreatic or peri-
pancreatic tissue necrosis lined by a fibro-collagenous wall
and granulation tissue appearing three or more weeks after
the initial episode of pancreatitis [10]. Mortality rates drop
sharply if surgical intervention for pancreatic necrosis is
delayed until WOPN has formed, since this facilitates the
ease and completeness of the necrosectomy [11]. Present
Table 2 Perioperative data and outcomes
Variables Data (range)
Laparoscopic 8
Open 14
Concurrent cholecystectomy 11
Median operative time (min) 182 (85–327)
Median blood loss (ml) 100 (20–500)
Intra-operative cultures
Positive/negative 6/16
Median length of stay
Post op days 7
Total days 13
Time (days) from operation to Median
ICU stay 0 (1–21)
Nasogastric tube removal 3 (2–13)
Flatus 4 (2–7)
Bowel movement 5 (3–12)
Tolerate liquid diet 5 (2–17)
Morbidity
Total number of patients with complications 8
Reoperation 1
Late complication (CBD stricture) 1
Wound infection 4
Recurrent fluid collection 1
Readmissions 3
Mortality 0
Median follow-up (months) 12 (2–20)
Symptom resolution 20/22
Surg Endosc
123

surgical practice strongly recommends against any inter-
vention until there is evidence of WOPN on imaging
studies.
Surgical transgastric debridement is a novel approach to
treatment of pancreatic necrosis and is feasible only in the
presence of WOPN. The present is the largest study
reported to date of transgastric surgical pancreatic
debridement. Our study suggests that this technique is safe
as our overall mortality was 0 % and significant morbidity
(Clavien grade 3 or higher) was 18 %. Symptoms were
resolved in 90 % of patients with long-term follow-up and
only one patient required a second surgical procedure
(4.5 %). Two small previously reported studies mirror our
outcomes with surgical transgastric approach for pancreatic
debridement. Munene et al. have reported their experience
on open transgastric debridement through a cystogastros-
tomy in 10 symptomatic non-infected WOPN patients with
a morbidity of 30 % and a mortality of 0 % [12] and Bo-
land et al. reported eight patients with 0 % mortality and
12 % morbidity [13]. Surgical transgastric debridement
based on this limited experience warrants further evalua-
tion as the procedure is associated with a low morbidity
and mortality.
Transgastric pancreatic debridement was first pioneered
by gastroenterologists who developed per oral endoscopic
debridement techniques that create an opening between the
posterior gastric wall and the WOPN cavity often with the
assistance of endoscopic ultrasound (EUS) guidance [3, 8,
10]. Endoscopic transgastric debridement requires multiple
endoscopic procedures under prolonged anesthesia with a
median of 3–6 procedures/patient. The reported mortality
of endoscopic transgastric debridement is up to 20 % and
complications occur in 15–26 % of patients, including
perforation, peritonitis, bleeding and air embolism,
requiring additional treatments with angiography or sur-
gery [3, 10, 11]. Endoscopic transgastric necrosectomy
using metal stents have been reported but the experience is
very limited [14]. Endoscopic necrosectomy is time con-
suming and complex procedure that requires specialized
advanced endoscopic expertise in endoscopic retrograde
cholagiopancreatography, EUS, endoscopic devices, and
accessories used for necrosectomy. The feasibility of
endoscopic necrosectomy outside of a few highly special-
ized pioneering pancreatic endoscopic centers is unclear.
Comparatively, surgical transgastric debridement does not
require specialized equipment, appear to be safe in the
hands of an experienced pancreatic surgeon and the sur-
gical technique is well established as it is similar to
approaches for lesser sac pseudocyst. Further studies
comparing endoscopic and surgical transgastric debride-
ment are necessary.
The major advantage of transgastric debridement is the
near absence of a posttreatment pancreatic fistula.
Disconnected pancreatic duct syndrome after severe nec-
rotizing pancreatitis is a known entity where the pancreatic
body or tail is often disconnected from rest of the gland due
to necrosis [15]. The separated pancreatic gland will con-
tinue to secrete pancreatic juices and this leads to the
development of a persistent pancreatic fistula in up to 70 %
of patients that often takes months to resolve following
transabdominal and retroperitoneal debridement [10, 16–
18]. None of our patients developed an external pancreatic
fistula after the surgery. The reported incidence of pan-
creatic fistulae is 3.7 % in endoscopic studies after per oral
transgastric pancreatic necrosectomy [8] and in the two
prior surgical studies an incidence of 12 % [12] and 0 %
[13] of pancreatic fistulae was reported.
The traditional treatment for pancreatic necrosis has
been open surgical debridement; however, a median
mortality rate of 25 % (range of from 6 to 56 %) has been
reported for open surgical debridement [3–6]. In the post
WOPN era, the emphasis has shifted to minimally invasive
treatment approaches such as video-assisted retroperito-
neal debridement (VARD) and laparoscopic trans-abdom-
inal or transgastric debridement. VARD has been the most
widely reported surgical minimally invasive surgical pro-
cedure for pancreatic debridement; however, this proce-
dure is feasible as the primary treatment in only 40–50 %
of eligible patients according to recently reported phase II
single arm multicenter study by Horvath et al. [19]. Forty
patients were evaluated with infected pancreatic necrosis
with the step-up approach and 31 patients required sur-
gery. VARD was initially possible in 25 of the 31 patients;
however, of this group an additional 10 (40 %) required
further open surgery because of the failure to drain cen-
trally located collections that were not accessible by
VARD. Therefore, only 15 (48 %) of the eligible 31 sur-
gical patients were treated primarily by VARD. Van
Santvoort et al. reported the results of a randomized con-
trolled trial comparing open necrosectomy to the step-up
approach with VARD [20]. Twenty-four patients in this
study underwent VARD and in 14 of 24 patients (58 %)
further surgical procedures were necessary to address
residual areas of necrosis or complications associated with
VARD. The overall morbidity of VARD treated patients
was 36 % and 30 days mortality 0 % in Horvath study
[19]. The pancreatic fistula rate was 20 %. The experience
with laparoscopic transabdominal debridement is more
limited. We have reported the largest experience of lapa-
roscopic pancreatic necrosectomy. In 56 consecutive sur-
gically treated patients with pancreatic debridement 49
patients were approached laparoscopically and the proce-
dure was completed laparoscopically in 47 patients. The
overall incidence of serious postoperative complications
was 35 % with the majority of the complications being
non-life threatening (Clavien grade 3 in 27 %, grade 4 in
Surg Endosc
123

4.2 % and grade 5 in 4.2 %) and the mortality rate was
6 % [21, 22]. In this study, eight patients underwent lap-
aroscopic transgastric debridement with 0 % mortality and
18 % morbidity suggesting that it is a safe procedure.
These studies support the trend toward minimally invasive
approaches as the published results suggest that minimally
invasive approaches are safe with low morbidity and
mortality compared to that previously reported for open
surgery. A prolonged close follow-up is necessary for
these patients. These patients are at risk of postoperative
complications such as incisional hernia, infection, reoper-
ation, and bleeding. Other issues such as failure to thrive,
poor oral intake, persistent pain, addiction to pain medi-
cations, repeated hospital admissions, pancreatic insuffi-
ciency (exocrine as well as endocrine), anemia, need for
rehabilitation and feeling of being unwell may prolong for
months after the surgery.
There are important limitations of this study. Our sam-
ple size is small and the patients in this study were highly
selected as shown by the fact that only three patients had
organ failure and none of the patients included in this study
had evidence of clinical sepsis or radiological sign of
infection such as presence of air bubbles at the time of
surgery. We were particularly worried about including
patients with evidence of infected pancreatic necrosis in
this study due to the concern over the effect of persistent
postoperative sepsis the gastric suture line. The cultured
necrosis did showed evidence of infection in seven patients
who did not have any preoperative clinical evidence of
invasive sepsis. In none of these patients any dehiscence of
the gastric suture line was seen. Our study suggests that
transgastric debridement through a cystogastrostomy is a
safe procedure in selected group of patients with clinically
symptomatic but non-infected WOPN with a low morbid-
ity, short length of stay and low incidence of postoperative
pancreaticocutaneous fistulae. The application of this
technique to a wider population of patients requiring pan-
creatic debridement is unclear and further experience is
necessary to assess the feasibility of this technique in
subgroups of patients who were excluded from this study in
particular patients with a large burden of necrotic tissue
extending into the retroperitoneal or periduodenal spaces,
presence of multiple organ failure and critically ill patients
with severe sepsis. The markedly lower incidence of pan-
creatic fistulae after transgastric debridement makes this
approach attractive compared to other surgical treatment
options for pancreatic debridement and warrants further
evaluation.
Acknowledgements Grants/Financial support: none
Disclosure Drs. Kulkarni, Boagart, Matsuoka, Buxbaum, Selby and
Parekh have no conflicts of interests or financial ties to disclose.
References
1. Connor S, Raraty MG, Howes N, Evans J, Ghaneh P, Sutton R,
Neoptolemos JP (2005) Surgery in the treatment of acute pan-
creatitis—minimal access pancreatic necrosectomy. Scand J Surg
94:135–142
2. Gluck M, Ross A, Irani S, Lin O, Hauptmann E, Siegal J, Fotoohi
M, Crane R, Robinson D, Kozarek RA (2010) Endoscopic and
percutaneous drainage of symptomatic walled-off pancreatic
necrosis reduces hospital stay and radiographic resources. Clin
Gastroenterol Hepatol 8:1083–1088
3. Stamatakos M, Stefanaki C, Kontzoglou K, Stergiopoulos S,
Giannopoulos G, Safioleas M (2010) Walled-off pancreatic
necrosis. World J Gastroenterol 16(14):1707–1712
4. Babu BI, Siriwardena AK (2009) Current status of minimally
invasive necrosectomy of post-inflammatory pancreatic necrosis.
HPB 11:96–102
5. Babu BI, Sheen AJ, Lee SH, O’Shea S, Eddleston JM, Siriwar-
dena AK (2010) Open pancreatic necrosectomy in the multidis-
ciplinary management of postinflammatory necrosis. Ann Surg
251(5):783–786
6. Rodriguez JR, Razo O, Targarona J, Thaver SP, Rattner DW,
Warshaw AL, Fernandez-del Castillo C (2008) Debridement and
closed packing for sterile or infected necrotizing pancreatitis:
insights into indications and outcomes in 167 patients. Ann Surg
247:294–299
7. Palanivelu C, Senthilkumar K, Madhankumar M, Rajan PS,
Shetty AR, Jani K, Rangarajan M, Maheshkumaar GS (2007)
Management of pancreatic pseudocyst in the era of laparoscopic
surgery—experience from a tertiary center. Surg Endosc
21:2262–2267
8. Papachristou GI, Takahashi N, Chahal P, Sarr MG, Baron TH
(2007) Peroral endoscopic drainage/debridement of walled off
pancreatic necrosis. Ann Surg 245:943–951
9. Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J,
Neoptolemos J, Sarr M, Traverso W, Buchler M (2005) Postop-
erative pancreatic fistula: an international study group (ISGPF)
definition. Surgery 138(1):8–13
10. Frey CF (1993) Management of necrotizing pancreatitis. West J
Med 159:675–680
11. Buchler MW, Gloor B, Muller CA, Friess H, Seiler CA, Uhl W
(2000) Acute necrotizing pancreatitis: treatment strategy
according to the status of infection. Ann Surg 232:619–626
12. Munene G, Dixon E, Sutherland F (2011) Open transgastric
debridement and internal drainage of symptomatic non-infected
walled-off pancreatic necrosis. HPB 13:234–239
13. Boland B, Colquhoun S, Menon V, Kim A, Lo S, Nissen NN
(2010) Current surgical management of infected pancreatic
necrosis. Am Surg 76:1096–1099
14. Hritz I, Fejes R, Szekely A, Szekely I, Horvath L, Sarkany A,
Altorjay A, Madacsy L (2013) Endoscopic transluminal pancre-
atic necrosectomy using a self-expanding metal stent and high-
flow water-jet system. World J Gastroenterol 19(23):3685–3692
15. Sandrasegaran K, Tann M, Jennings SG, Maglinte DD, Peter SD,
Sherman S, Howard TJ (2007) Disconnection of the pancreatic
duct: an important but overlooked complication of severe acute
pancreatitis. Radiographics 27:1389–1400
16. Fernandez-del Castillo C, Rattner DW, Makary MA, Mostafavi
A, McGrath D, Warshaw AL (1998) Debridement and closed
packing for the treatment of necrotizing pancreatitis. Ann Surg
228:676–684
17. Van Santvoort HC, Besselink MG, Horvath KD, Sinanan MH,
Bollen TL, Van Ramshorst B, Gooszen HG, Dutch Acute Pan-
creatitis Study Group (2007) Videoscopic assisted retroperitoneal
Surg Endosc
123

debridement in infected necrotizing pancreatitis. HPB 9:
156–159
18. Parekh D (2006) Laparoscopic assisted pancreatic necrosectomy:
a new surgical option for treatment of severe necrotizing pan-
creatitis. Arch Surg 141:895–903
19. Horvath K, Freeny P, Escallon J, Heagerty P, Comstock B,
Glickerman DJ, Bulger E, Sinanan M, Langdale L, Kolokythas O,
Andrews RT (2010) Safety and efficacy of video- assisted ret-
roperitoneal debridement for infected pancreatic collections: a
multicenter, prospective, single-arm phase 2 study. Arch Surg
145(9):817–825
20. Van Santvoort HC, Besselink MG, Bakker OJ, Hofker HS, Bo-
ermeester MA, Dejong CH, Van Goor H, Schaapherder AF, van
Eijck CH, Bollen TL, van Ramshorst B, Nieuwenhuijs VB,
Timmer R, Lameris JS, Kruyt PM, Manusama ER, van der Harst
E, Van der Schelling GP, Karsten T, Hesselink EJ, van Laarhoven
CJ, Rosman C, Bosscha K, de Wit RJ, Houdijk AP, van Leeuwen
MS, Buskens E, Gooszen HG, Dutch Pancreatitis Study Group
(2010) A step-up approach or open necrosectomy for necrotizing
pancreatitis. N Engl J Med 362:1491–1502
21. Kulkarni S, Selby R, Boswell W, Matsuoka L, Parekh D (2011)
Laparoscopic assisted transabdominal pancreatic debridement: a
safe and effective treatment option for necrotizing pancreatitis.
Gastroenterology 140:S383
22. Matsuoka L, Parekh D (2012) The minimally invasive approach
to surgical management of pancreatic diseases. Gastroenterol
Clin N Am 41:77–101
Surg Endosc
123